GUIDELINE Academic Detailing - CCATESccates.org.br/content/_pdf/en_PUB_1437678333.pdf ·...
47
Faculdade de Farmácia - UFMG Dep. de Farmácia Social www.ccates.org.br GUIDELINE Academic Detailing Belo Horizonte - MG April - 2015
Transcript of GUIDELINE Academic Detailing - CCATESccates.org.br/content/_pdf/en_PUB_1437678333.pdf ·...

Faculdade de Farmácia - UFMG
Dep. de Farmácia Social
www.ccates.org.br
GUIDELINE
Academic Detailing
Belo Horizonte - MG
April - 2015

METHODOLOGICAL GUIDELINES
Academic Detailing
This work was developed under the cooperation agreement between the Department
of Management and Incorporation of Health Technologies of the Ministry of Health of
Brazil, the Pan American Health Organization and the SUS Collaborating Centre for
Technology Assessment and Excellence in Health.
Elaboration:
Juliana de Oliveira Costa (CCATES/UFMG)
Celline Cardoso Almeida Brasil (CCATES/UFMG)
Augusto Guerra Afonso Júnior - coordination (CCATES/UFMG)
Collaborating:
Ana Alice Pandolfi de Abreu (SES-MG)
Gustavo Simões Santos Leal (PPMAF/UFMG)
Haliton Alves de Oliveira Junior (PPMAF/UFMG)
Isabella Piassi Godói (PPMAF/UFMG)
Lívia Lovato Pires de Lemos (CCATES/UFMG)
Lucas Fonseca Rodrigues (FM/UFMG)
Wallace Breno Barbosa (PPMAF/UFMG)
Specialist review:
Aine Heaney (NPS/ Australia)
Jonathan Dartnell (NPS/ Australia)
Brian Godman (Karolinska Institute, Stockholm, Sweden and Strathclyde Institute of
Pharmacy and Biomedical Sciences, Strathclyde University, Glasgow, UK)
Technical review:
Juliana Álvares (CCATES/UFMG)
Francisco de Assis Acurcio (CCATES/UFMG)

METHODOLOGICAL GUIDELINES
Academic Detailing
LIST OF TABLES
Table 1. Examples of academic detailing purposes…………………………………………………….16
Table 2. Basic structure of the visits……………………………………………………………………………26

METHODOLOGICAL GUIDELINES
Academic Detailing
LIST OF FIGURES
Figure 1. Steps of the process involved to perform an Academic Detailing Program (CCATES/UFMG)...........................................................................................13
Figure 2. Academic Detailing carried out by SUS Collaborating Centre (CCATES) in Belo Horizonte about Alzheimer's disease: materials37.........................................18
Figure 3. Academic Detailing carried out by SUS Collaborating Centre (CCATES) in Belo Horizonte about Alzheimer's disease: standardized form for notes about the visit................................................................................................................ 30

METHODOLOGICAL GUIDELINES
Academic Detailing
LIST OF ABREVIATIONS
CADTH - Canadian Agency for Drugs and Technologies in Health
NARCAD – National Resource Center for Academic Detailing
NICE - National Institute for Clinical Excellence and Health
NIHR - Health Technology Assessment Program
NPS – National Prescribing Service
PCDT - Clinical Protocols and Therapeutic Guidelines
REBRATS - Brazilian Network for Health Technology Assessment
SUS – Brazilian National Health System

5
METHODOLOGICAL GUIDELINES
Academic Detailing
SUMMARY
PRESENTATION ....................................................................................................................... 6
1. INTRODUTION ............................................................................................................. 8
2. ACADEMIC DETAILING .............................................................................................. 11
5. RECOMMENDATIONS FOR EACH STAGE OF ACADEMIC DETAILING ........................ 14
5.1. Stage 1: Prospection and identification of problems ............................................... 14
5.2. Stage 2: Definition of the purpose of the academic detailing .................................. 14
5.3. Stage 3: Budget estimate, elaboration of schedule and technical team
designation ............................................................................................................... 16
5.4. Stage 4: Elaboration and purchase of the support material .................................... 17
5.4.1. Bulletin contents ....................................................................................................... 18
5.4.2. Format and layout of the bulletin ............................................................................. 20
5.4.3. Use of materials during the visit ............................................................................... 21
5.5. Stage 5: Identification of prescribers and organization of visitation goals .............. 22
5.6. Stage 6: Recruitment of facilitators and workshop training .................................... 23
5.7. Stage 7: Prescribers visiting for academic detailing ................................................. 25
5.7.1. The objective of academic detailing ......................................................................... 25
5.7.2. Structure of a visit ..................................................................................................... 26
5.8. Stage 8: Release the material ................................................................................... 30
5.9. Stage 9: Evaluation of results ................................................................................... 30
5.9.1. Analysis of the effect ................................................................................................ 31
5.9.2. Analysis of feasibility ................................................................................................ 33
5.9.3. Satisfaction analysis .................................................................................................. 33
5.10. Stage 10: Release the results .................................................................................... 34
7. Final considerations .................................................................................................. 35
REFERENCES .......................................................................................................................... 36
APPENDIX 1 ........................................................................................................................... 40
APPENDIX 2 ........................................................................................................................... 44
APPENDIX 3 ........................................................................................................................... 45

6
METHODOLOGICAL GUIDELINES
Academic Detailing
PRESENTATION
The Academic Detailing is a strategy used by many countries with the overall aim of
promoting the continuing education of prescribers to enhance the rational use of
medicines (RUM). Academic Detailing consists of face-to-face visits, of a health
professional to a prescriber, in which pertinent topics are addressed including the use
of current medicines, diagnostic techniques, new therapies, and implementing
guidelines.
The concept derives from “detailing”, a marketing technique used by pharmaceutical
companies, in which company representatives make one-to-one visits to individual
prescribers in order to persuade them to prescribe the company’s products. It is
hoped that a personal relationship will develop over a number of visits which will
reinforce the effect of the information presented by the representative. Educational
outreach aims to employ some of the techniques developed in pharmaceutical
marketing to promote prescribing which is rational, evidence-based and adherent to
guidelines. It is typically carried out by health professionals (often pharmacists, also
doctors or nurses) employed by non-profit organizations.
This method combines the level of interactivity employed by the pharmaceutical
industry, illustrated by their representatives, with the evidence based on evidence
information from academia. The objective is to minimize the gap between available
scientific evidence and the clinical practice. As a result, improve the future use of
medicines and hence improve overall efficiency in the context of health systems.
This document was based on an extensive search of the scientific literature, the
Academic Detailing experience of the National Prescribing Service - an independent
nonprofit Australian organization that performs this activity for more than fifteen
years, the National Resource Center for Academic Detailing (United States), of the
Canadian Academic Detailing Collaboration (Canada) and the experience of a pilot
project of the Academic Detailing for Alzheimer's disease in the city of Belo Horizonte
conducted by the SUS Collaborating Centre (CCATES).

7
METHODOLOGICAL GUIDELINES
Academic Detailing
The purpose of this document is to present the concepts and the description of the
steps needed to guide the planning and execution of Academic Detailing among
prescribers.
This guideline provides an overview of the academic detailing service. We wish to
assure the quality of academic detailing service and the processes and outcomes that
under pin it. As a result, the main concepts of this technique and examples of materials
and forms necessary for the documentation and evaluation of performance of the
visits are provided.

8
METHODOLOGICAL GUIDELINES
Academic Detailing
1. INTRODUTION
According to the World Health Organization, more than 50% of all medicines are
incorrectly prescribed, dispensed and sold; and more than 50% of patients use them
incorrectly. In developing countries, less than 40% of patients in the public sector and
less than 30% in the private sector are treated in accordance with clinical guidelines1.
The opposite of this situation is the rational use of medicines (RUM) including the
quality use of medicines, which the World Health Organization refers to as "the need
for the patient to receive the appropriate medication in the right dose, for an
adequate period of time, at low cost to him and to the community"2,3. It is well known
that overuse and inappropriate use of medicines can lead to higher rates of adverse
drug reactions and events3. A systematic review found that the median percentage of
preventable drug-related admissions to hospital was 3.7%, with approximately a third
being due to inappropriate prescribing3. Average treatment costs for a single adverse
drug reaction in Germany have been estimated at approximately €2250, equating to
€434million per year, and it is estimated that more than 2 million people are
hospitalised annually in the US due to serious adverse events with the cost of drug-
related morbidity and mortality exceeded US$177.4bn in the US in 20004.
To improve the quality of their prescribing, the prescribers need updated and reliable
sources of information about the comparative effectiveness, safety and cost of
available treatments5. Obtaining this information from the literature can be a long
process and not applicable to the work context of the vast majority of the prescribers
with their limited time available with patients. Due to limitations including time
constraints, difficulties with language and other time-consuming demands, lack of
continuous medical education programs, prescribers often use other sources of
information, including information from representatives of pharmaceutical industries6.
This is augmented by pharmaceutical companies spending up to one third of their
income on promotional expenses, which translated into pharmaceutical companies
spending for instance US$57.5 billion on promotional expenses alone in the US in
20047,8,9.

9
METHODOLOGICAL GUIDELINES
Academic Detailing
Representatives of pharmaceutical companies are internationally known as "drug
detailers" because they provide detailed information about their products, visit
prescribers in their offices and deliver marketing materials focused on the products
they promote6. This approach is known be effective with sales of patented products,
including new products, driving increasing pharmaceutical expenditure10, with the
information disseminated typically in the interest of the pertinent company. As a
result, many prescribers are unaware of the existence of more effective, safer or
cheaper therapeutic options. A recent meta-analysis of studies of physicians exposed
to information from pharmaceutical companies found with rare exceptions that
exposure was associated with for instance higher prescribing frequency, higher costs,
or lower prescribing quality. The authors could not find evidence of net improvements
in prescribing. Consequently, they suggested practitioners should avoid exposure to
information from pharmaceutical companies7.
Such concerns have already resulted in a number of countries introducing measures to
limit pharmaceutical company activities which can be accompanied with fines and
other measures for abuse 11,12,13. In addition, introducing academic detailing and other
activities to counter-act their influence. Intensive measures in e.g. Sweden and the UK
to encourage the prescribing of multiple sourced and considerably cheaper proton
pump inhibitors and statins versus patented products resulted in appreciable
increases in prescribing efficiency compared with countries with few demand side
measures, e.g. expenditure on PPIs and statins in Sweden in 2007 was one tenth of
that seen in Ireland when adjusted for population size with no suggestion in patient
care with the products in each class therapeutically similar at appropriate
doses14,15,16,17. There have also been concerns with the bias of current guidelines
unless there are rigorous approaches regarding conflicts of interest which academic
detailing addresses 18,19,20.
From the behavioral science and several trials in the field, methods to contribute to
better decision-making of prescribers for quality and cost-effectiveness of care have
been detected 3-21. In general, educational campaigns are interventions that potentially

10
METHODOLOGICAL GUIDELINES
Academic Detailing
alter the practice of health professionals, especially prescribers regarding
prescription22.

11
METHODOLOGICAL GUIDELINES
Academic Detailing
2. ACADEMIC DETAILING
Academic detailing is a one on one educational visiting service involving a peer to peer
interaction between two professionals. It uses behavior change methodologies to
provide education and information in an objective, service based approach (rather
than a sales focus), that can be directly related to a health professional's clinical
situation.
The academic detailing is carried out by universities or non-profit institutions, in which
the visitor and his team have no financial relationship with the pharmaceutical
industry, and aims to minimize the gap between the best available science and the
prescription in actual practice6. This method refers to a face-to-face visit with the
objective of improving the care of the health system user, selecting the best evidence
and clinical guidelines on what should be done for a given clinical situation and
presented in usable language by a professional health trained for this purpose6.
The practice of academic detailing to prescribers as a means of improving the quality
of their drug therapy decisions and reducing unnecessary expenditure was pioneered
some thirty years ago by Dr. Jerry Avorn and Dr. Stephen Soumerai of Harvard Medical
School in the USA. According to Soumerai and Avorn 21, 23, some of the most important
features include:
Conducting interviews to investigate baseline knowledge and motivations for
current prescribing patterns;
focusing programs on specific categories of physicians as well as on their
opinion leaders;
defining clear educational and behavioural objectives;
establishing credibility through a respected organisational identity, referencing
authoritative and unbiased sources of information and presenting both sides of
controversial issues;
stimulating active physician participation in educational interactions;
using concise graphic educational materials, highlighting and repeating the
essential messages; and

12
METHODOLOGICAL GUIDELINES
Academic Detailing
providing positive reinforcement of improved practices in follow-up visits.
Academic detailing programs are carried out in several countries, such as Australia -
National Prescribing Servicea, United States - National Resource Center for Academic
Detailingb and Canada-The Canadian Academic Detailing Collaboration24.
Published studies have demonstrated the effectiveness and cost-effectiveness of
academic detailing. A systematic review with meta-analysis22 that included 69 studies
involving more than 15,000 health professionals concluded that educational visits
isolated or combined with other interventions have consistent effects on improving
subsequent prescribing behavior to benefit patients and healthcare services. In
relation to cost-effectiveness, an American randomized study25 that evaluated the
economic effects of face-to-face visit to reduce inappropriate prescribing of medicines
involving 435 prescribers, showed that educational sessions reduced the cost of
prescription drugs inappropriately in 13% and the effect was stable over three
quarters.
a National Prescribing Service: http://www.nps.org.au/
b National Resource Center for Academic Detailing: http://www.narcad.org/

13
METHODOLOGICAL GUIDELINES
Academic Detailing
3. STAGES OF ACADEMIC DETAILING
The Academic Detailing is an activity that must be performed by a qualified and trained
health professional (referred in this document as "facilitator"), properly identified by
the promoting institution and with supporting material for the execution of the visits.
Features of the academic detailing technique have been described 23,26 and include:
that the visitor is well presented and well briefed; the timing is at the doctor’s
convenience; the doctor does not need to interrupt the normal routine of the working
day; the doctor is on his/her own ground rather than at a disadvantage; and the
message is concise and clearly relevant to patient care. The authors of this paper
commented from their own experience that to present an educational message in such
a format requires considerable preparation, with high quality written and pictorial
material and a standardised presentation.
The steps involved in the process, from planning to the dissemination of results are
illustrated in the figure below and discussed in the following sections of this document.
Figure 1. Steps of the process involved to perform an Academic Detailing Program (CCATES/UFMG)

14
METHODOLOGICAL GUIDELINES
Academic Detailing
4. RECOMMENDATIONS FOR EACH STAGE OF ACADEMIC DETAILING
4.1. Stage 1: Prospection and identification of problems
The problems that generate the demand for the Academic Detailing in general are
related to a gap between what the scientific evidence or clinical guidelines recommend
and what treatment approaches are actually undertaken in clinical practice through
other influences including the influence of pharmaceutical companies. The health
system and the health professionals should know the health situation of the
population (i.e. prevalence of diseases and epidemiological transition, and the type of
care that is currently being provided to check if there are alternatives with improved
efficiency, i.e. improved effectiveness for similar expenditure or lower costs for the
same expenditure than could be offered. In this context, the problems may be related
to the need for a guideline, to update existing guidelines, to the over- or under-
utilization of medical technologies, or the use of more expensive treatments when less
expensive but equally effective treatments are available, among others. These
problems can be identified through consultation with specialists; telephone interviews;
database analysis; drug utilization studies; reports and alerts of health surveillance;
literature review; or detection of similar problems observed in other countries.
After identifying the problem, it is necessary to evaluate whether this could be
addressed by the education of the prescribers, that is, if Academic Detailing can be
considered an effective strategy to solve this problem. This technique can be
considered effective when the solution of the identified problem depends on a change
in behavior, and for which other simpler techniques such as computer systems
reminders or dissemination of reports are not sufficient. For the success of the visits, it
is important that the theme selected has local relevance, in order to contribute to the
prescribers and patients’ needs in the context of health care.
4.2. Stage 2: Definition of the purpose of the Academic Detailing
The visits should be carried out in order to solve a specific problem, i.e. have a specific
aim and objective that is measurable. The purposes of academic detailing found in the

15
METHODOLOGICAL GUIDELINES
Academic Detailing
literature are varied and can be directed to the development and dissemination of
Clinical Protocols and Therapeutic Guidelines (PCDT, acronym in Portuguese), changes
in drug prescribing patterns, among others. The visits can be directed to health
professionals (individually or in group), to the community, and to patients. The main
purposes are described in Table 1.
Important principles of academic detailing involve:
understanding existing behavior – what are the key motivations and barriers for
current behavior;
understanding where people are currently at – what people feel/think about
the issue - not where you want them to be;
providing information to improve knowledge and patient care rather than
focusing on what not to do;
focusing on how to encourage and achieve ‘voluntary action’ not coercion or
enforcement.
Objectives of academic detailing include:
Knowledge transfer
Affirming current decision making
Altering future decision making

16
METHODOLOGICAL GUIDELINES
Academic Detailing
Table 1. Examples of academic detailing purposes Purpose Examples Study/country
Change the pattern of resource utilization
Reduction in the use of images diagnostic for shoulder problems
Increase the screening for breast cancer
Broadhurst NA., 200727
Australia
Gorin SS., 200728
United States
Change the pattern of drug prescription
Reduction in the use of broad-spectrum antibiotics in an academic center
Reduction of inappropriate prescriptions in a hospital in relation to the legal criteria of the country
Solomon DH., 200129
United States
Shaw J., 200330
Australia
Development and implementation of Clinical Protocols and Therapeutic Guidelines
Development of Clinical Protocol about anticoagulants in four hospitals
Development of Clinical Protocol and its dissemination for treatment of respiratory tract infections, media otitis and urinary tract infections with antibiotics
Compliance of the Clinical Protocol for Streptococcus B screening prenatal
Compliance of the Clinical Protocol for colorectal cancer screening
Roberts GW., 200631
Austrália
Ilett KF., 200032
Australia
Silva JM., 201333
Brazil
Curry WJ., 201134
United States
Change the incidence of events
Control and weight reduction in African-american low-income women, in primary care
Control and reduction of tobacco use in health systems
Davis M., 200635
United States
Schauer GL., 201236
United States
4.3. Stage 3: Budget estimate, elaboration of schedule and technical team designation
Once the problem and the purpose of the Academic Detailing are established, a
technical team should be formed. This team should be composed of at least one
specialist on the subject to be addressed, as well as researchers and interns, it is
recommended that at least one person (coordinator) manage the process, orient the
other members of staff, and conduct the training of facilitators.
To increase the chances of success of the visits and identify prescribers to be visited, it
is important to establish partnerships with institutions such as the Medical Societies
and Prescribers Councils.
The technical team should define the number of visits required to resolve/minimize
the problem identified. The materials to be produced and/or eventually purchased will
be defined based on the number of visits.

17
METHODOLOGICAL GUIDELINES
Academic Detailing
The estimation of the budget will depend on the scope of the program, i.e. local or
national, the number of prescribers to be visited - which can range from all specialists
registered in the Council, or be restricted to the prescribers of the Brazilian National
Health System; alternatively, a chosen subset of physicians where a specific problem
was observed.
The budget for the implementation of the Academic Detailing should consider the
following costs (i) Staff: experts, researchers and interns (ii) Freelance services: graphic
designer and consultants, among others (iii) Facilitators: health professionals who will
be recruited to carry out the visits, including time taken to upskill and train them (iv)
Graphics services: print newsletters, bulletins, folders, badges and business cards (v)
Materials: tablet, pen drive, suitcase with wheels and notebooks.
4.4. Stage 4: Elaboration and purchase of the support material
The technical team should develop strategies of influence focused on the prescribers,
the multidisciplinary health team and on patients and their families regarding the
disease/treatment in question, through the elaboration of key messages. It is
important that the materials are attractive, objective and simple. They will be used to
support the visit and as a 'leave-behind' information source for the prescriber, who is
often busy and with little time available. The material must be adjusted to the number
of visits required to the individual doctor. At each visit, it is suggested to give different
and complementary material to re-enforce the message. This will help with
relationship building and trust. It helps to build rapport and place the visitor as a
service provider.
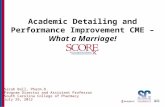
In addition, we recommend the development of in house material, through bulletins
with technical language for professionals and others focused on patients and families
(Figure 2).

18
METHODOLOGICAL GUIDELINES
Academic Detailing
Figure 2. Academic Detailing carried out by SUS Collaborating Centre (CCATES) in Belo
Horizonte about Alzheimer's disease: materials37
4.4.1. Bulletin contents
The elaboration of the bulletin for academic detailing should include as many of the
following items to ensure their quality38,39,40. Commented bulletins can be found in
Appendix 1 and sources of information for their preparation in Appendix 2.
The bulletins should be structured based on key messages
It is recommended to include only three or four key messages in a bulletin according to
the purpose of the intervention. If multiple information is needed, the ideal is to
prepare bulletins in series. The key messages should be highlighted and easily
retrieved and behavioral goals should be highlighted. Different color boxes with
strategic positioning in the document can be used, for example, at the first page or at
the end of the bulletin, as an abstract.
The bulletin should be based on systematic review of the literature.
This criterion is intended to assure the reader that the literature used to prepare the
bulletin was not selected with a bias to support a particular point of view. When using
Materials delivered in Academic Detailing about the Clinical Protocol and Therapeutic Guidelines for
Alzheimer's disease.
The several materials used for the visits were distributed as follows: Visit 1:
• Clinical Protocols and Therapeutic Guidelines of the Ministry of Health, volumes 1 and 2.
• Bulletin for prescribers volume 1 in folder containing business cards;
• Folder for caregivers and patients.
Visit 2: • Book "Multidimensional
Assessment of the Elderly"
• Bulletins for prescribers volumes 2 and 3;
• Pen drive containing all the material needed to request medicines in the Specialized Component.

19
METHODOLOGICAL GUIDELINES
Academic Detailing
this method, it is good to provide this information in the bulletin. It is important to
address aspects of the disease, such as pathophysiology, etiology and epidemiology.
The team should seek information on diagnosis, differential diagnosis, selection of
medicines for prescription, non-pharmacological treatment, among others.
The scientific evidence found must be translated into useful clinical information
to patients and prescribers with appropriate language according to the target
audience.
Supporting information for the therapeutic decision-making should be
included.
When the focus is drug treatment, the bulletin may include dosage recommendations,
alternative therapies, duration of therapy, and/or information on comparative prices.
This information, with their sources, shall be provided in frames, graphs, tables or flow
charts to facilitate their identification in the text.
There must be a mechanism to facilitate the storage and retrieval of the
bulletin.
Possible strategies include the publication of a series volume/issue, to be delivered in
different visits and stored in a folder or a specific packaging; provision of a website for
recovery of the items; delivery of printed materials and also in pen drives.
Should contain case studies.
It is good if the bulletin contains commented case studies, with real and/or complex
clinical situations. Real stories, personas and case vignettes can be very engaging and
illustrative for readers.
The newsletter shall include references and be peer reviewed.
It is recommended references are included in the bulletin to inspire the reader's
confidence in the content. Documents drawn up and published by the Ministry of
Health and Health Departments are relevant as well as those produced by Brazilian or
non-Brazilian medical societies. It is important to seek information in agencies that
evaluate health technologies such as the Brazilian Network for Health Technology

20
METHODOLOGICAL GUIDELINES
Academic Detailing
Assessment (REBRATS, acronym in Portuguese), National Institute for Clinical
Excellence and Health (NICE/England and SMC/Scotland), Health Technology
Assessment Program (NIHR/ United Kingdom) and the Canadian Agency for Drugs and
Technologies in Health (CADTH/Canada).
4.4.2. Format and layout of the bulletin
The development of an Academic Detailing bulletin should incorporate as many of the
formatting items described below 38.
Preferably hire a graphic designer to prepare the layout of the bulletin and its
illustrations, as infographics.
Contain logo or "distributed by" to facilitate the identification of the promoting
institution and partner organizations.
The smallest/minimum number of sections should be appropriate to the topic
being discussed and generally should not exceed five (e.g. introduction,
diagnosis, inclusion criteria, non-pharmacological treatment, pharmacological
treatment).
If more than five sections are required, they must be allocated into broader categories
(e.g. treatment of disease, which includes both pharmacological and non-
pharmacological treatment).

21
METHODOLOGICAL GUIDELINES
Academic Detailing
There must be editorial consistency in the bulletin and its various volumes.
Any bulletin must observe the hierarchy of information, by standardizing ordering of
subtitles, which should be a maximum of three; formatting text and tables, such as
font, size, table headings, text justification; insert standard for highlights in the text
and colors.
Textual sections in the bulletin should be formatted in columns with
appropriate widths, avoiding excessively long stretches; the text should be structured
in topics, whenever possible; the font size should be appropriate and aligned and the
use of colors can be used to enhance readability.
4.4.3. Use of materials during the visit
It has been shown in many different circumstances that printed materials alone
(especially if unsolicited) rarely produce significant changes in clinical practice.
However, the use of print materials that are well presented and structured to support
the focus of the face to face visit are useful adjuncts for getting the messages across.
Consistent use of logos and credibility building program associations’ details,
references and reviewer can help to build 'brand recognition' as well as building
confidence in the integrity and reliability of program materials.
Such helpful printed material can provide a gift of value to be left with the prescriber,
as well as providing a structure in a flow for the interaction. In programs where
multiple visits (or visitors) are involved, printed materials can help with consistency of
message delivery.
However because of the systemization of the placement of information in a specific
location on a printed page, it is also possible that print materials can deflect a
facilitator from their core responsibility in each encounter: that of first establishing and
understanding the needs of the individual prescriber with respect to the key messages
which are to be imparted.

22
METHODOLOGICAL GUIDELINES
Academic Detailing
Thus care, practice and conscious skill is needed to effectively use printed materials
during a visit. It is important to maintain physical control of the materials during the
visit. Do not allow them to get in the way of the dialogue - maintain eye contact with
prescriber and only occasionally point out areas of interest on the page. Reassure the
clinician that you will be leaving the materials behind at the end of the visit so they do
not become too distracted.
4.5. Stage 5: Identification of prescribers and organization of visitation goals
After the definition of the target population, it should be decided which prescribers
should receive a visit as resources (time and money) may be scarce. Often due to lack
of financial resources and time, it is impossible to cover all prescribers of the target
population. This creates need to select those physicians who will receive a visit. It may
then be appropriate to identify those prescribers that can serve as opinion leaders for
other prescribers. Alternatively, select those physicians with the greatest concern with
their prescribing41. If this is difficult, methods such as random sampling can be
considered.
It is important to emphasize the need to select about 30% more prescribers for the
visitation, since expected losses due to refusals, not identifying the selected prescriber
or loss of follow-up between one visit and another.
The selected prescribers should be grouped according to the clinical care area
(preferably in their office, if they work in hospitals as well), to maximize the number of
daily visits by facilitator. The number of prescribers by facilitator should be calculated
based on the number of visits and the medical specialty, since the number of visits will
be influenced by specialist involved. For example, consultations with geriatricians may
take up to four times longer than with general practitioners. We recommend the goal
of four prescribers per facilitator per day. However, this will vary if a greater density of
experts is required.

23
METHODOLOGICAL GUIDELINES
Academic Detailing
4.6. Stage 6: Recruitment of facilitators and workshop training
To ensure a successful visit, the organizers of the academic detailing should follow as
many of the items described below as possible 39,42,43:
Selection of facilitators
A facilitator should ideally have the following characteristics: be a good communicator;
have availability; be friendly; have some understanding of concepts related to Evidence
Based Medicine; know the scope/ workings of the health care system; have practical
experience in the subject; understand and internalize the importance of the work to be
developed in order to carry out the visits with conviction and efficiency; and have his/
her own vehicle (if pertinent for transport between physicians).
The professional background of the facilitator is less important than their
communication skills and the soundness and breadth of their understanding of clinical
therapeutics and barriers to prescribing change. If the facilitator does not have these
characteristics, these should be addressed in the workshop training. If the facilitator
does not have his own vehicle, the potential for taxis should be explored.
Provide identification material for facilitators
To ensure greater credibility to the prescriber, the visitors should be provided with
identification badges and business cards. Facilitators should introduce themselves and
the institution they represent at the beginning. It establishes credibility through a
respected organisational identity. This provides reassurance to the prescriber and can
open a warm and friendly dialogue as they know the conversation will be informed and
independent.
Ensure adequate training
At this stage, the team will hold workshop training to the facilitators, with the
minimum duration of approximately 12 hours. The training should include the
following items:
Study of the theme: The facilitators should receive the materials to read and study
about Academic Detailing and the problem in question. After this study, the

24
METHODOLOGICAL GUIDELINES
Academic Detailing
facilitators should be encouraged to develop key messages with their own
language. The dedication of time for this item is variable, and it is estimated to be a
minimum of three hours.
Training on visitation techniques: In training, the facilitators will be exposed to the
methods of different approaches (visitation techniques) during the academic
detailing visit, with the participation of non-Brazilian guests with experience in this
area, as representatives of pharmaceutical industries (drug detailers) or
professionals that have already performed academic detailing visits. The estimated
time for this item is four hours, but can be reduced to further training in other
subjects if the visiting team is maintained.
Training on the content of the visits: At this time, the facilitators will be exposed to
the contents/material to be covered in each of the visits, with the participation of
the specialist in the field. The estimated time for this item is two hours.
Individual test application on visitation techniques and content: At the end of the
individual study and training, a multiple choice test covering the visitation
techniques, the scientific evidence documented in the bulletin and other aspects
that must or may be addressed during the visit likely to be asked by prescribers is
highly recommended.
Simulation of the visit: It is recommended to simulate the visits among the
facilitators so that all can act either as prescriber or as facilitators, with the
handling and the "delivery" of the material. These simulations should be recorded
to enable harmonization of the approach. If possible, a final simulation can be
made between the facilitator and a specialist in the field. The estimated time for
this item is three hours.
Release the visit materials for the facilitators
After training the facilitators should receive and organize the materials that will be
distributed during the visits. It is recommended that the coordination of the project
provide, in addition to the materials to be delivered to prescribers and customized
business card, other materials to assist in the visit, e.g. suitcase with wheels for all the

25
METHODOLOGICAL GUIDELINES
Academic Detailing
materials to be distributed, a tablet or notebook for notes. Alongside this, the use of
standardized forms to the production of post visit notes and feedback.
4.7. Stage 7: Prescribers visiting for academic detailing
Each facilitator should receive a list of prescribers to be visited, containing their
specialty, address and contact phone number. Before the visit, the facilitator should
call to the prescriber workplace and confirm the address and check the days and times
that that the physician will be available. Scheduling must be done, preferably at a time
that the prescriber has no patients, to avoid prolonged time in the waiting room.
It is important to remember that Academic Detailing aims to encourage the voluntary
change of attitude, not through coercion or other means. The facilitator should
estimate the duration of the visit between 15 and 20 minutes.
4.7.1. The objective of academic detailing
Is to move beyond communication of just information;
involves understanding existing behavior and what key motivators & barriers
are for current behavior;
understanding where people are at - what they think/feel about issues;
focuses on how to encourage and achieve voluntary action - not about coercion
or enforcement.

26
METHODOLOGICAL GUIDELINES
Academic Detailing
4.7.2. Structure of a visit
A visit to Academic Detailing should go through all the steps listed in Table 2, ranging
from the introduction of the facilitator and the visit reason as to maintain the
relationship with the prescriber. Then other topics that should be observed are
presented.
Table 2. Basic structure of the visits Stages Actions Introduction
Create a suitable space for the visit
Attend to the immediate needs of the doctor
Practice the art of small talk to establish rapport
Demonstrate attentiveness through your body language
Explain the purpose of your visit
Confirm time/availability is still convenient Build trust and establish your credibility
Mention organisational imprimatur or credentials
Mention to be unbiased and independent
Conduct a clinically based visit
Present credible and related to patient care information
Demonstrate empathy, honesty, commitment, expertise Identify the needs of the prescriber
Use open questions to get the person talking
Use minimal encouragers to keep the conversation flowing
Reflect what you’ve heard to show that you’re listening and to check that you’ve understood correctly
Helps to gain information but also guage opinion, feelings and ideas Present the features and benefits “key messages”
Present the key messages of your visit so that they relate to the beliefs, needs, values and interests of the doctor as you perceive them.
Turn features or 'facts' of your message into benefits/value for the doctor and patient
Target them to overcome barriers to change Overcome any objections and handle any challenging responses
E.g. anger or indifference that stands in the way of the staff “buying” your message.
Be alert (listening, observing non-verbal cues) for barriers to your messages
Close the communication loop
Use ‘reflecting’ skills to make sure your messages have been ‘received’
Offer further support
Gain commitment for subsequent visit
Offer the materials for reciprocal obligation Follow-up and maintain your relationship with the clinic staff
Service philosophy
Commitment to mutual goals
Important for behaviour change

27
METHODOLOGICAL GUIDELINES
Academic Detailing
Personal presentation
To conduct the visit, is recommended facilitators value their personal appearance, i.e.
wear social discrete colors costumes, avoid excessive makeup and chewing gum, keep
the nails manicured and in the case of men be clean shaven. The facilitator should
identify himself/herself with discretion (avoid conversations and speak softly) and
greet everyone related to the activity.
Basic guide for the visit
Schedule the visit first, or go in person to the office; arrive in the reception, present
yourself and give your business card (treating the attendant by name); check the
availability of the prescriber to visit; wait in a place in the office that does not disturb
the workings of the surgery and sit only if there is space (the patients and their
companions always have priority); expect the prescriber to invite you to enter; sit only
when there is availability or when you are invited; use the tablet or an agenda to take
notes; have clear the main points of approach to avoid forgetting them during the visit;
be prepared to hear different opinions and for the visit to be refused due to recent
extenuating circumstances.
The wait can be hours. If the attendant warns that there will be a long waiting time,
the facilitator can visit other prescribers in nearby locations.
During the visit the facilitator should:
Be punctual;
turn off the cellphone or put it on silence;
act naturally and be attentive;
compliment the prescriber with warmth and friendliness and identify themselves
with the business card as well as avoid actions that demonstrate intimacy (unless
the gesture comes from the prescriber);
summarize the proposal of the visit;
report on the confidentiality of data;

28
METHODOLOGICAL GUIDELINES
Academic Detailing
ask about the experience of the prescribing and their clinical practice experience,
seeking for their participation;
address the issues planned for the visit;
combine talking with the use of the printed material;
be firm, demonstrate knowledge, provide a good service;
be prepared to reduce the time of the visit, if this is needed;
observe signs of interest/disinterest, haste, impatience, misunderstanding and
other signs shown by the prescriber and react to these changes or even end the
visit;
deliver the material always at the end of the visit, avoiding to distract the
prescriber;
at the end of each visit, always ask if something was not understood, if the
prescriber has any questions that you can clarify, and schedule the next visit, if
there is any;
in subsequent visits, try to resume the subject under discussion and answer the
questions raised.
During the visit the facilitator should avoid:
Address the issues of future visits, if there are any.
issues that deviate from their goal and with personal matters;
come into direct confrontation with the prescriber, even if it is a controversial
subject;
expressions or sudden gestures;
use of slang or treat the prescriber by "you" (unless if it is requested by the
prescriber).
Conduct in specific situations:
if the prescriber has limited availability to meet representatives, the facilitator
should explain briefly their work, clarifying that it is not representative of the
pharmaceutical industry and that the activity stems from the need for public

29
METHODOLOGICAL GUIDELINES
Academic Detailing
health. Inform the physician of the estimated time required for the visit, the
frequency and then check if you can count on prescriber collaboration;
if the prescriber still has time and has shown interest, the facilitator should take
advantage of this and fully explore the material and content for the visit;
if the facilitator does not know how to respond any inquiry, they must say that will
get the answer and send it by email or phone message, or reply personally in the
next visit, rather than give false information. It is very important to follow up on
this.
After the visit;
the facilitator should thank the attendant by his/ her name when they leave the
office.
if any material or content is not addressed, try to address this during the next visit,
if there is any. The continuity of the visits is very important, and the notes about
the visit are essential to ensure a good relationship with the prescriber, giving them
the impression that this facilitator paid special attention to the questions raised
and remembered what was discussed during the last visit
the facilitator should write down all the information that he/she found relevant on
the visit, right after the contact with the prescriber. It is recommended to pay
attention to any barriers identified in the visit to improve the academic detailing
program. To do that, the facilitator should carry a notebook or tablet with a
standardized form and a free space for insights and questions of prescribers (Figure
3).

30
METHODOLOGICAL GUIDELINES
Academic Detailing
Figure 3. Academic Detailing carried out by SUS Collaborating Centre (CCATES) in Belo Horizonte about Alzheimer's disease: standardized form for notes about the
visit
4.8. Stage 8: Release the material
All materials developed for the visit, as well as those used for the training of
facilitators, should be made available in digital media by the promoting institution of
the Academic Detailing Program, for free access by other researchers, prescribers and
the public in general.
It is good to develop a list of the most frequently asked questions of the prescribers,
answer them and provide these together with the other materials. Coordinators
should circulate this list among all facilitators to ensure they answer a greater number
of questions and to provide standardized answers for the facilitator to use.
4.9. Stage 9: Evaluation of results
Evaluation and planning should be built in to all stages of development of a program. It
is important that this be part of the thinking from the outset and an evaluation plan
developed during the design of the program. This will then determine the evaluation
methodology – be careful not to over-complicate the evaluation approach – need to be

31
METHODOLOGICAL GUIDELINES
Academic Detailing
clear what is really important to measure, and if it is measurable, can be interpreted,
and will make a difference to future work. The availability of data sets is an important
consideration here.
It is critical to evaluate the results achieved, any identified areas to improve the
strategy adopted, demonstrate the relevance of the Academic Detailing, and ensure
the continuity of the work. The academic detailing program can be evaluated in terms
of analysis of the effect, its feasibility and prescriber’s or patient’s satisfaction38.
4.9.1. Analysis of the effect
The effect obtained after the end of the visits should be evaluated in order to validate
the usefulness and cost-effectiveness of the Academic Detailing as an intervention to
achieve the proposed objective. To do this, one must define what the outcomes are at
the beginning and which study design is more appropriate to identify and measure
these outcomes. In addition, the costs involved.
Definition of the outcomes
The impact of the intervention can be evaluated in terms of outcomes related to the
prescriber or the patient.
The outcomes related to prescribers include, in many cases, knowledge, attitudes and
behavior change and can be identified through self-evaluation of the prescribing of
their knowledge in the area before and after the intervention. Also the changes in the
pattern of drug prescriptions or the compliance of prescribers to Clinical Guidelines
can be measured after the Academic Detailing through drug utilization studies.
If it is not possible to assess the outcomes related to the prescriber, or, if there is
interest to extend these results, it is possible to assess the outcomes related to
patients. It can be evaluated though self-reported symptoms, treatment adherence,
satisfaction with the care provided by the prescriber, the reduction in the incidence of
some events, or the quality of life of patients treated by prescribers who received the

32
METHODOLOGICAL GUIDELINES
Academic Detailing
intervention. However, this can be much more difficult, time consuming and
expensive.
The two different levels of outcome (patients and prescribers) are not exclusive, since
the same study may examine the results in more than one level.
Study design:
Depending on the outcome of interest, the method of evaluation can be a randomized
controlled trial, or quasi-experimental studies.
Randomized controlled trials are used when the randomized group is the same as the
group that will be evaluated (i.e., the level of randomization and the level of analysis
are the same). For example, studies that attempt to assess the change in knowledge of
prescribing before and after the intervention compared with the control group, also of
prescribers. The control group may receive no intervention or just printed educational
material. A limitation of this study design would be the "educational contamination" of
the control group by prescribers who received the intervention and share information
with co-workers. Conduct the randomization in clusters, in other words, randomize
clinics or regions instead of prescribers would be an option to minimize this problem.
In quasi-experimental studies there is no control group and the measurements are
made before and after the intervention. It is a suitable study design for studies that
cover the entire target population of prescribers or studies where the outcome can’t
be measured individually, but only in groups. However, it may be difficult to interpret
the results due to potential changes over time that may have altered the outcome and
that are not related to the intervention.
The assessment can be done in statistical terms, considering the differences in the
percentage or average outcomes, or descriptively. Qualitative studies of prescriber’s,
patient’s and/or facilitator’s perceptions on academic detailing can also be used. For
evaluation of programs of Academic Detailing already established and programs in
progress, ecological studies to analyze changes in certain outcome over time or a

33
METHODOLOGICAL GUIDELINES
Academic Detailing
series of cross-sectional studies can also be used. The Australian organization NPS, for
example, publishes an annual report presenting the results of the activities carried out
and the improvement in some outcomes over the years, such as quality of
prescription, quality use of medicines and improved practice of health professionals44.
4.9.2. Analysis of feasibility
The feasibility analysis is generally descriptive and should consider:
costs associated with the facilitator work (recommended to pay per visit
performed);
costs associated with materials (development and print);
time spent in training;
time spent in visit;
loss of prescribers;
difficulty of scheduling;
perceptions of the facilitator in relation to the visit.
This analysis may be conducted by the organizing team. If this is not the case, the costs
involved with hiring this team should be considered as well as the time to develop the
material in any subsequent evaluation.
4.9.3. Satisfaction analysis
The perception of the professionals visited is critical to assess the acceptability,
relevance and quality of the academic detailing. This inquiry can be carried out by
questionnaire administered by telephone, forms to be filled online using, visual
analogue scales or numerical scales applied after the last visit. A model of
questionnaire for a telephone interview and visual analogue scales are provided in
Appendix 3.
In the case of telephone inquiry, the interviewer should not be the facilitator who
conducted the visit. This method ensures that the respondent does not feel pressured
to positively evaluate the visit by the facilitator presence. Other advantages of this

34
METHODOLOGICAL GUIDELINES
Academic Detailing
approach are: does not depend of equipment and internet availability for submission
of information and is more convenient to the prescriber.
To avoid memory bias, this inquiry should preferably be done within seven calendar
days after the last visit made to each prescriber. The presentation of results should
consider the number of survey respondents and description of the answers of the
questionnaire.
4.10. Stage 10: Release the results
The dissemination of results in the scientific community is essential, especially when
the first intervention provides evidence about the effectiveness and efficiency of
Academic Detailing. The results should also be disseminated to medical societies in
order to strengthen relations for future interventions and to provide feedback to the
prescribers visited. Another equally important role is raising awareness of other
prescribers regarding the Academic Detailing and the information transmitted.
It is recommended to prepare a report containing all the steps of detailing for
dissemination in electronic and physical format, and a scientific article that addresses
the process as a whole, with emphasis on evaluation of the impact of intervention.

35
METHODOLOGICAL GUIDELINES
Academic Detailing
5. FINAL CONSIDERATIONS
In this document, we sought to address in a simple and practical way the main steps
for planning and implementing an Academic Detailing Program. This guideline does not
exhaust the subject, so those wishing to carry out visits toward to prescribers should
deepen the content in specific readings.
The focus of this document was the visitation of prescribers, but there are other forms
of Academic Detailing, addressed to patients, community and professional groups.
Published evidence also shows the effectiveness of other teaching strategies and
continued education, such as audits and feedback which can be used complementary
to the Academic Detailing strategy. Although a visit face-to-face is preferable,
telephone or videoconference contact are alternatives, especially when it is the
extension of an existing Academic Detailing Program.
The success of Academic Detailing depends on several factors; among the main ones
are the programming and carefully training to address a topic considered relevant to
clinical practice. The attractiveness of visits and the support material should be
targeted and carefully planned to ensure prescriber confidence in the disseminated
content and to address the barriers identified for changing the behavior of the
prescribers.
Although the principal evidence found addressed the use of this technique for the
dissemination of clinical protocols and compliance with its recommendations,
Academic Detailing can also be used to track issues, challenges and suggestions
reported by the prescribers. In this case, the perception of the prescribers would help
to update or develop new protocols, possibly increasing their acceptability and the
rate of implementation of its recommendations.

36
METHODOLOGICAL GUIDELINES
Academic Detailing
REFERENCES
1. W O R L D H E A L T H O R G A N I Z A T I O N . Medicines: rational use of medicines. Fact sheet n° 338. May 2010. Disponível em: <http:// www.who.int/mediacentre/factsheets/fs338/en/ print.html> Access in: March 06, 2013.
2. CONFERENCIA DE EXPERTOS, 1985, Nairobi. Uso Racional de Medicamentos. Informe de La Conferencia de Expertos, Nairobi, 25-29 de noviembre de 1985. Ginebra: Organización Mundial de La Salud, 1986. 304 p.
3. HOLLOWAY KA. Combating inappropriate use of medicines. Expert review of clinical pharmacology. 2011;4(3):335-48.
4. GODMAN B, FINLAYSON AE, CHEEMA PK, ZEBEDIN-BRANDL E, GUTIERREZ-IBARLUZEA I, JONES J, et al. Personalizing health care: feasibility and future implications. BMC medicine. 2013;11:179
5. TABA P, ROSENTHAL M, HABICHT J, TARIEN H, MATHIESEN M, HILL S, et al. Barriers and facilitators to the implementation of clinical practice guidelines: a cross-sectional survey among physicians in Estonia. BMC health services research. 2012;12:455
6. NATIONAL RESOURCE CENTER FOR ACADEMIC DETAILING (NaRCAD). About Academic Detailing. Disponível em http://www.narcad.org/about/aboutad/ Access in: March 06, 2015.
7. SPURLING GK, MANSFIELD PR, MONTGOMERY BD, LEXCHIN J, DOUST J, OTHMAN N, et al. Information from pharmaceutical companies and the quality, quantity, and cost of physicians' prescribing: a systematic review. PLoS medicine. 2010;7(10):e1000352.
8. CIVANER M. Sale strategies of pharmaceutical companies in a "pharmerging" country: the problems will not improve if the gaps remain. Health policy (Amsterdam, Netherlands). 2012;106(3):225-32.
9. GODMAN B, GUSTAFSSON LL. A new reimbursement system for innovative pharmaceuticals combining value-based and free market pricing. Applied health economics and health policy. 2013;11(1):79-82
10. MOUSNAD MA, SHAFIE AA, IBRAHIM MI. Systematic review of factors affecting pharmaceutical expenditures. Health policy (Amsterdam, Netherlands). 2014;116(2-3):137-46
11. YU SY, YANG BM, KIM JH. New anti-rebate legislation in South Korea. Applied health economics and health policy. 2013;11(4):311-8
12. BRKICIC LS, GODMAN B, VONCINA L, SOVIC S, RELJA M. Initiatives to improve prescribing efficiency for drugs to treat Parkinson's disease in Croatia: influence and future directions. Expert review of pharmacoeconomics & outcomes research. 2012;12(3):373-84

37
METHODOLOGICAL GUIDELINES
Academic Detailing
13. ROEHR B. Drug companies will have to report all payments to US doctors from March 2014. BMJ (Clinical research ed). 2013;346:f826
14. GODMAN B, SHRANK W, ANDERSEN M, BERG C, BISHOP I, BURKHARDT T, et al. Comparing policies to enhance prescribing efficiency in Europe through increasing generic utilization: changes seen and global implications. Expert review of pharmacoeconomics & outcomes research. 2010;10(6):707-22
15. WENG TC, YANG YH, LIN SJ, TAI SH. A systematic review and meta-analysis on the therapeutic equivalence of statins. Journal of clinical pharmacy and therapeutics. 2010;35(2):139-51
16. USHER-SMITH J, RAMSBOTTOM T, PEARMAIN H, KIRBY M. Evaluation of the clinical outcomes of switching patients from atorvastatin to simvastatin and losartan to candesartan in a primary care setting: 2 years on. International journal of clinical practice. 2008;62(3):480-4.
17. NORMAN C, ZARRINKOUB R, HASSELSTROM J, GODMAN B, GRANATH F, WETTERMARK B. Potential savings without compromising the quality of care. International journal of clinical practice. 2009;63(9):1320-6.
18. BJORKHEM-BERGMAN L, ANDERSEN-KARLSSON E, LAING R, DIOGENE E, MELIEN O, JIRLOW M, et al. Interface management of pharmacotherapy. Joint hospital and primary care drug recommendations. European journal of clinical pharmacology. 2013;69 Suppl 1:73-8
19. NEUMAN J, KORENSTEIN D, ROSS JS, KEYHANI S. Prevalence of financial conflicts of interest among panel members producing clinical practice guidelines in Canada and United States: cross sectional study. BMJ (Clinical research ed). 2011;343:d5621.
20. DE SOUZA AL, ACURCIO FD, GUERRA JUNIOR AA, DO NASCIMENTO RC, GODMAN B, DINIZ LM. Authors' Reply to Dr. Malerbi: "Insulin Glargine in a Brazilian State: Should the Government Disinvest?". Applied health economics and health policy. 2014
21. SOUMERAI SB, AVORN J. Principles of educational outreach ('academic detailing') to improve clinical decision making. JAMA. 1990 Jan 26;263(4):549-56. PubMed PMID: 2104640.
22. O’BRIEN, MA et al. Educational outreach visits: effects on professional practice and health care outcomes. Cochrane Database of Systematic Reviews, 2007; Issue 4. Art. No.: CD000409.
23. AVORN J, SOUMERAI S. Improving drug therapy decisions through educational outreach: A randomised controlled trial of academically based ‘detailing’. New Engl J Med 1983;308:1457-63
24. JIN M, NAUMANN T, REGIER L, et al. A brief overview of academic detailing in Canada: Another role for pharmacists. Canadian Pharmacists Journal: CPJ2012;145(3):142-146.e2. doi:10.3821/145.3.cpj142

38
METHODOLOGICAL GUIDELINES
Academic Detailing
25. SOUMERAI SB, AVORN J. Economic and policy analysis of university-based drug "detailing". Med Care. 1986 Apr;24(4):313-31. PubMed PMID: 3083161.
26. POND CD, MANT A, KEHOE L, HEWITT H, BRODATY H. General practitioner diagnosis of depression and dementia in the elderly: Can academic detailing make a difference? Family Practice 1994;11 (2) 141-147.
27. BROADHURST, NORM A., et al. "A before and after study of the impact of academic detailing on the use of diagnostic imaging for shoulder complaints in general practice." BMC family practice 8.1 (2007): 12.
28. GORIN SS, ASHFORD AR, LANTIGUA R, DESAI M, TROXEL A, GEMSON D. Implementing academic detailing for breast cancer screening in underserved communities. Implementation science : IS 2007;2:43. doi:10.1186/1748-5908-2-43.
29. SOLOMON DH, VAN HOUTEN L, GLYNN RJ, BADEN L, CURTIS K, SCHRAGER H, AVORN J. Academic detailing to improve use of broad-spectrum antibiotics at an academic medical center. Arch Intern Med. 2001 Aug 13-27;161(15):1897-902.
30. SHAW J, HARRIS P, KEOGH G, GRAUDINS L, PERKS E, THOMAS PS. Error reduction: academic detailing as a method to reduce incorrect prescriptions. Eur J Clin Pharmacol. 2003 Nov;59(8-9):697-9. Epub 2003 Oct 18. PubMed PMID: 14566443.
31. ROBERTS GW, ADAMS R. Impact of Introducing Anticoagulation-Related Prescribing Guidelines in a Hospital Setting using Academic Detailing. Therapeutics and Clinical Risk Management 2006;2(3):309-316.
32. ILETT KF, JOHNSON S, GREENHILL G, et al. Modification of general practitioner prescribing of antibiotics by use of a therapeutics adviser (academic detailer).British Journal of Clinical Pharmacology 2000;49(2):168-173. doi:10.1046/j.1365-2125.2000.00123.x.
33. SILVA JM, STEIN AT, SCHÜNEMANN HJ, BORDIN R, KUCHENBECKER R, DE LOURDES DRACHLER M. Academic detailing and adherence to guidelines for Group B streptococci prenatal screening: a randomized controlled trial. BMC Pregnancy Childbirth. 2013 Mar 19;13:68. doi: 10.1186/1471-2393-13-68.
34. CURRY WJ, LENGERICH EJ, KLUHSMAN BC, et al. Academic detailing to increase colorectal cancer screening by primary care practices in Appalachian Pennsylvania. BMC Health Services Research 2011;11:112. doi:10.1186/1472-6963-11-112.
35. DAVIS MARTIN P, RHODE PC, DUTTON GR, REDMANN SM, RYAN DH, BRANTLEY PJ. A primary care weight management intervention for low-income African-American women. Obesity (Silver Spring). 2006 Aug;14(8):1412-20.
36. SCHAUER GL, THOMPSON JR, ZBIKOWSKI SM. Results from an outreach program for health systems change in tobacco cessation. Health Promot Pract. 2012 Sep;13(5):657-65. doi: 10.1177/1524839911432931. Epub 2012 Apr 11.

39
METHODOLOGICAL GUIDELINES
Academic Detailing
37. GODMAN B, ACURCIO F, GUERRA JUNIOR AA, ALVAREZ-MADRAZO S, FARIDAH ARYANI MY et al Initiatives among authorities to improve the quality and efficiency of prescribing and the implications. J Pharma Care Health Sys 2014;1(3):1-15
38. CANADIAN AGENCY FOR DRUGS AND TECHNOLOGIES IN HEALTH (CADTH). Academic Detailing Templates. 2015. Available in: < http://www.cadth.ca/en/resources/academic-detail-toolkit>
39. MACLURE M, ALLEN M, BACOVSKY R, et al. Show me the evidence: best practices for using educational visits to promote evidence-based prescribing. Victoria (BC): Drug Policy Futures; 2006. 2015. Available in: http://web.law.columbia.edu/sites/default/files/microsites/attorneys-general/files/Show_me_the_evidence_report.pdf
40. WORLD HEALTH ORGANISATION. Promoting the Rational Use of Medicines. In: Drug and Therapeutics Committees - A Practical Guide. 2015. Available in http://apps.who.int/medicinedocs/pdf/s4882e/s4882e.pdf.
41. PICHETTI S, SERMET C, GODMAN B, CAMPBELL SM, GUSTAFSSON LL. Multilevel analysis of the influence of patients' and general practitioners' characteristics on patented versus multiple-sourced statin prescribing in France. Applied health economics and health policy. 2013;11(3):205-18
42. AGENCY FOR HEALTHCARE RESEARCH AND QUALITY. The Practice Facilitation Handbook: Training Modules for New Facilitators and Their Trainers. Module 10. Academic Detailing as a Quality Improvement Tool. May 2013., Rockville, MD. Available in: http://www.ahrq.gov/professionals/prevention-chronic-care/improve/system/pfhandbook/mod10.html
43. NATIONAL RESOURCE CENTER FOR ACADEMIC DETAILING (NaRCAD). About Academic Detailing. Available in: http://www.narcad.org/services/training/academic-detailing-training/ Access in: March 06, 2015.
44. NATIONAL PRESCRIBING SERVICE (NPS). NPS MedicineWise Annual Evaluation Report 2012/13. Available in: http://www.nps.org.au/about-us/what-we-do/our-research/publications/reports/annual-evaluation-report. Access in: January 27, 2015.

40
METHODOLOGICAL GUIDELINES
Academic Detailing
APPENDIX 1
Examples of bulletins
Example 1 – Bulletin for prescribers developed by the Prescription Information Services of Manitoba (PrISM – Canada)
Publication in volumes
Supporting information for the therapeutic decision-making
Key messages
References Identification of the promoter institution and partnerships
Source: CANADIAN AGENCY FOR DRUGS AND TECHNOLOGIES IN HEALTH (CADTH). Newsletter Evaluation: NL-02. Available in: http://www.cadth.ca/media/compus/cac_review/Jan_2007/Appendix%2026%20-%20Newsletters_Evaluation_Catalogue.pdf

41
METHODOLOGICAL GUIDELINES
Academic Detailing
Example 2 – Bulletin for prescribers, containing cases study, developed by Prescription Information Services of Manitoba (PrISM – Canada)
Narrative of the case
Question to the prescriber
Correct answer and comment
Source: CANADIAN AGENCY FOR DRUGS AND TECHNOLOGIES IN HEALTH (CADTH). Prescribing Aid Evaluation: PA-07. Available in: http://www.cadth.ca/media/compus/cac_review/Jan_2007/Appendix%2029%20-%20Prescribing%20Aid%20Evaluation%20Catalogue.pdf

42
METHODOLOGICAL GUIDELINES
Academic Detailing
Example 3 – Folder for patients and caregivers developed by SUS Collaborating Centre (CCATES – Brazil)
Key messages
Identification of the promoter institution and partnerships
Language appropriate to patients / caregivers

43
METHODOLOGICAL GUIDELINES
Academic Detailing
Example 4 – Folder for patients and caregivers developed by National Prescribing Service (NPS - Australia) ]
Aspects of the disease, etiology, epidemiology and treatment
Non-pharmacological care
Language appropriate to patients/ caregivers

44
METHODOLOGICAL GUIDELINES
Academic Detailing
APPENDIX 2
Frame 1 – Information sources for Academic Detailing Program
Information sources Address
Health technology assessment agencies
Brazilian Network of Health-Technology Assessment - REBRATS
http://200.214.130.94/rebrats/
Cadadian Agency for Drugs and Technologies in Health – CADTH (Canada)
http://www.cadth.ca/
National Institute for Clinical Excellence and Health – NICE (United Kingdom)
http://www.nice.org.uk/
Agencias y Unidades de Evaluación de Tecnologías Sanitarias – AUbETS (Spain)
http://aunets.isciii.es/web/guest/home
Helth Technology Assessment Program – NIHR (United Kingdom)
http://www.hta.ac.uk/
NHS Evidence https://www.evidence.nhs.uk
Effective Health Care –AHRQ (United States)
http://www.effectivehealthcare.ahrq.gov/
Clinical protocols and therapeutic guidelines
Ministry of Health http://portalsaude.saude.gov.br/index.php/component/content/article?id=9315
National Guideline Clearinghouse http://www.guideline.gov/
Best Practice (BMJ) http://portalsaude.saude.gov.br/ Access through the Portal Saúde Baseada em Evidências
Dynamed http://portalsaude.saude.gov.br/ Access through the Portal Saúde Baseada em Evidências
Support materials for the visit
Alosa Foundation (United States) http://www.alosafoundation.org/clinical-materials/
Cadadian Agency for Drugs and Technologies in Health – CADTH (Canada)
http://www.cadth.ca/en/resources/academic-detail-toolkit/supporting-information-appendices
RxFiles Academic Detailing Program (Canada)
http://www.rxfiles.ca/rxfiles/modules/druginfoindex/druginfo.aspx Free access to the Newsletter
New York State Prescriber Education Program(United States)
http://nypep.nysdoh.suny.edu/

45
METHODOLOGICAL GUIDELINES
Academic Detailing
APPENDIX 3
Evaluation models of satisfaction of prescribers
Example 1 - Questionnaire prepared for telephone survey
Example 2 – Visual analog scale for satisfaction research applied in the end of the visit

46
METHODOLOGICAL GUIDELINES
Academic Detailing
Source: Jackson SL, Peterson GM, Vial JH. A community-based educational intervention to improve antithrombotic drug use in atrial fibrillation. Ann Pharmacother. 2004 Nov;38(11):1794-9. Epub 2004 Sep 28.