GRAMPIAN WINTER (SURGE) PLAN 2018/19 · This document is t he Grampian Winter (Surge) Plan for...
82
1 GRAMPIAN WINTER (SURGE) PLAN 2018/19 APPROVED 1 st November 2018
Transcript of GRAMPIAN WINTER (SURGE) PLAN 2018/19 · This document is t he Grampian Winter (Surge) Plan for...

1
GRAMPIAN
WINTER (SURGE) PLAN
2018/19
APPROVED 1st November 2018
2
Contents Page
Executive Summary 3 Introduction Aim of Plan 7 Rationale and Planning Assumptions 7 Approach 8 Funding of the Plan 9 Approval of Plan 10 Governance Arrangements 11 Key Drivers and Changes from Previous Winters Striving to Deliver High Quality, Safe, Person-centred Care 11 Trends in Data from Previous Years 14 Lessons Learned from 2017/18 16 New Developments & Service Changes Since Winter 2017/18 17 Action Plan for Winter 2018/19 Information, Communication and Escalation 21 Joint Working and Integration 25 Prevention and Anticipating Demand 27 Planned Healthcare Capacity and Demand 31 Unscheduled Care Capacity and Demand 34 Specific Plans for During and Post the Festive Period 38 References 43 Appendices Appendix 1 – Summary of Winter Plan Actions 44 Appendix 2 – Process and Timescales for Development & Review of Winter Plan 47 Appendix 3 – Winter Trends Intelligence Report 2017/18 48 Appendix 4 – Preparing for Winter 2018/19 – Supplement to 1st Draft Winter Plan 2018/19 54 Appendix 5 – Preparing for Winter 2018/19 Grampian Self Assessment Checklist 59 Appendix 6 – Strengthening Capacity for Winter 2018/19 Across Grampian – Summary 83 Contact: Kate Livock, 6 EA Programme Manager, NHS Grampian – [email protected]

3
Executive Summary This document is the Grampian Winter (Surge) Plan for 2018/19. It is an overarching document for three Health and Social Care Partnerships in Aberdeen City, Aberdeenshire and Moray and for the Acute Sector of Grampian. It is representative of local Winter Plans of each of these areas and has been coordinated and produced by NHS Grampian. This Grampian Winter (Surge) Plan sets out the planning and preparations for Winter that have taken place in each of the sectors and settings at a high level and also describes some of the investments and improvements undertaken in Grampian since the previous winter of 2018/9. The shared learning across boards has been enhanced by the 6 Essential Actions Learning Workshops and the recently established Regional Programme Managers monthly meetings which also facilitate sharing of the approaches taken to ensuring robust winter planning across other boards. The Strategic Planning of Unscheduled Care across Grampian is led by an Integrated Planning Board for Unscheduled Care (the 3 H&SCP Chief Officers and Acute General Manager) with four identified priority areas, Anticipatory Care plans, Discharge Planning, Out of Hours and Palliative Care, focused across the 6 delegated services of Rehabilitation Medicine, Geriatric Medicine, Emergency Medicine, Respiratory Medicine, Palliative Care and General Medicine. Some key aspects of this plan include: Winter Resilience
• The provision of an immediate, high-level leadership steer to practitioner staff in all sectors from Grampian Medical Director and Nurse Director with consistent support and performance management across the Senior Leadership Team.
• The continued application of the 6 Essential Actions framework with extended membership of
the 6 Essential Actions Project Boards on both acute sites- including representatives from the Partnerships, Clinical Support Services and Facilities. This incorporates weekly monitoring of the existing winter performance indicators as well as the agreed trajectories for earlier and weekend discharges
• The robust winter planning approach adopted by Grampian since 2015/16 which continues to
support a thorough planning process and a cross-system Final Plan.
• The improved model of safety & flow briefs established in Grampian Acute and Community Hospitals since 2017/18 provides a better “grip” on the hospital state and creates an informed management position that is more ready to respond to barriers to flow on a daily basis.
• The implementation of the Daily Dynamic Discharge Approach across inpatient areas in both acute sites and a number of community hospitals is supporting flow through the sites by facilitating discharges earlier in the day.
• Following the introduction of a dedicated Occupational Therapy Resource shared across the
Emergency Department, Acute Medical and Surgical Assessment Unit at Dr Gray’s hospital,

4
Elgin there has been an increase in discharges directly from these areas. This model is now replicated in the Emergency Department at Aberdeen Royal Infirmary providing identification and focused management of frail elderly at the front door.
• A test of change modelling the Integration of Aberdeen City Social Work presence within the Emergency Department at Aberdeen Royal Infirmary provides the opportunity to access resource links / knowledge to facilitate flow directly out of ED prior the patient being admitted.
• Those areas that are required to respond immediately to periods of acute peaks in demand
have ensured that staffing rotas are aligned accordingly, for example in the Emergency Departments and in the Acute Medical Initial Assessment areas of both Acute Sites. All frontline staffing rotas are complete at the end of October 2018.
• The management of elective inpatient capacity and elective activity will be supported by the approved Surgical Resilience Plan, led by a dedicated Divisional General Manager, Divisional Clinical Director and General Manager Acute Sector and supported by approved local policies for managing elective activity. The aim of the Surgical Resilience Plan is to safeguard elective activity (including day case activity) from the impact of winter pressures and ensure the maximised utilisation of elective theatre capacity.
• Establishment of a Surgical Ambulatory Care service at ARI has led to a reduction in admissions to the Surgical Receiving Unit. An extension to the operating hours of this service is planned for Winter 2018/19.
• The established Ambulatory Emergency (Medical) Clinic which has continued to deliver a reduction in admissions to the Acute Medical Assessment Unit will extend to a 7 day service.
• A test of change introducing the provision of increased Physiotherapy and Occupational Therapy assessment at weekends within the Respiratory Service at ARI is planned to facilitate the increase of weekend and Monday morning discharges.
• Proactive discharge planning to ensure safe, effective and timely discharge at Dr Gray’s
hospital is to be further supported by the introduction of a site wide discharge co-ordinator role.
• To enhance good practice in ensuring the right patient is cared for in the right place by the right person at the right time the Older Peoples Assessment and Liaison team which supports decision making about admissions and transfers in the community will be directed to areas of pressure at times of surge. In addition there will be optimisation of the synergies between the OPAL team and the newly established Acute Hospital at Home team within Aberdeen City HSCP
• In Dec 2018 Aberdeen City Delayed Discharge Group will increase the frequency of meeting from monthly to fortnightly in anticipation of increased activity and to take action to address delays. In addition the group will be able to increase the frequency of meetings in times of surge and take action to address delays.

5
• In Aberdeen City, Care Home Bed capacity (minimum of 27 social care beds) will be reserved specifically to support discharge and improve flow out of hospital.
• Procedures governing the allocation of Interim beds, in Aberdeen City, which are dedicated to supporting discharge, have been updated to allow their priority criteria to vary to reflect and address cross system demand.
• In Aberdeenshire a test of change focused on enhancing the daily safety and flow huddle
model on Thursdays to encompass planning for predicted demand in the community over the weekend and public holidays is being implemented with the aim of supporting increased discharges over the weekends.
Avoiding Unnecessary Admissions • A Test of Change in the Respiratory (COPD) Pathway in the community aims to reduce the
number of respiratory hospital admissions. It includes focused interventions to support increased self management of adults with COPD alongside specific support from GP’s, Community Pharmacists, and Community Physiotherapists. The model also includes enhanced targeting through direct communication to encourage appropriate vaccination ahead of the festive period.
• The existing Virtual Community Ward model across GP practices in Aberdeenshire & Moray
has ensured preventative measures are in place to maintain vulnerable patients in the community and reduced inappropriate hospital admissions. In addition closer working between the Virtual Community Ward and the Integrated Discharge Hub at ARI facilitates earlier discharge to home of patients in ARI.
• A number of care home beds in Aberdeen City HSCP will be identified to provide a “step –
up” community bed provision that support avoidance of hospital admission. In addition Community Hospital beds across Aberdeenshire provide the required “step-up capacity” to avoid unnecessary acute hospital admissions and deliver care closer to patient’s homes.
• The Acute Hospital at Home Service in Aberdeen City and the Aberdeenshire Response Care
at Home Team (ARCH) operating across the Community respond to surges in demand by preventing unnecessary admissions, providing augmented care in the patients home, supporting discharge and end of life care.
• The Moray Out of Hours Pilot Project will provide a resource to support vulnerable adults for
short periods between the hours of 17.00 and 08.00, who would otherwise have potentially been admitted to an acute hospital. Requests for support from this service can be made by the Emergency department, Out of Hours GP service, Social Work and the Scottish Ambulance Service.
• Hanover Housing Development introduced in Moray provides a “close to home” nursing care
model when the patients home is not an option, delivering a “step up” community bed provision that avoids admission to an acute hospital
• GP Practices will be set up to flex and offer additional “on the day” appointments immediately
following the festive period public holidays, based on actual fluctuations in demand/surge.

6
Surge Capacity Provision In addition to the local investment made in Grampian by the NHS Board and the Health and Social Care Partnerships to improve responsiveness and resilience ahead of winter 2018/19, Grampian has received a winter allocation to support the system in dealing with an anticipated surge in demand. This funding has been allocated on a cross system basis and a summary of the additional surge capacity and resource is tabled below, with more detail provided throughout this Plan. Site Surge Capacity Staffing Resource Aberdeen Royal Infirmary
Ward 305 – 13 beds Ward 306 – 16 beds Ward 211 – 12 beds Ward 402/203 – 4 beds. Total 45 beds
Nursing – 47.05 wte Consultant – 1.00wte Junior Medical Staff – 3.00wte AHP – 6.20wte (Physio/OT/SALT/Dietician) Pharmacists & Technicians – 1.50wte Phlebotomist – 1.20 wte Facilities – 6.00wte (Portering /Domestics)
Dr Grays Hospital Elgin
Total 11 Beds
Nursing – 20.58 wte Consultant – 1.00 wte AHP – 2.00 wte (0.5 Physio 0.5 OT/0.5 Physio Support Worker/0.5 OT Support Worker) Phlebotomist – 0.5 wte
Aberdeen City HSCP
4 Additional Beds ring fenced for admission avoidance
Appropriate staffing levels
Aberdeenshire & Moray Community Hospitals
Ensure all beds are open and areas staffed appropriately.
This will remain a challenge with the various workforce and winter pressures.
Key investments are described in section J. New Developments & Service Changes Introduced Since Winter 2017/18 on page 15 of this plan.

7
Introduction A. Aim of Plan 1. To set out the key partnership actions, timescales and planning processes in effectively
managing the potential challenges associated with the winter period for 2018/19 and delivering against the national and local targets and standards for health and care.
2. To ensure that Grampian is as prepared as possible for the coming winter period in order to
minimise any potential disruption to services or diminished experience for patients and carers.
B. Rationale and Planning Assumptions 3. This Plan is informed and guided by various formal sources both external and internal as
well as planned discussions and workshops to learn from previous experience, assess winter risk and agree shared approaches. Those sources include;
• 6 Essential Actions National Improvement Programme • 6 Essential Actions Grampian Improvement Programme • NHS Scotland Directorate for Health Performance and Delivery; Preparing for Winter
2018/19. • NHS Scotland Directorate for Health Performance and Delivery; Winter
Preparedness: Self Assessment Guidance • Grampian Local Health & Social care Review of Winter 2017/18 • Grampian Integrated Winter Planning Process; cross system planning workshops,
debriefs and table top testing exercises. • Partners’, sectors’ and services’ winter plans and surge plans
4. Evidence and review of local experience demonstrates that the winter period November to
March creates a number of challenges for all partners delivering health and social care services. The main challenges are outlined below and this plan attempts to use learning points in addition to demand and capacity data sourced from System watch based on activity levels from previous years to support a robust implementation plan to deliver its aim.
5. Winter 2017/18 saw many of the expected challenges associated with the period; an
increase in levels of activity for NHS24, the Scottish Ambulance Service. Daily emergency admissions averaged 153 per day, an increase of 5.2% compared to the same period in 2017/18 and elective admissions averaged 156 per day, a decrease of 6.8% from the same period in 2017/18. In addition there was a continued decrease in delayed discharges in ARI & Woodend Hospital.
6. The increased rate of emergency admissions underlines the importance of surge and
capacity planning; forward and surge planning is required at system and team level in order to be sufficiently prepared for the winter period. Space and available equipment should be identified in these plans and there is a requirement for a focus on workforce capacity at a time when Christmas and New Year holidays fall. Workforce rotas that are robust and where

8
possible, eliminate the need for locum staff are required to be in place in advance of winter. 7. Intelligence shows that for some services there are significant surges in activity at particular
points during the festive period, particularly when the calendar presents 4 day breaks for public holidays over Christmas and New Year. This can cause a backlog of activity that then presents as a surge when services resume or it can cause demand to shift elsewhere in the system, for example an increase in calls to the out of hours service.
8. Increased risk of severe weather incidents can result in significant, even extreme disruption
to the normal delivery of health and social care services in Grampian. Previous experience of weather related major incidents has increased the organisational and service level understanding of the potential of such events to test the staff’s ability to attend for duty; to present a risk to populations for whose care and safety we are responsible and prevent some patients from accessing clinical care. Local Business Continuity plans reflect the requirement for enhanced partnership working in such situations
9. It is critical that we can continuously deliver high quality, person-centred care in the right
place, at the right time and by the most appropriate person/team in an integrated way as far as possible. Underpinning this is a number of standards which supports the quality of care, in addition to the delivery of effective and efficient care. Performance against these standards and targets must be optimised despite the challenges outlined above.
C. Approach
10. In Grampian there is an established process for winter planning which is undertaken as a
year-round planning cycle and incorporates an integrated approach with business continuity principles. Partners such as the acute services, NHS24, SAS, Health and Social Care Partnerships are key to the process and participate in joint planning and debrief exercises.
11. It is recognised that winter planning is complex and can be challenging, this is addressed by
early planning at local and even team level, and by building this into sector, divisional and Board level plans. This ensures local ownership and understanding of responsibilities, actions and responses to surge levels and scenarios.
12. Another important step in the planning cycle for winter is the opportunity to learn from
previous experience; much of our predictions and planning assumption come from reviewing the previous years’ activity and identifying lessons to be learned. Undertaking this activity allows local teams and services to be clear about what can be improved and how plans can be refined. Doing so in an integrated way across services, sectors and partners enables a supportive forum for sharing experiences and learning across a whole system. The output from this step in the process is produced in a Local Health & Social Care Winter Report which is shared across the system and with Scottish Government.
13. Services, sectors and partners across the health and social care system in Grampian
(Health and Social Care Partnerships, acute sites, G-MED, NHS 24, Scottish Ambulance Service) prepare annually updated business continuity plans relevant to their own respective organisations/services. These can include detailed flu responses, business continuity actions and the prioritisation for core service delivery in times of surge, reduced capacity or critical incidents, escalation plans, delayed discharge plans and communication plans as

9
appropriate. 14. Rates of delayed discharges are closely monitored by the system and each of the
Partnerships is focused on managing the return of people to local communities as early as can be managed. Challenges across Grampian continue around staffing and recruitment for the care workforce, however the focus is on prioritising those patients who can and should be transferred from acute to community settings as early as possible. This is supported by integrated working across the Discharge Hub in ARI and the daily huddles in Dr Grays and in addition a weekly Moray Cross System Discharge huddle.
15. Health and Social Care Partnerships developed and are continuing to deliver against
delayed discharge action plans which aim for local solutions to reduce the rate of delayed discharges. The focus includes accurate data on bed capacity in community hospitals and use of goal setting to support the transfer from acute to community settings, and use of Daily Dynamic Discharge board rounds in the acute & community hospitals to support positive challenges for the inpatient journey.
16. In Aberdeen City & Aberdeenshire, a number of key actions deliver improvements; namely
the successful recruitment and subsequent introduction of additional social work capacity that is now embedded in both the ARI and Woodend hospital sites. In Aberdeen City data has indicated a notable reduction in delays pertaining to social work/care assessment. The ‘building up’ of interim bed capacity to support the early discharge of patients/clients whilst they await a more permanent care setting of their choice has produced a total 27 beds in this part of the system.
17. It is recognised that it can be very difficult to ‘flex’ certain elements within the system, such
as staffing and bed capacity in hospitals and nursing home settings, especially when there is limited additional funding to meet the additional and specific challenges. Winter planning in Grampian therefore acknowledges the importance of keeping people healthy, preventing unnecessary hospital admissions, anticipating demand and the reorganisation of capacity and resources to ensure effective patient flow throughout the health and care system.
18. The Scottish Government winter planning guidance and supporting self-assessment
checklist informs the development of this Plan.
D. Funding of the Plan 19. In October, Scottish Government announced £928,022 funding for Grampian Health Board
and Integration Joint Board to augment local winter resilience funding; however at this stage much of the winter planning has already been undertaken. The additional funding is helpful in mitigating the increased spending that can be associated with surges in demand. An integrated approach has been taken to allocating this resource with all three Chief Officers and the Acute Director agreeing on how this could best be allocated. Funded activity will include surge capacity in ARI & Dr Grays Hospital and will also support activities focused on improving patient flow and avoiding unnecessary admissions in Aberdeen City, Aberdeenshire and Moray.
20. As in previous years it is imperative that early planning and sufficient testing of plans is
10
complete ahead of winter to enable Grampian to be prepared to meet the challenges of winter, and within budgets. Tabletop testing has proved highly useful and practical for all partners in previous years and these activities have been undertaken across Grampian in 2018.
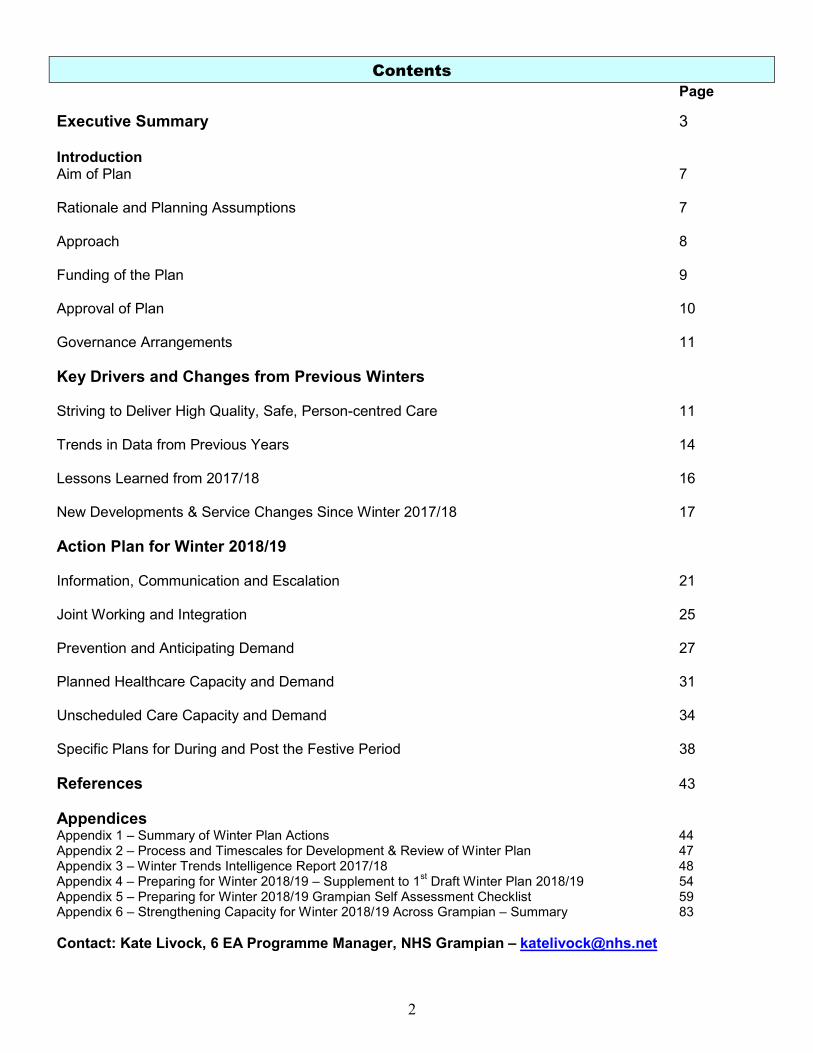
21. The dates of the facilitated and scenario-based tabletop test exercises have been –
Aberdeen City HSCP 31st August Acute Sector ARI/DGH 17th October Aberdeenshire HSCP 12th October Moray HSCP 20th September Cross System/Sector 28thSeptember
22. Timing of these exercises is designed to provide opportunity for all partners and staff to challenge their planning and to refine and amend plans based on any learning points identified by the test. All of the tabletop testing exercises are supported by NHS Grampian colleagues and involve input from NHS Grampian Civil Contingencies, with use of appropriate and national processes for resilience management.
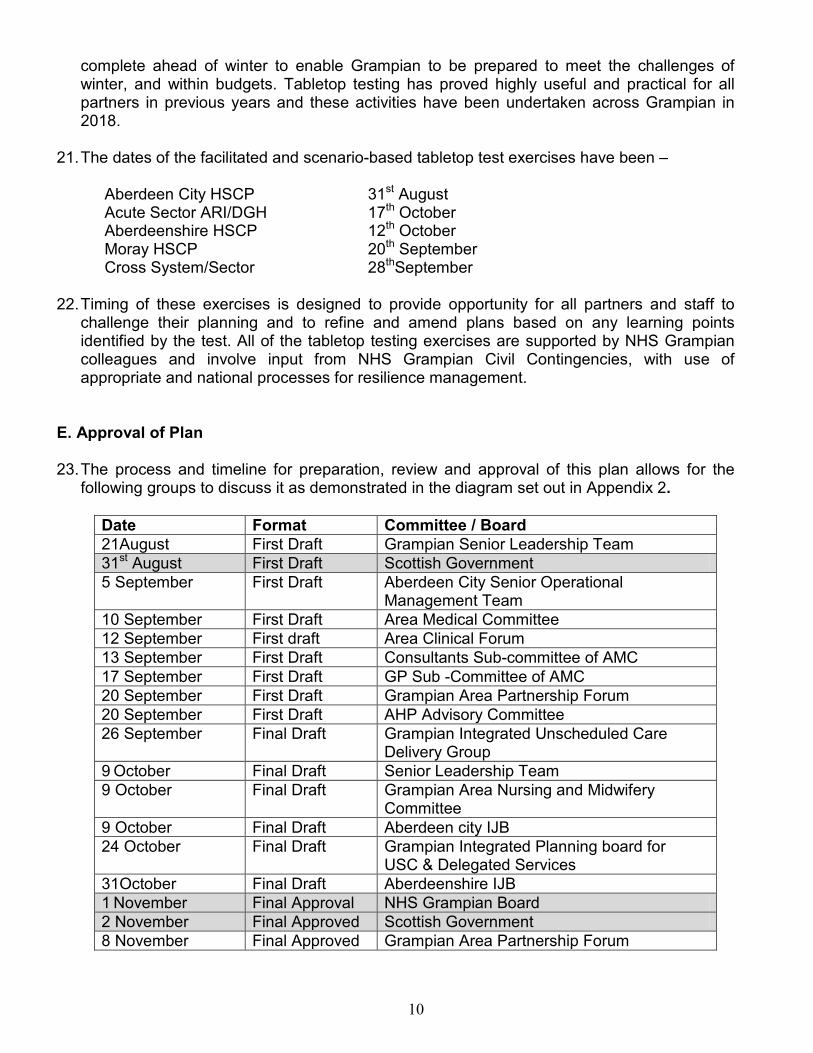
E. Approval of Plan 23. The process and timeline for preparation, review and approval of this plan allows for the
following groups to discuss it as demonstrated in the diagram set out in Appendix 2.
Date Format Committee / Board 21August First Draft Grampian Senior Leadership Team 31st August First Draft Scottish Government 5 September First Draft Aberdeen City Senior Operational
Management Team 10 September First Draft Area Medical Committee 12 September First draft Area Clinical Forum 13 September First Draft Consultants Sub-committee of AMC 17 September First Draft GP Sub -Committee of AMC 20 September First Draft Grampian Area Partnership Forum 20 September First Draft AHP Advisory Committee 26 September Final Draft Grampian Integrated Unscheduled Care
Delivery Group 9 October Final Draft Senior Leadership Team 9 October Final Draft Grampian Area Nursing and Midwifery
Committee 9 October Final Draft Aberdeen city IJB 24 October Final Draft Grampian Integrated Planning board for
USC & Delegated Services 31October Final Draft Aberdeenshire IJB 1 November Final Approval NHS Grampian Board 2 November Final Approved Scottish Government 8 November Final Approved Grampian Area Partnership Forum

11
8 November Final Approved Consultants Sub Committee 12 November Final Approved Area Medical Committee 14 November Final Approved Area Clinical Forum 19 November Final Approved GP Sub Committee Final Approved AHP Advisory Committee Final Approved Grampian Area Nursing and Midwifery
Committee 29 November Final Approved Moray IJB
24. As in previous years, the final Grampian Winter Plan will be available on the NHS Grampian
website following submission to and approval by the Scottish Government. F. Governance Arrangements 25. High level performance management of the Grampian Winter (Surge) Plan for 2018/19 will
be through the Senior Leadership Team which is chaired by the Chief Executive and includes the chief accountable officers from each of the Partnerships and the acute sector as well as executive team members from NHS Grampian.
26. Each of the Health and Social Care Partnerships will follow its own local governance
arrangements ensuring the local winter plan and the overarching Grampian Winter Plan are included for discussion on agenda at relevant meetings ahead of the final submission to Scottish Government. The calendar for this is outlined in the table above.
27. Performance management of underpinning organisational/sector/service winter plans is
undertaken as per agreed mechanisms within local teams and areas. In support of the various plans and to ensure effective communication and integrated working over the winter period, the daily cross system huddle, which has been identified as crucial to integrated working, will support business continuity for winter as it would for any surge period.
28. The Unscheduled Care operational division within the acute sector will, on behalf of NHS
Grampian, submit the routine weekly management information to the Scottish Government as and when required as per an agreed template. As is currently required the Acute Sector of ARI will submit additional daily reports on any key pressures and unusually long waits in the Emergency Department; with details of the actions being taken to address the delays.
Key Drivers & Changes from Previous Winters G. Striving To Deliver High Quality, Safe, Person-Centred Care 29. Regardless of the time of the year, we continuously strive to meet local and national
standards and performance targets which focus on delivering high quality, safe person-centred care at the right time, in the right place and by the right person/team. A key element of this is delivering national standards and
12
targets on an ongoing basis regardless of the pressures across the system;
• 98% of NHS 24 Priority 1 calls responded to within 60 minutes and 90% of Priority 2 calls responded to within 120 minutes
• 75% of all Scottish Ambulance Category A calls are responded to within 8 minutes
• Reduction in inappropriate attendances at Emergency Departments (ED / Minor Injury Units (MIU’s)
• 95% performance against the 4 hour standard for Emergency Departments (ED) and
Minor Injury Units (MIUs)
• Elimination of patients waiting over 12 hour for admission or discharge within ED
• Maintain delivery of the 18 week Treatment Time Guarantee (TTG) • 95% of all patients diagnosed with cancer to begin treatment within 31 days of
decision to treat, and 95% of those referred urgently with a suspicion of cancer to begin treatment within 62 days of receipt of referral.
• Maximise the number of patients who receive care in the most appropriate setting
• Minimise the number of patients waiting to go to a community hospital
• No delayed discharges beyond 14 days
There has been further development and progress of the 6 Essential Actions Improvement Programme, which focuses on key actions to improve unscheduled care in all settings. Grampian is committed to an integrated approach to achieving improvement and demonstrating excellence in the 6 Essential Actions Programme locally and significant senior, executive, partnership and operational staff are dedicated to and involved in its delivery. Consequently, this Plan is developed in the context of the 6 Essential Actions and unsurprisingly there are shared priorities, focus and projects as well as partnerships and groups. Key drivers informed by the 6 Essential Actions Programme are included here:

13

14
H. Trends in Data from Previous Years 30. The NHS Grampian Health Intelligence Department, with partner colleagues, produces trend
data for the winter period focussing on the previous three years, to support planning for the resources that will be required and in identifying thresholds for surge planning. In addition demand and capacity predictive data based on data sourced from System Watch is used. For example it can be seen from the graph below that peaks in emergency admissions take place on key dates such as Mondays and particularly following a 4 day closure.
31. The full set of trend data with key highlights is attached at Appendix 4. Activity trends and performance levels have been discussed and shared across sectors and services as part of reflecting on the previous winter in the Cross System Winter debrief event held in May 2018

15
80
100
120
140
160
180
200
220
01-Nov 08-Nov 15-Nov 22-Nov 29-Nov 06-Dec 13-Dec 20-Dec 27-Dec 03-Jan 10-Jan 17-Jan 24-Jan 31-Jan 07-Feb 14-Feb 21-Feb 28-Feb 07-Mar 14-Mar 21-Mar 28-Mar
Num
ber o
f Em
erge
ncy
Adm
issi
ons
Daily Emergency Admissions: November - March
2015/16 2016/17 2017/18

16
I. Lessons Learned from 2017/18
32. The following section outlines the key lessons learned from the review of the 2017/18 winter
period. The full report is available separately.
• The significant value of timely partnership, whole-system and intelligence driven winter planning.
• Acknowledgement in all areas that a more robust approach to winter planning and enhanced communication contributed greatly to wards maintaining patient care and services during period of adverse weather and increased instances of influenza.
• Many features developed in 2017 had a positive impact on sectors’ and teams’ ability to manage demand and challenges.
• Cross system huddle, safety brief models and the discharge hub were all referenced as beneficial.
• It was recognised that the enhanced whole-system approach and joined-up working through the development of the plan itself, cross-system huddles, regular reviews and communication led to minimal disruption to patient care during challenging times.
• Extended operational hours of Ambulatory Care services effectively supported admission avoidance reducing pressure on in-patient capacity.
• Staffing levels due to high numbers of vacancies posed a challenge for several services in terms of managing business continuity as well as surge planning.
33. A number of areas were also highlighted for further improvement which were generally
focussed around the following themes:
• Communication/Cross-System Working • Robust communication across health and social care services still has room for
improvement to ensure all health & social care operational staff are appraised of local plans.
• There is still the requirement to further improve the accuracy of data such as predictive activity data. Consideration to be given to the use of System Watch data alongside local predictors to plan surge capacity and staffing resource effectively
• Anticipatory Care plans could have been more effective and better communicated.
• Communication with the public (Know Who To Turn To) re expectations and responsibilities is important and key to ensuring local services are used appropriately.
• A desire to see equity in the degree of risk and level of responsibility held by partners across the system
• Flow and Discharge Planning
• The importance of sustaining the principles of the Daily Dynamic Discharge Approach across all inpatient areas is key to effective discharge planning and management.
• Building on criteria led discharge is key to timely discharge. • Ensuring patients are in the right place will continue to be a focus for work to

17
reduce the number of boarded patients across both sites • Practice of ring-fenced acute beds in the community could be further improved
to support flow. • The availability of Allied Health Professional Staff, especially physiotherapists
are key to facilitating discharge over the festive period in particular. • Increased rehabilitation and enablement services are key to preventing
admissions/reduce the length of stay and improved flow through Acute and Community Hospitals.
• Operation of the integrated discharge hub over public holiday periods significantly improves patient flow.
J. New Developments & Service Changes Introduced Since Winter 2017/18 34. Some of the key service and system changes that have occurred (or are due to occur) since
last winter and prior to winter 2017/18 are listed below; System
• In support of the established and embedded Integrated Joint Boards and Health and Social Care Partnerships, Grampian has established a Grampian Unscheduled Care Programme Board with membership from the Executive Lead for USC, Director of Acute & Chief Officers
• The role of the Unscheduled Care Programme Board is to guide the strategic direction, delivery and commissioning plans for Unscheduled Care and to monitor performance in relation to the acute services delegated for strategic planning by the Integrated Joint Boards.
• The UC Programme Board’s aim is to improve people’s experience of unscheduled health
and social care through improving access to good quality care; in community and hospital settings.
• The Unscheduled Care Programme Board is supported by the Unscheduled Care Delivery Group, a multidisciplinary group of clinical and operational staff from across the Health and Social Care partnerships, who are responsible for delivery of the commissioned model and for a system-level overview of improvements across Unscheduled Care.
• The membership of both Acute site 6 Essential Actions Project Boards includes representatives from the Health and Social Care Partnerships, Clinical Support Services, Facilities teams and Scottish Ambulance Services.
• Shared learning across boards has been enhanced by the 6 Essential Actions Learning Workshops and the recently established Regional Programme Managers monthly meetings at which Tayside, Highland and Islands and Grampian teams benefit from learning and sharing regional approaches to ensuring robust winter planning.
Acute
• The models of safety briefs in Grampian Acute and Community Hospitals have been further developed throughout 2017/18 and are now well established as a daily occurrence with capacity and management data shared across ARI and Dr Gray’s hospitals. This has provided a better ‘grip’ on the hospital state and creates a management position that is more ready to respond to surges in
18
demand and barriers to flow on a daily basis. • The knowledge and information gained from this daily event can then be shared across
teams, escalated across sectors and up to the Cross System Huddle as well as to Scottish Government and NHS Resilience as appropriate and if necessary.
• The Discharge Hub is well established in Aberdeen Royal Infirmary and constitutes liaison
nursing staff, OPAL team, social work colleagues from each of the three Partnerships and hospital discharge coordinators. A test of change providing ongoing assessment of complex discharges during the weekend periods is being run prior to winter.
• Redirection has been a feature of hospital operations for a number of years, however
lessons learned from previous winters indicated the value of clinical conversations taking place face to face with patients at the front door. As a result this practice is well established in both acute hospitals utilising the availability of GPWSI undertaking sessions in the Emergency department undertaking the face to face clinical conversations.
• The Daily Dynamic Discharge Approach designed to ensure that local teams have everything they need to deliver tangible improvements in patient safety and flow has been introduced across inpatient wards on both acute sites and a number of community hospitals. A number of Discharge Co-ordinator posts across acute sites support timely and effective discharge planning and the agreed improvement trajectories for weekend and earlier in the day discharges
• Following the introduction of a dedicated Occupational Therapy Resource shared across
the Emergency Department, Acute Medical and Surgical Assessment Unit at Dr Gray’s hospital, Elgin there has been an increase in discharges directly from these areas. This model is now replicated in the Emergency Department at Aberdeen Royal Infirmary providing identification and focused management of frail elderly at the front door.
• A test of change modelling the Integration of Aberdeen City Social Work presence within the Emergency Department at Aberdeen Royal Infirmary provides the opportunity to access resource links / knowledge to facilitate flow directly out of ED prior the patient being admitted.
• Extending the operating hours of the Surgical Ambulatory Care service has seen a further
reduction in admissions to the Surgical Receiving Unit.
• A test of change seeing the provision of increased Physiotherapy and Occupational Therapy assessment at weekends within the Respiratory Service is planned to increase weekend and Monday morning discharges.
• Proactive discharge planning to ensure safe, effective and timely discharge at Dr Gray’s hospital is further supported by the introduction of a site wide discharge co-ordinator role.
Community
19
• A Test of Change in the Respiratory (COPD) Pathway in the community aimed at
reducing the number of respiratory hospital admissions includes focused interventions to support increased self management of adults with COPD alongside specific support from GP’s, Community Pharmacists, Community Physiotherapists. The model also includes enhanced targeting through direct communication to encourage appropriate vaccination ahead of the festive period.
• The introduction of a Virtual Community Ward model across GP practices in
Aberdeenshire & Moray has ensured preventative measures are in place to maintain vulnerable patients in the community and reduced inappropriate hospital admissions. In addition closer working between the Virtual Community Ward and the Integrated Discharge Hub at ARI facilitates earlier discharge to home of patients in ARI.
• In addition to the weekly care home vacancy report (held by Aberdeen city)
Aberdeenshire has established a ‘real time’ resource which monitors vacancies across all resources, including community hospitals, care homes, very sheltered and sheltered housing. This ensures practitioners have up to date information enabling patients/service users have access to the most appropriate environment at the right time and maximises the use of resources, supporting effective whole system flow.
• In Aberdeenshire a test of change focused on enhancing the daily safety and flow huddle model on Thursdays to encompass planning for predicted demand in the community over the weekend and public holidays is being implemented with the aim of supporting increased discharges over the weekends.
• In Dec 2018 Aberdeen City Delayed Discharge Group will increase the frequency of meeting from monthly to fortnightly in anticipation of increased activity and to take action to address delays. In addition the group will be able to increase the frequency of meetings in times of surge and take action to address delays
• To enhance good practice in ensuring the right patient is cared for in the right place by the right person at the right time the OPAL team which supports decision making about admissions and transfers in the community will be directed to areas of pressure at times of surge. In addition there will be optimisation of the synergies between the OPAL team and the newly established Hospital at Home team within Aberdeen City HSCP
• In Aberdeen City, Care Home Bed capacity (27 social care beds + 4 surge beds) will be reserved specifically to support discharge and improve flow out of hospital.
• Procedures governing the allocation of Interim beds, in Aberdeen City, which are dedicated to supporting discharge, have been updated to allow their priority criteria to vary to reflect and address cross system demand.
• In Aberdeen City arrangements are in place to enable staff to consistently triage and update patients/ clients homecare provision needs in advance of winter to ensure that those in greatest need (including hospital based delayed patients ) have any care home capacity directed to them on a priority basis. In addition Home care packages will be

20
prepared in advance for activation over the festive public holidays
• A number of care home beds in Aberdeen City HSCP will be identified to provide a “step – up” community bed provision that support avoidance of hospital admission. In addition Community Hospital beds across Aberdeenshire provide the required “step-up capacity” to avoid unnecessary acute hospital admissions and deliver care closer to patient’s homes.
• Hanover Housing Development introduced in Moray provides a “close to home” nursing care model when the patients home is not an option, delivering a “step up” community bed provision that avoids admission to an acute hospital.
• The Moray Out of Hours Pilot Project will provide a resource to support vulnerable adults for short periods between the hours of 17.00 and 08.00, who would otherwise have potentially been admitted to an acute hospital. Requests for support from this service can be made by the Emergency department, Out of Hours GP service, Social Work and the Scottish Ambulance Service.
• The Hospital at Home Service in Aberdeen City and the Aberdeenshire Response Care at Home Team (ARCH) operating across the Community respond to surges in demand by preventing unnecessary admissions, providing augmented care in the patients home, supporting discharge and end of life care.
• GP Practices will be set up to flex and offer additional “on the day” appointments based on actual fluctuations in demand/surge.

21
Action Plan for Winter 2018/19 35. The Grampian 2018/19 Winter Plan actions are set out in the following themes:
• Information, Communication and Escalation • Joint Working and Integration
• Prevention and Anticipating Demand
• Planned Healthcare Capacity and Demand
• Unscheduled Care Capacity and Demand
• Plans for Pre, During and Post Festive Period
K. Information, Communication & Escalation
36. Reporting to Scottish Government
Reporting to the Scottish Government will focus on the points below: • Regular submission of admission data to ISD to inform the national modelling System
Watch Project as usual practice. • NHS Grampian will ensure that Weekly Winter Monitoring information is timeously
submitted as and when requested. • Exception/daily reporting such as a daily performance and pressures report will be
undertaken as requested by the Scottish Government. This will be ensured by the Acute Sector Division of Unscheduled Care and linked to the daily, site based Safety Huddles.
• Immediate notification of significant incidents will occur as per current agreed reporting procedure for each partner organisation. Communication and sharing of such incidents will be highlighted at the daily safety huddles and the daily system huddles.
• In addition, and if required, NHS Grampian will participate in daily/exceptional reporting to NHS Scotland Resilience
37. Staff Communication
• Each partner organisation and service has plans in place for effectively communicating with local staff. Key mechanisms and focus for communicating with staff in partnership are outlined below.
• The Winter Plan for 2018/19 and any other supporting documents/plans, along
with bulletins (weather, transport, flu vaccination, norovirus etc) will be available on the NHS Grampian staff intranet and NHS Grampian website.
• ‘Attendance at Work – Adverse Conditions’ is the NHS Grampian policy informally known as the ‘Snow Policy’ and will be highlighted to appropriate staff ahead of winter.
• Links to the national NHS Scotland winter campaign will be available on the NHS
22
Grampian websites • Campaigns to proactively encourage all NHS Grampian, Aberdeenshire,
Aberdeen City and Moray HSCP staff, community healthcare workers, residential care home staff, social care staff, unpaid carers and paid carers to have the flu vaccinations. Targeted communication via displaying posters in key staff areas, electronic bulletins and details posted on the NHS Grampian and local authority intranet sites as well as messages on payslips will run from 1st October 2018. In addition flu vaccination will be offered to Aberdeenshire Transport and Infrastructure staff, in particular those essential workers associated with snow clearing and gritting.
• Know Who To Turn To (KWTTT) key messages will be displayed as a banner on the NHS Grampian intranet as well as circulated via team brief, newsletter and global email alert for staff. A local article, based on national messages will be prepared for inclusion in existing newsletters (NHS, local authorities and carers) from December 2018.
• Communication of key information on services available over the festive period such as infection control advice, pharmacy dispensing services, access to social care assessment and care packages, etc will be made available through daily safety briefs and available in each nursing and doctors ward station/room across NHS Grampian in response to communication issues highlighted in previous years.
38. Key Messages for Public.
Communication Plans for 2018/19 will be agreed and implemented between October and January with the aim of:
• promoting winter health and reducing pressure on local services • encouraging individuals to take responsibility for their own health and seek advice
appropriately via the Know Who To Turn To (KWTTT) Campaign • Supporting local winter health priorities such as respiratory health via the ‘Don’t waste
a Breath’ campaign and the Antibiotic Campaign. • adding value to existing national campaigns such as flu and pneumococcal
immunisation
Key messages to be communicated in partnership to the public via mechanisms outlined below.
• Targeted staff and public flu campaigns beginning early October 2017, linking with
and utilising resources available through the national campaign. • Media releases will be distributed to all local press informing the public on basic self-
help messages, stocking of medications, repeat medications, surgery closures and available services over the festive period.
• From December 2018 the KWTTT campaign will communicate the self help messages and highlight the services available to the public and is likely to include
A targeted mail drop to households across Grampian – postcodes with the highest Emergency department attendances in Aberdeen and Elgin.
Re-direction Flyer to be handed out by ED staff when appropriate TV and radio advertising

23
Targeted Social Media messages including video messages – Using Facebook’s audience definition, we can target a particular demographic Males and females, Aged 18+, who live within an 80 km radius of Inverurie and 40 km radius of Inverness (which covers the entire Grampian area). This campaign could potentially reach 530,000 people.
Maintenance of the KWTTT website • An Antibiotic Campaign from November through December 2018. • Health points (NHS Grampian’s Health Information Centres) are located in Aberdeen,
Fraserburgh, Peterhead and Elgin. Staff working in these units will be fully briefed to provide information on all our key messages to members of the public.
• NHS Inform/Healthline advice lines • NHS Grampian will use social media, such as Twitter and Facebook, to communicate
key messages and alerts • NHS Grampian’s public website reiterates the above key messages, along with useful
links to other appropriate websites e.g. NHS 24, national campaigns. • Specific communication will be in place relating to repeat prescriptions and regarding
pharmacy opening times over the Christmas and New Year holidays. 39. Communication Between Key Partners
Since the embedding of new structures and strengthened relationships with the Health and Social Care partnerships, communications across Grampian are integrated with each of the partners fully represented as drivers of the production of the Winter Plan for Grampian and the actions that will underpin the achievement of its aims.
• This Plan has been developed and agreed as part of the Grampian Unscheduled Care 6
Essential Actions Programme, including communications and participation from partners such as SAS and NHS24.
• The planning process has included collaboration with the Head of Civil Contingencies. • Approval of the plan includes all 3 Health and Social Care Partnerships. • Approval of the planning process and timescales as well as the plan itself includes a wide
range of committees within the NHSG governance structure as well as the NHS Grampian Board.
• Daily cross system huddle meetings, includes representation from the acute sector, each Health and Social Care Partnership and the ambulance service. Partners participate virtually, joining via teleconference and in this way there is no barrier to participation.
• Escalation and communication in real-time with partners is as per agreed protocols. • Effective communication protocols are in place between key partners in relation to local
authority housing, equipment and adaptation services, mental health services and the independent sector.
• To use links with voluntary organisations and related weekly e-bulletins to promote key winter related messages
• Community Pharmacies opening times are communicated to partners • Review communication mechanisms between NHS Grampian and other NHS Boards
40. Press/Media

24
• All interview or information requests from the press or media groups will, in the first instance, be managed or if appropriate directed to the relevant organisation’s Corporate Communications Department. Opportunities will also be taken to reinforce key winter messages to the public.
41. Escalation
• Each organisation/sector/service has in place agreed business continuity plans that are intelligence based and include responses to winter challenges, staff shortages and escalation procedures. These plans are underpinned by human resources policies which support and guide staff in relation to weather and travel disruption.
• Each sector will test their business continuity plans and policies during September &
October 2018. • All business continuity plans have clear escalation procedures if services are affected by
weather, staff shortages or any other situations affecting delivery. This includes the provision of situation reports at operational and tactical level within the organisation and onward reporting, as necessary, to NHS Resilience and the Local Resilience Partnership.
• NHS Grampian acute sector has developed escalation policies to a high standard, based on the national publication of guidance on ED and hospital wide escalation.
Summary of Key Actions for Information, Communication and Escalation Reporting
- Submission of weekly management information to the Scottish Government. - Submission of daily performance and pressures reports to the Scottish Government if required. - Exception reporting and immediate notification of any significant issues to Scottish Government.
Communicating to Public/Staff
- Implementation and regular review of the Winter Health Communication Plan which includes flu, ‘, KWTTT and antibiotic campaigns.
- Targeted communication to staff on wards regarding key information during the festive period e.g. infection control advice, access to social care assessment/care packages etc, Know Who To Turn To
- Targeted KWTTT campaign in those areas with the highest users of Unscheduled Care and used in redirection.
Communication between Partners / Escalation
- Daily cross system huddles to include all partners and acute sector with Senior Decision Maker to chair. - All sectors to test winter/business continuity plans during Sept/Oct 18.
Key Areas of Risk - People may choose to ignore communication messages - Ensuring wide-spread dissemination of key messages is challenging due to the wide geographical spread and
vast number of staff, partners and public across Grampian. - Ensuring penetration of messages across partner organisations.

25
L. Joint Working and Integration 42. Good communication is a key aspect of effective integrated working. This principle is an
important aspect of the Grampian approach and is particularly critical when staff and services are under significant pressure. This section covers the various aspects being taken forward in Grampian around ensuring effective joint working over the challenging winter period.
43. In Partnership across NHS Organisations/Sectors/Services Specific actions to enhance integrated partnership working across Grampian will occur at
different levels based on the situation and are summarised below.
• Safety Briefs are now embedded features in both acute hospitals and in ARI occur up to 3 times per day. Attendance is generally around 50-60 individuals and include representation from Security, Facilities, SAS and all areas of the acute hospital. The 8am session is lead by the Senior Site management team supported by the Site and Capacity Team and information is shared with staff across the hospital twice each day.
• Models of Safety briefs in Community hospitals are established but vary in format due to local requirements.
• Cross system huddles which support individual partners to anticipate and manage surges in activity at the earliest opportunity have been improved and developed even further since they were embedded.
• Feedback from winter debrief discussions has confirmed that this approach can facilitate system-wide resolutions to delivering safe care whilst effectively managing risk.
• Identified through Winter Debrief events the consistency of cross system representation at Cross System huddles now features in H&SCP planning
44. NHS Grampian, Health & Social Care Partnerships & Third Sector
• The Senior Leadership Team includes each of the three Chief Officers, the Director of Acute Services and members of NHS Grampian’s leadership team. The Team meet weekly, alternating with formal meetings and huddles to discuss operational issues and this provides a regular and valuable opportunity to share key pressures and issues. During times of increased pressure this will support the assessment of risk equally across the whole system and the implementation of a system solution.
• The Grampian Integrated Unscheduled Care Programme Board established in May 2017
guides strategies, delivery and commissioning plans and to monitor performance in relation to the acute services delegated for strategic planning by the Integrated Joint Boards. The Programme Board’s aim is to improve people’s experience of unscheduled health and social care through improving access to good quality care; in community and hospital settings. The Programme Board comprises the three Chief Officers, NHS Grampian’s Medical Director, Director of Nursing, General Manager of Acute Services and Director of Modernisation. The Programme Board is supported by a multidisciplinary group of advisors.
• The Integrated Discharge Hub has developed further since 2017-18 and is a partnership operational team focused on ensuring appropriate supported discharge for prioritised patients by coordinating an integrated plan

26
and actions. Actions include liaison with professionals and families.
• NHSG has a memorandum of understanding with Community Off-Road Transport Action Group (COTAG) to assist with all logistical support during severe weather.
Summary of Key Joint Working and Integration Actions - Establishment of Integrated Unscheduled Care Programme Board. - Establishment of an Integrated Unscheduled Care Delivery Group. - Use of the daily partnership Cross System Huddle for Winter 2018/19. - Regular meetings at all levels to understand prioritise and resolve system issues. - Discharge Hub to support integrated approach to priority & complex discharges.
Key areas of Risk - Ensuring representatives attend the daily huddle meetings and actions are followed though. - Agencies don’t fully comply with exception reporting mechanisms. - Additional SAS Discharge Transport arrangements are not delivered in time for winter period.
27
M. Prevention and Anticipating Demand 45. A key purpose of the winter plan is to prevent, anticipate and manage potential demand.
This section sets out the key actions for preventing, anticipating and managing demand over the winter period 2018/19.
46. Influenza (Flu) Immunisation Programme Seasonal influenza is an acute, viral illness that spreads easily from person to person. Annually from October to March there is a predicted increase of flu cases and it is well recognised that health and social care staff are significantly more likely to be exposed to influenza through the course of their work. Organisations and sector/services business continuity plans include both the prevention and the containment of flu and also how services continue core business when flu increases demand on services and creates staff shortages. The flu immunisation programme is central to all preventative initiates. During 2017/18 there was an increase in vaccine uptake across all risk and occupational groups with the exception of the immunosuppressed which had a very small decrease of 0.1%. This could be accounted for by the increase in circulating disease and also the additional promotional initiatives implemented by the NHS Grampian Flu Advisory Group. The target uptake of 75% was not achieved (corresponding with the Scottish average) but the uptake in people aged 65 years and older increased by 1.4% to 73.4% (Scottish average was 73.7%). Vaccination in people at increased clinical risk aged 64 years or less also increased from 43.7% to 44.3%. Significant increases of 6.3% and 6.7% were identified in patients with chronic liver disease and pregnant women in at risk groups respectively. 57.6% of Grampian pre-school children aged 2-5 years old were vaccinated and 69.8% of our primary school children. Uptake targets for 2018/19 are:
• 75% Over 65 yrs Under 65 years in at-risk groups Primary school children
• 65% Pre-school children (2-5years) • 60% Health and social care staff
The Grampian Flu Immunisation Programme run in conjunction with the national programme and will commence on the 1st October 2018. The programme will continue to focus on the following target groups:
• All those aged 65 and over • All those aged 6 months or over in a clinical risk group • All pre-school children aged 2 -5 years • All primary school children • All pregnant woman, irrespective of their stage of pregnancy • Those living in long-stay residential care homes or other long-stay facilities where rapid
spread is likely to follow introduction of infection and cause high morbidity and mortality (not including prisons, halls of residence, boarding schools etc)
• Unpaid Carers (including young carers) • All NHS Grampian staff, as well as all health and social care staff involved in the
delivery of personal care. community

28
health care workers, residential care staff, social care staff, unpaid carers and young carers.
• In addition Aberdeenshire H&SCP will offer vaccination to essential Aberdeenshire Council Transport and Infrastructure Colleagues and in particular those essential workers associated with snow clearing and gritting.
The flu vaccination publicity campaign to encourage NHSG staff as well as social care staff, including those working in care homes, providing care at home and in the voluntary sector, will commence during September 2018. There is extensive access to vaccination for health and social care staff via GO Health services and around 65 community pharmacies across Grampian. Communication with staff and partners on flu vaccination will be undertaken, using a wide range of media routes including Global Electronic Notices, Manager’s letters, posters and National Campaign resources. Local initiatives will also run alongside the national publicity campaign for the public to promote immunisation among Grampian residents who are eligible to be vaccinated. 47. Pandemic Flu
• The Multi Agency Grampian Major Infectious Disease/Pandemic Flu Plan sets out the
structures and processes that will be used in the event of an infectious disease incident, such as pandemic influenza. The plan outlines a co-ordination of health and social care response.
• Planning assumptions for Pandemic Flu are based on the UK Influenza Pandemic Preparedness Strategy 2011 and follow a fluid DATER structure, alongside WHO pandemic phase designations
Detection Phase - characterised by normal health service delivery and increased surveillance for pandemic influenza strain activity locally through the Health Protection Team, Primary Care and hospital virology services, either with or without activation of Board operational, tactical and strategic structures and functions;
Assessment Phase - characterised by increased public health protection, primary care and pharmacy activity, with standing-up of sector and cross-system control rooms; Treatment Phase - which may be low, medium or high impact, with increasing prioritisation of service delivery in relation to scale of impact of the pandemic on health and social care delivery;
Escalation phase leading to postponement of elective non-urgent activity across potentially all sectors and
Recovery Phase - characterised by a return to ‘normal’ activities (e.g catch-up on other clinical activity, staff leave and bereavement), and preparation for a potential second wave.
• Civil contingency arrangements are in place for a Local Resilience Partnership (LRP) at
Grampian level and Regional Resilience Partnership (RRP) at North of Scotland Level. In pandemic influenza, these multi-agency groupings may be convened. It is critical that partner agencies make joint decisions and respond in a unified manner, with efficient and effective use of available resources, to mitigate potential consequences. An integrated health and social care response to a major infectious disease incident aims to:

29
Ensure that the Grampian health and social care systems are prepared for MID/
pandemic flu by using existing systems and governance mechanisms as the basis of the response supporting the continuation of everyday activities as far as practicable.
Ensuring the health and social care systems are ready to provide treatment and support for the large numbers likely to suffer from influenza or its complications whilst maintaining other essential care.
Ensure that the public receive informed and timely advice and information. Promoting a return to normality and the restoration of disrupted services at the
earliest opportunity
• There are additional supporting plans for excess death and specific response actions such as anti-viral collection mechanisms.
48. Norovirus in Community care Establishments e.g. Care Homes
• There are long standing systems in place for reporting outbreaks in community establishments with vulnerable individuals for example care homes. Following reporting of the outbreak to the Health Protection Team (HPT), immediate risk assessment is undertaken and infection prevention and control measures discussed and then followed up in writing to the manager. Infection prevention and control measures usually include closure of the establishment to all new residents, residents returning from hospital and day care. Regular monitoring of the outbreak is undertaken until the establishment has been free of symptomatic residents and staff for 48 hours.
• The Consultant in Public Health Medicine (CPHM) will, if required, activate the NHS
Infectious Disease Incident Plan.
• The Infection Prevention and Control Team and Health Protection Team contribute to the daily Norovirus SITREPs that are communicated widely throughout NHS Grampian for the duration of the norovirus season.
• The HPT recommend that community residential establishments affected by an
outbreak of gastrointestinal illness advise a hospital admitting a symptomatic resident of the potential infection risk. The HPT seeks to reinforce this communication by also advising, wherever possible, the IPCT directly when such a patient is being admitted.
• The Health Protection Team participates in national surveillance carried out by Health
Protection Scotland
49. Norovirus in NHSG. All inpatient & hospital site departments & facilities
• The IPCT will advise via the safety brief and HAI groups that all staff members should be informed that they should notify their workplace, but not report for duty if they have unexplained vomiting and or diarrhoea until free of symptoms for at least 48 hours.
• The IPCN’s & on call Microbiologist (out with office hours) will continue to support clinical

30
teams with outbreak management & decision making • The IPCT will advise temporary suspension of therapets and other voluntary ward attendees
until any affected facility is fully operational and an outbreak declared over. This may extend to an indefinite suspension for hospitals who have a high number of closures or for all sites if seasonal averages are exceeded and control proves difficult to establish
• The IPCT will include cordless telephones within outbreak management advice when discussing environmental and equipment decontamination
• When necessary an Incident Management Team IMT)will be activated at the request of the Lead Infection Prevention & Control Doctor
• The daily situation report (SITREP) describes ward / departmental / hospital closures will include current norovirus outbreak information. This will continue to be communicated by the IPCT admin team.
• The IPCT & HPT recommend transfers to residential settings from affected wards / departments are delayed until the outbreak declared over (once the affected facility is fully operational again), unless risk assessed as safe by IPCT and HPT in exceptional circumstances.
• The IPCT will participate with national point prevalence Norovirus surveillance programme for winter illness and submit reports to Health Protection Scotland on behalf of NHSG every Tuesday (retrospectively for the previous week).
• The IPCNs will alert the organisation when the Scottish Norovirus season has started (when declared by HPS) via the daily SITREP, attendance at Acute and DGH safety briefs and via HAI groups.
• The IPCNs may attend further bed management meetings upon request, but may require prioritising outbreak management. They will contact site and capacity teams with rolling updates.
• Alternative working hours for IPCNs during the winter period are being considered but have not been approved nor finalised as at October 31st 2018.
• A seasonal overview will be provided by the IPCT for the NHSG cross system winter debrief 2018-2019 upon request
N. Planned Healthcare Capacity and Activity
Summary of Key Anticipating Demand and Prevention Actions -75% of those deemed at risk of flu and those over 65 year of age should receive a flu vaccination. -Over 50% of front line staff should receive a flu vaccination. -Campaigns to support uptake of immunisation for both staff and public is in place. -All sectors/service plans reflect the NHS Grampian Major Infectious Disease Plan and the phased response set out. -Robust communication mechanisms between HPT and ICPT
Key areas of Risk -Flu immunisation target may not be achieved due to personal choice amongst staff. -Flu immunisation target may not be achieved due to personal choice amongst individuals in target groups.

31
50. Optimising Elective Care and Delivery of the Treatment Time Guarantee
• NHS Grampian is committed to managing its elective and unscheduled capacity successfully and is obligated to meet the Treatment Time Guarantee (TTG) for patients. To manage the gap between capacity and demand NHS Grampian has a clinical prioritisation process, which places the patient in a queue by the clinician. As we are not currently in the position that we can guarantee meeting the TTG, the clinical prioritisation process is to provide risk mitigation, ensuring that the patients with the highest priority are seen first, not to address the deficit between capacity and demand. Due to the tension between planned and unscheduled care in terms of bed capacity, activity is reviewed on a daily basis.
• NHS Grampian intelligently flexes the TTG lists in the early weeks of the year to
maximise the throughput of lengthy or complex cases. This supports optimal utilisation of our theatre capacity with a minimal bed base impact.
• Individual wards can view their elective and predicted unscheduled care activity two
weeks in advance with a view to managing their demand proactively and avoiding any risk of cancelling patients at short notice. To provide further assurance on this issue NHS Grampian has developed an Elective Activity Management Standard Operating Procedure. This procedure sets out a clinically appropriate escalation process that is clear about protecting capacity for firstly cancer cases and then patients prioritised through the new process as needing urgent care.
• The management of Elective activity during Winter 2018/19 is supported by the
development of a Surgical Resilience Plan which aims to maximise elective theatre capacity, including day-case, over the winter/festive period to ensure that elective performance is not adversely affected.
• The key actions of the Surgical Resilience Plan are:
1. Daily meetings of the Surgical Division Senior Multidisciplinary team with a remit to ensure effective booking processes, management of surgical bed capacity, increases in day-case procedures, booking of any identified theatre and bed capacity for priority patients such as cancer and urgent procedures and maintain elective activity, being cognisant of bed availability across the acute hospital site. 2. An additional ward round on Fridays with a focus on planning and facilitating anticipated weekend discharges. 3. Patients will receive twice daily reviews by consultants to ensure clear discharge decisions and consideration of alternative places of care for patients. 4. Prevention of unavoidable admissions by extending the operating hours of the Surgical Assessment Clinic. 5. Increase scheduled Day of Surgery Admissions to provide increased capacity and support patient flow. 6. Establishment of a Surgical Division delayed discharge group to monitor and manage surgical patient discharge in a timely manner, eliminating unnecessary delays.
• Acute Business Continuity planning sets out the essential services to be delivered in
the context of planned care should it be necessary to activate plans.
32
51. Outpatient Clinics
• Acute and community outpatient activity will continue for most of the holiday period with
the exception of the public holidays.
52. Admission Capacity & Effective Discharge
• The Acute Sector recognises that to maximise flow and bed efficiency, the number of patients admitted the day before surgery must be minimised. Reducing the number of patients admitted the night before surgery/procedure is a focus in the Acute Sector and the Day of Surgery Admissions unit opened in August 2018 supporting this approach
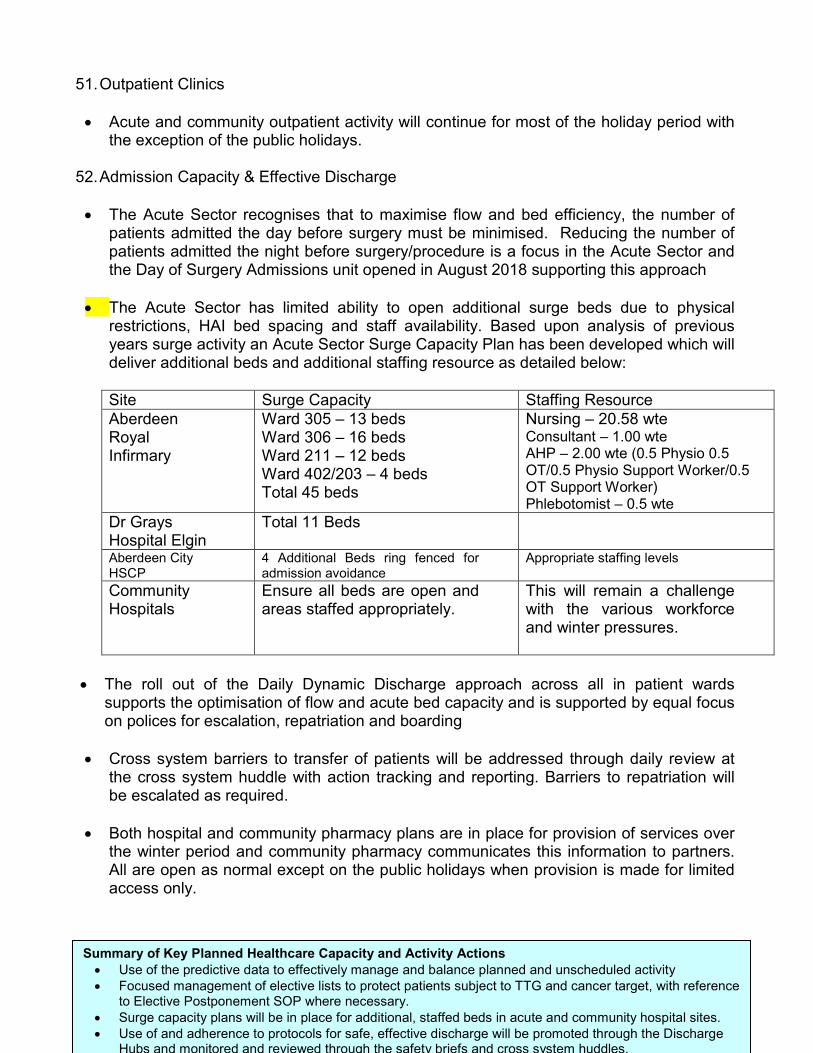
• The Acute Sector has limited ability to open additional surge beds due to physical
restrictions, HAI bed spacing and staff availability. Based upon analysis of previous years surge activity an Acute Sector Surge Capacity Plan has been developed which will deliver additional beds and additional staffing resource as detailed below:
Site Surge Capacity Staffing Resource Aberdeen Royal Infirmary
Ward 305 – 13 beds Ward 306 – 16 beds Ward 211 – 12 beds Ward 402/203 – 4 beds Total 45 beds
Nursing – 20.58 wte Consultant – 1.00 wte AHP – 2.00 wte (0.5 Physio 0.5 OT/0.5 Physio Support Worker/0.5 OT Support Worker) Phlebotomist – 0.5 wte
Dr Grays Hospital Elgin
Total 11 Beds
Aberdeen City HSCP
4 Additional Beds ring fenced for admission avoidance
Appropriate staffing levels
Community Hospitals
Ensure all beds are open and areas staffed appropriately.
This will remain a challenge with the various workforce and winter pressures.
• The roll out of the Daily Dynamic Discharge approach across all in patient wards
supports the optimisation of flow and acute bed capacity and is supported by equal focus on polices for escalation, repatriation and boarding
• Cross system barriers to transfer of patients will be addressed through daily review at
the cross system huddle with action tracking and reporting. Barriers to repatriation will be escalated as required.
• Both hospital and community pharmacy plans are in place for provision of services over
the winter period and community pharmacy communicates this information to partners. All are open as normal except on the public holidays when provision is made for limited access only.
Summary of Key Planned Healthcare Capacity and Activity Actions • Use of the predictive data to effectively manage and balance planned and unscheduled activity • Focused management of elective lists to protect patients subject to TTG and cancer target, with reference
to Elective Postponement SOP where necessary. • Surge capacity plans will be in place for additional, staffed beds in acute and community hospital sites. • Use of and adherence to protocols for safe, effective discharge will be promoted through the Discharge
Hubs and monitored and reviewed through the safety briefs and cross system huddles.

33

34
P. Unscheduled Care Capacity and Demand 53. Across the unscheduled system the overall activity seen over the winter period is slightly
higher with wider peaks and troughs of activity evident during the three weeks covering the festive period. It is also evident that the flow through the system is more challenging.
54. SAS
• The Scottish Ambulance Service continues to experience pressure on services over the winter periods. During 2017/18, the number of emergency incidents was on average 130 per day during the period November 2017 to March 2018. SAS report that this is compounded by increasing complexity and frailty in the population, staffing and recruitment challenges and longer turnaround times.
• Agreed Key actions include: • To provide adequate emergency resources for care and transport of
emergency patients by e.g. re-deploying vehicles. • Increased collaboration with acute sites including regular involvement in cross
system huddles. • Increased collaborative planning for improvement at strategic level. • Co-hosted, (HALO) Hospital Ambulance Liaison Officer, at Dr Gray’s Hospital,
Elgin. • Planned approach to supporting additional discharge at weekends and
evenings through collaborative improvement project. • Provide additional Ambulance cover at local Hogmanay events. • Increased Specialist Paramedic Cover in both Aberdeen and Elgin Stations.
55. NHS 24
• There was a slight increase in the volume of calls received per day by NHS 24 between 2016/17 and 2017/18 – an additional 33 calls per week.
• NHS 24 detailed Winter Plan is being developed and it is anticipated that it will incorporate:
• Prediction of activity with associated planning, to align workforce to times of peak demand Internal and External Communication strategies
• Consideration of previous performance and lessons learned incorporating elements identified within the detailed planning to minimise potential risk going forward
• Maximising use of call handlers, call operators and pharmacists • Maximising National Clinical and Call Handler support lines. • Contingency planning and escalation process. • Agreement with NHS Grampian Unscheduled Care Team to secure slots to send
pre-prioritised calls during key dates. • Telephony screening messages can be applied to the telephony system in a timely
manner to inform the Public of a changing situation. Through constant reappraisal of the Service Delivery Model NHS 24 have ensured that real time deployment of resource and effective utilisation of multiple skill sets aids the delivery of an efficient
35
service. 56. G-MED Out of Hours Services • GMED calls followed a very similar pattern to 2016/17, as the average number of calls was
comparable (757 calls per day in 2016/17 and 724 calls in 2017/2018). Calls per day over the Festive period were around 724 per day compared to the average 432 during the rest of the year. (Please note that these numbers include the MIU & District Nurse Consultations).
• The G-Med Out-of-Hours Service Winter Plan has been updated. The plan takes full account of:
• The need for a robust plan covering the full winter period; • The possibility of an outbreak of flu or other seasonal illness; • The possibility of adverse weather conditions; • Prioritisation of service to enhance capacity; • Above normal demands on primary care at that time of year particularly on Saturdays
and public holidays throughout the period; • The need to provide the service over the festive period.
• The Plan discusses in detail the management of demand and capacity, what the escalation
triggers are and the actions to be taken at each change of state and by whom.
• The duty rota will be finalised during November 2018.
• Contingency plans in case of a breakdown of IT and/or telephone/fax systems are described as is the escalation process and how to communicate this to the media.
• Separate communications designed with Grampian Corporate Communications will be
issued in order to support the public in preparation for the winter. 57. Emergency Department & Minor Injury Units
• Key actions to effectively manage the demand are outlined below. • Use of triage as part of initial assessment. • Implementing use of redirection protocol as part of triage at front door supported by
the Know Who To Turn To Messaging • Workforce will be deployed to cover the predictable peaks in demand. • In ARI & Dr Gray's, the Surgical Assessment Units reduce the numbers going through
A&E and therefore alleviates pressure. • Ongoing availability of Clinical Decision Support to provide support and advice to
professionals to ensure patients receive the right care, at the right time, in the right place and by the right person/team.
• Communication with public actions e.g. KWTTT, national campaigns to minimise inappropriate demand.
• Ensuring the flow across the hospital and the community is effectively maintained so patients are able to receive the right care, at the right time and in the right place.
36
58. Acute Sector
• Policies are operational with regard to escalation, boarding and discharge which ensure clarity and consistency of practice and provide a clear understanding of patient placement and bed allocation within ARI & DGH. The decision where to place a patient in terms of speciality of care is made by medical staff only: however, bed allocation can only be undertaken by the Site and Capacity Management Teams or those working on their behalf.
• Supported by the Head of Operations and in discussion with clinicians Site and Capacity
Managers will give priority status to appropriate patients in both the elective and non-elective scenarios. They will work closely with the Senior Charge Nurses, Nurse Managers and the Duty Manager who will advise the Site Manager as to the current bed state and all actions taken to improve the situation. Decisions to transfer, board or discharge patients will be supported through daily safety and flow huddles providing opportunity to highlight, discuss and escalate any barriers to flow in the sector. This will be overseen by the Head of Operations and implemented by the supporting framework for site management.
• Business Continuity Plans are in place for all Grampian hospitals.
59. Primary/Community/Social Care.
Community Pharmaceutical Services will support service delivery over the winter 2018/19 and specifically the festive period via the following:
• Pharmacy First service – treatment of uncomplicated urinary tract infections and
treatment of impetigo. • Community pharmacy provision of emergency contraception • Community Pharmacy Urinary Tract Infection (UTI) Service. • Community pharmacy will continue to provide advice and treatment via the Minor
Ailments Service. • Community Pharmacy Unscheduled Care Patient Group Directive (urgent supply
of medication). • Both hospital and community pharmacy plans are in place for provision of services
over the winter period. All are open as normal except on the public holidays when provision is made for limited access only. Exceptions to normal opening times will be notified.
• Community Pharmacy opening on public holidays will be notified to partners (G-MED, NHS 24, Substance misuse service etc) via the Primary Care Contracts Team and corporate communications. There will be some pharmacy coverage in all communities every day.
60. Key actions in Primary/Community Social Care are:
• Ensuring high risk individuals are identified within practices and up to date Anticipatory
Care Plans are in place.
37
• Accessing real-time decision support via local networks to ensure patients receive the right care in the right place at the right time. This approach will also reduce inappropriate admissions.
• Provision of a Virtual Community Ward Model across Aberdeenshire & Moray H&SCP’s • Introduction of Hospital at Home Team Model in Aberdeen City H&SCP. • Utilising the capacity within Community Hospitals to predict and effectively manage
demand for admissions and transfers. Contributing to the intelligence regarding bed capacity across Grampian.
• Community healthcare provision continues throughout winter period and business continuity plans are in place
• The main action for surge activity is to ensure all beds are open and areas staffed appropriately. This will remain a challenge with the various workforce and winter pressures.
• No additional primary care capacity has been identified; however Health & Social Partnerships will undertake work with community planning colleagues to ensure maximum use of community resources. The management of surge activity or workforce capacity issues will be managed on the basis of service prioritisation for that day.
• Increased social care provision can be commissioned during peaks throughout the winter period. Collaborative communication will make staff aware that social care provision (and on call) is available 365 days per year through.
• During times of increased pressure social care resources are allocated according to priority and, wherever possible, Partnerships will ensure that priority is given to hospital discharge or prevention of admission.
61. Cross System Challenges
• NHS Grampian, and the three Health and Social Care Partnerships all see the crucial role that delayed discharges play in the delivery of a successful winter plan as well as an optimal experience for public and staff. Partnerships are focused on reducing the number of people who are delayed within hospitals.
• Aberdeen City HSCP will vary the allocation of Interim Social care Beds to support cross
system pressures and reserve a minimum of 27 Care Home beds specifically to support discharge and improve flow out of hospital.
• Key aspects of each of the Partnerships’ winter plans coincide with the delayed
discharge plans and the use of the resource envelope across the whole system.
Summary of Key Unscheduled Care Capacity and Demand Actions - Local Winter Plans which meet predicted challenges are agreed and tested during September/October
2018. - Implementing enhanced use of redirection protocol in ED. - Site Capacity and Management Approach in acute hospitals. - Minimising delayed discharges by reducing the number prior to winter. - Surge capacity plans agreed and in place.
Key areas of Risk - Pattern of increasing demand for SAS & G Med services in the face of recruitment difficulties. - People may choose not to use self care and may present at ED inappropriately. - People may wait until closed primary care services reopen and the volume of demand at that time
maybe overwhelming.
38
R. Specific Plans for During and Post the Festive Period 62. All organisations and services within Grampian have/will have in place the following:
• Agreed rotas for the festive period in place by October 2018 which aims to match the forecasted demand.
• Business continuity plans which cover the delivery of resilient services over the festive period.
• Regular communication regarding local actions in their surge or winter plans via established channels e.g. safety briefs, cross system huddles, Senior Leadership Team huddles.
63. SAS
• As set out in the SAS Winter Plan, arrangements are in place to respond to and manage the
predicted peaks in demand, including early preparation of staffing rotas during the festive period.
64. NHS 24
• The NHS 24 Winter Plan for 2018/19 will set out how the predicted peak in service activity will be appropriately managed through adequate workforce capacity maximising the use of Call Handlers, Call Operators and Pharmacist and maximising National Clinical and Call Handler support lines. Contingency plans and escalation processes will be in place.
65. G-Med & Community Hospitals
• G-MED Winter Plan outlines the key actions for ensuring appropriate delivery of quality services which meet the demand over the winter and festive period.
66. In-Hours General Practice/Community
• GP practices will be open on the days between the public holidays. On these days some practices will embargo additional appointments for same day booking, managed via established practice of telephone triage .They have also noted that general practice is not, when fully staffed, under increased pressure at the period over Christmas and New Year but with a surge usually occurring in the first week of January and are prepared for this.
• Any significant General Practice vulnerabilities that may impact on service delivery over winter 2018/19 will be identified and escalated to senior management for action in advance of winter period.
• The three Partnerships will have community nursing cover arrangements in place for 25th
and 26th December and for 1st and 2nd of January. The Out-of-Hours nurses based in G-MED will continue as normal.
67. Social Care

39
Key actions to effectively manage demand over the festive period are:
• Reduce number of patients with a delayed discharge prior to the festive period. • Delivery of prompt assessment and implementation of social care packages over the
festive period. • Commissioning of specific dedicated care home beds to support discharge pressures over
the winter period. • Operation of the integrated discharge hub over public holidays including staffing by
Aberdeen City and Aberdeenshire H&SCP Social Workers to support discharge activity from hospitals without significant holiday period interruption.
• Work with cross system huddle and integrated discharge hub in acute sector to ensure staff are aware that social care packages are available over the festive period.
• During times of increased pressure resources are allocated according to priority and wherever possible, priority is given to hospital discharge or prevention of admission
68. Pharmacists Community Pharmacy
• A pharmacy plan for the festive season is in place. Community pharmacists offering public holiday cover will be encouraged to stagger the hours they open to give the widest possible cover to the public. During October – early December public information will be in place regarding repeat prescriptions to remind them to order their repeat prescriptions in plenty of time. Community Pharmacy opening on public holidays will be notified to partners (G-MED, NHS 24, ED Departments, Minor Injury Units Substance misuse service etc) via the Primary Care Contracts Team and corporate communications. There will be some pharmacy coverage over all HSCP areas every day.
Hospital Pharmacy
• There will be adequate pharmacy cover for hospital wards with emergency only on 25th December and 1st January, weekend level of service on 22nd/23rd/ 29th/30thDecember and 5th/ 6th January, and 8.30 am – 5.00 pm cover on 26th December and 2nd January. All other days during the festive period will operate as normal. Ordering pharmacy supplies for emergency out-of-hours centres and community hospitals will be planned well in advance taking account of transport arrangements and ensuring adequate medicine stock. Within the acute sector, pharmacy distribution and dispensary opening information will be provided directly to wards and clinics. It is essential that pharmacy staff are included in plans for patient discharge at the earliest time to ensure required medication is available in a timely manner.
• The above arrangements will be widely publicised to the public and NHS staff
69. Dental Services
During the festive period the following arrangements will be in place:
• Excluding public holidays, Public Dental Services and independent dental practices will be expected to provide access to dental advice and treatment between 08:00 – 18.00hrs Monday to Friday.

40
• During in-hours 08.00 – 18.00, unregistered patients and visitors to the region can access dental advice and treatment if required, by contacting the Dental Information and Advice Line (DIAL) on 0345 45 65 990.
• Out of hours will be available as below: Aberdeen GDENS emergency dental clinics operate 18.15-21.15 on Fridays, 09.00-12.30 and 13.00-16.00 on Saturdays and 09.00-12.30 on Sundays. Elgin clinic operates on Sundays 09.00-12.30. Public holiday cover is scheduled for: Sat 22nd Dec Aberdeen clinic 09.00-12.30 13.00-16.00 Sun 23rd Dec Aberdeen clinic 09.00-12.30 Elgin clinic 09.00-12.30 Tue25th Dec Aberdeen clinic 09.00-12.30
Elgin clinic 09.00-12.30 Wed 26th Dec Aberdeen clinic 09.00-12.30 Elgin clinic 09.00-12.30 Sat 29th Dec Aberdeen clinic 09.00-12.30 13.00-16.00 Sun 30th Dec Aberdeen clinic 09.00-12.30 Elgin clinic 09.00-12.30 Tue 1st Jan Aberdeen clinic 09.00-12.30
Elgin clinic 09.00-12.30 Wed 2nd Jan Aberdeen clinic 09.00-12.30 Elgin clinic 09.00-12.30 For unregistered dental patients and patients of practices participating in the SEDS national service, out of hours and public holiday services are accessed via NHS 24 on 111 between 18.00 – 08.00 weekdays and throughout the weekend and public holidays. Patients will be triaged according to national Emergency Dental Service standards and directed to appropriate care as required, with an agreed escalation policy for emergency dental cases in place. Registered dental patients should contact their practice directly in the first instance.
70. Diagnostics
• Elective activity will be managed in accordance with unscheduled care need and available capacity. Detailed planning of activity levels for ultrasound, CT and MRI will be in place after the end of October 2018 and will help to ensure that no elective activity will be postponed as a result of pressures on the diagnostics service.
71. ED/MIUs
• Intelligence shows us that the week prior to Christmas and the first two weeks in January ED and MIU departments tend to be significantly busier than usual. Key actions to manage this are outlined in paragraph 59 with specific emphasis in ensuring workforce capacity is in place to manage predicted demand.

41
72. Mental Health Services
• Intelligence demonstrates that there are surges in demand on mental health services prior to and post the festive period. The unscheduled care team work 365 days per year and will absorb this as part of their work pattern. On call consultants are available to attend the hospital if activity increases.
73. Modelling and Testing
Aberdeen City HSCP 31st August Acute Sector ARI 17th October Aberdeenshire HSCP 12th October Moray HSCP & Dr Gray’s 20th September Cross System/sector 28th September
• Surge planning is closely linked to the degree of preparedness that will be in place for
likely challenges over winter. Preparation for, and integral to surge planning, is an understanding of what capacity the current system has, what levels or thresholds will challenge that capacity beyond manageable levels and what ability and resources can be put in place to step up to a ‘surge’ response.
• From experience of participating in tabletop tests in previous years, all stakeholders
recognise the value in exercising winter plans ahead of finalisation and implementation. Based on this value, the sectors have tested their plans, using tabletop exercises and supported by Grampian’s Unscheduled Care 6 Essential Actions Programme Manager, which have afforded the opportunity to identify barriers and flaws to implementing the plans and a chance to refine them, in sufficient time to address any issues that will prevent successful activation.
• A joint Cross Sector Winter Tabletop Test exercise for all stakeholders and partners and
supported by Grampian USC 6 Essential Actions Programme Manager has also been held to test winter planning and collaborative working.
Themes explored and tested were:
• The potential activation of four winter plans and the initial response to a disruptive event that has a direct impact on patient care.
• The joint approach that is in place across all the organisations and how the plans dovetail together; how risk is assessed across the board and how Command and Control functions across the joint approach.
• How the sectors and others will continue to deliver services and maintain performance against key measures and standards during a period of significant challenge.
In each case, the exercise process followed national resilience protocol and utilised standardised documentation, enabling a consistent method for review and feedback, as well as ensuring quality control.
42
References Scottish Government: 6 Essential Actions Improvement Programme.
Summary of Key Festive Period Actions - All organisations and services will have in place the following
• Agreed rotas for the festive period by 31st October 2018. • Locally tested business continuity plans. • Clear communication channels for discussing pressures and agreeing key actions.
- There is an established partnership approach to festive period planning, acknowledging interdependencies of services.
- Rostering of Aberdeen City and Aberdeenshire H&SCP Social Workers at ARI during the public holiday festive periods.
- Focus is business continuity and minimising the impact of any closures. - Testing of Sector and Cross Sector Winter Plans has contributed to the efficacy of continuity planning
Key areas of Risk - Certain staff rotas, over the Festive Period may not be optimal and compounded by staff vacancies - Higher than predicted unscheduled care activity.

43
Scottish Government Cabinet Secretary for Health and Sport: • Preparing for Winter 2018/19 • Winter Preparedness : Self Assessment
Scottish Government Health Workforce, Leadership & Service Transformation Directorate:
• Draft Winter Plans 2018-19
Grampian Health and Social Care: Local Review of Winter Report 2017/18 Grampian Winter Trends Intelligence Report 2017/18 The NHS Grampian Major Infectious Disease Plan version 5.3. Approved October 2013. Sector/Organisation Winter Plans which underpin the Grampian Winter Plan 2018/19 Acute Sector Winter Plan (ARI and Dr Grays) for 2018/19 Aberdeenshire Health & Social Care Winter Plan for 2018/19 Aberdeen City Health & Social Care Surge, Capacity Planning and Festive Preparedness Plan for 2018/19 Moray Health & Social Care Winter Plan for 2018/19 Scottish Ambulance Service Winter Plan for 2018/19 NHS24 Winter Plan for 2018/19

44
Appendix 1
Summary of Winter Plan Actions & Finance Status for 2018/19
The table below sets out the key actions within this plan along with the nominated lead, timescales for delivery and financial status.
Ref. Action Timescales Lead/s Financial Cost/Status
1. Reporting
Reporting to the Scottish Government in a timely manner by: i. Submitting weekly management information
commencing October 2018 ii. Producing daily performance and pressures reports
as and when required iii. Providing exception reports and immediate
notification of any significant issues.
Oct 2018 As required As required
V. Fox V. Fox F Francey
Via existing resources. Via existing resources. Via existing resources.
2. Communication Between Partners & Escalation
i. Partnerships, Acute sector and other Departments along with Partners to test winter/business continuity plans.
ii. Daily Cross System Huddles Chaired by Senior Decision Maker and include all partners to be held
iii. Real-time reporting of critical incidents to partners as per agreed protocols
iv. All partners contribute to/inform the submission of exception reports to the Scottish Government
During August/September/October 2018 Ongoing Ongoing Ongoing
Chief Officers, General and Lead Managers Fiona Francey, Sandra Ross, Pam Gowans & Adam Coldwells Fiona Francey, Sandra Ross, Pam Gowans & Adam Coldwells Fiona Francey, Sandra Ross, Pam Gowans & Adam Coldwells
Via existing resources.
3. Communicating to Public/Staff
i. Implementation and regular review of the Winter Health Communication Plan which includes flu, ‘Be Ready for Winter’, KWTTT and antibiotic campaigns.
ii. Targeted communication to staff on wards regarding key information during the festive period e.g. infection control advice, access to social care assessment/care packages and KWTTT
iii. Targeted KWTTT public campaign
From October 2018 From November 2018 From Nov 2018
K Livock V. Sandison K.Livock
Via existing resources Via existing resources 6 Essential Actions Funding

45
Ref. Action Timescales Lead/s Financial Cost/Status
4. Joint Working and Integration
i. Regular meetings involving Partnerships, Acute Sector and NHS Grampian to prioritise system issues
ii. Discharge Hub to support integrated approach to priority discharge
iii. Maintaining the agreed pathway of care for elderly patients to ensure appropriate individuals, who require urgent geriatric assessment, receive this at the earliest opportunity when they present via ED or decision support.
Weekly Daily In place / ongoing
Senior Leadership Team A. Hardy P. Bachoo
Via existing resources Via existing resources Via existing resources
5. Anticipatory Demand and Prevention
i. To facilitate managing patents at home ii. Encouraging and promoting flu vaccination for all
individuals over 65 years, all patients in at risk groups under 65 years in a clinical risk group, to achieve a 75% uptake rate
iii. Promoting flu vaccination for all staff and aim to achieve a 50% uptake of front line staff
iv. All sector/service plans reflect details within the NHS Grampian Major Infectious Disease Plan
v. Robust communication mechanisms between Health Protection Team and Infection Prevention and Control Team
Ongoing From October 2018 From October 2018 October 2018 Ongoing
HSCPs S. Webb Fiona Francey, Sandra Ross, Pam Gowans & Adam Coldwells
S. Webb
Via existing resources Via existing resources Via existing resources Via existing resources Via existing resources
6. Planned Healthcare Capacity and Activity
i. Use of predictive data to effectively manage and balance planned and unscheduled activity
ii. Realistic Surge Capacity plans are in place for additional staffed beds in acute and community hospital sites
iii. Use of and adherence to protocols for safe, effective discharge will be promoted through the Discharge Hubs and monitored and reviewed through the safety briefs and cross system huddles
Ongoing September 2017 Monthly
F. Francey Fiona Francey, Sandra Ross, Pam Gowans & Adam Coldwells
A Hardy
Via existing resources Via existing resources Via existing resources

46
Ref. Action Timescales Lead/s Financial Cost/Status
7. Unscheduled Care Capacity and Demand
i. Robust Winter Plans, which reflect predicted demand, are agreed and tested
ii. Minimising delayed discharges by reducing the number prior to winter
iii. Surge capacity plans agreed and in place iv. Rotas, across the local health and social care
system, are in place and are focussed on meeting predicted demand
v. Information and communication regarding the availability of assessment and care packages
vi. Access to infection control and prevention advice
August – October 2018 August – October 2018 October 2018 Early November 2018 November 2018 November 2018
Fiona Francey, Sandra Ross, Pam Gowans , Adam Coldwells & Directorate Leads Sandra Ross, Pam Gowans & Adam Coldwells Fiona Francey, Sandra Ross, Pam Gowans & Adam Coldwells Fiona Francey, Sandra Ross, Pam Gowans & Adam Coldwells Sandra Ross, Pam Gowans & Adam Coldwells
L Bruce
Via existing resources Via existing resources Via existing resources Via existing resources Via existing resources Via existing resources
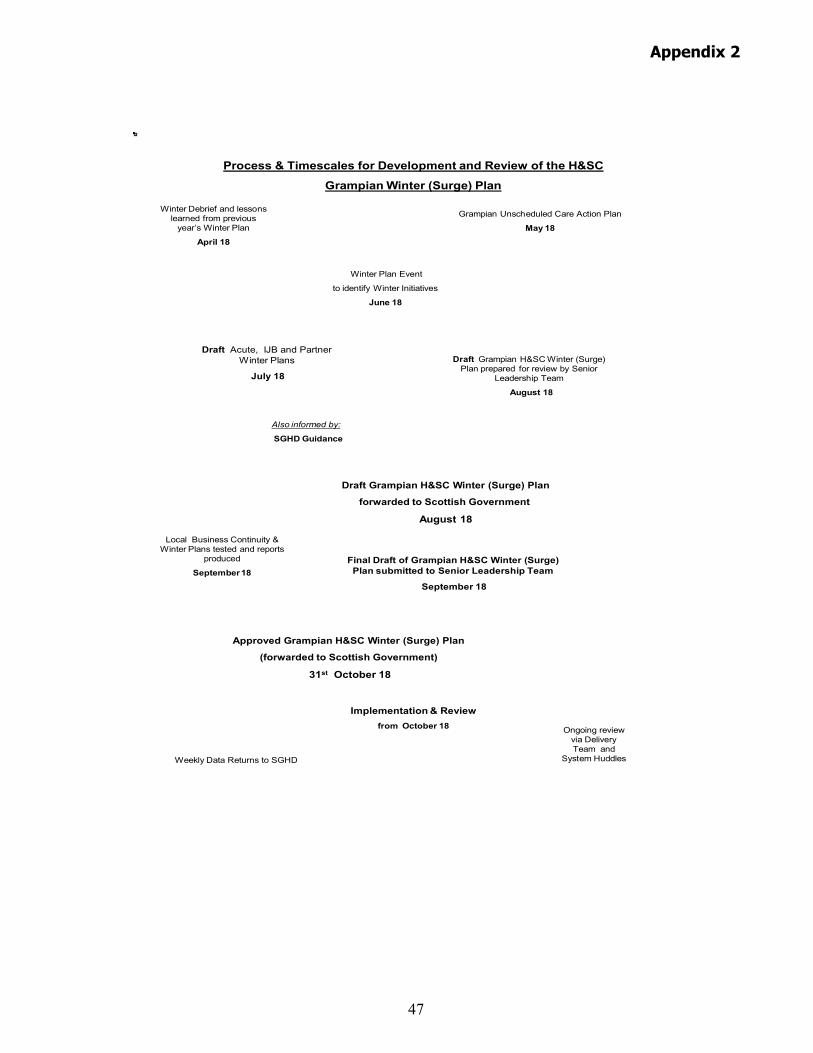
47
Process & Timescales for Development and Review of the H&SC
Grampian Winter (Surge) Plan
Grampian Unscheduled Care Action Plan
May 18
Draft Grampian H&SC Winter (Surge) Plan prepared for review by Senior
Leadership Team
August 18
Also informed by:
SGHD Guidance
Local Business Continuity & Winter Plans tested and reports
produced
September 18
Implementation & Reviewfrom October 18 Ongoing review
via Delivery Team and
System HuddlesWeekly Data Returns to SGHD
Winter Debrief and lessons learned from previous
year’s Winter Plan
April 18
Winter Plan Event
to identify Winter Initiatives
June 18
Draft Grampian H&SC Winter (Surge) Plan
forwarded to Scottish Government
August 18
Draft Acute, IJB and Partner Winter Plans
July 18
Approved Grampian H&SC Winter (Surge) Plan
(forwarded to Scottish Government)
31st October 18
Final Draft of Grampian H&SC Winter (Surge) Plan submitted to Senior Leadership Team
September 18
Appendix 2
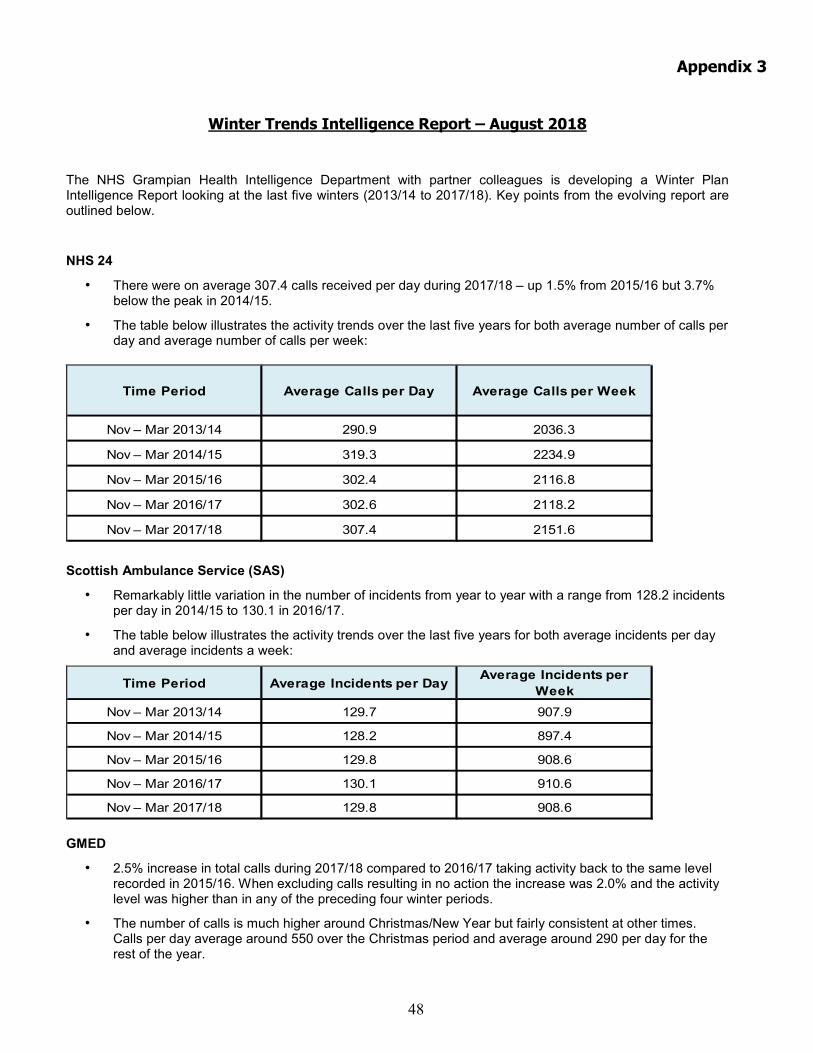
48
Appendix 3
Winter Trends Intelligence Report – August 2018
The NHS Grampian Health Intelligence Department with partner colleagues is developing a Winter Plan Intelligence Report looking at the last five winters (2013/14 to 2017/18). Key points from the evolving report are outlined below.
NHS 24
• There were on average 307.4 calls received per day during 2017/18 – up 1.5% from 2015/16 but 3.7% below the peak in 2014/15.
• The table below illustrates the activity trends over the last five years for both average number of calls per day and average number of calls per week:
Time Period Average Calls per Day Average Calls per Week
Nov – Mar 2013/14 290.9 2036.3
Nov – Mar 2014/15 319.3 2234.9
Nov – Mar 2015/16 302.4 2116.8
Nov – Mar 2016/17 302.6 2118.2
Nov – Mar 2017/18 307.4 2151.6
Scottish Ambulance Service (SAS)
• Remarkably little variation in the number of incidents from year to year with a range from 128.2 incidents per day in 2014/15 to 130.1 in 2016/17.
• The table below illustrates the activity trends over the last five years for both average incidents per day and average incidents a week:
Time Period Average Incidents per Day Average Incidents per Week
Nov – Mar 2013/14 129.7 907.9
Nov – Mar 2014/15 128.2 897.4
Nov – Mar 2015/16 129.8 908.6
Nov – Mar 2016/17 130.1 910.6
Nov – Mar 2017/18 129.8 908.6 GMED
• 2.5% increase in total calls during 2017/18 compared to 2016/17 taking activity back to the same level recorded in 2015/16. When excluding calls resulting in no action the increase was 2.0% and the activity level was higher than in any of the preceding four winter periods.
• The number of calls is much higher around Christmas/New Year but fairly consistent at other times. Calls per day average around 550 over the Christmas period and average around 290 per day for the rest of the year.
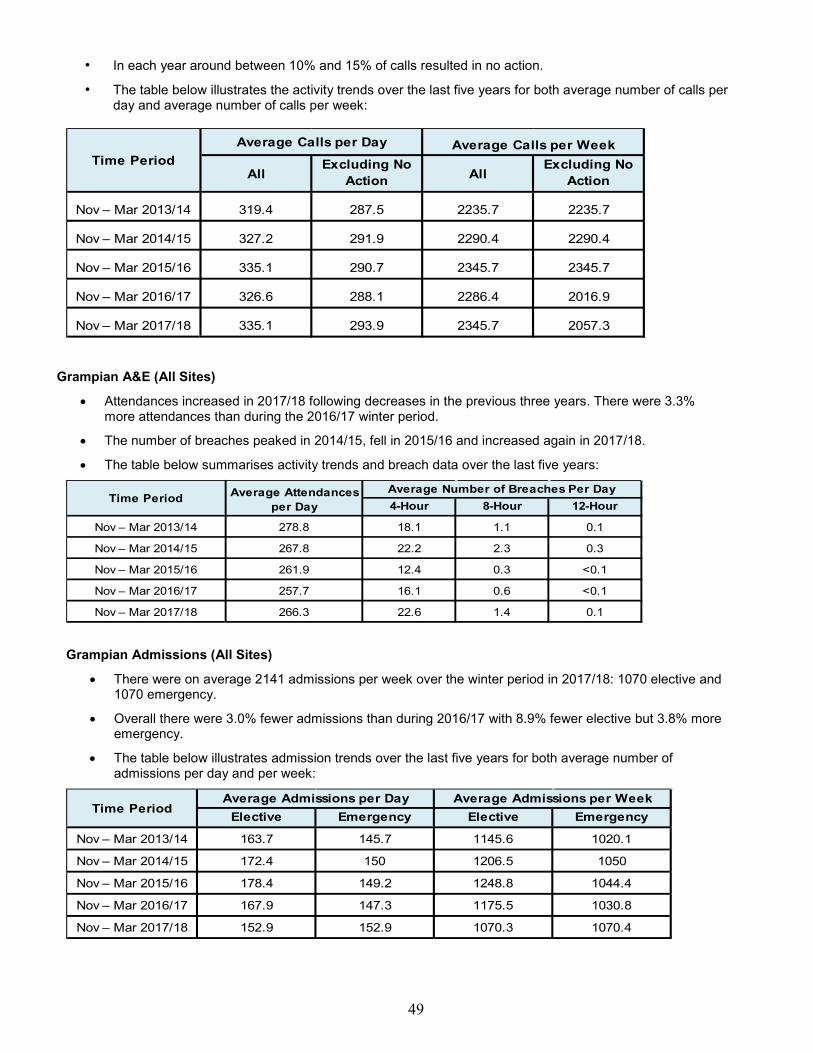
49
• In each year around between 10% and 15% of calls resulted in no action.
• The table below illustrates the activity trends over the last five years for both average number of calls per day and average number of calls per week:
AllExcluding No
Action AllExcluding No
Action
Nov – Mar 2013/14 319.4 287.5 2235.7 2235.7
Nov – Mar 2014/15 327.2 291.9 2290.4 2290.4
Nov – Mar 2015/16 335.1 290.7 2345.7 2345.7
Nov – Mar 2016/17 326.6 288.1 2286.4 2016.9
Nov – Mar 2017/18 335.1 293.9 2345.7 2057.3
Average Calls per WeekAverage Calls per DayTime Period
Grampian A&E (All Sites)
• Attendances increased in 2017/18 following decreases in the previous three years. There were 3.3% more attendances than during the 2016/17 winter period.
• The number of breaches peaked in 2014/15, fell in 2015/16 and increased again in 2017/18.
• The table below summarises activity trends and breach data over the last five years:
4-Hour 8-Hour 12-Hour
Nov – Mar 2013/14 278.8 18.1 1.1 0.1
Nov – Mar 2014/15 267.8 22.2 2.3 0.3
Nov – Mar 2015/16 261.9 12.4 0.3 <0.1
Nov – Mar 2016/17 257.7 16.1 0.6 <0.1
Nov – Mar 2017/18 266.3 22.6 1.4 0.1
Average Number of Breaches Per DayTime Period Average Attendances
per Day
Grampian Admissions (All Sites)
• There were on average 2141 admissions per week over the winter period in 2017/18: 1070 elective and 1070 emergency.
• Overall there were 3.0% fewer admissions than during 2016/17 with 8.9% fewer elective but 3.8% more emergency.
• The table below illustrates admission trends over the last five years for both average number of admissions per day and per week:
Elective Emergency Elective Emergency
Nov – Mar 2013/14 163.7 145.7 1145.6 1020.1
Nov – Mar 2014/15 172.4 150 1206.5 1050
Nov – Mar 2015/16 178.4 149.2 1248.8 1044.4
Nov – Mar 2016/17 167.9 147.3 1175.5 1030.8
Nov – Mar 2017/18 152.9 152.9 1070.3 1070.4
Time PeriodAverage Admissions per Day Average Admissions per Week
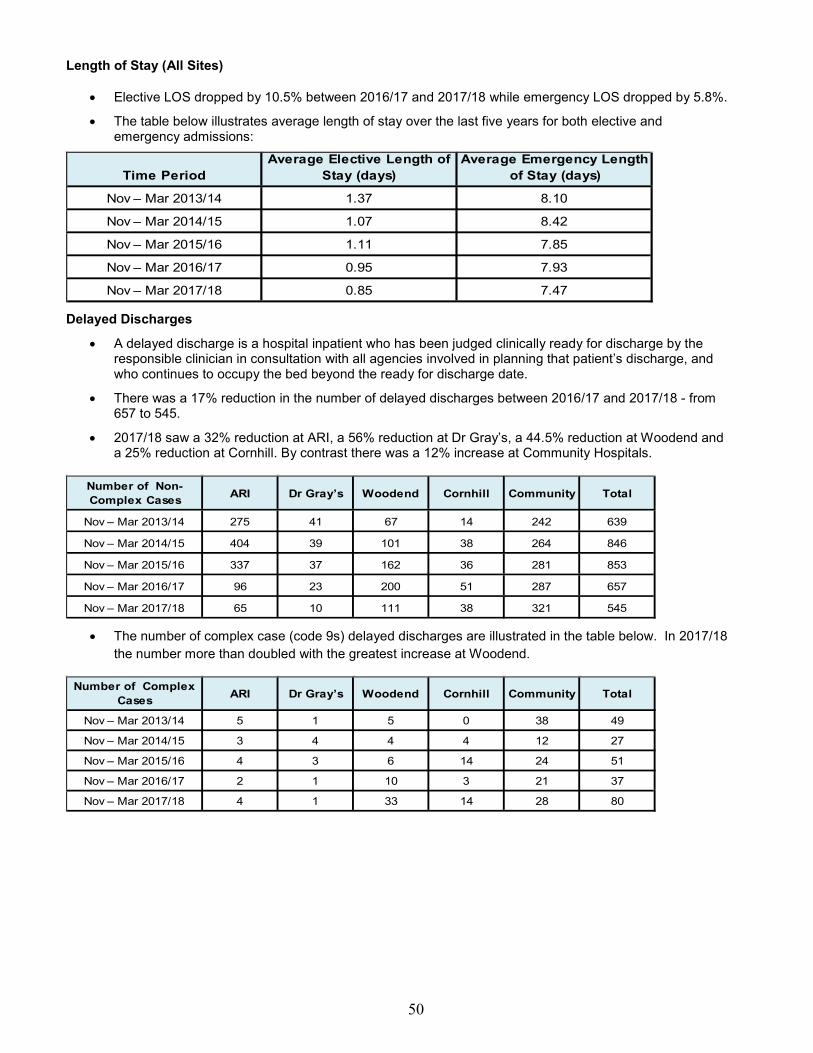
50
Length of Stay (All Sites)
• Elective LOS dropped by 10.5% between 2016/17 and 2017/18 while emergency LOS dropped by 5.8%.
• The table below illustrates average length of stay over the last five years for both elective and emergency admissions:
Time PeriodAverage Elective Length of
Stay (days)Average Emergency Length
of Stay (days)
Nov – Mar 2013/14 1.37 8.10
Nov – Mar 2014/15 1.07 8.42
Nov – Mar 2015/16 1.11 7.85
Nov – Mar 2016/17 0.95 7.93
Nov – Mar 2017/18 0.85 7.47 Delayed Discharges
• A delayed discharge is a hospital inpatient who has been judged clinically ready for discharge by the responsible clinician in consultation with all agencies involved in planning that patient’s discharge, and who continues to occupy the bed beyond the ready for discharge date.
• There was a 17% reduction in the number of delayed discharges between 2016/17 and 2017/18 - from 657 to 545.
• 2017/18 saw a 32% reduction at ARI, a 56% reduction at Dr Gray’s, a 44.5% reduction at Woodend and a 25% reduction at Cornhill. By contrast there was a 12% increase at Community Hospitals.
Number of Non-Complex Cases ARI Dr Gray’s Woodend Cornhill Community Total
Nov – Mar 2013/14 275 41 67 14 242 639
Nov – Mar 2014/15 404 39 101 38 264 846
Nov – Mar 2015/16 337 37 162 36 281 853
Nov – Mar 2016/17 96 23 200 51 287 657
Nov – Mar 2017/18 65 10 111 38 321 545 • The number of complex case (code 9s) delayed discharges are illustrated in the table below. In 2017/18
the number more than doubled with the greatest increase at Woodend.
Number of Complex Cases ARI Dr Gray’s Woodend Cornhill Community Total
Nov – Mar 2013/14 5 1 5 0 38 49
Nov – Mar 2014/15 3 4 4 4 12 27
Nov – Mar 2015/16 4 3 6 14 24 51
Nov – Mar 2016/17 2 1 10 3 21 37
Nov – Mar 2017/18 4 1 33 14 28 80
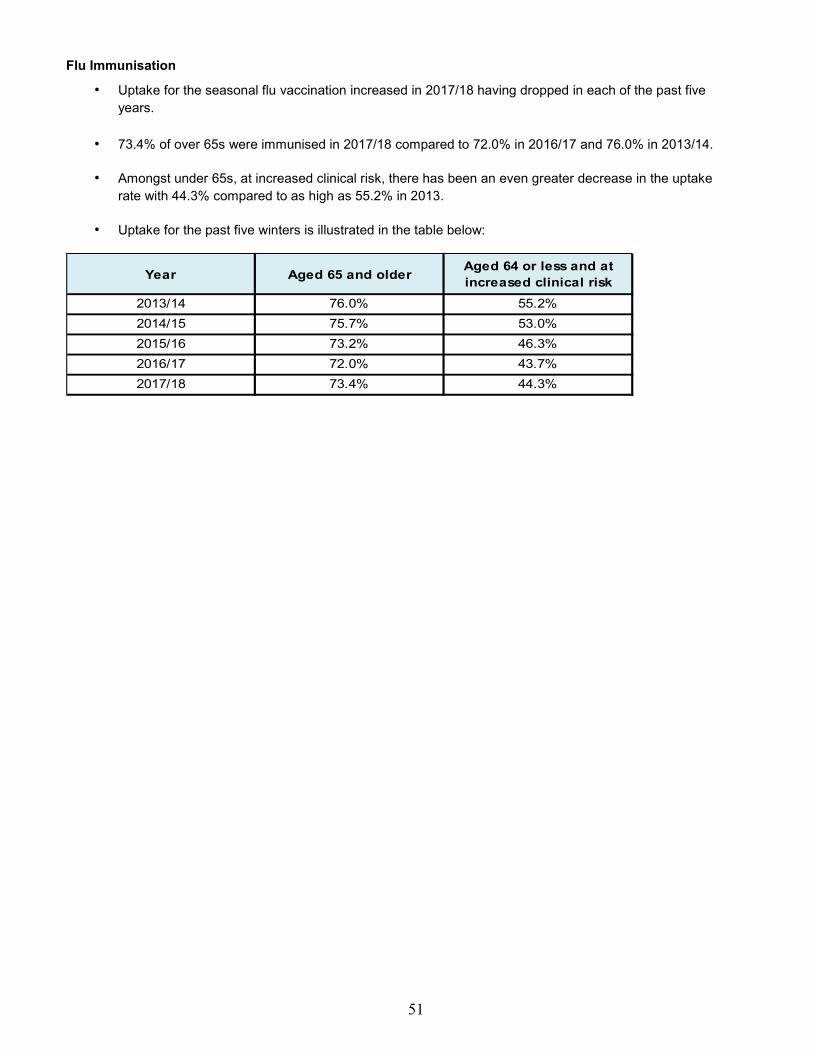
51
Flu Immunisation
• Uptake for the seasonal flu vaccination increased in 2017/18 having dropped in each of the past five years.
• 73.4% of over 65s were immunised in 2017/18 compared to 72.0% in 2016/17 and 76.0% in 2013/14.
• Amongst under 65s, at increased clinical risk, there has been an even greater decrease in the uptake rate with 44.3% compared to as high as 55.2% in 2013.
• Uptake for the past five winters is illustrated in the table below:
Year Aged 65 and older Aged 64 or less and at increased clinical risk
2013/14 76.0% 55.2%2014/15 75.7% 53.0%2015/16 73.2% 46.3%2016/17 72.0% 43.7%2017/18 73.4% 44.3%

52
Preparing For Winter 2018-19 Appendix 4 Purpose of this Supplement In accordance with Cabinet Secretary Letter (31 August 2018) the following supplementary information is provided to offer assurance of the ongoing planning processes across the NHS Grampian acute sector and Health and Social Care Partnerships, led by the Grampian Senior Leadership Team which incorporates senior leadership from each organisation. There is further assurance that Nick Fluck, Medical Director and Caroline Hiscox, Nurse Director will provide an immediate, high-level leadership steer to practitioner staff in all sectors, with consistent support and performance management across the Senior Leadership Team. This will incorporate weekly monitoring of the existing winter performance indicators as well as the agreed discharge trajectories for earlier and weekend discharges. Background In Grampian we operate a robust annual planning process with regard to the known challenges of the winter period from November to March and a key output is the Grampian Winter (Surge) Plan. The Plan is an overarching document for the three Health and Social Care Partnerships and the Acute Sector of Grampian. It is representative of local Winter Plans of each of these areas and is coordinated by NHS Grampian. Our local planning process is in part informed by national guidance from the Scottish Government and a recent letter from the Cabinet Secretary (31 August 2018) highlighted some key priorities that are required to be evidenced within the Final Grampian Winter (Surge) Plan due for submission on 2 November 2018. Further Winter Planning as of September 2018 The following table summarises the issues that are required to be evidenced or included in the Final Grampian Winter (Surge) Plan 2018/19, due for submission nationally by 31 October 2018; there is special dispensation for Grampian to submit by 2 November 2018 to allow time for NHS Grampian Board approval. It should also be noted that the national tool ‘Supplementary Checklist of Winter Preparedness: Self Assessment’ has also been completed for the acute sector and for Grampian overall, offering an assurance that the priorities noted in the appendix to the Cabinet Secretary’s letter are also addressed within the Grampian Winter (Surge) Plan Issue requiring Assurance Assurance of Inclusion in Winter Plan Agreed trajectory for weekend
discharges
Discussed by cross system representatives and attached as
Appendix 1
Agreed trajectory for discharges
earlier in the day
Discussed by cross system representatives as 5%
improvement for discharges by 2pm and 10% improvement
for discharges by 4pm.Attached as Appendix 2
Assurance of adequate festive staffing
cover
Discussed by cross system representatives and attached as
Appendix 3

53
Demand and capacity predictions
based on data sourced from System
Watch
Predictive data used routinely in NHS Grampian can be
from multiple sources to ensure optimum reliability;
however predictions based solely on System Watch have
been produced. In particular data for Respiratory,
Cardiology and Care of the Elderly has been developed to
support management of these key flows.
Available by site, by specialty, by day, by week
Agreement with local authorities
regarding gritting and other winter
related priorities
Discussed with cross system representatives and assurance
will be provided by each sector in final Plan.
Final submission of Plan will be
accompanied by a joint cover letter
confirming final approval
Joint cover letter will be approved by NHSG Chief
Executive, HSCP Chief Officers and Chairs.
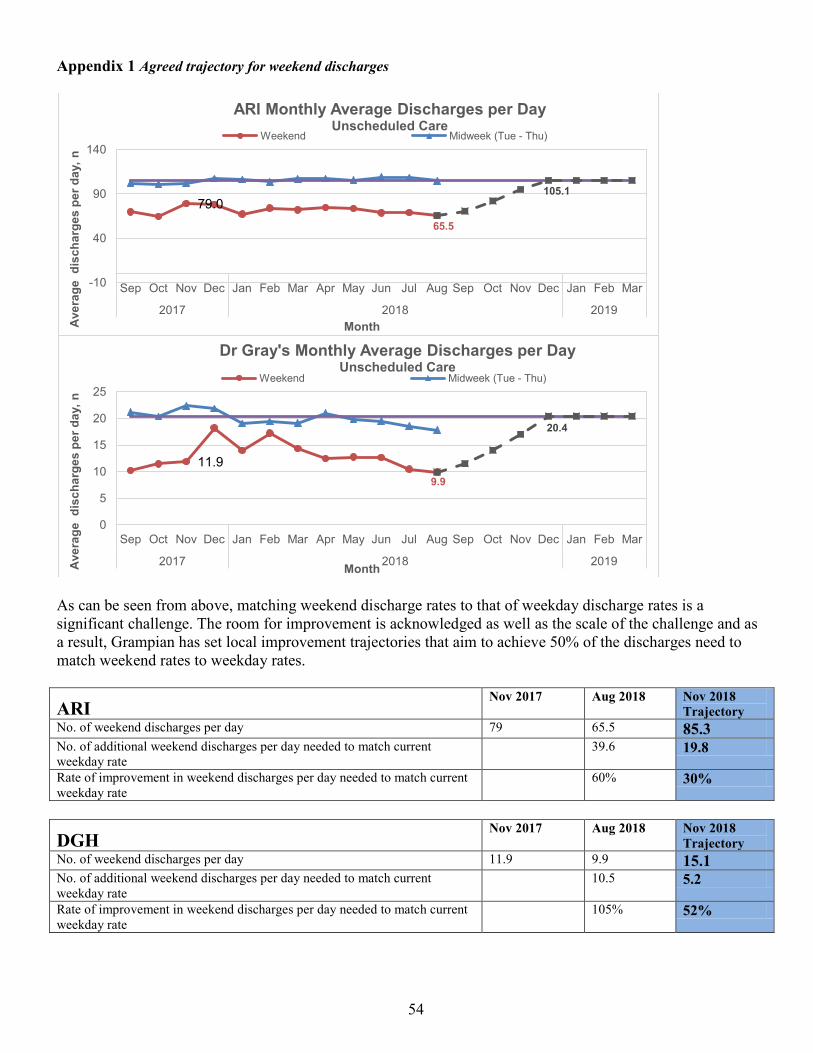
54
Appendix 1 Agreed trajectory for weekend discharges
As can be seen from above, matching weekend discharge rates to that of weekday discharge rates is a significant challenge. The room for improvement is acknowledged as well as the scale of the challenge and as a result, Grampian has set local improvement trajectories that aim to achieve 50% of the discharges need to match weekend rates to weekday rates.
ARI Nov 2017 Aug 2018 Nov 2018
Trajectory No. of weekend discharges per day 79 65.5 85.3 No. of additional weekend discharges per day needed to match current weekday rate
39.6 19.8
Rate of improvement in weekend discharges per day needed to match current weekday rate
60% 30%
DGH Nov 2017 Aug 2018 Nov 2018
Trajectory No. of weekend discharges per day 11.9 9.9 15.1 No. of additional weekend discharges per day needed to match current weekday rate
10.5 5.2
Rate of improvement in weekend discharges per day needed to match current weekday rate
105% 52%
79.0 65.5
105.1
-10
40
90
140
Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2017 2018 2019
Ave
rage
dis
char
ges
per d
ay, n
Month
ARI Monthly Average Discharges per Day Unscheduled Care
Weekend Midweek (Tue - Thu)
11.9 9.9
20.4
0
5
10
15
20
25
Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2017 2018 2019 Ave
rage
dis
char
ges
per d
ay, n
Month
Dr Gray's Monthly Average Discharges per Day Unscheduled Care
Weekend Midweek (Tue - Thu)
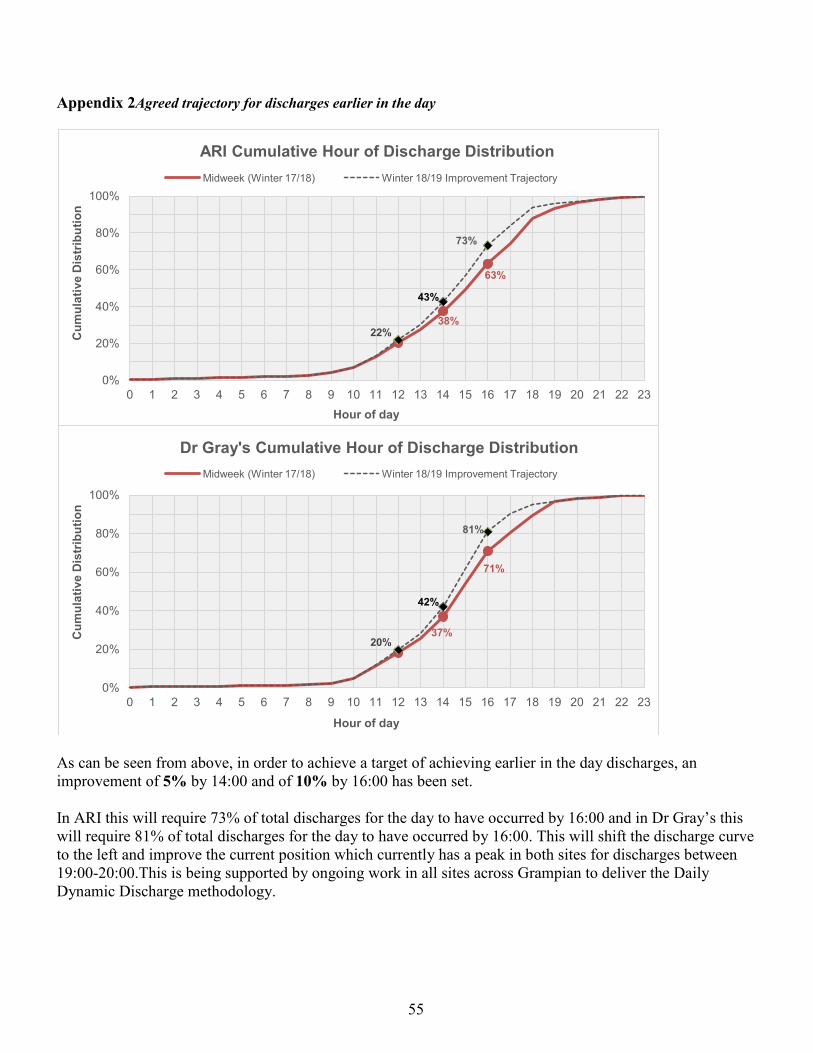
55
Appendix 2Agreed trajectory for discharges earlier in the day
As can be seen from above, in order to achieve a target of achieving earlier in the day discharges, an improvement of 5% by 14:00 and of 10% by 16:00 has been set. In ARI this will require 73% of total discharges for the day to have occurred by 16:00 and in Dr Gray’s this will require 81% of total discharges for the day to have occurred by 16:00. This will shift the discharge curve to the left and improve the current position which currently has a peak in both sites for discharges between 19:00-20:00.This is being supported by ongoing work in all sites across Grampian to deliver the Daily Dynamic Discharge methodology.
38%
63%
22%
43%
73%
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Cum
ulat
ive
Dis
trib
utio
n
Hour of day
ARI Cumulative Hour of Discharge Distribution Midweek (Winter 17/18) Winter 18/19 Improvement Trajectory
37%
71%
20%
42%
81%
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Cum
ulat
ive
Dis
trib
utio
n
Hour of day
Dr Gray's Cumulative Hour of Discharge Distribution Midweek (Winter 17/18) Winter 18/19 Improvement Trajectory

56
Appendix 3 Assurance of staffing cover for weekends and holidays Sector Assurance of adequate festive staffing cover Acute • Confirmation that the Monday following the festive weekend breaks is not routinely used as a
day off. • Participation in the Cross System Huddle on Public Holidays • Cross system use of the Discharge Hub which is open on weekends and Public Holidays • All consultant ward rounds to continue across 7 days • Site and capacity team to continue across 7 days • Management support team in place and on call 24/7 with escalation • Consultant, FY2, Pharmacy, Nursing (inc. agency)Phlebotomy, Portering staffing levels
checked for Pubic Holiday cover
Aberdeen City • Confirmation that the Monday following the festive weekend breaks is not routinely used as a day off.
• Participation in the Cross System Huddle on Public Holidays • Cross system use of the Discharge Hub which is open on weekends and Public Holidays • Social Work staff operating in the Discharge Hub on Public Holidays
Aberdeenshire • Confirmation that the Monday following the festive weekend breaks is not routinely used as a day off.
• Participation in the Cross System Huddle on Public Holidays • Cross system use of the Discharge Hub which is open on weekends and Public Holidays • Homecare responders (ARCH) will liaise with the Discharge Hub on Public Holidays to put in
place care and facilitate discharge • enhanced number of homecare responder coordinators to deal with increased demand and pull
people out of hospital
Moray • Confirmation that the Monday following the festive weekend breaks is not routinely used as a day off.
• Participation in the Cross System Huddle on Public Holidays • Cross system use of the Discharge Hub which is open on weekends and Public Holidays • Social Work staff operational on Public Holidays • Dr Grays huddle to increase in frequency to facilitate discharges/transfers • Community Hospitals Flow facilitator operational on Pubic Holidays • Management support team on call with escalation
57
Appendix 5
Preparing for Winter 2018/19: Supplementary Checklist of Winter Preparedness: Grampian Self-Assessment
This checklist supports the strategic priorities for improvement identified by local systems from their review of last winter and includes other areas of relevance. This list is not exhaustive and local systems should carefully consider where additional resources might be required to meet locally identified risks that might impact on service delivery. NHS Special Boards should support local health and social care systems to develop their winter plans as appropriate.
Priorities 1. Resilience
2. Unscheduled / Elective Care
3. Out of Hours
4. Norovirus
5. Seasonal Flu
6. Respiratory Pathway
7. Key Partners / Services

58
Winter Preparedness: Self-Assessment Guidance
• Local governance groups can use these checklists to self-assess the quality of overall winter preparations and to identify where further action may be required.
• There is no requirement for these checklists to be submitted to the Scottish Government.
• The following RAG status definitions are offered as a guide to help you evaluate the status of your overall winter preparedness.
RAG Status Definition Action Required Green Systems / Processes fully in place & tested where appropriate.
Routine Monitoring
Amber Systems / Processes are in development and will be fully in place by the end of October.
Active Monitoring & Review
Red Systems/Processes are not in place and there is no development plan.
Urgent Action Required
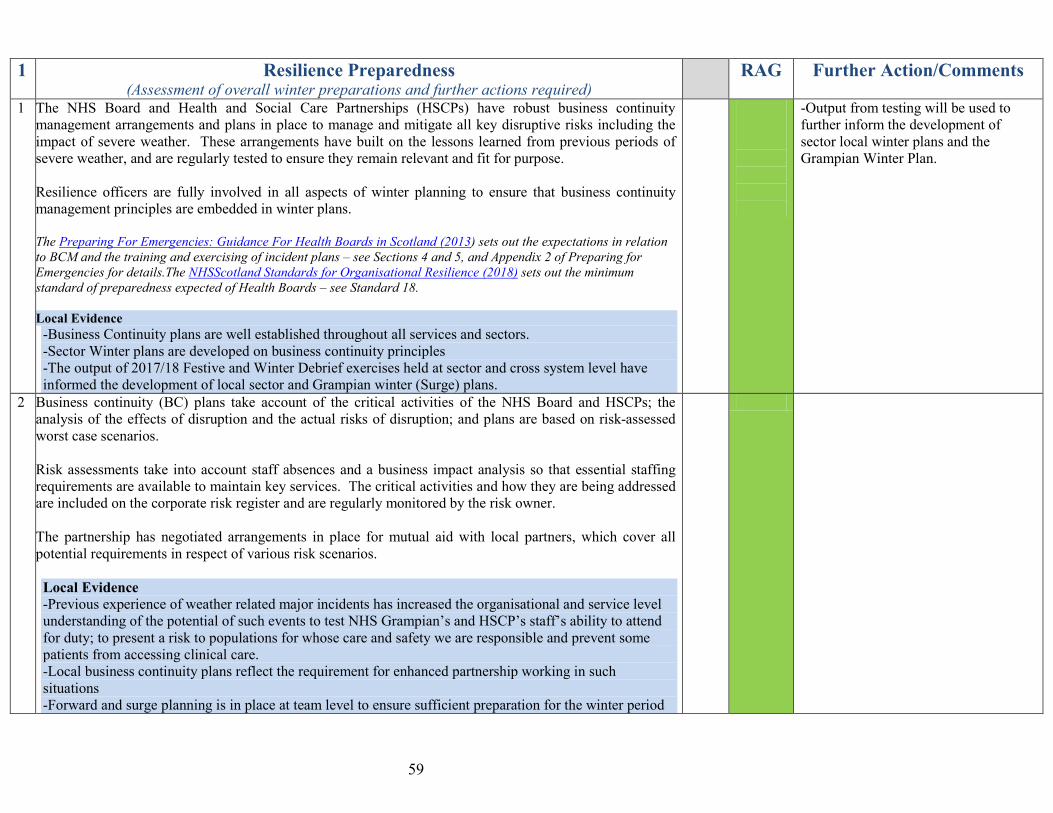
59
1 Resilience Preparedness (Assessment of overall winter preparations and further actions required)
RAG Further Action/Comments
1 The NHS Board and Health and Social Care Partnerships (HSCPs) have robust business continuity management arrangements and plans in place to manage and mitigate all key disruptive risks including the impact of severe weather. These arrangements have built on the lessons learned from previous periods of severe weather, and are regularly tested to ensure they remain relevant and fit for purpose. Resilience officers are fully involved in all aspects of winter planning to ensure that business continuity management principles are embedded in winter plans. The Preparing For Emergencies: Guidance For Health Boards in Scotland (2013) sets out the expectations in relation to BCM and the training and exercising of incident plans – see Sections 4 and 5, and Appendix 2 of Preparing for Emergencies for details.The NHSScotland Standards for Organisational Resilience (2018) sets out the minimum standard of preparedness expected of Health Boards – see Standard 18. Local Evidence -Business Continuity plans are well established throughout all services and sectors. -Sector Winter plans are developed on business continuity principles -The output of 2017/18 Festive and Winter Debrief exercises held at sector and cross system level have informed the development of local sector and Grampian winter (Surge) plans.
-Output from testing will be used to further inform the development of sector local winter plans and the Grampian Winter Plan.
2 Business continuity (BC) plans take account of the critical activities of the NHS Board and HSCPs; the analysis of the effects of disruption and the actual risks of disruption; and plans are based on risk-assessed worst case scenarios. Risk assessments take into account staff absences and a business impact analysis so that essential staffing requirements are available to maintain key services. The critical activities and how they are being addressed are included on the corporate risk register and are regularly monitored by the risk owner. The partnership has negotiated arrangements in place for mutual aid with local partners, which cover all potential requirements in respect of various risk scenarios. Local Evidence -Previous experience of weather related major incidents has increased the organisational and service level understanding of the potential of such events to test NHS Grampian’s and HSCP’s staff’s ability to attend for duty; to present a risk to populations for whose care and safety we are responsible and prevent some patients from accessing clinical care. -Local business continuity plans reflect the requirement for enhanced partnership working in such situations -Forward and surge planning is in place at team level to ensure sufficient preparation for the winter period

60
-Space and available equipment is identified in these plans at sector level and there is a focus on workforce capacity in particular at a time when Christmas and New Years public holidays fall.
3 The NHS Board and HSCPs have appropriate policies in place that cover: • what staff should do in the event of severe weather hindering access to work, and • how the appropriate travel advice will be communicated to staff and patients • How to access local resources (including voluntary groups) that can support the transport of staff to
and from their places of work during periods of severe weather. Policies should be communicated to all staff on a regular basis.
Resilience officers and HR departments will need to develop a staff travel advice and communications protocol to ensure that travel advice and messages to the public are consistent with those issued by Local /Regional Resilience Partnerships to avoid confusion. This should be communicated to all staff.
Local Evidence -Adverse weather policies for staff are in place across sectors and available through local human resources depts. and recognised communication channels. -Civil Contingencies Services have established recognised methods of communicating travel advice to patients and staff in place. -A memorandum of understanding is in place with COTAG to provide a 4X4 vehicle response support in times of need to emergency services and local authorities
4 The NHS Board’s and HSCPs websites will be used to advise on travel to appointments during severe weather and prospective cancellation of clinics. Local Evidence -The previous experience of NHS Grampian in communicating the impact of severe weather on clinics and providing travel advice to patient and the public has led to an increased DNA rates and additional confusion.
5 The NHS Board, HSCPs and local authority have created a capacity plan to manage any potential increase in demand for mortuary services over the winter period; this process has involved funeral directors. Local Evidence -Mortuary Cross system plans have been agreed to double capacity with additional mobile mortuary facilities available
6 The effectiveness of winter plans will be tested with all stakeholders by 30 October The final version of the winter plan has been approved by NHS Board and HSCPs Local Evidence -Table top testing exercises of all sector winter (surge) plans are ongoing, culminating in a Cross System table top testing exercise
• Aberdeen City HSCP 31st August 2018
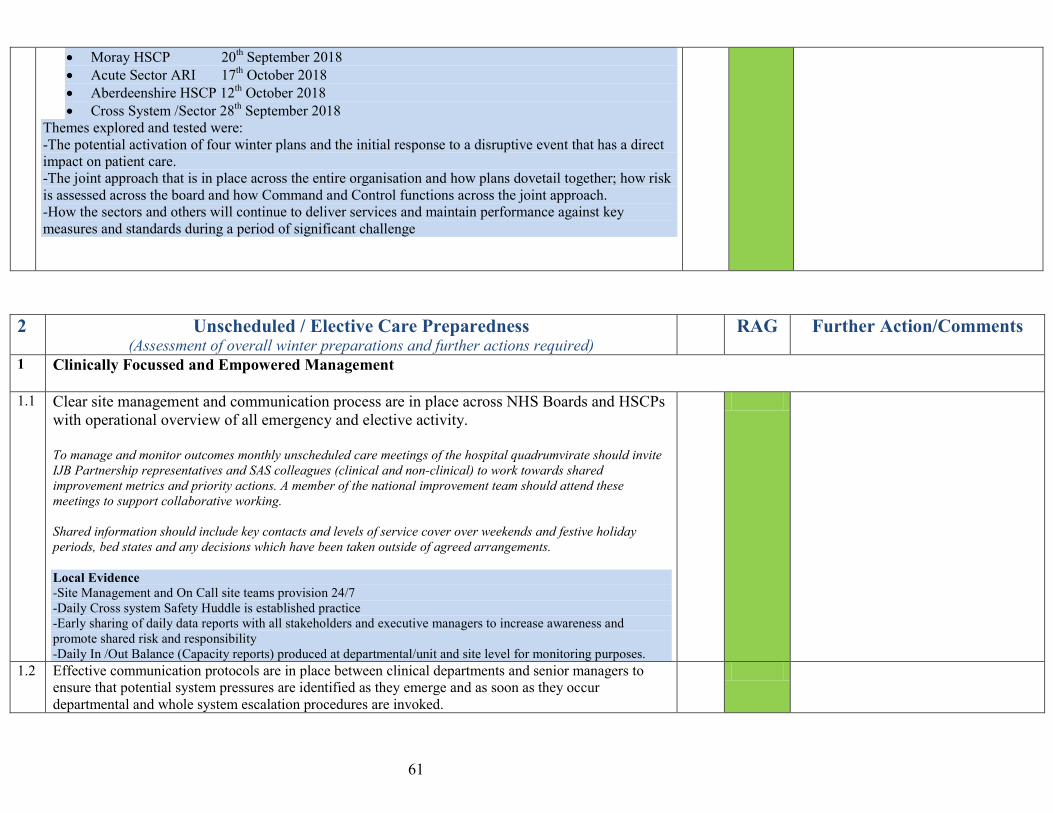
61
• Moray HSCP 20th September 2018 • Acute Sector ARI 17th October 2018 • Aberdeenshire HSCP 12th October 2018 • Cross System /Sector 28th September 2018
Themes explored and tested were: -The potential activation of four winter plans and the initial response to a disruptive event that has a direct impact on patient care. -The joint approach that is in place across the entire organisation and how plans dovetail together; how risk is assessed across the board and how Command and Control functions across the joint approach. -How the sectors and others will continue to deliver services and maintain performance against key measures and standards during a period of significant challenge
2 Unscheduled / Elective Care Preparedness (Assessment of overall winter preparations and further actions required)
RAG Further Action/Comments
1 Clinically Focussed and Empowered Management
1.1 Clear site management and communication process are in place across NHS Boards and HSCPs with operational overview of all emergency and elective activity. To manage and monitor outcomes monthly unscheduled care meetings of the hospital quadrumvirate should invite IJB Partnership representatives and SAS colleagues (clinical and non-clinical) to work towards shared improvement metrics and priority actions. A member of the national improvement team should attend these meetings to support collaborative working. Shared information should include key contacts and levels of service cover over weekends and festive holiday periods, bed states and any decisions which have been taken outside of agreed arrangements. Local Evidence -Site Management and On Call site teams provision 24/7 -Daily Cross system Safety Huddle is established practice -Early sharing of daily data reports with all stakeholders and executive managers to increase awareness and promote shared risk and responsibility -Daily In /Out Balance (Capacity reports) produced at departmental/unit and site level for monitoring purposes.
1.2 Effective communication protocols are in place between clinical departments and senior managers to ensure that potential system pressures are identified as they emerge and as soon as they occur departmental and whole system escalation procedures are invoked.

62
Local Evidence -Site and Capacity teams monitor admission/discharge balance on a daily basis with support from capacity meetings held throughout the day. -Boarded Patients are highlighted as priorities as part of daily safety briefs and repatriation is a priority action at all huddles. -Daily Sitrep briefings are widely communicated across local and whole system. - Daily Cross System Conference Call at 21.45
1.3 A Target Operating Model and Escalation policies are in place and communicated to all staff. Consider the likely impact of emergency admissions on elective work and vice versa, including respiratory, circulatory, orthopaedics, cancer patients, ICU/PICU. This should be based on detailed modelling, pre-emptive scheduling of electives throughout the autumn, and early spring, and clear strategies regarding which lists may be subject to short-notice cancellation with a minimum impact.
Pressures are often due to an inability to discharge patients timeously. Systems should be in place for the early identification of patients who no longer require acute care and discharged without further delay Local Evidence -Ongoing development of Target Operating Models by services in Acute Sector -Respiratory admissions to ARI & DGH are monitored via Site and Capacity teams at the safety and flow briefs. -A planned respiratory bundle that includes focused interventions aimed at supporting increased self management of adults with COPD alongside remote patient management by clinicians is being developed for implementation across HSCP’s in Dec 2018. Level of non-essential elective activity over the surge period is planned well in advance of winter.
Ongoing development of self management Respiratory Bundle to include the following interventions- Flu Vaccinations, Inhaler Awareness, Medication review, access to Pulmonary rehab, early access to antibiotics, weather warnings.
1.4 Escalation procedures are linked to a sustainable resourcing plan, which encompasses the full use of step-down community facilities, such as community hospitals and care homes. HSCPs should consider any requirement to purchase additional capacity over the winter period. All escalation plans should have clearly identified points of contact and should be comprehensively tested and adjusted to ensure their effectiveness. Local Evidence -Surge capacity plans are in place across Acute sector and HSCP’s. -27 Interim Care Home beds available in Aberdeen City dedicated to supporting discharge. -2 Care Home beds identified to provide “Step Up” capacity for GP’s in support of Acute Hospital admission avoidance.
Awaiting detail of Aberdeenshire Community Hospital surge capacity plans.
2 Undertake detailed analysis and planning to effectively manage schedule elective and unscheduled activity (both short and medium-term) based on forecast emergency and elective demand, to optimise whole systems business continuity.
63
This has specifically taken into account the surge in unscheduled activity in the first week of January. 2.1 Pre-planning and modelling has optimised demand, capacity, and activity plans across urgent, emergency
and elective provision are fully integrated, including identification of winter surge beds for emergency admissions Weekly projections for scheduled and unscheduled demand and the capacity required to meet this demand are in place. Plans for scheduled services include a specific ‘buffering range’ for scheduled queue size, such that the scheduled queue size for any speciality/sub-speciality can fluctuate to take account of any increases in unscheduled demand without resulting in scheduled waiting times deteriorating. This requires scheduled queue size for specific specialities to be comparatively low at the beginning of the winter period. NHS Boards can evidence that for critical specialities scheduled queue size and shape are such that a winter surge in unscheduled demand can be managed at all times ensuring patient safety and clinical effectiveness without materially disadvantaging scheduled waiting times. Local Evidence -Winter planning is an ongoing year round activity across Grampian and this includes the production of post festive performance and activity reports. This data is reviewed in February (post festive period) and again in May at the Cross System debrief and the wider Local Health and Social Care Local review of Winter report. -Winter (Surge) beds identified in the Acute Sector - Level of non-essential elective activity over the surge period is planned well in advance of winter. -A balanced approach to the development of a TTG plan is ongoing.
2.2 Pre-planning has optimised the use of capacity for the delivery of emergency and elective treatment, including identification of winter surge beds for emergency admissions and recovery plans to minimise the impact of winter peaks in demand on the delivery of routine elective work This will be best achieved through the use of structured analysis and tools to understand and manage all aspects of variation that impact on services, by developing metrics and escalation plans around flexing or cancelling electives, and by covering longer term contingencies around frontloading activity for autumn and spring. Ensure that IP/DC capacity in December/January is planned to take account of conversions from OPD during Autumn to minimise the risk of adverse impact on waiting times for patients waiting for elective Inpatient/Day-case procedures, especially for patients who are identified as requiring urgent treatment. Local Evidence -A balanced approach to the planning and scheduling of elective surgical activity is supported by the development of a Surgical Resilience Plan within the Surgical Division of the Acute Sector. -Fully staffed and supported surge beds will be available of ARI & DGH sites to support response to demand
Awaiting additional detail on Surge bed plans for ARI & DGH
64
3 Agree staff rotas in October for the fortnight in which the two festive holiday periods occur to match planned capacity and demand and projected peaks in demand. These rotas should ensure continual access to senior decision makers and support services required to avoid attendance, admission and effective timely discharge.
3.1 System wide planning should ensure appropriate cover is in place for Consultants (Medical and Surgical), multi-professional support teams, including Infection, Prevention and Control Teams (IPCT), Social Workers, home care and third sector support. This should be planned to effectively manage predicted activity across the wider system and discharge over the festive holiday periods, by no later than the end of October. This should take into account predicted peaks in demand, including impact of significant events (e.g.). Hogmanay Street parties on services, and match the available staff resource accordingly. Any plans to reduce the number of hospitals accepting emergency admissions for particular specialties over the festive period, due to low demand and elective activity, need to be clearly communicated to partner organisations. Local Evidence -Workforce capacity plans and rotas for winter/festive period agreed by October 31st 2018. -Staffing levels and any associated risks and mitigation are key to discussion at the daily safety and flow briefs/huddles in both acute and community hospital settings. -Annual leave and rotas are effectively managed at local levels to ensure safe staffing levels across Acute Sector. -The Integrated Discharge Hub team, including social work colleagues with provide a service over the festive public holidays.
3.2 Extra capacity should be scheduled for the ‘return to work’ days after the festive break and this should be factored into annual leave management arrangements across Primary, Secondary and Social Care services. The Monday following the festive weekend breaks should not be routinely used as a day off thereby creating a 5 day weekend. Local Evidence -Primary Care GP services and HSCP Social care services will be fully operational on the Monday following the festive weekend breaks. -G Med (OOH’s GP Services) has developed plans to address additional demand over the festive period and into the Monday’s following the festive weekends.
3.3 Additional festive services are planned in collaboration with partner organisations e.g. Police Scotland, SAS, Voluntary Sector etc. NHS Boards and HSC Partnerships are aware of externally provided festive services such as minor injuries bus in city centre, paramedic outreach services and mitigate for any change in service provision from partner organisations Local Evidence -SAS and Voluntary sector services that support festive services have plans in place to provide a festive period
65
service in line with predicted demand. 3.4 Out of Hours services, GP, Dental and Pharmacy provision over festive period will be communicated to
clinicians and managers including on call to ensure alternatives to attendance are considered. Dental and pharmacy provision should be communicated to all Health and Social Care practitioners across the winter period to support alternatives to attendance at hospital. Local Evidence -There will be early and wide communication and promotion of the winter plan across sectors by local managers -Local and National Winter Campaigns are in place, supporting local winter health priorities and featuring self care and self management advice via the Know Who To Turn To campaign. -Corporate Communications team attends safety and flow briefings when appropriate and use the Grampian Website and Social Media to keep patients informed of winter pressures and how to access out of hours services over the Festive period.
4 Optimise patient flow by proactively managing Discharge Process utilising 6EA – Daily Dynamic Discharge to shift the discharge curve to the left and ensure same rates of discharge over the weekend and public holiday as weekday.
4.1 Discharge planning in collaboration with HSCPs, Transport services, carer and MDT will commence prior to, or at the point of admission, using, where available, protocols and pathways for common conditions to avoid delays during the discharge process. Patients, their families and carers should be involved in discharge planning with a multi-disciplinary team as early as possible to allow them to prepare and put in place the necessary arrangements to support discharge. Utilise Criteria Led Discharge wherever possible. Supporting all discharges to be achieved within 72 hours of patient being ready. Where transport service is limited or there is higher demand, alternative arrangements are considered as part of the escalation process – this should include third sector partners (e.g. British Red Cross) Utilise the discharge lounge as a central pick-up point to improve turnaround time and minimise wait delays at ward level. Local Evidence -Early sharing of daily data reports with all Cross System stakeholders to increase awareness of discharge plans and required support. -Daily Dynamic Discharge Principles applied to discharge management & process across Acute and Community Hospital settings. -Continued use of criteria led discharge in appropriate settings to ensure timely discharge. -A Test of Change integrating the presence of Aberdeen City Social Work teams in the Emergency department at ARI to commence discharge planning at the earliest point of admission and to support admission avoidance. - Community hospital bed occupancy levels are part of the discussions at the daily 09.30 Cross Sector huddle following data collection at HSCP level. HSCP Social Work/care assessments are discussed as part of both daily Discharge Hub actions at ARI and Board
66
Rounds at DGH.
4.2 To support same rates of discharge at weekend and public holiday as weekdays regular daily ward rounds and bed meetings will be conducted to ensure a proactive approach to discharge. Discharges should be made early in the day, over all 7 days, and should involve key members of the multidisciplinary team, including social work. Pharmacy services should also be available to issue timely prescriptions to support discharge. Criteria Led Discharge should be used wherever appropriate. Ward rounds should follow the ‘golden hour’ format – sick and unwell patients first, patients going home and then early assessment and review. Test scheduling and the availability of results, discharge medication, transport requirements and availability of medical and nursing staff to undertake discharge should all be considered during this process to optimise discharge pre-noon on the estimated date of discharge. Criteria Led Discharge should be used wherever appropriate. Local Evidence - Agreed trajectory for weekend discharges - Agreed trajectory for discharges earlier in the day -Daily Dynamic Discharge Principles applied to discharge management & process across Acute and Community Hospital settings. -Test of Change to support continued assessment of complex discharges at weekends and public holidays by the Integrated Discharge hub team is planned. -Integrated Discharge hub will be staffed and operational over the festive public holidays. - HSCP Social Work/care assessments are discussed as part of both daily Discharge Hub actions at ARI and Board Rounds at DGH. -Daily ward rounds across all Acute Hospital wards will continue 7 days a week. -Capacity meetings at ARI will continue 4 x daily at ARI and 2 x daily at DGH.
4.3 Discharge lounges should be fully utilised to optimise capacity. This is especially important prior to noon. Processes should be in place to support morning discharge at all times (e.g.) breakfast club, medication, pull policy to DL, default end point of discharge. Utilisation should be monitored for uptake and discharge compliance. Extended opening hours during festive period over public Holiday and weekend Local evidence - Establishment of discharge lounges at ARI & DGH is not currently confirmed for winter 2018/19. However a Discharge Lounge Test of Change action plan is being developed and considered should it be required.
RAG Status – Systems/Processes are not in place and there is no development plan has been assigned as currently there are no confirmed plans to establish discharge lounges at ARI or DGH on a permanent basis.
67
4.4 Key partners such as: pharmacy, transport and support services, including social care services, will have determined capacity and demand for services and be able to provide adequate capacity to support the discharge process over winter period. These services should be aware of any initiatives that impact on increased provision being required and communication processes are in place to support this. e.g. surge in pre Christmas discharge There should be a monitoring and communication process in place to avoid delays, remove bottlenecks and smooth patient discharge processes Local Evidence -Based on previous year’s intelligence, plans have been developed for Pharmacy services to operate a normal service throughout the winter period with appropriate availability over the festive periods. Key information will be provided directly to wards, departments and clinics to ensure timely access to pharmacy dispensary and distribution services. -As set out in the SAS Winter Plan, arrangements are in place to respond to and manage the predicted peaks in demand, including early preparation of staffing rotas during the festive period. -Aberdeen City have prioritisation and triage of all homecare provision for clients in place to ensure that those in greatest need(including hospital discharges) have any care at home capacity directed to them on a priority basis. Aberdeen City HSCP & Moray HSCP have increased care at home capacity available to support discharge.
Awaiting Aberdeenshire H&SCP social care surge plans.
5 Agree anticipated levels of homecare packages that are likely to be required over the winter (especially festive) period and utilise intermediate care options such as Rapid Response Teams, enhanced supported discharge or reablement and rehabilitation (at home and in care homes) to facilitate discharge and minimise any delays in complex pathways.
5.1 Close partnership working between stakeholders, including the third and independent sector to ensure that adequate care packages are in place in the community to meet all discharge levels. This will be particularly important over the festive holiday periods. Partnerships will monitor and manage predicted demand supported by enhanced discharge planning and anticipated new demand from unscheduled admissions. Partnerships should develop local agreements on the direct purchase of homecare supported by ward staff. Assessment capacity should be available to support a discharge to assess model across 7 days. Local Evidence -In addition to the weekly care home vacancy report (held in Aberdeen City HSCP) Aberdeenshire has established a “real-time” resource which monitors vacancies across all resources, including community hospitals, care homes, very sheltered and sheltered housing. -The Moray Out of Hours Project (Pitgaveny Team) will provide a resource to support vulnerable adults for short periods between the hours of 17.00 and 02.00 who would otherwise be potentially admitted to an acute hospital. This service can be accessed by the Emergency Department, Out of Hours GP service, Social Work and the Scottish Ambulance Service.

68
5.2 Intermediate care options, such as enhanced supported discharge, reablement and rehabilitation will be utilised over the festive and winter surge period, wherever possible. Paertnerships and Rapid Response teams should have the ability to directly purchase appropriate homecare packages, following the period of Intermediate care. All delayed discharges will be reviewed for alternative care arrangements and discharge to assess where possible Local Evidence -Hanover Housing Development in Moray provides “close to home” nursing care model when patients home is not an option, delivering “step up” community bed provision that avoids admission to hospital -In Aberdeen city HSCP additional care home capacity has been reserved to support diversion from hospital admission – prevent in appropriate admission at times of surge. -In Aberdeen HSCP – a minimum of 27 Social care beds have been identified specifically to support discharges and improve flow out of hospital. -In Dec 2018 Aberdeen city HSCP Delayed Discharge Group will increase the frequency of meetings from monthly to fortnightly in anticipation of increased activity and to take action to address delays. In times of surge the group will be able to increase the frequency of the meetings to take action and address delays. -Procedures governing the allocation of Interim beds in Aberdeen City, which are dedicated to supporting discharge, have been updated to allow priority criteria to vary to reflect and address cross system demand.
5.3 Patients identified as being at high risk of admission from, both the SPARRA register and local intelligence, and who have a care manager allocated to them, will be identifiable on contact with OOH and acute services to help prevent admissions and facilitate appropriate early discharge. Key Information Summaries (KIS) will include Anticipatory Care Planning that is utilised to manage care at all stages of the pathways. Local Evidence -Virtual Community wards are established across GP practices in Aberdeenshire and Moray HSCP’s -Aberdeen City HSCP Hospital at Home team provides support to frail elderly patients in the community at high risk of admission with the aim of avoiding hospital admission. - GP Practices will be set up to flex and offer additional ‘on the day’ appointments based on actual demand fluctuations/surge.
5.4 All plans for Anticipatory Care Planning will be implemented, in advance of the winter period, to ensure continuity of care and avoid unnecessary emergency admissions / attendances. KIS and ACPs should be utilised at all stages of the patient journey from GP / NHS 24, SAS, ED contact. If attendances or admissions occur Anticipatory Care Plans and key information summaries should be used as part of discharge process to inform home circumstances, alternative health care practitioners and assess if fit for discharge. Local Evidence
69
-A Planned Respiratory bundle model across Grampian that included focused interventions aimed at supporting increased self management of adults with COPD alongside remote patient management by clinicians is being developed.
6.0 Ensure that communications between key partners, staff, patients and the public are effective and that key messages are consistent.
6.1 Effective communication protocols are in place between key partners, particularly across emergency and elective provision, local authority housing, equipment and adaptation services, Mental Health Services, and the independent sector. Collaboration between partners, including NHS 24, Locality Partnerships, Scottish Ambulance Service, SNBTS through to A&E departments, OOH services, hospital wards and critical care, is vital in ensuring that winter plans are developed as part of a whole systems approach. Shared information should include key contacts and levels of service cover over weekends and festive holiday periods, bed states and any decisions which have been taken outside of agreed arrangements. Local evidence -All key partners have on call personnel available at all levels. - Details of on call personnel and contact details are held and available on Rotawatch.
6.2 Communications with the public, patients and staff will make use of all available mediums, including social media, and that key messages will be accurate and consistent. NHS 24 are leading on the 2018/19 ‘Be Healthwise This Winter’ media campaign, and SG Health Performance & Delivery Directorate is working with partners and policy colleagues to ensure that key winter messages, around repeat prescriptions’, respiratory hygiene, and norovirus are effectively communicated to the public. The public facing website http://www.readyscotland.org/ will continue to provide a one stop shop for information and advice on how to prepare for and mitigate against the consequences from a range of risks and emergencies. This information can also be accessed via a smartphone app accessible through Google play or iTunes. The Met Office National Severe Weather Warning System provides information on the localised impact of severe weather events. Promote use of NHS Inform, NHS self-help app and local KWTTT campaigns Local evidence -Each partner organisation and service has plans in place for effectively communicating with local staff. Key mechanisms and focus for communicating with staff in partnership are:
- The Winter Plan 2018/19 and any other supporting documents/plans, along with bulletins (weather, transport, flu vaccination, norovirus etc) will be available on the NHS Grampian staff internet and NHS Grampian Website.
- Links to the national NHS Scotland Winter Campaign will be available on the NHS Grampian websites

70
and NHS Grampian Facebook page. - Know Who To Turn To (KWTTT) key messages will be displayed as a banner on the NHS Grampian
Intranet as well as circulated via team briefs, newsletters and global email alert for staff - Communication of key information on services available over the festive period such as infection control
advice, will be made available to each ward/department across NHS Grampian - Access to social care assessment and care packages will continue to be available through the integrated
Discharge Hub. Key Messages to the Public form part of the 2018/19 Communication Plan and will be implemented between October 2018 and January 2019 with the aim of:
- Promoting winter health and reducing pressures on local services - Encouraging individuals to take responsibility for their own health and seek advice appropriately via
KWTTT Campaign. - Adding value to existing national campaigns such as flu and pneumococcal immunisation.
3 Out of Hours Preparedness (Assessment of overall winter preparations and further actions required)
RAG Further Action/Comments
1 The OOH plan covers the full winter period and pays particular attention to the festive period. This should include an agreed escalation process. Have you considered / discussed local processes with NHS 24 on providing pre-prioritised calls during the OOH period? Local Evidence The Out of Hours GP Service Winter Plan takes full account of:
The need for a robust plan covering the full winter period The possibility of an outbreak of flu or other seasonal illness The possibility of adverse weather conditions Prioritisation of service to enhance capacity Above normal demand on primary care at that time of year particularly on Saturdays and public holidays throughout the period The need to provide service over the festive period
2 The plan clearly demonstrates how the Board will manage both predicted and unpredicted demand from NHS 24 and includes measures to ensure that pressures during weekends, public holidays are operating effectively. The plan demonstrates that resource planning and demand management are prioritised over the festive period. Local Evidence Specific actions to enhance integrated partnership working across Grampian will occur at different levels based on

71
the situation and can be summarised as: Embedded safety briefs in both Acute hospital with representation from all areas of the acute hospital including Security, IP&C, Facilities and SAS. Safety briefs in are established in HSCP Community Hospitals and vary in format to suit the needs of the local environment. Cross System huddles which support individual partners, anticipate and manage surges in activity at the earliest opportunity
3 There is evidence of attempts at enabling and effecting innovation around how the partnership will predict and manage pressures on public holidays/Saturday mornings and over the festive period. The plan sets out options, mitigations and solutions considered and employed.
4 There is reference to direct referrals between services. For example, are direct contact arrangements in place, for example between Primary Care Emergency Centres (PCECs)/Accident & Emergency (A&E) Departments/Minor Injuries Units (MIUs) and other relevant services? Are efforts being made to encourage greater use of special notes, where appropriate? Local Evidence -Direct referral processes are in place across a number of services, with the availability of Senior Clinical Decision Support advice to support delivery of Right Patient, Right Place, and Right Team.
5 The plan encourages good record management practices relevant to maintaining good management information including presentations, dispositions and referrals; as well as good patient records.
6 There is reference to provision of pharmacy services, including details of the professional line, where pharmacists can contact the out of hours centres directly with patient/prescription queries and vice versa Local Evidence -The Out of Hours GP service provides a Professional to Professional Advice line to support Community Pharmacist and other community based clinical services
7 In conjunction with HSCPs, ensure that clear arrangements are in place to enable access to mental health crisis teams/services, particularly during the festive period. Local Evidence Intelligence demonstrates that there are surges in demand on mental health services prior to and post festive period. The Unscheduled Care team work 365 days per year and will absorb this as part of their work pattern. On call consultants are available to attend the acute hospital and support the Psychiatric Liaison Team if activity increases
8 In conjunction with HSCPs, ensure that there is reference to provision of dental services, to ensure that services are in place either via general dental practices or out of hours centres This should include an agreed escalation process for emergency dental cases; i.e. trauma, uncontrolled bleeding and increasing swelling. Local Evidence

72
Excluding public holidays, Public Dental services and Independent dental practices will be expected to provide access to dental advice and treatment between 08.00 – 18.00. Out of Hours emergency dental clinics will operate on normal working weekdays and at weekends. Public Holiday emergency dental services will be available through the Dental Information and Advice line
9 The plan displays a confidence that staff will be available to work the planned rotas. While it is unlikely that all shifts will be filled at the moment, the plan should reflect a confidence that shifts will be filled nearer the time. If partnerships believe that there may be a problem for example, in relation to a particular profession, this should be highlighted.
10 There is evidence of what the Board is doing to communicate to the public how their out of hours services will work over the winter period and how that complements the national communications being led by NHS 24. This should include reference to a public communications strategy covering surgery hours, access arrangements, location and hours of PCECs, MIUs, pharmacy opening, etc. Local Evidence A joint communication plan supports the dissemination of key messages communicated in partnership to the public. Key messages and communication methods include Public Flu campaign Media releases informing the public of surgery closures, the requirement to stock up on medications, repeat prescriptions and services available over the festive period. A targeted mail drop to households across Grampian highlighting the KWTTT campaign TV and Radio advertising Targeted Social Media messages using Facebook’s audience definition information and Twitter e.g. Antibiotic campaign NHS Grampians Public Website
11 There is evidence of joint working between the HSCP, the Board and the SAS in how this plan will be delivered through joint mechanisms, particularly in relation to discharge planning, along with examples of innovation involving the use of ambulance services.
12 There is evidence of joint working between the Board and NHS 24 in preparing this plan. This should confirm agreement about the call demand analysis being used. Local Evidence Grampian has had an established robust winter planning process since 2015/16, that has included identifying lesson learned from local sector and cross sector debrief sessions and from an early cross sector winter planning session in July 2018. In conjunction the sectors have been engaged in preparing their own draft plans which were shared at the end of July 2018. The 2018/19 Grampian Winter (Surge) Plan has been developed and agreed as part of the Grampian Unscheduled Care 6 Essential Actions Programme, including communications and participation from partners such as NHS 24 and

73
SAS. The NHS 24 Winter Plan for 2018/19 sets out how predicted peaks in service activity will be appropriately managed through adequate workforce capacity maximising the use of call handlers, call operators and Pharmacists and maximising national clinical and call handler support lines. Contingency plans and escalation processes are in place and involve support in period of peak demand from the Out of Hours GP service.
13 There is evidence of joint working between the acute sector and primary care Out-of-Hours planners in preparing this plan. This should cover possible impact on A&E Departments, MIUs and any other acute receiving units (and vice versa), including covering the contact arrangements. Local evidence The co-location of the Primary Care Out of Hours services with the Emergency departments on both Acute Hospital sites enhances the joint working between services and is supported by established redirection processes.
14 There is evidence of joint planning across all aspects of the partnership and the Board in preparing this plan. This should be include referral systems, social work on-call availability, support for primary care health services in the community and support to social services to support patients / clients in their own homes etc. Local Evidence The Senior Leadership Team includes each of the 3 Chief Offices, the Director of Acute Services and members of NHS Grampians Leadership team. The SLT meet weekly alternating with formal meetings and huddles to discuss operational issues and this provides a regular and valuable opportunity to share key pressures, issues and the joint planning of Grampians Winter Surge Plan
15 There is evidence that Business Continuity Plans are in place across the partnership and Board with clear links to the pandemic plan including provision for an escalation plan. The should reference plans to deal with a higher level of demand than is predicted and confirm that the trigger points for moving to the escalation arrangements have been agreed with NHS 24.
4 Prepare for & Implement Norovirus Outbreak Control Measures (Assessment of overall winter preparations and further actions required)
RAG Further Action/Comments
1 NHS Boards must ensure that staff have access to and are adhering to the national guidelines on Preparing for and Managing Norovirus in Care Settings
This includes Norovirus guidance and resources for specific healthcare and non-healthcare settings.
74
2 IPCTs will be supported in the execution of a Norovirus Preparedness Plan before the season starts. Boards should ensure that their Health Protection Teams (HPTs) support the advance planning which nursing and care homes are undertaking to help keep people out of hospital this winter and provide advice and guidance to ensure that norovirus patients are well looked after in these settings. Local Evidence
-There are long standing systems in place for reporting outbreaks in community establishments with vulnerable individuals for example care homes. Following reporting of the outbreak to the Health Protection Team (HPT), immediate risk assessment is undertaken and infection prevention and control measures discussed and then followed up in writing to the manager. Infection prevention and control measures usually include closure of the establishment to all new residents, residents returning from hospital and day care. Regular monitoring of the outbreak is undertaken until the establishment has been free of symptomatic residents and staff for 48 hours.
3 HPS Norovirus Control Measures (or locally amended control measures) are easily accessible to all staff, e.g. available on ward computer desk tops, or in A4 folders on the wards.
Local Evidence -Information guidance/polices and support are easily accessible to NHS Grampian Staff and other colleagues in relation to preventing and containing incidents of norovirus
4 NHS Board communications regarding bed pressures and norovirus ward closures are optimal and everyone will be kept up to date in real time. Boards should consider how their communications Directorate can help inform the public about any visiting restrictions which might be recommended as a result of a norovirus outbreak. Local Evidence -When necessary an Incident Management Team IMT)will be activated at the request of the Lead Infection Prevention & Control Doctor
5 Debriefs will be provided following individual outbreaks or end of season outbreaks to ensure system modifications to reduce the risk of future outbreaks. Multiple ward outbreaks at one point in time at a single hospital will also merit an evaluation. Local evidence -The IPCT will participate with national point prevalence Norovirus surveillance programme for winter illness and submit reports to Health Protection Scotland on behalf of NHSG every Tuesday (retrospectively for the previous week). - The IPCNs may attend further bed management meetings upon request, but may require prioritising outbreak management. They will contact site and capacity teams with rolling updates

75
- A seasonal overview will be provided by the IPCT for the NHSG cross system winter debrief 2018-2019 upon request
6 IPCTs will ensure that the partnership and NHS Board are kept up to date regarding the national norovirus situation. Local Evidence -The IPCNs will alert the organisation when the Scottish Norovirus season has started (when declared by HPS) via the daily SITREP, attendance at Acute and DGH safety briefs and via HAI groups
7 Before the norovirus season has begun, staff in emergency medical receiving areas will confirm with the IPCTs the appropriateness of procedures to prevent outbreaks when individual patients have norovirus symptoms, e.g. patient placement, patient admission and environmental decontamination post discharge. Local evidence -An established process of patient placement is place and operated in conjunction with the Hospital Site and Capacity teams
8 NHS Boards must ensure arrangements are in place to provide adequate cover across the whole of the festive holiday period. While there is no national requirement to have 7 day IPCT cover, outwith the festive holiday period, Boards should consider their local IPC arrangements. Local Evidence -IPCT rotas provide cover across the whole of the festive holiday period
9 The NHS Board is prepared for rapidly changing norovirus situations, e.g. the closure of multiple wards over a couple of days. As part of their surge capacity plan, Boards should consider how wards will maintain capacity in the event that wards are closed due to norovirus.
10 There will be effective liaison between the IPCTs and the HPTs to optimise resources and response to the rapidly changing norovirus situation. This could include the notification of ‘tweets’, where appropriate, to help spread key message information. HPT/IPCT and hospital management colleagues should ensure that the they are all aware of their internal processes and that they are still current. Local Evidence -The HPT participate in the national health care infection outbreaks reporting system operated by Health protection Scotland. The IPCT produce daily Norovirus SITREP’s that are communicated widely throughout NHS Grampian for the duration of the norovirus season.

76
11
The partnership is aware of norovirus publicity materials and is prepared to deploy information internally and locally as appropriate, to spread key messages around norovirus and support the ‘Stay at Home Campaign’ message. This could include HPT supporting schools to have awareness raising prior to norovirus season and the notification of ‘tweets’, where appropriate, to help spread key message information. Local Evidence Norovirus publicity messages are prepared for deployment which is supported by the Corporate Communications Team
5 Seasonal Flu, Staff Protection & Outbreak Resourcing (Assessment of overall winter preparations and further actions required)
RAG Further Action/Comments
1 Staff working in areas with high risk patients such as paediatric, oncology, maternity, care of the elderly, haematology, ICUs, etc., have been vaccinated to prevent the potential spread of infection to patients, as recommended in the CMOs seasonal flu vaccination letter due to be published in Aug 2018. This will be evidenced through end of season vaccine uptake submitted to HPS by each NHS board. Local trajectories have been agreed and put in place to support and track progress. Local Evidence Grampian actively encourages staff to access the influenza vaccination programme, with the Senior Leadership team and Acute Sector Leadership teams showing leadership by example
2 All of our staff have easy and convenient access to the seasonal flu vaccine. In line with recommendations in CMO Letter (2018) clinics are available at the place of work and include clinics during early, late and night shifts, at convenient locations. Drop-in clinics are also available for staff unable to make their designated appointment and peer vaccination is facilitated to bring vaccine as close to the place of work for staff as possible. It is the responsibility of health care staff to get vaccinated to protect themselves from seasonal flu and in turn protect their vulnerable patients, but NHS Boards have responsibility for ensuring vaccine is easily and conveniently available; that sufficient vaccine is available for staff vaccination programmes; and that senior management and clinical leaders with NHS Boards fully support vaccine delivery and uptake. Local Evidence Grampian staff influenza vaccination programme commenced on the 1st October offering a wide range of access to vaccination for all eligible staff.

77
3 The winter plan takes into account the predicted surge of flu activity that can happen between October and March and we have adequate resources in place to deal with potential flu outbreaks across this period. If there are reported flu outbreaks during the season, where evidence shows that vaccination uptake rates are not particularly high, NHS Boards may undertake targeted immunisation. In addition, the centralised contingency stock of influenza vaccine, purchased by the Scottish Government can be utilised if required and an agreed protocol is in place with NHS Boards on the use of the contingency stock. Antiviral prescribing for seasonal influenza may also be undertaken when influenza rates circulating in the community reach a trigger level (advice on this is generated by a CMO letter to health professionals) Local Evidence The multiagency Grampian Major Infectious diseases/Pandemic Fle plan sets out the structures and processes that will be used in the event of an infectious disease incident such as pandemic influenza, that requires an extraordinary organisational response.
4 HPS weekly updates, showing the current epidemiological picture on influenza infections across Scotland, will be routinely monitored over the winter period to help us detect early warning of imminent surges in activity. Health Protection Scotland and the Health Protection Team within the Scottish Government monitor influenza rates during the season and take action where necessary, The Health Protection Team brief Ministers of outbreak/peaks in influenza activity where necessary. HPS produce a weekly influenza bulletin and a distillate of this is included in the HPS Winter Pressures Bulletin.
Local Evidence NHS Grampian Public Health and IPCT Services monitor weekly influenza bulletins and disseminate information through established organisation communication channels
5 Adequate resources are in place to manage potential outbreaks of seasonal flu that might coincide with norovirus, severe weather and festive holiday periods. NHS board contingency plans have a specific entry on plans to mitigate the potential impact of potential outbreaks of seasonal influenza to include infection control, staff vaccination and antiviral treatment and prophylaxis. Contingency planning to also address patient management, bed management, staff redeployment and use of reserve bank staff and include plans for deferral of elective admissions and plans for alternative use of existing estate or opening of reserve capacity to offset the pressures. Local Evidence Sector Surge plans contain contingency plans to mitigate the impact of seasonal flu coinciding with norovirus outbreaks, severe weather and festive holiday periods that include bed management, patient placement principles and surge capacity details
6 Respiratory Pathway (Assessment of overall winter preparations and further actions required)
RAG Further Action/Comments
78
1 There is an effective, co-ordinated respiratory service provided by the NHS board. 1.1 Clinicians (GP’s, Out of Hours services, A/E departments and hospital units) are familiar with their local
pathway for patients with different levels of severity of exacerbation in their area. Local Evidence Respiratory and Exacerbation of COPD Pathways established across all services/departments
1.2 Plans are in place to extend and enhance home support respiratory services over a 7 day period where appropriate.
1.3 Anticipatory Care/ Palliative care plans for such patients are available to all staff at all times. Consider use of an effective pre admission assessment/checklist i.e. appropriate medication prescribed, correct inhaler technique, appropriate O2 prescription, referred to the right hospital/right department, referred directly to acute respiratory assessment service where in place.. Consider use of self-management tools including anticipatory care plans/asthma care plans and that patients have advice information on action to take/who to contact in the event of an exacerbation. Patients should have their regular and emergency medication to hand, their care needs are supported and additional care needs identified (should they have an exacerbation). Local Evidence Anticipatory Care plans and Key Information summaries are available to staff at all times. Review and updating of ACP’s and KIS information is a key action highlighted through local partnership winter plans and table top testing exercises
1.4 Simple messages around keeping warm etc. are well displayed at points of contact, and are covered as part of any clinical review. This is an important part of ‘preparing for winter for HCPs and patients. Simple measures are important in winter for patients with chronic disease/COPD. For example, keeping warm during cold weather and avoiding where possible family and friends with current illness can reduce the risk of exacerbation and hospitalisation. Local Evidence A planned Respiratory Bundle that includes focused interventions aimed at supporting increased self management of adults with COPD alongside remote patient management by clinicians is being developed for implementation across all 3 HSCP’s in Dec 2018. This includes advice to patients on:
- Keeping warm during cold weather & using the weather check on your smart phone. - Protect your lungs by wearing a scarf around your nose and mouth on colder days. - Accessing inhaler technique instruction from community pharmacies. - Avoiding infections by not being in the company of people with coughs and colds. - Getting the flu vaccination. - Joining a pulmonary rehabilitation exercise class
79
2 There is effective discharge planning in place for people with chronic respiratory disease including COPD 2.1 Discharge planning includes medication review, ensuring correct usage/dosage (including O2), checking
received appropriate immunisation, good inhaler technique, advice on support available from community pharmacy, general advice on keeping well e.g. keeping warm, eating well, smoking cessation. Local arrangements should be made to ensure that the actions described are done in the case of all admissions, either in hospital, before discharge, or in Primary Care soon after discharge, by a clinician with sufficient knowledge and skills to perform the review and make necessary clinical decisions (specifically including teaching or correcting inhaler technique).
2.2 All necessary medications and how to use them will be supplied on hospital discharge and patients will have their planned review arranged with the appropriate primary, secondary or intermediate care team.
3 People with chronic respiratory disease including COPD are managed with anticipatory and palliative care approaches and have access to specialist palliative care if clinically indicated.
3.1 Anticipatory Care Plan's (ACPs) will be completed for people with significant COPD and Palliative Care plans for those with end stage disease. Spread the use of ACPs and share with Out of Hours services. Consider use of SPARRA/Risk Prediction Models to identify those are risk of emergency admission over winter period. SPARRA Online: Monthly release of SPARRA data, https://www.bo.scot.nhs.uk/. This release estimates an individual’s risk of emergency admission. Consider proactive case/care management approach targeting people with heart failure, COPD and frail older people. Local evidence ACP’s are accessible by Emergency departments and Out of Hours Services. Predictive data including SPARRA and COPD registers are used by GP practices to identify those at risk of emergency admission. Patients with COPD and chronic respiratory illness are managed through the Virtual Ward model to avoid unnecessary admission to acute hospitals
4 There is an effective and co-ordinated domiciliary oxygen therapy service provided by the NHS board 4.1 Staff are aware of the procedures for obtaining/organising home oxygen services.
Staff have reviewed and are satisfied that they have adequate local access to oxygen concentrators and that they know how to deploy these where required. If following review, it is deemed that additional equipment is needed to be held locally for immediate access, please contact Health Facilities Scotland for assistance (0131 275 6860)
80
7 Key Roles / Services RAG Further Action/Comments Heads of Service Nursing / Medical Consultants Consultants in Dental Public Health AHP Leads Infection Control Managers Managers Responsible for Capacity & Flow Pharmacy Leads Mental Health Leads Business Continuity / Emergency Planning Managers OOH Service Managers GP’s
Appropriate emergency plans/contacts are in place to enable patients to receive timely referral to home oxygen service over winter/festive period. Contingency arrangements exist, particularly in remote and rural areas, and arrangements are in place to enable clinical staff in these communities to access short term oxygen for hypoxaemic patients in cases where hospital admission or long term oxygen therapy is not clinically indicated. Take steps to remind primary care of the correct pathway for accessing oxygen, and its clinical indications.
5 People with an exacerbation of chronic respiratory disease/COPD have access to oxygen therapy and supportive ventilation where clinically indicated.
5.1 Emergency care contact points have access to pulse oximetry. Take steps to ensure that all points of first contact with such patients can assess for hypoxaemia, and are aware of those patients in their area who are at risk of CO2 retention. Such patients should be known to Ambulance services, Out of Hours Emergency centres and A/E departments, either through electronic notifications such as eKIS, or by patient help cards, message in a bottle etc. Local Evidence Emergency Care summaries and eKIS records are accessible to SAS, Emergency Departments and Out of Hours services in Grampian.

81
NHS 24 SAS Territorial NHS Boards Independent Sector Local Authorities Integration Joint Boards Strategic Co-ordination Group (Grampian SLT) Third Sector SG Health & Social Care Directorate
The summary table below outlines the further actions taken across Grampian to strengthen capacity for Winter 2018/19. This is by no means an exhaustive list but gives an indication of the many initiatives in place to strengthen capacity and provide resilience.
STRENGTHENING CAPACITY FOR WINTER 2018/19 ACROSS GRAMPIAN Appendix 6
SECTOR INCREASED CAPACITY INTENDED IMPACT
82
Acute Sector Aberdeen Royal Infirmary Dr Grays Hospital, Elgin. Winter Planning Allocation - £426,880 Total Board planned expenditure - £1.032m
• Extended Operational Hours of Ambulatory Emergency
(Medical) Clinic (AEC) • Establishment of Surgical Ambulatory Care Service. • Identification and focused management of frail elderly patients
through Occupational Therapy assessment in the Emergency Department.
• Redirection of patients attending the Emergency Department. • Application of the Daily Dynamic Discharge Approach • Additional bed capacity (56 beds)
• Provision of a safe and effective response to
surges in inpatient activity. • Avoid /reduce unnecessary emergency
admissions. • Reduction in Length of Stay. • Proactive and timely discharge planning to
support patient flow. • Increased weekend discharge rates.
Health and Social Care Partnerships Aberdeen City HSCP Aberdeenshire HSCP Moray HSCP Winter Planning Allocation - £501,120
• A Respiratory Bundle of focused interventions delivered across all HSCP communities to support self management of adults with COPD.
• Dedicated Social work resource within the Emergency Department (ARI) to provide patient assessment and access to expertise on community based resources.
• H&SCP Social work presence in the Integrated discharge Hub over the festive period public holidays to ensure ongoing assessment and discharge planning of complex discharges
• Provision of rapid response community based In and Out of Hours support services (including OT & PT) providing augmented care in patient’s homes, supporting discharge and end of life care.
• Provision of Nursing Home “step –up” beds in addition to Community Hospital inpatient capacity (4 in Aberdeen City and 2 in Elgin)
• Increase effective self-management of adults with COPD.
• Preventing unnecessary acute hospital admissions.
• Maintain patients safely at home or in a community setting.