Group A streptococcal (GAS) pharyngitis: food-borne outbreak
11
• Case study: outbreak of tonsillopharyngitis in 42 soldiers (Israel) • Signs/symptoms at presentation: fever, sore throat, headache • Physical examination: exudative pharyngitis • Final diagnosis: acute tonsillitis • Transmission: via food stored outdoors (unrefrigerated) for several hours and consumed the day before clinical presentation • Treatment: iv penicillin V + iv fluid replacement during hospitalisation Group A streptococcal (GAS) pharyngitis: food-borne outbreak Hussein A. ECCMID 2014 abs. P1802 Transmission via contaminated food may cause GAS tonsillitis outbreaks Data from poster
-
Upload
annabella-oral -
Category
Documents
-
view
67 -
download
1
description
Group A streptococcal (GAS) pharyngitis: food-borne outbreak. Case study: outbreak of tonsillopharyngitis in 42 soldiers (Israel) Signs/symptoms at presentation: fever, sore throat, headache Physical examination: exudative pharyngitis Final diagnosis: acute tonsillitis - PowerPoint PPT Presentation
Transcript of Group A streptococcal (GAS) pharyngitis: food-borne outbreak
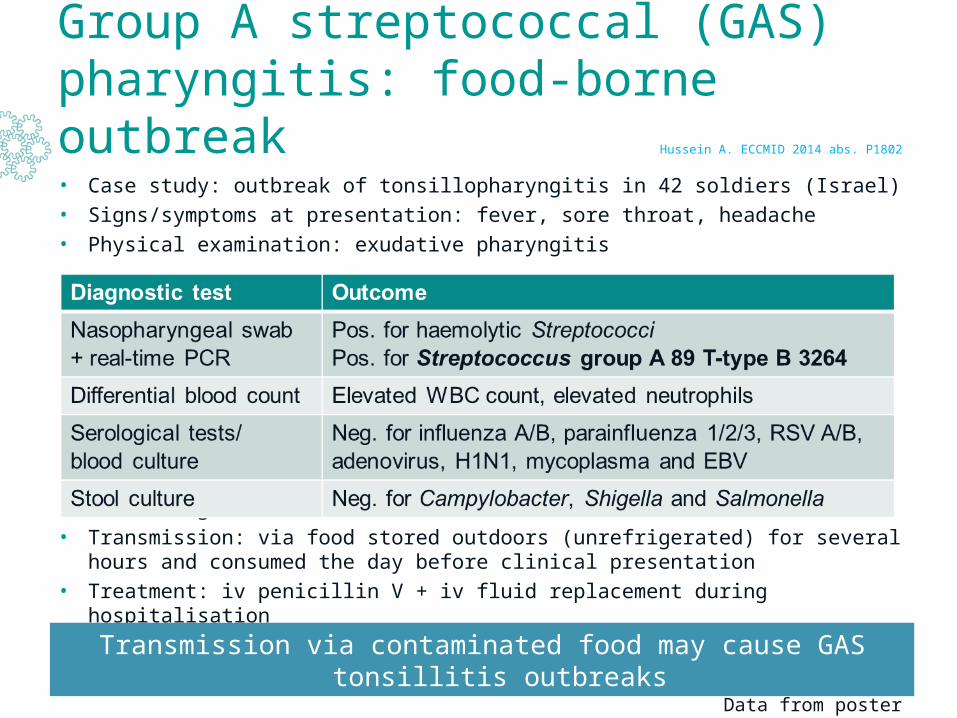
• Case study: outbreak of tonsillopharyngitis in 42 soldiers (Israel)
• Signs/symptoms at presentation: fever, sore throat, headache
• Physical examination: exudative pharyngitis
• Final diagnosis: acute tonsillitis
• Transmission: via food stored outdoors (unrefrigerated) for several hours and consumed the day before clinical presentation
• Treatment: iv penicillin V + iv fluid replacement during hospitalisation
Group A streptococcal (GAS) pharyngitis: food-borne outbreak
Hussein A. ECCMID 2014 abs. P1802
Transmission via contaminated food may cause GAS tonsillitis outbreaks
Data from poster

Adults hospitalised with respiratory syncytial virus (RSV) infection: characteristics and outcomes
• Multi-centre, retrospective cohort study (09/2012-06/2013; 4 tertiary care teaching hospitals; Canada): N=86 hospitalised adults with RSV infection diagnosed by PCR (exluding pts with nosocomial RSV infection or whose RSV infection was not the cause of hospital admission)
• Median age: 74 yr (range: 19-102: 34% <65 yr); 56% females
• Most common reasons to attend ED: shortness of breath, productive cough
Volling C. ECCMID 2014 abs. eP070
1 of 2
Data from poster
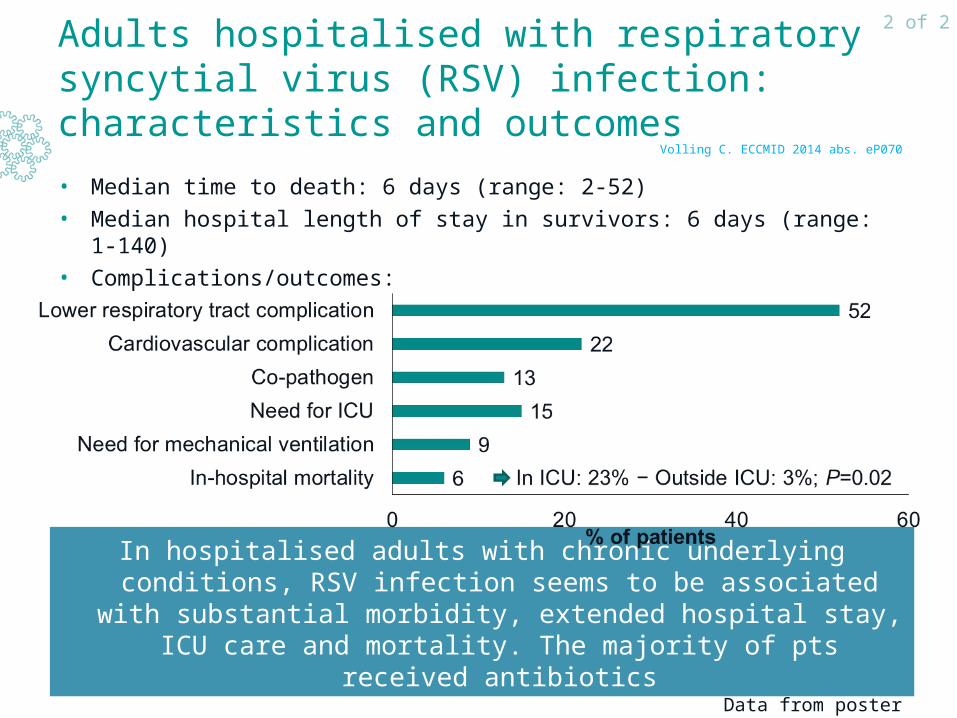
Adults hospitalised with respiratory syncytial virus (RSV) infection: characteristics and outcomes
• Median time to death: 6 days (range: 2-52)
• Median hospital length of stay in survivors: 6 days (range: 1-140)
• Complications/outcomes:
• Pts receiving antibiotics: 78% − anti-influenza therapy: 36%
In hospitalised adults with chronic underlying conditions, RSV infection seems to be associated with substantial morbidity, extended hospital stay, ICU care and mortality. The majority of pts received antibiotics
Volling C. ECCMID 2014 abs. eP070
2 of 2
Data from poster
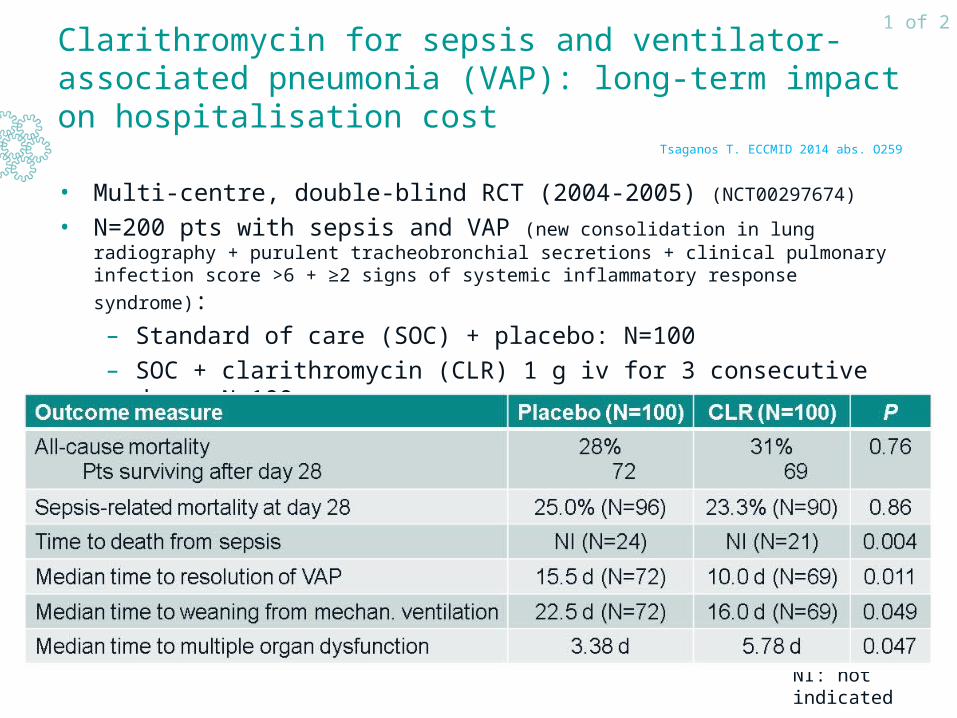
Clarithromycin for sepsis and ventilator-associated pneumonia (VAP): long-term impact on hospitalisation cost
• Multi-centre, double-blind RCT (2004-2005) (NCT00297674)
• N=200 pts with sepsis and VAP (new consolidation in lung radiography + purulent tracheobronchial secretions + clinical pulmonary infection score >6 + ≥2 signs of systemic
inflammatory response syndrome):
– Standard of care (SOC) + placebo: N=100
– SOC + clarithromycin (CLR) 1 g iv for 3 consecutive days: N=100• Short-term results: Giamarellos-Bourboulis EJ et al. Clin Infect Dis 2008;46:1157-64
Tsaganos T. ECCMID 2014 abs. O259
1 of 2
NI: not indicated

Clarithromycin for sepsis and ventilator-associated pneumonia (VAP): long-term impact on hospitalisation cost
• Cumulative hospitalisation cost up to day 45 after diagnosis of VAP
(including imaging tests, interventions e.g. catheterisations, haemodialysis, consumables, lab
tests, drugs, iv fluid, (par)enteral nutrition):
CLR < placebo: P<0.05 starting from day 25 after study enrolment
Addition of clarithromycin to SOC may considerably reduce the long-term hospitalisation cost in pts with sepsis and VAP
Tsaganos T. ECCMID 2014 abs. O259
2 of 2

• Multi-centre, open-label, rater-blinded, randomised non-inferiority study (Switzerland) in adults hospitalised for moderately severe CAP (Pneumonia Severity Index (PSI) ≤IV) confirmed on X-ray (mean age: 76 yr; mean PSI: ±84)
• Mono Tx: amoxicilline/clavulanate or cefuroxime: N=291
• Combi Tx: amoxicilline/clavulanate or cefuroxime + clarithromycine: N=289
Primary endpoint: % of pts not reaching clinical stability* at day 7
β-lactam + macrolide vs β-lactam monotherapy in pts hospitalised for community-acquired pneumoniae (CAP)
Garin N. ECCMID 2014 abs. eP064
1 of 2
Data from poster
*Heart rate <100 bpm, systolic blood pressure >90 mmHg, temperature <38.0°C, respiratory rate <24/min, oxygen saturation >90% on room air

• Predictors of delayed clinical stability:
– Infection with atypical pathogens: HR=0.33; 95% CI: 0.13-0.85; P=0.02
– PSI category IV: HR=0.81; 95% CI: 0.59-1.10; P=0.18 (trend)(vs PSI category I-III: HR=1.06; 95% CI: 0.82-1.36; P=0.66)
β-lactam + macrolide vs β-lactam monotherapy in pts hospitalised for community-acquired pneumoniae (CAP)
Non-inferiority of β-lactam mono Tx vs macrolide combi Tx could not be demonstrated in pts hospitalised for moderately severe CAP
Garin N. ECCMID 2014 abs. eP064
2 of 2
Data from poster
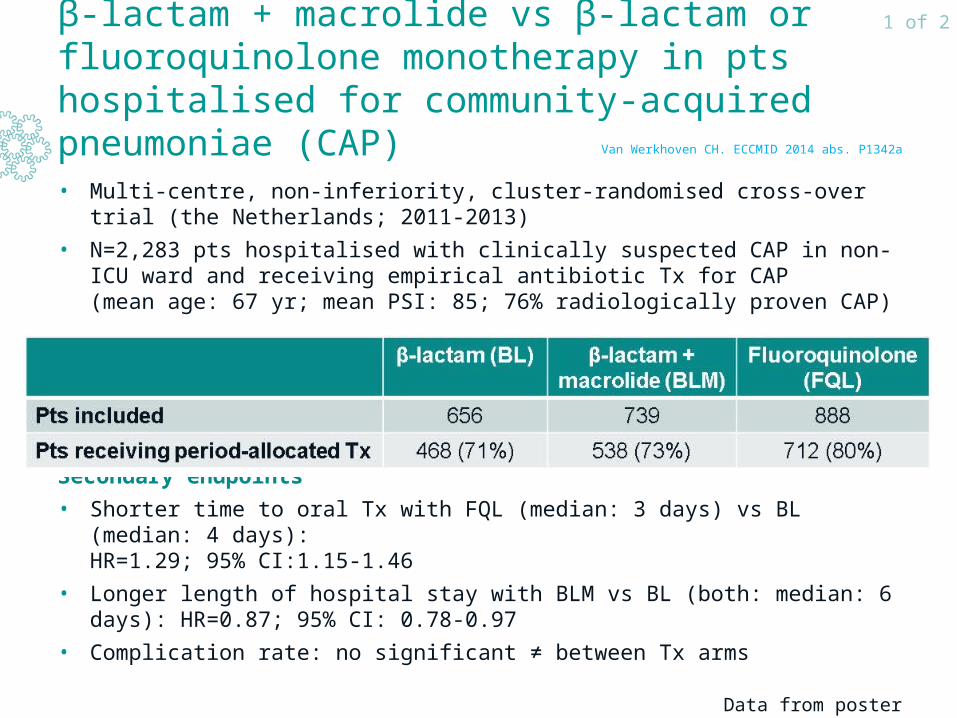
β-lactam + macrolide vs β-lactam or fluoroquinolone monotherapy in pts hospitalised for community-acquired pneumoniae (CAP)
• Multi-centre, non-inferiority, cluster-randomised cross-over trial (the Netherlands; 2011-2013)
• N=2,283 pts hospitalised with clinically suspected CAP in non-ICU ward and receiving empirical antibiotic Tx for CAP (mean age: 67 yr; mean PSI: 85; 76% radiologically proven CAP)
Secondary endpoints
• Shorter time to oral Tx with FQL (median: 3 days) vs BL (median: 4 days): HR=1.29; 95% CI:1.15-1.46
• Longer length of hospital stay with BLM vs BL (both: median: 6 days): HR=0.87; 95% CI: 0.78-0.97
• Complication rate: no significant ≠ between Tx arms
Van Werkhoven CH. ECCMID 2014 abs. P1342a
1 of 2
Data from poster

β-lactam + macrolide vs β-lactam or fluoroquinolone monotherapy in pts hospitalised for community-acquired pneumoniae (CAP)
Empirical Tx with BL for pts hospitalised to non-ICU wards with clinically suspected CAP was non-inferior to BLM or FQL for 90-day
mortality
Van Werkhoven CH. ECCMID 2014 abs. P1342a
2 of 2
Data from poster

Impact of macrolide use on mortality in ICU pts with community-acquired pneumoniae (CAP)
• Systematic literature review + meta-analysis: 28 observational studies
(no RCTs) comparing macrolide Tx with other regimens in ICU pts with CAP
• N=9,850 pts: mean age: 58-78 yr; ♀: 14-49%
Sligl WI et al. Crit Care Med 2014;42:420-32
1 of 2
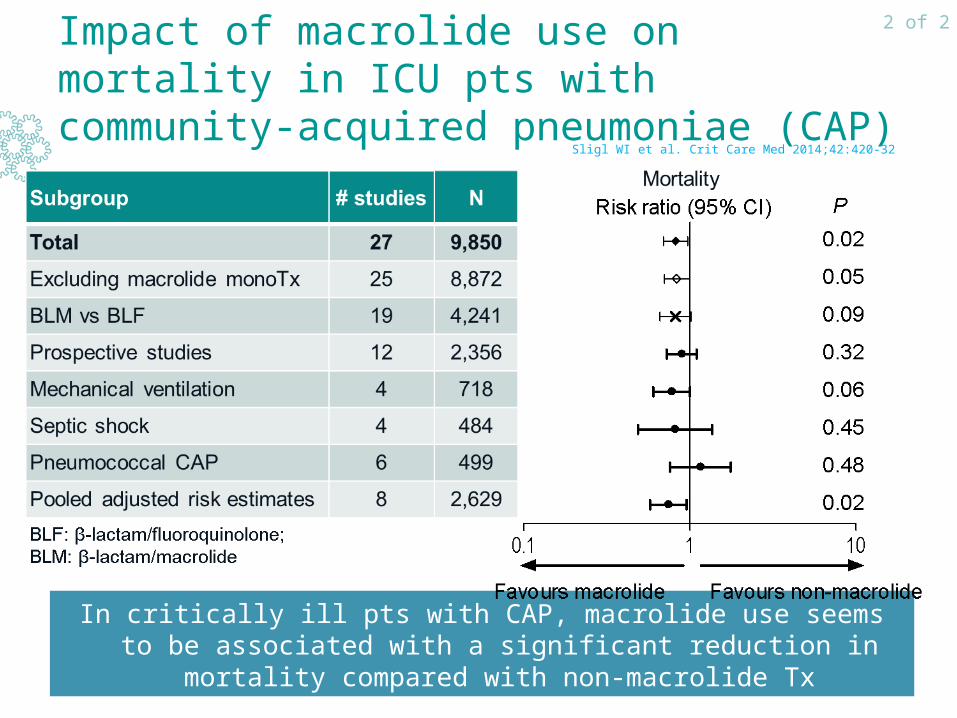
Impact of macrolide use on mortality in ICU pts with community-acquired pneumoniae (CAP)
In critically ill pts with CAP, macrolide use seems to be associated with a significant reduction in mortality compared with non-macrolide Tx
Sligl WI et al. Crit Care Med 2014;42:420-32
2 of 2