Growing number of seniors caring for other · PDF fileGrowing number of seniors caring for...
42
Growing number of seniors caring for other seniors By MATT SEDENSKY January 6, 2014 10:30 AM In this Nov. 21, 2013 photo, caregiver Warren Manchess, left, laughs with Paul Gregoline and Paul's wife, Mary, as they work on a puzzle, in Noblesville Ind. Burgeoning demand for senior services like home health aides is being met by a surprising segment of the workforce: Other seniors. Twenty-nine percent of so-called direct-care workers are projected to be 55 or older by 2018 and in some segments of that population older workers are the single largest age demographic. With high rates of turnover, home care agencies have shown a willingness to hire older people new to the field who have found a tough job market as they try to supplement their retirement income.(AP Photo/Darron Cummings) NOBLESVILLE, Ind. (AP) — Paul Gregoline lies in bed, awaiting the helper who will get him up, bathed and groomed. He is 92 years old, has Alzheimer's disease and needs a hand with nearly every task the day brings. When the aide arrives, though, he doesn't look so different from the client himself — bald and bespectacled. "Just a couple of old geezers," jokes Warren Manchess, the 74-year-old caregiver.
Transcript of Growing number of seniors caring for other · PDF fileGrowing number of seniors caring for...

Growing number of seniors caring for other seniors
By MATT SEDENSKY January 6, 2014 10:30 AM
In this Nov. 21, 2013 photo, caregiver Warren Manchess, left, laughs with Paul Gregoline and
Paul's wife, Mary, as they work on a puzzle, in Noblesville Ind. Burgeoning demand for senior
services like home health aides is being met by a surprising segment of the workforce: Other
seniors. Twenty-nine percent of so-called direct-care workers are projected to be 55 or older by
2018 and in some segments of that population older workers are the single largest age
demographic. With high rates of turnover, home care agencies have shown a willingness to hire
older people new to the field who have found a tough job market as they try to supplement their
retirement income.(AP Photo/Darron Cummings)
NOBLESVILLE, Ind. (AP) — Paul Gregoline lies in bed, awaiting the helper who will get him
up, bathed and groomed. He is 92 years old, has Alzheimer's disease and needs a hand with
nearly every task the day brings. When the aide arrives, though, he doesn't look so different from
the client himself — bald and bespectacled.
"Just a couple of old geezers," jokes Warren Manchess, the 74-year-old caregiver.

As demand for senior services provided by nurses' aides, home health aides and other such
workers grows with the aging of baby boomers, so are those professions' employment of other
seniors. The new face of America's network of caregivers is increasingly wrinkled.
Among the overall population of direct-care workers, 29 percent are projected to be 55 or older
by 2018, up from 22 percent a decade earlier, according to an analysis by the Paraprofessional
Healthcare Institute, or PHI, a New York-based nonprofit advocating for workers caring for the
country's elderly and disabled. In some segments of the workforce, including personal and home
care aides, those 55 and older are the largest single age demographic.
"I think people are surprised that this workforce is as old as it is," said Abby Marquand, a
researcher at PHI. "There's often people who have chronic disease themselves who have to
muster up the energy to perform these really physically taxing caregiving needs."
Manchess came out of retirement to work for Home Instead Senior Care after caring for his
mother-in-law, who, too, had Alzheimer's and whom he regarded as his hero. The experience,
though taxing, inspired his new career.
Three days a week, he arrives at Gregoline's house, giving the retired electrician's wife a needed
break. He carefully shaves and dresses his client, prepares breakfast and lunch, cleans the house
and quickly remedies any accidents. He does the laundry and swaddles Gregoline in a warm
towel from the dryer, reads him the sports page to keep him updated on his beloved Bears and
sometimes pulls out dominoes or puzzles to pass the time.
Gregoline is rather sedate this afternoon, relaxing in his favorite chair while occasionally
offering glimpses of his trademark wit. Asked if he remembered anything about the Army, he
says: "It was a bitch!" Offered the chance to go outside, he responds: "No! I'll freeze my ass off
out there!" Describing an abrasive personality of long ago, he offers: "He followed me around
like a bad conscience."
Manchess has worked for Gregoline for about a year, and the men are at ease around each other.
Past aides to Gregoline have been in their 20s, but Manchess says he thinks his age is an asset.
"Age can be an advantage," he said, pointing to the common conversation points and life
experience, including his own health troubles and aches and pains that can come with age. "We
hit it off pretty well. Maybe I didn't seem to be too much out of the ordinary."
Around the country, senior service agencies are seeing a burgeoning share of older workers.
About one-third of Home Instead's 65,000 caregivers are over 60. Visiting Angels, another in-
home care provider, says about 30 percent of its workers are over 50. And at least one network,
Seniors Helping Seniors, is built entirely on the model of hiring older caregivers.
Like most occupations, some of the growth in older caregivers is driven by the overall aging of
the population and the trend of people working later in life. But with incredibly high rates of
turnover and a constant need for more workers, home care agencies have also shown a

willingness to hire older people new to the field who have found a tough job market as they try
to supplement their retirement income.
The jobs are among the fastest-growing positions in the U.S., but are also notoriously physically
demanding, with low pay and high rates of injury. Manchess has had spinal surgery and says he's
especially careful when vacuuming. He's not sure how many years he'll be able to continue this
work, and he acknowledges it can be tough.
"Halfway through my shift, I'm a little weary myself," he said. "It takes its toll."
Manchess had worked as an Air Force pilot, then in real estate, then as a school bus driver,
before becoming a professional caregiver. As Gregoline contentedly nibbles on his ham
sandwich, Manchess wraps up his shift, turning reflective when considering his life's careers.
"I think this is about as rewarding, if not more rewarding, than any of them," he said.
___
Matt Sedensky, an AP reporter on leave, is studying aging and workforce issues as part of a one-
year fellowship at the AP-NORC Center for Public Affairs Research, which joins NORC's
independent research and AP journalism. The fellowship is funded by the Alfred P. Sloan
Foundation and supported by APME, an association of AP member newspapers and broadcast
stations.
___
Follow Matt Sedensky on Twitter at http://twitter.com/sedensky
EDITOR'S NOTE _ Aging America is a joint AP-APME project examining the aging of the
baby boomers and the impact that this so-called silver tsunami has had on society
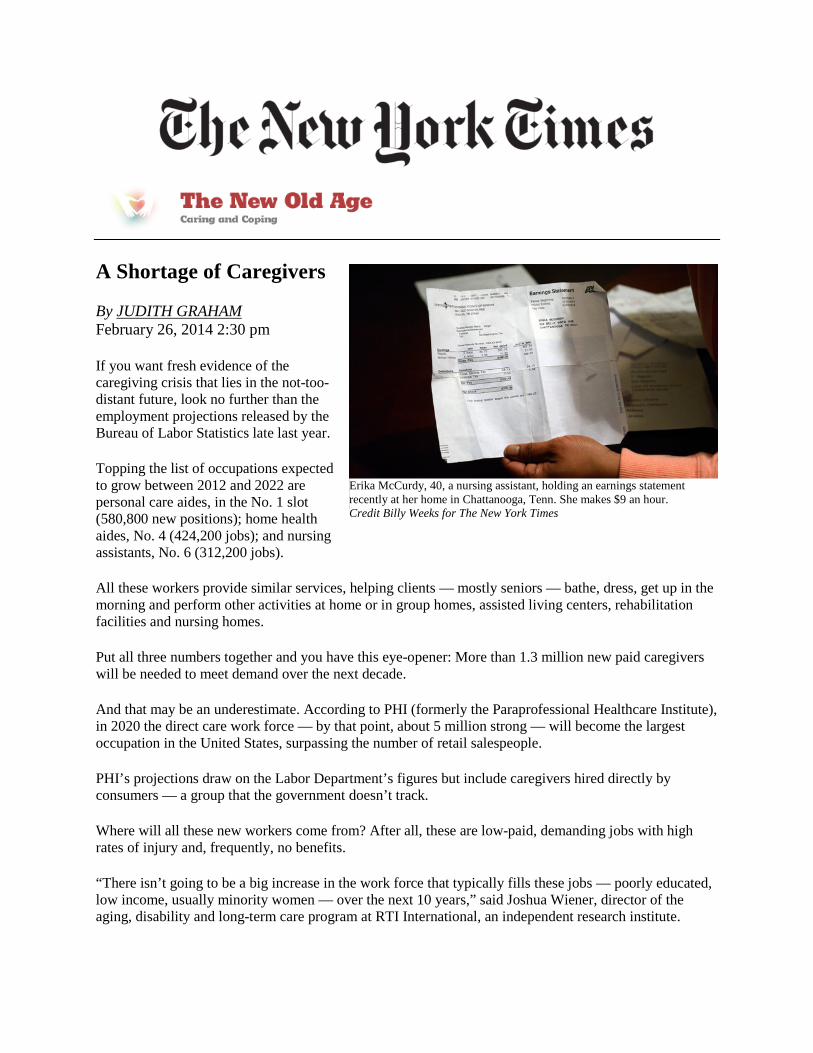
Erika McCurdy, 40, a nursing assistant, holding an earnings statement recently at her home in Chattanooga, Tenn. She makes $9 an hour. Credit Billy Weeks for The New York Times
A Shortage of Caregivers
By JUDITH GRAHAM February 26, 2014 2:30 pm
If you want fresh evidence of the caregiving crisis that lies in the not-too-distant future, look no further than the employment projections released by the Bureau of Labor Statistics late last year.
Topping the list of occupations expected to grow between 2012 and 2022 are personal care aides, in the No. 1 slot (580,800 new positions); home health aides, No. 4 (424,200 jobs); and nursing assistants, No. 6 (312,200 jobs).
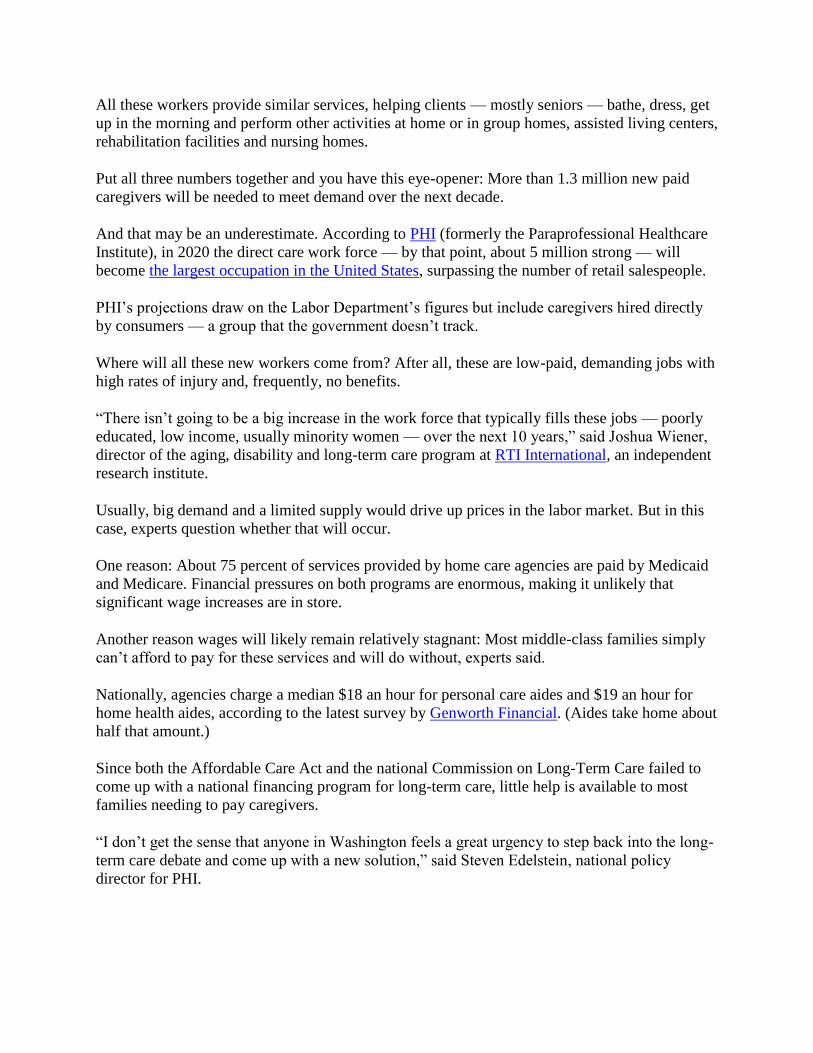
All these workers provide similar services, helping clients — mostly seniors — bathe, dress, get up in the morning and perform other activities at home or in group homes, assisted living centers, rehabilitation facilities and nursing homes.
Put all three numbers together and you have this eye-opener: More than 1.3 million new paid caregivers will be needed to meet demand over the next decade.
And that may be an underestimate. According to PHI (formerly the Paraprofessional Healthcare Institute), in 2020 the direct care work force — by that point, about 5 million strong — will become the largest occupation in the United States, surpassing the number of retail salespeople.
PHI’s projections draw on the Labor Department’s figures but include caregivers hired directly by consumers — a group that the government doesn’t track.
Where will all these new workers come from? After all, these are low-paid, demanding jobs with high rates of injury and, frequently, no benefits.
“There isn’t going to be a big increase in the work force that typically fills these jobs — poorly educated, low income, usually minority women — over the next 10 years,” said Joshua Wiener, director of the aging, disability and long-term care program at RTI International, an independent research institute.

Usually, big demand and a limited supply would drive up prices in the labor market. But in this case, experts question whether that will occur.
One reason: About 75 percent of services provided by home care agencies are paid by Medicaid and Medicare. Financial pressures on both programs are enormous, making it unlikely that significant wage increases are in store.
Another reason wages will likely remain relatively stagnant: Most middle-class families simply can’t afford to pay for these services and will do without, experts said.
Nationally, agencies charge a median $18 an hour for personal care aides and $19 an hour for home health aides, according to the latest survey by Genworth Financial. (Aides take home about half that amount.)
Since both the Affordable Care Act and the national Commission on Long-Term Care failed to come up with a national financing program for long-term care, little help is available to most families needing to pay caregivers.
“I don’t get the sense that anyone in Washington feels a great urgency to step back into the long-term care debate and come up with a new solution,” said Steven Edelstein, national policy director for PHI.
What can be done about the impending caregiver crisis? Organizations that represent direct care workers argue that these jobs need to be made more attractive with better supervision and training, more opportunities for advancement, and, yes, higher wages.
The Labor Department’s decision last fall to extend the federal Fair Labor Standards Act to direct care workers — a move that guarantees them minimum wage and overtime pay — is “a step in the right direction” but it doesn’t go far enough, Mr. Edelstein said.
“The direction of Medicaid policy is to provide more services to frail seniors in the home and fewer in institutions,” he said. Yet this won’t be possible unless steps are taken to create a more stable, better trained work force.
Filling paid caregiving jobs with immigrants is another option — indeed, already one in five direct care workers today is foreign born. But there is strong political opposition to increased immigration, which may limit the number of potential caregivers. Cultural and language differences can also complicate the caregiving relationship.
Lynn Feinberg, a senior strategic policy adviser at AARP, has two interesting suggestions. Family members who had previously looked after loved ones could be recruited and trained to become paid caregivers, she proposed. Or retired nurses, social workers and other health care professionals could be encouraged to see this as valuable part-time work once their full-time careers are over.

Opportunity’s knocks Tereza Sedgwick is seeing the economy from the bottom up, where the fastest-growing job in America is also one of the hardest. Written by Eli Saslow Photos by Sarah L. Voisin Published on May 31, 2014
MARIETTA, Ohio — She had made it as far as the career school's parking
lot for the December training class and the February class, only to drive away each time
in a tangle of anxiety and self-doubt. Now it was March, and here Tereza Sedgwick came
again: dressed in the mandatory class uniform of red-and-black scrubs, a lit cigarette
dangling in her fingers out the busted window of her '88 Plymouth. She parked in the lot
and watched a procession of unemployed workers enter the school building in
southeastern Ohio, trying to will herself to join them.
A steady accumulation of losses brought Tereza Sedgwick to the only house she could
afford, an abandoned farm building with meager heat and sporadic electricity. There
was her layoff from a furniture factory; the expiration of her unemployment insurance
after 66 weeks; the eviction from her one-bedroom apartment; the loss of her cable TV,
her cellphone and 50 pounds to stress. She had stayed at friends’ houses with her son,
Sebastian, and worked whatever hours the local McDonald’s would give her. But before
long she had exhausted her savings and her friends’ patience.
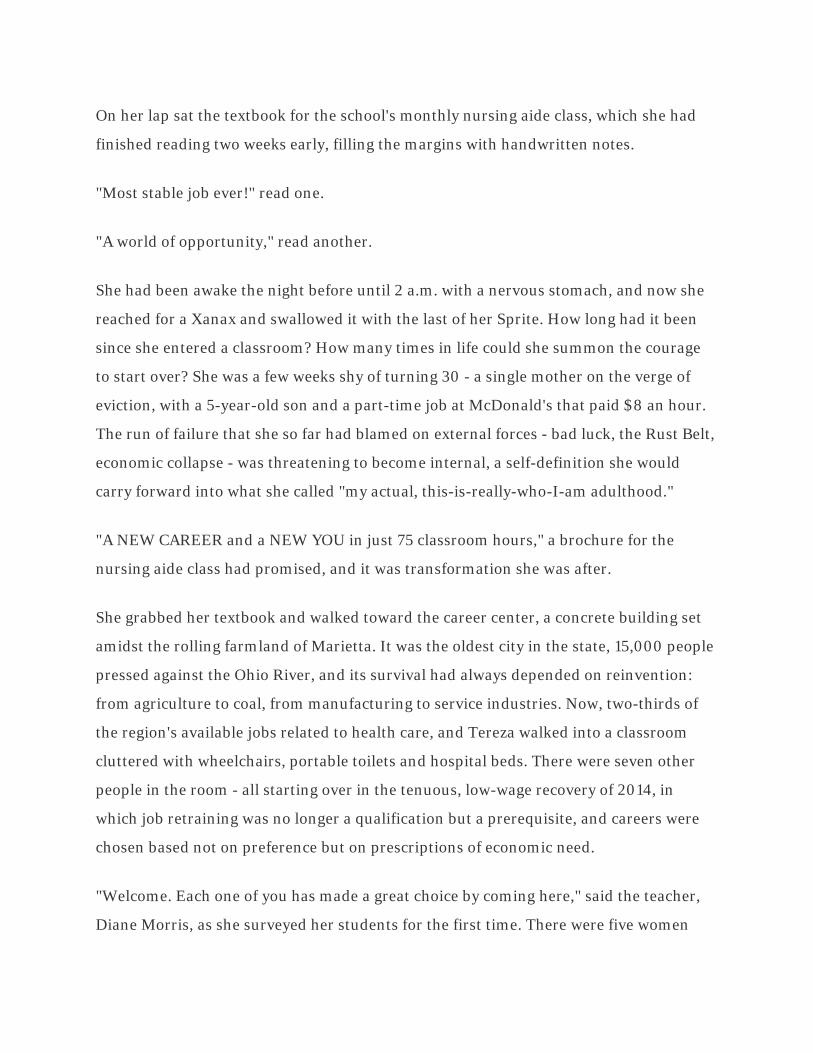
On her lap sat the textbook for the school's monthly nursing aide class, which she had
finished reading two weeks early, filling the margins with handwritten notes.
"Most stable job ever!" read one.
"A world of opportunity," read another.
She had been awake the night before until 2 a.m. with a nervous stomach, and now she
reached for a Xanax and swallowed it with the last of her Sprite. How long had it been
since she entered a classroom? How many times in life could she summon the courage
to start over? She was a few weeks shy of turning 30 - a single mother on the verge of
eviction, with a 5-year-old son and a part-time job at McDonald's that paid $8 an hour.
The run of failure that she so far had blamed on external forces - bad luck, the Rust Belt,
economic collapse - was threatening to become internal, a self-definition she would
carry forward into what she called "my actual, this-is-really-who-I-am adulthood."
"A NEW CAREER and a NEW YOU in just 75 classroom hours," a brochure for the
nursing aide class had promised, and it was transformation she was after.
She grabbed her textbook and walked toward the career center, a concrete building set
amidst the rolling farmland of Marietta. It was the oldest city in the state, 15,000 people
pressed against the Ohio River, and its survival had always depended on reinvention:
from agriculture to coal, from manufacturing to service industries. Now, two-thirds of
the region's available jobs related to health care, and Tereza walked into a classroom
cluttered with wheelchairs, portable toilets and hospital beds. There were seven other
people in the room - all starting over in the tenuous, low-wage recovery of 2014, in
which job retraining was no longer a qualification but a prerequisite, and careers were
chosen based not on preference but on prescriptions of economic need.
"Welcome. Each one of you has made a great choice by coming here," said the teacher,
Diane Morris, as she surveyed her students for the first time. There were five women
and two men, ranging in age from 19 to 50. Morris asked them to introduce themselves
and explain their interest in the class.
"I was told by my mom, 'Get a job or move out,' " said one, a laid-off factory worker.
"The only job openings I saw were in this."
"This is my second go-round in this class," said another, a former cafeteria worker. "I'm
just trying to pass."
Morris turned to Tereza, who was twirling a pencil through the blonde highlights in her
bangs. She knew little about health care beyond its abundant job openings, and she had
difficulty with math and a phobia for needles. But she had gone three years without full-
time work, and she liked the idea of caring for people. She had a framed picture of her
son attached to her key chain and tattoos on her arms symbolizing peace and love.
Maybe in this career, she thought, compassion and eagerness would be qualification
enough.
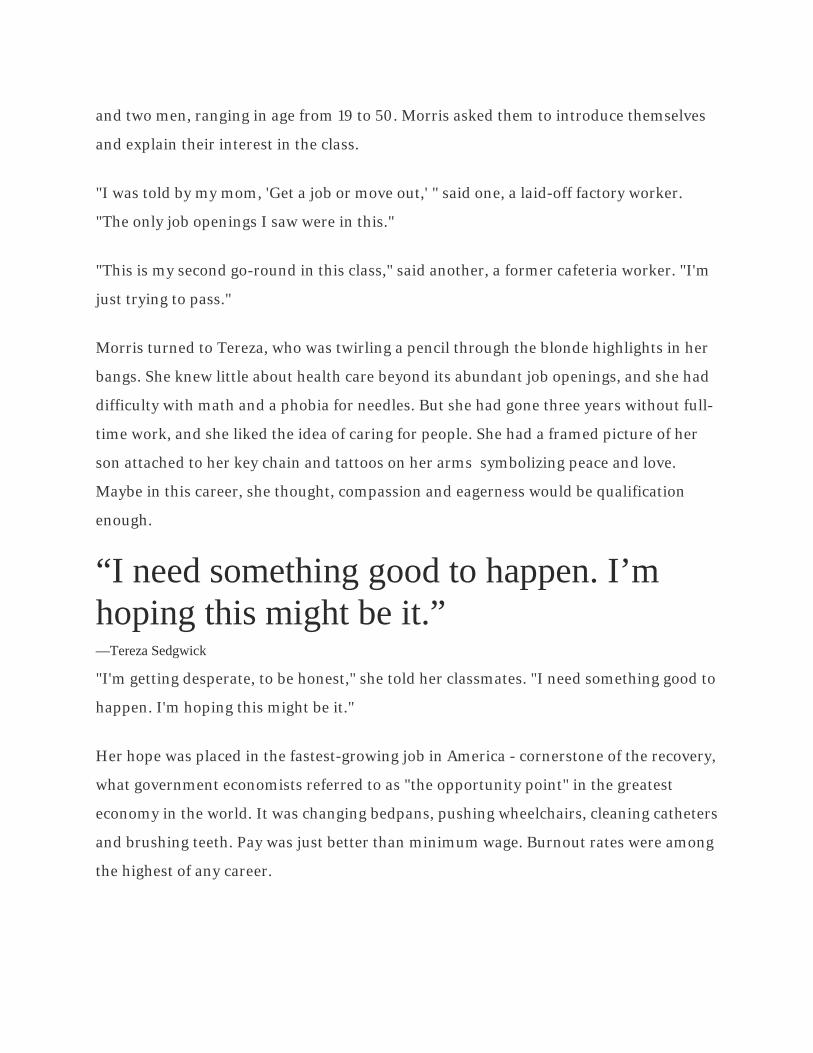
“I need something good to happen. I’m hoping this might be it.” —Tereza Sedgwick
"I'm getting desperate, to be honest," she told her classmates. "I need something good to
happen. I'm hoping this might be it."
Her hope was placed in the fastest-growing job in America - cornerstone of the recovery,
what government economists referred to as "the opportunity point" in the greatest
economy in the world. It was changing bedpans, pushing wheelchairs, cleaning catheters
and brushing teeth. Pay was just better than minimum wage. Burnout rates were among
the highest of any career.
This was how the economy looked from the bottom up in 2014: the fastest-growing job
was also among the hardest, and the place of opportunity was in fact the place of last
resort.
"What Does It Mean To Be A Nurse Aide?" read the cover of the first class handout, and
Tereza flipped the page to see a series of charts. The number of Americans age 65 and
older was expected to double by 2050, to more than 84 million. That meant double the
nursing homes, double the hospice personnel and double the home health agencies.
"Need: Urgent," the handout read.
"Necessary work experience: None."
"Necessary skills: None."
Underneath the charts Tereza saw a series of pictures that showed a smiling young
woman feeding, washing, and checking the vital signs of an elderly patient. "This is
basically what I already do for my son," Tereza said, feeling encouraged, and then she
flipped to the next page, which listed signs of "caregiver stress" that nurse aides
sometimes experience in their first year of work: Tension headaches. Teeth grinding.
Reckless driving. Apathy. Depression. Fits of anger.
"On the way home from work, try to focus on one good thing that occurred during the
day," the handout suggested.
Tereza closed the pamphlet and followed her classmates to a sink at the back of the
room for their first lesson, a tutorial on hand washing. One student rolled his eyes and
another played chess on her cellphone, but Tereza jotted notes. The proper hand wash
involved 15 distinct skills, Morris said. Each skill would be graded as part of a test the
next morning. Their two-week course consisted of one week in the classroom and
another spent working at a nursing home. Students needed an average grade of 80
percent to pass the class and receive their state certification. "If you get to that point,
you'll have a job for as long as you want it," Morris told them as she dried her hands.
"Congratulations on joining the health-care movement," she said.
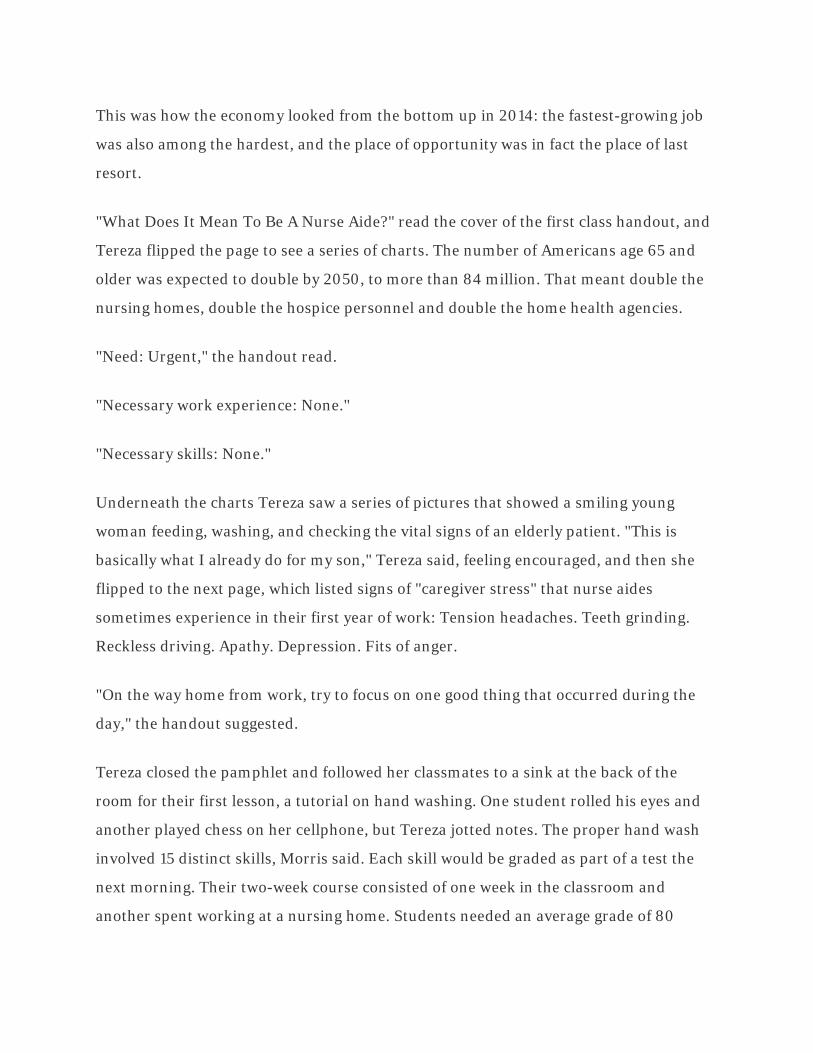
Tereza Sedgwick in the kitchen of her Bartlett, Ohio, home. Living in a borrowed house with no water, she
uses tap water from jugs for brushing teeth and other chores.
A job of last resort
It had never occurred to Tereza that she would be congratulated, because nothing that
brought her into the class had seemed like an accomplishment, or even a choice.
The past several years had amounted to a steady accumulation of losses - her layoff from
a furniture factory; the expiration of her unemployment insurance after 66 weeks; the
eviction from her one-bedroom apartment; the loss of her cable TV, her cellphone and
50 pounds to stress. She had stayed at friend's houses with her son, Sebastian, and
worked whatever hours the local McDonald's would give her. But before long she had

exhausted her savings and her friends' patience, so she moved into the only house she
could afford, an abandoned farm building with meager heat and sporadic electricity.
Only then had she gone to her mother to ask for help. And only then had her mother,
Carol, who had spent the past decade helping, offered one final lifeline. Yes, she would
allow Sebastian to live with her for two weeks so Tereza could focus exclusively on
passing the nursing aide class. Yes, she would lend Tereza the $600 enrollment fee out
of Sebastian's college account.
“Where Carol had seen a world made up of things to take, Tereza was mostly preoccupied with hanging on – to jobs that never lasted, to men who never lasted, to the bottom rung of a middle class that wasn’t lasting, either.” "Your 5-year-old is paying for this," Carol had told her, in case the stakes weren't already
clear enough. "If you fail, you're failing him."
Tereza had never been apart from Sebastian for more than a few days. He was her
Valentine's Day baby, the one happy result of an abusive relationship, and she had his
birth date tattooed across the back of her neck. But now, after her first day of class, she
dropped him off with a small duffel bag at her mother's house. Carol was inside, already
sorting through classified advertisements for nurse aide jobs. "You should start applying
for some of these tomorrow," she told Tereza.
"I haven't even passed the class yet," Tereza said.
"You will," Carol said.
"How do you figure?" Tereza said. "Haven't you been watching me these last 10 years?"

Carol's optimism came from her own experience a generation before, when she had been
a little like Tereza - adrift a decade after high school, spending everything she earned
waiting tables, wanting better. She had enrolled in a career school and taken its most
popular class, Introduction to Computers, and soon she was writing code, programming
and graduating from college.
It was the early 1980s, the beginning of the tech boom, and it felt to Carol like life was all
promise, everything hers to take. She accepted a job at General Electric and bought a
three-story house on the Ohio River. She wanted a daughter, so she searched
international adoption catalogues until she found a picture of a 6-year-old girl at an
orphanage in Brazil. The girl stared straight into the camera, with beautiful, searching
eyes and a weary grin. Here was someone with whom Carol could share so much
possibility. She purchased a plane ticket to Rio, submitted the adoption paperwork and
brought the girl home.
All these years later, that girl was still searching, still weary, and Carol had spent a
lifetime trying to help her fulfill the promise that once seemed so assured. But where
Carol had seen a world made up of things to take, Tereza was mostly preoccupied with
hanging on - to jobs that never lasted, to men who never lasted, to the bottom rung of a
middle class that wasn't lasting, either.
Carol had bought Tereza a car, lent her money and finally introduced her to the Marietta
career school. "This is the kind of place where I got started," she had told Tereza,
encouraging her to follow suit by also signing up for her generation's version of the most
popular class. It wasn't computers, and it wasn't the tech boom. But it was something.

Sedgwick gives her 5-year-old son, Sebastian, a kiss while buying a new phone.
"This could be your start," Carol said now, walking with Sebastian back into her house.
Tereza said goodbye to her son and drove alone to the place she was starting from - out
of the city, off the highway, over a hill and onto a 35-acre farm owned by a guy she had
known in high school. The Plymouth rattled over the potholed dirt road, and the engine
belched smoke whenever she took it over 50, but somehow the car still ran. "Tough like
me," she said, patting her hand against the dashboard. She drove past a farmhouse and
parked in front of a small wooden building that her high school classmate had lent to
her for free. Three cow skulls hung on a tree near the door, and the porch smelled like
the goats and alpacas that had been there before.
Her mom hated to visit the place, but Tereza didn't mind it. There was a horse to ride
and a lake to swim in. She had strung Christmas lights in Sebastian's bedroom and

taped eight rolls of car-themed wrapping paper into an oval on his ceiling. Maybe if she
turned his room into a racetrack, she thought, he would never notice the flies or the
leaking roof.
The latest problem was that her classmate wanted the building back, and he had cut off
the water to make the point. Tereza and Sebastian were showering at friends' houses
and going to the bathroom outside, and now she began to worry about something else:
Her hand-washing test. It was the next day. How could she practice?
She walked to a neighbor's and filled gallon jugs with water, carrying them back into a
house where nothing was simple. She tipped a jug onto the counter so water ran over
her hands, and then she began to follow the steps she had written in her notes.
"Wet hands."
"Interlace fingers."
"Rinse until no longer contaminated."

Students with watches take the teacher's pulse in a Marietta, Ohio, training class for nurse aides. At left, a student checklist for completing a nursing procedure hangs on the classroom wall. The nation's need for caretakers is expected to explode as the number of Americans age 65 or older doubles by 2050.
A million regrets
Their exams covered hand washing, hair care, making a bed and bathroom etiquette -
two or sometimes three tests each day, 50 questions per test. By the time the students
reached the last exam of their first week, emptying a urinary bag, they had begun to seek
out distractions. One drummed heavy-metal songs with his fingers against the desk.
Another sank into a wheelchair used for training and tried to fall asleep. "Wake me up
when I'm in a different career," he said.
When Morris scanned her students during lectures, eager for eye contact, only Tereza
looked up from her incessant note-taking. "I hear you," she said, again and again,
although her exam grades had begun to suggest otherwise: 67, 91, 82, 68. She completed
additional homework for extra credit. She continued to wear her mandatory uniform
even after other students had gone to sweatpants and torn baseball hats. She dutifully
kept a list in her notebook of vocabulary terms: "voiding" rather than peeing;
"incontinent garments" instead of diapers.
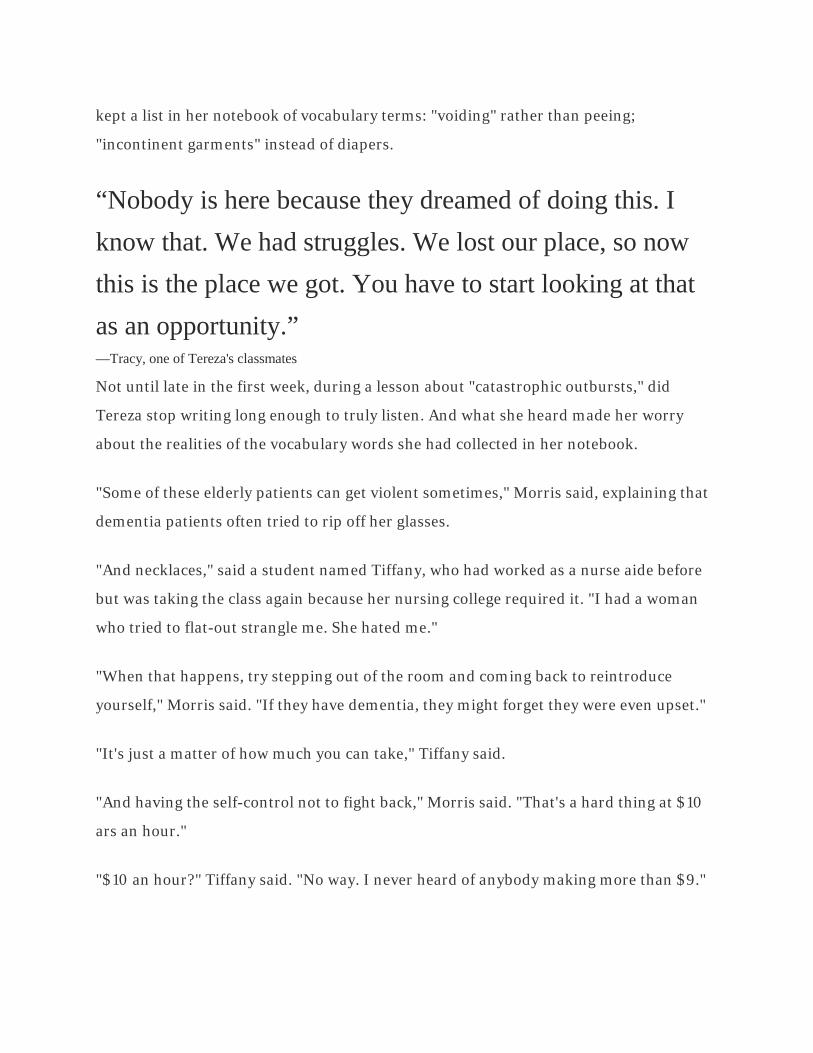
“Nobody is here because they dreamed of doing this. I know that. We had struggles. We lost our place, so now this is the place we got. You have to start looking at that as an opportunity.” —Tracy, one of Tereza's classmates
Not until late in the first week, during a lesson about "catastrophic outbursts," did
Tereza stop writing long enough to truly listen. And what she heard made her worry
about the realities of the vocabulary words she had collected in her notebook.
"Some of these elderly patients can get violent sometimes," Morris said, explaining that
dementia patients often tried to rip off her glasses.
"And necklaces," said a student named Tiffany, who had worked as a nurse aide before
but was taking the class again because her nursing college required it. "I had a woman
who tried to flat-out strangle me. She hated me."
"When that happens, try stepping out of the room and coming back to reintroduce
yourself," Morris said. "If they have dementia, they might forget they were even upset."
"It's just a matter of how much you can take," Tiffany said.
"And having the self-control not to fight back," Morris said. "That's a hard thing at $10
ars an hour."
"$10 an hour?" Tiffany said. "No way. I never heard of anybody making more than $9."

Morris gave the students a 20-minute lunch break, and Tereza walked outside carrying a
bag of Funyuns and a pack of cigarettes. "What am I doing here?" she wondered. She
thought about going to the front office and asking for a refund. In 35 minutes she could
be at her mom's house, lying with Sebastian and escaping into cartoons. She tried to
light a cigarette, but her hand was shaking. "Damn it," she said, and she started to cry.
She felt a hand on her back and turned to see one of her classmates standing ready with
a lighter. It was Tracy, a mother of two from West Virginia. "Tell me what's wrong,
honey," she said.
"It's probably fail or quit, so I'm going to quit," Tereza said.
Tracy reached into her car for a bologna sandwich and handed Tereza half. She was 44
years old and she knew what it felt like to fail and to quit, which was why she was setting
her alarm for 4 each morning to drive 75 miles through the mountains to class, hoping a
graduation certificate might help her reclaim something of herself.
She had withered within a bad marriage for a decade until her husband grew audacious
enough to move his latest in a series of girlfriends into the family house, and Tracy, with
no place else to go, consented to move into that girlfriend's unoccupied trailer. "The old
switcheroo," Tracy had called it then, and in the trade she forfeited her husband, her
self-esteem and the respect of her 17-year-old daughter.
Now, each day in class, Tracy was taking cellphone pictures of her test scores - 100, 92,
97 - and sending them to her daughter, who was suddenly responding to her mother's
texts more quickly. "So freaking proud!" she had responded once, and Tracy had held up
her phone to show the message to the entire class.
"Let me ask you something," she said now, to Tereza. "Do you have any regrets? 'Cause I
have a lot."
"Yeah. About a million."

"Do you want quitting this class to be another?"
Tereza didn't answer, and Tracy stepped closer. "Nobody is here because they dreamed
of doing this," she said. "I know that. We had struggles. We lost our place, so now this is
the place we got. You have to start looking at that as an opportunity."
"I'm looking at it as bathing people, cleaning them up," Tereza said.
Tracy checked her watch. Their break was over. The teacher was about to hand out
another test. "It's all about mind-set," she said, turning toward the school. "You
coming?"
Tereza shook her head and lit another cigarette. She took a long drag and watched the
smoke spill from her mouth.
"How am I ever going to do this job?" she said, but then she stamped out the cigarette
and headed back to class.

Sedgwick puts her head down in class after working at a nursing home during the day.
After a few days on the job, she became the only student that the patients requested by
name.
Battling for five bites
A few days later, as the second week of class began, Tereza walked inside a nursing
home for the first time. She had tucked an anti-anxiety pill into her pocket and tied her
hair into a bun. She put on surgical gloves and pinned a name tag to the breast of her
rewashed scrubs.
“She knew what it was like to be fragile. To be alone ... During her difficult first year in the U.S., she sometimes thought about the last words she had heard in Portuguese, from a priest at the orphanage. ‘Can’t you see this is good luck?’ the priest had told her. ‘America.’” "Welcome to the most desirable nursing facility in the Ohio River Valley," Karen Metz,
the training supervisor, said to the students during their initial tour. She explained that
their job for the next week was to act as "guardian angels" for the 86 residents of
Harmar Place - to bathe and feed them, to keep them comfortable and calm.
"If you're lucky, these are the things you'll soon be getting paid to do," Metz said,
knowing that Harmar Place itself had three openings, at $8.35 an hour.
She told the students their first task would also be the most simple: delivering and
feeding breakfast. She handed Tereza a plastic tray loaded with cereal, bananas and
yogurt and directed her to a room at the end of the hallway, pulling back a curtain to
reveal a woman lying flat on the mattress, her face turned to the wall. "Advanced
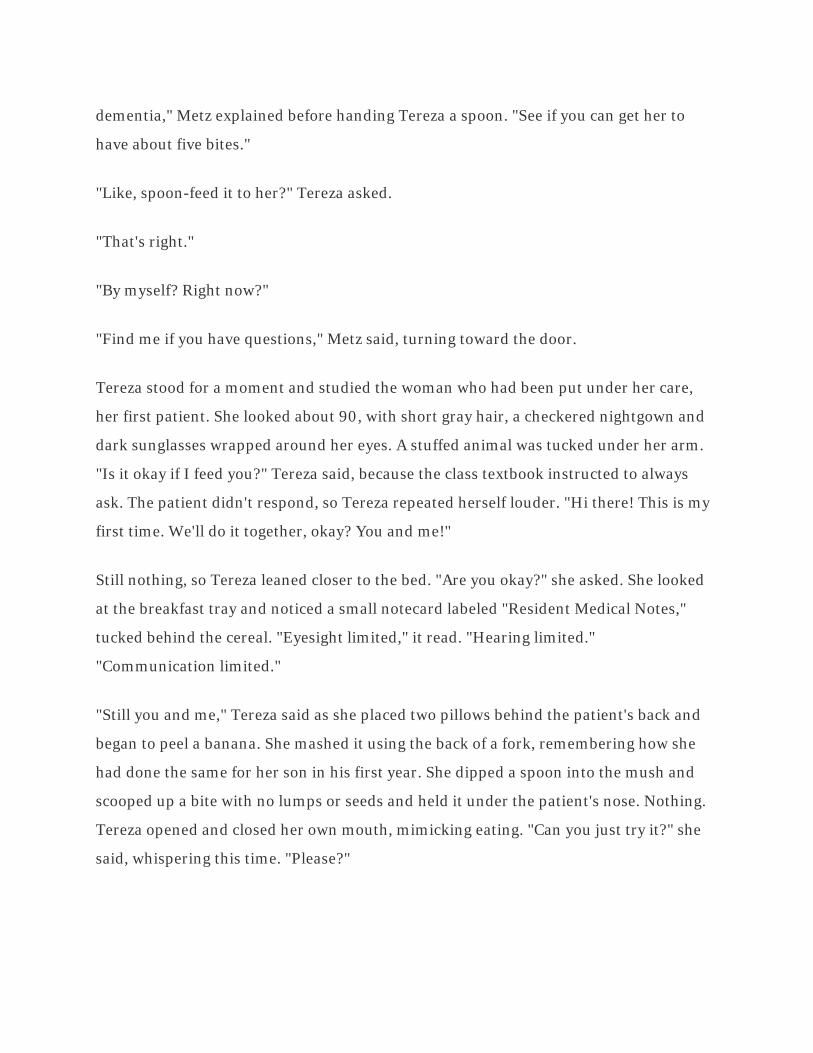
dementia," Metz explained before handing Tereza a spoon. "See if you can get her to
have about five bites."
"Like, spoon-feed it to her?" Tereza asked.
"That's right."
"By myself? Right now?"
"Find me if you have questions," Metz said, turning toward the door.
Tereza stood for a moment and studied the woman who had been put under her care,
her first patient. She looked about 90, with short gray hair, a checkered nightgown and
dark sunglasses wrapped around her eyes. A stuffed animal was tucked under her arm.
"Is it okay if I feed you?" Tereza said, because the class textbook instructed to always
ask. The patient didn't respond, so Tereza repeated herself louder. "Hi there! This is my
first time. We'll do it together, okay? You and me!"
Still nothing, so Tereza leaned closer to the bed. "Are you okay?" she asked. She looked
at the breakfast tray and noticed a small notecard labeled "Resident Medical Notes,"
tucked behind the cereal. "Eyesight limited," it read. "Hearing limited."
"Communication limited."
"Still you and me," Tereza said as she placed two pillows behind the patient's back and
began to peel a banana. She mashed it using the back of a fork, remembering how she
had done the same for her son in his first year. She dipped a spoon into the mush and
scooped up a bite with no lumps or seeds and held it under the patient's nose. Nothing.
Tereza opened and closed her own mouth, mimicking eating. "Can you just try it?" she
said, whispering this time. "Please?"
Braden Hewitt, 19, shaves John Childress during student training with residents of the Harmar Place nursing home in Marietta.
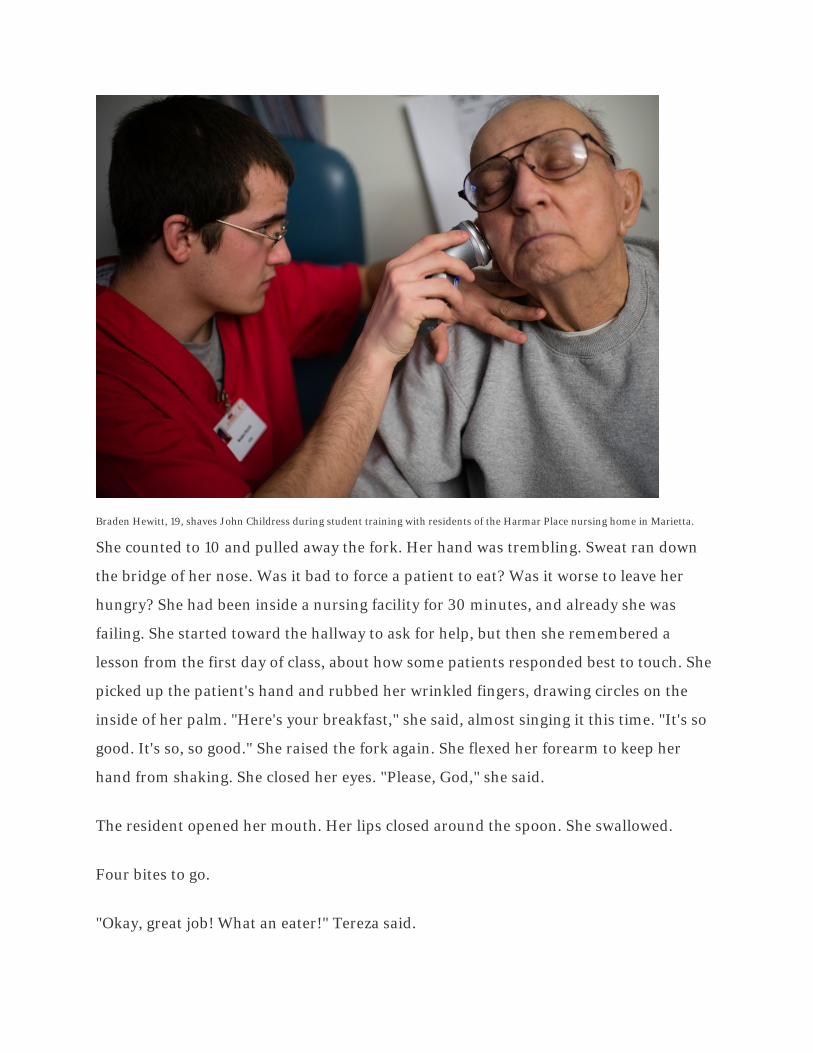
She counted to 10 and pulled away the fork. Her hand was trembling. Sweat ran down
the bridge of her nose. Was it bad to force a patient to eat? Was it worse to leave her
hungry? She had been inside a nursing facility for 30 minutes, and already she was
failing. She started toward the hallway to ask for help, but then she remembered a
lesson from the first day of class, about how some patients responded best to touch. She
picked up the patient's hand and rubbed her wrinkled fingers, drawing circles on the
inside of her palm. "Here's your breakfast," she said, almost singing it this time. "It's so
good. It's so, so good." She raised the fork again. She flexed her forearm to keep her
hand from shaking. She closed her eyes. "Please, God," she said.
The resident opened her mouth. Her lips closed around the spoon. She swallowed.
Four bites to go.
"Okay, great job! What an eater!" Tereza said.
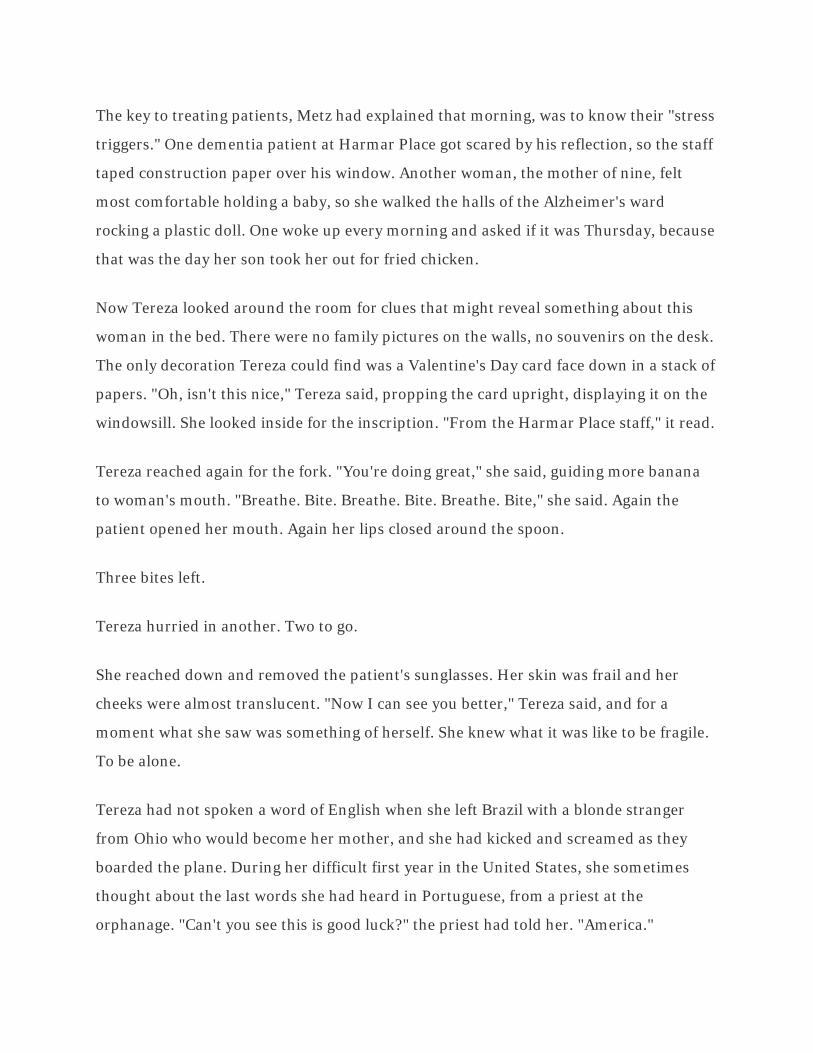
The key to treating patients, Metz had explained that morning, was to know their "stress
triggers." One dementia patient at Harmar Place got scared by his reflection, so the staff
taped construction paper over his window. Another woman, the mother of nine, felt
most comfortable holding a baby, so she walked the halls of the Alzheimer's ward
rocking a plastic doll. One woke up every morning and asked if it was Thursday, because
that was the day her son took her out for fried chicken.
Now Tereza looked around the room for clues that might reveal something about this
woman in the bed. There were no family pictures on the walls, no souvenirs on the desk.
The only decoration Tereza could find was a Valentine's Day card face down in a stack of
papers. "Oh, isn't this nice," Tereza said, propping the card upright, displaying it on the
windowsill. She looked inside for the inscription. "From the Harmar Place staff," it read.
Tereza reached again for the fork. "You're doing great," she said, guiding more banana
to woman's mouth. "Breathe. Bite. Breathe. Bite. Breathe. Bite," she said. Again the
patient opened her mouth. Again her lips closed around the spoon.
Three bites left.
Tereza hurried in another. Two to go.
She reached down and removed the patient's sunglasses. Her skin was frail and her
cheeks were almost translucent. "Now I can see you better," Tereza said, and for a
moment what she saw was something of herself. She knew what it was like to be fragile.
To be alone.
Tereza had not spoken a word of English when she left Brazil with a blonde stranger
from Ohio who would become her mother, and she had kicked and screamed as they
boarded the plane. During her difficult first year in the United States, she sometimes
thought about the last words she had heard in Portuguese, from a priest at the
orphanage. "Can't you see this is good luck?" the priest had told her. "America."
She mashed more banana and loaded it onto the spoon. One bite left. "Terrific," she
said. "Really terrific."
She looked out the window and fanned herself with a plastic plate. How long had this
breakfast lasted? Fifteen minutes? An hour? She could see a bench out there, and birds,
and a maple tree with sunlight shining through its newly green leaves. "I would kill for a
cigarette," she said. Why did it feel so hot in this room? Why was it so hard to breathe?
"Almost done," she said. "Almost almost almost done." She filled the spoon one last
time. She rubbed the patient's palm. She coaxed in another bite.
"Five!" she said, standing up to stretch her back. In two hours, she would come back to
feed this patient a snack. In three and a half hours, she would be back again for lunch.
She took out a pen and wrote a note on the patient's chart.
"Five bites," she wrote. "Great breakfast!"
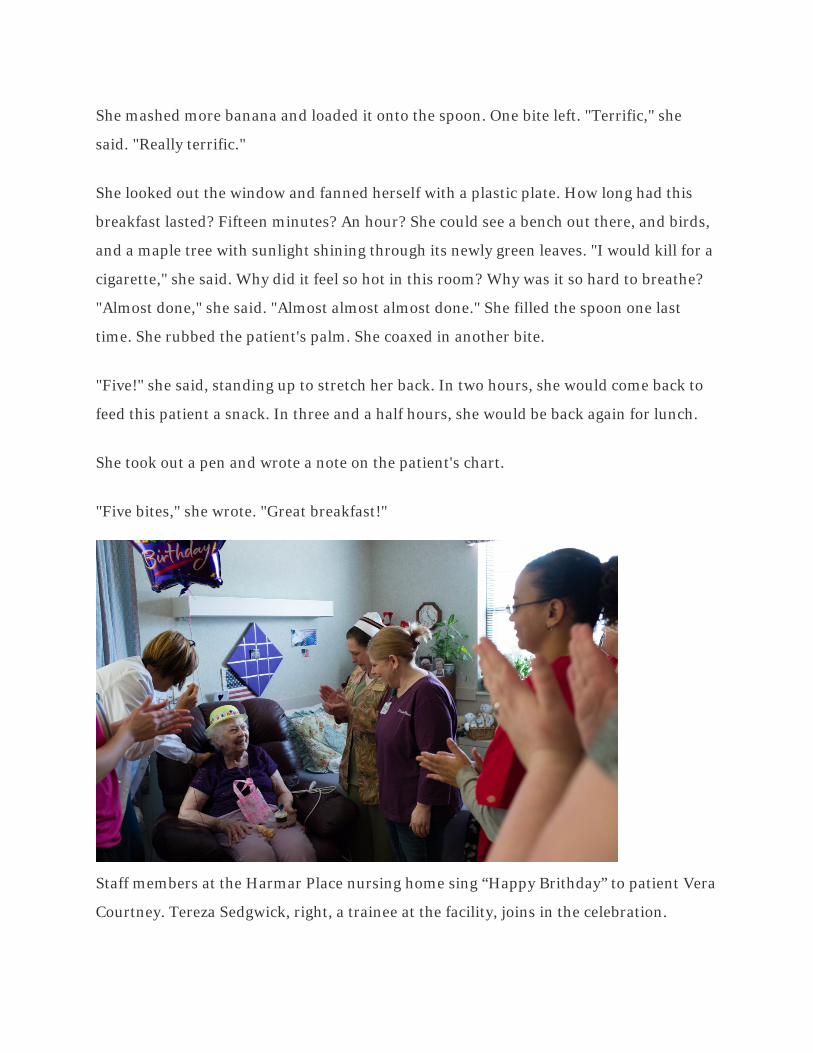
Staff members at the Harmar Place nursing home sing “Happy Brithday” to patient Vera
Courtney. Tereza Sedgwick, right, a trainee at the facility, joins in the celebration.
A system serving no one well
After a few days at the nursing home, Tereza had become the only student whom
patients requested by name. She asked to hear the stories behind family pictures on
their walls, and she remembered who liked ice cream and who preferred pudding. A
Harmar Place supervisor began following her during rounds with a clipboard, evaluating
her for a full-time position. "She's green," the supervisor said. "But she's learning."
Tereza, though, was still preoccupied with all she didn't know. What was the code again
to unlock the linen closet? Was that high-pitched noise a routine call button or an
emergency alarm? "Why can't I ever locate a pulse?" she said, one day, searching the
wrist of a motionless resident for so long she began to wonder if he might be dead. "Is it
possible?" she said. "Dead?" The patient opened his eyes. "No," he said. "Not possible."
She returned home each night with sore legs and bloodshot eyes, but she could never
stop thinking about the job long enough to rest. Her skin reeked of antiseptic. She
stayed awake and imagined the patients alone in their rooms, the medical equipment
blinking in the dark, the hallways quiet. She wondered what beds she might find empty
when she returned in the morning.
"I can't wait to be done," she said a few days before graduation as she began to fill out a
Harmar Place job application. She sped through the form until she reached the last line.
"Requested start date," it read, and she left question blank. She put the application in
the glove box of her car, to complete another day. She started extending her smoke
breaks from three minutes to five, and then from five to 10, until her supervisors
wondered where she had gone.
"There isn't a Florence Nightingale in the bunch," said Morris, the classroom teacher,
when she visited the nursing home one morning to observe the students' work. One had
forgotten to wear gloves during a bed bath, risking infection for the patient. Another had
been soaked by urine while cleaning a catheter and then stormed off, leaving the patient
unattended.
None of them were fully prepared. Of that much Morris was sure. "We crammed six
months of work into 75 hours," she said, and she had spent the last days wondering
whom this training system served. The students, who would make $8 an hour in jobs
they weren't prepared for? Their future employers, who would be hiring novice workers?
The 72 million aging Americans, who would spend their last years living through these
caretakers' mistakes?
"What can I do?" Morris said, and she had already made up her mind. She had another
class to teach in a few days, and then another after that. America's elderly needed
caretakers. America's unemployed needed jobs.
Tracy Doll, 42, of Middlebourne, W.Va., left, cries after calling her daughter to say she had earned her certificate.

At right, Sedgwick celebrates with fellow students Tiffany Riggs, left, and Braden Hewitt after completing the course.
She passed the student who had forgotten to wear his gloves.
She passed the student who had stormed out on a resident.
She passed Tracy with a grade of 103.5 percent, and Tracy took photos of her certificate
and called her daughter, who answered on the first ring. "You won't believe this," Tracy
told her.
And she passed Tereza, just barely, giving her the absolute minimum score necessary to
graduate: 80 percent, buoyed significantly by extra credit.
"I made it?" Tereza asked.
"You did," Morris said.
"So, I can use this to go out and get a job?" Tereza said.

"You can," Morris said.
Tereza stared at her certificate, looking from her printed name to her grade, from her
name to her grade.
"Did I deserve this, or did you, like, give it to me?" she asked.
"What do you think?" Morris said, gathering up her papers, heading toward the door.
"I don't know," Tereza said, and by the time she looked up she was alone in the room.
Outside the house where she grew up in Little Hocking, Ohio, Tereza Sedgwick shows her mother, Carol Sedgwick,
and her son Sebastian, 5, her new nurse aide certificate.
The meaning of success
Her mother, Carol, wanted to celebrate. "Please?" she asked, so Tereza agreed to meet
her at Golden Corral. Carol had spent the afternoon calling relatives to tell them about
Tereza's graduation, and she raised her water glass to offer a toast. "The health-care
field is so great," she said. "To new beginnings. To you, for making us all so proud."
Tereza wondered if her mother's exuberance was partly for show - an attempt at
generosity, maybe, or desperation to see her daughter claim some small piece of the
promise she remembered from long ago. Either way, Tereza decided her version of
generosity would be to let the moment last. She set her graduation certificate on the
table. She raised her own glass to meet her mother's. "Thanks for everything," she said.
"You really did it," Carol said. "You passed."
"Thanks," Tereza said, even though what she was thinking to herself was, so did
everybody else.
"You learned a new career in two weeks!" Carol said. "And all these years you've been
saying you can't learn."
The fastest-growing job is also among the hardest, and the place of opportunity is in fact
the place of last resort.
"I guess this time I got it," Tereza said, but in fact she was thinking about the 80 percent
and all of that extra credit.
"And you'll be making good money."
"Uh-huh," she said, remembering the teacher's advice on the last day, about how to
answer questions on job applications about salary requirements by writing either
"Flexible" or "Minimum Wage."
"And you're going to be taking care of people, making their lives better."
"Uh-huh," she said again, thinking about the patient she had fed that morning, a man
with dementia who, after eating a few bites of mashed peas, gently placed his trembling
hand on her wrist and said he would shove the spoon down her throat if she fed him one
more bite.
"You're on a great track," Carol said.
Tereza nodded, but she couldn't stop thinking about where that track led. Even if she got
a job and worked full time, her income would still qualify her for food stamps. She
would still be unable to afford her own apartment. She would likely burn out before she
saved up any money. Within a year, most nurse aides return to the ranks of the
unemployed, back into the economic churn, choosing uncertainty over the one certain
career in a low-wage recovery.
Carol stood from the table and handed Tereza back her class certificate. "Hang this up
somewhere, okay?" she said, and Tereza drove home with Sebastian and took the
certificate inside. She placed it on a shelf above the sink that didn't run, but then
changed her mind. She carried it into her bedroom, but what was the point in hanging it
where no one else could see it? She brought it back into the living room, where most of
her belongings were already packed into garbage bags, ready for an eviction that was
only days away.
"Do I really want to look at this thing every day?" she said, pressing her hand against the
certificate's edge, feeling its texture against her fingertips.
She was already staring into a future that the certificate foretold. That seemed like more
than enough. She tucked the certificate into her textbook and dropped it into a drawer.

Letters to the Editor
With the proper support, direct-care work can be a job with a future
June 4
The June 1 front-page article “ ‘We lost our place, so now this is the place we got’ ”
painted a stark picture of a common reality of direct-care occupations — nursing
assistants, home health aides and personal-care aides. While these are “jobs of the
future,” given the United States’ rapidly aging population, we invest too little as a
nation, in terms of training and wages, to ensure a sufficiently skilled and
compassionate workforce.
The federal training requirements for nursing assistants remain unchanged after 30
years despite a nursing home population that is older, frailer and more likely to be living
with dementia. And there are no federal training standards for personal-care aides, who,
in many states, provide care in people’s homes without any preparation or on-site
supervision. Little wonder that new workers lack confidence and turnover is high.
Direct care is challenging, but it can also be rewarding, offering workers a chance to
make a difference in someone’s life. If we care about building the workforce we need
with the qualities we want for our grandparents, our parents and ourselves, it is time to
improve training, increase wages and provide opportunities for advancement for direct-
care workers. With greater public investment in direct-care jobs, these occupations
could be a real career opportunity for women like Tereza Sedgwick — as technology was
for her mother — providing a pathway to a stable and fulfilling life.
Jodi M. Sturgeon, New York
The writer is president of the Paraprofessional Healthcare Institute.

Opinion: Home-care workers deserve better Published: June 11, 2014 4:57 PM
By JODI M. STURGEON AND CHRISTINE L. OWENS
Home health aide. (Credit: iStock)
This month marks the seventh anniversary of the U.S. Supreme Court decision in a case brought by Evelyn Coke, a home-care worker who sought payment of back wages from her former East Meadow employer for unpaid overtime. The court upheld the U.S. Department of Labor's regulatory authority to exclude Coke and other home-care workers from federal minimum wage and overtime protections, under a decades-old exemption to the Fair Labor Standards Act. Today, 2 million home-care aides are excluded from these basic federal labor protections.
Fortunately, the Obama administration has addressed this injustice. After years of review by the Labor Department, including lengthy public comment, a revision to the rule was published in October that will at long last grant federal labor protections to this vast and rapidly growing workforce.
But while most regulations take effect 30 or 60 days after being published, the implementation of the revised "companionship exemption" was delayed for 15 months. The intention was to allow

stakeholders time to budget for modest cost increases to cover overtime pay and on-the-job travel time.
Now the National Association of Medicaid Directors, a voluntary professional association of state Medicaid directors, is requesting an additional 18-month delay to further consider the regulations' impact. That would mean a nearly 3-year wait since the regulation was published for these low-wage employees to achieve the basic labor protections afforded nearly every other worker in the country.
Home-care aides deserve better. Almost entirely a workforce of women -- predominantly women of color -- these workers have for far too long been asked to sacrifice their own incomes to hold down the cost of home-care services. Earning, on average, less than $10 an hour, often at part-time jobs, about half of the workforce must rely on public benefits to support their families.
At a time when many agree that the federal minimum wage is insufficient, home-care workers aren't guaranteed even that basic wage floor. And few home-care workers receive employer-sponsored health coverage or paid sick leave.
Consumers deserve better, too. Eventually most of us will need home-care services for someone we love or ourselves. At that moment, we discover how much we value the skills and compassion these aides bring to their work. But low wages mean the industry is plagued by high turnover. The worker coming to care for your mother or grandmother has most likely been on the job less than a year. And just as you get to know her, she may leave for a better-paying job, with less stress, at the local mall.
About 10,000 baby boomers turn 65 each day. Our nation will need more than a million additional home-care aides over the next decade to meet their demands for home care. Providing basic labor protections is essential to building the workforce we need.
The estimated cost of extending Fair Labor Standards Act protections -- minimum wage, overtime pay and compensation for on-the-job travel time -- to our home-care workforce is manageable: The Labor Department projects it to be just one-10th of 1 percent of the industry's $90 billion in annual revenues.
State Medicaid programs should move quickly to adapt to the new regulations. If we want and expect quality home care for every American who needs it, we can't wait any longer to take this first step to improve the quality of home-care jobs.
Jodi M. Sturgeon of Huntington is president of the Paraprofessional Healthcare Institute.
Christine L. Owens is executive director of the National Employment Law Project.

Promised Labor Protections for Home Care Workers in Jeopardy
June 13, 2014
Jodi Sturgeon
This week marks the seventh anniversary of the 2007 U.S. Supreme Court decision Coke vs.
Long Island Care at Home. In that case, Evelyn Coke, a Jamaican immigrant who had been a
home care worker for over two decades, sought payment of back wages from her employer for
unpaid overtime.
Ms. Coke lost her case. The Court upheld the U.S. Department of Labor’s regulatory authority to
exclude Ms. Coke and countless other home care workers from federal minimum wage and
overtime protections, under a decades-old exemption to the Fair Labor Standards Act (FLSA).
Today, like the late Ms. Coke, 2 million home care aides are still excluded from these basic
federal labor protections. That means, even if the campaign to raise the federal minimum wage to
$10.10 an hour is successful, home care aides could be left out.
Fortunately, the Obama Administration has made it a priority to address this injustice. The
administration has published a revised rule that essentially ends the exclusion of home care aides
from federal labor laws beginning January 1, 2015. After decades of organizing and advocacy,
home care workers will finally be recognized for the important work that they do each day
assisting individuals who, due to age or disability, need some extra help to live independently in
their communities.
But there is a hitch. The opposition to this rule change is pushing for it to be delayed another 18
months. That would be almost three years from the time the rule was published in October
2013—whereas most rules take effect in just 30 to 60 days.
The administration purposefully delayed implementation for 15 months to give states—which
fund most home care services through their Medicaid programs—time to adjust their budgets to
accommodate the modest costs associated with this change. Further delay is unconscionable.
Home care aides deserve better. They have waited long enough to be recognized for the vital role
they play in our system of eldercare and disability services.
Almost entirely a workforce of women, predominantly women of color, home care workers have
for far too long been asked to sacrifice their own incomes to hold down the cost of home care
services. Earning, on average, less than $10/hour, often at part-time jobs, about half of the

workforce must rely on public benefits to support their own families. To put it simply, this is
not fair.
Consumers deserve better, too.
The poor quality of these jobs affects us all. Eventually we will need home care services for
someone we love or ourselves. At that point, a reliable, skilled caregiver is the most valuable
person on earth. Juggling eldercare and childcare, jobs and after-school programs, volunteer
work and friends—it’s more than most of us can do alone. A quality paid caregiver relieves us of
the constant stress and worry that we can’t “do it all.” Whether the person we love and care for
lives halfway across the country, or town, home care aides are a lifeline. They provide the peace
of mind we all crave.
But finding aides like Evelyn Coke—those who continue to serve their clients in spite of the low
wages—is difficult because most home care aides cannot afford to stay in this occupation.
The industry is plagued by low retention and high turnover. The worker coming to care for your
mother or grandmother has most likely been on the job less than one year. And just as you get to
know her, she may leave for a better paying job, with less stress and risk of injury, at the local
mall.
Rising demand makes it essential that we move to stabilize and grow the home care workforce
today. Providing basic labor protections is an essential first step. Make sure President Obama
carries through on his commitment to home care workers and the families that rely on them. Ask
the Department of Labor to stand firm—and to begin enforcing minimum wage and overtime
protections for the home care workforce on January 1, 2015. Take action today.

February 26, 2014, 2:30pm
A Shortage of Caregivers
By JUDITH GRAHAM
Erika McCurdy, 40, a nursing assistant, holding an earnings statement recently at her home in
Chattanooga, Tenn. She makes $9 an hour.
If you want fresh evidence of the caregiving crisis that lies in the not-too-distant future, look no
further than the employment projections released by the Bureau of Labor Statistics late last year.
Topping the list of occupations expected to grow between 2012 and 2022 are personal care aides,
in the No. 1 slot (580,800 new positions); home health aides, No. 4 (424,200 jobs); and nursing
assistants, No. 6 (312,200 jobs).
All these workers provide similar services, helping clients — mostly seniors — bathe, dress, get
up in the morning and perform other activities at home or in group homes, assisted living centers,
rehabilitation facilities and nursing homes.
Put all three numbers together and you have this eye-opener: More than 1.3 million new paid
caregivers will be needed to meet demand over the next decade.
And that may be an underestimate. According to PHI (formerly the Paraprofessional Healthcare
Institute), in 2020 the direct care work force — by that point, about 5 million strong — will
become the largest occupation in the United States, surpassing the number of retail salespeople.
PHI’s projections draw on the Labor Department’s figures but include caregivers hired directly
by consumers — a group that the government doesn’t track.
Where will all these new workers come from? After all, these are low-paid, demanding jobs with
high rates of injury and, frequently, no benefits.
“There isn’t going to be a big increase in the work force that typically fills these jobs — poorly
educated, low income, usually minority women — over the next 10 years,” said Joshua Wiener,
director of the aging, disability and long-term care program at RTI International, an independent
research institute.
Usually, big demand and a limited supply would drive up prices in the labor market. But in this
case, experts question whether that will occur.
One reason: About 75 percent of services provided by home care agencies are paid by Medicaid
and Medicare. Financial pressures on both programs are enormous, making it unlikely that
significant wage increases are in store.
Another reason wages will likely remain relatively stagnant: Most middle-class families simply
can’t afford to pay for these services and will do without, experts said.
Nationally, agencies charge a median $18 an hour for personal care aides and $19 an hour for
home health aides, according to the latest survey by Genworth Financial. (Aides take home about
half that amount.)
Since both the Affordable Care Act and the national Commission on Long-Term Care failed to
come up with a national financing program for long-term care, little help is available to most
families needing to pay caregivers.
“I don’t get the sense that anyone in Washington feels a great urgency to step back into the long-
term care debate and come up with a new solution,” said Steven Edelstein, national policy
director for PHI.

What can be done about the impending caregiver crisis? Organizations that represent direct care
workers argue that these jobs need to be made more attractive with better supervision and
training, more opportunities for advancement, and, yes, higher wages.
The Labor Department’s decision last fall to extend the federal Fair Labor Standards Act to
direct care workers — a move that guarantees them minimum wage and overtime pay — is “a
step in the right direction” but it doesn’t go far enough, Mr. Edelstein said.
“The direction of Medicaid policy is to provide more services to frail seniors in the home and
fewer in institutions,” he said. Yet this won’t be possible unless steps are taken to create a more
stable, better trained work force.
Filling paid caregiving jobs with immigrants is another option — indeed, already one in five
direct care workers today is foreign born. But there is strong political opposition to increased
immigration, which may limit the number of potential caregivers. Cultural and language
differences can also complicate the caregiving relationship.
Lynn Feinberg, a senior strategic policy adviser at AARP, has two interesting suggestions.
Family members who had previously looked after loved ones could be recruited and trained to
become paid caregivers, she proposed. Or retired nurses, social workers and other health care
professionals could be encouraged to see this as valuable part-time work once their full-time
careers are over.

FAMILY ECONOMIC SECURITY
Promised Labor Protections for Home Care Workers in Jeopardy June 13, 2014
Jodi Sturgeon This week marks the seventh anniversary of the 2007 U.S. Supreme Court decision Coke vs. Long Island Care at Home. In that case, Evelyn Coke, a Jamaican immigrant who had been a home care worker for over two decades, sought payment of back wages from her employer for unpaid overtime.
Ms. Coke lost her case. The Court upheld the U.S. Department of Labor’s regulatory authority to exclude Ms. Coke and countless other home care workers from federal minimum wage and overtime protections, under a decades-old exemption to the Fair Labor Standards Act (FLSA).
Today, like the late Ms. Coke, 2 million home care aides are still excluded from these basic federal labor protections. That means, even if the campaign to raise the federal minimum wage to $10.10 an hour is successful, home care aides could be left out.
Fortunately, the Obama Administration has made it a priority to address this injustice. The administration has published a revised rule that essentially ends the exclusion of home care aides from federal labor laws beginning January 1, 2015. After decades of organizing and advocacy, home care workers will finally be recognized for the important work that they do each day assisting individuals who, due to age or disability, need some extra help to live independently in their communities.
But there is a hitch. The opposition to this rule change is pushing for it to be delayed another 18 months. That would be almost three years from the time the rule was published in October 2013—whereas most rules take effect in just 30 to 60 days.
The administration purposefully delayed implementation for 15 months to give states—which fund most home care services through their Medicaid programs—time to adjust their budgets to accommodate the modest costs associated with this change. Further delay is unconscionable.

Home care aides deserve better. They have waited long enough to be recognized for the vital role they play in our system of eldercare and disability services.
Almost entirely a workforce of women, predominantly women of color, home care workers have for far too long been asked to sacrifice their own incomes to hold down the cost of home care services. Earning, on average, less than $10/hour, often at part-time jobs, about half of the workforce must rely on public benefits to support their own families. To put it simply, this is not fair.
Consumers deserve better, too.
The poor quality of these jobs affects us all. Eventually we will need home care services for someone we love or ourselves. At that point, a reliable, skilled caregiver is the most valuable person on earth. Juggling eldercare and childcare, jobs and after-school programs, volunteer work and friends—it’s more than most of us can do alone. A quality paid caregiver relieves us of the constant stress and worry that we can’t “do it all.” Whether the person we love and care for lives halfway across the country, or town, home care aides are a lifeline. They provide the peace of mind we all crave.
But finding aides like Evelyn Coke—those who continue to serve their clients in spite of the low wages—is difficult because most home care aides cannot afford to stay in this occupation.
The industry is plagued by low retention and high turnover. The worker coming to care for your mother or grandmother has most likely been on the job less than one year. And just as you get to know her, she may leave for a better paying job, with less stress and risk of injury, at the local mall.
Rising demand makes it essential that we move to stabilize and grow the home care workforce today. Providing basic labor protections is an essential first step. Make sure President Obama carries through on his commitment to home care workers and the families that rely on them. Ask the Department of Labor to stand firm—and to begin enforcing minimum wage and overtime protections for the home care workforce on January 1, 2015. Take action today.
TakeAction Stand Up For Basic Worker Protections!
MomsRising.org strongly encourages our readers to post comments in response to blog posts. We value diversity of opinions and perspectives. Our goals for this space to be educational, thought-provoking, and respectful. So, we actively moderate comments and we reserve the right to edit or remove comments that undermine these goals. Thanks!

Jodi M. Sturgeon President, Paraprofessional Healthcare Institute (PHI)
Better Jobs for Direct-Care Workers Help All Working Families Posted: 06/23/2014 12:57 pm EDT Updated: 06/23/2014 12:59 pm EDT
This week the White House convenes its Summit on Working Families -- shining light on the needs of America's working women and the challenges they face managing jobs, raising children and caring for aging parents.
Regional events leading up to the summit have primarily focused on professional, middle-class women. But changes are needed for the millions of American women who work in low-wage jobs that provide little financial security for themselves or their families. One example is providers of direct care: nurse aides, home health aides and personal care aides who provide hands-on care to our nation's growing population of elders and people with disabilities.
These are among the nation's fastest-growing jobs with direct-care workers expected to number nearly 5 million by 2022 -- more than nurses, school teachers and all public safety workers. Nearly 90 percent of direct-care workers are women.
Unfortunately, while plentiful, these jobs are not the quality jobs that American workers need. With median wages near $10 per hour, many direct-care workers struggle to support their families. About half the workforce lives in households that rely on public benefits such as housing support, food stamps and Medicaid to make ends meet.
Moreover, these jobs have all the qualities that make low-wage work problematic: hours tend to be uncertain, the work is physically challenging with high occupational injury rates, the jobs rarely offer benefits like health insurance or paid time off and workers often lack adequate training or on-the-job support. We can do better. And we should do better.

Direct-care workers are indispensable. A skilled and compassionate caregiver can be a lifeline -- not just for the person she assists, but for the entire family. These workers provide the paid services that enable other women to continue to work with the peace of mind of knowing their family member is well cared for day in and day out.
Improving the jobs of direct-care workers can improve the lives of millions of women across America. Let's add direct-care workers to the White House Summit on Working Families agenda. We can start with the following:
Better wages: Direct-care workers need better wages and benefits. Raising the minimum wage to $10.10 per hour would certainly help many of the women in these occupations. But the White House also needs to make sure it follows through on the new regulation that extends to home care aides minimum wage and overtime protections through the Fair Labor Standards Act (FLSA). There should be no delay in the January 1, 2015 implementation date for this important change.
Paid Leave: Many direct-care workers have no paid sick leave or family leave. The Healthy Families Act, which would guarantee paid leave for all of America's workers, is essential to quality jobs and to good care. No one wants a caregiver to put herself and her client at risk by coming to work sick or injured.
Advancement: Rapid changes in our health care system are creating opportunities to rethink the roles of direct-care workers. Senator Bob Casey (D-PA) and Congressman Matt Cartwright (D-PA) have introduced legislation to fund federal demonstrations that would test different "advance aide" models -- for example, incorporating "senior aides" into interdisciplinary care coordination teams or using advanced training of aides to improve care for clients with specific chronic conditions such as diabetes or dementia.
These models could give workers opportunities for career advancement while improving the health of individuals receiving care and reducing unnecessary hospitalizations. Providing real opportunities for career advancement will help to move this workforce out of poverty and help to build and sustain the workforce we will need to meet the coming demand for direct care.
The Working Families Summit can address the needs of all working women by addressing the dual challenge of improving direct-care jobs and providing quality supports and services for our nation's elders and people living with disabilities. Doing so will also bring relief to millions of working American women who need a stable, skilled and compassionate direct-care workforce to help them balance full-time work responsibilities with caring for their families and communities.
More: Home Health Aide White House Summit on Working Families Working Families Summit Working Families Home Health Care