GROUP AMERICAN FIDELITY ASSURANCE COMPANY APPLICATION 2000 ... · GROUP AMERICAN FIDELITY ASSURANCE...
39
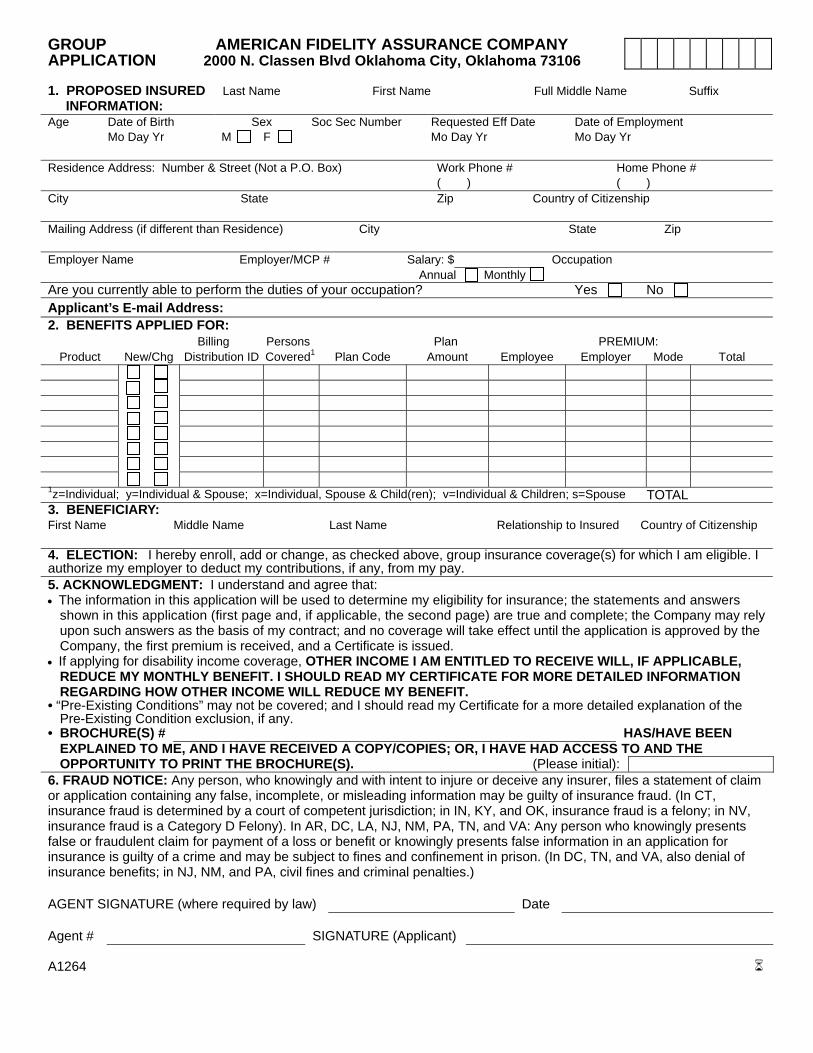
GROUP AMERICAN FIDELITY ASSURANCE COMPANY APPLICATION 2000 N. Classen Blvd Oklahoma City, Oklahoma 73106 1. PROPOSED INSURED Last Name First Name Full Middle Name Suffix INFORMATION: Age Date of Birth Sex Soc Sec Number Requested Eff Date Date of Employment Mo Day Yr M F Mo Day Yr Mo Day Yr Residence Address: Number & Street (Not a P.O. Box) Work Phone # Home Phone # ( ) ( ) City State Zip Country of Citizenship Mailing Address (if different than Residence) City State Zip Employer Name Employer/MCP # Salary: $ Occupation Annual Monthly Are you currently able to perform the duties of your occupation? Yes No Applicant’s E-mail Address: 2. BENEFITS APPLIED FOR: Billing Persons Plan PREMIUM: Product New/Chg Distribution ID Covered 1 Plan Code Amount Employee Employer Mode Total 1 z=Individual; y=Individual & Spouse; x=Individual, Spouse & Child(ren); v=Individual & Children; s=Spouse TOTAL 3. BENEFICIARY: First Name Middle Name Last Name Relationship to Insured Country of Citizenship 4. ELECTION: I hereby enroll, add or change, as checked above, group insurance coverage(s) for which I am eligible. I authorize my employer to deduct my contributions, if any, from my pay. 5. ACKNOWLEDGMENT: I understand and agree that: • The information in this application will be used to determine my eligibility for insurance; the statements and answers shown in this application (first page and, if applicable, the second page) are true and complete; the Company may rely upon such answers as the basis of my contract; and no coverage will take effect until the application is approved by the Company, the first premium is received, and a Certificate is issued. • If applying for disability income coverage, OTHER INCOME I AM ENTITLED TO RECEIVE WILL, IF APPLICABLE, REDUCE MY MONTHLY BENEFIT. I SHOULD READ MY CERTIFICATE FOR MORE DETAILED INFORMATION REGARDING HOW OTHER INCOME WILL REDUCE MY BENEFIT. • “Pre-Existing Conditions” may not be covered; and I should read my Certificate for a more detailed explanation of the Pre-Existing Condition exclusion, if any. • BROCHURE(S) # HAS/HAVE BEEN EXPLAINED TO ME, AND I HAVE RECEIVED A COPY/COPIES; OR, I HAVE HAD ACCESS TO AND THE OPPORTUNITY TO PRINT THE BROCHURE(S). (Please initial): 6. FRAUD NOTICE: Any person, who knowingly and with intent to injure or deceive any insurer, files a statement of claim or application containing any false, incomplete, or misleading information may be guilty of insurance fraud. (In CT, insurance fraud is determined by a court of competent jurisdiction; in IN, KY, and OK, insurance fraud is a felony; in NV, insurance fraud is a Category D Felony). In AR, DC, LA, NJ, NM, PA, TN, and VA: Any person who knowingly presents false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison. (In DC, TN, and VA, also denial of insurance benefits; in NJ, NM, and PA, civil fines and criminal penalties.) AGENT SIGNATURE (where required by law) Date Agent # SIGNATURE (Applicant) A1264
Transcript of GROUP AMERICAN FIDELITY ASSURANCE COMPANY APPLICATION 2000 ... · GROUP AMERICAN FIDELITY ASSURANCE...
GROUP AMERICAN FIDELITY ASSURANCE COMPANY APPLICATION 2000 N. Classen Blvd Oklahoma City, Oklahoma 73106 1. PROPOSED INSURED Last Name First Name Full Middle Name Suffix
INFORMATION: Age Date of Birth Sex Soc Sec Number Requested Eff Date Date of Employment Mo Day Yr M F Mo Day Yr Mo Day Yr Residence Address: Number & Street (Not a P.O. Box) Work Phone # Home Phone # ( ) ( ) City State Zip Country of Citizenship Mailing Address (if different than Residence) City State Zip Employer Name Employer/MCP # Salary: $ Occupation Annual Monthly Are you currently able to perform the duties of your occupation? Yes No Applicant’s E-mail Address: 2. BENEFITS APPLIED FOR: Billing Persons Plan PREMIUM:
Product New/Chg Distribution ID Covered1 Plan Code Amount Employee Employer Mode Total
1z=Individual; y=Individual & Spouse; x=Individual, Spouse & Child(ren); v=Individual & Children; s=Spouse TOTAL 3. BENEFICIARY: First Name Middle Name Last Name Relationship to Insured Country of Citizenship 4. ELECTION: I hereby enroll, add or change, as checked above, group insurance coverage(s) for which I am eligible. I authorize my employer to deduct my contributions, if any, from my pay. 5. ACKNOWLEDGMENT: I understand and agree that: • The information in this application will be used to determine my eligibility for insurance; the statements and answers
shown in this application (first page and, if applicable, the second page) are true and complete; the Company may rely upon such answers as the basis of my contract; and no coverage will take effect until the application is approved by the Company, the first premium is received, and a Certificate is issued.
• If applying for disability income coverage, OTHER INCOME I AM ENTITLED TO RECEIVE WILL, IF APPLICABLE, REDUCE MY MONTHLY BENEFIT. I SHOULD READ MY CERTIFICATE FOR MORE DETAILED INFORMATION REGARDING HOW OTHER INCOME WILL REDUCE MY BENEFIT.
• “Pre-Existing Conditions” may not be covered; and I should read my Certificate for a more detailed explanation of the Pre-Existing Condition exclusion, if any.
• BROCHURE(S) # HAS/HAVE BEEN EXPLAINED TO ME, AND I HAVE RECEIVED A COPY/COPIES; OR, I HAVE HAD ACCESS TO AND THE OPPORTUNITY TO PRINT THE BROCHURE(S). (Please initial):
6. FRAUD NOTICE: Any person, who knowingly and with intent to injure or deceive any insurer, files a statement of claim or application containing any false, incomplete, or misleading information may be guilty of insurance fraud. (In CT, insurance fraud is determined by a court of competent jurisdiction; in IN, KY, and OK, insurance fraud is a felony; in NV, insurance fraud is a Category D Felony). In AR, DC, LA, NJ, NM, PA, TN, and VA: Any person who knowingly presents false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison. (In DC, TN, and VA, also denial of insurance benefits; in NJ, NM, and PA, civil fines and criminal penalties.) AGENT SIGNATURE (where required by law) Date Agent # SIGNATURE (Applicant) A1264
asapdao
Initial Here
asapdao
Sign Here
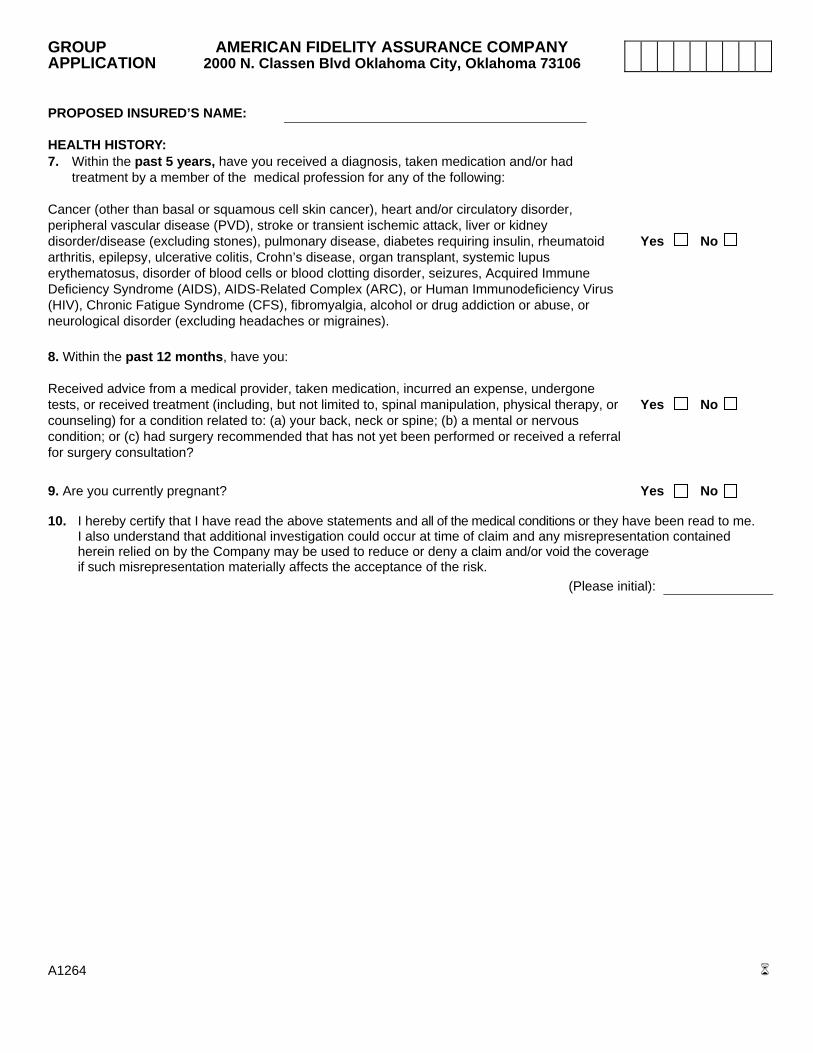
GROUP AMERICAN FIDELITY ASSURANCE COMPANY APPLICATION 2000 N. Classen Blvd Oklahoma City, Oklahoma 73106 PROPOSED INSURED’S NAME: HEALTH HISTORY: 7. Within the past 5 years, have you received a diagnosis, taken medication and/or had treatment by a member of the medical profession for any of the following: Cancer (other than basal or squamous cell skin cancer), heart and/or circulatory disorder, peripheral vascular disease (PVD), stroke or transient ischemic attack, liver or kidney disorder/disease (excluding stones), pulmonary disease, diabetes requiring insulin, rheumatoid Yes No arthritis, epilepsy, ulcerative colitis, Crohn’s disease, organ transplant, systemic lupus erythematosus, disorder of blood cells or blood clotting disorder, seizures, Acquired Immune Deficiency Syndrome (AIDS), AIDS-Related Complex (ARC), or Human Immunodeficiency Virus (HIV), Chronic Fatigue Syndrome (CFS), fibromyalgia, alcohol or drug addiction or abuse, or neurological disorder (excluding headaches or migraines). 8. Within the past 12 months, have you: Received advice from a medical provider, taken medication, incurred an expense, undergone tests, or received treatment (including, but not limited to, spinal manipulation, physical therapy, or Yes No counseling) for a condition related to: (a) your back, neck or spine; (b) a mental or nervous condition; or (c) had surgery recommended that has not yet been performed or received a referral for surgery consultation?
9. Are you currently pregnant? Yes No 10. I hereby certify that I have read the above statements and all of the medical conditions or they have been read to me. I also understand that additional investigation could occur at time of claim and any misrepresentation contained herein relied on by the Company may be used to reduce or deny a claim and/or void the coverage if such misrepresentation materially affects the acceptance of the risk. (Please initial): A1264
asapdao
Initial Here
Group Disability Claim Filing Instructions
(Not for use when filing for Physician’s Expense Benefits)Disability Claim form is to be completed after you become disabled.
1. Complete Employee’s Disability Benefits Application in full.2. Have the treating physician complete the Attending Physician’s Statement and return to you.3. Have your Employer complete the Employer’s Report of Claim.4. Submit the completed: a. Employee’s Disability Benefits Application B. Employer’s Report of Claim C. Attending Physician’s Statement to the address below or submit via our toll-free fax @ 1-800-818-34535. Please complete if you desire benefits deposited directly into your bank account.
I authorize AFAC to initiate credit entries to my account at the depository named below. This authorization is to remain in force and effect until AFAC receives written notification from me of its termination in such time and in such manner as to afford AFAC and the Depository opportunity to act on it. this authorization applies to benefits payable under all insurance policies held with aFaC.
Signature: ________________________________________________________________________________________________ notE: you must attach a voided check to begin direct deposit.
all portions of this form package must be completed to avoid undue delay in processing claimant’s request for benefits. if you have any questions regarding completion of this form please call:
Toll Free: 1-800-662-1113 Local: 405-523-5025
Educational Services DivisionBenefits Department
P.O. Box 25160Oklahoma City, Oklahoma 73125-0160
www.afadvantage.com
Warning: Any person who knowingly and with intent to injure, defraud, or deceive an insurer files a statement of claim containing any false, incomplete, or misleading information may be guilty of insurance fraud and subject to criminal and civil penalties.California - For your protection, California law requires the following to appear on this form. any person who knowingly presents false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.ar, dC, La, Md, nJ, nM, tX, and WV - ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM FOR PAYMENT OF A LOSS OR BENEFIT OR KNOWINGLY PRESENTS FALSE INFORMATION IN AN APPLICATION FOR INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON.dE, id, in, Mn, oh, and oK - Warning: Any person who knowingly, and with intent to injure, defraud or deceive any insurer, files a statement of claim containing any false, incomplete, or misleading information is guilty of a felony.Colorado - It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado division of insurance within the department of regulatory agencies.new hampshire - Any person who, with a purpose to injure, defraud or deceive any insurance company, files a statement of claim containing any false, incomplete or misleading information is subject to prosecution and punishment for insurance fraud, as provided in RSA 638:20.Kentucky - Any person who knowingly and with intent to defraud any insurance company or other person files a statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.oregon - Any person who knowingly and with intent to defraud or solicit another to defraud an insurer: (1) by submitting an application, or (2) by filing a claim containing a false statement as to any material fact, may be guilty of insurance fraud.Pennsylvania - Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
arizona - For your protection, Arizona law requires the following statement to appear on this form: Any person who knowingly presents a false or fraudulent claim for payment of a loss is subject to criminal and civil penalties.Florida - Any person who knowingly, and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete, or misleading information is guilty of a felony of the third degree.
BN-658-0212
Mail to: AFES Benefits Department P.O. Box 25160 Oklahoma City, OK 73125-0160 Local: (405) 523-5025 toll Free: 1-800-662-1113 Fax: 1-800-818-3453 www.afadvantage.com
EMPLoyEE’s disaBiLity BEnEFits aPPLiCationSee front page for fraud warnings.
Full Name: (last, first, middle initial) Maiden Name Account Number:
Residence: (street, city, state and zip code) Social Security Number:
Mailing Address: (P.O. Box or street, city and zip code) Date of Birth:
Telephone Number: (including area code) r Single r Married r Widowed r Divorced
Occupation: Has your employment terminated? If so, date:
Names & birth dates of _____________________________/_____/_____ _____________________________/_____/_____
_____________________________/_____/_____ _____________________________/_____/_____
1. Date accident or illness began: 2. If accident, explain where and how it happened?
3. Have you ever had the same or similar condition in the past? r Yes r No If so, when? ____________________________________________
If yes, names and address of treating physicians and/or hospitals:4. Nature of illness or injury: 5. Dates of medical treatment:
6. If hospitalized give full name(s) and addresses
of hospitals: (attach additional list if necessary)
7. Full names and addresses of all treating physicians: 8. Is your disability related to your employment/occupation? r Yes r No (attach additional list if necessary) If yes, have you or do you intend to file for Worker’s Compensation?r Yes r No
10. If your request for benefits is approved, do you want us to withhold Federal Taxes from each benefit check? r Yes r No
If yes, amount: $ _______________________ (indicate amount per month $86.00 minimum)
11. Identify other income sources and amount of income for which you are receiving or may be entitled to receive during this disability Your Social Security: (disability or retirement) r Yes r No $_______Mo. V.A. Benefits: r Yes r No $_______Mo. Dependent Social Security: r Yes r No $_______Mo. Worker’s Compensation: r Yes r No $_______Mo. Sick Leave or Wage Continuation: r Yes r No $_______Mo. Other Disability Coverage: r Yes r No $_______Mo Retirement: (normal early or disability) r Yes r No $_______Mo. (identify)_____________________________________________ State Disability Income r Yes r No $_______Mo. Unemployment r Yes r No $_______Mo signature: ____________________________________________________ date: ____________________________________________________ I certify this information is true and correct.
aUthoriZation to disCLosE ProtECtEd hEaLth inForMationI hereby authorize the entities specified below to disclose any information about my entire medical record, benefits payable, or benefit eligibility for this disability and history of treatment for physical and/or emotional illness to include psychological testing, except psychotherapy notes, to individuals representing American Fidelity Assurance Company (AFAC) who are involved in determining whether I am eligible for benefits under my insurance coverage. Those so authorized are: a) licensed physicians or medical practitioners; b) hospitals, clinics or medically-related facilities; c) health plans; d) Veteran’s Administration; e) past or present employers; f) pharmacy; g) insurance companies; h) the Social Security Administration; i) retirement systems; j) Department of Motor Vehicles; and k) Workers’ Compensation Carrier. notiCE: Information authorized for release may include information on communicable or venereal diseases such as hepatitis, syphilis, gonorrhea, HIV/AIDS (Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome) or other conditions for which you may have been treated. This authorization excludes disclosure of the result of a test for HIV if you have tested HIV positive but have not developed symptoms of the disease AIDS. Such test results shall not be discovered or published. Nothing in this caveat will prohibit this authorization from including the fact that you have AIDS.i understand that i may refuse to sign this authorization; however, if i do not sign the authorization, my failure to sign the authorization may result in a denial or a delay of benefits. I understand that I may revoke this authorization at any time by writing to AFES Benefits Department, PO Box 25160, Oklahoma City, OK 73125-0160 or by calling, toll-free, 1-800-662-1113. I understand that my right to revoke this authorization is limited to the extent that: AFAC has taken action in reliance on the authorization; or, the law provides AFAC with the right to contest my insurance coverage or a claim under my insurance coverage. A copy of this authorization will be as valid as the original.I understand that if protected health information is disclosed to a person or organization that is not required to comply with federal privacy regulations, the information may be redisclosed and no longer protected by the federal privacy regulations.For health insurance coverage this authorization will expire twenty-four months from the date it is signed or upon termination of my insurance policy, whichever occurs first. For insurance coverage other than health insurance, this authorization will expire twenty-four months from the date it is signed or upon expiration of my claim for benefits, whichever occurs first.
_______________________________________________________________ ______________________________________________ Signature (Patient) or Personal Representative (if applicable) Printed Name (Patient)
_____________________________________________________________ ______________________________________________Relationship of Personal Representative to Patient DateIf authorization is supplied by a personal representative a description of the authority to act on behalf of the Insured must be included.
Please retain a copy for your personal records, or you may request a copy from our company.
/ /
( )
- -
Name Birth date Name Birth date
Name Birth dateName Birth date
include a copy of your award or denial letter for any source in which one has been received.
spouse & dependents:
Date of next doctor’s appointment:
9. On what date did you last work?______________ Dates of total disability: From ______________ Thru ________________ On what date did you return to work? Part Time ________/________/________ Full Time ________/________/________ If not returned to work, when do you anticipate returning to work?___________________________
Admit Date: _______/_______/_______ Discharge Date: _______/_______/_______
BN-658-0212
american Fidelity assurance Company Mail to: AFES Benefits Department P.O. Box 25160 Oklahoma City, OK 73125-0160 Local: (405) 523-5025 toll Free: 1-800-662-1113 Fax: 1-800-818-3453 www.afadvantage.com
EMPLoyEr’s rEPort oF CLaiMName of Employer: Phone No.: Mailing Address: (include street, city, state and zip code) Fax No.:
Name of Employee: Social Security Number:
Address: (include street, city, state and zip code) Phone No.:
Date of Hire: Effective date of employee’s coverage: Occupation: (please attach job description)
Status of employment at time employee last worked: r Full-Time r Part-Time r Leave of Absence r Terminated r Retired
Number of hours worked per week at time of leave:______________________
Number of contract days: _______________________ for ____________ school year.
Has employee’s status of employment changed? r Yes r No If yes, current status and date of status-change? __________________
Does employee participate in Social Security? r Yes r No If no, hired after 4/1/86? r Yes r No
Please furnish the percentage of the employee’s AFA disability premium you pay: short term ______________%
Are the AFA disability premiums withheld before or after taxes? Long term ______________%
short term Plan r Before r After Long term Plan r Before r After
ContraCtEd saLary at tiME oF disaBiLity
Annual: $_____________________ Effective Date: _________________________ r 9 r 10 r 12 Month Work Schedule r 9 r 10 r 12 Month Pay Schedule Date employee last worked:_______________________________ Have AFA Disability premiums been withheld Has employee returned to work? r Yes r No through the last date worked? r Yes r No
If Yes, date returned to work:
Full Time: __________________________ Part Time: ________________________Did Employee’s disability result from employment? r Yes r No
If yes, name, address and phone number of Worker’s Compensation carrier: _______________________________________________________
Has employee made a claim for or is entitled to Worker’s Compensation? r Yes r No
If yes, weekly rate of compensation: $___________________
Provide: The final date the employee is entitled to fully paid sick leave __________________________________________________________ Is this employee eligible to receive any other form of wage continuation? r Yes r No If so, please advise the amount and the final date the employee is entitled to receive this pay. ____________________________________________________________________
The first date the employee is entitled to differential/sabbatical pay, if any ________________________________________________
The last date the employee is entitled to differential/sabbatical pay _____________________________________________________
The daily rate of differential/sabbatical pay $ _______________________________________________________________________
Name, address and phone number of any other disability carrier: (include street, city, state and zip code)
Is employee eligible for disability retirement benefits? r Yes r No
remember - to attach a copy of the applicable school calendar for any contracted employee.FaiLUrE to do so CoULd rEsULt in dELayEd BEnEFits
I hereby certify that the above named employee is a member of our Group Disability Program. The Information stated above is correct to the best of my knowledge and belief.
Authorized signature of employer firm or authorized official: _________________________________________________________________________
Title: ______________________________________________________ Date: ________________________________________________________
E-mail Address:______________________________________________ Extension: ____________________________________________________
P
r
E
M
i
U
M
s
s
a
L
a
r
y
disaBiLity
o
t
h
E
r
i
n
C
o
M
E
( )
( )
- -
( )
In-house days:First Day ________________Last Day ________________
E
M
P
L
o
y
M
E
n
t
If not, what is the last date disability premiums were deducted? _________________________
BN-658-0212
Name of Patient: Date of Birth: Social Security Number: Account Number:
Diagnosis: (including complications) ICDA Code:
Is disability due to injury or sickness arising out of or in the course of patient’s employment? r Yes r No
Is disability the result of pregnancy? r Yes r No If yes, type of delivery: ___________________________ Date pregnancy was diagnosed? ____/____/____ Date of delivery:(if delivered) ____/____/____ Expected date of delivery? ____/____/____
When did symptoms first appear or accident happen? Date patient first consulted you for this condition?
Has the patient ever had the same or similar condition? r Yes r No If yes, indicate when and describe:
Was the patient referred to you? r Yes r No If yes, full name and address of referring physician:
Frequency of treatment: r Monthly r Weekly r Other
Date of next appointment : _______/______/______
Nature of treatment being rendered (including surgery and any medications being prescribed)
List all dates of treatment or medical attention since the disability began:
Is patient still under your regular care for this condition? r Yes r No If no, please explain and provide name of the current treating physician:
Has the patient been confined to a hospital? r Yes r No Admitted: _____/_____/_____ Discharged: _____/_____/_____
If yes, give admit and discharge dates along with name and address of hospital. Admitted: _____/_____/_____ Discharged: _____/_____/_____
Name:___________________________________________________ Address: ___________________________________________________
Dates of total disability: (unable to work) From: ____________________ Through: ____________________
Disabled from: Patient’s Job r Yes r No Any other work r Yes r No
If the patient is currently disabled, what is the anticipated length of disability?
r 1-2 Months r 2-3 Months r 3-6 Months
r 6-12 Months r More than 12 Months r Permanent
When, in your opinion, will the patient recover sufficiently to return to work?
Functional Limitations that render your patient totally disabled:
Current Treatment Plan:
Attending Physician’s Name: (print) Specialty: Telephone #: Fax #:
Street Address: City: State: Zip Code:
Signature: Federal Tax ID #: Date:
Email address:
d
i
a
g
n
o
s
i
s
h
i
s
t
o
r
y
t
r
E
a
t
M
E
n
t
P
r
o
g
n
o
s
i
s
i
M
P
a
i
r
M
E
n
t
s
BN-658-0212
______/______/______ ______/______/______
( ) - ( ) -
Dates of partial disability?
From: ____________________ Through: ____________________
american Fidelity assurance CompanyMail to: AFES Benefits Department P.O. Box 25160 Oklahoma City, OK 73125-0160 Local: (405) 523-5025toll Free: 1-800-662-1113Fax: 1-800-818-3453
attEnding PhysiCian’s statEMEnt
See front page for fraud warnings.
BN-688-0212
Routine Pregnancy Claim Filing Instructions
Do not use this form for any benefit other than routine child birth.
1. Complete Employee’s Disability Benefits Application in full.
2. Have the treating physician complete the Attending Physician’s Statement and return to you.
3. Have your Employer complete the Employer’s Report of Claim.
4. Submit the completed:
A. Employee’s Disability Benefits Application
B. Employer’s Report of Claim
C. Attending Physician’s Statement
to the address below or submit via our toll-free fax @ 1-800-818-3453.
All portions of this form package must be completed to avoid undue delay in processing claimant’s request for benefits. If you
have any questions regarding completion of this form please call:
Toll Free: 1-800-662-1113
Educational Services DivisionBenefits Department
P.O. Box 25160Oklahoma City, Oklahoma 73125-0160
www.afadvantage.com
Warning: Any person who knowingly and with intent to injure, defraud, or deceive an insurer files a statement of claim containing any false, incomplete, or misleading information may be guilty of insurance fraud and subject to criminal and civil penalties.California - For your protection, California law requires the following to appear on this form. Any person who knowingly presents false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.AR, DC, LA, MD, NJ, NM, TX, and WV - ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM FOR PAYMENT OF A LOSS OR BENEFIT OR KNOWINGLY PRESENTS FALSE INFORMATION IN AN APPLICATION FOR INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON.DE, ID, IN, MN, OH, and OK - WARNING: Any person who knowingly, and with intent to injure, defraud or deceive any insurer, files a statement of claim containing any false, incomplete, or misleading information is guilty of a felony.Colorado - It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado division of insurance within the department of regulatory agencies.New Hampshire - Any person who, with a purpose to injure, defraud or deceive any insurance company, files a statement of claim containing any false, incomplete or misleading information is subject to prosecution and punishment for insurance fraud, as provided in RSA 638:20.Kentucky - Any person who knowingly and with intent to defraud any insurance company or other person files a statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.Oregon - Any person who knowingly and with intent to defraud or solicit another to defraud an insurer: (1) by submitting an application, or (2) by filing a claim containing a false statement as to any material fact, may be guilty of insurance fraud.Pennsylvania - Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
Arizona - For your protection, Arizona law requires the following statement to appear on this form: Any person who knowingly presents a false or fraudulent claim for payment of a loss is subject to criminal and civil penalties.Florida - Any person who knowingly, and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete, or misleading information is guilty of a felony of the third degree.
Hawaii - For your protection, Hawaii law requires you to be informed that presenting a fraudulent claim for payment of a loss or benefit is a crime punish-able by fines or imprisonment, or both.
SECTION 1: EMPLOYEE’S DISABILITY BENEFITS APPLICATIONSee page 1 for fraud statements.
Full Name: (last, first, middle initial) Maiden Name Account Number:
Social Security Number: Date of Birth: Telephone Number: (including area code)
Mailing Address: (P.O. Box or street, city and zip code) Occupation:
1. Full names and addresses of all treating physicians: (attach additional list if necessary) 2. If hospitalized, give full name(s) and addresses of hospitals: (attach additional list if necessary)
____________________________________________________________________ Admit Date Discharge Date ____________________________________________________________________ Name(s) ___________________________________________________________________ ____________________________________________________________________ Addresses ___________________________________________________________________
5. If your request for benefits is approved do you want us to withhold Federal Taxes from each benefit check? r Yes r No
If yes, amount: $ _______________________________________ (indicate amount per month $86.00 minimum)
6. Are you receiving or eligible to receive other income during this period of disability? r Yes r No $ __________ Month
Sick Leave or Wage Continuation: r Yes r No $ __________ Month
Signature: __________________________________________________________________________________________________ Date:___________________________________________I certify this is true and correct information.
AUTHORIZATION TO USE OR DISCLOSE PROTECTED HEALTH INFORMATION
I hereby authorize the entities specified below to disclose any information about my entire medical record or benefits payable for this disability and history of treatment for physical and/or emotional illness to include psychological testing, except psychotherapy notes, to individuals representing American Fidelity Assurance Company (AFAC), who are involved in determining whether I am eligible for benefits under my insurance coverage. Those so authorized are: a) licensed physicians or medical practitioners; b) hospitals, clinics or medically-related facilities; c) health plans; d) Veteran’s Administration; e) past or present employers; f) pharmacy; g) insurance companies; h) the Social Security Administration; i) retirement systems; j) Department of Motor Vehicles; and k) Workers’ Compensation Carrier.NOTICE: Information authorized for release may include information on communicable or venereal diseases such as hepatitis, syphilis, gonorrhea, HIV/AIDS (Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome) or other conditions for which you may have been treated. This authorization excludes disclosure of the result of a test for HIV if you have tested HIV positive but have not developed symptoms on the disease AIDS. Such test results shall not be discovered or published. Nothing in the caveat will prohibit this authorization from including the fact that you have AIDS.I understand that I may refuse to sign this authorization; however, if I do not sign the authorization, my failure to sign may result in a denial or a delay of benefits. I understand that I may revoke this authorization at any time by writing to AFES Benefits Department, PO Box 25160, Oklahoma City, OK 73125-0160 or by calling, toll-free, 1-800-662-1113. I understand that my right to revoke this authorization is limited to the extent that: AFAC has taken action in reliance on the authorization; or, the law provides AFAC with the right to contest my insurance coverage or a claim under my insurance coverage. A copy of this authorization will be as valid as the original.I understand that if protected health information is disclosed to a person or organization that is not required to comply with federal privacy regulations, the information may be redisclosed and no longer protected by the federal privacy regulations.For health insurance coverage this authorization will expire twenty-four months from the date it is signed or upon termination of my insurance policy, whichever occurs first. For insurance coverage other than health insurance, this authorization will expire twenty-four months from the date it is signed or upon expiration of my claim for benefits, whichever occurs first.
Signature (Patient) or Personal Representative (if applicable) Printed Name (Patient)
Relationship of Personal Representative to Patient DateIf authorization is supplied by a personal representative a description of the authority to act on behalf of the Insured must be included.
Please retain a copy for your personal records, or you may request a copy from our company.
SECTION 2: EMPLOYER’S REPORT OF CLAIM Name of Employer: Phone No.: Fax No.: Mailing Address: (include street, city, state and zip code)
Name of Employee: Social Security Number: Occupation: Date of Hire: Does employee participate in Social Security? r Yes r No If no, hired after 4/1/86? r Yes r No Have you withheld the employee’s disability premium for the current month?
Please furnish the percentage of the employee’s AFA disability premium you pay: __________% r Yes r No
Are the AFA disability premiums withheld before or after taxes? r Before r After If not, what is the last month you deducted disability premiums? _____________ CONTRACTED SALARY AT TIME OF DISABILITY Annual: $ __________________________________ Effective Date: _______________________________ Number of hours worked per week at time of disability ____________________. Number of Contract days: ______________ for _______________ school year.
Date employee last worked:_______________________________________ Has employee returned to work? r Yes r No If Yes, date returned to work: Full Time: ______________________ I hereby certify that the above named employee is a member of our Group Disability Program. The Information stated above is correct to the best of my knowledge and belief. Authorized signature of employer firm or authorized official: ________________________________________________________________________________________________________________ Title: _______________________________________________________________________________________________ Date: __________________________________________________
- - / / ( )
/ / / /
3. On what date did you last work?___________________ Dates of total disability: From _________________ Thru __________________ On what date did you return to work? If not returned to work, when do you anticipate returning to work?______________________________________
4. Please complete if you desire benefits deposited directly into your bank account. I authorize AFAC to initiate credit entries to my account at the depository named below. This authorization is to remain in force and effect until AFAC receives written notification from me of its termination in such time and in such manner as to afford AFAC and the Depository opportunity to act on it. This authorization applies to benefits payable under all insurance policies held with AFAC. Bank/Credit Union Name:
Signature: NOTE: You must attach a voided check to begin direct deposit.
( ) ( )
r 9 r 10 r 12 Month Work Schedule
Routine Pregnancy- Do not use this form for any benefit other than routine child birth.
BN-688-0212
ATTN: AFES BENEFITS DEPT.P.O. Box 25160
Oklahoma City, Oklahoma 73125Toll Free: 1-800-662-1113
Fax: 1-800-818-3453www.afadvantage.com
REQUEST FOR ROUTINE PREGNANCY BENEFITS
Name of Patient: Date of Birth:
Social Security Number:
Diagnosis: ICDA Code:
Type of delivery: _________________________________________________________________________________________________________________
Date pregnancy was diagnosed? ____/____/____
Date of delivery: (if delivered) ___/____/_____
When did symptoms first appear?
Date patient first consulted you for this condition?
Was the patient referred to you? r Yes r No If yes, full name and address of referring physician: _________________________________________
____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
Has the patient been confined to a hospital? r Yes r No
Admitted: _____/_____/_____ Discharged: _____/_____/_____
If yes, give admit and discharge dates along with name and address of hospital.
Name: _______________________________________________________________________________________________________________________
Address:______________________________________________________________________________________________________________________
Dates of total disability: (unable to work) From: ______________________________________ Through: ________________________________________
Attending Physician’s Name: (print) Degree: Telephone #: Fax #:
Street Address: City: State: Zip Code:
Signature: Federal Tax ID #: Date:
H
I
S
T
O
R
Y
T
R
E
A
T
M
E
N
T
P R O G N O S I S
( ) - ( ) -
____/____/____
____/____/____
D
I
A
G
N
O
S
I
S
ATTN: AFES BENEFITS DEPT.P.O. Box 25160
Oklahoma City, Oklahoma 73125Toll Free: 1-800-662-1113
Fax: 1-800-818-3453www.afadvantage.com
REQUEST FOR ROUTINE PREGNANCY BENEFITS
SECTION 3: ATTENDING PHYSICIAN’S STATEMENT
BN-688-0212
ATTN: AFES BENEFITS DEPT.P.O. Box 25160
Oklahoma City, Oklahoma 73125Toll Free: 1-800-662-1113
Fax: 1-800-818-3453www.afadvantage.com
Name_______________________________________ Date of Birth_____________________ AFA Account #______________ (Policyholder)
Residence Address_______________________________________________________ Social Security No.________________ (Street) (Town) (State) (Zip)
Mailing Address_________________________________________________________ (Street) (Town) (State) (Zip)
I am employed at_________________________________________________________________________________________ (Employer) (Address) (City) (State) (Zip)
Telephone No. Home_______________________ Work_______________________ Occupation______________________
BN-PE-0511
PHYSICIAN EXPENSE FOR INJURY OR SICKNESS ONLY
(Do NOT use this form when filing for disability)Warning: Any person who knowingly and with intent to injure, defraud, or deceive an insurer files a statement of claim containing any false, incomplete, or misleading information may be guilty of insurance fraud and subject to criminal and civil penalties.California - For your protection, California law requires the following to appear on this form. Any person who knowingly presents false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.AR, DC, LA, MD, NJ, NM, TX, and WV - ANY PERSON WHO KNOWINGLY PRESENTS A FALSE OR FRAUDULENT CLAIM FOR PAYMENT OF A LOSS OR BENEFIT OR KNOWINGLY PRESENTS FALSE INFORMATION IN AN APPLICATION FOR INSURANCE IS GUILTY OF A CRIME AND MAY BE SUBJECT TO FINES AND CONFINEMENT IN PRISON.DE, ID, IN, MN, OH, and OK - WARNING: Any person who knowingly, and with intent to injure, defraud or deceive any insurer, files a statement of claim containing any false, incomplete, or misleading information is guilty of a felony.Colorado - It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado division of insurance within the department of regulatory agencies.New Hampshire - Any person who, with a purpose to injure, defraud or deceive any insurance company, files a statement of claim containing any false, incomplete or misleading information is subject to prosecution and punishment for insurance fraud, as provided in RSA 638:20.Kentucky - Any person who knowingly and with intent to defraud any insurance company or other person files a statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.Oregon - Any person who knowingly and with intent to defraud or solicit another to defraud an insurer: (1) by submitting an application, or (2) by filing a claim containing a false statement as to any material fact, may be guilty of insurance fraud.Pennsylvania - Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
Arizona - For your protection, Arizona law requires the following statement to appear on this form: Any person who knowingly presents a false or fraudulent claim for payment of a loss is subject to criminal and civil penalties.Florida - Any person who knowingly, and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete, or misleading information is guilty of a felony of the third degree.Hawaii - For your protection, Hawaii law requires you to be informed that presenting a fraudulent claim for payment of a loss or benefit is a crime punishable by fines or imprisonment, or both.
STATEMENT OF THE INSURED
AUTHORIZATION TO USE OR DISCLOSE PROTECTED HEALTH INFORMATION
I hereby authorize the entities specified below to disclose any information about my entire medical record or benefits payable for this disability and history of treatment for physical and/or emotional illness to include psychological testing except psychotherapy notes, to individuals representing American Fidelity Assurance Company (AFAC), who are involved in determining whether I am eligible for benefits under my insurance coverage. Those so authorized are: a) licensed physicians or medical practitioners; b) hospitals, clinics or medically-related facilities; c) health plans; d) Veteran’s Administration; e) past or present employers; f) pharmacy; g) insurance companies; h) the Social Security Administration; i) retirement systems; j) Department of Motor Vehicles; and k) Workers’ Compensation Carrier.NOTICE: Information authorized for release may include information on communicable or venereal diseases such as hepatitis, syphilis, gonorrhea, HIV/AIDS (Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome) or other conditions for which you may have been treated. This authorization excludes disclosure of the result of a test for HIV if you have tested HIV positive but have not developed symptoms on the disease AIDS. Such test results shall not be discovered or published. Nothing in the caveat will prohibit this authorization from including the fact that you have AIDS.I understand that I may refuse to sign this authorization; however, if I do not sign the authorization, my failure to sign may result in a denial or a delay of benefits. I understand that I may revoke this authorization at any time by writing to AFES Benefits Department, PO Box 25160, Oklahoma City, OK 73125-0160 or by calling, toll-free, 1-800-662-1113. I understand that my right to revoke this authorization is limited to the extent that: AFAC has taken action in reliance on the authorization; or, the law provides AFAC with the right to contest my insurance coverage or a claim under my insurance coverage. A copy of this authorization will be as valid as the original.I understand that if protected health information is disclosed to a person or organization that is not required to comply with federal privacy regulations, the information may be redisclosed and no longer protected by the federal privacy regulations.For health insurance coverage this authorization will expire twenty-four months from the date it is signed or upon termination of my insurance policy, whichever occurs first. For insurance coverage other than health insurance, this authorization will expire twenty-four months from the date it is signed or upon expiration of my claim for benefits, whichever occurs first.
Signature (Patient) or Personal Representative (if applicable) Printed Name (Patient)
Relationship of Personal Representative to Patient DateIf authorization is supplied by a personal representative a description of the authority to act on behalf of the Insured must be included.
Please retain a copy for your personal records, or you may request a copy from our company.
Yes o No o If no Explain (semester break, holiday, week-end, etc.):
Yes o No o Date unable to work ______________________
Office_____________________________________________________Hospital___________________________________________________Admit. Date:_____________________ Discharge Date:_____________
_________________
__________________________________________________________
Yes oNo o__________________________________________________________
__________________________________________________________
__________________________________________________________
DIRECT DEPOSIT AUTHORIZATION
Please complete if you desire benefits deposited directly into your bank account.I authorize AFAC to initiate credit entries to my account at the depository named below. This authorization is to remain in force and effect until AFAC receives written notification from me of its termination in such time and in such manner as to afford AFAC and the Depository opportunity to act on it. This authorization applies to benefits payable under all insurance policies held with AFAC.
Signature: ________________________________________________________________________________________________NOTE: You must attach a voided check to begin direct deposit.
1. Date accident or illness began
2. Nature of illness or accident
3. Was accident or illness work related?4. If accident, where and how did it happen? (Explain fully)
5. Dates of all Treatment What date(s) were you unable to work a full day?
6. Were you scheduled to work on the day of medical treatment? If yes, were you totally disabled and unable to work one full day on the date of medical treatment?
PLEASE ATTACH DIAGNOSIS AND ITEMIZED CHARGES FROM THE DOCTOR
BN-PE-0511

AMERICAN FIDELITY AssuRANCE CoMPANY’s
Accident OnlyInsurance Plan
Accidents Happen…Are You Prepared?
This is not a policy of Workers’ Compensation insurance. The employer does not become a subscriber to the Workers’ Compensation system by purchasing this
policy. And, if the employer is a non-subscriber, the employer loses those benefits which would otherwise accrue under the Workers’ Compensation laws. The
employer must comply with the Workers’ Compensation law as it pertains to non subscribers and the required notifications that must be filed and posted.
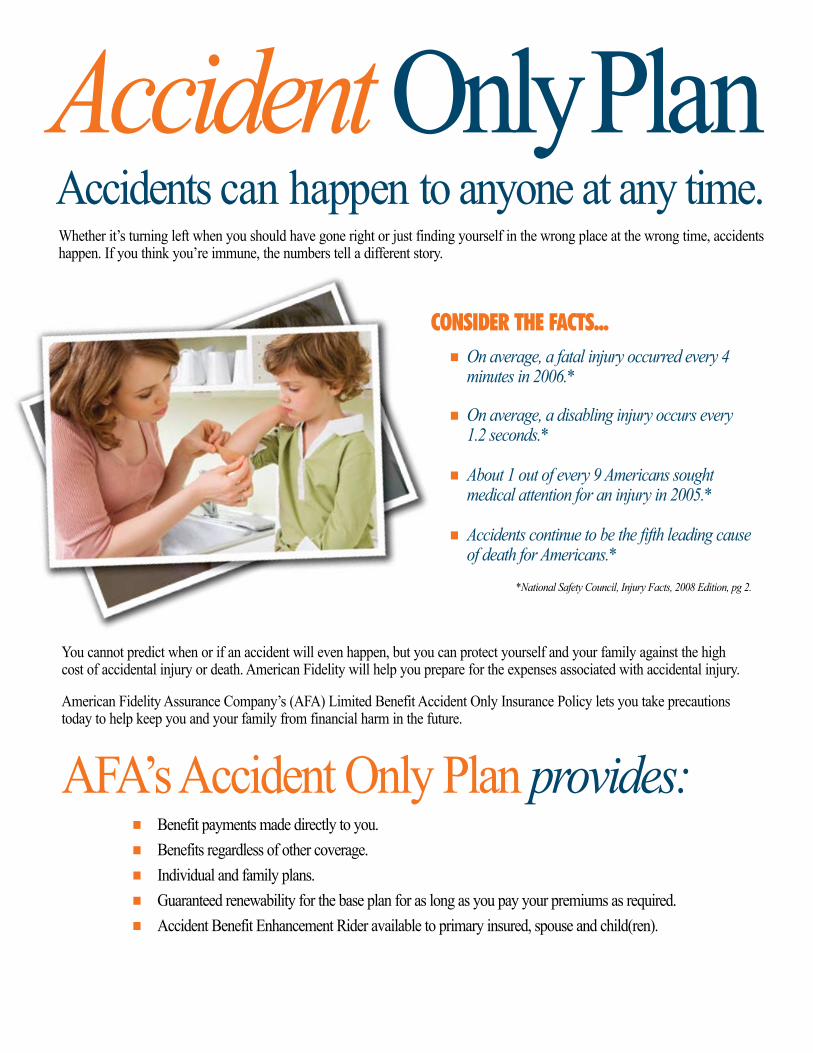
Whether it’s turning left when you should have gone right or just finding yourself in the wrong place at the wrong time, accidents happen. If you think you’re immune, the numbers tell a different story.
Accidents can happen to anyone at any time. Accident Only Plan
CoNsIDER THE FACTs... g On average, a fatal injury occurred every 4
minutes in 2006.*
g On average, a disabling injury occurs every 1.2 seconds.*
g About 1 out of every 9 Americans sought
medical attention for an injury in 2005.*
g Accidents continue to be the fifth leading cause of death for Americans.*
*National Safety Council, Injury Facts, 2008 Edition, pg 2.
You cannot predict when or if an accident will even happen, but you can protect yourself and your family against the high cost of accidental injury or death. American Fidelity will help you prepare for the expenses associated with accidental injury.
American Fidelity Assurance Company’s (AFA) Limited Benefit Accident Only Insurance Policy lets you take precautions today to help keep you and your family from financial harm in the future.
AFA’s Accident Only Plan provides:g Benefit payments made directly to you.g Benefits regardless of other coverage.g Individual and family plans.g Guaranteed renewability for the base plan for as long as you pay your premiums as required.g Accident Benefit Enhancement Rider available to primary insured, spouse and child(ren).

Help When You Need It.A Covered Person under AFA’s Limited Benefit Accident Only Policy can expect the following benefits when a covered accident happens: (All benefits are only paid as a result of injuries received in an Accident that occurs while coverage is in force. All treatment, procedures, and medical equipment must be diagnosed, recommended and treated by a Physician. All benefits are paid once per Covered Person per Covered Accident unless otherwise specified.)
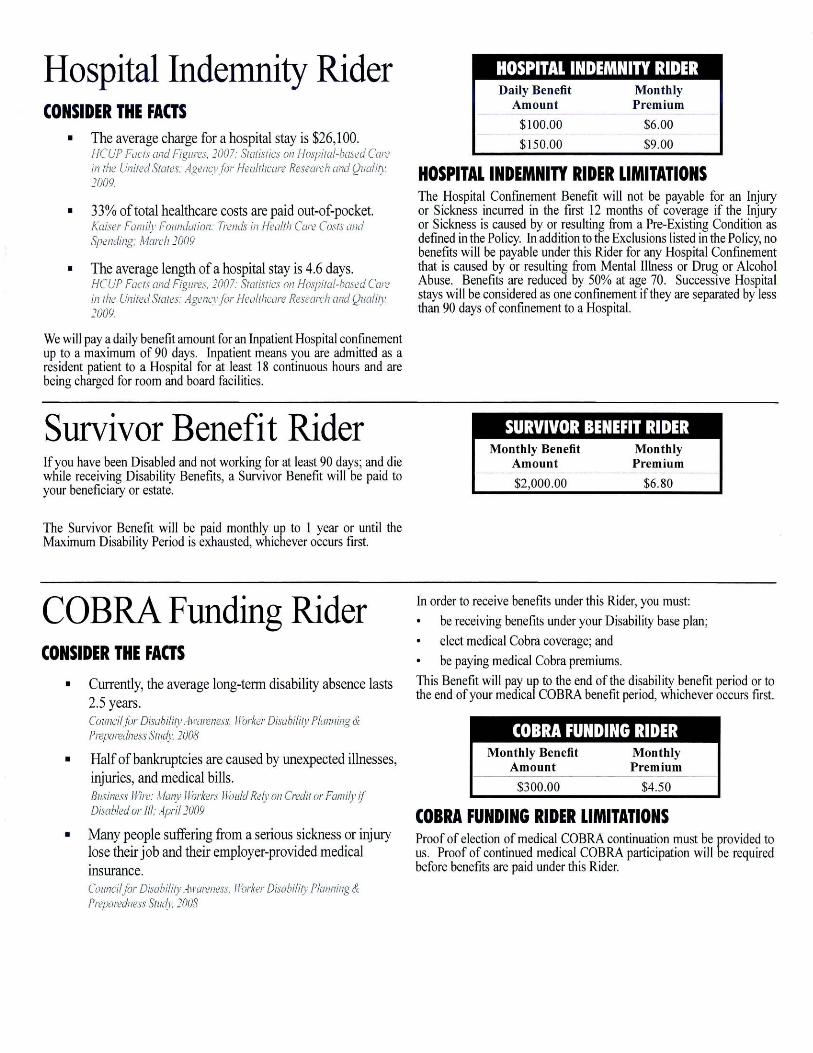
ACCIDENT EMERgENCY TREATMENT BENEFITHospital Emergency Room Basic Plan - $100 Enhanced Plan - $150Doctor’s Office Basic Plan - $75 Enhanced Plan - $100These benefits are provided for a Covered Person who receives emergency treatment in a Physician’s office or hospital emergency room within 72 hours of the Covered Accident, including physician fees, x-rays and emergency services.
ACCIDENT FoLLow-uP TREATMENT BENEFIT$50 per treatment for both Basic and Enhanced PlansThis benefit provides for necessary follow-up treatment of injuries in addition to the emergency treatment administered within 72 hours of a Covered Accident for up to four treatments per Covered Person per Covered Accident. This benefit is not payable for a visit in which a Physical Therapy Benefit is paid. This benefit is also not payable if the Non-Emergency Accident Follow-up benefit is paid under the Benefit Enhancement Rider.
MEDICAL IMAgINg BENEFIT$150 for both Basic and Enhanced PlansYou receive this benefit for a Covered Person who has either a Magnetic Resonance Imaging (MRI), a Computed Tomography (CT) scan, a Computed Axial Tomography (CAT) scan, a Positron Emission Tomography (PET) scan or an ultrasound.
HosPITAL CoNFINEMENT BENEFITsHospital Admission Basic Plan - $500 Enhanced Plan - $1,000Intensive Care Confinement Basic Plan - $300 Enhanced Plan - $600Hospital Confinement Basic Plan - $100 Enhanced Plan - $200You will receive a one-time Hospital Admission Benefit per Covered Accident if a Covered Person is Hospital Confined due to accidental injuries (does not include emergency room and outpatient treatment). You will also receive a daily benefit for a Hospital Confinement that is longer than 18 hours for up to 365 days and an additional daily benefit for Confinement in an Intensive Care Unit up to 15 days.
A hospital is not an institution, or part thereof, used as: a hospice unit, including any bed designated as a swing bed; a convalescent home; a rest or nursing facility; a rehabilitative facility; an extended-care facility; a skilled nursing facility; or a facility primarily affording custodial, educational care, or care or treatment for persons suffering from mental diseases or disorders, or care for the aged, or drug or alcohol addiction.
wELLNEss BENEFITBasic Plan - $50Enhanced Plan - $75After coverage is in force 12 months, you or any other Covered Person can receive a benefit for an annual routine physical exam, including immunizations and preventive testing. Services must be supervised by a Physician and a charge must be incurred for the service. The benefit does not apply to dental or eye exams and is payable once per policy per calendar year.
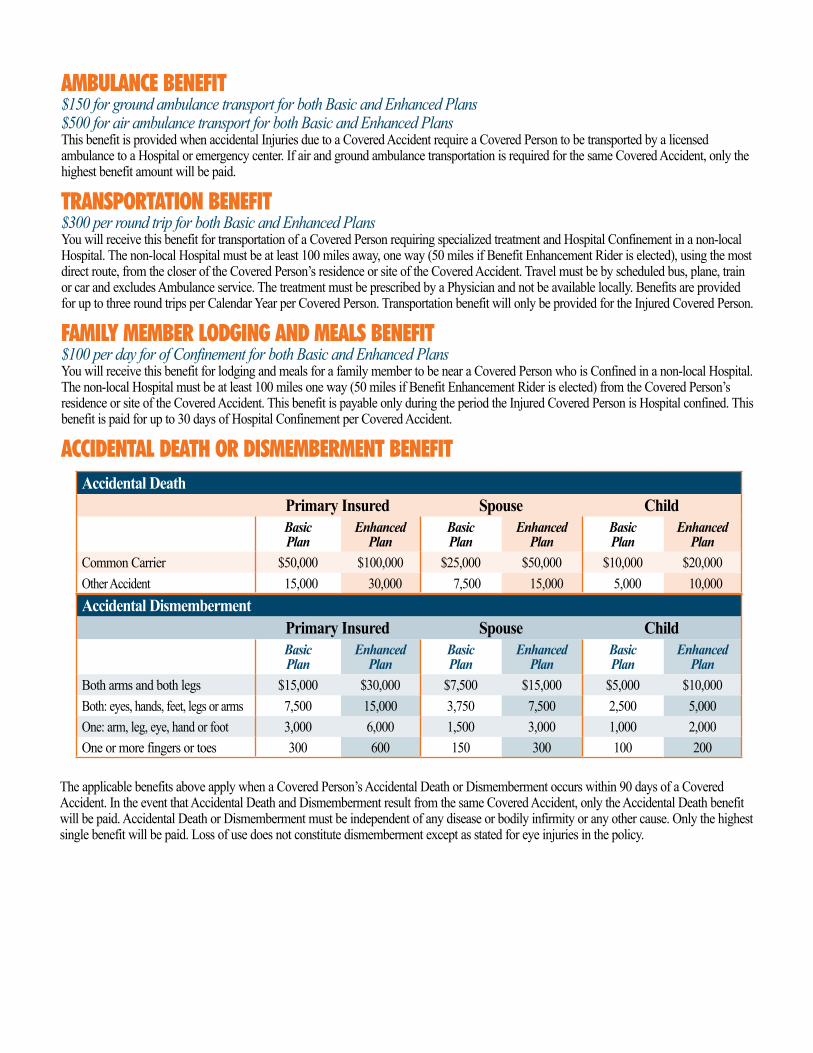
AMBuLANCE BENEFIT$150 for ground ambulance transport for both Basic and Enhanced Plans$500 for air ambulance transport for both Basic and Enhanced PlansThis benefit is provided when accidental Injuries due to a Covered Accident require a Covered Person to be transported by a licensed ambulance to a Hospital or emergency center. If air and ground ambulance transportation is required for the same Covered Accident, only the highest benefit amount will be paid.
TRANsPoRTATIoN BENEFIT$300 per round trip for both Basic and Enhanced PlansYou will receive this benefit for transportation of a Covered Person requiring specialized treatment and Hospital Confinement in a non-local Hospital. The non-local Hospital must be at least 100 miles away, one way (50 miles if Benefit Enhancement Rider is elected), using the most direct route, from the closer of the Covered Person’s residence or site of the Covered Accident. Travel must be by scheduled bus, plane, train or car and excludes Ambulance service. The treatment must be prescribed by a Physician and not be available locally. Benefits are provided for up to three round trips per Calendar Year per Covered Person. Transportation benefit will only be provided for the Injured Covered Person.
FAMILY MEMBER LoDgINg AND MEALs BENEFIT$100 per day for of Confinement for both Basic and Enhanced PlansYou will receive this benefit for lodging and meals for a family member to be near a Covered Person who is Confined in a non-local Hospital. The non-local Hospital must be at least 100 miles one way (50 miles if Benefit Enhancement Rider is elected) from the Covered Person’s residence or site of the Covered Accident. This benefit is payable only during the period the Injured Covered Person is Hospital confined. This benefit is paid for up to 30 days of Hospital Confinement per Covered Accident.
ACCIDENTAL DEATH oR DIsMEMBERMENT BENEFIT
The applicable benefits above apply when a Covered Person’s Accidental Death or Dismemberment occurs within 90 days of a Covered Accident. In the event that Accidental Death and Dismemberment result from the same Covered Accident, only the Accidental Death benefit will be paid. Accidental Death or Dismemberment must be independent of any disease or bodily infirmity or any other cause. Only the highest single benefit will be paid. Loss of use does not constitute dismemberment except as stated for eye injuries in the policy.
Accidental DismembermentPrimary Insured Spouse ChildBasic Plan
EnhancedPlan
Basic Plan
EnhancedPlan
Basic Plan
EnhancedPlan
Both arms and both legs $15,000 $30,000 $7,500 $15,000 $5,000 $10,000Both: eyes, hands, feet, legs or arms 7,500 15,000 3,750 7,500 2,500 5,000One: arm, leg, eye, hand or foot 3,000 6,000 1,500 3,000 1,000 2,000One or more fingers or toes 300 600 150 300 100 200
Accidental DeathPrimary Insured Spouse ChildBasic Plan
EnhancedPlan
Basic Plan
EnhancedPlan
Basic Plan
EnhancedPlan
Common Carrier $50,000 $100,000 $25,000 $50,000 $10,000 $20,000Other Accident 15,000 30,000 7,500 15,000 5,000 10,000
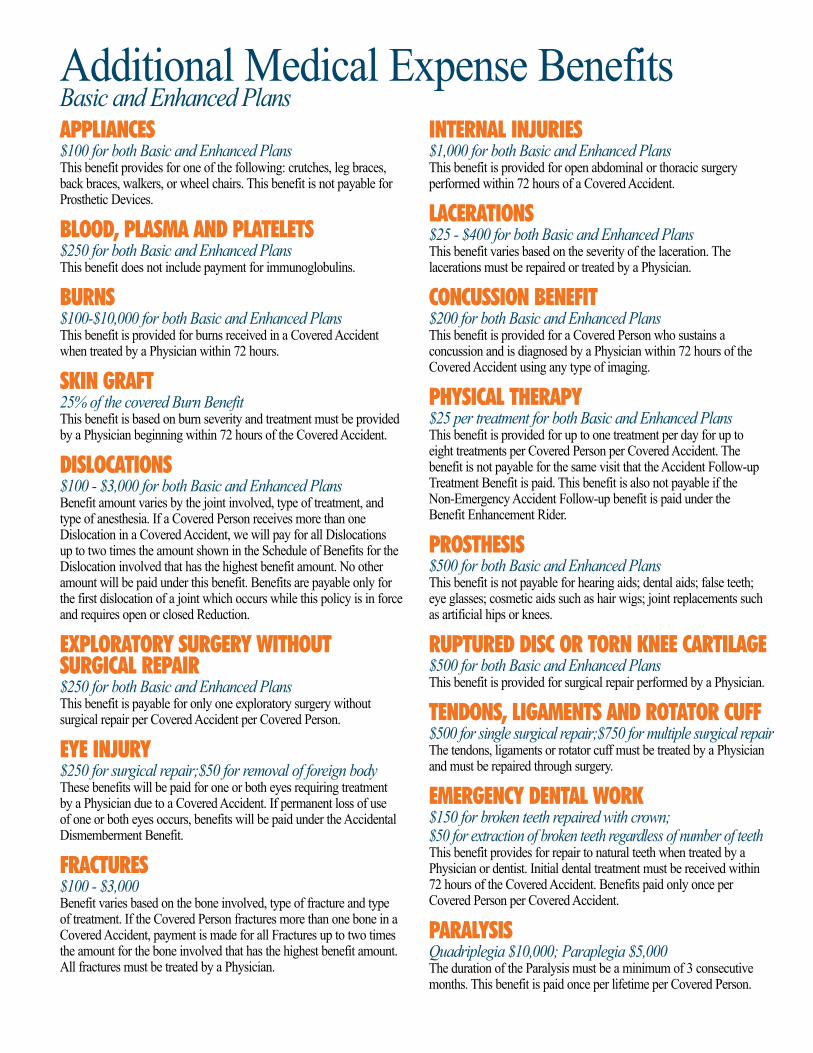
APPLIANCEs$100 for both Basic and Enhanced PlansThis benefit provides for one of the following: crutches, leg braces, back braces, walkers, or wheel chairs. This benefit is not payable for Prosthetic Devices.
BLooD, PLAsMA AND PLATELETs$250 for both Basic and Enhanced PlansThis benefit does not include payment for immunoglobulins.
BuRNs $100-$10,000 for both Basic and Enhanced PlansThis benefit is provided for burns received in a Covered Accident when treated by a Physician within 72 hours.
skIN gRAFT25% of the covered Burn BenefitThis benefit is based on burn severity and treatment must be provided by a Physician beginning within 72 hours of the Covered Accident.
DIsLoCATIoNs$100 - $3,000 for both Basic and Enhanced PlansBenefit amount varies by the joint involved, type of treatment, and type of anesthesia. If a Covered Person receives more than one Dislocation in a Covered Accident, we will pay for all Dislocations up to two times the amount shown in the Schedule of Benefits for the Dislocation involved that has the highest benefit amount. No other amount will be paid under this benefit. Benefits are payable only for the first dislocation of a joint which occurs while this policy is in force and requires open or closed Reduction.
EXPLoRAToRY suRgERY wITHouT suRgICAL REPAIR $250 for both Basic and Enhanced PlansThis benefit is payable for only one exploratory surgery without surgical repair per Covered Accident per Covered Person.
EYE INjuRY $250 for surgical repair;$50 for removal of foreign bodyThese benefits will be paid for one or both eyes requiring treatment by a Physician due to a Covered Accident. If permanent loss of use of one or both eyes occurs, benefits will be paid under the Accidental Dismemberment Benefit.
FRACTuREs $100 - $3,000Benefit varies based on the bone involved, type of fracture and type of treatment. If the Covered Person fractures more than one bone in a Covered Accident, payment is made for all Fractures up to two times the amount for the bone involved that has the highest benefit amount. All fractures must be treated by a Physician.
INTERNAL INjuRIEs $1,000 for both Basic and Enhanced PlansThis benefit is provided for open abdominal or thoracic surgery performed within 72 hours of a Covered Accident.
LACERATIoNs $25 - $400 for both Basic and Enhanced PlansThis benefit varies based on the severity of the laceration. The lacerations must be repaired or treated by a Physician.
CoNCussIoN BENEFIT $200 for both Basic and Enhanced PlansThis benefit is provided for a Covered Person who sustains a concussion and is diagnosed by a Physician within 72 hours of the Covered Accident using any type of imaging.
PHYsICAL THERAPY $25 per treatment for both Basic and Enhanced PlansThis benefit is provided for up to one treatment per day for up to eight treatments per Covered Person per Covered Accident. The benefit is not payable for the same visit that the Accident Follow-up Treatment Benefit is paid. This benefit is also not payable if the Non-Emergency Accident Follow-up benefit is paid under the Benefit Enhancement Rider.
PRosTHEsIs $500 for both Basic and Enhanced PlansThis benefit is not payable for hearing aids; dental aids; false teeth; eye glasses; cosmetic aids such as hair wigs; joint replacements such as artificial hips or knees.
RuPTuRED DIsC oR ToRN kNEE CARTILAgE$500 for both Basic and Enhanced PlansThis benefit is provided for surgical repair performed by a Physician.
TENDoNs, LIgAMENTs AND RoTAToR CuFF$500 for single surgical repair;$750 for multiple surgical repairThe tendons, ligaments or rotator cuff must be treated by a Physician and must be repaired through surgery.
EMERgENCY DENTAL woRk $150 for broken teeth repaired with crown; $50 for extraction of broken teeth regardless of number of teethThis benefit provides for repair to natural teeth when treated by a Physician or dentist. Initial dental treatment must be received within 72 hours of the Covered Accident. Benefits paid only once per Covered Person per Covered Accident.
PARALYsIs Quadriplegia $10,000; Paraplegia $5,000The duration of the Paralysis must be a minimum of 3 consecutive months. This benefit is paid once per lifetime per Covered Person.
Additional Medical Expense BenefitsBasic and Enhanced Plans

FAMILY CovERAgEYou can take advantage of several options to extend coverage to your family:
gIndividual and Spouse Plan – Covers you and your Spouse.
gFamily Plan – Covers you, your Spouse and each Eligible Child, as defined in the policy.
gSingle Parent Family Plan – Covers you and each Eligible Child, as defined in the policy.
guARANTEED RENEwABLEYou are guaranteed the right to renew your base policy during your lifetime as long as you pay premiums when due or within the premium grace period. Accident Disability Income Riders are Guaranteed Renewable until Primary Insured reaches age 70. You cannot be singled out for a rate increase for any reason. Rates can be changed only if rates for all policies in this class change.
LIMITATIoNs AND EXCLusIoNsAn Accident is defined as a sudden, unexpected and unintended event, which results in bodily injury, which is independent of disease or bodily infirmity or any other cause. The policy will not pay benefits for injuries received prior to the Effective Date of coverage that are aggravated or re-injured by any event that occurs after the Effective Date.
No benefits will be provided for an Accident or Total Disability that is caused by or occurs as a result of:
g intentionally self-inflicted bodily injury, suicide or attempted suicide, whether sane or insane;
g participation in any form of flight aviation other than as a fare-paying passenger in a fully licensed/passenger-carrying aircraft;
g any act that was caused by war, declared or undeclared, or service in any of the armed forces;
g participation in any activity or event while under the influence of any narcotic unless administered by a Physician or taken according to the Physician’s instructions;
g participation in, or attempting to participate in, a felony, riot or insurrection. (A felony is as defined by the law of the jurisdiction in which the activity takes place.)
g participation in any sport for pay or profit;
g participation in any contest of speed in a power driven vehicle for pay or profit;
g participation in parachuting, bungee jumping, rappelling, mountain climbing or hang gliding.
Benefits will not be paid for services rendered or Total Disability verified by a member of the immediate family of a Covered Person.
Benefits will not be provided for medical treatment or Total Disability for an Accident received outside the United States or its territories.
Benefits provided by the Accident Disability Income Riders will only be paid for one disability at a time, even if the Covered Person becomes Totally Disabled due to more than one injury or more than one Covered Accident. Benefits are not payable due to an Accident occurring during a period of time the Covered Person is incarcerated in any type of penal institution.
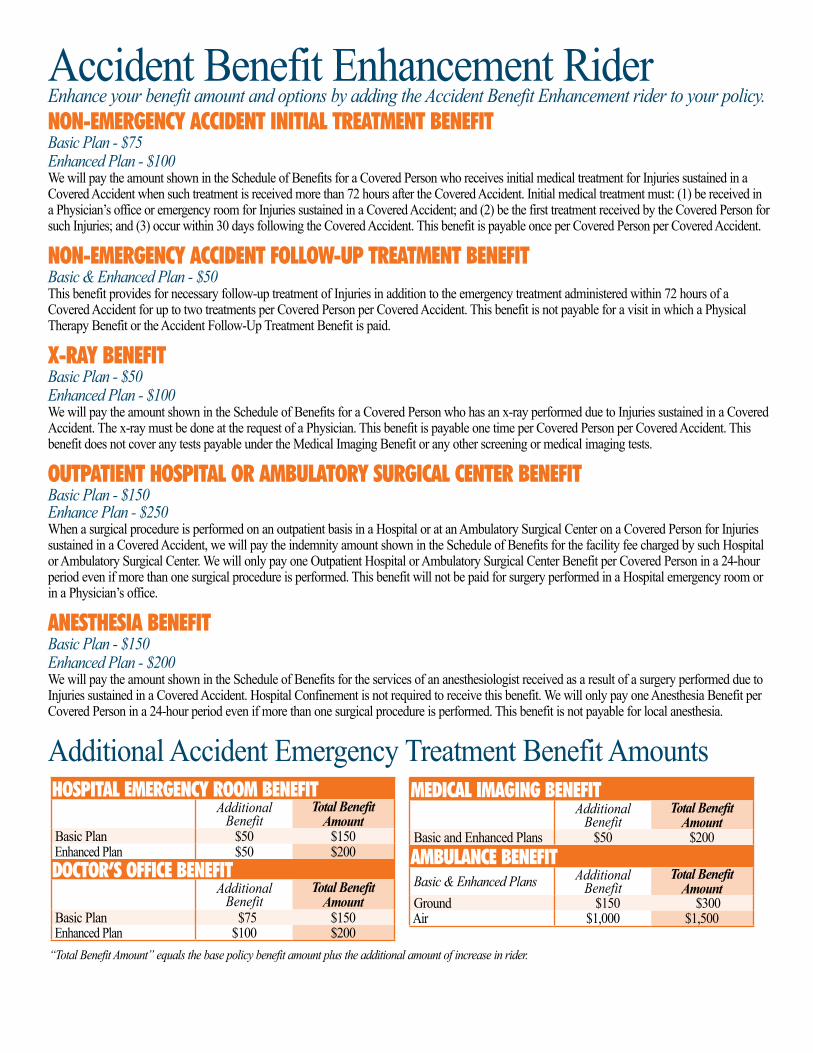
Accident Benefit Enhancement RiderEnhance your benefit amount and options by adding the Accident Benefit Enhancement rider to your policy.NoN-EMERgENCY ACCIDENT INITIAL TREATMENT BENEFITBasic Plan - $75Enhanced Plan - $100We will pay the amount shown in the Schedule of Benefits for a Covered Person who receives initial medical treatment for Injuries sustained in a Covered Accident when such treatment is received more than 72 hours after the Covered Accident. Initial medical treatment must: (1) be received in a Physician’s office or emergency room for Injuries sustained in a Covered Accident; and (2) be the first treatment received by the Covered Person for such Injuries; and (3) occur within 30 days following the Covered Accident. This benefit is payable once per Covered Person per Covered Accident.
NoN-EMERgENCY ACCIDENT FoLLow-uP TREATMENT BENEFITBasic & Enhanced Plan - $50 This benefit provides for necessary follow-up treatment of Injuries in addition to the emergency treatment administered within 72 hours of a Covered Accident for up to two treatments per Covered Person per Covered Accident. This benefit is not payable for a visit in which a Physical Therapy Benefit or the Accident Follow-Up Treatment Benefit is paid.
X-RAY BENEFITBasic Plan - $50Enhanced Plan - $100We will pay the amount shown in the Schedule of Benefits for a Covered Person who has an x-ray performed due to Injuries sustained in a Covered Accident. The x-ray must be done at the request of a Physician. This benefit is payable one time per Covered Person per Covered Accident. This benefit does not cover any tests payable under the Medical Imaging Benefit or any other screening or medical imaging tests.
ouTPATIENT HosPITAL oR AMBuLAToRY suRgICAL CENTER BENEFITBasic Plan - $150Enhance Plan - $250When a surgical procedure is performed on an outpatient basis in a Hospital or at an Ambulatory Surgical Center on a Covered Person for Injuries sustained in a Covered Accident, we will pay the indemnity amount shown in the Schedule of Benefits for the facility fee charged by such Hospital or Ambulatory Surgical Center. We will only pay one Outpatient Hospital or Ambulatory Surgical Center Benefit per Covered Person in a 24-hour period even if more than one surgical procedure is performed. This benefit will not be paid for surgery performed in a Hospital emergency room or in a Physician’s office.
ANEsTHEsIA BENEFITBasic Plan - $150Enhanced Plan - $200We will pay the amount shown in the Schedule of Benefits for the services of an anesthesiologist received as a result of a surgery performed due to Injuries sustained in a Covered Accident. Hospital Confinement is not required to receive this benefit. We will only pay one Anesthesia Benefit per Covered Person in a 24-hour period even if more than one surgical procedure is performed. This benefit is not payable for local anesthesia.
Additional Accident Emergency Treatment Benefit AmountsHosPITAL EMERgENCY RooM BENEFIT
Additional Benefit
Total Benefit Amount
Basic Plan $50 $150 Enhanced Plan $50 $200DoCToR’s oFFICE BENEFIT
Additional Benefit
Total Benefit Amount
Basic Plan $75 $150 Enhanced Plan $100 $200
MEDICAL IMAgINg BENEFITAdditional
BenefitTotal Benefit
Amount Basic and Enhanced Plans $50 $200AMBuLANCE BENEFIT Basic & Enhanced Plans Additional
BenefitTotal Benefit
Amount Ground $150 $300 Air $1,000 $1,500
“Total Benefit Amount” equals the base policy benefit amount plus the additional amount of increase in rider.
SB-15986(TX)-1208 1-800-654-8489 • 2000 North Classen Blvd • Oklahoma City, Oklahoma 73106 • www.afadvantage.com AO-03 Series
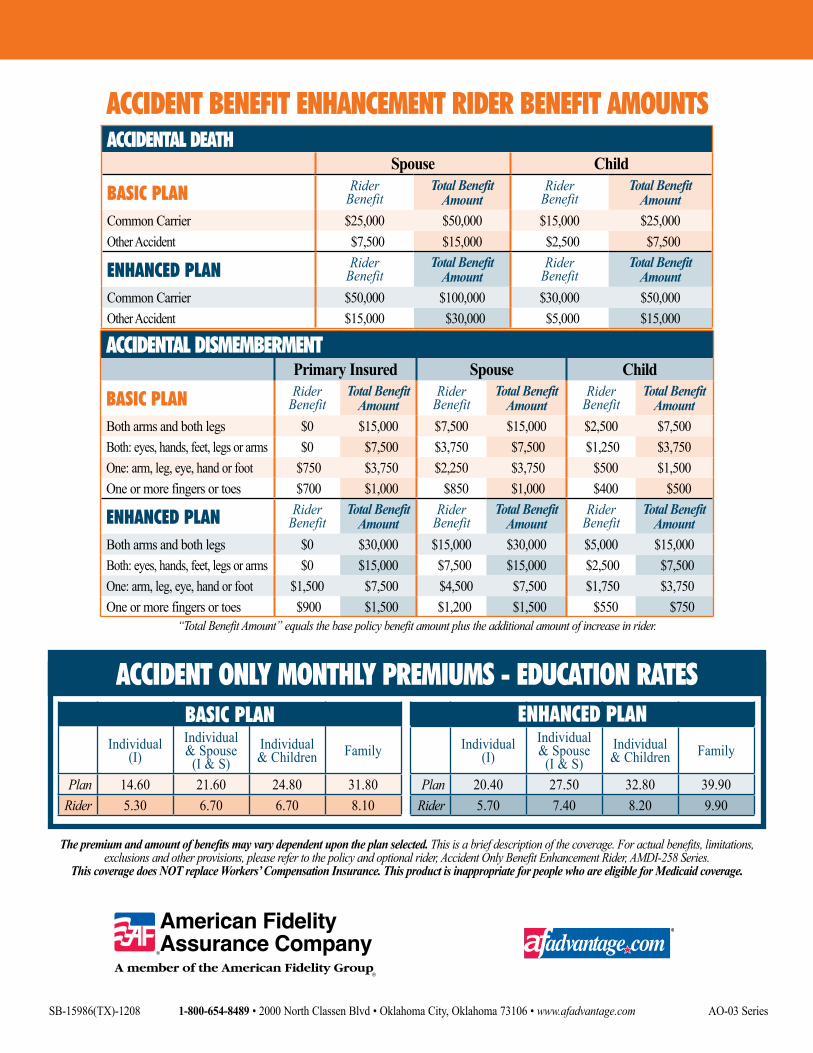
ACCIDENT BENEFIT ENHANCEMENT RIDER BENEFIT AMouNTs
The premium and amount of benefits may vary dependent upon the plan selected. This is a brief description of the coverage. For actual benefits, limitations, exclusions and other provisions, please refer to the policy and optional rider, Accident Only Benefit Enhancement Rider, AMDI-258 Series.
This coverage does NOT replace Workers’ Compensation Insurance. This product is inappropriate for people who are eligible for Medicaid coverage.
“Total Benefit Amount” equals the base policy benefit amount plus the additional amount of increase in rider.
ACCIDENT oNLY MoNTHLY PREMIuMs - EDuCATIoN RATEs
Individual(I)
Individual & Spouse
(I & S)Individual & Children Family
Plan 14.60 21.60 24.80 31.80Rider 5.30 6.70 6.70 8.10
BAsIC PLANIndividual
(I)Individual & Spouse
(I & S)Individual & Children Family
Plan 20.40 27.50 32.80 39.90Rider 5.70 7.40 8.20 9.90
ENHANCED PLAN
ACCIDENTAL DIsMEMBERMENTPrimary Insured Spouse Child
BAsIC PLAN Rider Benefit
Total Benefit Amount
Rider Benefit
Total Benefit Amount
Rider Benefit
Total Benefit Amount
Both arms and both legs $0 $15,000 $7,500 $15,000 $2,500 $7,500Both: eyes, hands, feet, legs or arms $0 $7,500 $3,750 $7,500 $1,250 $3,750One: arm, leg, eye, hand or foot $750 $3,750 $2,250 $3,750 $500 $1,500One or more fingers or toes $700 $1,000 $850 $1,000 $400 $500
ENHANCED PLAN Rider Benefit
Total Benefit Amount
Rider Benefit
Total Benefit Amount
Rider Benefit
Total Benefit Amount
Both arms and both legs $0 $30,000 $15,000 $30,000 $5,000 $15,000Both: eyes, hands, feet, legs or arms $0 $15,000 $7,500 $15,000 $2,500 $7,500One: arm, leg, eye, hand or foot $1,500 $7,500 $4,500 $7,500 $1,750 $3,750One or more fingers or toes $900 $1,500 $1,200 $1,500 $550 $750
ACCIDENTAL DEATHSpouse Child
BAsIC PLAN Rider Benefit
Total Benefit Amount
Rider Benefit
Total Benefit Amount
Common Carrier $25,000 $50,000 $15,000 $25,000Other Accident $7,500 $15,000 $2,500 $7,500
ENHANCED PLAN Rider Benefit
Total Benefit Amount
Rider Benefit
Total Benefit Amount
Common Carrier $50,000 $100,000 $30,000 $50,000Other Accident $15,000 $30,000 $5,000 $15,000