Grim Diagnosis of Obamacare
28
- 0- GRIM DIAGNOSIS A check-up on the federal health law United States Senate 111th Congress Senator Tom Coburn, M.D. Senator John Barrasso, M.D. October 2010
Transcript of Grim Diagnosis of Obamacare
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 1/27
- 0
GRIM DIAGNOSISA check-up on the federal health law
United States Senate
111th Congress
Senator Tom Coburn, M.D.
Senator John Barrasso, M.D.
October 2010

8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 2/27
- 1
Contents
Introduction………………………………………………………………………………………………… ..…2
1. Hundreds of Thousands of Jobs Being Lost……………………………………………………………4
2. New Penalty Lowers Income………………………..……………………………………………………7
3. Higher Spending, Rising Deficits………………………………………………………………………11
4. Washington Mandates Send State Costs Skyrocketing……………………………………….……13
5. Increasing ER Wait Times, Costs………..………..…………………………………………………...16
6. Risky Insurance ―Scheme‖ To Cost Taxpayers.………………………………………………………18
7. Medicare Outlook Growing Worse...…………………………………………………………………...21
8. Higher Costs, Fewer Jobs For Young Americans……………………………………………………23
9. Costs Increasing for Employers……….………….…………………………………………………….25
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 3/27
- 2
Introduction
Before it became law, supporters argued the federal health care overhaul would become more popular
after it passed Congress.1 However, more than two hundred days later, Americans remain deeply divided
about the new law. Today, most Americans remain opposed to the law or are still unsure about the law‘s
impact.2 And as Americans learn more about the new law, they have more reasons to be concerned about
the future of our health care system.
Proponents of the health care overhaul often pledged that health reform would allow Americans who liked
their current health plan to keep it. But In June, the U.S. Department of Health and Human Services
issued rules limiting changes employers can make to health insurance plans, and still be considered to be
―grandfathered‖ – or exempt from many of the new mandates in the law. Under the Department‘s own
estimates, more than half of companies may have to give up their current health coverage because of the
new law by 2013.3 And, in their estimate, the Administration predicts that eight in 10 small businesses
could lose their current health plans.4
Supporters of the health care legislation said it would reduce the deficit. However, in June, the
Congressional Budget Office (CBO) estimated that, even with the new health care overhaul, ―rapidly
rising health care costs will sharply increase federal spending for health care programs.‖5 CBO Director
Doug Elmendorf told Congress that the health care overhaul did little to put the country on track toward
fiscal responsibility.6
Advocates for the legislation also dismissed concerns we raised that cuts to Medicare to fund new
government programs could also negatively impact seniors‘ access to care. Yet in August, the Medicare
trustees‘ examined the nearly $530 billion in cuts to the Medicare program and concluded that ―there is a
strong likelihood‖ that the Medicare changes under the new law ―will not be viable.‖7 This means that
promised savings from the Medicare cuts are unrealistic and that future changes to the law could
increase spending and the deficit. The official Chief Actuary of Medicare warned that ―the financial
projections shown in [the] report for Medicare do not represent a reasonable expectation for actual
program operations in either the short range … or the long range,‖ and even issued a second analysis
based on ―more sustainable assumptions‖ that showed costs to federal taxpayers continuing to skyrocket. 8
1On Sunday, March 21, 2010, the House of Representatives passed the Patient Protection and Affordable Care Act (HR 3590)—which the Senate previously passed on
December 24, 2009—and a reconciliation package (HR 4872) designed to amend certain provisions of the Senate bill. HR 3590 became Public Law Number 111-148 on
March 23, 2010. HR 4872 was cleared for the White House and President Obama signed it into law on March 30, 2010.2
Pew Research Center/National Journal Congressional Connection Poll, September 9-12, 2010. http://people-press.org/reports/questionnaires/653.pdf 3 U.S. Department of Health and Human Services, “Group Health Plans and Health Insurance Coverage Relating to Status as a Grandfathered Health Plan Under the
Patient Protection and Affordable Care Act; Interim Final Rule and Proposed Rule,” June 17, 2010. http://www.regulations.gov/search/Regs/contentStreamer?objectId=0900006480b03a90&disposition=attachment&contentType=pdf 4 U.S. Department of Health and Human Services, “Group Health Plans and Health Insurance Coverage Relating to Status as a Grandfathered Health Plan Under the
Patient Protection and Affordable Care Act; Interim Final Rule and Proposed Rule,” June 17, 2010.
http://www.regulations.gov/search/Regs/contentStreamer?objectId=0900006480b03a90&disposition=attachment&contentType=pdf 5 Congressional Budget Office, “The Long Term Budget Outlook,” June 2010, Revised August 2010. http://www.cbo.gov/ftpdocs/115xx/doc11579/06-30-LTBO.pdf
6 Congressional Budget Office, “The Long Term Budget Outlook,” June 2010, Revised August 2010. http://www.cbo.gov/doc.cfm?index=11579, page 11 of PDF.
7 The Boards Of Trustees, Federal Hospital Insurance And Federal Supplementary Medical Insurance Trust Funds, “ 2010 Annual Report Of The Boards Of Trustees Of
The Federal Hospital Insurance And Federal Supplementary Medical Insurance Trust Funds.” http://www.cms.gov/ReportsTrustFunds/downloads/tr2010.pdf , page
287 of PDF.8 The Boards Of Trustees, Federal Hospital Insurance And Federal Supplementary Medical Insurance Trust Funds, “ 2010 Annual Report Of The Boards Of Trustees Of
The Federal Hospital Insurance And Federal Supplementary Medical Insurance Trust Funds.” http://www.cms.gov/ReportsTrustFunds/downloads/tr2010.pdf , page
288 of PDF.
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 4/27
- 3
The finances of the federal government are in even worse shape. This year the federal budget deficit is
projected to climb to $1.3 trillion.9 Our national debt stands at a whopping $13.6 trillion. The interest
that taxpayers pay on the national debt totals more than $20 billion a month.10
The outlook for the economy could get worse if action is not taken. According to a CBO analysis from
earlier this year, ―further increases in federal debt …almost certainly lie ahead if current policies remain
in place.‖11 ―Persistent deficits and continually mounting debt would have several negative economic
consequences for the United States,‖ CBO said, including an ―increase [in] the probability of a sudden
fiscal crisis.‖12
With our economic situation dire and our country‘s future hanging in the balance, the issues of the
economy, debt, spending, and jobs are among most Americans‘ top concerns.13 A recent survey found that
nearly nine in 10 voters were deeply concerned about the overall economic situation, with unemployment
a close second concern.14
Unfortunately, the overhaul that passed Congress this spring did not represent the real health reform
Americans want and need. The new law focused on some of the symptoms in our health care system, but
failed to address the underlying disease. For a majority of Americans, the cost of health coverage is their
primary concern.15 For too many, cost is the access problem. Unfortunately, the new law increases costs
to patients, consumers, and taxpayers, while exacerbating many existing problems in health care.
This report presents the American people with a second opinion on the economic and financial impacts of
the new health care law. Americans have a right to know how their health care, jobs, and financial
stability will be impacted by the new law. The health overhaul threatens our nation‘s economic recovery,
increases costs, and reduces job growth.
As practicing physicians, we are committed to real health care reform. Costs are too high. Choices are too
few. Health coverage remains out of reach for too many Americans. Interference from government
bureaucrats and insurance companies is too constant and pervasive. We believe real reform begins with
replacing the new law with sensible provisions that will lower costs, increase patient control, reduce
bureaucracy and government interference, and put affordable, high quality health coverage within the
reach of every American.
Tom Coburn, M.D. and John Barrasso, M.D.
U.S. Senators
9 Congressional Budget Office, “The Budget and Economic Outlook: An Update,” August 2010.http://www.cbo.gov/ftpdocs/117xx/doc11705/2010_08_19_SummaryforWeb.pdf 10
U.S. Department of the Treasury, Financial Management Service. “Monthly Treasury Statement of Receipts and Outlays of the United States Government For Fiscal
Year 2010 Through August 31, 2010.” http://www.fms.treas.gov/mts/mts0810.pdf See highlight on cover page and detail on page 2811
Congressional Budget Office, “Federal Debt and the Risk of a Fiscal Crisis,” July 27, 2010.
http://www.cbo.gov/ftpdocs/116xx/doc11659/07-27_Debt_FiscalCrisis_Brief.pdf 12
Congressional Budget Office, “Federal Debt and the Risk of a Fiscal Crisis,” July 27, 2010.
http://www.cbo.gov/ftpdocs/116xx/doc11659/07-27_Debt_FiscalCrisis_Brief.pdf 13
Jones, Jeffrey. “Voters Rate Economy as Top Issue for 2010,” April 8, 2010. http://www.gallup.com/poll/127247/voters-rate-economy-top-issue-2010.aspx 14
Buhr, Tami. “Fox News Poll: Economic Worries Plague American Voters,” September 6, 2010.
http://www.foxnewsinsider.com/2010/09/06/fox-news-poll-economic-worries-plague-american-voters/ 15
U.S. Department of Health and Human Services, “America Speaks on Health Reform: Report on Health Care Community Discussions,” page 101, March 2009,
http://www.healthreform.gov/reports/hccd/report_on_communitydiscussions.pdf .
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 5/27
- 4
Hundreds of Thousands of Jobs Being Lost
Before the health care legislation became law, proponents of the overhaul claimed that health reform
would create jobs. At the White House health care summit in February, the Speaker of the House of
Representatives asserted the federal health care overhaul would create ―400,000 jobs almost
immediately,‖ both in the health care industry and ―in the entrepreneurial world as well.‖16 However,
recent independent reviews have contradicted such rosy scenarios and found the legislation will wipe out
hundreds of thousands of jobs.17
Nonpartisan Experts Conclude Health Overhaul Reduces Labor Force By 788,000 Jobs
The nonpartisan Congressional Budget Office (CBO)
released an analysis of the ―effects of recent health care
legislation on labor markets.‖18 The CBO‘s findings painted
a troubling picture. The massive Medicaid expansion will
―encourage some people to work fewer hours or to withdraw
from the labor market.‖19 Additionally, phasing out the
subsidies to buy expensive insurance ―will effectively
increase marginal tax rates, which will also discouragework.‖20 CBO said ―other provisions in the legislation are
also likely to diminish people‘s incentives to work.‖ 21
The CBO ―estimates that the legislation, on net, will reduce
the amount of labor used in the economy by a small
amount — roughly half a percent — primarily by reducing the
amount of labor that workers choose to supply‖, which is more than 788,470 employees.22 Another
independent estimate predicted the overhaul will ―destroy a total of 120,000 to 700,000 jobs by 2019.‖23
This is a huge number of future jobs and future workers that will be effectively sidelined because of the
health reform legislation. With more than 14 million Americans out of work today, we cannot afford to
lose more jobs.
New Provisions Kill Health Care Industry Jobs
The CBO‘s analysis did not even take into account the overhaul‘s job impact on specific industries.
Unfortunately, the lost jobs count can be expected to climb even higher because of a simple provision
16Pelosi, Nancy. “Remarks by the President, Senator Alexander, Speaker Pelosi, and Senator Reid in Opening Statements at Bipartisan Meeting on Health Care
Reform,” The White House, February 25, 2010.
http://www.whitehouse.gov/the-press-office/remarks-president-senator-alexander-speaker-pelosi-and-senator-reid-opening-stateme17 In addition to the analysis on CBO’s findings in this report, see Tuerck, David, et. al. “Killing Jobs through National Health Care Reform,” Beacon Hill Institute Policy
Study, March 2010. http://www.atr.org/userfiles/BHI%20Health%20Care%20Reform%20as%20Job%20Killer(7).pdf 18
Congressional Budget Office, “The Budget and Economic Outlook: An Update,” August 2010, page 66-67 of PDF.
http://cbo.gov/ftpdocs/117xx/doc11705/08-18-Update.pdf 19
Congressional Budget Office, “The Budget and Economic Outlook: An Update,” August 2010, page 66-67 of PDF.
http://cbo.gov/ftpdocs/117xx/doc11705/08-18-Update.pdf 20
Congressional Budget Office, “The Budget and Economic Outlook: An Update,” August 2010, page 66-67 of PDF.
http://cbo.gov/ftpdocs/117xx/doc11705/08-18-Update.pdf 21
Congressional Budget Office, “The Budget and Economic Outlook: An Update,” August 2010, page 66-67 of PDF.
http://cbo.gov/ftpdocs/117xx/doc11705/08-18-Update.pdf 22
Congressional Budget Office, “The Budget and Economic Outlook: An Update,” August 2010, page 66-67 of PDF.
http://cbo.gov/ftpdocs/117xx/doc11705/08-18-Update.pdf . According to a U.S. Department of Labor estimate, the 2010 labor force is estimated to comprise
157,695,000 workers. Half of one of percent of our nation’s 157 million workforce equals 788,475 workers. Lee, Marlene and Mather, Mark. “U.S. Labor Force
Trends,” Population Bulletin, Vol. 63, No. 2, June 2008. http://www.prb.org/pdf08/63.2uslabor.pdf 23
Tuerck, David, et. al. “Killing Jobs through National Health Care Reform,” Beacon Hill Institute Policy Study, March 2010.
http://www.atr.org/userfiles/BHI%20Health%20Care%20Reform%20as%20Job%20Killer(7).pdf
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 6/27
- 5
tucked into the legislation. Section 6001 of the health overhaul prohibits hospitals owned by physicians
from expanding and denied Medicare reimbursements to any physician-owned hospitals not certified by
Medicare by the end of the year.
According to a Washington Times report, ―the Physician Hospitals of America (PHA) identified 39 projects
under development whose owners had canceled outright, knowing they could not win Medicare
certification by the end-of-year deadline, plus another 45 that will be hard-pressed to meet Medicare
certif ication criteria in time.‖24 Sadly, according to PHA conversations with its member hospitals, the
canceled projects could have created ―roughly 25,000 jobs.‖25
As the Times article notes, the ―job-killingprovisions‖ of the overhaul are ―particularly ironic given that physician-owned facilities tend to be
economically efficient and deliver superior medical outcomes.‖26
Ironically, while the new law has made it illegal for physicians to have further ownership in a hospital,
the law has the effect of increasing a hospital system‘s ―ownership‖ of an individual physician. The
legislation embraces a pilot payment model of ―accountable care organizations‖ (ACOs). While integrated
care delivery teams are a good goal, the manner in which the legislation designed ACOs could accelerate
the trend of physicians leaving private practice to work in a centralized hospital setting. Over the next
three years, three in four hospitals or health systems reported they plan on hiring more physicians, and
more than half said they will buy entire medical practices.27
A former policy advisor at the Centers for Medicare and Medicaid Services (CMS) described the approachof the law as envisioning ―that doctors will fold their private offices to become salaried hospital
employees, making it easier for the federal government to regulate them and centrally manage the costly
medical services they prescribe.‖28 The former CMS official suggested that the centralization of physician
employment has already begun, noting that ―in 2005, more than two-thirds of medical practices were
doctor-owned, a share that was largely constant for many years. By next year, the share of practices
owned by physicians will probably drop below 40 percent, according to data from the Medical Group
Management Association.‖29 Even a White House official who helped push the overhaul through
Congress recently admitted in an article that ―the economic forces put in motion by the [health
legislation] are likely to lead to vertical organization of providers and accelerate physician employment by
hospitals and aggregation into larger physician groups.‖30 Coordinated care is admirable, but greater consolidation of providers under a hospital would increase a
hospital system‘s market share and negotiating power over remaining providers. With less choice and
competition in the health care marketplace, costs to consumers would likely increase even further.31 As
the Center for Studying Health System Change concluded from a recent study of California‘s experience
in similar attempted reforms, ―proposals to promote integrated care through models such as accountable
24 Bacon, James. “Casualties Heavy at hospitals,” The Washington Times, August 27, 2010.
http://www.washingtontimes.com/news/2010/aug/27/casualties-heavy-at-hospitals/ 25
Bacon, James. “Casualties Heavy at hospitals,” The Washington Times, August 27, 2010.
http://www.washingtontimes.com/news/2010/aug/27/casualties-heavy-at-hospitals/
26 Bacon, James. “Casualties Heavy at hospitals,” The Washington Times, August 27, 2010. http://www.washingtontimes.com/news/2010/aug/27/casualties-heavy-at-hospitals/ 27
Gottlieb, Scott. “Killing Marcus Wellby,” The New York Post, October 18, 2010.
http://www.nypost.com/p/news/opinion/opedcolumnists/killing_marcus_welby_FLnABqCKwpyF9j2i9YYpCP#ixzz12qe8huWV28
Gottlieb, Scott. “Killing Marcus Wellby,” The New York Post, October 18, 2010.
http://www.nypost.com/p/news/opinion/opedcolumnists/killing_marcus_welby_FLnABqCKwpyF9j2i9YYpCP#ixzz12qe8huWV29
Gottlieb, Scott. “Killing Marcus Wellby,” The New York Post, October 18, 2010.
http://www.nypost.com/p/news/opinion/opedcolumnists/killing_marcus_welby_FLnABqCKwpyF9j2i9YYpCP#ixzz12qe8huWV30
Kocher, Robert MD; Emanuel, Emanuel MD; and DeParle, Nancy-Ann. “The Affordable Care Act and the Future of Clinical Medicine: The Opportunities and
Challenges,” Annals of Internal Medicine, August 23, 2010.
http://www.annals.org/content/early/2010/08/23/0003-4819-153-8-201010190-00274.1.full?aimhp 31
Terry, Ken. “Why Hospitals Shouldn’t Run ‘Accountable Care Organizations,’” Critical Condition, BNET.com, September 28, 2010.
http://www.bnet.com/blog/healthcare-business/why-hospitals-shouldn-8217t-run-8220accountable-care-organizations-8221/1836
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 7/27
- 6
care organizations could lead to higher rates for private payers.‖ In other words, consumers could pay
even more for health insurance and health care.32
Stifling Innovation and Jobs
It is not only hospitals that are seeing health care jobs threatened.
Companies that innovate, create, and develop life-saving, life-
improving devices will likely lose jobs too. Manufacturers of
medical devices are reeling from a provision of the law that willlevy a $20 billion excise tax on their industry. The Boston Globe
reported that the ―2.3 percent excise tax on companies that supply
medical devices like heart defibrillators and surgical tools to
hospitals, health centers and ambulance services,‖ will force
industry leaders to ―lay off workers and curb the research and
development of new medical tools.‖33 One CEO said the new tax
threatens his business‘ sustainability because it has relegated his
company‘s profitability to merely ―a break-even position.‖34
The basic problem with the tax is one of math. ―‗Many small to midsize medical device companies will owe
more to the federal government in taxes than they make in profits,‘‖ according to Mark Leahy, head of the
Medical Device Manufacturers Association.35 "We're talking about a 2.3 percent tax on total sales,irrespective of whether a company is making a profit."36 The device tax will hamper innovation, since the
amount of money available for a company to reinvest in its business development will be reduced. Some
companies are already contemplating moving jobs overseas to avoid losing their competitive edge.
Outsourcing is just one of many adverse unintended consequences of the new law.37
32 Berenson, Robert; Ginsburg, Paul; and Nicole Kemper. “Unchecked Provider Clout In California Foreshadows Challenges To Health Reform,” Health Affairs, 29, NO.4, 2010. http://content.healthaffairs.org/cgi/reprint/hlthaff.2009.0715v1 33
LeBlanc, Steve. “Medical device makers: New tax will cost jobs,” The Boston Globe, June 7, 2010.
http://www.boston.com/business/taxes/articles/2010/06/07/medical_device_makers_new_tax_will_cost_jobs/ 34
LeBlanc, Steve. “Medical device makers: New tax will cost jobs,” The Boston Globe, June 7, 2010.
http://www.boston.com/business/taxes/articles/2010/06/07/medical_device_makers_new_tax_will_cost_jobs/ 35
LeBlanc, Steve. “Medical device makers: New tax will cost jobs,” Bloomberg Businessweek, June 7, 2010.
http://www.businessweek.com/ap/financialnews/D9G6G7HG0.htm 36
LeBlanc, Steve. “Medical device makers: New tax will cost jobs,” Bloomberg Businessweek, June 7, 2010.
http://www.businessweek.com/ap/financialnews/D9G6G7HG0.htm 37
Fitzgerald, Jay. “Beware: the ‘jobs killer,’” The Boston Herald, March 25, 2010.
http://www.bostonherald.com/business/general/view/20100325beware_the_jobs_killer_companies_threaten_to_quit_state_over_new_tax_on_medical_devices/sr
vc=home&position=0
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 8/27
- 7
New Penalty Lowers Income
New Penalty Reduces Income, Job Growth
Many Americans are aware of the controversial ―individual mandate‖ in the health care overhaul . But an
equally problematic provision is that one that fines businesses who do not provide government approved
health insurance to their employees.
Sections 1513 and 1003 of health care bills that
passed Congress created new penalties for
businesses that do not offer health insurance to
their employers. While proponents insist this is not
a mandate because businesses are penalized but
not required to offer coverage, in function this
requirement is a defacto ―employer mandate.‖
Beginning in 2014, businesses with more than 50
employees will be fined $2,000 per employee if they
do not provide government approved health
insurance for their employees.38
This intervention in the labor market creates a
permanent disincentive against business growth. If a 50-employee small business that did not offer
health insurance wanted to expand by merely adding one new employee, they would become subject to the
employer requirements of the law. So it is actually in the business‘ interest not to hire an additional
employee, lest they be hit with thousands of dollars in fines. For a fraction of that money, the business
could hire a part-time employee or independent contractors to perform tasks, rather than grow the
business by adding an employee.39
Businesses and Employees Concerned about Employer Provision
Sadly, this employer provision hurts low-income, minority workers the most. Dr. Kate Baicker found in astudy that one-third of ―uninsured workers earn within $3 of the minimum wage, putting them at risk of
unemployment if their employers were required to offer insurance.…‖ 40 Even worse, ―workers who
would lose their jobs are disproportionately likely to be high school dropouts, minority, and female.…
Thus, among the uninsured, those with the least education face the highest risk of losing their jobs under
employer mandates.‖41
In a letter last year, more than 1,500 business and pro-business organizations told Congress ―this
provision will kill many jobs.‖42 Earlier this year, the National Federation of Independent Businesses
(NFIB) arrived at a similar conclusion. ―Economic research has shown time and again that mandates are
a ‗one-two punch‘ where the cost is first borne by the employer, but is ultimately paid by the employee –
38The first 30 employees do not count when calculating compliance with this requirement.
39 To examine the impact of this provision, consider a hypothetical small business owner. If a business employed 51 individuals but did not provide these employees
with health insurance, the company would be required to pay the $2,000 fine for each employee, with the first 30 employees in the count exempted from the
requirement. The firm would only be required to pay the $2,000 fine on the remaining 21 employees, but the cost of $2,000 fine for 21 employees is not
insignificant: $42,000. The $42,000 is money that the business cannot use to invest in capital, hire a new employee, or cover administrative costs.40
Katherine Baicker and Amitabh Chandra, “Myths and Misconceptions about U.S. Health Insurance,” Health Affairs, (2008).
http://content.healthaffairs.org/cgi/content/full/27/6/w533 41
Katherine Baicker and Amitabh Chandra, “Myths and Misconceptions about U.S. Health Insurance,” Health Affairs, (2008).
http://content.healthaffairs.org/cgi/content/full/27/6/w533 42
U.S. Chamber of Commerce, et al. Letter to Members of the U.S. Congress, July 28, 2009. Signed by 43 national organizations, as well as 1,473 regional, state, and
local chambers and businesses.
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 9/27
- 8
through job loss and lower wages.‖43 In May, NFIB said that small businesses across the country are
gravely concerned ―the health care law will devastate their business and their ability to create jobs.‖44
The employer provision means businesses either reduce jobs and wages or just stop offering health
coverage. Many businesses have already begun questioning whether or not it makes financial sense under
the new law for them to even continue to offer health insurance. In August, the hamburger chain White
Castle announced that changes to health insurance in health overhaul will consume ―roughly 55 percent
of its yearly net income after 2014.‖45 This massive hit to the company‘s business model may make it hard
for the company – which employs more than 10,000 individuals across the country – to keep its doorsopen.46
Other restaurant chains are weighing their options as
well. The ―entire restaurant industry will have
trouble dealing with costs the bill imposes in 2014,
including a $2,000-per-worker penalty,‖ according to
the National Council of Chain Restaurants.47 One
such example is George Ebinger, the owner of several
International House of Pancakes restaurants.
Ebinger anticipates he will increase prices and
perhaps layoff employees to generate the $220,000 he
expects will be needed to cover the cost of thepenalty.48
Many retailers, who employ thousands of entry-level and part-time employees, are facing a similar
dilemma in calculating the trade-offs between coverage for employees and costs to their business. The
new health overhaul is so complex that the National Retail Federation (NRF) created a ―Health Mandate
Cost Calculator‖ to assist employers in evaluating the landscape of choices they face.49 The business
group says its member companies are concerned about the ―job-killing mandates on employers‖ under the
new law.50 In analyzing the employer provision, a representative of the business group admitted, ―We do
worry about this discouraging employment, particularly when employment hasn't taken off.‖51
Nonpartisan Experts Agree on Negative Impact of Employer Provision
The cost of health insurance remains the primary concern for most companies. According to the
Congressional Research Service, less than half of small businesses offer health coverage and these
employers cite the cost of health care as their primary reason for not offering coverage. 52 Unfortunately,
the defacto employer mandate not only penalizes businesses that do not purchase expensive health
coverage, it creates damaging distortions in the labor market that will lead to lower wages and fewer jobs.
43Visit NFIB.com/healthcare under “Work on the Hill” to read the full letter sent to Leader Reid and Speaker Pelosi on January 11, 2010.
44 http://www.nfib.com/press-media/press-media-item/cmsid/51584
45Eaton, Sabrina. “Ohio hamburger chain says insurance reform will bite into profits,” The Plain Dealer, Cleveland, Ohio.
http://www.cleveland.com/open/index.ssf/2010/07/ohio_hamburger_chain_says_insu.html 46
Eaton, Sabrina. “Ohio hamburger chain says insurance reform will bite into profits,” The Plain Dealer, Cleveland, Ohio.
http://www.cleveland.com/open/index.ssf/2010/07/ohio_hamburger_chain_says_insu.html 47
Eaton, Sabrina. “Ohio hamburger chain says insurance reform will bite into profits,” The Plain Dealer, Cleveland, Ohio.
http://www.cleveland.com/open/index.ssf/2010/07/ohio_hamburger_chain_says_insu.html 48
Eaton, Sabrina. “Ohio hamburger chain says insurance reform will bite into profits,” The Plain Dealer, Cleveland, Ohio.
http://www.cleveland.com/open/index.ssf/2010/07/ohio_hamburger_chain_says_insu.html 49
National Retail Federation, “Health Mandate Cost Calculator.” http://www.nrf.com/modules.php?name=Pages&sp_id=1290 50
Trautwine, Neil. “Pass the scalpel: it’s time for a ‘mandate-ectomy,’” August 27, 2010.
http://blog.nrf.com/2010/08/27/pass-the-scalpel-it%e2%80%99s-time-for-a-%e2%80%9cmandate-ectomy%e2%80%9d/ 51
Eaton, Sabrina. “Ohio hamburger chain says insurance reform will bite into profits,” The Plain Dealer, Cleveland, Ohio.
http://www.cleveland.com/open/index.ssf/2010/07/ohio_hamburger_chain_says_insu.html 52
Chaikind, Hinda, et al. “Private Health Insurance Provisions of H.R. 3962,” (R40885), Congressional Research Service, November 6, 2009. Page 9 of PDF.
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 10/27
- 9
This is the conclusion reached by nonpartisan experts, and even one of the President‘s former advisors.53
The Congressional Budget Office concluded that ―employers‘ decisions to hire workers will also be affected
in some cases by the health care legislation.‖ CBO specifically noted:
―Employers with 50 or more employees will be required to pay a penalty if they do not offer
insurance or if the insurance they offer does not meet certain criteria and at least one of their
workers receives a subsidy from an exchange. Those penalties, whose amounts are based on the
number of full-time workers in the firm, will, over time, generally be passed on to workers through
reductions in wages or other forms of compensation. However, firms generally cannot reduceworkers‘ wages below the minimum wage, which will probably cause some employers to respond by
hiring fewer low-wage workers. Alternatively, because firms are penalized only if their full-time
employees receive subsidies from exchanges, some firms may instead hire more part-time or
seasonal employees.” 54
The employer provision will lower wages and lead to less jobs because workers, not businesses, ultimately
feel the impact of taxes and fines. The Congressional Budget Office also found that an employer penalty
―would impose a new cost on employers‖ which will be passed on to employees.55 ―Employers who chose to
pay the fee rather than offer health benefits would be likely to offset at least some of those costs by paying
lower wages or employing fewer people.” 56
A member of the Congressional Budget Office's panel of health advisers, Dr. Kate Baicker, agrees. Her research
found that ―when it is not possible to reduce wages,
employers may respond in other ways: employment can be
reduced for workers whose wages cannot be lowered,
outsourcing and reliance on temp agencies may increase,
and workers can be moved into part-time jobs where
mandates do not apply.‖57
Experts at the Congressional Research Service (CRS) expect
the same outcomes as well. ―Economic theory suggests the
penalty should ultimately be passed through [as] lowerwages [to an employee].58 But, ―if firms cannot pass on the
cost in lower wages, the higher cost of workers may lead
firms to reduce output and the number of workers‖59
Unfortunately, CRS estimates that about one in five
employees work for a business that could be negatively
impacted by the new employer penalty.60
Even the former director of the Office of Management and Budget, Peter Orzag, has said that increased
costs to employers will be passed on to employees as reduced pay. While serving as director of the
53Peter Orzag, former director of the Office of Management and Budget under President Obama from 2009 through mid-2010.
53 Congressional Budget Office, “The Budget and Economic Outlook: An Update,” August 2010, page 66-67 of PDF, emphasis added.http://cbo.gov/ftpdocs/117xx/doc11705/08-18-Update.pdf 55
Congressional Budget Office, “Budget Options, Volume 1: Health Care,” December 2008, page 25 of PDF.
http://www.cbo.gov/ftpdocs/99xx/doc9925/12-18-HealthOptions.pdf 56
Congressional Budget Office, “Budget Options, Volume 1: Health Care,” December 2008, page 25 of PDF.
http://www.cbo.gov/ftpdocs/99xx/doc9925/12-18-HealthOptions.pdf 57
Baicker, Katherine and Chandra, Amitabh, “Myths and Misconceptions about U.S. Health Insurance,” Health Affairs, 2008.
http://content.healthaffairs.org/cgi/content/full/27/6/w533 58
Gravelle, Jane. “Health Reform and Small Business,” Congressional Research Service, April 8, 2010 (R40775).
http://crs.gov/Pages/Reports.aspx?Source=cli&ProdCode=R40775#_Toc268786482 59
Gravelle, Jane. “Health Reform and Small Business,” Congressional Research Service, April 8, 2010 (R40775).
http://crs.gov/Pages/Reports.aspx?Source=cli&ProdCode=R40775#_Toc268786482 60
Gravelle, Jane. “Health Reform and Small Business,” Congressional Research Service, April 8, 2010 (R40775). http://crs.gov/ReportPDF/R40775.pdf

8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 11/27
- 10
Congressional Budget Office, Mr. Orzag said that ―the economic evidence is overwhelming, the theory is
overwhelming, that when your firm pays for your health insurance you actually pay through reduced
take-home pay. The firm is not giving that to you for free. Your other wages or what have you are reduced
as a result. I don‘t think most workers realize that.‖61
It is not difficult to see why the employer community is deeply concerned. Health care costs continue to
climb. An employer penalty will reduce wages and jobs. It is clear that sections 1513 and 1003 of the
health care overhaul will lead to lower wages and fewer jobs.
61Orszag, Peter. Testimony before the Senate Finance Committee, June 17, 2008, in his capacity as CBO Director.
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 12/27
- 11
Higher Spending, Rising Deficits
While proponents of the health care law argued it would reduce the deficit, in reality, the new law will
blow a hole in the federal budget. Fewer than two in 10 Americans believe the health law will reduce the
deficit, while more than six in 10 believe the overhaul will increase it.62
Americans have ample basis to doubt the massive, 2,700 pages of legislation will decrease the deficit. The
authors of the overhaul purposefully ignored the looming problem of Medicare physician reimbursementsthat could have added more than $250 billion to the law‘s price tag and erased claims of deficit
reduction.63 More recently, the official Actuary of the Centers for Medicare and Medicaid Services
concluded it is ―implausible‖ to pretend Congress will not avert pending Medicare cuts – cuts that if
reversed, would increase spending and could further inflate the deficit. As the Actuary noted, ―current
law would require physician fee reductions totaling an estimated 30 percent over the next 3 years — an
implausible result.‖64
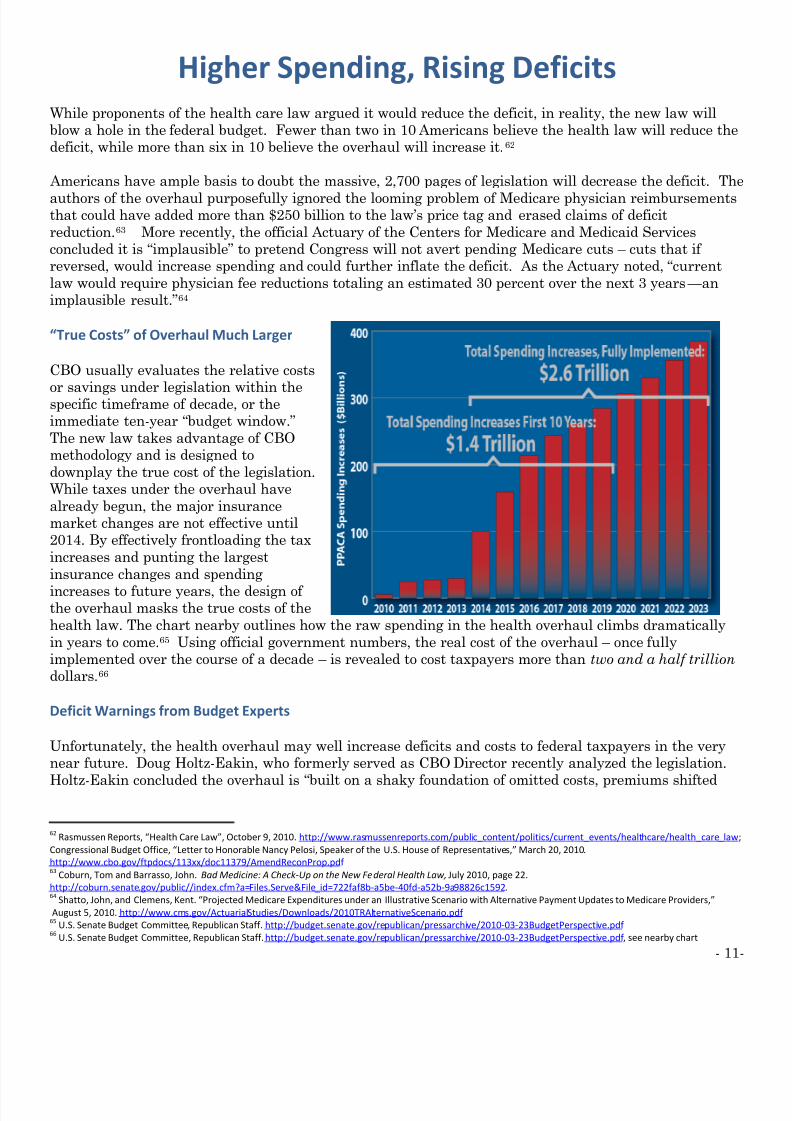
“True Costs” of Overhaul Much Larger
CBO usually evaluates the relative costs
or savings under legislation within thespecific timeframe of decade, or the
immediate ten-year ―budget window.‖
The new law takes advantage of CBO
methodology and is designed to
downplay the true cost of the legislation.
While taxes under the overhaul have
already begun, the major insurance
market changes are not effective until
2014. By effectively frontloading the tax
increases and punting the largest
insurance changes and spending
increases to future years, the design of the overhaul masks the true costs of the
health law. The chart nearby outlines how the raw spending in the health overhaul climbs dramatically
in years to come.65 Using official government numbers, the real cost of the overhaul – once fully
implemented over the course of a decade – is revealed to cost taxpayers more than two and a half trillion
dollars.66
Deficit Warnings from Budget Experts
Unfortunately, the health overhaul may well increase deficits and costs to federal taxpayers in the very
near future. Doug Holtz-Eakin, who formerly served as CBO Director recently analyzed the legislation.
Holtz-Eakin concluded the overhaul is ―built on a shaky foundation of omitted costs, premiums shifted
62 Rasmussen Reports, “Health Care Law”, October 9, 2010. http://www.rasmussenreports.com/public_content/politics/current_events/healthcare/health_care_law;
Congressional Budget Office, “Letter to Honorable Nancy Pelosi, Speaker of the U.S. House of Representatives,” March 20, 2010 .
http://www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp.pdf 63
Coburn, Tom and Barrasso, John. Bad Medicine: A Check-Up on the New Federal Health Law, July 2010, page 22.
http://coburn.senate.gov/public//index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592.64
Shatto, John, and Clemens, Kent. “Projected Medicare Expenditures under an Illustrative Scenario with Alternative Payment Updates to Medicare Providers,”
August 5, 2010. http://www.cms.gov/ActuarialStudies/Downloads/2010TRAlternativeScenario.pdf 65
U.S. Senate Budget Committee, Republican Staff. http://budget.senate.gov/republican/pressarchive/2010-03-23BudgetPerspective.pdf 66
U.S. Senate Budget Committee, Republican Staff. http://budget.senate.gov/republican/pressarchive/2010-03-23BudgetPerspective.pdf , see nearby chart
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 13/27
- 12
from other entitlements, and politically dubious spending cuts and revenue increases.‖67 Mr. Holtz-Eakin
suggested ―a more comprehensive and realistic projection suggests that the new reform law will raise the
deficit by more than $500 billion during the first ten years and by nearly $1.5 trillion in the following
decade.‖68
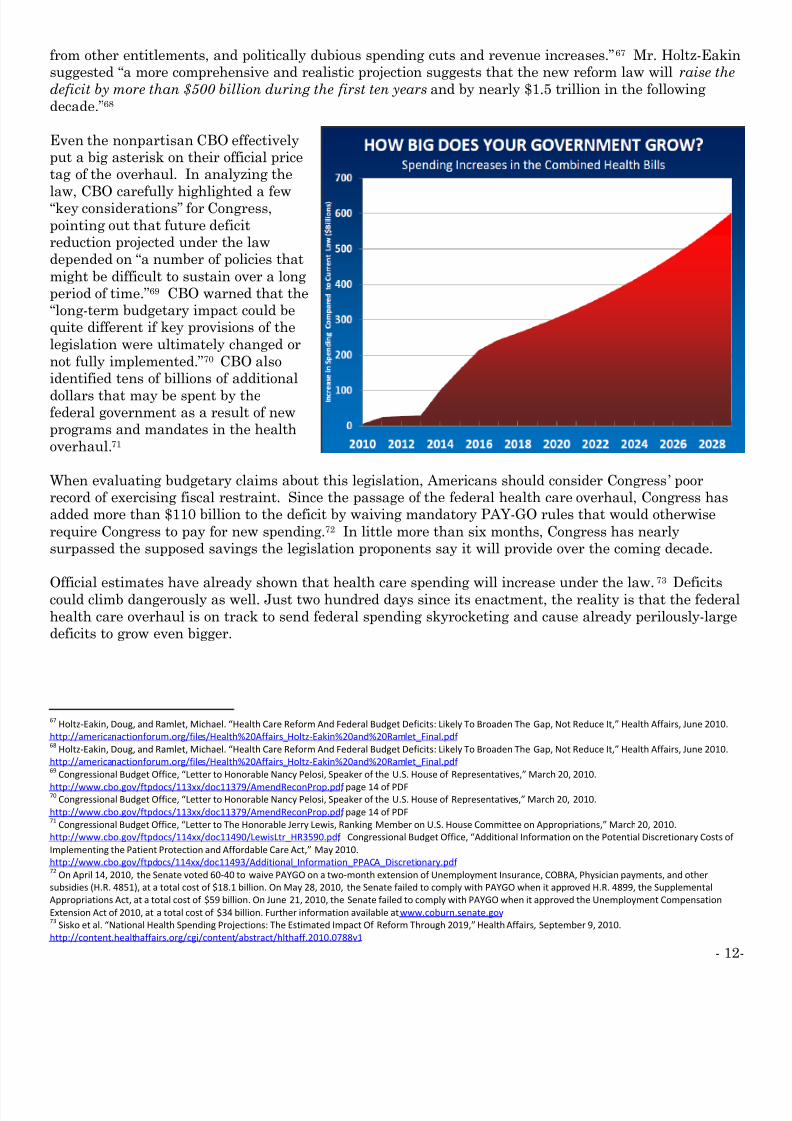
Even the nonpartisan CBO effectively
put a big asterisk on their official price
tag of the overhaul. In analyzing the
law, CBO carefully highlighted a few―key considerations‖ for Congress,
pointing out that future deficit
reduction projected under the law
depended on ―a number of policies that
might be difficult to sustain over a long
period of time.‖69 CBO warned that the
―long-term budgetary impact could be
quite different if key provisions of the
legislation were ultimately changed or
not fully implemented.‖70 CBO also
identified tens of billions of additional
dollars that may be spent by thefederal government as a result of new
programs and mandates in the health
overhaul.71
When evaluating budgetary claims about this legislation, Americans should consider Congress ‘ poor
record of exercising fiscal restraint. Since the passage of the federal health care overhaul, Congress has
added more than $110 billion to the deficit by waiving mandatory PAY-GO rules that would otherwise
require Congress to pay for new spending.72 In little more than six months, Congress has nearly
surpassed the supposed savings the legislation proponents say it will provide over the coming decade.
Official estimates have already shown that health care spending will increase under the law.73
Deficitscould climb dangerously as well. Just two hundred days since its enactment, the reality is that the federal
health care overhaul is on track to send federal spending skyrocketing and cause already perilously-large
deficits to grow even bigger.
67Holtz-Eakin, Doug, and Ramlet, Michael. “Health Care Reform And Federal Budget Deficits: Likely To Broaden The Gap, Not Reduce It,” Health Affairs, June 2010.
http://americanactionforum.org/files/Health%20Affairs_Holtz-Eakin%20and%20Ramlet_Final.pdf 68
Holtz-Eakin, Doug, and Ramlet, Michael. “Health Care Reform And Federal Budget Deficits: Likely To Broaden The Gap, Not Reduce It,” Health Affairs, June 2010.
http://americanactionforum.org/files/Health%20Affairs_Holtz-Eakin%20and%20Ramlet_Final.pdf 69
Congressional Budget Office, “Letter to Honorable Nancy Pelosi, Speaker of the U.S. House of Representatives,” March 20, 2010.
http://www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp.pdf , page 14 of PDF70
Congressional Budget Office, “Letter to Honorable Nancy Pelosi, Speaker of the U.S. House of Representatives,” March 20, 2010.
http://www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp.pdf , page 14 of PDF71
Congressional Budget Office, “Letter to The Honorable Jerry Lewis, Ranking Member on U.S. House Committee on Appropriations,” March 20, 2010.
http://www.cbo.gov/ftpdocs/114xx/doc11490/LewisLtr_HR3590.pdf ; Congressional Budget Office, “Additional Information on the Potential Discretionary Costs of
Implementing the Patient Protection and Affordable Care Act,” May 2010.
http://www.cbo.gov/ftpdocs/114xx/doc11493/Additional_Information_PPACA_Discretionary.pdf 72
On April 14, 2010, the Senate voted 60-40 to waive PAYGO on a two-month extension of Unemployment Insurance, COBRA, Physician payments, and other
subsidies (H.R. 4851), at a total cost of $18.1 billion. On May 28, 2010, the Senate failed to comply with PAYGO when it approved H.R. 4899, the Supplemental
Appropriations Act, at a total cost of $59 billion. On June 21, 2010, the Senate failed to comply with PAYGO when it approved the Unemployment Compensation
Extension Act of 2010, at a total cost of $34 billion. Further information available at www.coburn.senate.gov 73
Sisko et al. “National Health Spending Projections: The Estimated Impact Of Reform Through 2019,” Health Affairs , September 9, 2010.
http://content.healthaffairs.org/cgi/content/abstract/hlthaff.2010.0788v1
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 14/27
- 13
Washington Mandates
Send State Costs Skyrocketing
Today, many states are experiencing budget shortfalls, and some are in precarious financial situations.
The state of California faces a $19 billion deficit.74 Wisconsin faces an upcoming $2.7 billion budget gap.75
Washington state faces a $3.3 budget shortfall for the coming two fiscal years.76 In Georgia, according to
local media coverage, ―without changes in taxes or spending policies, annual deficits of $1.5 billion to $2.1
billion‖ are expected for the near future.77
Unfortunately, the outlook is not expected to improve much in the near future. According to the U.S.
Census Bureau data, state and local government tax receipts rose only slightly in the last quarter. 78 As
the Wall Street Journal concluded, ―the slow revival of tax revenue suggests budgets and spending will
remain tight through this year and beyond.‖79
During these challenging economic times, when states are still grappling with difficult budget situations,
a provision in the health care law increases costs to states by billions of dollars. The expansion of the
costly Medicaid program, as well as a host of other mandates, shifts billions of dollars onto state
taxpayers, leaving state legislatures and governors stuck holding the tab.
Even After “Cornhusker Kickback” Debate, State Costs Still Increase
Of the sweetheart deals that greased the process
for the health care overhaul to slide through
Congress, perhaps none is as famous as the
Section 10201 in the Senate-passed Patient
Protection and Affordable Care Act. Described as
the ―Cornhusker Kickback,‖ this Section granted
the State of Nebraska special treatment. Under
Section 10201, federal taxpayers would absorb
the full $100 million cost for the Medicaid
expansion in Nebraska.80 But in every other
state, state taxpayers would bear significant costs
for the expansion of Medicaid in their own state.
Indeed, a number of Governors expressed concern
publicly about ―unfunded mandates‖ on states in the form of a Medicaid expansion. Because the health
program for low-income Americans is funded by both the federal and state governments, expanding the
program would dramatically increase costs for states. Governor Phil Bredesen of Tennessee said he
74 Lin, Judy. “Calif. budget impasse about to become longest ever,” Associated Press, September 15, 2010.
http://www.google.com/hostednews/ap/article/ALeqM5jJ7uUDlO1sEo7K7bEfHpj4G7wuLQD9I8JU3G0 75
Spicuzza, Mary. “State Deficit Looms Over Candidates’ Vows To Spur Growth,” Wisconsin State Journal, September 21, 2010.
http://host.madison.com/wsj/news/local/govt-and-politics/elections/article_1330169e-c403-11df-b61f-001cc4c002e0.html 76
Garber, Andrew. “State Budget Likely To Go From Bad to Much Worse,” Seattle Times, Olympia bureau, September 11, 2010.
http://seattletimes.nwsource.com/html/localnews/2012873178_budget12m.html 77
Salzer, James. “State Deficit Challenges Candidates’ School Plans,” The Atlanta Journal-Constitution, August, 1, 2010. http://www.ajc.com/news/georgia-politics-
elections/state-deficit-challenges-candidates-582864.html 78
U.S. Census Bureau, “Quarterly Summary of State and Local Government Tax Revenue,” September 27, 2010.
http://www2.census.gov/govs/qtax/information_sheet.pdf 79
Dougherty, Conor. “State and Local Tax Revenue Inches Up,” The Wall Street Journal, September 29, 2010.
http://online.wsj.com/article/SB10001424052748703694204575518210026268450.html 80
H.R. 3590, “The Patient Protection and Affordable Care Act,” as passed by the Senate on December 24, 2009, pg. 801.
http://democrats.senate.gov/reform/patient-protection-affordable-care-act-as-passed.pdf .

8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 15/27
- 14
worried Congress was close to passing ―the mother of all unfunded mandates.‖81 Governor Christine
Gregoire of Washington said her concern was that if there was a ―cost-shift to the states, we‘re not going
to be in a position to pick up the tab.‖82 Governor Brian Schweitzer of Montana was perhaps the clearest
when he said: ―governors are concerned about unfunded mandates, another situation where the federal
government says you must do x and you must pay for it.‖83 Nebraska Governor Dave Heineman warned
the federal health law put the ―future of education spending‖ in jeopardy in a letter to state education
groups.84 And recently, Nevada gubernatorial contender Rory Reid warned that ―there is potential for [the
new health law] to put significant pressure on states because Medicaid rates could go up significan tly.‖85
Perhaps in an attempt to reduce a swell of concern from state
governors and or to squelch criticism about the lack of
transparency in the process, President Obama publicly called for
the elimination of the Cornhusker Kickback and that provision
was removed.86 Now, under the law, the federal government will
pay about 90 percent of the costs for the newly eligible Medicaid
population, at a cost of $20 billion to federal taxpayers.87 This
change removes some costs from states, but it does not eliminate
all the additional costs states must absorb because of the law.
State Taxpayers Face Huge Costs From Mandates
Earlier this spring before the passage of the health overhaul, the Congressional Budget Office (CBO)
estimated that ―state spending on Medicaid‖ would increase by tens of billions of dollars ―as a result of the
coverage provisions.‖88 In pegging the costs to states, they noted that ―under current law, states have the
flexibility to make programmatic and other budgetary changes to Medicaid and the Children‘s Health
Insurance Program.‖89 But now that the health overhaul has been signed into law, states are stuck with
federal mandates buried in the law that dictate many of the operations of the state-level Medicaid
programs.
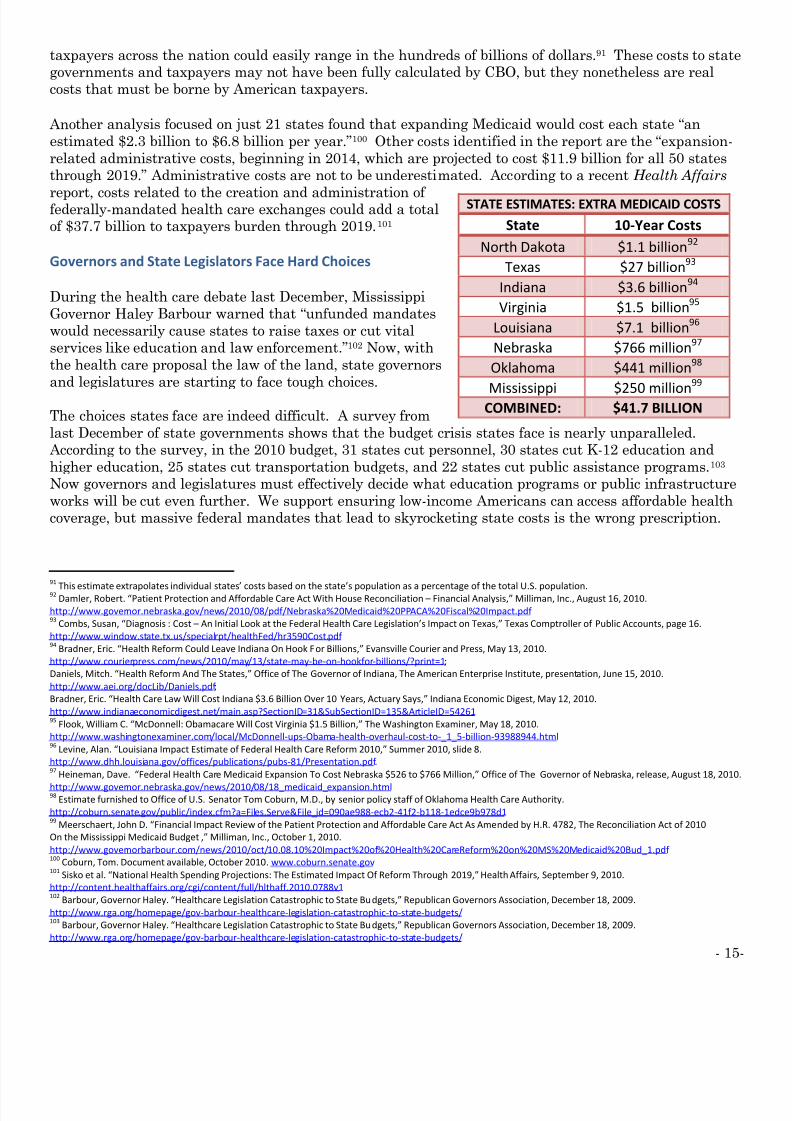
So how big are the costs state taxpayers must absorb from the massive Medicaid expansion or other
mandates? A nearby chart lists estimates that several governors produced calculating the costs to their
states – primarily from the Medicaid program. While the federal government may cover $30 billion of costs, the State of Texas alone estimates their state will face $27 billion in extra costs. 90 Looking at these
estimates, it is clear that the extra costs forced upon state taxpayers and state governments could climb
into the hundreds of billions of dollars. While base data and calculations may vary, the total costs to state
81 Sack, Kevin, and Pear, Robert. “Governors Fear Medicaid Costs in Health Plan,” The New York Times, July 19, 2009.
http://www.nytimes.com/2009/07/20/health/policy/20health.html?hp 82
Sack, Kevin, and Pear, Robert. “Governors Fear Medicaid Costs in Health Plan,” The New York Times, July 19, 2009.
http://www.nytimes.com/2009/07/20/health/policy/20health.html?hp 83
Gomez, Serafin. “Many Governors Against Health Care Bill, Label It Unfunded Mandate,” FOX News, July 19, 2009.
http://www.foxnews.com/politics/2009/07/19/governors-health-care-label-unfunded-mandate/ 84
Hicks, Nancy. “Dave Heineman Urges Nebraska Education Groups to Fight Health Reform,” Lincoln Journal Star, August 27, 2010.
http://journalstar.com/news/local/education/article_55cb11d6-b218-11df-ad9d-001cc4c03286.html 85
Starkey, Melanie. “Rory Reid Warns That Health Care Law Poses Risk to Nevada,” Roll Call, October 8, 2010. http://www.rollcall.com/news/50596-1.html
86 President Barack H. Obama, “The President’s Proposal,” The White House, February 22, 2010, page 1.http://www.whitehouse.gov/sites/default/files/summary-presidents-proposal.pdf 87
Congressional Budget Office, “Letter to Honorable Nancy Pelosi, Speaker of the U.S. House of Representatives,” March 20, 2010.
http://www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp.pdf , Look at Table 4. Estimated Effects of the Insurance Coverage Provisions of the Reconciliation
Proposal Combined with H.R. 3590 as Passed by the Senate. See footnote C: ...CBO estimates that state spending on Medicaid and CHIP in the 2010-2019 period
would increase by about $20 billion as a result of the coverage provisions." 88
Congressional Budget Office, “Letter to the Honorable Harry Reid, U.S. Senate Majority Leader,” March 11, 2010.
http://www.cbo.gov/ftpdocs/113xx/doc11307/Reid_Letter_HR3590.pdf . CBO budget89
Congressional Budget Office, “Letter to the Honorable Harry Reid, U.S. Senate Majority Leader,” March 11, 2010.
http://www.cbo.gov/ftpdocs/113xx/doc11307/Reid_Letter_HR3590.pdf 90
Suehs, Thomas. Executive Commissioner of the Texas Health and Human Services Commission, presentation to Texas House Select Committee on Federal
Legislation on the impact of federal health care reform on Texas Health and Human Services, April 22, 2010.
http://www.hhsc.state.tx.us/news/presentations/2010/HouseSelectFedHlthReform.pdf
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 16/27
- 15
taxpayers across the nation could easily range in the hundreds of billions of dollars.91 These costs to state
governments and taxpayers may not have been fully calculated by CBO, but they nonetheless are real
costs that must be borne by American taxpayers.
Another analysis focused on just 21 states found that expanding Medicaid would cost each state ―an
estimated $2.3 billion to $6.8 billion per year.‖100 Other costs identified in the report are the ―expansion-
related administrative costs, beginning in 2014, which are projected to cost $11.9 billion for all 50 states
through 2019.‖ Administrative costs are not to be underestimated. According to a recent Health Affairs
report, costs related to the creation and administration of federally-mandated health care exchanges could add a total
of $37.7 billion to taxpayers burden through 2019.101
Governors and State Legislators Face Hard Choices
During the health care debate last December, Mississippi
Governor Haley Barbour warned that ―unfunded mandates
would necessarily cause states to raise taxes or cut vital
services like education and law enforcement.‖102 Now, with
the health care proposal the law of the land, state governors
and legislatures are starting to face tough choices.
The choices states face are indeed difficult. A survey from
last December of state governments shows that the budget crisis states face is nearly unparalleled.
According to the survey, in the 2010 budget, 31 states cut personnel, 30 states cut K-12 education and
higher education, 25 states cut transportation budgets, and 22 states cut public assistance programs.103
Now governors and legislatures must effectively decide what education programs or public infrastructure
works will be cut even further. We support ensuring low-income Americans can access affordable health
coverage, but massive federal mandates that lead to skyrocketing state costs is the wrong prescription.
91
This estimate extrapolates individual states’ costs based on the state’s population as a percentage of the total U.S. population.92 Damler, Robert. “Patient Protection and Affordable Care Act With House Reconciliation – Financial Analysis,” Milliman, Inc., August 16, 2010.
http://www.governor.nebraska.gov/news/2010/08/pdf/Nebraska%20Medicaid%20PPACA%20Fiscal%20Impact.pdf 93
Combs, Susan, “Diagnosis : Cost – An Initial Look at the Federal Health Care Legislation’s Impact on Texas,” Texas Comptroller of Public Accounts, page 16.
http://www.window.state.tx.us/specialrpt/healthFed/hr3590Cost.pdf 94
Bradner, Eric. “Health Reform Could Leave Indiana On Hook For Billions,” Evansville Courier and Press, May 13, 2010.
http://www.courierpress.com/news/2010/may/13/state-may-be-on-hookfor-billions/?print=1;
Daniels, Mitch. “Health Reform And The States,” Office of The Governor of Indiana, The American Enterprise Institute, presentation, June 15, 2010.
http://www.aei.org/docLib/Daniels.pdf ;
Bradner, Eric. “Health Care Law Will Cost Indiana $3.6 Billion Over 10 Years, Actuary Says,” Indiana Economic Digest, May 12, 2010.
http://www.indianaeconomicdigest.net/main.asp?SectionID=31&SubSectionID=135&ArticleID=54261 95
Flook, William C. “McDonnell: Obamacare Will Cost Virginia $1.5 Billion,” The Washington Examiner, May 18, 2010.
http://www.washingtonexaminer.com/local/McDonnell-ups-Obama-health-overhaul-cost-to-_1_5-billion-93988944.html 96
Levine, Alan. “Louisiana Impact Estimate of Federal Health Care Reform 2010,” Summer 2010, slide 8.
http://www.dhh.louisiana.gov/offices/publications/pubs-81/Presentation.pdf . 97
Heineman, Dave. “Federal Health Care Medicaid Expansion To Cost Nebraska $526 to $766 Million,” Office of The Governor of Nebraska, release, August 18, 2010.
http://www.governor.nebraska.gov/news/2010/08/18_medicaid_expansion.html 98
Estimate furnished to Office of U.S. Senator Tom Coburn, M.D., by senior policy staff of Oklahoma Health Care Authority.
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=090ae988-ecb2-41f2-b118-1edce9b978d1 99
Meerschaert, John D. “Financial Impact Review of the Patient Protection and Affordable Care Act As Amended by H.R. 4782, The Reconciliation Act of 2010
On the Mississippi Medicaid Budget ,” Milliman, Inc., October 1, 2010.
http://www.governorbarbour.com/news/2010/oct/10.08.10%20Impact%20of%20Health%20CareReform%20on%20MS%20Medicaid%20Bud_1.pdf 100
Coburn, Tom. Document available, October 2010. www.coburn.senate.gov 101
Sisko et al. “National Health Spending Projections: The Estimated Impact Of Reform Through 2019,” Health Affairs , September 9, 2010.
http://content.healthaffairs.org/cgi/content/full/hlthaff.2010.0788v1 102
Barbour, Governor Haley. “Healthcare Legislation Catastrophic to State Budgets,” Republican Governors Association, December 18, 2009.
http://www.rga.org/homepage/gov-barbour-healthcare-legislation-catastrophic-to-state-budgets/ 103
Barbour, Governor Haley. “Healthcare Legislation Catastrophic to State Budgets,” Republican Governors Association, December 18, 2009.
http://www.rga.org/homepage/gov-barbour-healthcare-legislation-catastrophic-to-state-budgets/
STATE ESTIMATES: EXTRA MEDICAID COSTS
State 10-Year Costs
North Dakota $1.1 billion92
Texas $27 billion93
Indiana $3.6 billion94
Virginia $1.5 billion95
Louisiana $7.1 billion96
Nebraska $766 million97
Oklahoma $441 million98
Mississippi $250 million
99
COMBINED: $41.7 BILLION
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=090ae988-ecb2-41f2-b118-1edce9b978d1
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=090ae988-ecb2-41f2-b118-1edce9b978d1
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 17/27
- 16
Increasing ER Wait Times, Costs
One of the cost-savings arguments used by proponents of the health care
law was that expanding health coverage to 30 million previously
uninsured Americans would reduce ―uncompensated care costs‖ due to
things like emergency room visits. Experts generally agree that a
contributing factor to increasing insurance premiums is that uninsured
people do not pay the full cost of their emergency care. Instead, the costsof uncompensated care are shifted to Americans with health coverage,
ultimately resulting in higher premiums for businesses and families.
Supporters of the legislation suggest that Americans without health
insurance only seek health care in a hospital‘s emergency room (ER) or
emergency department, where federal law mandates that everyone
receive basic treatment. They cited figures that estimate an average
American family with private insurance pays an additional $1,017 in
premiums each year to pay the cost of uncompensated care.104
President Obama repeated this line of reasoning, saying ―the insurance reforms rest on everybody having
access to coverage … taxpayers currently end up subsidizing the uninsured when they're forced to go to
the emergency room for care, to the tune of about a thousand bucks per family. You can't get those
savings if those people are still going to the emergency room.‖105
The problem is that under the new overhaul, ER wait times and costs are will not be eliminated. In fact,
overall costs, as well as ER costs and wait times, are on track to increase even further.
National spending on health care will increase because as more Americans gain health care coverage,
they will use more health care services. The Actuary of the Centers for Medicare and Medicaid Services
(CMS) found that the national spending will increase by more than $310 billion in the first decade alone,
in part because of ―greater utilization of health care services by individuals becoming newly covered (or
having more complete coverage.‖106
But uncompensated care costs certainly will not be eliminated. The Congressional Budget Office (CBO)
estimated that at the end of a ten-year period, there will still be at least 23 million individuals without
health insurance.107 So, uncompensated care costs will not be eradicated, as individuals will seek care in
hospital ERs across the country.108
The new law dramatically expands the Medicaid program, a federal-state insurance program offering
coverage to low-income Americans. Under the law, more than 16 million Americans will be enrolled in
Medicaid.109 In part because Medicaid patients are denied access to roughly half of physicians, patients
on Medicaid use hospital ERs more frequency than uninsured patients. According to the Centers for
Disease Control and Prevention‘s most recent report on nationwide ER use, Medicaid patients accounted
104 Families USA, “Hidden Health Tax: Americans Pay a Premium,” 2009. http://www.familiesusa.org/assets/pdfs/hidden-health-tax.pdf
105 105
President Barack H. Obama, “Remarks by the President on Health Care Reform,” The White House, March 3, 2010.
http://www.whitehouse.gov/the-press-office/remarks-president-health-care-reform 106
Foster, Richard. “Estimated Financial Effects of the ‘Patient Protection and Affordable Care Act of 2009,’ as Amended.” Office of the Actuary, Centers for Medicare
and Medicaid Services, April 22, 2010107
http://www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp.pdf , page 21 of PDF.108
Additionally, as we noted in our previous report, Americans may still be paying hundreds of dollars in hidden costs to subsidize the health care costs of illegal
immigrants. Coburn, Tom and Barrasso, John. Bad Medicine: A Check-Up on the New Federal Health Law, July 2010, page 27.
http://coburn.senate.gov/public//index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592, 109
Congressional Budget Office, “Letter to Honorable Nancy Pelosi, Speaker of the U.S. House of Representatives,” March 20, 2010 .
http://www.cbo.gov/ftpdocs/113xx/doc11379/AmendReconProp.pdf , page 21 of PDF.
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 18/27
- 17
for 25 percent of all ER visits during the year.110 With 16 million additional Americans in Medicaid,
Americans could be paying hundreds of dollars more each year for the new Medicaid patients who will use
the ER frequently.
Another analysis of Medicaid and ER use has found that
costs and wait times will increase because of the
overhaul. Former CBO director, Doug Holtz-Eakin,
recently concluded the federal overhaul is ―likely to
dramatically expand the use of emergency room care‖ byMedicaid patients and increase the overhaul costs in our
nation‘s health care system.111 Under the new law,
Medicaid patients will ―generate 68 million visits [to
ERs] and add $36 billion to the nation‘s health care bill,‖
the analysis concluded. 112
Health care practitioners reach a similar conclusion.
According to a recent national survey of emergency physicians, seven in 10 of responding physicians
expect ER visits to increase under the new law.113 The same percentage of physicians say their ER is
already overcrowded at least half the week, so it is unsurprising that half of responding physicians also
anticipate conditions under the new law will worsen for ER patients. 114
Massachusetts: A Cautionary Tale
Despite Massachusetts having passed health care reform legislation in 2006, thousands of state-
subsidized patients with the lowest incomes still used ERs at a rate a third higher than the state
average.115 This is an expensive pattern which drives up health care costs for privately insured citizens in
Massachusetts. The average charge for treating a non-emergency illness in the ER is $976, while it costs
between $84 and $164 to treat a typical ailment in a primary care doctor's office.116 Emergency physicians
identified a lack of primary care physicians as one major reason patients still flooded the ERs for routine
care. Years after ―reform,‖ newly insured patients in Massachusetts were still waiting months for their
first visits.117 An examination of the data leads one to conclude that under the federal health care
overhaul, all Americans might be waiting longer and paying more for care in the ER.
110 Garcia, Tamyra; Bernstein, Amy; and Bush, Mary Ann. “Emergency Department Visitors and Visits: Who Used the Emergency Room in 2007?” National Center for
Health Statistics, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services, May 2010.
http://www.cdc.gov/nchs/data/databriefs/db38.pdf 111
Holtz-Eakin, Doug, and Ramlet, Michael. “Health Care Reform and Medicaid: Patient Access, Emergency Department Use, and Financial Implications for States and
Hospitals,” American Action Forum, September 2010. http://americanactionforum.org/files/HCR_Medicaid.pdf 112
Holtz-Eakin, Doug, and Ramlet, Michael. “Health Care Reform and Medicaid: Patient Access, Emergency Department Use, and Financial Implications for States and
Hospitals,” American Action Forum, September 2010. http://americanactionforum.org/files/HCR_Medicaid.pdf 113
American College of Emergency Physicians, “More Than Two-Thirds of Emergency Physicians Expect ER Visits to Increase Despite National Health Care Reform,”
press release, May 17, 2010. http://www.acep.org/pressroom.aspx?id=48442 114
American College of Emergency Physicians, “More Than Two-Thirds of Emergency Physicians Expect ER Visits to Increase Despite National Health Care Reform,”
press release, May 17, 2010. http://www.acep.org/pressroom.aspx?id=48442 115
Lazar, Kay. “Costly ER Still Draws Many Now Insured,” The Boston Globe, October 6, 2008.
http://www.boston.com/news/health/articles/2008/10/06/costly_er_still_draws_many_now_insured/ 116
Lazar, Kay. “Costly ER Still Draws Many Now Insured,” The Boston Globe, October 6, 2008.
http://www.boston.com/news/health/articles/2008/10/06/costly_er_still_draws_many_now_insured/ 117
Lazar, Kay. “Costly ER Still Draws Many Now Insured,” The Boston Globe, October 6, 2008.
http://www.boston.com/news/health/articles/2008/10/06/costly_er_still_draws_many_now_insured/
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 19/27
- 18
Risky Insurance “Scheme” To Cost Taxpayers
What Is The CLASS Program And How Does It Work?
Section 8002 created the Community Living Assistance Services and
Supports program (CLASS), a ―voluntary federal program for long-term
care insurance that would be administered by the Secretary of Health
and Human Services (HHS).‖ 118 Unlike traditional health insurance thatcovers medical benefits, long-term insurance generally covers services
that assist individuals in their day-to-day activities of life, such as
bathing, eating, or dressing. Under the program, CBO said ―premiums
would vary only according to the enrollee‘s age when he or she enters the
program. Once enrolled, an individual‘s premium would generally remain
the same for as long as that individual remained in the program.‖ 119 To
receive benefits from the program, the participating individual must have
paid into the program for five years and met certain requirements.
While the purpose sounds good, the CLASS program is misguided policy.
The financial structure of the program is so shaky it could require ataxpayer-funded bailout while saddling taxpayers with mountains of debt.
Unfortunately, CLASS is being used as a budget trick to raise the amount
of money the health care overhaul will have to spend. As the Washington Post said bluntly, the CLASS
provision was simply a budget ―gimmick‖ that was ―designed to pretend that health reform is fully paid
for.‖120
The Post explained: ―premiums would flow into the system beginning in 2011, but benefits would not
begin to be paid out until five years later; consequently, over the 10-year budget window through which
the Congressional Budget Office assesses legislation, the program would bring in $58 billion, according to
CBO estimates.‖121 However, as the Post pointed out, ―the money that flows in during the 10-year budget
window will flow back out again. These are not ‗savings‘ that can be honestly counted on the balance
sheet of reform.‖122
CLASS Program Criticized By Budget Experts
According to the Congressional Budget Office (CBO), this provision could ―add to budget deficits …. in
succeeding decades – by amounts on the order of tens of billions of dollars for each 10-year period.‖123
The problems with the structure of the program are so systemic that the American Academy of Actuaries
118 Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009.http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf 119
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009.http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf 120
The Washington Post, “How Not Fix Health Care,” Editorial, July 10, 2009.
http://www.washingtonpost.com/wp-dyn/content/article/2009/07/09/AR2009070902607_pf.html 121
The Washington Post, “How Not Fix Health Care,” Editorial, July 10, 2009.
http://www.washingtonpost.com/wp-dyn/content/article/2009/07/09/AR2009070902607_pf.html 122
The Washington Post, “How Not Fix Health Care,” Editorial, July 10, 2009.
http://www.washingtonpost.com/wp-dyn/content/article/2009/07/09/AR2009070902607_pf.html 123
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 20/27
- 19
concluded ―an actuarially sound program may not be possible to achieve‖ despite changes that might be
sought.124
In fact, the financial structure for this new provision is so untenable that one Senator who voted for the
health care overhaul called it ―a Ponzi scheme of the first order, the kind of thing that Bernie Madoff
would have been proud of.‖125 The CLASS program could effectively self-destruct for several reasons.
First, Section 8002 created a trust fund. Most insurance trust
funds normally are used to stash premiums and grow them into
large reserves that pay benefits and cover program liabilities.However, as others have pointed out, premiums paid into the
CLASS trust fund are not required to be stashed away to build
reserves for paying out future benefits. Instead, HHS will
immediately send the incoming dollars back out the door to pay
for benefits, starting as soon as 2016.
Supporters of the program will point out that under the law, the
Secretary of HHS is required to set premiums at a level to ensure
the program‘s long term sustainability. Supporters of the
program might point to CBO‘s finding that HHS ―would invest
CLASS program premium receipts in federal securities and would
incorporate that expected income into calculations of appropriatepremiums to charge.‖ 126
But such optimism would be misplaced. As CBO pointed out, ―trust fund income from investments in
federal securities would be an intragovernmental transfer within the federal budget. As a result, from a
budget scorekeeping perspective, the CLASS program would inevitably add to future deficits…. by more
than it reduces deficits in the near term, even though the premiums would be set to ensure solvency of the
program.‖127
A second problem with the program is that CBO determined that the ―CLASS program could be subject to
considerable financial risk in the future if it were unable to attract a sufficiently healthy group of
enrollees.‖128
Unfortunately, CBO also found this is a likely outcome, saying ―attracting healthy enrolleescould be challenging for several reasons.‖129 Because the law requires the CLASS program to enroll all
eligible individuals who apply, CBO said it is ―likely that some enrollees would be people who were unable
to obtain coverage in the private market because of their poor health status.‖ 130 So, with a higher
percentage of the CLASS program participants consisting of individuals who are sicker and more needy –
and therefore cost more to care for – CBO concluded the ―relatively small enrollment would increase the
risk of adverse selection and could undermine the long-run stability of the program.‖ 131
124 American Academy of Actuaries, “Community Living Assistance Services and Supports Act,” Critical Issues in Health Reform, November 2009.
http://www.actuary.org/pdf/health/class_nov09.pdf 125
Lori Montgomery, “Proposed Long-Term Health Insurance Program Raises Questions,” The Washington Post, October 27, 2009.
http://www.washingtonpost.com/wp-dyn/content/article/2009/10/27/AR2009102701417.html. 126
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf 127
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf 128
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf 129
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf 130
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” Novembe
25, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf 131
Congressional Budget Office, “Letter to The Honorable Tom Harkin, Chairman of the U.S. Senate Committee on Health, Education, Labor, and Pensions,” November
25, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10823/CLASS_Additional_Information_Harkin_Letter.pdf
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 21/27
- 20
The Chief Actuary of the Centers for Medicare and Medicaid Services issued a similar warning earlier
this year about the long-term financial threat the CLASS program poses. The Actuary expects that ―in
2025 and later, projected benefits exceed premium revenues, resulting in a net federal cost in the long
term.‖132 But the problems with the CLASS program cannot be rectified by mere administrative tweaks.
―In general,‖ the Actuary concluded, ―voluntary, unsubsidized, and non-underwritten insurance programs
such as CLASS face a significant risk of failure as a result of adverse selection by participants.‘‘133 Because of the downward spiral created by adverse selection, HHS could be forced to severely increase
premiums for enrollees to unaffordable levels — which could effectively end participation in the program —
or taxpayers could be asked to fund another bailout a government-backed enterprise.
Supporters of Health Care Bill Criticize CLASS
Even Members of Congress who voted for the health care
legislation have come forward with a variety of concerns with
the provision. One Senator said the CLASS provision ―will be
financially upside down in a very short period of time, [and]
needs to be out of the bill.‖134
As Politico reported, this same Senator joined six other
Senators — all who also supported the health overhaul — in
sending a letter to the Majority Leader ―asking him not toinclude the class act‖ in the overhaul, because ―they are concerned the provision would increase long-term
deficits.‖135 In the letter, the Senators said they had ―grave concerns that the real effect of the provisions
would be to create a new federal entitlement with large, long-term spending increases that far exceed
revenues.‖136 And late last year, twelve Senate Democrats – most of whom supported the health care
overhaul – even voted to remove the CLASS provision from the new law.137 However, despite their public
comments, the provision remained in the health care bill – and is now the law of the land.
Despite its design being soundly criticized by nonpartisan budget experts and even politicians who
supported the health care overhaul, CLASS is now the law of the land. Unfortunately, the Chairman of
the Budget Committee was right: the CLASS provision is indeed ―a Ponzi scheme of the first order.‖ 138
Supporters of the overhaul should be embarrassed that the new law uses a budget gimmick to appear tooffset new spending, while it will likely expose taxpayers to tens of billions of dollars of loss when the
program eventually collapses.
132 Foster, Richard. “Estimated Financial Affects of the ‘America’s Affordable Health Choices Act of 2009’ (HR 3962) as Passed By the House on November 7, 2009.”Office of the Actuary, Centers for Medicare and Medicaid Services, November 13, 2009.
http://republicans.waysandmeans.house.gov/UploadedFiles/OACT_Memorandum_on_Financial_Impact_of_H_R__3962__11-13-09_.pdf#page=11 133
Foster, Richard. “Estimated Financial Effects of the ‘Patient Protection and Affordable Care Act of 2009,’ as Amended.” Office of the Actuary, Centers for Medicare
and Medicaid Services, April 22, 2010. http://s3.amazonaws.com/thf_media/2010/pdf/OACT-Memo-FinImpactofPPACA-Enacted.pdf 134
Sen. Ben Nelson, Fox News’ “On The Record,” December 1, 2009. 135
Budoff Brown, Carrie. “Mods Say No to CLASS Act,” Politico Pulse, October 28, 2009. http://www.politico.com/livepulse/1009/Mods_say_no_to_CLASS_act_.html 136
Stephanie Condon, “Moderate Senators Oppose Long Term Health Care Proposal,” CBS News, October 28, 2009, at http://www.cbsnews.com/8301-503544_162-
5439102-503544.html (July 21, 2010).137
U.S. Senate. S. Amdt. 2901 to S. Amdt. 2786 to H.R. 3590, with the purpose “to eliminate new entitlement programs and limit the government control over the
health care of American families.” http://www.senate.gov/legislative/LIS/roll_call_lists/roll_call_vote_cfm.cfm?congress=111&session=1&vote=00360 138
Lori Montgomery, “Proposed Long-Term Health Insurance Program Raises Questions,” The Washington Post, October 27, 2009.
http://www.washingtonpost.com/wp-dyn/content/article/2009/10/27/AR2009102701417.html.
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 22/27
- 21
Medicare Outlook Growing Worse
Medicare began running a cash flow deficit in 2008. To date, Medicare‘s total long-term unfunded
liabilities total in the tens of trillions of dollars – a gap so big that politicians have no idea of how to
resolve it. The federal health overhaul made the prognosis worse by taking nearly $530 million from
Medicare to spend on new government programs.
In a December 2009 letter to Senator Sessions, the Congressional Budget Office (CBO) said that theappearance of savings to the Medicare program was because the Medicare trust fund is ―essentially an
accounting mechanism.‖139 Cuts to Medicare are effectively double-counted, giving the appearance of extending Medicare‘s solvency while actually being used to pay for the cost of the new law.
CBO has not only challenged claims of Medicare
savings – it has undermined them.140 The conclusion
from the Director of CBO is that the cuts to Medicare
cannot ―pay for future Medicare spending [and
therefore increase its solvency] and, at the same time,
pay for current spending on other parts of the
legislation…‖141
The Chief Actuary of the Centers for Medicare and
Medicaid Services (CMS), Richard Foster, echoed
CBO, stating plainly that the reduced spending
resulting from the significant Medicare cuts in the new
health care law, "cannot be simultaneously used to
finance other Federal outlays (such as coverage expansions) and to extend the trust fund.‖ In a more
recent analysis, the Actuary reiterated that the Medicare ―fund is still not adequately financed over thenext 10 years.‖142
In his most recent report on the financial health of Medicare, the CMS Chief Actuary outlined alternate
financial scenarios for Medicare, drawing attention to the negative impact to the program under thefederal health overhaul. The Actuary concluded that projected savings are not likely to materialize. He
judged there is a strong ―likelihood that certain of these changes will not be viable in the long range‖
because ―the financial projections shown in [the official] report f or Medicare do not represent a reasonable
expectation for actual program operations in either the short range … or the long range.‖143
In fact, if the Medicare reimbursement cuts in the law were allowed to be fully implemented, providers
would either drop out of Medicare and jeopardize access for seniors, or Congress would intervene – thus
increasing spending. ―Medicare prices would be considerably below the current relative level of Medicaid
prices, which have already led to access problems for Medicaid enrollees, and far below the levels paid by
private health insurance,‖ according to the actuary.144 Medicaid patients have many restrictions on
139 Congressional Budget Office, “Effects of the Patient Protection and Affordable Care Act on the Federal Budget and the Balance in the Hospital Insurance Trust
Fund,” December 23, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10868/12-23-Trust_Fund_Accounting.pdf 140
Congressional Budget Office, “Effects of the Patient Protection and Affordable Care Act on the Federal Budget and the Balance in the Hospital Insurance Trust
Fund,” December 23, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10868/12-23-Trust_Fund_Accounting.pdf 141
Congressional Budget Office, “Effects of the Patient Protection and Affordable Care Act on the Federal Budget and the Balance in the Hospital Insurance Trust
Fund,” December 23, 2009. http://www.cbo.gov/ftpdocs/108xx/doc10868/12-23-Trust_Fund_Accounting.pdf 142
Shatto, John and Clemens, Kent. “Projected Medicare Expenditures under an Illustrative Scenario with Alternative Payment Updates to Medicare Providers,”
Office of the Actuary, Centers for Medicare and Medicaid Services, August 5, 2010. http://www.cms.gov/ActuarialStudies/Downloads/2010TRAlternativeScenario.pd143
Shatto, John and Clemens, Kent. “Projected Medicare Expenditures under an Illustrative Scenario with Alternative Payment Updates to Medicare Providers,”
Office of the Actuary, Centers for Medicare and Medicaid Services, August 5, 2010. http://www.cms.gov/ActuarialStudies/Downloads/2010TRAlternativeScenario.pd144
Shatto, John and Clemens, Kent. “Projected Medicare Expenditures under an Illustrative Scenario with Alternative Payment Updates to Medicare Providers,”
Office of the Actuary, Centers for Medicare and Medicaid Services, August 5, 2010. http://www.cms.gov/ActuarialStudies/Downloads/2010TRAlternativeScenario.pd
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 23/27
- 22
accessing care because of very low reimbursements, so it is difficult to assume Congress would allow rates
to be reduced so low. ―Well before that point,‖ the Actuary concluded, ―Congress would have to intervene
to prevent the withdrawal of providers from the Medicare market and the severe problems with
beneficiary access to care that would result.‖145
Both the CBO Director and CMS Actuary agree. Estimated savings from cuts to Medicare are unlikely
and it is not possible to double count savings from Medicare.
Other Medicare experts arrive at the same conclusion. Dr. Tom Saving, a former Medicare trustee from2000- 2007, said that ―while some savings are necessary to shore up the Medicare program, we know that
the new law‘s unrealistic cuts will hurt care for seniors. Instead of reducing the existing program‘s
tremendous burden on taxpayers, the new law commits future taxpayers to a bigger burden through a
bigger trust fund.‖146
Another former Medicare trustee, David Walker, noted a Medicare dollar cannot be simultaneously spent
and saved. If ―the Medicare savings are used to pay for expanded health care coverage, the economic
capacity of the federal government to meet its Medicare obligations will not be enhanced.‖147
Independent Medicare and budget experts conclude that the appearance of Medicare‘s extended solvencyis actually only a mirage. In reality, under the new law, Medicare‘s unfunded liabilities will grow worse.
145Shatto, John and Clemens, Kent. “Projected Medicare Expenditures under an Illustrative Scenario with Alternative Payment Updates to Medicare Providers,”
Office of the Actuary, Centers for Medicare and Medicaid Services, August 5, 2010. http://www.cms.gov/ActuarialStudies/Downloads/2010TRAlternativeScenario.pd146
Cornyn, John. “Cornyn & Former Public Trustees Highlight How The New Health Law Worsens Washington’s Fiscal Crisis ,” Press Release, Office U.S. Senator John
Cornyn, August 5, 2010. http://tiny.cc/i6ie6 147
Cornyn, John. “Cornyn & Former Public Trustees Highlight How The New Health Law Worsens Washington’s Fiscal Crisis ,” Press Release, Office U.S. Senator John
Cornyn, August 5, 2010. http://tiny.cc/i6ie6

8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 24/27
- 23
Higher Costs, Fewer Jobs For Young Americans
Much attention has been focused on how the federal health care overhaul, six months after enactment,
mandates all insurance companies must allow young adults up of to age 26 to remain on their parents‘
health insurance. These blanket mandates will increase health insurance costs for millions of
Americans.148 But the relative benefits or costs of this specific provision should not obscure a larger
totality: the next generation of Americans faces a grim future.
Gloomy Outlook
Government has grown rapidly in recent years, choking
out progress and opportunity with increasing costs,
mandates, and taxes.
A recent survey found that fewer than half of all
Americans were confident that their children will have
better lives than they have.149 Certainly, young
Americans in high school and college face a bleak
economic outlook on the horizon.
Less than half of Americans age 16 to 24 were
employed this summer – the lowest level on record in
more than six decades.150 Youth employment – which
always rises in the summer – was roughly only half as robust as it was the previous years. 151
Our national debt stands at a staggering $13.6 trillion. Young adults already face a current debt burden
of more than $120,000 per taxpayer.152
Employer Penalty Penalizes Young Workers
Unfortunately, the future does not look much brighter. Young Americans‘ financial future as taxpayersand employees is made worse by the health overhaul.
The employer penalty buried in the health overhaul will discourage hiring and reduce wages. Dr. Kate
Baicker, a member of the Congressional Budget Office's (CBO) Panel of Health Advisers, noted in
research that among the uninsured, Americans with the lowest levels of education are at the highest risk
of losing their jobs.153 This means that many young adults coming out of high school and even college
may be in at an increased competitive disadvantage under the law, compared to other Americans.
148 148
Coburn, Tom and Barrasso, John. Bad Medicine: A Check-Up on the New Federal Health Law, July 2010, page 29.
http://coburn.senate.gov/public//index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592.149
Miller, Rich. “Americans See Children's Future Dim in Poll as 50% Pessimistic,” Bloomberg News, October 13, 2010.
http://www.bloomberg.com/news/2010-10-13/americans-see-children-s-future-dim-in-poll-as-50-pessimistic.html. 150
Stafford, Diane. “Bad Statistics for Summer Employment for Youth,” Kansas City Star, August 27, 2010.
http://www.mcclatchydc.com/2010/08/27/99763/bad-statistics-for-summer-employment.html 151
Stafford, Diane. “Bad Statistics for Summer Employment for Youth,” Kansas City Star, August 27, 2010.
http://www.mcclatchydc.com/2010/08/27/99763/bad-statistics-for-summer-employment.html 152
U.S. Debt Clock.org as of September 26, 2010. http://www.usdebtclock.org/#. 153
Katherine Baicker and Amitabh Chandra, “Myths and Misconceptions about U.S. Health Insurance,” Health Affairs, 2008.
http://content.healthaffairs.org/cgi/content/abstract/hlthaff.27.6.w533
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 25/27
- 24
Health Insurance Costs Increase Even Further
Currently, about one in three Americans ages 18 to 24 does not have health insurance, despite that health
insurance is the most affordable for young, healthy Americans.154 In Oklahoma for example, high quality,
affordable health plans are available to young Americans up to age 32 for about the same monthly price
as the cost of cable television and a cell phone plan.155
Under the health overhaul however, premiums for young adults will spike dramatically because of newly-
mandated rating rules. Beginning in 2014, new rules in the law mandate insurance companies may onlycharge an older person three times the premium cost they charge a younger person. This has the effect of
increasing premium costs on young adults. In fact, some independent actuaries estimate that premiums
for the youngest third of the population could increase by as much as 35 percent under the new law‘s tight
age bands.156
And not only will insurance be more expensive, health
care will be more expensive. The Joint Committee on
Taxation has confirmed that the new health taxes
included in the overhaul – on medical devices, health
plans, and prescription drugs – will be passed on
directly to consumers.157
Faced with increased insurance and medical costs,
many young adults are likely to forgo purchasing
health insurance altogether. In 2014 when the
individual mandate is effective, the penalty for not
maintaining health insurance will only be several
hundred dollars per person. Many younger, healthier
Americans will make an economic decision to pay the
penalty, rather than paying more for health insurance
they may be unlikely to need. Unfortunately, because millions of younger, healthier Americans may not
purchase health insurance and spread risk in the insurance risk pool, this will cause premiums to
increase even more rapidly for those with insurance.
Indeed, the reality young adults face under the overhaul is concerning. A massive debt burden. Rising
costs. Fewer jobs and labor disincentives. While the law does mandate that young adults up to age 26 be
allowed to remain on their parents‘ health insurance, the core elements of the legislation paint a grim
future.
154DeNavas-Walt, Carmen; Proctor, Bernadette; and Smith, Jessica. “Income, Poverty, and Health Insurance Coverage in the United States: 2009,” September 2010.
http://www.census.gov/prod/2010pubs/p60-238.pdf 155
Holland, Kim. “Letter to Senator Coburn on The Patient Protection and Affordable Care Act,” Office of the Commissioner, Oklahoma Insurance Department,
December 1, 2009. http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=494070c0-a06f-4b26-989e-dddda162d27f 156
Grau, Jason and Giesa, Kurt, “Impact of the Patient Protection and Affordable Care Act on Costs in the Individual and Small-Employer Health Insurance Markets,
December 1, 2009, http://www.oliverwyman.com/ow/pdf_files/YBS009-11-28_PPACA120309.pdf . 157
Joint Committee on Taxation, “Technical Explanation of the Revenue Provisions of the ‘Reconciliation Act of 2010,’ as Amended, In Combination with the ‘Patient
Protection and Affordable Care Act,’” March 21, 2010, http://www.jct.gov/publications.html?func=startdown&id=3673.
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=494070c0-a06f-4b26-989e-dddda162d27f
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=494070c0-a06f-4b26-989e-dddda162d27f
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=494070c0-a06f-4b26-989e-dddda162d27f
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 26/27
- 25
Costs Increasing For Employers
Proponents of the new health law argue the legislation needs time to work . Unfortunately, businesses‘
costs will increase with time because of the law, rather than decrease. The new law increases the cost of
pharmaceutical drugs, medical devices, and health insurance and bends the ―cost curve‖ up.158
Regrettably, businesses and employees will bear the brunt of these costs.
The Wall Street Journal recently reported that a survey of more than 70 large companies found thatbusinesses ―expect their health-care costs to rise nine percent next year.‖159 Nearly two-thirds of
businesses surveyed anticipate they will increase the proportion of premiums paid by employees.160 And
nearly half say they will increase the maximum out-
of-pocket costs for employees in the coming year.161
Another independent analysis has reached similar
conclusions. Hewitt Associates recently released an
analysis projecting a nearly nine percent premium
increase for employer-sponsored health insurance
coverage in 2011 alone.162 Similarly, an Aon
Consulting survey expects an increase of more than
10 percent for employer-sponsored health insurance
for the year ahead.163
Small Business Tax Credits Fail To Improve Outlook
Businesses continue to bear an increasing burden in health care costs. Unfortunately, business leaders
are now learning that new small business tax credits in the law actually do very little and do not prevent
health care costs for businesses from climbing higher.
Sections 1421 and 10105 of the health care bills created a small business tax credit for some employers‘
contributions toward employees‘ health insurance premiums. In April, President Obama said the ―health
care tax credit is pro- jobs, it‘s pro-business.‖ But business owners are now learning that the credits willactually have a negligible impact on the costs to businesses. While the Congressional Budget Office (CBO)
says the credit is available to ―for-profit and nonprofit employers with fewer than 25 full-time equivalent
employees with average annual wages of less than $50,000,‖ according to CBO data only about three
million employees – or one percent of the American population – will benefit from the credit in 2016. 164
Not only are few employees eligible for the credit, few businesses appear interested in the credit. Despite
the Administration‘s eagerness to promote the small business tax credit by mailing postcards about the
158 Johnson, Avery. “Firms Find Changing Their Insurance Is Trickier,” The Wall Street Journal, June 23, 2010.
http://online.wsj.com/article/SB10001424052748703513604575311013340405940.html; Coburn, Tom and Barrasso, John. Bad Medicine: A Check-Up on the New Federal Health Law, July 2010, page 5. http://coburn.senate.gov/public//index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592. 159
Hobson, Katharine. “Big Employers Estimate Health Care Costs Will Rise 8.9% in 2011,” The Wall Street Journal Health Blog, August 19, 2010.
http://blogs.wsj.com/health/2010/08/19/big-employers-estimate-health-care-costs-will-rise-89-in-2011/ 160
Hobson, Katharine. “Big Employers Estimate Health Care Costs Will Rise 8.9% in 2011,” The Wall Street Journal Health Blog, August 19, 2010.
http://blogs.wsj.com/health/2010/08/19/big-employers-estimate-health-care-costs-will-rise-89-in-2011/ 161
Lillis, Mike. “Faced with rising health costs, large employers plan to shift burden to workers,” The Hill, Healthwatch blog, August 18, 2010.
http://thehill.com/blogs/healthwatch/health-reform-implementation/114823-faced-with-rising-health-costs-large-employers-plan-to-shift-burden-to-workers- 162
Hewitt Associates. “U.S. Health Care Cost Rate Increases Reach Highest Levels in Five Years, According to New Data from Hewitt Associates,” September 27, 2010.
http://www.hewittassociates.com/Intl/NA/en-US/AboutHewitt/Newsroom/PressReleaseDetail.aspx?cid=9106 163
Sharon, Bill. “2010 Health Care Trend Survey,” Aon Consulting, Summer 2010. http://www.aon.com/attachments/2010_health_care_trend_survey_summer.pdf 164
Chaikind, Hinda, and Peterson, Chris. “Summary of the Small Business Health Insurance Tax Credit Under the Patient Protection and Affordable Care Act (PPACA),”
September 21, 2010. http://www.ncsl.org/documents/health/SBtaxCredits.pdf (link is to publicly available document dated April 5, 2010)
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
http://coburn.senate.gov/public/index.cfm?a=Files.Serve&File_id=722faf8b-a5be-40fd-a52b-9a98826c1592
8/6/2019 Grim Diagnosis of Obamacare
http://slidepdf.com/reader/full/grim-diagnosis-of-obamacare 27/27
program to four million eligible companies, a recent Business Week article noted that ―the response has
been tepid.‖165
The problem with the credit is the credit itself. Many businesses simply crunch their numbers and find
the credit does not work for them because they have too many employees or their employees earn too
much to be eligible.166 ―The credit starts to phase out for companies that pay average annual wages of
more than $25,000 or employ more than 25 workers,‖ Business Week notes. And, ―the value of the benefit
declines quickly, so many business owners in high-cost states get no tax break, and those elsewhere often
say the credit is too small to make much of a difference.‖167
These problems with the tax credit mean, of the few businesses
that are eligible for the tax credit, few businesses are likely to even
apply. The Washington Post reported that the Commonwealth
Fund found that of the three million employees at firms that would
be eligible to utilize the tax credit, ―for the most part, those are
firms that already offer their employees health insurance.‖168
Commonwealth‘s analysis found that, even with the credit,
businesses not already offering health coverage ―are unlikely to
consider the tax breaks enough of a financial incentive to start
doing so.‖169
But even if the estimated three million employees at eligible firms enjoy temporary relief from
skyrocketing health costs because of the tax credit, this group represents less than two percent of
Americans with commercial health insurance.170 Rather than lowering health costs for all businesses and
workers, the new law only offers a temporary credit from which one percent of individuals in America will
actually benefit.
Even worse than failing to soften the blow of rising costs for businesses, the tax credit itself also
interferes in the labor market, creating perverse incentives for small employers to not expand their
businesses and hire employees. According to recent analysis by one think tank, ―employers with 15
workers, taking on an additional hire will reduce the credit by $1,400.‖171 The reduction in credit is most
severe for companies hiring a twenty-fifth employee, as they would see a $5,600 reduction in the credit atthat point.172
All of this is headed the wrong direction. Congress should be embracing policies which will spur business
expansion and job growth – not policies that will increase health care costs for businesses and employees.
165 Lerman, David, and Smith, Liz. “Small Businesses Skip the Health-Care Tax Credit,” Bloomberg Businessweek, August 26, 2010.
http://www.businessweek.com/print/smallbiz/content/aug2010/sb20100825_366429.htm 166
National Federation of Independent Businesses. “2010 Health Insurance Reform Tax Credit Calculator for Small Business.” Summer 2010.
http://www.nfib.com/issues-elections/healthcare/credit-calculator 167
Lerman, David, and Smith, Liz. “Small Businesses Skip the Health-Care Tax Credit,” Bloomberg Businessweek, August 26, 2010.
http://www.businessweek.com/print/smallbiz/content/aug2010/sb20100825_366429.htm 168
Aizenman, N.C. “Health insurance tax credit likely to affect small part of small-business workforce,” The Washington Post, September 2, 2010.
http://www.washingtonpost.com/wp-dyn/content/article/2010/09/02/AR2010090200044_pf.html 169
Aizenman, N.C. “Health insurance tax credit likely to affect small part of small-business workforce,” The Washington Post, September 2,
2010.http://www.washingtonpost.com/wp-dyn/content/article/2010/09/02/AR2010090200044_pf.html 170
DeNavas-Walt, Carmen; Proctor, Bernadette; and Smith, Jessica. “Income, Poverty, and Health Insurance Coverage in the United States: 2009,” September 2010.
http://www.census.gov/prod/2009pubs/p60-236.pdf 171
Heflin, Jay. “Report: Healthcare law tax credits encourage small businesses to stay small, not hire,” The Hill, Healthwatch blog, May 23, 2010.
http://thehill.com/blogs/on-the-money/domestic-taxes/99387-study-healthcare-law-encourages-small-businesses-to-stay-small?tmpl=component&print=1&page=;
Herrick, Devon and Villarreal, Pamela. “Obama’s Tax on Job Creation,” National Center for Policy Analysis, Brief Analysis No. 703, May 18, 2010.
http://www.ncpa.org/pub/ba703172
Heflin, Jay. “Report: Healthcare law tax credits encourage small businesses to stay small, not hire,” The Hill, Healthwatch blog, May 23, 2010.
http //thehill com/blogs/on the money/domestic taxes/99387 study healthcare law encourages small businesses to stay small?tmpl component&print 1&page














![GRIM commission BEHR]](https://static.fdocuments.in/doc/165x107/623ef96b04c3026a683d0fec/grim-commission-behr.jpg)