
Governing Body Public Meeting - East and North ... Governing... · Page 9 – Amend Cephalosporin...
506
Governing Body Public Meeting Thursday 24 th September 2015, 9:00am – 12:00pm Focolare Centre (Meeting Room 1) – Welwyn Garden City AGENDA Item Subject Report Action 1. WELCOME AND APOLOGIES FOR ABSENCE Chair - Verbal 2. DECLARATIONS OF INTERESTS To receive any new declarations of interest or declarations relating to matters on the Agenda. Chair - Verbal 3. MINUTES OF THE LAST MEETING AND MATTERS ARISING To approve the Minutes of the meeting held on 4 th June 2015. Chair Approve Enclosed 4. ACTION TRACKER To discuss the progress against the Action Tracker. Chair Discuss Enclosed 5. CHIEF EXECUTIVE’S REPORT To receive the report. Chief Executive Note Enclosed GOVERNANCE 6. GOVERNANCE REPORT To approve the report. Director of Nursing & Quality Approve Enclosed 7. INFECTION PREVENTION AND CONTROL ANNUAL REPORT To receive the report. Director of Nursing & Quality Note Enclosed FINANCE AND PERFORMANCE 8. FINANCE REPORT To receive the report. Chief Finance Officer Note Enclosed 9. INTEGRATED PERFORMANCE AND QUALITY REPORT To receive the report. Director of Nursing & Quality / Director of Operations Discuss Enclosed 10. SAFEGUARDING ANNUAL REPORTS To receive the reports: 10.1 Children 10.2 Adults Director of Nursing & Quality Note Enclosed
Transcript of Governing Body Public Meeting - East and North ... Governing... · Page 9 – Amend Cephalosporin...

Governing Body Public Meeting
Thursday 24th September 2015, 9:00am – 12:00pm Focolare Centre (Meeting Room 1) – Welwyn Garden City
AGENDA
Item Subject Report Action
1. WELCOME AND APOLOGIES FOR ABSENCE
Chair - Verbal
2. DECLARATIONS OF INTERESTS To receive any new declarations of interest or declarations relating to matters on the Agenda.
Chair
-
Verbal
3. MINUTES OF THE LAST MEETING AND MATTERS ARISING To approve the Minutes of the meeting held on 4th June 2015.
Chair
Approve
Enclosed
4. ACTION TRACKER To discuss the progress against the Action Tracker.
Chair
Discuss
Enclosed
5. CHIEF EXECUTIVE’S REPORT To receive the report.
Chief Executive
Note
Enclosed
GOVERNANCE 6. GOVERNANCE REPORT
To approve the report.
Director of Nursing &
Quality
Approve
Enclosed
7. INFECTION PREVENTION AND CONTROL ANNUAL REPORT To receive the report.
Director of Nursing &
Quality
Note
Enclosed
FINANCE AND PERFORMANCE 8. FINANCE REPORT
To receive the report.
Chief Finance Officer
Note
Enclosed
9. INTEGRATED PERFORMANCE AND QUALITY REPORT To receive the report.
Director of Nursing & Quality /
Director of Operations
Discuss
Enclosed
10. SAFEGUARDING ANNUAL REPORTS To receive the reports: 10.1 Children 10.2 Adults
Director of Nursing &
Quality
Note
Enclosed

Item Subject Report Action
POLICY, STRATEGY, CONTRACTS AND COMMISSIONING 11. PRESCRIBING REPORT
To receive the report.
Director of Strategic
Partnerships
Note
Enclosed
12. JOINT COMMITTEE CO-COMMISSIONING REPORT To receive the report.
Director of
Commissioning
Note
Enclosed
13. HOME-START To approve the recommendations.
Chief Executive
Approve
Enclosed
FOR INFORMATION 14. ANNUAL AUDIT LETTER
To receive the letter.
Chief Finance Officer
Note
Enclosed
15. COMMISSIONING FRAMEWORK REPORT To receive the report.
Director of
Commissioning
Note
Enclosed
16. EMERGENCY PREPAREDNESS, RESILIENCE AND RESPONSE (EPRR) To receive the report.
Director of Operations
Note
Enclosed
17. PUBLIC ENGAGEMENT REPORT To receive the report.
Deputy Chair
Note
Enclosed
18. GOVERNANCE & AUDIT COMMITTEE MINUTES To note the Minutes of the meeting held on 20th May 2015.
Lay Member – Governance &
Audit
Note
Enclosed
19. HBL ICT STAKEHOLDER BOARD MINUTES To note the Minutes of the meeting held on 15th June 2015.
Chief Finance
Officer
Note
Enclosed
20. JOINT COMMISSIONING PARTNERSHIP BOARD UPDATE To receive an update.
Director of Strategic
Partnerships
Discuss
Verbal
21.
ANY OTHER URGENT BUSINESS To consider any other matters which, in the opinion of the Chair, should be considered as a matter of urgency.
All
Discuss
Verbal
22. QUESTIONS FROM MEMBERS OF THE PUBLIC To receive any questions from members of the public.
-
Note
-
23. DATE OF NEXT MEETING Thursday 26th November 2015, Focolare Centre, 9:00am – 11:00am
-
-
-

Agenda Item No: 3
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Minutes of the Last Meeting
Decision Discussion Information Follow up from last meeting
Report author: Sarah Feal, Company Secretary
Report signed off by: Beverley Flowers, Interim Chief Executive
Purpose of the paper: To approve the Minutes of the meeting held on
4th June 2015.
Conflicts of Interest involved:
There are none identified.
Recommendations to the Governing Body:
To approve the Minutes.

Page 1 of 9
GOVERNING BODY PUBLIC MEETING
THURSDAY 4th JUNE 2015 FOCOLARE CENTRE FOR UNITY, WELWYN GARDEN CITY, MEETING ROOM 1
Present: Hari Pathmanathan (HP) Chair Lesley Watts (LW) Chief Executive (Accountable Officer) Alan Pond (AP) Chief Finance Officer Sheilagh Reavey (SR) Director of Nursing and Quality (Nurse Member) Beverley Flowers (BF) Director of Strategic Partnerships (left meeting 09:55am) Denise Boardman (DB) Interim Director of Commissioning Harper Brown (HP) Director of Planning and Procurement Ed Bosonnet (EB) Lower Lea Valley Locality Alison Jackson (AJ) Lower Lea Valley Locality Nabeil Shukur (NS) Stort Valley and Villages Locality Russell Hall (RH) Stevenage Locality Peter Shilliday (PS) Welwyn and Hatfield Locality Ashish Shah (AS) Welwyn and Hatfield Locality Mark Andrews (MA) Upper Lea Valley Locality Stephen Kite (SK) Upper Lea Valley Locality Fiona Sinclair (FS) North Herts Locality (left meeting at 09:45am) Linda Farrant (LF) Lay Member, Governance and Audit Dianne Desmulie (DD) Lay Member, Public and Patient Engagement
In Attendance: Sarah Feal (SF) Company Secretary (Minutes) Peter Chapman (PC) Patient Representative Michael Taylor (MT) Patient Representative Tim Napper (TN) Commissioning Manager (Carers) - Community Wellbeing,
Health and Community Services, Hertfordshire County Council (Item 9.)
Item Subject Action By 1. WELCOME AND APOLOGIES FOR ABSENCE
HP welcomed all to the meeting. Apologies were received from: Nicky Williams Deputy Chair Rob Graham North Herts Locality Prag Moodley Stevenage Locality Deborah Kearns Stort Valley and Villages Locality Dermot O’Riordan Secondary Care Specialist Doctor Sharn Elton Director of Operations
2. DECLARATIONS OF INTEREST
There were no Declarations of Interest received.

Page 2 of 9
3. MINUTES OF THE LAST MEETING AND MATTERS ARISING
The Minutes of the last meeting held on 26th March 2015 were agreed, as an accurate record, with the following amendments requested: DD advised she hadn’t left the meeting at 12:45pm, as stated Page 6, 4th Bullet – Remove Cancer Boards sentence Page 6, 6th Bullet – Amend PAH to SR Page 9 – Amend Cephalosporin to Co-Amoxiclav Page 9 – Amend BCMG to PCMMG
The Governing Body held a discussion regarding nurse revalidation and SR provided an update about the workstream she was leading on, to allow nurses and midwifes to demonstrate safe practice. SR advised of a group, which had been established in Leicestershire and Lincolnshire to provide a leadership role in implementing revalidation. A presentation will be provided at the Practice Nurse Conference in June.
4. ACTION TRACKER
The contents of the Action Tracker were discussed and applicable actions were agreed as closed.
5. CHIEF EXECUTIVE’S REPORT
LW presented the report to provide the Governing Body with information on activities being undertaken by the NHS East and North Hertfordshire Clinical Commissioning Group (CCG). The Governing Body discussed the recent Council of Members event and LW advised that the feedback received was very positive. It had been a very good day and the Workshops went really well. The CCG needs to think about how to expand this to the wider GP Community. LF reflected that last year colleagues were negative about the event but this year there was a different tone to it. MA thanked the Communications Team. NS reflected on the similarities of conclusions following discussions; this demonstrates that decisions and discussions had infiltrated significantly across localities. LW advised of the amazing response rate for the 360 Degree Stakeholder Survey and paid tribute to clinical colleagues. Positive responses had been received from GP Practices. LW believes this reflects the ongoing work that member practices are aware of. HP requested LW’s opinion on healthcare in Essex following a recent news article. LW advised there would be some imminent announcements coming from Simon Stevens, the Chief Executive Officer of NHS England. LW is in discussion with the NHS Trust Development Authority and NHS England’s Area Team to follow up. This will take place quickly to see if the CCG needs to do anything differently. A future paper will be presented to the Governing Body. ACTION: A paper to be presented to Governing Body following Simon Steven’s announcement.
BF

Page 3 of 9
RH advised the Governing Body on five areas of change, including mental health and learning disabilities. LW advised that this is about transforming care and the transfer arrangements around individuals in residential institutions. LW advised that the CCG had fed back saying a small group of individuals should not be the sole concentration, as there is a need to address the whole pathway. The beds do not serve just Hertfordshire, and the CCG does not have a large population of individuals in residential institutions.
6. GOVERNANCE REPORT
SR introduced the Governance Report. The Governing Body were asked to RATIFY endorsements made in their Workshops of 16th and 30th April 2015. SR highlighted the Quarter Three 2014-15 Assurance letter, which had been received from Trish Thompson, NHS England’s Interim Director of Commissioning Operations. HP thanked the Executives for their hard work in achieving the Assurance letter. SR advised of the Information Governance Forum in place and that the CCG had achieved a ‘Satisfactory’ level of compliance with the Information Governance Toolkit v12. The Governing Body RATIFIED the endorsements they had made at their Workshops on 16th and 30th April 2015.
7. HEALTH AND SAFETY ANNUAL REPORT
SR introduced the annual report for Health and Safety advising the Governing Body that a significant amount of work had been undertaken across the CCG by the Governance and Corporate Affairs Team in this area. SR highlighted that a new policy had been approved by the Governance and Audit Committee on 18th March 2015, which has now been made available to all staff on the Intranet. The next area identified for improvement will be Display Screen Equipment self-assessments by Line Managers for their staff. SR advised the Governing Body that four Health and Safety related incidents had been reported by staff between November 2014 and April 2015, although none of those were Reporting of Injuries, Diseases and Dangerous Occurrences (RIDDOR) type incidents. Good progress has been made on the Health and Safety Implementation Action Plan in Appendix 1 of the report.
8. INTEGRATED PERFORMANCE AND QUALITY REPORT
SR introduced the Integrated Performance and Quality Report and highlighted key areas of concern and underperformance that the Governing Body need to be aware of. At East and North Hertfordshire NHS Trust, stroke performance was challenged in March 2015 but significant improvement has been seen in April 2015. The Trust now has a Cancer Forum. Accident and Emergency performance is still fragile, and saw an improvement in April 2015 but by May 2015 this was again challenged.

Page 4 of 9
The Consultant Led Referral to Treatment Times 18 week pathway work is still on-going. At The Princess Alexandra Hospital NHS Trust, a performance meeting is to be set up for Stroke. Cancer performance is more positive. Accident and Emergency performance is below target and below the improvement trajectory. The Consultant Led Referral to Treatment Times has been challenged. Letters are being sent to GPs in relation to 52 week breaches. Staffing also remains challenged. At The Royal Free London NHS Foundation Trust, Infection Prevention and Control performance is challenging. Maternity is also an area of ongoing concern. At Herts Urgent Care there are some difficulties with shift fill. At Hertfordshire Community NHS Trust the Integrated Community Teams are experiencing pressures. Hertfordshire Partnership University NHS Foundation Trust recovery rates dipped throughout Quarter 4 due to a concerted effort to achieve the access target. The Dementia Diagnosis figure has significantly improved throughout 2014-15. There has been a reduction in calls to the Hotline regarding The Pathology Partnership, and analysis has revealed the majority of calls are in relation to rejected or leaked specimens. RH advised that when notified regarding insufficient samples, GP Practices are being asked to recall patients instead of The Pathology Partnership who should be administering this process. ACTION: Harper Brown to liaise with The Pathology Partnership. The East of England Ambulance Service NHS Trust has improved their performance overall. MA queried the difference between Red 1 and Red 2 Targets on Page 52. Michael Taylor advised that he felt there were huge improvements in the Ambulance Trust at the moment, and their recent Board meeting, which he attended, was really positive. ACTION: Sharn Elton / Gerry Moir to add Red 1 and Red 2 definition to Glossary. The Governing Body discussed the Integrated Performance and Quality Report. LF raised a concern about the Summary Hospital-Level Mortality Indicator at East and North Hertfordshire NHS Trust, advising the Governing Body that the CCG has had external reviews. The findings were not substantive and LF wondered where to go next. SR believed the focus should be on clinical pathways internally and out to primary care. Clinical audit on Urinary Tract Infection pathway is a common cause. SR advised the data had been extensively scrutinised and coding was appropriate. The focus will be on clinical care, cancelled Out Patient Department appointments, delays in appointments and individuals getting through on the telephone. SR assured the Governing Body that the CCG would not be complacent and The Royal College of Physicians felt the CCG had robust processes in place.
HB SE

Page 5 of 9
LW queried the NHS Constitution Scorecard on Page 7 (A&E attendances) and wondered what the movement was telling the CCG. SR advised it would show movement each time the report comes in terms of local delivery. PC advised of figures published recently regarding late cancellations of operations. LW advised there was a recent national audit on this topic. LW advised on issues regarding stroke performance, which is not at an acceptable level. LW added that she wished to reassure the Governing Body that this was being tackled and that April figures show improvements made in the 4 hours target to 70.3%. SR confirmed that there had been a huge focus over a number of months on stroke performance. The step change came about since the CCG issued a contract query through the Trust. The Trust recognised there is strong clinical need in Accident and Emergency where there were issues around individuals not recognising the symptoms of stroke early enough. SR reiterated that the CCG needs to be vigilant in other important areas so that the Trust delivers across the piece. HP queried whether the CCG collect data from The Princess Alexandra Hospital NHS Trust on how many miss targets and SR confirmed that the CCG does. SR advised that the Quality Team gain feedback from both patient and individual breach reports. However, the same feedback is always given by the Trust, stating that they will provide training, and it may now be time to take stronger action. FS confirmed that the CCG needs to continue to focus on this, as individuals will still present in Accident and Emergency. Although it is known they are still in transition, there is a need to keep a focus, especially when patients need to be transferred. SR concurred with this view. PC advised of a Stroke article recently in the Guardian regarding “fit people” having strokes, referring to Andrew Marr and the age bracket where there has been a huge rise in the incidences. The most obvious predicate of stroke is high blood pressure and PC queried whether the CCG could have a communications campaign to focus on blood pressure. HP advised that there had been public campaigns and the issue for GPs is regarding getting “well people” to attend surgeries. HP concurred with PC that more general awareness is needed. EB queried the 100 Days Cancer Breach figures and questioned why they got so far down the line, for example, 250 days. SR confirmed formal action is being taken with the Trust. BF agreed that there is some huge variation and the CCG must not become complacent. EB advised that The Royal Free London NHS Foundation Trust had identified through learning and are suggesting a clinical harm process. MA advised that some of these delays had been down to patient choice, which is surprising and may need further analysis. LW advised she had attended the Trust’s Board meeting and suggested Governing Body members attend if they could. The Trust has an academic and research approach - which is dynamic and interesting - to overall quality and improvement. SR confirmed that at East and North Hertfordshire NHS Trust, all cancelled Cancer operations were rebooked within 28 days. LW advised that the CCG was learning from Science and Diagnostics and work is being done on diagnostics in pharmacies.

Page 6 of 9
9. CARERS STRATEGY
BF introduced Tim Napper; Commissioning Manager from Hertfordshire County Council and advised that the CCG has had a Carers’ Strategy in place for some time. BF advised that the strategy was being presented at the public meeting to demonstrate the CCG’s support and commitment to this area. Work is currently being undertaken to identify carers and integration with GP systems. There will be a development session on this on 18th June 2015. TN confirmed that this is a multi-agency strategy; commitments apply equally between all partners, and the strategy speaks to all of them. BF asked the Governing Body if they had any concerns they wanted to raise. LW welcomed the document and felt it was well put together. LW believed the challenge for the CCG would be with regards to the pushback received from carers and the need for all partners to be more challenging. MA believed the strategy was well scoped but felt that the interaction for the CCG was not very clear. BF confirmed that the delivery plan will be refreshed and brought to a future Governing Body Public Meeting. There is a lot of work ongoing and it is good to raise general awareness of the topic. There are workshops planned for carers in July 2015. LW suggested the need to treat young carers as heroes. AP advised that it was vital to measure the outcomes but it is not currently clear to the Governing Body what those measures would be. AP suggested that when a target is set there is a greater determination to meet it. HB queried whether there is an obvious linkage to personalisation budgets and SR confirmed this is a good opportunity to use health budgets as enablers going forward. The Governing Body thanked Tim Napper for attending the meeting and providing a presentation.
10. EQUALITY AND DIVERSITY REPORT
SR introduced the Equality and Diversity report and highlighted key headings, advising that this duty is taken very seriously by the CCG. SR drew the Governing Body’s attention to the Equality Delivery System Action Plan in Appendix 1, advising where there were amber areas and that while the CCG had over achieved what it had set out to do in some areas, the CCG was not complacent, and remained committed to delivery of all actions. A new Workforce Race Equality Standard was published in April 2015, which the CCG is working towards. There has been an increase in the workforce of employees from Asian / Asian British and Black British / African backgrounds. There is a need to target hard to reach groups and there will be work on this going forward. Employment of ‘younger’ employees is challenging and the CCG do invite interns into the CCG on a regular basis. LW advised of an intern who had recently received 3 offers for Medical School following a successful placement with the CCG. AP advised that interns are paid for the work they undertake with the CCG. The focus currently is on the CCG staff and recruitment. AP reflected on whether this meets the needs of our Commissioning Strategy. LW concurred that Locality Commissioning Plans should be challenged to ensure they reflect this. SR advised that there will be opportunity to refresh and look at a more holistic perspective.

Page 7 of 9
11. COMPLAINTS ANNUAL REPORT
SR introduced the annual report for 2014-15 and confirmed that since the Francis Enquiry, when complaints were identified as a great source of intelligence; complaints are an area that the CCG takes really seriously. To ensure assurance, the Complaints Team has a robust process in place and the Chief Executive formally signs off all complaint letters. There has been an increase in multi-organisational complaints and the team is working on bringing providers and complainants together to identify and analyse any root causes. End of Life Care has been raised on more than one occasion. Individual Funding Requests and Continuing Health Care complaints, in particular retrospective reviews, have also been received; however, this is not unusual for CCGs. SR directed the Governing Body to page 5 of the report where there were examples of learning and actions, which had been taken, as a result of investigated complaints. SR confirmed that one complaint was investigated by the Parliamentary and Health Service Ombudsman and was partially upheld. The Ombudsman was complimentary about how the CCG had handled the complaint and made some recommendations regarding a provider’s health record keeping. The Quality Team audit on a regular basis and feedback is used to triangulate reports. LF confirmed that she had met with the Quality Team recently and acknowledged the hard work that they undertake. DD also confirmed the Quality Team had provided her with assurance of the triangulation process. The information put together is impressive. HP queried why there is not a section regarding complaints about Primary Care Practices. SR confirmed this report is a look back and she currently does not manage this process.
12. PRESCRIBING REPORT
AS introduced the report advising the end of financial year position is approximately £188,000 overspend, which is 0.24% above allocation. The main area for overspending was primary care prescribing, for example, increases in community nursing prescribing spends and good uptakes in patient numbers to anti-coagulant testing. Scriptswitch is working well and the CCG’s acceptance rate is higher compared to the national level. AS directed the Governing Body to Appendix 1b highlighting that an improvement had been achieved in most areas. There has been increased adherence to local antimicrobial prescribing guidelines. A final draft of local primary care guidelines has been circulated to stakeholders, to be presented to the Hertfordshire Medicines Management Committee in July 2015 for ratification. SK advised the Governing Body that if they upgrade their personal computers that this may affect the Scriptswitch software.

Page 8 of 9
DB assured the Governing Body regarding the Medicines Optimisation Dashboard. DB advised that information had been linked to localities and is not duplication.
13. ORGANISATIONAL PERFORMANCE AND DELIVERY
LW asked the Governing Body to note the update report, which summarises the discussions and key actions from the Organisational Performance and Delivery meeting of 5th May 2015. LF queried the content of the Action Tracker and LW advised this had already been picked up by the Executives and actioned by the Head of Programme Office.
14. GOVERNANCE AND AUDIT COMMITTEE MINUTES
LF requested the Governing Body to note the Minutes of the meeting held on 18th March 2015. The minutes of the Governance and Audit Committee minutes were NOTED by the Governing Body.
15. HBL ICT STAKEHOLDER BOARD MINUTES
AP requested the Governing Body to note the Minutes of the meeting held on 20th April 2015. AP confirmed that since the CCG had taken the service on, they were getting to the point where all partners were becoming more positive and proactive. LF queried whether all service agreements had been signed and AP confirmed that only the CCG’s remained outstanding. The minutes of the HBL ICT Stakeholder Board were NOTED by the Governing Body.
16. ANNUAL CYCLE OF BUSINESS
The Governing Body reached consensus and APPROVED the Annual Cycle of Business 2015-16 Governing Body Public and Private Meetings.
17. ANY OTHER URGENT BUSINESS
QEII opening LW advised that the QEII is now open and functioning and that other services are starting to transfer. There have been positive Tweets. The Governing Body were encouraged to have a look at the site and LW advised that the CCG are planning the official opening.

Page 9 of 9
Home First PC advised he was perplexed by the lack of openness or detail on how the Home First service is progressing. In its infancy there were constant updates but this no longer occurs. ACTION: LW advised that an update will be carried out and sent to patient representatives PC and MT. There are ongoing discussions in localities about how this might be provided.
LW
18. QUESTIONS FROM MEMBERS OF THE PUBLIC
There were no questions from members of the public.
19. DATE OF NEXT MEETING
24th September 2015 – Focolare Centre, Meeting Room 1
9:00am – 12:00pm

Agenda Item No: 4
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Action Tracker
Decision Discussion Information Follow up from last meeting
Report author: Sarah Feal, Company Secretary
Report signed off by: Beverley Flowers, Interim Chief Executive
Purpose of the paper: To discuss/note the Action Tracker.
Conflicts of Interest involved:
There are none identified.
Recommendations to the Governing Body:
To discuss/note the Action Tracker.

NHS East and North Hertfordshire Clinical Commissioing Group Governing Body Action Trackeritems for deletion in yellow
18-09-2015 1
Meeting date
Committee Subject Action Responsible manager
Deadline Current position Status
30-Oct-14 GBMIP Prescribing Report
To initiate an informed project on the NICE CG 181 Lipid Modification and to analyse the cost implication thoroughly
Sue Russell Jan-15 Medicine Management Lead Dr Shah acting on this and will be taking papers to the Primary Care Medicine Management Group (PCMMG) 2nd June 2015.04-06-15: AS advised this will be presented to the Governing Body shortly.
16-09-15-Dr Ash Shah reported that "This has been discussed at the PCMMG and is planned to be taken to the OPD for discussion of implications of implementation by Sue Russell."
Ongoing

NHS East and North Hertfordshire Clinical Commissioing Group Governing Body Action Trackeritems for deletion in yellow
18-09-2015 2
Meeting date
Committee Subject Action Responsible manager
Deadline Current position Status
30-Oct-14 GBMIP Planned Care To support the development of a specification for community anti-coagulation monitoring by G.P. practices.
Helen Edmondson
Oct-15 Helen Edmondson & Rachel Joyce with support from the Programme Office leading work to review current pathway and agree future model and commissioning route.Task and Finish group met on 181214. Follow up meeting with lead clinician for ENHT on 110515. Meeting agreed pathways which will be presented to OPD on 030615 to consider along with proposed commissioning routes.Other pathways agreed, specification to be developed and providers secured.04-06-15: BF advised this was discussed 03-06-15 and is work ongoing. There are now more clinicians involved.
14-09-15 Helen Edmondson reported that a development session is scheduled for 02-10-15 to present draft pathways and consider commissioniong options.
Ongoing
NHS East and North Hertfordshire Clinical Commissioing Group Governing Body Action Trackeritems for deletion in yellow
18-09-2015 3
Meeting date
Committee Subject Action Responsible manager
Deadline Current position Status
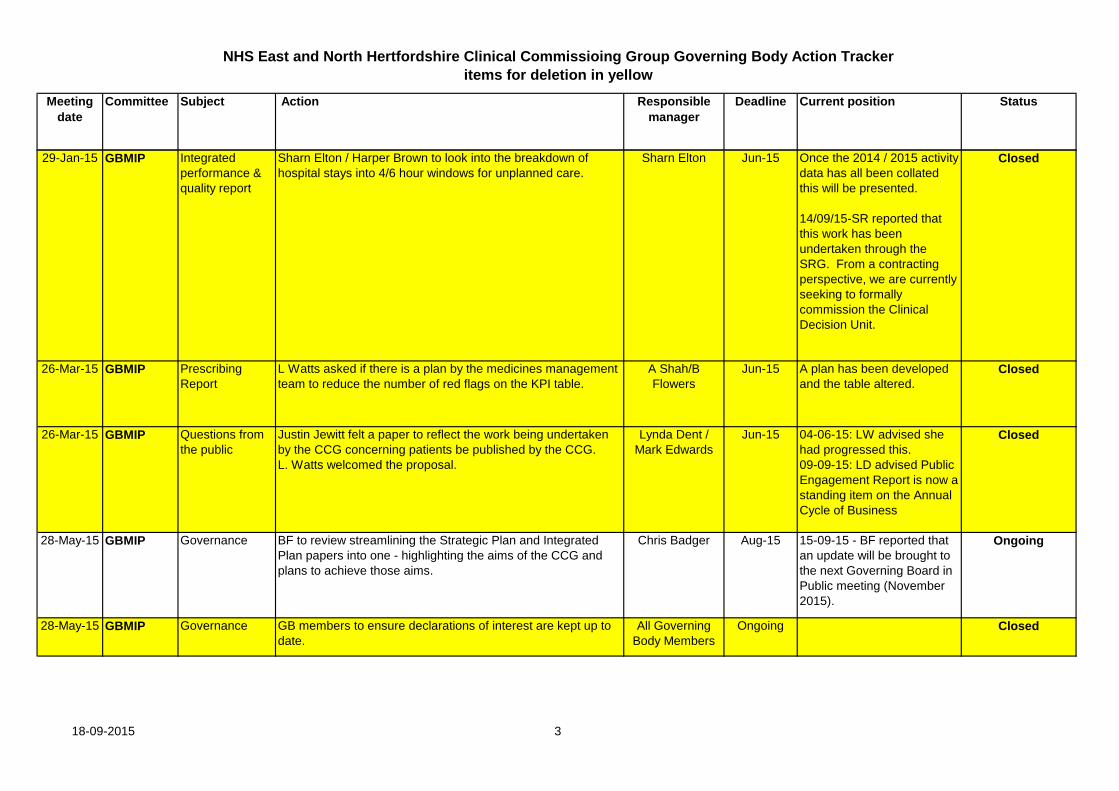
29-Jan-15 GBMIP Integrated performance & quality report
Sharn Elton / Harper Brown to look into the breakdown of hospital stays into 4/6 hour windows for unplanned care.
Sharn Elton Jun-15 Once the 2014 / 2015 activity data has all been collated this will be presented.
14/09/15-SR reported that this work has been undertaken through the SRG. From a contracting perspective, we are currently seeking to formally commission the Clinical Decision Unit.
Closed
26-Mar-15 GBMIP Prescribing Report
L Watts asked if there is a plan by the medicines management team to reduce the number of red flags on the KPI table.
A Shah/B Flowers
Jun-15 A plan has been developed and the table altered.
Closed
26-Mar-15 GBMIP Questions from the public
Justin Jewitt felt a paper to reflect the work being undertaken by the CCG concerning patients be published by the CCG.L. Watts welcomed the proposal.
Lynda Dent / Mark Edwards
Jun-15 04-06-15: LW advised she had progressed this.09-09-15: LD advised Public Engagement Report is now a standing item on the Annual Cycle of Business
Closed
28-May-15 GBMIP Governance BF to review streamlining the Strategic Plan and Integrated Plan papers into one - highlighting the aims of the CCG and plans to achieve those aims.
Chris Badger Aug-15 15-09-15 - BF reported that an update will be brought to the next Governing Board in Public meeting (November 2015).
Ongoing
28-May-15 GBMIP Governance GB members to ensure declarations of interest are kept up to date.
All Governing Body Members
Ongoing Closed

NHS East and North Hertfordshire Clinical Commissioing Group Governing Body Action Trackeritems for deletion in yellow
18-09-2015 4
Meeting date
Committee Subject Action Responsible manager
Deadline Current position Status
04-Jun-15 GBMIP Integrated Performance and Quality
HB to liaise with The Pathology Partnership (TPP). Harper Brown Sep-15 15-09-15 - HB reported that weekly meetings with The Pathology Partership continue on Remedial Action Plan. Local ENH clinical forum set up and meeting monthly.
Ongoing
04-Jun-15 GBMIP Integrated Performance and Quality
Sharn Elton / Gerry Moir to add Red 1 and Red 2 definition to Glossary of the Integrated Performance and Quality Report. (Red 1 and Red 2 Targets are mentioned on Page 55.)
Sharn Elton / Gerry Moir
Sep-15 15-09-15 - SE reported this action has been completed.
Closed
04-Jun-15 GBMIP Home First To carry out an update on the progress of Home First and send findings to Patient Representatives Peter Chapman and Michael Taylor.
Beverley Flowers Nov-15 15-09-15 - BF reported that a paper will be brought to the Governing Body Meeting in Public in November.
Ongoing

Agenda Item No: 5
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Chief Executive’s Report
Decision Discussion Information Follow up from last meeting
Report author: Sarah Feal, Company Secretary
Report signed off by: Beverley Flowers, Interim Chief Executive
Purpose of the paper: To provide information on activities being undertaken by
the Clinical Commissioning Group.
Conflicts of Interest involved:
There are none.
Recommendations to the Governing Body:
Please note the contents of the report.

1.0 Introduction The purpose of this paper is to provide information on activities being undertaken by the Clinical Commissioning Group (CCG). 2.0 Terms / Acronyms Used in the Report
CCG Clinical Commissioning Group NHS National Health Service
3.0 Tier One Dementia Training for Primary Care staff
We have arranged with Hertfordshire Partnership University NHS Foundation Trust Consultants to provide a 2 hour training session for GPs regarding dementia screening and diagnosis. The aim is to up skill GPs to give them the confidence to make the diagnosis and then to refer directly to the Consultant for confirmation and initiation of treatment. There are 2 confirmed dates on the 30th September and 28th October 2015.
4.0 Stakeholder Engagement - You Said… We Did…
The communications team has used social media, the CCG’s website and worked with patient participation groups to actively seek public opinion on the content of the CCG’s newly-created hospital website, www.newqeii.info. As a result, the hospital website has been updated to include improved internal and external maps, more precise parking information and telephone contact numbers for specific clinics. In response to comments from the public received through our ‘enquiries’ inbox and via local media, we have worked with a patient representative, the building’s landlords and East and North Hertfordshire NHS Trust to plan improvements to both external and internal hospital signage.
5.0 NHS Constitution and Handbook updated
Amendments to the NHS Constitution have been made around the following areas: prioritising patients; protecting patients from avoidable harm; providing assistance that patients need and staff compliance with guidance. The Department of Health has also introduced a new duty of candour into the NHS Constitution, to promote a culture of openness within the NHS. The inclusion of a patient right to candour helps to achieve this. The revised documents can be found at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/448466/NHS_Constitution_WEB.pdf
6.0 Transforming Care
In June 2015, Hertfordshire was selected by NHS England, as one of five Transforming Care Fast Track areas to help achieve the ambitions of the Learning Disability Transforming Care programme, which aims to significantly re-shape services for people with learning disabilities and/or autism with a mental health problem, or behaviour that challenges, to ensure that more services are provided in the community and closer to home, rather than in hospital settings.
As a Fast-Track area Hertfordshire had an opportunity to bid against a £10 million transformation fund (provided this was match-funded, the bid was credible and the funding could be spent in year) and was provided with external technical support, to accelerate plans for service re-design.

The Fast-Track guidance set out the principles and timetables for the development of local plans. Within this guidance was a timetable for submission and an indication that plans would be reviewed thereafter to test both the quality and overall deliverability. The Hertfordshire transformation plan was submitted on Monday 7th September together with a bid for approx. £1.5m funding from the transformation fund. There now follows a process of review of the plans and bids which will involve two groups of stakeholders in order to ensure local ownership of plans whilst supporting consistent improvement at a national level.
The Fast-Track plans will help shape the transformation of learning disability services more widely across England, including: • the future model of care for people with learning disabilities and/or autism – a
new Service Model – that will describe what good services look like, with clear outcomes for individuals;
• national planning assumptions for re-designing services to be reflected in planning guidance for 2016/17;
• more flexible ways of using funding to get the best outcomes for individuals. 7.0 Vanguard
The Vanguard programme to enhance care in care homes continues at pace. We have successfully recruited to the new dedicated Medicines Management Team for care homes, and our local providers of community health, mental health and social care colleagues are busy recruiting to teams to deliver rapid response services. We’re working with social care and the East of England Ambulance Trust on two rapid response vehicles who will work with care homes on supporting patients when their condition deteriorates, to try and prevent unnecessary hospital admissions. Care home staff in 11 care homes have nearly completed their intensive training, as part of the Complex Care Premium. We have submitted a Value Proposition to NHS England to secure extra investment funding to accelerate progress on the initiatives we are planning. We’ll find out if we have been successful later this month.
8.0 Stroke
East and North Hertfordshire NHS Trust are proposing changes to improve early acute stroke care. We want patients, who may have suffered a stroke, to be diagnosed as quickly as possible and to receive highly - specialist care on a dedicated stroke unit. This will improve their chances of surviving and recovering well, as well as improving our performance against national stroke indicators. We are recommending investment in stroke services at East and North Hertfordshire NHS Trust to support these changes, establish high quality seven day services and attract high calibre staff. There are additionally proposed changes to stroke services at The Princess Alexandra Hospital NHS Trust in Harlow, Essex, which is currently used by approximately 25% of Hertfordshire patients who suffer a stroke. We expect that, in future, patients with a suspected stroke will not be able to be treated at The Princess Alexandra Hospital NHS Trust and we are, therefore, making alternative arrangements and adapting our stroke pathway to take into account the expected change. Patients presenting with stroke symptoms will be taken by ambulance to the nearest hospital with a specialist stroke unit. For the majority of Hertfordshire patients, this would be the Lister Hospital in Stevenage. However, a small number, approximately 60 per year, will be taken to Mid Essex Hospital Trust at Chelmsford. Although, some patients and carers may have further to travel, outcomes such as 30 day mortality and long term disability are expected to be better.

To minimise the numbers of transfers of care and support care closer to home, the CCG is suggesting further investment in our successful stroke early supported discharge service. This will mean that after acute care people can be seen by stroke specialist teams at home or as an in-patient at Danesbury Neurological Unit at Welwyn or Herts and Essex Hospital in Bishop’s Stortford. The Princess Alexandra Hospital NHS Trust will continue to provide out-patient transient ischaemic attack clinics to Hertfordshire residents in their catchment area. A joint business case, with East and North Hertfordshire NHS Hospital Trust and Hertfordshire Community NHS Trust is in development and will be presented over the next two months. We have a stakeholder discussion document available on our website: www.enhertsccg.nhs.uk and are encouraging local people, interested parties and service providers to give us their feedback regarding our stroke proposals. West Essex CCG has also launched a ‘consultation’ regarding proposed changes in stroke care at The Princess Alexandra Hospital NHS Trust. The document can be accessed and feedback given via www.westessexccg.nhs.uk/have-your-say/give-your-views
9.0 Child and Adolescent Mental Health Service and Schools Link Pilot Scheme
The East and North Hertfordshire CCG and Herts Valley CCG application to be part of the Child and Adolescent Mental Health Service and Schools Link Pilot Scheme has been successful. There were 87 applications in total so this is a real achievement. Full training will be provided, which will commence in the autumn. The pilot allows up to 10 schools / colleges / special schools per CCG to be included in the training. The Department for Education and NHS England are planning a co-ordinated approach to the publicity for the pilots later in the autumn term once the training is underway.

Page 1 of 4
Agenda Item No: Item 6
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Governance Report
Decision Discussion Information Follow up from last meeting
Report author: Sarah Feal, Company Secretary
Report signed off by: Sheilagh Reavey, Director of Nursing & Quality (Item 5.0) Linda Farrant, Lay Member – Governance and
Audit Purpose of the paper: To seek the approval of the Governing Body to a number of
matters, as required by the CCG’s Constitution, that have been agreed at Governing Body Workshops since the last Governing Body Meeting in Public on 4th June 2015, including: Matters approved that require reporting to the Governing
Body Meeting in Public for ratification. To provide the Governing Body in Public with a summary of key corporate governance activities.
Conflicts of Interest involved:
There are none identified.
Recommendations to the Governing Body:
The Governing Body is asked to: note and ratify the decisions made at the Governing
Body Workshops; ratify the updates to the Standards of Business
Conduct Policy; note the report from the Governance and Audit
Committee; ratify the Terms of Reference of the Committees of the
Governing Body; note the Strategic Risk Register and Risk Controls
Assurance Dashboard; receive the declarations of interests and Register of
Gifts and Hospitality reported in 2015-16; note the changes to Financial Policies.

Page 2 of 4
Governance Report 1.0 Introduction This paper provides information on corporate governance activities being undertaken by the Clinical Commissioning Group (CCG). 2.0 Terms / Acronyms Used in the Report CCG Clinical Commissioning Group NHS National Health Service QEII The new QEII Hospital in Welwyn Garden City is a modern,
welcoming and sustainable place for local people to access the hospital services that they use most often.
3.0 CCG Governing Body Workshops Summarised below are key discussions and actions agreed from the Governing Body Workshops that have taken place since the last Governing Body Meeting in Public on 4th June 2015:
3.1 Governing Body Workshop 18th June 2015: agreed to re-procure the NHS 111/Out-Of-Hours Service; approved a Business Case to invest in developing, and delivering an integrated,
Pharmacist led medicines optimisation service in care homes; agreed their investment priorities for 2015-16 with regards to mental health and learning
disability services; agreed to cancel the contract for the Florence Simple Telehealth Pilot Project. 3.2 Governing Body Workshop 2nd July 2015: agreed to fund Target, Locality and CCG led Prescribing meetings from locality
management funds; approved a Business Case to invest in Falls and Geriatric Response Vehicles; agreed to pilot a new Out-Of-Hours Service within the QEII; agreed to support the process to populate the Carers Register; agreed to continue to fund the Community Assessment and Rehabilitation Service. 3.3 Governing Body Workshop 30th July 2015: approved a Business Case to invest in in Primary Care Workforce, Planning and
Education, which included a 6 month fixed term appointment for a Clinical Lead; agreed to re-procure a long-term Wheelchair Service. 3.4 Governing Body Workshop 20th August 2015: approved a Business Case to invest in Diabetes for younger people, and Type II and
Chronic Kidney Disease; agreed the recommendations made by Hertfordshire Medicines Management
Committee, and their work plan 2015-16; agreed a number of recommendations to improve the quality of Stroke Services.

Page 3 of 4
3.5 Governing Body Workshop 3rd September 2015: agreed the National Flu Immunisation Programme for 2015-16; approved the Winter Resilience Schemes. 4.0 Standards of Business Conduct Policy v3.0 On the 2nd July 2015, the Governing Body approved a recommendation to no longer accept commercial funding for meeting refreshments or room hire due to any conflict of interest that may be perceived. The Standards of Business Conduct Policy (Appendix A) was updated and also included minor changes regarding the acceptance of gifts and hospitality to make the policy easier for staff to follow. This Policy was reviewed by the Executive Team on 25th August 2015 and is recommended by them to the Governing Body for approval (this decision is reserved to the Governing Body, as per the Scheme of Reservation and Delegation). The Governing Body is asked to ratify the Standards of Business Conduct Policy. 5.0 Governance and Audit Committee Meeting The Minutes of the Governance and Audit Committee meeting of 20th May 2015, as approved at the 22 July 2015 meeting are being submitted to this meeting, as required by the Committee’s Terms of Reference. Items of business considered by the Committee at its July meeting have included: review of the Strategic Risk Register and Principal Risks; approval of the Prime and Detailed Financial Policies (see section 10.0); review of the Annual Audit Letter from External Audit; review of the progress report from the Information Governance Forum; scrutiny of the Committee’s Terms of Reference.
The Governing Body is asked to note the report from the Governance and Audit Committee. 6.0 Terms of Reference The Terms of Reference of the following Committees of the Governing Body are being presented for approval: Governance and Audit Committee (Appendix B); Lower Lea Valley Locality (Appendix C); North Herts Locality (Appendix D); Stevenage Locality (Appendix E); Stort Valley and Villages Locality (Appendix F); Upper Lea Valley Locality (Appendix G); Welwyn and Hatfield Locality (Appendix H). The Governing Body is asked to ratify the Terms of Reference. 7.0 Strategic Risk Register (SRR) and Risk Controls Assurance Dashboard (RCAD) The SRR and RCAD were reviewed by the Governance and Audit Committee at its meeting on 22 July 2015, and subsequently have been discussed by the Executive Team at their meeting on 15 September 2015.

Page 4 of 4
The SRR (Appendix I) is a summary of key risks the organisation faces in delivering its objectives and is refreshed regularly to reflect changing circumstances. The Executive Team have approved the addition of a new risk regarding the Financial Sustainability of Providers in the Health Economy (Strategic Risk 6).
The RCAD enables the CCG to have an understanding of its risk profile and the effectiveness of controls to mitigate the risks. There are currently 38 risks on the RCAD in the following categories, and details of the red risk scoring 16+ (ID 1.50) are included in Appendix J:
Red Amber Yellow Green 1 15 11 11
The Governing Body is asked to note the SRR and RCAD. 8.0 Declarations of Interest Registers / Register of Gifts and Hospitality The CCG has recently undertaken a proactive exercise to update its declarations of interests registers. Interests have been recorded for Governing Body members, Band 8a staff members and above, and the 60 member Practice Representatives. All registers (Appendix K and L) were scrutinised by the Governance and Audit Committee on 16th September 2015. The Governing Body is asked to receive the declarations of interests and Register of Gifts and Hospitality reported in 2015-16. 9.0 Governing Body Annual Cycle of Business 2015-16 Public and Private The Annual Cycle of Business was approved by the Governing Body in June 2015 and is available from this link: http://www.enhertsccg.nhs.uk/governing-body-meetings-in-public 10.0 Changes to Financial Policies Following the annual review of the CCG’s Prime Financial Policies and Detailed Financial Policies, the following minor changes were proposed to the Governance and Audit Committee in July, and were agreed: Prime Financial Policies Para 2.1 – reference to paragraph in constitution updated to reflect revised
constitution.
Detailed Financial Policies Para 2.1 – reference to paragraph in constitution updated to reflect revised
constitution.
New paragraph 13.14 – “No contract incurring expenditure or leading to a disposal shall be structured in a way solely to avoid any of the thresholds within this section 13, e.g. purchase splitting to avoid the requirement to tender is prohibited.”

Appendix A
Standards of Business Conduct Policy
(Including hospitality, acceptance of gifts, sponsorship and joint working with the pharmaceutical industry)
Document Owner
Director of Nursing and Quality
Document Author
Associate Director of Governance and Corporate Affairs
Version 3.0 Draft2.1 Final
Directorate Nursing and Quality
Authorised By Governing BodyGovernance and Audit Committee
Date of Approval
24th September 20157th August 2014
Date of Review 24th September 20177th August 2016
Change History
Version Date Name Revision Description
0.1 Draft February 2013 John Paton
1.0 September 2013 Julie Andrews Quality Assurance
2.0 July 2014 Mel Brown Revised
2.1 October 2014 Sarah Feal Amended following Governance and Audit Committee feedback and minor formatting
3.0 August 2015 Sarah Feal Update to Sections 9, 10 and 12

Page 2 of 26
Table of Contents
1.0 Introduction .................................................................................................................... 4
2.0 Purpose .......................................................................................................................... 4
3.0 Scope ............................................................................................................................. 4
4.0 Guidance and Legal Framework ..................................................................................... 4
5.0 ....................................................................................................................................... 5
The Seven Principles of Public Life ......................................................................................... 6
6.0 Openness and Public Responsibilities ............................................................................ 7
7.0 Roles and Responsibilities – Standards of Business Conduct ......................................... 7
8.0 The Policy in Practice ..................................................................................................... 8
9.0 The Acceptance of Gifts ................................................................................................. 8
10.0 The Acceptance of Hospitality ..................................................................................... 9
11.0 The Provision of Hospitality by the Clinical Commissioning Group ............................ 10
12.0 Hospitality for Locality Committee Group meetings by commercial organisations ...... 10
13.0 Donations in relation to the organisation ................................................................... 10
14.0 Payment for speaking at a meeting / conference ....................................................... 10
15.0 Commercial sponsorship ........................................................................................... 12
16.0 Joint working with the Pharmaceutical Industry ......................................................... 13
17.0 Placing of orders and contracts ................................................................................. 13
18.0 Commissioning of Services where GP Practices are potential providers of CCG-commissioned services. ............................................................................................... 14
19.0 Private Transactions ................................................................................................. 14
20.0 Employees’ outside employment ............................................................................... 14
21.0 Donations in relation to the organisation ................................................................... 14
22.0 Donations to an individual ......................................................................................... 15
23.0 Rewards for Initiative ................................................................................................ 15
24.0 Candidates for appointment ...................................................................................... 15

Page 3 of 26
25.0 Canvassing for appointments .................................................................................... 16
26.0 Failure to Disclose/Declare ....................................................................................... 16
27.0 Dissemination and implementation ............................................................................ 16
28.0 Monitoring, Audit and Review .................................................................................... 16
29.0 References & Bibliography ........................................................................................ 18
Appendices ........................................................................................................................... 19
Appendix 1 ............................................................................................................................ 20
Notification of Receipt of Hospitality, Gifts or Sponsorship ..................................................... 21
Appendix 2 ............................................................................................................................ 22
Institute of Purchasing and Supply (IPS) – Ethical Code ....................................................... 22
Appendix 3 ............................................................................................................................ 23
FRAMEWORK FOR JOINT WORKING BETWEEN THE NHS AND PHARMACEUTICAL INDUSTRY ........................................................................................................................... 23
Appendix 4 ............................................................................................................................ 22
Managing Conflicts of Interest - Commissioning Services from GP Practices / organisations in which GPs have a Financial Interest ...................................................................................... 22
...................................................................................................................................................................

Page 4 of 26
1.0 Introduction 1.1 This policy underpins the NHS East and North Hertfordshire Clinical Commission
Group’s (CCG) Constitution and sets out further details of the expected conduct of all those who work within it.
2.0 Purpose 2.1 The purpose of this policy is to ensure exemplary standards of business conduct are
adhered to, as public servants, by Governing Body members, committee and sub-committee members and employees of the CCG (as well as individuals contracted to work on behalf of the CCG or otherwise providing services or facilities to the CCG such as those within commissioning support services).
2.2 Through this policy individuals will be aware of their own responsibilities, as well as
the CCG’s responsibilities as corporate bodies (including the constituent Member Practices). The Policy also sets out the responsibilities of the CCG as an employer, especially in light of the individual and corporate obligations set out in the Bribery Act 2010.
3.0 Scope 3.1 This policy applies to:
• The Governing Body, its committees and sub-committees;
• Employees of the CCG;
• Member practices (and their employees), when undertaking duties on behalf of the CCG;
• Third parties acting on behalf of the CCG. 4.0 Guidance and Legal Framework 4.1 The NHS Management Executive published guidance, “Standards of Business
Conduct for NHS Staff”, HSG (93) 5, which remains extant and which provides specific guidance on:
• the standards of conduct expected of all NHS staff where their private interests may conflict with their public duties; and,
• the steps which NHS employers should take to safeguard themselves and the NHS against conflicts of interest.
4.2 Specifically, it makes it clear that it is the responsibility of staff to ensure that they are
not placed in a position which risks, or appears to risk, conflict between their private interests and their NHS duties.
4.3 The Department of Health’s document, “Code of Conduct for NHS Managers”,
(October 2002), provides guidance on core standards of conduct expected of NHS Managers to act in the best interests of the public and patients / clients to ensure that decisions are not improperly influenced by gifts or inducements. Professional Codes of Conduct governing health care professionals are also pertinent. Similarly, the General Medical Council’s guidance, “Leadership and management for all doctors” (March 2012), details the standards and expectations required of clinicians in leadership and management positions. The Professional Standards Authority has also published Standards for members of NHS Boards and Clinical Commissioning Group Governing Bodies in England.

Page 5 of 26
4.4 Other important guidance on conduct is to be found in “The Code of Conduct: Code of Accountability in the NHS” (Appointments Commission/DOH – 2nd Rev: 2004) and the Department of Health’s guidance on “Commercial Sponsorship – Ethical Standards for the NHS” (Department of Health, November 2000).
4.5 The underpinning legal framework is provided by the Bribery Act 2010, which repeals
the Prevention of Corruption Acts, and which:
• creates two general offences covering the offering, promising or giving of an advantage, and requesting, agreeing to receive or accepting an advantage;
• creates a new offence of failure by a commercial organisation to prevent a bribe being paid for or on its behalf (it will be a defence though if the organisation has adequate procedures in place to prevent bribery).
4.6 Bribery is defined as giving someone a financial or other advantage to encourage that
person to perform their functions or activities improperly or to reward that person for having already done so.
4.7 Any employee breaching the provisions of this Act will be liable to prosecution which
may also lead to the loss of their employment and superannuation rights in the NHS. 4.8 Section 25, 14(O) of the Health and Social Care Act 2012 imposes duties on the CCG
in relation to maintaining registers of interest and managing conflicts of interest. Guidance has been set out in “Towards establishment: Creating responsive and accountable clinical commissioning groups, Technical Appendix 1 – Managing conflicts of interest” and an associated Code of Conduct where GP practices are potential providers of clinical commissioning group-commissioned services. This guidance will be embodied in documentation published by the NHS EnglandCommissioning Board to the CCG on managing conflicts of interest.
4.9 This policy has been produced taking into account all of the current guidance and
legal framework. 5.0 Application of Public Service Values and Principles to the NHS Public service values must be at the heart of the NHS. High standards of corporate and personal conduct based on recognition that patients come first, have been a requirement throughout the NHS since its inception. Moreover, since the NHS is publicly funded, it is accountable to Parliament for the services it provides and for the effective and economic use of taxpayers’ money. The Code of Conduct: Code of Accountability in the NHS (Appointments Commission / DOH - 2nd Rev: 2004) defines three crucial public service values which must underpin the work of the health service: Accountability – everything done by those who work in the NHS must be able to stand the test of parliamentary scrutiny, public judgements on propriety and professional codes of conduct. Probity – there should be an absolute standard of honesty in dealing with the assets of the NHS: integrity should be the hallmark of all personal conduct in decisions affecting patients, staff and suppliers, and in the use of information acquired in the course of NHS duties.

Page 6 of 26
Openness – there should be sufficient transparency about NHS activities to promote confidence between the NHS body and its staff, patients and the public. Following the findings of the Nolan Committee in 1994, a set of recommendations was published by the government setting out ‘Seven Principles of Public Life’ which apply to all in the public service and which are embodied within the CCG Constitutions. These are attached at Appendix 1.The Seven Principles of Public Life 5.1 The principles of public life apply to anyone who works as a public office-holder.
This Policy respects the seven principles promulgated by the Nolan Committee, as outlined below:
The Seven Principles of Public Life
Selflessness Holders of public office should act solely in terms of the public interest. Integrity Holders of public office must avoid placing themselves under any obligation to
people or organisations that might try inappropriately to influence them in their work. They should not act or take decisions in order to gain financial or other material benefits for themselves, their family, or their friends. They must declare and resolve any interests and relationships.
Objectivity Holders of public office must act and take decisions impartially, fairly and on merit, using the best evidence and without discrimination or bias.
Accountability Holders of public office are accountable to the public for their decisions and actions and must submit themselves to the scrutiny necessary to ensure this.
Openness Holders of public office should act and take decisions in an open and transparent manner. Information should not be withheld from the public unless there are clear and lawful reasons for so doing.
Honesty Holders of public office should be truthful. Leadership Holders of public office should exhibit these principles in their own behaviour.
They should actively promote and robustly support the principles and be willing to challenge poor behaviour wherever it occurs.

Page 7 of 26
6.0 Openness and Public Responsibilities 6.1 The NHS East and North Herts CCG understands the requirement to consult upon
major changes before decisions are reached and will be open with the public, patients and staff. Information supporting decisions will be made available in a way that is understandable and responses to requests for information in accordance with the Freedom of Information Act 2000 will be provided in this spirit.
6.2 Our business will be conducted in a way that is socially responsibility, forging an
open and positive relationship with the local community and in consideration of the impact of the organisation’s activities on the environment.
7.0 Roles and Responsibilities – Standards of Business Conduct 7.1 NHS Employers
7.1.1 The CCG is responsible for ensuring that the requirements of this policy and
supporting documents are brought to the attention of all staff and that machinery is put in place for ensuring that the guidelines are effectively implemented. These responsibilities are particularly important given the corporate responsibility set out in the Bribery Act 2010 for organisations to ensure that their anti-corruption procedures are robust.
7.2 Such awareness will be promoted in:
A clause in written statements of terms and conditions or employment;
Publication on the CCG Intranet sites for staff. 7.3 NHS Staff are expected to:
Ensure that the interests of patients remain paramount at all times;
Be impartial and honest in the conduct of their official business;
Use the public funds entrusted to them to the best advantage of the service, always ensuring value for money;
Register with the CCG any interest outside the workplace which could be construed as affecting any part of their work within the CCG.
7.4 It is also the responsibility of staff to ensure that they do not:
Abuse their official position for personal gain or to benefit their family or friends;
Seek to advantage or further private business or other interests, in the course of their official duties.
7.5 It is the responsibility of all staff to raise any concerns regarding staff business conduct. The organisation’s Raising Concerns at Work/Whistleblowing Policy provides advice to enable staff to raise any concerns.
7.6 All NHS staff should ensure that they are not placed in a position that risks, or
appears to risk, conflict between their private interests and their NHS duties. 7.7 Governing Body, Committee / Sub-Committee members and individuals acting on
behalf of the CCG.

Page 8 of 26
7.8 Governing Body, Committee/Sub-Committee members and individuals acting on behalf of the CCGs), must act in accordance with this policy in circumstances whether they are either employed fully by the CCG, hold appointments with the CCG, are employed on a sessional basis or on an honorary contract, or provide services under a service level agreement with the CCG.
7.9 All individual and practices acting on behalf of the CCG commissioning functions
must act in accordance with this policy. 8.0 The PolicyGuidance in Practice 8.1 Overriding Principle
Employees of the CCG, Governing Body and committee members, and individuals acting on behalf of the CCG must not accept any fee or reward for work done whilst on CCG duty other than that agreed under their terms and conditions of employment.
8.2 As a general rule employees should not accept gifts or hospitality arising from their
employment or appointment with the CCG, except where these are of a token nature only, in which case employees should inform their line manager. This includes gifts or hospitality offered by suppliers and potential suppliers of goods and services to the CCGs, and any participation in quasi-official and social events either within or outside normal working hours.
8.3 Allny offers of gifts, hospitality or sponsorship shall be recorded in accordance with
section 9 – 11 of this policy. 9.0 The Acceptance of Gifts 9.1 Less than £25 per gift
Articles of low intrinsic value, i.e. less than £25 per gift, for example, diaries, calendars or small tokens of gratitude from individuals, need not necessarily be refused. Casual gifts of low intrinsic value offered by contractors or others, (for example, at Christmas time) , may not be in any way connected with the performance of duties so as to constitute an offence at law. Such gifts should, nevertheless, be politely but firmly declinArticles of low intrinsic value, i.e. less than £25 per gift, such as diaries or calendars, or small tokens of gratitude from patients or their relatives, need not necessarily be refused.
9.2 Gifts £25 and over G However, gifts over £25 should be declared and generally declined using the form at
Appendix 1. WhenIf several casual gifts of low intrinsic valuesmall gifts worth a total of over £1200 have beenare received from the same or closely related source in a 12 month period any further gift offered should be declared and declinedthey should generally be declined. In cases of doubt, advice should be sought from the Company Secretary or the gift should be politely declined.
9.3 Gifts of money must never be accepted from individuals and should be declared and declined using the form at Appendix 1.
9.4 All gifts, whether accepted or not, willmust be entered into the register of gifts and
hospitality, which is managedoverseen by the Governance and Corporate Affairs TeamCompany Secretary.

Page 9 of 26
10.0 The Acceptance of Hospitality 10.1 Hospitality less than £25
Modest hospitality, provided thit is does not exceed £25 may be accepted and needn’t be declared. Lunch in the course of a working visit is also acceptable.

Page 10 of
10.2 Hospitality £25 and over There may be circumstances where hospitality over £25 may be accepted, for example, attending an NHS funded event or to receive an award at a ceremony on behalf of the CCG. The amount of hospitality must be determined by contacting the event organiser and if this exceeds £25, Executive Director approval is also required on the declaration ‘where relevant’, and using the form at Appendix 1.
10.3 All other offers of hospitality or entertainment should be decAll hospitality over £25, whether
accepted or not, will be entered into the register of gifts and hospitality, which is managed by the Governance and Corporate Affairs Team.
11.0 The Provision of Hospitality by the Clinical Commissioning Group 11.1 The Code of Conduct: Code of Accountability in the NHS advises that the use of NHS
monies for hospitality and entertainment, including hospitality at conferences or seminars, should be carefully considered. It advises that all expenditure on these items should be capable of justification, as reasonable in the light of general practice in the public sector. It reminds NHS organisations that hospitality or entertainment is open to challenge by auditors and that ill-considered actions can damage respect for the NHS in the eyes of the community.
12.0 Hospitality for Locality Committee Group meetings by commercial
organisations 12.1 FDrug company funding of refreshments / room hire for Locality Committee Group
(LCG) meetings by commercial organisations, including but not limited to, TARGET, Locality and CCG led Prescribing meetings is not acceptablesubject to the drug company representatives not attending the meetings or receiving meeting papers. . These meetings must be funded from locality management funds. All other offers of hospitality or entertainment should be decAll hospitality over £25 should be declared and declined using the form at Appendix 1, and will be entered into the register of gifts and hospitality, which is managed by the Governance and Corporate Affairs Team.
All such hospitality in respect of LCG meetings must be reported to the Company Secretary who maintains the Register of Gifts, Hospitality and Sponsorship.
13.0 Donations in relation to the organisation 13.1 Employees must check with their line manager or Executive Ddirector before
making any requests for donation to clarify appropriateness and / or financial or contractual consequences of acquisition. Requests for equipment or services should not be made without the express permission of a senior manager.
13.2 Donations / gifts from individuals, charities, companies (as long as they are not
associated with known health-damaging products) – often related to individual pieces of equipment or items – provide additional benefits to patients but may have resource implications for the CCG. Further guidance regarding charitable funds and gifts and donations can be requested from the Chief Finance Officer.
14.0 Payment for speaking at a meeting / conference 14.1 Should a member of staff, Member Practices, Governing Body and Committee
members and individuals acting on behalf of the CCG, be asked to speak at an event relating to CCG business for which a payment is offered and it is delivered in working hours then there are two choices open to the member of staff which must be agreed with their line manager:
The payment should be credited to the CCG;
The member of staff takes annual leave or unpaid leave and the payment is made

Page 11 of
to the member of staff as a private matter between the organisation making the payment and the individual member of staff. The member of staff remains responsible for any tax liability which arises.

Page 12 of
15.0 Commercial sponsorship 15.1 In recognition that NHS bodies work together, and in collaboration with other
agencies, to improve health services for the populations they serve, the Department of Health published guidance “Commercial Sponsorship: Ethical Standards for the NHS” (November 2000).
15.2 The guidance acknowledges that collaborative partnerships with industry can have a
number of benefits. It advises that it is important to have a transparent approach about any proposed sponsorship which would be of benefit for the CCG to consider fully the implications of a proposed sponsorship deal before entering into any arrangement. If any such partnership is to work, there must be trust and reasonable contact between the sponsoring company and the NHS.
15.3 For the purpose of this policy, commercial sponsorship is defined as including “NHS funding from an external source, including funding of all, or part of, the costs of a member of staff, NHS research, staff training, pharmaceuticals, equipment, meeting rooms, costs associated with meetings, meals, gifts, hospitality, hotel and transport costs (including trips abroad), provision of free services (speakers), buildings or premises”.
15.4 In all these cases, Governing Body, Committee members, CCG employees, and
individuals acting on behalf of the CCG must declare sponsorship or any commercial relationship linked to the supply of goods or services and be prepared to be held to account for it. This should be recorded in the Hospitality, Gifts or Sponsorship Register (see section 9 - 11).
15.5 Where such collaborative par tnersh ips invo lve a pharmaceutical company, the
proposed arrangements must also comply fully with the relevant regulations. 15.6 As a general rule, sponsorship arrangements involving the CCG will be at a
corporate, rather than individual level. 15.7 If publications are sponsored by a commercial organisation, that organisation should
have no influence over the content of the publication. The company logo can be displayed on the publication, but no advertising or promotional information should be displayed. The publication should contain a disclaimer which states that sponsorship of the publication does not imply that the CCG endorses any of the company’s products or services.
15.8 All Governing Body, Committee members, CCG employees, and individuals acting on
behalf of the CCG should discuss the implications, with their manager/Accountable officer (Chief Executive Officer), before accepting an invitation to speak at a meeting organised by a pharmaceutical company. The company should have no influence over the content of any presentation made by the CCG’s employee/representative. It should be made clear that CCG’s’ presence does not imply that the CCG endorses any of the company’s products or services.
15.9 Under no circumstances will the CCG agree to ‘linked deals’ whereby sponsorship is
linked to future purchase of particular products or to supply from particular sources. 15.10 Before entering into any sponsorship agreement, reference should be made to the
Department of Health’s Policy ‘Commercial Sponsorship – Ethical Standards for the NHS’. http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/document s/digitalasset/dh_4076078.pdf

Page 10 of 26
15.11 If it is considered that an exception to this prohibition is justified in exceptional circumstances, an application must be made in advance to the Chief Finance Officer for approval and reported to the next Governance and Audit Committee, which will consider if such an application is consistent with the Nolan Principles and considerations set out in the CCG’s Standards of Business Conduct Policy.
16.0 Joint working with the Pharmaceutical Industry 16.1 DH Guidance encourages NHS organisations and their staff to consider opportunities
for joint working with the pharmaceutical industry, where the benefits that this could bring to patient care and the difference it can make to their health and well-being are clearly advantageous. Such initiatives should be managed in an effective and efficient way.
16.2 Joint working must be for the benefit of patients or of the NHS and preserve patient
care. Any joint working between the NHS and the pharmaceutical industry should be conducted in an open and transparent manner. Arrangements should be of mutual benefit, the principal beneficiary being the patient. The length of the arrangement, potential implications for patients and the NHS, together with the perceived benefits for all parties, should be clearly outlined before entering into any joint working.
16.3 Prior to entering any joint working initiatives, staff (including member practices) must
seek advice fromof the CCG’s Assistant Director and Head of Pharmacy and Medicines Optimisation Head of Medicines Management to ensure that the correct process is followed for all joint working initiatives. Appendix 3.4 outlines the areas against which all joint working initiatives should be assessed by a group within the CCG.
17.0 Placing of orders and contracts 17.1 Fair and open competition between prospective contractors or suppliers for CCG
contracts (including where the CCG is commissioning a service through Any Qualified Provider) is a requirement of NHS Standing Orders and of EC Directives on Public Purchasing for Works and Supplies. This means that:
No private, public or voluntary organisation or company which may bid for CCG
business should be given any advantage over its competitors, such as advance notice of CCG requirements. This applies to all potential contractors, whether or not there is a relationship between them and the CCG, such as a long-running series of previous contracts.
Each new contract should be awarded solely on merit, taking into account the
requirements of the CCG and the ability of the contractors to fulfil them.
No special favour is to be shown to current or former employees or their close relatives or associates in awarding contracts to private or other businesses run by them or employing them in any capacity. Contracts may be awarded to such businesses when they are won in fair competition against other tenders, but scrupulous care must be taken to ensure that the selection process is conducted impartially, and that staff who are known to have a relevant interest play no part in the selection.

Page 14 of 26
17.2 All Governing Body, Committee members, CCG employees, and individuals acting on behalf of the CCG , in contact with suppliers and contractors (including external consultants), and in particular those who are authorised to sign orders or place contracts for goods, materials or services, are expected to adhere to professional standards of a kind set out in the ethical code of the Institute of Purchasing and Supply (attached at Appendix 3). They are also required to declare any interest if they are participating in a specific procurement and tendering processes.
18.0 Commissioning of Services where GP Practices are potential
providers of CCG-commissioned services. 18.1 In the circumstances of commissioning of such services including Local Enhanced
Services all individuals must comply with the principles and main content of the NHS England's Code of Conduct in this area. Arrangements for managing any such declarations of interest are set out in the Managing Conflicts of Interest Policy.
19.0 Private Transactions 19.1 Individual staff, Member Practices, Governing Body and Committee members and
individuals acting on behalf of the CCG, must not seek or accept preferential rates or benefits in kind for private transactions carried out with companies with which they have had, or may have, official dealings on behalf of the CCG. (This does not apply to concessionary agreements negotiated with companies by NHS management, or by recognised staff interests, on behalf of all staff – for example, NHS staff benefits schemes).
20.0 Employees’ outside employment 20.1 The standard contract used across the CCG sets out terms concerning outside
employment: ‘You shall not be employed by any other person, firm or company, without the express permission of the CCG. If you have employment other than your employment with the CCG, you must write to your Line Manager giving details of the hours and days worked and duties carried out, seeking agreement that this work will not be detrimental to your employment within the CCG.
20.2 Any employee who may be considering outside employment should discuss this in
the first instance with their Line Manager before undertaking the employment. 20.3 Employees should be advised not to engage in outside employment during any
periods of sickness absence from the CCG. To do so may lead to a referral being made to the Local Counter Fraud Specialist for investigation, which may lead to criminal and / or disciplinary action in accordance with the CCG’s Anti-Fraud and Bribery Policy.
21.0 Donations in relation to the organisation 21.1 Employees must check with their Line Manager or Executive Director before making
any requests for donations to clarify appropriateness and/or financial or contractual consequences of acquisition. Requests for equipment or services should not be made without the express permission of a senior manager.
21.2 Donations / gifts from individuals, charities, companies (as long as they are not associated with known health-damaging products) – often related to individual pieces of equipment or items – provide additional benefits to patients but may have resource implications for the CCG. Further guidance regarding charitable funds and gifts and donations can be requested from the Chief Finance Officer.
21.3 Any gifts to the organisation should be receipted and a letter of thanks should
be sent.

Page 15 of 26
22.0 Donations to an individual 22.1 Personal monetary gifts to an employee or appointed member should be politely
but firmly declined. Where a member of staff is a beneficiary to a Will of a patient who has been under their care, the member of staff must inform their Line Manager of the gift or gifts so that consideration can be given to whether or not it is appropriate in all the circumstances for that member of staff to retain the gift or gifts in order to avoid subsequent claims by the beneficiaries to the Estate of inducement, reward or corruption.
22.2 In order to determine whether the bequest should be accepted it may be necessary
to have the gift valued and where the gift has a value over a certain amount for the gift to either be returned to the Estate or the gift to be donated to a Charity of the member of staff’s choice. Where the gift is to be returned to the Estate and the Trustees of the Estate are of the view having regards to all the circumstances that the member of staff should retain the gift regardless of its value, it may be appropriate for the Trustees to provide a disclaimer for future claims against the gift to avoid subsequent claims on the gift or allegations of inducement or reward being made against the member of staff or the CCG at some point in the future.
23.0 Rewards for Initiative 23.1 The CCG will identify potential intellectual property rights (IPR), as and when they
arise, so that they can protect and exploit them properly, and thereby ensure that they receive any rewards or benefits (such as royalties), in respect of work commissioned from third parties, or work carried out by individuals in the course of their NHS duties. Most IPR are protected by statute; e.g. patents are protected under the Patents Act 1977 and copyright (which includes software programmes) under the Copyright Designs and Patents Act 1988. To achieve this, NHS organisations and employers should build appropriate specifications and provisions into the contractual arrangements which they enter into before the work is commissioned, or begins. They should always seek legal advice if in any doubt, in specific cases.
23.2 With regard to patents and inventions, in certain defined circumstances the
Patents Act gives employees or individuals in the course of their duties a right to obtain some reward for their efforts, and the CCG will see that this is affected. Other rewards may be given voluntarily to employees or other individuals who, within the course of their employment or duties, have produced innovative work of outstanding benefit to the NHS.
23.3 In the case of collaborative research and evaluative exercises with manufacturers, the CCG will obtain a fair reward for the input they provide. If such an exercise involves additional work for a CCG employee or individual outside that paid for by the CCG under his or her contract of employment, or sessional arrangements, arrangements will be made for some share of any rewards or benefits to be passed on to the employee(s) or individuals concerned from the collaborating parties. Care will, however, be taken that involvement i n this type of arrangement with a manufacturer does not influence the purchase of other supplies from that manufacturer.
24.0 Candidates for appointment 24.1 Candidates for any appointment with the CCG must disclose in writing if they
are related to or in a significant relationship with (e.g. spouse or partner) any Governing Body member or employee of the CCG. The NHS Jobs application form requests this information and therefore must be disclosed before submission.
24.2 A member of an appointment panel which is to consider the employment of a person
to whom he/she is related must declare the relationship before an interview is held.

Page 16 of 26
24.3 Candidates for any appointment with the CCG shall, when applying, also disclose cases where they or their close relatives or associates have a controlling and/or significant financial interest in a business (including a private company, public sector organisation, other NHS employer and/or voluntary organisation), or in any other activity or pursuit, which may compete for an NHS contract to supply either goods or services to the CCG.
25.0 Canvassing for appointments 25.1 It is acknowledged that informal discussions concerning an advertised post can
be part of the recruitment process, canvassing or lobbying of CCG employees. Governing Body members or any members of an appointments committee, either directly or indirectly, shall disqualify a candidate. This shall not preclude a member from giving a written reference or testimonial of a candidate’s ability, experience or character for submission to an appointments panel. Jobs will be awarded on the merit of the individual candidate and not through any such canvassing or lobbying.
26.0 Failure to Disclose/Declare 26.1 The CCG is committed to the national code of Conduct and Code of Accountability
in the NHS (revised 2004) and such takes the failure to disclose such information as required by this policy seriously. It is an offence under the Fraud Act 2006, for a member or employee to fail to disclose information to the CCG in order to make a gain for themselves or another. It is also an offence to cause a loss or expose the organisation to a loss. Therefore, where an employee has failed to disclose information in line with this policy, the Anti-Fraud and Bribery Policy should be consulted and an appropriate referral made.
27.0 Dissemination and implementation 27.1 This policy and accompanying procedures are available for all staff to access via
the intranet. 27.2 All staff will be notified of a new or reviewed policy via ‘Weekly news round-up’.staff
update and briefing 27.3 This document will be included in the CCG’s Publication Scheme in compliance with
the Freedom of Information Act 2000. 28.0 Monitoring, Audit and Review 28.1 Version controlInformation relating to this policy is recorded in a database run by
the Governance and Corporate Affairs Team. 28.2 The Company Secretary will ensure this document is reviewed in accordance with
the Review Date. 28.3 This policy and accompanying procedures are available for all staff to access via the
Intranet. 28.4 All staff will be notified of a new or reviewed policy via staff update and briefing.
28.5 This document will be included in the CCG Publication Schemes in compliance with
the Freedom of Information Act 200. 28.6 28.728.3 Where staff become aware of changes in practice, changes to statutory
requirements, revised professional or clinical standards and local/national directives that affect, or could potentially affect policy documents, they should advise the Sponsoring Director as soon as possible, via line management arrangements. The Sponsoring Director will then consider the need to review the procedural document outside of the agreed timescale.

Page 17 of 26

Page 18 of 26
29.0 References & Bibliography 29.1 Other relevant policies and reference material that should be read in conjunction with
this policy include:
The CCG’s Constitution;
Managing Conflicts of Interests Policy;
Anti-Fraud and Bribery Policy;
Code of Conduct and Code of Accountability in the NHS;
Code of Conduct for NHS Managers;
Raising Concerns at Work/Whistleblowing Policy.

Page 19 of 26
Appendices Appendix 1: Hospitality, Gifts or Sponsorship Declaration Form Appendix 2: Institute of Purchasing and Supply (IPS) – Ethical Code Appendix 3: Framework for joint working between the NHS and
Pharmaceutical Industry Appendix 4: Managing Conflicts of Interests form Appendix 5: Equality Impact Assessment Appendix 6: Privacy Impact Assessment

Page 20 of 26
Appendix 1 The Nolan Principles on Standards in Public Life
The Nolan Committee was set up in 1994 to examine concerns about standards of conduct of all holders of public office, including arrangements relating to financial and commercial activities, and make recommendations as to any changes in arrangements which might be required to ensure the highest standards of propriety in public life. The committee published “seven principles of Public Life”, which it believes should apply to all those operating in the public sector. These principles should be adopted by CCG staff and are as follows:
Selflessness Holders of public office should act solely in terms of the public interest. They should not do so in order to gain financial or other benefits for themselves, their family or their friends.
Integrity Holders of public office should not place themselves under any financial or other obligation to outside individuals or organisations that might seek to influence them in the performance of their official duties.
Objectivity In carrying out public business, including making public appointments, awarding contracts, or recommending individuals for rewards and benefits, holders of public office should make choices on merit.
Accountability Holders of public office are accountable for their decisions and actions to the public and must submit themselves to whatever scrutiny is appropriate to their office.
Openness Holders of public office should be as open as possible about all the decisions and actions that they take. They should give reasons for their decisions and restrict information only when the wider public interest clearly demands.
Honesty Holders of public office have a duty to declare any private interests relating to their public duties and to take steps to resolve any conflicts arising in a way that protects the public interest.
Leadership Holders of public office should promote and support these principles by leadership and example.
All staff will be expected to adopt these principles when conducting official business for and on behalf of the CCG so that appropriate ethical standards can be demonstrated at all times.

Page 21 of 26
Appendix 2 Notification of Receipt of Hospitality, Gifts or Sponsorship
Name: (please print)
Position within the CCG:
Contact Telephone Number:
Details of the Hospitality, Gift or Sponsorship and approximate Value:
Please also give details of the form in which the hospitality was accepted e.g. tickets, cheque, vouchers
Organisation / Person offering the hospitality, gift or sponsorship:
The reason for accepting the offer:
Or The reason for refusing the offer:
Any other relevant information:
Signed:
Date:
Signature of Line Manager: (where relevant >25)
Please forward to:
[email protected] Company Secretary
This Register is established in accordance with the CCG Standards of Business Conduct PolicyConduct Policy. It will be reported on a six monthly basis to the Governance and Audit Committee.

Page 22 of 26
Appendix 23 Institute of Purchasing and Supply (IPS) – Ethical Code
Introduction 1. The code set out below was approved by the Institute's Council on 26 February 1977 and is binding on IPS members.
Precepts 2. Members shall never use their authority or office for personal gain and shall seek to uphold and enhance the standing of the Purchasing and Supply profession and the Institute by:
a. maintaining an unimpeachable standard of integrity in all their business relationships both inside and outside the organisations in which they are employed; b. fostering (the highest possible standards of professional competence amongst those for whom they are responsible; c. optimising the use of resources [or which they are responsible to provide the maximum benefit to their employing organisation; d. complying both with the letter and the spirit of;
i. the law of the country in which they practise; ii. such guidance on professional practice as may be issued by the Institute from time to time; iii. contractual obligations;
e. rejecting any business practice which might reasonably be deemed improper. Guidance 3. In applying these precepts, members should follow the guidance set out below:
a. Declaration of interest Any personal interest which may impinge or might reasonably be deemed by others to impinge on a member's impartiality in any matter relevant to his or her duties should be declared. b. Confidentiality and accuracy of information The confidentiality of information received in the course of duty should be respected and should never be used for personal gain; information given in the course of duty should be true and fair and never designed to mislead. c. Competition While bearing in mind the advantages to the member's employing organisation of maintaining a continuing relationship with a supplier, any relationship which might, in the long term, prevent the effective operation of fair competition should be avoided. d. Business Gifts Business gifts other than items of very small intrinsic value such as business diaries or calendars should not be accepted. e. Hospitality Modest hospitality is an accepted courtesy of a business relationship. However, the recipient should not allow him or herself to reach a position whereby he or she might be deemed by others to have been influenced in making a business decision as a consequence of accepting such hospitality; the frequency and scale of hospitality accepted should not be significantly greater than the recipient's employer would be likely to provide in return. When it is not easy to decide between what is and is not acceptable in terms of gifts or hospitality, the offer should be declined or advice sought from the member's superior.

Page 23 of 26
Appendix 34
FRAMEWORK FOR JOINT WORKING BETWEEN THE NHS AND PHARMACEUTICAL INDUSTRY
I. JOINT WORKING PROJECT SUMMARY
1. TITLE OF PROJECT
2. SUMMARY OF INTENDED AIMS & OBJECTIVES
3. SUMMARY OF EXPECTED OUTCOMES
4. NAMES OF THE PARTNER ORGANISATIONS
INVOLVED IN THE JOINT WORKING ARRANGEMENT
5. NAMES OF LEAD REPRESENTATIVES FOR EACH ORGANISATION
6. EXACT NATURE OF THE JOINT WORKING PROPOSAL
7. START DATE
8. FINISH DATE
9. EXIT STRATEGY
II. RESOURCES AND COSTS
1. OVERALL COST OF THE JOINT WORKING
PROJECT
2. DIRECT AND INDIRECT RESOURCES / COST
COMMITMENTS BY EACH PARTNER
3. METHOD FOR MONITORING AND RECORDING
RESOURCE AND COSTS
4. INFORMATION ON COST EFFECTIVENESS (Has value for money been shown?)
5. ARRANGEMENTS FOR LONGER TERM FUNDING
IMPLICATIONS OF PROJECT
(To be clear and unambiguous)
III. GOVERNANCE ARRANGEMENTS
1. PARTIES CONSULTED PRIOR TO INITIATING
JOINT WORKING PROJECT AND HOW
CONSULTATION WAS CONDUCTED
2. METHOD FOR INFORMING PATIENTS OF THE
JOINT WORKING PROJECT

Page 20 of 26
3. DECISION MAKING PROCESSES WITHIN THE
JOINT WORKING PROJECT
(To be open and transparent)
4. OPERATIONAL AND MANAGEMENT
ACCOUNTABILITIES
(Include identified conflicts of interest)
5. PILOTING ARRANGEMENTS
(State if this project is a pilot)
6. RELATIONSHIP TO EXISTING SYSTEMS OF CARE
IN PRIMARY AND SECONDARY CARE SECTORS
7. FOR CLINICAL SERVICES, PROFESSIONAL
INDEMNITY AND LIABILITY ARRANGEMENTS
8. WRITTEN AGREEMENT STATING OBLIGATIONS
OF CONFIDENTIALITY, SECURITY STANDARDS
AND LIMITS OF USE OF INFORMATION TO THE
PURPOSES SPECIFIED
IV. MONITORING AND EVALUATION
1. MANAGEMENT ARRANGEMENTS
2. LIST DESIGNATED RESPONSIBILITY AT EACH
STAGE OF THE PROPOSAL
3. METHOD OF EVALUATING PATIENT BENEFITS ON
COMPLETION
4. LEARNING OPPORTUNITIES FROM THIS
PROJECT
5. AUDIT ARRANGEMENTS
6. METHOD FOR HIGHLIGHTING SIGNIFICANT
PROBLEMS
V. DATA AND PATIENT PROTECTION
1. LIST INTERESTS OF PARTNERS IN RELATION TO
THE JOINT WORKING PROPOSAL, AND WHERE
THESE COINCIDE
2. LIST POTENTIAL CONFLICTS OF INTEREST

Page 21 of 26
3. IDENTIFY “OWNERSHIP” OF THE DATA
GENERATED BY THE PROJECT
4. DESCRIBE ACCESS ARRANGEMENTS FOR
THE DATA, AND FORMAT
(Bearing in mind the requirements of the Data Protection Act and patient confidentiality of healthcare records)
5. USE DATA WILL BE PUT TO
VI. DECLARATION OF INTERESTS YES NO
If Yes, qualify by inserting a tick in one box in column A and one in column B
A B
Personal Specific
Non-Personal Non Specific
Signature Date
Personal implies that you (or your spouse / partner) receive direct payment for services or hold shares in the relevant company concerned or a competitor. Non-Personal implies that your unit benefits by receiving funding from the company. Specific implies that you have undertaken work or given advice on other products made by the relevant manufacturer.
This system is based on that used by the Commission on Human Medicines and other national drug regulatory bodies.

Page 22 of 26
Appendix 45 Managing Conflicts of Interest - Commissioning Services from GP Practices / organisations in which GPs have a Financial Interest
Service:
Question Comment / Evidence
Questions for all three procurement routes
How does the proposal deliver good or improved outcomes and value for money – what are the estimated costs and the estimated benefits? How does it reflect the CCG’s proposed commissioning priorities?
How have you involved the public in the decision to commission this service?
What range of health professionals have been involved in designing the proposed service?
What range of potential providers have been involved in considering the proposals?
How have you involved your Health and Wellbeing Board(s)? How does the proposal support the priorities in the relevant joint health and wellbeing strategy (or strategies)?
What are the proposals for monitoring the quality of the service?
What systems will there be to monitor and publish data on referral patterns?
Have all conflicts and potential conflicts of interests been appropriately declared and entered in registers which are publicly available?

Page 23 of 26
Why have you chosen this procurement route 1 ?
What additional external involvement will there be in scrutinising the proposed decisions?
How will the CCG make its final commissioning decision in ways that preserve the integrity of the decision-making process?
1 Taking into account S75 regulations and NHS Commissioning Board guidance, Monitor guidance, and existing procurement rules.

Page 24 of 26
Additional question for AQP or single tender (for services where national tariffs do not apply)
How have you determined a fair price for the service?
Additional questions for AQP only (where GP practices are likely to be qualified providers)
How will you ensure that patients are aware of the full range of qualified providers from whom they can choose?
Additional questions for single tenders from GP providers
What steps have been taken to demonstrate that there are no other providers that could deliver this service?
In what ways does the proposed service go above and beyond what GP practices should be expected to provide under the GP contract?
What assurances will there be that a GP practice is providing high-quality services under the GP contract before it has the opportunity to provide any new services?

Page 25 of 26
Appendix 56 – Equality Impact Assessment Stage 1 Screening
1. Policy EIA Completion Details Title: Standards of Business Conduct
Proposed Date of Completion: Existing July 2014
Review Date: July 2015
Names & Titles of staff involved in completing the EIA: Mel Brown
2. Details of the Policy. Who is likely to be affected by this policy? Staff Patients Public
3. Impact on Groups with Protected Characteristics Probable impact on group? High,
Medium or Low
Please explain your answers Positive Adverse None
Age
Being married or in a civil partnership
Disability, inc. learning difficulties, physical disability, sensory impairment etc.
Having just had a baby or being pregnant
Race, ethnicity, nationality, language etc
Religion or belief
Sex (inc. being a transsexual person)
Sexual Orientation
Other:
No impact on any of the groups above.
Please explain and provide evidence N/A
4. Which equality legislative Act applies to the policy?
Human Rights Act 1998 Equality Act 2010 Health & Safety Regulations
Mental Health Act 1983 Mental Capacity Act 2005
5. How could the identified adverse effects be minimised or eradicated? N/A
6. How is the effect of the policy on different Impact Groups going to be monitored? N/A

Page 26 of 26
Appendix 67 – Privacy Impact Assessment – Stage 1 Screening
1. Policy PIA Completion Details
Title: Standards of Business Conduct
Names & Titles of staff involved in completing the PIA: Mel Brown Proposed
Existing Date of Completion: July 2014
Review Date: July 2015
2. Details of the Policy. Who is likely to be affected by this policy?
Staff Patients Public Yes No Please explain your answers Technology Does the policy apply new or additional information technologies that have the potential for privacy intrusion? (Example: use of smartcards) Identity By adhering to the policy content does it involve the use or re-use of existing identifiers, intrusive identification or authentication? (Example: digital signatures, presentation of identity documents, biometrics etc.)
Potentially staff may be required to divulge private data
By adhering to the policy content is there a risk of denying anonymity and de-identification or converting previously anonymous or de-identified data into identifiable formats? Multiple Organisations Does the policy affect multiple organisations? (Example: joint working initiatives with other government departments or private sector organisations) Data By adhering to the policy is there likelihood that the data handling processes are changed? (Example: this would include a more intensive processing of data than that which was originally expected) If Yes to any of the above have the risks been assessed, can they be evidenced, has the policy content and its implications been understood and approved by the department?
N/a

Page | 1
Appendix B
Governance and Audit Committee
Terms of Reference v2.10

Page | 2
1. Introduction 1.1 The Governance and Audit Committee (the Ccommittee) is established in accordance
with NHS East and North Hertfordshire Clinical Commissioning Group’s Constitution. These Tterms of Rreference set out the membership, remit, responsibilities and reporting arrangements of the Ccommittee and shall have effect as if incorporated into the Cconstitution. The role of the Committee is primarily about providing assurance to the Governing BodyBoard that appropriate and robust risk management and internal control procedures processes are in place. The Committee will also maintain appropriate relationships with the organisation’s Internal and External Auditors.Much of the detailed Clinical Governance work of this committee will be undertaken by sub-groups, some long-standing and some appointed to address a particular issue
2. Membership 2.1 The committee shall be appointed by the clinical commissioning group as set out in the clinical commissioning group’s constitution and may include individuals who are not on the governing body. 2.1 2.2. The Mmembership of the Ggovernance and Aaudit Ccommittee shall include:
the Llay Mmember of the Governing Body with a lead role for overseeing key elements of Ggovernance and Audit (Chair);
the nurse member of the Governing Body; and one Cclinician member of the Governing Body; (not including the nurse member). another Llay Mmember of the Governing Body.assurance
2.2 In the event of the Chair of the Committee being unable to attend all or part of the
meeting, they will nominate a replacement from within the Membership to deputise for that meeting.
2.3. The lay member on the governing body, with a lead role in overseeing key elements of governance, will need to be able to chair the governance an audit committee. 2.3 The Chair of the Governing Body shall not be a member of the Governance and Audit
Committee. 2.4 The Clinician members of the Committee shall be selected from the Clinician members
of the Governing Body. 2.5 Members of the Committee shall cease to be members of the Committee if they are no
longer members of the Governing Body. 2.6 The Committee may from time to time appoint sub-committees to review particular
issues. In establishing such sub-committees The Governance and Audit Committee will: 1. Nominate the membership of the Sub-Committee; 2. State the Terms of Reference of the Sub-Committee; 3. The deadline for it to report its conclusions to the main Committee; 4. Report the establishment of a Sub-Committee to the Governing Body.CCG Board
2.7 Representatives in attendance

Page | 3
Individuals who are in attendance, who are not members of the Committee, shall not vote and must withdraw from the Committee if requested to do so. The following representatives will usually be in attendance: Chief Finance Officer; Internal Auditor; External Auditor; Local Counter Fraud Specialist; Company Secretary; Head of Risk Management; Governing Body Administrator (Minutes).
The Committee shall invite the Chief Financial Officer, the respective internal and external auditors and a representative of NHS Protect to attend meetings of the committee. Additionally the committee may invite any individual to attend any or part of its meetings. The committee may invite any person to attend meetings to provide advice and/or expertise as required. Any such person shall not be a member of the committee and shall withdraw upon request. Any individual invited to attend the committee may contribute to the proceedings and provide advice and/or guidance to the committee as requested. 2.8 Notwithstanding the above provisions; External Audit, Internal Audit, Local Counter
Fraud and Local Security Management Specialists will have full and unrestricted rights of access to the Chair of the Committee in respect of their audit functions.
3. Quorum 3.1 Two members of the Committee must be present including at least one Clinician
member for the quorum to be established.
3.2 No formal business shall be transacted where a quorum is not reached.
4. Frequency of meetings and attendance 4.1 A minimum of 6 scheduled meetings shall be held per year. 4.2 Members of the Committee should make every effort to attend all meetings of the
Committee. The Secretary to the Committee will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report and Accounts.
The Committee shall meet not less than six times each financial year. Meetings shall be no
more than nine weeks apa4.3 The Chair of the Committee may convene additional meetings as required.
4.4 ATwo members of the Committee may requisition a meeting by writing to the Chair of
the Committee. 4.5 The External Auditor and / or the Clinical Commissioning Group employee responsible
for Internal Auditor may requisition a meeting of the Committee by writing to the Chair of the Committee.

Page | 4
4.6 Written notice of meetings and the Agenda shall be provided to Committee members of the Committee not less than 55 working days before the meeting. No meeting of the Committee shall be invalid for want of service of notice and / or the Agenda.
4.7 Notice of Committee meetings and the Agenda shall also be provided to the
Accountable Officer, Chief Financial Officer and the Clinical Commissioning Group employee responsible for internal audit.
4.78 The Committee shall meet in private with the Internal and External Auditors not less
than annually. 4.89 The Committee shall meet with the Accountable Officer not less than annually to
discuss and consider the process for assurance that supports the Annual Governance StatementStatement on internal control.
4.910 The Chair of the Committee shall report the outcome and any recommendations of the
Committee to the Governing Body.
5. Authority 5.1 The Committee is authorised by the Governing Body to obtain professional advice,
including the appointment of external advisor and / or consultants, related to its functions as it deems fit at the expense of the Clinical Commissioning Group.
5.2 The Committee shall recommend appropriate action(s) should be taken by the Governing Body in allowing the Committee to fulfil its Terms of Reference.
6. Emergency powers 6.1 Where an urgent decision needs to be made in between scheduled meetings,
members of the Committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or the exchange of emails. The exercise of such powers shall be reported and minuted at the next Committee meeting.
7. Duties 7.1 The Committee shall critically review the Clinical Commissioning Group’s financial
reporting and internal control principles and ensure an appropriate relationship with both Internal and External Auditors is maintained. The committee shall also critically review the quality of the services for which it is responsible, both clinical and non-clinical.
7.12 The key audit duties of the Committee are:
Integrated Governance, Risk Management and Internal Control
7.23 The Committee shall review the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the Clinical Commissioning Group’s activities that support the achievement of the Clinical Commissioning Group’s objectives.
7.34 In particular, the Committee will review the adequacy and effectiveness of:
All risk and control related disclosure statements (in particular the Annual Governance Statement), together with any appropriate independent assurances, prior to endorsement by the Clinical Commissioning Group.

Page | 5
The underlying assurance processes that indicate the degree of achievement of Clinical Commissioning Group objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements.
The policies for ensuring compliance with relevant regulatory, legal and code of conduct requirements and related reporting and self-certification.
The policies and procedures for all work related to fraud and corruption as set out in Secretary of State Directions and as required by the NHS ProtectCounter Fraud and Security Management Service.
7.45 In carrying out this work the Committee will primarily utilise the work of Internal Audit, External Audit and other assurance functions, but will not be limited to these sources. It will also seek reports and assurances from Directors and Managers as appropriate, concentrating on the over-arching systems of integrated governance, risk management and internal control, together with indicators of their effectiveness.
7.56 This will be evidenced through the Committee’s use of an effective assurance framework to guide its work and that of the audit and assurance functions that report to it.
Internal Audit
7.67 The Committee shall ensure that there is an effective Internal Audit function that meets mandatory NHS Public Sector Internal AuditInternal Audit Standards and provides appropriate independent assurance to the Governance and Audit Committee, Accountable Officer and Clinical Commissioning Group. This will be achieved by:
Consideration of the provision of the Internal Audit service, the cost of the audit and any questions of resignation and dismissal.
Review and approval of the Internal Audit Strategy, operational plan and more detailed programme of work, ensuring that this is consistent with the audit needs of the organisation, as identified in the assurance framework.
Considering the major findings of Internal Audit work (and management’s response) and ensuring co-ordination between the Internal and External Auditors to optimise audit resources.
Ensuring that the Internal Audit function is adequately resourced and has appropriate standing within the Clinical Commissioning Group.
An annual review of the effectiveness of Internal Audit.
External Audit
7.78 The Committee shall review the work and findings of the External Auditors and consider the implications and management’s responses to their work. This will be achieved by:
Consideration of the performance of the External Auditors, as far as the rules governing the appointment permit.
Discussion and agreement with the External Auditors, before the audit commences, on the nature and scope of the audit as set out in the annual plan, and ensuring co-ordination, as appropriate, with other External Auditors in the local health economy.
Discussion with the External Auditors of their local evaluation of audit risks and assessment of the Clinical Commissioning Group and associated impact on the audit fee.
Review of all External Audit reports, including the report to those charged with governance, agreement of the Annual Audit Letter before submission to the Clinical

Page | 6
Commissioning Group and any work undertaken outside the annual audit plan, together with the appropriateness of management responses.
Other Assurance functions
7.89 The Committee shall review the findings of other significant assurance functions, both internal and external and consider the implications for the governance of the Clinical Commissioning Group.
7.910 These will include, but will not be limited to, any reviews by Department of Health arm’s length bodies or regulators / inspectors (for example, the Care Quality Commission and NHS Litigation Authority) and professional bodies with responsibility for the performance of staff or functions (for example, professional leadership bodies and accreditation bodies).
Counter Fraud
7.101 The Committee shall satisfy itself that the Clinical Commissioning Group has adequate arrangements in place for countering fraud and shall review the outcomes of counter fraud work. It shall also approve the Counter Fraud Work Programme.
Management
7.112 The Committee shall request and review reports and positive assurances from Directors and Managers on the overall arrangements for governance, risk management and internal control.
7.123 The Committee may also request specific reports from individual functions within the Clinical Commissioning Group, as they may be appropriate to the overall arrangements.
Financial reporting
7.134 The Governance and Audit Committee shall monitor the integrity of the financial statements of the Clinical Commissioning Group and any formal announcements relating to the Clinical Commissioning Group’s financial performance.
7.145 The Committee shall ensure that the systems for financial reporting to the Clinical Commissioning Group, including those of budgetary control, are subject to review as to completeness and accuracy of the information provided to the Clinical Commissioning Group.
7.156 The Committee shall review the Annual Report and financial statements before submission to the Governing Body and the Clinical Commissioning Group, focusing particularly on:
The wording in the Annual Governance Statement and other disclosures relevant to the Terms of Reference of the Committee;
Changes in, and compliance with, accounting policies, practices and estimation techniques;
Unadjusted mis-statements in the financial statements; Significant judgements in preparing of the financial statements; Significant adjustments resulting from the audit; Letter of representation; and Qualitative aspects of financial reporting.
Clinical Quality

Page | 7
7.167 The Committee shall seek assurance that robust clinical quality is in place.
7.178 The Committee shall have regard to the priorities of the Clinical Commissioning Group and any associated risks or areas of quality improvement in this respect.
7.189 The key quality duties of the Committee are to:
Seek assurance that the Commissioning Strategy for the Clinical Commissioning Group fully reflects all elements of quality (patient experience, effectiveness and patient safety), keeping in mind that the strategy and response may need to adapt and change.
Seek assurance from the Quality Committee, or any other sources of assurance, that commissioned services are being delivered in a high quality and safe manner, ensuring that quality sits at the heart of everything the Clinical Commissioning Group does.
Seek assurance from the Quality Committee, or any other sources of assurance, that commissioned services are being delivered to fully reflect all elements of quality (patient experience, effectiveness and patient safety), ensuring that quality sits at the heart of everything the Clinical Commissioning Group does.
Oversee and be assured by the Quality Committee that effective management of risk is in place to manage and address clinical governance issues.
Have oversight of the process and compliance issues concerning Serious Incidents Requiring Investigation (SIRIs) and Serious Case Reviews (SCRs); being informed of all Never Events and informing the Governing Body of any escalation or sensitive issues in good time.
Seek assurance on the performance of NHS organisations in terms of the Care Quality Commission, Monitor and any other relevant regulatory bodies.
Receive and scrutinise independent investigation reports relating to patient safety issues and SCRs, agree action plans and publication plans.
Ensure a clear escalation process, including appropriate trigger points, is in place to enable appropriate engagement of external bodies on areas of concern.
8. Reporting arrangements to the Governing Body 8.1 The Committee will report to the Governing Body on a bi-monthly basis and the
following documents will be presented:
Minutes of the Committee’s meetings; Update Report via the Governance Report.
9. Reporting arrangements of other Committees and Groups 9.1 The following Committees and groups will report into the Committee and provide
Assurance Reportsminutes of their meetings:
Meeting Name Frequency Quality Committee at least 4 reports per year Information Governance Forum every 6 months
10. Annual review of the Committee 10.1 The Committee will undertake an annual self-assessment to:
Review that these Terms of Reference have been complied with and whether they remain fit for purpose;

Page | 8
Determine whether its planned activities and responsibilities for the previous year have been sufficiently discharged; and,
Recommend any changes and / or actions it considers necessary, in respect of the above;
Provide the Governing Body with an annual report, which details the outcome of the annual review.
11. Committee servicing 11.1 The Committee shall be supported administratively by the Governing Body
Administrator (or other nominated representative), who’s duties in this respect will include:
Agreement of the Agenda with the Chair and collation of papers in-line with the Committee’s Annual Cycle of Business;
Providing written notice of meetings to Committee members, and the papers, not less than 55 working days before the meeting;
Taking the Minutes and keeping a record of matters arising and issues to be carried forward;
Producing a single document to track the Committee’s agreed actions and report progress to the Committee;
Producing draft Minutes for approval within 5 working days of the meeting.
Terms of Reference reviewed by: Governance and Audit Committee Review Date: 22 July 2015 Governing Body Approval Date: 24 September 2015 Next Review Date: July 2016
Monitoring and Reporting Mechanism 8.3. The minutes of each meeting of the committee shall be formally recorded and retained by the clinical commissioning group. The minutes shall be submitted to the Governing Body. 8.4. The Chair of the committee shall draw to the attention of the Governing Body any issues that require disclosure to the Council of Members and/or require executive action. The Governance and Audit Committee shall scrutinise the proceedings of the committee. 8.5. The committee shall report to the Governing Body annually on its work in support of the Statement of Internal Control, specifically commenting on the fitness for purpose of the Assurance Framework, the completeness of risk management in the organisation and the integration of governance arrangements - the elements of which include clinical, corporate, financial and legal governance. 9. Policy and best practice 9.1. The committee shall have regard to: a. current good practice b. policies; and c. guidance; issued by the National Commissioning Board, the clinical commissioning group and other relevant bodies.

Page | 9
10. Conduct of the committee 10.1. The committee shall conduct its business in accordance with these terms of reference and the clinical commissioning group’s governance arrangements. It shall be informed by the aims, mission and values of the group. 11. Review 11.1. These terms of reference shall be reviewed not less than every three years by Governing Body. 11.2. In particular the terms of reference will be reviewed in the light of Francis Inquiry.

Final Version
Appendix C
Lower Lea Valley Locality Commissioning Board Committee
Terms of Reference 2015/16

Final Version
1. Introduction 1.1 The Lower Lea Valley Locality Commissioning Board (LCB) Committee (The
Committee) is established in accordance with section 6 of NHS East and North Hertfordshire Clinical Commissioning Group’s Constitution, as a Committee of the Governing Body.
2. Membership 2.1 Member practices are The Maples Health Centre, Cromwell and Wormley Medical
Centre, High Street Surgery, Stockwell Lodge Medical Centre, Warden Lodge, Cuffley and Goffs Oak Medical Centre, Abbey Road and Stanhope Surgery. The membership of the committee shall include:
Co-chairs Practice Date of current appointment
Dr Alison Jackson The Maples Health Centre
1st April 2015
Dr Ed Bosonnet Warden Lodge 1st April 2013
Practice: GP Clinical Lead / Clinical Representative:
The Maples Health Centre Dr Alison Jackson Cromwell and Wormley Medical Centre Dr Nikunji Malde High Street Surgery Dr Kalpana Misra Stockwell Lodge Medical Centre Dr Navina Sullivan Warden Lodge Dr Ed Bosonnet Cuffley and Goffs Oak Medical Centre Dr Pauline Taylor Abbey Road Dr William Neville Stanhope Surgery Dr Mo Hossain
Members of the committee should make every effort to attend all meetings of the committee. The Locality team will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report and Accounts.
2.2 In the event of the Co- Chairs of the committee being unable to attend all or part of the
meeting, they will nominate a replacement from within the Membership to deputise for that meeting.
2.3 The following representatives will usually be in attendance:
Partner agencies / patient representative: Practice Managers from member practices Pharmaceutical Adviser, CCG Locality Manager, CCG Associate Director CCG Director, CCG Chair of the Patient Commissioning Group

Final Version
• The LCB will provide a Prescribing Lead GP; a Mental Health Lead GP; a Patient Engagement Lead, and a Long Term Conditions Lead to sit on subcommittees of the CCG.
• The Lead representatives will act in a liaison role for the development of the specific areas, and feedback formally to the LCB in writing or verbally. These roles will be funded from the locality management allowance.
Lead Roles: Name: Patient Engagement & Involvement Dr Angela Goodwin Long Term Conditions Dr Alison Jackson & Nurse Emma Ross Mental Health Dr Chika Uduchukwu Prescribing Dr Mo Dabbagh Workforce Dr Louise Monk 3. Quorum 3.1 No formal business of the Committee(s) shall be transacted unless at least one half of
the whole number of members is present and at least one of the Co-Chairs is present.
4. Frequency of meetings and attendance 4.1 A minimum of 12 meetings per annum to include Locality Commissioning Board
meetings and TARGET events. Locality Commissioning Board meetings will be approximately 2 hours duration. TARGET events will normally be held 3 times a year.
4.2 Minimum Expectations of Member Practices
• A representative from each practice to attend 100% of meetings identified in Para 4.1.
• An identified GP Lead or their clinical representative from each practice to attend 80% of meetings for attendance linked payments.
• In recognition of possible difficulties in attendance for the smaller practices, should a GP attendance be difficult please inform the Locality Manager as soon as possible so that the issues can be documented. Evidence of consideration of the previous LCB minutes and comments to be forwarded to the Locality Manager prior to the meeting.
• Commitment to the three components of the Commissioning Framework (see appendix 1). Practices may select which elements of component 3 they wish to undertake.
• Engagement in regular practice reviews with the Co-Chairs of the LCB to analyse practice activity, performance in relation to key priorities and expenditure against the individual action plans
• It is expected that information from the committee meetings is disseminated at Practice level, as deemed appropriate by attendees. This may be via in-house meetings. It is advised that notes/minutes are taken so that they can be taken into account should the level of engagement be questioned.
• To support involvement of Practice Managers and other relevant Practice Staff in the CCG. All Practice Managers are encouraged to attend the LCB meetings.
• Participation in data collection, audits, reviews and validation as determined by the locality
• GP participation in locality TARGET days/locality wide events • All Practice staff to be involved in Locality TARGET events over the year. • GP participation in prescribing forum – attendance criteria as defined by the Forum -
and engagement with Prescribing Advisors

Final Version
• Practices to endorse patient representation to attend the Lower Lea Valley Patient Commissioning Group
• The Patient representative or their deputy will be invited to attend LCB meetings to provide a summary of the issues raised, either verbally or in writing, at the Patient Commissioning Group that related to the LCB.
5. Authority 5.1 The committee is authorised by the Governing Body to:
• Appoint and remove practice representatives
6. Emergency powers 6.1 Where an urgent decision needs to be made in between scheduled meetings,
members of the committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or
the exchange of emails. The exercise of such powers shall be reported and minuted at the next committee meeting.
7. Duties 7.1 The duties of the committee can be categorized as follows:
• Encourage full clinical engagement of member practices to help to develop and deliver CCG objectives.
• Be involved in commissioning high quality services for our patients including service redesign and review, to improve outcomes for patients while making appropriate use of resources. When required they should have the mandate of their practices, after consultation with practices, to vote on issues of policy of the Locality Commissioning Board (LCB).
• Analyse locality expenditure and activity against the Locality Plan/budget allocation with the intention of achieving financial balance by managing elective, unplanned and prescribing spend.
• Take collective action if Locality plans drift from targets. • Work with the CCG to validate and monitor patient pathways to ensure their care is
planned to improve their outcomes and use resources efficiently. • Facilitate two-way communication between the committee and the locality patient
commissioning group.
8. Reporting arrangements to the Governing Body 8.1 The committee will report to the Governing Body on a quarterly basis and the following
documents will be presented:
• Locality Update • Locality Commissioning Plan
8.2 The LCB is accountable to East and North Herts CCG. The Chairs of the LCB will sit
on the CCG Governing Body and the locality will have one vote as detailed in the CCG Constitution.

Final Version
9. Reporting arrangements of other Committees and Groups 9.1 The following committees and groups will report into the committee and provide an
update to the LCB as necessary.
Meeting Name Frequency Locality Prescribing Group Bi-Monthly Patient Commissioning Group Quarterly
10. Statement of Interest Declaration 10.1 All LCB Members have completed a Statement of Interest Declaration. They are
declared prior to discussion of relevant items. They are re-issued annually by the CCG.
11. Voting
Each of the 8 practices will be represented at the LCB meeting and there will be 1 practice 1 vote. Only GP Clinical Lead/Clinical Representatives identified in Section 2, Membership, or their nominated representative are entitled to vote. A majority vote will be required when decisions are to be taken.
12. Annual review of the Committee The committee will undertake an annual self-assessment to:
Review that these Terms of Reference have been complied with and whether they remain fit for purpose;
Determine whether its planned activities and responsibilities for the previous year have been sufficiently discharged; and,
Recommend any changes and / or actions it considers necessary, in respect of the above.
Provide the Governing Body with an annual report, which details the outcome of the annual review.
13. Committee servicing 14.1 The committee shall be supported administratively by the Locality team, whose duties
in this respect will include:
Agreement of the Agenda with the Chair and collation of papers in-line with the committee’s Annual Cycle of Business;
Providing written notice of meetings to committee members, and the papers, not less than 4 working days before the meeting;
Taking the minutes and keeping a record of matters arising and issues to be carried forward;
Producing a single document to track the committee’s agreed actions and report progress to the committee;
Producing draft minutes for approval within 10 working days of the meeting.

Final Version
Terms of Reference reviewed by: Lower Lea Valley Locality Commissioning LCB Committee
Date approved: August 2015 Review Date: April 2016 Governing Body Approval Date: <insert date>

Final Version
Appendix 1 Commissioning Framework 2015/16 Allocation of Finance The total available per registered patient under commissioning framework is £5.00; it is broken down in the table below.
1. Engagement
• Attendance at meetings, defined within Locality Terms of Reference
• Responses to information requests within four weeks’ timeframe
• Support practice nurse network.
£1.00
2. Achieving Financial Balance
£1.00
3. Working to improve outcomes of patients with LTCs.: • Facilitating self-management and integrated care
planning for patients with Long Term Conditions • Proactive management of patients with long term
conditions (LTC) by making use of multi-disciplinary team working.
• Advanced care planning (ACP) undertaken to support
patients’ decisions and choices which will facilitate high quality end of life (EOL) care.
• Safe and appropriate prescribing to support practitioners
to adhere to the broad spectrum antibiotic guidance. • Support improvements in line with CCG Ambitions for
Carers
• Support improvements in line with CCG Ambitions for patients with Cancer
£0.50
£0.50
£0.50
£0.50
£0.50
£0.50
Total
£5.00

FINAL
Appendix D
North Herts Locality Commissioning Board Committee
Terms of Reference 2015/16

FINAL
1. Introduction 1.1 The North Herts Locality Commissioning Board (LCB) Committee (The Committee) is
established in accordance with section 6 of NHS East and North Hertfordshire Clinical Commissioning Group’s Constitution, as a sub-committee of the Governing Body.
2. Membership 2.1 Member practices are Ashwell Surgery, The Baldock Surgery, Birchwood Surgery,
Courtenay House, Garden City Surgery, Knebworth & Marymead Surgery, Nevells Road Surgery, Orford Lodge, Portmill Surgery, Regal Chambers, Sollershott Surgery, Whitwell Surgery. The membership of the committee shall include:
Co-chairs Practice Date of current appointment
Dr Rob Graham Birchwood Surgery 01/04/2013 Dr Fiona Sinclair Regal Chambers 01/04/2015
Practice: GP Clinical Lead / Clinical
Representative: Ashwell Surgery Dr Matthew Jarvis The Baldock Surgery Dr Richard Stanley Birchwood Surgery Dr Rob Graham Courtenay House Dr Keith Greenish Garden City Surgery Dr Adrian Wood Knebworth & Marymead Surgery Dr Rob Newby Nevells Road Surgery Dr Tim Ramsbottom Orford Lodge Dr Jeremy Cox Portmill Surgery Dr Suhail Alam Regal Chambers Dr Fiona Sinclair Sollershott Surgery Dr Richard Nevard Whitwell Surgery Dr Rajpreet Milan
Members of the committee should make every effort to attend all meetings of the committee. The Locality team will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report and Accounts.
2.2 In the event of the Co-Chairs of the committee being unable to attend all or part of the
meeting, they will nominate a replacement from within the Membership to deputise for that meeting.
2.3 The following representatives will usually be in attendance:
Partner agencies / patient representative: Practice Managers from member practices Community Pharmacist Pharmaceutical Adviser, CCG Locality Manager, CCG Associate Director, CCG Director, CCG Chair of the Patient Commissioning Group (PCG)

FINAL
• The LCB will provide a Prescribing Lead GP; a Community Pharmacist; a Mental Health Lead GP; a Patient Engagement Lead, a Long Term Conditions Lead and a Pathology Lead to sit on subcommittees of the CCG.
• The Lead representatives will act in a liaison role for the development of the specific areas, and feedback formally to the LCB in writing or verbally. These roles will be funded from the locality management allowance.
Lead Roles: Name: Patient Engagement & Involvement Dr Simon Chatfield Long Term Conditions
Dr Simon Chatfield
Mental Health vacant Pathology Dr Matt Jarvis Prescribing Lee Doherty
3. Quorum 3.1 No formal business of the Committee(s) shall be transacted unless at least one half of
the whole number of members is present and at least one of the Co-Chairs is present.
4. Frequency of meetings and attendance 4.1 A minimum of 11 meetings per annum to include Locality Commissioning Board
meetings and TARGET events. Locality Commissioning Board meetings will be approximately 2 hours duration. TARGET events will normally be held 3 times a year.
4.2 Minimum Expectations of Member Practices
• A representative from each practice to attend 100% of meetings identified in Para 4.1.
• An identified GP Lead or their clinical representative from each practice to attend 80% of meetings for attendance linked payments.
• In recognition of possible difficulties in attendance for the smaller practices, should GP/Clinical representation be difficult please inform the Locality Manager as soon as possible so that the issues can be documented. Evidence of consideration of the previous LCB minutes and comments to be forwarded to the Locality Manager prior to the meeting.
• If a practice is struggling to meet the attendance target, the remaining locality lead GPs will take a view on extenuating circumstances and the overall level of practice engagement in locality business.
• Commitment to the three components of the Commissioning Framework (see appendix 1). Practices may select which elements of component 3 they wish to undertake.
• Engagement in regular practice reviews with the Co-Chairs of the LCB to analyse practice activity, performance in relation to key priorities and expenditure against the individual action plans
• It is expected that information from the committee meetings is disseminated at Practice level, as deemed appropriate by attendees. This may be via in-house meetings. It is advised that notes/minutes are taken so that they can be taken into account should the level of engagement be questioned.
• To support involvement of Practice Managers and other relevant Practice Staff in the CCG. All Practice Managers are encouraged to attend the LCB meetings.
• Participation in data collection, audits, reviews and validation as determined by the locality
• GP participation in locality TARGET days/locality wide events

FINAL
• All Practices are to be represented at Locality TARGET events over the year. • GP participation in prescribing forum – attendance criteria as defined by the Forum -
and engagement with Prescribing Advisors • Practice Managers encouraged to attend the monthly Practice Manager forums. • Practices to endorse patient representation to attend the North Herts Patient
Commissioning Group • The patient representative or their deputy to be invited to attend LCB meetings to
provide a summary of the issues raised, either verbally or in writing, at the Patient Commissioning Group that relate to the LCB.
5. Authority 5.1 The committee is authorised by the Governing Body to:
• Appoint and remove practice representatives
6. Emergency powers 6.1 Where an urgent decision needs to be made in between scheduled meetings,
members of the committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or
the exchange of emails. The exercise of such powers shall be reported and minuted at the next committee meeting.
7. Duties 7.1 The duties of the committee can be categorised as follows:
• Encourage full clinical engagement of member practices to help to develop and deliver CCG objectives.
• Be involved in commissioning high quality services for our patients including service redesign and review, to improve outcomes for patients while making appropriate use of resources. When required they should have the mandate of their practices, after consultation with practices, to vote on issues of policy of the Locality Commissioning Board (LCB).
• Analyse locality expenditure and activity against the Locality Plan/budget allocation with the intention of achieving financial balance by managing elective, unplanned and prescribing spend.
• Take collective action if Locality plans drift from targets. • Work with the CCG to validate and monitor patient pathways to understand high
cost patients and ensure their care is planned to improve their outcome and use of resources.
• Facilitate two-way communication between the LCB and the locality patient commissioning group.
8. Reporting arrangements to the Governing Body 8.1 The committee will report to the Governing Body on a quarterly basis and the following
documents will be presented:
• Locality Update • Locality Commissioning Plan

FINAL
8.2 The LCB is accountable to East and North Herts CCG. The Chairs of the LCB will sit on the CCG Governing Body and the locality will have one vote as detailed in the CCG Constitution.
9. Reporting arrangements of other Committees and Groups 9.1 The following committees and groups will report into the committee and provide an
update to the LCB as necessary.
Meeting Name Frequency Locality Prescribing Group Bi-monthly North Herts Management LCB Monthly
10. Statement of Interest Declaration 10.1 All LCB Members have completed a Statement of Interest Declaration. They are
declared prior to discussion of relevant items. They are re-issued annually by the CCG.
11. Voting
Each of the 12 practices will be represented at the LCB meeting and there will be 1 practice 1 vote. Only GP Clinical Leads/Clinical Representatives identified in Section 2, Membership, or their nominated representative are entitled to vote. A majority vote will be required when decisions are to be taken.
12. Annual review of the Committee The committee will undertake an annual self-assessment to:
• Review that these Terms of Reference have been complied with and whether they remain fit for purpose;
• Determine whether its planned activities and responsibilities for the previous year have been sufficiently discharged; and,
• Recommend any changes and / or actions it considers necessary, in respect of the above.
• Provide the Governing Body with an annual report, which details the outcome of the annual review.
13. Committee servicing 11.1 The committee shall be supported administratively by the Locality team, whose duties
in this respect will include:
• Agreement of the Agenda with the Chair and collation of papers in-line with the committee’s Annual Cycle of Business;
• Providing written notice of meetings to committee members, and the papers, not less than 5 working days before the meeting;
• Taking the minutes and keeping a record of matters arising and issues to be carried forward;
• Producing a single document to track the committee’s agreed actions and report progress to the committee;
• Producing draft minutes for approval within 5 working days of the meeting.

FINAL
Terms of Reference reviewed by: North Herts Locality Commissioning LCB Committee
Date approved: August 2015 Review Date: April 2016 Governing Body Approval Date: <insert date>

FINAL
Appendix 1 Commissioning Framework 2015/16 Allocation of Finance The total available per registered patient under commissioning framework is £5.00; it is broken down in the table below.
1. Engagement
• Attendance at meetings, defined within Locality Terms of Reference
• Responses to information requests within four weeks’ timeframe
• Support practice nurse network.
£1.00
2. Achieving Financial Balance
£1.00
3. Working to improve outcomes of patients with LTCs.: • Facilitating self-management and integrated care
planning for patients with Long Term Conditions • Proactive management of patients with long term
conditions (LTC) by making use of multi-disciplinary team working.
• Advanced care planning (ACP) undertaken to support
patients’ decisions and choices which will facilitate high quality end of life (EOL) care.
• Safe and appropriate prescribing to support practitioners
to adhere to the broad spectrum antibiotic guidance. • Support improvements in line with CCG Ambitions for
Carers
• Support improvements in line with CCG Ambitions for patients with Cancer
£0.50
£0.50
£0.50
£0.50
£0.50
£0.50
Total
£5.00

Version 4
Appendix E
Stevenage Locality Commissioning Board Committee
Terms of Reference 2015/16

Version 4
1. Introduction 1.1 The Stevenage Locality Commissioning Board (LCB) Committee (The Committee) is
established in accordance with section 6 of NHS East and North Hertfordshire Clinical Commissioning Group’s Constitution, as a Committee of the Governing Body.
2. Membership 2.1 Member practices are Bedwell Medical Centre, Canterbury Way Surgery, Chells Way
Surgery, King George Surgery, Manor House Surgery, Shephall Way Surgery, St Nicholas Health Centre, Stanmore Medical Centre, and Symonds Green Health Centre. The membership of the committee shall include:
Co-chairs Practice Date of current appointment
Dr Prag Moodley Stanmore Medical Centre
1st April 2015
Dr Russell Hall Chells Way Surgery 1st April 2013
Practice: GP Clinical Lead / Clinical Representative:
Bedwell Medical Centre Dr Raveendram Canterbury Way Surgery Dr Selvadurai Chells Way Surgery Dr Russell Hall King George Surgery Dr Ramkissen Manor House Surgery Dr Duggan Shephall Way Surgery Dr Cormack St Nicholas Health Centre Dr Aziz Stanmore Medical Centre Dr Prag Moodley Symonds Green Health Centre Dr Masood
Members of the committee should make every effort to attend all meetings of the committee. The Locality team will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report and Accounts.
2.2 In the event of the Co- Chairs of the committee being unable to attend all or part of the
meeting, they will nominate a replacement from within the Membership to deputise for that meeting.
2.3 The following representatives will usually be in attendance:
Partner agencies / patient representative: Practice Managers from member practices Pharmaceutical Adviser, CCG Locality Manager, CCG Associate Director CCG Director, CCG Chair of the Patient Commissioning Group

Version 4
• The LCB will provide a Prescribing Lead GP; a Mental Health Lead GP; a Patient Engagement Lead, and a Long Term Conditions Lead to sit on subcommittees of the CCG.
• The Lead representatives will act in a liaison role for the development of the specific areas, and feedback formally to the LCB in writing or verbally. These roles will be funded from the locality management allowance.
Lead Roles: Name: Patient Engagement & Involvement Dr Raj Kaja Long Term Conditions Dr Chakraborty and Nurse Karen Smith Mental Health Dr Prag Moodley Prescribing Dr Rini Saha 3. Quorum 3.1 No formal business of the Committee(s) shall be transacted unless at least one half of
the whole number of members is present and at least one of the Co-Chairs is present.
4. Frequency of meetings and attendance 4.1 A minimum of 11 meetings per annum to include Locality Commissioning Board
meetings and TARGET events. Locality Commissioning Board meetings will be approximately 2 hours duration. TARGET events will normally be held 3 times a year.
4.2 Minimum Expectations of Member Practices
• A representative from each practice to attend 100% of meetings identified in Para 4.1.
• An identified GP Lead or their clinical representative from each practice to attend 80% of meetings for attendance linked payments.
• In recognition of possible difficulties in attendance for the smaller practices, should a GP attendance be difficult please inform the Locality Manager as soon as possible so that the issues can be documented. Evidence of consideration of the previous LCB minutes and comments to be forwarded to the Locality Manager prior to the meeting.
• Commitment to the three components of the Commissioning Framework (see appendix 1). Practices may select which elements of component 3 they wish to undertake.
• Engagement in regular practice reviews with the Co-Chairs of the LCB to analyse practice activity, performance in relation to key priorities and expenditure against the individual action plans
• It is expected that information from the committee meetings is disseminated at Practice level, as deemed appropriate by attendees. This may be via in-house meetings. It is advised that notes/minutes are taken so that they can be taken into account should the level of engagement be questioned.
• To support involvement of Practice Managers and other relevant Practice Staff in the CCG. All Practice Managers are encouraged to attend the LCB meetings.
• Participation in data collection, audits, reviews and validation as determined by the locality
• GP participation in locality TARGET days/locality wide events • All Practice staff to be involved in Locality TARGET events over the year. • GP participation in prescribing forum – attendance criteria as defined by the Forum -
and engagement with Prescribing Advisors • Practices to endorse patient representation to attend the Stevenage Patient
Commissioning Group

Version 4
• The Patient representative or their deputy will be invited to attend LCB meetings to provide a summary of the issues raised, either verbally or in writing, at the Patient Commissioning Group that related to the LCB.
5. Authority 5.1 The committee is authorised by the Governing Body to:
• Appoint and remove practice representatives
6. Emergency powers 6.1 Where an urgent decision needs to be made in between scheduled meetings,
members of the committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or
the exchange of emails. The exercise of such powers shall be reported and minuted at the next committee meeting.
7. Duties 7.1 The duties of the committee can be categorized as follows:
• Encourage full clinical engagement of member practices to help to develop and deliver CCG objectives.
• Be involved in commissioning high quality services for our patients including service redesign and review, to improve outcomes for patients while making appropriate use of resources. When required they should have the mandate of their practices, after consultation with practices, to vote on issues of policy of the Locality Commissioning Board (LCB).
• Analyse locality expenditure and activity against the Locality Plan/budget allocation with the intention of achieving financial balance by managing elective, unplanned and prescribing spend.
• Take collective action if Locality plans drift from targets. • Work with the CCG to validate and monitor patient pathways to ensure their care is
planned to improve their outcomes and use resources efficiently. • Facilitate two-way communication between the committee and the locality patient
commissioning group.
8. Reporting arrangements to the Governing Body 8.1 The committee will report to the Governing Body on a quarterly basis and the following
documents will be presented:
• Locality Update • Locality Commissioning Plan
8.2 The LCB is accountable to East and North Herts CCG. The Chairs of the LCB will sit
on the CCG Governing Body and the locality will have one vote as detailed in the CCG Constitution.
9. Reporting arrangements of other Committees and Groups 9.1 The following committees and groups will report into the committee and provide an
update to the LCB as necessary.

Version 4
Meeting Name Frequency
Locality Prescribing Group Bi-Monthly Stevenage Patient Commissioning Group
Quarterly
10. Statement of Interest Declaration 10.1 All LCB Members have completed a Statement of Interest Declaration. They are
declared prior to discussion of relevant items. They are re-issued annually by the CCG.
11. Voting
Each of the 9 practices will be represented at the LCB meeting and there will be 1 practice 1 vote. Only GP Clinical Lead/Clinical Representatives identified in Section 2, Membership, or their nominated representative are entitled to vote. A majority vote will be required when decisions are to be taken.
12. Annual review of the Committee The committee will undertake an annual self-assessment to:
Review that these Terms of Reference have been complied with and whether they remain fit for purpose;
Determine whether its planned activities and responsibilities for the previous year have been sufficiently discharged; and,
Recommend any changes and / or actions it considers necessary, in respect of the above.
Provide the Governing Body with an annual report, which details the outcome of the annual review.
13. Committee servicing 14.1 The committee shall be supported administratively by the Locality team, whose duties
in this respect will include:
Agreement of the Agenda with the Chair and collation of papers in-line with the committee’s Annual Cycle of Business;
Providing written notice of meetings to committee members, and the papers, not less than 4 working days before the meeting;
Taking the minutes and keeping a record of matters arising and issues to be carried forward;
Producing a single document to track the committee’s agreed actions and report progress to the committee;
Producing draft minutes for approval within 10 working days of the meeting.

Version 4
Terms of Reference reviewed by: Stevenage Locality Commissioning LCB Committee
Date approved: August 2015 Review Date: April 2016 Governing Body Approval Date: <insert date>

Version 4
Appendix 1 Commissioning Framework 2015/16 Allocation of Finance The total available per registered patient under commissioning framework is £5.00; it is broken down in the table below.
1. Engagement
• Attendance at meetings, defined within Locality Terms of Reference
• Responses to information requests within four weeks’ timeframe
• Support practice nurse network.
£1.00
2. Achieving Financial Balance
£1.00
3. Working to improve outcomes of patients with LTCs.: • Facilitating self-management and integrated care
planning for patients with Long Term Conditions • Proactive management of patients with long term
conditions (LTC) by making use of multi-disciplinary team working.
• Advanced care planning (ACP) undertaken to support
patients’ decisions and choices which will facilitate high quality end of life (EOL) care.
• Safe and appropriate prescribing to support practitioners
to adhere to the broad spectrum antibiotic guidance. • Support improvements in line with CCG Ambitions for
Carers
• Support improvements in line with CCG Ambitions for patients with Cancer
£0.50
£0.50
£0.50
£0.50
£0.50
£0.50
Total
£5.00

Appendix F
Stort Valley and Villages Locality Commissioning Board Terms of Reference
2015/16

1. Introduction 1.1 The Stort Valley and Villages Locality Commissioning Board (LCB) Committee (The
Committee) is established in accordance with Section 6 of the NHS East and North Hertfordshire Clinical Commissioning Group’s (E&NH CCG) constitution as a Committee of the Governing Body.
2. Membership
Member practices include Central Surgery, Sawbridgeworth, Much Hadham Surgery, Church Street Surgery Group, Parsonage Surgery and South Street Surgery in Bishop’s Stortford. The Locality group will also represent the Sawbridgeworth Medical Services Practice. The membership of the committee shall include: Co-chairs Practice Date of appointment Dr Deborah Kearns Central Surgery
Sawbridgeworth 01.04.2013
Dr Nabeil Shukur South Street, Surgery
01.04.2013
Practice: GP Clinical Lead/
Clinical Representative: Central Surgery, Sawbridgeworth Dr Deborah Kearns Church Street, Bishops Stortford
Dr Mark Penwill
Much Hadham Health Centre Much Hadham
Dr Nathalie Oates
Parsonage Surgery Bishops Stortford
Dr Jag Takhar
South Street Surgery Bishops Stortford
Dr Nabeil Shukur
2.2 Members of the committee should make every effort to attend all meetings of the
committee. The Locality team will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report and Accounts.
2.3 In the event of the Co- Chairs of the committee being unable to attend all or part of the
meeting, they will nominate a replacement from within the Membership to deputise for that meeting.
2.4 Representatives in Attendance 2.4.1 The following representatives will usually be in attendance:
Chair of the Patient Commissioning Group Practice Managers from member practices Nurse / AHP Representative Pharmaceutical Adviser CCG Locality Manager CCG Patient Representative Associate Director CCG Director CCG

2.4.2 Lead Roles The LCB will provide a Prescribing Lead GP; a Mental Health Lead GP; a Patient
Engagement Lead, a Long Terms Conditions Lead to sit on subcommittees of the CCG.
The Lead Representatives will act in a liaison role for the development of their specific
areas, and feedback formally to the LCB in writing or verbally. These roles will be funded from the locality management allowance.
Lead Roles:
Name:
Patient Engagement & Involvement Dr Sarah Dixon (South Street Surgery)
Long Term Conditions Lead – Managing Respiratory pathways redesign
Dr Jag Takhar (Parsonage Surgery)
Mental Health Dr Vishal Kapil (Central Surgery)
Prescribing
Dr Sarah Dixon (South Street Surgery)
Lead Nurse To be advised
3. Quorum 3.1 No formal business of the committee(s) shall be transacted unless at least one half of the
whole number of members is present and at least one of either the Chair or Deputy Chair is present.
4. Frequency of meetings and attendance 4.1 Attendance of at least 11 meetings per annum to include LCB meetings and TARGET
events. 4.2 Minimum Expectations of Member Practices
A representative from each practice to attend 100% of meetings identified in para 4.1.
An identified GP Lead, or their clinical representative, from each practice to attend 80% of meetings identified in para 4.1 for attendance linked payments
In recognition of possible difficulties in attendance for the smaller practices, should a GP attendance be difficult please inform the Locality Manager as soon as possible so that the issues can be documented. Evidence of consideration of the previous LCB minutes and comments to be forwarded to the Locality Manager prior to the meeting.
All Practices are to be represented at all Locality TARGET events over the year. GP participation in locality TARGET days/locality wide events Commitment to all components of the Commissioning Framework
(see Appendix 1). Engagement in regular practice reviews with the co-leads of the LCB to analyse
practice activity, performance in relation to key priorities and expenditure against the individual action plans.
It is expected that information from the committee meetings is disseminated at Practice level, as deemed appropriate by attendees. This may be via in-house

meetings. It is advised that notes/minutes are taken so that they can be taken into account should the level of engagement be questioned.
To support involvement of Practice Managers and other relevant Practice Staff in CCG, all Practice Managers are encouraged to attend the LCB meetings.
Participation in data collection, audits, reviews and validation as determined by the locality.
GP participation in prescribing forum and engagement with Prescribing Advisors; Attendance criteria as defined by the Forum.
Practice Managers are encouraged to attend the monthly Practice Manager forums, attendance at a minimum of 10 meetings per year.
Practices to endorse patient representation to attend the Stort Valley and Villages Patient Commissioning Group.
The Patient representative or their deputy, will be invited to attend meetings to provide an outline of the issues raised, either verbally or in writing, at the Patient Commissioning Group that relate to the LCB.
5. Authority 5.1 The committee is authorised by the Governing Body to
Appoint and remove Practice Representatives.
6. Emergency powers 6.1 Where an urgent decision needs to be made in-between scheduled meetings,
members of the committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or
the exchange of emails. The exercise of such powers shall be reported and minuted at the next committee meeting.
7. Duties 7.1 The duties of the committee can be categorised as follows:
Encourage full clinical engagement of member practices to help to develop and deliver CCG objectives.
Be involved in commissioning high quality services for our patients including service redesign and review, to improving outcomes for patients while making appropriate use of resources. When required they should have the mandate of their practices, after consultation with practices, to vote on issues of policy of the Locality Commissioning LCB.
Analyse locality expenditure and activity against the Locality Plan/budget allocation with the intention of achieving financial balance by managing elective, unplanned and prescribing spend.
Take collective action if Locality Plans drift from targets. Work with the CCG to validate and monitor patient pathways to understand high
cost patients and ensure their care is planned to improve their outcome and use of resources.
Facilitate two-way communication between the committee and the locality patient commissioning group
8. Reporting arrangements to the Governing Body 8.1 The committee will report to the Governing Body on a quarterly basis and the following
documents will be presented:

Locality Update Locality Commissioning Plan
8.2 The LCB is accountable to East and North Herts CCG. The Chairs of the LCB will sit
on the CCG Governing Body and the locality will have one vote as detailed in the CCG Constitution.
9. Reporting arrangements of other Committees and Groups 9.1 The following committees and groups will report into the committee and provide an
update to the LCB as necessary.
Meeting Name Frequency Locality Prescribing Group Quarterly
10. Statement of Interest Declaration 10.1 All LCB Members to have completed a Statement of Interest Declaration. They are
declared prior to discussion of relevant items. They are re-issued annually by the CCG.
11. Voting 11.1 Each of the 5 practices will be represented at the LCB meeting and there will be 1
practice 1 vote. Only practice representatives named in Section 2.1, Membership, or their nominated clinical representative are entitled to vote. A majority vote will be required when decisions are to be taken.
12. Annual review of the Committee 12.1 The committee will undertake an annual self-assessment to:
Review that these Terms of Reference have been complied with and whether they remain fit for purpose.
Determine whether its planned activities and responsibilities for the previous year have been sufficiently discharged; and,
Recommend any changes and / or actions it considers necessary, in respect of the above.
Provide the Governing Body with an annual report, which details the outcome of the annual review.
13. Committee servicing 13.1 The committee shall be supported administratively by the Locality team, whose duties
in this respect will include:
Agreement of the Agenda with the Chair and collation of papers in-line with the committee’s Annual Cycle of Business;
Providing written notice of meetings to committee members, and the papers, not less than 5 working days before the meeting;
Taking the minutes and keeping a record of matters arising and issues to be carried forward;
Producing a single document to track the committee’s agreed actions and report progress to the committee;
Producing draft minutes for approval within 5 working days of the meeting.

Terms of Reference reviewed by: Stort Valley and Villages Locality Commissioning Committee
Date approved: July 2015 Review Date: July 2016 Governing Body Approval Date:

Appendix 1
Commissioning Framework 2015/16 Allocation of Finance The total available per registered patient under commissioning framework is £5.00; it is broken down in the table below.
1. Engagement
• Attendance at meetings, defined within Locality Terms of Reference
• Responses to information requests within four weeks’ timeframe
• Support practice nurse network.
£1.00
2. Achieving Financial Balance
£1.00
3. Working to improve outcomes of patients with LTCs.: • Facilitating self-management and integrated care
planning for patients with Long Term Conditions • Proactive management of patients with long term
conditions (LTC) by making use of multi-disciplinary team working.
• Advanced care planning (ACP) undertaken to support
patients’ decisions and choices which will facilitate high quality end of life (EOL) care.
• Safe and appropriate prescribing to support practitioners
to adhere to the broad spectrum antibiotic guidance. • Support improvements in line with CCG Ambitions for
Carers
• Support improvements in line with CCG Ambitions for patients with Cancer
£0.50
£0.50
£0.50
£0.50
£0.50
£0.50
Total
£5.00

Appendix G
Upper Lea Valley Locality Commissioning Board Terms of Reference
2015/16

1. Introduction 1.1 The Upper Lea Valley Locality Commissioning Board (LCB) Committee (The
Committee) is established in accordance with Section 6 of the NHS East and North Hertfordshire Clinical Commissioning Group’s (E&NH CCG) constitution as a Committee of the Governing Body.
2. Membership 2.1 Member practices are: Amwell Street Surgery, Castlegate Surgery, Church Street
Surgery, Dolphin House Surgery, Hailey View Surgery, Hanscombe House Surgery, The Limes Surgery, The Maltings Surgery, Orchard Surgery, Park Lane Surgery, Wallace House Surgery, Watton Place Clinic, Ware Road Surgery, Puckeridge & Buntingford Medical Centre. The Locality group will also represent Haileybury College Practice. The membership of the committee shall include:
Co-chairs Practice Date of appointment Dr Steve Kite The Maltings Surgery 01.04.2013 Dr Nicky Williams Ware Road Surgery 01.04.2013 Dr Mark Andrews The Limes Surgery 01.04.2013
Practice: GP Clinical Lead / Clinical Representative
Amwell Street Surgery, Hoddesdon Dr Jo Roberts Castlegate Surgery Hertford
Dr Alice Baldock
Church Street Surgery, Ware Dr Nicky Williams Dolphin House Surgery, Ware Dr David Maddams Hailey View Surgery, Hoddesdon Dr Rob Mayson Hanscombe House Surgery, Hertford Dr Anita Oates The Limes Surgery, Hoddesdon Dr Mark Andrews
(Locality Co-Chair) The Maltings Surgery, Ware
Dr Steve Kite (Locality Chair)
Park Lane Surgery, Broxbourne Dr Jacqui Sheridan Wallace House Surgery, Hertford Dr Jay Kuruvatti Watton Place Clinic, Watton-on-Stone
Dr Dilesh Shah
Ware Road Surgery, Hertford
Clinical Directors from Ephedra on rotation: Dr Neil Dytham Dr Michael Rule Dr Sejun Adeuja
Orchard Surgery, Buntingford Buntingford Surgery, Buntingford Dr Megan Phillimore-Brown Puckeridge Surgery Dr Will Nicholson
2.2 Members of the committee should make every effort to attend all meetings of the committee. The Locality team will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report and Accounts.

2.3 In the event of the Co- Chairs of the committee being unable to attend all or part of the meeting, they will nominate a replacement from within the Membership to deputise for that meeting.
2.4 Representatives in Attendance 2.4.1 The following representatives will usually be in attendance:
Chair of Patient Commissioning Group (PCG) Practice Managers from member practices Nurse / AHP Representative Pharmaceutical Adviser CCG Locality Manager CCG Associate Director CCG Director CCH
2.4.2 Lead Roles The LCB will provide a Prescribing Lead GP; a Mental Health Lead GP; a Patient
Engagement Lead, a Long Terms Conditions Lead, a Diabetes Lead to sit on subcommittees of the CCG.
The Lead representative will act in a liaison role for the development of their specific
areas and engage formally with the LCB either verbally or in writing. These roles will be funded from the locality management allowance.
Lead Roles:
Name:
Long Term Conditions Lead – Managing Respiratory pathways redesign
Dr Martyn Davies (Dolphin House Surgery)
Mental Health Dr Jay Kuruvatti (Wallace House Surgery)
Prescribing
Dr Nick Condon (Park Lane Surgery)
Finance Dr Jacqui Sheridan
Practice Nurse Lead Lucy Eldon
3. Quorum 3.1 No formal business of the committee(s) shall be transacted unless at least one half of the
whole number of members is present and at least one of either the Chair or Deputy Chair is present.
4. Frequency of meetings and attendance 4.1 Attendance of at least 11 meetings per annum to include Locality Committee Board
meetings and TARGET events.

4.2 Minimum Expectations of Member Practices An identified GP Lead or Representative from each Practice to attend 100% of
meetings identified in Para 4.1 An identified GP lead or a clinical representative from each practice to attend 80%
of meetings for attendance linked payments. In recognition of possible difficulties in attendance for the smaller practices, should
a GP attendance be difficult please inform the Locality Manager as soon as possible so that the issues can be documented. Evidence of consideration of the previous LCB minutes and comments to be forwarded to the Locality Manager prior to the meeting.
All Practices are to be represented at all Locality TARGET events over the year. GP participation in locality TARGET days/locality wide events Commitment to all components of the Commissioning Framework
(see Appendix 1). Engagement in regular practice reviews with the co-leads of the LCB to analyse
practice activity, performance in relation to key priorities and expenditure against the individual action plans.
It is expected that information from the committee meetings is disseminated at Practice level, as deemed appropriate by attendees. This may be via in-house meetings. It is advised that notes/minutes are taken so that they can be taken into account should the level of engagement be questioned.
To support involvement of Practice Managers and other relevant Practice Staff in CCG, all Practice Managers are encouraged to attend the LCB meetings.
Participation in data collection, audits, reviews and validation as determined by the locality.
GP participation in prescribing forum and engagement with Prescribing Advisors; Attendance criteria as defined by the Forum.
Practice Managers are encouraged to attend the monthly Practice Manager forums, attendance at a minimum of 10 meetings per year.
Practices to endorse patient representation to attend the Upper Lea Valley Patient Commissioning Group.
The Patient representative or their deputy will be invited to attend meetings to provide an outline of the issues raised, either verbally or in writing, at the Patient Commissioning Group that relate to the LCB.
5. Authority 5.1 The committee is authorised by the Governing Body to
Appoint and remove Practice Representatives.
6. Emergency powers 6.1 Where an urgent decision needs to be made in-between scheduled meetings,
members of the committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or
the exchange of emails. The exercise of such powers shall be reported and minuted at the next committee meeting.
7. Duties 7.1 The duties of the committee can be categorised as follows:
Encourage full clinical engagement of member practices to help to develop and deliver CCG objectives.

Be involved in commissioning high quality services for our patients including service redesign and review, to improving outcomes for patients while making appropriate use of resources. When required they should have the mandate of their practices, after consultation with practices, to vote on issues of policy of the Locality Commissioning LCB.
Analyse locality expenditure and activity against the Locality Plan/budget allocation with the intention of achieving financial balance by managing elective, unplanned and prescribing spend.
Take collective action if Locality Plans drift from targets. Work with the CCG to validate and monitor patient pathways to understand high
cost patients and ensure their care is planned to improve their outcome and use of resources.
Facilitate two-way communication between the committee and the locality patient commissioning group
8. Reporting arrangements to the Governing Body 8.1 The committee will report to the Governing Body on a quarterly basis and the following
documents will be presented:
Locality Update Locality Commissioning Plan
8.2 The LCB is accountable to East and North Herts CCG. The Chairs of the LCB will sit
on the CCG Governing Body and the locality will have one vote as detailed in the CCG Constitution.
9. Reporting arrangements of other Committees and Groups 9.1 The following committees and groups will report into the committee and provide an
update to the LCB as necessary.
Meeting Name Frequency Locality Prescribing Group Quarterly Finance Sub Committee Quarterly
10. Statement of Interest Declaration 10.1 All LCB Members to have completed a Statement of Interest Declaration. They are
declared prior to discussion of relevant items. They are re-issued annually by the CCG.
11. Voting 11.1 Each of the 15 practices will be represented at the LCB meeting and there will be 1
practice 1 vote. Only practice representatives named in Section 2.1, Membership, or their nominated clinical representative are entitled to vote. A majority vote will be required when decisions are to be taken.
12. Annual review of the Committee 12.1 The committee will undertake an annual self-assessment to:
Review that these Terms of Reference have been complied with and whether they remain fit for purpose.

Determine whether its planned activities and responsibilities for the previous year have been sufficiently discharged; and,
Recommend any changes and / or actions it considers necessary, in respect of the above.
Provide the Governing Body with an annual report, which details the outcome of the annual review.
13. Committee servicing 13.1 The committee shall be supported administratively by the Locality team, whose duties
in this respect will include:
Agreement of the Agenda with the Chair and collation of papers in-line with the committee’s Annual Cycle of Business;
Providing written notice of meetings to committee members, and the papers, not less than 5 working days before the meeting;
Taking the minutes and keeping a record of matters arising and issues to be carried forward;
Producing a single document to track the committee’s agreed actions and report progress to the committee;
Producing draft minutes for approval within 5 working days of the meeting.
Terms of Reference reviewed by: Upper lea Valley Locality Commissioning Committee
Date approved: Review Date: July 2016 Governing Body Approval Date:

Appendix 1 Commissioning Framework 2015/16 Allocation of Finance The total available per registered patient under commissioning framework is £5.00; it is broken down in the table below.
1. Engagement
• Attendance at meetings, defined within Locality Terms of Reference
• Responses to information requests within four weeks’ timeframe
• Support practice nurse network.
£1.00
2. Achieving Financial Balance
£1.00
3. Working to improve outcomes of patients with LTCs.: • Facilitating self-management and integrated care
planning for patients with Long Term Conditions • Proactive management of patients with long term
conditions (LTC) by making use of multi-disciplinary team working.
• Advanced care planning (ACP) undertaken to support
patients’ decisions and choices which will facilitate high quality end of life (EOL) care.
• Safe and appropriate prescribing to support practitioners
to adhere to the broad spectrum antibiotic guidance. • Support improvements in line with CCG Ambitions for
Carers
• Support improvements in line with CCG Ambitions for patients with Cancer
£0.50
£0.50
£0.50
£0.50
£0.50
£0.50
Total
£5.00

Version 4
Appendix H
WelHat Locality Commissioning Board Committee
Terms of Reference 2015/16

Version 4
1. Introduction 1.1 The WelHat Locality Commissioning Board (LCB) Committee (The Committee) is
established in accordance with section 6 of NHS East and North Hertfordshire Clinical Commissioning Group’s Constitution, as a Committee of the Governing Body.
2. Membership 2.1 Member practices are Bridge Cottage Surgery, Burvill House Surgery, Garden City
Practice, Hall Grove Surgery, Lister House Surgery, Peartree Lane Surgery, Potterells Medical Centre, Spring House Medical Centre and Wrafton House Surgery. The membership of the committee shall include:
Co-chairs Practice Date of current appointment
Dr Ashish Shah Wrafton House 1st November 2014 Dr Peter Shilliday Garden City Practice 1st July 2014 (resign 31st
August 2015) Dr Sachin Gupta Garden City Practice 1st November 2015
Practice: GP Clinical Lead / Clinical Representative:
Bridge Cottage Surgery Dr Segun Adeuja Burvill House Surgery Dr Neil Dytham The Garden City Practice Dr Sachin Gupta Hall Grove Surgery Dr Francis Cranfield Lister House Surgery Dr Richard Lavelle Peartree Lane Surgery Dr Mick Rule Potterells Medical Centre Dr Sarah Hoole Spring House Medical Centre Dr Eva Kreye Wrafton House Surgery Dr Anne Kelley
Members of the committee should make every effort to attend all meetings of the committee. The Locality team will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report and Accounts.
2.2 In the event of the Co- Chairs of the committee being unable to attend all or part of the
meeting, they will nominate a replacement from within the Membership to deputise for that meeting.
2.3 The following representatives will usually be in attendance:
Partner agencies / patient representative: Practice Managers from member practices Pharmaceutical Adviser, CCG Locality Manager, CCG Associate Director CCG Director, CCG Chair of the Patient Commissioning Group

Version 4
• The LCB will provide a Prescribing Lead GP; a Mental Health Lead GP; a Patient Engagement Lead, and a Long Term Conditions Lead to sit on subcommittees of the CCG.
• The Lead representatives will act in a liaison role for the development of the specific areas, and feedback formally to the LCB in writing or verbally. These roles will be funded from the locality management allowance.
Lead Roles: Name: Patient Engagement & Involvement Dr Tina Archdeacon and Dr Carrie Keane Long Term Conditions Dr Sarah Hoole Mental Health Dr Barbara Hanak Pathology Dr Richard Lavelle Prescribing Dr Steve Price 3. Quorum 3.1 No formal business of the Committee(s) shall be transacted unless at least one half of
the whole number of members is present and at least one of the Co-Chairs is present.
4. Frequency of meetings and attendance 4.1 A minimum of 11 meetings per annum to include Locality Commissioning Board
meetings and TARGET events. Locality Commissioning Board meetings will be approximately 2 hours duration. TARGET events will normally be held 2 times a year.
4.2 Minimum Expectations of Member Practices
• A representative from each practice to attend 100% of meetings identified in Para 4.1.
• An identified GP Lead or their clinical representative from each practice to attend 80% of meetings for attendance linked payments.
• In recognition of possible difficulties in attendance for the smaller practices, should a GP attendance be difficult please inform the Locality Manager as soon as possible so that the issues can be documented. Evidence of consideration of the previous LCB minutes and comments to be forwarded to the Locality Manager prior to the meeting.
• Commitment to the three components of the Commissioning Framework (see appendix 1). Practices may select which elements of component 3 they wish to undertake.
• Engagement in regular practice reviews with the Co-Chairs of the LCB to analyse practice activity, performance in relation to key priorities and expenditure against the individual action plans
• It is expected that information from the committee meetings is disseminated at Practice level, as deemed appropriate by attendees. This may be via in-house meetings. It is advised that notes/minutes are taken so that they can be taken into account should the level of engagement be questioned.
• To support involvement of Practice Managers and other relevant Practice Staff in the CCG. All Practice Managers are encouraged to attend the LCB meetings.
• Participation in data collection, audits, reviews and validation as determined by the locality
• GP participation in locality TARGET days/locality wide events • All Practice staff to be involved in Locality TARGET events over the year. • GP participation in prescribing forum – attendance criteria as defined by the Forum -
and engagement with Prescribing Advisors

Version 4
• Practices to endorse patient representation to attend the WelHat Patient Commissioning Group
• The Patient representative or their deputy will be invited to attend LCB meetings to provide a summary of the issues raised, either verbally or in writing, at the Patient Commissioning Group that related to the LCB.
5. Authority 5.1 The committee is authorised by the Governing Body to:
• Appoint and remove practice representatives
6. Emergency powers 6.1 Where an urgent decision needs to be made in between scheduled meetings,
members of the committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or
the exchange of emails. The exercise of such powers shall be reported and minuted at the next committee meeting.
7. Duties 7.1 The duties of the committee can be categorised as follows:
• Encourage full clinical engagement of member practices to help to develop and deliver CCG objectives.
• Be involved in commissioning high quality services for our patients including service redesign and review, to improve outcomes for patients while making appropriate use of resources. When required they should have the mandate of their practices, after consultation with practices, to vote on issues of policy of the Locality Commissioning Board (LCB).
• Analyse locality expenditure and activity against the Locality Plan/budget allocation with the intention of achieving financial balance by managing elective, unplanned and prescribing spend.
• Take collective action if Locality plans drift from targets. • Work with the CCG to validate and monitor patient pathways to ensure their care is
planned to improve their outcomes and use resources efficiently. • Facilitate two-way communication between the committee and the locality patient
commissioning group.
8. Reporting arrangements to the Governing Body 8.1 The committee will report to the Governing Body on a quarterly basis and the following
documents will be presented:
• Locality Update • Locality Commissioning Plan
8.2 The LCB is accountable to East and North Herts CCG. The Chairs of the LCB will sit
on the CCG Governing Body and the locality will have one vote as detailed in the CCG Constitution.

Version 4
9. Reporting arrangements of other Committees and Groups 9.1 The following committees and groups will report into the committee and provide an
update to the LCB as necessary.
Meeting Name Frequency Locality Prescribing Group Bi-Monthly WelHat Management LCB Monthly
10. Statement of Interest Declaration 10.1 All LCB Members have completed a Statement of Interest Declaration. They are
declared prior to discussion of relevant items. They are re-issued annually by the CCG.
11. Voting
Each of the 9 practices will be represented at the LCB meeting and there will be 1 practice 1 vote. Only GP Clinical Lead/Clinical Representatives identified in Section 2, Membership, or their nominated representative are entitled to vote. A majority vote will be required when decisions are to be taken.
12. Annual review of the Committee The committee will undertake an annual self-assessment to:
Review that these Terms of Reference have been complied with and whether they remain fit for purpose;
Determine whether its planned activities and responsibilities for the previous year have been sufficiently discharged; and,
Recommend any changes and / or actions it considers necessary, in respect of the above.
Provide the Governing Body with an annual report, which details the outcome of the annual review.
13. Committee servicing 14.1 The committee shall be supported administratively by the Locality team, whose duties
in this respect will include:
Agreement of the Agenda with the Chair and collation of papers in-line with the committee’s Annual Cycle of Business;
Providing written notice of meetings to committee members, and the papers, not less than 4 working days before the meeting;
Taking the minutes and keeping a record of matters arising and issues to be carried forward;
Producing a single document to track the committee’s agreed actions and report progress to the committee;
Producing draft minutes for approval within 10 working days of the meeting.

Version 4
Terms of Reference reviewed by: WelHat Locality Commissioning LCB Committee
Date approved: August 2015 Review Date: April 2016 Governing Body Approval Date: <insert date>

Version 4
Appendix 1 Commissioning Framework 2015/16 Allocation of Finance The total available per registered patient under commissioning framework is £5.00; it is broken down in the table below.
1. Engagement
• Attendance at meetings, defined within Locality Terms of Reference
• Responses to information requests within four weeks’ timeframe
• Support practice nurse network.
£1.00
2. Achieving Financial Balance
£1.00
3. Working to improve outcomes of patients with LTCs.: • Facilitating self-management and integrated care
planning for patients with Long Term Conditions • Proactive management of patients with long term
conditions (LTC) by making use of multi-disciplinary team working.
• Advanced care planning (ACP) undertaken to support
patients’ decisions and choices which will facilitate high quality end of life (EOL) care.
• Safe and appropriate prescribing to support practitioners
to adhere to the broad spectrum antibiotic guidance. • Support improvements in line with CCG Ambitions for
Carers
• Support improvements in line with CCG Ambitions for patients with Cancer
£0.50
£0.50
£0.50
£0.50
£0.50
£0.50
Total
£5.00

Page 1 of 6
Appendix I
2015/16 Strategic Risk Register – Quarter 2 (July - September 2015)
Linked with: Previous Risk RatingJune 2015
Current Risk RatingSept 2015
Key Controls Assurance Gaps in Controls/Assurances Actions required Date Target Risk Rating
Progress Update
SO1 - To commission safe and appropriate health care services
RCAD Risks:Ref 1.9 - Score 12 (4/3)Ref 1.10 - Score 9 (3/3)Ref 1.17 - Score 8 (4/2)Ref 1.24 - Score 8 (4/2)Ref 1.25 - Score 12 (4/3)Ref 1.26 - Score 9 (3/3)Ref 1.27 - Score 12 (3/4)Ref 1.32 - Score 12 (4/3)Ref 1.33 - Score 12 (4/3)Ref 1.34 - Score 12 (3/4)Ref 1.41 - Score 12 (4/3)Ref 1.46 - Score 12 (3/4)Ref 1.49 - Score 9 (3/3)Ref 1.50 - Score 16 (4/4)Ref 1.51 - Score 12 (3/4)Ref 1.52 - Score 12 (3/4)Ref 2.1 - Score 8 (4/2)Ref 2.2 - Score 9 (3/3)Ref 2.11 - Score 12 (3/4)Ref 2.12 - Score 9 (3/3)Ref 2.14 - Score 12 (3/4)Ref 2.15 - Score 4 (2/2)Ref 3.5 - Score 12 (3/4)Ref 3.11 - Score 12 (3/4)Ref 3.13 - Score 9 (3/3)Ref 4.1 - Score 9 (3/3)Ref 4.11 - Score 8 (4/2)Ref 4.19 - Score 12 (4/3)
Strategic Risk 1: Failure of the CCG to ensure delivery of safe, high quality and effective services from appropriately commissioned providersLead Director – Sheilagh Reavey – Director of Nursing and Quality
• Robust programme of quality monitoring and assurance visits• Quarterly Quality Committee • Quality review meetings with providers• CCG directly responsible for the team undertaking quality monitoring.• Programme to monitor CQUINs, and requirements of quality and information schedules in contracts.• Programme of announced and unannounced quality visits• PPG involvement in quality monitoring• Programme of Section 11 visits to providers.• Increased control of infection capacity• Memorandum of Understanding with HVCCG for safeguarding adults service• Monitoring of the enhanced framework• Hotline Resource recruited to and Hotline Transfer to Quality Team• On-going monitoring of staffing returns• Health needs assessment and profile for Looked After Children developed• Ward level indicators analysed (safer staffing information and safety metrics from all providers monthly now in place)• Utilise specialist support for deep dives• Enhanced operational support to providers to EN Herts• Implemented the LAC model.
• Governance and Audit Committee deep dive• Internal audit recommendations implemented:- Risk management (amber/green)- Performance (amber/green)• Bi-monthly quality reports to Governance and Audit• Externally commissioned report on LAC• Use of patient stories.• CQC visit for safeguarding• CQC inspection outcomes of providers.• Area Team Check Point Reviews and Quality Surveillance Group• Bi- monthly Quality and performance reports to Governing Body.• Mortality data framework agreed• Palliative and respiratory care review with EN Herts agreed• Royal Free now responsible for Barnet and Chase Farm• Exec to Exec held with West Essex• C Diff rates lower than same period last year in provider organisations (increase in community acquired infections)• Provider cost improvement programmes are signed off by the CCG• Quality monitoring visits undertaken by CCG• Maternity Deep Dive in relation to PAH• HCT and HPFT CQC reports• Quality Assurance visits now being carried out at BCF
04/09/2015 - Remedial action plan in place for ENHT regarding stroke performance. Follow-up IPC visits carried out.Mock CQC inspection at PAH completed.
1) Review progress of IPC arrangements against action plan2) Participate in mortality review day re. ENHT with TDA
On-going
30-Sept-15
3x3 = 9• Levers for ENHCCG in relation to associate contracts regarding quality
4x3 = 12 4x3 = 12

Page 2 of 6
Linked with: Previous Risk RatingJune 2015
Current Risk RatingSept 2015
Key Controls Assurance Gaps in Controls/Assurances Actions required Date Target Risk Rating
Progress Update
SO2 - To commission effective services that enhance the well-being of our residents within the available resources
SO3 - To engender a culture of engagement in the decision making processes amongst partners and stakeholders to ensure ownership of service priorities
Ref 1.22 - Score 12 (3/4)Ref 1.32 - Score 12 (4/3)Ref 1.51 - Score 12 (3/4)Ref 2.14 - Score 12 (3/4)Ref 3.2 - Score 4 (2/2)Ref 3.5 - Score 12 (3/4)Ref 3.11 - Score 12 (3/4)
Strategic Risk 2:Failure to establish an adequate and appropriate commissioning plan that is informed by member practicesLead Director - Denise Boardman, Interim Director of Commissioning
3x1 = 33x3 = 9 30-Sept-15• Regular monitoring of the commissioning framework for practices to incentivise engagement in place• Governing Body approved strategic plan that incorporates future financial outlook• Significant clinical involvement in Programme Management via OPD• Established locality structure with additional senior management resources including finance and information input - locality meetings allow the opportunity for feedback to the localities on the outcome of the Commissioning Intentions process and the formulation of contracts for 2015/16• Clear Exec lead for strategic plan, with Programme Management Office and Exec Team meetings• Regular reviews of all incentive payments• Ensure active member engagement on the design of the commissioning framework• Commissioning intentions meetings held with all localities and locality patient groups• Quarterly Reporting regarding the monitoring of the commissioning framework• Council of Members• Commissioning Framework 2015/16 agreed
• Member practices inform plans via the Locality Groups• GP GB leads• Regular check and challenge review of strategy and framework by GB• On-going engagement with practices regarding development of Primary Care Strategy • Regular updates provided to NHSE, including the Joint Co-Commissioning Committee and Health and Well Being Board• Positive assurance from Area Team on the CCG 5-year strategic plan which has been developed in partnership with localities
1) Develop locality commissioning plans2) Primary Care Strategy to be finalised and signed-off
01/09/2015 - Member practices consulted on the Primary Care Strategy. Each Director has been assigned a locality.Draft Locality Plans are being discussed in localities.
3x3 = 9 • Localised plans

Page 3 of 6
Linked with: Previous Risk RatingJune 2015
Current Risk RatingSept 2015
Key Controls Assurance Gaps in Controls/Assurances Actions required Date Target Risk Rating
Progress Update
SO3 - To engender a culture of engagement in the decision making processes amongst partners and stakeholders to ensure ownership of service priorities
RCAD Risks:Ref 2.11 - Score 12 (3/4)Ref 3.2 - Score 4 (2/2)Ref 3.13 - Score 9 (3/3)
3x1 = 33x2 = 6 31-Oct-15• Area Team checkpoint reviews• 360 degree stakeholder survey results• Joint communications strategy agreed with key partners to ensure cooperation and delivery• SCG stakeholder engagement groups (check and challenge)• Service and procurement redesign with amended spec• No actions to be implemented from the 360 degree stakeholder survey• Scrutiny Committee attendance and engagement - positive contribution• Representation and focus on services delivered by HCC and ENHCCG• Membership in stakeholder engagement groups• Engagement with PPG's.
1) Steering Group and Stakeholder Forum to be re-established2) Engage in phase 2 of West Essex configuration work3) Timetable for Operational Plan to be refreshed and shared with partners4) CCG to coordinate development of Health and Wellbeing Strategy
Strategic Risk 3:Inability to achieve engagement/buy-in from our external stakeholders to ensure appropriate collaboration in developing plans that manage, meet and maintain their expectations.Lead Director - Chris Badger, Interim Director of Strategic Partnerships
3x2 = 6 Review of engagement activity, past and future
03/09/2015 - Clear objectives in place for the locality groups. Crisis Care Concordat agreed and signed off, now in 3-year implementation phase, CCG chairing county-wide group.Reviewed Joint Commissioning Patient Engagement Groups with Local Authority.Engagement in the "Your Care Your Future" Programmes
• Operation strategy outlines the two year communications strategy• Patient representative sits on the Governing Board • Director of Strategic Partnerships to develop external stakeholder relationships• New drive in engagement and enabling strategic partnerships • Attendance at strategic programmes which includes the facilitation of meetings• Engagement with Local Authority and Health Scrutiny which includes participation with council education programmes and direct engagement with the local community• Enabling Effective Partnership Programme with Barnet and Chase Farm• The Governance arrangements in relation to the Better Care Fund have been agreed• Members meetings• Annual General Meetings• 6 month impact review of Effective Enabling Programme – Barnet and Chase Farm• Governing Body builds on engagement with GPs through the provision of clearer objectives for the locality groups

Page 4 of 6
Linked with: Previous Risk RatingJune 2015
Current Risk RatingSept 2015
Key Controls Assurance Gaps in Controls/Assurances Actions required Date Target Risk Rating
Progress Update
SO2 - To commission effective services that enhance the well-being of our residents within the available resources
RCAD Risks:
Ref 1.6 - Score 9 (3/3)Ref 1.10 - Score 9 (3/3)Ref 1.17 - Score 8 (4/2)Ref 1.22 - Score 12 (3/4)Ref 1.27 - Score 12 (3/4)Ref 1.32 - Score 12 (4/3)Ref 1.33 - Score 12 (4/3)Ref 1.34 - Score 12 (3/4)Ref 1.49 - Score 9 (3/3)Ref 1.51 - Score 12 (3/4)Ref 1.53 - Score 9 (3/3)Ref 2.14 - Score 12 (3/4)Ref 3.4 - Score 12 (4/3)Ref 3.5 - Score 12 (3/4)Ref 3.11 - Score 12 (3/4)Ref 4.1 - Score 9 (3/3)
3x3 = 9
Lead Director – Alan Pond – Chief Finance Officer
Strategic Risk 4: Failure of the CCG to manage the financial budget and meet its financial target
• Regular finance reports to Executive Team, Governance and Audit, Governing Body and NHS England• Detailed Financial Policies • Budgetary framework in place which is rated as adequate by internal audit• Agreed budget for 2015/16 which included new investment funding, contingency reserves and funds for transformation• Efficiency savings are low (in comparison to other CCG’s) with plans in place to ensure delivery • Approved Scheme of Delegation which details responsibilities of budget holders• Financial processes in place to easily identify overspends• Early Warning Signals, forecasts for early year• Contract monitoring and validation processes• Trends in activity monitored and contracts set out responsibility levels within overall financial plan• Enforcing contract terms, including sanctions• Monthly review of expenditure and forecasts - to review whether any action is necessary
• Implementation of all internal audit recommendations.• Regular reports to Governing Body• Regular audit coverage by internal and external audit• Regular report on Finance Risks to Governance and Audit Committee• Internal Audit report on Budgetary Control
1) Improve reporting for non-PbR reporting2) To improve integrated care across providers3) To create more aligned incentives across providers
08-09-20153x3 = 9 31-Aug-15
30-Sept-15
31-Dec-15
3x1 = 3• Non-PbR reporting• Provision of real-time data and reporting to the CCG• Lack of aligned incentives between Community Providers and Acute Providers

Page 5 of 6
Linked with: Previous Risk RatingJune 2015
Current Risk RatingSept 2015
Key Controls Assurance Gaps in Controls/Assurances Actions required Date Target Risk Rating
Progress Update
SO1 - To commission safe and appropriate health care services
SO2 - To commission effective services that enhance the well-being of our residents within the available resources
SO4 - To build an organisation with the capacity and capability to deliver agreed service priorities
RCAD Risks:
Ref 1.9 - Score 12 (4/3)Ref 1.17 - Score 8 (4/2)Ref 1.22 - Score 12 (3/4)Ref 1.24 - Score 8 (4/2)Ref 1.25 - Score 12 (4/3)Ref 1.26 - Score 9 (3/3)Ref 1.32 - Score 12 (4/3)Ref 1.40 - Score 12 (3/4)Ref 1.41 - Score 12 (4/3)Ref 1.46 - Score 12 (3/4)Ref 1.50 - Score 16 (4/4)Ref 1.53 - Score 9 (3/3)Ref 2.6 - Score 9 (3/3)Ref 2.8 - Score 9 (3/3)Ref 3.4 - Score 12 (4/3)Ref 3.5 - Score 12 (3/4)Ref 4.11 - Score 8 (4/2)Ref 4.14 - Score 12 (4/3)Ref 4.15 - Score 12 (4/3)Ref 4.16 - Score 12 (4/3)Ref 4.17 - Score 12 (4/3)Ref 4.19 - Score 12 (4/3)
• Talent mapping and succession plan• No dedicated OD lead
31-Jul-15
30-Sept-15
3x1 = 3
Strategic Risk 5: Failure to implement key work streams to ensure delivery of the CCG’s strategic planLead Director – Chris Badger - Interim Director of Strategic Partnerships
• Established Programme management with documented systems and processes• Objective setting for all staff including Governing Body members• Executive receive regular update on workforce performance indicators• Agreed programme of mandatory training and monitoring of compliance• Board development programme• New Clinical Development Group meetings:- clinical forum/meeting with main provider to test clinical aspects of quality and delivery• Monthly Organisational Performance Delivery days to:- progress actions and processes for escalation to the Governing Body,- identify areas of poor performance,- highlight schemes to Governing Body for pilots and funding.
• Regular reports to Board and Executive Team• CCG directly responsible for undertaking contracting, information, performance and human resources management• Staff leadership development programmes underway e.g. Mary Seacole leadership programme• Systems Resilience Group, delivery across a number of areas - reporting and scrutiny• Clinical Development Group• Regular Board to Board with main providers (to ensure work streams are progressing)
1) Talent mapping and succession planning to be developed2) Ensure that clinical sub-groups (MH leads and LTC) engage with localities in consultation with service changes3) Development of locality commissioning plans4) AD development programme agreed and big event due to commence
03/09/2015 - Stock-take to be reported to the Board every 6 months.Clinical job descriptions drafted for GP Leads to outline responsibilities clearly for the specific areas - to ensure professional clinical input.AD Development programme running on 16/17 September 2015.Agreement to push for MH leads for each locality
3x3 = 9 3x3 = 9

Page 6 of 6
Linked with: Previous Risk RatingJune 2015
Current Risk RatingSept 2015
Key Controls Assurance Gaps in Controls/Assurances Actions required Date Target Risk Rating
Progress Update
SO1 - To commission safe and appropriate health care services
SO2 - To commission effective services that enhance the well-being of our residents within the available resources
N/A - new risk
4x4 = 16 • Oversight of operational delivery and quality of services by CCG directorate teams provides an early warning of any deterioration in performance or quality or of proposed changes in service provision that could lead to deterioration.• Formal meetings with Trust, NHS TDA, NHS England and CCG ensures CCG Chief Executive and CFO are party to formal discussions with ENHT and able to ensure a balanced and risk assessed approach is taken.
• Reporting of performance and quality metrics by Trust.
• There is no agreed solution to the incresing deficit being run by ENHT and acute trusts generally across the country. Part of the problem is the increasing demand for staffing arising from safer staffing guidance against a backdrop of reduced supply leading to premium costs being paid for staff.
1) NHS financial settlement to be published following this a system wide service and financial recovery plan to be agreed and implemented.
TBC 3x3 = 9 15/09/2015 - New risk added following discussion at Executive Meeting on 15/09/2015
Strategic Risk 6: Financial Sustainability of Providers in the Health Economy - Depatment of Health's departmental expenditure limit could be breached unless acute trust deficits (nationally and locally) are reduced. Deficit reduction might be attempted by driving down costs and staffing, which could impact on performance and/or the quality of services; or by increasing national prices and/or topclicing CCG funds, leading to cost pressures for CCGs nationally and ENHCCG too. In response ENHCCG would have to restrict investment and/or reduce services to achieve its financial plan.
Lead Director – Alan Pond – Chief Finance Officer
Strategic Objectives:
SO1: To commission safe and appropriate healthcare services.
SO2: To commission effective services that enhances the well-being of our residents within the available resources.
SO3: To engender a culture of engagement in the decision making processes amongst partners and stakeholders to ensure ownership of service priorities.
SO4: To build an organisation with the capacity and capability to deliver agreed service priorities.

Item 6j - 2015-09-15 RCAD risk 1.50 v4.1 DRAFT.xlsx
1 of 1
Appendix J PROGRESS KEY:
RCAD Ref. Risk Responsible Manager -
Area of ResponsibilityAccountable
DirectorLink to SR
and SOInherent Risk
Profile I/L Control (descriptors) Gaps in Controls and Assurances
Assurance in place (descriptors)
Current Risk Profile I/L Action Plans (descriptor) Action Owner
and TimescaleTarget Risk Profile I/L
Risk profile Acceptable? Progress Update
1.50 Princess Alexandra Hospital: Potentially failing trust across a number of areas - does not appear to have robust systems to assure itself and commissioners regarding the quality and delivery of the services it provides or provide data in a consistent manner.
Cath Slater- Provider Performance
Sheilagh Reavey
SR1SR5
SO1SO2
4/4 Quality contracting and performance at monthly SPQRG meetings - scrutiny of forthcoming data.Separate quality forum has been set-up, with PAH and WE CCG.Quality and performance AD's now attend PAH Cancer Board.CCG attendance at joining quality visits at PAH.CC attends stroke meetings.
Lack of robust data due to EPR project delays.Clinical engagement lacking in some areas.
Link with WE CCG as lead commissioner, to raise concerns and ensure issues are addressed on SPQRG agenda (+ve).
4/4 1) Link with WE CCG to gain assurance for EPR project progress via SPQRG.2) Review of patients waiting over RTT targets3) Assurance requested re. harm review process
1) C SlaterSept 20152) C AllbrightonSept 20153)
4/2 Yes 04/09/2015 4/3 to 4/4
- CQC inspection completed, formal performance notices issued by West Essex
Risk rating reduced from last report
Risk rating remains the same as last reportedRisk rating increased from last report
Strategic Objectives:SO1: To commission safe and appropriate healthcare services.SO2: To commission effective services that enhances the well-being of our residents within the available resources.SO3: To engender a culture of engagement in the decision making processes amongst partners and stakeholders to ensure ownership of service priorities.SO4: To build an organisation with the capacity and capability to deliver agreed service priorities.
Strategic Risks:SR1: Failure of the CCG to ensure delivery of safe, high quality and effectives services from appropriately commissioned providers.SR2: Failure to establish an adequate and appropriate commissioning plan that is informed by member practices.SR3: Inability to achieve engagement/buy-in from our external stakeholders to ensure appropriate collaboration in developing plans that manage, meet and maintain their expectations.SR4: Failure of the CCG to manage the financial budget and meet its financial target.SR5: Failure to implement key work streams to ensure delivery of the CCG’s strategic plan.

Appendix KBand 8A and above KeyDeclaration of Interest Register Form completed Form completed
Form submitted but incomplete
Abc Unable to complete form
Comment Title Known As First Name Surname Position Read Policy
Nothing to Declare
Have interests to declare
To the best of my knowledge and belief…
Type of Interests Your Details / Company Details (Registered office address, Company number etc.)
Spouse, Family member,Close friend etc. Details
Nature of Conflict
Long term sickMs. Debra Brice Elisabeth Brice Designated Nurse -
Safeguarding Children
Mat leaveMiss Kamelia Singh Business Relationship
Manager
leftMs. Yinka Soetan Islamiyyat Soetan Senior Pharmaceutical
AdvisorOn secondment Mr. Martin Wallis Chief Enterprise Architectleft Ms. Lesley Watts Chief Executive
Mr. Gary Adams Service Desk Manager y y yMrs. Allison Baldwin Senior Pharmaceutical
Advisory y y Other specific interests GSK Husband is employee of GSK Potential conflict of interests
as this is a pharmaceutical company and my role is pharmaceutical adviser.
Miss Kate Barker Catherine Barker AD - Maternity, Children & Young Peoples
y y y
Mrs. Natalie Bhakhri Senior Pharmaceutical Advisor
y y y
Mr. Keith Bringloe Informatics Programme Manager
y y y
Mrs. Jean Britten Financial Accountant y y yMrs. Jacqui Bunce Jacqueline Bunce Associate Director of
Strategyy y y Other specific interests Built Environment Expert -
Design Council/Commission for Architecture and the Built Environment
None Identified
Miss Jo Burlingham Joanne Burlingham Associate Director of Commissioning
y y y
Mr. Simon Carey AD Business Relationships and Assurance
y y y
Mrs. Gillian Catchpole Commissioning Development Manager
y y y
Mr. Gary Cobden Database Management Team Lead
y y y
Mrs. Noreen Coles Assistant Director of Finance y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Husband is a self employed management consultant working within the NHS.
Position of influence
Mrs. Rosie Connolly
Rosemarie Connolly Quality Manager y y y
Mr. Guy Crosby Head of Customer Services y y y
Mrs. Maxine Davis Lead Pharmaceutical Advisor - Care Prescribing
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
GSK Husband employed by GSK. Position of Authority
Mrs. Maxine Davis Lead Pharmaceutical Advisor - Care Prescribing
y y y Other specific interests I provide training for Herts Care Providers Association to their members.
None identified.
Mrs. Jas Dosanjh Jasjit Dosanjh Head of Risk Management y y y

Mrs. Alison Dossetter Senior Pharmaceutical Advisor
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Spouse - Lee Dosseter - Systems Manager GOSH (Great Ormond Street Hospital).
None identified.
Mr. Nick Downer Nicholas Downer Business Change Manager (Technical)
y y y
Miss Holly Edwards Head of Contract Management
y y y
Mrs. Anne Ephgrave Head of HR y y yMr. Keith Fairbrother Head of Infrastructure y y yMrs. Sarah Feal Company Secretary y y yMiss Joanne Field Head of Performance y y yMs. Rose Francis Rosemarie Francis Business Relationship
Managery y y
Mr. James Gleed Associate Director of Primary Care & Strategy
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
James Gleed Married to another CCG Employee - Helen O'Keefe, Locality Manager
Conflict of Loyalties
Mrs. Stacey Golding Lead Pharmaceutical Advisor - Governance
y y y
Ms. Joanne Goulden HO Clinical Safety& Business Change
y y y
Mr. Marco Guttadauro Networks & Telecoms Manager
y y y
Mrs. Susan Haigh Communication Service Manager
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Welwyn Hatfield Borough Council
Spouse is Head of Planning at Welwyn Hatfield Borough Countil
Potential for conflict with regards to applications for NHS Premises
Mr. David Hodson Head of Information - Planning & Strategy
y y y
Mr. Edward James AD Financial Services y y yDr Rachel Joyce Clinical Advisor y y y Any other role or relationship
which the public could perceive would impair or otherwise influence the individual's judegement or actions in their role within the CCG.
East and North Herts NHS Trust and Private Hospitals.
Husband is a consultant Ear Nose and Throat Surgeon working at East and North Herts NHS Trust and Private Hospitals.
None perceived.
Mr. Usman Khan Head of Financial Services, HBL ICT NHS
y y y Directorships Director of Spouse's company. Medops Ltd, 18 Leasowes Road, London, E10 7BE 07907320
Dr Mehreen Mizra None identifiedNone perceived
Mr. Thomas Kwok Financial Accountant y y yMrs. Jessica Linskill Lead Nurse - Quality y y yMr. Phil Lumbard Philip Lumbard Assistant Director Urgent
Carey y y
Miss Teresa Maczugowska Senior Finance Officer y yMr. Stephen Matthews Release & Deployment
Managery y y
Mrs. Nuala Milbourn Assistant Director of Communications
y y y
Mrs. Cath Slater Catherine Moir-Slater AD Quality & Patient Safety y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Partner works for ENHCCG Could be seen to influence judgements and/or decisions.

Mrs. Gerry Moir Geraldine Moir-Slater Assistant Director Performance
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Gerry Moir, AD Performance, ENHCCG
Partner works for CCG Could be seen to influence judgements and/or decision making
Miss Laura Moore Senior Contract Manager y y yMiss Beverly Mukandi Deputy Designated Nurse
Safeguarding Childreny y y Directorships Director
Twelve5 LtdCo number 8918637Address: 33 Forrester's Drive, Panshanger, Welwyn Garden City, AL7 2JA
No perceived conflict
Mr. Grant Neofitou Head of Programme Office y y yMr. Peter Newton AD Service Development y y y Any connection with a
voluntary or other organisation contracting for NHS Services:
Marie Stopes International Friends in IT Department.Friend in HR and IT
No conflict
Miss Sarah Newton HBLICT - ICT Business Change Manager and Interim RA Manager
y y y
Ms. Fiona Oliver Commissioning Development Manager
y y y
Mr. Philip O'Meara Senior Finance Manager y y y Any connection with a voluntary or other organisation contracting for NHS Services
HPFT. Provider of Services to ENHCCG
Wife Employee only. I am involved in Commissioning from HPFT.
Mr. Mark Peedle Head of Operational IT (GP & Corp)
y y y
Ms. Pauline Power Senior Finance Manager y y yMrs. Sue Russell Susan Russell Lead Pharmacist y y y Roles and Responsibilities
held within member practiceOrford Lodge Surgery, 100 Bancroft, Hitchin, Herts
Self Member of Orford Lodge Patient Participation Group
Mrs. Sue Russell Susan Russell Lead Pharmacist y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Daughter - Helena Russell Daughter employed as Contracts Support Officer in ENHCCG
Mr. Colin Sach Lead Pharmaceutical Advisor - Acute Commissioning
y y y Other specific interests Rickmansworth School Wife is a teacher at Rickmansworth School
None Perceived
Mrs. Alison Sansom Clinical Services Manager y y yMs. Alison Saward Senior Finance Manager y y yMr. Shane Scott Head of Primary Care ICT y y yMrs. Bhavini Shah Senior Pharmaceutical
Advisory y y Any connection with a
voluntary or other organisation contracting for NHS Services
Ware Dental Care, 3 West Street, Ware, Herts
Husband is a dentist. Contract for NHS Services managed by Area Team/NHS England
Mr. Sanjeev Sharma Senior Pharmaceutical Advisor
y y y Other Specific Interests Do occasional Locum Pharmacist Work (not with East and North Herts CCG).
Miss Paula Simms Senior Contract Manager y y yMrs. Trudi Southam Interim AD - Operations y y y
Mr. Tawanda Tagwireyi ICT Systems Manager y y yMr. Philip Turnock ICT Shared Service Director y y y
Mr. Mihir Varia Senior Pharmaceutical Advisor
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Community Pharmacist Locums – No locums done in East and North Herts CCG.
Wife – Sonal Dhanani. Wife works as a Community Pharmacist for Lloyds Pharmacy (National Chain) in another CCG.
None Perceived
None Percieved.

Mrs. Pauline Walton Associate Director of Pharmacy & Medicines Optimisation
y y y
Mrs. Claire Warren Senior ICT Project Manager y y y
Ms. Linda Whiteley Clinical Safety & Business Change Lead
y y y
Back on 4th SepMrs. Rohini Widyaratna Intermediate Care Clinical
Commissioning Managery y y
Ms. Julie Williams Senior Finance Manager y y y Any connection with a voluntary of other organisation contracting for NHS Services
Luton and Dunstable NHS Trust
Partner is Managing Director of Trust
Mrs. Amber Willson Senior Finance Officer y y yMrs. Geraldine Woods Clinical Decisions Lead y y y
Did not tick box to say has read policy
Ms. Helen Edmondson Associate Director Commissioning - Localities
y y
Did not tick bottom box
Mrs. Samantha Potts Head of Programme Management
y y

Governing Body Members KeyDeclaration of Interest Register Form completed
Form submitted but incomplete
Abc Unable to complete form
Comment
Known As First Name Surname Position Read Policy
Nothing to Declare
Have interests to declare
To the best of my knowledge and belief
Type of Interests Your Details / Company Details (Registered office address, Company number etc.)
Spouse, Family member,Close friend etc. Details
Nature of Conflict
Ed Edward Bosonnet Interim Director of Clinical Integration
GP Board Member
y y y Roles and Responsibilities Held within member practice
Partner, Warden Lodge Medical Practice.
Ed Edward Bosonnet Interim Director of Clinical Integration
GP Board Member
y y y Shareholdings Warden Lodge Shareholder Lea Valley Health Limited (Federation)
Ed Edward Bosonnet Interim Director of Clinical Integration
GP Board Member
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Wife is employee of NHS Professionals. Works for PAH (Princess Alexandra Hospital) / East and North Herts NHS Trust / Herts Community NHS Trust. (Nurse.)
Mark Andrews Governing Body Board Member
y y y Roles and Responsibilities Held with Member Practices:
Partner (Principal)Dr Blankfield < Partners, Limes Surgery, 8-14 Limes Court, Conduit Lane. Hoddesdon, Herts EN11 8EP
Member of Generating Health as Partner of Practice
Myself Provider Practice within ENHCCG (locality) boundary
Provider of NHS Services to Upper Lea Valley
Mark Andrews Governing Body Board Member
y y y Any Connection with Voluntary or other Organisatoin contracting for NHS services:
Health Visitor: Hertfordshire Community Trust
Spouse Employee of said provider

Chris Badger Assistant Director of Health and Social Care Integration. From 01-09-15: Interim Director of Strategic Partnerships
y y y Position of Authority in an organisation.
Employed by Hertfordshire County Council
Conflict regarding pooled budgets, etc
Denise Boardman Interim Director of Commissioning
y y y Other specific interests I am an external assessor for the college of Occupational Therapy COT Annual Awards for Education, Research, and Continuing Professional Development. This is a three year term of office which runs from 2013-16.
Sharn Elton Director of Operations
y y y
Linda Farrant Lay Member: Governance and Audit
y y y • Board Member of OFSTED-----------------• Independent Member of Audit and Governance Committee of Care Quality Commission wef 27/07/15
• No direct conflict. OFSTED inspects children’s care services provided by local authorities.------------------• No direct conflict. CQC regulates and inspects NHS providers and adult social care with whom CCG commissions services.
Beverley Flowers Interim Chief Executive
y y y
Robert Graham GP Lead, NH y y y Roles and Responsibilities Held within member practices
Birchwood Surgery, 232-240 Nevells Road, LetchworthHertfordshireSG6 4UBI am a GP Partner at Birchwood Surgery. Practice is a member of 12 Point Care Federation of Practices in North Herts. I have no role with the federation.
Wife Sue Graham. Wife Sue Graham: • works as a salaried GP at Birchwood Surgery. • She works at Pinehill Hospital offering “Well Woman Clinic” once a week.• She works for Herts Urgent Care Out of Hours approx. once per week.
Russell Hall GP Lead, Stevenage y y y Roles and Responsibilities Held within member practices
Partner Chells Way Surgery
Position of influence

Hari Pathmanathan y y y Directorships, including non-executive Directorships, held in Private Companies or PLCs:
Director: Bridge Cottage Pharmacy Ltd
Commissioned by NHS England
Hari Pathmanathan y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG.
Fairbrook Medical Centre, a Practice in Herts valley CCG
Wife is a Partner in this practice.
Neighbouring CCG
Alison Jackson GP Board Member, Lower Lea Valley. Principle GP, The Maples.
y y y Roles and Responsibilities within member practice
Principle GP In a position of influence
Alison Jackson GP Board Member, Lower Lea Valley. Principle GP, The Maples.
y y y Directorships Member of Lea Valley Health Federation
In a position of influence
Deborah Kearns GP Lead, SV&V. Governing Body Member.
y y y Roles and Responsibilities Held within member practices
Partner at Central Surgery.Bell StreetSawbridgeworthHertsCM21 9AQMedical PracticeStaff and Business Management of the practice.
Member Practice.Property owner seeking to improve premises through Primary Care Infrastructure bid. The Practice has joined a federation, Stort Valley Health Care Limited.
Deborah Kearns GP Lead, SV&V. Governing Body Member.
y y y Any connection with a voluntary or other organisation contracting for NHS Services
Mantle(Saffron) Ltd Company Number 5752770.
Husband is director. Mantle(Saffron) maintains a freehold interest in Saffron Ground in Stevenage, which is a 4 story office building. 2 floors are let to the NHS.
Stephen Kite GP Lead, ULV. Governing Body Member.
y y y Roles and Responsibilities held within member practice
GP Practice is a member of Local GP Federation: Generating Health.
Stephen Kite GP Lead, ULV. Governing Body Member.
y y y Ownership or Part Ownership of private companies, businessess or consultancies likely or possibly seeking to do business with the CCG
Shareholder of Generating Health Ltd.
Provider Arm of ULV LCG (Upper Lea Valley Locality Commissioning Group).
Stephen Kite GP Lead, ULV y y y Any connection with a voluntary or other organisation contracting for NHS Services
Trustee of Libury Hall (Mental Health Facility for patients with long term Mental Health Conditions)
Many residents are under contracts with HPFT (Hertfordshire Partnership Foundation Trust).

Louise Monk Deputy Practice Rep, LLV
y y y Roles and Responsibilities Held within member practices
Warden Lodge Medical PracticeCheshuntHertsEN8 8NW
• GP Partner• Practice is shareholding member of Lea Valley Health GP Federation
Louise Monk Deputy Practice Rep, LLV
y y y Any connection with a voluntary or other organisation contracting for NHS Services
Adam Whereat (husband), Chartered Surveyor, Director Portfolio Valuations Savills PLC
Savills are involved in NHS and provider property valuations.
Prag Moodley GP Lead, Stevenage y y y Roles and Responsibilities Held within member practices
GP-Stanmore Medical Group - Senior Partner
Commissioner and Provider
Prag Moodley GP Lead, Stevenage y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG.
Wife is a consultant (CAMYS) working for Hertfordshire Partnerships Foundation Trust (HPFT)
Wife I am a Mental Health Lead for CCG, we contract HPFT.
Hari Pathmanathan Chair y y y Roles and Responsibilities Held within member practice
Partner in Bridge Cottage Surgery
Member Practice.
Alan Pond Chief Finance Officer
y y y Roles and Responsibilities Held within member practice
Partner is a GP Partner in HVCCG (Haverfield Surgery, Kings Langley) and Chair of Dacorum Locality
None
Alan Pond Chief Finance Officer
y y y Directorships Director of Assemble Community Partnership Ltd and associated companies (of 128 Buckingham Palace Road, London). ACP is the LIFT (Local Improvement Finance Trust) company for South East Midlands and the directorship is unpaid, nominated by Community Health Partnerships to act on behalf of ENHCCG and other commissioners in the LIFT area.
None
Sheilagh Reavey Director of Nursing and Quality
y y y

Nabeil Shukur GP Lead, SV&V y y y Roles and Responsibilities Held within member practice
GP Provider in South Street Surgery83 South StreetBishops StortfordHertsCM23 3AP
GPSI (GP with Special Interest) Orthopaedics for West Essex CCG
GP Provider
Orthopaedics Provider
Nabeil Shukur GP Lead, SV&V y y y Directorships Director of NHA Medical Ltd4 Beech DriveSawbridgeworthCM21 0AA
Wife and Son are Directors
Provides Dermatology and Orphopaedic Services
Nabeil Shukur GP Lead, SV&V y y y Ownership or Part Ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG:
Shareholder in NHA Medical Ltd
Nabeil Shukur GP Lead, SV&V y y y Any other role or relationship… I have a position of Mentor to Nurse Specialists in Minor Injury Unit of Herts and Essex Hospital
Through HCT (Hertfordshire Community NHS Trust)
Nabeil Shukur GP Lead, SV&V y y yFiona Sinclair GP Lead, NH y y y Roles and Responsibilities
Held within member practiceRegal Chambers Surgery, 50 Bancroft, Hitchin, SG5 1LL
Fiona Sinclair - Partner and Associate Trainer
Regal Chambers: my practice provides services commissioned by the CCG. My Practice teaches GP registrars.
Fiona Sinclair GP Lead, NH y y y Ownership or Part Ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG:
Twelve Point CareC/O Regal Chambers Surgery, 50 Bancroft, Hitchin, SG5 1LL
Fiona Sinclair: My price is a shareholder in the local federation.
Federation likely to bid to provide CCG Commissioned Services.
Nicolette Williams Deputy Clinical Chair/ GP Lead Upper Lea Valley Locality
y y y Roles and Responsibilities Held within member practice
GP Partner: Church Street Surgery, Ware.
GP Practice is member of Local GP Federation, Generating Health.
Senior Partner
Dianne Desmulie Lay Member: Public and Patient Engagement
y y y Roles and Responsibilities within member practice
Member of Hanscombe House Patient Participation Group
None currently. Potential conflict re. funding allocations or issues concerning performance.

Dianne Desmulie Lay Member: Public and Patient Engagement
y y y Ownership or part ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG.
Director of my own company:Pieve Solutions LtdCompany No, 5600186. Registered address:Orchard House, Park Lane, REIGATE, Surrey, RH2 8JX. I work through this company as a freelance Management Consultant.
My husband, Robert Pinkham, is also a director of Pieve Solutions Lrd and works as a freelance HR consultant.
None currently.
Harper Brown Director of Planning and Procurement
y y y Directorships Director Harper Brown Consulting Ltd
None
Harper Brown Director of Planning and Procurement
y y y Ownership or part ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG
Director Harper Brown Consulting Ltd
None
Needs manual signature and to tick boxes
Dermot O'Riordan Secondary Specialist Doctor: Chief Clinical Information Officer & Consultant Surgeon, West Suffolk NHS Foundation Trust
Any connection with a voluntary or other organisation contracting for NHS Services
Consultant Surgeon West Suffolk NHS FT
Wife is Consultant Surgeon Ipswich Hospital Trust
Did not tick box at bottom
Ashish Shah GP Lead, WelHat y y Roles and Responsibilities Held within member practice
Principal GPWrafton House Surgery9-11 Wellfield RoadHatfieldAL1 OBS
Ashish Shah GP Lead, WelHat y y Directorships Director (Joined) or Abhirush Limited.Company registered address5 ChedburghWelwyn Garden CityAL7 2PU
Work involves GP Locum and OOH work through Limited Company
Ashish Shah GP Lead, WelHat y y Shareholdings Partner in Wrafton House Surgery, which is a shareholder of Ephedera Healthcare Limited

Ashish Shah GP Lead, WelHat y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
GP Trainer at Wrafton House Surgery. Do OOH (Out of Hours) work for HUC OOH (Herts Urgent Care Out of Hours).Practice has a pharmacy hub from Quantum Pharmacy for which it receives a service charge.
Ashish Shah GP Lead, WelHat y y Other specific interests Wife works as Lucum GP in Hertfordshire and does out of hours work with Herts Urgent Care (HUC).
Left Peter Shilliday GP Lead, WelHatLeft Lesley Watts Chief Executive /
Accountable Officer

Lead GPs KeyDeclaration of Interest Register Form completed
Form submitted but incompleteAbc Unable to complete formAbc Have completed form - entry registered elsewhereAbc Form submitted but incomplete. Entry registered under Governing Body Members
Comments Surgery Locality First Name Surname Email Read Policy
Nothing to Declare
Have interests to declare
To the best of my knowledge and belief…
Type of Interests Your Details / Company Details (Registered office address, Company number etc.)
Spouse, Family member,Close friend etc. Details
Nature of Conflict
No longer in post
St Nicholas Health Centre
Stevenage Dr Rafid Aziz [email protected]
Ashwell North Herts Dr Matt Jarvis [email protected]
Cromwell & Wormley Medical Centre
Lower Lea Valley
Dr Nikunj Malde [email protected]
Church Street Partnership SV&V
Stort Valley & Villages
Dr Mark Penwill [email protected]
Canterbury Way Stevenage Dr Naomi Selvadurai [email protected] Stockwell Lodge Lower Lea
ValleyDr Navina Sullivan [email protected]
Bridge Cottage Welwyn Hatfield
Dr Segun Adeuja [email protected] y y y Roles and Responsibilities held within member
Bridge Cottage Surgery, 41 High Street, Welwyn, AL6
None
Bridge Cottage Welwyn Hatfield
Dr Segun Adeuja [email protected] y y y Directorships Director of Ephedera (WelHat Federation)
Director of Bridge Cottage Pharmacy
Director of JILOA Innovations Limited. Reg No - 6937850. Address5 Aspen Way, Welwyn Garden City, AL7 1HR
My wife is 50% share holder
Provider services for East and North Herts CCG and NHS Trust.
Retail Pharmacy
GP Locum Work
Portmill North Herts Dr Suhail Alam [email protected] y y yThe Limes Upper Lea
ValleyDr Mark Andrews Mark.Andrews@enherts
ccg.nhs.ukPortmill North Herts Dr Tara Belcher
y y y Directorships
Director, 12 Pointcare Ltd. 09214266
Provider of Healthcare Services
Shephall Way Stevenage Dr Andrew Cormack [email protected]
y y y

Amwell Street Upper Lea Valley
Dr Andrew Davies [email protected]
y y y Roles and Responsibilities held within member practices.
GP and Principal Partner, Amwell Street Surgery.
The Amwell Street Surgery is a Shareholder of the health provider "Generating Health" Ltd, the provider arm of Upper Lea Valley Locality Commissing Group.
Manor House Stevenage Dr Michael Duggan [email protected]
y y y Directorships Chair of Stevenage Health Limited.
Am a provider and might be a Commissioner.
Burvill House Welwyn Hatfield
Dr Neil Dytham [email protected]
y y y Roles and responsibilit GP Partner at Burvill House Surgery
Burvill House Welwyn Hatfield
Dr Neil Dytham [email protected]
y y y Directorships Clinical Director of Ephedra Healthcare. Provider of Service: for:• Spring House Medical Centre• UCC Welwyn Garden CityEphedra has Care Taker Role for one year for:• Ware Road, Hertford• Orchard Surgery – BuntingfordClinical Director of Capra HealthcareSuite 3, Middlesex HouseRutherford CloseStevenage, Herts, SG1 2EF – No Contracts
Warden Lodge Lower Lea Valley
Dr Angela Goodwin [email protected] y y y Shareholdings Lea Valley Health LtdStanhope SurgeryStanhope RoadWaltham CrossHertsEN8 7DJCompnay number: 09114753
Member of Lower Lea Valley CCG and shareholder of Lea Valley Health which is a GP Federation encomapssing the eight practices in Lower Lea Valley.
Birchwood North Herts Dr Rob Graham [email protected]
Courtenay House North Herts Dr Keith Greenish [email protected] y y y Roles and Responsibilities held within member practices.
Courtenay House Surgery
Senior PartnerFinance Partner
Courtenay House North Herts Dr Keith Greenish [email protected] y y y Shareholdings. 12 Point Care Shareholder for Courtenay House

Courtenay House North Herts Dr Keith Greenish [email protected] y y y CCG/NHS England Personal Friend Member of GP Premises Team NHSE - who has requested not to be engaged in any work pertaining to Courtenay House.
Need more info Garden City, Wel Hat
Welwyn Hatfield
Dr Sachin Gupta y y y Directorships Medical Director, Herts Urgent Care
Garden City, Wel Hat
Welwyn Hatfield
Dr Sachin Gupta y y y Other specific interests
Director - SG Healthcare LimitedBracey's Accountants
Wife is co-Director
For appraiser and OOH (our of hour) work.
Potterells Welwyn Hatfield
Dr Sarah Hoole [email protected] y y y Roles and Responsibilities held within member practice
Potterells Medical Centre
Practice Lead on Local WelHat Board.Practice Partner.
Potterells Welwyn Hatfield
Dr Sarah Hoole [email protected] y y y Directorships Director, Ephedera Healthcare Limited
Potterells Welwyn Hatfield
Dr Sarah Hoole [email protected] y y y Shareholdings Shareholder, Ephedera Healthcare Limited.
Stanhope Lower Lea Valley
Dr Mo Hossain [email protected]
y y y Ownership or part ownership of private companies, businesses or
Medical DirectorLower Lea Valley Health LtdHigh Street Surgery
Spring House Medical Centre
Welwyn Hatfield
Dr Eva Kreye [email protected] y y y
Wallace House Upper Lea Valley
Dr Jay Kuruvatti [email protected] y y y Roles and Responsibilities Held within Member Practices:
Upper Lea Valley Locality Mental Health Lead and GP Lead for Practice (Wallace House Surgery)
Wallace House Upper Lea Valley
Dr Jay Kuruvatti [email protected] y y y Shareholdings Partner in a practice which is a shareholder in GP Federation, "Generating Health".
Lister House Welwyn Hatfield
Dr Richard Lavelle [email protected] y y y
Dolphin House Upper Lea Valley
Dr David Maddams [email protected]
y y y
Symonds Green Stevenage Dr Rashid Masood [email protected] y y y Other Specific Interest
Working in Out of Hours for Herts Urgent Care
Has stepped down
Whitwell North Herts Dr Rajpreet Millan [email protected] y y y Shareholdings Shareholder of 12 Point Care

High Street Lower Lea Valley
Dr Kalpana Misra [email protected] y y y Roles and Responsibilities held within member
Senior Partner, High Street Surgery
Stanmore Road HC
Stevenage Dr Prag Moodley [email protected]
Sollershott North Herts Dr Richard Nevard [email protected] y y y Roles and Responsibilities held within member practice
Senior Partner, The Sollershot Surgery, 44 Sollershot East, Letchworth Garden City, Herts, SG6 3HJ
N/A
Sollershott North Herts Dr Richard Nevard [email protected] y y y Shareholdings I am the practice stakeholder in 12PointCare Ltd, (GP Federation),Orbital House, 20 Easter Road
Stakeholder with voting rights in locality GP Federation
Sollershott North Herts Dr Richard Nevard [email protected] y y y Positions of Authority Trustee ofChoice Pregnancy Counselling CentreMrs Howard Memorial HallNorton Way SouthLetchworth Garden CityHertsSG6 1NXRegistered Charity 1088101
Choice provides free pregnancy counselling services within this locality and Stevenage. We are not currently NHS funded although work alongside NHS sexual health services locally.
Abbey Road Lower Lea Valley
Dr Bill Neville [email protected] y y y
Knebworth North Herts Dr Rob Newby [email protected] y y y Roles and Responsibilities held within member practices
Practice Partner, Knebworth and Marymead
Knebworth North Herts Dr Rob Newby [email protected] y y y Ownership or part ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG.
12 Point Care Limited. Shareholder on behalf of practice.

Puckeridge Upper Lea Valley
Dr Will Nicolson [email protected] y y y
Much Hadham Stort Valley & Villages
Dr Nathalie Oates [email protected]
y y y Roles and Responsibilities held within member practices
Practice Partner
Much Hadham Stort Valley & Villages
Dr Nathalie Oates [email protected]
y y y Directorships Stort Valley Health Care: Director
Hanscombe House Upper Lea Valley
Dr Anita Oates [email protected] y y y Roles and Responsibilities Held within Member Practices:
• Hanscombe House Surgery52A St Andrew StreetHertfordSG14 1JA• Generating Healthcare Ltd – Provider Arm of ULV LG
• Practice Partner
• Shareholder
Castlegate Upper Lea Valley
Dr Giles Pratt [email protected] y y y
Nevells Road North Herts Dr Tim Ramsbottom [email protected]
y y y Shareholdings Shareholder in 12 Point Care Ltd - the local federation.
Bedwell Medical Centre
Stevenage Dr Perumal Raveendran [email protected] y y y Roles and Responsibilities held within member practices
Full time clinician Commissioner - provider issues
Bedwell Medical Centre
Stevenage Dr Perumal Raveendran [email protected] y y y Directorships Practice Representative for Stevenage Health Ltd, federation of provider services.
Commissioner - provider issues

Bedwell Medical Centre
Stevenage Dr Perumal Raveendran [email protected] y y y Position of authority in an organisation…
1. GP Appraiser working for NHS England2. GP Trainer - Health Education East of England3. Undergraduate GP Tutor UCL - (University College London)
Bias in workforce planning
Bedwell Medical Centre
Stevenage Dr Perumal Raveendran [email protected] y y y Other specific interests
Previously worked with Macmillan Cancer Charity
None perceived
Amwell Street Upper Lea Valley
Dr Joanne Roberts y y y Roles and Responsibilities held within member practices.
GP Partner. No other interests.
Amwell Street Upper Lea Valley
Dr Joanne Roberts y y y Ownership or part ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG.
The Practice is a Shareholder of Generating Health Ltd
Watton Place Upper Lea Valley
Dr Dilesh Shah [email protected] y y y
Park Lane Upper Lea Valley
Dr Jacqueline Sheridan [email protected] y y y Roles and Responsibilities held within member practices:
Finance and personel lead
Like all partners in practice, balance between Locality / CCG / country wide impact on decisions.
Park Lane Upper Lea Valley
Dr Jacqueline Sheridan [email protected] y y y Shareholdings (more than 5%) of companies in the field of Health and Social Care
The Practice is a member of Generating Health, a Federation Group of all the Locality Practices. I'm not directly involved.
Astonia House North Herts Dr Richard Stanley [email protected]
y y y Roles and Responsibilities held within member practices
Astonia House, Baldock 25/02/2015 Dr Richard Stanley GP Partner, The Baldock Surgery
Wife is a GP Partner at same practice
None
Astonia House North Herts Dr Richard Stanley [email protected]
y y y Shareholdings Shareholder in '12 Point Care' (GP Federation Body) on behalf of practice.
None
Astonia House North Herts Dr Richard Stanley [email protected]
y y y Any connection with a voluntary or other organisation contracting for NHS Services.
GP Trainer (Health Education East of England) and GP Appraiser (Central Midlands Area Team, NHS England)
None

Parsonage Stort Valley & Villages
Dr Jag Takhar [email protected]
y y y Roles and Responsibilities held within member practices:
GP PrincipalParsonage Surgery, Herts and Essex Hospital, Cavell Drive, Bishops Stortford, Hertfordshire, CM23 5JH
Position of authority
Parsonage Stort Valley & Villages
Dr Jag Takhar [email protected]
y y y Directorships, Including Non-Executive Directorships, held in Private Companies or PLCs:
Director and Chair of Stort Valley Healthcare Limited
Position of Influence
Parsonage Stort Valley & Villages
Dr Jag Takhar [email protected]
y y y Ownership or Part Ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG:
Director and Chair of Stort Valley Healthcare Limited
Position of Influence
Parsonage Stort Valley & Villages
Dr Jag Takhar [email protected]
y y y Shareholdings (more than 5%) of companies in the field of Health and Social Care
Director and Chair of Stort Valley Healthcare Limited
Position of authority
Parsonage Stort Valley & Villages
Dr Jag Takhar [email protected]
y y y Research funding/grants that may be received by the individual or any organisation they have an interest or role in
Reseach via National Institute of Health Research (NIHR)
None identified
Parsonage Stort Valley & Villages
Dr Jag Takhar [email protected]
y y y Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG.
GPWSI (GP With Specific Interest) in Cardiology
None identified
Parsonage Stort Valley & Villages
Dr Jag Takhar [email protected]
y y y Other Specific Interest
Cardiology
Cuffley & Goffs Oak Medical Centre
Lower Lea Valley
Dr Pauline Taylor [email protected]
y y y Roles and Responsibilities held within member practices
Senior and Finance Partner

Garden City, Letchworth, North Herts
North Herts Dr Adrian Wood [email protected] y y y Roles and Responsibilities held within member practices
GP Partner and Lead GP for practice re CCG/LocalityGarden City SurgeryLetchworth Garden City
Garden City, Letchworth, North Herts
North Herts Dr Adrian Wood [email protected] y y y Directorships, including Non-Executive Directorships,held in private companies or PLCs:
Director12PointCare(GP Federation in North Herts)
Orchard Upper Lea Valley
Dr Ephedra Clinical Directors on rotation. GPs Neil Dytham, Michael Rule and Alister Parry. Ephedera have a caretaker role for one year for Orchard. Please see individual declarations from these 3 GPs.
Ware Road Upper Lea Valley
Dr Ephedra Clinical Directors on rotation. GPs Neil Dytham, Michael Rule and Alister Parry. Ephedera have a caretaker role for one year for Ware. Please see individual declarations from these 3 GPs.
Did not tick boxes or sign
Orford Lodge North Herts Dr Jeremy Cox [email protected] Directorships Director of Herts and Beds LMC

did not tick bottom box
Hailey View Upper Lea Valley
Dr Rob Mayson [email protected]
did not tick bottom box
Hall Grove Welwyn Hatfield
Dr Alister Parry [email protected] y y Roles and Responsibilities held within member practices.
Executive Partner Hall Grove Group Practice
No Conflict
did not tick bottom box
Hall Grove Welwyn Hatfield
Dr Alister Parry [email protected] y y Directorships Non Executive Director, Ephedera Health Care
No Conflict
Need more info Hall Grove Welwyn Hatfield
Dr Alister Parry [email protected] y y Any connection with a voluntary or other organisation contracting for NHS S i
GPWSI (GP With Specific Interest) dermatology. Employed by Skin H lth S i HCT Did not tick
bottom boxBuntingford MC Upper Lea
ValleyDr Megan Philimore-Brown megan.phillimore-
Need more info. King George Stevenage Dr Vishen Ramkisson [email protected] y y y Roles and Responsibilities held within member practices
GP Partner - King George Surgery
Wife - Dr H Ramkisson - GP Partner Brichwood Surgery
None declared
Need more info King George Stevenage Dr Vishen Ramkisson [email protected] y y y Directorships 1. Director - Protea Impilo Ltd2. Director - KGS Medical Services3. Director - Shakespeare Rd Management
Wife - Director Protea Impilo Ltd
None Declared
Need more info King George Stevenage Dr Vishen Ramkisson [email protected] y y y Position of authority in an organisation…
Stevenage LMC MemberMember of Hertfordshire LMC Executive Committee
Needs to provide more detail about Directorships
King George Stevenage Dr Vishen Ramkisson [email protected] y y y Any other roles or relatinships which th public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG
Regional GP Lead for University of Cambridge

Peartree Welwyn Hatfield
Dr Mick Rule [email protected]
y y y Directorships Maill Smith
Ephedera HealthcareKemp Town Medical
Pharmacy at Paritree Lane SurgeryWelHat FederationAudiology Provider
Has not ticked all boxes or put job title
Wrafton House Welwyn Hatfield
Dr Ashish Shah [email protected]
Will probably be new GP lead but not certain yet.
St Nicholas Health Centre
Stevenage Dr J Turner y

None compulsory Submissions KeyDeclaration of Interest Register Form completed
Form submitted but incomplete
Abc Unable to complete form
Comments Title Known As
First Name Surname Position Read Policy
Nothing to Declare
Have interests to declare
To the best of my knowledge and
Type of Interests Your Details / Company Details (Registered office address, Company number etc.)
Spouse, Family member,Close friend etc. Details
Nature of Conflict
Helen Moth
Practice Manager, Warden Lodge and member of Lower Lea Valley Commissioning Group
y y y
Directorships Commercial DirectorLea Valley Health LtdStanhope SurgeryStanhope RoadWaltham CrossHertsEN8 7DJCompany No: 09114753
Member of Lower Lea Valley CCG and Director of Lea Valley Health which is a GP Federation encompassing the eight practices in Lower Lea Valley.
Claire Arno
Practice Manager, High Street Surgery
y y y
Roles and Responsibilities held within member practices
Practice Manager, High Street Surgery.
Claire Arno
Practice Manager, High Street Surgery
y y y
Directorships Governance DirectorLea Valley Health LimitedStanhope Surgery, Stanhope RoadWaltham CrossHertsEN8 7DJCo No 09114753
Director of Lea Valley Health
Catherine Church
Practice Manager, The Maples Health Centre
y y y
Directorships CEO Lea Valley Health Limited.Company Reg no. 09114753Reg. Address: 13-15 High StCheshuntHerts, EN8 0XB
Member of Lower Lea Valley CCG and CEO of Lea Valley Health which is a GP federation encompassing the 8 practices in Lower Lea Valley.
Julie Sampson
Prescribing Advisor
y y y
Any other role or relationship which the public could perceive would impair or otherwise influence the individual's judgement or actions in their role within the CCG:
Husband - UK Medical Affairs Consultancy
Provides advice on development and marketing of prescribed medicines to pharmaceautical companies.

Did not tick all boxes - have not sent back M Delaney
GP, St Nicholas Health Centre
yDid not tick all boxes - have not sent back R Osman
GP, St Nicholas Health Centre y y

Page 1
Appendix L
REGISTER OF GIFTS AND HOSPITALITY REPORTED IN THE FINANCIAL YEAR 2015 TO 2016 This Register is established in accordance with the CCG’s Standards of Business Conduct Policy and will be reported on a six monthly basis to the Governance and Audit Committee.
Date reported
Reported by Nature of Hospitality or gift received Amount
01-06-2015 Anne Walker, Interim Manager – Commissioning Directorate
Social Event held by Dr Deborah Kearns and Roger Hawkin to celebrate 25 years in their house.
Wine and a BBQ were provided, and a bottle of Champagne and bunch of flowers received by Dr Kearns.
05-06-2015 Nichola Goddard, Locality Manager for North Herts and Welwyn Hatfield
Welwyn Hatfield 7 May 2015 Target Meeting. 10 Companies paid £250 each for a promotional table at the event. This money went towards funding, refreshments and premises hire. Companies: Astra Zeneca, Bayer, DB Ashbourne Ltd, Dermal, Merck, Novonordisk, NAPP, Pfizer, Sanofi Diabetes, Takeda.
£2500
05-06-2015 Nichola Goddard, Locality Manager for North Herts and Welwyn Hatfield
Welwyn Hatfield Implementation Panel (WHIP) meeting May 2015. Sponsorship provided in the form of a sandwich lunch for 12 delegates (10 GPs and 2 Practice Managers) Company: GlaxoSmithKline (GSK)
Circa Total Cost: £48 Estimated cost per head: £4
10-06-2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Lower Lea Valley Locality and Federation Meeting 2 April 2015. Each Company are told by the organiser to cater for 20 delegates, which comes to £80. 25 delegates attended. Company: Novo Nordisk.
£80 £3.20 per head

Page 2
Date reported
Reported by Nature of Hospitality or gift received Amount
10-06-2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Lower Lea Valley Locality Meeting 22 April 2015 Hospitality provided in the form of lunch by alternating companies. Lunch comes in the form of sandwiches, crisps, fruit and drinks. Each Company are told by the organiser to cater for 20 delegates, which comes to £80. However, 25-30 delegates usually attend. Company: Teva.
£80 £2.67-£3.20 per head
10-06-2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Lower Lea Valley Locality and Home First Meeting 7 May 2015. Hospitality provided in the form of lunch by alternating companies. Lunch comes in the form of sandwiches, crisps, fruit and drinks. Each Company are told by the organiser to cater for 20 delegates, which comes to £80. However, 30-35 delegates usually attend. Company: Pfizer
£80 £2.29-£2.67 per head
10-06-2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Lower Lea Valley Locality and Federation Meeting 2 April 2015. Each Company are told by the organiser to cater for 20 delegates, which comes to £80. 25 delegates attended. Company: Napp
£80 £3.20 per head
11-06-2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Stevenage Locality Meeting 21 April 2015. Bayer provided sponsorship towards premises hire and lunch. Premises used: Stevenage Football Club. 28-38 delegates usually attend.
£150 £3.95-£5.36 per head

Page 3
Date reported
Reported by Nature of Hospitality or gift received Amount
11-06-2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Stevenage Locality Meeting 12 May 2015. Merck, Sharp & Dohme Limited provided sponsorship towards premises hire and lunch. Premises used: Stevenage Football Club. 28-38 delegates usually attend.
£300. £7.89-£10.71 per head
16-06-2015 Phil Turnock, ICT Shared Services Director
Complimentary delegate pass and hotel accommodation at the Healthcare Strategy Forum.
Approximate value circa £400
16-06-2015 Simon Carey, Assistant Director, Business Relationships and Assurance
Complimentary delegate pass and hotel accommodation at the Healthcare Strategy Forum.
Approximate value circa £400
27/06/2015 Nichola Goddard, Locality Manager for North Herts and Welwyn Hatfield
17th June 2015 North Herts TARGET event. Funds received for Hospitality and premises hire from ten Pharmaceutical Companies: MSD, Steifel, GSK, AGA Matrix, Ashfield Healthcare, Astra Zeneca, Dermal UK, Leo, Boehringher, Bayer
Companies sponsored £200 each- Total received: £2000. Around 90 delegates attended. This worked out at £22.22 per head.
21/07/2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Lower Lea Valley Locality TARGET event. 7 Pharmaceutical Companies sponsored the TARGET event. The funds went towards catering and premises hire. The venue was asked to cater for 60 delegates. Companies: Pfizer, Leo-Pharma, BMS, Boehringer, Napp, Ashfield, Astra Zeneca.
7 Companies paid £250 each. £1750 in total. £29.17 per head.

Page 4
Date reported
Reported by Nature of Hospitality or gift received Amount
21/07/2015 Helen O’Keefe, Locality Manager for Stevenage and Lower Lea Valley
Lower Lea Valley Locality Meetings: 17th June 2015 – Lower Lea Valley Locality Meeting. Sponsor: Boehringer. Company Rep: Judy Humphreys from Boehringer. Hospitality provided in the form of lunch: sandwiches, crisps, fruit and drinks. 25-30 delegates usually attend. 2nd July 2015 – Lower Lea Valley Locality/Home First Meeting. Sponsor: Ashfield. Rep: Kashmira from Ashfield. Hospitality provided in the form of lunch: sandwiches, crisps, fruit and drinks. 30-35 delegates usually attend.
Approximate total value circa £80. Circa £2.67-£3.20 per delegate. Approximate total value circa £80. Circa £2.29-2.67 per delegate.
21/07/2015 Pam Jardine, Locality Manager for Stort Valley & Villages and Upper Lea Valley
Stort Valley and Villages TARGET: 30th June 2015 Sponsored by three companies: Leo Pharma, Astra Zeneca and DB Ashbourne.
£200 each towards Hospitality. Total sponsorship: £600 Catering was ordered for 40 people. This worked out at £15 per head.
21/07/2015 Pam Jardine, Locality Manager for Stort Valley & Villages and Upper Lea Valley
Upper Lea Valley TARGET: 25th June 2015 Merck Sharp and Dohme provided premises and catering.
Catering cost £13.42 per head. Catering was ordered for 84 people. Catering total: £1127.28
20-08-2015 Sue Russell, Lead Pharmacist
“Bursary place” at Pharmacy Management National Forum London 18-11-14. www.pharman.co.uk Workshop between NHS medicines payers and pharmaceutical industry, sponsored by Novartis Pharmaceuticals UK Ltd and Shire Pharmaceuticals Ltd.
Value unknown. Place covered day attendance at venue, satellite sessions, buffet lunch and hot drinks.

Page 5
09-09-2015 Helen
Edmondson – Associate Director of Commissioning – Localities
Stevenage Locality Meetings. Locality Meetings sponsored by Pharmaceutical Companies. The money goes towards premises hire and lunch (premises used is Stevenage football club). 16th June 2015 Sponsored by Astra Zeneca. 28-38 delegates usually attend. 21st July 2015 Sponsored by Merck. 28-38 delegates usually attend.
£150. Circa £3.95 to £5.36 per head. £150. Circa £3.95 to £5.36 per head.
09-09-2015 Helen Edmondson – Associate Director of Commissioning – Localities
Stevenage TARGET: 16th July 2015 6 companies paid for a promotional table at the event. Sponsored by GSK, Merck, Bayer, Lilly, Astra Zeneca and Ashfield Healthcare. The money went towards funding refreshments and premises hire.
6 companies paid £250 each. Total: £1500.

Agenda Item No: 7
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Infection Prevention and Control Annual Report
Decision Discussion Information Follow up from last meeting
Report author: Fiona Simpson
Head of Infection Prevention and Control, ENH CCG & HV CCG
Report signed off by: Sheilagh Reavey Director of Nursing and Quality, ENH CCG
Purpose of the paper: ENH CCG Annual Infection Prevention and Control Report
for 2014/2015 provides information on the delivery of the infection prevention and control activity for ENH CCG for the year. The aim of the report is to provide assurance that patients receiving care from services commissioned by ENH CCG are protected from the risks of HCAI (Healthcare Associated Infections) and cared for by staff providing the highest standards of infection prevention and control.
Conflicts of Interest involved:
None
Recommendations to the Governing Body:
This paper is for information

East and North Hertfordshire Clinical Commissioning Group
Infection Prevention & Control
Annual Report 2014/2015
Lead Director Sheilagh Reavey Director of Nursing and Quality ENH CCG Author Fiona Simpson Head of Infection Prevention and Control ENH CCG & HV CCG

2
Contents
Item Page
1. Executive Summary 3
2. Introduction 5
3. Infection Control arrangements 6
4. HCAI (Healthcare Associated Infections) reported through national mandatory surveillance
8
5. Current HCAI challenges 19
6. Outbreaks and incidents 20
7. Supporting providers to deliver best practice standards 21
8. Priorities for 2015/16 21
9. Summary 22
10. Key documents 23
11. Abbreviations used in this report 23
12. Appendix 1: East and North Hertfordshire and Herts Valleys Clinical Commissioning Groups’ Health Care Associated Infection (HCAI) Reduction Plan 2014/2015

3
1. Executive Summary 1.1 Introduction NHS East and North Hertfordshire Clinical Commissioning Group’s (ENH CCG) Annual Infection Prevention and Control Report for 2014/2015 provides information on the delivery of the infection prevention and control activity for ENH CCG for the year. The aim of the report is to provide assurance that patients receiving care from services commissioned by ENH CCG are protected from the risks of HCAI (Healthcare Associated Infections) and cared for by staff providing the highest standards of infection prevention and control. ENH CCG is committed to reducing the risk of infections through the provision of the highest standards of infection prevention practice. Patient welfare and safety is a high priority, as is reducing the risk of infection to a minimum. 1.2 Infection Control arrangements ENH CCG has robust governance structures in place for the management of healthcare associated infections within the Hertfordshire health economy. This includes:
• The ENH CCG Infection Control Strategy • An annual plan to deliver reduction in cases of infection across Hertfordshire • Reporting mechanisms for infection prevention and control risks which ensure The ENH CCG Board
is kept informed of infection control issues • The Director of Nursing and Quality as the named member of the board for infection prevention and
control. • Forums including the Herts Health Economy Infection Control Group to facilitate partnership working
and the effective delivery of improvements to infection prevention and control practice. • Provision of leadership for the infection control agenda through the post of ENH CCG Head of
Infection Prevention and Control. • Review of infection prevention and control issues at quality review Meetings
1.3 Key achievements delivered in 2014/15 The following achievements for infection prevention and control have been delivered in 2014/15:
• Following the 43% increase in Clostridium difficile (C. difficile) cases in 2013/14 and during a period when a 7.5% increase in cases across the Midlands and East of England has been experienced, there has been no increase in cases for ENH CCG during 2014/15.
• A 12% reduction in C. difficile cases occurring in acute trusts has been delivered. • ENH CCG’s rate for C. difficile is the 3rd lowest out of the 7 CCGs in the SMH Area and is below the
average for the South Midlands and Hertfordshire Area and below the National Average. • ENHT has been supported to achieve a 14% reduction cases of C. difficile and has delivered it’s NHS
England annual limit for cases • HCT has been supported to achieve a 69% reduction cases of C. difficile and has delivered it’s NHS
England annual limit for cases • A 14% reduction in primary care prescribing levels for the antibiotics targeted with associated high
risk for C. difficile infection has been delivered. 1.3 Key practice developments implemented in 2014/15 Through the successful development of partnership working in infection prevention and control across the health economy the following developments in practice have been implemented:
• A standard tool to investigate C. difficile cases has been developed and implemented across the health economy.

4
• The completion of case reviews for patients with C. difficile in the community setting has been implemented.
• ENHT was supported to set up monitoring of the isolation of patients with diarrhoea in line with the national guidance time frame of 2 hours.
• The Medicines Management Team have developed data covering primary care antibiotic prescribing to show trends over time and give practice specific results.
• Education events have been delivered in all ENH CCG Localities to raise awareness of C. difficile infection and support compliance to antibiotic guidelines in primary care.
• Antibiotic prescribing was included in ENH CCG’s local commissioning framework for 2014/15, with the requirement for practices to demonstrate improvement through audit results.
• A competency assessment tool for staff taking blood cultures has been developed and shared across the health economy.
• An information sheet has been produced which gives guidance on the infection control requirements for the on-going care of urinary catheters in the community setting.
• A communications cascade has been set up to alert organisations about outbreaks of diarrhoea and vomiting in community settings across the health economy.
• In response to the Public Health England toolkit for hospitals to detect, manage and control antibiotic-resistant bacterial infections caused by Carbapenemase-producing Enterobacteriaceae (CPE), local measures have been put in place to identify and manage cases in the health economy.
• Providers have been supported to put procedures in place in order that potential cases of Ebola could be identified and managed safely.
1.4 End of year position for HCAI 2015/16 C. difficile ENH CCG had a total of 110 cases of C. difficile in 2015/16. This is 13 cases over the NHS England limit for the CCG of 97 cases for the year and equal to the number of cases that occurred in 2013/14. NHS England has set a limit of 112 cases for ENH CCG for 2015/16. MRSA bacteraemia NHS England has a national target to achieve zero cases of MRSA bacteraemia for all CCGs and acute trusts. During 2014/15 there were 10 cases of MRSA bacteraemia in ENH CCG patients. 5 cases were assigned to acute trusts, all of which occurred at ENHT. There was an additional case which was assigned as a 3rd party case by NHS England and was, therefore, not included in monitoring data. 1.5 Priorities for 2015/16 The infection prevention and control priorities for ENH CCG for 2015/16 include: • Further developing partnership working across the health economy, which is crucial to the continued
improvement of infection control practice. By way of continued support for the work of the Herts Health Economy Infection Control Group and working actively with providers to facilitate developments to improve standards of infection prevention and control.
• The continued close monitoring of the incidence of infections and infection control incidents and awareness of new emerging infections, in order to be able to effectively respond to current and new infection prevention and control challenges.
• The provision of continued leadership to promote excellence in infection prevention and control and to challenge any identified lapses in standards of care.
• The delivery of the NHS England annual target of 112 C. difficile cases for ENH CCG for 2015/16. Following the 6% increase in non-acute cases in 2014/15, focus must be kept on the reduction in non-acute cases and further develop participation in joint case review meetings and support providers to deliver their annual limits through the provision of the highest standards of infection prevention and control.

5
• The continuation of the work of the ENH CCG Medicines Management Team in promoting compliance to antibiotic prescribing guidelines and supporting the delivery of the NHS England antibiotic quality premium.
• Working towards delivery of NHS England’s target of reducing MRSA bacteraemias to achieve zero avoidable cases. Following the increase in MRSA bacteraemia cases in 2014/15 action is needed in the following key areas:
o Improving the management of intravenous devices o Reducing risks of contamination of samples when blood cultures are taken o Improving the risks associated with urinary tract infections and urinary catheters o Improving the management of the screening and treatment of patients with MRSA
• Supporting providers to ensure that excellent standards of infection prevention and control are in place and the requirements of the Care Quality Commission (CQC) are met, through quality review meetings and quality assurance visits.
The success of the continued drive to reduce the cases of infection and provide the highest standards of infection prevention and control practice for the population of Hertfordshire is dependent on the continued commitment of key partners across the Hertfordshire Health Economy. The sustained effort of providers across Hertfordshire, which has resulted in significant reductions in the incidence of HCAI, is acknowledged. There has been considerable progress by ENH CCG in the provision of infection prevention and control which has been achieved by working very closely with provider organisations, and through the delivery of initiatives to improve the quality and safety of healthcare in Hertfordshire. By strengthening the current systems and implementing new evidence based initiatives, ENH CCG is committed to reducing the risk of infection to a minimum for patients, staff and the population of Hertfordshire.
2. Introduction ENH CCG’s Annual Infection Prevention and Control Report for 2014/2015 provides information on the delivery of the infection prevention and control activity for ENH CCG for the year. The aim of the report is to provide assurance that patients receiving care from services commissioned by ENH CCG are protected from the risks of HCAI and cared for by staff providing the highest standards of infection prevention and control. ENH CCG is committed to reducing the risk of infections through the provision of the highest standards of infection prevention and control practice. Patient welfare and safety is a high priority, as is reducing the risk of infection to a minimum. The overall aim is to minimise the harm to patients, staff and the population by preventing and controlling infections in hospitals, primary care and community settings. This is achieved by developing a culture whereby patient, staff and visitor safety is ensured through the provision of excellence in all aspects of infection prevention practice. The Health and Social Care Act (2008) emphasised that the prevention and control of Healthcare Associated Infections (HCAI) is a high priority for all parts of the NHS and other healthcare providers. It is estimated about 1 in 10 patients acquire a HCAI whilst they are in hospital. HCAI costs the NHS in excess of £1billion per annum and potentially causes 5,000 deaths per year. As well as increased morbidity or mortality, HCAI have a social-economic impact for patients. Up to 30% of HCAI’s are preventable through good infection control practices, therefore, the risk of poor infection prevention practice by Healthcare workers presents a significant risk to both patients and commissioning bodies. ENH CCG works in partnership with key organisations across the health economy to ensure best practice standards for infection control with the Hertfordshire Health Economy Infection Control Group providing the forum to facilitate this joint working. Key partners include:
• The Public Health Team at Herts County Council (HCC). HCC have overall responsibility to ensure that the population of Hertfordshire is protected from the risks of infection and that strategies are in place to manage the risks of infection for the population.

6
• South Midlands and Hertfordshire Public Health England Centre (SMH PHEC). SMH PHEC provide expert advice and support to enable EN HCCG to fulfil their health protection responsibilities. This support includes the surveillance and control services for communicable disease. The SMH PHEC team provide support and advice in the management of outbreaks of infection and leadership for the delivery of national strategies for the reduction of HCAI.
• The Hertfordshire and South Midlands Area Team (HSM Area Team) - HSM Area Team provide the leadership for quality and safety across the HSM Area and are responsible for providing assurance to the Department of Health that systems are in place which protect patients from the risks of HCAI and promote best practice standards for infection control.
• Healthcare providers including; NHS East and North Hertfordshire NHS Trust (ENHT), West Hertfordshire Hospitals NHS Trust (WHHT), Herts Community NHS Trust (HCT), Herts Urgent Care (HUC).
• The Local Medical Committee (LMC).
3. ENH CCG Infection Control arrangements ENH CCG has a framework through which the delivery of the highest standards of infection control is assured. 3.1 Roles and responsibilities • ENH CCGs’ Accountable Officer has overall responsibility for ensuring that effective commissioning of
services takes place to minimise risks of infection for the population of ENHCCG and that the requirements of the Health and Social Care Act 2008 are met.
• The Director of Nursing and Quality is the ENHCCG board member with responsibility for Infection Prevention and Control. The Director for Nursing and Quality provides the organisational overview for infection control and ensures the quality and safety of commissioned services.
• The Head of Infection Prevention and Control employed by Herts Valleys CCG (HV CCG) in a joint post across both CCGs, provides the strategic lead for the infection control agenda for ENHCCG and for countywide initiatives to achieve the reduction of HCAI across the health economy.
ENHCCG Governance Structure for Infection Control
ENHCCG SMH HCC PHEC HVCCG LMC Rep HSM
Area Team
ENHCCG Board
Quality Committee
Hertfordshire Health Economy Infection Control Group
Providers: ENHT WHHT HCT HPFT HUC GP

7
3.2 Implementation and governance arrangements ENH CCG has an Infection Prevention and Control Strategy through which the CCG prioritises and delivers actions to effectively manage the risks of HCAI for the population of Hertfordshire. An annual Health Care Associated Infection Reduction Plan details key objectives and actions required to deliver the infection prevention agenda for ENH CCG. Effective implementation of this annual plan provides assurance on the delivery of the ENH CCG Infection Prevention and Control Strategy. ENH CCG Board is informed of infection control issues through individual infection control reports and the provision of the minutes of the ENH CCG Quality Committee. Engagement of key partners and the implementation of countywide actions to improve standards of infection control practice is achieved through the Hertfordshire Health Economy Infection Control Group (HHEICG). This group reports to the ENHCCG Quality Committee through the provision of minutes to the committee. Standards of infection control practice delivered by ENH CCG commissioned services are monitored through quality dashboards, quality review meetings, quality assurance visits and the delivery of Department of Health (DH) limits for HCAI. Countywide action plans are used to manage the delivery of specific programmes of work and responses to infection control concerns. 3.2.1 The Hertfordshire Health Economy Infection Control Group (HHEICG) The role of HHEICG is to provide a countywide forum to drive improvements in the standards of infection control provided by healthcare services in Hertfordshire. Membership of HHEICG includes representatives from key providers of healthcare across the county, Public Health England: South Midlands and Hertfordshire Centre (PHE SMH) and The Public Health Team in Hertfordshire County Council. This group meets bimonthly. The role of the HHEICG includes: • Developing and sustaining working partnerships with relevant organisations in order to reduce the risk of
infection for patients, staff and visitors in the acute and community setting. • Providing assurance that infection prevention and control issues across healthcare providers in
Hertfordshire are being managed appropriately. • Providing challenge where standards of infection control need to improve. • Advising ENHCCG Quality Committee of infection control and prevention issues and any significant risks
that may impact on Hertfordshire services and making recommendations to eliminate or reduce them. • Reviewing significant incidents and outbreaks relating to infections in the county and monitoring progress
on any related action plans. • Having an overview of infection rates and trends across the county and using this information to drive
action across the county to improve standards of infection prevention and control. • Proactively identifying and implementing new measures based on scientific evidence for reducing the
burden of infections in the community and hospitals 3.2.2 C. difficile Task and Finish Group In response to the identified need to reduce levels of C. difficile infections across Hertfordshire the Hertfordshire C. difficile Task and Finish Group was formed by the Hertfordshire Health Economy Infection Control Group. The group was set up on 22/10/13 with the primary role to identify and deliver actions to reduce the incidence of C. difficile infections for the population of Hertfordshire through collaborative working across the whole health economy. The group reported to and was monitored by the Herts Health Economy Infection Control Group. Following the successful delivery of actions to reduce the risks of C. difficile, the group held its last meeting on 24/06/14. However members of the group found this a very effective forum for

8
discussion and joint problem solving. Therefore, the group agreed to set up the Herts HCAI reduction Group as a working group with a wider infection control agenda. 3.2.3 Herts HCAI reduction Group The Herts HCAI Reduction Group was set up on 19/08/14 to provide a forum to discuss and implement responses to on-going infection control challenges across the health economy. This multi-agency group reports to and is monitored by the Herts Health Economy Infection Control Group. The work of this group includes actions to reduce risks of C. difficile, MRSA bacteraemia, Ebola, and Norovirus across the health economy. The group provides the opportunity for communication and problem solving to improve standards of infection control. 3.3 Internal Audit of infection control processes During 2014/15 internal auditors carried out an audit of the governance arrangements in place within the CCG to provide assurance that infections within provider organisations are effectively managed and that there is adequate reporting of infection control issues to the Quality Committee and Governing Body. The outcome of the audit was to confirm that ENH CCG has robust governance structures in place for the management of healthcare associated infections within the Hertfordshire health economy. As an outcome of the audit, there were 3 low priority recommendations and one medium priority recommendation which was the completion of the planned formal ratification of ENH CCG’s Infection Prevention and Control Strategy. The strategy was ratified by the ENH CCGs Quality Committee on 04/12/14. 4. HCAI reported through national mandatory surveillance This section covers the infections that are required to be reported on the Public Health England Surveillance scheme. This includes:
• C. difficile • MRSA bacteraemia • MSSA bacteraemia • E. coli bacteraemia
Data for this report is sourced from the HPA HCAI Data Capture System and directly from provider organisations. The report includes all cases in patients that are registered with ENH CCG GPs. This includes cases in ENH CCG patients that are reported from acute services outside Hertfordshire. Cases of C. difficile and MRSA bacteraemia are allocated as follows:
• C. difficile cases identified in the community setting or in patients on the day of admission or in the two days following the day of admission to an acute trust are designated as non-acute cases. Other cases are designated as acute cases. When the review of a case does not identify any lapses in care, a Trust can appeal to the commissioning CCG for the case not to be counted against their annual limit.
• From April 2014 NHS England changed the way in which MRSA bacteraemia cases are allocated. This change resulted in cases being assigned to the organisation best placed to implement the learning identified through the completion of a post infection review.
• Non-acute cases include patients in their own home, in care homes and in care homes with nursing. • Cases are allocated to HCT inpatient areas as above and are included in non-acute cases in the data
given below.

9
4.1 C. difficile 4.1.1 Overview Clostridium difficile (C. difficile) infection is the most important cause of hospital acquired diarrhoea. Significant numbers of C. difficile infections also occur in the community setting. When antibiotics disturb the balance of bacteria in the gut, C. difficile can multiply rapidly and produce toxins which cause illness which can range from mild symptoms to severe illness. Certain antibiotics have an associated higher risk for the development of C. difficile infection and therefore best prescribing practice for these antibiotics which include Co-amoxiclav, Cephalosporins & Quinolones is a key area of work for ENH CCG. C. difficile spores can survive for prolonged periods in the environment. Effective environmental cleaning and hand hygiene are essential for the control of this infection. Acute NHS Trusts in England are required to report all cases of C. difficile in patients aged two years and over. This information is used to monitor the number of infections and the progress of trusts towards meeting annual targets for the reduction in the number of C. difficile infections. Cases are reported via national mandatory surveillance and local incidence by provider is monitored by ENH CCG. Case reviews are completed in order to identify learning which can be implemented to reduce the risk of further cases. Acute Trusts and Clinical Commissioning Groups are set trajectory annual limits by NHS England as part of the national approach to reducing the number of cases. ENH CCG set a locally agreed annual limit for HCT. 4.1.2 Data on C. difficile cases C. difficile rates are given as cases per 100,000 population. The following graph illustrates that the Hertfordshire and South Midlands Area has the 3rd lowest rate for C. difficile in NHS England in 2013/14.

10
During 2014/15 ENH CCG has the 3rd lowest rate out of the 7 CCGs in the Hertfordshire and South Midlands Area as shown in the graph below.
ENH CCG C. difficile rate in 2014/15 was 20.53. The national average was 26.71. ENH CCG had the 45th lowest rate of C. difficile out of the 211 CCGs in England as shown in the graph below.
The relatively good position of ENH CCG with respect to C. difficile needs to be taken into account when considering the actions put into place in 2014/15 and the outcomes achieved.

11
4.1.3 The challenge for 2014/15
The graph above shows the 62% reduction in cases achieved from 2009/10 to 2012/13. However, ENH CCG experienced 43% increase in cases during 2013/14 and failed to deliver the CCG’s Department of Health annual trajectory limit for 2013/14. The greater reduction in cases had been achieved in the cases occurring in hospital settings. Work to reduce the number of non-acute cases was needed. Due to the fact that cross infection is a less significant risk for patients in their own home, ensuring best practice for antibiotic prescribing in line with antibiotic guidelines is the key opportunity to reduce non acute cases. ENH CCG also worked with acute providers to ensure that best practices standards for hand hygiene and standards of cleaning of the clinical environment and patient equipment were in place. 4.1.4 Actions taken during 2014/15 to reduce risks of C. difficile infection across the health economy. Countywide initiatives taken to reduce the risk of C. difficile infection included:
• A health economy action plan to deliver improvements to standards of patient management and infection control.
• Advice and input from Public Health England to ensure that all appropriate actions were in place. • Surveillance processes set up to ensure that accurate information is available to monitor cases
across the county. • A standard tool to investigate cases developed and implemented across the health economy. • All cases investigated with learning shared across the health economy via the Herts Health Economy
Infection Control Group. • Activities delivered across services to raise awareness for The European Antibiotic Awareness Day.
Actions targeted to reduce cases in primary care included:
• A data base developed to collate themes and lessons learned from cases. • Antimicrobial Prescribing Strategy supporting best practice standards for antibiotic prescribing in the
primary care setting. • The Medicines Management Team monitored and fed back monthly data on antibiotic prescribing
levels to GP practices. The data was developed to clearly show trends over time and give practice specific results.
• Education events delivered in all ENH CCG Localities to raise awareness of C. difficile infection and support compliance to antibiotic guidelines in primary care. Presentations were jointly facilitated by

12
ENH CCG Antibiotic Specialist Pharmacist, ENH CCG Head of Infection Prevention and Control and ENHT Consultant Microbiologist.
• Promotion of the Primary Care Antibiotic Guidelines. • Antibiotic prescribing included in ENH CCG’s local commissioning frame work, with the requirement
for practices to demonstrate improvement through audit results. • Antibiotic prescribing discussed at all primary care medicines locality meetings. • ENH CCG Head of Infection Prevention and Control completed and presented a thematic review of
learning from cases across the H&SM Area, at an Area Education Event. • ENH CCG Head of Infection Prevention and Control delivered an education session to care home
staff at a Herts Care Providers Association training event. This provided the opportunity to promote the use of the Bristol Stool Chart and the use of Chlorine based cleaning agents.
Actions taken to reduce cases in Hertfordshire providers included:
• • Assurance on delivery of best practice standards and challenge to identify lapses of care at Quality
Review Meetings, Quality assurance visits, and case review meetings. • Monitoring performance of providers in relation to incidence of cases against trajectories. • On-going work with providers to ensure that high standards of infection control including hand
hygiene and cleanliness are maintained. • Effective engagement of providers at the Herts Health Economy Infection Control Group Meetings
and attendance by the CCG Lead for Infection Prevention and Control at provider Infection Control Committee meetings.
• ENHT was supported to set up monitoring of the isolation of patients with diarrhoea in line with national guidance time frame of 2 hours.
• Antibiotic prescribing audited by acute providers and results shared with ENH CCG. • In response to the Department of Health’s guidance ‘Clostridium difficile infection objectives for NHS
organisations in 2014/15 and guidance on sanction implementation’ a countywide process has been developed and implemented to review individual cases.
4.1.5 Learning achieved from C. difficile case reviews. During 2014/15 a system to complete case reviews for non-acute cases of C. difficile was put in place. The following themes were identified in the case reviews as risk factors for developing C. difficile:
• antibiotic treatment • older age • recent admission to hospital • complex medical conditions • treatment with proton pump inhibitors
Provider services have continued to complete case reviews for those cases associated with their services and this has facilitated the review of standards of infection control and processes for managing the risks of C. difficile in in-patient areas. During 2014/15 the undertaking of joint case reviews for C. difficile cases involving more than one service has been developed. This has facilitated greater understanding of the cases and provided greater opportunity for the identification and implementation of learning to improve patient care. 4.1.6 Outcomes achieved The 43% increase in C. difficile cases experienced in 2013/14 has been halted and a 12% reduction in cases associated with acute services has been achieved. This was during a period when the Midlands and East of England Region experienced an overall 7.5% increase in cases. During 2014/15 the ENH CCG rate for C. difficile was the 3rd lowest out of the 7 CCGs in the SMH Area and was below the average for the SMH area and below the National Average.

13
The total number of cases that occurred in ENH CCG patients during 2014/15 was 110. This was 13 cases more than the annual limit for the CCG and is equal to the number of cases that occurred in 2013/14. The graph below illustrates the incidence of cases through the year.
Local providers have been supported to deliver improvements to standards of infection prevention and control and achieve the following percentage reduction in cases in 2014/15 when compared to the number of cases in 2013/14. All delivered their annual limit for C. difficile cases.
NHS Trust Percentage reduction in C. difficile achieved during 2014/15 Annual limit delivered. ENHT 14% Yes PAH 11% Yes WHHT 18% Yes HCT 69% Yes HPFT No cases Yes
The following graph illustrates the trusts at which ENH CCG acute cases of C. difficile occurred. The majority of cases occurred in trusts other than ENHT.
0
20
40
60
80
100
120
Apr
May Jun Jul
Aug
Sep
Oct
Nov De
c
Jan
Feb
Mar
ENCCG C. diff cases 2014/15
Monthly cases
Cumulative cases
Cumulative limit
2013/14 cumulativecases

14
Work by ENH CCG Medicines Management Team has resulted in a 14% reduction prescribing levels for the antibiotics targeted with associated high risk for C. difficile infection from the position in 2013/14. This is a further improvement from that achieved in 2012/13 as shown in the graph below.
The following graph illustrates how the comparative percentage prescribing rate for Co-amoxiclav, Cephalosporins & Quinolones for ENH CCG (in Blue) is significantly lower than the national rate (in red).
4.1.7 Challenges for 2015/16 In addition to the impact on individual patients, the 110 C. difficile cases that occurred in 2014/15 had a potential cost of £770,000 and potentially used 2,310 hospital bed days.
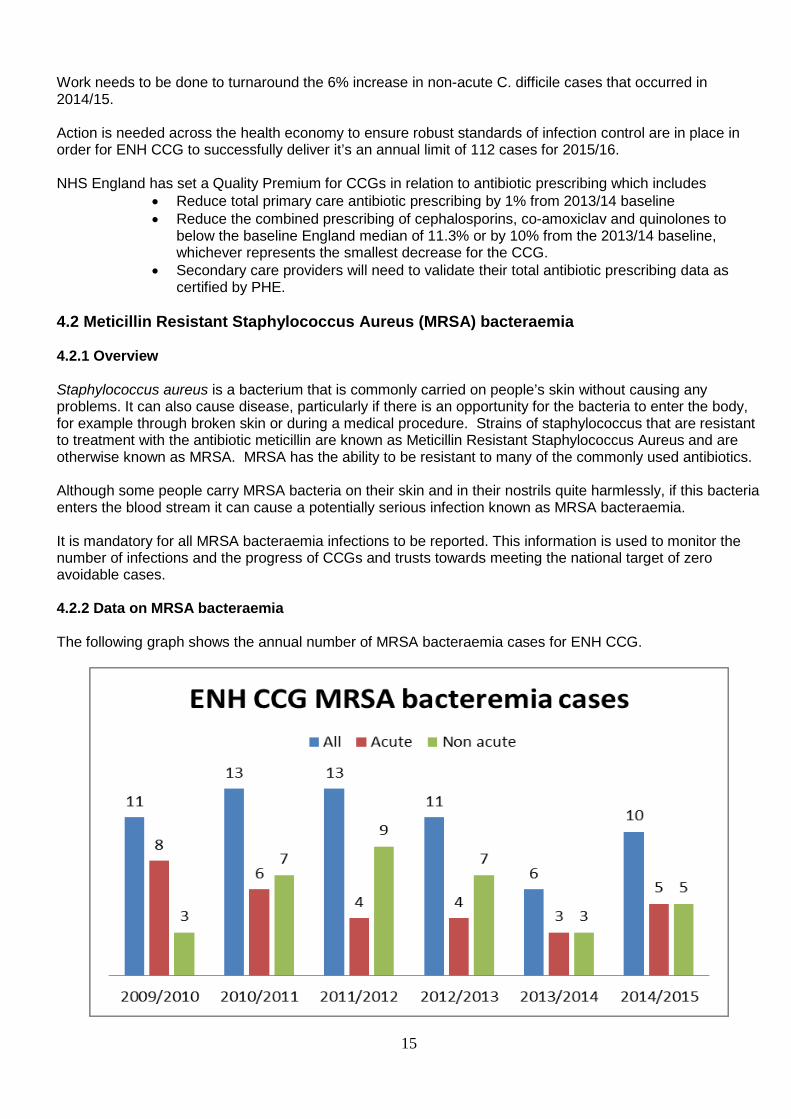
15
Work needs to be done to turnaround the 6% increase in non-acute C. difficile cases that occurred in 2014/15. Action is needed across the health economy to ensure robust standards of infection control are in place in order for ENH CCG to successfully deliver it’s an annual limit of 112 cases for 2015/16. NHS England has set a Quality Premium for CCGs in relation to antibiotic prescribing which includes
• Reduce total primary care antibiotic prescribing by 1% from 2013/14 baseline • Reduce the combined prescribing of cephalosporins, co-amoxiclav and quinolones to
below the baseline England median of 11.3% or by 10% from the 2013/14 baseline, whichever represents the smallest decrease for the CCG.
• Secondary care providers will need to validate their total antibiotic prescribing data as certified by PHE.
4.2 Meticillin Resistant Staphylococcus Aureus (MRSA) bacteraemia 4.2.1 Overview Staphylococcus aureus is a bacterium that is commonly carried on people’s skin without causing any problems. It can also cause disease, particularly if there is an opportunity for the bacteria to enter the body, for example through broken skin or during a medical procedure. Strains of staphylococcus that are resistant to treatment with the antibiotic meticillin are known as Meticillin Resistant Staphylococcus Aureus and are otherwise known as MRSA. MRSA has the ability to be resistant to many of the commonly used antibiotics. Although some people carry MRSA bacteria on their skin and in their nostrils quite harmlessly, if this bacteria enters the blood stream it can cause a potentially serious infection known as MRSA bacteraemia. It is mandatory for all MRSA bacteraemia infections to be reported. This information is used to monitor the number of infections and the progress of CCGs and trusts towards meeting the national target of zero avoidable cases. 4.2.2 Data on MRSA bacteraemia The following graph shows the annual number of MRSA bacteraemia cases for ENH CCG.

16
The data illustrates the reduction in numbers achieved from 2011/12 to 2013/14. However during 2014/15 there has been an increase in the number of cases. 5 of the cases occurred in the non-acute setting and 5 were acute cases occurring at ENHT. There was an additional case which was assigned as a 3rd party case by NHS England and was therefore not included in monitoring data. The graph below shows the increase in cases that occurred at ENHT in 2014/15. 2 of the 5 cases at ENHT were the result of contaminated samples. 3 cases were actual clinical infections.
All cases of MRSA have a post infection review to investigate the case and identify the learning that can be used to reduce future cases. The graph below shows the learning for services across Hertfordshire identified through the review of the cases for ENH CCG and Herts Valleys CCG patients.

17
4.2.3 Actions taken to reduce cases of MRSA bacteraemia The following actions have been taken to reduce the risk of MRSA bacteraemia:
• Reducing the risks related to intravenous (IV) access o ENH CCG has incorporated review of the management of IV devices in the CCG assurance
visits to Trusts. o Providers have reviewed their policies in light of the EPIC 3 guidelines (Dec 2013) to ensure
best practice standards for the management of IV access. o Providers have audit processes in place to monitor the standards of practice for the care of IV
devices. • Reducing the risk of contamination of samples
o Providers have specific training in place for staff who take blood culture samples. o A competency assessment tool for staff taking Blood cultures has been developed and shared
across the health economy. o A poster ‘Taking Blood Cultures Using a Safe Needle Collection System’ has been developed
and shared across the health economy. • Supporting best practice infection control standards for the on-going management of urinary
catheters in the community an information sheet has been produced which gives guidance on the infection control requirements for the on-going care of urinary catheters.
4.2.4 Outcomes achieved Targeted work has been completed which is specifically aimed at reducing risks associated with MRSA bacteraemia. However, despite this work the number of cases for ENHCCG patients has increased during 014/15. 4.2.5 Challenges for 2015/16 Using the learning achieved through the review of the cases during 2014/15 is a priority to reduce the risk of future cases. This work will be driven through the Herts HCAI Reduction Group and will need to include:
• Improving the management of IV devices • Reducing risks of contamination of samples when blood cultures are taken • Improving the risks associated with urinary tract infections and urinary catheters • Improving the management of the screening and treatment of patients with MRSA.
4.3 Meticillin Sensitive Staphylococcus Aureus (MSSA) 4.3.1 Overview Staphylococcus aureus that is sensitive to and can therefore be treated with the antibiotic meticillin is referred to as meticillin sensitive staphylococcus aureus or MSSA. The Department of Health commenced mandatory surveillance of MSSA bacteraemias on 1st January of 2011 with the aim of gaining a better understanding of the levels of infection at a local and national level and to support actions to reduce the number of cases.

18
4.3.2 Data on MSSA
The number of cases of MSSA bacteraemia reported from within the county is stable when compared with 2013/14. The overall increase in cases for ENH CCCG patients in 2014/15 as illustrated in the graph above is due to an increase in acute and non-acute cases reported by services outside the county. ENHT complete case reviews for cases occurring at the Trust with learning identified implemented across the Trust to improve infection control practice. ENH CCG monitors the incidence of MSSA across the county, supports best practice standards to manage risks of MSSA. 4.4 Escherichia coli (E. coli) bacteraemia E. coli is a species of bacteria commonly found in the intestines of humans and animals. There are many different types of E. coli, and while some live in the intestine quite harmlessly, others may cause a variety of diseases. The most common disease caused by E. coli is infection of the urinary tract. E. coli can also cause blood stream infections, E. coli bacteraemia which is a more serious infection. The Department of Health commenced mandatory surveillance of E. Coli bacteraemia infections on 1st June 2011 with the aim of gaining a better understanding of the levels of infection at a local and national level, and to support actions to reduce the number of cases. 4.4.1 Data on E. coli bacteraemia

19
During May 2014 there was an isolated increase in the number of cases of E. coli bacteraemia for ENH CCG patients. The surveillance data for these cases was reviewed but no common themes that explained the increase in cases was identified. Overall there was a decrease in the number of cases from the previous year. The majority of cases do not have any specific risk factors. However, as significant number of cases is linked to urinary sepsis, it will be useful to take forward countywide work to reduce risks of urinary tract infections.
5. Current challenges 5.1 Norovirus Norovirus, also known as winter vomiting disease, causes gastroenteritis and is highly infectious. The virus is usually mild and lasts for 1 to 2 days. Symptoms include vomiting, projectile vomiting, diarrhoea and fever. Most people make a full recovery within a couple of days but it can be dangerous for the very young and elderly people. The virus is easily transmitted through contact with infected individuals from one person to another. Outbreaks are common in semi-enclosed environments such as hospitals, nursing homes, schools and cruise ships and can also occur in restaurants and hotels. Outbreaks have an impact on the individuals affected by Norovirus, however, the closure of beds and wards can severely adversely affect the operational activity of organisations and so prevention and effective management of outbreaks is a high priority. There has been significant incidence of Norovirus in Hertfordshire during 2014/15 with 18 outbreaks occurring in health services. ENH CCG has taken the following actions to manage the risk of Norovirus:
• Proactively working with health services to ensure effective outbreak measures are in place. • A communications cascade has been set up to ensure that key individuals across the health
economy are aware of outbreaks. This reduces the risk of outbreaks being seeded to other organisations by making sure that organisations are aware of potential risks associated with patients who are unavoidably transferred from units with outbreaks.
• Supporting health services during periods of outbreak.
Further work to support the health economy to better manage the risks of Norovirus outbreaks is needed during 2015/16. 5.2 Carbapenemase-producing Enterobacteriaceae (CPE) Enterobacteriaceae are a group of bacteria carried in the gut of all humans and animals, which is perfectly normal. While they are usually harmless they may sometimes spread to other parts of the body such as the urinary tract or into the bloodstream (bacteraemia) where they can cause serious infections. Carbapenemase-producing Enterobacteriaceae (CPE) is the name given to some strains of Enterobacteriaceae that have developed the ability to destroy an important group of antibiotics called carbapenems, making them resistant to these drugs. Carbapenems are considered to be antibiotics of ‘last resort’ and doctors rely on them to treat certain difficult infections when other antibiotics would or have failed. Infections caused by CPE can usually still be treated with antibiotics. However, treatment is more difficult and may require a combination of drugs or the use of older antibiotics to be effective. In response to the sustained increase in the number of CPE infections identified Public Health England launched a toolkit for hospitals to detect, manage and control antibiotic-resistant bacterial infections caused

20
by CPE. This tool kit has been shared across the health economy and local measures have been put in place in response to the guideline to identify and manage cases in the health economy. In March 2015 ENH CCG provided feedback on the draft Public Health England Toolkit for Managing Carbapenemase-producing Enterobacteriaceae in Non-acute and Community Settings. Implementation of measures to respond to CPE infections in the community will need to be put in place during 2015/16. 5.3 Ebola Ebola virus is a rare but severe infection in humans and non-human primates. It is caused by the Ebola virus. The Ebola virus has caused sporadic outbreaks since in several African countries. During 2015 a large outbreak occurred in West Africa. Due to the size of the outbreak and the difficulty in containing it locally, this outbreak posed a potential health threat to the UK through the risk of individuals potentially affected by the virus traveling to the UK during the period during which cross infection of others was possible. PHE has led nationally and regionally on the response to the Ebola threat. ENH CCG took action to ensure local responses were in place in order that potential cases could be identified and managed safely. This included ensuring health workers had appropriate understanding of the risks associated with the disease, services had appropriate process in place and adequate provision of supplies for patient care. ENH CCG actions included:
• Participating in county and regional preparedness planning meetings. • Working with local providers to ensure safe processes were in place to identify and treat potential
cases. This included attending planning meetings held at ENHT. • Cascading information and guidance to EN CCG GP surgeries. • Providing relevant information and guidance for health care professionals on the ENH CCG website
Potential cases of Ebola were identified and appropriately managed by services but no confirmed cases of Ebola were diagnosed in Hertfordshire. 6. Outbreaks and incidents 6.1 Tuberculosis (TB) case Following the identification of a member of staff working in an outpatient area with TB a multiagency, cross county, incident control group was set up and led by PHE to manage the response to the incident. Learning achieved from the incident was shared at the Herts Health Economy Infection Control Group. 6.2 Hepatitis C Cross infection of hepatitis C infection to one patient was identified at an outpatient unit. The Provider Trust led the incident control group with input from PHE and the CCG. Learning identified through the investigation of the case has been shared across the Trust and across the health economy via the Herts Health Economy Infection Control Group. 6.3 Congenital Rubella PHE set up a multiagency incident control group to investigate a case of congenital rubella. Learning from the case related to immunisation services, obstetric services, primary care services and laboratory services is being shared across the health economy.

21
6.4 MRSA outbreaks During 2014/15, two wards at ENHT and one ward at HCT were affected by outbreaks of MRSA. The cross infection identified in all 3 outbreaks involved new colonisation for patients but did not result in any clinical infections. For these outbreaks, an outbreak control group was formed by the Trust to plan and monitor the delivery of actions to control the outbreak and ensure learning achieved during the outbreak to reduce the risk of infections were implemented across the Trusts. 7. Supporting providers to deliver best practice standards ENH CCG works closely with key health providers to support the provision of the highest standards of infection control for patients. ENH CCG Quality Team has completed a program of assurance visits which included ENHT, HCT. Areas of infection control assessed during these visits have been aligned to key priorities in the annual infection control program. ENH CCG completed an infection prevention and control assurance visit to 12 Wards at The Lister Hospital, ENHT on 30th March 2015. The visit identified good infection control practice with standards of cleaning being very good in some areas and when all patients were asked, stated that staff decontaminated their hands before and after providing care. However, the visit identified the need for improvement and the Trust is being supported to improve standards of infection control in the following areas:
• Standard of cleaning for the clinical environment and patient equipment • The management of IV devices and urinary catheters
ENH CCG Head of Infection Control attends provider Infection Control Committee Meetings and infection control incident meetings. Providers are monitored by ENH CCG on the delivery of their annual infection control improvement plans. 8. Priorities for 2015/16 The infection prevention and control priorities for ENH CCG for 2015/16 include: • Further developing partnership working across the health economy, which is crucial to the continued
improvement of infection control practice. By way of continued support for the work of the Herts Health Economy Infection Control Group and work actively with providers to facilitate developments to improve standards of infection prevention and control.
• The continued close monitoring of the incidence of infections and infection control incidents and awareness of new emerging infections, in order to be able to effectively respond to current and new infection prevention and control challenges.
• The provision of continued leadership to promote excellence in infection prevention and control and to challenge any identified lapses in standards of care.
• The delivery of the NHS England annual target of 112 C. difficile cases for ENH CCG for 2015/16. Following the 6% increase in non-acute cases in 2014/15, focus must be kept on the reduction in non-acute cases and further develop participation in joint case review meetings and support providers to deliver their annual limits through the provision of the highest standards of infection prevention and control.
• The continuation of the work of the ENH CCG Medicines Management Team in promoting compliance to antibiotic prescribing guidelines and supporting the delivery of the NHS England antibiotic quality premium.
• Working towards delivery of NHS England’s target of reducing MRSA bacteraemia cases to achieve zero avoidable cases. Following the increase in MRSA bacteraemia cases in 2014/15, action is needed in the following key areas:

22
o Improving the management of intravenous devices o Reducing risks of contamination of samples when blood cultures are taken o Improving the risks associated with urinary tract infections and urinary catheters o Improving the management of the screening and treatment of patients with MRSA
• Supporting providers to ensure that excellent standards of infection prevention and control are in place and the requirements of CQC are met, through quality review meetings and quality assurance visits.
9. Summary ENH CCG’s Annual Infection Prevention and Control Report for 2014/2015 provides information on the delivery of the infection prevention and control activity for ENH CCG. The aim of the report is to provide assurance that patients receiving care from services commissioned by ENH CCG are protected from the risks of HCAI and cared for by staff providing the highest standards of infection prevention and control. ENH CCG is committed to reducing the risk of infections through the provision of the highest standards of infection prevention and control practice. Patient welfare and safety is a high priority, as is reducing the risk of infection to a minimum. ENH CCG has robust governance structures in place for the management of healthcare associated infections within the Hertfordshire health economy. Significant achievements have been delivered which include a 6% reduction in cases of C. difficile associated with acute providers and a 14% reduction in primary care prescribing levels for the antibiotics targeted with associated high risk for C. difficile infection. ENHT, WHHT, HCT have been supported to successfully deliver their annual limits for C. difficile. Through the successful development of partnership working, practice developments have been delivered to support the continued improvements in the standards of infection prevention and control across the Health Economy. Key priories for delivery in 2015/16 have been identified to facilitate the reduction in cases of C. difficile and MRSA bacteraemia and support the on-going improvements to standards of infection prevention and control. The success of the continued drive to reduce the cases of infection and provide the highest standards of infection prevention and control practice for the population of Hertfordshire is dependent on the continued commitment of key partners across the Hertfordshire Health Economy. The sustained effort of providers across Hertfordshire, which has resulted in significant reductions in the incidence of HCAI, is acknowledged. There has been considerable progress by ENH CCG in the provision of infection prevention and control which has been achieved by working very closely with provider organisation and through the delivery of initiatives to improve the quality and safety of healthcare in Hertfordshire. By strengthening the current systems and implementing new evidence based initiatives, ENH CCG is committed to reducing the risk of infection to a minimum for patients, staff and the population of Hertfordshire.

23
10. Key documents The Health and Social Care Act (2008): Code of Practice for the NHS on the prevention and control of healthcare associated infections and related guidance. Department of Health. January 2011. EPIC 3: National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England. December 2013. Clostridium difficile infection objectives for NHS organisations in 2014/15 and guidance on sanction implementation. NHS England, March 2014. Acute trust toolkit for the early detection, management and control of Carbapenemase-producing Enterobacteriaceae. PHE, December 2013. 11. Abbreviations used in this report Abbreviation C. difficile Clostridium difficile CDI Clostridium difficile CPE Carbapenemase-producing Enterobacteriaceae CQC Care Quality Commission DH Department of Health E. coli Escherichia coli ENH CCG NHS East and North Hertfordshire Clinical Commissioning Group ENHT NHS East and North Hertfordshire NHS Trust GP General Practitioner HCAI Health Care Associated Infections HCC Hertfordshire County Council HCT Hertfordshire Community NHS Trust HHEICG Hertfordshire Health Economy Infection Control Group HSM Hertfordshire and South Midlands HUC Herts Urgent Care HV CCG NHS Herts Valleys Clinical Commissioning Group IV Intravenous LMC The Local Medical Committee MRSA Meticillin Resistant Staphylococcus Aureus MSSA Meticillin Sensitive Staphylococcus Aureus PHE Public Health England PHEC Public Health England Centre SMH South Midlands and Hertfordshire Area TB Tuberculosis WHHT West Hertfordshire Hospitals NHS Trust

Appendix 1
East and North Hertfordshire and Herts Valleys Clinical Commissioning Groups’
Health Care Associated Infection (HCAI) Reduction Plan 2014/2015 Version 6. Updated on: 17/04/15 East and North Hertfordshire (ENCCG) and Herts Valleys (HVCCG) Clinical Commissioning Groups are committed to ensuring that the population of Hertfordshire are protected from the risks of healthcare associated infections and that healthcare services maintain best practice standards for infection prevention and control. The Hertfordshire Health Economy Infection Control Group provides a countywide forum to drive forward improvements in the standards of infection control and deliver actions to reduce the number of patients affected by healthcare associated infections. The Department of Health (DH) sets annual limits for the maximum number of cases of C. difficile for CCGs and Acute Trusts and a zero limit for MRSA bacteraemia cases for all organisations. This plan provides an overview of the actions that will be taken to manage the risks of infection within healthcare services and deliver the reduction in cases required to meet the DH limits for cases. Governance processes Objectives Action required Time
frame Date completed
Progress, issues raised and lessons learned.
Commissioning structures are in place which provide assurance that services providing treatment and care for the population of Hertfordshire meet the requirements of the Health and Social Care Act 2008 and effectively manage risks of infection for their patients/clients, employees and visitors.
HVCCG Director of Nursing and Quality to Chair bi monthly meetings of the Hertfordshire Health Economy Infection Control Group with attendance from key individuals across services in Hertfordshire. Meetings are to facilitate improvements to the standards of infection control in healthcare services for the population of Hertfordshire.
31/03/15 31/03/15 Bi monthly meetings being held. Minutes being sent to ENHCCG Quality Committee and HVCCG Quality and Performance meetings.
There is a strategy in place which details the processes of ENHCCG and HVCCG have in place to effectively manage the risk if HCAI in health care services for the population of Hertfordshire.
31/08/14 4/12/14 HVCCG – Quality Strategy incorporates infection control strategy. ENHCCG Infection Control Strategy draft written. Approved at ENHCCG Quality Committee on 4/12/14.
There is annual plan (The ENCCG and HVCCG Clinical Commissioning Groups’ HCAI Reduction Plan) in place to implement strategic actions for the management of risks associated with HCAI and the facilitation of best practice standards for infection prevention and control.
31/07/14 26/06/14 Completed. Plan updated on a regular basis through the year
Risks related to infection control to be recorded and effectively managed.
Significant infection control risks to be included in relevant CCG risk register and progress on the management of the risks to be recorded on the registers. Significant risks to be escalated as appropriate.
31/03/15 31/03/15 27/11/14 ENHCCG & HVCCG risk registers have been updated in relation to infection control risks. 31/03/15 risk registers updated regularly

2
Developing excellence in infection prevention and control practice and Leadership of the Health Economy Objectives Action required Time
frame Date completed
Progress, issues raised and lessons learned.
Developments in infection prevention and control practice are developed and implemented across the county through the bimonthly meetings of the Hertfordshire Health Economy Infection Control Group (HHEICG) which is chaired by the Director of Nursing and Quality for HVCCG.
Terms of reference of the group to be reviewed including the membership of the group to ensure that key partners are represented.
30/11/14 18/11/14 Terms of reference reviewed at HHE ICG meeting on 18/11/14 and approved with the addition to the membership of Directors of Nursing and Deputy Director of Nursing for provider organisations.
Agendas for the meeting to address local and national concerns, new and emerging risks and include actions to improve standards of practice across providers.
31/03/15 31/03/15 Agenda set to broaden the scope of the meeting with guest speakers attending to present specialist areas.
Data reports to be provided to the committee to highlight improvements achieved and areas of concern.
31/03/15 31/03/15 Annual report for 2013/14 provided. Other data provided by CCG and PHE.
Whole health economy action plans to be developed to drive required changes in practice to reduce risk and improve practice and delivered through the HHEICG
31/03/15 31/03/15 C. diff and MRSA action plans in place and improvements to practice implemented.
Examples of best practice to be shared between providers to facilitate the delivery of the highest standards of infection control across Hertfordshire.
31/03/15 31/03/14 Best practice developments shared include: • Hand out for carers inpatients own
homes – best practice for the on-going management of urinary catheters.
• Staff information booklet covering information and best practice for the management C. difficile infections.
• A competency tool for the assessment of staff who undertake the taking of blood culture specimens.
• An infection control staff work book to support best practice in infection control.
Standard setting and contracting Objectives Action required Time
frame Date completed Progress, issues raised and lessons
learned. All contracts with providers incorporate essential components to
Review on-going contracts and quality schedules to ensure content covers essential requirements for infection prevention and control.
31/02/15 31/03/15 Input to Quality schedules provided
Review contracts for new services to ensure essential requirements 31/03/15 31/03/15 Advice on services provided

3
ensure: • Patients are cared for
in a clean environment and are protected from the risks of infection.
• Services are compliant with the Health and Social Care Act 2008
• Services have current registration with the CQC
included.
Review national guidelines on commissioning frameworks to ensure recommendations are included in local commissioning processes
Commissioning leads to ensure CCG Head of Infection Prevention and Control is informed of /is aware of relevant national commissioning guidance.
31/03/15 31/03/15 Documents shared including C. diff annual limits.
CCG Head of Infection Prevention and Control to identify national infection control guidance for inclusion in contracts
31/03/15 31/03/15 Actions include MRSA screening targets in light of 2014 DH guidance.
CCG Head of Infection Prevention and Control to incorporate recommendations in advice given to commissioners for the content of contracts.
31/03/15 31/03/15 MRSA screening . C. diff annual limit for HCT negotiated locally in line with national guidance.
Performance management of providers
Objectives Action required Time frame
Date completed
Progress, issues raised and lessons learned.
Provision of assurance to South Midlands and Hertfordshire NHS England Area Team that measures are in place
Provision of HCAI update for quarterly checkpoint meetings between CCG and SMH Area Team and additional updates as needed.
31/03/15 31/03/15 Reports and comment provided.
Attendance by CCG Head of Infection Prevention and Control at SMH Area Team meetings as required.
31/03/15 31/03/15 Meetings attended and Hertfordshire initiatives shared. CCG presented thematic review of learning from AMH area C. diff case reviews to Area Team meeting .
Provision of assurance to CCG Governing body that measures are in place.
Provision of quarterly update for Quality Reports to ENCCG & HVCCG Quality and Safety committees.
31/03/15 31/03/15 Reports provided as requested for committees
Gaining of assurance from providers that measures are
Monitoring of monthly PHE data capture figures for HCAI 31/03/15 31/03/15 Data monitored and action taken when expected number of cases Monitoring of PHE HCAI data reports
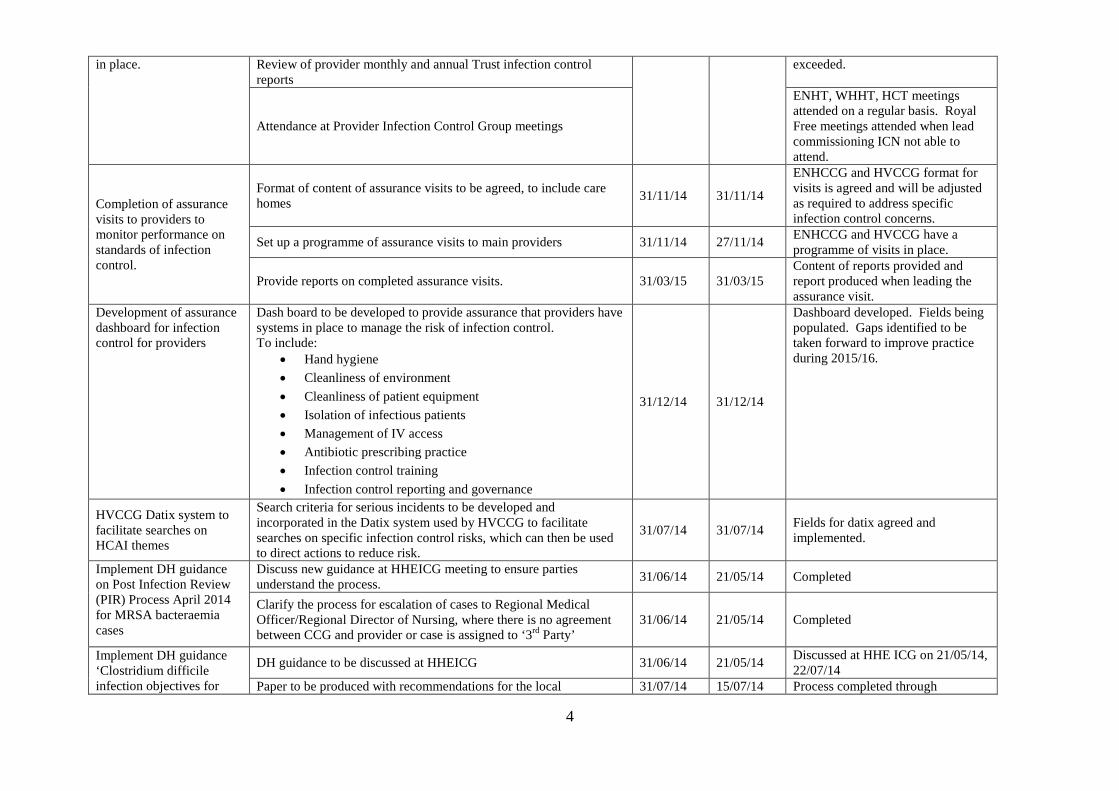
4
in place. Review of provider monthly and annual Trust infection control reports
exceeded.
Attendance at Provider Infection Control Group meetings
ENHT, WHHT, HCT meetings attended on a regular basis. Royal Free meetings attended when lead commissioning ICN not able to attend.
Completion of assurance visits to providers to monitor performance on standards of infection control.
Format of content of assurance visits to be agreed, to include care homes 31/11/14 31/11/14
ENHCCG and HVCCG format for visits is agreed and will be adjusted as required to address specific infection control concerns.
Set up a programme of assurance visits to main providers 31/11/14 27/11/14 ENHCCG and HVCCG have a programme of visits in place.
Provide reports on completed assurance visits. 31/03/15 31/03/15 Content of reports provided and report produced when leading the assurance visit.
Development of assurance dashboard for infection control for providers
Dash board to be developed to provide assurance that providers have systems in place to manage the risk of infection control. To include:
• Hand hygiene • Cleanliness of environment • Cleanliness of patient equipment • Isolation of infectious patients • Management of IV access • Antibiotic prescribing practice • Infection control training • Infection control reporting and governance
31/12/14 31/12/14
Dashboard developed. Fields being populated. Gaps identified to be taken forward to improve practice during 2015/16.
HVCCG Datix system to facilitate searches on HCAI themes
Search criteria for serious incidents to be developed and incorporated in the Datix system used by HVCCG to facilitate searches on specific infection control risks, which can then be used to direct actions to reduce risk.
31/07/14 31/07/14 Fields for datix agreed and implemented.
Implement DH guidance on Post Infection Review (PIR) Process April 2014 for MRSA bacteraemia cases
Discuss new guidance at HHEICG meeting to ensure parties understand the process. 31/06/14 21/05/14 Completed
Clarify the process for escalation of cases to Regional Medical Officer/Regional Director of Nursing, where there is no agreement between CCG and provider or case is assigned to ‘3rd Party’
31/06/14 21/05/14 Completed
Implement DH guidance ‘Clostridium difficile infection objectives for
DH guidance to be discussed at HHEICG 31/06/14 21/05/14 Discussed at HHE ICG on 21/05/14, 22/07/14
Paper to be produced with recommendations for the local 31/07/14 15/07/14 Process completed through

5
NHS organisations in 2014/15 and guidance on sanction implementation’
implementation of the guidance. Paper to be presented at HHE ICG to gain provider input into the process.
negotiation by DoN for CCGs and input from HHEICG meetings.
Local implementation of process to be via HHEICG. 31/07/14 28/08/14
CCGs have incorporated provider feedback on process, amendments made delayed completion of process but ensured providers inputted into final document.
Delivering reductions in HCAI and achieving best practice standards for infection prevention and control. Objectives Action required Time
frame Date completed
Progress, issues raised and lessons learned.
CCG websites to host information on HCAI and guidance on best practice for infection control.
Infection control content for CCG websites to be developed to provide information on HCAIs and guidance on infection control best practice standards
31/12/14 31/03/15 Documents and links provided to websites. Work to be further developed in 2015/16
Definition of C. difficile outbreak to be agreed
Definition of an outbreak of C. difficile to be agreed through the C. difficile Task and Finish Group.
31/06/14 24/06/14 Completed
Zero tolerance for MRSA bacteraemias to achieve reduction in cases.
Post infection reviews to be held for all cases in line with DH guidance and learning shared at HHEICG. CCG Head of Infection Prevention and Control to complete PIRs for non-acute cases and participate with providers for acute cases.
31/03/15 31/03/15 Completed
Common themes identified through post infection case reviews to be summarised through the year and used to identify priorities for actions to reduce cases.
31/03/15 31/03/15 Completed
Country wide MRSA reduction plan to be developed to deliver reduction in cases
31/07/14 22/07/14 Action plan developed.
Country wide MRSA reduction plan to be implemented to deliver reduction in cases
31/03/15 31/03/15 Action plan delivered.
Incidence of C. difficile infections to be reduced to deliver DH limits for maximum number of cases for CCGs and Trusts.
Countywide C. difficile reduction plan to be developed 31/07/14 01/07/14 Action plan developed. Countywide C. difficile reduction plan to be implemented.
31/03/15 All actions due by 31/03/15. Actions for 15/16 to be incorporated into new action plan for 15/16.
Learning from RCA case reviews to be shared across the health economy and used to identify priorities for actions to reduce cases. These actions are to be incorporated in the countywide C. difficile action plan.
31/03/15 31/03/15 Completed

6
Response to outbreaks and infection control incidents Objectives Action required Time
frame Date completed
Progress, issues raised and lessons learned.
Infection Control incidents and outbreaks of infection are identified, actions to manage outbreaks put in place. Lessons learned are shared across the health economy.
Increase in incidence of infection or occurrence of infection control incidents to be identified through surveillance and close partnership working across organisations.
31/03/15 31/03/15 Completed
CCG Head of Infection Prevention and Control to work with organisations and PHE in the response to infection control incidents and ensure that relevant individuals are kept informed of progress.
31/03/15 31/03/15 Completed Incidents included: Hep C, C. diff, rubella, TB.
Lessons learned are to be shared across the health economy via the HHEICG meetings
31/03/15 31/03/15 Lessons learned fed back via HHE ICG
Ensure providers are aware of the need for timely information on infection control incidents to be communicated to CCGs
Email to be sent to ENHT, WHHT, HCT & HPFT to clarify arrangements for early notification of CCG of infection control issues.
31/07/14 31/07/14 Completed
Access to infection control specialist advice Objectives Action required Time
frame Date completed
Progress, issues raised and lessons learned.
Ensure on-going access to infection control specialist advice
Head of infection prevention and control employed by HVCCG works across ENCCG and HVCCGs as agreed through memorandum of understanding. Memorandum of understanding established March 2014 to last until 31/3/16. To be reviewed in June 2014 and then quarterly to ensure it continues to meet the needs of the individual parties.
Quarterly to 31/03/15
22/08/14 Review complete and decision made that reviews will be annual going forward.
Head of Infection Prevention and Control to ensure on-going updating of specialist knowledge through: • Attendance at Infection Prevention Specialist meetings and
conferences • Present work and share learning to other specialists and
professionals. • Attendance at non infection control training to develop
professional and leadership skills. • Maintain on-going membership of Infection Prevention Society
31/03/15 31/03/15 23/09/14 CCG presented on C. difficile cases to HHC Safer Care study day for care home staff. 25/11/14 CCG presented thematic review of learning from C. diff RCAs collated across H&SMs Area at H&SM Area HCAI Quality Collaborative Workshop.

7
Abbreviations CCG- Clinical Commissioning Group ENHCCG – East and North Hertfordshire Clinical Commissioning Group HCAI- Healthcare Associated Infection HCC- Hertfordshire County Council HHEICG- Hertfordshire Health Economy Infection Control Group HVCCG- Hertfordshire Valleys Clinical Commissioning Group PHE- Public Health England PIR- Post infection review RCA- Root cause analysis SMH – South Midlands and Hertfordshire

1
Agenda Item No: 8
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Finance Report Month 4 2015/16
Decision Discussion Information Follow up from last meeting
Report author: Noreen Coles, Deputy Chief Finance Officer
Report signed off by: Alan Pond, Chief Finance Officer
Purpose of the paper: This paper provides details of the finance position at the end of
July.
Conflicts of Interest involved:
n/a
Recommendations to the Governing Body
To note the Month 4 position.
2
Finance Report 2015/16 CCG Governing Body Public Meeting 24th September 2015
1 PURPOSE OF THE PAPER
To provide the financial position of the CCG at the end of July 2015.
2 APPENDICES
Appendix 1 –Acute Commissioning
3 TERMS/ACRONYMS USED IN THE REPORT Initials In full B&CF Barnet and Chase Farm Hospital Trust BEH Barnet, Enfield and Haringey BSA Business Services Authority CCG Clinical Commissioning Group CHC Continuing Healthcare CUFT Cambridge University Foundation Trust FNC Funded Nursing Care HCT Hertfordshire Community Trust HPFT Hertfordshire Partnership Foundation Trust FYE Full Year Effect RAID Rapid Assessment, Interface and Discharge RTT Referral to treatment UCC Urgent Care Centre UCLH University College London Hospitals PAH Princess Alexandra Hospital YTD Year to date

3
4 LATEST SUMMARY POSITION
Overall Position G 69 G 0
Recurrent Position G 69 G 0
Acute contracts R (1,008) R (2,764)Based on month 4 reports
GP Prescribed Drugs R (330) R (1,003)
Non acute commissioning and Primary Care G 411 G 103
Transformation reserve and investments G 0 G 0
Running Costs G 435 G 900
% Utilised % UtilisedContingency G 16.68% G 82.31%
£ committed £ committedG 560 G 2,764
Value
Better Payments Practice Code (BPPC) NHS 88.3% 96.1%(Target is 95% of invoices by value and number are paid within 30 days) Non-NHS 97.0% 98.6%
Invoices
FORECASTYTD£'000
VARIANCE AGAINST PLANJULY 2015

4
5 EXPENDITURE REPORT
5.1.1 CCG Allocation and Budgets The CCG’s allocation is summarised in the table below. Since last month it has increased by £298k which is related to an allocation for eating disorders. The £488k (9 months funding) in respect of the walk-in service at Spring House, which was “expected” last month has now been received.
5.1.2 CCG Overall Position
The planned position is an underspend of £7,743k at year end. The year to date position shows a small underspend of £19k against plan. The table below shows further detail of the financial position by broad budget heading. A forecast year end position is reported this month.
Month 3 In month Month 4£'000 £'000 £'000
Allocation 672,681 672,681New allocations:
NHSE Brokerage Return 1,500 1,500Luton & Beds CCGs Brokerage Return 6,000 6,000Vanguard Care Homes 150 150GP IT 1,495 1,495IAPT allocation 21 21B&CF acquisition costs (700) (700)Transfer from NHSE re Spring House walk-ins 488 488Eating disorders allocation 298 298
Total notified allocation 681,635 298 681,933

5
There has been an increase in the overspend year to date on continuing healthcare and prescribing. The forecast position expects this trend to continue. To achieve breakeven and assuming all investment funds are spent in the year requires utilisation of £2,764k of the contingency reserve, (82%) leaving £594k. In terms of year to date the finance report brings in half of the year to date proportion. Therefore, although the financial position is becoming tighter it is still relatively healthy compared to others and remains a low risk of not achieving the agreed underspend. The running costs allocation is £12,634k, i.e. £300k higher than the running costs budget shown above, because £300k has been transferred to programme budgets. 5.2 Locality Positions 5.2.1 Locality year to date position Due to the timing of the Governing Body meeting, the position by locality is not available. This will be reported at the next Governing Body workshop at the beginning of October.
DescriptionAnnual budget £'000
YTD budget £'000
YTD Actual £'000
YTD Variance
£'000
FOT £'000
FOT Variance
£'000
Allocation 681,933 681,933
Budget HeadingAcute Commissioning 373,275 124,238 125,246 (1,008) 376,039 (2,764)Non Acute Commissioning 168,283 57,870 57,818 52 169,120 (836)GP Prescribed Drugs 76,901 25,208 25,538 (330) 77,904 (1,003)Other Primary Care 18,652 6,199 5,840 359 17,713 939Running Costs 12,334 4,111 3,676 435 11,434 900Transformation reserve 9,839 632 632 9,839Recurrent investment fund 3,909 3,909Resilience funding 4,259 528 528 4,259MH investment fund 3,380 3,380Contingency reserve 3,358 560 560 594 2,764
Total 674,190 219,346 219,277 69 674,190 0
TOTAL UNDER/(OVER) SPEND 7,743 7,743
POSITION AS AT 31st JULY 2015

6
5.3 Commissioning – Acute 5.3.1 Financial Performance
• East and North Herts Trust At Month 4, East and North Herts Trust (ENHT) is showing an over performance of £168k against plan. This includes the application of penalties totalling just under £365k and the agreement of additional investment (worth £3,538k) towards additional elective and outpatient activity to reduce patients waiting over 18 weeks. When taking the additional funding agreed in contract variations into account, elective activity (including day cases) is showing an over performance of £204k. Outpatients is showing an under performance of £429k. This is due to ENHT converting outpatient capacity to support admitted pathways due to staffing challenges, and a slow mobilisation of the additional activity agreed as part of the additional RTT investment. A&E is showing an under performance of £242k against financial plan at Month 4. However, there has been an increase in A&E activity in Month 4. This is due to the additional Spring House unregistered patients flowing through the Urgent Care Centre (UCC) at QEII as of 1 July 2015. It should be noted that whilst number of attendances have increased in Month 4, the average cost has reduced from £125 in April 2015 to £92 in July 2015, which may be reflective of the different case mix represented in the Spring House flows. Work is being undertaken to define a local tariff for the UCC in order to ensure that the price adequately reflects the different patient flows being seen within the unit. As previously reported, the non-elective activity includes activity undertaken in the Clinical Decision Unit (CDU). There are ongoing discussions around the pathways and tariffs related to the CDU, and there is now agreement to undertake a clinical audit of patients seen in the unit to support this piece of work.
DescriptionAnnual budget £'000
YTD budget £'000
YTD Actual £'000
YTD Variance
£'000
FOT £'000
FOT Variance
£'000
East and North Herts Trust (incl MVCC) 196,564 65,334 65,502 (168) 196,979 (415)Princess Alexandra Hospital 54,503 18,168 19,083 (916) 57,250 (2,747)Royal Free FT 23,197 7,732 8,370 (638) 24,689 (1,492)Independent Sector 22,464 7,488 7,506 (18) 22,518 (54)Cambridge University Hospitals 10,982 3,661 3,661 (0) 10,982 0Other Acute 64,188 21,396 21,123 273 63,622 566Reserve for potential contract shortfalls 1,377 459 0 459 1,377
TOTAL 373,275 124,238 125,246 (1,008) 376,039 (2,764)
COMMISSIONING - ACUTE POSITION AS AT 31st JULY 2015

7
High Cost Drug spend is significantly over performing at just under £636k. ENHT are yet to submit supporting information for Month 3 and Month 4 and so validation has not yet been undertaken. However, analysis will be undertaken to understand this variation and to also identify any changes in guidance or drug costs that may underpin this. Critical Care and Direct Access to Radiology are also showing over performance against plan. Direct Access to Radiology is showing a 9.5% over performance in activity (equal to £174k). Work is being undertaken to understand if there has been any corresponding changes in unbundled diagnostics and outpatient activity and whether the increased activity is due to better use of the pathway. Further work is required to understand performance within critical care, which is subject to monthly fluctuations.
• Princess Alexandra Hospital (PAH) At Month 4, PAH is showing an over performance of £916k against straight-line plan. This figure is not adjusted for penalties - these will be calculated once PAH resumes national reporting (October for September reports). The main driver for the over performance is maternity antenatal pathways - £629k over plan. The CCG is disputing the quality of the maternity data as the high numbers reported suggest PAH is claiming lead provider status for all women delivering at PAH. Historically, ENHT have claimed lead provider status for most women delivering at PAH because the ENHT Community Midwifery team see most Hertfordshire patients, regardless of where they deliver. Work is on-going to review the data and establish the true level of antenatal activity being provided by PAH. Although the position may be overstated, it is likely that the Trust may have been under-recording antenatal pathways. Once an accurate position is established, a formal contract variation will be agreed with the Trust with funding being moved from the acute reserve to fund this. High Cost Drugs (HCD) is over plan by £153k, however £130k has been disputed via the validation process. Of this, £36k relates to drugs invoiced to the CCG in error, £92k relates to treatments for which the appropriate notifications have not been received (largely wet age-related macular deterioration). Critical care is over plan by £203k (157 bed days). Work is underway to review the long stay activity with GPs to confirm that the episodes have been coded appropriately. Outpatient attendances are also over plan by £138k (c.6%), with significant over-performance in gynaecology, cardiology and ophthalmology. Elective (including day cases) is under plan by £106k, this is being driven by a large under spend (£142k) in day case activity. In non-elective there is an overspend in same day activity of £205k, although this is offset by a large underspend across all other non-elective areas bringing the overall non-elective position to an under performance of £203k.

8
• Royal Free Foundation Trust
At Month 4 there is an overspend of £638k at the Royal Free Trust, of which £567k is at the Barnet and Chase Farm Hospitals site. The main area of over performance at Barnet and Chase Farm continues to be critical care which has an over performance of £303k as a result of actual bed days being 221 higher than the plan (151%). As previously reported a patient discharged in May had a spell of 125 days in critical care costing £208k and in July there were two patients that had spells of 28 and 29 days. There is also an overspend in non-elective (NEL) activity of £212k; activity is 12% higher than the plan. The Trust reported an increase in the number of ambulances arriving at A&E in July. Although outpatients continues to underspend (£68k), in activity terms 6% under for first attendances and 14% for follow-ups, this is a reduction on last month. The Royal Free over performance relates to day cases, which is £138k above plan and results from an increase in cardiology stents. Critical care is underspent by £61k. Further detail by Trust is given in Appendix 1. 5.3.2 Activity The following charts show activity from April 2013 to July 2015.

9
Elective activity is slightly higher in the current month, and this holds true for most of the Localities. Welwyn Hatfield along with Stevenage are showing much higher levels than in previous years.
A&E activity has seen a considerable increase in month 4 which is applicable to all localities. The most significant activity increases has been seen in Lower Lea Valley, closely followed by Upper Lea Valley and Welwyn Hatfield. There are still data issues Cheshunt MIU and Herts & Essex Hospital, so no comparisons are possible with previous years.

10
5.4 Commissioning – Non Acute
Emergency Rate Per 1000 Weighted Population Table
Lower Lea Valley 74.0 1Stort Valley & Villages 78.4 2Upper Lea Valley 80.8 3Welwyn Hatfield Locality 93.6 5North Herts 92.8 4Stevenage 102.0 6
CCG Total 88.1
Weighted Rate Per 1000 Population
Rank 1 = Lowest
DescriptionAnnual budget £'000
YTD budget £'000
YTD Actual £'000
YTD Variance
£'000
FOT £'000
FOT Variance
£'000
MH/LD Contracts and NCAs 68,142 22,713 22,536 177 67,608 534IAPT 5,106 1,702 1,725 (23) 5,174 (68)Hertfordshire Community Trust 38,595 12,865 12,865 0 38,595 0Community Services excl HCT 5,001 1,667 1,578 89 4,836 165Continuing Healthcare & FNC 26,228 10,519 11,199 (680) 28,270 (2,041)Intermediate Care 2,520 840 812 28 2,569 (49)Better Care Fund 14,063 4,688 4,688 0 14,063 0Hospices 3,395 1,132 1,106 26 3,348 47NHS Property Services Ltd 1,886 629 629 0 1,886 0
Other Non Acute 3,347 1,115 680 435 2,770 577
TOTAL 168,283 57,870 57,818 52 169,120 (836)
COMMISSIONING - NON ACUTE POSITION AS AT 31st JULY 2015

11
The underspend on mental health is largely related to learning disabilities and adult mental health, based on the month 4 report and NCAs. There has been a significant deterioration in the position reported against continuing healthcare (CHC) and funded nursing care (FNC). The overspend of £680k is made up of £1,115k overspend on CHC and £535k underspend on FNC. Further analysis has been undertaken to compare spend with last year to identify the greatest areas of increase. This compares spend derived from the CHC database across the years. The 2014/15 figures shown are therefore actual for this CCG, rather than a capitation share of the estimated Hertfordshire total (which is how spend was included in the CCG 2014/15 outturn). The most significant % movement is in home care. Further work is being undertaken to understand the position and whether the year to date figure is likely to continue at the same rate.
In addition to the financial analysis carried out assurance work has been completed in relation to the integrity of the data on the “QA” database. Patients with a package of care costing more than £2,000 per week have also been reviewed. Further work is being undertaken to
• Review all high cost care packages (above £1k per week) • Review all high cost placements (above £900 per week) • Ensure continued adherence to CHC funding policy
• Set out options for reducing spend in the latter half of the year
The underspend on “Other non acute” includes a benefit of c£500k related to write back of accruals related to 2014/15, the most significant of these is the charge from NHS Property Services which has now been agreed at an amount lower than estimated.

12
5.5 Commissioning – Primary Care
The prescribing figures are based on the April to June figures issued by the Business Services Authority, which show a forecast overspend of approx. £1m. This is based on the latest national profile of spend across the year. Key areas of growth have been in cardiovascular disease (increased use of newer anticoagulants), endocrine therapy (in particular new oral hypoglycaemic agents for diabetes), and in nutrition (more patients in the community with PEG feeds) There have also been notable increases in the cost of dressings and incontinence appliances. This may be related to more patients in intermediate care settings. GP practices have been set five prescribing KPIs this year, three of which are cost related. If implemented widely these could provide significant savings. However, there is a risk that these savings will not materialise. An underspend is shown against the £5 per head budget. It is unlikely that the full year budget will be spent by year end as the health check programme is being completed this year and new primary care service development will be rolled into a bigger programme in 2016/17.
DescriptionAnnual budget £'000
YTD budget £'000
YTD Actual £'000
YTD Variance
£'000
FOT £'000
FOT Variance
£'000
GP Prescribed Drugs 76,901 25,208 25,538 (330) 77,904 (1,003)Central Drugs 2,159 702 698 4 2,159 0Oxygen 754 251 248 3 754 0Scriptswitch 245 82 82 0 245 0Local Enhanced Services 4,363 1,454 1,453 1 4,464 (101)Primary Care IT 1,495 498 498 0 1,495 0Out of Hours 4,545 1,515 1,515 0 4,545 0£5 and £1 per head 3,524 1,175 836 339 2,484 1,040Acute in hours visiting service 1,567 522 510 13 1,567 0
TOTAL 95,553 31,407 31,377 30 95,617 (64)
COMMISSIONING - PRIMARY CARE POSITION AS AT 31st JULY 2015

13
5.6 Transformation Reserve The table below shows the list of schemes which, at Month 4, are currently assumed to be funded from the non-recurrent transformation reserve.
Alan Pond Chief Financial Officer September 2015
Schemes funded from Transformation Funds AllocationIncluded in
Budgets Total £'000 £'000 £'000
Funds available1.5% of recurrent baseline 9,768 9,768 Brokerage return CCGs 6,000 6,000 Brokerage return NHSE 1,500 1,500 Continuing Healthcare national top-slice (2,664) 2,664 - Royal Free acquisition costs (700) 700 - Homefirst N Herts April - June (526) 526 - ENHT reduced waiting times (3,538) 3,538 - Total 9,840 7,428 17,268
Commitments: Map of medicine 80Isabel Hospice (Homefirst pilot) 80Leg ulcer project Upper Lea Valley 109CHC Retrospective team 300Integrated geriatric response vehicles 752Interface geriatricians ENHT 200Pharmacist-led care home medicines optimisation 294Get Healthy Get Active funding 50CARS service PAH 30
Total spend committed 1,895 - -
Balance of funding available 7,946 -

14
APPENDIX 1
EAST & NORTH HERTS CCGACUTE REPORT 2015-16 MONTH 4
DescriptionAnnual budget £'000
YTD budget £'000 Actual £'000 Variance
£'000
ContractsLocal TrustsEast & North Herts 196,564 65,334 65,502 (168)Princess Alexandra 54,503 18,168 19,083 (916)Royal Free 23,197 7,732 8,370 (638)Independent Sector 22,464 7,488 7,506 (18)Cambridge University Hospitals 10,982 3,661 3,661 (0)West Herts Hospitals 2,705 902 869 33Luton & Dunstable 1,190 397 354 42Other TrustsUCLH 7,183 2,394 2,397 (2)North Middlesex 6,360 2,120 2,394 (274)Moorfields 3,949 1,316 1,247 69Royal National Orthopaedic 3,103 1,034 1,075 (41)Barts Health 2,294 765 886 (122)Royal Brompton & Harefield 1,809 603 486 117Papworth 1,361 454 378 75Mid Essex 1,300 433 504 (71)Guys & St Thomas 1,077 359 450 (91)Imperial College 1,062 354 301 53North West London 928 309 229 81Great Ormond Street 856 285 291 (6)Basildon & Thurrock 1,033 344 219 125Chelsea and Westminster 323 108 101 7Kings 289 96 147 (51)Bedford 336 112 81 31Whittington 291 97 57 40The Royal Marsden 222 74 63 11East of England Ambulance & PTS 19,391 6,464 6,283 180Other AcuteNon Contract Activity (NCAs) 4,991 1,664 1,674 (11)IVF 1,131 377 338 39Cheshunt MIU & ENHT UCC 757 252 291 (39)Services Outside Contracts 82 27 35 (8)IFRs 165 55 55 (0)Reserves 1,377 459 459Prior year balance (84) 84
TOTAL 373,275 124,238 125,246 (1,008)

Agenda Item No: 9
Date of Meeting: 24 September 2015
Governing Body Meeting in Public
Paper Title: Integrated Performance and Quality Report
Decision Discussion Information Follow up from last meeting
Report author: Gerry Moir Assistant Director Performance
Cath Slater Associate Director Quality and Patient Experience
Report signed off by: Sharn Elton, Director of Operations Sheilagh Reavey, Director of Nursing and Quality
Purpose of the paper: To update the Board
Conflicts of Interest involved:
None
Recommendations to the Governing Body
The Governing Body is asked to note the current performance and actions described in the paper
1

Integrated Performance and Quality Report
September 2015

Contents ׀
Description Page Number
Introduction 3
NHS Constitution - CCG Level 6
Provider Profiles 17
ENHT 18
PAH 32
BCF 43
HCT 47
EEAST 57
HPFT 64
HUC 71
Glossary 76
2

Introduction ׀ This Integrated Performance and Quality report provides an update on the performance and quality of local NHS Trusts in relation to key national performance standards. It includes quality and performance information at CCG level and also at provider level. The performance and quality metrics included within the report are published information predominantly for the June position, and includes information for Q1 where available. All metrics have been included with commentary for exceptions where performance standards have not been met for in the month of June of Q1 2015-16. A glossary of terms used in this report is provided in the back of this document In this report the data that is being reported for Current Period in the metrics is for June 2015 unless stated otherwise Data Sources • Cancer Open Exeter data • RTT, A&E, HCAI, Diagnostics, MSA, FFT, DToC and Cancelled Operations UNIFY2 data • Ambulance, DToC (national metric), Stroke, HPFT Trust Reports • HCAI, Safer Staffing, SI’s, Safeguarding, LAC ENHCCG Quality Dashboard Please note: all Trust data is looking at the Trust wide position unless stated as ENHCCG only data.
Key: ↑ Improved/Increased performance/activity as compared to prior period. Deteriorated/reduced performance/activity as compared to prior period. → No Change
3

Headline Summary Comments ׀ Outline below is a summary of the key areas of concern and underperformance that the CCG Governing Body need to be aware of. Detailed commentary is provided for each of the areas listed within the report.
CCG
1. Referral to Treatment 2. Accident & Emergency 3. Ambulance Performance 4. Cancer Waits 5. Stroke
Slide 8 Slide 9 Slide 10 Slide 11 Slide 12
5. Diagnostics 6. HCAI 7. Safeguarding Adults 8. Safeguarding Children
Slide 13 Slide 14 Slide 15 Slide 16
Acute Trusts
ENHT PAH RFH
1. Referral to Treatment 2. Accident & Emergency 3. Ambulance Performance 4. Stroke 5. Cancer Waits 6. Serious Incidents 7. Friends and Family 8. Safer Staffing 9. Other
Slide 20 Slide 21 Slide 22 Slide 23 Slide 25 Slide 27 Slide 28 Slide 29 Slide 30
1. Referral to Treatment 2. Accident & Emergency 3. DToC 4. Stroke 5. Serious Incidents 6. Maternity 7. Friends and Family 8. Safer Staffing
Slide 34 Slide 35 Slide 36 Slide 37 Slide 39 Slide 40 Slide 41 Slide 42
Summary • Cancer 62 day waits • Diagnostics • RTT • C.Diff • MRSA • CQC Intelligent Monitoring • Maternity • Serious Incidents
Slide 44
Other Providers
HCT EEAST HPFT HUC
1. ALOS 2. ICT 3. Serious Incidents 4. Pressure Ulcers 5. Workforce 6. Safer Staffing 7. Other
Slide 48 Slide 50 Slide 51 Slide 52 Slide 53 Slide 54 Slide 55
1. STEMI 2. Cardiac Arrest 3. Response Times 4. Turnaround Times 5. Other
Slide 58 Slide 59 Slide 60 Slide 62 Slide 63
1. IAPT 2. Waiting Times 3. Adults 4. EMDASS 5. Serious Incidents
Slide 66 Slide 67 Slide 68 Slide 69 Slide 70
1. Out of Hours & NHS 111 2. Serious Incidents 3. Workforce
Slide 72 Slide 74 Slide 75
4

Key Headlines Comments ׀ Stroke Both ENHT and PAH have been issued with Contract Performance Notices (formerly Contract Query) as a consequence of poor performance against the key stroke metrics. Performance at ENHT was expected to be recovered and sustained from July 2015, however, this has not been achieved. Subsequently, a new Contract Performance Notice was issued under the 2015/16 Contract on 24th July 2015. A new RAP has been agreed with increased financial consequences. PAH have continued to fail a number of key national indicators for stroke services and West Essex CCG submitted a Contract Performance Notice to PAH on the 26th August 2015. RTT ENHT has met the incomplete target consistently in Q1. The Trust has been asked to produce a report detailing progress against the planned additional activity and the CCG will be working with the Trust to test some of the assumptions that were used in the original submission. PAH continue with the validation exercise of patients that have been waiting in excess of 52 weeks. Cancer PAH continues to meet all the required performance standards against cancer waiting times although a full detailed breach analysis is undertaken for all 62 day breaches. ENHT failed to achieve the 62 day standard in June as a result of a large number of late referrals from other Trusts. The CCG has written to the host commissioners of the Trusts concerned. Both Trusts have been required to submit a response to the national initiative to improve and sustain cancer performance and to detail progress against 8 key priorities. Feedback has been provided to ENHT and a revised plan is required for 16th September. A&E The nationally published position shows ENHT Trust failing to meet the target in June as it uses 4 week blocks. Taking into account the full calendar month, the Trust exceeded 95%. However, performance has since deteriorated and the Trust has submitted an Emergency Care Working Plan to improve performance. The national Emergency Care Intensive Support Team (ECIST) will be going in to ENHT to review the Emergency Department on 1st October. PAH performance continues to be poor and has been issued with a Contract Performance Notice by West Essex CCG.
5

NHS Constitution Scorecard ׀
6
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
4 hours direct to stroke unit (ASI 2) 90% Jun 0.0% 47.8% 57.8% ↓90% of time on the stroke unit (ASI 3, IPMR) 80% Jun 0.0% 66.0% 76.9% ↓Thrombolysed within 3 hours 12% Jun 0.0% 9.3% 8.5% ↓TIA - high risk, not admitted, treated within 24 hours (IPMR) 60% Jun 0.0% 55.6% 69.9% ↓TIA - low risk, treated within 7 days from onset 65% Jun 0.0% 46.2% 48.1% ↓
Admitted patients 90% Jun 88.39% 89.49% 89.6% ↓Non-admitted patients 95% Jun 94.80% 95.32% 95.2% ↓Incomplete pathways 92% Jun 94.14% 93.78% 94.1% ↑Patients waiting at the end of the month None Jun 29,166 29,762 29,166 ↑Number of 52 week breaches 0 Jun 12 19 33 ↑
Total number on waiting list None Jun 8,158 7,710 7,710 ↓No patient should wait > 6 weeks 99% Jun 98.32% 98.44% 98.55% ↓
2 weeks for urgent cancer referrals 93% Jun 94.54% 95.62% 95.13% ↓2 weeks for breast symptom referrals 93% Jun 96.45% 98.15% 95.90% ↓31 days to first definitive treatment for all cancers 96% Jun 98.92% 98.92% 98.03% →31 days for subsequent surgery 94% Jun 94.92% 91.89% 94.07% ↑31 days for subsequent drug 94% Jun 98.41% 100.00% 99.44% ↓31 days for subsequent radiotherapy 94% Jun 94.44% 98.44% 97.03% ↓62 days to first definitive treatment for all cancers 85% Jun 79.12% 87.50% 83.15% ↓62 days following screening referral 90% Jun 95.45% 95.00% 95.24% ↑62 days following consultant upgrade 85% Jun 94.44% 100.00% 90.20% ↓
Stroke
Consultant Led Referral to Treatment Times (RTT)
Diagnostic waiting times
Cancer waits

NHS Constitution Scorecard ׀
7
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
A&E attendances None Jun 14,155 13,454 43,193 ↓Percentage seen within 4 hours 95% Jun 91.32% 91.35% 94.49% ↓Emergency Admissions None Jun 3,804 4,048 12,888 ↓
Cat A calls response arriving within 8 minutes - Red 1 75% Jun 79.41% 77.01% 82.22% ↑Cat A calls response arriving within 8 minutes - Red 2 75% Jun 67.78% 72.88% 73.68% ↓Cat A calls ambulance arriving within 19 mins 95% Jun 92.33% 95.31% 95.76% ↓
Mixed Sex Accommodation Breaches 0 Jun 0 0 0 →
No. Clostridium - Hospital Acquired 8 Jun 8 5 16 ↓No. MRSA - Hospital Acquired 0 Jun 0 0 0 →
HCAI
A&E
Ambulances
Mixed Sex Accomodation

ENHCCG ׀ Referral to Treatment
Comments ׀ Performance The metrics show performance against the RTT 18 week standards for ENHCCG patients, irrespective of where they have had their treatment. This information is largely related to the performance at ENHT as PAH have not been reporting on the RTT position since July 2014. The Royal Free returned to national reporting for May 2015. The admitted and non-admitted standards were abolished from June, and only the 92% incomplete target remains. Actions All RTT targets have been met at ENHCCG level although specific actions for individual trusts are detailed in the Provider section. The numbers of patients waiting in excess of 18 weeks on an incomplete pathway is being closely monitored by the CCG and plans are in place to reduce this figure significantly by the end of 2015/16.
Number of Incomplete specialities not meeting standard
Pathway June
General Surgery 91.01%
Urology 90.82%
Trauma & Orthopaedics 88.88%
Cardiothoracic Surgery 73.33%
52 week breaches 12 8
Target 92% Waiting
MonthAdmitted
(ADJ)
Total Admitted Pathways
Non-Admitted
Total Non-admitted pathways Incomplete
Total Incomplete pathways
April 91.37% 2,074 95.70% 8,673 93.54% 25,313May 89.49% 2,445 95.32% 8,596 93.78% 29,762June 88.39% 2,618 94.80% 10,528 94.14% 29,166July 0.00% 0 0.00% 0 0.00% 0August 0.00% 0 0.00% 0 0.00% 0September 0.00% 0 0.00% 0 0.00% 0October 0.00% 0 0.00% 0 0.00% 0November 0.00% 0 0.00% 0 0.00% 0December 0.00% 0 0.00% 0 0.00% 0January 0.00% 0 0.00% 0 0.00% 0February 0.00% 0 0.00% 0 0.00% 0March 0.00% 0 0.00% 0 0.00% 0YTD 89.63% 7,137 95.24% 27,797 94.14%
Completed Completed
RFH returned to national reporting PAH have not reported
RTT activity since July 2014. They are due to resume reporting by the end of Q2 2015.

ENHCCG ׀Accident and Emergency
89%
90%
91%
92%
93%
94%
95%
96%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHCCG seen within 4 hours
% Achieved Target
24%25%26%27%28%29%30%31%32%33%
0
5,000
10,000
15,000
20,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENCCG A&E Attendances & Admission
NonAdmit Admitted Total Attnd Conv
9
Comments ׀ Performance Performance against the A&E 4 hour operational standard is largely reflective of performance at both ENHT and PAH. Performance has deteriorated with only 91% of ENHCCG patients being treated, admitted or discharged within the required 4 hours against the 95% target. Actions Specific actions for ENHT and PAH are detailed in the Provider Sections. The CCG continues to chair a System Resilience Group (SRG) for the health and social care system in East and North Herts, and support the West Essex SRG. The CCG is developing an SRG dashboard to monitor key metrics across the health and social care system to gauge status of the system and to provide early identification of system pressures. The national Emergency Care Intensive Support Team (ECIST) is providing support to trusts across the country to bring about improved and sustained performance in A&E targets.
The previous IPQR only included proxy information. This shows actual ENHCCG patient information which can be subject to change monthly.

ENHCCG ׀Ambulance Performance Comments ׀ Performance Although Red 1 category calls are meeting required response rates, performance has deteriorated for the Red 2 and combined Red category calls. Actions A Remedial Action Plan has been developed to bring about improvements to response times and also handover times. More information is provided against EEAST in the Provider Section.
65%70%75%80%85%90%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses Red 1 calls ENHCCG (8 minutes)
% Achieved Target
60%
65%
70%
75%
80%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses Red 2 calls ENHCCG (8 minutes)
% Achieved Target
10
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance arriving at scene <19 minutes (Red 1/Red 2)
% Achieved Target

ENHCCG ׀Cancer Waits Comments ׀ Performance The 62 day standard continues to be a challenge for Trusts and has prompted a national response from NHS England, Monitor and the National Trust Development Authority who have agreed to lead a national delivery group for improving and sustaining 62 day performance working closely with the Cancer Waiting Times Taskforce (CWTT) and Intensive Support Team.
Actions The CWTT has identified 8 key priorities for local health systems to implement as a matter of urgency. All Trusts were expected to have completed a self-assessment of compliance against the 8 key priorities and, by the end of August, to have returned a plan to achieve full compliance or provide an explanation of non-compliance. All Trusts will also be expected to produce weekly Patient Tracking Lists (PTLs) for the 62 day standard and local health systems will be required to prepare a cancer capacity plan and further guidance is expected to support this piece of work.
Recovery Full compliance is expected to be achieved by the end of March 2016.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer 62 day to first definitive treatment (all cancers)
% Achieved Target Linear (% Achieved)
11
62 day All Standards
Total Treated 135
Accountable Breaches 45
ENHCCG 100+ waiters (all metrics) Q1 12
0
20
40
60
80
100
120
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Activity treated – 62 day first definitive treatment
ENHCCG 15-16 ENHCCG 14-15 ENHT 15-16
ENHT 14-15 PAH 15-16 PAH 14-15

ENHCCG ׀Stroke Comments ׀ Due to the national stroke data records website closing down, CCG level data is unavailable for June. This has been raised as a concern but still has not been resolved and is an ongoing issue as it has been used to provide useful benchmarking information against which performance at ENHT and PAH could be assessed. Performance Performance for April, May and June for ENHT and PAH is detailed in the provider section. Performance remains a key concern within the CCG as performance continues to be poor at both Trusts against key stroke metrics. Actions The Stroke Board within the CCG continues to meet with the main focus being the developments around the Hyper Acute Stroke Unit and contract levers are being used at both Trusts in addition to providing advice and support to bring about improved stroke performance.
0%20%40%60%80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHCCG 4 hours to stroke unit
% Achieved Target 90%
0%5%
10%15%20%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHCCG Thrombolysed within 3 hours
% within 3hrs Target 12%12
0%20%40%60%80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHCCG 90% of time on stroke unit
% on unit Target 80%

ENHCCG ׀ Diagnostics
Comments ׀ Performance Although ENHT has met the required 99%, at CCG level performance has not been met. This is largely due to issues with endoscopy capacity which have arisen at the Royal Free. Actions The Royal Free has been asked to provide a detailed breakdown of patients waiting by CCG and are providing additional clinics internally and also outsourcing endoscopy to improve capacity. The CCG is requesting diagnostic plans from local providers in support of cancer waiting times action plans and these will be reviewed and monitored.
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar<6wks 98.7% 98.4% 98.3%Target 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%Waiting 7,783 7,710 8,158
7,4007,5007,6007,7007,8007,9008,0008,1008,200
94%
96%
98%
100%
Patients waiting
% se
en w
ithin
6 w
eeks
ENHCCG Diagnostics Waiting Times
13

14
Comments ׀
Performance The annual limit for C. difficile cases for ENHCCG for 2015/16 is 112 cases. In Q1 there have been 17 cases. ENHCCG is currently 11 cases below its cumulative limit for the quarter and there have been 14 fewer cases than occurred for the period in 2014/15. ENHCCG has the lowest rate for C. difficile out of the 20 CCGs in the East of England Region (EoE) and is below the average rate for EoE and England. The increase in cases occurring in the non-acute setting during 2014/15 has been halted and a reduction in cases delivered in Q1. Cases in the acute setting have also been reduced. Actions Actions to reduce cases includes continued work with primary care to facilitate compliance to antibiotic prescribing and work with providers to ensure best practice standards are in place for hand hygiene and cleanliness of patient equipment and the clinical environment. A root cause analysis case review is completed for all cases to identify learning to be implemented to reduce the risk of further cases. MRSA bacteraemia There have been no cases of MRSA bacteraemia for ENHCCG in Q1.
0
2
4
6
8
10
12
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHCCG C. diff
Acute NonAcute Limit
ENHCCG ׀ HCAI

ENHCCG ׀Safeguarding Adults MCA/DoLS Action Plan As part of the CCG Mental Capacity Action Plan the CCG commissioned a scrutiny and challenge audit of MCA practice at ENHT, HCT and HPFT by an external expert, this involved conducting case file audits and interviews with the workforce on specific units chosen by the provider. Reports including recommendations have been shared with providers and the CCG, and actions will be monitored via the provider Safeguarding Committees. The CCG Head of Adult Safeguarding has reviewed the reports and produced a summary overview with county wide recommendations. The recommendations include: • Developing a county wide Knowledge & Competency Framework
• Developing and implementing a peer review process
• Implement use of balance sheet
• MCA Conference
Delays in processing DOLS applications continue. Progress is being monitored by the HSAB.
15

ENHCCG ׀Safeguarding Children Comments ׀ Serious Case Reviews ENHCCG has 4 open SCR’s, 3 of which are at various stages of completion and 1 SCR is at the initial stages. Multi-Agency Safeguarding Hub (MASH) MASH went live on 8th July. The CCG Safeguarding Team is working with the Named GP’s and CCG Communications Team to communicate with GP practices to raise awareness, and improve information sharing practices. Looked After Children (LAC) The implementation of the newly commissioned Looked After Children model started in April. Three GP’s with a specialist interest in LAC began undertaking assessments in June, contributing to improvements in the timeliness of assessments (see below) as well showing a marked improvement in the quality of assessments and care planning.
ENHCCG is currently reviewing the provision of assessments for Hertfordshire children placed out of county to establish a more robust approach, and are planning to have put measures in place to improve this pathway by Q3.
16

PROVIDER PROFILES
17

ENHT ׀
18
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
4 hours direct to stroke unit (ASI 2) 90% Jun 62.5% 61.9% 70.3% ↑90% of time on the stroke unit (ASI 3, IPMR) 80% Jun 80.9% 72.1% 86.1% ↑Thrombolysed within 3 hours 12% Jun 4.4% 13.9% 17.9% ↓TIA - high risk, not admitted, treated within 24 hours (IPMR) 60% Jun 76.2% 45.5% 58.8% ↑TIA - low risk, treated within 7 days from onset 65% Jun 60.0% 35.0% 36.0% ↑
Admitted patients 90% Jun 90.35% 90.66% 90.53% ↓Non-admitted patients 95% Jun 95.07% 95.92% 95.58% ↓Incomplete pathways 92% Jun 94.94% 94.57% 94.94% ↑Patients waiting at the end of the month None Jun 22,311 22,674 22,311 ↑Number of 52 week breaches 0 Jun 2 3 8 ↑
Total number on waiting list None Jun 7,490 7,024 21,591 ↓No patient should wait > 6 weeks 99% Jun 99.70% 99.67% 299.03% ↑
2 weeks for urgent cancer referrals 93% Jun 94.60% 96.07% 95.32% ↓2 weeks for breast symptom referrals 93% Jun 93.52% 98.05% 94.35% ↓31 days to first definitive treatment for all cancers 96% Jun 96.20% 98.34% 97.60% ↓31 days for subsequent surgery 94% Jun 97.92% 91.30% 96.04% ↑31 days for subsequent drug 94% Jun 99.29% 99.12% 99.18% ↑31 days for subsequent radiotherapy 94% Jun 95.53% 97.04% 97.42% ↓62 days to first definitive treatment for all cancers 85% Jun 76.88% 81.75% 81.51% ↓62 days following screening referral 90% Jun 92.00% 91.30% 89.39% ↑62 days following consultant upgrade 85% Jun 0.00% 0.00%
Stroke
Consultant Led Referral to Treatment Times (RTT)
Diagnostic waiting times
Cancer waits

ENHT ׀
19
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
Caesarean Section rate (total) 27% Jun 24% 21% 0% ↑Planned Caesarean Section None Jun 12% 9% 0% ↑Unplanned Caesarean Section None Jun 12% 12% 0% →
Inpatient Percentage Recommended None Jun 97.1% 96.2% 0.00% ↑Inpatient Response Rate None Jun 46.5% 49.2% 0 ↓A&E Percentage Recommended None Jun 80.8% 80.0% 0.00% ↑A&E (Type 1 & 2) Response Rate None Jun 14.1% 13.1% 0.00% ↑
A&E attendances None Jun 12,523 11,648 36,953 ↓Percentage seen within 4 hours 95% Jun 94.92% 92.63% 94.04% ↑Emergency Admissions None Jun 3,532 3,355 11,229 ↓
Handovers from ambulance to A&E <15mins 100% Jun 79.90% 75.60% 0.00% ↑Handovers from ambulance to A&E 30 - 60mins None Jun 280 162 594 ↑Handovers from ambulance to A&E >60mins None Jun 9 8 24 ↑
Mixed Sex Accommodation Breaches 0 Jun 0 0 0 →
No. Clostridium - Hospital Acquired 1 Jun 2 0 2 ↓No. MRSA - Hospital Acquired 0 Jun 0 0 0 →
A&E
Maternity
Friends and Family
Ambulances
Mixed Sex Accomodation
HCAI

ENHT ׀ Referral to Treatment Comments ׀ Performance As a result of the recommendations from Sir Bruce Keogh on improving the current waiting time standards and reporting arrangements, the TDA, Monitor and NHS England agreed to abolish the admitted and non-admitted standards from 24th June 2015. It was also agreed that any financial sanctions against these standards would not be applied from 1st April 2015. The incomplete standard will be the sole RTT standard that will be measured going forward. ENHT are achieving the aggregate position against the incomplete standard year to date. There are two specialties that are failing the incomplete standard, Trauma and Orthopaedics and Urology. However, there has been a gradual improvement in performance in each of the three months in the first quarter. An RTT model has been developed jointly between the CCG and Trust to reduce the number of patients waiting over 18 weeks on the incomplete pathway by 31st March 2016. Although there has been a reduction for patients waiting for treatment in May and June, the Trust are to focus on reducing the number of patients waiting over 18 weeks. The Trust will be working with the CCG to jointly test the initial assumptions within the model and will be developing a detailed monitoring template to assess progress against trajectories 52 weeks In quarter 1, 2015/16, there have been three 52 week breaches at ENHT. All patients have now been treated. The reasons for the delays have varied and relate to data validation, complexities in a patient’s pathway and issues with referral processes.
Number of Incomplete specialities not meeting standard
Pathway June/Q1
Urology 88.63%
Trauma & Orthopaedics 87.45%
52 week breaches 3
20
MonthAdmitted
(ADJ)
Total Admitted Pathways
Non-Admitted
Total Non-admitted pathways Incomplete
Total Incomplete pathways
April 90.03% 1,494 95.83% 8,490 93.13% 21,538May 90.66% 1,542 95.92% 7,419 94.57% 22,674June 90.35% 1,493 95.07% 9,076 94.94% 22,311July 0.00% 0 0.00% 0 0.00% 0August 0.00% 0 0.00% 0 0.00% 0September 0.00% 0 0.00% 0 0.00% 0October 0.00% 0 0.00% 0 0.00% 0November 0.00% 0 0.00% 0 0.00% 0December 0.00% 0 0.00% 0 0.00% 0January 0.00% 0 0.00% 0 0.00% 0February 0.00% 0 0.00% 0 0.00% 0March 0.00% 0 0.00% 0 0.00% 0YTD 90.35% 4,529 95.58% 24,985 94.94%

ENHT ׀ Accident & Emergency Comments ׀ Performance Performance against the 4 hour standard dipped to 91% in July 2015. The issues predominantly relates to staffing and pathways within the emergency department. A number of beds have also closed in Q2 die to staffing issues which has impacted on patient flow. Actions An Emergency Care Working Plan has been submitted to the CCG and the TDA so that performance improves and is sustained at the required threshold. There are ten key areas within this action and include: • Implementation of Medical Staffing Strategy for recruitment • Review of Fast Track of patient pathways to AMU and
Ambulatory Care • Maintaining patient flow Performance will continue to be closely monitored on a daily basis and the CCG is developing a system dashboard around ENHT to provide an early identification of pressures within the system. Recovery The Trust is forecasting to achieve the 95% threshold by the end of November.
75%
80%
85%
90%
95%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E patients seen within 4 hours
% Target Linear (%)
21
0%5%10%15%20%25%30%35%40%
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Emergency attendances and admissions
Admissions Non-admissions Total Attends Conv

ENHT ׀ Ambulance Handovers Comments ׀ Performance Whilst there had been a reduction in the number of handover delays from the ambulance to A&E over 30 minutes from February to April 2015, these levels were not sustained from May 2015. Actions Thames Ambulance has been commissioned through the CCG to improve the handover delays and turnaround times continue to be monitored closely on a weekly basis. This is also part of the ED action plan. The job specification for HALO is currently under review. The updated specification will detail joint working arrangements between Thames Ambulance and HALO. Recovery There are ongoing actions to improve performance and reduce the number of delays over 30 and 60 minutes
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar0
5
10Handovers delays from ambulance to A&E >60mins
>60mins
22
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar0
100
200
300Handover delays from ambulance to A&E 30-60mins
30-60mins
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Handovers from ambulance to A&E within 15mins
% <15mins Target

ENHT ׀ Stroke ׀page 1 of 2
Comments ׀ 4 hours direct to stroke unit performance Performance against the key stroke standards continues to remain a significant concern. A Contract Query Notice was issued to ENHT on 20th March 2015 and a Remedial Action Plan was agreed for delivery in quarter 1, 2015. Whilst a number of the actions were delivered, performance did not improve to the required thresholds. Subsequently, a new Contract Performance Notice (formerly Contract Query) was issued under the 2015/16 Contract on 24th July 2015. A new RAP has been agreed with increased financial consequences for not meeting the below three standards. • Proportion of patients admitted to the stroke unit within 4
hours of hospital arrival • Proportion of patients spending 90% of their time on the
stroke unit • Proportion of urgent CTs that take place within one hour Performance was expected to be recovered and sustained from July 2015, however, this has not been achieved. Discharged with Early Supportive Discharge There are some issues with the data and further work is underway. This is addressed through the monthly stroke performance management meetings.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT 4 hours direct to stroke unit
% in 4hrs Target 90% Linear (% in 4hrs)
23
0%
10%
20%
30%
40%
50%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Discharged with Early Supportive Discharge
% Achieved Target 40% Linear (% Achieved)

ENHT ׀ Stroke ׀page 2 of 2
Comments ׀ TIA low risk, treated within 7 days from onset performance Whilst there had been an improvement in the June performance, this is still below target. The Trust has been requested to complete TIA breach templates so we can understand the main reasons for the delays and agree joint actions to improve performance. Thrombolysed within 3 hours Performance against the thrombolysis target has been variable. Concerns remain on the variance in the higher thrombolysis rates that have been reported out of hours in comparison to in hours, and this is being reviewed.
24
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT TIA - low risk, treated within 7 days from onset
% treated Target 65%
0%
5%
10%
15%
20%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT Thrombolysed within 3 hours
% <=3hrs Target 12%

ENHT ׀ Cancer Waits page 1 of 2
25
Comments ׀ The Trust has produced a Cancer 62 Day Standard Action Plan in response to the national tripartite letter Improving and Sustaining Cancer Performance. This letter stated that Trusts should submit action plans to meet the required standard by 31 March 2016 at the latest. The Trust has detailed that performance will be on track for November 2015. Joint feedback provided to ENHT from CCG and TDA on action plan includes: • Further detail required for the deterioration in performance
against the 62 day standard and how the trajectory for recovery has been calculated
• ENHT to prioritise specialities and undertake further work
on the diagnostic action plan to support NICE guidance and the development of one stop clinics
• ENHT to review previous breaches and ensure that all
themes are incorporated into the action plan
72%74%76%78%80%82%84%86%88%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
62 day for first definitive treatment
% Achieved Target
Comments ׀ 62 day for first definitive treatment all cancers This standard deteriorated in May and June to 81.8% and 76.9%. However, 13 out of the 18.5 breaches in June related to late referrals from other Trusts where ENHT received the referral after day 43. Excluding the late referrals, ENHT would have met the required performance of 85% but there are also internal actions to improve pathways that are also required. Actions: The Chief Executive at ENHT has written to the Chief Executive at each of these Trusts regarding the late referrals. In addition, the CCG have also written to the Trusts Host CCGs setting out their concerns

ENHT ׀ Cancer Waits page 2 of 2
26
Comments ׀ 110+ day cancer waits Gynaecological and Urological tumour sites account for the majority of the 100+ day waiters, often as a consequence of complete pathways. Detailed analysis will be undertaken with ENHT of all patients breaching 62 days. This involves reviewing all patients who have breaches the 62 days by tumour site and will identify the reasons for the breaches and actions that are being undertaken to avoid similar issues arising.
0
1
2
3
4
5
6
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
100+ Day Cancer Waits – ENHCCG Patients
Breaches

ENHT ׀ Serious Incidents
Comments ׀ Year to date the Trust have reported 4 Never Events, 2 in Q1 and 2 in Q2 – all investigations are on-going; • Wrong-route administration of medication – no patient harm occurred. • Wrong site surgery – patient due to have a fixation of closed fracture of ring finger middle phlanx. Wrong finger opened. Correct
procedure subsequently undertaken. • Retained vaginal pack following a C-section in August 2015 Retained swab following an orthopaedic (shoulder surgery). The
patient has learning disabilities.
In Q2 to date the Trust has reported 9 Serious Incidents, the most common of which is a patient fall resulting in harm. No Never Events have been reported in this period. It is anticipated there will be a decrease in the number of Serious Incidents reported by ENHT, and all CCG provider organisations, due to the application of the new Serious Incident Framework, published by NHS England.
27

ENHT ׀ Friends and Family Comments ׀ Performance During Q1 ENHT performed above the national average for inpatient score and response rate, with 97% of patients recommending the Trust in June. The Trust’s A&E FFT score remains below the national average during each month in Q1, with 81% of patients recommending the Trust in June. The response rate was also just below the national average in May and June. The Trust has advised that when benchmarked against other Trusts using the same data collection methodology ENHT compares well. Actions The Trust has a patient experience action plan for each division, incorporating actions identified from FFT feedback. The CCG continues to seek assurance through Quality Review Meetings and Quality Assurance Visits.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT Inpatient FFT
Recommended Responses
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT A&E FFT
A&E Recommended A&E Response Rate28

ENHT ׀ Safer Staffing Comments ׀ Performance Fill rates have remained stable during Q1. The overall fill rate for qualified and non-qualified nursing staff is adequate during the day and night, however a number of wards remain below 90% fill rate for registered nurses during the day. The Trust monitors staffing levels on a daily basis, and action is taken to address any ward areas flagging red to ensure safe levels of staffing are in place. The Trust continues to have a number of vacancies including ED and ward areas. Actions Safer staffing is reviewed during Quality Review Meetings as well as during Quality Assurance Visits. The CCG continues to monitor vacancies by ward on a monthly basis to ensure improvement in line with the Trust’s trajectory. Sickness absence and bank and agency usage is reviewed at the same time.
Day Night
Month Nurse HCA Nurse HCA
April 98.68% 119.98% 97.31% 128.88%
May 96.69% 114.91% 98.49% 120.97%
June 96.58% 120.24% 98.77% 119.67%
29

ENHT ׀ Other CQC Intelligent Monitoring Report ENHT has moved from band 5 to band 4 in the latest CQC Intelligent Monitoring Report published in June. Bandings range from 1 to 6 with band 1 being highest risk. One elevated risk is included relating to SHMI. 6 risks were detailed; 3 of these were not previously included and relate to the inpatient survey, diagnostic waiting times and in hospital mortality for respiratory conditions. The Treatment Centre Whilst a number of quality issues regarding ophthalmology services have been resolved, including the backlog of clinic letters, concern remains regarding the availability of medical records for some clinics. Overall pull rate has improved. Issues also remain with the newly installed telephone system, with both patients and GPs raising concerns directly with the Trust as well as through the CCG hotline. The issues relate to a lack of staff as well as technical issues with the system itself. The CCG has requested an urgent update regarding the actions being taken and timescale for resolution. Mortality-SHMI The latest HSCIC quarterly release of SHMI data was released in July (to year end December 2014), showing a rise for ENHT to 113.3 from 112.0 which means it is one of 11 trusts above the statistically expected “observable deaths” limit (for ENHT 110.5). The TDA are now members of our E&N Hospital Mortality Review group, and are coordinating a “Deep Dive” Mortality Day with ENHT, ENCCG and relevant partners in September, to review the position & whether there are additional actions that can be taken. ENHT are on track to be up to date in reviewing 100% of hospital deaths by September, and at the last Mortality Review meeting presented the themes from reviews for Q4 14/15. The Trust also has learning from the re-audit of unexpected admissions to ITU, with the appropriate escalation of concerns an on-going issue. The reintroduction of ward level nursing indicators (which include a NEWS audit) will be useful in monitoring this. The report of the Royal College of Physicians Invited Service Review of the ENHT Respiratory Services and the ENHCCG plans for a community service has now been received, with the review team’s assessment of the high respiratory SHMI as a “lag” indicator that will come down as the impact of improvements made take effect. Infection control and cleaning A number of cleanliness issues have been identified during recent visits undertaken by the CCG Infection Control Lead. Additionally a joint visit with the TDA identified the need to improve processes for auditing standards of cleaning, and the need to ensure correct use of personal protective equipment. This continues to be a focus during Quality Assurance Visits. 30

ENHT ׀ Other Radiology waiting times The latest inpatient radiology dashboard shows poor compliance against a number of internal KPIs relating to waiting times for MRI, CT and Ultrasound. There has been deterioration in a number of metrics over the last few months. The CCG has previously suggested radiology as one of the areas appropriate for full 7 day working. The Trust has advised that GP referrals for MRI are using significant resource and have increased demand. It has been agreed that an audit of MRI requests from GPs will be undertaken to review appropriateness of referrals. Sepsis A sepsis CQUIN has been set nationally for all acute trusts in 2015/16. The CQUIN incentivises Trusts to screen all appropriate patients for sepsis, and to initiate IV antibiotics within one hour of presentation for patients with suspected severe sepsis or septic shock. The Q1 audit results for ENHT have shown the one hour door to needle time compliance is 27%; the CQUIN target is 90%. This is despite an intensive education programme being delivered over the past 5 years. The Trust has recently approved fixed term recruitment to help facilitate achievement of this CQUIN. This is also a focus of the mortality work. Paediatric Services ENHCCG has expressed concern regarding paediatric services following a rise in complaints, 2 recent SIs on Bluebell Ward, a rise in clinical claims and issues cleanliness and facilities issues identified on a recent visit undertaken by the CCG Infection Control Lead. Whilst the complaints do not relate to clinical care and the numbers of claims remain small, the Trust acknowledges improvements are required. A new Head of Paediatrics is in post and progress will be monitored closely by the Trust and CCG. A number of recommendations have been made to the Trust following a recent Quality Assurance Visit. PLACE survey The recently published PLACE survey results show ENHT has deteriorated in all areas compared to last year, and are reported to be the 2nd lowest ranked organisation for food, and the 3rd lowest ranked organisation for ‘privacy, dignity and wellbeing’. The Trust are undertaking a further internal assessment to understand whether the results are a true reflection of the care environment. ENHCCG has written to ENHT regarding the above on-going quality issues, and further discussions will be held at the next Contract Review Meeting.
31

PAH ׀
32
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
4 hours direct to stroke unit (ASI 2) 90% Jun 24.0% 20.0% 0.0% ↑90% of time on the stroke unit (ASI 3, IPMR) 80% Jun 60.0% 62.5% 0.0% ↓Thrombolysed within 3 hours 12% Jun 0.0% 0.0% 0.0% →TIA - high risk, not admitted, treated within 24 hours (IPMR) 60% Jun 57.1% 36.4% 0.0% ↑TIA - low risk, treated within 7 days from onset 65% Jun 89.7% 90.0% 0.0% ↓
Admitted patients 90% Jun 0.00% 0.00% 0.0% →Non-admitted patients 95% Jun 0.00% 0.00% 0.0% →Incomplete pathways 92% Jun 0.00% 0.00% 0.0% →Patients waiting at the end of the month None Jun 0 0 0 →Number of 52 week breaches 0 Jun 24 22 65 ↓
Total number on waiting list None Jun 0 0 0 →No patient should wait > 6 weeks 99% Jun 99.70% 99.72% 0.00% ↑
2 weeks for urgent cancer referrals 93% Jun 98.16% 97.07% 97.49% ↑2 weeks for breast symptom referrals 93% Jun 99.33% 98.28% 98.89% ↑31 days to first definitive treatment for all cancers 96% Jun 98.10% 97.59% 97.52% ↑31 days for subsequent surgery 94% Jun 100.00% 100.00% 100.00% →31 days for subsequent drug 94% Jun 100.00% 100.00% 100.00% →31 days for subsequent radiotherapy 94% Jun 0.00% 0.00% Zero62 days to first definitive treatment for all cancers 85% Jun 86.73% 88.25% 86.93% ↓62 days following screening referral 90% Jun 100.00% 0.00% 100.00% ↑62 days following consultant upgrade 85% Jun 87.95% 96.15% 91.63% ↓
Stroke
Consultant Led Referral to Treatment Times (RTT)
Diagnostic waiting times
Cancer waits

PAH ׀
33
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
Caesarean Section rate (total) 25% Jun 22.7% 29.9% 0% ↑Planned Caesarean Section 10% Jun 9.6% 11.7% 0% ↑Unplanned Caesarean Section 14% Jun 13.1% 18.2% 0% ↑
Inpatient Percentage Recommended None Jun 97.2% 98.4% 0.0% ↓Inpatient Response Rate None Jun 37.1% 35.7% 0.0% ↑A&E Percentage Recommended None Jun 93.0% 95.4% 0.0% ↓A&E (Type 1 & 2) Response Rate None Jun 17.6% 12.6% 0.0% ↑
A&E attendances None Jun 7,748 7,576 24,300 ↓Percentage seen within 4 hours 95% Jun 87.83% 92.21% 92.37% ↓Emergency Admissions None Jun 2,134 2,185 7,145 ↑
Handovers between ambulance and A&E <15mins 100% Jun 61.60% 63.50% 56.50% ↓Handovers between ambulance and A&E 30 - 60mins None Jun 112 139 437 ↑Handovers between ambulance and A&E >60mins None Jun 13 16 41 ↑
Mixed Sex Accommodation Breaches 0 Jun 0 0 0 →
No. Clostridium - Hospital Acquired 1 Jun 2 1 5 ↓No. MRSA - Hospital Acquired 0 Jun 0 0 0 →
Friends and Family
Maternity
A&E
Ambulances
Mixed Sex Accomodation
HCAI

PAH ׀ Referral to Treatment Comments ׀ Performance Following issues with the implementation of the new EPR system, the Trust has been unable to report on RTT national standards. There are weekly teleconference calls with the TDA and NHSE. PAH are suggesting they are on track to deliver national reporting by end of Q2. However there is no plan to retrospectively report once national reporting commences, this was endorsed by the TDA and has not been supported by NHSE. PAH have sought the services of Interim Management and Support (IMAS) services to work with the Trust to review PTL management processes, diagnostic process and their access policy, which is due to go the board and planned programme board in September for sign off. IMAS have already undertaken some audit work and put in place recommendations to help the Trust improve performance and processes, including reviewing the Access Policy and Diagnostics pathways. WECCG submitted a Contract Performance Notice to PAH on the 26th August 2015, against the Trust’s failure to deliver the incomplete target. 52 Week Breaches PAH has been undertaking a validation exercise to the PTL which has identified number of patients who have been waiting over 52 weeks. All breaches are monitored and updates on the patients pathways are given on a weekly basis via the weekly RTT meetings which both WECCG and ENHCCG attend. All patients that have waited over 52 weeks are reviewed for clinical harm. WECCG are to undertake an audit of the harm reviews to give assurance that all findings are correct. The Trust are working with other providers to give long waiting patients a choice of having their treatment elsewhere. The Trust are to start discussions with North Middlesex Hospital at the beginning of September to work jointly in Ophthalmology and Cardiology services. WECCG submitted a Contract Performance Notice to PAH on 26th August 2015, relating to the Trust failure to treat patients within 52 weeks. Action ENHCCG are attending weekly RTT recovery meetings with WECCG to ensure there is a focus on treating all patients who have waited over 52 week, receiving updates from PAH on the progress of the new the EPR system and national reporting deadlines and ensuring that there is open communications between the Trust and CCGs. IMAS will continue to work with the Trust to support their improvements.
34

PAH ׀ Accident & Emergency Comments ׀ Performance PAH continue to fail to meet the 4 hour A&E target. The Trust submitted a revised plan for recovery by end of July, which it has also failed to achieve. Contributory factors for failing to delivery the recovery plan are: • Increased acuity of patients • Significant Norovirus outbreak in May affecting PAH and
Community Providers • Delays in moving patients through the system • Medical delays with specialty reviews • Care Home availability • Re-ablement capacity • Workforce shortages
Actions As a consequence of failure to meet the recovery plan WECCG submitted a Contract Performance Notice to PAH on the 26th August 2015. A Performance Notice meeting was held between PAH and Commissioners, during the second week of September 2015. ENHCCG has requested WECCG to approve the revised action plans through the SRG.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E seen within 4 hours
% seen Target Linear (% seen)
27%27%28%28%29%29%30%30%31%31%32%
01,0002,0003,0004,0005,0006,0007,0008,0009,000
10,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Emergency attendances & admissions
Admissions Non-admissions Attendances Conv35

PAH ׀ Delayed Transfer of Care Comments ׀ Performance The Trust are still unable to achieve the performance target of 3.5% currently recording 5.1% in June and 5% in July which were NHS delays attributable by the Trust. The Trust have a trajectory to achieve 3.5% target by the end of September 2015. The Trust face challenges internally due to staffing shortages with 200 Nurse/Midwife/Health Care Assistant vacancies. The staff shortages have a significant impact on delays in discharge processes. The other main challenges are finding suitable residential placements and complex packages of care in the community. Actions The Trust has taken the following actions to address the underperformance: • Creation of single integrated discharge team • Implementation of 100 day challenge methodology to
accelerate the work • Specialist discharge nurses. • Home to Assess (Trusted Assessor Model) • Increase in medical staffing out of hours to improve safety
and performance. • Frailty service development • Nursing recruitment to improve assessment timescales. • Appointment of patient journey co-ordinators. • On going “ Every Minute Matters” programme which
includes Front door, assessment and discharge process. • Older people programme 36

PAH׀ Stroke ׀page 1 of 2
Comments ׀ Performance PAH have continued to fail a number of key national indicators for stroke services. WECCG submitted a Contract Performance Notice to PAH on the 26th August 2015. 4 Hours to stroke unit The main themes for failure to meet this target are lack of bed availability, complex and late diagnosis, slow transfers and failure to refer to stroke team by ED staff. 90% of time on stoke unit The themes for failure to deliver this target are the same as above for ‘4 Hours to stroke unit’. Thrombolysed within 3 hours The main themes for failure to deliver this target are patients not meeting the criteria or arriving outside the time window. Actions Following the Contract Performance Notice sent on 26th August, a meeting is in September to agree revised, deliverable Remedial Action Plans (RAP). ENHCCG has confirmed with WECCG its expectations of what the RAP should include, and is seeking confirmation from WECCG the process for signing the RAP off.
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
4 hours direct to stroke unit
% in 4hrs Target 90%
37
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
90% of time on stroke unit
% on stroke unit Target 80% Linear (% on stroke unit)
0%
5%
10%
15%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Thrombolysed within 3 hours of onset
% <3hrs Target 12% Linear (% <3hrs)

PAH ׀ Stroke ׀page 2 of 2
Comments ׀ High Risk TIA Main themes for failure to meet the target are due to timing of clinics, delays in referrals and communication errors. Actions in place include roll out of electronic referrals by ENHCCG GPs to improve the process over the weekends, and regular reviews of timings of clinics. For Note: Work continues across the system to re-commission the Stroke Pathways for Hertfordshire patients.
0%10%20%30%40%50%60%70%80%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
TIA - high risk, not admitted, treated within 24 hours
% treated <24hrs Target 60% Linear (% treated <24hrs)
38

PAH ׀ Serious Incidents
Comments ׀ PAH reported 38 Serious Incidents during Q1, 7 of which related to ENHCCG patients. The main theme for PAH SIs remains pressure ulcers. A breakdown of the types of incident reported during Q1 can be found in the above graph. As previously advised, PAH reported one Never Event in Q1 regarding wrong site surgery. The incident did not relate to an ENHCCG patient. In Q2 to date, PAH has declared 6 Serious Incidents relating to ENHCCG patients.
39

PAH ׀ Maternity Comments ׀ Unplanned caesarean Section Following an increase in unplanned caesarean section rate in May, there has been a decrease in June with a rate of 13.1%. The total c-section rate remained high in April and May with a rate of 26.7% and 29.9% respectively. This decreased to 22.7% in June; within the 25% threshold. The Trust continues to review all emergency caesarean sections within 24 hours to see whether the procedure was the correct management of the labour. Actions The CCG continues to monitor performance and progress through the monthly Quality Review Meetings.
40
0%
5%
10%
15%
20%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Unplanned caesarean section
unplanned Target <14%

PAH ׀ Friends and Family Comments ׀ Performance During Q1 PAH performed below the national average for inpatient FFT in April, however they performed above the national average in May and June, with 97% of patients recommending the Trust in June. The inpatient response rate was above the national average throughout Q1. The A&E FFT score was above the national average each month with 93% of patients recommending the Trust in June. The response rate was above the national average in April and June. Actions ENHCCG continues to accompany West Essex CCG on Quality Assurance Visits to PAH, during which patients are spoken with regarding their experiences.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
PAH Inpatient Survey
Recommended Response Rate
41
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
PAH A&E Survey
Recommended Response Rate

PAH ׀ Safer Staffing Comments ׀ Performance The June safer staffing data shows PAH continue to report a fill rate below planned levels for registered nursing staff during the day and night. The planned registered nurse fill rate for day shifts in June was 81.7%. PAH report that at times wards have converted supervisory time to direct clinical care to ensure staffing levels are adequate and safe care is provided. This continues to be monitored closely at both ward and directorate level within the Trust. Actions The CCG continues to review the ward level data and any wards or units with poor fill rates, as well as recruitment plans, are discussed at Quality Review Meetings. Staffing levels are also monitored during Quality Assurance visits.
Day Night
Month Nurse HCA Nurse HCA
April 78.72% 105.58% 103.29% 108.87%
May 80.24% 109.53% 110.98% 108.54%
June 81.70% 104.30% 109.10% 105.23%
42

RFH ׀ Barnet & Chase Farm Hospital
43
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
No patient should wait > 6 weeks 99% Jun 91.6% 91.6% 91.8% →
2 weeks for urgent cancer referrals 93% Jun 94.40% 93.70% 93.40% ↑2 weeks for breast symptom referrals 93% Jun 98.40% 98.30% 98.30% ↑31 days to first definitive treatment for all cancers 96% Jun 100.00% 100.00% 100.00% →31 days for subsequent surgery 94% Jun 100.00% 100.00% 100.00% →31 days for subsequent drug 94% Jun 100.00% 100.00% 100.00% →62 days to first definitive treatment for all cancers 85% Jun 68.70% 74.30% 80.60% ↓62 days following screening referral 90% Jun 100.00% 96.20% 100.00% ↑
Inpatient Percentage Recommended None Jun 88.8% 85.4% ↑A&E Percentage Recommended None Jun 86.0% 86.6% ↓
A&E attendances None Jun 682 741 2244 ↑Percentage seen within 4 hours 95% Jun 96.9% 98.3% 97.7% ↓Emergency Admissions None Jun 153 185 517 ↑
Handovers from ambulance to A&E 30 - 60mins None Jun 58 59 173 ↑Handovers from ambulance to A&E >60mins None Jun 1 0 4 ↓
Mixed Sex Accommodation Breaches 0 Jun 1 0 6 ↓
No. Clostridium - Hospital Acquired Jun 4 0 7 ↓No. MRSA - Hospital Acquired 0 Jun 1 0 1 ↓
HCAI
Diagnostic waiting times
Friends and Family
A&E ENHCCG patients only
Ambulances
Mixed Sex Accomodation
Cancer waits

RFH׀ Summary page 1 of 3
Comments ׀ 62 Days from GP referral. The trust failed the indicator in quarters 3 & 4. For May the trust recorded 78.5%, for BCF the performance was 74.3%. Performance was largely affected by the increase in the Urology pathway, specifically delays in diagnostics and tertiary referrals to UCLH. The Trust has been issued with a Contract Query Notice. The Trust has implemented a Cancer Recovery Plan, Sustainability Plan and Urology Recovery Plan. A recent waiting list validation has informed the recovery trajectory to ensure a return to national compliance but this may not be until December 2015. Diagnostics waiting 6 week or over. During June BCF site recorded 91.6% against a target of 99%. The most significant performance driver is Endoscopy where BCF performance equated to 43.3% in June. In order to reduce waiting times the Trust has developed a series of contracts with the Independent Sector focussing on those patients waiting over 6 weeks. In addition, two endoscopy rooms will be constructed by November 15. A revised and comprehensive recovery trajectory including all breaching modalities will be made available to the Performance Review Group via a separate report. RTT National reporting resumed for BCF on 17th June for May data which was the first submission for the whole Trust following an intensive recovery programme which required a completely new reporting process. June data was submitted on July 15th. The incomplete pathway performance is at 88.3% for the Trust. Measures have been put in place to increase clinics, theatre sessions, beds, staff and outsourcing to improve performance. 52 Weeks Breaches The Trust has reported 11 ENHCCG patients who have waited longer than 52 weeks. These are al follow-up patients. The Trust is providing detail for each patients delay which ENHCCG will review. 44

RFH ׀ Summary page 2 of 3 Comments ׀ C-difficile The trust has been in breach of the quarterly cumulative trajectory for four consecutive quarters and breached the annual target for 2014/15, the trust has also breached for qtr1. A governance concern may be triggered. The trust advised Monitor that it expects to return to compliance in qtr3 2015/16. There have been 7 cases of C. difficile at BCF sites which is 2 cases below the cumulative trajectory for Q1 for these sites. MRSA There have been 2 cases of MRSA bacteraemia in Q1 at BCF sites. Both were at Barnet Hospital. Both cases have been investigated to identify learning for the Trust. CQC Intelligent Monitoring Report The RF has moved from band 4 to band 3, into a higher risk band, in the latest CQC Intelligent Monitoring Report published in June. In total there are 2 elevated risks and 6 risks. The new elevated risks relate to hip Patient Reported Outcome Measures (PROMS) data and Sentinel Stroke National Audit Programme (SSNAP) data. The new risks relate to knee PROMS data, NHS staff survey and ESR data regarding staff stability. Maternity A Contract Query Notice has been issued by Barnet CCG in relation to concerns around maternity services and outlying performance indicators. The RF has undertaken a comprehensive review of maternity services including learning from SIs and complaints, which was presented to the CQRG in July. Barnet Hospital maternity dashboard has a number of metrics flagging amber or red including c-section rate, induction of labour rate, major haemorrhages and 3rd and 4th degree tears. Validation has identified that 3rd and 4th degree tears have been incorrectly classified in some cases and the actual rate is lower than has been reported. A detailed integrated action plan is in place. There are 4 immediate areas of focus; • Clinical Governance • Maternity Dashboard triggers • Antenatal and new-born screening • Themes from SIs
45

RFH ׀ Summary page 3 of 3 Comments ׀ Serious Incidents During Q1 Royal Free reported 21 SIs across the organisation. Due to the format of the report it is not possible to determine the number of SIs that relate to Barnet and/or Chase Farm Hospital specifically. A breakdown of the types of SIs reported by Royal Free can be found below. During Q1 Royal Free reported 2 Never Events; both relating to surgical procedures and neither affected ENHCCG patients.
46

HCT ׀
47
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
Stroke 35 Jun 55.0 17.0 28.0 ↓Stroke rehab pathway 35 Jun 30.0 17.0 17.8 ↓Stroke neuro rehab patients 42 Jun 29.5 30.9 34.7 ↑Non-stroke 21 Jun 21.0 25.5 22.8 ↑Non-stroke rehab pathway 19 Jun 14.3 17.5 16.0 ↑Readmission rates within 30 days 0.5% Jun 0.0% 0.0% 0.0% →
Non-admitted patients 95% Jun 98.8% 98.5% 98.8% ↑Incomplete pathways 92% Jun 99.5% 99.4% 99.5% ↑Patients waiting at the end of the month None Jun 3,643 3,759 3,643 ↑Number of 52 week breaches 0 Jun 0 0 0 →
Patients to start treatment within 18 weeks from referral 98% Jun 98.1% 99.5% 0.0% ↑
Mixed Sex Accommodation Breaches 0 Jun 0 0 0 →
No. Clostridium - Hospital Acquired (annual target) 13 Jun 1 1 2 →No. MRSA - Hospital Acquired 0 Jun 0 0 0 →
Number of Acquired Pressure Ulcers (Grades 3 & 4) None Jun 0 1 6 ↑Number of pressure ulcers determined to be 'avoidable' 0 Jun 0 0 1 →
Non-Consultant Led Referral to Treatment Times (RTT)
Mixed Sex Accomodation
HCAI
Average Length of Stay
Consultant Led Referral to Treatment Times (RTT)
Pressure Ulcers
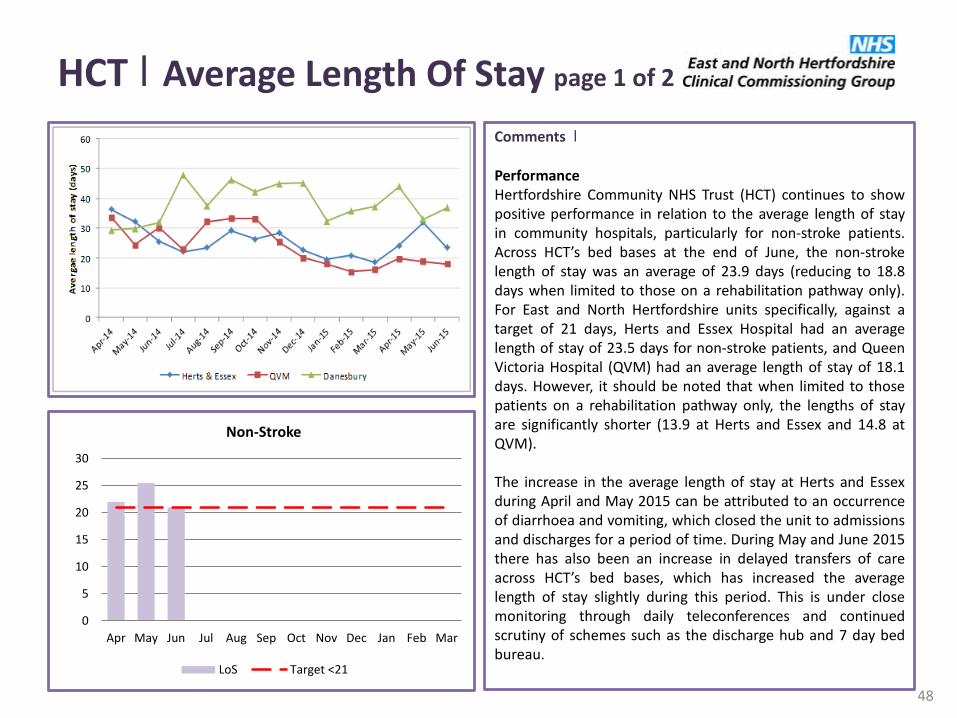
HCT ׀ Average Length Of Stay page 1 of 2
Comments ׀ Performance Hertfordshire Community NHS Trust (HCT) continues to show positive performance in relation to the average length of stay in community hospitals, particularly for non-stroke patients. Across HCT’s bed bases at the end of June, the non-stroke length of stay was an average of 23.9 days (reducing to 18.8 days when limited to those on a rehabilitation pathway only). For East and North Hertfordshire units specifically, against a target of 21 days, Herts and Essex Hospital had an average length of stay of 23.5 days for non-stroke patients, and Queen Victoria Hospital (QVM) had an average length of stay of 18.1 days. However, it should be noted that when limited to those patients on a rehabilitation pathway only, the lengths of stay are significantly shorter (13.9 at Herts and Essex and 14.8 at QVM). The increase in the average length of stay at Herts and Essex during April and May 2015 can be attributed to an occurrence of diarrhoea and vomiting, which closed the unit to admissions and discharges for a period of time. During May and June 2015 there has also been an increase in delayed transfers of care across HCT’s bed bases, which has increased the average length of stay slightly during this period. This is under close monitoring through daily teleconferences and continued scrutiny of schemes such as the discharge hub and 7 day bed bureau.
48
0
5
10
15
20
25
30
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Non-Stroke
LoS Target <21

HCT ׀ Average Length Of Stay page 2 of 2
Comments ׀ Performance Overall, HCT has shown improvement in the average length of stay for stroke patients during the first quarter of 2015-16; achieving an average length of stay of 25.9 days against a target of 30-35 days across all of its bed bases. Danesbury has achieved an average 37.9 day average length of stay, which is partially explained by a number of Neuro-rehab patients at the unit and delayed transfers of care over recent months. There does however, continue to be positive progress in terms of the service offer to stroke patients: • A greater proportion of stroke patients are being seen by a stroke
specialist team (64%) • 41.5% against a threshold of 40% of East and North Hertfordshire
CCG stroke survivors are being discharged from acute or community units with Early Supportive Discharge
• There has been a significant proportion of stroke survivors being offered a 6 month review (87% of patients have been offered a 6 month review in quarter 1 2015-16), but there is still work to be done to ensure that patients accept and engage.
Homecare capacity has been identified as being one of the main reasons for HCT delays (largely in the West of the county). The following actions are being undertaken: • New block providers on clear trajectories for increasing capacity
ahead of winter • New short-term providers being accredited for delivering in
September • Average package of care increasing which puts pressure on capacity • Review of all HCT patients that also receipt of homecare to
streamline process to become more efficient and release social care capacity.
0
10
20
30
40
50
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Stroke Neuro Rehab Patients
LoS Target <42
49

HCT ׀ Integrated Community Teams Comments ׀ Performance The reported response times to referrals to the Community Teams continues to be below target. An audit of urgent referrals during June 2015 indicated that all but one reported breach was due to a data quality or recording issue as opposed to a performance issue. HCT has agreed to ensure that all urgent referrals are seen within timescale from July 2015 onwards, and that accurate reporting of these response times will be sent through to the CCG. Priority 2 referrals will undergo the same scrutiny during August 2015, and Priority 3 referrals will be scrutinised by October 2015, with agreement that full and accurate reporting will be in place for month 7 onwards. Actions The Information Breach will remain in place until the CCG is assured that all recording and reporting issues have been resolved.
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Face to face response 2-4hrs for priority 1 referral
% Achieved Target 100%
50
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Face to face response 24-48hrs for priority 2 referral
% Achieved Target 100%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Face to face response 24-48hrs for priority 2 referral
% Achieved Target 100%

HCT ׀ Serious Incidents
Comments ׀ During Q1 HCT reported 29 Serious Incidents across the organisation, 10 of which fell under the management of ENHCCG. Out of the total number of ENHCCG cases reported by HCT in Q1, 7 related to Grade pressure ulcers. The main theme in Q1 continued to relate to Grade 3 Pressure Ulcers and the above graph shows a breakdown of Serious Incidents relating to ENHCCG patients. In Q2 to date, HCT has reported 10 Serious Incidents across the organisation, 3 of which relate to ENHCCG patients. As previously advised it is expected for there to be a decrease in the number of Serious Incidents reported in Q2 due to the application of the revised NHS England SI Framework, particularly regarding Grade 3 and 4 pressure ulcers. It is only if acts or omissions have contributed to the pressure ulcer developing and the patient suffers severe harm as a consequence that this meets the new criteria for reporting as an SI.
51

HCT ׀ Pressure Ulcers Performance In Q1 HCT reported 4 avoidable grade 3 and 4 pressure ulcers, 2 relate to ENHCCG patients. In Q2, one pressure ulcer Serious Incident has been declared by the Trust but this does not relate to an ENHCCG patient. Following the implementation of the new Serious Incident Framework and the changes to the reporting criteria there has been a significant reduction in Pressure Ulcer SI as expected. If acts or omissions have contributed to the pressure ulcer developing and the patient suffers severe harm as a consequence then this meets the new criteria for reporting as an SI.
0.0
0.5
1.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of pressure ulcers determined to be 'avoidable'
Number
52

HCT ׀ Workforce Comments ׀ Staff Appraised in the last 12 months Appraisal rates are expected to increase from Q3 when the roll out of appraisal process has cascaded from managers to staff. This is currently in progress. Agency and Bank Staff Agency and Bank has reduced in June but remains above the threshold during the period due to escalation beds and winter resilience funding. The escalation beds have been closed and this had a significant effect on staffing levels. The CCG continues to review the ward level data and any units with poor fill rates are discussed at Quality Review Meetings. The July safer staffing data shows HCT to have an adequate overall fill rate for qualified and non-qualified staff during the day and night.
53
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staff Appraised in the last 12 months
% Turnover Target 90% Linear (% Turnover)
0%
2%
4%
6%
8%
10%
12%
14%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Agency and Bank Staff
% Turnover Target 4.5% Linear (% Turnover)

HCT ׀ Safer Staffing Performance The CCG continues to review the ward level data and any units with poor fill rates are discussed at Quality Review Meetings. The July safer staffing data shows HCT to have an adequate overall fill rate for qualified and non-qualified staff during the day and night. The CQC reports highlighted the need for HCT to improve recruitment, manage vacancies and work with commissioners to ensure services are safely resourced. HCT’s overseas recruitment drive has been successful with 13 members of staff due to start on 20th July. The qualified nursing levels at Herts and Essex Hospital have increased since April to have an adequate fill rate. Herts and Essex continue to be monitored at the Quality Review Meetings.
Day Night
Month Nurse HCA Nurse HCA
April 95.56% 103.14% 95.96% 117.42%
May 98.88% 125.20% 99.76% 127.25%
June 98.48% 121.50% 100.20% 128.18%
Herts and Essex Day
Month Nurse HCA
April 84.86% 74.69%
May 100.82% 119.88%
June 95.51% 122.54%
54

HCT ׀ Other Comments ׀ Physiotherapy The average waiting time for physiotherapy was 12 weeks at the end of June 2015. Vacancies within the core MSK and physiotherapy team at HCT meant that progress against the backlog was slower than anticipated during the first quarter of 2015-16. Agreement was made that HCT could have until mid-August to clear the backlog and the most recent information provided shows that the average wait is now 7.8 weeks. However, there are still a number of patients waiting over 8 weeks to access the Service, and HCT are being challenged to set out the actions and associated timescales to ensure that anyone waiting over 8 weeks has been seen, and to then sustain this moving forward. Wheelchairs Following Hertfordshire Business Service (HBS) signalling its intent to give notice on the repair, maintenance and delivery elements of the Wheelchair Service, East and North Hertfordshire CCG has started work to specify what it would require from a new service, both in terms of pathways and service model. The Governing Body in July 2015 approved the recommendation for an interim provider of repair, maintenance and delivery to be sought whilst work was undertaken to specify and procure a longer-term service. The intention had been for HCT to act as the lead provider for this interim solution. However, HCT has written to both East and North Hertfordshire CCG and Herts Valley CCG to state that it is unable to support the interim model and has given notice that it will cease to provide the clinical assessment and prescription elements of the Service from March 2016. Work is underway to ensure that there is no reduction in clinical support to patients accessing the Wheelchair Service, and to negotiate a safe and effective interim Service to ensure there is no loss of provision.
55

HCT ׀ Other Comments ׀ Respiratory Service Discussions between HCT, East and North Hertfordshire Trust and the CCG are ongoing around the enhanced Community Respiratory Service. It should also be noted that the Strategic Clinical Network has benchmarked Pulmonary Rehabilitation across the East of England, and East and North Hertfordshire is performing above average for the uptake and the completion rates of Pulmonary Rehab. East and North Hertfordshire was, however, rated as below average for the number of commissioned Pulmonary Rehab places. There has been positive progress in increasing the capacity of the Pulmonary Rehab Service in East and North Hertfordshire, with increased recruitment and resources being put in place so that there will be capacity for 750 places within the Service by early 2016-17. Diabetes During August 2015, it has come to light that there are significant challenges to the effective delivery of the HCT diabetes service. HCT are reporting high levels of staff sickness, vacancies and are also seeing increased demand for diabetes structured education. As a result, HCT have cancelled a number of clinics in August and September. ENHCCG has held an urgent meeting with HCT to understand the current issues and have negotiated am action plan for close scrutiny over the coming weeks. HCT have been asked to confirm any risks to patients and to provide transparency over the clinics that have been cancelled. This will be further followed up at the contact review meeting on the 14th September 2015.
56

EEAST ׀
57
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
Outcome from cardiac arrest measured by ROSC at point of handover of the patient to hospital 21.5% May 25.9% 24.4% 0.0% ↑Percentage of patients who survive cardiac arrest to discharge from hospital 6% May 4.8% 6.8% 0.0% ↓
Percentage of patients suffering a STEMI PPCI and receive angioplasty within 150 minutes of call 95% May 94.0% 86.1% 0.0% ↑Percentage of STEMI patients receiving appropriate care bundle (ENHCCG) 80% May 76.1% 84.5% 0.0% ↓
Percentage of suspected stroke patients who received appropriate care bundle 95% May 98.0% 96.5% 0.0% ↑Percentage of FAST positive stroke patients who arrived at a hyper acute stroke centre within 60 minutes of call 56% May 52.5% 62.4% 0.0% ↓
Cat A calls response arriving within 8 minutes - Red 1 (immediately l ife-threatening) 75% Jun 80.70% 79.88% 0.00% ↑Cat A calls response arriving within 8 minutes - Red 2 (serious but not the most l ife threatening) 75% Jun 69.60% 71.53% 0.00% ↓Cat A calls ambulance arriving within 19 mins 95% Jun 94.80% 95.54% 0.00% ↓
% of handovers to clear <15mins - Lister 100% Jun 76.60% 71.90% 0.00% ↑% of handovers to clear <15mins - PAH 100% Jun 41.80% 39.70% 0.00% ↑
Ambulances Turnaround
Response Times - Red 1 and Red 2 Calls
Cardiac Arrest (ENHCCG patients)
STEMI (ST segment elevation myocardial infarction)
Stroke (ENHCCG patients)

EEAST ׀ STEMI Comments ׀ Beds Herts and Luton locality met 5/8 Ambulance Quality Indicators (ROSC, Survival to discharge, STEMI care bundle, Stroke 60 and Stroke care bundle). Actions across the Trust: • Ongoing monitoring • Performance Improved Action Plan (PIAP) focusing on the
required resource to deliver the 6 Trust priorities as referred to on slide 63.
• Revised resource allocation guidelines have been released looking at back up/deployment.
• Monitoring of contractual performance of Unit Hour Production (UHP) and those patients who waited the longest for an ambulance
• Reviewing practices to support reducing the time spent on scene.
• Individual case reviews to identify where patients could have been managed differently.
• Recruitment ongoing of Student Paramedic and qualified staff.
• Reinforcement of care bundle documentation including guidance on completion
75%
80%
85%
90%
95%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Patients suffering a ST segment elevation myocardial infarction (STEMI) PPCI and receive angioplasty within
150 minutes of call
<150mins Target 95% Linear (<150mins)
58
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ST segment elevation myocardial infarction patients receiving appropriate care bundle (Beds, Herts &
Luton)
% received Target 80% Linear (% received)

EEAST ׀ Cardiac Arrest Comments ׀ Actions across the Trust: • Ongoing monitoring • Community First responders (CFR) deployment
improvement, expected to see impact from August • Critical Care/Helicopter Emergency Medical Services
deployment to support cardiac arrest outcomes • Review of improvements to cardiac arrest, to trial
automated Cardio Pulmonary Resuscitation devices • New defibrillator roll out improving quality of CPR • Assessment of all clinical staff on Advanced Life
Support/Intermediate Life Support • Focus on deployment to reduce time for first arriver on
scene • Recruitment ongoing of student paramedic and qualified
staff • Review of acute providers on Out of Hospital Cardiac Arrest
and hospital process
Actions: ENHCCG continues to review monthly and seek assurance through the Quality Review Meetings.
0%
2%
4%
6%
8%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Patients who survive cardiac arrest to discharge from hospital
% Achieved Target 7%
59
0%
5%
10%
15%
20%
25%
30%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outcome from cardiac arrest measured by ROSC at point of handover of the patient to hospital
% Achieved Target 25%

EEAST ׀ Response Times page 1 of 2
Comments ׀ Performance EEAST continue to have significant pressures throughout the system with an increase of 9,000 conveyances compared to the same period last year. In E&N Herts, for Q1 there was an increase in demand for Red 2 calls by 29,904, 4.1% compared to Q1 2014-15 and contracted activity is up by 6%. In response, EEAST have compiled a draft remedial action plan (RAP) to address the issues and have asked commissioners to review activity plans where significantly over contracted levels. EEAST has ceased the funding for private ambulance service EEAST are working with Primary care to prioritise home visits to alleviate the impact this has upon front line resources during busy periods of the day. As part of the initiatives for EEAST to increase the use of alternative pathways, two frailty vehicles have been commissioned to come online from December 2015.
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulances arriving at the scene within 19 minutes Red 1/2 Calls
% arriving Target 95% Linear (% arriving)
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Red 2 calls responded to within 8 minutes
Calls Target 75% Linear (Calls)
60
East and North Hertfordshire Red 2 Comparison
Performance Activity
Q1 2014
Q1 2015 Change Q1
2014 Q1
2015 Change
61.6% 71.7% 10.1% 5,744 6,089 6.0%

EEAST ׀ Response Times page 2 of 2
Comments ׀ Actions • All 19 CCG’s in EoE have committed additional investment for student paramedics to complete their 2 year programme. • Investment to continue to improve performance and continue with schemes that worked well over the winter period , such
as HALO. • Trust to review trajectories with the RAP as these were seen as unacceptable by commissioners. An action plan has been drafted for conveyance and non-conveyance, key headlines include: • 111 HCP advice line • EEAST CQUIN GP advice line • EEAST to use alternative pathways (frailty vehicles and Homefirst) • Introduction of ECP/paramedic at UCC • Explore possibilities to use other means of transport for non emergency patients • Review high users of ambulance services
61

EEAST ׀ Turnaround Times Comments ׀ Performance Handover hours lost at Hospital has deteriorated by 25% against a plan to reduce lost hours by 38%. ENHCCG continues to commission HALO to strengthen the relationship between EEAST and ENHT. Since the introduction of HALO in October 2014, EEAST has seen a reduction in the delays from handover to clear in 30 and 60 minuets and an improvement in handover to clear within 15 minutes at the Lister Hospital from 45% - 50% achieved prior to October 2014 to 70% - 75% achieved (still unable to meet the full target of 100%). Performance at Princess Alexandra Hospital remains under the 100% target achieving 37% - 55%. EEAST and PAH have developed a draft policy to address the underperformance. There are now 3 full time HALO’s recruited at ENHT who work between them 12 hours per day, 7 days per week, which should see a continued improvement in the turnaround targets over the coming months. Actions Turnaround performance is discussed at monthly contract meetings with EEAST and at EEAST SLA meetings. This issue is also a key focus of the draft remedial action plan that EEAST have complied. 0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Handover to Clear – PAH
<15mins Target 100% Linear (<15mins)
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Handover to Clear – Lister Hospital
<15mins Target 100% Linear (<15mins)
62

EEAST ׀ Other Comments ׀ EEAST’s priorities for 15/16 are: 1. Recruit 400 Student Paramedics. 2. Increase the skills of staff and convert 60 Emergency Care Assistant’s to Emergency Medical Technician's (EMT) and 40 EMT’s
to Paramedic. 3. Continue Fleet replacement Programme to maintain all frontline vehicles less than five years old. 4. Reinvest the corporate spend into frontline delivery through robust benchmarking. 5. Implement an organisational development Programme. 6. Secure Computer Aided Dispatch system. Workforce Part of the contract negotiation within 15/16 meant that EEAST received 2% of the 2.5% allocated to CQUIN to fund the Year 2 Student training Programme. EEAST remain 7% under budgeted establishment, recovery remains dependent upon Student Ambulance Paramedic programme to deliver qualified skill mix upgrades. This was a known challenge to performance when EEAST entered contractual agreement. Staffing remains a key challenge within ENHCCG. There are currently 53 wte vacancies however, 27 wte have been recruited and are expected to be in post by end of December. EEAST are targeting recruitment to local areas. Local teams with HR support are attending graduate days, recruitment fairs and advertising locally via the media, such as the radio.
63

HPFT ׀
64
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
Patients on a Care Programme Approach (CPA) for at least 12 months who had a CPA review within the last 12 months 95% Jun 98.3% 96.8% 0 ↑Admissions to acute wards that were gate kept by the Crisis Resolution Home Treatment (CRHT) teams (QA) 95% Jun 100.0% 100.0% →Patients on Care Programme Approach (CPA) who were followed up <7 days after discharge from psychiatric inpatient care (QA) 95% Jun 100.0% 100.0% →Number of new cases of psychosis served by early interventions teams 6 Jun 6 12 0 ↓IAPT 18 week RTT 95% Jun 100.0% 99.7% ↑IAPT 6 week RTT 75% Jun 97.4% 95.6% ↑EIP 14 day wait 50% Jun 100.0% 100.0% →
Routine referrals: community eating disorder services <28 day wait 98% Jun 100.0% 100.0% 0 →Routine referrals: early intervention in psychosis service <14 day wait 98% Jun 100.0% 100.0% 0 →Routine referrals: community mental health team <28 day wait 98% Jun 98.2% 98.9% 0 ↓Crisis Referrals meeting <4 hour wait 98% Jun 100.0% 100.0% 0 →Routine referrals: Specialist Community Learning Disability Services <28 day 98% Jun 92.3% 100.0% 0 ↓Early Memory Diagnosis Service <6 week wait 90% Jun 48.0% 48.9% 0 ↓Referrals: 18 weeks for all mental health and learning disability services 98% Jun 99.1% 99.6% 0 ↓Number of people entering IAPT treatment 689 Jun 699 587 1,883 ↑IAPT Access (Prevalence 13% annually) 1.08% Jun 1.1% 0.9% 0 ↑
Emergency re-admissions to hospital within 30 days of discharge 8% Jun 5.0% 4.8% 0 ↑IAPT % clients moving towards recovery 50% Jun 50.1% 43.9% 0 ↑People with severe mental illness receive a list of physical checks (inpatients) 98% Jun 95.6% 97.3% 0 ↓Employment of people with mental illness 8% Jun 0.0% 0.0% 0 →
Access
Monitor
Safe & Effective

HPFT ׀
65
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
Referrals: Assessment waiting time standards - Crisis (4 Hours) 90% Jun 92.7% 86.2% 0 ↑Referrals: Assessment waiting time standards - P1 (7 days) 75% Jun 100.0% 100.0% 0 →Referrals: Assessment waiting time standards - Targeted service (14 days) 75% Jun 0.0% 0.0% 0 →Referrals: Assessment waiting time standards - Routine (28 DAYS) 75% Jun 68.2% 71.4% 0 ↓
Service users going through EMDASS who have been diagnosed with dementia None Jun 33% 0 1 ↑service users going through EMDASS who have been diagnosed with mild cognitive impairment None Jun 2% 1% 0 +Service users with dementia offered an end of life plan None Jun 62.9% 64.3% 0 ↑Service users with dementia with an end of life plan in place None Jun 2% 2% 0 +
No. Clostridium - Hospital Acquired (annual target) 2 annually Jun 0 0 0 →No. MRSA - Hospital Acquired 0 Jun 0 0 0 →
Sickness absence rate 4% Jun 5% 4% 0 ↓Staff turnover rate None Jun 15% 15% 0 ↑
Child and Adolescent Mental Health Services (CAMHS)
Dementia
HCAI
Workforce

HPFT ׀IAPT Comments ׀ IAPT Entry into Treatment The number of people entering IAPT treatment is below target across Hertfordshire. A new trajectory has been agreed with commissioners for both services. Additional promotional work and an assessment week resulted in June targets being achieved for E&N Herts and an increase in referrals for Herts Valleys. A comprehensive plan has been put in place to increase the number of referrals into the services. This includes allocation of surgeries to clinicians in each team to promote the service clinician to clinician; quarterly assessment weeks planned across the remainder of the year with targeted marketing to support these and on-going work on the analysis of sources of referral to support market intelligence. IAPT Recovery Rates A revised internal trajectory for E&N Herts for Q1 was set for 44.6% by HPFT and weekly performance management implemented which resulted in the service exceeding their revised target, although it is still below the 50% that needs to be achieved. Weekly monitoring of recovery rates will continue in addition, a proactive approach on following up Did Not Attends (DNAs) and close monitoring of data quality and recording. The service forecasts that it will meet the 50% recovery rate by the end of Q2.
66
-0.1%0.1%0.3%0.5%0.7%0.9%1.1%1.3%1.5%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Improving Access to Psychological Therapies (IAPT)
% Achieved Target 1.08% Linear (% Achieved)
0%
10%
20%
30%
40%
50%
60%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
IAPT % clients moving towards recovery
% Achieved Target 50% Linear (% Achieved)

HPFT ׀ Waiting Times Comments ׀ Routine referrals to Specialist Community Learning Disability Services meeting 28 day wait, Herts 33/34, ENCCG 12/13. There was one service user who was not seen within 28 days, due to patient choice in ENCCG. An earlier appointment was offered but declined by the service user. CAMHS referrals meeting assessment waiting time standards ROUTINE (28 DAYS) Herts 104/163, ENCCG 58/85. CAMHS 28 day waits fell to below 70% against a target of 75%. Performance in this area has been affected by demand and capacity issues in CAMHS clinics and has been particularly sensitive to changes in the use of agency staff. Considerable work has been carried out on improving the pathway and on reducing waiting times. As a result the underlying performance for new referrals waiting, improved significantly in June. The Trust have put forward a report for demand and capacity and have identified that they require 3 additional staff. This is currently being reviewed and shared by Hertfordshire County Council.
67
87%
89%
91%
93%
95%
97%
99%
101%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% Achieved Target 98%
64%
66%
68%
70%
72%
74%
76%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Assessment waiting time - Routine (28 DAYS) CAMHS
% Achieved Target 75%

HPFT ׀ Adults Comments ׀ People with Severe Mental Illness Receiving Physical Health Checks A key area for the commissioners was for HPFT to improve the physical health of people experiencing mental ill health in 2015/16, although considerable progress was made in 2014/15, there is further work to do. The target is easily effected by low numbers, April 17/17, May 36/37 and June 43/45. Patients who decline the health check have the ability to reconsider their decision at anytime. Actions The action plan put in place ensures staff offer a physical health check to all new patients.
68
100.00%
97.30%
95.56%
90%91%92%93%94%95%96%97%98%99%
100%
Apr-15 May-15 Jun-15
Physical Health Checks

HPFT ׀ EMDASS Comments ׀ EMDASS referrals meeting 6 week wait The performance fell to 48% for the quarter, a drop of 12.8% on the previous quarter, reflecting the increased numbers being referred into the service (508 referrals received in June 2015 compared with 215 in June 2014 and a total of 1,670 for the quarter). As at 7th September 232 people from E&N Herts were waiting for their initial appointment with EMDASS. Additional investment has been agreed for the EMDASS service and HPFT have recruited to these additional posts. This additional capacity will come onto stream from September and will result in weekly capacity increasing from 28 appointments a week to 50 appointments a week. A detailed action plan has been agreed with Commissioners and is in the process of being implemented.
69
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Early Memory Diagnosis Specialist Service
<6 weeks Target 90% Linear (<6 weeks)

HPFT ׀ Serious Incidents
Comments ׀ ENHCCG have acknowledged the continued progress in HPFT submitting finalised serious incident action plans and in the Trust providing examples and assurance about how learning has been implemented and being shared Trust wide. The Patient Safety Team sends out a serious incident position statement to the SBU which enables ongoing monitoring of cases in process and highlights where actions are required. This has, in turn, enabled older cases that were still open on STEIS to be closed. In Q1 17 SIs were reported across the organisation, 9 of which related to ENHCCG patients or services. Whilst the above graph is a breakdown of HPFT Serious Incidents relating to ENHCCG services and patients, the themes remain largely the same across the county. In Q2 to date the Trust has declared 7 SIs across the organisation, 1 of which relates to ENHCCG patients concerning on-going prescribing and administration of medication for service users within EMDASS East and EMDASS North teams. 70

HUC ׀
71
Description Target PeriodCurrent Period
Prior Period
YTD Actual
Movement
Urgent calls: definitive clinical assessment commenced within 20 minutes 95% Jun 92.8% 92.9% 0.0% ↓Routine calls: definitive clinical assessment commenced within 60 minutes 95% Jun 90.6% 85.1% 0.0% ↑
Urgent visits undertaken within 2 hours 95% Jun 91.4% 89.4% 0.0% ↑Routine visits undertaken within 6 hours 95% Jun 95.5% 93.4% 0.0% ↑
Urgent consultations undertaken within 2 hours 95% Jun 94.8% 82.1% 0.0% ↑Routine consultations undertaken within 6 hours 95% Jun 99.9% 99.3% 0.0% ↑
Urgent clinical assessment within 20 minutes of patient arriving 95% Jun 100.0% 100.0% 0.0% →Routine clinical assessment within 60 minutes of patient arriving 95% Jun 100.0% 90.3% 0.0% ↑
Percentage abandoned calls after 30 seconds 5% Jun 1.0% 1.0% 2.0% →Percentage answered within 60 seconds 95% Jun 96.9% 97.0% 97.4% ↓Percentage ambulance dispatches 10% Jun 7.6% 6.5% 6.7% ↓
Number of visits None Jun 1,226 1,089 3,565 ↑Number of routine cases None Jun 1,010 917 2,952 ↑Routine breaches None Jun 11 37 89 ↑Routine % achieved None Jun 99% 96% 0% ↑Number of urgent cases None Jun 201 154 553Urgent breaches None Jun 1 8 19 ↑Urgent % achieved None Jun 100% 95% 289% ↑
AiHVS
Out of Hours Telephone clinical assessment
Home Visits
Base face to face consultations following definitive clinical assessment
Base face to face walk in clinical assessment
NHS 111

HUC ׀Out of Hours & NHS 111 page 1 of 2
Comments ׀ Telephone Clinical Assessment A paper that outlines why NQR9 is no longer appropriate in a GP Out of Hours Service was to have been presented to ENHCCG directors, however, NHSE guidelines already exist that suggest that NQR need not be reported, as long as call backs in NHS111 are undertaken within 10 minutes. HUC are compliant with NQR9 as definitive clinical assessment has taken place in NHS111. 6.9% of patients to NHS111 are offered a call back, of these 70% are called back within 10 minutes, so 97.8% of patients receive a definitive clinical assessment within 10 minutes, thereby meeting the threshold of 95%. Nationally, this is one the best performances by a 111 provider. NHSE are reviewing datasets for integrated Out of Hours/NHS111 services over the autumn 2015 and more unified datasets and KPIs with guidance are expected. Actions A local stretch threshold for call backs will be agreed before the next CRM.
75%
80%
85%
90%
95%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Telephone Clinical Assessment (NQR9)
<20mins <60mins Target
72

HUC ׀Out of Hours & NHS 111 page 2 of 2
Comments ׀ Base Face to Face Consultations: urgent consultations undertaken within 2 hours and Home Visits Performance Both of these KPIs are affected by the same issues. June performance was affected by shift fill at weekends, which has improved but continued to be unstable in June and July. Although the service has trained GPs on the register HUC continues to experience difficulties filling shifts at weekends. There have also been issues around sickness rates with GPs calling in sick at late notice. Performance is expected to improve further once new pay rates begin in September. Shifts are advertised 3 months in advance. For September uptake of 66% was reported in the first week it was published. Actions 1. Monitoring of shift fill is taking place twice a week to ensure
maximum effort on HUCs part. 2. GP performance measures are now in place to monitor
sickness and lateness, these are also monitored through contract review.
3. HUC has begun to introduce new incentive schemes to encourage shift fill, such as only allowing GPs revised remuneration rates for bank holidays if they have worked consecutive shifts in previous months.
82%84%86%88%90%92%94%96%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Base Face to Face Consultations : urgent consultations undertaken within 2 hours NQR 12B
Urgent <2hrs Target Linear (Urgent <2hrs)
73
82%84%86%88%90%92%94%96%98%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Home Visits NQR12/F
<2 hrs <6 hrs Target

HUC ׀ Serious Incidents
74
Comments ׀ Performance In Q4 HUC declared 2 SIs across the organisation both of which related to ENHCCG patients. No SIs have been reported in Q2.

HUC ׀ Workforce Comments ׀ Performance: HUC are recruiting Call Handlers (now called Health Advisors nationally), but turnover means that this is an on-going process. The vacancy rate for these staff in June was over 35%. The position for Clinical Advisors has improved, with enhanced pay rates and some development opportunities offered. GP shift fill has improved, due to increased pay rates and the move to the summer rota. ENHCG is maintaining a focus on double shifts being worked by reception staff. Compliance against mandatory training continues at 100% for all staff groups, although we expect that to fall slightly as new starters join. The CCG Clinical Lead has advised that GPs working in the service will be expected to have a higher level of safeguarding children training in the future.
0%
5%
10%
15%
20%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staff Vacancy Rate
% vacancies Target <6%
Exception Report
75

Glossary Acronyms used in this report KPI Key Performance Indicators LAC Looked After Children MRI Magnetic Resonance Imaging MRSA Methicillin-resistant Staphylococcus Aureus PCR Patient Care Record OoH Out of Hours QRM Quality Review Meeting RCA Root Cause Analysis Red 1 life-threatening conditions where speed of response may be
critical in saving life or improving the outcome for the patient , for example - heart attack, trauma, serious bleeding.
Red 2 Serious but not the most life threatening RTT Referral To Treatment ROSC Return of spontaneous circulation SCG Specialist Commissioning Group STEMI ST segment elevation myocardial infarction SHMI Summary Hospital-Level Mortality Indicator SI Serious Incident SRG System Resilience Group TCI To Come In TDA Trust Development Authority TIA Transient Ischemic Attack WTE Whole Time Equivalent YTD Year to Date
Acronyms used in this report ENHCCG East and North Hertfordshire Clinical Commissioning Group ENHT East and North Herts NHS Trust PAH Princess Alexandra Hospital NHS Trust HCT Hertfordshire Partnerships Foundation NHS Trust EEAST East of England Ambulance Service NHS Trust HCT Hertfordshire Community NHS Trust HUC Herts Urgent Care WECCG West Essex Clinical Commissioning Group HVCCG Herts Valley Clinical Commissioning Group H&SM Hertfordshire and South Midlands A&E Accident and Emergency AIHVS Acute in Hours Visiting Service ALOS Average Length of Stay CCG Clinical Commissioning Group CARS Clinical Assessment Referral Service C-Diff Clostridium Difficile CNS Cancer Nurse Specialist CQC Care Quality Commission CQUIN Commissioning for Quality and Innovation CSR Community Service Review DH Department of Health ED Emergency Department EMDASS Early Memory Diagnosis & Support Service FFT Friends & Family Test GP General Practitioner HCAI Healthcare Acquired Infection HES Hospital Episode Statistics IAPT Increased Access to Psychological Therapies IPC Infection Prevention Control
76

1
Agenda Item No: 10.1
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Safeguarding Children, Looked after Children and Care Leavers Annual Report 2014/2015
Decision Discussion Information Follow up from last meeting
Report author: Beverly Mukandi, Deputy Designated Nurse
Safeguarding Children Beaulah Madziwa Chizimba, LAC & Care Leavers
Nurse Commissioning Carole-Anne Colford Designated Doctor Looked
After Children Report signed off by: Sheilagh Reavey, Director of Nursing & Quality
Purpose of the paper: The purpose of the report is to provide the Governing
Body with an overview of the safeguarding activity undertaken in 2014 – 2015 and outline areas requiring further development.
Conflicts of Interest involved:
None
Recommendations to the Governing Body:
The Governing Body is asked to receive the Annual Report.

2
Contents Item Page
1 Introduction 4
2 Local Context 5
3 CCGs Governance Arrangements 6
4 Health’s Participation in HSCB and Local Partnership Arrangements 6
5 Safeguarding Monitoring of Commissioning Services 6
6 Implementing CQC Recommendations 12
7 Looked After Children and Care Leavers 14
8 Safeguarding Children Priorities for 2015/16 19
9 Conclusion 19

3
Glossary of terms and abbreviations
CCG Clinical Commissioning Group CDOP Child Death Overview Panel CL Care Leavers CAMHS Child and Adolescent Mental Health Service CP-IS Child Protection Information Sharing CQC Care Quality Commission DfE Department of Education DHR Domestic Homicide Review ENHT East and North Hertfordshire Trust GP General Practice HCC Hertfordshire County Council HCT Hertfordshire Community Trust HPFT Hertfordshire Partnership Foundation Trust HSCB Hertfordshire Safeguarding Children Board IHA Initial Health Assessment LAC Looked After Children LSCB Local Safeguarding Children Board LA Local Authority LAC Looked After Children MASH Multi-agency Safeguarding Hub MARAC Multi Agency Risk Assessment Conference RHA Review Health Assessment SCR Serious Case Review SI Serious Incident SLAC Safeguarding and Looked After Children WHHT West Hertfordshire Hospital Trust

4
1. Introduction For the purposes of this report, East and North Herts and Herts Valley Clinical Commissioning Groups will be referred to as the “CCGs”. This is the CCGs second year Safeguarding Children and Looked After Children (LAC) and Care Leavers Report. The purpose of this report is to provide East and North Herts and Herts Valley CCGs with the assurance and information regarding compliance with safeguarding children arrangements and duties as per section 11 of the Children Act 2004, Working Together to Safeguard Children 2013 (updated March 2015) and the Accountability Framework 2013 (updated July 2015). This report covers the period April 2014- March 2015. 2014/2015 key achievements Last year’s annual Safeguarding Children Report set out 6 priorities for the year: • A review and update of the Safeguarding Children Training Strategy will be carried
out Achieved – the training strategy was reviewed and is line with the Intercollegiate Document 2014
• Implementation of the service model recommended by the Looked After Children
review Achieved – new LAC model went fully live end July 15
• Ensuring that Service Level Agreements are in place with all organisations providing Designated Professional functions Partially achieved – Formal agreements with providers are being finalised to ensure effective governance arrangements and delivery of the Designated Professional functions.
• CQC recommendations (2013 Review) Partially achieved – Four areas remain amber with full compliance expected by all providers by December 2015.
• Develop a more robust process to link and cross-reference learning from the Child
Death Overview, Rapid Response, Serious Incident and Serious Case Review processes Partially achieved – Child Death Overview and Rapid Response processes review completed. Work to review health’s SCR processes has been instigated and is progressing.
• The quality schedule of all contracts will include an outcome based section (KPIs
and metrics) on Safeguarding and Looked After Children Achieved

5
2. Local Context The East and North Hertfordshire and Herts Valley Clinical Commissioning Groups (CCGs) commission health services for almost 250,000 children and young people across Hertfordshire. The CCGs share co-terminus boundaries with the Local Authority which supports a mutual focus on the welfare of children. Table 1 and table 2 highlights the number of children in Hertfordshire subject to the Child Protection Plan, table 3 highlights the number of children in Hertfordshire by District Councils.
Table 1 - Number of children subject to Child Protection Plan by category
Neglect Emotional Abuse
Sexual Abuse
Physical Abuse Multiple
Q1 14/15 644 375 32 23 2 Q2 14/15 672 350 29 10 4 Q3 14/15 703 311 30 8 1 Q4 14/15 627 221 18 12 3 Data Source:
LCS 2646 1257 109 53 10 4075
Table 2 - Number of children subject to Child Protection Plan by age
Unborn Under 1 1 to 4 5 to 9 10 to 15 16+
Q1 14/15 53 154 288 337 230 14 Q2 14/15 50 155 297 332 220 11 Q3 14/15 60 147 304 320 203 19 Q4 14/15 59 125 241 262 180 14 Data Source:
LCS 222 581 1130 1251 833 58 4075
Table 3 - Number of children subject to Child Protection Plan by District Council District (Primary Postcode) Q1 14/15 Q2 14/15 Q3 14/15 Q4 14/15 Broxbourne 87 87 96 75 Dacorum 144 135 121 122 East Hertfordshire 73 70 51 44 Hertsmere 88 74 79 77 North Hertfordshire 96 86 92 69 St. Albans 116 106 106 83 Stevenage 132 126 102 97 Three Rivers 79 71 66 65 Watford 104 123 129 92 Welwyn Hatfield 113 133 134 92 Out of County/Unknown 44 54 77 65 Total 1076 1065 1053 881
Data Source: LCS

6
3. CCGs Governance Arrangements
The CCGs hold a statutory responsibility for ensuring that the health contribution to safeguarding and promoting the welfare of children is carried out effectively. CCGs are required to employ or have in place a contractual agreement to secure the expertise of Designated Professionals to provide senior strategic leadership across the health economy. The Designated roles are defined in the statutory guidance ‘Working Together to Safeguard Children’ (HM Government 2015). The CCGs have access to a safeguarding and LAC team made up of the following staff:
• Designated Safeguarding Children & Looked After Children Nurse • Deputy Designated Nurse Safeguarding Children • Looked After Children & Care Leavers Nurse Commissioning • Designated Doctor for Safeguarding Children (4 PAs) • Designated Doctor for Child Death (2 PAs) • Designated Doctor for Looked After Children
To ensure compliance with section 11 of the Children’s Act 1989, the CCGs have to ensure the staff they employ are trained, knowledgeable and competent in safeguarding children. For the reporting period Herts Valley CCG’s training compliance for level one training1 was 81.3% and East and North Herts CCG’s level one compliance was 85.5%, this is below CCG internal target of 90%. Steps have been put into place to bring about the necessary improvement; these include working with HR to produce quarterly reports on training uptake by CCG staff.
4. NHS England
NHS England is responsible for ensuring that the health commissioning system as a whole is working effectively to safeguard and promote the welfare of children and adults. It is accountable for the services it directly commissions including general practice and health visiting. (From October 2015 commissioning responsibility for health visiting will transfer to the local authority). NHS England leads and defines improvement in safeguarding practice and outcomes. The CCGs work co-operatively and constructively with NHS England to fulfil their safeguarding statutory duties.
5. Hertfordshire Safeguarding Children Board (HSCB) The Hertfordshire Safeguarding Children Board is the key statutory mechanism for agreeing how organisations co-operate to ensure effectiveness of what they do. The full engagement of health agencies in the work of the HSCB is a key section 11 responsibility of the CCGs. 5.1 Health’s Participation in HSCB and Local Partnership Arrangements The CCGs and all of their NHS partners are fully committed to safeguarding children and take their responsibilities seriously in order that they fulfil their statutory duties, as
1 Level 1 safeguarding children training provides a baseline understanding of safeguarding principles and practice.

7
outlined in Section 11 Children Act 2004 and Working Together 2013 (updated July 2015). Assurances have, and continue to be provided to the HSCB by the submission of the annual Section 11 Audits, which illustrate the quality of safeguarding children practice in provider organisations. The CCGs have a statutory requirement to be a partner member of the HSCB. The Directors of Nursing attend the Board as the CCGs representatives. The Designated Doctors and Designated Nurse are professional advisors and attend to provide expert advice related to the health aspects of child protection and safeguarding children. There is also Director representation at the HSCB from all CCG commissioned NHS providers who are also represented at the HSCB sub-groups. The Designated Professionals are members of HSCB Serious Case Review Panel. The Designated Nurse is a member of the Child Death Overview panel subgroup and also chairs the Learning and development subgroup. The CCGs together contribute £124,360 to the work of the HSCB. The CCGs also make a significant additional contribution through the work undertaken by Designated Professionals. Such work includes Chairing and contributing to the work of Board subgroups; leading and contributing to multi-agency audits and peer reviews as well as providing the health perspective into serious case reviews and learning reviews. 5.2 Serious Case Reviews (SCR’s) Partnership Reviews (PCR) HSCB recognises the importance of learning lessons from cases where failures in partnership working have resulted in adverse outcomes for a child. The CCGs have a statutory duty to work in partnership with HSCB and/or any other Safeguarding Children Board in conducting Serious Case Reviews and other case reviews in accordance with Working Together to Safeguard Children 2013 (updated 2015). When a child dies or is seriously harmed from abuse or neglect or there are concerns about how professionals worked together to protect the child, the LSCB responsible for child protection conducts a review to identify how local professionals and organisations can improve the way they work together. The CCGs designated professionals coordinate and evaluate the health services inputs into the SCR and provide professional scrutiny and challenge. The CCGs must ensure that the review and all actions following the review are carried out according to the timescale set out by the SCR panel. During the reporting period, seven cases were discussed at the SCR panel with two cases progressing to SCR and with one case still pending. The remaining cases did not meet the SCR threshold. During the period of this report two SCRs were published, child B and child X. Child B 17 year old girl who committed suicide whilst in a Mental Health Unit, there were 2 recommendations for health providers:

8
1. There should always be consideration of the need to make contact with Hertfordshire Children’s Services when a young person presents with significant mental ill-health, especially in relation to self-harming and where there are concerns about the impact the family dynamics may have on the young person in terms of any risk or protective factors. This contact should include information gathering and discussion about whether there is a need to make a referral and how a full psychosocial assessment can be undertaken.
HPFT’s action: Developed the Crisis Assessment and Treatment Team (CCATT), operating in both East and North Herts Hospital NHS Trust and West Herts Hospital NHS Trust A&E departments 9am-9pm Monday to Friday.
2. It is important that A&E departments record decisions and recommendations
made in respect of a young person’s attendance with mental health issues, to ensure records are available to support future treatment decisions and for reference if there are repeat A&E attendances.
West Hertfordshire Hospital Trust’s action: compliance was audited in April 2015 with satisfactory results, re-audit will be undertaken to ensure compliance continues. East and North Hertfordshire Hospital Trust’s action: compliance was audited in May 2015 with satisfactory results, re-audit to be completed in October 2015.
Child X child killed by her father there was one recommendation for GPs. Hertfordshire LSCB should monitor the way in which the learning points for GPs identified in this review will be addressed by NHS England, Hertfordshire and South Midlands Area Team.” This ‘learning point for GPs’ is that “safeguarding training for GPs should encourage safe, accurate, precise record keeping with use of codes. NHSE/CCGs action: A record keeping update was undertaken in 2014, a re-audit to be undertaken by end of 2015. 5.3 Developing Multi-Agency Working The HSCB have been undertaking work to develop and improve multi-agency communications and working within Hertfordshire. 5.4 Multi-Agency Safeguarding Hub (MASH)
The Local Authority has worked with the CCGs; Police; Probation and partner agencies to develop the MASH. The MASH involves the co-location of a range of agencies who share pertinent information at the point of first contact to help inform decisions about safeguarding and risk to children. This is a significant achievement in Hertfordshire. Despite an initial slow start MASH went live end July 2015 The CCGs have commissioned two health practitioners to be core members of the MASH team and have made a financial contribution to the role of the Service Manager. 5.5 Child Protection Information Sharing (CP-IS)

9
The Child Protection Information Sharing (CP-IS) is a joint health and social care national initiative giving the NHS a higher level of protection to children who visit unscheduled care settings such as emergency departments, walk in centres, minor injury. The secure web system allows access by appropriate heath staff to a cohort of children who are subject to a plan or who are looked after children. This is an important initiative as previous serious case reviews have demonstrated that abusive and neglectful parents can mask this behaviour by moving between different healthcare services. CP-IS was rolled out in Hertfordshire in early April 2015. 5.6 Child Sexual Exploitation (CSE) Whilst CSE is receiving a high level of media attention it can remain a hidden problem. Recently there have been several high profile cases in Oxford and Rochdale involving groups of men sexually exploiting vulnerable young girls. In July 2012 the government published a ministerial statement following the publication of two reports pertaining to sexual exploitation of children in gangs and groups of children going missing from care. The HSCB directed that a CSE strategy be established to tackle the issue and manage risks to vulnerable young people who go missing, are sexually exploited or trafficked. There is an associated action plan which all partner agencies are signed up to. The functions and actions of e-safety and the SEARCH Strategic Group have been consolidated into a new sub-group, the Strategic Safeguarding Adolescents Group (SSAG), the Designated Nurse will represent health on this subgroup. 5.7 Domestic Abuse and the Impact Upon Children The impact that domestic abuse has upon children is widely known and well researched. The CCGs Safeguarding Team receives domestic abuse notifications from the police for all cases where there is child under the age of 5. Between April 2013 and March 2014 there were 4935 notifications for children under the age of 5 received by health from the police, this is an increase from 4009 for 2013/2014 period.

10
Table 4
A domestic homicide review (DHR) undertaken in 2014 following the murder of a 19 year old girl (AA) who had an under 5 year old child by her partner. The DHR was published in January 2015, there was one recommendation for Hertfordshire Community NHS Trust (HCT). Hertfordshire Community NHS Trust should ensure health visitors carry out screening for domestic abuse in line with their existing best practice guidance. Alongside the DHR recommendations, Hertfordshire Community NHS Trust, East and North Hertfordshire Hospital Trust and Hertfordshire Partnership Foundation NHS Trust identified recommendations as part of their IMR process. Completion date for all recommendations is December 2015. Progress is monitored through their safeguarding committees. 5.8 Multi-Agency Risk Assessment Conference (MARAC) MARAC is a process where a group of representatives from a number of agencies meet on a regular basis to share information about individuals who are considered to be at ‘high risk’ of homicide or serious harm. The aim of these meetings is to provide a forum for sharing information and taking action to reduce future harm to very high-risk victims of domestic abuse and their children. The Deputy Designated nurse for safeguarding sits on the MARAC steering group. 5.9 Child Death Overview Panel (CDOP)
Apr-Jun July-Sept Oct-Dec Jan-Mar
Dacorum 147 138 148 143Hertsmere 98 79 103 91North Herts & Stevenage 261 264 287 336RBS 9 10 8 13SE Herts 211 220 234 217St Albans & Harpenden 85 83 111 131Watford & 3 Rivers 216 231 204 217WCG & Hatfield 159 154 159 168
0
50
100
150
200
250
300
350
400DA notifications to HV Totals for 2014/15
Dacorum
Hertsmere
North Herts &StevenageRBS
SE Herts

11
The HSCB is responsible for ensuring that review of each death of a child normally resident in the Hertfordshire area is undertaken by the CDOP. The panel is chaired by the Deputy Director of Public Health. The functions of the CDOP include: • reviewing all child deaths up to the age of 18, excluding those babies who are
stillborn and planned terminations of pregnancy carried out within the law • collecting and collating information on each child and seeking relevant information from professionals and, where appropriate, family members • discussing each child’s case, and providing relevant information or any specific actions related to individual families to those professionals who are involved directly with the family so that they, in turn, can convey this information in a sensitive manner to the family • determining whether the death was deemed preventable, that is, those deaths
in which modifiable factors may have contributed to the death and decide what, if any, actions could be taken to prevent future such deaths
• making recommendations to the LSCB or other relevant bodies promptly so that action can be taken to prevent such future deaths where possible Between March 2014 and April 2015 a total of 45 cases were reviewed by the panel. There were no consistent trends identified from these deaths, there were 18 neonatal deaths (only 3 had modifiable factors), 14 deaths due to life limiting illness, 6 sudden unexpected infant deaths, 1 drowning 1 homicide, 1 suicide and 3 deaths listed as other for cause of death. The most common cause of child deaths for 2014/2015 was neonatal deaths, a more detailed CDOP report will be published in the Autumn 2015. 5.10 Rapid Response to a Child Death The rapid response team in Hertfordshire is led by Hertfordshire Community Trust (HCT), and they respond to every unexpected child death in Hertfordshire under the guidance of a multi-agency protocol. The nature of the process is twofold, a forensic investigation of the child death, and also supportive in that it ensures a bereavement plan is in place for the family. The table below illustrates the figures for the rapid response team for last 2 years. Table 5
2013/2014 2014/2015
Total number of unexpected child deaths reported to team
25
23
Number of unexpected child deaths managed as a Rapid Response
21
16
Deaths under 1-year of age 6 8 6. Safeguarding Monitoring of Commissioned services

12
Through monitoring of commissioned Services, the CCGs gain assurance that staff across all NHS provider organisations safeguard and protect children at risk of harm and ensure that processes are in place to support practitioners to respond to concerns. The providers are performance managed via Quality and Contract meetings and through monitoring of Service Level Agreements and Contract Schedules through Quality Committees;
In addition the following arrangements are in place to strengthen the CCGS’s assurance processes: • The Designated nurses are members of each providers trust’s internal safeguarding committees • Annual NHS provider section 11 visits with scrutiny of the self-assessment tools, followed by Section 11 dip sample audits • All Serious Incidents regarding safeguarding children are notified to the Safeguarding Children Team. • Supervision of provider Named Professionals by Designated Professionals • Monitoring and reviewing action plans from SCR’s DHR’s and other pertinent reviews • Commissioned health providers safeguarding children performance data is
collected quarterly via a dashboard which is part of the quality schedule, enabling the Designated team to monitor the quality of services and activity trends.
• In 2014/15 providers were also required to demonstrate compliance with the CQC action plan and this was monitored through CCG led Task and Finish groups.
6.2 Challenges in monitoring commissioned services 2014/2015 • Supervision to Named professionals not provided as should be by the Designated
professionals due to sick leave in the team. 2015/2016 Designated Professionals now providing supervision to all Named professionals.
• Provider organisations not meeting the 95% training target compliance across level ;2 and 3. 2015/2016 Designated office will monitor provider’s training quarterly via the dashboard and providers safeguarding committees to address poor compliance.
• Safeguarding Children dashboard not fully functional. 2015/2016 functionality complete and being monitored by Designated office.
6.3 Areas of good practice • Introduction of s11 dip sample audits • Good working relationship between the Named professionals and Designated
professionals now established through the Whole System Safeguarding Children Named professionals meeting
6.4 Single Agency Training The CCGs routinely seek assurance that the services they commission have competent, skilled workforces who are able to respond to the safeguarding needs of children. Provider organisations report training compliance to their safeguarding committees, quarterly to the CCGs via the dashboard and at quality review contract meetings.

13
The CCGs has safeguarding children standards in every contract and the providers are expected to achieve at least 95% compliance across levels one, two, three and four safeguarding children training. The table below highlights the trend in each organisation’s training compliance across all levels during the reporting period. Table 6 Provider Safeguarding Training Uptake HPFT HCT ENHT WHHT Q1 Q2 Q3 Q
4 Q1
Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Level One
92%
78%
80%
83%
87% 83%
85%
87%
91%
84%
84%
86%
85%
Level Two
93%
90%
97%
98%
99%
96% 81%
83%
86%
90%
80%
81%
83%
90%
Level Three
88%
93%
95%
100%
66%
65%
75%
71%
71%
68%
73%
91%
During the reporting period HFPT, did not report on their level three training compliance and for quarters two, three and four the level one and level two training was recorded as a single level. During the next reporting period the CCGs will closely monitor HPFT’s training activity to ensure ongoing compliance. ENHT have been challenged on their Level 3 training compliance, early 2015/2016 figures shows an improvement from 71% to 79%. The Trust has an action plan in place to meet the 95% training target compliance which is being monitored closely by the Designated Nurse via the Dashboard and the Trusts safeguarding committee. NHS England is responsible for ensuring GP’s and other primary care professionals’ access safeguarding training as part of their performance monitoring responsibilities.
6.5 Implementing CQC Recommendations
The CQC undertook a Review of Safeguarding Children and Looked After Children activities within Hertfordshire in November 2013. They made 37 recommendations as outlined in last year’s Annual Safeguarding Children Report. To ensure robust monitoring of the recommendations, a Task and Finish group was set up. The group met six weekly. Due to changes in the safeguarding teams within Provider organisations, there was a slow start in implementing the CQC action plans. The action plan has since made reasonable progress. Training compliance remains outstanding for ENHT, WHHT and HPFT. HPFT have two areas where action has been taken but the impact of these requires assessment.
• Ensure that management oversight and supervision arrangements in adult mental health services and CAMHS are robust in ensuring practice is compliant with national guidance and demonstrates continuous improvement.

14
• Ensure that the needs of young people are fully reflected in CAMHS assessments and that young people have an opportunity to be seen alone when they are competent to choose.
Action plan to be fully completed by December 2015. 7. Looked After Children and Care Leavers (LAC) 7.1 Background and Statutory Responsibilities Looked After Children and young people share many of the same health risks and problems as their peers, but often to a greater degree. Generally they have worse levels of health on entry to the care system and poorer longer term outcomes. (Statutory Guidance on promoting the health and wellbeing of Looked After Children, DCSF, 2009). Neglect and chaotic family circumstances may mean that children’s basic health needs have not always been met consistently before coming in to care. The prevalence of emotional, behavioural and mental health difficulties is greatly increased in the LAC population, often as a long term consequence of abusive experiences. East and North Herts CCG and Herts Valley CCG have the statutory responsibility for the commissioning of health services for Hertfordshire’s Looked After Children from 1st April 2013. Both CCGs are also the responsible commissioner for Hertfordshire children who are placed outside the county. The LAC and Care Leavers Health service is jointly commissioned by the CCGs and Hertfordshire County Council for social care. The CCGs take the lead on the commissioning of the provision and co-ordination of the LAC health assessments 7.2 Local Context The numbers of children in care, placed out of County and care leavers remain relatively consistent. In addition, there are 231 Care leavers (16 -18 years of age). Table 7 The age of the Looked-after cohort in Hertfordshire as of 31 March
for the given year Year Under 1 1-4 5-9 10-15 16 + Total LAC 2012 55 175 180 370 275 1055 2013 60 169 184 359 265 1037 2014 50 159 183 352 297 1041 2015 54 141 200 346 283 1024
CLA Source: SSDA903 7.3 Performance Indicators National performance indicators are produced in partnership with Hertfordshire Children’s Services. Data for health assessments is collected by the Department for

15
Education (DfE) annually for all children looked after for a year or more on the 31st March. These figures do not reflect the actual workload as all children taken into care require an Initial Health Assessment (IHA) within 28 days of entering care, and there are children entering and leaving care throughout the year. 7.4 Comparative Data These are the SSD 903 returns provided by Hertfordshire County Council to the Department for Education. It reports on the percentage of children looked after for 12 months or more who have had dental and health checks within the last financial year. Table 8 Indicator
Herts 12/13
Herts 13/14
Herts 14/15
% LAC who had annual Health check 87.5
79.1
81.5
National Average % 87.0 88.0 Below national average
% LAC who had annual dental check 84.2
82.4
80.0
National Average % 82% 84.0
Below national average
% LAC with Immunisations up to date 91.7
90.5
88.8
National Average % 87.0 83.0
Above national average
7.5. Health Assessments There are two different timescales in place for providers when completing Health Assessments: • IHA (Statutory) must be completed within 28 days of a child coming into care. • RHA is required every 6 months for children under 5 years and annually
thereafter. 7.5.1 Performance against IHA statutory 28 day time frame: Table 9 Number of requests received within 1 week entering care 80

16
Number of requests received within 28 days entering care 272 Number of IHA’s completed within 28 days entering care 49 % IHA’s received and completed within 28 days entering care 18
The percentage completion within the 28 days statutory timeframe is disappointingly and unacceptably low and well below CCG comparator authorities. Although it should be noted 14/15 achievement was an improvement on the 13/14 figure which was 1.04%. Performance in 2015/2016 has improved further with introduction of the new model and currently stands at 38%. 7.5.2 IHA – Provider Performance Health providers are allocated 10 working days to return completed health assessments to the LAC health team to meet these statutory requirements (see Appendix One). Children under 10 years or those with complex needs attending specialist schools are seen by community paediatricians from either HCT or East and North Herts NHS Trust (ENHT). Children and young people age 10-18 are seen by GPs. For those children who are difficult to engage the LAC Nurse Team will undertake the IHA. Table 10 Provider Performance against allocated 10 day timescales
PROVIDERS
2014/2015 N
o of
HA
's R
equi
ring
Com
plet
ion
No
Ret
urne
d w
ithin
Ti
mes
cale
s
% C
ompl
eted
With
in
Tim
e Sc
ales
E&N Herts Paeds 99 49 49 HCT Paeds 82 53 65 Out of County Paeds 26 1 4 GP E&N Herts 76 9 12 GP West Herts 73 7 10 Adoption Advisor E&N Herts 13 5 38 Adoption Advisor West Herts 26 20 77 GP Out of County 29 1 3 Herts LAC Health Team Nurses 6 4 67 LAC Nurses out of County 19 0 0 Total 449 149 33
7.5.3 Review Health Assessments (RHA)
RHAs to be completed by providers within 5 weeks of receipt of health assessment request from HCC by LAC health team (see Appendix Two). RHA’s are undertaken

17
by the health visitor or school nurse. Care Leavers (age 16-18yrs) are seen either by their GP or the LAC Nurses. Table 11 Provider Performance against allocated 5 weeks (35 days) timescales:
PROVIDERS
2013/2014 2014/2015
No
of H
A's
Req
uirin
g C
ompl
etio
n
No
Ret
urne
d w
ithin
Ti
mes
cale
s
% C
ompl
eted
With
in T
ime
Scal
es
No
of H
A's
Req
uirin
g C
ompl
etio
n
No
Ret
urne
d w
ithin
Ti
mes
cale
s
% C
ompl
eted
With
in T
ime
Scal
es
Paediatrician - East & North 44 21 48 50 40 80 Paediatrician - West 20 9 45 14 7 50 Paediatrician - Out of County 7 1 14 5 0 0 General Practitioner - East & North 2 1 50 1 0 0 General Practitioner - West 3 0 0 1 0 0 General Practitioner Out of County 26 7 27 43 8 19 Adoption - East & North 108 59 55 82 64 78 Adoption - West 113 34 30 118 78 66 Adoption - Out of County 7 1 14 10 4 40 Health Visitors - East & North 4 2 50 3 0 0 Health Visitors - West 12 0 0 4 3 75 School Nurses - East & North 41 20 49 0 0 0 School Nurses - West 64 33 52 0 0 0 School Nurses - Out of County 10 2 20 5 2 40 CUS LAC Nurse 157 87 55 276 198 72 Herts LAC Nursing Team 109 87 80 107 89 83 LAC Nurses - Out of County 91 8 9 94 17 18 Total 818 372 45 813 510 63
37 % of RHAs completed by health providers missed the 5 week (35 days) timescale by between 1- 200 days. In order to bring about improvements to the timescales and quality health assessments, a number of actions were employed by the CCG and its partners in health and social care:
• A joint partnership approach to meeting the 28 day national timescales for health assessments across health and Children’s’ Services was introduced to ensure a shared responsibility for outcomes.

18
• A single pathway referral system within the Children’s’ Services Brokerage Team for all initial health assessments was established to improve timescales and improve the interface between the LAC Health Team in HCT and Children Services.
• Achievement of the 10 working days timeframe has been added to all relevant providers Quality Schedules.
• Fostering of stronger engagement from Community Paediatric teams in HCT and E&N NHS Trust, standardised clinic provision and stronger contract monitoring.
• A new GP Service Model was commissioned and implemented in July 2015 to support the IHA pathway and build additional resilience. It is anticipated that this new delivery will further improve the performance. The evidence of impact will be seen from July clearance rates onwards
• Formation of LAC leadership group to drive forward the LAC agenda and improve health outcomes.
• Formal LAC contract monitoring meetings with all commissioned providers to ensure that providers meet their target performance and therefore improve overall performance against national timescales.
• Strengthening of escalation processes within and across partner organisations to ensure a rapid response to identifying risks and mitigating them.
• Quarterly deep dive audits by providers and the CCGs to review the quality of health assessments with the aim of improving the health outcomes for Looked After Children in Hertfordshire.
With these measures implemented, the early 2015/16 performance against timescales and quality of health assessments is showing consistent improvement each month and remains a key priority for the CCG and its partners. 7.6 Data Collection and Health Outcomes The CQC review in 2013 recommended that the CCGs improve their awareness of the health needs of LAC. As a result during the reporting period a LAC Health Dashboard and Health Data Diagnostic Template was created for SystmOne users. A sample deep dive looking at the individual health needs of LAC in Hertfordshire using SystmOne information system was completed in March 2015 and a number of health needs were highlighted. (See Appendix Three) 7.6.1 Challenges within Safeguarding Children and LAC Team during 2014 – 2015 Due to long term sick leave the team has had at times to function using interim staffing arrangements which inevitably did cause a level of instability. The situation was managed and mitigated by close oversight from the senior team. The post of Deputy Designated nurse has now been recruited to substantially. This impacted on the delivery of objectives described in section 1.

19
In addition there were changes within the safeguarding teams for all statutory healthcare providers which resulted in the slow implementation of the CQC action plan and was a risk for the system. 7.6.2 LAC Priorities for 2015/2016 • To ensure a step change in performance against timeliness for the completion
of both Initial and Review Health Assessments. • To work with Hertfordshire Children Services and health providers to ensure a
full dataset for attendance at dental appointments and immunisations are captured accurately.
• To work with Hertfordshire Children Services and health providers to ensure that Hertfordshire LAC have their emotional and mental health needs adequately assessed and timely support given through the SDQ process.
• To monitor the “You are Welcome” status of LAC providers and the results of audits and feedback from LAC and carers regarding service(s) received to ensure that their
experiences are routinely sought and used to improve services. 8. Safeguarding Children Priorities for 2015 – 2016 • Review the 3 year Safeguarding Strategy • To further strengthen provider quality monitoring systems and processes as part of
the quality and patient safety agenda
• To ensure that there is the same level of performance monitoring for General Practice Out of Hours Services (HUC)
• To evidence the impact of learning from serious case reviews across the health economy
• To review current Female Genital Mutilation activities and identify gaps developing a time limited action plan as appropriate
• To review current CSE activities and identify gaps developing a time limited action plan as appropriate
• Ensure all CQC actions are completed 9. Conclusion
Whilst there were notable health and social care system achievements in 2014/15 including the newly commissioned GP led LAC Initial Health Assessment Service and the ‘going live’ of the MASH; there remains a number of key challenges for both the Safeguarding and LAC Team and health and social care system going into 2015/2016. These challenges are clearly outlined in the CCG priorities for 2015/16 and will require effective partnership working across the whole health and social care economy if we are to continue to support our most vulnerable children.

20
Appendix One

21
Appendix Two

22
Appendix Three:
DIAGNOSTIC CATEGORY NUMBER % Allergic Disorder 49 2.2 ADHD 46 2.0 Autistic Spectrum Disorder 65 2.9 Bipolar disorder 2 0.1 Cerebral Palsy 20 0.9 Childhood Asthma 27 1.2 Congenital Heart Disease 8 0.4 Cystic Fibrosis 3 0.1 Depressed Mood 11 0.5 Disorder of Hearing 42 1.9 Epilepsy 32 1.4 Metabolic disorders 4 0.2 Ophthalmological disorder 119 5.3 Other Nervous System Disorder 0 0 Self-injurious behaviour 4 0.2 Sickle Cell Anaemia 1 0.0 Thalassaemia 0 0 Thyroid disorder 0 0 Type I Diabetes 6 0.3 Type II Diabetes 2 0.1 BMI > 98th Centile under 16 yrs 29 1.3 BMI > 98th Centile all ages 184 8.1 Smoker under 16 yrs 13 0.6 Smoking cessation under 16 yrs 2 0.1 Smoker > 16 yrs 256 11.3 Smoking cessation 29 1.3 C Card issued 52 2.3 Chlamydia Screen < 16 yrs 3 0.1 Chlamydia Screen >16 yrs 54 2.4 Pregnant < 18 yrs 10 0.4 Pregnant > 18 yrs 53 2.3
LAC & CL Health Team – Health Outcome KPI Data from SystmOne
(as of 17th March 2015)

1
Agenda Item No: 10.2
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Safeguarding Adults Annual Report
Decision Discussion Information Follow up from last meeting
Report author: Tracey Cooper
Report signed off by: Sheilagh Reavey
Purpose of the paper: To provide the Governing Body with an overview of adult
safeguarding for 2014 – 2015.
Conflicts of Interest involved:
Recommendations to the Governing Body:
For information

2
Introduction
The purpose of this Annual report for 2014 - 2015 is to assure the committee of the progress the CCG has made in relation to adult safeguarding and outline the priorities for 2015/16. It will also provide assurance that the Head of Adult Safeguarding is actively leading the delivery of ENCCG safeguarding adult responsibilities and will inform the committee of any gaps and the measures being taken to address these. Head of Adult Safeguarding
The key areas of focus of the Adult Safeguarding work programme for 2014 – 2015 included;
• Developing a CCG strategy, to set out the CCGs priorities and deliverables for adult safeguarding • Provide General Practice adult safeguarding education • Monitoring and reporting on provider’s safeguarding adult activity and performance • Leading the health aspect of adult safeguarding investigations • Leading the agenda on domestic abuse
Hertfordshire Safeguarding Adult Board (HSAB)
The Care Act 2014 places safeguarding Adults Boards on a statutory basis, similar to Safeguarding Children Boards, and will require each Board to produce an Annual Report in consultation with their local community/ies which will have to be presented to specified bodies, including the local authority and the local Health watch, as part of a process of scrutiny and accountability.
The eighth and final HSAB Annual Report to be written in its current format was published in October. The report contained the recently agreed Strategic Objectives which formed the basis of a new three year Business Plan, 2014/17 which had been developed by statutory partners. The HSAB is compliant with the Act.
In January the HSAB participated in a topic scrutiny session with members of the County Council including the CCG Director of Nursing & Quality and the Head of Adult Safeguarding. The table below sets out a number of observations and recommendations which were made following this process. These will be monitored by the Scrutiny Committee of the County Council and reported to the HSAB.
Recommendations:
Outcomes/further action:
• To be kept informed of progress in
implementing the Care Act requirements and the financial situation of the board.
• To be advised of the outcomes of the HSAB
Away Day on 24 April.
• For the Independent Chair of the HSAB to
action
• For the Independent Chair of the HSAB to action

3
• That a scrutiny of HSAB becomes an annual
scrutiny, mirroring that of the HSCB, commencing in June/July 2016.
• To provide members with a structure chart
of HSAB showing how members and activities fit together.
• For HCC Head of Scrutiny to implement and
provide the HSAB with an outline of the programme in advance
• For the Independent Chair of the HSAB to
action
A statutory Strategic Safeguarding Adult Board has been established made up of the core membership identified in the Care Act legislation. This board will provide direction to the Safeguarding Adults Operational Board. The CCG is represented on both of these boards. In February 2015 the Hertfordshire Safeguarding Adult Board (HSAB) successfully recruited an Independent Chair for a one year term that commenced in March and agreed the funding of the boards activities for the year. Serious concerns The Head of Adult Safeguarding working in partnership with the Local Authority Head of Adult Safeguarding reviewed the serious concerns process of the HSAB multi-agency policy and produced a draft version. A work shop was then held with key partners and the CCG was represented by the Director of Nursing & Quality and the Heads of Adult Safeguarding and Quality Improvement. Following the workshop the Head of Adult Safeguarding produced a further version of the serious concerns process which was agreed at a second workshop. The new policy has now been signed off by the HSAB. The following are systems and processes developed as part of the serious concerns process to monitor quality, contract compliance and to support provider improvement. Improving the quality of care needs to be addressed on three fronts.
1. Preventative activity: Developing a care and support market economy that delivers care to required standards.
2. Pro-active work: Supporting improvements and raising standards through identifying and tackling emerging concerns in the quality of care and support.
3. Responsive work: Collaborative and assertive approaches to managing concerns when the care provided by a service to adults who are at risk of harm is causing them to experience, or be at risk of, abuse or neglect.
This process is used for services which are regulated by the Care Quality Commission (CQC) and for care and support services that are not regulated but provide a service to adults at risk of harm, for example day services.
The process applies to both health and social care provision; it includes concerns about NHS providers, independent hospitals, and services directly delivered by HCC.

4
The serious concerns process provides an overarching framework which will ensure a coordinated response with:
• All aspects of the investigation planned • Organisations and individual professionals clear about their respective roles and responsibilities
There have been 6 care homes within East & North subject to the Serious Concern Process in 2014-2015 Appendix 1 outlines some of the issues and interventions that form the basis for the Serious Concerns investigations. Providers are required to produce and implement an action plan which is monitored by CCG, CQC and HCC staff. The reduction in the numbers is due to work described earlier and will be followed up through the Strategic Quality Improvement Group which has been formed by the Head of Adult Safeguarding and Head of Quality Improvement in partnership with colleagues from the Local Authority, Police and Care Quality Commission. The purpose of this group is to establish and maintain a multi-agency coordinated approach to the safeguarding and quality agendas to support the commissioning of care home and home care services across Hertfordshire. The group is chaired by the Head of Adult Safeguarding and the objectives of the group are:
1. To develop and implement a proactive partnership approach to strategic quality monitoring which is based upon benchmarking and clinical evidence.
2. To provide an oversight of the care home and support at home market by effectively sharing information across relevant health and social care services to prevent provider failure.
3. To share responsibility and set goals for quality and service improvement throughout the care
home and support at home market in Hertfordshire.
4. To share and deploy resources and processes across health and social care in pursuit of quality improvement
5. To own, manage and mitigate as far as possible commissioning risks with regards to provider
failure and the responsibilities under the Care Act 2014.
6. To ensure effective decision making and accountability for the agreed actions
7. To provide direction and guidance to the contracting monitoring / CQC group.
8. To escalate concerns to relevant boards
9. Develop a system of learning and improvement in response to thematic concerns

5
Serious Incidents
There have been 8 safeguarding adult serious incidents reported by NHS Commissioned services 2014 -2015. These serious incidents are reviewed by the Head of Adult Safeguarding who also attends provider organisations safeguarding adult committee’s to discuss these serious incidents and review the implementation of the identified learning. In previous years the number of serious incidents in relation to adult safeguarding incidents has been significantly higher as grade 3 and 4 pressure ulcers were routinely declared as serious incidents and also investigated under the safeguarding procedures. As a result of this the Head of Adult Safeguarding developed practice guidance for when a pressure ulcer should be investigated under the adult safeguarding procedures as well as a serious incident and this now forms part of the Hertfordshire Safeguarding Adult Board policy. Appendix2 sets out the overview of the incidents for each provider.
CCG Strategy
The adult safeguarding assurance Framework has been developed and shared with key partners. The aim of the CCG is to:
• Keep people safe and free from potential or actual abuse or neglect • To be a leading county in adult safeguarding
The vision is to support and embed adult safeguarding processes within all the commissioned services, and to embark on a programme to sustain and improve adult safeguarding in line with the Commissioning Strategy and local priorities related to adult safeguarding and the Care Act 2014. The Framework was agreed at the Quality Committee meeting in November and a draft action place will be developed by the end of May 2015.
GP training
The Head of Adult Safeguarding completed a programme of GP training to a number of clinical staff from each practice within the 6 localities. As part of this work a register of GP Safeguarding Leads is now in place and will be reviewed annually.
CCG staff training
As part of mandatory training all CCG staff are required to complete the safeguarding adult training module and safeguarding adult and Prevent training is delivered as part of the induction programme 3 times a year.
Prevent
Prevent is one strand of the Government’s counter terrorism strategy and Channel is a multi-agency approach to identify and provide support to individuals who are at risk of being drawn into terrorism and forms a key part of the Government’s Prevent strategy. The health sector has a non- enforcement approach to prevent and focuses on protection for vulnerable individuals and healthcare organisations. Heath care

6
professionals may meet and treat people who are vulnerable to radicalisation. The key challenge for the health organisations is to ensure that, where there are signs that someone has been or is being drawn into terrorism; health care workers can interpret the signs correctly, are aware of the support that is available and are confident in referring the person.
NHS England have developed a Prevent Training and Competencies Framework which will enable a consistent and proportionate approach to Prevent awareness raising throughout the NHS. In response to this framework the Head of Adult Safeguarding who is the CCG Prevent Lead, received training from the Hertfordshire Constabulary’s Prevent Lead and will then provide Prevent basic awareness training as part of the induction programme. The Counter Terrorism and Security Bill received Royal Assent on Thursday 12 February and places Channel on a legislative footing as part of this Act, and comes into force on 12 April. Channel is intended not only to prevent terrorism but to protect people who are vulnerable to being drawn into terrorism. Both the Safeguarding Children’s team and the Head of Adult Safeguarding are members of the Channel panels. The Channel Panel meets monthly to discuss individuals who have been referred as being at risk of radicalisation and require protection plans to be put in place. At the end of March 2015 there were 4 protection plans in place and 10 referrals for discussion by the panel. Interventions range from treatment for Post-Traumatic Stress Disorder and referral to Children’s Services. The role of the CCG Prevent Lead is to ensure that NHS provider services undertake any required actions and to advise on adult safeguarding issues.
Domestic Abuse
A review was undertaken by Co-ordinated Action Against Domestic Abuse (CAADA) commissioned by the Police and Crime Commissioner, the Domestic Abuse Strategic Programme Board and the County Community Safety Unit to undertake a review of service provision for domestic abuse in Hertfordshire. The CAADA report was received by the Police and Crime Commissioner and the Domestic Violence Strategic Programme Board in December 2014. The report highlighted a significant number of issues relating to commissioning of services especially Independent Domestic Violence Advocates, the role and function of the Strategic Board, and referral pathways. A working group was formed and an action plan developed which included:
• Developing the vision and structure of the board • Development of strategic objectives • Identifying work streams and how these will be taken forward • Establishing governance and assurance systems and processes
An Executive Domestic Abuse Board is now place and the CCG is represented by the Director of Nursing & Quality. The Head of Adult Safeguarding is the CCG representative on the operational Domestic Abuse Partnership Board and the Vice Chair of the Domestic Homicide Review sub group and is leading the review of recommendations and actions from domestic homicides to establish themes and trends which can guide the

7
development of strategic objectives and service improvement. The Head of Adult Safeguarding is also part of the Commissioning sub group and has successfully recruited to a Senior Commissioning Manager within the Local Authority who will work with the Commissioning Group to procure and commission a robust Independent Domestic Violence Advocate Service as a priority. The Head of Adult Safeguarding will develop the quality measures as part of this process. Domestic Homicide Review
There is currently 2 domestic homicide reviews in progress following incidents in the Hatfield and Bishop Stortford areas. The Head of Adult Safeguarding is a panel member and monitors progress to ensure that recommendations and actions are achievable for health organisations
Mental Capacity Act and Deprivation of Liberty Safeguards
A deprivation of liberty which safeguards a person lacking capacity must be authorised in accordance with one of the following legal regimes: a deprivation of liberty authorisation or Court of Protection order under the Deprivation of Liberty Safeguards (DoLS) in the Mental Capacity Act (2005), or(if applicable) under the Mental Health Act 1983.
In March, the Supreme Court handed down a judgement referred to as Cheshire West. The judgement is significant in lowering the threshold in the determination of whether arrangements made for the care and or/ treatment of an individual lacking capacity to consent to those arrangements amount to a deprivation of liberty.
The Cheshire West judgement has been significant in lowering the threshold in the determination of whether arrangements made for the care and or/ treatment of an individual lacking capacity to consent to those arrangements amount to a deprivation of liberty.
The key points from the Supreme Court Judgement are: • A Revised test for deprivation of liberty which is; the person is under continuous supervision and
control AND is not free to leave, AND the person lacks capacity to consent to these arrangements. The Implications / Actions for the CCG are to:
• Seek assurance from provider organisations that they have sought legal advice regarding the ruling and are aware of the implications for their organisation
• Ensure that the Continuing Health Care team seek legal advice in terms of commissioning care packages for the domestic setting which might constitute a deprivation of liberty
The lowering of the threshold has increased the applications to the Local Authority Supervisory Body by Managing Authorities, such as hospitals, as they are required to make more applications for DoLS assessments. This has resulted in delays with processing applications and so this means that Managing Authorities will be depriving patients of their liberty without authorisation. To mitigate this HCC recruited a number of additional staff to deal with the increased work load. All NHS provider organisations undertook a number of actions to comply with this ruling:

8
• Dip sampling of MCA and DoLS documentation. • A MCA/DOLS newsletter for Bed based MCA/DOLS champions. • A DOLS checklist developed and available on the safeguarding adult intranet page. • Establishing a system that the Safeguarding team are notified of all patients who require 1 to 1 care
so that consideration can be given as to whether a DoL is required • Patients with mental health problems are referred to the RAID team, who review the patient from
a mental health perspective and inform the safeguarding team if they think a DoLS is required. • All relevant teams issued with a briefing on the implications of the decision for HPFT. • The CQC briefings on this case have been circulated to all relevant staff. • Some of the applications have been assessed and deemed to be ineligible for DOLS so Mental
Health Assessments have taken place to ensure the lawful deprivation of liberty of these patients.
These actions are partly responsible for the increasing number of applications being made this year compared with previous years.
The number of DoLS applications and authorisations for 2014 - 2015 is set out below and mirror figures nationally:
Provider No of DoLS
applications made 2013 - 2014
No of DoLS applications authorised 2013 - 2014
No of DoLS applications made 2014 - 2015
No of DoLS applications authorised 2014 - 2015
HCT 2 2 44 17 ENHT 19 7 98 17 HPFT 7 0 451 253 Due to the substantial increase in the numbers of applications being made following the Cheshire West judgement there has been significant delays in assessments and notification of outcomes for authorisation. The reasons for the difference between the numbers of applications made compared with the numbers authorised are due to patients regaining mental capacity before the application is completed or the patient being discharged. The Local Authority Supervisory Body has taken action to manage the delays and organisations have reported this issue to their Boards and placed it on their risk registers.
Responding to the recommendations set out in the House of Lord’s report NHS England Hertfordshire and South Midlands Area Team have allocated each CCG with money to support MCA and DoL development. Herts Valleys CCG received 54,771 and East and North Herts CCG received 51,284. The CCGs agreed to pool the money and undertake a joint approach.
The CCGs were required to demonstrate the following outputs by the end of the financial year to enable NHS England to demonstrate their contribution to the Government’s plan as well as ensuring value for money.

9
• Submission of a self-assessment summary report for 2014/15. This report will give an assessment of the extent to which MCA is complied with and requires sign off from the CCG Director of Nursing & Quality. This report should reference any evidence used to reach the conclusion and any gaps or proposed future activity for 2015/16. This should also take into account the views of relevant stakeholders across the local system.
• Submission of a case study from the CCG for sharing through the national programme, this should highlight MCA good practice in implementing the appropriate options.
• Numbers of health professionals trained as Best Interest Assessors (BIAs) in 2014/15
See appendix 3 for MCA action plan
Internal audit Adult safeguarding went through an internal audit in January and was rated as green. There were a small number of low risk recommendations in relation to having the draft strategy ratified and HSAB activity. Assurance
The Head of Adult Safeguarding and the Director of Nursing and Quality undertook annual assurance visits to each of the following providers in December 2014 and January 2015. As part of the visit each organisation completed a self-assessment audit tool. Following the visit a letter was sent outlining the findings and recommendations. The provider organisation is then expected to complete an action plan which the Head of Adult Safeguarding can monitor at the safeguarding adult committees. The high level summary for each organisation is shown in Appendix 4

10

11
Provider performance The year-end performance for providers is set out below. WHHT have recently reviewed their adult safeguarding training with support from the Head of Adult Safeguarding and this should lead to better uptake from staff. HCT have developed in year level 3 training for their safeguarding adult champions and the Head of Adult safeguarding is part of this training programme. Until now HPFT have only been required to produce training figures for level 2 training but this will change in 2015 – 2016 when they will need to supply the same data as other providers.
Trust Quality requirement Threshold Year end ENHT % of relevant staff who have undertaken level 1
Safeguarding adult training at induction 90% 100 %
% of relevant staff who have undertaken level 1 Safeguarding adult training every 3 years
90% 91.83%
% of relevant staff (all clinical staff including staff in supervisory roles requiring a clinical registration) who have undertaken level 2 safeguarding adults training. To include domestic violence training
90% 88.9%
% of all relevant staff (all clinical staff including staff in supervisory roles requiring a clinical registration) who have undertaken DOLS training
90% 100%
% of relevant staff (all clinical staff including staff in supervisory roles requiring a clinical registration) who have undertaken Mental Capacity Act training
90% 100%
% of relevant staff who have undertaken PREVENT training (not to be included as part of induction as training is bespoke and time specific)
By Q1 trust to have agreed with commissioner groups of ‘relevant staff’ and target training rates for the different staff groups in accordance with national guidance due to be published end of January 2014
313 staff
HCT % of relevant staff who have undertaken level 1 Safeguarding adult training at induction
95% 96%
% of relevant staff who have undertaken level 2 safeguarding adult training annually
90% 85%
% of relevant staff who have undertaken level 3 Safeguarding adult training
90% 64%
% of relevant staff who have undertaken Mental Capacity Act training
90% 83%

12
% of relevant staff who have undertaken Prevent training 90% 98% HPFT % of relevant staff who have who have undertaken level 2 training 95% 94%
Priorities 2015/16
• To develop and implement the safeguarding adult strategy action plan. • Working in partnership with other statutory partners lead the development of domestic abuse services • Embed the adult safeguarding assurance mechanisms • Develop multi-agency information sharing governance structure • Provide on-going support and training to General Practice staff • Implementation of the MCA action plan
Tracey Cooper Head of Adult Safeguarding July 2015

13
Appendix 1
Type of service Overview of concerns Outcome
Residential Care • Non-compliant with CQC • Lack of management oversight • Pressure Care • Staffing levels • Staffing attitudes • Staffing knowledge • Lack of attendance to residents
• Lack of Deprivation of Liberty and Mental Capacity Act understanding
• Serious concerns process began February 2015 • Action plan in place overseen by serious concerns process • Local Authority staff visited the home daily 7 days a week to provide support • All residents reviewed by health and social care staff • Head of Adult Safeguarding met with GPs to discuss their concerns and responsibilities • LA commissioners sent performance notification letter • Head of Adult Safeguarding visited the home on a number of occasions to meet with executive
team and observe progress • District Nurses visited home regularly • Hertfordshire Constabulary Safeguarding Team visited the home to ensure management
understood the seriousness of the concerns • Continuing Health Care Team reviewed a number of residents
Nursing & residential • Strategic concerns relating to care practice issues
• Failure to secure necessary improvements in relation to:
• Poor documentation and follow up
• No initial assessment on admission
• Poor OT support & rehabilitation
• Regular visits from CCG Quality Lead, CHC and contract manager • Serious concerns meeting attended by Director of Nursing & Quality or Deputy • A strategic plan is now operational across all levels where certain duties are assigned to
managers to ensure they are carried out. • Westgate need to demonstrate they are embedding Quality Assurance Plan into practice

14
Nursing & residential • Non-compliant with CQC in relation to infection control
• A number of safeguarding referrals substantiated as neglect
• Care planning • Staffing • Environment • Care of dementia care patients
• Serious concerns process July – October • Action plan in place overseen by serious concerns process • Manager questioned under PACE by CQC and issued with a caution • Residents reviewed by social care staff • District Nurses and CHC staff reviewed a small number of residents • Head of Adult Safeguarding visited the home to meet with owner and observe the home
environment • Contract monitoring officer visited the home several times • Head of Adult Safeguarding liaised with the GP practices
Residential & Nursing • Moving and handling • Pressure area care • Lack of dignity • Lack of snacks • Lap belt used without DoLS
referral • Lack of escalation processes • Staff attitude
• Serious concerns process May – August • Action plan in place overseen by serious concerns process • Experienced Manager bought in to oversee turnaround • Embargo on admissions by CQC • Suspension on admissions by LA and CHC • Home visited by Head of Adult Safeguarding and Head of Continuing Health care • CCG Quality Lead visited home with Contract Monitoring Officer
Nursing & residential
• Failures in assessing and monitoring the quality of care
• No permanent manager for 12 months
• Failures in care practice and procedures
• Serious concerns process November to April 2015 • Action plan in place • Voluntary embargo of admissions in place • Liaison with GPs regarding their view of home • Owner requested to provide letter to submit letter formally stating provision of safe care • Multi-agency review of residents

15
Appendix 2
Residential & Nursing • Lack of management oversight • Staffing • Hydration & nutrition • Poor environment • Inadequate level of care
• Serious concerns process November to April 2015 • Action plan in place • Voluntary embargo of admissions in place • Liaison with GPs regarding their view of home • Owner requested to provide letter to submit letter formally stating provision of safe care • Multi-agency review of residents

16
Provider Overview of incidents Outcome / learning ENHT Allegation Against HC Professional The chaperone policy has been widely circulated
On-going police investigation PAH
Patient safety issue Clear care plans documenting how to deliver care for complex patients and meeting their nutritional care needs involving family/carers All staff to be made aware of need for correct temperature of warm drinks, not hot, for vulnerable patients and highlight risk to patients Discussion at dementia steering and nutritional steering group to identify any changes to procedure/policy required TVNs to share appropriate training for ‘first aid’ in the event of a scald Senior Management Team to ensure clinicians comply with Duty of Candour.
Patient safety issue To write to the patient’s wife with a copy of the investigation report. All Security staff working at PAH to undertake training in Safeguarding Vulnerable Adults. Dementia. Values and Behaviours. Whistle Blowing and Escalation. Task and Finish Group established to review the current Close Monitoring Policy for patients and Criteria for Bedwatch (Security presence) To share report findings and actions taken with Directorate Quality and Safety Committee and Directorate Performance review Meetings with the Trust Executive Team
HCT Allegation against HC Professional Staff to be reminded that an MCA assessment should be undertaken by the ward staff if there is reason to doubt a person’s capacity to consent to treatment or make an informed decision regarding any aspect of their care. All staff to have further training in caring for patients with a cognitive impairment. Service delivery – establishment to increase to full establishment of staff to avoid utilising staff bank when possible. Improved record keeping and report writing skills amongst staff. Learning from lessons in practice. Promote the 6cs model of care within the unit to ensure all staff are delivering compassionate care.

17
Patient safety issue SOVA updates to be completed for those staff outstanding. To share with other bed based units the importance of being vigilante when visitors are on the ward.
Allegation against HC Professional Investigation on-going Allegation against HC Professional Investigation on-going
HPFT Patient safety issue Investigation on-going Staff conduct Investigation on-going

18
Appendix 3
Herts Valleys CCG and East & North Herts CCG Mental Capacity Action Plan
Mental Capacity Action Plan 2014 – 2015
Introduction
In March 2014 the House of Lords Select Committee published their final report following a post legislative scrutiny of the Mental Capacity Act 2005 (MCA). This concluded that while the MCA was well thought through, there is a lack of awareness and lack of understanding. The report identified issues with the implementation of the MCA across health and social care sectors due to paternalism and risk aversion. The report also found that the Deprivation of Liberty Safeguards (DoLS) were not fit for purpose and should be replaced that are easier to understand and implement.
Responding to the recommendations set out in the report NHS England Hertfordshire and South Midlands Area Team allocated each CCG with money to support MCA and DoL development. Herts Valleys CCG received 54,771 and East and North Herts CCG received 51,284. The CCG Directors of Nursing and Quality agreed to pool the money and develop an action plan covering both CCGs.
The CCGs are required by NHS England to demonstrate the following outputs by the end of the financial year to enable NHS England demonstrate their contribution to the Government’s plan as well as ensuring value for money.
• Submission of a self-assessment summary report for 2014/15. • Submission of a case study from the CCG for sharing through the national programme, this should
highlight MCA good practice in implementing the least restrictive option • Numbers of health professionals trained as Best Interest Assessors (BIAs) in 2014/15

19
Appendix 3 (Continued)
Recommendation Action Timescale Lead Outputs A self-assessment summary report should be completed from each CCG for the period 2014/15.
Review MCA section of the CCG self-assessment audit tool used for assurance visits to provider organisations.
Completed
TC Submission of a self-assessment summary report from each CCG for the period 2014/15.
Send out self-assessment tool to Directors of Nursing of provider organisations November / December 2014
Completed TC Self-assessment from: WHHT HCT HPFT ENHT
Review submissions and identify non-compliance Follow up at assurance visits
Completed TC JN SR Adult safeguarding annual assurance visits to each provider completed January 2015. Actions will be monitored by TC at provider Safeguarding Committees
Produce summary of provider organisations self-assessments
Completed TC Summary of self-assessments including compliance, gaps and proposed future activity
Identify an Independent Provider to undertake scrutiny and challenge work across provider organisations and identify gaps
Completed TC 12 days’ work to be undertaken days’ May – July 2015 £8,000

20
and agree a proposal
Completed TC Completed scrutiny and
challenge work and action with recommendations.
Both CCGs should identify a case study to share through the national programme, which highlights good practice in implementing the least restrictive option.
Liaise with the HCS DoLS Lead to identify cases
March 2015
TC Provide a case study from each CCG for sharing through the national programme.
Ensure case studies available to NHS England
March 2015
The CCG should provide NHS England with the numbers of health professionals trained as Best Interest Assessors (BIAs) in 2014/15 for each CCG
Establish the numbers of BIAs already working in health organisations
Completed TC Provide NHS England with the number of BIAs in each CCG area.
Provider organisations to identify the staff they would like trained as BIAs TC to work with the LA DoLS Lead to develop extra courses at the University of Hertfordshire. The application process will be managed by the DoLS Lead and the courses will run 2015 – 2016. These staff will then go on the BIA rota to do an assessment every month or every 2 months to maintain practice.
Completed TC There will be 30 BIAs trained at a cost of £45,450
Improve the level of knowledge of MCA / DOLS across health and
Work with the LMC re: training for GPs.
January 2015
Funding of 2 conferences £5000 10.4.15 – D/W Rachel Lea to

21
primary care This money will be used to fund a conference in each CCG on MCA for GPs organised by LMC. TC will work with the LMC to draft the conference agenda
meet later in the Spring to discover how this can be taken forward
Identify an independent trainer to work with provider organisations re: train the trainer approach incorporating case studies
December 2014 Independent trainer TC Trainer to work across 3 provider organisations and Continuing Health Care Teams £6,000
Fund a Band 7 for 1 month in the mental health trust to undertake training for specific staff groups. This post holder already exists and doing training.
May 2015 TC £4,200 This will ensure consistency of knowledge across the organisation
Link with any CCG initiatives that require MCA knowledge
Completed TC Link made with Care Home Premium and identify any training needs
Improve the level of knowledge of MCA / DOLS across health and primary care (cont’d)
Work with the independent trainer and providers to implement the proposed work
February -April 2015
TC / Independent trainer Consistent training used across all providers Train the trainer approach implemented across all providers
Work with Independent provider to undertake scrutiny and challenge work
May – July 2015 TC / Independent provider
Gaps identified and recommendations made for further work
Develop a system of peer quality checks of MCA recording within services / organisations
August 2015 TC and provider MCA Leads
Implement the system of peer September – TC and provider MCA

22
Key:
TC – Tracey Cooper, Head of Adult Safeguarding Herts Valleys / East & North Herts
JN – Jan Norman, Director of Nursing & Quality Herts Valleys CCG
SR – Sheilagh Reavey, Director of Nursing & Quality, East & North Herts CCG
quality checks of MCA recording within services / organisations
October 2015 Leads
Develop action plan from the above work
July - August 2015
TC Implementation of the action plan
Identify, commission and hold a half day training for MCA Leads focussing on case law
June 4th 2015 TC £600 CCG and provider MCA Leads will have up to date knowledge of case law

23
Appendix 4
Provider Findings Recommendations E&NHT • The Trust demonstrated that adult safeguarding forms part of the
Trusts objectives and values and links. • The Trust has policies, procedures and training in place to support
safeguarding adults at risk. • The Trust provided evidence of outcomes resulting from safeguarding
adults at risk and provided examples of learning. • All new doctors receive safeguarding adult training as part of their
induction. • Concern was expressed by the CCG regarding the resilience of the
Safeguarding Lead Nurse as a single post, although this is mitigated by a number of Matrons and the Deputy Director of Nursing also supporting the agenda.
• Under A7 of the audit the Trust agreed to change the rag rating from green to amber due to concerns raised by GPs about discharge summaries not being provided for vulnerable patients. The CCG would like the Trust to resolve this as a matter of urgency.
• The Trust undertakes DBS checks at the commencement of employment for all staff.
• The Trust remains amber in relation to monitoring the understanding of MCA / DoLS and training of staff.
• The Trust should review their appraisal documentation to include a specific section on safeguarding to align with a competency framework.
• The Trust should undertake a formal audit of the implementation of the MCA.
• The Trust need to improve their patient discharge summaries. • The Trust to identify additional staff to undertake Best
Interest Assessors course to increase the level of expertise within the organisation.
Progress is being made against a number of these recommendations
HCT • Safeguarding adults is embedded within the Quality Strategy and forms part of the Patient Safety work plan and updates are provided to the Healthcare Governance Committee.
• HCT have a Learning Disability action plan through which a number of initiatives have been developed such as a ‘My teeth’ DVD to help people with dental visits/treatments and generally improving signage within units.
• Mental Capacity is a Quality Priority for 2014/15 with an action plan
• HCT need to achieve the necessary training levels set out in the Quality Schedule for safeguarding adults and MCA for all Business Units.
• HCT to complete the process for accessing legal advice out of hours and place information in the on call folder.
• HCT to develop a system and process to ensure reporting of quality intelligence within care homes. This process should also include how HCT will share this intelligence and actions

24
to improve implementation and competency. • HCT are formalising access to legal advice for Out of Hours in response
to recommendations made following a recent MASIR. This is in particular reference to contacting the Court of Protection.
• HCT are compliant in all areas with CQC. • The role of Specialist Nurse for Safeguarding Adults is to be a
permanent post. • The role of local safeguarding adult champions is being strengthened
to improve accountability.
that might be taken. • HCT need to ensure that staff make appropriate safeguarding
alerts, particularly in relation to care homes. • HCT need to develop an improved system to monitor themes
and trends emerging from adult safeguarding and quality issues.
Progress is being made with these recommendations some of which link to work regarding care homes being led by the CCG Head of Quality Improvement
HPFT • The Trust demonstrated that adult safeguarding forms part of the Trusts objectives and values
• There is a new safeguarding team structure and the team are reviewing the current safeguarding adult systems and processes within HPFT
• HPFT need to implement robust data collection systems and processes to enable effective reporting of safeguarding metrics to the CCGs.
• There has been a loss of organisational memory with staff moving to new posts and recruiting new staff. There are other pressures including; the Cheshire West judgement and PARIS.
• HPFT acknowledge the need to re-energise their internal quality monitoring.
• The Safeguarding Lead Consultant only has one session per week to focus on adult safeguarding
• HPFT have a representative for each of the Care Act groups. • The safeguarding adult policy and strategy are currently being
developed.
• HPFT to audit the experiences of clients who have been subject to a safeguarding adult intervention as there is inconsistency in the way this data is collected.
• To review the safeguarding adult lead Consultant’s job description and number of sessions with a view to increase capacity to enable the agenda to be delivered.
• The Safeguarding Lead Consultant to meet with the CCG Head of Adult Safeguarding to understand the expectations of the CCGs.
• HPFT to write to the Director of Adult Social Services at Hertfordshire Community Services regarding clarification of their delegated responsibilities.
• HPFT to ensure that adult safeguarding is embedded within appraisal and supervision processes.
• To continue with the current review to ensure effective systems, processes and outcomes are in place to safeguard all service users.
Progress has been made with these recommendations as the CCG Head of Adult Safeguarding has met with the Lead Consultant and set out expectations for that role. HPFT are working with HCS regarding the delegated responsibility.

1
Agenda Item No: 11
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: PRESCRIBING REPORT
Decision Discussion Information Follow up from last meeting
Report author:
Sue Russell – Lead Pharmacist, Pharmacy & Medicines Optimisation Team (PMOT), East & North Hertfordshire CCG
Report signed off by:
Dr Ash Shah (Lead GP for Medicines Optimisation) Chris Badger (Interim Director of Strategic Partnerships)
Purpose of the paper:
To inform the Governing Body of:
• the financial position of ENHCCG practices against their respective budgets at June 2015.
• progress against the local medicines optimisation agenda to date of meeting.
Appendix 1a & b – Locality-level Prescribing Report to Board:
These present an overall summary of all the key performance indicators and QIPP projects related to prescribing at year-end including GP prescribing costs, oxygen costs ScriptSwitch® activity, and Prescribing Key Performance Indicators (KPIs) including anti-bacterials usage. (Each element is available to practice level to support local monitoring, and this data is shared with each Locality and practice prescribing lead by their Pharmaceutical Adviser regularly throughout the year).
Conflicts of Interest involved:
Dr Shah is a partner in Wrafton House Surgery, Welwyn & Hatfield Locality.
Recommendations to the Governing Body:
• To note the financial position at June 2015, the work
undertaken to date this year by practices & PMOT, and make any decisions pertaining to medicines management as may be highlighted from the discussion

2
Prescribing Report 1. Purpose of the Paper 1.1 The prescribing finance, performance and pharmacy & medicines optimisation report for East & North Hertfordshire CCG is presented, using June 2015 ePACT Data, July 2015 oxygen data (CCG level only), and ScriptSwitch® (SS) information. 2. Terms / Acronyms Used in this Report not otherwise defined Initials In full PMOT Pharmacy & Medicines Optimisation Team of CCG HMMC Hertfordshire Medicines Management Committee QIPP Quality, Innovation, Productivity and Prevention initiatives PCMMG Primary Care Medicines Management Group NHSE NHS England 3. Executive Summary At June 2015 the CCG shows an overspend against its prescribing allocation of £925,081(1.21%). This is an improvement on earlier months of 2015-16 but data can be unreliable this early in the year. The rate of growth overall in spend (4.68%) is now slightly above that nationally which is at 3.11% The domiciliary oxygen supply budget has a small underspend. Practice progress against new prescribing KPIs is already encouraging across the board. The CCG is currently in-line to achieve the antimicrobial prescribing Quality Premium targets set by NHSE. Engagement with secondary care continues on various levels. 4. Risks & Mitigating Actions 4.1 Primary Care Prescribing Expenditure As at June 2015 ENHCCG spent £19,686,315 and the forecast spend for the year after adjustments is £77,377,021 or +£925,081 on primary care prescribing. Prescription items numbers were up by 68,055 in Q1 versus last year, and costs up by £1.4 million. Forecast annual growth is 4.68% However, the NHS prescribing forecast is less accurate in the early months of the year, but national growth is currently only 3.11% so PMOT is currently analysing data to try to understand what is fuelling the rise locally. 4.2 Domiciliary Oxygen There is currently a forecast underspend of approximately £4K on the oxygen budget. 4.3 ScriptSwitch® electronic messages at the point of prescribing Scriptswitch® costs have risen slightly in 2015-16 as Dolphin House Surgery is now using the system. Only 3 practices do not have ScriptSwitch®. 4.4 KPIs Appendix 1b sets out Locality performance against the five key prescribing metrics agreed by PCMMG in June. Two are carried over from last year, with another new financially-driven KPI. Two KPIs are related to antimicrobial prescribing and are based on the targets set for the CCG to achieve part of the Quality Premium payment for 2015-16. Nationally produced data confirms that the total antibiotic prescribing has decreased by 1.84% from the 2013-14 baseline and broad spectrum antibiotic prescribing has also shown a 14% decrease in items over the period 2014/15. 4.5 Self-care (including over the counter medicines) & Community Pharmacy NHSE locally announced the mandatory Health Promotion Programme for community pharmacy in 2015-16 on 18 June 2015. Campaigns will cover breast and gastro-oesophageal cancers, mental health, seasonal flu vaccination, antibiotic awareness and smoking cessation. NHSE is yet to

3
publish the service specification and the Patient Group Direction (PGD) for the use of pharmacy to provide flu vaccination on the NHS this winter. (see also section 5.7) 4.6 ‘Specials’ – medicinal products produced to order and/or unlicensed products Prescribing costs of ‘specials’ continue to decrease, with a 21% drop in Q1,with 40% less expenditure on ‘’individual’’ formulations. In Q1 specials cost the CCG £163K 4.7 Improving Prescribing of Antibacterials (‘Antimicrobials Stewardship’) including self-care
• Guidelines for the Management of Infection in Primary Care Across Hertfordshire were revised and approved by HMMC in July. The restricted antibiotics list has been updated. Both documents are available on the CCG website.
• A leaflet entitled ‘When should I worry’ aimed at educating parents has been uploaded to the CCG website and provides information on how to self- care, length of illness, safety netting etc. http://www.enhertsccg.nhs.uk/infections
• ‘Treating your infection’ is a resource that GPs can use when they decide an antibiotic is not appropriate. http://www.enhertsccg.nhs.uk/infections
• ‘Top tips to tackle antibiotic resistance’ is live on the website and is aimed at helping GPs to reduce inappropriate antibiotic prescribing in line with the Quality Premium target. http://www.enhertsccg.nhs.uk/infections
• All (anonymised) C. difficile root cause analyses are now discussed at locality prescribing meetings as part of a peer review process
4.8 High Cost Drugs Use in Secondary Care The Tariff- Excluded High Cost Drugs validation process by PMOT continues and over £200K is outstanding from last year and this is being pursued by the contracting team. It is not likely that there will be as many credits for 2015-16 as Trusts are much improved at charging the correct commissioner now. 4.9 Engagement with AcuteTrusts Pharmaceutical Advisers continue to investigate GP reports of requests to prescribe that breach local formulary guidelines and feed this back to the Trust for resolution. Lead Pharmacist & GP support for both of East & North Herts Trust’s New Drugs & Formulary Committee and their Therapeutics Policy Committee continues. The Head of PMOT leads a local working group of provider senior pharmacists illustrating how medicines contribute to the integrated care agenda 4.10 Acute In-Hours Visiting Service Prescribing costs to June 2015 totalled £9185.Last year the total spent for this period was £ 10,666 5. Other (Risk) Issues The PCMMG met on June 2nd and again on September 9th to provide direction on the implementation of the decisions of HMMC. Decisions from the April HMMC meeting and the annual workplan and predicted cost pressures have been taken to the Governing Body according to the due process agreed in April. PMOT continues to assist practices in QIPP savings for the year and provide practical support. Specialist pharmacists have been recruited as part of the CCG’s Vanguard Bid around Care Homes. In addition the team is providing professional advice to those Localities that wish to bid for funding under the NHSE pilot for clinical pharmacists in GP practices. Medicines optimisation input into two local intermediate care settings and End of Life project work continues. The team has a workplan for 2015-16, with a focus on ‘business as usual’, repeat prescribing processes and increasing access to emergency medicines – an enhanced service for community pharmacy is being expanded and a new scheme to provide emergency supplies of prescription medicines at NHS expense (to reduce demand on Unscheduled Care) is in development. 6. Recommendations To note the financial position at June 2015, the work undertaken to date this year by practices & PMOT, and make any decisions pertaining to medicines management as may be highlighted.

GP Prescribing
LOWER LEA VALLEY £121,739 1.29% 4.81% NORTH HERTS £136,671 0.88% 3.66% STEVENAGE £292,601 2.42% 6.21% STORT VALLEY & VILLAGES 1 -£320,408 -3.75% -0.40% STORT VALLEY & VILLAGES 2 -£299,220 -4.05% -0.71% UPPER LEA VALLEY £550,641 3.62% 7.24% WELWYN HATFIELD £201,458 1.34% 4.90% SPRING HOUSE MEDICAL CENTRE (UNREGD) £42,391 187.71% 28.43%
ENHCCG £1,025,094 1.35% 4.73%
New QEII UCC -£63,235 -100.00% 0.00%Community Nurse Prescribing -£22,481 -5.68% -2.03% Herts Urgent Care - E&N OOH -£3,036 -2.13% 1.66% Isabel Hospice -£4,969 -99.38% -83.46% Intermediate Care £598 1.91% 4.45% Deputising Services £0 0.00% 0.00% Unidentified Prescribing -£6,889 -92.44% -92.14% TOTAL OTHERS -£100,012 -15.50% -1.96%
ENHCCG TOTAL £925,081 1.21% 4.68%
HERTFORDSHIRE ANDSOUTH MIDLANDS AREA TEAM N/A N/A 3.31%
NATIONAL N/A N/A 3.11%
Oxygen 2015-16 (N.B to July)
Month Oxygen SpendYear to Date
Oxygen Budget
Forecast Outturn
£ Variance
% Variance Against Budget
Apr-15 £59,461May-15 £62,773Jun-15 £66,044Jul-15 £61,624
ENHCCG Total £249,902 £754,000 £749,706 -£4,294 -0.57%
In 2014-15 the monthly spend on oxygen varied from £52k to £69k and the average monthly spend was £61k.
ScriptSwitch 3
LOWER LEA VALLEYNORTH HERTSSTEVENAGESTORT VALLEY & VILLAGES 2UPPER LEA VALLEYWELWYN HATFIELDENHCCG
* Total actual cost charged to budget** ScriptSwitch net saving to date includes repeat savings for previous roling 12 months and the cost of ScriptSwitch to date.
1 including St Elizabeths & Sawbridgeworth Medical Services2 excluding St Elizabeths & Sawbridgeworth Medical Services3 the following practices do not have ScriptSwitch installed: Haileybury College, King George Surgery, Orchard Surgery, Sawbridgeworth Medical Services
Key
No change
N/A
N/A £7,981
£140
£395,556£139,575
£31
£19,550,695
£7,087,481£15,759,771£15,204,466
£64,974
£76,831,851
£22,583
£31,327
£7,453
£16,127
£15,003,009 £3,852,708£3,996,585£15,209,129
£7,386,701 £1,824,323
£8
£63,235 £0 £0 N/A
£75,806,757
£0 £0 N/A
£373,075£142,611
£5,000£31,925
£135,620
ASO-PUs is a national validated weighting system applied to practice list sizes which corrects for differences in age/sex breakdown. It is not appropriate to use in services without a regular list.
£ differencevs Budget
Improvement on previous monthNo improvement on previous month
£2,432,350
2015/2016Prescribing Budget*
(excludes PH, CRI & NHSE Commissioned Drugs)
Cumulative Spendto June 2015 *
£564
Cumulative spend to date
per 1,000 ASO-PUs
N/A£9,878£8,868
£9,256£9,240£10,142
£9,714
£0
£9,528
N/A N/A
£545,170
£92,597£34,894
£50,220 £81,872 £60,887 £10,667
Annual Cost of Service inc VAT
Supplier PROJECTED savings
Savings ACTUALISED over previous 12 months
Not Available £91,193,168 £354,561,355
Not Available £2,056,806,236 £8,056,504,768
Net Savings**
£32,524£51,477 £103,666 £66,238 £14,761
£3,551
£33,487 £54,659 £33,225 -£262
£27,545 £45,371 £26,005 -£1,540£50,832 £80,819 £54,383
£248,393 £430,803 £280,917
£34,832 £64,417 £40,180 £5,347
£645,182
N/A £0
% growth2015/16 vs 2014/15
£8,543,256 £2,107,922
% differencevs Budget
£9,419,231£15,511,008 £3,974,692£12,098,542
Forecast spend positionposition
@June 2015 (excluding drugs commissioned elsewhere)
£3,170,311
£9,540,970£15,647,679£12,391,144
£8,222,848
N/A
N/A£77,377,021£76,451,939 £19,686,315
APPENDIX 1a - East & North Herts CCG Prescribing Finance Board Report – September 2015

QP - All Antibacterials
QP - Broad Spectrum Antibiotics
BGT Strips Generic Sildenafil
Budesonide / Formoterol combination inhalers
LOWER LEA VALLEY 1.128 7.8% 33.27% 76.98% 0.90%
NORTH HERTS 1.040 8.8% 49.54% 65.77% 1.60%
STEVENAGE 1.186 8.1% 34.79% 72.79% 1.35%
STORT VALLEY & VILLAGES 1.058 8.9% 19.58% 72.06% 0.27%
UPPER LEA VALLEY 1.070 8.8% 31.52% 70.59% 1.05%
WELWYN HATFIELD 1.059 7.1% 35.64% 67.43% 3.31%
ENHCCG 1.175 8.2% 36.00% 70.34% 1.45%
Key 25.00% 85.00% 67.07% 6.08 9.50
Threshold not achieved >1.185 ≥11.3% <40% <70% <50%
Threshold to achieve Indicator ≤1.185 <11.3% ≥40% ≥70% ≥50%
Proportion of CCG practices achieving threshold 69% 97% 41% 49% 0%
Highest practice achievement in CCG this month 0.714 4.00% 82.00% 94% 15%
Y
Y
N
Y
Y
Y
Indicator Indicator Type Indicator Basis Description of Indicator
BGTS < £10 FinancialHMMC/ PCMMG
This indicator is the percentage of prescriptions issued for blood glucose testing strips currently costing under £10 per pack as a proportion of all blood glucose testing strips.
QP - All Antibacterials Quality
NHSE / PCMMG
This indicator is the subject of a Quality Premium target for the CCG. It is the ratio of number of antibiotic items prescribed per antibacterial STAR-PU
(list size weighting specific to the therapeutic area)
QP - Broad Spectrum Antibiotics Quality
NHSE / PCMMG
This indicator is the subject of a Quality Premium target for the CCG. It is the % of cephalsporin, co-amoxiclav and quinolone (broad spectrum) items
out of all prescribing of oral antibiotics
Budesonide / Formoterol combination inhalers medium and high strength
Financial/Quality PCMMG
This indicator is the total number of prescription items for DuoResp® brand of inhalers out of prescribing of all inhalers containing budesonide/formoterol 200/6mcg or 400/12mcg. Specifying brand allows prescriber to control device type supplied
Generic Sildenafil Financial PCMMGThis indicator is the total number of generic sildenafil items prescribed as a proportion of the the total number of PDE5 items.
Y Y Y Y
Y Y Y Y
Y Y Y Y
Y N Y Y
Y Y N Y
Y Y Y Y
Appendix 1b - East & North Hertfordshire CCG Prescribing KPIs 2014/15 - Rolling 3 Months to June 2015
Improved on Previous
Report?
Improved on
Previous Report?
Improved on
Previous Report?
Improved on
Previous Report?
Improved on
Previous Report?
The table below shows Locality performance against achievement thresholds that were set based on performance at the end of 2013/14for the NHSE antibacterials targets and an aspirational expectation for the other indicators as agreed with Primary Care Medicines Management Group . Numbers in green font mean the threshold was achieved, red equals not achieved. Improvement is also stated and is shown by green-filled cells
with red indicating a deterioration.
Y Y Y Y Y

Agenda Item No: 12
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Co-Commissioning Update and Joint Committee Report
Decision Discussion Information Follow up from last meeting
Report author: James Gleed
Associate Director Commissioning Primary Care Projects Report signed off by: Denise Boardman
Interim Director Commissioning
Purpose of the paper: To:
1. Present a brief summary of the work of the Co-Commissioning Joint Committee
2. Highlight the opportunity for the CCG to transition from a ‘joint’ to ‘delegated’ co-commissioning model from 1 April next year
Conflicts of Interest involved:
The GPs on the governing body declare and manage conflicts of interest on a case by case basis where decisions could impact on their role as providers of healthcare. The CCG’s policy on management of conflicts of interest has been reviewed and updated to ensure alignment with the recently published guidance from NHS England
Recommendations to the Governing Body:
To note the update To discuss consideration of the co-commissioning model next year

Page 2 of 8
1. Terms/acronyms used in this report
NHSE: NHS England CCG: East and North Herts Clinical Commissioning Group LMC: Local Medical Committee GPHLI: General Practice Higher Level Indicators GPOS: General Practice Outcome Standards PIA: Privacy Impact Assessment (this is an assessment undertaken
to ensure that new developments involving the transfer of personal data meet all of the relevant laws and regulations)
2. Appendices
Appendix 1: Joint Committee final terms of reference
3. Co-commissioning recap and update
3.1 During 2014-15 CCGs were asked to select from the following three co-commissioning models to be operational for the start of the 2015-16 financial year:
• Influence • Joint • Delegated
3.2 A risks and benefits exercise was undertaken and the conclusions drawn from this together with information about the process of co-commissioning was shared with member practices through locality events. The members voted and returned a majority decision for joint co-commissioning. The governing body at its meeting on 18th December 2015 formally agreed ‘joint’ co-commissioning as the most appropriate option for ENHCCG during 2015-16. 3.3 A new joint committee between the CCG and NHS England Central Midlands has subsequently been established; the committee met formally for the first time on 17 June 2015. The meeting has a public part 1 and a private part 2 section consistent with CCG governing body meetings. 3.4 At the point the first meeting was held the CCG had not yet appointed a Lay Member for co-commissioning. The Joint Committee therefore agreed that the CCG Lay Member for Audit and vice chair of the Joint Committee would chair the first meeting. A third lay member has now been recruited to lead on co-commissioning; the post holder has commenced in post and is currently in the process of receiving a handover from the Lay Member for Audit. The CCG Lay Member for Audit will continue to remain a substantive member of the Joint Committee as vice chair as per the terms of reference.

Page 3 of 8
3.5 With regards to the CCG’s board structure the Joint Committee reports to the governing body; the governing body annual cycle of business requires a quarterly update on the work of the committee. This report is the first quarterly update. 4. Summary of the Joint Committee’s work in the last quarter
4.1 The following agenda items were taken and discussed at the first public meeting:
• Terms of reference • Work streams and annual cycle of business • Quality Assurance • PMS contract reviews • Care record sharing
4.2 The terms of reference were reviewed and finalised (appendix 1), the chief amendment was in relation to the role of the LMC on the committee – the LMC is now represented on the committee as a non-voting member as opposed to an observer; the attendance of the LMC at only the part 1 public meetings remains unchanged however. NHS England Central Midlands also confirmed both medical and nursing directorate representation on the membership. 4.3 The committee identified the importance of having a targeted work plan in order to ensure that it adds value and makes a significant difference to the future quality, quantity and sustainability of primary care locally. The top priority work streams for the committee were debated and ultimately agreed as being:
• Quality Assurance/improvements • Premises • Primary care workforce and education • Consolidation of funding
4.4 The committee noted the fact that the NHS England Hertfordshire and South Midlands Area Team (now NHS England Central Midlands) quality assurance process that had operated last year had been paused to make way for new processes as part of co-commissioning which would be taken forward with individual CCGs. NHS England had previously developed a dashboard of data termed the ‘Primary Care Web Tool Plus’, which combined the nationally published data sets GPHLI and GPOS with local intelligence e.g. complaints information. The committee also noted the recently refreshed CCG Locality Information Packs. The committee discussed if and how the data included in the previous NHS England dashboard should be used and presented going forwards as part of quality assurance and improvement. The committee decided that it was important to review data in the round and that having multiple separate data packs was not helpful. The committee therefore agreed the two data sets should be brought together into one single pack and a draft pack was requested for the next meeting. 4.5 The committee also discussed the medical input for practice quality visits, previously this was provided by NHSE Medical Advisors, however due to the organisational changes this resource was no longer available. It was agreed that CCG GP Locality Leads would participate in any visits that are required. Future visits will however be a joint process between NHSE and the CCG, with the NHSE contracts team supporting the process and attending visits.

Page 4 of 8
4.6 The committee received a presentation on the Care Record Sharing Project (Stevenage). This project has three key aims:
• Sharing electronic GP patient record between GPs • Sharing electronic GP patient record with community nursing services • Creation of a new nursing home electronic patient record
4.7 It was confirmed that the patient records were only being shared locally with other healthcare professionals that are involved in a given patient’s care. This will ensure that they have up-to-date clinical information and therefore able to provide the best possible quality of care. The project’s Privacy Impact Assessment (PIA), Data Sharing Agreement and process for patient consent were all discussed. The presentation was well received and attracted positive comments from Local Healthwatch. 5. Next Steps
5.1 NHS England has requested that CCGs review their current co-commissioning arrangements and submit a request for an alternative model, should this be the outcome of the review. 5.2 Submissions for CCGs wishing to move from joint to delegated arrangements in 2016-17 can only be made once during this year, the original submission date was 2nd October however NHSE has recently extended this to 6th November. 5.3 A transition from joint to delegated co-commissioning would require the CCG’s constitution to be reviewed and amended. This in turn would necessitate consultation with the CCG’s membership. The newly created co-commissioning joint committee’s terms of reference would also need to be amended accordingly. 5.4 A risks and benefits analysis was previously undertaken to help the CCG make a decision on the co-commissioning model for this (the current) year, this aimed to forecast overall net gain or losses for the CCG and its local population. Since little has changed and the CCG has limited experience of its current joint co-commissioning arrangements the risks, benefits and their relative weightings are likely to remain largely unchanged since the previous analysis and vote.
The next Joint Committee meeting is scheduled to take place 15th October 2015.
6. Conclusion and recommendations
The first meeting of the Joint Committee was constructive. The CCG will need to decide by 6th November 2015 whether it wishes to transition to ‘delegated’ co-commissioning. This change would require an amendment to the CCG’s constitution and therefore for member practices to be consulted. Co-commissioning is still a relatively recent development and consequently there is little experience to draw on or new information available to guide the decision. Any decision to change the current model must be founded upon clearly identified health and wellbeing benefits for the local population.

Page 5 of 8
Appendix 1: Terms of Reference for Joint Committee
Introduction 1. The NHS England and NHS East and North Hertfordshire Clinical Commissioning Group
Joint Commissioning Committee is a (“Joint Committee”) with the primary purpose of jointly commissioning primary medical services for the people of East and North Hertfordshire.
Statutory Framework 2. The National Health Service Act 2006 (as amended) (“NHS Act”) provides, at section 13Z,
that NHS England’s functions may be exercised jointly with a CCG, and that functions exercised jointly in accordance with that section may be exercised by a joint committee of NHS England and the CCG. Section 13Z of the NHS Act further provides that arrangements made under that section may be on such terms and conditions as may be agreed between NHS England and the CCG.
Role of the Joint Committee 3. The role of the Joint Committee shall be to carry out the functions relating to the
commissioning of primary medical services under section 83 of the NHS Act except those relating to individual GP performance management, which have been reserved to NHS England
4. This includes the following activities:
• General Medical Services (GMS), Personal Medical Services (PMS) and Alternative Provider Medical Services (APMS) contracts (including the design of PMS and APMS contracts, monitoring of contracts, reviewing proposed contractual action such as issuing breach / remedial notices, and removing a contract);
• Newly designed enhanced services (“Local Enhanced Services” and “Directed Enhanced Services”);
• Design of local incentive schemes as an alternative to the Quality Outcomes Framework (QOF);
• Decision making on whether to establish new GP practices in an area; • Approving practice mergers; and making decisions on ‘discretionary’ payment (e.g. returner /
retainer schemes).

Page 6 of 8
5. In performing its role the Joint Committee will exercise its management of the functions in accordance with the agreement entered into between NHS England and NHS East and North Hertfordshire Clinical Commissioning Group, which will sit alongside the Scheme of Reservation and Delegation and Terms of Reference. This is the proposed agreement to deal with activities such as information sharing, resource sharing, contractual mechanisms for service delivery (and ownership) and interplay between contractual and performance list management.
Geographical coverage
6. The Joint Committee will comprise of NHS England (Central Midlands) and NHS East and North Hertfordshire Clinical Commissioning Group (“the Group”). It will undertake the function of jointly commissioning primary medical services for East and North Hertfordshire.
Membership 7. The Joint Committee shall consist of:
• The Group’s Lay Member for Governance • The Group’s Lay Member for Co-Commissioning • Three Executive members of the Group:
o Chief Finance Officer o Director of Commissioning o Director of Operations
• Three GP members of the Group’s Governing Body • Three NHS England Central Midlands Executives:
o Locality Director o Medical Director o Director of Nursing.
The membership will meet the requirements of the Group’s Constitution.
8. The Chair of the Joint Committee shall be the Group’s Lay Member for Co-Commissioning 9. The Vice Chair of the Joint Committee shall be the Group’s Lay Member for Governance 10. The following representatives will usually be in attendance:
• Secretariat; • Associate Director of Primary Care Commissioning of the Group; • GP Contract Manager NHS England Central Midlands; • Health Watch representative; • Health and Wellbeing Board representative; • Local Medical Committee representative.
Meetings and Voting 11. The Joint Committee shall adopt the Standing Orders of the Group insofar as they relate to
the:
• Notice of meetings; • Handling of meetings;

Page 7 of 8
• Agendas; • Circulation of papers; and • Conflicts of interest.
12. The Joint Committee shall reach decisions by a simple majority vote of members present.
However, because the Group has eight members on the Joint Committee and NHS
England (Central Midlands) has three members, the Group members shall have one vote
each and NHS England (Central Midlands) members shall have two and two-third
votes each.
In the event of a tied vote, the Group shall have a casting vote on any CCG statutory functions
included within the scope of the joint committee’s responsibilities and NHS England (Central
Midlands) shall have a casting vote on any NHS England statutory functions included within the
scope of the joint committee’s responsibilities.
13. To be quorate each of the following criteria must be met:
• Six members of the Joint Committee are present, including at least one member of The Group and at least one member of NHS England Central Midlands
• There is a non-GP majority within the members present
No formal business shall be transacted where a quorum is not reached.
14. A minimum of 4 scheduled meetings shall take place per year. Where required additional meetings will be arranged.
15. Meetings of the Joint Committee:
a) Shall, subject to the application of 17(b), be held in public; b) The Joint Committee may resolve to exclude the public from a meeting that is open
to the public (whether during the whole or part of the proceedings) whenever publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted or for other special reasons stated in the resolution and arising from the nature of that business or of the proceedings or for any other reason permitted by the Public Bodies (Admission to Meetings) Act 1960 as amended or succeeded from time to time.
16. Members of the Joint Committee have a collective responsibility for the operation of the
Joint Committee. They will participate in discussion, review evidence and provide objective expert input to the best of their knowledge and ability, and endeavor to reach a collective view.
17. The Joint Committee may call additional experts to attend meetings on an ad hoc basis to
inform discussions.
18. Members of the Joint Committee shall respect confidentiality requirements as set out in
the Standing Orders referred to above unless separate confidentiality requirements are set out for the Joint Committee in which event these shall be observed

Page 8 of 8
19. Secretariat to the Joint Committee will be provided by The Group
20. The Secretariat to the Joint Committee will circulate the minutes and action log within 5 working days of the meeting to all members.
21. These Terms of Reference will be reviewed annually, reflecting experience of the Joint
Committee in fulfilling its functions and the wider experience of NHS England and CCGs in primary medical services co-commissioning.
Decisions 22. The Joint Committee will make decisions within the bounds of its remit.
23. The decisions of the Joint Committee shall be binding on NHS England and the Group.
24. Decisions will be published by both NHS England and The Group.
25. The Secretariat will produce an Executive Summary Report on a quarterly basis, which will
presented to the NHS England Central Midlands and the Governing Body of the Group for information.
Key Responsibilities 26. This will include but not be limited to areas such as planning, including carrying out needs
assessments, primary medical care services for the geographical area in question; undertaking reviews as appropriate; co-ordinating a common approach to primary care commissioning as appropriate; managing relevant budgets.
Review of Terms of Reference 27. These Terms of Reference will be formally reviewed by the NHS England Central Midlands
and the Group in April of each year, following the year in which the Joint Committee is created, and may be amended by mutual agreement between the NHS England Central Midlands and the Group at any time to reflect changes in circumstances, which may arise.
[Signature provisions]
Schedule 1 – List of Members – populate once membership agreed

Agenda Item No: 13
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Home-Start Home-Visiting support service in NHS East and North Hertfordshire CCG
Decision
Discussion
Information
Follow up from last meeting
Report author: Kate Barker, Assistant Director for Maternity, Children and
Young People Report signed off by: Beverley Flowers, Interim Chief Executive
Purpose of the paper: To provide Governing Body members with the background
of the current Home-Start home visiting service in East and North Hertfordshire. (Including a summary report from Hertfordshire Home-Start.) To highlight the improved level and purpose of statutory funded provision that has been increased due to significant change in the statutory duties for local authorities to provide in their local offer for children 0 -5 years, this includes a higher level of support to vulnerable families. To enable Governing Body members to make recommendations on the future funding arrangements for the home visiting service (Home-Start) for ENHCCG localities
Conflicts of Interest involved:
None

Recommendations to the Governing Body:
It is recommended that:
• the CCG Governing Body members agree to cease the CCG’s funding for a home visiting service from 30 September, in line with decisions taken by Hertfordshire County Council, Herts Valleys CCG and Cambridge and Peterborough CCG
• the CCG’s Children’s lead works with localities and the voluntary sector to review and agree how the existing budget of £86,100 is used to support vulnerable families who may not be accessing children’s centre services, to improve their health outcomes. The proposed recommendations from this exercise should be reviewed in January 2016 at the latest.
• notes that Hertfordshire County Council scrutiny committee will be reviewing children’s centres in autumn/winter 2016, including the extended scope to reflect the changes in home visiting service provision.

1
Proposal for the future of funding for the Home Visiting Service (Home-Start)
1. Purpose of the Paper To provide an overview and summary of the current provision within East & North Hertfordshire CCG, including recent improvements in statutory service provision and to provide the Governing Body with recommendations on the development of future provision.
2. Context and Background A volunteer-led, befriending, home visiting service for families with young children is currently provided through nine Home-Start schemes across the county. The CCG currently jointly funds this service with Hertfordshire County Council, Herts Valleys CCG and Cambridge and Peterborough CCG. There are only four home visiting schemes within the East and North Herts CCG area: (Stevenage, North Herts, East Herts and Welwyn and Hatfield). Each scheme has a contract with Hertfordshire County Council. The CCG’s contribution is in the region of £86,000 per annum, representing about 14% of the total costs of the current schemes across the county.
The CCG has received a paper from Home-Start Hertfordshire setting out the work they undertake across the County. (Attached to this paper as an appendix). The CCG is aware that feedback from service users of the home visiting service is very positive, with a range of benefits identified by families themselves including support with mental health issues and accessing services. This is work which aligns with our strategic objectives around reducing health inequalities, our commitment to supporting vulnerable families’, and giving a focus to the prevention of ill-health. There is also acknowledgement of the important role that “third sector” organisations and volunteers play in working across the County.
In July 2015, Hertfordshire County Council considered a report setting out the funding proposals for Home-Start’s home visiting service. Hertfordshire County Council agreed that the current home visiting service, provided by the nine Home-Start contracts, will not be retendered when they expire in September 2015.
Hertfordshire County Council’s scrutiny committee plans to scrutinise Children’s Centres in autumn/winter 2016. In the light of the decision to cease funding for Home-Start’s home visiting service, the scope of this scrutiny has been expanded to include ‘the effect on the provision of a Home Visiting Service caused by the change in policy’.
A range of evidence was considered to inform this decision. For example, the funding to support 395 families countywide per annum, at a cost of approximately £1450 per family is approximately twice the cost per family of services delivered via Children’s Centres.
2
The Home-Start home visiting service has been operational for many years and its existence pre-dates the following developments in statutory services:
• An increase in statutory duties for under-5s and their families in
Hertfordshire. This includes the development and expansion of the free offer of nursery education to three and four year olds, free early education places for eligible two year olds and an early years pupil premium for three to four year olds with additional needs
• The major expansion of 82 Children’s Centres as the main avenue of support to families with children under the age of 5, including a higher level of support to vulnerable families.
• The expansion of the Health Visiting Service and the introduction, in targeted areas, of the Family Nurse Partnership.
• The re-commissioning of the children’s centre programme has focused on retaining an element of the universal offer whilst increasing targeted support. Children’s centres record any risk factors families have, and now offer a higher level of support to vulnerable families. The contract includes service targets to register 100% of all families within a group, including 100% targeted families, and to maintain meaningful contact with 80% of those targeted families
• Health visitors are now distributed across the county, on weighted deprivation by caseload and not GP practice. Health visitors continue to have monthly partnership meetings with GP practices to discuss with the Safeguarding GP lead any concerns re safeguarding, mental health, or domestic violence within the locality. There is one named Health visitor per children’s centre.
• The number of formal targeted health visitor assessments /reviews have been increased. Reviews now take place within the first 10-14 days, at 6-8 weeks, 8-12 months, 24-30 months and 36 months- 5 years. Children assessed as having high levels of need are additionally reviewed at 5-7 years.
• The work force growth as a result of the Healthy Child Implementation plan is from 177 to 229 whole time equivalents including 6 Family Nurse Partnership nurses. This is to deliver a significantly greater offer in the Healthy Child programme to families across the county.
• As part of developing better access to mental health services by 2020, Hertfordshire CCGs will receive approximately £2m in additional funding per year from 2016/17. One of the priorities areas for commissioners will be the expansion of local perinatal mental health services for vulnerable women.

3
3. Children’s Centres Current Capacity and Reach 2015
Access targets are monitored monthly: • 100% registration • 65% engaged, • 80% of targeted families to have meaningful contact
Current position: • 90.8% registered – 69,920 children • 76.7% engaged – 59,038 children • 24% one or more risk factors – 18,350 children
Capacity of Outreach work from Children’s Centres since April 2015
Impact of outreach work 2015/16 countywide: Families are supported to access services and develop peer support groups
Number of families receiving intensive outreach support from children’s centres
Number of families who have received outreach and then go on to access other children’s centre services
5119 3737

4
Children‘s Centre Quality
Core menu of Children’s Centre Services
• All Sure Start children’s centres work closely with parents and support parents to access a range of services. Each group of children’s centres supports young children and their families by offering a core menu of services in the following areas:
Supporting child development
All centres support child development, particularly speech and language and run groups for babies and toddlers or link with community based toddler groups
All children’s centres work closely with the child-minders, pre-schools, day nurseries, nursery schools and nursery classes in their geographical area and can support parents to access a place for their child
All centres can support parents to access free early education places for 2, 3 and 4 year olds
Outreach and family support
All centres provide support and information for all families as well as specific one-to one support for more vulnerable families through home visits or targeted groups
All centres use assessment tools such as eCAF, Graded Care Profile or Family Plus Outcome Star to assess the needs of a family and develop an action plan to support them

5
Parenting support All centres provide information and advice on parenting skills at significant transition points for the family (e.g. pre- birth, early days and settling into childcare or school
All centres offer Bookstart activities to encourage parents to read with their children
All centres offer access to evidence based parenting programmes i.e. Family Nurturing Links Programme (also known as the Parenting Puzzle)
Access to training and work opportunities
All centres provide support for parents and carers who want to access training via the centre or local adult learning providers
All centres providing support for parents to find employment including links with local Job Centre Plus advisors
All centres encourage and support volunteering Child and family health services (including those delivered by community midwives and health visitors)
Each children’s centre group provides a range of family support, health and information services for all families.
Many centres host baby clinics run by the local health visiting team and some centres offer access to community midwives
Support Hertfordshire Public Health strategy
All centres provide sessions on healthy eating, breastfeeding-support and first aid training for parents
All centres distribute FREE Healthy Start vitamins Centres promote childhood immunisations, stop smoking
programmes and dental health
It should be noted that health visiting and children’s centre outreach services do not provide a like-for-like replacement for Home-Start’s home visiting services.
4. The Hertfordshire Financial Context
The key elements of the system financial context are: • £62.5m spent on early education provision, following rapid growth, funded by
Direct Schools Grant • £16m is shortly expected to be transferred from Public Health England in a
grant for Health visitors, to reflect the increased ‘universal offer’ to be provided by Health Visitors in delivering the Healthy Child programme.
• £13m from Hertfordshire County Council for Children’s Centres after recent reconfiguration and reductions.
• The Health Visitor Implementation plan has increased the numbers of whole time equivalent health visitors by 68, to 229
Comparative costs of family support
The Home-Start home visiting service is for families in need in the areas with a Home-Start scheme, who have at least one child under five. The service is provided

6
on a weekly basis by trained and supervised volunteers for up to 9 months, more in exceptional cases. The current level of service is determined by the available funding rather than any assessment of the need and/or impact. Referrals are mainly through self-referrals (20%), health visitors (36%) and Children’s Centres. Overall 3% of referrals come from GPs.
The cost for the current contract is £1,450 per funded family for a home visiting package of support from Home-Start, or £16.50 per hour of a Home-Start volunteer’s time.
Children’s centres in Hertfordshire are funded to provide an average of approximately £170 of support per child registered with that Children’s Centre. This is universal funding, for every child in Hertfordshire aged from 0-5. Children centres qualified outreach support staff cost on average £14 an hour
There are four Home-Start home visiting schemes currently funded by the CCG as summarised in the table below: Scheme name Referrals target CCG contribution
(per annum) Number of new referrals supported between 01 January 15 and 31 March 2015
Stevenage 43 • £20,260 6 North Herts 43 • £20,351 10 East Herts 46 • £25,290 2 Welwyn Hatfield 43 • £20,200 2 175 Total £86,100
A limited qualitative review of referrals to home visiting by Home-Start was completed in November 2014. The review identified the following areas in which Home-Start had offered support:
• Mental health • social isolation • physical health • advice and access to other services and increasing self-confidence
Of the areas highlighted, the highest demand was for help with mental health and social isolation issues. The service was found to be popular with service users. However, although the service is both personalised and valued by service users and health visitors, it has been difficult to measure the impact on health outcomes. 5. Transition Arrangements
To support the transition period associated with ending the contract, the County Council has provided £200,000 in 2015/16 for transition funding. A more detailed plan for the use of this will be developed with the managers and trustee of the nine

7
Home-Start schemes in Hertfordshire. The on-going needs of families currently being supported through the contract will be assessed on a case-by-case basis. If a family is currently receiving support through the contract:
• Where families are actively involved with their local children’s centre, the Home-Start co-ordinator and children’s centre manager will agree on the best future support for the family
• Where it is agreed that support from Home-Start should continue for the remainder of the 9 month support period, the scheme will be funded to continue that support at the current contract rate.
• Home-Start schemes currently also support families who are not funded through the HCC and CCG contract. Discussions will take place with the schemes to clarify what the criterion for any support in the future will be. Children’s centres are funded to reach all families within their community and to provide access to a universal offer of early year’s services- health, care and education.
• HCC has established a new Children’s centre online service request form,
which is ready to launch to all GP practices. This will provide a quick and easy way to request support for a family from their local children’s centre.
6. Recommendations
It is recommended that:
• the CCG Governing Body members agree to cease the CCG’s funding for a home visiting service from 30 September, in line with decisions taken by Hertfordshire County Council, Herts Valleys CCG and Cambridge and Peterborough CCG
• the CCG’s Children’s lead works with localities and the voluntary sector to review and agree how the existing budget of £ 86,100 is used to support vulnerable families who may not be accessing children’s centre services, to improve their health outcomes. The proposed recommendations from this exercise should be reviewed in January 2016.
• notes that Hertfordshire County Council scrutiny committee will be reviewing children’s centres in autumn/winter 2016, including the extended scope to reflect the changes in home visiting service provision.
Kate Barker Assistant Director- Children, Young People and Maternity Commissioning September 2015

8
Appendices
1. Report received from Home-Start- The future of Funding for Home-Start- East and North Hertfordshire CCG.

Home-Start Hertfordshire supporting families countywide
5, Bedwell Park, STEVENAGE, Herts. SG1 1NB Tel: 01438-367788/365533 Fax: 01438-365533
E-mail: [email protected]
Company Number 8301552
09 September 2015 Dear Kate The Future of Funding for Home-Start I understand that East and North Herts Clinical Commissioning group is considering this matter and a decision regarding the funding for Home-Start will be decided at the next meeting of the Governing Body on 24th September. I have attached a detailed report with further information that I hope you will find useful when this matter is under consideration. Summary of Report
• Home-Start is a home visiting service for families in need with at least one child under five across the whole of the county, urban and rural, deprived and affluent
• The service is provided on a weekly basis by trained and supervised volunteers for up to 9 months (more in exceptional cases)
• No other service provides ongoing regular support to families for 2 – 3 hours per week.
• Health Visitors visit a family twice – once after the birth and the second time at 10 weeks. They do not provide ongoing practical support. Where this is needed – a referral is made to Home-Start. Health Visitors do not have the capacity to take on this service- hence the referral rate from Health Visitors to the service.
• At present, outreach services provided by Children’s Centres are limited to up to 6 weeks with a task specific focus, spasmodically and with no continuity –hence the number of referrals from Children's Centres for ongoing support.
• Home-Start works with families who will not access statutory services and we then work with the family to access those services.
• Our service is cost effective - approximately £1300 to support a family for a year. • Our service saves the NHS money through its preventative work, avoidance of
missed hospital appointments etc. • Our service enables the CCG to meet its stated priorities • Hertfordshire risks losing the experience, skills, and commitment of our volunteers.

2
Conclusion The County Council’s decision to cease funding Home-Visiting services will fundamentally change the landscape of the services available to families and children across the county. In the East and North Herts area, a well-used, well-respected local service is now under threat. Our Boards of Trustees, staff and volunteers are doing all that we can to ensure some form of service continues. We are currently looking at our organisational structure and developing a business plan for the future which will involve considerable re-structuring to support a more cost effective delivery model. However, it is an enormous challenge to make up the shortfall over such a short period and secure the service beyond the end of this financial year. The loss of our service will impact on health provision and we hope that that the CCG will decide to continue to fund this invaluable service. Many thanks for your time in reading this letter and if you require anything further, please do not hesitate to get in touch. Yours sincerely
Pauline Kellett Chair, Home-Start Herts

3
Home-Start in East and North Herts Introduction Home-Start UK was established forty years ago and is now one of the largest providers of support to families with children under five in the United Kingdom. There are four Home-Start schemes in the East and North Herts area.
• East Herts
• North Herts
• Stevenage
• Welwyn/Hatfield
The above schemes were formed to meet local demands for the service. Our core service provides volunteers, who are themselves parents, to provide impartial support, befriending and practical help to families under stress, preventing crises arising and the family unit breaking down. Trained volunteers visit families in their homes on a regular basis. Service delivery is based on a network of locally governed and managed centres. Each centre is an individual charity, with a Board of Trustees from the local community Families supported face difficult situations, have to deal with a wide range of problems and are from very different backgrounds. The service provided is holistic, based on the needs of the whole family. Volunteers are carefully selected and are required to undertake a training programme including child protection, cultural and disability awareness and confidentiality. Contribution to the CCG’s Strategic Priorities Healthy Child Programme The Healthy Child Programme (covering pregnancy and the first five years of a child’s life) is the early intervention and prevention public health programme for children and families. It supports improvements in the health and wellbeing of children, as part of an integrated approach to supporting children and families. The focus of our work is with children under five and there is clear evidence to show that what happens to children before they are born and in their early years can affect their health and opportunities later in life. Children who grow up in a safe environment and have a healthy relationship with their parents are more likely to do better as they go through life.

4
Our work is focused on helping parents give their children the best possible care. The aim is to help children be as healthy as possible by preventing illness, and encouraging healthy behaviours from pregnancy onwards. We do this by :-
• helping parents develop a strong bond with children
• identify problems in children’s health and development (e.g learning difficulties) and safety (e.g parental neglect), so that they can get help with their problems as early as possible
• make sure children are prepared for school
• enable parents to access other services e.g. health appointments
• refer parents to other support networks e.g. community groups, food banks etc. ·
• providing parents with information and advice on Home-Start and other services
• providing advice to parents on how to encourage a healthy diet and physical activity in young children
The Case for Change As indicated above, much of our work is preventive, working with families to address a range of issues that can impact on a child’s development in later life. We are an integrated service and work in partnership with a range of agencies – in particular with the health visiting service. We also work with other statutory and community organisations and help to fill the ‘gaps’ in current provision. Our services are local – we are unique in working with families in their own homes to work on the needs of the families as identified in the initial referral. Much of our work is supporting mothers and children with mental health problems, to ensure that help is received as early as possible, to reduce the impact of poor mental health on a child, and to prevent problems extending into a child’s later years. As can be seen from the figures below, we have seen a significant rise in the number of referrals because of mental health issues. Removing funding for Home-Start further erodes the limited options for women with mental health issues and places further pressure on the already over stretched local mental health services. The Mental Health Foundation Trust in Hertfordshire is itself under budget pressures and any loss of the service provided by Home-Start will inevitably result in greater delays in vulnerable women and children receiving treatment.

5
What we do
Children and families experience a range of needs at different times in their lives. However, while all children and families require access to high-quality universal services, some of them also benefit from extra support to address additional needs, which may relate to health, social welfare, education or other areas. An estimated 20-30% of the population have additional needs at some point in their lives. In order to achieve the best outcomes for all children it is important that this additional support is delivered at the earliest opportunity via a whole systems approach through integrated practice. This supports both national and local policy drivers. The key partners we work with to deliver this whole system approach include:
• Health Visitors
• Children’s Centres
• GPs;
• School Nurses.
• HCC Social Workers;
• Relevant Voluntary and Community Sector organisations e.g. Women’s Refuge, Asian Women’s’ Organisation, CAB;
• HCC’s Thriving Families Service;
• Schools
We were commissioned by the County Council to offer a family focussed service over a defined period agreed with the family at the initial meeting based on outcomes identified, for a maximum period of up to 9 months (longer in exceptional circumstances). The core offer is two – three hours per week for each family, which is determined by identified need. Referrals to the schemes come from a number of routes by various different agencies. As well as one to one work, we also undertake the following work;
- Supporting parents who have experienced Domestic Violence and Abuse
- Support groups for parents who are socially isolated
- Supporting parents with mental health issues including post-natal depression , stress and anxiety
- Positive Beginnings sessions. All provide extra support for families with a range of professionals on hand including Speech Therapy Assistants, Nursery Nurses, Children’s Centre Staff and Home-Start Group Worker.

6
- Qualified to teach Nurturing Links Parenting Puzzle course and have taught our volunteers to embed the learning in family’s own home.
- Enabling families to access healthy eating and parenting programmes
- Providing employability courses for volunteers and families enabling them back to a work environment
- Welfare assistance scheme to support families in financial crisis to access cleaning products for their home
FAMILY REFERRALS to HOME-START Referral demographics: Years Families supported
ST NH E W/H Children supported ST NH E W/H
Volunteers ST NH E W/H
2012-2013 90 83 126 47 220 254 232 116 45 49 57 29 2013-2014 91 84 98 50 216 234 220 115
37 51 55 33
2014-2015 100 57 106 34 201 200 185 78 32 45 64 24 Top 3 Presenting Issues 2014/15:
Stevenage North Herts East Herts Welwyn Hatfield Mental Health Mental health Mental health Mental health Isolation & low self esteem
Lone parent Lone parent Isolation & low self esteem
Managing children’s behaviour
Domestic abuse Postnatal depression
Managing children’s behaviour/
Referral Source 2014/15: Stevenage North Herts East Herts Welwyn/Hatfield Self 44% 18% 12% 8%
HV/GP 35% 61% 41% 44% Children’s Services
11% 7% 2% 3%
Children’s Centres
7% 8% 24% 22%
Other inc Education
3% 8% 21% 20%

7
The report to the County Council’s Children’s panel in June, made clear that the main justification for the decision not to commission a Home Visiting Service was the expansion of children’s centres and the extension of Health Visiting services. The above figures (and those of the first three months of this year mirror them) fundamentally challenge this view. If Health Visitor services are expanding to such an extent that our service is no longer required why are over 36% of our referrals from Health Visitors and 20% from Children’s Centres and other Children’s Services? Experience suggests the opposite is the case. Demand from statutory services is rising not falling and we are increasingly filling the gaps in statutory provision. There is also a big increase in self referrals. Our referrer’s views on the service are: This service is very valuable. Home-Start provided a bridge that took a young mother living at home to independent living. CSF is not able to do this.’ (Social worker)
Having the ability to refer families to Home-Start is invaluable. Their volunteers are competent, friendly and non-judgemental, enabling them to form good relationships with and provide vital support to families who are experiencing adversity.(Health Visitor)
‘Home-Start did well to encourage the family to accept help in the first place. It has made it easier for them to physically get out and emotional support for the mum who has an awful lot to cope with.’ (Health Visitor) ‘This family suffered a colossal bereavement and the volunteer was literally a life-line. Mum was agoraphobic and the volunteer was instrumental in getting her out and about again.’ (Health Visitor) ‘Home-Start helped this family with isolation and practical everyday support.’ (Health Visitor) Finance The Hertfordshire Home-Start schemes were jointly funded between Hertfordshire County Council’s Children’s Services, Herts Valley Clinical Commissioning Group, East and North Herts Clinical Commissioning Group and Cambridgeshire and Peterborough Clinical Commissioning Group. The total cost for the nine schemes across Hertfordshire for the 2014/2015 financial year was £598,085.00, and is split as follows: Children’s Services £391,565 East and North Herts CCG £86,100 Herts Valley £103,220

8
Cambridgeshire and Peterborough £17,200 TOTAL £598,085 The individual schemes in this area were funded as follows: Scheme Name
CCG Children's Services
NHS Herts Contribution
Total
Stevenage East & North Herts £44,546 £20,260 £64,806
North Herts East & North Herts £44,343 £20,351 £64,694
East Herts East & North Herts £44,284 £25,290 £69,574
Welwyn Hatfield
East & North Herts £44,783 £20,200 £64,983
TOTALS £177,956 £86,101 £264,057 . Across North and East Hertfordshire, the average cost of supporting a family for a year is approximately £1300. Our service is cost effective and saves money in the long term through our early intervention work with families. Impact of our Service The report to the Children’s Panel in June dismissed the impact of the service we provide. Historically, the monitoring of the individual schemes to the County Council mainly revolved around quantitative analysis of numbers of families supported and the types of issues with which each family was being supported. The qualitative aspect revolved around each scheme submitting 2–3 case studies of families supported. However, in order to gain a more accurate analysis of the effectiveness of the schemes and whether identified family outcomes are being met, a further two monitoring processes were introduced for the 2014/2015 financial year focussing on outcomes and direct family feedback. Children’s Services also sought direct feedback from a sample of those families that had received Home-Start support to gain their views of the value of this service. Each Home-Start scheme was visited in early October 2014 and commissioners posed a number of questions to supported families. Below is a summary of the key benefits raised by families:
• There are a number of different referral routes into the Home-Start scheme and Home-Start volunteers can signpost families to other support networks;
• Many families supported initially feel isolated and do not have a wider family or friendship circle;

9
• A number of families lack the confidence in some key areas of family life, such as family planning, family finance, accessing benefits/other services, parenting skills (especially where a family has a child with additional/special needs), forward planning to attend GP/Dentist/hospital appointments, effective homework regime;
• A number of families feel that the statutory sector can be too judgemental and that the Home-Start volunteers are not, which gives families the confidence to try new methods of developing their children and wider family life;
• When the volunteer visits this can enable the parent(s) to be able to spend more quality time with their children;
• Non-invasive support; • All the families questioned looked forward to their volunteer’s visit, as a means of
friendship and support.
The value of our service is exemplified by one family‘s experience and how input from our service enable the whole family to cope. Our service not only enables children to thrive but whole families when faced with the worst of times – often health related.
A family perspective
"When my child was injured during her birth, as first time parents all our dreams, hopes, expectations and intentions fell apart there and then. All we had was a dark and foreboding prognosis. A bleak and virtually hopeless future. And there is no doubt, none whatsoever, that without Home-Start, we would not be here today. I would have been unable to return to work (under threat of redundancy) in order to pay the bills and keep the roof above our heads. My wife would have been unable to attend the multiple weekly consultants, doctors, specialist, educational, physiotherapy and hospital appointments. Without Home-Start, my wife would have spent much more than the first five months of our child's life locked in a hospital room. Believe me, I could go on, and on, and on... and on. We are intelligent, logical and high-functioning individuals. Without Home-Start, we would have collapsed. Failed. crumbled and who knows what more. We have been through three years of utter terror, complete and unyielding horror. Thank the gods for Home-Start. Thank everyone and everything for Home-Start. I don't dare imagine the terror less educated and financially able families now face. Nor the increased financial costs on the NHS, local doctors, medical providers and suppliers – and the wider community infrastructure. No-one who has had need of Home-Start would ever doubt your commitment, your value - or the financial impact of not having you there." A Father with a disabled child

10
Set out below are further examples of how our work supports the work of health services, Stakeholder Input
Outcome
Parent suffering from depression
- Provided emotional support and encouragement - Helped parents develop routines and manage the children’s behaviour positively - Mother’s confidence grew and she came off of anti depressants
- Medical intervention no longer necessary. - Family came off benefits and into employment - Reduced worklessness
Parent with disabled child
- Helped parents identify and access appropriate services - Transported/accompanied parents to appointments for support or to help with other children. - Medically trained Volunteer provided information and reassurance where appropriate
- Parents more informed about available services so accessed them sooner - Reduced financial implication of hospital visits (public transport, parking, child care for siblings) - Reduction in number of appointments cancelled or changed - Less demand on the community nursing team
Socially Isolated parent
- Support parental engagement with their children’s play and learning - Enabling parents to get out so their children can develop social skills and exercise - Practical support around cooking and diet
- Child achieved developmental milestones, no intervention required from paediatric services - Improved School readiness reduced the need for extra support in schools - Less need for additional services such as speech and language therapy
Volunteers
- Extensive ongoing training covering a range of subjects and areas
- Professional qualifications/ higher educational attainment - Increased employability

11
- Experience of meeting ad working with a diverse range of people - Back to work skills enhanced
-Financial stability - Increased self-worth and confidence - Improved mental health
Our families said of our service ‘I appreciate that my volunteer helps me because she wants to, not because she’s paid. She’s helped me to be more confident when dealing with my children and to use my voice. I am more able to access services for my child with special needs. I look forward to my volunteer’s visit every week. Without Home-Start I would have been isolated, depressed and felt unsupported. My children would have suffered.
If it wasn’t for Home-Start I wouldn’t be here, and my children would be in care!’.
Very professional and informative, my volunteer was extremely helpful, caring and non-intrusive, a lovely person who I felt I could trust. Home-Start gave me light at the end of the tunnel I knew the day I saw my helper I would be ok. Thank you to everyone at Home-Start who helped and supported me.
A fantastic service – should be on the NHS! I, Volunteers The importance of using volunteers to deliver directly our service should not be underestimated. We have no difficulty in recruiting volunteers and for example in Stevenage have just completed a Preparation Course for 8 new volunteers. They will be matched shortly with families. Comments on the training and the supervision received
‘The supervision and support offered by the co-ordinators is extensive and easily accessible.’ ‘We have 1-1 supervision every 4 weeks, and our supervisor is always at the end of the phone. I find group supervision really helpful, where we share our experiences with other volunteers.’ ‘An excellent well-structured course that was delivered in a very professional way.’
‘The course helped me to be clear about the role of a volunteer, their responsibilities and boundaries.’
Our families recognise the value of the support they receive from the scheme, especially from their allocated volunteer. All families consulted by HCC view our service as critical and

12
not just for providing support, practical advice and friendship but as a non-critical friend that the families can use to improve the quality of their lives and use the volunteer’s practical experiences to benefit the family unit as a whole. The report to the Children’s panel stated that children’s centres will be encouraged to make contact with existing volunteers who might wish to explore continuing to volunteer but with a somewhat different remit and via a different service provider. This statement displays the lack of understanding of the unique volunteering experience offered by Home-Start. Volunteers chose to volunteer with us – because we are not a statutory agency, the quality of the training provided and the ongoing training support and supervision. As an organisation Home-Start has over 40 years’ experience of training volunteers and matching them with the needs of families. Our type of volunteering requires a high level of commitment, training, support, and supervision. It could be categorised as ‘formal volunteering’ and is therefore distinct from the model of informal volunteering that is common in most other organisations. Research has shown that Home-Start Volunteers are motivated to become volunteers with Home-Start, as the work is perceived to be close to their own personal experience (volunteers must have parenting experience) and they feel they have something to offer. Hertfordshire risks losing the experience, skills, and commitment not only of our volunteers but all the other scheme's volunteers. Anecdotal evidence from our volunteers is that they are unlikely to continue volunteering and would not wish to work in the children’s centre context should the scheme be unable to continue. Home-Start offers a unique service to families experiencing difficulty in times of crisis. The service is tailored to individual requirement and is responsive to local unmet need. The service is preventive and offers early intervention thereby reducing the need for families to require further intervention from statutory services particularly health services that is more costly.
Agenda Item No: 14
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Annual Audit Letter
Decision Discussion Information Follow up from last meeting
Report author: PricewaterhouseCoopers LLP
Report signed off by: Anna Blackman / Alan Pond
Purpose of the paper: Required by statute following the completion of the audit.
This letter relates to the 14/15 audit, and summarises key findings of our audit.
Conflicts of Interest involved:
None known.
Recommendations to the Governing Body:
Review and consideration.

www.pwc.co.uk
Annual Audit Letter
East and North HertfordshireClinical Commissioning Group
Year ended 31 March 2015
July 2015

PricewaterhouseCoopers LLP, Savannah House, 3 Ocean Way, Ocean Village, Southampton, SO14 3TJT: +44 (0) 23 8033 0077, F: +44 (0) 23 8020 2244, www.pwc.co.uk
PricewaterhouseCoopers LLP is a limited liability partnership registered in England with registered number OC303525. The registered office ofPricewaterhouseCoopers LLP is 1 Embankment Place, London WC2N 6RH. PricewaterhouseCoopers LLP is authorised and regulated by the Financial Conduct Authorityfor designated investment business.
The Audit CommitteeEast and North Hertfordshire Clinical Commissioning GroupCharter House,Parkway,Welwyn Garden City,AL8 6JL
July 2015
Ladies and Gentleman
We are pleased to present our Annual Audit Letter summarising the results of our audit for the yearended 31 March 2015. We look forward to presenting it to the Governing Body of East and NorthHertfordshire Clinical Commissioning Group on 22 July 2015.
This is our final year as auditors of East and North Hertfordshire Clinical Commissioning Group andwe would like to thank management and staff for their assistance during the course of our audit work.
Yours faithfully
PricewaterhouseCoopers LLP
Code of Audit Practice and Statement of Responsibilities of Auditors and of Audited Bodies
In March 2014 the Audit Commission issued a revised version of the ‘Statement of responsibilities of auditors and of audited
bodies’. It is available from the Chief Officer of each audited body. The purpose of the statement is to assist auditors and
audited bodies by explaining where the responsibilities of auditors begin and end and what is to be expected of the audited
body in certain areas. Our reports and management letters are prepared in the context of this Statement. Reports and letters
prepared by appointed auditors and addressed to members or officers are prepared for the sole use of the audited body and no
responsibility is taken by auditors to any member or officer in their individual capacity or to any third party.

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC Contents
Contents
Introduction 2
Audit findings 3
Appendices 5
Appendix A. Summary of recommendations 6
Appendix B. Final fees 8

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC 2
The purpose of this letter
This letter provides the Governing Body of East and North Hertfordshire ClinicalCommissioning Group (“the CCG”) with a high level summary of the results of ouraudit for the year ended 31 March 2015, in a form that is accessible for you and otherinterested stakeholders.
We have already reported the detailed findings from our audit to the AuditCommittee in the following reports:
Audit opinion on the financial statements for the year ended 31 March 2015,incorporating the value for money conclusion and the regularity opinion.
Report to those charged with Governance (ISA (UK&I) 260).
We have included in this report our significant audit findings. You can find asummary of our key recommendations in Appendix A.
Scope of work
We carried out our audit work in accordance with the Audit Commission’s Code ofAudit Practice (NHS), International Standards on Auditing (UK and Ireland) andother relevant guidance issued by the Audit Commission.
You are responsible for preparing and publishing the CCG’s financial statements,including the Annual Governance Statement. You are also responsible for putting inplace proper arrangements to secure economy, efficiency and effectiveness in youruse of the CCG’s resources.
As auditors we need to:
form an opinion on the financial statements; form an opinion on the regularity of the CCG’s transactions; form a conclusion on the arrangements that you have in place to secure
economy, efficiency and effectiveness in your use of the CCG’s resources; review the CCG’s Annual Governance Statement; and carry out any other work specified by the Audit Commission.
We have carried out our audit work in line with our 2014/15 Audit Plan that weissued in March 2015.
Introduction

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC 3
AccountsWe audited the CCG’s accounts in line with approved Auditing Standards and issuedan unqualified audit opinion on 28 May 2015.
We did not identify any significant issues during the course of our audit work.
Our Regularity OpinionWe give our opinion on whether, in all material respects, you have used the CCG’smoney as Parliament intended and whether you have done so in accordance with thevarious authorities governing the transactions. We issued an unqualified regularityopinion on 28 May 2015.
Our value for money conclusionWe carried out sufficient, relevant work, in line with the Audit Commission’sguidance, so that we could conclude on whether you had in place, for the year ended31 March 2015, proper arrangements to secure economy, efficiency and effectivenessin your use of the CCG’s resources.
In line with Audit Commission requirements, our conclusion was based on twocriteria:
The organisation has proper arrangements in place for securing financialresilience; and
The organisation has proper arrangements for challenging how it secureseconomy, efficiency and effectiveness.
To reach our conclusion, we carried out a programme of work that was based on ourrisk assessment.
We issued an unqualified value for money conclusion. However, we found thefollowing matters which we wish to bring to your attention:
Monitoring QIPP deliveryThe QIPP target for the year was £7.47m, and this was reported as met by the CCG.As part of our work, we have reviewed the CCG’s arrangements for monitoring thedelivery of the QIPP programme. The Strategic Plan assigns clear ownership ofschemes to the CCG’s four Programme Boards – and as part of work we reviewed thepapers and minutes of the Programme Boards to determine if there was evidenceavailable to demonstrate the delivery of QIPP programmes was being monitored. Ourreview of the reports produced for the Programme Boards and the minutes of themeeting indicated there was minimal evidence of monitoring of budgeted versusactual spend for individual QIPP schemes.
Due to the nature of the QIPP programmes it is challenging for the CCG to monitorthe financial impact of individual schemes as a number are designed to impact thesame area (i.e. reducing emergency admissions) so the CCG tracks financial deliverythrough its monitoring of the overall financial position.
The CCG has successfully delivered a 1% surplus for the past two years and hastherefore delivered its QIPP schemes but as QIPP schemes become more challenging
Audit findings

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC 4
or complex, the CCG may benefit from more specific reporting and/or projectmanagement to support the delivery of the QIPP schemes.
Local health economyAs part of our work, we have reviewed how the CCG has responded to the financialissues identified at Princess Alexandra Hospital (PAH) and East and NorthHertfordshire Trust (ENHT), both of which reported significant deficits in excess ofthose budgeted for 2014/15. PwC has reviewed evidence which demonstrates that theCCG has engaged in ongoing dialogue with both Trusts including through regularperformance meetings held with ENHT or in the case of PAH signing up to theCommissioning for Value: integrated care pathways initiative, a work programmethat provides CCGs with support to identify priority programmes which offer the bestopportunities to improve healthcare for populations.
In future periods, financial pressures are likely to increase on the CCG’s localproviders, in line with the national trends of increasing demand and pressures onfunding. A review was undertaken in 2007 to review the future strategic direction ofservices in the local health economy – this remains the work that underpins theCCG’s strategic and operational plans. There are significant pressures on all CCGsand providers and that context it is important that the CCG continue to workproactively with its partners and local providers to address issues of financial andoperational sustainability.
Financial positionThe CCG reported a surplus of £7.74m for 2014/15 and is forecasting a QIPP saving of£11.98m for 2015/16 but the various financial pressures faced by its local providerswill need to be considered in the long-term if increasing surpluses are hoped to bemet. The forecast surplus for 2015/16 is £7.74m.
Annual Governance StatementThe aim of the Annual Governance Statement is to give a sense of how successfullythe CCG has coped with the challenges it faces and of how vulnerable theorganisation’s performance is, or might be.
We reviewed the Annual Governance Statement to see whether it complied withrelevant guidance and whether it was misleading or was inconsistent with what weknow about the CCG. We found no areas of concern to report in this context.

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC 5
Appendices

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC 6
Recommendation Management’s response TargetImplementationDate
Retention of signed contractsWe have noted during our testing that theCCG has not retained a signed copy of theSecondary Care expenditure contract forHertfordshire County Council.
We recommended that the CCG retain allcurrent signed documents.
East and North HertfordshireCCG’s policy is to retain allsigned contracts.We will endeavour toimplement controls whichensure that all significantcontracts retained and areaccessible.
September 2015
Monitoring of QIPP programmesThe CCG has successfully delivered a 1%surplus for the past two years and hastherefore delivered its QIPP schemes but asQIPP schemes become more challenging orcomplex, the CCG may benefit from morespecific reporting and/or projectmanagement to support the delivery ofthe QIPP schemes.
We recommended the implementation ofrobust monitoring procedures of the QIPPprogramme.This could involve agreeing measurementsaround appropriate KPIs, the introductionof clearly defined milestones, andperforming actual vs budget monitoring ona regular basis.
East and North HertfordshireCCG will reassess the currentQIPP programmes that are inplace, and look to ensure thatthese offer specific andmeasurable targets which canhelp achieve the savingsrequired over the coming years.
September 2015
Onboarding of the CSUFollowing the on-boarding of theCommissioning Support Unit, ICT andFinance services were taken in-house fromOctober 2014. However we note that:(i) the Shared Service Agreement for ICTservices was not finalised until March 2015and the KPIs for the service were only at adraft stage at the date of audit fieldwork(May 2015)(ii) No formal set of KPIs had been agreedfor the Finance Services, and these servicesare monitored only
We recommended that KPIs relating to in-house ICT and Finance services should befinalised and formally approved at theearliest opportunity. In addition,performance monitoring meetings should beminuted to ensure that all actions arerecorded and followed up on a regular basis.
Now that the services beingdelivered by the CCG arestabilised, we will look toimplement KPI’s to ensure thatthe services offered are of anappropriate standard, as wellas the fees being exchanged areappropriate.
September 2015
Appendix A. Summary ofrecommendations

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC 7
Better Care FundThe Better Care Fund S75 agreement wasnot finalised prior to the go-live date on 1April 2015, and was not signed by the dateof audit fieldwork (May 2015)
We recommended that this documentshould be finalised and signed at the earliestopportunity
East and North HertfordshireCCG are looking to arrange thesigning of these documents atthe earliest opportunity.
September 2015

East and North Hertfordshire Clinical Commissioning Group - Annual Audit Letter July 2015
Annual Audit Letter PwC 8
We reported our fee proposals in our audit plan. Our actual fees charged were asfollows:
2014/15 outturn 2014/15 feeproposal
2013/14 finaloutturn
Financial statements 75,000 75,000 80,000
Use of resources 20,000 20,000 25,000
Total scale fee 95,000 95,000 105,000
Appendix B. Final fees


In the event that, pursuant to a request which East and North Hertfordshire Clinical Commissioning Group has received under the Freedom of Information Act 2000 or the EnvironmentalInformation Regulations 2004 (as the same may be amended or re-enacted from time to time) or any subordinate legislation made thereunder (collectively, the “Legislation”), East andNorth Hertfordshire Clinical Commissioning Group is required to disclose any information contained in this report, it will notify PwC promptly and will consult with PwC prior to disclosingsuch report. East and North Hertfordshire Clinical Commissioning Group agrees to pay due regard to any representations which PwC may make in connection with such disclosure andto apply any relevant exemptions which may exist under the Legislation to such report. If, following consultation with PwC, East and North Hertfordshire Clinical Commissioning Groupdiscloses any this report or any part thereof, it shall ensure that any disclaimer which PwC has included or may subsequently wish to include in the information is reproduced in full in anycopies disclosed.©2015 PricewaterhouseCoopers LLP. All rights reserved. 'PricewaterhouseCoopers' refers to PricewaterhouseCoopers LLP (a limited liability partnership in the United Kingdom) or, asthe context requires, other member firms of PricewaterhouseCoopers International Limited, each of which is a separate and independent legal entity.150602-113648-CM-UK

1
Agenda Item No: 15
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Commissioning Framework 2015/16
Decision Discussion Information Follow up from last meeting
Report author: Helen Edmondson
Associate Director Commissioning and Locality Development
Report signed off by: Denise Boardman Interim Director of Commissioning
Purpose of the paper: To provide an update on the Commissioning Framework
for 2015/16.
Conflicts of Interest involved:
None in the preparation of this paper
Recommendations to the Governing Body:
To note the contents of the paper

2
1. Introduction
This paper will update the Governing Body on the implementation and monitoring of the Commissioning Framework for 2015/16.
2. Acronyms
Commissioning Framework CF Long Term Conditions LTC
3. Appendices
Appendix 1 Performance Headlines from Quarter 1 of the 2015/16 Commissioning Framework
4. Background
The Commissioning Framework (CF) for 2015/16 was approved by the Governing Body in April 2015 following its development in consultation with Long Term Conditions (LTC) leads and practices. The CF has three elements:
1. Engagement 2. Supporting financial balance 3. Working to improve outcomes for patients with Long Term Conditions
(LTCs) The total available to practices through the CF in 2015/16 is £5 per registered patient, an increase of 50p on the previous year. The increase is to reflect the increased requirements for practices and additional of areas of carers and patients with cancer. The £5 is split across the three elements, £1 each for engagement and supporting financial balance and £3 for the third element. The Governing Body made the decision to pay 50% of the total sum available to each practice as an aspirational payment upfront. This payment was made to practices at the end of July with a clear message that there will be an end of year-end process to assess achievement against each of the indicators. The practices were also informed that there is an expectation that practices need to achieve 50% of the indicators by value and that further payment will be made to practices once this assessment has been completed. And where a practice achieves less than 50% by value, the aspiration payment will be clawed back to ensure that all practices only receive funding associated with their achievement.
5. Performance at Quarter 1
The Commissioning team has established a quarterly reporting process, to bring consistency across localities. Practices were required to submit their quarter 1 return at the end of July. These have been pulled together in a CCG wide spread sheet to enable monitoring. One practice has contacted the CCG to explain that they were having difficulties with the monitoring tool due to the changeover of their clinical system and changes to staff. The practice manager confirmed they would start submitting from quarter 2.

3
The practice achievement of the majority of the targets in the CF will be measured at the end of the year and there are no targets that require practices to have achieved them in totality by the end of quarter 1. The locality team will review and analyse the quarter 1 position and if practices are continuing to show poor progress in quarter 2, the practices will be followed up individually with support from relevant GP leads. The established reporting process provides a clear line of sight on how practices are performing. The information is reviewed at team and locality meetings, and some items inform the new Locality Information Pack e.g. Post Death Audits. During the implementation of the CF the team have responded to queries and points of clarification as they have arisen. Advice has also been sought from relevant GP Leads and Long Term Advisory Group.
The tables in appendix 1 provide the performance headlines from the quarter 1 returns.
6. Next Steps
The Commissioning team are committed to maintaining close monitoring of the CF and in line with this the team will provide a report to GP locality leads on each quarter. There will continue to be quarterly reports to the Governing Body, which is in line with the recommendations of the Internal Audit report as good practice.

1
Appendix 1: Performance Headlines from Quarter 1 of 2015/16 Commissioning Framework Please Note: The practice achievement of the majority of the targets in the CF will be measured at the end of the year and there are no targets that require practices to have achieved them in totality by the end of quarter 1. A. Facilitating self-management and integrated care planning for patients with Long Term Conditions
Measures Headline Performance at Quarter 1 At least once a year practices to develop a COPD action plan focusing on the practice’s performance with regard to COPD, in particular prevalence and emergency admissions. Action plan to be developed in either quarter 1 or quarter 2 and shared with locality LTC lead.
9 out the 58 practices have submitted their action plan. All plans are to be reviewed the locality LTC lead and the key themes to be discussed at the LTC Advisory Group meeting in November 2015
Accredited spirometry Training (standardised protocol) is accessed by at least 1 practice nurse. Evidence of the training and protocol being disseminated throughout the practice, across all staff groups. A calibrated spirometry machine is available for use, and evidence that is used.
14 practices reported that accredited training has been accessed. 20 practices reported that calibrated machine is available and been used.
Personalised Care Plan offered to patients with a LTC (those with any/all of the 3 diagnoses noted below) and in place for 50% of patients with:
• Diabetes - all type 2 • COPD – all • Heart Failure - all
Mixed picture of levels of achievement in making progress to meeting the target.

2
B. Proactive management of patients with long term conditions (LTC) by making use of multi-disciplinary team working
Measures Headline Performance at Quarter 1 Where indicated, patients will be referred to the Enhanced Primary Care Mental Health / IAPT Long Term Condition services, anticipated referral rate of least 15% of practice population.
Mixed picture of levels of achievement in making progress to meeting the target.
Practice hold an annual diabetes review meeting with the community diabetes team. Practice undertake pre visit questionnaire to prepare for the visit. At the end of the visit a diabetes action plan will be agreed to implement any recommendations.
8 out of the 58 practices reported that they have held their meeting. 5 out of 58 practices have provided action plan.
C. Advanced care planning (ACP) is initiated to support patients’ decisions and choices which will facilitate high quality end of life (EOL) care.
Measures Headline Performance at Quarter 1 Advanced Care Planning is undertaken for 0.75% of the practice population. A READ code will be added to the clinical notes to indicate Advanced Care Planning initiated or otherwise indicated.
15 out of 58 practices are making good progress with this target.
A Post Death Audit (PDA) is completed for all practice deaths where appropriate. A review of deaths will be undertaken at the monthly multi-disciplinary review meeting. The completed PDA will be submitted quarterly via the locality team, for review by the EOL GP clinical commissioning lead or Locality or LTC lead, to support practice learning.
Based on quarter one, 34 practices have completed PDAs on over 90% of deaths in their practice population.

3
D. Safe and appropriate prescribing to support practitioners to adhere to the broad spectrum antibiotic guidance
Measures Payment Proposal The practice will be required to develop and review the action plan by end of quarter 2 to follow up the baseline and re-audit undertaken in 2014/15 for the areas of Cephalosporins, Co-amoxiclav and Quinolones.
5 practices reported that have provided the action plan to pharmaceutical advisors
Practices should by means of an audit review and where appropriate, revise current prescribing practice to ensure that 3 day courses of antibiotics are prescribed where appropriate, in line with CCG prescribing guidance. All practices should review women with uncomplicated UTI who have been treated.
A small number of practices ( 4) have started to review relevant patients
E. Support improvements in line with CCG Ambitions for patients with Carers
Measures Payment Proposal Identify a Carer Champion by the end of quarter 2
24 of the 58 practices have identified their practice carer champion
Add those identified to the practice system and register, with the aim of having 3% of the practice population identified and added to the register.
6 practices have reported that they have identified over the half the patients required to meet the 3% target
F. Support improvements in line with CCG Ambitions for patients with Cancer
Measures Payment Proposal Review all cancer diagnoses made during emergency/unplanned admission to identify lessons learnt. Quarterly report provided to the CCG
16 out of 58 practice have reported that have reviewed diagnoses made during emergency/unplanned admission
Review all new cancer diagnosis for bowel, lung, gynaecology and breast: Quarterly report provided to the CCG
37 out of 58 practices have reported that they have reviewed new cancer diagnoses.

1
Agenda Item No: Item 16
Date of Meeting: 24 September 2015
Governing Body Meeting in Public
Paper Title: Emergency Preparedness, Resilience and Recovery
Decision Discussion Information Follow up from last meeting Report author: Sharn Elton, Director of Operations
Report signed off by: Beverley Flowers, Interim Accountable Officer
Purpose of the paper: This paper forms part of the annual business cycle within
East and North Hertfordshire CCG for Emergency Planning Resilience and Response (EPRR). The paper services 2 purposes:
1. To inform the board of the CCGs self-assessment against the annual core standards assurance framework for 2015/16 and
2. To inform the board of the work undertaken over the last 12 months to maintain the CCGs compliance with the Civil Contingencies Act (2004),state of readiness and resilience.
Conflicts of Interest involved:
None noted
Recommendations to the Governing Body:
The Governing Body is asked to note the work undertaken in the last 12 months and the progress that the CCG has made to increasing it resilience

2
Emergency Planning Resilience and Response (EPRR) Purpose of the Paper This paper forms part of the annual business cycle within East and North Hertfordshire CCG for Emergency Planning Resilience and Response (EPRR). The paper services 2 purposes: 1. To inform the board of the work undertaken over the last 12 months to maintain the CCGs
compliance with the Civil Contingencies Act (2004) our state of readiness and resilience and 2. To inform the board of the CCGs self-assessment against the annual core standards
assurance framework for 2015/16. Appendices
1. Core Standards Assurance self-assessment and compliance statement 2. Major Incident Plan 3. Incident Coordination Plan 4. Severe Weather Plan
Core Standards Assurance Self-Assessment 2015/16 This statement provides an overview of the CCG’s compliance with the NHS Core Standards for 2015/16. The compliance statement provides an update on the actions addressed over the last 12 months to ensure compliance in the outstanding areas identified following the 2014/15 assessment. Self-Assessment Process The CCG has self-assessed its emergency planning arrangements against the NHS Core Standards for EPRR (see appendix 1). Each compliance standard is RAG rated and details associated supporting evidence. Compliance against each standard has been assessed by the Director of Operations; peer reviewed by the Director of Nursing and Quality and signed off by the executive team. Compliance Statement The CCG has self- assessed itself as fully compliance against all 8 domains:
• Governance • Duty to maintain plans- emergency and business continuity • Command and Control • Duty to communicate with the public • Information sharing • Co-operation • Training and exercising • Deep dive subject- pandemic flu
Following the assurance statement from 2014/15 from NHS England the CCG has over the last 12 months focused on:
• Establishing a resource to ensure that it fulfils its statutory duties as a category 2 responder • Aligning risks to National and Local Resilience Forum (LRF) risk registers and sharing risk
assessments across the Local Health Resilience Partnership (LHRP) • Agreeing an interagency information sharing Memorandum of Understanding (MoU) • Supporting the development of the Hertfordshire Mass Casualties Plan • Training and exercising and • Securing Director level Accountable Emergency Officer attendance at the LHRP
The self-assessment process for 2015/16 has supported the development of the CCGs priorities for the forthcoming year notably: • Capability to deal with the most concerning issues on the community risk register

3
• Further development of the Hertfordshire Mass Casualties Plan to include designated P3 centres
• Supporting the development of the Hertfordshire pandemic influenza plan • Business Continuity including fuel planning EPRR Plans Major Incident Plan (appendix 2) In the last 12 months the plan has been updated as follows:
• Reviewing the communications section to reflect the coordination required across partner agencies
• Strengthening the referencing to the information sharing MoU • Strengthening the referencing to the finance process • Clear reference to the data protection policy • Adding a pandemic flu section to reflect the Hertfordshire Pandemic Flu Plan
In addition all NHS England references have been amended to reflect the organisational changes in the last 12 months. Incident Coordination Centre (ICC) Plan (appendix 3) In the last 12 months the plan has been updated as follows:
• To include a process for mobilisation of a remote ICC • Clear referencing to intranet access, outlining which documents can be accessed remotely • Clear process for accessing the incident email address
Business Continuity Plan In the last 12 months the plan has been updated to reflect the following structural changes to the CCG:
• The operations directorate • CSU transfers
Directorate Business Impact Assessments are currently being reviewed. Severe weather plan (appendix 4) In the last 6 months the CCG has written it severe weather plan to ensure that is aligns with NHS England guidance for 2015. The plan covers the response and actions required in response to the following adverse weather conditions:
• Heat • Wind • Rain • Snow and Ice • Fog
Health assumes the responsibility for leading the system response to severe heat. In particular CCGs are responsible for leading the system and co-ordinating the system response. At the declaration of alert level 3 the CCG must take the lead in ensuring that key providers and partners have taken appropriate action, including:
• Conducting risk assessments • Implementing response plans and ensuring message to the public and other multi agency
partners, as required Testing and Exercising

4
Training On call training was delivered during February 2015 to the majority of staff who participate in the duty manager rota (09.00-16.00hrs Mon-Friday) and those staff who are on call out of hours (including weekends and bank holidays). During the week of the 6 July 2015 the CCG focused on EPRR to raise awareness of the local and national EPRR agenda and more importantly allow staff to consider their individual contribution to EPRR delivery and build capability within the CCG. The following training was available to staff:
• General awareness • ICC training to familiarise staff with the ICC and its function • Loggist training for key staff identified to fulfil this function in the event of a major or prolonged
incident. In addition staff who participate in on call out of hours are accessing the NHS England strategic leadership in a crisis training which is aligned to the National Occupational Standards. This one day course is designed to support those who would be leading and coordinating the health response to an incident. In the last months six staff have attended the programme. Exercise In line with both the NHS Guidance and the Civil Contingencies Act (2004) the CCG undertook a pandemic flu table top exercise on the 9 July 2015 to exercise our staff and plans. Pandemic Flu remains a serious threat; NHS organisations therefore, are required to ensure that its ability to operationalise and coordinate a pandemic response across local areas can be maintained and is tested with local partners. All local plans should be able to deal with a range of potential levels of pressure, from the relatively mild, such as swine flu, through to much more severe pandemics. Whilst the table top exercise was specifically for the CCG, partner agencies attended to test the effectiveness of our information flows and as such making the exercise as realistic as possible. The CCG also lead a communications test in July 2015 to test the organisations ability to effectively receive and cascade critical information. The actions below were taken following the delivery of the training and exercising programme: TRAINING Actions Pandemic flu exercise • Ensure future exercises continue to engage a wide range of partner
agencies and board members • Review Business Impact Assessments within Business Continuity Plan • Business Continuity development session being run in October 2015 • Business Continuity exercise in October will be available to a wider
range of internal staff Communications exercise
• Key contact numbers to be at the front of the on call pack and visible in the ICC
• Local authority on call number to be included in the on call pack • The two Direct Dial telephone lines are clearly labelled • Second contact number is obtained for ambulance control • Add a clock in the ICC • Place all relevant material on the CCG intranet and communicate
where it is held • Place the guide on how to log in, access the NHS Net and the EPRR
mailbox on the notice board in the ICC • Provide an additional telephone charger for the new blackberry’s
Conclusion Over the last 12 months the CCG has focused heavily on building internal resilience, ownership and understanding of EPRR in particular, the roles and responsibilities pertaining to the CCG as a category 2 responder and system leader. In addition there has been a greater level of scrutiny applied to our own EPRR processes to the level of that expected of our providers.

5
In support of NHS Guidance which requires the acute providers to complete a live exercise every three years, the CCG will ensure an annual exercise occurs covering either Business Continuity or a Major Incident. This will incorporate a number of different methods, but predominately it will be based around a table top exercise and involve partner agencies and contractors. The CCG is now well placed to enter into a yearly exercising cycle which will ensure all elements of the CCG are able to operate effectively if they are required to respond to an incident. Recommendations Over the next year the CCG will be focusing on business continuity, specifically to:
• Review the current plan against the NHS England framework • Testing and exercising the plan and the organisations ability to function during times of
disruption.
In addition the CCG will continue to run EPRR training for all staff groups to support resilience across the CCG focusing specifically on:
• Awareness training across all staff groups • Promote EPRR ‘on line’ awareness training which introduces EPRR to those staff who have
limited exposure to the subject on a day to day basis • ICC training which will be structured to enable small groups to familiarise themselves with the
layout and equipment within the ICC and gain an understanding of how a coordination centre would run during an incident
Sharn Elton Director of Operations

NHS England Core Standards for Emergency preparedness, resilience and responsev3.0
The attached EPRR Core Standards spreadsheet has 6 tabs: EPRR Core Standards tab - with core standards nos 1 - 37 (green tab) Pandemic Influenza :- with deep dive questions to support the pandemic influenza 'deep dive' for EPRR Assurance 2015-16 (blue) tab) HAZMAT/ CBRN core standards tab: with core standards nos 38- 51. Please note this is designed as a stand alone tab (purple tab) HAZMAT/ CBRN equipment checklist: designed to support acute and ambulance service providers in core standard 43 (lilac tab) MTFA Core Standard: designed to gain assurance against the MTFA service specification for ambulance service providers only (orange tab) HART Core Standards: designed to gain assurance against the HART service specification for ambulance service providers only (yellow tab). This document is V3.0. The following changes have been made : • Inclusion of Pandemic Influenza questions to support the pandemic influenza 'deep dive' for EPRR Assurance 2015-16 • Inclusion of the HART service specification for ambulance service providers and the reference to this in the EPRR Core Standards • Inclusion of the MTFA service specification for ambulance service providers and the reference to this in the EPRR Core Standards • Updated the requirements for primary care to more accurately reflect where they sit in the health economy • update the requirement for acute service providers to have Chemical Exposure Assessment Kits (ChEAKs) (via PHE) to reflect that not all acute service providers have been issued these by PHE and to clarify the expectations for acute service providers in relation to supporting PHE in the collection of samples

Core standard Clarifying information
CC
Gs
Evidence of assurance
Self assessment RAG
Red = Not compliant with core standard and not in the EPRR work plan within the next 12 months.
Amber = Not compliant but evidence of progress and in the EPRR work plan for the next 12 months.
Green = fully compliant with core standard.
Action to be taken Lead Timescale
Governance
1 Organisations have a director level accountable emergency officer who is responsible for EPRR (including business continuity management) Y Director of Operations
2
Organisations have an annual work programme to mitigate against identified risks and incorporate the lessons identified relating to EPRR (including details of training and exercises and past incidents) and improve response.
Lessons identified from your organisation and other partner organisations. NHS organisations and providers of NHS funded care treat EPRR (including business continuity) as a systematic and continuous process and have procedures and processes in place for updating and maintaining plans to ensure that they reflect: - the undertaking of risk assessments and any changes in that risk assessment(s)- lessons identified from exercises, emergencies and business continuity incidents- restructuring and changes in the organisations- changes in key personnel- changes in guidance and policy
Y
Training and exercising programme in place for 15/16, endorsed by Governing Body. Plans reviewed for 15/16 include major incident (incorporating revised Hertfordshire plans for mass casualty and pandemic flu), incident coordination centre, business continuity. Severe weather policy in place. Programme for 15/16 in place and outlined in covering letter
3
Organisations have an overarching framework or policy which sets out expectations of emergency preparedness, resilience and response.
Arrangements are put in place for emergency preparedness, resilience and response which: • Have a change control process and version control• Take account of changing business objectives and processes• Take account of any changes in the organisations functions and/ or organisational and structural and staff changes• Take account of change in key suppliers and contractual arrangements• Take account of any updates to risk assessment(s)• Have a review schedule• Use consistent unambiguous terminology, • Identify who is responsible for making sure the policies and arrangements are updated, distributed and regularly tested;• Key staff must know where to find policies and plans on the intranet or shared drive.• Have an expectation that a lessons identified report should be produced following exercises, emergencies and /or business continuity incidents and share for each exercise or incident and a corrective action plan put in place. • Include references to other sources of information and supporting documentation
Y
EPRR annual business cycle paper to be signed off by GB in September. Outlines programme of work for 2015/16 which is also outlined in the covering letter and includes; business continuity plan priorities within business impact assessments - reduced workforce numbers, utility including fuel disruptions and changes to organisation functions. Subject matter expert engagaged to support review. EP and BC resilience developed within the CCG. Training and exercise outcomes and acions
4
The accountable emergency officer will ensure that the Board and/or Governing Body will receive as appropriate reports, no less frequently than annually, regarding EPRR, including reports on exercises undertaken by the organisation, significant incidents, and that adequate resources are made available to enable the organisation to meet the requirements of these core standards.
After every significant incident a report should go to the Board/ Governing Body (or appropriate delegated governing group) .Must include information about the organisation's position in relation to the NHS England EPRR core standards self assessment.
Y
Part of annual business cycle as 3 above
Duty to assess risk
5
Assess the risk, no less frequently than annually, of emergencies or business continuity incidents occurringwhich affect or may affect the ability of the organisation to deliver it's functions.
Y
Reviewed quarterly and documented within EPRR action notes
6
There is a process to ensure that the risk assessment(s) is in line with the organisational, Local HealthResilience Partnership, other relevant parties, community (Local Resilience Forum/ Borough ResilienceForum), and national risk registers.
Y
CCG risks aligned to National and LRF risks. Risks fromally reviewed quarterly at EPRRmeeting
7There is a process to ensure that the risk assessment(s) is informed by, and consulted and shared with yourorganisation and relevant partners.
Other relevant parties could include COMAH site partners, PHE etc. Y
Multiagency exercising and testing informs risk the process
Duty to maintain plans – emergency plans and business continuity plans Incidents and emergencies (Incident Response Plan (IRP) (Major Incident Plan)) Y Key risks identified within the Major Incident Plan
corporate and service level Business Continuity (aligned to current nationally recognised BC standards) Y As per 3 above
HAZMAT/ CBRN - see separate checklist on tab overleaf xSevere Weather (heat wave, flooding, snow and cold weather) Y Plan in place - updated with 15/16 national guidance
Pandemic Influenza (see pandemic influenza tab for deep dive 2015-16 questions) Y As per 2 above. Exercise undertaken in July 2015Mass Countermeasures (eg mass prophylaxis, or mass vaccination) x
Mass Casualties xFuel Disruption Y Included in BCP
Surge and Escalation Management (inc. links to appropriate clinical networks e.g. Burns, Trauma and Critical Care) Y Referenced in MIP. Provider surge plans in placeInfectious Disease Outbreak Y Hertfordshire plan in place
Evacuation Y Part of fire planLockdown x
Utilities, IT and Telecommunications Failure Y Included in BCP Excess Deaths/ Mass Fatalities x
having a Hazardous Area Response Team (HART) (in line with the current national service specification, including a vehicles and equipment replacement programme) - see HART core standard tab
x
firearms incidents in line with National Joint Operating Procedures; - see MTFA core standard tab x
9
Ensure that plans are prepared in line with current guidance and good practice which includes: • Aim of the plan, including links with plans of other responders• Information about the specific hazard or contingency or site for which the plan has been prepared and realistic assumptions• Trigger for activation of the plan, including alert and standby procedures• Activation procedures• Identification, roles and actions (including action cards) of incident response team• Identification, roles and actions (including action cards) of support staff including communications• Location of incident co-ordination centre (ICC) from which emergency or business continuity incident will be managed• Generic roles of all parts of the organisation in relation to responding to emergencies or business continuity incidents• Complementary generic arrangements of other responders (including acknowledgement of multi-agency working)• Stand-down procedures, including debriefing and the process of recovery and returning to (new) normal processes• Contact details of key personnel and relevant partner agencies• Plan maintenance procedures(Based on Cabinet Office publication Emergency Preparedness, Emergency Planning, Annexes 5B and 5C (2006))
Y
• Being able to provide documentary evidence that plans are regularly monitored, reviewed and systematically updated, based on sound assumptions:• Being able to provide evidence of an approval process for EPRR plans and documents• Asking peers to review and comment on your plans via consultation• Using identified good practice examples to develop emergency plans• Adopting plans which are flexible, allowing for the unexpected and can be scaled up or down• Version control and change process controls • List of contributors • References and list of sources• Explain how to support patients, staff and relatives before, during and after an incident (including counselling and mental health services).
Version control in place to evidence review cycle of all plans. All plans approved by Governing Body once review process completed. Plans reviewed by subject matter expert. BCP reviewed by subject matter expert. Reviewed against NHS England guidance and action plan in place to a address gaps. Advice sort from NHS Engalnd regional EPRR lead on specific elements of plans.
10
Arrangements include a procedure for determining whether an emergency or business continuity incident has occurred. And if an emergency or business continuity incident has occurred, whether this requires changing the deployment of resources or acquiring additional resources.
Enable an identified person to determine whether an emergency has occurred- Specify the procedure that person should adopt in making the decision- Specify who should be consulted before making the decision- Specify who should be informed once the decision has been made (including clinical staff)
Y
• On call Standards and expectations are set out• Include 24-hour arrangements for alerting managers and other key staff.
Plans support decision making. 24/7 on call arrangements in place. Training aligned to National Occupational Standards. 5 Directors have undertaken SLC training in the last 12 months. SLC training extended to ADs to develop organisational resilience
11
Arrangements include how to continue your organisation’s prioritised activities (critical activities) in the event of an emergency or business continuity incident insofar as is practical.
Decide: - Which activities and functions are critical- What is an acceptable level of service in the event of different types of emergency for all your services- Identifying in your risk assessments in what way emergencies and business continuity incidents threaten the performance of your organisation’s functions, especially critical activities
Y
As per 3 above
12 Arrangements explain how VIP and/or high profile patients will be managed. This refers to both clinical (including HAZMAT incidents) management and media / communications management of VIPs and / or high profile management
x
13Preparedness is undertaken with the full engagement and co-operation of interested parties and key stakeholders (internal and external) who have a role in the plan and securing agreement to its content Y
• Specify who has been consulted on the relevant documents/ plans etc. As per 9 above
14 Arrangements include a debrief process so as to identify learning and inform future arrangements Explain the de-briefing process (hot, local and multi-agency, cold)at the end of an incident. Y Included in Major Incident and Incident Coordination (ICC) plans
Command and Control (C2)
15Arrangements demonstrate that there is a resilient single point of contact within the organisation, capable of receiving notification at all times of an emergency or business continuity incident; and with an ability to respond or escalate this notification to strategic and/or executive level, as necessary.
Organisation to have a 24/7 on call rota in place with access to strategic and/or executive level personnelY
Explain how the emergency on-call rota will be set up and managed over the short and longer term. Duty manager in place Mon-Friday 09.00-16.00hrs. Year round on call Director rota in place 24/7
16Those on-call must meet identified competencies and key knowledge and skills for staff. NHS England published competencies are based upon National Occupation Standards .
YTraining is delivered at the level for which the individual is expected to operate (ie operational/ bronze, tactical/ silver and strategic/gold). for example strategic/gold level leadership is delivered via the 'Strategic Leadership in a Crisis' course and other similar courses.
EPRR training for those undertaking on call aligned to National Occupational Standards
17Documents identify where and how the emergency or business continuity incident will be managed from, ie the Incident Co-ordination Centre (ICC), how the ICC will operate (including information management) and the key roles required within it, including the role of the loggist .
This should be proportionate to the size and scope of the organisation. Y
Arrangements detail operating procedures to help manage the ICC (for example, set-up, contact lists etc.), contact details for all key stakeholders and flexible IT and staff arrangements so that they can operate more than one control/co0ordination centre and manage any events required.
ICC plan in place. Includes remote activation of the plan using IT
18 Arrangements ensure that decisions are recorded and meetings are minuted during an emergency or business continuity incident.
Y Role and responsibilities of the loggist outlined with the plan
19Arrangements detail the process for completing, authorising and submitting situation reports (SITREPs) and/or commonly recognised information pictures (CRIP) / common operating picture (COP) during the emergency or business continuity incident response.
YContained within the Major Incident plan
20 Arrangements to have access to 24-hour specialist adviser available for incidents involving firearms or chemical, biological, radiological, nuclear, explosive or hazardous materials, and support strategic/gold and tactical/silver command in managing these events.
Both acute and ambulance providers are expected to have in place arrangements for accessing specialist advice in the event of incidents chemical, biological, radiological, nuclear, explosive or hazardous materials
x
21 Arrangements to have access to 24-hour radiation protection supervisor available in line with local and national mutual aid arrangements;
Both acute and ambulance providers are expected to have arrangements in place for accessing specialist advice in the event of a radiation incident
x
Duty to communicate with the public
• Ensuring accountable emergency officer's commitment to the plans and giving a member of the executive management board and/or governing body overall responsibility for the Emergency Preparedness Resilience and Response, and Business Continuity Management agendas• Having a documented process for capturing and taking forward the lessons identified from exercises and emergencies, including who is responsible.• Appointing an emergency preparedness, resilience and response (EPRR) professional(s) who can demonstrate an understanding of EPRR principles.• Appointing a business continuity management (BCM) professional(s) who can demonstrate an understanding of BCM principles.• Being able to provide evidence of a documented and agreed corporate policy or framework for building resilience across the organisation so that EPRR and Business continuity issues are mainstreamed in processes, strategies and action plans across the organisation. • That there is an appropriate budget and staff resources in place to enable the organisation to meet the requirements of these core standards. This budget and resource should be proportionate to the size and scope of the organisation.
• Being able to provide documentary evidence of a regular process for monitoring, reviewing and updating and approving risk assessments• Version control• Consulting widely with relevant internal and external stakeholders during risk evaluation and analysis stages• Assurances from suppliers which could include, statements of commitment to BC, accreditation, business continuity plans.• Sharing appropriately once risk assessment(s) completed
8
Effective arrangements are in place to respond to the risks the organisation is exposed to, appropriate to the role, size and scope of the organisation, and there is a process to ensure the likely extent to which particular types of emergencies will place demands on your resources and capacity.
Have arrangements for (but not necessarily have a separate plan for) some or all of the following (organisation dependent) (NB, this list is not exhaustive):
Risk assessments should take into account community risk registers and at the very least include reasonable worst-case scenarios for:• severe weather (including snow, heat wave, prolonged periods of cold weather and flooding);• staff absence (including industrial action);• the working environment, buildings and equipment (including denial of access);• fuel shortages;• surges and escalation of activity;• IT and communications;• utilities failure;• response a major incident / mass casualty event• supply chain failure; and• associated risks in the surrounding area (e.g. COMAH and iconic sites)
There is a process to consider if there are any internal risks that could threaten the performance of the organisation’s functions in an emergency as well as external risks egg. Flooding, COMAH sites etc.
Relevant plans:• demonstrate appropriate and sufficient equipment (inc. vehicles if relevant) to deliver the required responses• identify locations which patients can be transferred to if there is an incident that requires an evacuation; • outline how, when required (for mental health services), Ministry of Justice approval will be gained for an evacuation; • take into account how vulnerable adults and children can be managed to avoid admissions, and include appropriate focus on providing healthcare to displaced populations in rest centres;• include arrangements to co-ordinate and provide mental health support to patients and relatives, in collaboration with Social Care if necessary, during and after an incident as required;• make sure the mental health needs of patients involved in a significant incident or emergency are met and that they are discharged home with suitable support• ensure that the needs of self-presenters from a hazardous materials or chemical, biological, nuclear or radiation incident are met.• for each of the types of emergency listed evidence can be either within existing response plans or as stand alone arrangements, as appropriate.

Core standard Clarifying information
CC
Gs
Evidence of assurance
Self assessment RAG
Red = Not compliant with core standard and not in the EPRR work plan within the next 12 months.
Amber = Not compliant but evidence of progress and in the EPRR work plan for the next 12 months.
Green = fully compliant with core standard.
Action to be taken Lead Timescale
22 Arrangements demonstrate warning and informing processes for emergencies and business continuity incidents.
Arrangements include a process to inform and advise the public by providing relevant timely information about the nature of the unfolding event and about: - Any immediate actions to be taken by responders- Actions the public can take- How further information can be obtained- The end of an emergency and the return to normal arrangementsCommunications arrangements/ protocols: - have regard to managing the media (including both on and off site implications)- include the process of communication with internal staff - consider what should be published on intranet/internet sites- have regard for the warning and informing arrangements of other Category 1 and 2 responders and other organisations.
Y
• Have emergency communications response arrangements in place • Be able to demonstrate that you have considered which target audience you are aiming at or addressing in publishing materials (including staff, public and other agencies)• Communicating with the public to encourage and empower the community to help themselves in an emergency in a way which compliments the response of responders• Using lessons identified from previous information campaigns to inform the development of future campaigns• Setting up protocols with the media for warning and informing• Having an agreed media strategy which identifies and trains key staff in dealing with the media including nominating spokespeople and 'talking heads'.• Having a systematic process for tracking information flows and logging information requests and being able to deal with multiple requests for information as part of normal business processes.• Being able to demonstrate that publication of plans and assessments is part of a joined-up communications strategy and part of your organisation's warning and informing work.
Major Incident plan contains communications plan. Hertfordshire wide process in place to manage public messaging and ensure consistency of approach

Core standard Clarifying information
CC
Gs
Evidence of assurance
Self assessment RAG
Red = Not compliant with core standard and not in the EPRR work plan within the next 12 months.
Amber = Not compliant but evidence of progress and in the EPRR work plan for the next 12 months.
Green = fully compliant with core standard.
Action to be taken Lead Timescale
23Arrangements ensure the ability to communicate internally and externally during communication equipment failures Y
• Have arrangements in place for resilient communications, as far as reasonably practicable, based on risk.
Detailed in BCP
Information Sharing – mandatory requirements
24
Arrangements contain information sharing protocols to ensure appropriate communication with partners. These must take into account and include DH (2007) Data Protection and Sharing – Guidance for Emergency Planners and Responders or any guidance which supersedes this, the FOI Act 2000, the Data Protection Act 1998 and the CCA 2004 ‘duty to communicate with the public’, or subsequent / additional legislation and/or guidance.
Y
• Where possible channelling formal information requests through as small as possible a number ofknown routes. • Sharing information via the Local Resilience Forum(s) / Borough Resilience Forum(s) and othergroups.• Collectively developing an information sharing protocol with the Local Resilience Forum(s) / BoroughResilience Forum(s). • Social networking tools may be of use here.
Information sharing protocols in place across LRF and Health
Co-operation
25 Organisations actively participate in or are represented at the Local Resilience Forum (or Borough Resilience Forum in London if appropriate) Y Director of Operations is a member of the LRF
26 Demonstrate active engagement and co-operation with other category 1 and 2 responders in accordance with the CCA
Y Receive action notes from key provider EPRR meeting. CCG represented at provider and multi-agency training and exercises where appropriate
27
Arrangements include how mutual aid agreements will be requested, co-ordinated and maintained. NB: mutual aid agreements are wider than staff and should include equipment, services and supplies.
Y
EPRR clauses within standard national contact in place across all providers which includes the provision of mutual. CCG coordination of provider response is included with CCG and Hertfordshire wide plans. Information sharing protocols als support mutual aid
28 Arrangements outline the procedure for responding to incidents which affect two or more Local Health Resilience Partnership (LHRP) areas or Local Resilience Forum (LRF) areas.
x
29 Arrangements outline the procedure for responding to incidents which affect two or more regions. x
30 Arrangements demonstrate how organisations support NHS England locally in discharging its EPRR functions and duties
Examples include completing of SITREPs, cascading of information, supporting mutual aid discussions, prioritising activities and/or services etc. Y Detailed in MIP plan
31 Plans define how links will be made between NHS England, the Department of Health and PHE. Including how information relating to national emergencies will be co-ordinated and shared
x
32Arrangements are in place to ensure an Local Health Resilience Partnership (LHRP) (and/or Patch LHRP for the London region) meets at least once every 6 months
x
33Arrangements are in place to ensure attendance at all Local Health Resilience Partnership meetings at a director level Y
Director of Operations is a member of the LHRP
Training And Exercising
34
Arrangements include a training plan with a training needs analysis and ongoing training of staff required to deliver the response to emergencies and business continuity incidents
• Staff are clear about their roles in a plan • Training is linked to the National Occupational Standards and is relevant and proportionate to the organisation type. • Training is linked to Joint Emergency Response Interoperability Programme (JESIP) where appropriate• Arrangements demonstrate the provision to train an appropriate number of staff and anyone else for whom training would be appropriate for the purpose of ensuring that the plan(s) is effective• Arrangements include providing training to an appropriate number of staff to ensure that warning and informing arrangements are effective
Y
Training and exercise plan in place for 2015/16, endorsed by the CCG Governing Body. Training and exercising programme development informed by outputs,
35
Arrangements include an ongoing exercising programme that includes an exercising needs analysis and informs future work.
• Exercises consider the need to validate plans and capabilities• Arrangements must identify exercises which are relevant to local risks and meet the needs of the organisation type and of other interested parties.• Arrangements are in line with NHS England requirements which include a six-monthly communications test, annual table-top exercise and live exercise at least once every three years.• If possible, these exercises should involve relevant interested parties. • Lessons identified must be acted on as part of continuous improvement.• Arrangements include provision for carrying out exercises for the purpose of ensuring warning and informing arrangements are effective
Y
As 34 above
36 Demonstrate organisation wide (including oncall personnel) appropriate participation in multi-agency exercises
Y CCG attendance at all relevant multi-agency exercise
37Preparedness ensures all incident commanders (oncall directors and managers) maintain a continuous personal development portfolio demonstrating training and/or incident /exercise participation. Y
As per 10 and 34 above
• Attendance at or receipt of minutes from relevant Local Resilience Forum(s) / Borough Resilience Forum(s) meetings, that meetings take place and membership is quorate.• Treating the Local Resilience Forum(s) / Borough Resilience Forum(s) and the Local Health Resilience Partnership as strategic level groups• Taking lessons learned from all resilience activities• Using the Local Resilience Forum(s) / Borough Resilience Forum(s) and the Local Health Resilience Partnership to consider policy initiatives• Establish mutual aid agreements• Identifying useful lessons from your own practice and those learned from collaboration with other responders and strategic thinking and using the Local Resilience Forum(s) / Borough Resilience Forum(s) and the Local Health Resilience Partnership to share them with colleagues• Having a list of contacts among both Cat. 1 and Cat 2. responders with in the Local Resilience Forum(s) / Borough Resilience Forum(s) area
• Taking lessons from all resilience activities and using the Local Resilience Forum(s) / Borough Resilience Forum(s) and the Local Health Resilience Partnership and network meetings to share good practice• Being able to demonstrate that people responsible for carrying out function in the plan are aware of their roles• Through direct and bilateral collaboration, requesting that other Cat 1. and Cat 2 responders take part in your exercises• Refer to the NHS England guidance and National Occupational Standards For Civil Contingencies when identifying training needs.• Developing and documenting a training and briefing programme for staff and key stakeholders• Being able to demonstrate lessons identified in exercises and emergencies and business continuity incidents have been taken forward• Programme and schedule for future updates of training and exercising (with links to multi-agency exercising where appropriate)• Communications exercise every 6 months, table top exercise annually and live exercise at least every three years

APPENDIX 1
Core standard Clarifying information
CC
Gs
Evidence of assurance
Self assessment RAG
Red = Not compliant with core standard and not in the EPRR work plan within the next 12 months.
Amber = Not compliant but evidence of progress and in the EPRR work plan for the next 12 months.
Green = fully compliant with core standard.
Action to be taken Lead Timescale
2015 Deep Dive
DD1
Organisation have updated their pandemic influenza arrangements to reflect changes to the NHS and partner organisations, as well as lessons identified from the 2009/10 pandemic including through local debriefing
• changes since April 2013 are reflected in local plans including formation of NHS England, CCGs and PHE; as well as the move of the previous PCT public health function into local authorities• key changes to the national pandemic influenza strategy (such as de-coupling from WHO, development of DATER phases, and removal of UK alert levels) as well as relevant local learning is reflected
Y
• updated planning arrangements reflect changes and learning• version control indicates changes made and timeliness
Hertfordshire pandemic flu plan in place
DD2
Organisations have developed and reviewed their plans with LHRP and LRF partners • relevant local partners (particularly other NHS providers/ commissioners, PHE and local authority public health and social care teams where appropriate) have been engaged in the development of local plans - at a minimum through an opportunity to comment on draft versions Y
• indication of the process used to develop updated arrangements, including identification of organisations involved in contributing or commenting on drafts• agendas/ minutes illustrating where the updated arrangements have been discussed
As DD1 above
DD3
Organisations have undertaken a pandemic influenza exercise or have one planned in the next six months • local organisations have held an internal exercise or participated in a multi-organisation exercise since updating their local arrangements to reflect changes and learning described in DD1• if this has not taken place, there is a clear plan to deliver an exercise in the next six months Y
• documentation related to exercise since the 2013 publication, including lessons identified OR • invitation letters/ documentation related to exercise scheduled to take place in next six months, including an indication of how lessons identified will be addressed
CCG pandemic flu exercise undertaken in July 2015
DD4Organisations have taken their plans to Boards / Governing bodies for sign off • updated arrangements that reflect changes and learning described in DD1 have been taken to Boards or Governing Bodies, and even if
they have not yet have been signed off by such bodies, the process towards this has been started Y• Board/ Governing Body agenda or meeting papers indicating updated pandemic influenzaarrangements have been discussed and/ or signed off
Part of annual business cycle

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 1 of 48
MAJOR INCIDENT PLAN 2015
EAST AND NORTH HERTFORDSHIRE CLINICAL COMMISSIONING GROUP PLAN FOR RESPONDING TO
MAJOR INCIDENTS IN HERTFORDSHIRE

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 2 of 48
DOCUMENT CONTROL SHEET Document Owner: Director of Operations Document Author(s): EPRR Lead Version: 2.2 FINAL Directorate: Operations Approved By: Governing Body Date of Approval: 15 January 2015 Date of Review: 15 January 2016 Change History:
Implementation Plan:
Development and Consultation
EPRR Consultant Executive Team
Dissemination Staff can access this policy via the intranet and will be notified of new/revised versions via the staff briefing. This policy will be included in CCG Publication Scheme in compliance with the Freedom of Information Act 2000. External Distribution List: NHS England (Midlands and East (South Locality)) East of England Ambulance Service NHS Trust Hertfordshire Community NHS Trust Hertfordshire Partnership University NHS Foundation Trust Public Health England (Hertfordshire) East and North Hertfordshire NHS Trust Hertfordshire County Council Herts Urgent Care and 111 Operational Delivery Network
Training
Training is provided for key staff that may be required to carry out essential tasks in response to a major incident. Staff are provided with training that ensures they understand the role they are to fulfill in the event of an incident and have the necessary competencies to fulfill that role. All staff members should familiarise themselves with the Major Incident Plan. This training will include skills allowing staff to operate at operational (Bronze), tactical (Silver) and strategic (Gold) levels
Version Date Reviewer(s) Revision Description
1.0 Final October 2013 Steven Moore EEAST Annual update
1.1 Draft January 2015 Oskan Edwardson Annual update
2.0 Final January 2015 Jas Dosanjh Formatting
2.1 Final March 2015 Sharn Elton Minor Amendments – formatting and references
2.2 Final September 2015 Sharn Elton Updated in line with NHSE EPRR Toolkit requirements

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 3 of 48
and will also include training for Loggist and Business Continuity Awareness, depending on their role both within the Trust and during an incident. Staff members that are likely to follow an Action Card are sent an annual reminder that cards should be reviewed. Staff are also be given the opportunity to participate in NHS and multi-agency exercises.
Monitoring and Review
Assurance: ENH CCG will ensure that its business continuity plans are fit
for purpose in line with the NHS England Business Continuity Framework 2013. It will be able to respond to any incident as part of a multiagency response.
ENH CCG will be assured of plans and organisational resilience from all its providers. These are listed in the in accordance with the NHS England Core Standards 2015/16.
NHS England (South Locality) will seek similar assurance from the CCGs using the NHS England Core Standards 2015/16.
Providers of NHS funded care are responsible for providing assurance to the CCGs and NHS England (South Locality). In accordance with the NHS England Core Standards 2015/16.
In gathering wide ranging assurances from individual NHS organisations, NHS England (South Locality) will provide assurance to the NHS England-Midlands and East that all providers of NHS funded care within their area, are fit for purpose.
Directors of Public Health will seek NHS EPRR assurance through the LHRP.
In the event of legal advice being required this can be obtained from “Capsticks” solicitors. Details are held by the Senior Information Risk Owner (The Director of Finance)
Equality and Diversity
January 2015 - Equality Impact Assessment (Appendix 4) January 2015 - Privacy Impact Assessment (Appendix 5)
Associated Documents
This document should be read in conjunction with: • ENHCCG Business Continuity Plan • ENHCCG Escalation Framework • ENHCCG Surge Capacity Plan contained within the • ENHCCG Integrated Escalation Framework • ENHCCG Severe Weather Response Plan NHS England Business Continuity Management Framework
(Service Resilience) (2013) NHS England Emergency Preparedness Framework (2013) NHS England Core Standards for Emergency Preparation,
Resilience and Response (2015) NHS England Command and Control Framework 2013 Hertfordshire Resilience Forum Multi Agency Response Plan Public Health England Centre (PHEC) major incident
frameworks and incident response plans. East and North Hertfordshire Clinical Commissioning Group
Escalation Framework Hertfordshire LRF Mass Casualties Plan

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 4 of 48
Hertfordshire Infectious Disease Plan East and North Hertfordshire Clinical Commissioning Group
Business Continuity Plan Surge Capacity Plan contained within the ENHCCG
Integrated Escalation Framework

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 5 of 48
CONTENTS Section No Section Name Page No.
1.0 Introduction 6
2.0 Scope 6
3.0 Purpose 6
4.0 Definitions 10
5.0 Role and Responsibilities 12
6.0 Command and Control Structure 16
6.1 ENH CCG Response to a Major Incident 20
6.2 Communications 20
6.3 Business Continuity 21
6.4 Vulnerable Adults 21
6.5 Exercise and Test Plans 22
Appendix 1 Initial Risk Assessment 23
Appendix 2 NHS Major Incident Situation Report - SITREP 31
Appendix 3 Planning Structure 32
Appendix 4 Equality Impact Assessment 35
Appendix 5 Privacy Impact Assessment 36 Appendix 6 Privacy Impact Assessment Stage 1 Screening 37
Appendix 7 Memorandum of Understanding, Information Sharing
38
Appendix 8 ICC Plan 45

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 6 of 48
1.0 Introduction
The NHS carries out emergency planning to ensure it is able to respond appropriately and effectively to major incidents. The major incident plan for East and North Hertfordshire Clinical Commissioning Group (ENHCCG) is built on the principles of risk assessment, cooperation with partners, emergency planning, communicating with the public, and information sharing. This plan is sufficiently flexible to deal with a range of situations and comprises of two parts. The first part is the overarching Major Incident Plan which sets out the role of the Clinical Commissioning Group (CCG) in a major incident and explains how this role fits with those of other NHS organisations and the emergency services. This is the strategic part of the plan and is designed to be read by all staff, especially those on call. The second part is the Operational response action cards. This is designed to be used during a major incident. It summarises the practical steps that need to be taken in the event of a major emergency. This Plan will be published on ENHCCG website and on the intranet, all senior managers who have on call responsibilities will have this plan included in their on call packs and will be required to sign for it.
2.0 Scope NHS Guidance The ENHCCG Major Incident Plan is based on the NHS England South Locality Incident Response Plan; it follows a set of general principles that guide all NHS organisations in developing their ability to respond to major incidents, significant incidents and other emergencies and to manage recovery locally within the context of the requirements of the Civil Contingencies Act 2004 (CCA 2004). 3.0 Purpose NHS Standard Contracts & NHS England Emergency Preparedness Framework The Civil Contingencies Act 2004 outlines a single framework for civil protection in the United Kingdom. Part 1 of the Act establishes a clear set of roles and responsibilities for those involved in emergency preparation and response at local level. The Act divides local responders into two categories, imposing a different set of duties on each. Category one responders are those organisations at the core of the response to most emergencies. This category includes all Acute Trusts and Ambulance NHS Trusts, NHS England and Public Health England. They are subject to the following civil protection duties:- • assess the risk of emergencies occurring and use this to inform
contingency planning; • put in place emergency plans; • put in place business continuity management arrangements; • put in place arrangements to make information available to the public about

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 7 of 48
civil protection matters and maintain arrangements to warn, inform and advise the public in the event of an emergency;
• share information with other local responders to enhance co-ordination; • co-operate with other local responders to enhance co-ordination and efficiency.
Primary care, community providers, mental health and other NHS organisations (NHS Blood and Transplant, NHS Logistics and NHS Protect) are not listed in the Civil Contingencies Act 2004. However, Department of Health (DH) and NHS England guidance expects them to plan for and respond to incidents in the same way as category one responders. Category two responders are required to cooperate and share relevant information with other Category one and two responders. Category two responders, such as Clinical Commissioning Groups (CCGs), are seen as ‘co-operating bodies’. They are less likely to be involved in the heart of the planning, but they will be heavily involved in incidents that affect their sector. It is vital that they share relevant information with other responders (both category one and two) if Emergency Preparedness, Resilience and Response (EPRR) arrangements are to succeed. To support this requirement the LHRP has a MOU in place (see appendix 7) Category one and two responders come together to form local resilience forum based on police areas. These forums help to co-ordinate activities and foster co-operation between local responders. For ENHCCG the strategic forum for joint planning for emergencies is the Hertfordshire Local Health Resilience Partnership (LHRP). They provide the health sector’s contribution to multi-agency planning through Hertfordshire Local Resilience Forum (LRFs). Hertfordshire LHRP will coordinate health input and support the NHS England (South Locality), Local Authorities and Public Health England (PHE) in ensuring that member organisations develop and maintain effective planning arrangements for major incidents, significant incidents and emergencies. There are two Hertfordshire Accountable Emergency Officers representing East and North Hertfordshire and Herts Valleys CCGs on the LHRP. The Director of Operations is the Accountable Emergency Officer for ENHCCG and attends the LHRP. 3.1 Risk Assessment The Civil Contingencies Act 2004 places a risk assessment duty on all category one responders to ensure that planning is proportionate to each risk. A Community Risk Register is compiled by the H e r t f o r d s h i r e Local Resilience Forum and consists of a table of hazards summarising hazard information, outcome descriptions, risk rating and mitigation plans). http://wwwhertsdirect.org/emergency The top five risks currently identified on the Hertfordshire Resilience Community Risk register are: • Pandemic flu • Terrorist and malicious attacks • Road accidents • Extreme temperatures • Flooding
The national and community risk registers have informed local health and multi-agency planning and the Hertfordshire Local Health Resilience Partnership Three Year Strategy and work Programme, 2013 reflects this.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 8 of 48
The CCG has its own Risk Register which is maintained and will hold information specific to EPRR risks which are identified within the CCG. The EPRR risks will be reviewed, amended and update at the CCG EPRR Meetings. These meetings will feed into the Governance and Audit Committee. 3.2 Requirements applicable within the Health and Social Care Act 2012 The Health and Social Care (2012) Act embeds the requirement of NHS services to respond effectively to incidents and emergencies. The key elements are:- • NHS England and each CCG must take appropriate steps for ensuring that it is
properly prepared for dealing with a relevant emergency. • NHS England must take steps as it considers appropriate for securing that
each relevant service provider is properly prepared for dealing with a relevant emergency.
3.3 Core standards The minimum core standards, which NHS organisations and providers of NHS funded care must meet, are set out in the NHS England Core Standards for EPRR. These standards are in accordance with the Civil Contingencies Act 2004, the Health and Social Care Act 2012, the NHS England planning framework (‘Everyone Counts: Planning for Patients’) and the NHS standard contract. NHS organisations and providers of NHS funded care must: • nominate an accountable emergency officer who will be responsible for EPRR; • contribute to area planning for EPRR through local health resilience
partnerships; • contribute to an annual NHS England (South Locality) report on the health
sector’s EPRR capability and capacity in responding to national, regional and LRF incidents.
• Reports must include control and assurance processes, information-sharing, training and exercise programmes and national capabilities surveys. They must be made through the organisation's formal reporting structures;
• have suitable, up to date incident response plans which set out how they plan for, respond to and recover from significant incidents and emergencies. The plans should fulfill the testing schedule as detailed in the CCA 2004;
• have suitably trained, competent staff and the right facilities (incident coordination centres) available round the clock to effectively manage a major incident or emergency;
• share their resources as required to respond to a major incident or emergency. 3.4 Business Continuity (service resilience) planning The CCA 2004 places a statutory duty on organisations to develop a comprehensive approach to business continuity. This framework follows the principles of ISO 22301 and PAS 2015. Some elements of ISO 22301 must be done in partnership with other health organisations and this will be led by the Hertfordshire Local Health Resilience Partnership and Hertfordshire Local Resilience Forum.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 9 of 48
The NHS England Business Continuity Framework 2013 can be found at: http://www.England.nhs.uk/ourwork/gov/eprr
3.5 Local cooperation At the local level, it is important that planning for major and significant incidents and emergencies is co-ordinated within individual NHS organisations, between NHS funded organisations and at a multi-agency level with emergency services, local authorities, voluntary agencies, the independent health and social care sector and other partner organisations. Training, exercising and testing of all EPRR plans within ENHCCG, between NHS funded organisations and with multi-agency partners will be an important part of emergency preparedness and will be documented as part of the annual work programme. NHS England (South Locality) is responsible for maintaining a mechanism that will enable NHS organisations to plan and cooperate appropriately and to performance manage these organisations for this aspect of their responsibilities. This will be supported by the Hertfordshire LHRP, the memorandum of understanding and annual assurance process. Provider responsibilities are contained within the NHS Standard Contract (http://www.commissioningboard.nhs.uk/nhs-standard-contract/ - The independent healthcare sector may be used in a disruptive incident to assist with service delivery by providing capacity, resources including staff, equipment and consumables. The CCG has contract in place with some independent sector providers. The contract outlines the responsibility to respond in a major incident in line with NHS providers. 3.6 Mutual Aid Mutual Aid can be defined as an arrangement between Category one and two responders, other organisations not covered by the CCA 2004, within the same sector or across sectors and across boundaries, to provide assistance with additional resource during any incident that may overwhelm the resources of a single organisation. The NHS England (South Locality) will be responsible for the co-ordination and implementation of mutual aid requests if a disruptive incident occurs. ENHCCG will respond to any requests received to provide mutual aid during a major or significant incident or emergency. Provider responsibilities are contained within the NHS Standard Contract (http://www.commissioningboard.nhs.uk/nhs-standard-contract/) 3.7 Networks (critical care, trauma, burns) The Operational Delivery Network co-ordinates specialist areas of care, including critical care trauma and burns and ensures that patients can access the optimum care for their condition. The Operational Delivery Network that covers East of England including Hertfordshire is hosted by Cambridge University Hospitals Foundation Trust which effectively ensures mutual aid arrangements when needed.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 10 of 48
3.8 Information Sharing Under the CCA 2004 local responders have a duty to share information and this is seen as a crucial element of civil protection work, underpinning all forms of co-operation. The sharing of information will include, if required for the response, details of vulnerable people. The general definition of a vulnerable person is a person:
“present or resident within an area known to local responders who, because of dependency or disability, need particular attention during incidents”
See appendix 7 for the Hertfordshire MOU regarding information sharing. 4.0 Definitions
4.1 Major or Significant Incident or Emergency This section describes various definitions of major incidents, significant incidents and emergencies as they may apply to NHS organisations and providers of NHS funded care and the varying scale of these incidents. There may be times of severe pressure such as during winter periods, or where there is an increase in demand for service (surges) or an infectious disease outbreak. These should be managed through normal process and business continuity plans. A significant incident or emergency is any event that cannot be managed within routine service arrangements. It requires the implementation of special procedures and may involve one or more of the emergency services, the NHS or a local authority. Within local NHS organisations these emergencies are often referred to as Major Incidents. The term ‘emergency’ is used as defined in the Civil Contingencies Act 2004:
‘To describe an event or situation that threatens serious damage to human welfare in a place in the UK or to the environment of a place in the UK, or war or terrorism this threatens serious damage to the security of the UK. The term ‘‘major incident’’ is commonly used to describe such emergencies. These may include multiple casualty incidents, terrorism or national emergencies such as pandemic influenza.’
For the NHS, a significant incident is defined as:
‘Any occurrence that presents serious threat to the health of the community, disruption to the service or causes (or is likely to cause) such numbers or types of casualties as to require special arrangements to be implemented by hospitals, ambulance trusts or other acute or community provider organisations.’
Individual NHS organisations can self-declare a significant incident when their own facilities and/or resources, or those of its neighbours, are overwhelmed. What is a significant incident or emergency to the NHS may not necessarily be a significant

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 11 of 48
incident or emergency for other local agencies and the reverse is also true. A major incident, significant incident or emergency may arise in a variety of ways:
• big bang: a serious transport accident, explosion, or series of smaller incidents
• rising tide: a developing infectious disease epidemic, or a capacity/staffing crisis
• cloud on the horizon: a serious threat such as a major chemical or nuclear release developing elsewhere and needing preparatory action, dangerous epidemics, armed conflict
• headline news: wave of public or media alarm over health issue or perceived threat
• internal incidents: fire, breakdown of utilities, equipment failure, hospital acquired infections, violent crime
• deliberate release of chemical, biological, nuclear or explosive materials • mass casualties • pre-planned major events that require planning such as demonstrations,
sports fixtures, air shows. There are a number of incidents which may need to be dealt with under the Major Incident Plan, some of which will not necessarily be either affecting other organisations or which will have a different impact on other organisations. These will include industrial action (IA) which will be dealt with by the CCG Business Continuity Plan. Other incidents such as those involving the need for locking down part, or all, of the CCG HQ building during an incident such as one which involved CBRN material can be found in Action Card 5.
Incidents such as wide spread flooding or other weather related incidents (ie snow, heat wave, prolonged periods of cold weather) will be dealt with in line with the CCG’s Severe Weather Plan and in conjunction with the Major Incident Plan and Business Continuity Plan.
4.2 Abbreviations CCA Civil Contingencies Act CCG Clinical Commissioning Group DCLG Department for communities and Local government DH Department of Health EPRR Emergency Preparedness, Resilience and Response ICC Incident Co-ordinating Centre ISO International Standards Organisation LHRP Local Health Resilience Partnership LRF Local Resilience Forum ENHCCG East and North Hertfordshire Clinical Commissioning Group PALS Patient Advice and Liaison Service PAS Publicly Available Specification PHE Public Health England PHEC Public Health England Centre SAGE Scientific Advisory Group for Emergencies SCG Strategic co-ordinating Group STAC Science and Technical Advice Cell

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 12 of 48
5.0 Roles and Responsibilities
5.1 Clinical Commissioning Groups (CCGs) ENHCCG has a senior manager on call available at all times through a mobile phone system should a provider of NHS funded care have a problem that needs escalating either in or out of normal hours. The senior manager will be available to providers or NHS England (South Locality). ENHCCG will use the NHS England Framework (as detailed in appendix 2) to determine how and when issues should be escalated. As category two responders under the CCA 2004, CCGs must respond to reasonable requests to assist and cooperate during an emergency. NHS England – Midlands and East (South Locality) may decide to include CCG members in the formal command and control structure and to assist in any response to a major incident. CCG’s may assist and support NHS England (South Locality) by undertaking the following tasks:
• Mobilising resources from locally commissioned services • Providing local NHS leadership if required liaise with relevant
partner organisations • Cascading information to relevant service level providers • Inform and maintain dialogue with neighboring CCGs where
appropriate • Support CCG commissioned organisations with any local demand,
capacity and systems resilience issues 5.2 Providers of NHS funded Care Providers of NHS funded care will fulfill relevant legal and contractual EPRR requirement, including the Civil Contingencies Act 2004 (CCA), and ensure a robust and sustainable 24/7 response to emergencies and:
• provide the resilience to manage incidents and emergencies that affect only them, with escalation where necessary;
• provide an Accountable Emergency Officer to take executive responsibility and leadership for EPRR at service level;
• collaborate with local multi-agency partners to facilitate inclusive planning and response;
• ensure preparedness to maintain critical services in periods of disruption; • facilitate NHS EPRR assurance, including business continuity.
5.3 NHS England (South Locality) NHS England (South Locality) will provide leadership across Hertfordshire. If an incident requires a wider NHS or multi-agency response, this co-ordination and leadership is provided by a NHS England (South Locality) Director. The NHS England (South Locality) Director has overall responsibility for ensuring that NHS England (South Locality) and the local health economy are able to respond to a major or significant incident or emergency.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 13 of 48
The NHS England (South Locality) on-call director; may take command and control of the situation if several NHS and partner organisations need to be involved and the need for a coordinating role arises. If a Strategic Coordination Group is convened, ‘health’ will be represented by the NHS England (South Locality) on-call director (NHS Gold). If necessary, Public Health England, local authority directors and the East of England Ambulance Service will also attend. (see section 6.0, Escalation for further details) NHS England (South Locality) may be required to respond actively by:
• escalating the use of GP surgeries as necessary, to see patients that, but for the major or significant incident or emergency, would normally be at or would go to the local acute hospital e.g. patients with less serious problems that, because of the incident, cannot be readily seen in the emergency department.
• mobilising support from GPs to help at a local acute hospital receiving the casualties and/or by referring other patients to other hospitals.
• mobilise assistance from GPs to support at a rest centre. A rest centre is managed by the Local Authority and is for people evacuated from a scene of a major incident.
• Coordinating and managing NHS response to the public and media.
5.4 NHS England- Midlands and East (Regional team) If an incident affects two or more areas, the NHS response will normally be led by the Regional Team first affected and responding to it. If the NHS England Midlands and East have to take command of all NHS resources across the region, the Regional team’s on-call director will if necessary provide leadership and direction across the region. Actions for local organisations will be actioned through the Regional Team. 5.5 NHS England (National team) In extreme situations such as pandemic influenza, a national fuel shortage or extreme weather, the NHS England national team may take command of all NHS resources across England. In this situation, direction from the national team will be actioned through the regional teams. Where this occurs the resources from East and North Herts CCG will be put at NHS England’s disposal for appropriate use. 5.6 Public Health England Public Health England (PHE) provides expert advice to the DH, Regional Directors of Public Health and the NHS on health protection policies and programmes. It also provides specialist emergency planning advice to NHS organisations to:
• ensure that PHE has plans for emergencies in place across the local area. Where appropriate, these will be joint emergency plans with the NHS and local authorities,
• through the LHRP; • discharge the local PHE EPRR functions and duties; • have the capability to lead the PHE response to an emergency at a local

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 14 of 48
level. Ensure a 24/7 on-call rota for emergency response in the local area; • ensure that staff has the appropriate competencies and authority to
coordinate the health protection response to an emergency.
5.7 PHE Regional Offices The Regional Office provides strategic EPRR advice and support to PHE Centres and maintains PHE’s capacity and capability to coordinate regional public health responses to emergencies 24/7.
5.8 PHE National Level At a national level they provide leadership and co-ordination of PHE and national information on behalf of the PHE during periods of national emergencies. They support the response to incidents that affect two or more PHE regions and will act as the national link on EPRR matters between PHE, DH and NHS England. 5.9 Local Authorities Through the Director of Public Health (DPH), the local authorities within Hertfordshire will take steps to ensure that plans are in place to protect the health of their populations and escalate any concerns or issues to the relevant organisation or to the LHRP as appropriate. The DPH will co-chair the LHRP alongside the Director of Commissioning Operations for the NHS England (South Locality). ENHCGG has a Memorandum of Understanding in place with Hertfordshire Public Health Team, which outlines roles, responsibilities and expectations (see appendix 9) Each DPH will provide initial leadership with PHE for the response to public health incidents and emergencies within their local authority area. The DPH will maintain oversight of population health and ensure effective communication with local communities. PHE will deliver and manage the specialist health protection services. In addition they fulfill the responsibilities of a Category one responder under the CCA 2004 5.10 Department of Health The Department of Health (DH) Emergency Preparedness Division advises Ministers on the development of policy and promulgates agreed policy. It oversees and ensures planning and preparedness in the NHS and coordinates the overall NHS response to major incidents where necessary. The division also supports the Central Government response through the Cabinet Office Briefing Room (COBR). The structures of Emergency Preparedness, Response and Recovery are shown in Appendix 3 5.11 Pandemic Influenza The initial response to the early stages of the pandemic (Detect and Assessment phases) will be based on the agreed mechanisms for management of an outbreak. This will be led by Public Health England, supported by NHS England, CCGs and NHS funded providers. At a point agreed with PHE, NHS England will activate the wider

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 15 of 48
response when societal impacts become significant. Authorisation for the activation of this plan will be given by NHS England following consultation with Directors of Public Health and Public Health England. On activation of the plan, Strategic and Tactical Co‐ordinating Groups will be convened by NHS England in line with the agreed multi agency approach. Strategic Co-ordinating Group The Strategic Co-ordinating Group (SCG) will be chaired by the Police. Particularly in the early stages of a pandemic they will be supported by Public Health England. The SCG will be run as for any co-ordinated multi agency response. Any requirements for scientific and technical advice would be from a national level by the Scientific Advisory Group for Emergencies (SAGE); no local or regional STAC would be in place. Tactical level Co-ordination When a Tactical Co-ordinating Group (TCG) is convened its purpose is to ensure that actions taken by the operational level are co-ordinated and integrated in order to achieve effectiveness and efficiency. During the initial response to a pandemic (Detection and Assessment phases) the impact will be focussed on the health and social care sectors. It is likely therefore that only a Health Co-ordinating Group (HCG, led by Clinical Commissioning Groups) would be in place during this time, as opposed to a wider tactical level structure as would be in place for other incidents. All member organisations of the health and social care community and voluntary sector, will be required to provide representation at the HCG to ensure that the main aims and objectives of the HCG can be fulfilled. Public Health England will lead a single Outbreak Control Team across the PHE Centre area to support this process. During the Treatment phase, consideration will need to be given to initiating a wider co-ordinated response, including a full TCG, with supporting cells and command support. Once escalation phase is reached, a full tactical level co-ordination is likely to be required, with cells created as required. In making this response, the LRF partners will work to the strategic objectives as defined by the SCG. Initial strategic objectives would be confirmed at the first meeting, but could include:
• Protect Hertfordshire’s communities and visitors against the health and wider consequences of influenza as far as this is possible.
• Support National efforts to prevent and detect its emergence and prevent, slow, or limit its spread
• Organise and adapt the health and social care systems to provide treatment and support for the large numbers likely to suffer from influenza or its complications whilst maintaining other essential care.
• Support the continuity of essential services and protect critical national infrastructure as far as possible.
• Support the continuation of everyday activities as far as practical. • Uphold the rule of law and the democratic process. • Instill and maintain trust and confidence by ensuring that the public and the
media are engaged and well informed in advance of and throughout the pandemic period.
• Promote a return to normality and the restoration of disrupted services at the earliest opportunity.
• Ensure that all Business Continuity Plans are operational and ready to support the wider SCG response and recovery plans.
• Ensure that thorough, comprehensive and adequately resourced preparation and planning is conducted for a possible second phase.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 16 of 48
In the event of pandemic influenza there will be severe constraints on all category 1 and 2 agencies in responding to the impact of the pandemic whilst managing the effects on their own organisation. The co‐ordination arrangements set out here attempt to reduce the burden on any individual agency and to provide clear guidance on roles, responsibilities, chain of command and lines of communication. The response may be varied to reflect what is likely to be a rapidly changing environment during some stages of a pandemic situation. For all organisations, robust business continuity plans will be the foundation of maintaining their own critical services, as well as the collective response. In addition CCGs are responsible for:
• supporting the national pandemic response arrangements as laid out in Department of Health and NHS England guidance issued prior to or during a pandemic occurring
• in line with other guidance, ensure 24/7 on-call arrangements remain robust and maintained, particularly with respect to surge and responding to major incidents
• lead the management of pressure surge arrangements with their commissioned services as a result of increased activity as part of the overall response
• support NHS England Regional Teams in the local coordination of the response, e.g. through tried and tested surge capacity arrangements, appropriate mutual aid of staff and facilities and provision of support to the management of clinical queries
• as necessary share communications with locally commissioned healthcare providers through established routes
• participate in the multi-agency response as appropriate and agreed with NHS England Regional Teams to ensure a comprehensive local response
• maintain close liaison with local NHS England colleagues, particularly when considering changes to delivery levels of NHS commissioned services
• enact business continuity arrangements as appropriate to the developing situation to ensure critical activities can be maintained
• maintain local data collection processes to support the overall response to the pandemic, including completion and submission of relevant situation reports and participation in coordination teleconferences
• throughout the pandemic, undertake and contribute to appropriate, timely and proportionate debriefs to ensure best practice is adopted through the response
• HSM Plan for
Infectious Diseases a
6.0 Command and Control Structure This section describes how the NHS will respond when a major incident, significant incident or emergency has been formally declared and the NHS has been asked to activate its major incident plans. It is important that all health services respond to each incident in a coordinated and consistent manner, information provided includes the alerting mechanisms for external and self-declared incidents, including trigger points and escalation procedures.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 17 of 48
The Incident Control Centre Plan provides support to the Major Incident Plan in terms of the management of command and control arrangements. The NHS response to an incident needs to be:
• Proportionate: Different approaches are necessary both to the varying size of incidents and also to the health implications of an incident.
• Flexible: The implications of incidents can change rapidly during their course. The NHS needs to have flexible systems which ensure that it has a response appropriate to the incident at any time.
• Clear: In particular, it must be clear at any time both to NHS organisations and to partner organisations which part of the NHS has taken overall command and control in a particular geographical area. The taking of command and control does not preclude other organisations from establishing their incident operations centers for their own organisations.
At all times during the course of an incident, it is the responsibility of the NHS England to ensure that there is clarity about which organisation is leading the NHS response. Escalation
Table 1 describes the three broad levels of escalation and provides broad parameters for decision making. It is the responsibility of the senior manager leading the NHS response at any particular time to decide, in conjunction with colleagues, what level of command is appropriate for the local NHS.
Table 1 NHS England incident alert and response levels
Alert Activity Action NHS England Incident levels
A
lert
D
ynam
ic R
isk
Ass
essm
ent
D
ecla
ratio
n of
Inci
dent
leve
l
1 A health related incident that can be responded to and managed by a local health provider that
requires co-ordination by the local CCG 2 A health related incident that requires the
response of a number of health provider organisations across NHS England (South
Locality) and will require NHS England (South Locality) to co-ordinate the NHS local support
3 A health related incident, that requires the response of a number of health provider organisations across the NHS England –
Midlands and East and requires NHS England regional co-ordination to meet the demands of
the incident the incident 4 A health related incident, that require NHS
England National co-ordination to support the NHS and NHS England response
*Adapted from NHS England incident alert and response levels

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 18 of 48
The establishment of a Strategic Coordinating Group (SCG) has been excluded from Table 1, as this is at the discretion of the Chief Constable of Hertfordshire Police and the NHS follows these arrangements. NHS England (South Locality) will provide NHS input to the SCG if required. In some circumstances the ENHCCG may provide the NHS input to a SCG, but this will be the exception rather than the rule.
ENHCCG On Call The CCG Senior Manager On Call is available at all times on 07909 913275. The On call rota is manned by the Chief Executive, Directors and Associate Directors. The on call shift runs from 10am Tuesday morning to 9.59am Tuesday morning of the following week. The on call rota is manned on a daily basis over Christmas, New Year and Easter. The phone is switched over by a member of the CCG administrative team and a text confirming the switch is sent to the outgoing and incoming manager. Each Senior Manager On Call has an on call folder which includes the contact details of CCG staff.
The rota is produced and communicated on a six monthly basis by the Governance Team. ENHCCG may establish an Incident coordinating centre (ICC) from which the incident can be managed. The incident coordinating centre for ENHCCG is based in The office next to the Board room, Floor Two, Charter House, Parkway, Welwyn Garden City, AL8 6JL. In the event that Charter House is not accessible see page 6 of the ICC Plan for alternative provision and remote ICC management. The role of the Incident coordinating centre is to: • manage the operational response to the incident • Co-ordinate response across the local health economy report to the NHS
England (South Locality) • handle media issues/enquiries • coordinate with district councils • manage the return to normality ensure liaison with other key partners as required
The Incident Co-ordination Centre has its own ICC Plan (see appendix 9) which details how it should be established, run and resourced. Incident Level 1 – East and North Hertfordshire CCG - GREEN The response will initially be led by the ENHCCG senior manager on call. If required the senior manager on call responding to the major incident may convene an Incident Management team with relevant expertise from within the CCG and externally (as necessary). The Incident Management team will manage the incident. Where the incident is managed from the ENHCCG Incident Coordination Centre (ICC) (see separate plan which can be found in appendix 9), there will be sufficient supplies / stores present to ensure logging and other administration tasks can be completed. It is likely that the ENHCCG Escalation Framework will be triggered, but at level 1 the incident would normally be managed by the CCG with escalation to NHS England (South Locality). See East and North Hertfordshire Clinical Commissioning Group Escalation Framework.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 19 of 48
Incident Level 2 – NHS England (South Locality) - YELLOW The NHS England (South Locality) on-call director may convene an incident management team with relevant expertise from within and external to the NHS England (South Locality) to direct and coordinate the management of the major incident. The team will take executive decisions in the light of best available information and obtain input from all relevant sources of expertise and agencies and convene quickly. An NHS England (South Locality) Incident Co-ordination Centre (ICC) may be set up to co-ordinate the incident. The location of which will be determined by the nature of the incident. The ICC will have direct contact with all responding NHS providers. Its role is to remain informed of their current status and provide relevant information to the SCG Health Gold representative. Incident level 3 - NHS England - AMBER An NHS England Regional ICC will normally be based at the offices in Cambridge. The role of the ICC will be:
• strategic management of the incident and return to normality; • reporting to the NHS England National team; downwards links with NHS
England (South Locality) ICC; communications and media management.
Incident level 4 - NHS England – National Command - RED An NHS England – National ICC could be established, where appropriate, feeding into either local or regional ICCs to ensure a consistent management approach across the incident area Multi-agency Command and Control There are three commonly accepted levels within emergency management command and control (Table 2) and adherence to these by all organisations ensures a coordinated response to a major incident.
Table 2: Levels within command and control structures
Level Role Colour Strategic Establish strategic objectives and overall
management framework. Ensure long-term resourcing/expertise.
Gold
Tactical Determine priorities in obtaining and allocating resources. Plan and co-ordinate overall response.
Silver
Operational Manage front line operations. Bronze
The multi-agency response to a major or significant incident or emergency is described below:
• The DH will be the source of information regarding the NHS for the Cabinet

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 20 of 48
Office Briefing Room at national level; • NHS England – (South Locality) will represent the NHS at regional level; • NHS England (South Locality) will attend the Strategic Coordinating Group led
by Hertfordshire Police. • Public Health England Centre will provide the Public Health Consultant to
attend and chair the Scientific and Technical Advice Cell (STAC); • NHS England (South Locality) may attend multi-agency silver and interact at a
bronze level; • Local CCGs may attend county wide silver and interact at a local bronze level.
Science and Technical Advice Cell (STAC) The Scientific and Technical Advice Cell (STAC) provides technical advice to the Strategic Coordinating Group. The STAC would be expected to advice on issues such as the impact on the health of the population, public safety, environmental protection, and sampling and monitoring of any contaminants. In the event of a major incident the STAC is activated by the Police Gold Commander through the cell lead or relevant duty officer. However, a senior public health professional (i.e. Director of Public Health or the PHE Director) may recommend to the Gold Commander that a STAC needs to be established due to the potential impact on the health of the local population from an actual or evolving incident. 6.1 ENH CCG response to a major incident 6.1.1 Alerting arrangements The ambulance service is likely to be the first NHS service to be notified of, and respond to, a no notice major incident. The ambulance service will:
• immediately notify or confirm with the police and the fire and rescue service the location and nature of the incident, including identification of specific hazards, for example, chemical, radiation or other known hazards
• alert the most appropriate receiving hospital(s) • alert the wider health community via the appropriate NHS England (South
Locality) • alert appropriate voluntary sector services
The standard alerting messages are:
1. Major Incident – standby
This alerts staff members that a major incident may need to be declared. Preparatory arrangements are then made appropriate to the incident
2. Major Incident declared – activate plan
This alerts staff members that the plan should be activated and additional resources mobilised.
3. Major Incident – stand down
Following the conclusion of an incident or the involvement of health in an incident, a Major Incident Stand Down message should be cascaded

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 21 of 48
to all stakeholders who were initially informed of the incident or who have become involved during the incident.
The CCG will review their own requirements, in conjunction with NHS England (South Locality), following a Major Incident Stand Down message to determine the most appropriate response from the CCG. Where the incident is a slow burn incident, for example pandemic flu. The Senior Manager on Call for East and North Hertfordshire Clinical Commissioning Group could be alerted to a major incident by one of a number of NHS organisations. Each CCG can declare its own major incident when its own services and/or assets are affected (or potentially) by, for example, fire, flood, major equipment breakdown, or civil disturbance (firearms).
In the event of being advised of a major incident standby or declared, the senior manager on call will implement actions outlined in the Major Incident Response action cards (which are referenced including contacting key ENH CCG staff including a Loggist). In cases where the CCG is alerted to a local incident within a local provider the CCG Senior Manager on call will determine whether there is a need to inform the Director on call for NHS England (South Locality) or any other local NHS providers or neighboring CCGs. In line with NHS England incident alert and response levels and utilising the template in Appendix 2. 6.1.2 Incident Management Team (IMT) In exceptional circumstances and if required, the ENHCCG Senior manager on Call responding to the major incident will convene an incident management team (see Operational Response Action Card 5) with relevant expertise from within and external to the CCG to direct and co-ordinate the management of the major incident and provide SITREP reports as required.
Specialist advice will be sought from the NHS England (South Locality) or Public Health England Centre, according to the particular nature of the incident being faced. The team will take executive decisions in the light of best available information and obtain input from all relevant sources of expertise and agencies and convene quickly. The Team will include a Loggist, who will record all actions and decisions by the Senior Manager On Call and decisions made by the Incident Management Team (see Operational Response Action Card 10). The template in Appendix 2 will be used for any reports generated by the IMT to NHS England.
In the event of a mass casualty situation ENH CCG will work together with Herts Valleys CCG in line with the Hertfordshire LRF Mass Casualties Plan. The incident management team will take responsibility for local communication with the Accountable Officer / CEO and other external provider organisations. It will also ensure (through the NHS England (South Locality) and with communication managers) that the public is informed and the media is briefed. It is likely that any communications would be through the NHS England (South Locality) or Public Health England.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 22 of 48
Meetings, investigations and actions will be properly documented. 6.1.3 Finances
The CCG recognises its obligations with regards to emergency planning, resilience, responding to major incidents and business continuity. Funds, as identified as being necessary, will be made available in the event of a major incident to ensure the CCG meets its obligations with respect to these. A dedicated cost code will be made available to track costs associated with the major incident. The cost code can be requested through the Finance Department by contacting Noreen Coles or Alison Saward.
6.1.4 Health and Safety Issues During and after a major incident the welfare of staff is of paramount concern to the CCG. Staff should, as under normal circumstances, pay due regard to the health, safety and welfare of themselves and other employees at all times. The need to regularly ‘risk assess’ during major incidents is extremely important and employees should not expose themselves to unnecessary risks. Where a higher risk situation is identified this should be assessed with the support of a line manager. It is also particularly important during emergency situations, where staff may experiencing higher levels of stress than normal, that regular meal breaks and periods of ‘off duty’ are observed. 6.1.5 Shift arrangements In the event of a significant / major incident or emergency having a substantial impact on the population and health services, it may be necessary to continue operation of the IMT for a number of days or weeks. In particular, in the early phase of an incident, the IMT may be required to operate continuously 24/7. Responsibility for deciding on the scale of response, including maintaining teams overnight, rests with the lead director.
A robust and flexible shift system will need to be in place to manage an incident through each phase. These arrangements will depend on the nature of the incident and must take into consideration any requirements to support external (for example SCG) meetings and activities. The Incident Manager is accountable for ensuring appropriate staffing of all shifts. During the first two shift changes 1-2 hours of hand over time is required. All changes in responsible senior manager will be preceded by a formal recorded handover. The CCG may need to consider staff accommodation dependent on the nature of the incident. A list of local hotels is available and accessible via the internet – search hotels in Welwyn Garden City. 6.1.6 Stand down arrangements at the end of a major incident As the incident diminishes and emergency services declare ‘major incident - stand

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 23 of 48
down’ a decision should then be made by the Senior Manager on Call from the CCG when it is appropriate to disband the IMT. This is because the CCG is likely to have a continuing role after emergency services have stood down.
Before the IMT team is disbanded an incident report should be prepared and supported via a ‘hot debrief’ and arrangements made to formally review the incident and the outcome. The conclusions of the report and any debriefings will help to inform future training and improve procedures.
6.1.7 Records Management An essential element of any response to an incident is to ensure that all records and data are captured and stored in a readily retrievable manner. These records will form the definitive record of the response and may be required at a future date as part of an inquiry process (judicial, technical, inquest or others). Such records are also invaluable in identifying lessons that would improve future response. The Incident Senior Manager is formally responsible for signing off the decision log and all briefing papers and documents relating to the incident. All records will be maintained by the CCG in line with the Data Protection Act and the CCG’s policy on this. This can be found in https://www.gov.uk/data-protection/the-data-protection-act Staff must be mindful when completing documentation that any record pertaining to an incident may be requested under the Freedom of Information Act. 6.1.8 Debriefing In order to identify lessons learned from an incident that will affect future plans, a series of debriefs post incident are seen as good practice. • Hot debrief: Immediately after incident with incident responders (at each location); • Organisational debrief: 48-72 hours post incident; • Multi-agency debrief: within one month of incident; • Post incident reports: within six weeks of incident. These will be supported by action plans and recommendations in order to update ENH CCG plans and provide any training and further exercising required. ENH CCG may also contribute to multiagency debriefing and actions from incident reports. The Incident Control Centre Plan includes the process for the maintenance of incident logs and minutes of meetings during and after the meeting. 6.1.9 Recovery Recovery and the return to normal working is an important part of the management of all major incidents. In many incidents, the aftermath of the major incident becomes another phase, taking stock of the overall impact and facilitating the restoration of normal health services in line with ENHCCG Business Continuity Plan. The Business Continuity Plan references the Business Impact Assessments which include recovery time objectives, restoration principles and how they will be managed. The recovery from an incident in many situations will be run in parallel to the

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 24 of 48
management of the incident and may require the appointment of a separate Incident Manager to lead this function. East and North Hertfordshire Clinical Commissioning Group’s role in recovery might include:
• renegotiating priorities with commissioned services; • assessing and arranging for the continuing need of primary
and community health services such as psychological support and counselling;
• provision of care and support to staff that may have been personally affected;
• consideration of legal and financial risks that might ensue. 6.2 Communications Effective communication is paramount to any major incident response. East and North Hertfordshire Clinical Commissioning Group have an effective communications cascade system and full details are set out in the Operational Response Action Cards 15. This cascade is tested through regular exercises. The communications cascade which is activated on declaration of a major incident includes alerting the communications desk (in hours) or on–call Communication Manager (out of hours) in the first tranche of contacts. The communications manager is responsible for media handling and represents the CCG in multi-agency press briefing arrangements. Additional responsibilities of the communications manager might include:
• to agree with other NHS agencies locally the procedure for coordinating information in an incident;
• to plan facilities which can be made available at short notice, e.g. rooms for the media;
• to prepare simple, easily understood information about NHS organisations;
• to ensure communications leads and designated spokespersons have appropriate training.
6.2.1 Media
The presence of media can be used effectively to support the coordination of a major incident response. Press statements will be coordinated through Hertfordshire Police when there is a Strategic Coordinating Group established.
In the event that a Scientific and Technical Advice Cell is set up to advise the Strategic Coordinating Group, the Director of Public Health and Public Health England Centre will be responsible for agreeing clear public health messages to be given to the public.
At levels below this the senior manager on call responsible for co-ordinating the incident will ensure advice/active involvement is sought from the communications desk (in hours) or Communication Manager (out of hours). 6.2.2 Public
APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 25 of 48
Information will be required to ensure public / patients and their next of kin are appropriately informed. Depending on the nature of the incident, provision of suitable facilities for the public will also need to be made. The provision of help lines for ENHCCG will be via Herts Urgent Care (HUC) (111 and GP OOH) who will assist by diverting enquires away from NHS switchboards (e.g. hospitals, GP Practices) which may already be experiencing a high volume of calls. 6.2.3 Languages Where necessary, support in interpretation will be requested from HUC who uses the services of Language Line, for who HUC have a contract with. 6.3 Business Continuity
The Civil Contingencies Act (CCA) 2004 places a statutory duty on organisations to develop a comprehensive approach to business continuity. As a category two responder ENHCCG is required to maintain plans to ensure that services are provided in the event of an incident so far as is reasonably practical. Business continuity plans have been developed in line with these requirements and link to arrangements for the recovery phase after a major incident. (See ENH CCG Business Continuity Plan for more details, which can be found via the intranet www.enhertsccg.nhs.uk ENHCCG will also ensure that providers have in place adequate business continuity plans and major emergency plans for their own organisation, as laid out in the NHS Standard Contract. http://www.commissioningboard.nhs.uk/nhs-standard-contract/ 6.4 Vulnerable Persons Within the Civil Contingencies Act (2004) the particular needs of vulnerable persons are recognised. These individuals are defined as “people present or resident within an area known to local responders who, because of dependency or disability, need particular attention during incidents”.
Vulnerable persons could therefore include children and older people; BME communities, particularly those for whom English is a second language, and people with disabilities, including physical disabilities and impairments, learning disabilities, mental illness and those with complex needs. 6.4.1 Black and Minority Ethnic Communities Care will be taken when producing and distributing information to ensure that it is accessible to all. This may necessitate the production of translated materials, the use of health advocates, and the use of interpreting services. 6.4.2 Children Many major incidents involve children and in some cases children are the main casualties. Children have special needs that are different from adults in terms of their size, physiology and psychological needs – all of which have an impact on their care. The Senior Manager on call and the IMT will need to consider and take account of

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 26 of 48
the children’s needs in planning and response to a major incident. Special consideration must be given to schools, nurseries, childcare centers and medical facilities for children. 6.4.3 People with inhibited physical ability This may be by reason of age, illness, disability, pregnancy or other reason. Attention should be paid to hospitals, residential homes, care homes and day centers likely to be housing any people with inhibited physical ability. Access to records of residents in the community who have inhibited physical ability is also important and may be achieved in partnership with Social and Community Services. 6.4.4 People with learning disabilities and mentally ill people ENHCCG will respond as appropriate in order to assist people with learning disabilities or mental illness by using existing facilities and arrangements wherever possible. If there is a need for additional or specialist assistance then help will be sought from Hertfordshire Partnership Foundation Trust as appropriate. 6.5 Exercises and Testing Plans
In accordance with emergency planning guidance, plans are tested through regular exercises, in partnership with other partners and dependent stakeholders including: Providers including primary care neighboring CCGs, social care, county and borough councils. Exercises can be led by the NHS England (South Locality) or be multiagency and ENHCCG will participate in all those that are relevant. A communication exercise is held on at least a six monthly basis, a CCG exercise is carried out annually. Details of all exercises are reported to the ENHCCG Governing Body annually and amendments as a result of training are incorporated into annual reviews of all EPRR plans, as appropriate. The Accountable Emergency Officer is responsible for ensuring that plans are regularly reviewed to ensure that they reflect legislative and/or organisational change and the on- going risk assessment process.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 27 of 48
Appendix 1 Pandemic flu
• The following provides a summary of the • definition of a pandemic, • disease (influenza or respiratory type disease) • national planning assumptions • UK strategic aims and objectives and • CCGs responsibilities in the event of a pandemic and the • Proportionate response in a pandemic
Please refer to the Hertfordshire and south midlands plan for infectious disease at pandemic level: with specific reference for pandemic influenza for full details. Definition of a pandemic A pandemic refers to a worldwide spread of an infectious disease, with outbreaks or epidemics occurring in many countries and in most regions of the world. A pandemic results when a new virus or new virus strain emerges which is markedly different from previously circulating strains and is able to:
• infect people (rather than, or in addition to, other mammals or birds); • spread from person to person; • cause illness in a high proportion of the people infected; and • spread widely, because most people will have little or no immunity to the new • virus/strain and will be susceptible to infection.
The Disease (Influenza or respiratory type disease) Outbreaks can be characterised by the sudden onset of a number of symptoms, notably fever, chills, headache, muscle pains, prostration and usually cough, with or without a sore throat or other respiratory symptoms. In a non-pandemic situation, most healthy people recover from these symptoms without complication after about a week, although they may be lethargic and have mild symptoms for longer. Complications are mainly respiratory, due to secondary bacterial infections such as middle ear infection (in children), bronchitis and pneumonia. This can lead to admission to hospital, severe illness and death. Respiratory infections may also exacerbate underlying diseases such as asthma, diabetes or coronary heart disease. Those at higher risk of more serious illness may include the very young, people aged 65 and over and patients with chronic chest, heart or kidney disease, pregnant women, persons with diabetes or reduced immunity due to other disease or treatment. For specific information on the outbreak always refer to www.phe.org.uk. The National guidance provides specific detail on infectivity and mode of spread, this can be accessed at www.dh.gov.uk/publications. For specific information on pandemic influenza please refer to Appendix D of the Hertfordshire and south midlands plan for infectious disease at pandemic level: with specific reference for pandemic influenza (appendix XX) . National planning assumptions A pandemic is most likely to be caused by a new subtype of the Influenza A virus but the plans could be adapted and deployed for scenarios such as an outbreak of another infectious disease, e.g. Severe Acute Respiratory Syndrome (SARS). A pandemic can emerge at any time, at any time of the year, anywhere in the world, including in the UK. Regardless of where or when it emerges, it is likely to reach the UK very quickly. It will not be possible to stop the spread of or eradicate the pandemic, either in the country of

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 28 of 48
origin or in the UK, as it will spread too rapidly and too widely. From arrival in the UK, it may be a further one to two weeks until sporadic cases and small clusters of disease are occurring across the country. Initially, pandemic activity in the UK may last for three to five months, depending on the season. There may be subsequent substantial activity (of the virus) weeks or months apart, even after the WHO has declared the pandemic to be over. Although it is not possible to predict in advance what proportion of the population will become infected with the new virus, previous studies and modelling suggest that half of the population will display symptoms of some kind (ranging from mild to severe). The transmissibility of the virus and the proportion of people in which severe symptoms are produced will not be known in advance. One of the main challenges for planning for a pandemic is the uncertainty surrounding the nature of the pandemic virus when it emerges and its likely impact. The UK influenza pandemic preparedness strategy 2011, and the additional material, provides planning assumptions to aid consistent and coherent planning. Planning must be sufficiently flexible to cope with both the lower and upper ends of the range of possible outcomes; Clinical Attack Rate
Cumulative clinical attack rates of up to 50% of the total population, spread over one or more waves each of around 12-15 weeks A second or more subsequent wave could be more severe than the first
Peak Clinical Attack Rate
Locally, 10% - 12% of the population per week
Hospitalisation Rate
Between 1% - 4% of those who are symptomatic may require hospital admission
Case Fatality Rate
Up to 2.5% of clinical cases (of those that are symptomatic may die) Local level planning target of excess deaths in the range of 210,000 – 315,000 nationally (approximately 0.4 – 0.5% of the population)
Peak Absence Rate
Up to 15% - 20% of workforce (large organisation) Up to 30% - 35% of workforce (small organisation)
Planning assumes that, once it has reached the UK, the infection will spread quickly and outbreaks are inevitable across the whole country. Based on past pandemics, the scale and severity of illness caused by (and hence the consequences of) pandemic influenza generally exceed those of even the most severe winter epidemics.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 29 of 48
UK Strategic Aims and objective The overall strategic objectives of the UKs approach to preparing for an influenza pandemic are: Minimise the potential health impact of a future influenza pandemic by:
• Supporting the international efforts to detect its emergence • Promoting individual responsibility and action to reduce the spread of infection
through good hygiene practices and uptake of seasonal influenza vaccination of in high risk groups
• Ensuring the health and social care systems are ready to provide treatment and support for the large numbers likely to suffer from influenza or its complications whilst maintain other essential care
Minimise the potential impact of a pandemic on society and economy by: • Supporting the continuity of essential services, including the supply of medicines, and
protecting critical national infrastructure as far as possible • Supporting the continuation of everyday activities as far as practicable • Upholding the rule of law and the democratic process • Preparing to cope with the possibility of significant numbers of additional deaths • Promoting a return to normality and the restoration of disrupted services at the
earliest opportunity
Instil and maintain trust and confidence by: Ensuring that health and other professionals, the public and the media are engaged and well informed in advance of and throughout the pandemic period and that health and other professionals receive information and guidance in a timely way so they can respond to the public appropriately. Clinical Commissioning Groups (CCGs) Before a pandemic, each CCG will:
• Identify a Pandemic Influenza Executive Lead (likely to be the AEO) to lead internal organisational pandemic planning activities in light of national and international developments, advice and guidance
• undertake internal business continuity planning in the context of pandemic influenza • communicate plans with employees, contractors, and affiliated organisations • participate in relevant planning groups to discuss, plan, exercise and share best
practice • ensure early engagement of communications professionals to devise, deliver and
maintain internal, external and stakeholder/ cross-partnership communications before, during and after a pandemic
• work with their commissioned service providers, in planning for surge in relation to elective work and the possible financial implications if there is on-going disruption to normal service levels over the period of a pandemic and its recovery phase
• participate in appropriate assurance processes regarding their arrangements and be assured that their commissioned services have adequate provisions in place for managing a pandemic
• work with NHS England Regional and South Localities to identify appropriate local providers to support the delivery of a pandemic influenza response, particularly regarding the provision of antiviral collection points through community pharmacies

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 30 of 48
During a pandemic, each CCG will: • support the national pandemic response arrangements as laid out in Department of
Health and NHS England guidance issued prior to or during a pandemic occurring • in line with other guidance, ensure 24/7 on-call arrangements remain robust and
maintained, particularly with respect to surge and responding to major incidents • lead the management of pressure surge arrangements with their commissioned
services as a result of increased activity as part of the overall response • support NHS England Regional and South Localities in the local coordination of the
response, e.g. through tried and tested surge capacity arrangements, appropriate mutual aid of staff and facilities, and provision of support to the management of clinical queries
• as necessary share communications with locally commissioned healthcare providers through established routes
• participate in the multi-agency response as appropriate and agreed with NHS England Regional and South Localities to ensure a comprehensive local response
• maintain close liaison with local NHS England colleagues, particularly when considering changes to delivery levels of NHS commissioned services
• enact business continuity arrangements as appropriate to the developing situation to ensure critical activities can be maintained
• maintain local data collection processes to support the overall response to the pandemic, including completion and submission of relevant situation reports and participation in coordination teleconferences
• throughout the pandemic, undertake and contribute to appropriate, timely and proportionate debriefs to ensure best practice is adopted through the response
After a pandemic, each CCG will: • contribute to local, regional and national health post-pandemic debriefs and consider
the implementation of recommendations from any subsequent reports • acknowledge staff contributions • assess the impact of the pandemic on the provision of commissioned services and
ensure that the ongoing service level is sufficient to meet the demands of the system • ensure the recovery of services to business-as-usual as soon as appropriate • review response update plans, contracts and other arrangements to reflect lessons
identified, particularly where these have been commissioned locally • collect financial and contractual impact information from commissioned providers

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 31 of 48
Impact Nature and Scale of illness
Key healthcare delivery Impact on wider society Public Messages
Initial Phase
Response led by public health services supported by primary care and pharmacy services, and making preparations for extra support should this initial phase be extended
• Sporadic cases may be reported from the community
• Possible limited local outbreaks (schools, care homes)
• Possible increased ratio of virus cases in critical care
• Health services no longer able to continue all activity
• Detection, diagnosis and reporting of early cases through testing etc
• ICUs may be under pressure
• Local and regional decisions to cease some health care activity
• Virus (e.g. Influenza) information line function active
• NPFS not activated. Initial preparations to use NPFS/ACP’s may occur in local areas
• Contingency plans for supporting care at home and respite care
• Normal health service continues
• Supplies of electricity, gas and fuel will remain at near-normal levels of supply. Routine maintenance afforded a lower level of priority if there are staffing shortfalls, essential repairs expected to continue
• Potential disruption to general supplies if peak staff absence coincides with technical or weather related supply difficulties
• Prepare to implement business continuity arrangements for management of excess deaths, if necessary
• Concern among teachers and parents about infection spread in educational settings may lead to teacher and pupil non-attendance
• Supply chain companies implement business continuity plans
• Possible review of legislation regarding drivers’ hours
• Justice system affected by absence of staff, judiciary and other parties. Maintain essential services in accordance with established business priorities
• the clinical effects of the infection
• Advice on seeking medical assessment when not improving or getting worse
• Information on NPFS • Information on collection
of medicines • Information about
antiviral medicines and tailored messages for children, pregnant women, elderly; and other at-risk groups (in liaison with expert bodies and support groups)
• Infection control and business continuity advice for specific occupations. E.g. funeral directors, registrars, cemetery and crematorium managers, police etc as appropriate
• Managing expectations of Critical Care

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 32 of 48
Impact Nature and Scale of illness
Key healthcare delivery Impact on wider society Public Messages
Low • Similar numbers to moderate or severe seasonal influenza outbreaks
AND • In the vast majority of
cases - mild to moderate clinical features
Business as usual activities to continue for as long as possible except in areas with “hot-spots” of high activity and social care services may remain largely unaffected.
• Primary and hospital services coping with increased pressures associated with respiratory illness, with maximum effort
• Intensive care units (ICUs) nearing or at maximum pressure
• No significant deferral of usual activities
• Virus (e.g. Influenza) information line function active
• ACPs established in hotspots only
• NPFS active depending on pressures in primary care
• Use existing legislation to allow the supply of antiviral medicines at premises that are not a registered pharmacy
• Increase in staff absence due to sickness – similar to levels seen in seasonal influenza outbreaks
• No significant or sustained impact on service and business capacity
• Consider arrangements for sickness absence surveillance
• As above; • Information on the
pandemic and the clinical effects of infection, and what to do
• Information about antiviral medicines and tailored messages for children, pregnant women, elderly and other at risk groups (in liaison with expert bodies and support groups)
• How to use your local health service
• Employers planning in advance for sickness absence, service re- prioritisation and alternative ways of working

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 33 of 48
Moderate • Higher number of cases than large seasonal epidemic
• Young healthy people and those in at-risk groups severely affected
AND/OR • more severe illness
All health and social care services will be stretched and will need to reduce or cease non-urgent activity in order to make the maximum capacity available to meet the health care needs of those who are severely ill as a result of the virus.
• Health services no longer able to continue all activity
• ICUs under severe pressure
• Local and regional decisions to cease some health care activity
• information line function active
• NPFS activated as required in each country
• Local areas establish ACPs as required in each country
• Contingency plans for supporting care at home and respite care
• Continued compliance with statistical reporting standards
• Supplies of electricity, gas and fuel will remain at near-normal levels of supply. Routine maintenance afforded a lower level of priority if there are staffing shortfalls, essential repairs expected to continue
• Potential disruption to general supplies if peak staff absence coincides with technical or weather related supply difficulties
• Prepare to implement business continuity arrangements for management of excess deaths, if necessary
• Concern among teachers and parents about infection spread in educational settings may lead to teacher and pupil non-attendance
• Supply chain companies implement business continuity plans
• Possible review of legislation regarding drivers’ hours
• Justice system affected by absence of staff, judiciary and other parties. Maintain essential services in accordance with established business priorities
• Information on the pandemic and the clinical effects of the infection
• Advice on seeking medical assessment when not improving or getting worse
• Information regarding NPFS
• Information regarding collection of medicines
• Information about antiviral medicines and tailored messages for children, pregnant women, elderly; and other at-risk groups (in liaison with expert bodies and support groups)
• Infection control and business continuity advice for specific occupations. E.g. funeral directors, registrars, cemetery and crematorium managers, police, healthcare professionals as appropriate
• Managing expectations the public

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 34 of 48
High • Widespread disease in
the UK AND/OR • most age-groups
affected AND/OR • severe, debilitating
illness with or without severe or frequent complications
All health and social care services will be stretched and will need to reduce or cease non-urgent activity in order to make the maximum capacity available to meet the health care needs of those who are severely ill as a result of the virus.
• GPs, community pharmacies, district nurses and social carers, independent sector, residential homes and voluntary organisations fully- stretched trying to support essential care in the community WITH consequential pressure on secondary care
• Hospitals can only provide emergency services
• NPFS working to capacity; ACPs under pressure
• Virus (e.g. Influenza) information line function active
• Critical Care services: demand outstrips supply, even at maximum expansion
• Emphasis on maintaining supplies and staffing
• Transport, schools, shops affected by sickness and family care absences;
• Numbers of deaths putting pressure on mortuary and undertaker services
• Possible implementation of national legislative changes to facilitate changes in working practice (eg death certification, drivers’ hours, sickness self-certification requirements, Mental Health Act, benefits payments)
• Justice system affected by absence of staff, judiciary and other parties. Maintain essential services in accordance with established business priorities
• Messages about progress of the pandemic, availability of healthcare and other services
• Advice on how to minimise risks of transmission.
• Information on how to support family members and neighbours
• Advice on where to get help for emergencies
• Truth about how services are coping and what they are doing to cope and managing health service demand
• Explanation of triage systems to align demand and capacity
• Some civil contingencies advice, including advice to specific occupations such as paramedics, funeral directors, registrars, cemetery and crematorium managers, police etc as appropriate

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 35 of 48
Appendix 2 ACTION: Initial risk assessment
The following need to be considered by the Senior Manager on Call An assessment of the situation will determine what action needs to be taken. Using the information at hand and taking account of a worst case scenario where knowledge is limited, consider the following and record all relevant information.
Questions to consider Information Collected?*
What is the size and nature of the incident? Area and population likely to be affected - restricted or widespread Level and immediacy of potential danger - to public and response personnel
Timing - has the incident already occurred or is it likely to happen? What is the status of the incident? Under control Contained but possibility of escalation Out of control and threatening Unknown and undetermined What is the likely impact? On people involved, the surrounding area On property, the environment, transport, communications On external interests - media, relatives, adjacent areas and partner organisations
What specific assistance is being requested from the NHS? Increased capacity - hospital, primary care, community Treatment - serious casualties, minor casualties, worried well Public information Support for rest centers, evacuees Expert advice, environmental sampling, laboratory testing, disease control
Social/psychological care How urgently is assistance required? Immediate Within a few hours Standby situation
*Key √ = Yes X = no ? = Information awaited N/A = Not applicable

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 36 of 48
Appendix 3
NHS MAJOR INCIDENT SITUATION REPORT - SITREP
Note: Please complete all fields. If there is nothing to report, or the information request is not applicable, please insert NIL or N/A.
Organisation: Date:
Name (completed by): Time:
Telephone number:
Email address:
Authorised for release by (name & title):
Type of Incident (Name)
Organisations reporting serious operational difficulties
Impact/potential impact of incident on services / critical functions and patients

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 37 of 48
Impact on other service providers
Mitigating actions for the above impacts
Impact of business continuity arrangements
Media interest expected/received

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 38 of 48
Mutual Aid Request Made (Y/N) and agreed with?
Additional comments
Other issues
NHS CB Regional Incident Coordination Centre contact details: Name: Telephone number: Email:

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 39 of 48
Appendix 4 Planning Structure
Response structure

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 40 of 48
Appendix 5 – Equality Impact Assessment Stage 1 Screening
1. Policy EIA Completion Details Title: Major Incident Plan Names & Titles of staff involved in completing the
EIA: - Sarah Feal - Company Secretary - Jas Dosanjh - Head of Risk Management
Proposed Existing
Date of Completion: January 2015
Review Date: January 2016 2. Details of the Policy. Who is likely to be affected by this policy?
Staff Patients Public 3. Impact on Groups with Protected Characteristics Probable impact on group? High,
Medium or Low
Please explain your answers Positive Adverse None
Age
Being married or in a civil partnership
Disability, inc. learning difficulties, physical disability, sensory impairment etc.
Having just had a baby or being pregnant
Race, ethnicity, nationality, language etc.
Religion or belief
Sex (inc. being a transsexual person)
Sexual Orientation
Other:
No impact on any of the groups above.
No action to be taken/planned as a result of the equality impact assessment as the impact assessment showed that this policy had a neutral effect on each of the protected characteristics.
4. Which equality legislative Act applies to the policy? Human Rights Act 1998 Equality Act 2010 Health & Safety Regulations
Mental Health Act 1983 Mental Capacity Act 2005
5. How could the identified adverse effects be minimised or eradicated? N/A 6. How is the effect of the policy on different Impact Groups going to be monitored? N/A

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 41 of 48
Appendix 6 Privacy Impact Assessment Stage 1 Screening
1. Policy PIA Completion Details Title: Major Incident Plan Names & Titles of staff involved in completing the
PIA: - Sarah Feal - Company Secretary - Jas Dosanjh - Head of Risk Management
Proposed Existing
Date of Completion: January 2015
Review Date: January 2016
2. Details of the Policy. Who is likely to be affected by this policy? Staff Patients Public
Yes No Please explain your answers Technology Does the policy apply new or additional information technologies that have the potential for privacy intrusion? (Example: use of smartcards)
Identity By adhering to the policy content does it involve the use or re-use of existing identifiers, intrusive identification or authentication? (Example: digital signatures, presentation of identity documents, biometrics etc.)
By adhering to the policy content is there a risk of denying anonymity and de-identification or converting previously anonymous or de-identified data into identifiable formats?
Multiple Organisations Does the policy affect multiple organisations? (Example: joint working initiatives with other government departments or private sector organisations)
Data By adhering to the policy is there likelihood that the data handling processes are changed? (Example: this would include a more intensive processing of data than that which was originally expected)
If Yes to any of the above have the risks been assessed, can they be evidenced, has the policy content and its implications been understood and approved by the department?
N/A

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 42 of 48
Appendix 7 Memorandum of Understanding Information Sharing
Memorandum of Understanding on EPRR – Hertfordshire Local Health Resilience Partnership

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 43 of 48
Memorandum of Understanding on EPRR Hertfordshire Local Health Resilience Partnership Version number: 2 First published: April 2013 Updated: June 2015 Prepared by: Andy Kelly – EPRR / Delivery Lead NHS England Classification: OFFICIAL Contents Contents 43
1 Introduction 44
2 Key principles 44
3 NHS England role in EPRR 44
4 Commissioners’ and Providers’ role in EPRR 45
5 Signatories 47

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 44 of 48
Introduction This memorandum of understanding (MOU) sets out the agreed contribution to emergency preparedness, resilience and response (EPRR) within Hertfordshire between:
The NHS England Central Midlands sub region (NHS England) who lead on EPRR, acting in its EPRR functions on behalf of the NHS at the Hertfordshire local resilience forum (LRF); and The following commissioners and providers of NHS funded care or services:
• Clinical Commissioning Groups
o NHS East and North Hertfordshire CCG
o NHS Herts Valleys CCG
• West Hertfordshire Hospitals NHS Trust
• East and North Hertfordshire NHS Trust
• East of England Ambulance Service NHS Trust
• Hertfordshire Community NHS Trust
• Hertfordshire Partnership University NHS Foundation Trust
• Herts Urgent Care
Key principles a. That NHS England is empowered to use / call upon such relevant resources as may be
necessary from any one or all of the NHS funded providers within the LRF area of Hertfordshire in response to a major incident.
b. That each provider is required to maintain appropriate plans detailing how the organisations plan for, respond to and recover from a major incident. Provider incident response plans should contain provision for training key staff and provision for exercising the plan to ensure it is effective.
c. That no organisation should be expected to suffer financially from being asked to respond to an emergency (unless under SC 30.10 - 30.19); equally, no organisation should wait until full financial consequences are clear before initiating a response
NHS England’s role in EPRR NHS England must ensure that the commissioners’ and providers’ incident response plans are coordinated and complementary, and enable the NHS England to command, control and coordinate the NHS response when appropriate within Hertfordshire.
In order to ensure the Hertfordshire health economy is resilient and has appropriate levels of preparedness to respond effectively to a significant

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 45 of 48
incident or emergency, NHS England will performance manage all applicable providers ensuring:
a) Facilitation and overseeing the emergency planning and preparedness functions of the area/county/district NHS health systems;
b) That communications strategies and procedures are in place to deal with any event within the scope of a major incident and service continuity planning;
c) That it represents the Hertfordshire health systems in the local resilience forum in accordance with the Civil Contingencies Act 2004;
d) That it co-chairs the local health resilience partnership (LHRP) in Hertfordshire to facilitate health sector preparedness and planning for emergencies at LRF level;
e) That an appropriate representative from the NHS England gold (strategic) command rota attends a multi-agency strategic coordination group (SCG);
f) That, through the NHS gold (strategic) command arrangements, it leads the local NHS response to support the combined response of all emergency services and other agencies;
g) That, through the NHS gold (strategic) command arrangements, it leads the local / county NHS health systems response to support the NHS England Midlands and East in regional and/or national incidents;
h) Robust mutual-aid agreements exist across the county health systems within the NHS, and other partner agencies, including business continuity plans;
i) Liaison with NHS England Midlands and East over the provision of wider NHS assistance during major incidents; and
j) That it assists the NHS England Midlands and East with any internal and/or independent emergency planning reviews.
Commissioners’ and Providers’ role in EPRR All commissioners and providers of NHS funded care and services are expected to:
a) Comply with the standards and principles for emergency planning laid down in the:
• NHS England Emergency Preparedness Framework 2013;

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 46 of 48
• NHS England Command and Control Framework for the NHS during significant incidents and emergencies (2013);
• Other applicable NHS England EPRR guidance;
• The NHS Standard Contract, and;
• The Civil Contingencies Act 2004
b) Produce, review and validate up-to-date incident response plans, in accordance with current NHS England guidance;
c) Train and exercise staff internally as well as in cooperation with the Hertfordshire LRF training and exercising programme;
d) Ensure that communications strategies and procedures are in place to deal with any event within the scope of a major incident and service continuity planning;
e) Implement internal organisational incident response plans and maintain the health response in support of NHS England as appropriate;
f) Effectively contribute to the combined response of all emergency services and other agencies, including by mutual aid;
g) Deliver (as appropriate) primary and community health services, including the mobilisation of community resources and support designated receiving hospitals where appropriate;
h) Assist NHS England to compile an annual report for the NHS England regional director on the health sector’s emergency planning, capability and capacity in responding to national, regional or LRF level incidents;
i) Participate in NHS England’s annual reviews of compliance against EPRR Core Standards;
j) Plan for surges in activity due to seasonal or other predictable causes, as well as maintain robust staffing rotas
k) Undertake vaccination of front-line staff against seasonal influenza to the level agreed nationally
l) Send appropriate representation to the LRF, LHRP or sub-groups when required to do so; and
m) Liaise with local authority and voluntary agencies in the provision and receipt of wider assistance during major incidents.
This memorandum of understanding will be subjected to an annual review.

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 47 of 48
Signatories Sign Date
Dominic Cox
NHS England Locality Director and Co-Chair of Local Health Resilience Partnership
Sign Date
Jim McManus
Director of Public Health and Co-Chair of Local Health Resilience Partnership
Sign Date
Sharn Elton
NHS East and North Hertfordshire CCG
Sign Date
Alan Warren
NHS Herts Valleys CCG
Sign Date
[ ]
West Hertfordshire Hospitals NHS Trust
Sign Date
[ ]
East and North Hertfordshire NHS Trust
Sign Date
[ ]
East of England Ambulance Service NHS Trust
Sign Date
[ ] Hertfordshire Community NHS Trust
Sign Date
[ ]
Hertfordshire Partnership University NHS Foundation Trust
Sign Date
[ ]
Herts Urgent Care

APPENDIX 2
Major Incident Plan – Jan 2015 to Jan 2016 (FINAL v.2.0) East and North Hertfordshire Clinical Commissioning Group
Page 48 of 48
Appendix 9 Incident Control Centre Plan ..\Incident Co-ordination Centre\Incidence Coordination Centre Plan.docx

APPENDIX 3
April 2015 Version: draft 1
Page |1 of 27
Incident Coordination Centre Plan Location of ENCCG Incident Control Centre: Floor Two Charter House Parkway Welwyn Garden City Herts AL8 6AE

APPENDIX 3
April 2015 Version: draft 1
Page |2 of 27
Document Management Document Title Incident Coordination Centre Plan
Document Type EPRR Operational Plan
Description Instructions for establishing a full Incident Coordination Centre
Target Audience On Call Directors and Managers, EPRR Lead
Author Sharn Elton, Director of Operations
Responsible Directorate Director of Operations
Approved by Governing Body
Date issued
Version number Version 1 Draft April 2015
Next review date
Supersedes Related documents
Version 1 Draft July 2013
On-Call Pack
Major Incident Plan
ICT Systems Disaster Recovery Plan Hertfordshire
Internal Distribution On Call Managers & Directors
External Distribution Area Team
Contact Details: Name: Sharn Elton, Director of Operations
Address: 2nd Floor, Charter House, Parkway, Welwyn Garden City,
Herts AL8 6JL
Telephone: 01707 367278
Email: [email protected]
Dedicated Incident Email: [email protected]

APPENDIX 3
April 2015 Version: draft 1
Page |3 of 27
Contents
Document Management
Guide Introduction 4
Activating the Incident Coordination Centre 4 Authorised Persons 4 In Hours Incident Coordination Centre Setup 4 Out of Hours Incident Coordination Centre Setup 5 Activation Principles 5
Accessing the Incident Coordination Centre 5 Location 5 Out of Hours Access 5 Alternative Incident Coordination Centres 5 Remote ICC Management 5 IT Equipment 6 Photocopying 6 Staff Welfare 6 Room security 7
Incident Coordination Centre command structure 7
Key Considerations 8
Incident Coordination Centre strategy & meetings 8
Recovery 8
Major Incident Stand Down 9
Debrief 11
Finances 11
Appendix 1 – Charter House Location 12 Appendix 2 - Floor Plan 13 Appendix 3 – Setting up the ICC 13 Appendix 4 – ICC Contact Details 15 Appendix 5 – Incident Draft Strategy 16 Appendix 6 – Draft agenda for Incident Team Meeting 17 Appendix 7 – Major Incident Plan 27 Appendix 8 – ENCCG Action Cards 27

APPENDIX 3
April 2015 Version: draft 1
Page |4 of 27
Guide Introduction This guide sets out the arrangements for establishing and running an Incident Coordination Centre (ICC) for East and North Herts Clinical Commissioning Group (ENCCG) to provide support to the NHS within its boundaries in an emergency scenario.
This guide provides the reader with:
• The information to gain access to the building that accommodates the ICC • Guidance on how to lay out the ICC • Details of the computer login and telephone arrangements • The ICC management structure • Guidance on how to stand down the ICC
Activation of the ICC is set against specific timescales within the NHS England Command and Control Framework:
• Within 45 minutes of notification of an incident: An initial operating capability is established after being informed of an incident i.e. a response mailbox monitored & 2 x telephones manned
• Within 2 hours of notification: A fully operational ICC capability is established
Activating the Incident Control Room Authorised Persons
The decision to activate the ICC can be taken by:
• ENCCG Manager On-Call • ENCCG Directors • ENCCG EPRR Lead
In-hours Incident Coordination Centre Setup
During office hours (Monday-Friday 08:00 hrs – 17:00 hrs, excluding public holidays), the Duty Manager/Director On-Call will lead the setting up of the ICC.
ENCCG will review the strategic objectives and ensure that enough support is present within the room. They, Duty Manager/Director on Call have the authority to release staff from their normal duties.

APPENDIX 3
April 2015 Version: draft 1
Page |5 of 27
Out-of-hours Incident Coordination Centre Setup (OOH)
During out-of-hours ENCCG Director On-Call is responsible for establishing the ICC; they also review the strategic objectives and ensure that enough support is present within the room. The Director on Call seeks active involvement from the communication desk and Communication Manager
Activation Principles
If requested to support the ICC, staff are to immediately make their way to it and begin setting it up. The most senior manager present is to assume the role of ICC Manager until relieved by the appropriate post holder.
Hard copies of plans will be available in the ICC. Electronic copies of this and other documents are held by on-call staff with electronic copies on the shared drive on the organisations servers:
..\Major Incident Plan\2015-01-29 Major Incident Plan FINAL v 2 0.docx
Accessing the Incident Coordination Centre
Location
The primary location for our ICC is: ICC room , Second Floor, Charter House, Parkway, Welwyn Garden City, Hertfordshire AL8 6AE [see Appendix 1 and 2 for location and building maps].
Out of Hours Access
Access to the building in an emergency is available 24 hours a day, 7 days per week, as there is a permanent security presence in the building. Entry should be via the car park accessible from Wigmores North, use the intercom to gain access if staff do not have personal access to the car park.
Entry to Charter House is via personal ID swipe cards, which are issued to all personnel based within Charter House.
Access to the ICC is controlled by the access control system using your ID Card
Alternative Incident Coordination Centres
The alternative off site location is the Headquarters of NHS Herts Valley CCG in Hemel Hempstead. (This is a reciprocal arrangement).
Remote ICC Management
In the event that Charter House is unavailable to establish the ICC, or travel to the IC is restricted, the ICC can be set up remotely through accessing the CCGs intranet. Intranet log On:

APPENDIX 3
April 2015 Version: draft 1
Page |6 of 27
The File Path is: www.enhertsccg.nhs.uk
Your user name is your firstname surname (there is a space between them)
Your password is your surname123
Once logged in you will have access to
• On call staff call out list (also available in the on call pack and NHS net account)
• EPRR plans via the NHS net account • HR also have remote access to an all staff contact list • The Incident email address is accessible via the NHS net website
at [email protected] and the pass word is July2015 (ie, month 2015)
IT Equipment
The ICC will have two dedicated phones and computers, printers and faxes are located in the general office just outside the room connected by the network.
The phone numbers are:
01707 333067 (incoming calls) and 01707 327898 (outgoing calls) The dedicated email address is: [email protected] and the password is Maymay2015 (this is changed every month, but is month and year format, only doubled in this instance to make up over 8 characters)
Photocopying
Photocopiers are located as shown on the building maps in Appendix 2.
Staff Welfare
The Incident Director will make every effort to ensure that all staff receive appropriate rest breaks and, in conjunction with the ICC Administration, ensure that

APPENDIX 3
April 2015 Version: draft 1
Page |7 of 27
adequate numbers of staff are available at all times. (i.e. loggists and minute takers having 2 hour shifts only)
Rest breaks may be taken in the open plan area of Floor Two in Charter House. Kitchen facilities are available, as well as refreshments from the board room next to the ICC. A water boiler is situated in the Kitchen (see Appendix 2)
Room Security
All staff must ensure they sign in and out of the ICC at the start and end of their shifts, including rest breaks.
ID must be worn at all times; people not expected in the ICC area must be challenged. Any visitors must be confirmed with the ICC Manager.
Incident Coordination Centre Command Structure
Action cards for these roles will be found in the ENCCG Incidence Response Plan. Depending on the incident and the level of involvement required not all of these roles may be necessary, but in some instances there may be the need to have multiple Operation Officers.
Director
Incident Director
ICC Manager
Loggist
EPRR Advisor/Lead
Communications Lead
Minute Taker
Operations Officer
Ops Coordinator(s)
Operations Officer
Operations Officer

APPENDIX 3
April 2015 Version: draft 1
Page |8 of 27
Key Considerations Within the ICC there are a number of items to consider including:
• A full record of decisions and actions, in addition to the information a log must be kept. The use of decision log books (stored in the Incident Box within the Incident Cupboard) is mandatory
• Individuals must maintain their own log books throughout the Incident. • All phone calls incoming and outgoing are to be logged • All entries in log books must be written in accordance to the guidance that can
be found on their inside covers • Post incident all incident related log books, note books, flip charts,
photographs of whiteboards, emails, faxes, and personal notes must be archived and secured for review and any future inquiries or enquiries.
Incident Coordination Centre Strategy & Meetings At the earliest possible time the Incident Director will convene an initial meeting of the incident management team and other relevant persons. A suggested initial meeting agenda and a generic draft strategy and objectives can be found in Appendix 5. Consider inviting other Health Partners to form a Health Coordination Group via teleconference:
The purpose of the first meeting is to:
• Brief the incident management team; • Confirm the strategy and priorities; • Develop the immediate actions of the team; • Confirm staffing is appropriate; and, • Ensure effective communication with internal and external partners is
commenced
Recovery If the strategy for the incident includes the commencement of a recovery cell this is to be initiated by the Incident Director, including appointing a separate incident manager to lead this function as described in the Major Incident Plan (section 6.1.9). Supported by staff from Finance and Information. The Recovery group’s aims are:
• Develop a strategy to enable the affected areas of the NHS to return to a normality phase at the earliest possibility.

APPENDIX 3
April 2015 Version: draft 1
Page |9 of 27
• Identify needs for instigating the recovery strategy • Review issues being considered by the NHS and partners in the region and
advise on any implications for longer term recovery strategies.
The ICC is to remain operational whilst the incident is in response phase, through to the initial parts of the recovery phase of an incident. The Incident Director is to review the organisations’ position with the incident management team on a continuous basis. Only the Incident Director can stand the incident down.
Major Incident Stand Down
This a formal process which must be communicated to all agencies in a succinct manner. This would usually take place via the communication routes you have been using to manage the incident and is most easily executed via a formal major incident stand down email to all partner organisations dedicated email address.
While emergencies are often triggered by ‘big bang’ events and alerts are cascaded by UK Ambulance Services there are other potential circumstances where an NHS incident occurs; for example infectious disease outbreaks. In such cases the ambulance service may or may not be involved and may not be the alerting mechanism for the health sector. In the event of such an incident the communication cascade mechanism should be via local commissioners who should ensure they also alert the NHS England regional team. In some instances such alerts may also arise directly from NHS England. NHS England will assist CCGs in implementing Command and Control mechanisms and the deployment of appropriate NHS resources should the response extend beyond the operational area of a single CCG. Health services should use standard alerting messages at all times

APPENDIX 3
April 2015 Version: draft 1
Page |10 of 27
STANDARD MESSAGES
1. Major incident – standby
This alerts the NHS that a major incident may need to be declared Major incident standby is likely to involve the participating NHS organisations in making preparatory
arrangements appropriate to the incident, whether it is a ‘big bang’ ,a ‘rising tide’ or a pre-planned event.
2. Major incident declared – activate plan
This alerts NHS organisations that they need to activate their plan and mobilise additional resources
3. Major incident – cancelled
This message cancels either of the first two messages at any time
4. Major incident stand down
• All receiving hospitals are alerted as soon as all live casualties have been removed from the site. Where possible, the Ambulance Incident Commander will make it clear whether any casualties are still enroute
• While ambulance services will notify the receiving hospitals(s) that the scene is clear of live casualties, it is the responsibility of each NHS organisation to assess when it is appropriate for them to stand down their own response

APPENDIX 3
April 2015 Version: draft 1
Page |11 of 27
Once the decision has been made to stand the response or recovery phase down the incident coordination centre manager will ensure that all records are collected, catalogued and archived for any subsequent review, inquiry or enquiry. All resources used a most are to be replenished as part of the stand down process. This is the responsibility of the Incident Coordination Centre Manager.
Debriefing
In order to identify lessons learned, a series of debriefs post incident are seen as good practice:
• Hot debrief: Immediately after incident with incident responders (at each location)
• Organisational debrief: 48-72 hours post incident • Multi agency debrief: within one month of incident • Post incident reports: within six weeks of incident
These will be supported by action plans and recommendations in order to update ENH CCG plans and provide any training and further exercising required.
ENH CCG may also contribute to multiagency debriefing and actions from incident reports.
A formal debrief is to be arranged by the Incident Director which will include all members of staff within the organisation involved in the incident. Individual debriefs are to be held with the Incident Director(s) and supporting manager(s) prior to the formal debrief.
Finances
All expenses and costs associated with the incident are to be collated, and a budget line allocated by finance to allow an auditable trace of expenditure for the incident. This includes all commissioned work undertaken.

APPENDIX 3
April 2015 Version: draft 1
Page |12 of 27
The CCG recognises its obligations with regards to emergency planning, resilience, responding to major incidents and business continuity. Funds, as identified as being necessary, will be made available in the event of a major incident to ensure the CCG meets its obligations with respect to these. A dedicated cost code will be made available to track costs associated with the major incident. This can be obtained by contacting Finance (Noreen Coles/Alison Saward) via email.

APPENDIX 3
April 2015 Version: draft 1
Page |13 of 27
Appendices
Appendix 1 – Charter House Location & Premises Maps Address: Charter House, Parkway, Welwyn Garden City, Hertfordshire AL8 6JL

APPENDIX 3
April 2015 Version: draft 1
Page |14 of 27
Appendix 2 – Floor Plan
Charter 2nd Meeting rooms.pdf
Appendix 3 – Setting up the ICC
Note: Within 45 minutes of notification of an incident we must have an initial operating capability established (i.e. a response mailbox monitored & 2 x telephones manned)
Within the ICC are 2 Networked work stations, each with a telephone and PC, conference telephone, whiteboards and marker pens will be available.
First Steps
1. To enable initial operating capability by the ICC Manager and Operation(s) Officer
2. Ensure all telephones are plugged in and the ringers are turned on. 3. Log on to a PC and sign in to the generic email account partner agencies as
required 4. List key contacts on the white board
Internal extensions: External Calls: Reception: 0 (External 01707 390855) Call Pick-Up: *3 Diverting: THIS IS NOT RECOMMENDED IN AN INCIDENT ROOM
Closing the ICC
When the decision to close the ICC is confirmed, all equipment must be returned to the correct locations.
All log books should be submitted to the EPRR Team or placed in the lockable cupboard in the ICC if this is not possible.

APPENDIX 3
April 2015 Version: draft 1
Page |15 of 27
Appendix 4 – Incident Coordination Centre Contact Details NB: Chief Executives may be expected to attend the Health Co-ordination Group
User Name Telephone Number Email Address ICC Number ICC Manager Ops Officer 2 Ops Coordinator ICC Admin Communications Officer 1 Incident Director Staff Officer / EPRR Adviser
Loggist Fax 1

APPENDIX 3
April 2015 Version: draft 1
Page |16 of 27
Appendix 5 – Incident Draft Strategy NHS Incident Strategy
It is the intention of the NHS to respond to and manage the on-going incident in a way which will promote and save life; reduce suffering; and, is compatible with the vision and values of the NHS. Through effective coordination, sound planning and good leadership the Incident Director will:
1. Maintain public confidence and minimise the impact of the incident by ensuring that the NHS is responding effectively to the incident.
2. Ensure that the NHS response is coordinated and integrated with all NHS organisations.
3. Where applicable, ensure that the NHS response is coordinated and integrated with all partner organisations.
4. Maintain effective capacity management within the health economies affected, by:
a. Assessing and identifying any gaps in the response capability of the organisations supporting this incident; and
b. Facilitating requests for mutual aid. 5. So far as is reasonably practicable take all measures to employ all
appropriately identified control measures to safeguard staff and patients under the terms of health and safety legislation.
6. Ensure public messages are coordinated with other NHS organisations, emergency services, and multi-agency partners.
7. Ensure that effective business continuity and recovery arrangements are in place across the organisation and review where necessary.
8. Provide support and representation at any multiagency coordinating groups as required.
9. Create and maintain a well-documented, auditable plan and decision log for the incident at all levels of command.
10. Review this strategy at least every 4 hours.
Signature:___________________________ (Gold Strategic Command)
Date: ____________________ Time: _______________ (24hour clock)

APPENDIX 3
April 2015 Version: draft 1
Page |17 of 27
Appendix 6 – Draft agenda for Incident Management Team meeting
1. Introductions a. Decision & Information Log Book maintenance overview b. Confirmation that everyone is present who is required
2. Situation a. Current Situation b. Update from Organisations present c. Summary by Incident Director
3. Strategy & Priorities a. Set Strategy, Objectives and Priorities b. Establish work routine (Battle Rhythm/Meeting schedule) c. Confirm reporting arrangements up and down hierarchy d. Review situational analysis, plan activation, mutual aid requirements e. Develop a Communication Plan for the incident f. Confirm critical care information
4. Incident Management Team a. Membership and Staffing requirement b. Role and Responsibilities c. Shifts & relief d. Administrative and Welfare Arrangements
5. Incident Control Room a. Equipment and resources b. Hours of operation
6. Any other business 7. Confirmation of Decisions and Actions 8. Next meeting at_____________________________________

APPENDIX 3
April 2015 Version: draft 1
Page |18 of 27
Appendix 7 – EN CCG Major Incident Plan
IN THE EVENT OF A MAJOR INCIDENT FOLLOW AND COMPLETE
THE MAJOR INCIDENT SHEETS
Call Out
Major Incident Standby
Major Incident Declared
Major Incident
Major Incident
This alerts the NHS that a Major Incident may be need to be declared
Likely to involve the participating NHS organisations in making preparatory arrangements appropriate to the incident whatever the cause.
Each NHS organisation to assess their own organisation’s appropriateness to stand down.
Ambulance services will notify the receiving hospital(s) that the scene is clear of live casualties.
Cancels
Major Incident: STANDBY
Alerts the NHS of the need to activate plans and mobilise resources as necessary
Incident Management Team to be activated (as necessary)
Notify all other trusts and Area Team
Incident Management Team to be put on standby/have initial meeting.
Identify lead director to be responsible for this incident
Communicate to all staff notified (of stand by or activate) that the incident has been cancelled and no further action is required
Communicate to all staff notified (of stand by or activate) that Major Incident Stand Down has been declared
Health Coordinating Group will be convened via Local Area Team

APPENDIX 3
April 2015 Version: draft 1
Page |19 of 27
MAJOR INCIDENT INITIATION FORM TRIGGERS & DEFINITIONS
User: East and North Hertfordshire Clinical Commissioning Group On Call
Purpose: To assist on-call staff in the event of a major incident DECLARED or a STANDBY declared
If one or more of the follow applies, the incident requires a response from the East and North Hertfordshire Clinical Commissioning Group
• A major incident or emergency has been declared by another agency
• This is an internal incident that cannot be managed within normal resources • This is a significant incident that threatens to overwhelm the resources of more than one
NHS organisation
• This is a significant incident that requires coordination of more than one NHS organisation
• This is an incident where mutual aid is required (countywide or regional) • This is an incident that requires the attendance of the CCG at a Strategic Coordinating
Group
• This is a significant internal incident within another CCG organisation adversely affecting the daily running of the organisation and necessitating special arrangements to be instigated
• This is a significant incident that requires media coordination, particularly with partner organisations
• This is a significant incident requiring support from the CCG
• This is an incident affecting large numbers of people or having catastrophic effects on smaller numbers of individuals
Definitions
If one of the following definitions is met, the incident should be treated as a major incident:
Major Incident Any occurrence that presents a serious threat to the health of the community, disruption to the service or causes (or is likely to cause) such numbers or types of casualties as to require special arrangements to be implemented by hospitals, ambulance trusts or primary care organisations. Any event whose impact cannot be handled within routine service arrangements.
Serious Incident An incident (including Infections) where care management failures are suspected, which resulted in serious neglect, serious injury, major permanent harm or death (or the risk of) to a

APPENDIX 3
April 2015 Version: draft 1
Page |20 of 27
patient as a result of NHS funded health care; or An accident occurring on NHS premises that resulted in serious injury, major permanent harm or death (or the risk of) to a patient, member of staff, contractor or member of the public or any other person; or The actions of staff providing NHS funded care that are likely to cause significant public concern i.e. serious instances of abuse (physical/sexual/mental); or An event that might adversely impact on the delivery of services causing invocation of the Trusts business continuity plan, initiation of the major incident policy or may reflect a serious breach of standards.

APPENDIX 3
April 2015 Version: draft 1
Page |21 of 27
MAJOR INCIDENT INITIATION FORM TIME OF CALL:………………………………….. DATE:…………………………………………….
NAME OF CALLER:…………………………….. ORGANISATION:………………………………..
CCG Strategic Coordinating Group (GOLD): Time…………….. Venue…………… CCG Tactical Coordinating Group (SILVER): Time……………. Venue……………. CCG Coordinating Group: Time……………. Venue……………. Dial In………………………….
Actions Tick
Major incident Declared or standby?
Exact location of incident?
(E.g. Grid Reference, building, street, village, town, landmark, etc.)
Type of incident?
Flooding/Fire/Utility Failure/Disease outbreak/CBRN/Heat wave
Hazards
Present and potential? (e.g. fuel spillage, weather conditions, etc.)
APPENDIX 3
April 2015 Version: draft 1
Page |22 of 27
Access
(Best routes avoiding hazards for staff, evacuation routes, road blocks, etc.)
Number (of those involved)
Including: injured and uninjured, fatalities?
Emergency services
Partner orgs etc. required/on scene (Contact details)
Trust Intentions
Intentions/Actions required/requested to take
Support Support/Mutual Aid required (whom from?)
Additional Free Text: Additional Information/thoughts and requirements

APPENDIX 3
April 2015 Version: draft 1
Page |23 of 27
MAJOR INCIDENT Initial Emergency Incident Cascade
The Director of Operations is the Lead for Emergency Planning, within the CCG. As Senior Manager On Call for the East and North Hertfordshire Clinical Commissioning Group you may be asked to assist the Director in discharging their Emergency Planning Duties and to implement those of the CCG. You may be asked to ensure that the following key agencies are informed immediately of the incident (METHANE) information. Please state that you are the Senior Manager On Call for the East and North Hertfordshire CCG in Hertfordshire.
Notify Actions Agreed Tick Box
If notified by the Ambulance Trust (EEAST) confirm that they have contacted/notified the Acute Trusts directly
If NO contact/notify East & North Herts Trust on their On Call numbers (see contacts list)
NHS England Contact the Area Team On Call Manager to ensure they are aware of the situation and to agree actions required and cascade to NHS Trusts

APPENDIX 3
April 2015 Version: draft 1
Page |24 of 27
East and North Hertfordshire Clinical Commissioning Group Support provider organisations response and East and North Hertfordshire Clinical Commissioning Group East and North Hertfordshire CCG - they may be a need to notify Senior Managers to provide support to manage an incident. • Set up an Incident Management Team • Support provider organisations response to the situation
In all such incidents contact (see Contacts List for numbers):
- Chief Operating Officer - Other Directors as indicated - Emergency planning and communications leads
Other Senior Managers are available for support; see Contacts List for details.

APPENDIX 3
April 2015 Version: draft 1
Page |25 of 27
PUBLIC HEALTH ENGLAND (PHE) PHE should be notified of a Major Incident and/or for specific health information and advice. A representative may be present at the SCG or Health Coordinating Group (in person via telephone as required)
- Contact name and follow up number - Time and date of call - Role - Inform of incident and actions being taken - Request any support or action required (staff or resources) - Agree follow up action
HCT and HPFT: Community and Mental Health Services An HCT and HPFT representative, if appropriate, can attend the Health Coordinating Group teleconference as a liaison officer. HCT and HPFT should be notified of any Major Incident
- Contact name and follow up number - Time and date of call - Role - Inform of incident and actions being taken - Request any support or action required (staff or resources) - Agree follow up action

APPENDIX 3
April 2015 Version: draft 1
Page |26 of 27
NHS England: To be notified via the Area Team Major Incidents will be reported to Midlands and East On Call
111 call service & OOH Provider (Herts Urgent Care) The Senior Nurse/On Call should be notified of a major incident or emergency situation so they can expect increased calls/demand on service
LOCAL AUTHORITY (Emergency Planning) The Hertfordshire County Council Duty Emergency Planning Officer should be contacted to provide contact details, to establish liaison and mutual aid/support required

APPENDIX 3
April 2015 Version: draft 1
Page |27 of 27
Appendix 7 – EN CCG Major Incident Plan
2015-01-29 Major Incident Plan FINAL v
Appendix 8 – EN CCG Action Cards
Action Cards.docx

1 of 38
APPENDIX 4
SEVERE WEATHER RESPONSE PLAN
Author:
Sharn Elton, Director of Operations
Date of Implementation:
1st February 2015
Reviewed:
Version
Issue 1

2 of 38
APPENDIX 4
FREEDOM OF INFORMATION The contents of this plan are assumed to be accessible to the public and to staff, unless an exemption under the Freedom of Information Act 2000 has been identified during the drafting process.
Please indicate opposite any exemptions you are claiming.
Remember that some exemptions can be overridden if it is in the public interest to disclose – as decided by the FOI multi- disciplinary team.
Exemptions normally apply for a limited time and the information may be released once the exemption lapses.
This plan contains information;
Please insert an “x” if relevant
1. That is personal data
2. Provided in confidence
3. Intended for future publication
X
4. Related to criminal proceedings
5. That might prejudice law enforcement
6. That might prejudice ongoing external audit investigations
7. That could prejudice the conduct of public affairs
8. Information that could endanger an individual’s health & safety
9. That is subject to legal privilege
10. That is commercially confidential
11. That may not be disclosed by law
12. Other Please describe
Remember to destroy all unnecessary drafts and unneeded correspondence, once the final version of this plan is agreed.

3 of 38
APPENDIX 4
CONTENTS
FREEDOM OF INFORMATION ..................................................................................... 2 CONTENTS ................................................................................................................... 3 DISTRIBUTION .............................................................................................................. 5 GLOSSARY ................................................................................................................... 6 INTRODUCTION ........................................................................................................... 7 1. AIM ........................................................................................................................ 8 2. OBJECTIVES ........................................................................................................ 8 3. RISK ...................................................................................................................... 8 6. ALERTING AND ACTIVATION OF EMERGENCY RESPONSE ..........................14 8. ROLES AND RESPONSIBILITIES .......................................................................16 9. WARNING AND INFORMING ..............................................................................19 10. RECOVERY .........................................................................................................20 12. TRAINING ............................................................................................................20 13. EQUIPMENT ........................................................................................................20 14. HEALTH AND SAFETY ........................................................................................20 15. FINANCE ..............................................................................................................20 ANNEX A SEVERE WEATHER ALERT LEVELS AND RESPONSE ACTIONS ........21 ANNEX B WEATHER ACTIVITY TABLE FOR EMERGENCY RESPONDERS .........22 ANNED C WARNING AND INFORMING - CCG COMMUNICATIONS ACTION PLAN FOR SEVERE WEATHER …………………………………………………………………..27 ANNEX D PROVIDERS - LEVELS 0-4 ………………………………………………….39 ANNEX E KEY TRIGGER TEMPERATURES ………………………………………….40 ANNEX F ACTION CARDS PUBLIC HEALTH ENGLAND …………………………….41

4 of 38
APPENDIX 4
AMENDMENTS
AMENDMENT DATE OF ORIGINAL
AMENDED
CHANGE

5 of 38
APPENDIX 4
DISTRIBUTION
East and North Herts Trust Hertfordshire Urgent Care Health and Community Services Hertfordshire Partnership Foundation Trust Hertfordshire Community Services Hertfordshire County Council Hertfordshire Borough Council Hertfordshire Fire & Rescue NHS England - East Anglia Area Team Hertfordshire CCGs East of England Ambulance Service NHS Trust Environment Agency Public Health England - Anglia Public Health Team

6 of 38
APPENDIX 4
GLOSSARY
Abbreviation Description
ACS Hertfordshire County Council Adult and Community Services Di t t CCGs Clinical Commissioning Groups
CYP Hertfordshire County Council Children’s and Young People’s Di t t DCLG Department for Communities and Local Government
EPRR Emergency Preparedness, Resilience and Response
HA Highways Agency HWB Health and Wellbeing Boards
HWS Health and Wellbeing Strategy
LA Local Authority LHRP Local Health Resilience Partnership
MIU Minor Injuries Unit
NRC Network Response Centre
NSWWS National Severe Weather Warning Service
OGD Other Government Department
PHE Public Health England
RED Resilience and Emergencies Division, DCLG
The Cabinet Office has produced the Civil Protection Lexicon. This is a single point of reference for terminology used in UK civil protection. The lexicon provides a common, agreed set of definitions for terms used across the range of Integrated Emergency Management activities.

7 of 29
APPENDIX 4
INTRODUCTION This plan is the multi-agency response plan for severe weather events in Hertfordshire and provides outline information on the response, management and roles and responsibilities of individual agencies.
This plan was devised and written by Sharn Elton, Director of Operations.

8 of 29
APPENDIX 4
1. AIM The aim of this plan is to provide a multi-agency emergency response framework for all agencies responding to a severe weather event in Hertfordshire.
2. OBJECTIVES
a. Identify the risks and provide advice and information to communities and
individuals to enable them to be prepared for the effects of a severe weather event.
b. To provide a clear and concise procedure for the assessment of weather
warnings, together with a corresponding escalation procedure and plan activation process.
c. Agree specific roles, responsibilities and actions for all agencies involved in the
response to a severe weather event.
d. Identify key response issues that should be considered at both strategic and tactical levels in responding to a severe weather event.
e. Determine activities to reduce disruption to the communities, utilities,
businesses, and to protect the environment.
f. Lead recovery activity to support the recovery of communities and businesses. 3. RISK
a. Overview. The nature of Hertfordshire is such that in the past it has been subject to a wide variety of severe weather events. These have included heavy snowfall in 2003, 2009 and 2010 which caused widespread disruption, heat waves in 2003 and 2006 and damage caused by the high winds in 1987 and 1990. The county will continue to be susceptible to severe weather conditions which are likely to change as the effects of climate change will present new challenges or effects of greater consequences.

9 of 29
APPENDIX 4
b. Community Risk Register. A variety of severe weather risks have been rated as to their likelihood and potential effects on the county in the Hertfordshire Community Risk Register. http://m.hertsdirect.org/services/commsafe/commprotect/emeresilience/hertsrespartnership/
Risk Rating Hazard Description
HIGH
Low Temperatures and Heavy Snow
Snow falling and lying over most of the county for at least one week. After an initial fall of snow there is further snow fall on and off for at least 7 days. Most areas experience some falls in excess of 10cm, some drifts in excess of 30cm and a period of at least 7 consecutive days with daily mean temperature below -3ºC. There is likely to be some disruption to transport networks, businesses, power supply and water supply, and also school closures.
HIGH
Storms and Gales
Storm force winds affecting most of a county for at least 6 hours. Most areas experience mean speeds in excess of 55mph with gusts in excess of 85mph. Short term disruption to infrastructure including power, transport networks, homes and businesses.
HIGH
Heatwave
Daily maximum temperatures in excess of 32°C and minimum temperatures in excess of 15°C over most of a county for at least 5 consecutive days. There is likely to be disruption to power supply and transport infrastructure.
• Severe Weather and Climate Change. Climate change forecasts indicate that Hertfordshire is likely to experience:
• Blocked weather patterns leading to prolonged periods of similar, possibly
extreme, weather. • Greater winter rainfall leading to an increase in flooding. • Reduction in summer rainfall amounts. • Increases in summer rainfall intensities. • More severe storm events – windstorms and extreme rainstorms • Overall increases in annual mean temperatures. • Increases in the number of very hot days. • Increase in fire risk due to changes in biodiversity for upland areas.
The Recovery Plan will need to be flexible in its approach and be responsive to severe weather as the climate changes and adapt its plans in an appropriate manner.

10 of 29
APPENDIX 4
4. VULNERABLE PEOPLE
a. During a significant severe weather event anyone has the potential to become vulnerable due to the factors in disaster-related incidents. However, for a significant number of people the experience can be serious as it has the potential to remove them from established support mechanisms or expose particular vulnerabilities.
b. Vulnerable groups within the community will need special provision both in implementing any preparatory and precautionary measures for a potential severe weather event, and also in response to an incident. There are 3 categories of individuals that may fall into a ‘vulnerable group’:
• People who are generally independent, albeit with a structured support
environment, in their normal daily circumstances, i.e. residential health / social home, or similar circumstances, or;
• People who due to an event or situation, such as illness, operation or accident who are now dependent upon others to support and care for them to survive independently within the community or;
• People who through individual circumstances (age, disability, or language barriers) may require extra support and care to deal with the consequences of being involved in an emergency.
c. Separate plans and guidance are being devised to assist in the identification of vulnerable groups and individuals. These provide a flexible process for collating and sharing information between responders whilst maintaining confidentiality, and detail additional support measures or actions that may be required to assist these groups or individuals during an incident. Individuals from the following key groups are considered to be particularly at-risk in the event of severe weather event:
• Older people (over 75 years old). • People assessed as being at risk of, or having had, recurrent falls. • Elderly people who live alone and do not have additional social services
support people who are housebound or otherwise low mobility. • Frail elderly. • Children under the age of five or with disabilities. • Homeless or people sleeping rough. • People who have had operations – temporary. • People with pre-existing or long term serious medical conditions medical
conditions, especially those requiring medical support equipment or regular medication.
• People with long term mental health problems or learning difficulties that reduces individual’s ability to self-care (including dementia).
• Pregnant women and new-born children. • People living in isolated rural villages. • People living in deprived circumstances or who are fuel poor • Other marginalised groups

11 of 29
APPENDIX 4
5. WEATHER AND INFORMATION SERVICES
The trigger for the activation of this plan will be by notification to responder agencies from:
a. Met Office National Severe Weather Warning Service1. This service notifies agencies through the provision of warnings of severe or hazardous weather which can cause problems ranging from widespread disruption of communications to conditions resulting in transport difficulties or threat to life. The National Severe Weather Warning Service provides two levels of warning for the following types of weather conditions and these will be reinforced using the following icons:
• rain; • ice; • wind; • fog. • snow;
The two levels of warning are:
(i) Alerts: These are issued more than 24 hours ahead.
(ii) Warnings: These are issued up to 24 hours ahead.
Weather warnings will be assigned a colour indicating a combination of the level of impact and the likelihood of the severe weather. The colours will be assigned according to a matrix (Fig 1) to give each warning a colour:
Fig 1:
High Likelihood
Medium Likelihood
Low Likelihood
Very Low Likelihood
Very Low Impact
Low Impact
Medium Impact
High Impact
The tables on the Met Office website provide examples of the level of disruption which might be found at each of the impact levels and for each weather element (rain, snow etc.). Note weather assessed as having a “Very Low” impact may still have some minor impacts.
The basic messages associated with each of the colour states are:
1 http://www.metoffice.gov.uk/publicsector/nswws

12 of 29
APPENDIX 4
No Severe Weather
Be Aware
Be Prepared
Take Action
In addition, the Chief Forecaster’s assessment explains why the warning has been issued and the likely impacts as well as indicating where any uncertainties lie.
Further advice on any warnings issued can be obtained from the duty forecasters at the Met Office, or from the regional Public Weather Service (PWS) Advisor2. The PWS Advisor for the Eastern Region can provide more localised interpretation of forecasts. They can also be called upon to provide advice at multi-agency or Strategic Coordinating Group (SCG) meetings.
b. Hazard Manager3. Hazard Manager is a one-stop information source for the emergency response community. It is designed to supplement the role of the PWS Advisors in providing consistent weather-related information and interpretation of severe weather events. The services currently available on Hazard Manager are:
• Interactive Map Viewer with weather information. • Flood Guidance Statements. • Weather warnings. • Hazard Advice. • FireMet and CHEMET services.
c. Heat-Health Watch System.4 The Heat-Health Watch system is operated by the Met Office and the Department of Health from the 1st of June until the 15th of September each year. The Met Office issues weekly notifications by email during this period. All agencies ensure they are signed up to receive these notifications and will act in accordance with the activity levels shown in Annex B. The Met Office may forecast a heatwave where regional trigger threshold temperatures are met or exceeded. The system operates with five levels – Blue, Green, Yellow, Amber and Red – full details can be found in Annex A of this plan. The JEPU and Hertfordshire Clinical Commissioning Groups (CCGs) receive email forecasts / alerts from the Met Office along similar lines of warnings received through the National Severe Weather Warning Service (NSWWS).
d. Cold Watch System. A Cold Watch system will operate from 1st November to 31st March each year. During this period, the Met Office may forecast extreme winter weather, as defined by forecasts of temperatures, snow and ice formation and their duration. There will be consultation between the Met Office and the Department of Health to raise alerts at appropriate level in view of the weather forecasts and their likely impacts. There are five levels of alert – 0 to 4 – full details can be found in Annex A of this plan.
2 http://www.metoffice.gov.uk/publicsector/PWSA 3 http://www.metoffice.gov.uk/publicsector/hazardmanager/access - please note: this service is not publicly available 4 http://www.metoffice.gov.uk/weather/uk/heathealth

13 of 29
APPENDIX 4
e. Highways. Hertfordshire County Council receives daily forecasts from which service decisions are made by the HCC Winter Service – Senior Decision Maker. When severe weather is predicted or in place, then direct contact can be made with the forecasters to discuss and plan accordingly. f. Highways Agency. A Highways Agency Winter Service is operated from the 1st
October to the 31st April each year. A daily road weather forecast enables winter decisions to be made. The Highways Agency Emergency Planning Team also has access to the Met Office weather updates from embedded forecasters at their National Traffic Control Centre.
g. Other Means of Notification. Any Hertfordshire Category 1 or 2 Responder can use the Hertfordshire Alerting Directory to initiate the generation of all or part of the Hertfordshire crisis management structure, in response to a severe weather warning. Notification may also be made to activate the plan due to the consequential issues that have arisen due to a severe weather event. Information may also be provided by members of the public contacting individual emergency services or other Hertfordshire partners in response to specific severe weather related events.

14 of 29
APPENDIX 4
Individual agencies conduct Risk Assessment
(Consider range of factors - other prevailing conditions, recent weather
conditions)
6. ALERTING AND ACTIVATION OF EMERGENCY RESPONSE
Receive NSWWS Alert / Warning
Met Off PWS Advisor email Intelligence from Cat 1/2 responder
Monitor Situation
Multi-agency No Teleconference
required?
Yes
Insufficient resources for single
No agency response? Coordinated
activity required?
Yes
Establish TCG and / or SCG,
as appropriate
Implement Multi-agency
Response

15 of 29
APPENDIX 4
7. GENERIC CONCEPT OF EMERGENCY RESPONSE TO AN SEVERE WEATHER EVENT
Emergency Management
The process of declaring a Multi-agency or Major Incident will follow procedures laid down in the Hertfordshire Generic Response and Recovery Plan. The management of severe weather events is split into 4 levels; these mirror the alert levels for the specific response plans:
a. Level 0 – Long-term planning
- Identify Emergency Services and other multi-agency partners likely to be affected by severe weather event.
- Review plans, contingency arrangements and responsibilities in the pre- seasonal period.
b. Level 2 – Prevention
- At start of appropriate severe weather season, review public information and advice.
- Issue general preparation messages to public and multi-agency partners.
c. Level 3 – Response
- On receipt of specific severe weather warnings, Emergency Managers conduct risk assessments and either monitor situation or: - Implement response plan activities. - Issue messages to public and other multi-agency partners.
d. Level 4 – Emergency Response
- As appropriate, implement multi-agency coordination or Major Incident command and control when services are being severely affected (power failure, major transport disruption, etc.).
The multi-agency action plan for severe weather events is at Annex B. Further details on specific agency response actions are included in individual organisation’s response plans.

16 of 29
APPENDIX 4
8. ROLES AND RESPONSIBILITIES The following roles and responsibilities are more specifically envisaged in a Hertfordshire response to a severe weather event:
Hertfordshire Resilience Forum (HRF):
• Monitor the situation for significant weather changes or new warnings being
issued; • Consider declaration of Multi-Agency Incident or Major Incident, as appropriate • Identify requirements for any cross-agency staff or resources from Multi-Agency
partners; • Provision of coordinated public warnings and advice in response to hazardous
situations. DCLG RED:
• Support the co-ordination of the response where the emergency crosses a number of counties within the region and brokerage of mutual aid across the region and between regions;
• Co-ordinate regional response activity with national response activity including coordination of resource requests.
East of England Ambulance Service NHS Trust (EEAST):
• Identify, in conjunction with partners, those persons who will require evacuation or special care measures from the ‘At Risk Register’;
• Coordinate the use of the voluntary and private sector in health emergency response.
Environment Agency (EA):
• Prevent/control and monitor the input of pollutants to the environment; • Provide advice and technical support to other partners on the disposal of waste; • Provide advice and technical support to partners on the environmental issues; • Monitor water resource situation and put in place appropriate measures if
required. Hertfordshire Constabulary:
• Lead and co-ordinate the evacuation of a given area if considered appropriate; • Traffic management, assisted by Highways Agency and Hertfordshire
Highways, as appropriate; • Closure of roads as appropriate; • Control of movement in areas where hazards are present.
Hertfordshire Fire and Rescue Service:
• In conjunction with other agencies, assist with rescue operations.

17 of 29
APPENDIX 4
Hertfordshire Local Authorities:
Hertfordshire County Council: • Disseminate warning messages to social care and voluntary providers; • Provide business continuity advice to businesses and voluntary
organisations to enable them to mitigate the effects of severe weather; • Provision of emergency transport if required; • Provide specialist advice on the safety of roads/bridges; • Social care support for vulnerable or displaced people; • Assist traffic management through provision of highways support - roads &
signs, road clearance; • Treatment of roads to clear snow and ice; • Mitigation of any environmental hazards (e.g. Closure of countryside parks or
Rights of Way); • Management of environmental, food and water safety, pollution issues; • Liaison and coordination of support to and from community resilience groups.
District / Borough:
• Provision of emergency welfare for people, pets and livestock who become unavoidably detained and stranded;
• Provision of temporary emergency accommodation; • Liaise with Town/Parish councils resilience groups; • Provision of emergency transport (IBC only); • Monitor/repair coastal protection structures; • Local management of environmental, food and water safety, pollution issues; • Confirm building structural safety and suitability for human occupation; • Assist in the clearance of debris; • Coordinate and provide advice on waste disposal and collection.
Public Health England and Director of Public Health:
• Provide clear and unambiguous advice on the health implications of a severe weather event;
• Provide health guidance and advice where necessary directly Hertfordshire Clinical Commissioning Groups (CCGs):
• The CCG is responsible for leading the system and co-ordinating the health system response. At the declaration of alert level 3 (p15) the CCG must take the lead in ensuring that key providers and partners have taken appropriate action, including:
• Conducting risk assessments • Implementing response plans and ensuring message to the public and other
multi agency partners, as required • Co-ordinating and leading the system response
Highways Agency:
• Provide temporary traffic management at any incident in support of the Police; • Set strategic and tactical Vehicle Management Signs to support road closures; • Provision of timely advice to the public on route availability and any diversion routes; • Restore the highway to operational use, by snow clearance, treatment of the road /
making the surface safe, removal of debris as a result of the conditions or incidents.

18 of 29
APPENDIX 4
Military:
• Provision of specialist advice and support, as available under the Military Aid to the
Civil Authorities (MACA) arrangements. Utilities:
Major utilities such as National Grid (Gas) and National Grid (Electricity), UK Power Networks, Anglian Water, Essex & Hertfordshire Water, British Telecom have their own contingency plans, which would be activated as required. Companies will be required to liaise closely with emergency services and local authorities during the response and recovery phase, including linking in with Hertfordshire crisis management structures.
Voluntary Sector:
• The numerous voluntary organisations, nationally, regionally and in Hertfordshire,
have the potential to provide additional capacity and specialist capability for any incident response or during the recovery phase;
• Responsibility for coordinating the response of voluntary groups is likely to rest with the Local Authority, through Hertfordshire Voluntary Organisations Group (HVOG).
Community Resilience
A number of Parish, Town Councils and other community groups, have developed Community Emergency Plans for their areas. The County Council and District Council Community Teams will liaise with and coordinate Community Emergency Teams to enable a coordinated and supported response of communities with the Emergency Services.

19 of 29
APPENDIX 4
9. WARNING AND INFORMING
a. Warning and Informing the Public
One of the key aspects of any preparation and response to a severe weather event is the timely dissemination of accurate information, advice and warnings to the public. As severe weather tends to be seasonal, advice and preparatory information will be circulated as part of a coordinated strategy, linked to the 4 preparedness and response levels. This strategy is aimed at raising awareness and escalating from advice to warnings on notification of specific severe weather. Hertfordshire District Council will lead on the planning and development of generic media advice in respect of warning / information. This will consider key messages (normally no more than 4), who the information is targeted at, what methods should be used for dissemination and what detailed information should be given (supplied by emergency planners). These messages should be pre-prepared and reviewed at Level 1 and available for release from Level 2 onwards in the appropriate annexes to this plan.
General advice to the public on preparing for and action to take in the event of severe weather is available from a number of sources listed below:
- Hertfordshire Resilience - general severe weather preparation information -http://m.hertsdirect.org/services/commsafe/commprotect/emeresilience/hertsrespartnership/
- Hertfordshire Community Emergency Preparedness - advice and information -http://m.hertsdirect.org/importantnews/
- The Met Office website - general severe weather preparation information - Met Office: What to do in severe weather.
- Department of Health, Public Health England websites – provide health-related information, guidance and advice.
- Department for Education - provide advice to educational establishments on preparation for severe weather.
- The Highways Agency provides information on routes and travel disruptions on their website Traffic England. UK wide travel information is available from Transport Direct.
- AA Roadwatch will also be used to broadcast warnings - http://www.theaa.com/travelwatch/travel_news.jsp.
- Regional or national television may broadcast weather warning information during major events.
- Local radio stations.
An outline of the likely advice, information and warnings that will be issued by the CCG communication team - Annex C.
b. Media
The media interest in any significant severe weather event, based upon historical evidence, is likely to be very high. The management of the Hertfordshire media response will be guided by Hertfordshire County Council

20 of 29
APPENDIX 4
10. RECOVERY
At, or shortly after the declaration of a Multi-Agency or Major Incident, the County Council will convene a Recovery Working Group (RWG) to prepare for the management of the post response activity aimed at restoring and rebuilding affected communities in the aftermath of a major severe weather event.
12. TRAINING Any additional staff brought in to augment Hertfordshire responders may require to be trained and equipped to complete assigned tasks. Training of responders will take place either by individual agencies or multi-agency to ensure people can conduct the required response role and operate collectively.
13. EQUIPMENT Procurement of equipment and supplies during an emergency response should wherever possible follow existing agency procedures. However, the multi-agency County Council Logistics Cell may co-ordinate the procurement and distribution of additional or specialist emergency supplies during a major incident
14. HEALTH AND SAFETY All organisations referred to in this plan will have relevant risk assessments in place to carry out their organisation’s responsibilities.
15. FINANCE Initially the provision of support to an emergency response is provided at the cost to the providing organisation. Where costs are significant, applications can be submitted by local authorities via the Bellwin Scheme which provides details on who is eligible for financial support
Annexes
Annex A – Severe Weather Alert Levels and Response Actions.
Annex B - Weather Activity Table for Emergency Responders
Annex C - Warning and Informing – CCG Communications Action Plan for Severe Weather Annex D – Health and social care staff in all settings (community, hospitals and care homes) Annex E – Key Trigger Temperatures Annex F – Action Cards from Public Health England

21 of 29
APPENDIX 4
ANNEX A SEVERE WEATHER ALERT LEVELS AND RESPONSE ACTIONS 1. HEATWAVE
The Heat-Health Watch system operates from 1 June to 15 September each year. The Met Office uses this system to trigger heatwave warnings where the regional threshold temperatures are met or exceeded. The average threshold temperatures for this region are:
• Day time temperature of 30°C or more. • Night time minimum threshold temperature of 15°C or more.
Level 0 Long-term planning All year
Level 1 Heatwave and Summer preparedness programme 1 June – 15 September
Level 2 Heatwave is forecast – Alert and readiness 60% risk of heatwave in the next 2–3 days
Level 3
Heatwave Action Temperature reached in one or more Met Office National Severe Weather Warning Service regions
Level 4
Major incident – Emergency response Central Government will declare a Level 4 alert in the event of severe or prolonged heatwave affecting sectors other than health
2. COLD WATCH
A Cold Watch system will operate in England and Wales from 1st November to 31st March each year. During this period, the Met Office consults with the Department of Health, the Cabinet Office and other experts to raise alerts at appropriate level in response to the weather forecasts and their likely impacts.
Level 0 Long-term planning All year
Level 1 Winter preparedness and action programme 1 November to 31 March
Level 2
Severe winter weather is forecast – Alert and readiness Mean temperature of 2°C and/or widespread ice and heavy snow are predicted within 48 hours, with 60% confidence.
Level 3
Response to severe winter weather – Severe weather action Severe winter weather is now occurring: mean temperature of 2°C or less and/or widespread ice and heavy snow.
Level 4
Major incident – Emergency response Central Government will declare a Level 4 alert in the event of severe or prolonged cold weather affecting sectors other than health

22 of 29
APPENDIX 4
ANNEX B WEATHER ACTIVITY TABLE FOR EMERGENCY RESPONDERS
Activity Level Level 0 Level 1 Level 2 Level 3 Level 4
Generic activity levels for ALL SEVERE WEATHER for emergency responder organisations
LONG TERM PLANNING
All year
PREPAREDNESS
ALERT AND READINESS
ACTION
MAJOR INCIDENT - EMERGENCY RESPONSE
Warning and Informing activity
Develop communications strategies to encourage resilience and preparedness.
Prepare core messages to be broadcast alongside national, PHE messages aligned to warnings and weather forecasts.
Appropriate agencies register to receive weekly Heat-Health Watch and Cold Weather Plan notifications and alerts.
Consider issue of general media messages.
Post advice links on agency’s websites.
Appropriate agencies receive weekly Heat- Health Watch and Cold Weather Plan notifications and alerts
Issue media messages – especially ‘hard to reach groups’.
Agencies to receive Met Office weekly notifications
Update Community Resilience partners and encourage review of community emergency plans.
Agencies to receive Met Office weekly notifications
Update Community Resilience partners and ask them to activate their community emergency plans
Specific activity levels associated with Heatwave
All Agencies
Make environmental improvements to provide a safe environment for clients in the event of a heatwave.
Prepare business continuity plans to cover the event of a heatwave (e.g. storage of medicines, computer resilience, etc.).
Work with partners and staff to raise awareness of the impacts of severe heat and on risk reduction awareness
All Agencies
Coordinate individual agency heatwave contingency plans & business continuity arrangements.
Liaise with partners on joint preparedness arrangements.
Circulate National heatwave guidance and advice – schools, care settings, prisons, and voluntary organisations.
All Agencies
Liaise and confirm status of heatwave response, logistics and monitoring mechanisms (Cat 2 responders as appropriate).
Communicate alerts to staff and make sure that they are aware of heatwave plans
Increase advice to health and social care workers working in community, care homes and hospitals
All Agencies
Convene Hertfordshire teleconference to identify particular heatwave related issues and potential mitigation strategies (NHS lead).
Review safety of public events.
Issue warning information and media alerts.
NHS & Local Authority (ACS & CYP)
Continue to distribute DH advice / guidance to…
All Agencies
Convene TCG/SCG to coordinate implementation of mitigation measures and national guidance (NHS lead).
Update warnings, information and media alerts.
NHS & Local Authority
Coordinate the implementation of DH advice / guidance
…cont…

23 of 29
APPENDIX 4
Activity Level Level 0 Level 1 Level 2 Level 3 Level 4
Hertfordshire District Council
Engaging the community & voluntary sector to support development of local community emergency plans
Encourage development of community emergency plans to identify and support vulnerable neighbours.
PHE / NHS England
Issue general advice to the public and professionals.
Health / Care providers
Identify high risk individuals and monitor care settings.
PHE / NHS England
Provide guidance to professional partners and advice to Public.
Routinely monitor syndromic and mortality surveillance
Health / Care providers
Communicate alerts to staff
Implement heatwave measures and arrangements to monitor those identified at high risk.
PHE / NHS England
Issue Level 2 alert to professional partners and advice to Public.
Continue to monitor syndromic and mortality surveillance
people at risk, residential care managers and carers.
Commission additional care and support, involving at least daily contact, as necessary for at risk individuals living at home. This may involve informal carers, volunteers and care workers.
Continue to distribute guidance to head teachers.
guidance to residential care managers, carers and head teachers.
Specific activity levels associated with WIND
All Agencies
Encourage development of community emergency plans to identify and support vulnerable neighbours.
All Agencies
Confirm individual agency contingency & business continuity plans.
Cat 1 and 2 agencies liaise on joint preparedness arrangements.
Review pre-prepared general information and guidance.
All Agencies
Cat 1 EP practitioners liaise and confirm status of response, logistics and monitoring mechanisms (Cat 2 responders as appropriate).
Identify public events likely to be affected.
Issue public information advice and guidance.
All Agencies
Convene Hertfordshire teleconference to identify particular issues and potential mitigation strategies (LA lead).
Review safety of public events.
Issue warning information and media alerts.
Police, LA & HA
Manage disruption to transport infrastructure
All Agencies
Convene TCG / SCG to coordinate implementation of mitigation measures and national guidance (LA lead).
Update warnings, information and media alerts.
LA & HA
Coordinate and prioritise route maintenance operations.

24 of 29
APPENDIX 4
Activity Level Level 0 Level 1 Level 2 Level 3 Level 4
Specific activity levels associated with RAIN
All Agencies
Business as usual
Activity as per WIND (above).
All Agencies
Business as usual
Activity as per WIND (above).
All Agencies5
Convene Hertfordshire Flood Advisory Telecon to identify particular issues and potential mitigation strategies (LA lead).
Inform partners of identified risk area(s).
Consider establishing TCG / SCG
Consider implementing Operational Flood Plan actions.
Review supporting Emergency Plans.
Consider mobilisations of resources – personnel, plant, flood protection, voluntary organisations
Consider / Implement activation of evacuation plans and arrange for rest centres to be set up.
All Agencies10
Convene Hertfordshire
TCG / SCG to coordinate implementation of mitigation measures and national guidance (LA lead).
Identify risk / effected areas.
Consider wider flood risks and refer to the Hertfordshire Flood Plan Activate Operational Flood Plan actions.
Consider / Implement activation of evacuation plans and arrange for rest centres to be set up.
5 Medium and High activity as detailed in the HERTFORDSHIRE Flood Plan v.5

25 of 29
APPENDIX 4
Activity Level Level 0 Level 1 Level 2 Level 3 Level 4
Specific activity levels associated with SNOW & ICE
All Agencies
Review actions and guidance from PHE Cold Weather Plan.
Work with partner agencies to ensure that cold weather planning features within wider winter resilience planning.
Work with partners and staff on risk reduction awareness (e.g. flu vaccinations, signposting for winter warmth initiatives.
Encourage development of community emergency plans to identify and support vulnerable neighbours.
Engage with local statutory partners to agree how voluntary organisations can contribute to local community resilience arrangements.
PHE and NHS England
Issue general advice to the public and professionals and work closely with other government departments
All Agencies
Confirm individual agency winter contingency & business continuity plans.
Cat 1 and 2 agencies liaise on joint preparedness arrangements.
Identify categories of vulnerable individuals & groups.
Review pre-prepared general information and guidance.
LA in consultation with HA
Review winter service plans (Snow clearance and gritting) strategy.
NHS & Local Authority
Identify measures to reduce effects of cold on at risk groups - vulnerable adults and young people.
All Agencies
Cat 1 EP practitioners liaise and confirm status of winter response, logistics and monitoring mechanisms (Cat 2 responders as appropriate).
Identify public events likely to be affected.
Issue public information advice and guidance.
NHS & Local Authority
Distribution of DH & DfE guidance to residential care managers and carers, schools, Sure Start centres and children’s nurseries.
LA
Deliver winter service plan, which includes actions for severe weather situation.
All Agencies
Convene Hertfordshire teleconference to identify particular snow-related issues and potential mitigation strategies (LA or NHS lead).
Review safety of public events.
Issue warning information and media alerts.
NHS & Local Authority
Continue to distribute DH & DfE guidance and advice.
Identify and provide any specific support requirements for at risk individuals or groups.
LA and HCC
Implement snow clearance and gritting contingency plans.
Police and HCC
Manage disruption to transport infrastructure.
Coordinate route information.
All Agencies
Convene TCG / SCG to coordinate implementation of mitigation measures and national guidance (LA lead).
Update warnings, information and media alerts.
NHS & Local Authority
Liaise on implementation of DH advice / guidance.
Continue distribution of guidance to residential care managers, carers and head teachers.
LA & HCS
Establish severe weather desk to manage and coordinate winter service activities.

26 of 29
APPENDIX 4
Activity Level Level 0 Level 1 Level 2 Level 3 Level 4 and other national
organisations that produce winter warmth advice.
Specific activity levels associated with FOG
All Agencies
Business as usual
Activity as per WIND (above).
All Agencies
Business as usual
Activity as per WIND (above).
All Agencies
Consider media messages
Police and HA
Manage transport disruptions
Activate matrix signs
All Agencies
N/A

27 of 29
APPENDIX 4
ANNEX C - WARNING AND INFORMING CCG communications action plan for severe weather CCG communications action plan for severe weather
Introduction
In anticipation of, and in the event of severe weather (either heat or cold) the CCG communications team will work collaboratively with communications leads from partner and provider organisations to ‘warn and inform’ the public, health professionals, staff and provider organisations. This is to ensure that anyone at risk and the organisations that care for them have the information they need to mitigate against weather-related health conditions, thereby safeguarding their own health and reducing the strain on NHS services.
The level and nature of severe weather communications activity is dictated by the nationally-agreed actions linked to the Met Office’s ‘watch alert’ system, which links communications actions to day and night-time temperatures and the duration of those temperatures. Met Office alerts are received by the communications team through the CCG’s ‘enquiries’ email inbox.
Who does what?
The Director of Public Health (based at Hertfordshire County Council) is responsible for population health outcomes, supported by Public Health England (PHE), which provides national leadership and expert services to support public health. East and North Hertfordshire CCG chairs regular county-wide communications meetings and collaborative working on shared objectives is already well-established. In the event of severe weather, the CCG will work closely with our partner organisations and providers, adhering to national communications guidance from Public Health England to ensure that all communications:
• follow public health advice consistently • are targeted to the health needs of specific groups of the population • are disseminated effectively and in a timely manner to their intended audiences.
CCG communications responsibilities
Specific communications responsibilities for CCGs in the event of severe weather have been outlined by Public Health England, NHS England and the Department of Health. East and North Hertfordshire CCG is responsible for:
1. Alerting and informing the public of the possible impacts of severe weather with accurate and timely information
2. Working with local partner agencies to undertake the actions prescribed in the action plans on pages 5-8 in response to weather alerts
3. Working with providers to keep all those involved informed of progress on the local response to the effects of severe weather
4. Communicating with CCG staff to activate/deactivate business continuity arrangements.
1. Alerting and informing the public: It falls within the CCG’s remit to communicate health messages1 directly to the public and to Hertfordshire County Council to manage the media response2 . By working together, the
1 according to Public Health England Action Card for Commissioners (health and social care) and local authorities 2 P19 ENH CCG Severe Weather Response Plan

28 of 29
APPENDIX 4
CCG can assist Hertfordshire County Council by providing clinical evidence and information to strengthen the council’s media output, i.e. by providing GP quotes and statistics. The resulting media coverage will in turn support the CCG to reach a large audience with public health messages. Other communications channels that the CCG will employ to alert and inform the public include: the organisation’s website, the New QEII Hospital website, information screens in GP surgeries, social media posts on Facebook and Twitter linked to health advice, our wide and established stakeholder contact group.
2. Working with local partner agencies and authorities: the CCG communications team plays an active part in fostering mutually beneficial relationships between local partner agencies and authorities. During severe weather, this joint working would step-up to enable the CCG to meet the challenge of the actions outlined in the action plan on pages 5-8. This could include daily communications teleconference calls, attendance at local health resilience forum events and the setting up of inter-agency staff briefings.
3. Working with providers: The CCG communications team will communicate to providers the risks to their patients associated with severe weather and will remind them to implement their own action plans in alignment with MET Office alerts. Correspondence should be emailed to CCG commissioned services such as: planned hospital care, rehabilitative care, urgent and emergency care, community health services, mental health and learning disability services. In addition, the CCG is now jointly or ‘co-commissioning’ primary care services in conjunction with NHS England and has close working relationships with its 60 member GP practices. There are established communications channels between the CCG and member practices, through which the CCG can pass on advice and support about planning and coping with severe weather. The CCG communications team is specifically responsible for the regular GP bulletin and also has access to email addresses for every practice manager.
4. Communicating with CCG staff It is essential that staff receive regular communications during severe weather. This is so that they can protect their own health and that of their families and also so that they can be kept informed of any business continuity arrangements that have been put into place. A variety of communications channels can be employed for these purposes:
• email – staff can be communicated with via the CCG-wide distribution list in normal working hours. A ‘read receipt’ option may be a useful consideration to confirm that messages have been received
• via a telephone cascade system through directorates and teams • through an update posted on the CCG intranet, which staff can log into from home (providing
they have created a login in advance)

29 of 29
APPENDIX 4
Specific considerations in the event of a heatwave In contrast to deaths associated with cold snaps in winter, the rise in mortality as a result of very hot weather follows very sharply – within one or two days of the temperature rising.3 This means that by the time a heatwave starts, the window of opportunity for effective communications action is very short indeed. Advanced planning and preparedness is essential. Public Health England has agreed the key messages below, which can be issued as necessary: Key public health messages4 Stay out of the heat:
• keep out of the sun between 11am and 3pm • if you have to go out in the heat, walk in the shade, apply sunscreen and wear a hat and light
scarf • avoid extreme physical exertion • wear light, loose-fitting cotton clothes
Cool yourself down:
• have plenty of cold drinks, and avoid excess alcohol, caffeine and hot drinks • eat cold foods, particularly salads and fruit with a high water content • take a cool shower, bath or body wash • sprinkle water over the skin or clothing, or keep a damp cloth on the back of your neck
Keep your environment cool:
• keeping your living space cool is especially important for infants, the elderly or those with chronic health conditions or who can’t look after themselves
• place a thermometer in your main living room and bedroom to check temperatures • keep windows that are exposed to the sun closed during the day, and open windows at night
when the temperature has dropped • close curtains that receive morning or afternoon sun, however, care should be taken with
metal blinds and dark curtains, as these can absorb heat – consider replacing or putting reflective material in-between them and the window space
• turn off non-essential lights and electrical equipment – they generate heat • keep indoor plants and bowls of water in the house as evaporation helps cool the air • if possible, move into a cooler room, especially for sleeping • electric fans may provide some relief, if temperatures are below 35°C
Look out for others:
• keep an eye on isolated, elderly, ill or very young people and make sure they are able to keep cool
• ensure that babies, children or elderly people are not left alone in stationary cars • check on elderly or sick neighbours, family or friends every day during a heatwave • be alert and call a doctor or social services if someone is unwell or further help is needed
If you have a health problem:
• keep medicines below 25 °C or in the refrigerator (read packaging instructions) • seek medical advice if you are suffering from a chronic medical condition or taking multiple
medications If you or others feel unwell:
• try to get help if you feel dizzy, weak, anxious or have intense thirst and headache; • move to a cool place as soon as possible and measure your body temperature
3 PHE Heatwave plan for England – Chapter 1 – Why this plan is needed 4 From 3.2 box 1 key public health messages – PHE Heatwave Plan for England 2015

30 of 29
APPENDIX 4
• drink some water or fruit juice to rehydrate • rest immediately in a cool place if you have painful muscular spasms (particularly in the legs,
arms or abdomen, in many cases after sustained exercise during very hot weather), and drink oral rehydration solutions containing electrolytes. Medical attention is needed if heat cramps last more than one hour
• consult your doctor if you feel unusual symptoms or if symptoms persist
Heat health advice during Ramadan Many members of the Muslim community may fast during the daylight hours in the month of Ramadan. All local areas should familiarise themselves with the dates of Ramadan each year and build appropriate actions into their local plans if it falls during the summer months. Suggested Public Health England quote for Ramadan: “It is common to have one meal just before sunrise and an evening meal after sunset during Ramadan. During hot weather, dehydration is a common and serious risk. It’s important to balance food and fluid intake between fasts and especially to drink enough water. If you start to feel unwell, disoriented or confused, or collapse or faint, advice is to stop fasting and have a drink of water or other fluid. This is especially important for older adults, those with poorly controlled medical conditions such as low/high blood pressure, diabetes and those who are receiving dialysis treatment. The Muslim Council of Britain has confirmed that breaking fast in such conditions is allowable under Islamic law. “Also, make sure to check on others in the community who may be at greater risk and keep an eye on children to ensure they are having a safe and healthy Ramadan. Guidance has been produced to help ensure that members of the Muslim community have a safe and healthy Ramadan – Ramadan Health Guide: A guide to healthy fasting produced in association with the NHS with further information available on NHS Choices – Healthy Ramadan.” Public health suggested quotes These official PHE warnings will provide the framework for locally transmitted messages. They can be modified with quotes from CCG clinical leads5: Alert Level 1 No warning is required unless there is a 60 per cent probability of the situation reaching level 2 somewhere in the UK within the next three days, then: “If this does turn out to be a heatwave, we will try to give you as much warning as possible. But in the meantime, if you are worried about what to do, either for yourself or somebody you know who you think might be at risk, for advice go to NHS Choices or ring NHS 111”.
Alert level 2 “Heatwaves can be dangerous, especially for the very young or very old or those with chronic disease. Advice on how to reduce the risk either for yourself or somebody you know can be obtained from NHS Choices, ring NHS 111, or visit your local chemist”. Alert level 3 and 4 “Stay out of the sun. Keep your home as cool as possible – shading windows and shutting them during the day may help. Open them when it is cooler at night. Keep drinking fluids. If there is anybody you know, for example an older person living on their own, who might be at special risk, make sure they know what to do.”
The action plans below show the required communications actions for the CCG, in alignment with Public Health England plans for heatwaves and cold severe weather.
5 Public health core messages. Annex 2 PHE Heatwave plan for England

31 of 29
APPENDIX 4
CCG communications heatwave action plan Actions taken from CCG severe weather plan (Annexe B) and PHE Heatwave plan (Figure 3.1 commissioners and local authority).
Activity Level Level 0 Level 1 Level 2 Level 3 Level 4 Specific activity levels associated with heatwave
Long Term Planning all year
Preparedness Alert and Readiness Action Major Incident – Emergency Response
Messages to service users and public
Develop communications strategies to encourage resilience and preparedness. Prepare core messages to be broadcast alongside national, PHE messages aligned to warnings and weather forecasts
Issue media messages in alignment with national messages from PHE
Issue media messages – especially with ‘hard to reach’ vulnerable groups.
Issue warning information and media alerts in alignment with national messages from PHE Media alerts about keeping cool
National Emergency Continue actions as per level 3 unless advised to the contrary
Communications with staff
Ensure business continuity plans cover the event of a heatwave and how they will be communicated to staff and how it may affect them
Communicate alerts to staff and make sure that they are aware of heatwave plans Implement business continuity
Business continuity in place
Continue actions as per level 3 unless advised to the contrary Business continuity in place
Communications with providers
Share information over the importance of heatwave preparation.
Work with partner agencies, providers and businesses to coordinate heatwave plans, ensuring vulnerable and marginalised groups are appropriately supported
Remind providers to: provide cool areas and monitor indoor temperatures to reduce the risk of heat-related illness and death in the most vulnerable populations
Ensure that key providers and partners have taken appropriate action including: conducting risk assessments.
Continue actions as per level 3 unless advised to the contrary

32 of 29
APPENDIX 4
Remind providers to: identify or create cool rooms/areas (able to be maintained below 26 °C) install thermometers where vulnerable individuals spend substantial time
Review and prioritise high risk people Ensure sufficient cold water and ice
Communications coordination with local agencies and authorities
Ensure that a local, joined-up programme is in place between partner communications teams
Liaise with partners on joint preparedness arrangements
Liaise with partners and communicate public media messages – especially to ‘hard to reach’ vulnerable groups
Convene Hertfordshire communications leads teleconference to coordinate joined up communications response. (NHS lead).
Continue actions as per level 3 unless advised to the contrary

33 of 29
APPENDIX 4
CCG communications action plan for cold weather Actions taken from PHE action cards for commissioners and local authorities.
Activity Level Level 0 Level 1 Level 2 Level 3 Level 4 Specific activity levels associated with cold weather
Long Term Planning all year
Preparedness Alert and Readiness Action Major Incident – Emergency Response
Messages to service users and public
Communicate public health media messages
Continue to communicate public health media messages
Continue to communicate public health media messages
Continue actions as per level 3 unless advised to the contrary
Messages to CCG staff
Work with partners and staff on risk reduction awareness (e.g. flu vaccination for staff in September/October), information and education
Review the distribution of the cold weather alerts across the system and ensure staff are aware of winter plans and advice
Communicate alerts to staff and make sure that they can take appropriate actions Activate business continuity arrangements and emergency plans as required
Communicate alerts to staff and make sure that winter plans are in operation
Continue actions as per level 3 unless advised to the contrary
Messages to providers
Ensure key partners, including all managers of care, residential and nursing homes are aware of the alert system and can access advice
Ensure key partners are undertaking action in response to alerts Ensure continuity arrangements are working with provider organisations
Continue actions as per level 3 unless advised to the contrary
Comms coordination with local agencies and authorities
Work with local organisations to coordinate locally appropriate cold weather plans in accordance with the local and national Cold
Support local community organisations to mobilise community emergency plans Work with partner
Continue actions as per level 3 unless advised to the contrary

34 of 29
APPENDIX 4
Weather Plan
agencies (e.g. transport) to ensure road and pavement gritting arrangements are in effect to allow access to critical services and high-use pedestrian areas

APPENDIX 4
CCG communications heatwave action plan Actions taken from CCG severe weather plan (Annexe B) and PHE Heatwave plan (Figure 3.1 commissioners and local authority). Activity Level Level 0 Level 1 Level 2 Level 3 Level 4 Specific activity levels associated with heatwave
Long Term Planning all year
Preparedness Alert and Readiness Action Major Incident – Emergency Response
Messages to service users and public
Develop communications strategies to encourage resilience and preparedness. Prepare core messages to be broadcast alongside national, PHE messages aligned to warnings and weather forecasts
Issue media messages in alignment with national messages from PHE
Issue media messages – especially with ‘hard to reach’ vulnerable groups.
Issue warning information and media alerts in alignment with national messages from PHE Media alerts about keeping cool
National Emergency Continue actions as per level 3 unless advised to the contrary
Communications with staff
Ensure business continuity plans cover the event of a heatwave and how they will be communicated to staff and how it may affect them
Communicate alerts to staff and make sure that they are aware of heatwave plans Implement business continuity
Business continuity in place
Continue actions as per level 3 unless advised to the contrary Business continuity in place
Communications with providers
Share information over the importance of heatwave preparation.
Work with partner agencies, providers and businesses to coordinate heatwave plans, ensuring vulnerable and marginalised groups
Remind providers to: provide cool areas and monitor indoor temperatures to reduce the risk of heat-related illness and death in the
Ensure that key providers and partners have taken appropriate action including: conducting risk assessments.
Continue actions as per level 3 unless advised to the contrary

APPENDIX 4
are appropriately supported Remind providers to: identify or create cool rooms/areas (able to be maintained below 26 °C) install thermometers where vulnerable individuals spend substantial time
most vulnerable populations Review and prioritise high risk people Ensure sufficient cold water and ice
Communications coordination with local agencies and authorities
Ensure that a local, joined-up programme is in place between partner communications teams
Liaise with partners on joint preparedness arrangements
Liaise with partners and communicate public media messages – especially to ‘hard to reach’ vulnerable groups
Convene Hertfordshire communications leads teleconference to coordinate joined up communications response. (NHS lead).
Continue actions as per level 3 unless advised to the contrary

APPENDIX 4
CCG communications action plan for cold weather Actions taken from PHE action cards for commissioners and local authorities. Activity Level Level 0 Level 1 Level 2 Level 3 Level 4 Specific activity levels associated with cold weather
Long Term Planning all year
Preparedness Alert and Readiness Action Major Incident – Emergency Response
Messages to service users and public
Communicate public health media messages
Continue to communicate public health media messages
Continue to communicate public health media messages
Continue actions as per level 3 unless advised to the contrary
Messages to CCG staff
Work with partners and staff on risk reduction awareness (e.g. flu vaccination for staff in September/October), information and education
Review the distribution of the cold weather alerts across the system and ensure staff are aware of winter plans and advice
Communicate alerts to staff and make sure that they can take appropriate actions Activate business continuity arrangements and emergency plans as required
Communicate alerts to staff and make sure that winter plans are in operation
Continue actions as per level 3 unless advised to the contrary
Messages to providers
Ensure key partners, including all managers of care, residential and nursing homes are aware of the alert system and can access advice
Ensure key partners are undertaking action in response to alerts Ensure continuity arrangements are working with provider organisations
Continue actions as per level 3 unless advised to the contrary
Comms coordination with local agencies and authorities
Work with local organisations to coordinate locally appropriate cold
Support local community organisations to mobilise community
Continue actions as per level 3 unless advised to the contrary

APPENDIX 4
weather plans in accordance with the local and national Cold Weather Plan
emergency plans Work with partner agencies (e.g. transport) to ensure road and pavement gritting arrangements are in effect to allow access to critical services and high-use pedestrian areas

39 of 29
APPENDIX 4
Annexe D Figure 3.2: Providers – health and social care staff in all settings (community, hospitals and care homes)
Level 0
Level 1
Level 2
Level 3
Level 4
Long-term planning All year See accompanying document ‘Making the Case’ for more detail
Heatwave and Summer preparedness programme 1 June – 15 September
Heatwave is forecast – Alert and readiness 60% risk of heatwave in the next 2–3 days
Heatwave Action Temperature reached in one or more Met Office National Severe Weather Warning Service regions
Major incident – Emergency response Central Government will declare a Level 4 alert in the event of severe or prolonged heatwave affecting sectors other than health
Professional Staff (all settings):
Develop systems to identify and improve resilience of high-risk individuals
Encourage cycling/walking where possible to reduce heat levels and poor air quality in urban areas.
Care Homes and Hospitals Work with
commissioners to develop longer term plans to prepare for heatwaves
Make environmental improvements to provide a safe environment for clients in the event of a heatwave
Prepare business continuity plans to cover the event of a heatwave (e.g. storage of medicines, computer resilience, etc)
Work with partners and staff to raise awareness of the impacts of severe heat and on risk reduction awareness (key public health messages – box 1)
Professional Staff (all settings)
Identify high-risk individuals on your caseload and raise awareness of heat illnesses and their prevention among clients and carers.
Include risk in care records and consider whether changes might be necessary to care plans in the event of a heatwave (e.g. initiating daily visits by formal or informal care givers for those living alone)
Care Homes and Hospitals Ensure business continuity
plans are in place and implement as required; ensure appropriate contact details are provided to LA/NHS emergency planning officers to facilitate transfer of emergency information
Identify or create cool rooms/areas (able to be maintained below 26°C)
Install thermometers where vulnerable individuals spend substantial time
Professional staff (all settings):
Check high-risk people have visitor/ phone call arrangements in place
Reconfirm key public health messages to clients
Check client’s room temperature if visiting
Care Homes and Hospitals Check indoor temperatures
are recorded regularly during the hottest periods for all areas where patients reside
Ensure cool areas are below 26°C
Review and prioritise high-risk people
Ensure sufficient cold water and ice
Consider weighing clients regularly to identify dehydration and rescheduling physio to cooler hours
Communicate alerts to staff and make sure that they are aware of heatwave plans
Ensure sufficient staffing Implement business continuity
Professional staff (all settings):
Visit/phone high-risk people Reconfirm key
public health messages to clients
Advise carers to contact GP if concerns re health
Care Homes and Hospitals Activate plans to maintain
business continuity – including a possible surge in demand
Check indoor temperatures are recorded regularly during the hottest periods for all areas where patients reside
Ensure staff can help and advise clients including access to cool rooms, close monitoring of vulnerable individuals, reducing internal temperatures through shading, turning off unnecessary lights/equipment, cooling building at night, ensuring discharge planning takes home temperatures and support into account
NATIONAL EMERGENCY Continue actions as per Level 3 unless advised to the contrary
Central government will declare a Level 4 alert in the event of severe or prolonged heatwave affecting sectors other than health and if requiring coordinated multi-agency response
High-risk Groups Community: Over 75, female, living on own and isolated, severe physical or mental illness; urban areas, south-facing top flat; alcohol and/or drug dependency, homeless, babies and young children, multiple medications and over-exertion Care home or hospital: over 75, female, frail, severe physical or mental illness; multiple medications; babies and young children (hospitals).
*Because Level 2 is based on a prediction, there may be jumps between levels. Following Level 3, wait until temperatures cool to Level 1 before stopping Level 3 actions. ** Level 4: A decision to issue a Level 4 alert at national level will be taken in light of a cross-government assessment of the weather conditions, co-ordinated by the Civil Contingencies Secretariat

40 of 29
APPENDIX 4
Annexe E This figure summarises the key trigger temperatures during a heatwave. Although excess seasonal deaths start to occur at approximately 25°C, for practical reasons the Health Heatwave alert system is based upon temperature thresholds where the odds ratio is above 1.15–1.2 (a 15–20% increased risk). The different trigger temperatures for local areas are summarised below with regional
Figure 4. Trigger temperatures
variations due to relative adaptation to heat. However, a significant proportion of excess summer deaths occur before the Health Heatwave alert is triggered, which emphasises the importance of long-term planning actions by local authorities and the health sector.
52°C and 48°C – when train rails reach these temperatures a Temporary Speed Restriction (TSR) is introduced. Train speeds are reduced by 50% and 30% respectively
41.5°C and 36.2°C Temperatures recorded on the tube and on the platform during 2003 heatwave.
38.5°C Highest daytime temperature recorded in the UK
33°C Tarmac Roads may
begin to melt.
36°C Network Rail would be experiencing railhead temperatures of 50+°C when air temperatures of 36°C are reached. Extreme precautions would then be introduced.
24.5°C Temperature at which any excess deaths may first become apparent
24°C (for 3 days running) – London Underground deploy hot weather notices and supply bottled water. Maintenance workers begin work to stop rails buckling. Network rail also begin additional precautions to their track

41 of 29
APPENDIX 4
Annexe F Action Cards from Public Health England
CVS_action_card_commissioners_21Octob
CVS_action_card_providers_17_October_
VCS_action_card_21October_2014.pdf
VCS_action_card_GPs_17October_2014.p
VCS_action_card_individuals_17October_2
VCS_action_card_professional_staff_21O

Agenda Item No: 17
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Public Engagement Report
Decision Discussion Information Follow up from last meeting
Report authors: Lynda Dent and Mark Edwards
Report signed off by: Dr Nicky Williams, Deputy Chair
Purpose of the paper: To provide the Governing Body with an update on
progress made in developing and implementing patient and carer engagement and influence in the commissioning and quality of health services in East and North Herts.
Conflicts of Interest involved:
None.
Recommendations to the Governing Body:
To note the report.

Public Engagement Report September 2015
1. Purpose To provide the Governing Body with an update on the progress made in developing and implementing patient and carer engagement and influence in the commissioning and quality of health services in east and north Herts.
2. The Patient and Carer Member Network Work has continued in developing the patient and carer member network which contributes discussion and influence to CCG commissioning deliberations and decision making. Since April 2015, it is a contractual requirement for all GP practices to develop and maintain a patient group. This we hope will provide an additional stimulus to have all our practice patients represented on our commissioning network
Our patient and carer members are now taking up additional positions of responsibility which relate to health and social care and the work of the CCG. As a result we will be introducing declarations of interest forms for members to complete, ensuring everyone is aware of any existing personal interests when discussing specific issues.
Members continue to be kept up to date through bi-monthly meetings and an email newsletter.
There is currently one vacancy for a GP Co-Chair role in Upper Lea Valley locality and we are working with the locality GP chairs and manager to find a replacement. 3. Patient Network Quality The Patient Network Quality continues to focus its work on areas of concern raised by its members. Discussions with the group have focussed on a variety of issues including System Pressures, the Falls Strategy, the CCG’s CQUINs, Mental Health services as well as a talk from Dr Rachel Joyce, CCG Medical Director explaining her role and responsibilities in relation to quality.
The group is currently in the process of undertaking a self-assessment review of its effectiveness.
• Quality Assurance Visits (QAV) Visits In 2014/15 to date, the CCG’s Quality Team has undertaken nine quality assurance visits which have involved a patient representative, including to East and North Herts Trust, Herts Community Trust, Herts Urgent Care OOH service at the QEII hospital and Pinehill Hospital. There has also been a visit to East and North Herts Trust Paediatrics Unit. The Quality Team was accompanied by a 16 year old, who gave valuable insight from a young person’s perspective and as a potential inpatient. Actions As a result of feedback from patient representatives the following recommendations were made to the relevant provider: East & North Herts Trust
• Patient access to wi-fi to be considered within the Trust IT Strategy

• Patient feedback to be shared with ward staff for learning • Staff reminded of the importance in communicating clearly with patients and
explaining clearly the reasons why they may/will be moved to another ward area. • Staff to ensure that broken equipment is correctly reported and escalated if not
repaired urgently • Designated member of staff to take responsibility for the patient information leaflet
displays and ensure compliant and re-stocked. Herts Community Trust
• Trust to consider re-arranging the information displayed within the unit to reflect a patient’s journey, i.e. admission, services available, discharge, future help
• To ensure all patients and visitors are aware of how to alert staff when in an outside patient area.
• To review whether there are sufficient activities to engage and stimulate patients Herts Urgent Care (HUC) Concerns from the Quality Assurance Visit have prompted wider CCG and Trust actions to resolve both the patient experience and safety concerns. With regards to patient experience the actions are as follows:
• To ensure staff have updated name badges • To review why NHS111 is not being publicised to patients • Further signage required • Leaflets to be displayed about the services available • To review how patients are being kept informed about waiting times • Information on car park charges to be made available especially as the car park is
not staffed at night. Training The Quality Team has trained two new patient representatives; both of whom have undertaken their first Quality Assurance Visits. The Quality Team will be hosting a Patient Representative Learning Session on 5th October to review the visits that have been undertaken in the year to date, to discuss changes to the quality assurance visit documentation, to ensure all representatives are familiar with visit conduct and to discuss/respond to any areas of concern. In addition, the Quality Team’s quarterly ‘You Saw, We Said, They Did’ newsletter is being circulated to all patient representatives. This provides a good opportunity for the group to reflect on the visits that have been undertaken and the subsequent recommendations and actions that have been put in place as a result of their feedback.
• Patient Stories Stories are continuing to be collected by our trained network of patient volunteers. It has been agreed that a patient story would be played at the beginning of every other Board meeting in public and a story was played at the March meeting on the rehabilitation education courses offered for patients living with Chronic Obstructive Pulmonary Disease and the benefits received by that particular patient.
A series of other stories have been collected looking to focus on key areas of work for the CCG, on topics such as neurological conditions, experiences of care in care homes and personal health budgets. These stories are currently being edited for use by the CCG and its partners’ respective programme teams.

4. Contributing to Programmes and Projects Out of Hours (OOH) / NHS 111 procurement As part of the out of hours urgent care procurement process a communications and engagement project team was established, chaired by Healthwatch Hertfordshire. The procurement process for this has been suspended temporarily as the CCG waits for national guidance from NHS England on the procurement requirements. During the interim, we have undertaken a research survey on the use and perceptions of OOH urgent care services. Over 500 street interviews have been conducted by a market research agency as well as the development of an online survey which has been shared with patient and carer members. A small group of patient and carer representatives from across Hertfordshire has been identified to contribute to the service design and procurement process. They were briefed on their role at a recent workshop. Stroke Services All of our patient and carer members have received written briefings on proposed changes to stroke services in east and north Hertfordshire and west Essex, which particularly affect residents of east Hertfordshire following the proposed changes to Princess Alexandra Hospital. Residents in east and north Hertfordshire have been given the opportunity to feedback their comments to the engagement team and these are being monitored and responded to during the engagement period. The public engagement team is now in the process of planning two events open to public, patient and carer members to hear and discuss the proposed changes to these services. Neurological services co-production The joint project between the CCG, Herts Valleys CCG and Hertfordshire County Council continues to progress. A series of listening events held for patients living with neurological conditions and their carers has been undertaken. A patient representative has now been appointed as chairperson for the group which includes other patient and carer members, health and social care professionals and voluntary sector representatives. The group is currently designing a pathway of support based on the information received; mapping existing services against it to identify any gaps or areas of support that could be improved or shared. Personal Health Plan workshop 10 patient and carer members attended a workshop to assess and amend a draft template for a Personal Health Plan. As a result, a number of significant changes have been made to the document which will be considered by the Long Term Conditions Board before being piloted in one or two areas. Patient representatives will continue to feed into the project as it progresses. Commissioning Intentions 2016/17 Patient and carer members are being consulted regarding potential changes to the commissioning of services in 2016/17. Over the year, patient and carer members have raised a number of concerns and issues about health services. One locality patient group has championed the need for improved hospital discharge correspondence.

5. Promoting self care and raising awareness
Health Maze Following a number of new members joining our patient and carer network, we found a need for members to get another chance of understanding some of the basics around the NHS and how it is structured. Two sessions have been held so far, one looking at who commissions what, and a second event looking at integrated care and current projects being developed by the CCG in this area. 40 members have attended so far, including members of various PPGs from across the area.
Health Walks All of our patient commissioning groups have invited Hertfordshire Health walks to attend their regular meetings and given them the opportunity to join the scheme. This has been particularly successful in Welwyn Hatfield where it has resulted in the GP Locality providing partnership funding alongside the local borough council to offer walks in the locality. Patient and carer members are now actively engaged and have become walk leaders for the project in their respective areas. Type 2 Together - Peer support groups for people living with Type 2 Diabetes
The engagement team, alongside patient and carer members and Diabetes UK have been promoting the availability of the Type 2 Together peer support groups across the area, and particularly looking to recruit volunteer facilitators for new groups. There are now groups meeting regularly in Hertford, Hitchin, Hoddesdon, Stevenage, Welwyn Garden City and Bishop’s Stortford.
Patient and carer members, alongside practice staff, in Upper Lea Valley ran a successful awareness day in Hoddesdon with over 70 people attending and taking blood sugar tests. Of those three people were found to have high blood sugar levels and referred to their GP practice. There has also been positive media coverage of the peer support groups in both the Welwyn Hatfield Times and the Stevenage Comet.
Upper Lea Valley Patient engagement and Health Promotion project The Patient Commissioning Group in Upper Lea Valley was successful in bidding for some funding as part of the £1 per patient locality commissioning budget. This is to be used to encourage greater levels of engagement within the locality, but also to promote healthy lifestyle messages for the public. An audit of current engagement within the locality has shown that 9 of the 14 surgeries in the locality have developed patient engagement, although with differing structures and remits. A working group has been formed including patient and carer members of PPGs and practice managers to develop a plan of action to further develop this work over the coming months.
Carers In Lower Lea Valley, the members of the patient commissioning group have been very active in their continuing support of carers at the monthly Carers’ Cafe. An Open Day was held in June and a number of new carers came along and enjoyed being made a fuss of.
Members of the Stevenage Patient Commissioning Group are taking opportunities that could help identify people who are carers. Flu vaccination clinics and visiting wards at the Lister Hospital are reaping dividends.

Public Events Patient and carer members have been involved in a number of local community events promoting key health messages and CCG campaigns. Over 400 people have been engaged with various messages including carers’ support, promotion of the Type 2 Together peer support groups, giving opinions on OOH urgent care and discussing healthy eating. Events attended included Broxbourne Civic Day, Health Fest events in Welwyn Garden City and Hatfield, Stevenage Health Action Day.
Dementia Friends The Public Engagement Manager is a trained Dementia Friends Champion and has delivered four awareness sessions to staff within the CCG as well as at the Nurse and Healthcare Assistant Conference for all attendees in June. As a result, over 100 people have become dementia friends through the project and it is hoped that a number of patient and carer members will benefit from the sessions at meetings later in the year.
Movers and Munchers project Members of the engagement team met with staff at Allsorts Children Centre in Broxbourne and attended a ‘Movers and Munchers’ session at St Mary’s High School in Cheshunt. The team have since supported the Centre in developing promotional tools for the project and shared a stall at the Broxbourne Civic Day mentioned earlier. 6. Upcoming projects
Winter resilience project - Flu Vaccination and Antibiotics Awareness
Following a successful joint bid from the Communications and Engagement team to the Winter Resilience Fund, we are developing activities aimed at promoting uptake of the annual flu vaccination for relevant groups, but particularly older people and young children.
We are planning two large scale events giving parents the opportunity for their young child to have the nasal vaccination as well as provide them with basic health and first aid messaging to improve their resilience. With the forthcoming flu clinics, PPG members are being asked to support their surgery by giving out key winter resilience messaging such as awareness of the issues around antibiotic usage and help with identifying carers. Take Over Challenge The engagement team are working with the Associate Director for Children and Young People in developing a proposal to participate in the national Take Over Challenge Day. This will enable a group of young people to be involved with the CCG and contribute their opinions. There will be a particular focus on Child and Adolescent Mental Health Services (CAMHS) following the recent review in Hertfordshire.

1
Agenda Item No: Item 18
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: Governance and Audit Committee Minutes
Decision Discussion Information Follow up from last meeting Report author: Rita Venus, Board Secretary
Report signed off by: Linda Farrant, Lay Member, Governance and Audit
Purpose of the paper: To note the minutes of the meeting held on 20th May 2015.
Conflicts of Interest involved:
There are none identified.
Recommendations to the Governing Body:
To note the Minutes.

1
GOVERNANCE AND AUDIT COMMITTEE MEETING
WEDNESDAY 20 MAY 2015 2.00PM – 4.30pm CHARTER 2.1, CHARTER HOUSE
Present: Linda Farrant (LF) Lay Member, Governance and Audit - Chair
Nicky Williams (NW) Governing Body, Deputy Chair Dianne Desmulie (DD) Lay Member, Public and Patient Engagement
Attending: Alan Pond (AP) Chief Finance Officer Chris Rising (CR) Baker Tilly, Internal Audit Claire Peacock (CP) PwC, External Audit Anna Blackman (AB) PwC, External Audit Laura Weaver (LW) Baker Tilly, Local Counter Fraud Specialist Sarah Feal (SF) Company Secretary
Rita Venus (RV) Board Secretary (Minutes)
Item Subject
Action
1. WELCOME AND APOLOGIES FOR ABSENCE LF welcomed everyone to the meeting.
2. DECLARATIONS OF INTEREST
There were no declarations of interest identified.
3. MINUTES OF THE PREVIOUS MEETING AND MATTERS ARISING
The minutes of the last meeting held on 18 March 2015 were approved, with the following amendment: To insert the initials of the action owner into the action column.
4. COMMITTEE DECISION TRACKER
The action tracker was noted and the items highlighted in yellow were approved to be closed. LF was encouraged that a majority of the actions were closed.

2
5. GOVERNANCE
5.1 Draft Annual accounts 2014-15 AP presented the Annual Accounts and LF praised the Finance team and PWC for their efforts in producing them. AP explained that normally there is a comparison of the previous year’s figure, but the biggest difference for this financial year is the addition of CSU and ITU staff, therefore some comparators are not like for like. LF asked PWC if they were satisfied with how the Pooled budgets were managed. AB confirmed they were. LF requested further clarification regarding programme income and admin revenue. AP explained that in the Oracle system certain departments sit in either category e.g. CHC in programme and medicine management in admin. Some of the figures this year have been skewed by the Quality Premium, but this has been noted in the Annual Report. PWC confirmed that random samples are chosen to ensure items are in the correct pot. DD was concerned at the average working days lost noted in the Accounts. AP explained that there have been individuals on long term sickness, including those that were at retirement age. Also, when CSU joined they had a number of staff on long term sickness also. AP advised that the aim is to have the figure nearer the 2& mark. AB added that in an organisation the size of the CCG it only takes a few individuals on long term sickness to skew the figures. The 2013/14 spend for Internal Audit was queried. AP confirmed the 2014/15 figure is correct and the 2013/14 figure will be reviewed. The committee were encouraged by the percentage of Non-NHS trade invoices paid within target reaching 95%. The Committee went through the draft Annual Accounts page by page making various amendments and these were to be reported back to the Communications Team for revision. Draft Annual Report AP stated that there were still some issues that needed to be finalised, including the final figures for the Quality Premium. Photographs are still to be included. The External Auditors requested that the final version us is sent to them by Tuesday 26 May 2015. The Committee went through the Annual Report page by page, making various amendments and these were to be reported back to the Communications Team including:
• A fuller explanation on Never Events at Princess Alexandra Hospital.

3
• Inconsistencies with the CCG workforce numbers and the Staff Absence figures to be reviewed. NW questioned whether the information on absence days in the Annual Report is consistent with the numbers in the Annual Accounts. AP confirmed both are showing the same information, but the percentages need to be adjusted in the Annual Report.
• Inclusion and exclusion of some members on certain tables to be amended.
• External Audit identified several pages for sign off by the Accountable Officer; it was explained only one sign off page is required.
• It was noted that the Declarations of Interest were incorrect; certain members had still not declared particularly interests, and there was disparity between members from the same Locality. AP and LF were disappointed at the lack of information being provided by members and asked SF to attempt to obtain up to date information from members whose declarations appeared to be incomplete. It was suggested that this issue be raised at the next Governing Body Workshop.
5.2 Draft Annual Audit Committee Report LF presented the report to the Committee. The Committee were pleased with the draft report and felt it had reflected the past year. This will now be ratified at the Governing Body meeting in Public on 28 May 2015.
6. EXTERNAL AUDIT REPORT
AB and CP presented the draft External Audit ISA260 Report to the Committee. AB and CP discussed significant audit and accounting matters, and LF was encouraged to see there were no uncorrected misstatements. AB discussed with the Committee whether there has been a sufficient review of the CCG’s financial resilience over the next 3-5 years. It is felt financial pressures are likely to increase on the CCG’s local providers, which is in line with the national trend, and are the CCG sighted on the issue, and are the CCG reacting in a way that is expected from the External Auditors. AP responded that the statement in the report relating to this issue was overly critical. The CCG is reviewing its strategy presently, in line with the published Five Year Forward View, and there are controls in place to ensure the CCG are sighted on any significant issues. AB will review the wording in the report, and emphasised that there was not an intention to be overly critical, but wanted assurances that resources are available, if needed.
AB

4
LF highlighted that the information on monitoring the QIPP delivery appears to be out of date. Over the last 6 months the Operational Performance and Delivery days have been introduced, replacing the 4 Programme Boards. LF emphasised that the difficulties measuring the performance of schemes has now been strengthened by the OPD. LF feels it would be beneficial to add recognition that the process has changed. AB acknowledged this and will review. The final version of the report will be completed by 29 May 2015. The report was NOTED by the Committee.
AB
7. INTERNAL AUDIT REPORT
7.1 To receive the Annual Internal Audit Report Opinion The purpose of the paper was to provide the CCG with the Head of Internal Audit Opinion for the year, together with the results of the Internal Audit work undertaken during 2014/15. CR presented the report and asked the Committee to particularly consider the Head of Internal Audit Opinion and any potential impact that this could have on the Annual Governance Statement. CR explained that the wording of the Head of Internal Opinion is mandated by the Department of Health (DOH), and the opinion is based on the work undertaken by Baker Tilly. The Internal Audit plan was driven by the CCG’s key risks, as identified by the Strategic Risk Register (SRR) and the Risks Controls and Assurances Dashboard (RCAD). Discussions were held with management to ensure any key emerging risks were included in the plan. 13 positive opinions were issued with one advisory opinion, confirming that a good control framework was found to be operating with minimal recommendations being made. During the year 2 ‘Amber Red’ opinions were issued, relating to Patient Transport System Procurement and the Transition of Continuing Healthcare Service to the CCG. Many of the issues raised within these opinions were historic. CR explained actions plans have been developed and does not feel there are any issues that need to be flagged as significant internal control issues. All recommendations made were accepted by management. Two reports remain in draft at the time of publication of this report and LF emphasised that it would be good to have reports finalised prior to coming to the meeting. CR responded that this is the intention, but there had been certain circumstances beyond their control that had not made this possible. The Committee NOTED the report.

5
7.2 To review the progress against the Internal Audit Tracker The actions highlighted in yellow were approved to be closed. An update on the Safeguarding Adults action, provided by Tracey Cooper, Head of Adult Safeguarding, was presented at the meeting. It was advised that revised implementation dates be applied to both actions.
• Locality Commissioning and Governance action (1.8/1.9) were agreed to be closed by the Committee.
• Payroll (1.5) was agreed to be closed. Edward James is to send LW the Debtor Management Policy for review.
The Committee NOTED the action tracker.
EJ
8. LOCAL COUNTER FRAUD
LW presented the Local Counter Fraud report to the committee, to provide the CCG with a detailed report outlining the activities undertaken for 2014/15. The CCG workplan for 2014/15 was agreed with the Chief Financial Officer and approved by the Audit Committee on 19 March 2014. The matches from the National Fraud Initiative were supposed to be published in January 2015, but were not published until May 2015. Priority was given to the Payroll to Payroll and Payroll to Immigration matches. The latter does not affect the CCG as much as it would within an Acute setting. One query was raised but LW suspects the system is not holding the correct information. The Standards for Commissioners has been released. They were finally published in January 2015 and partly mirror the standards already in place for Providers. An assessment will have to be completed by the Local Counter Fraud Specialist (LCFS) by 31 July 2045. LW stated that once this is done a draft will be brought to the attention of AP to review. LW commented that now more services have been taken in house a few more workshops on the work of the LCFS, including Conflicts of Interest, would be sensible. LF agreed with this and is also happy to take on recommendations used from other organisations. The Committee NOTED the report.
9. POLICIES
SF provided a draft copy of the revised Managing Conflicts of Interest Policy for approval. A review of the Policy was necessary following recent implementation, as areas were identified which needed to be strengthened.

6
New recommendations have since been provided by LW. LW explained that part of the recommendations referred to the Declarations of Interest needing to be explicit. LW will be doing 2 sessions on 12 June to raise awareness of Conflict of Interest/Declarations of Interest. Discussions on the Declarations of Interest were held by the Committee. It was felt that it has to be reiterated, once again, to Governing Body members the importance of declaring the correct interests. It had been suggested that failure to declare an interest be a disciplinary action. The following change to the Policy was made:
• Page 12, 5.12, It should not be “The Procurement Lead” but changed to “Whoever is involved in the procurement process”
• To reflect in the Policy that Declarations of Interest are explicit. The Committee APPROVED the Policy, subject to amendments.
SF
10. ANNUAL CYCLE OF BUSINESS
The Committee NOTED the Annual Cycle of Business.
11. WAIVERS
AP presented two Waivers to the Committee. Both Waivers were fully discussed and accepted by the Committee. NW questioned the Waiver where only one tender response was received, querying whether this was value for money and would the CCG not go out to tender again. AP responded that in this circumstance it was not deemed necessary as the one response was reasonable in terms of speculated estimates. Follow up emails were sent to Providers who had not responded; only 2 emails were received, and one explained that it had been on oversight on their part.
12. AOB
No items were raised by the Committee
13. DATE OF NEXT MEETING
22 July 2015, 10am – 12.30pm, Charter 2.1 (previously CCG Boardroom), Charter House

1
Agenda Item No: Item 19
Date of Meeting: 24th September 2015
Governing Body Meeting in Public
Paper Title: HBL ICT Stakeholder Board Minutes
Decision Discussion Information Follow up from last meeting Report author: Sue Holland, PA to ICT Directors
Report signed off by: Alan Pond, Chief Finance Officer
Purpose of the paper: To note the minutes of the meeting held on
15th June 2015.
Conflicts of Interest involved:
There are none identified.
Recommendations to the Governing Body:
To note the Minutes.

HBL ICT Stakeholder Board Meeting
Monday, 15th June 2015 at Charter House, WGC AL8 6JL
Present: Phil Turnock- ICT Shared Services Director Alan Warren – CFO HVCCG Ray Davey - Deputy CFO Luton CCG Phil Bradley – Director of Finance HCT Carol Sheridan - Associate Director of IM&T HPFT Malcolm Miller – Deputy CFO Beds CCG
Iain Eaves –Exec. Director - Strategy & Organisational Development HPFT Alan Pond – CFO E&NHCCG (Chair)
1 Welcome & Apologies (AP)
Welcome to Iain Eaves, Executive Director - Strategy & Organisational Development, HPFT All stakeholder organisations represented – no apologies received.
2 Register any Conflict of Interest(AP) None
3 Minutes from previous meeting (18/5/15) & matters arising (ALL/AP). Due to sickness absence, minutes from 18/5/15 not available. It was decided that minutes from 18/5/15 & today’s meeting 15/6/15 both be prepared for discussion prior to the next meeting on 20/7/15.
SH
4 Finance Report – Month 2 (AP) AP not aware of any major issues in respect of ICT. Need to sign off of income. PT – waiting for NHS England to sign & complete Service Agreement (pending budget allowance). The main cost for NHSE being RA services @ £152K. HUC & NHS PS have signed agreements.
5 ICT Service Charges 2015/16 – Sign Off (AP) Document – Schedule of Service Charges for 2015/16 – provided for members to sign. Organisations that signed this document at this meeting: HVCCG (Alan Warren) – AW requested a reconciliation schedule. PT to supply. HCT (Phil Bradley) – PB/PT have agreed values BEDSCCG (Malcolm Miller) had signed this document prior to this meeting. Phil Bradley to sign off HCT’s ‘Shared Services Agreement (SSA) and Service Level Agreement (SLA)
PT PB
6 HBL ICT Re-structure Update (PT) PT stated papers have now gone to staffside. 30 day consultation will now start 1/7/15 although this is likely to be extended to 45 days. All staff will be able to express an interest in any role via the appropriate interview path. All staff will have access to SMT members for discussion / 1:1s. Total of 118 staff involved although approx. 40 staff not directly affected. Impact will fall mainly of bands 8a being reduced to band 7s as well as 2x senior secondment posts currently with NHS England. Job positions for Band 7 & below would consist of an interview & test; band 8 & above – an interview & presentation. AP suggested that HR attendance from perhaps one of the partners at ICT interviews would give a level of transparency. PT said he wanted to bring all HBL ICT staff onto one site – WGC - & close Bedford GHH site. AP explained the usage of GGH Beds & stated that the Beds RA function could be based elsewhere in Bedfordshire. Possible saving - £700K. HR should provide support for the interview process as well as a ‘package’ for those staff that move on or are affected by the changes. PT stated that the process was well prepared overall & could be managed via MS SharePoint. PT stated that a ‘shift’ pattern of working would be introduced to help eliminate the high cost of overtime & on call. This would match a practice already in place on the ICT Service Desk.

Staff T&Cs are protected for 5 years; however, job status could be an issue for some staff. T&C should be kept in line with other departments that came over to the CCG from CECSU. AP – no savings this year & some expenditure would be deferred to next year. AP confident with current figures.
7 Strategic IT Roadmap – SITR (PT) Document – SITR Strategic IT Roadmap – prepared by CISCO & provided to members as handout. PT explained that this was a free exercise by CISCO (an expert in this field) and under no obligation. CISCO need access to senior persons from within the stakeholder groups to carry out structured & driven interviews for approx.. 45 – 60mins in order to understand the business ambitions within the groups. Business ambitions cover all aspects of the health economy, not just IT & new technologies. AP mentioned access & controls for patient records as this item will need to be addressed at some stage. ALL members to provide Executive names to PT for CISCO consultative interviews by 30th June 2015. PT/Sam Potts, PMO to project manage on ICT side. CS/AP summarised that this exercise would show what was needed and wanted by each organisation, including HBL ICT.
ALL
8 Service Performance against KPIs (PT) Document – KPIs May 2015 – provided to members. PT explained that figures detailed here were not adjusted in any way. Issue around response times needed to be addressed by ICT. CS stated that HPFT struggled to obtain reports they required from ICT. CS requested that a Service Improvement Plan (SIP) & KPI are produced together. KPIs will now be a standard agenda item. General discussion on ‘self help’ option as best use of service. AIG meeting is usual place where such topics are raised and discussed & brought to attention of this group if necessary. PT asked for more response from stakeholders & other customers. Members are invited to submit topics for discussion on the agendas of the AIG and/or the stakeholder board meetings at any time.
PT
9 Potential New Business Opportunities (PT) - New QEII/E&NH Acute Trust. PT to meet with new CIO – Anthony Lundrigan - 16/6/15.
New income £80K service contract for New QEII core infrastructure/networks & telephony services.
- Cambridge Community Services – currently as a consultancy managing SERCO one day per month; possibility to supplying a complete IT service in the future. SERCO contract up for renewal Sept 2015.
- Renew datacentres (6x). - Herts County Council (HCC) network contract up for renewal but penalty clauses within
contract are costly/restraining. CS expressed concern how any new business would impact on current customers. PT explained that the new structure takes this into account plus the possibility to recruit if required. Also the development of core infrastructures would be beneficial to the business. The CISCO survey would show more business integration possibilities. PT suggested that ‘Potential New Business Opportunities’ is also a regular agenda item.
PT
10 A O B CS stated that HPFT Medical Director, Geraldine O’Sullivan has retired. Interim substantive replacement is Dr Kaushik Mukhopadhaya. CS and/or Iain Eaves, HPFT will attend future stakeholder board meetings. Received after the meeting: PT invited to attend Luton CCG Exec. Board Mtg on 2/7/15 (to discuss how the Shared Service will support Luton CCG going forward e.g. strategy & developments.)
PT
11 Date of next meeting: Monday, 20th July 2015 at 2 - 4pm Room Charter House 2.2 – 2nd Fl Charter House WGC AL8 6JL.

Summary of Actions: 3
minutes from 18/5/15 & today’s meeting 15/6/15 both be prepared for discussion prior to the next meeting on 20/7/15.
SH
5 Alan Warren requested a reconciliation schedule. PT to supply. Phil Bradley to sign off HCT’‘Shared Services Agreement (SSA) and Service Level Agreement (SLA).
PT PB
7
ALL members to provide Executive names to PT for CISCO consultative interviews by 30th June 2015.
ALL
8 KPIs will now be a standard agenda item. .
PT
9 PT suggested that ‘Potential New Business Opportunities’ is also a regular agenda item.
PT
10 PT invited to attend Luton CCG Exec. Board Mtg on 2/7/15
PT


















