
Gravity infusions: troubleshooting “no-flow” situations
3
Gravity infusions rely entirely on gravity to deliver the infused fluid. Following a careful risk assessment that a patient’s condition is low-risk and not cause for concern, gravity infusions can be used to deliver medicines or fluid where a precise flow rate is not required, or crystalloid fluids such as additive-free 0.9% sodium chloride and 5% glucose (Barrott et al., 2020). When administering gravity infusions always use a drip rate formula to calculate the drip rate per minute of delivery (Brooks, 2017). It is important to maintain the flow of a gravity infusion device at the correct rate. If the flow is too fast, the patient could experience “speed shock”—a systemic reaction that occurs when a substance foreign to the body is rapidly introduced into the circulation (Barrott et al., 2020)—or become overloaded with fluid and/or electrolytes (NICE, 2017a). If the flow is too slow, the patient may become dehydrated or be treated with a subtherapeutic dose of the medication. Factors affecting the flow rate of an infusion include (Barrott et al., 2020): • The height of the infusion bag; • The condition and size of the vein; • The site and size of the cannula; • The type of infusion set (e.g., internal diameter and length of tubing); and • The viscosity, composition and concentration of the fluid being infused. You may need to explain to the patient the importance of keeping their arm down below the infusion bag. Check if the bag is too low as this will result in no flow, as the effect of gravity is reduced, with the risk of occlusion. If the flow rate slows down or stops, never try to restart the flow by pinching or kinking the tube, or winding it around a pen or other implement. Doing so will make the pressure in the vein rise and could enlarge the opening in the vein where the cannula enters it, so that fluid leaks from the cannula into the surrounding tissue (RCN, 2016). If this happens, the infusion will at first begin to flow again, because the pressure in the tissues is lower than that in the veins. After a while, the amount of fluid in the tissues will cause an increase in pressure, the limb will swell and the infusion will again stop. Depending on the type of medication being infused, this could result in local tissue damage. Ask the patient to immediately report any pain or burning at the injection site. If the flow stops completely, blood may enter the tip of the cannula and clot, resulting in an occlusion. It may be possible to remove the clot by flushing gently with a 10-mL syringe of 0.9% sodium chloride (Barrott et al., 2020). This procedure outlines troubleshooting strategies to help resolve problems with gravity infusions, such as slow running or obstructed flow. Read in conjunction with the clinicalskills.net procedures, “Care and maintenance of a peripheral intravenous cannula” and “Use of infusion pumps”. CHANGEIFPINK 1 8 7 07K16E2N 10 2024 Lot UN-35-01-357 Expiry 100 200 300 400 500 600 700 80 0 100 200 300 400 500 600 700 80 0 90 0 90 0 10 0 10 0 5 413760277691 P O M use. Donot reconnect partiallyusedbags. Foruseundermedical overwrapuntil readyforuse. Discardanyunusedportionafterfirst asepticmixingof anyadditiveismandatory. Donotremovefrom boththesolutionandthecontainerpriortouse.Thoroughandcareful isclearandcontainerisundamaged.Checkadditivecompatibilitywith Storeout of reachandsight of children. Donot useunlesssolution Forintravenousadministration supervision. pH 5.5(approx) Isotonic Osmolarity308mOsm/l (approx) Sterilenonpyrogenic Singledose Solutionforinfusion Formulafor1000ml mmol per1000ml (approx) SodiumChloride2.25g Sodium 38 Waterforinjections Chloride 38 1000ml IntravenousInfusionBP SodiumChloride0/9% w/v 0/9% w/v SodiumChloride Page 1 of 3 Intravenous Therapy Adults Gravity infusions: troubleshooting “no-flow” situations Edda Hensler, Senior Lecturer in Nursing, School of Health Sciences, University of Brighton ©2021 Clinical Skills Limited. All rights reserved Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person. Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution. As soon as you are aware that there is a problem with the infusion, reassure the patient and check the device. Determine whether the administration set may have been accidentally switched off, or whether the clamp on an extension has been left closed. If this is the case, switch the set back on or open the clamp and adjust the flow rate. Ask the patient if the cannula is causing any pain. Document your actions in the patient's notes and on the Visual Infusion Phlebitis (VIP) score chart. Using a recognised assessment scale, such as the VIP score, will guide the management of the device (Loveday et al., 2014), although the reliability of using a VIP score has been questioned (Ray-Barruel et al., 2014). Intravenous (IV) site appears healthy No signs of phlebitis OBSERVE CANNULA One of the following is evident: Slight pain near the IV site or slight redness near the IV site Possible first sign of phlebitis OBSERVE CANNULA Two of the following are evident: Pain near IV site Erythema Swelling Early stage of phlebitis RESITE CANNULA All of the following are evident: Pain along path of cannula Erythema Induration Medium stage of phlebitis RESITE CANNULA CONSIDER TREATMENT All of the following are evident: Pain along path of cannula Erythema Induration Palpable venous cord All of the following are evident and extensive: Pain along path of cannula Erythema Induration Palpable venous cord Pyrexia Advanced stage of phlebitis or start of thrombophlebitis RESITE CANNULA CONSIDER TREATMENT Advanced stage of phlebitis or start of thrombophlebitis INITIATE TREATMENT RESITE CANNULA Visual Infusion Phlebitis (VIP) score Developed by Andrew Jackson, Consultant Nurse Intravenous Therapy and Care, Rotherham General Hospitals, NHS Trust. 5 4 3 2 1 0 (b) Check the infusion rate Important observations: (a) Observe the cannula site
Transcript of Gravity infusions: troubleshooting “no-flow” situations

Gravity infusions rely entirely on gravity to deliver the infused fluid. Following a careful risk assessment that a patient’s condition is low-risk and not cause for concern, gravity infusions can be used to deliver medicines or fluid where a precise flow rate is not required, or crystalloid fluids such as additive-free 0.9% sodium chloride and 5% glucose (Barrott et al., 2020). When administering gravity infusions always use a drip rate formula to calculate the drip rate per minute of delivery (Brooks, 2017).
It is important to maintain the flow of a gravity infusion device at the correct rate. If the flow is too fast, the patient could experience “speed shock”—a systemic reaction that occurs when a substance foreign to the body is rapidly introduced into the circulation (Barrott et al., 2020)—or become overloaded with fluid and/or electrolytes (NICE, 2017a). If the flow is too slow, the patient may become dehydrated or be treated with a subtherapeutic dose of the medication.
Factors affecting the flow rate of an infusion include (Barrott et al., 2020):• The height of the infusion bag; • The condition and size of the vein;• The site and size of the cannula;• The type of infusion set (e.g., internal diameter and length of tubing); and• The viscosity, composition and concentration of the fluid being infused.
You may need to explain to the patient the importance of keeping their arm down below the infusion bag. Check if the bag is too low as this will result in no flow, as the effect of gravity is reduced, with the risk of occlusion. If the flow rate slows down or stops, never try to restart the flow by pinching or kinking the tube, or winding it around a pen or other implement. Doing so will make the pressure in the vein rise and could enlarge the opening in the vein where the cannula enters it, so that fluid leaks from the cannula into the surrounding tissue (RCN, 2016). If this happens, the infusion will at first begin to flow again, because the pressure in the tissues is lower than that in the veins. After a while, the amount of fluid in the tissues will cause an increase in pressure, the limb will swell and the infusion will again stop. Depending on the type of medication being infused, this could result in local tissue damage. Ask the patient to immediately report any pain or burning at the injection site.
If the flow stops completely, blood may enter the tip of the cannula and clot, resulting in an occlusion. It may be possible to remove the clot by flushing gently with a 10-mL syringe of 0.9% sodium chloride (Barrott et al., 2020).
This procedure outlines troubleshooting strategies to help resolve problems with gravity infusions, such as slow running or obstructed flow. Read in conjunction with the clinicalskills.net procedures, “Care and maintenance of a peripheral intravenous cannula” and “Use of infusion pumps”.
CHANGE IF PINK
THERAPY EQUIPMENPIPELINE PROTECTE
0
20
4060
80
100
HIGH VACUUMHIGH FLOW
AIR
AIR
o2
AIR
o2
15
10
OXYGEN
LITRES
perMINUTE
5
1
18 7
21
2 1
07K16E2N 10 2024
Lot UN-35-01-357 Expiry
100
200
300
400
500
600
700
800
100
200
300
400
500
600
700
800
900900
100100
5 413760 277691
POM 07
use. Do not reconnect partially used bags. For use under medical
overwrap until ready for use. Discard any unused portion after first
aseptic mixing of any additive is mandatory. Do not remove from
both the solution and the container prior to use. Thorough and careful
is clear and container is undamaged. Check additive compatibility with
Store out of reach and sight of children. Do not use unless solution
For intravenous administration
supervision.
pH 5.5 (approx) IsotonicOsmolarity 308 mOsm/l (approx) Sterile non pyrogenicSingle dose Solution for infusion
Formula for 1000ml mmol per 1000 ml (approx)Sodium Chloride 2.25g Sodium 38Water for injections Chloride 38
1000 ml
Intravenous Infusion BP
Sodium Chloride 0/9% w/v
0/9% w/v
Sodium Chloride
Page 1 of 3
Intravenous TherapyAdults
Gravity infusions: troubleshooting “no-flow” situations
Edda Hensler, Senior Lecturer in Nursing, School of Health Sciences, University of Brighton
©2021 Clinical Skills Limited. All rights reserved
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
As soon as you are aware that there is a problem with the infusion, reassure the patient and check the device. Determine whether the administration set may have been accidentally switched off, or whether the clamp on an extension has been left closed. If this is the case, switch the set back on or open the clamp and adjust the flow rate.
Ask the patient if the cannula is causing any pain. Document your actions in the patient's notes and on the Visual Infusion Phlebitis (VIP) score chart. Using a recognised assessment scale, such as the VIP score, will guide the management of the device (Loveday et al., 2014), although the reliability of using a VIP score has been questioned (Ray-Barruel et al., 2014).
Edda’s comments (Feb 2019)IV infusions- problem solving: I suggest to rename to gravity infusions- trouble shooting 'no-�ow' situationsI have proposed to move the ‘removal’ part of this procedure to the ‘care of a peripheral cannula’ procedure as it �ts betterI have made additional comments on the pdfEH: equipment providers provide guides for cannula selection- outlining gravity �ow rate, indication and insertion sites in relation to cannula size eg. Braun- could we reference this here?-can’t �nd anything - ask Edda to provide link/ref
Intravenous (IV) site appears healthy No signs of phlebitisOBSERVE CANNULA
One of the following is evident:Slight pain near the IV siteor slight redness near the IV site
Possible first sign of phlebitisOBSERVE CANNULA
Two of the following are evident:Pain near IV site Erythema Swelling
Early stage of phlebitisRESITE CANNULA
All of the following are evident:Pain along path of cannulaErythema Induration
Medium stage of phlebitisRESITE CANNULA CONSIDER TREATMENT
All of the following are evident:Pain along path of cannula Erythema Induration Palpable venous cord
All of the following are evident and extensive:Pain along path of cannula Erythema Induration Palpable venous cord Pyrexia
Advanced stage of phlebitis or start of thrombophlebitisRESITE CANNULA CONSIDER TREATMENT
Advanced stage of phlebitis or start of thrombophlebitisINITIATE TREATMENT RESITE CANNULA
Visual Infusion Phlebitis (VIP) score
Developed by Andrew Jackson, Consultant Nurse Intravenous Therapy and Care, Rotherham General Hospitals, NHS Trust.
5
4
3
2
1
0
Cannula is too far out of skin
(b) Check the infusion rateImportant observations: (a) Observe the cannula site
18 7 2121
18 7 21
21
DATE O
F BIRTH.........
NAME.....
..........
...........
WARD....
....
..........
........
SeaSalt
GroundPepper
AIR
AIR
CHANGE IF PINK
THERAPY EQUIPMENPIPELINE PROTECTE
o2
1 5
1 0
5
1
OXY
GEN
per M
INU
TELI
TRES
0
20
40 60
80
100
HIGH VACUUMHIGH FLOW
o2
1 5
1 0
OXY
GEN
LITR
ESpe
r MIN
UTE
5
1
o2 o2 AIR
DATE O
F BIRTH.........
NAME....
.....
..........
.......
WARD....
.........
.............
1 m
07K16E2N 10 2024
Lot UN-35-01-357 Expiry
100
200
300
400
500
600
700
800
100
200
300
400
500
600
700
800
900900
100100
5 413760 277691
POM 07
use. Do not reconnect partially used bags. For use under medical
overwrap until ready for use. Discard any unused portion after first
aseptic mixing of any additive is mandatory. Do not remove from
both the solution and the container prior to use. Thorough and careful
is clear and container is undamaged. Check additive compatibility with
Store out of reach and sight of children. Do not use unless solution
For intravenous administration
supervision.
pH 5.5 (approx) IsotonicOsmolarity 308 mOsm/l (approx) Sterile non pyrogenicSingle dose Solution for infusion
Formula for 1000ml mmol per 1000 ml (approx)Sodium Chloride 2.25g Sodium 38Water for injections Chloride 38
1000 ml
Intravenous Infusion BP
Sodium Chloride 0/9% w/v
0/9% w/v
Sodium Chloride
Intravenous Therapy
Adults
Gravity infusions: troubleshooting “no flow” situations Page 2
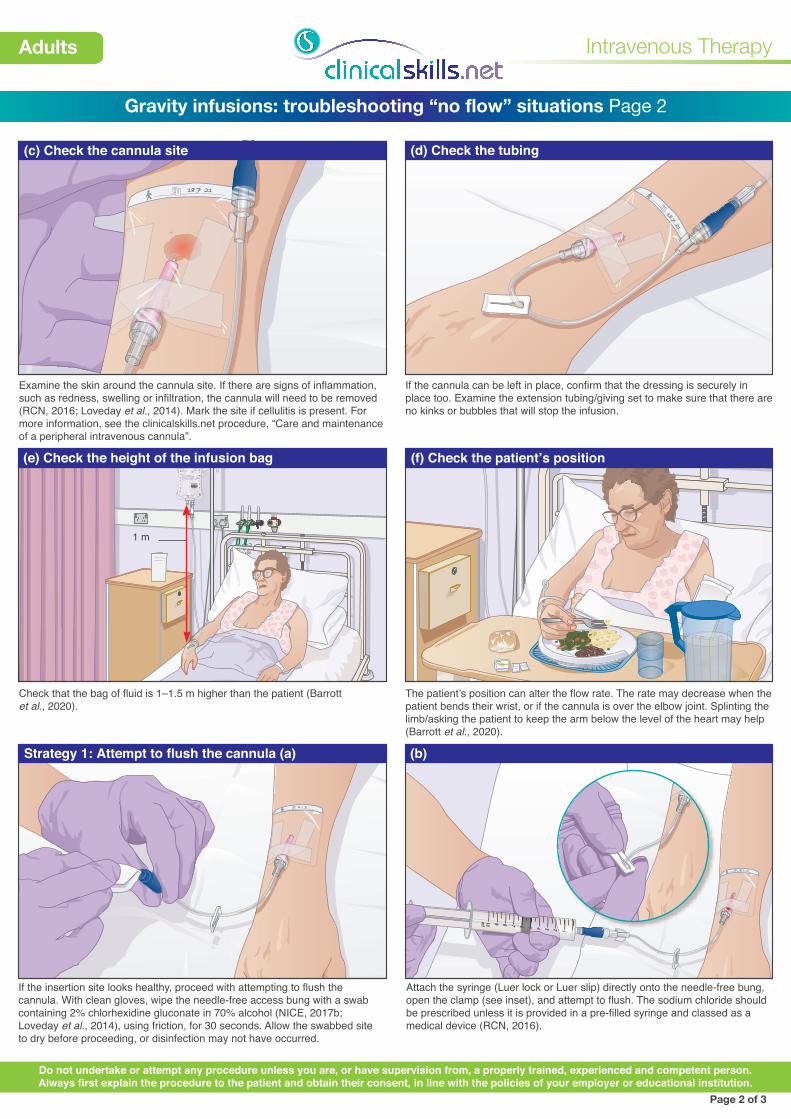
(c) Check the cannula site (d) Check the tubing
(e) Check the height of the infusion bag (f) Check the patient’s position
Examine the skin around the cannula site. If there are signs of inflammation, such as redness, swelling or infiltration, the cannula will need to be removed (RCN, 2016; Loveday et al., 2014). Mark the site if cellulitis is present. For more information, see the clinicalskills.net procedure, “Care and maintenance of a peripheral intravenous cannula”.
If the cannula can be left in place, confirm that the dressing is securely in place too. Examine the extension tubing/giving set to make sure that there are no kinks or bubbles that will stop the infusion.
Check that the bag of fluid is 1–1.5 m higher than the patient (Barrott et al., 2020).
Page 2 of 3
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
The patient’s position can alter the flow rate. The rate may decrease when the patient bends their wrist, or if the cannula is over the elbow joint. Splinting the limb/asking the patient to keep the arm below the level of the heart may help (Barrott et al., 2020).
If the insertion site looks healthy, proceed with attempting to flush the cannula. With clean gloves, wipe the needle-free access bung with a swab containing 2% chlorhexidine gluconate in 70% alcohol (NICE, 2017b; Loveday et al., 2014), using friction, for 30 seconds. Allow the swabbed site to dry before proceeding, or disinfection may not have occurred.
Attach the syringe (Luer lock or Luer slip) directly onto the needle-free bung, open the clamp (see inset), and attempt to flush. The sodium chloride should be prescribed unless it is provided in a pre-filled syringe and classed as a medical device (RCN, 2016).
18 7 2121
18 7 2121
12345
ml 678910
(b)Strategy 1: Attempt to flush the cannula (a)

18 7 21
21
Patient Notes ? X
OK Cancel
General Notes
18.7.21 09:30
The cannula was flushed twice due to intermittent problems with the flow. The flow problem may have been caused by the position of the cannula. The VIP score remains at 0. The patient does not report any pain.
Allergy Notes
Intravenous Therapy
Adults
Gravity infusions: troubleshooting “no flow” situations Page 3
(c)
Strategy 2: Using cold or irritant solutions
Documentation
If venous spasm does occur, apply a warm pack or compress to dilate the vein (Barrott et al., 2020).
Page 3 of 3
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Ensure that the patient is comfortable. Decontaminate your hands and dispose of equipment according to local policy. Document what has taken place in the patient’s notes.
Strategy 4: Apply a GTN patch
Application of a glyceryl trinitrate (GTN) patch can also help vasodilation (BNF, 2021). A low-dose (5 mg/24 hours) GTN patch that is licensed for maintenance of venous patency must be prescribed. As with the application of local heat, this method may help to relieve pain and resolve venous spasm, allowing free flow of the infusion to continue.
Ask if the patient feels any pain. If there is no swelling or pain, continue to inject the solution slowly, 1 mL at a time, over a period of about 1 minute. Use a pulsatile (push–pause) technique. This aims to create a turbulent flow that will remove debris from the internal wall of the cannula (Munoz-Mozas et al., 2020). (If resistance persists, remove the cannula.)
When removing the syringe of sodium chloride, use a positive-pressure technique: maintain pressure on the plunger of the syringe, and clamp the extension set before disconnecting the syringe from the cap. This method prevents blood from entering the tip of the cannula, reducing the risk of occlusion (Munoz-Mozas et al., 2020).
Irritant or cold solutions can cause venous spasm. Diluting the solution as recommended or taking the solution from the fridge shortly before use can help (Barrott et al., 2020).
AUX
AUX
OMINEN BP
Lubricating Gel
Lubricating Gel
Lubricating Gel
Lubricating Gel
GlycerinSuppositories BP
GlycerinSuppositories BP
GlycerinSuppositories BP
GlycerinSuppositories BP
(e)
18 7 21
21
12
34
5
ml
67
89
10
0
12
34
56
78
910
ml
2014-16
LOT 0077100
055
18 7 21
21
223
45
67
89
(c) (d)
WARM PACK
Strategy 2: Avoid using cold or irritant solutions Strategy 3: Apply local heat
! Ensure the compress is not too hot


















