Gram positive rods
132
GRAM POSITIVE RODS
-
Upload
syed-azfar-hussain-bokhari -
Category
Health & Medicine
-
view
119 -
download
6
Transcript of Gram positive rods

GRAM POSITIVE RODS
CLASSIFICATION Spore forming
1. Anaerobic• Clostridia
2. Aerobic• Bacillus species
Non spore forming1. Corynaebacteria.2. Listeria 3. Eryspilothrix.4. Eubacterium 5. Lactobacillus 6. Arachania7. Arcanobacterium 8. Bifidobacterium
9. Gardenalla (gram variable).
10. Mobiluncus 11. Sarcina
Branching 1. Actinomycetes
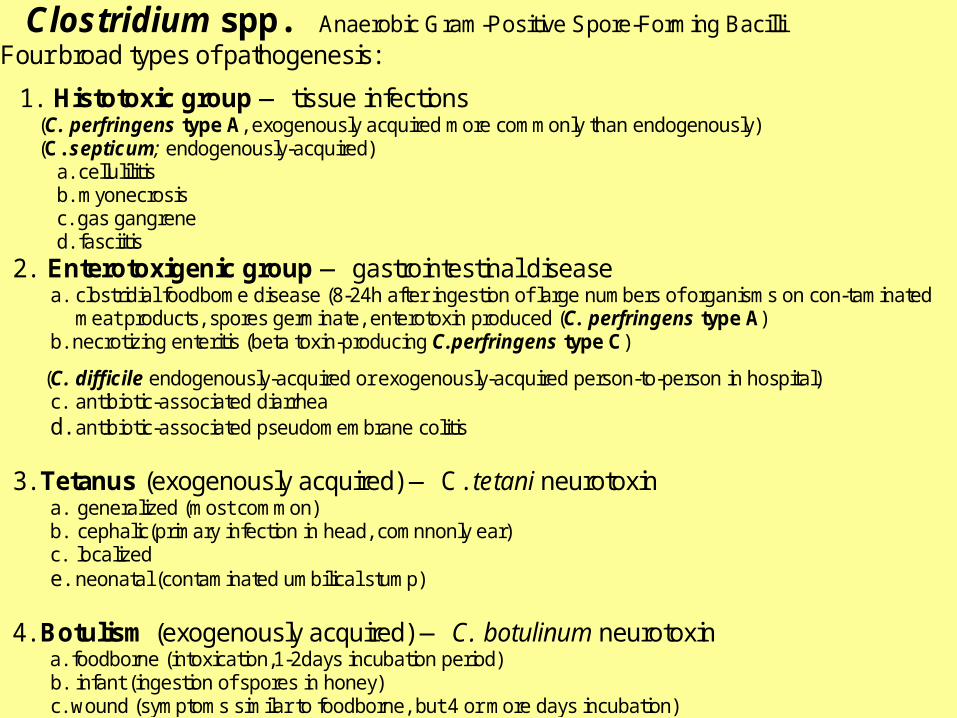
Clostridium spp. Anaerobic Gram-Positive Spore-Forming Bacilli Four broad types of pathogenesis:
1. Histotoxic group — tissue infections (C. perfringens type A, exogenously acquired more commonly than endogenously) (C. septicum; endogenously-acquired)
a. cellulilitis b. myonecrosis c. gas gangrene d. fasciitis
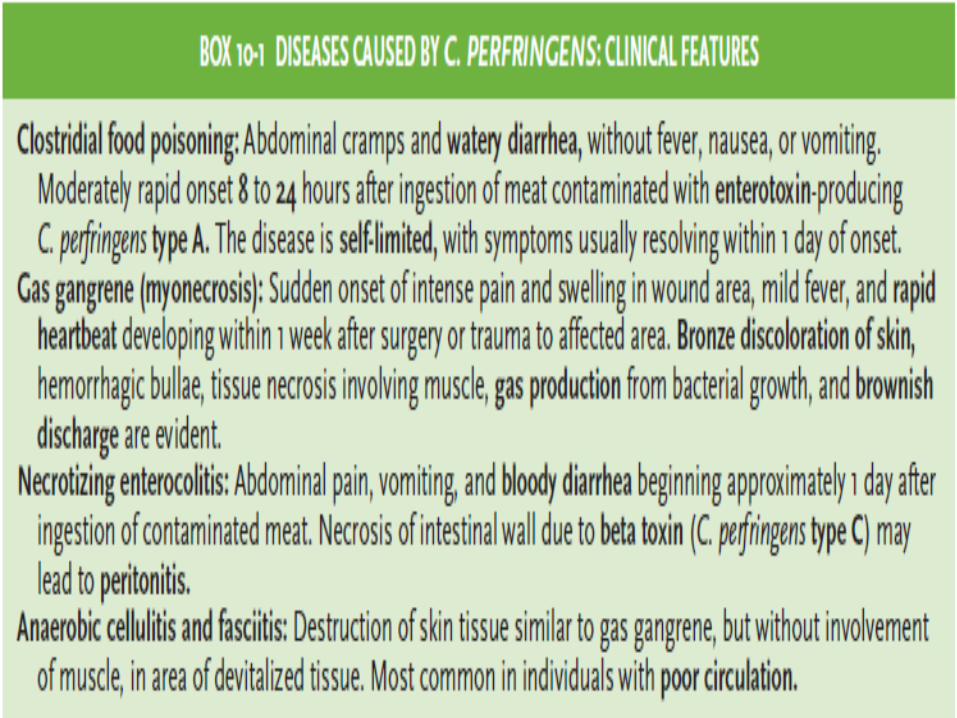
2. Enterotoxigenic group — gastrointestinal disease a. clostridial foodbome disease (8-24h after ingestion of large numbers of organisms on con-taminated
meat products, spores germinate, enterotoxin produced (C. perfringens type A) b. necrotizing enteritis (beta toxin-producing C.perfringens type C)
(C. difficile endogenously-acquired or exogenously-acquired person-to-person in hospital) c. antibiotic-associated diarrhea d. antibiotic-associated pseudomembrane colitis
3. Tetanus (exogenously acquired) — C. tetani neurotoxin
a. generalized (most common) b. cephalic(primary infection in head, comnnonly ear) c. localized e. neonatal (contaminated umbilical stump)
4. Botulism (exogenously acquired) — C. botulinum neurotoxin
a. foodborne (intoxication,1-2days incubation period) b. infant (ingestion of spores in honey) c. wound (symptoms similar to foodborne, but 4 or more days incubation)

CLOSTRIDIUM SPECIES Four clostridial species are important human
pathogens:
1. C. botulinum,
2. C. difficile,
3. C. perfringens,
4. C. tetani. All are gram positive, anaerobic, spore forming
rods that are motile in their vegetative form. They are ubiquitous in soil, water, savage, dung &
human GIT.

C. PERFRINGENS

Clostridium perfringens — histotoxic or enterotoxigenic infections
Morphology and Physiology • large, rectangular bacilli (rod) staining gram-positive • spores rarely seen in vitro or in clinical specimens (ovoid, subterminal) • non-motile, but rapid spreading growth on blood agar mimics growth of motile organisms • aerotolerant, especially on media supplemented with blood • grow at temperature of 20-50°C (optimum 45°C) and pH of 5.5-8.0
Pathogenicity Determinants (note that toxins include both cytolytic enzymes and bipartite exotoxins) • four major lethal toxins (alpha (), beta (), epsilon (), and iota () toxins) and an enterotoxin • six minor toxins (delta(), theta(), kappa(), lambda(), mu(), nu()toxins) & neuraminadase • C. perfringens subdivided into five types (A-E) on basis of production of major lethal toxins • C. perfringens Type A (only major lethal toxin is alpha toxin) responsible for histotoxic and
enterotoxigenic infections in humans; Type C causes necrotizing enteritis (not in U.S.)
Lab Identification • direct smear and Gram stain, capsules upon direct examination of wound smears • culture takes advantage of rapid growth in chopped meat media at 45° C to enrich and then
isolate onto blood agar streak plate after four to six hours • gas from glucose fermentation • in vivo toxicity testing and identification of the specific toxin types involved • double zone of hemolysis on blood agar (p-hemolytic theta(e) toxin, a-hemolytic alpha(oc) toxin) • Nagler rxn; precipitation in serum or egg yolk media; oc -toxin (phospholipase C) is a lecithinase • "stormy" fermentation (coagulaltion) of milk due to large amounts of acid and gas from lactose
Diagnosis/Treatment of systemic infection — Early diagnosis and aggressive treatment essential • removal of necrotic tissue (surgical debridement) • Penicillin G in high doses if more serious infection
Of poorly defined clinical value are: • administration of antitoxin • hyperbaric oxygen (dive chamber) adjunct therapy (??inhibit growth of anaerobe??)
PROPERTIES1. Large, boxcar-shaped, aerotolerant, rapidly growing rods.2. Double zone of beta hemolysis on blood agar.3. Positive Nagler reaction (characteristic diffuse zone
around colonies grown on egg yolk agar)4. Subtypes A to E defined based on production of major
toxins. 5. Clostridium grows well at body temperature; In stressful
environments, the bacteria produce spores that tolerate extreme conditions.
6. C perfingens produce large raised colonies rest produce flat small colonies.
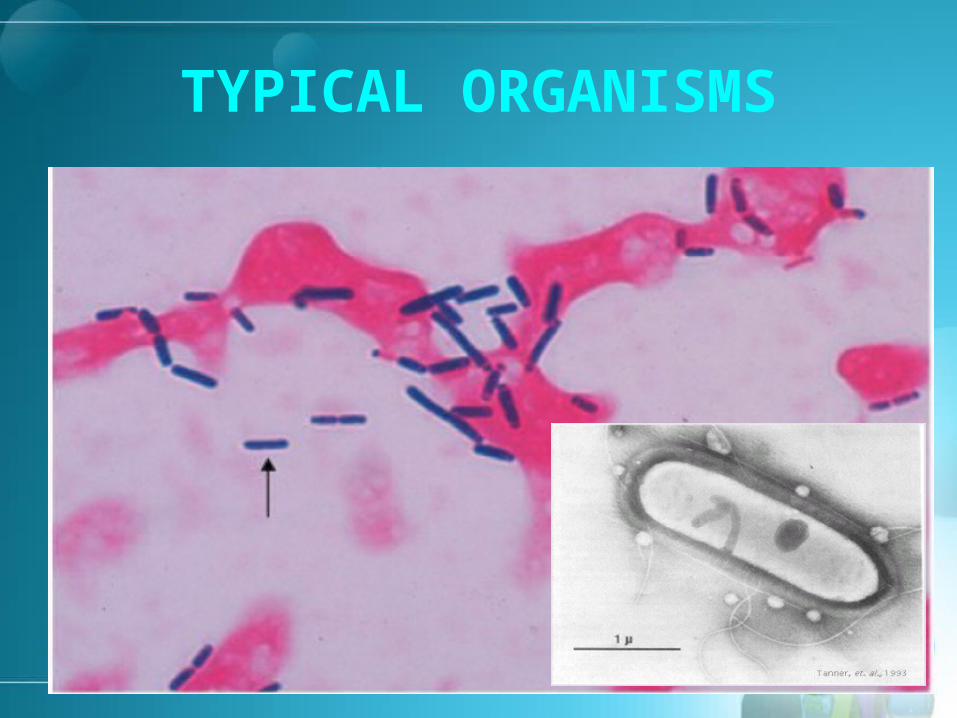
TYPICAL ORGANISMS

TYPICAL ORGANISMS

SPORES Spores are
characterized on the basis of position, size and shape
Most Clostridium spp., including C. perfringens and C. botulinum, have ovoid subterminal (OST) spores
C. tetani have round terminal (RT) spores
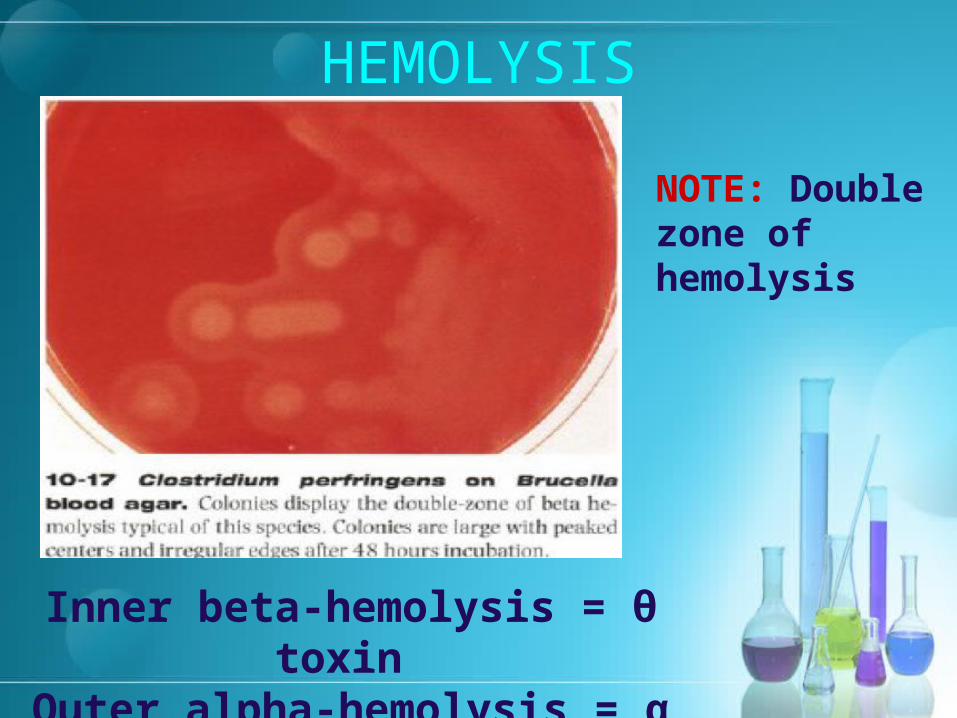
HEMOLYSIS
Inner beta-hemolysis = θ toxin Outer alpha-hemolysis = α toxin
NOTE: Double zone of hemolysis
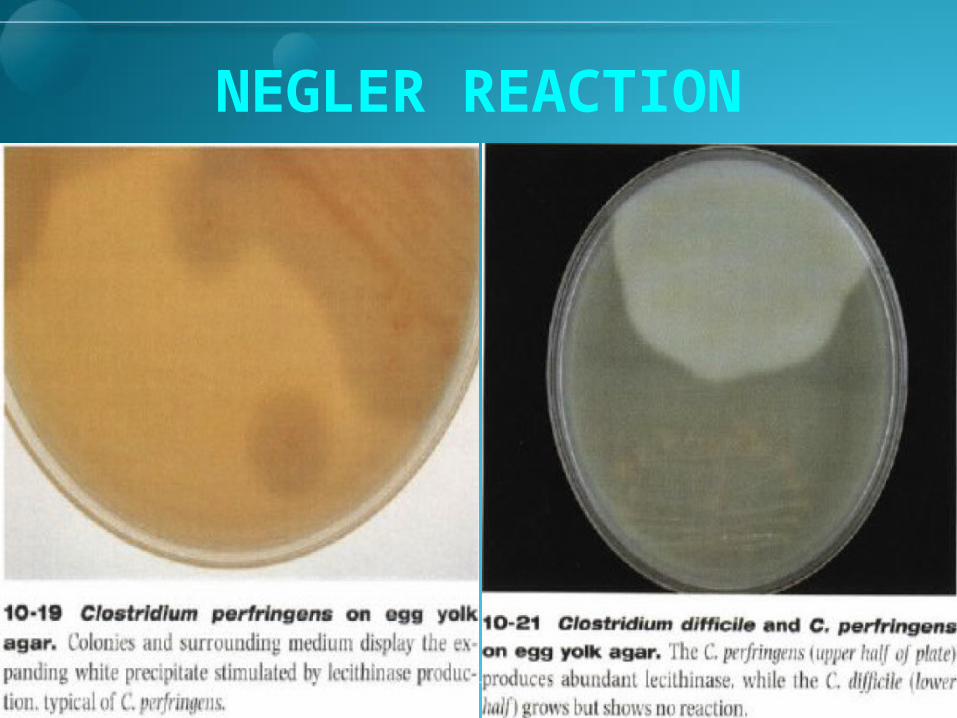
NEGLER REACTION
DISEASES Gas gangrene (clostridial myositis or
myonecrosis). (Type A)1. It can also be caused uncommonly by C. histolyticum,
C. septicum, C. novi & C sordillii.
2. C. sordillii can also cause TSS in postpartum or following an abortion.
Food poisoning (type A) Necrotizing enterocolitis (type C) Cellulitis and fasciitis

TRANSMISSION Gas Gangrene
Spores are found in the soil. Vegetative bacteria are in the human colon &
vagina. Gas gangrene is seen in wounds especially war
wounds, contaminated road side accidents. Septic abortion in the form of endometritis is.

TRANSMISSION Food Poisoning
The spores that are present in soil can contaminate food.
Spores are very heat resistant so are not activated by usual cooking. They especially grow in reheated meat products to a very large number.
Food poisoning occurs usually due to consumption of reheated meat.

Toxins
Although there are thirteen known toxins & enzymes following are inportant.
1. Alpha toxin; lecithinase splits cell membrane lecithin.
2. Theta toxin has hemolytic & necrotizing effects
3. Enterotoxin
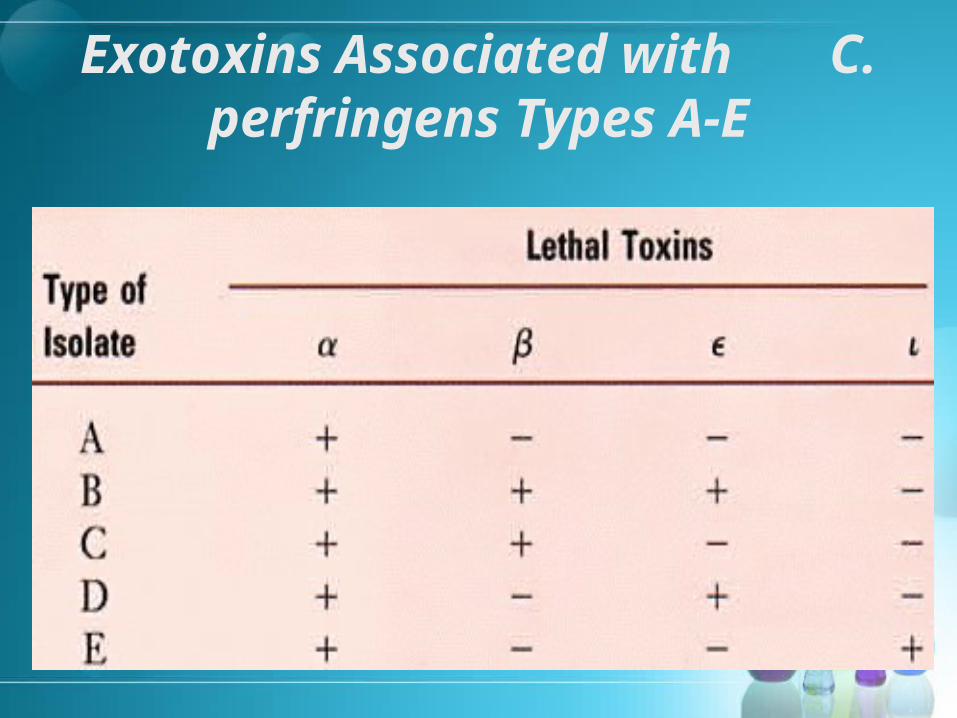
Exotoxins Associated with C. perfringens Types A-E
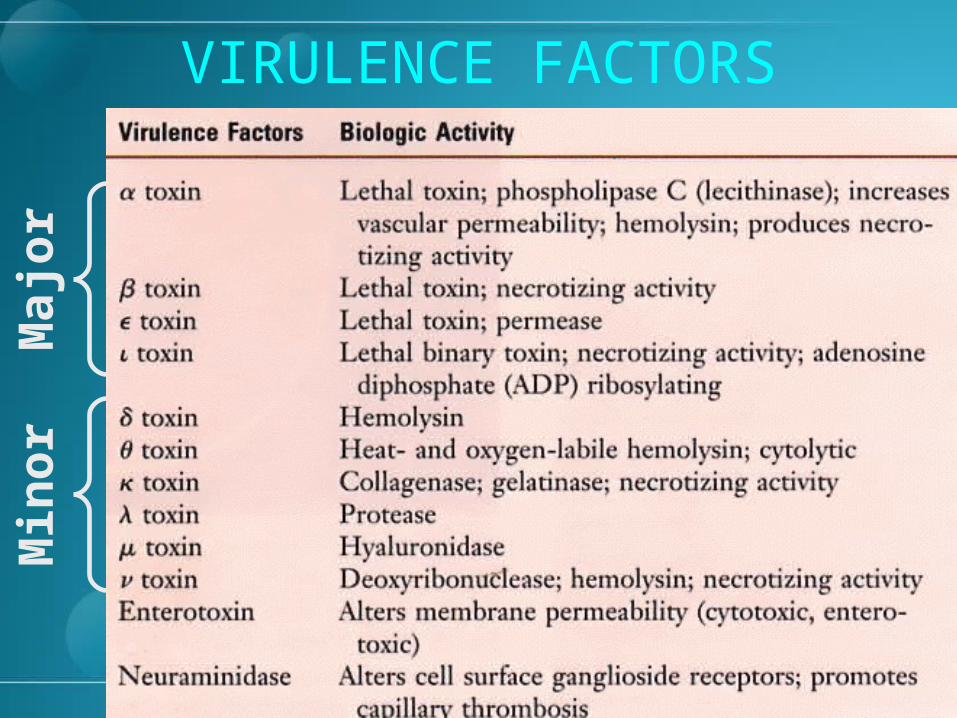
VIRULENCE FACTORSM
ajo
rM
ino
r

PATHOGENESIS Type A C. perfringens is most virulent in humans.1. Alpha toxin (phospholipase C and lecithinase),
produced by all types, causes lysis of blood cells and endothelial cells, leading to increased vascular permeability, hemolysis, and tissue destruction. When carbohydrates are fermented gas forms.
2. Hyaluronidase, collagenase, and other degradative enzymes cause tissue destruction.
3. Heat-labile enterotoxin disrupts ion transport in ileum, leading to watery diarrhea (food poisoning).
4. Beta and iota toxins have necrotizing activity.

PATHOGENESIS Spores germinate at low oxygen in traumatized
tissue. When the sachrolytic bacteria produce gas the
distension of the tissue interferes with the blood supply.
Secretion of hyaluronidase favors spread. Tissue necrosis extends leading to increased growth
hemolytic anemia, toxemia & death. Mixed infection is the rule. Bacteremia frequenly occurs in cancer patient.

CLINICAL Gas gangrene; crepetation, foul smelling discharge,
fever, hemolysis toxemia shock. CFR is 40%. Some times the superficial infection results cellulitis
& necrotizing fascitis; muscles are not involved, gas is not produced or minimally produced. Often seen in diabetics.
Food poisoning; diarrhea abdominal cramps with no fever & little nausea vomiting. Occurs 12 hours after ingestion & remains for one day.
Necrotizing enterocolitis occurs in New Guinea; there is fever cramps & peritonitis, fatal in children.

Clostridium Causing Gas Clostridium Causing Gas GangreneGangrene

CLOSTRIDIAL CELLULITIS

CLINICAL

DIAGNOSIS
Diagnosis is easily made clinically in case of gangrene.
Smears show typical organism Spores are not seen Cultured anaerobically Double zone of hemolysis Lecithinase is seen in the Negler reaction Acidifies litmus milk.
C. TETANI
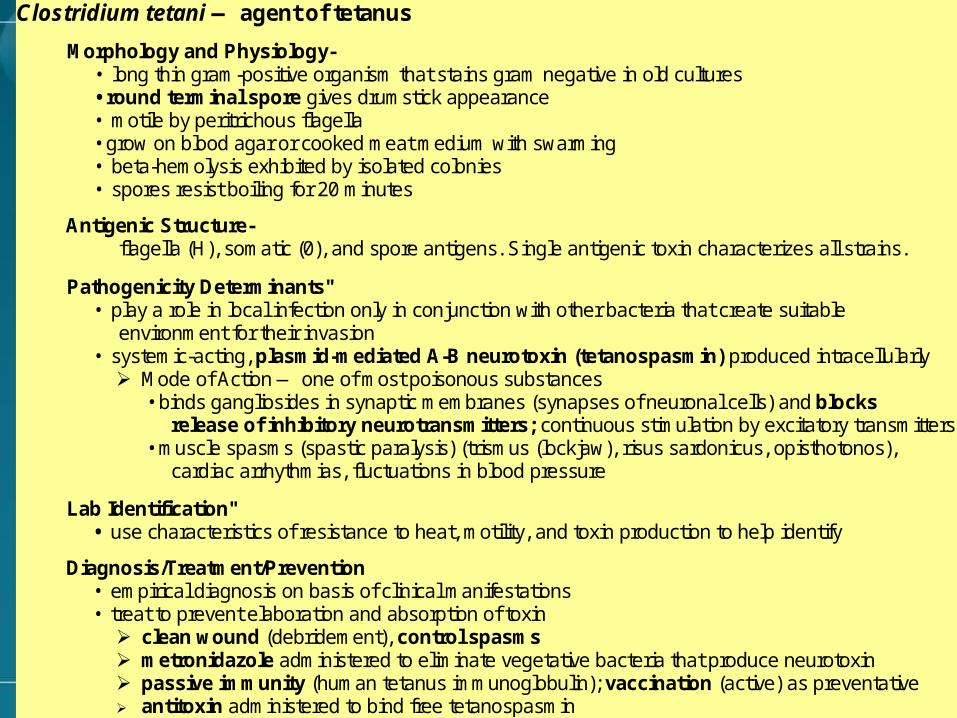
Clostridium tetani — agent of tetanus
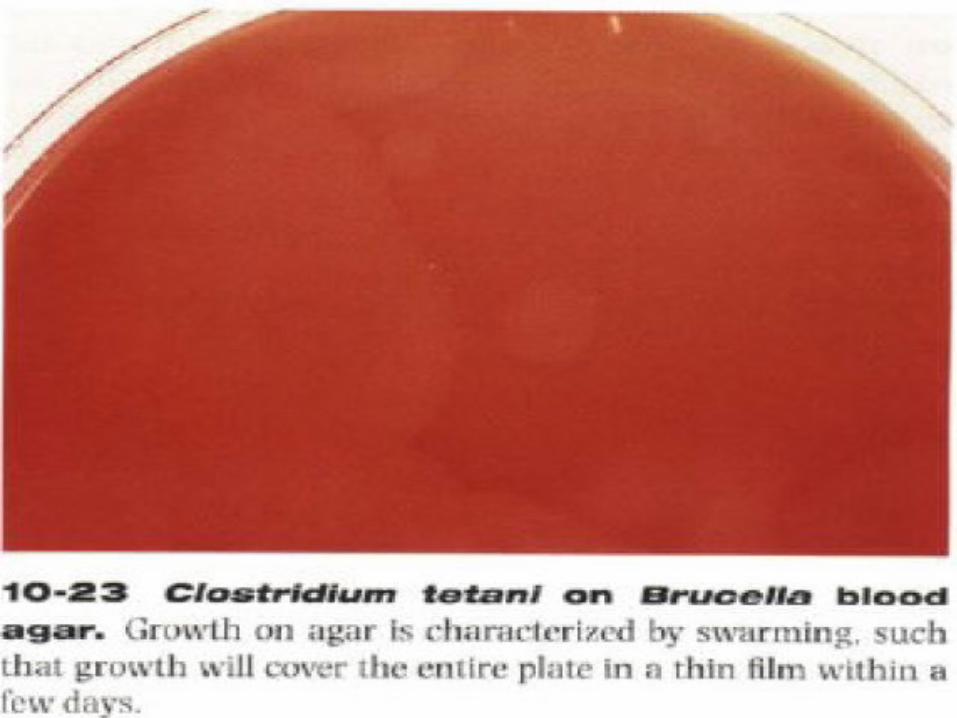
Morphology and Physiology- • long thin gram-positive organism that stains gram negative in old cultures • round terminal spore gives drumstick appearance • motile by peritrichous flagella • grow on blood agar or cooked meat medium with swarming • beta-hemolysis exhibited by isolated colonies • spores resist boiling for 20 minutes
Antigenic Structure- flagella (H), somatic (0), and spore antigens. Single antigenic toxin characterizes all strains.
Pathogenicity Determinants" • play a role in local infection only in conjunction with other bacteria that create suitable
environment for their invasion • systemic-acting, plasmid-mediated A-B neurotoxin (tetanospasmin) produced intracellularly
Mode of Action — one of most poisonous substances • binds gangliosides in synaptic membranes (synapses of neuronal cells) and blocks
release of inhibitory neurotransmitters; continuous stimulation by excitatory transmitters • muscle spasms (spastic paralysis) (trismus (lockjaw), risus sardonicus, opisthotonos),
cardiac arrhythmias, fluctuations in blood pressure
Lab Identification" • use characteristics of resistance to heat, motility, and toxin production to help identify
Diagnosis/Treatment/Prevention • empirical diagnosis on basis of clinical manifestations • treat to prevent elaboration and absorption of toxin
clean wound (debridement), control spasms metronidazole administered to eliminate vegetative bacteria that produce neurotoxin passive immunity (human tetanus immunoglobulin); vaccination (active) as preventative antitoxin administered to bind free tetanospasmin

Clostridium tetani Gram Stain
NOTE: Round terminal spores give cells a “drumstick” or “tennis racket” appearance.

Summary of Clostridium tetani Infections

DISEASES
Generalized tetanus Local tetanus Cephalic tetanus Neonatal tetanus

PROPERTIES Motile rods move with the help of a flagella. Show swarming on blood & cooked meat
cultures. Exhibit beta hemolysis in colonies that are
smaller than those of C perfringens. Aerotolerant and can grow in aerobic
conditions but spores are formed under anaerobic conditions.
Spores are resistant to boiling for 20 minutes.


ANTIGENIC STRUCTURE
They all produce same type i.e. of single serologic type of toxin; tetenospasmin so antitoxin is also of only one serotype.
All have a common somatic O antigen Can be typed on the basis of
1. Flagler H
2. Spore antigen.

TOXINS
Only the vegetative cells produce the toxin. Initially a large molecule is cleaved by the
bacterial proteases. It binds to receptors on the presynaptic
membranes at the local nerve endings & then migrates to the CNS.

EPIDEMIOLOGY
Spores are well spread in the soil & feces of horses & other animals.
Entry occurs through a wound in generalized &localized tetanus.
Addicts receive this through skin popping, Neonates receive it through the contaminated
umbilicus or circumcision wound. CNS disease develops through most
commonly an ear infection (rare).
EPIDEMIOLOGY Transmission Prognosis Incidence
Generalized Wounds Skin popping Idiopathic.
CFR is 50% with treatment
Common form
Localized Wounds Good prognosis but it may precede the generalized form.
Most common form
Neonatal Umbilical cord usually but can also occur through circumcision wound.
Very poor Rare usually seen in neonates who’s mother were not immunized
Cephalic Usually through an ear infection
Very poor Rare

PATHOGENESIS The organism is not invasive & the infection remains
localized in the area of devitalized tissue. The germination of spores is assisted by necrotic tissues,
calcium salts & associated pyogenic infections. The spores germinate at the site of infection & form
vegetative cells. The disease is mediated by an exotoxin tetanospasmin;
produced by vegetative cells. After production it moves by retrograde axonal flow to CNS In CNS it binds to the ganglioside receptors & block the
release of inhibitory transmitters glycine & GABA, It has only one antigenic type.

Mechanism of Action of Tetanus Toxin

CLINICAL FEATURESGeneralized disease; (incubation 4 days to weeks)1. Involvement of muscles
• Bulbar muscles; lockjaw, Risus Sordonicus, difficulty in swallowing,
• Involvement of skeletal muscles; Opisthotonos.• The patient is fully conscious & pain is severe. • Death is due to respiratory failure. CFR is 50%.
2. Involvement of autonomic nervous system• Sweating • Hyperthermia• Cardiac arrhythmias • Fluctuation in blood pressure.

Risus Sardonicus in Tetanus Patient

Opisthotonos in Tetanus Patient
CLINICAL FEATURES Localized disease
1. Spasm in the muscles of the area of initial injury.2. May proceed to generalized disease.
Neonatal disease;1. Generalized disease in the neonates. 2. A septic umbilical stump is usually seen & mother
will not be having immunization. CNS disease;
1. There is isolated or combined involvement of cranial nerves but the 7th nerve is most commonly involved.
2. An infection can commonly be found in ear or there is a history of such infection.
3. The prognosis is extremely poor.

DIAGNOSIS Usually the lab is not asked & the diagnosis is made
on the clinical grounds only. There is history of injury in 50% of cases means that
the injury may be so trivial that the patient does not remember.
Microscopy can reveal both forms vegetative & spores. Typical tennis racket or drum stick appearance is suggestive of the C tetani.
Neither the toxin nor antibody is elaborated. DD includes strychnine poisoning.

CLOSTRIDIUM BOTULINUM

Diseases
Classic food-borne botulism Infant botulism
Properties Gram positive spore forming rod Spores are heat resistant. Motile with flagella Strict anaerobes Fastidious growth requirement, There are seven botulism toxins A-G The disease causing organisms show following properties
1. Lipase is present,
2. Milk proteins are digested
3. Gelatin is liquefied.
4. Glucose is fermented.

Epidemiology
It is worldwide in distribution. Found in soil & animals feces. Disease is caused by ingestion of smoked
canned meat predominantly. Honey may be responsible for infantile
botulism. The spores are heat resistant.

TOXIN
There are seven distinct toxins. A-G. A,B, E or rarely F are principal toxins. Type E is particularly associated with fish
porducts. It is protein & an exotoxin. It inhibits the release of Ach. The toxin is destroyed by boiling for 20
minutes.
PATHOGENESIS It is an intoxication & results from ingestion of preformed
toxin in the food. Commonly occurs from ingestion of spiced, smoked,
canned, vacuumed, alkaline food that are eaten without cooking.
The anaerobic conditions in such foods cause germination of spores & the vegetative bacteria produce toxins.
The toxin inhibits the release of Ach at the neuromuscular junction.
There is flaccid paralysis is contrast to tetanus where there is spastic paralysis.
Death results from respiratory failure.
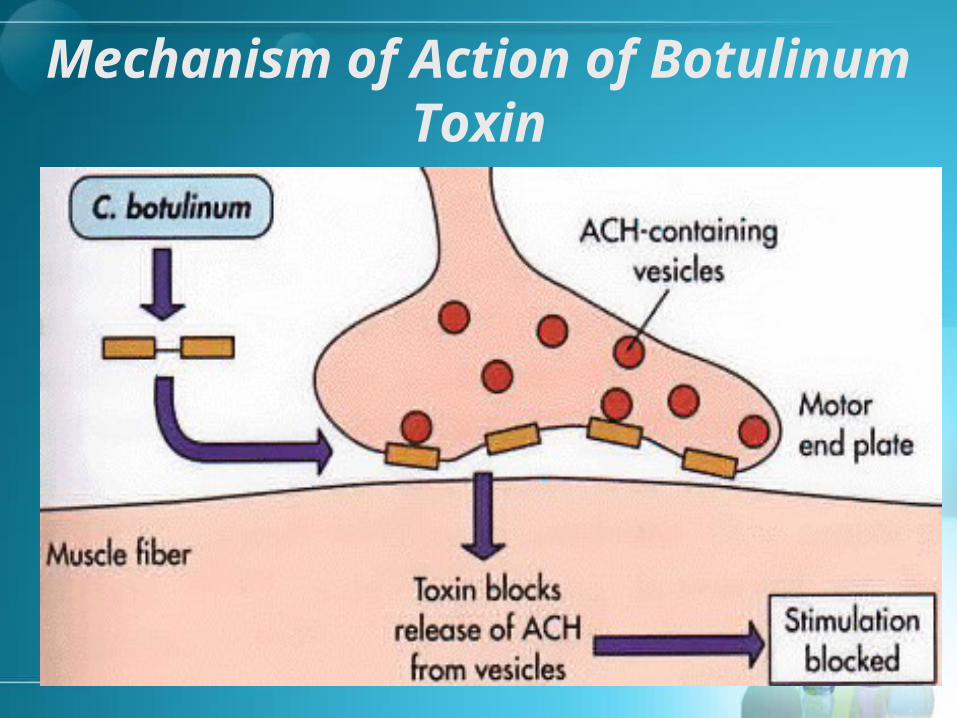
Mechanism of Action of Botulinum Toxin

CLINICALClassic food-borne botulism 18 to 24 hours incubation is followed by. Early Symptoms;
1. GIT symptoms are although not regularly present but if occur are the first symptoms, include nausea vomiting constipation.
2. Followed by dizziness, lassitude & weakness. Late symptoms;
1. Diplopia.2. Flaccid paralysis3. Dysphagia.4. Difficulty speaking5. Respiratory failure & death.
Untreated cases are sure death.

CLINICAL
Infantile botulism Occurs In the first month of life. Develop poor feeding & weekness. Followed by flaccidity “floppy baby syndrome” It is one cause of SIDS. Honey has been implicated as a cause of the
disease. Infants recover with supportive therapy in most
cases.
Diagnosis
Toxin is found in the 1. Serum
2. Remaining food.
Antigenic type of toxin is elaborated by using specific antitoxin in mice.
The organism may be isolated from the remaining food.
The organism can be detected in feces.
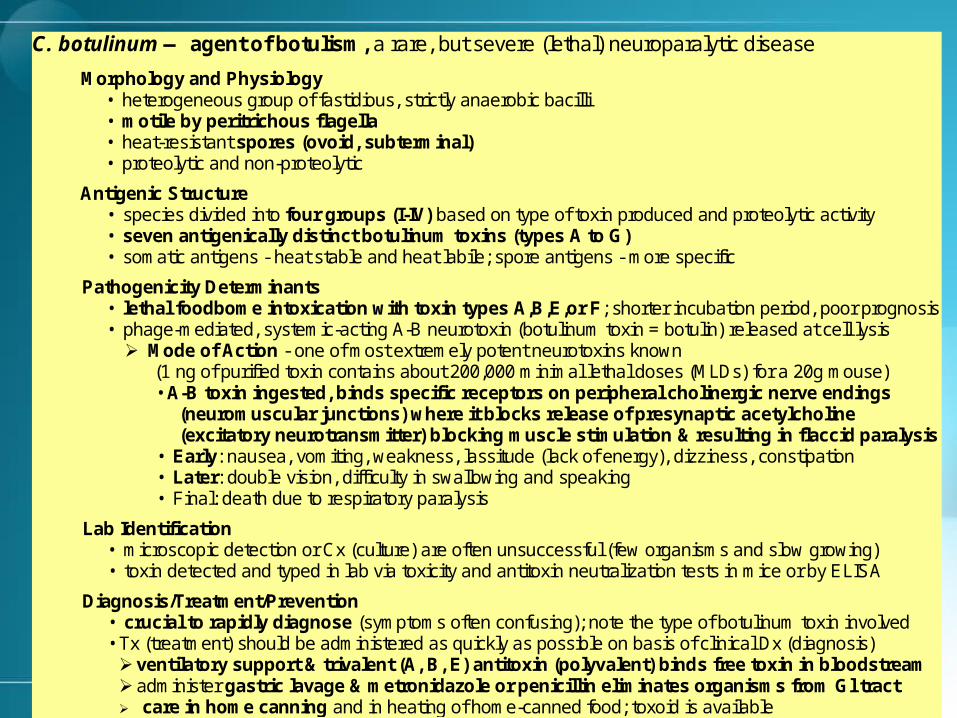
C. botulinum — agent of botulism, a rare, but severe (lethal) neuroparalytic disease
Morphology and Physiology • heterogeneous group of fastidious, strictly anaerobic bacilli • motile by peritrichous flagella • heat-resistant spores (ovoid, subterminal) • proteolytic and non-proteolytic
Antigenic Structure • species divided into four groups (I-IV) based on type of toxin produced and proteolytic activity • seven antigenically distinct botulinum toxins (types A to G) • somatic antigens - heat stable and heat labile; spore antigens - more specific
Pathogenicity Determinants • lethal foodbome intoxication with toxin types A,B,E,or F; shorter incubation period, poor prognosis • phage-mediated, systemic-acting A-B neurotoxin (botulinum toxin = botulin) released at cell lysis
Mode of Action - one of most extremely potent neurotoxins known (1 ng of purified toxin contains about 200,000 minimal lethal doses (MLDs) for a 20g mouse) • A-B toxin ingested, binds specific receptors on peripheral cholinergic nerve endings
(neuromuscular junctions) where it blocks release of presynaptic acetylcholine (excitatory neurotransmitter) blocking muscle stimulation & resulting in flaccid paralysis
• Early: nausea, vomiting, weakness, lassitude (lack of energy), dizziness, constipation • Later: double vision, difficulty in swallowing and speaking • Final: death due to respiratory paralysis
Lab Identification • microscopic detection or Cx (culture) are often unsuccessful (few organisms and slow growing) • toxin detected and typed in lab via toxicity and antitoxin neutralization tests in mice or by ELISA
Diagnosis/Treatment/Prevention • crucial to rapidly diagnose (symptoms often confusing); note the type of botulinum toxin involved • Tx (treatment) should be administered as quickly as possible on basis of clinical Dx (diagnosis) ventilatory support & trivalent (A, B, E) antitoxin (polyvalent) binds free toxin in bloodstream administer gastric lavage & metronidazole or penicillin eliminates organisms from Gl tract care in home canning and in heating of home-canned food; toxoid is available

C. DIFFICILE
Diseases
Antibiotic associated diarrhea Pseudomembranous colitis.

Properties Gram positive spore forming rod. Strict anaerobe. Potency disk pattern cultures are seen. Toxin production
1. Produce toxin A an enterotoxin binds to the brush border & is cytotoxic. It causes hemorrhagic necrosis.
2. Toxin B destroys actin & hence disrupts the cytoskeleton.
3. Both are exotoxins.
Enzymes 1. Hyaloronidase
Spores are commonly found in the hospital environment.



Epidemiology 5% of healthy individuals reside them in the colon Antibiotic therapy increases the growth & overgrowth
can result in disease. Spores are commonly found in the hospital
washrooms, beds, & is a serious source of nosocomial infections.
Commonly involve antibiotics are ampicillin amoxacillin, clindamycin & the third generation cephalosporins.
Risk factors for C. difficile–associated colitis include advanced age & hospitalization.
PATHOLOGYPseudomembranous colitis Disruption of the normal colonic flora by antibiotics allows
C. difficile overgrowth. The organism attaches to the brush border. Starts produce toxins that disrupt the mucosal barrier. Inward spread of the organism produce an inflammatory
response so intense that the exudate & necrotic debris sprout out into the lumen (volcanic eruption).
This debris form a carpet over the lumen giving the appearance of a membrane called pseudomembrane.

Antibiotic-Associated Colitis

CLINICAL
There is watery or bloody diarrhea following an antibiotic administration.
Associated with abdominal cramps fever, leukocytosis.
On endoscopy a reddish brown colored membrane with microabcesses is seen.
Diagnosis is made by isolating the organism & demonstrating the toxins.

BACILLUS SPECIES Bacillus anthracis Bacillus cereus

Bacillus anthracis
Causes Anthrax that is common in animals & uncommon in humans.
Cutaneous, pulmonary & GIT disease occur. The organism can be used in bioterrorism. It was used in the US in 2001 in mail powder
& there were 18 cases & 5 of them died.
Properties
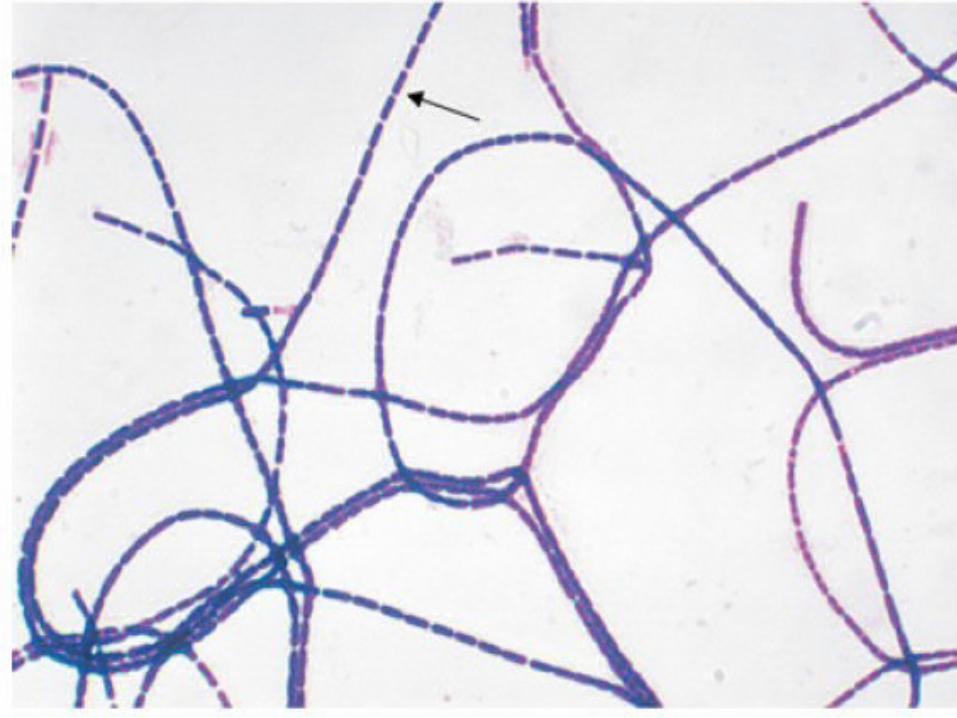
Large, gram-positive, aerobic, spore-forming rods that produce exotoxins.
Central spores that develop under all conditions except in the living body.
Nonmotile (unlike other bacilli) Forms Medusa’s head colonies on blood agar that are not
hemolytic. Capsule composed of glutamic acid polymer. The capsule is antiphagocytic. Anthrax toxins is encoded by a plasmid.



EPIDEMIOLOGY Spores are found on animals bristles & wool &
persist in soil for years. Humans get the infection usually from an animal
contact. Spores can also be inhaled. Contaminated meat ingestion leads to GIT anthrax. Inhalation anthrax is not communicable from person
to person. After inhalation the spores move to lymph nodes where they cause hemorrhagic mediastinitis.
Pathogenesis Based on the production of two exotoxins collectively
called anthrax toxin.1. Edema factor2. Lethal factor.
Each toxin has two subunits A & B.1. A is active unit is an enzyme.2. B is the binding unit is preventive.
Edema factor is adenylate cyclase that increases the intracellular cyclic AMP. It outpores the fluid into the tissues leading to edema.
The lethal factor is a protease that cleaves the phosphokinase & totally inhibits cell growth.
Antibodies against these toxins are protective so these are called protective antigens.
Pathogenesis The typical lesion of cutaneous anthrax is a painless
ulcer called black eschar. It is black with local edema. It is called malignant pustule. Untreated cases can lead to bacterimia & death.
Pulmonary anthrax is called woolsters disease. It starts as influenza like disease & rapidly spreads to cause hemorrhagic mediastinitis followed by pleural effusion shock & death.
Abdominal pain, nausea vomiting & bloody diarrhea are the symptoms of the GIT disease.

Clinical Presentation of Anthrax Cutaneous Anthrax
95% human cases are cutaneous infections 1 to 5 days after contact Small, pruritic, non-painful papule at inoculation site Papule develops into hemorrhagic vesicle & ruptures Slow-healing painless ulcer covered with black eschar
surrounded by edema Infection may spread to lymphatics w/ local adenopathy Septicemia may develop 20% mortality in untreated cutaneous anthrax
Clinical Presentation of Anthrax Inhalation Anthrax
– Virtually 100% fatal (pneumonic)– Meningitis may complicate cutaneous and inhalation
forms of disease– Pharyngeal anthrax
• Fever
• Pharyngitis
• Neck swelling

Clinical Presentation of Anthrax Gastrointestinal (Ingestion) Anthrax
– Virtually 100% fatal – Abdominal pain– Hemorrhagic ascites– Paracentesis fluid may reveal gram-positive rods
DIAGNOSIS
– Smears with no spores & no motility gram positive cocci in chains.
– Culture show non hemolytic colonies.– PCR is used in special labs in cases of terrorism.– Direct fluorescence– ELISA can also be used for detection.

Key Characteristics to Distinguish between B. anthracis & Other Species of
Bacillus
– Characteristic Bacillus anthracis Other Bacillus spp.– Hemolysis Neg Pos– Motility Neg Pos (usually)– Gelatin hydrolysis Neg Pos– Salicin fermentation Neg Pos– Growth on PEA
blood agar Neg Pos

Bacillus cereus

Diseases
Food poisoning

Properties
Microscopically very similar two bacillus anthracis but are motile may be gram variable.
Cause hemolysis on blood agar in contrast to B anthracis.
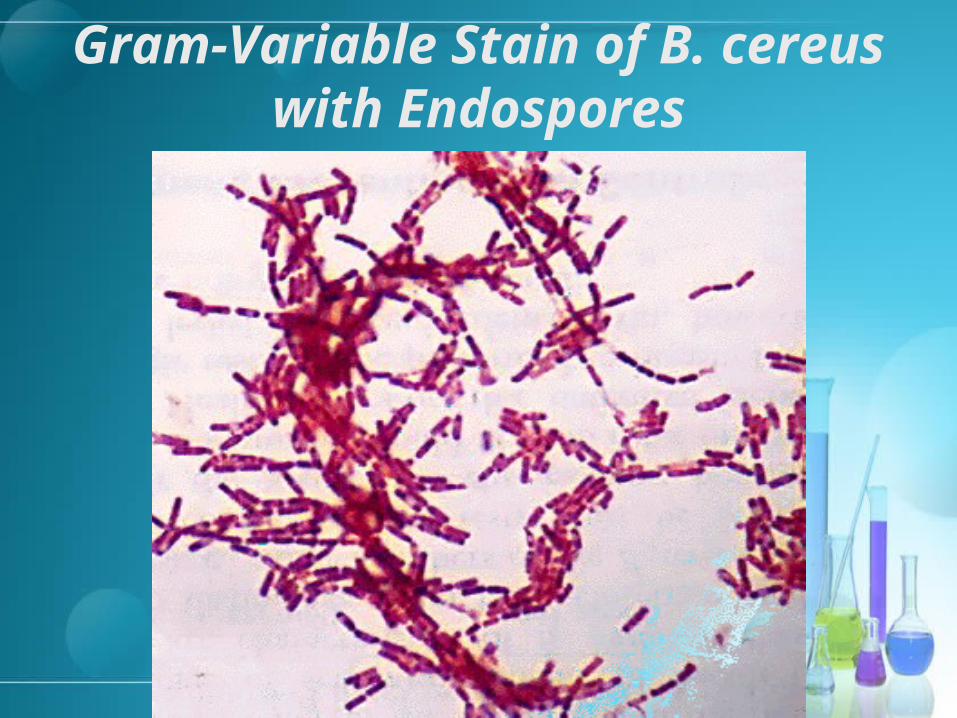
Gram-Variable Stain of B. cereus with Endospores

Transmission
Spores on grains resist steaming & rapid frying.
The spores germinate when kept for some hours. Reheated fried rice.
Portal is GIT.
Pathogenesis
Produce two enterotoxxins. One of them acts similar to cholera toxin as it
ribosylates the the G protein to stimulate adenylate cyclase. This leads to increase in cAMP in the enterocytes leading to diarrhea.
Other toxin is a superantigen.

Clinical
To type of food poisonings occur.
1. One with vomiting incubation 4 hours.
2. One with watery diarrhea incubation 18 hours.
Rarely ocular infection can result pertaining to eye injury.

Lab diagnosis
Not done

Actinobacteria
Introduction The Phylum Actinobacteria is a large group of
Gram-positive bacteria. Some are acid fast e.g. Nocardia This group of bacteria has a high content GC bases
in the DNA. Actinobacteria are known for their production of
secondary metabolites that have been used for medical purposes
Mycobacteria also belong to this phylum but will be discussed separately as they are not gram positive & have very different characteristics.

Medically Important Organisms
Two bacteria are of medical importance in this phylum belong to family Actinomycetes
1. Actinomyces israelii
2. Nocardia astroiditis.

Actinomyces israelii Properties
They are anaerobes & are part of the normal oral fauna. They can also be seen in GIT & genital tract.
They grow best in high carbon dioxide concentration They are fastedious & require enriched media. While individual bacteria are rod-shaped, the colonies
form fungus-like branched networks of hyphae These hyphae develop into cobweblike colonies that
later become heaped up to give a typical molar tooth colonies.
They give a hard abcess that is called sulfur granule.

Bacteria in filamentous growth

Organism in tissue

Sulfur granules
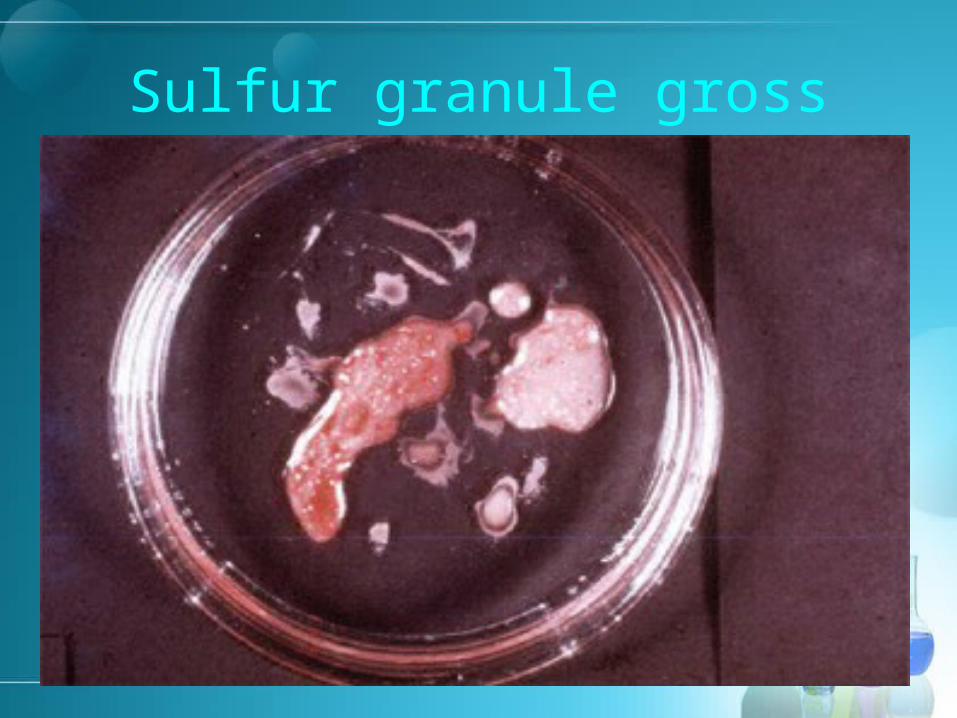
Sulfur granule gross

Cobweb colony
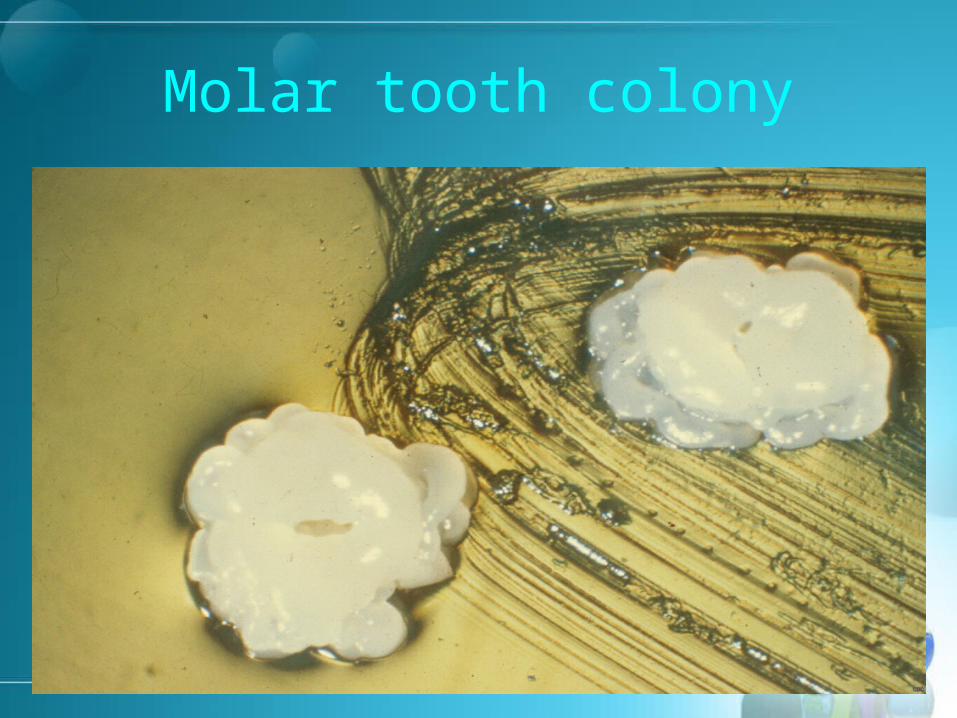
Molar tooth colony

Pathology
After a local oral trauma like broken jaw or tooth extraction the bacteria starts progressing.
They invade the tissue & form long filaments. The filaments are surrounded by area of
inflammation. There is also pus which forms hard yellow
granular mass called sulfur granule.

Clinical The disease is a hard non tender abscess. It develops slowly & then drains into sinuses. In 50% cases the initial lesion involves the face & neck. Other common area is the chest & abdomen. Pelvic disease can also occur but seen in women who use
IUDs. Uncommonly there are musculoskeletal lesions &
endocarditis, Meningitis, encephalitis, brain abscess & disseminated
disease & cutaneous are rare. The disease is not communicable.

Facial Actinomycosis

Facial Actinomycosis

Thoracic Actinomycosis

Cutaneous Disease
Diagnosis
It is made by seeing branching rods that are gram positive under the microscope.
Sulfur granule. Culturing under anaerobic conditions. Immunofluroscense.
Nocardia astroiditis
Properties Gram positive rods that form thin filaments May be weekly acid fast So dilute acid is used to decolorize them; use of
strong acid totally decolorizes them.

Nocardia Filaments

Nocardia colonies
Nocardia astroidis
Clinical It causes pneumonia, lung abcess, with cavity
formation, nodules or Empyma. It then can spread to various organs
particularly brain where it can cause abscess. More commonly the disease is seen in
immunocompromised. Mycetoma is caused by nocardia brasillenisis
in tropical countries.

Mycetoma

Actinomyces Nocardia
Gram stain: Filamentous, GPB Filamentous GPB
Modified AFB: Negative Positive (weakly)
Source: Mouth flora Soil
Diseases Facial abdominal thoracic pelvic disease commonly
Decreased cell mediated immunity leading to pulmonary infections
Clinical features:
Indurated, fistula sulfur granules
Indurated no sulfur granules
Course: Indolent Indolent
Growth condition
Anaerobic Aerobic
Corynebacterium
PROPERTIES Corynebacterium diphtheria is the organism that
causes diphtheria Gram positive aerobic rods. Individual organism appears club shaped. They are arranged in palisade in either V or L forms. They have beaded appearance & the bead consists
of highly polymerized phosphate. They are of high energy
They stain metachromatically & the stain that stains them blue or greenish stains the bead red.
Together they appear like Chinese letters.


Arrangement of C. diphtheria




Epidemiology
Humans are natural host Both toxigenic & nontoxigenic strains reside
in the human upper respiratory tract. The disease is transmitted by airborne
droplets. The organism can infect the preexisting
wounds or lesions seen commonly in the tropical countries.

Pathogenesis It causes disease by both invasion & toxin
production. The organism first adheres to the throat. It then produces toxins. Which acts as follows.
1. The toxin is an exotoxin & has two domains.2. One domain binds to the cell membrane glycoprotein.3. The other domain ADP ribosylates the elongation
factor 2 (EF2) thus inactivating it as it is enzymatic.4. This inhibits the protein synthesis.5. It effects all the eukaryotic cell regardless of types.6. The toxin production is transmitted by a lysogenic
phage & bacteria that are not lysogenised are not pathogenic.

Pathogenesis The host response.
1. A local inflammatory reaction takes place.
2. The exudate is fibrinous.
3. This exudate forms a grey colored pseudomembrane on the surface of the throat.
4. This membrane is thich hard & adheres firmly two the underlying tissue.
5. When removed the surface bleeds.
6. Antibody against this toxin is protective.

Clinical features The disease is still a problem in the developing countries. Rarely seen before the age of 1 because of maternal
antibodies. Peak 1-5 years, 5-10 years- decreases thereafter.Peak 1-5 years, 5-10 years- decreases thereafter. There is fever, chills, hoarseness of voice, sore throat, nasal There is fever, chills, hoarseness of voice, sore throat, nasal
discharge, malaise, lethargy & lymphadenopathy.discharge, malaise, lethargy & lymphadenopathy. Within two to three days, a thick coating can Within two to three days, a thick coating can build up in thebuild up in the
throatthroat. This makes it difficult to breath & swallow. On clinical examination there is a thick membrane over the
throat that if pulled leads to bleeding. The toxin may be absorbed into the blood stream and
may cause damage to the heart, kidneys and nerves.
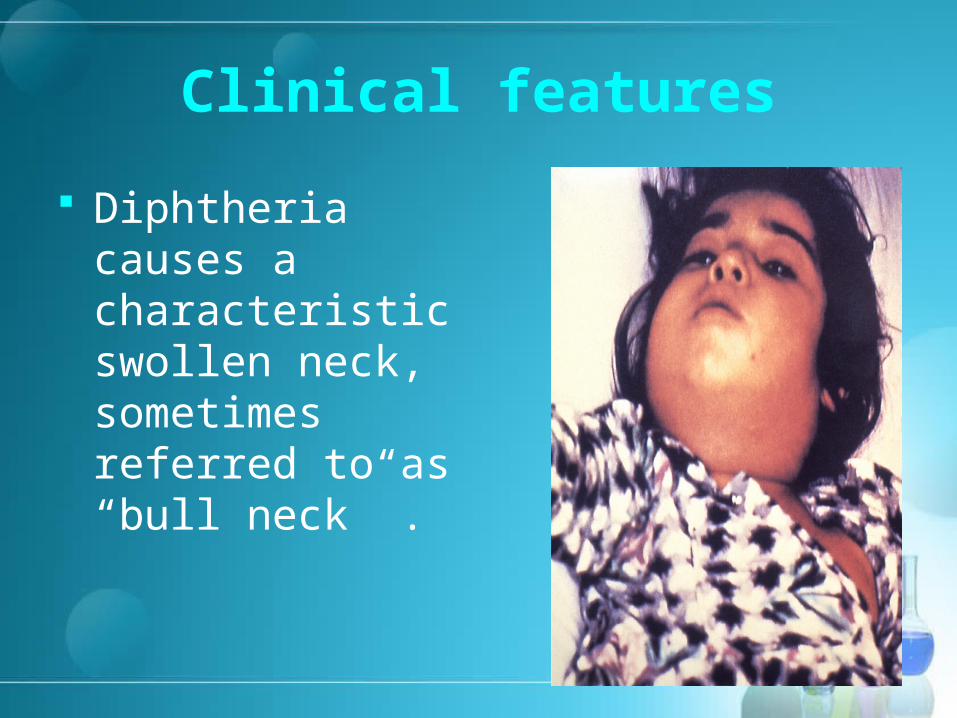
Clinical features
Diphtheria causes a characteristic swollen neck, sometimes referred to as “bull neck” .


Skin (cutaneous) diphtheria
A second type of diphtheria can affect the skin, causing the typical pain, redness and swelling associated with other bacterial skin infections.
Ulcers covered by a gray membrane also may develop in cutaneous diphtheria.
Most commonly sen in the developing countries & poor hygienic states.

Skin lesion

Complications
Extension of the membrane into the airways can lead to asphyxia & cyanosis.
Myocarditis can result leading to arrhythmia & collapse.
Nerve weakness & paralysis especially of the cranial nerves.
Peripheral neuritis of the extremities can also result.

Diagnosis Throat swab is taken. Cultured on loefler’s media or tellurite plate & blood
agar. The tellurite gives black colonies diagnostic of
bacteria. A PCR can be done. Gel diffusion tests may be done. Schick’s test; a person is injected intradermally with
the antitoxin & if inflammation takes place the person is not having antibodies & should be immunized.
Treatment should not wait lab report.

Tellurite plate

Loefflers serum slope– creamy white colonies in 6-8 hrs

Blood agar give grey colonies with minimal hemolysis