Guidelinecontent/pdf...Compliance with this Guideline is recommended Page 1 of 15 Guideline Neonatal...
15
Compliance with this Guideline is recommended Page 1 of 15 Guideline Neonatal anthropometry – measurement and reporting of newborn size and growth Document No: RPAH_GL(2020)_ Number(xxxxxxx) Functional Sub-Group: Clinical Governance Corporate Governance Summary: Brief summary of guideline National Standard: Author: Clinical Associate Professor David Osborn Approved by: Must be tier 2 position nominee (state specific title) and / or relevant committee Publication (Issue) Date: Next Review Date: Replaces Existing Guideline: Previous Review Dates:
Transcript of Guidelinecontent/pdf...Compliance with this Guideline is recommended Page 1 of 15 Guideline Neonatal...
-
Compliance with this Guideline is recommended Page 1 of 15
Guideline
Neonatal anthropometry – measurement and reporting of newborn size and growth
Document No: RPAH_GL(2020)_ Number(xxxxxxx) Functional Sub-Group: Clinical Governance
Corporate Governance Summary: Brief summary of guideline National Standard: Author: Clinical Associate Professor David Osborn Approved by: Must be tier 2 position nominee (state specific title) and / or
relevant committee Publication (Issue) Date: Next Review Date: Replaces Existing Guideline: Previous Review Dates:
-
Compliance with this Guideline is recommended Page 2 of 15
Neonatal anthropometry – measurement and reporting of newborn size and growth
CONTENTS 1. Introduction ........................................................................................................... 3
2. Statement ............................................................................................................. 3
3. Principles / Guidelines .......................................................................................... 4
4. Definitions ............................................................................................................. 4
5. Growth charts ....................................................................................................... 6
6. Anthropometry ...................................................................................................... 8
7. Reporting ............................................................................................................ 10
8. Performance Measures ...................................................................................... 11
9. Summary of practice guidelines ......................................................................... 11
10. definitions......................................................................................................... 11
11. References and links ....................................................................................... 12
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 3 of 15
Neonatal anthropometry – measurement of newborn size and growth 1. INTRODUCTION
The risks addressed by this guideline:
Preterm infants and neonates are more vulnerable to nutritional deficits than any other time of the life cycle.
The aims / expected outcome of this guideline:
Indicators are required to diagnose and document growth disorders as well malnutrition related to undernutrition in preterm and newborn populations.
2. STATEMENT
All newborn infants should have size at birth and subsequent growth measured to document normal size and growth, and to diagnose and document disorders of growth and nutrition. Size and growth should be recorded on an appropriate validated growth chart.
Routine anthropometry:
Size at birth: All infants should have weight, length and head circumference measured at birth as current charts reflect measurements taken in the first 24 hours after birth 1, 2.
Routine monitoring:
All infants should have weight measured at birth and day 3 if stable, then 2nd daily till discharge. o Weight should be assessed using a calibrated electronic scale with 10 g resolution and
tared to zero.
All infants should have length measured at birth, 28 days, 36 weeks postmenstrual age, discharge from admitting hospital and discharge to home.
o The Premie Stadiometer 26-50 cm is preferred for measurement of premature infants including within the incubator.
o The Newborn Stadiometer 35-70 cm is preferred for measurement of term infants.
All infants should have head circumference measured at birth and every 7 days to discharge. o Use a non-stretchable, disposable paper 1–2 cm wide marked in 0.1 cm increments. o To measure the head circumference, securely wrap the tape measure around the widest
possible circumference of the infant’s head (typically 1 to 2 finger-widths above the eyebrow (supraorbital ridges) on the forehead, above the ears, to the most prominent part of the back of the head (occiput). Repeat the measurement three times and select the largest measurement to the nearest 0.1 cm
Document in PowerChart. Use the Fenton Chart to monitor growth to 42 weeks (postmenstrual age) PMA and the WHO chart for term infants and preterm infants after 42 weeks PMA.
Audit (NICUS and ANZNN):
Growth: All infants should have weight, length and head circumference measured at the following intervals:
28 days
At 36 weeks postmenstrual age
At discharge from admitting hospital
At discharge to home.
Criteria for review
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 4 of 15
Weight: Average weight gain for infants 10% weight loss day 3 should have a lactation / feeding consult.
Term or late preterm infants with >12% weight loss day 3 or 10% on day 5 should have a medical review. 4
Term or late preterm infants with
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 5 of 15
The definition of SGA requires 12:
1. Accurate knowledge of gestational age (ideally based on first trimester ultrasound exam), 2. Accurate measurements at birth of weight, length, and head circumference, and 3. A cutoff against reference data from a relevant population. This cutoff has been variably set at
the 10th centile, 3rd centile, or > 2 standard deviations below the mean (~2nd centile).
Babies can then be subclassified into SGA for weight, SGA for length, or SGA for both weight and length. Additionally, those SGA babies who have small head circumference should be recognized.
Infants born small for gestational age are defined by the WHO Expert Committee 13 and the American College of Obstetrics and Gynecology 14 as those weighing below the 10th centile of birth weight by sex for a specific completed gestational age of a given reference population, which identifies infants at increased risk of perinatal morbidities 15. In low and middle income countries, infants born SGA defined as weight < 10th centile are at increased risk of mortality 15.
A Pediatric Endocrine Consensus recommended SGA be defined as weight and/or length more than 2 standard deviations below the mean as this identifies the majority of those in whom ongoing growth assessment is required 12.
Postnatal growth failure (extrauterine growth restriction - EUGR) and failure to thrive
Underweight at a given gestational age may result from stunting or wasting, or both phenotypes 6:
Wasting: low weight for length, or low body mass index [BMI] for age, often reflecting recent weight loss.
Stunting: short length for age, reflecting linear growth restriction.
Postnatal growth failure is commonly considered as weigh 90th centile compared with the size of infants of the same gestation at the time of birth 16. However, this cutoff is physiologically arbitrary, based on statistics rather than health status, and does not assess whether the infants are large relative to their individual genetic potential. Being born LGA (birth weight >90th centile) is a risk factor for prolonged first stage of labour, shoulder dystocia, caesarean, hypoglycaemia and jaundice 19.
The term macrosomia is used to describe an individual who is considerably larger than average. Fetal macrosomia is defined as birth weight >4000 g (or 4500 g) and is associated with maternal and fetal complications including maternal birth canal trauma, shoulder dystocia, and perinatal asphyxia 20, 21.
Constitutional (large parents), diabetes in pregnancy 19 and genetic syndromes 22 are causes of LGA and macrosomic infants.
Microcephaly
Microcephaly is usually defined by the measurement of occipitofrontal circumference (head circumference) that is more than 2 standard deviations below the mean for age and sex or < 3rd
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 6 of 15
centile for age and sex 23. Severe microcephaly is defined as head circumference > 3 standard deviations below the mean for age and sex 23.
Macrocephaly
Macrocephaly is defined as an abnormally large head with an occipitofrontal circumference greater than 2 standard deviations above the mean for a given age and sex 24, 25.
Short stature
Short stature is defined as length or height more than 2 standard deviations below the mean for a given age and sex 26, which corresponds to approximately 2.3% of the population and usually includes healthy individuals 27. Stricter classifications define short stature as heights 2.5 to 3 standard deviations less than the given population’s mean height, which represents 0.6 and 0.1% of the general population respectively 28 and is frequently associated with syndromic conditions 27.
Tall stature
Tall stature is defined as length or height more than 2 standard deviations above the mean for a given age and sex 29. Tall stature can also be defined relative to the target height, with height >2 standard deviations above the target height being considered tall. Ideally, both parents should be measured to calculate the target height 29. Tall stature is usually not a pathological condition and generally does not need treatment.
5. GROWTH CHARTS
Current reference growth curves include Fenton 2013 30, Olsen 2010 31, INTERGROWTH 2015 32, and World Health Organization Growth Standard (WHOGS) 2006 33, 34.
The Fenton 30, 35 size at birth and growth curves were created from 6 large population-based surveys of size at preterm birth representing 3986456 births (34639 births < 30 weeks) from Germany, United States, Italy, Australia, Scotland, and Canada. Smoothed growth chart curves were developed, while ensuring close agreement with the data between 24 and 36 weeks and at 50 weeks.
The Olsen 31 growth curves are gender-specific weight-, length-, and head circumference-for-age curves created from a USA hospital cohort of 257855 singleton infants born 1998 to 2006 aged 22 to 42 weeks at birth who survived to discharge 31.
The INTERGROWTH-21 Project 32 assessed fetal, newborn, and postnatal growth in 8 geographically defined populations from 2009 to 2013, in which maternal health care and nutritional needs were met. From these populations, low-risk women starting antenatal care before 14 weeks' gestation were selected and fetal growth monitored by ultrasonography. Preterm postnatal growth standards were selected from live singletons born between 26 and before 37 weeks' gestation without congenital malformations, fetal growth restriction, or severe postnatal morbidity. Only 408 infants born
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 7 of 15
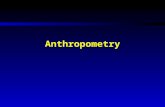
INTERGROWTH postnatal growth charts are based on limited data before 36 weeks so are also less precise and markedly deviate from the Fenton and Olsen curves, especially for weight g/kg/day and length less than 33 weeks (see figure below from ref: 3).
Figure: Weekly median growth velocity of common preterm growth references (Fenton 2013 30, Olsen 2010 31, INTERGROWTH 2015 32, and World Health Organization Growth Standard (WHOGS) 2006 33, 34) in g/kg/day using a constant gain of 15 g/kg/day superimposed. 3
For very preterm infants, INTERGROWTH reference and the Fenton charts ascribe SGA and extrauterine growth restriction differently 3, 37, 38. Several studies have now compared the performance of the INTERGROWTH reference and the Fenton charts for SGA or non-AGA status (SGA or LGA) for detection of neonatal morbidity 37, 38, 39, but none has compared the performance of the various charts in detecting extrauterine growth restriction (EUGR).
In the largest cohort to date in 45505 infants born 33 to 40 weeks gestation, the diagnostic test properties of various charts (WHO, INTERGROWTH, Fenton and GROW) for non-AGA status (SGA or LGA) for composite neonatal morbidity was compared. Similar sensitivity, specificity, positive likelihood ratio, positive predictive value and negative predictive values were reported for the various charts (see table). 39
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 8 of 15
Table: Diagnostic test properties of various charts (WHO, INTERGROWTH, Fenton and GROW) for non-AGA status (SGA or LGA) for composite neonatal morbidity.
In a cohort of 248 infants born
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 9 of 15
At discharge to home.
How to measure weight? 41
For birth weight the infant should be weighed within 24 hours of birth. Weight should be assessed using a calibrated electronic scale with 10 g resolution and tared to zero. The infant should be bare weighed. Any materials on the infant at the time of weighing should be weighed separately and subtracted from the total weight. How to measure length? 42
The Premie Stadiometer 26-50 cm is preferred for measurement of premature infants including within the incubator; whilst the Newborn Stadiometer 35-70 cm is preferred for measurement of term infants [https://www.ellardinstrumentation.com/stadiometers/].
The length-board measurement infantometer has been shown to be the most reliable and accurate measurement of neonatal length. The infantometer should be placed on a flat stable surface.
A rigid infantometer with an offset reading is preferred. For newborns either the ‘two leg’ or ‘one leg’ method may be used 43, 44. For infants, the ‘two leg’ method has greater accuracy 43.
The Neorule may be used as an alternative method 45.
he neonate is placed supine and unclothed on the board and held gently with his or her body aligned and head in a neutral position.
One person stands at the top of the length board and holds the baby’s head in contact with the headboard.
The other person extends the legs by placing the hand over the knees, depressing the knees, straightening the legs and moving the footboard to touch the plantar surface of the feet at a right angle to the legs. Recheck that the head has not moved from the headboard before taking the measurement. The actual reading is marked by an arrow as there is an offset for greater ease of reading and accuracy.
Read the measurement and record the child’s length in centimetres to the last completed 0.1 cm.
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 10 of 15
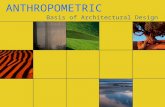
Measuring length: Top: rigid infantometer placed on stable flat surface. Below: Two people using the ‘two leg’ method on a rigid infantometer. Image reproduced from reference 42.
Alternative - the Neorule: Operator 1 holds the head gently with the eyes directly upwards with the lower margin of the orbit in the same vertical plane as the external auditory meatus and gently holds the headboard to the vertex. Operator 2 applies gentle traction to extend the legs without displacing the pelvis and then slides the footplate to meet the heel with just sufficient pressure to cause the skin to blanche; the CHL is then noted to the nearest mm 45.
How to measure head circumference? 23
Use a non-stretchable disposable paper 1–2 cm wide marked in 0.1 cm increments. To measure the head circumference, securely wrap the tape measure around the widest possible circumference of the infant’s head (typically 1 to 2 finger-widths above the eyebrow (supraorbital ridges) on the forehead, above the ears, to the most prominent part of the back of the head (occiput). Repeat the measurement three times and select the largest measurement to the nearest 0.1 cm.
Measuring head circumference: image reproduced from reference 1.
7. REPORTING
Numerical methods used to describe weight, length, and head circumference growth velocity in preterm infants include grams/kilogram/day (g/kg/d), centimetres/week (cm/week), and change in z scores 11 reported at 28 days and 36 weeks postmenstrual age.
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 11 of 15
Z scores should be calculated using a validated size at birth chart and growth chart (eg Fenton chart) up to 42 weeks postmenstrual age 30, 35. Subsequently the INTERGOWTH 21 / WHO growth chart will be used 32.
8. PERFORMANCE MEASURES
Complete anthropometry (weight, length and head circumference) will be collected on all NICUS enrolled infants at birth, 28 days, 36 weeks postmenstrual age, discharge from hospital and/or discharge to home.
9. SUMMARY OF PRACTICE GUIDELINES Within 24 hours of birth
All infants should have weight, length and head circumference measured at birth.
Weight Weight should be assessed using a calibrated electronic scale with 10 g resolution and tared to zero. Average weight gain for infants 10% weight loss day 3 should have a lactation / feeding consult.
Term or late preterm infants with >12% weight loss day 3 or 10% on day 5 should have a medical review.
Term or late preterm infants with
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 12 of 15
Primary indicators of neonatal malnutrition (Not appropriate for first 2 weeks of life except for days to regain birth weight) Mild malnutrition:
Days to regain birth weight 15-18
Decline in weight-for-age z score 0.8-1.2 SD
Weight gain velocity 1.2-2 SD
Weight gain velocity 21
Decline in weight-for-age z score >2 SD
Weight gain velocity2 standard deviations above the mean for a given age and sex.
11. REFERENCES AND LINKS 1. Prevention CfDCa. Measuring head circumference. CDC’s response to Zika. 2016. 2. Villar J, Giuliani F, Fenton TR, Ohuma EO, Ismail LC, Kennedy SH. INTERGROWTH-21st very preterm size at birth reference charts. The Lancet. 2016;387:844-5. 3. Fenton TR, Anderson D, Groh-Wargo S, Hoyos A, Ehrenkranz RA, Senterre T. An Attempt to Standardize the Calculation of Growth Velocity of Preterm Infants-Evaluation of Practical Bedside Methods. J Pediatr. 2018;196:77-83. 4. Bhutta ZA, Giuliani F, Haroon A, Knight HE, Albernaz E, Batra M, Bhat B, Bertino E, McCormick K, Ochieng R, Rajan V, Ruyan P, Cheikh Ismail L, Paul V, International F, Newborn Growth Consortium for the 21st C. Standardisation of neonatal clinical practice. BJOG. 2013;120 Suppl 2:56-63, v. 5. Goldberg DL, Becker PJ, Brigham K, Carlson S, Fleck L, Gollins L, Sandrock M, Fullmer M, Van Poots HA. Identifying Malnutrition in Preterm and Neonatal Populations: Recommended Indicators. J Acad Nutr Diet. 2018;118:1571-82.
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 13 of 15
6. Martinez JI, Roman EM, Alfaro EL, Grandi C, Dipierri JE. Geographic altitude and prevalence of underweight, stunting and wasting in newborns with the INTERGROWTH-21st standard. J Pediatr (Rio J). 2018. 7. Giuliani F, Ohuma E, Spada E, Bertino E, Al Dhaheri AS, Altman DG, Conde-Agudelo A, Kennedy SH, Villar J, Cheikh Ismail L. Systematic review of the methodological quality of studies designed to create neonatal anthropometric charts. Acta Paediatr. 2015;104:987-96. 8. Finken MJJ, van der Steen M, Smeets CCJ, Walenkamp MJE, de Bruin C, Hokken-Koelega ACS, Wit JM. Children Born Small for Gestational Age: Differential Diagnosis, Molecular Genetic Evaluation, and Implications. Endocr Rev. 2018;39:851-94. 9. Lee S, Walker SP. The role of ultrasound in the diagnosis and management of the growth restricted fetus. Australas J Ultrasound Med. 2010;13:31-6. 10. Beune IM, Bloomfield FH, Ganzevoort W, Embleton ND, Rozance PJ, van Wassenaer-Leemhuis AG, Wynia K, Gordijn SJ. Consensus Based Definition of Growth Restriction in the Newborn. J Pediatr. 2018;196:71-6 e1. 11. Fenton TR, Chan HT, Madhu A, Griffin IJ, Hoyos A, Ziegler EE, Groh-Wargo S, Carlson SJ, Senterre T, Anderson D, Ehrenkranz RA. Preterm Infant Growth Velocity Calculations: A Systematic Review. Pediatrics. 2017;139. 12. Clayton PE, Cianfarani S, Czernichow P, Johannsson G, Rapaport R, Rogol A. Management of the child born small for gestational age through to adulthood: a consensus statement of the International Societies of Pediatric Endocrinology and the Growth Hormone Research Society. J Clin Endocrinol Metab. 2007;92:804-10. 13. de Onis M, Habicht JP. Anthropometric reference data for international use: recommendations from a World Health Organization Expert Committee. Am J Clin Nutr. 1996;64:650-8. 14. American College of O, Gynecologists. ACOG Practice bulletin no. 134: fetal growth restriction. Obstet Gynecol. 2013;121:1122-33. 15. Lee ACC, Kozuki N, Cousens S, Stevens GA, Blencowe H, Silveira MF, Sania A, Rosen HE, Schmiegelow C, Adair LS, Baqui AH, Barros FC, Bhutta ZA, Caulfield LE, Christian P, Clarke SE, Fawzi W, Gonzalez R, Humphrey J, Huybregts L, Kariuki S, Kolsteren P, Lusingu J, Manandhar D, Mongkolchati A, Mullany LC, Ndyomugyenyi R, Nien JK, Roberfroid D, Saville N, Terlouw DJ, Tielsch JM, Victora CG, Velaphi SC, Watson-Jones D, Willey BA, Ezzati M, Lawn JE, Black RE, Katz J. Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21 st standard: Analysis of CHERG datasets. BMJ (Online). 2017;358 (no pagination). 16. Raiten DJ, Steiber AL, Carlson SE, Griffin I, Anderson D, Hay WW, Jr., Robins S, Neu J, Georgieff MK, Groh-Wargo S, Fenton TR, Pre BCWG. Working group reports: evaluation of the evidence to support practice guidelines for nutritional care of preterm infants-the Pre-B Project. Am J Clin Nutr. 2016;103:648S-78S. 17. Rochow N, Raja P, Liu K, Fenton T, Landau-Crangle E, Gottler S, Jahn A, Lee S, Seigel S, Campbell D, Heckmann M, Poschl J, Fusch C. Physiological adjustment to postnatal growth trajectories in healthy preterm infants. Pediatr Res. 2016;79:870-9. 18. Ross E, Munoz FM, Edem B, Nan C, Jehan F, Quinn J, Mallett Moore T, Sesay S, Spiegel H, Fortuna L, Kochhar S, Buttery J, Brighton Collaboration Failure to Thrive Working G. Failure to thrive: Case definition & guidelines for data collection, analysis, and presentation of maternal immunisation safety data. Vaccine. 2017;35:6483-91. 19. Rosen H, Shmueli A, Ashwal E, Hiersch L, Yogev Y, Aviram A. Delivery outcomes of large-for-gestational-age newborns stratified by the presence or absence of gestational diabetes mellitus. Int J Gynaecol Obstet. 2018;141:120-5.
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 14 of 15
20. Araujo Junior E, Peixoto AB, Zamarian AC, Elito Junior J, Tonni G. Macrosomia. Best Pract Res Clin Obstet Gynaecol. 2017;38:83-96. 21. Ye J, Torloni MR, Ota E, Jayaratne K, Pileggi-Castro C, Ortiz-Panozo E, Lumbiganon P, Morisaki N, Laopaiboon M, Mori R, Tuncalp O, Fang F, Yu H, Souza JP, Vogel JP, Zhang J. Searching for the definition of macrosomia through an outcome-based approach in low- and middle-income countries: a secondary analysis of the WHO Global Survey in Africa, Asia and Latin America. BMC Pregnancy Childbirth. 2015;15:324. 22. Neylon OM, Werther GA, Sabin MA. Overgrowth syndromes. Curr Opin Pediatr. 2012;24:505-11. 23. DeSilva M, Munoz FM, Sell E, Marshall H, Tse Kawai A, Kachikis A, Heath P, Klein NP, Oleske JM, Jehan F, Spiegel H, Nesin M, Tagbo BN, Shrestha A, Cutland CL, Eckert LO, Kochhar S, Bardaji A, Brighton Collaboration Congenital Microcephaly Working G. Congenital microcephaly: Case definition & guidelines for data collection, analysis, and presentation of safety data after maternal immunisation. Vaccine. 2017;35:6472-82. 24. Pavone P, Pratico AD, Rizzo R, Corsello G, Ruggieri M, Parano E, Falsaperla R. A clinical review on megalencephaly: A large brain as a possible sign of cerebral impairment. Medicine (Baltimore). 2017;96:e6814. 25. Tan AP, Mankad K, Goncalves FG, Talenti G, Alexia E. Macrocephaly: Solving the Diagnostic Dilemma. Top Magn Reson Imaging. 2018;27:197-217. 26. Seaver LH, Irons M, American College of Medical Genetics Professional P, Guidelines C. ACMG practice guideline: genetic evaluation of short stature. Genet Med. 2009;11:465-70. 27. Grunauer M, Jorge AAL. Genetic short stature. Growth Hormone & Igf Research. 2018;38:29-33. 28. Grunauer M, Jorge AAL. Genetic short stature. Growth Horm IGF Res. 2018;38:29-33. 29. Hannema SE, Savendahl L. The Evaluation and Management of Tall Stature. Hormone research in paediatrics. 2016;85:347-52. 30. Fenton TR, Kim JH. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013;13:59. 31. Olsen IE, Groveman SA, Lawson ML, Clark RH, Zemel BS. New intrauterine growth curves based on United States data. Pediatrics. 2010;125:e214-24. 32. Villar J, Giuliani F, Bhutta ZA, Bertino E, Ohuma EO, Ismail LC, Barros FC, Altman DG, Victora C, Noble JA, Gravett MG, Purwar M, Pang R, Lambert A, Papageorghiou AT, Ochieng R, Jaffer YA, Kennedy SH, International F, Newborn Growth Consortium for the C. Postnatal growth standards for preterm infants: the Preterm Postnatal Follow-up Study of the INTERGROWTH-21(st) Project. Lancet Glob Health. 2015;3:e681-91. 33. de Onis M, Onyango AW, Borghi E, Garza C, Yang H, Group WHOMGRS. Comparison of the World Health Organization (WHO) Child Growth Standards and the National Center for Health Statistics/WHO international growth reference: implications for child health programmes. Public Health Nutr. 2006;9:942-7. 34. WHO. Multicentre Growth Reference Study Group. Enrolment and baseline characteristics in the WHO Multicentre Growth Reference Study. Acta Paediatr Suppl. 2006;450:7-15. 35. Fenton TR, Nasser R, Eliasziw M, Kim JH, Bilan D, Sauve R. Validating the weight gain of preterm infants between the reference growth curve of the fetus and the term infant. BMC Pediatr. 2013;13:92. 36. Cole TJ, Wright CM, Williams AF, Group RGCE. Designing the new UK-WHO growth charts to enhance assessment of growth around birth. Arch Dis Child Fetal Neonatal Ed. 2012;97:F219-22.
-
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 15 of 15
37. Reddy KV, Sharma D, Vardhelli V, Bashir T, Deshbotla SK, Murki S. Comparison of Fenton 2013 growth curves and Intergrowth-21 growth standards to assess the incidence of intrauterine growth restriction and extrauterine growth restriction in preterm neonates