
GTSI Technology Leadership Series From Mobility to Homecare Dr. Mark Blatt Director Healthcare...
51
GTSI Technology Leadership Series From Mobility to Homecare Dr. Mark Blatt Dr. Mark Blatt Director Director Healthcare Industry Healthcare Industry Solutions Solutions Digital Health Group, Digital Health Group, Intel Intel
-
Upload
dominic-marshall -
Category
Documents
-
view
213 -
download
0
Transcript of GTSI Technology Leadership Series From Mobility to Homecare Dr. Mark Blatt Director Healthcare...

GTSI Technology Leadership Series
From Mobility to Homecare
Dr. Mark BlattDr. Mark BlattDirector Director Healthcare Industry SolutionsHealthcare Industry SolutionsDigital Health Group, IntelDigital Health Group, Intel

Agenda
•Mobility Now– Mobile Point of Care Components and Trends– Form Factors to fit Workflows– Model for Measuring Business Value and ROI – Network Design Considerations– Customization vs. Standardization– Use Case Studies
•Homecare: the next frontier Closing Remarks

PROCESS TECHNOLOGY
PEOPLE
Mobile Point of Care (MPoC)Workflow Transformation

MPoC: Five Components to Get to Solution
Right Hardware (w/ refresh roadmap)1
Right Software (needs to fit with workflow/use case)
2
Connectivity (robust network design)3
Integrated Solution (needs to fit with other pieces)
4
Workflow Transformation (people need to use it)
5

Mega-Trend: Extending Wireless Spectrum
Personal Area Network (PAN)
Bluetooth, Wireless
USB
ZigBee
10m/30ft
WiFi: IEEE 802.11a/b/g
Wireless Local Area Network (WLAN)
30m/100ftWireless Wide Area Network (WWAN)
CDMA2000, GPRS, GSM, CDPD, EDGE
100m/330ft max
WiMAX
IEEE 802.16
50km/31m
35km/22mi max
Wireless Medical Telemetry Service (WMTS)
Radio Frequency Identification (RFID)
Varies in Range
Healthcare ‘Shifts-Left’ & goes mobile without boundaries

“Walk Around”‘Grab & Go’ Patient-2-Patient
“Wheel Around”Room-2-Room
“Walk and Dock”Patient Care & Office
Usage Model
Usage Models Drive Design of MPoC Solution

What We Have Heard:Workflow Optimization – Where are the Bottlenecks?
AdmitFrom ER
DischargeAsset Tracking
Medication Management
End of Shift Handover

Mobile Use Cases (what mobility can do at the bedside)
Reference Architectures (available)
1. Vital signs capturing using Bluetooth 2. Vital signs capturing using WiFi3. Image capturing and input into EMR4. RFID for user authentication and Single-Sign On (SSO)5. Care team collaboration (communication using VoIP)6. Patient and medication identification using barcode7. Image (x-ray) review at bedside (PACS)8. Bedside device ordering and patient transport
request9. Blood transfusion verification10. Mobile ePaper11. CPOE at bedside12. Newborn tracking using RFID

Access 2 systems Capture vitals Drawing blood
Charting Nurse data entry Dr. data entry
MPoC in Action

What is the Best Device For My Needs?
Vital sign, I & O entry
Free-format text data-entry
Template data-entry
Mobility
Mobile Clinical Assistant Tablet PC’s Laptop’
s
Large diagnostic images
Medication Administration
Data Inquiry
Manageability
FixedPC’s

Improving Handwriting Recognition
• Improve handwriting recognition results by installing Microsoft Dictionary Tool for Tablet PC (freeware) and importing custom 9,883 Medical Term dictionary (.txt) from Microsoft PowerToys for Windows XP Tablet PC Edition site at:
• URL: http://www.microsoft.com/windowsxp/downloads/powertoys/tabletpc.mspx

eForms and the MCA
Skilled Nursing Visit
Wound Care
Signature Consent
Reimbursement Medical Charge Capture
The synergy of eForms and the MCA can help optimize workflows

Industry-Tested Approach to Identifying Business Value
• Business Value: Improved ability to achieve strategic business objectives
• Improve quality of care, patient safety, staff productivity, revenue, costs…
Business Value Model focuses on monetizable benefits
Business ValueBusiness Value
Increased Revenue (Growth)
Increased Revenue (Growth)
Lower Costs/ Better Efficiency Lower Costs/
Better Efficiency Better Use of
Assets (Productivity)
Better Use of Assets
(Productivity)
= one or more of = one or more of Overtim
e
expenditure
Physicia
n-
patient
rela
tionsh
ip
Time sp
ent
with p
atients
All Benefits
Quantifiable
Monetizable
Not all benefits are quantifiable
Not all quantifiable benefits are monetizable


Quick Summary TCO and ROI for MPOC Workflow At the Royal Salford, UK
•Gross annual savings of £47,000 through >20% time savings in Phlebotomy, £70,000 3yr NPV– Leading to one-year payback
•Equal mix of savings due to productivity and reduction in errors leading to fewer draws– Quality of Care aspect not quantified
•Opportunity to compress Phlebotomy Order Life Cycle leading to Workflow Optimization and further Quality of Care benefits
Salford Phlebotomy MCA Annual Savings
People Material TotalPhlebotomy 2,574 hrs £24,612 £12,355 £36,967Lab 468 hrs £4,475 £6,037 £10,512Total 3,042 hrs £29,086 £18,392 £47,479
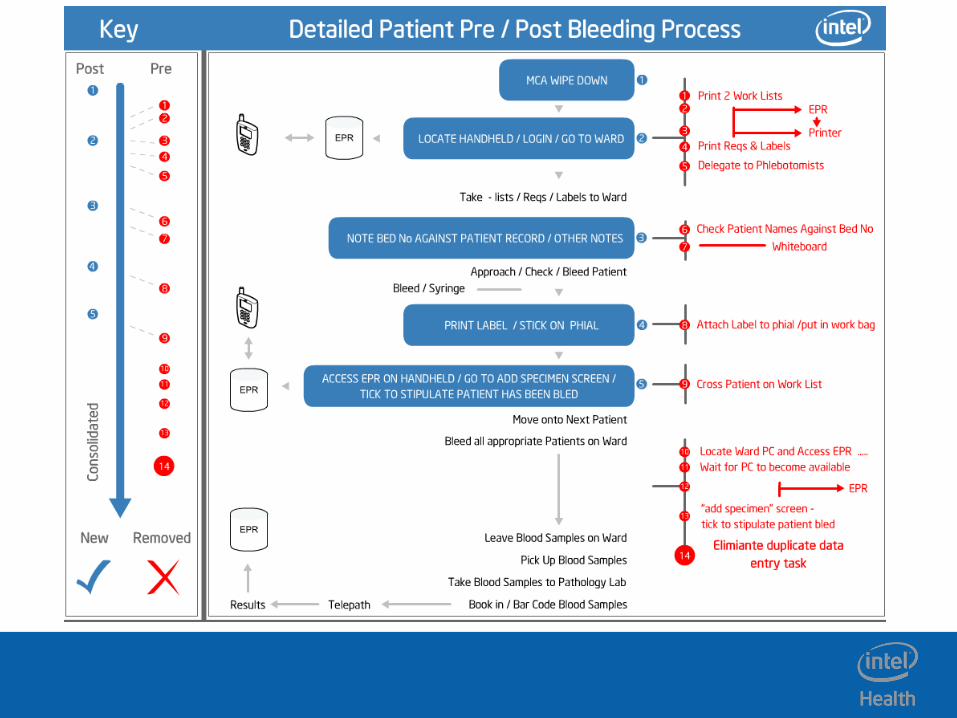

MPOC VM – Workflow Optimization
MPOC Workflow Optimization can• Reduce number of phlebotomists (by 2)• Increase the number of draws by 27-33% (50-60 draws)• Improve capacity management and timeliness of blood draws
- Prior to MCA Deployment- After MCA Deployment

Measuring Up the MCA
The MCA demonstrates results
65% clinician productivity60% clinician productivity
83% manual transcription of patient vital signs
62% clinician productivity
15% productivity and efficiency
25% patient vital sign charting accuracy
Compliance with medication administration guidelines
Source: Intel News Release, Studies Show Mobile Clinical Assistant from Intel and Motion Improves Care Delivery and Clinician Productivity, December 4, 2007

Mobile Technologie
s

Network Design Considerations
•How do you handle multiple devices on the network including personal devices?
•How do you manage to secure your wireless environment?
•How do you create a wireless environment robust enough to handle current and future demands?
•What’s the point of a wireless environment anyway?

When Wireless is Deployed Poorly
•Loss of connectivity – Cold spots -> poor roaming
– Crashed applications and systems -> lower clinical satisfaction
•Low Throughput– Slow system responsiveness
– Application time-out
•Security loop hole– Data theft -> Hospital Liability
Takes very little to frustrate customers

Mobile Usage Model Characteristics
Authentication and Encryption
Application Sensitivity to Latency
Throughput Requirements
Roaming Aggressiveness
Quality of Service
Virtual Private Networking
Remote Manageability
Characteristics
Walk-around Room-to-room
Roaming
Hybrid Room and Office Roaming
Office Roaming
HighLow MediumRelevance to User:
Targeted User
Level of Mobility
Nurse/Clinician/MD MD/SpecialistOffice Worker, or Remote MD
Wheel-around Room-to-room
Roaming
Usage models dictate wireless requirements

Site Survey• Conducted before
deployment and production• Analyzes
– Signal Strength (coverage)– Signal-to-Noise Ratio– Data Rate– Signal Overlap– Signals in a specific
channel– Roaming Prediction
• SW Tools available: – www.ekahau.com– www.airmagnet.com
The most crucial step in a wireless deployment

RF Spectrum NoiseFrequency Source
50/60 Hz All mains powered electrical equipment
~200 kHz Magnetic card security readers
~1 MHz Surgical diathermy (heating tissue via EM induction)
27 MHz Continuous shortwave physiotherapy diathermy
~50 MHz Pagers
~70-200 MHz Ambulance radios
~400 MHz TETRA radios
850, 900, 1800, 1900 MHz
Cell phones (GSM mobile phones)
2.45 GHz Microwave physiotherapy diathermy and microwave ovens, consumer cordless phones, Bluetooth devices, 802.11 b/g
5.0 GHz 802.11 a/n
20 GHz Automatic doorsNumerous sources of electromagnetic interference
exists; site surveys are very critical

Coverage Areas
Common Spaces (for shift changes)
Nurses Station
Building Connectors, Elevators, Staircases
Hallways
Patient Rooms
Key External Spaces
Others:
• OR Theaters
• Waiting rooms
• Cafe/Cafeteria
Follow the workflows to determine coverage areas to provide roaming availability

Customization vs. Standardization
•How much customization do you allow?
•Do you drive for uniformity and standardization or do you support individual customizations?
•When you change one workflow, how does it affect the adjacent workflows?
•Why do we need to address this issue?

As Much As You Can Drink!!!As Much As You Can Drink!!!

MCA in Home CareValue Proposition
• Improved documentation• Quicker time to reimbursement
• Increased patient face time• Lower operational costs
Challenges• Lower and slower
reimbursements due to documentation errors and omissions
• Patient care errors from incomplete information
• Low patient satisfaction due to longer wait times
• POC Documentation• Wireless Access to EMR • E -E Claims Submission• Real Time Dynamic
Scheduling• Task Based Charge Capture
Technology PartnersTechnology Partners
OEM Home Care EMR
eformsInfrastructure

MCA in PharmaValue Proposition
• Research and Development• Clinical Trials
• Sales Force Automation • Lower operational costs
Challenges
• R&D processes costly, slow, often paper based. Real time collaboration less than ideal
• Clinical trails management tools and processes remain manually intensive, costly and slow
• Sales force gets minimal FTF time with clinicians
• R&D Documentation• RT Wireless data synch• Ultra mobile eClincials
documentation • Real Time Dynamic
Scheduling• Improved meds
sampling SCM
Partners
Big Pharma eforms
MCA provides new workflow options for Pharma

Merck: Mobile Convergence Device Project
Background• Heavy reliance on inefficient paper based workflows in evaluated labs
– No access to eNotebook; Risk of contamination from paper
• Prior deployments of mobile technology devices in labs unsuccessful– Opportunity with Intel’s new Mobile Clinical Assistant (MCA) platform and C5 from Motion Computing
Description and Prediction• Hypothesis is that a mobile convergence device will lead to increase in
productivity and optimization of workflows, while reducing data errors and waste when deployed in the research laboratory environment
– Prototyping methodology employed for the project – Time studies were conducted with selected users to develop baselines for evaluation of productivity gains – MCA C5 devices and wireless infrastructure were deployed for use by the test groups– After a period of utilization the time study was repeated to gather updated metrics and process changes– A survey was conducted to gather qualitative data from test users
Outcome• C5 with supporting wireless network proven a success in research
labs– Enables our scientists to focus on value added research work in labs
– Reduces inefficient processes, waste, protocol submission time– 100% electronic records and electronic lab notebook (ELN) integration;
– Increase searchability of researcher data; Maximizes ELN investment– Demand for device exists now and positioned well for future demand

Challenges Facing Research Labs
• Research labs face many inefficiencies because:– No access to eNotebook
within the lab
– Large reliance on paper-based processes
– Limited access to information technology at the bench
– Contamination / Safety Risks

Photo taking
process
Scanning photos process
Biochemistry PCR ProtocolBefore C5
Biochemistry PCR ProtocolBefore C5
Print protocolprocess
Manualcalculation
process
Recopy paperrecords process

Biochemistry PCR ProtocolBefore C5
Biochemistry PCR ProtocolBefore C5
Biochemistry PCR ProtocolAfter C5 with ELN
Biochemistry PCR ProtocolAfter C5 with ELN

Experiment Analysis
ONE PROCESS (PCR Protocol)
Process: Taking picture of amplified gels
Without C5 With C5
1. Retrieve hood/stand for camera
2. Setup hood on light3. Load film into empty
camera4. Mount camera on hood5. Take picture6. Wait for Polaroid to
develop7. Evaluate picture for
shutter quality8. Carry photo to scanner9. Startup software10.Scan picture11.Save image to network
share
1. Take picture of gels with C5
2. Save picture to network share
Single Process: 9 min Single Process: 1.10 min
TOTAL EXP 2:35:00 TOTAL EXP 2:03:00
TIME SAVINGS \ COST AVOIDANCE (Differences)
One FTE Department (20 FTE)Time Savings Cost Avoidance * Time Savings Cost Avoidance *
Day 32 min $40.60 10.67 hrs $811
Week 160 min $203 53.3 hrs $4,051
Month
12 hrs $879 231 hrs $17,583
Year 138 hrs $10,550 2773 hrs $210,998• * Costs assume 46 working weeks per year after vacation/holidays/sick; Employee at $76 per hour• * Costs are based on time differences in order to complete tasks, and does not factor in other hardware/support/supplies
costs
AVERAGE PROTOCOL (ENTIRE PROCESS)
Average amount of time required to sign and submit completed protocol in ELN
Without C5 With C5
2 weeks 1 day

ContaminationMonitoring
Report
Recopy paper results into ELN
Printing / hanging sheets
Referencing sheets
Binding Assay ExperimentBefore C5
Binding Assay ExperimentBefore C5

Binding Assay Experiment Before C5
Binding Assay Experiment Before C5
Binding Assay ExperimentAfter C5 with ELN
Binding Assay ExperimentAfter C5 with ELN

Experiment Analysis
4 PROCESS ANALYSIS
PROCESS Without C5 With C5
Setup experiment
11.32 min 5.33 min
ReferencingProtocols
2.7 min 35 sec
Beta Counter
interactions
7.5 min 1.42 min
Finalize protocol
in ELN
11.37 1 min
4 Processes: 32.89 min
4 Processes: 8.33 min
TOTAL EXP 5:45:00
TOTAL EXP 3:36:00
TIME SAVINGS \ COST AVOIDANCE (Differences)
One FTE Department (20 FTE)Time Savings Cost Avoidance * Time Savings Cost Avoidance *
Day 129 min $163.58 43 hrs $3,271
Week 645 min $818 215 hrs $16,358
Month
46.58 hrs $3,544 931 hrs $70,882
Year 558.96 hrs $42,529 11,179 hrs $850,587• * Costs assume 46 working weeks per year after vacation/holidays/sick; Employee at $76 per hour• * Costs are based on time differences in order to complete tasks, and does not factor in other hardware/support/supplies
costs
AVERAGE PROTOCOL (ENTIRE PROCESS)
Average amount of time required to sign and submit completed protocol in ELN
Without C5 With C5
3 – 4 months 2 daysGOING GREEN – SAVINGS WITH C5
One FTE Department (20 FTE)
Paper Gloves Paper Gloves
Day 9 10
Week
45 50
Month
203 225 4050 4500
Year 2430 2700 48600 sheets
54000

Experiment Analysis
Survey Results• Surveys were deployed to users at
conclusion of pilot– Four users of C5 devices in study surveyed

Top 10 Do’s and Don’ts
Do1. Understand intended use case(s) for going Mobile2. Software and Form factor must fit with intended use case3. Wireless Network must be upgraded for ultra mobile 4. Plan for iterations5. Look for “ripple effects”6. Focus on workflows and how they overlap7. Consider both current and future (unknown) needs8. Seek input from all customers9. Engage executive leadership and governance processes10. Do more!!

Top 10 Do’s and Don’ts
Don’t1. Don't make decisions about workflow just from IT perspective
(include all stakeholders to map priority workflows)2. Don’t try to do this by the “seat of your pants”3. Don’t let IT be the Champion of this effort4. Don’t ignore existent RF devices and patterns5. Don’t forget to make security discussions broad-based6. Don’t forget to broadly survey wireless technologies and their
purported “next steps”7. Don’t ignore your application vendors – engage them early and
often8. Don’t forget to test the technologies with your “stuff”9. Don’t leave SLAs out of your environment and planning10. Don’t avoid asking numerous questions – the answers often
change!

Copyright © 2008, Intel Corporation. All rights reserved.
Intel HealthHomecare: The Next Frontier

What is Telemedicine?Here in Abuja (capital of Nigeria) we have immediate access to a vast amount of medical experts, healthcare education & information, and support from other physicians…How can we take all these resources and share them immediately and effectively with our rural hospitals and clinics?...Telemedicine
Using technology to connect people to healthcare

Telemedicine Models: Improving Access
Clinic Patient Volume
Case
Com
ple
xit
y
Real-time model:•Colds/Flu’s•Diarrhea•Hypertension checkups•AID’s/HIV/Malaria•Maternal/Child health
A differentapproach
Asynchronous model:•Tele-radiology•Tele-pathology•Tele-psychiatry•Tele-ophthalmology
Industry efforts over last 20 years

Homecare: Personal Health Technologies
•PHRs: a good start •Video conferencing (secure video phone)•Remote Sensors •DSS: Patient education and empowerment
•Virtual encounters•Web base Services….
–Reminders –Patient education
•

Promoters

Telemedicine Stages
Non regulated Regulated
Infrastructure Basic Multimedia Virtual CareFace-Face
Multiple Vitals Gathering
Stage 2AV Conferencing
Stage 3V-care Networks
Stage 4
Remote data Gathering by LOB
Stage 1Stage 0
Office may be (electronically) linked to ancillary care providers like lab or pharmacy to get inter-visit data on pts.
May have sensor in pts home (e.g. scale / BP cuff);
Pt sends data & doctor responds.
Structured chat.
May be ICD device that is remotely checked betwn visits
Multiple sensors with integrated data screens
Clinical Decision Support SW ; clinical treatment plans; branching algorithms
Managed by exception: CDM
Patient empowerment with data feedback
Pt education
Sensor standards (Continua)
Increased access to care; Cost avoidance; Improved quality of care
Convenience
Patient data integrated with EMR and PHR
Complex Continua compliant peripherals
Greater scope of remote medical services (PT, OT, Nutritional, Specialty Consults)
Increases access to care, Dramatic cost avoidance (v-care = minimal overhead), improved quality of care
EMR / PHR, integrated w/ labs, pharmacy, radiology, long term care
Improved med adherence; automated refills
Alliances with bricks and mortar systems
E-Commerce
Traditional face to face visits with clinician at the medical mainframe (hospital or clinic)
Follow ups and CDM require repeat return visits
Very little interaction between clinicians and pt between visits

Intel ConfidentialIntel Confidential
Legal Disclaimer
The Intel Health Guide
a) requires a broadband connection in the patient’s home to enable communications with the care team and back-end data hosting;
b) is designed for use by health care professionals and their patients and should only be used under the guidance of a health-care professional;
c) is not intended for emergency medical communications or real-time patient monitoring.

Intel ConfidentialIntel Confidential
Intel® Health Guide
The Intel® Health Guide connects patients and their care teams for personalized care management at home
Intel® Health Guide
Intel® Health Care Management Suite
MedicalPeripherals
Patient EducationalContent

CLOSING REMARKS

Summary
•Mobility in healthcare matters (more and more)
•Mobile Workflow transformation requires:– Clear understanding of the preexisting workflows– Clear vision of what you are trying to accomplish– Strong stakeholder involvement; pick the right
processes; pick the best technologies
•Homecare and virtual encounters are coming– Rising costs and growing issues with access will
demand new care delivery models

Q&A
Dr. Mark BlattDr. Mark BlattDirector Director Healthcare Industry SolutionsHealthcare Industry SolutionsDigital Health Group, IntelDigital Health Group, Intel


















