
Gram positive Cocci Staphylococci Streptococci Enterococci Bacilli Bacillus Clostridia...
37
Gram positive Cocci Staphyloco cci Streptococ ci Enterococc i Bacilli Bacillus Clostridia Corynebact eria
-
Upload
russell-payne -
Category
Documents
-
view
255 -
download
18
Transcript of Gram positive Cocci Staphylococci Streptococci Enterococci Bacilli Bacillus Clostridia...
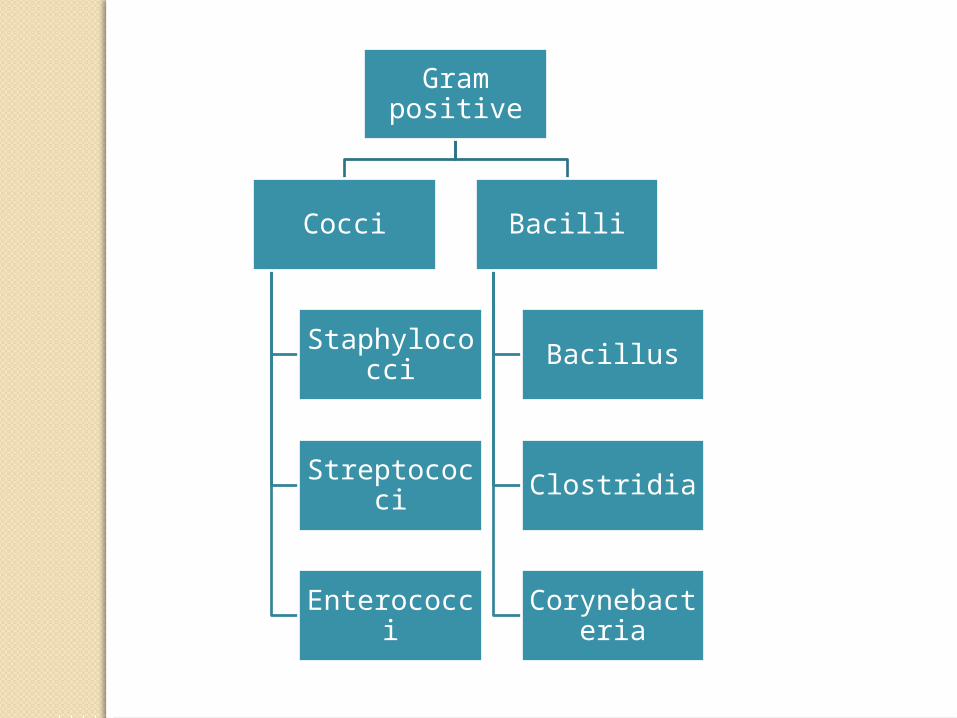
Gram positive
Cocci
Staphylococci
Streptococci
Enterococci
Bacilli
Bacillus
Clostridia
Corynebacteria


Genus Clostridium

Learning objectives:
Describe the basic microbiological features of the
genus Clostridium
Describe clinical significance of the genus Clostridium
List the most clinically important Clostridium species
List the main clinical conditions caused by C.
perfringens, C. tetani, C. botulinum and C. difficile
and describe their major virulence factors

Learning objectives:
Describe the major differences between the
main clinical conditions caused by C.
perfringens, C. tetani, C. botulinum and C.
difficile and describe the laboratory methods
used in the diagnosis of each infection
Describe in general the management of the
main infections caused by genus Clostridium

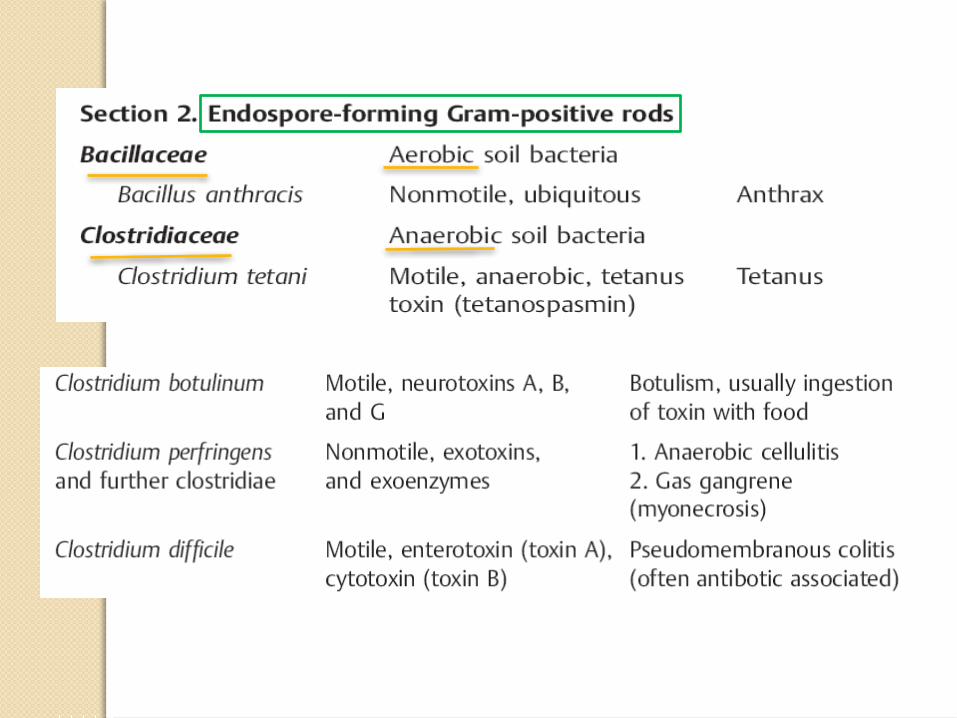
Clostridium
> 200 species and sub-species
Thick, Gram-positive, sporing rod
Strict anaerobes
Soil is natural habitat
GIT
Exotoxins and enzymes

Medically important speciesC. perfringens
◦Anaerobic cellulitis and gas gangrene (clostridial myonecrosis)
C. tetani◦Tetanus
C. botulinum◦Botulism
C. difficile◦Pseudomembranous colitis

Diagnosis of clostridial infections
Identification of the pathogen
◦Gas gangrene
Identification of the pathogen +
toxins
◦Tetanus, botulism and colitis

Morphology and culturingLarge, Gram-positive rod
Flagellated (except C. perfringens)
Sporulated
Anaerobic atmosphere at 37°C
C. perfringens colonies are convex, smooth, and hemolytic
Colonies of motile clostridia have an irregular edge

Management Penicillin GAntitoxins are used in therapy of
tetanus and botulismHyperbaric O2 is used to treat
gas gangreneThe most important preventive
measure against tetanus is active vaccination with tetanus toxoid

Gas gangrene (clostridial myonecrosis)
Anaerobic cellulitis

Pathogen spectrumClostridium perfringens
C. novyi
C. septicum
C. histolyticum

Toxins and enzymesToxins:
◦Necrotizing, hemolytic, and/or lethal activity
Enzymes:◦Collagenases, proteinases, DNases,
lecithinases, and hyaluronidase

Pathogenesis and clinical pictureFrequently contaminate open
wounds
Types of infections:
◦Anaerobic cellulitis
◦Gas gangrene (clostridial myonecrosis)

Anaerobic cellulitis
Infection restricted to the fascial spaces that does not affect musculature
There is no toxemia

Gas gangrene (clostridial myonecrosis)
An aggressive infection of the muscles
Gas, myonecrosis and toxemia
Medical emergency


Laboratory diagnosisSpecimens
Direct examination
Anaerobic culture
Identification


Clostridium tetani
(Tetanus)

Tetanus (lockjaw)
Acute clostridial disease
Clinical manifestations caused by
strong neurotoxin
(tetanospasmin)
Pathogenesis and clinical picture
Pathogens invade tissues following injuries
Toxin produced
Increased muscle tone and spasms
Diagnosis
Toxin detection in wound material
The pathogen is difficult to culture


Treatment
Anti-toxin
Wound cleaning
Muscle relaxants
Clostridium botulinum
(botulism)

Botulism
Rare but serious paralytic illness
The toxin enters the human body in one of three ways:
◦Ingestion of spores (infant botulism)
◦Toxin ingested with food (adult botulism)
◦Infected wounds (wound botulism)
Clostridium botulinum toxin
Very strong neurotoxin
Heat-labile protein
Flaccid paralysis

Clinical picture of classic botulismParalysis especially in the nerves
of the headFrequent symptoms: seeing
double, difficulty swallowing and speaking, constipation, and dry mucosa

Mortality and cause of death
Mortality: 25–70%, depending on
the amount of toxin ingested
Death usually results from
respiratory paralysis

Diagnosis and treatment
Diagnosis:
◦Toxin detection
Therapy:
◦Anti-toxin
Clostridium difficile
(pseudomembranous colitis)

Clostridium difficileFecal flora of 1–4% of healthy
adults and in 30–50% of children during the first year of life
Pseudomembranous colitis:◦Clindamycin◦Aminopenicillins◦Cephalosporins
Antibiotic-associated colitis

Pathological mechanism
Based on formation of two toxins:
◦Toxin A is an enterotoxin
◦Toxin B is a cytotoxin

Laboratory diagnosis
Isolation of the pathogen
Cytotoxin detection in stool
filtrates by cytopathic effect
ELISA for toxins “A” and “B”

Treatment
Not always required
Indicated only in severe cases
Metronidazole is the drug of choice















![[Micro] clostridia](https://static.fdocuments.in/doc/165x107/55d6fc72bb61ebfa2a8b47f2/micro-clostridia.jpg)