
Gordon Robb Operations Director
21
Transcript of Gordon Robb Operations Director


Gordon RobbOperations Director
Aim of presentationAim of presentation
• Overview of Alba Bioscience Microarray developments
• Highlight manufacturing implications
• Review development and regulatory issues and strategy
• Presentation of some preliminary data

• Focus on microarray technology as the next generation test platform for blood donation screening
• Protein/carbohydrate/cell based arrays (not genetic testing)
• A single platform to combine blood typing, microbiology and virology testing
MicroarrayMicroarray Project AimProject Aim

Current blood testing Current blood testing proceduresprocedures
Y
Based on the principle of antibody:antigen interactions to determine presence or absence
of a target e.g. blood group
Usually performed in liquid phase

Current Testing v Current Testing v MicroarrayMicroarray SystemsSystems
Donation
Blood grouping NAT testingMicrobiology serology
IT Systems
Release of Blood Donation
RESULTSRESULTS
Donation
Single microarrayplatform
Release of Blood Donation
RESULTSRESULTS
CURRENT CURRENT FutureFuture((MicroarrayMicroarray))
Blood grouping NAT testingMicrobiology serology
Confirmatory Testing
IT Systems

MicroarraysMicroarrays: Benefits: Benefits• Speed / Multiplexing / Multiparameter
High throughput testing – all required tests on one platformExtended assay profile – include all desirable as well as mandatory testsNo confirmatory testing required – replicate testing performed simultaneously
• Reduced CostsSingle Instrument v 3 instruments (capital, maintenance etc)Staff: 1 lab v 3 labs No repeat/confirmatory testingReduced sample requirement
• Patient SafetySingle sampleImproved sensitivity & specificitySingle IT interface

Design of the blood typing Design of the blood typing microarraymicroarray
Immobilised antibody probes
Block NSB
Incubate with test red cell suspension
Scan for fluorescence
Wash the microarray
Addition of test cells

Design of the antibody screening Design of the antibody screening microarraymicroarray
Chip surface
Immobilised antigen*
Plasma/serum added(may contain antibody
to blood group antigens)
Fluorescent detection antibody**
* Immobilised antigen must represent clinically significant blood group antigens e.g. red cells/peptides/alternative source antigen
** Fluorescent detection antibody must bind to clinically significant human blood group antibodies e.g. anti-human IgG/IgM

Design of the DAT Design of the DAT microarraymicroarray
Gold surface
Immobilised antibody probes
Block NSB
Incubate with test red cell suspension
Anti-D (IgG1)
Anti-IgG (Rabbit)
Anti-D (IgG3) Anti-IgG1 Anti-IgG3 Anti-C3
Addition of test cells
Scan for fluorescence
Wash the microarray
Manufacturing ConsiderationsManufacturing Considerations
• Production of Antibodies- monoclonal /polyclonal- purification methods - IgM/IgG- Specificity/best probes
• Production of Antigens- antigen form- purification ?
• Surface chemistry

Manufacturing Considerations
• Process Scale-Up & Validation
• Stability of components (bulk storage, finished product)
• Resources– Facility– Equipment - High throughput printing
• Quality Control

Development and Regulatory Development and Regulatory StrategyStrategy……11• Fully optimise all aspects of comprehensive microarraying
platform• Phased launch to market • Package developed in collaboration • Field trials, validation and verification of platform• Test purchase controlled by software
• Compliance with and approval by regulatory bodies-ISO 13485-European IVD Medical Devices Directive

Development and Regulatory Development and Regulatory StrategyStrategy……22• In the US…
- FDA Center for Devices and Radiological Health is the lead authority for equipment submissions - FDA Center for Biologics Evaluation and Research is lead authority for biological submissions
• Equipment normally cleared first (instrument and software) and is normally submitted by equipment manufacturer.
• However, combination product applications can be accepted• Each case reviewed by FDA and best route agreed• Software validation is likely to be the most complex step in the
validation ( minimised by limited chip options)
• Related guidance listed in July 2007 issue of Transfusion.

Preliminary results Preliminary results –– blood typingblood typing
0
5
10
15
20
25
30
Group O group A1 group B Group A1B
Anti-B (LB2) Anti-A (LA2) Anti-A (ES9) Anti-A(B) (ES15)

Preliminary results Preliminary results –– blood typingblood typing
Probe antibody specificity and concentration
Anti-K 0.5 mg/ml
S/N
0
10
20
30
60
80
100
120
140
160
K heterozygous K homozygous K negative Col 8 Col 10 Col 12 Col 14
K negative

Preliminary results Preliminary results –– antibody antibody screeningscreening
0
0.5
1
1.5
2
2.5
3
3.5
Anti-D Anti-C Anti-E Anti-c Anti-e
R1R1 (CCDDee) R2R2 (DDccEE) rr (ccee)
Red cell membrane fragments immobilised on proprietary surface, antibodies added and detected by addition of anti-human IgG/IgM
Result >1 is positive
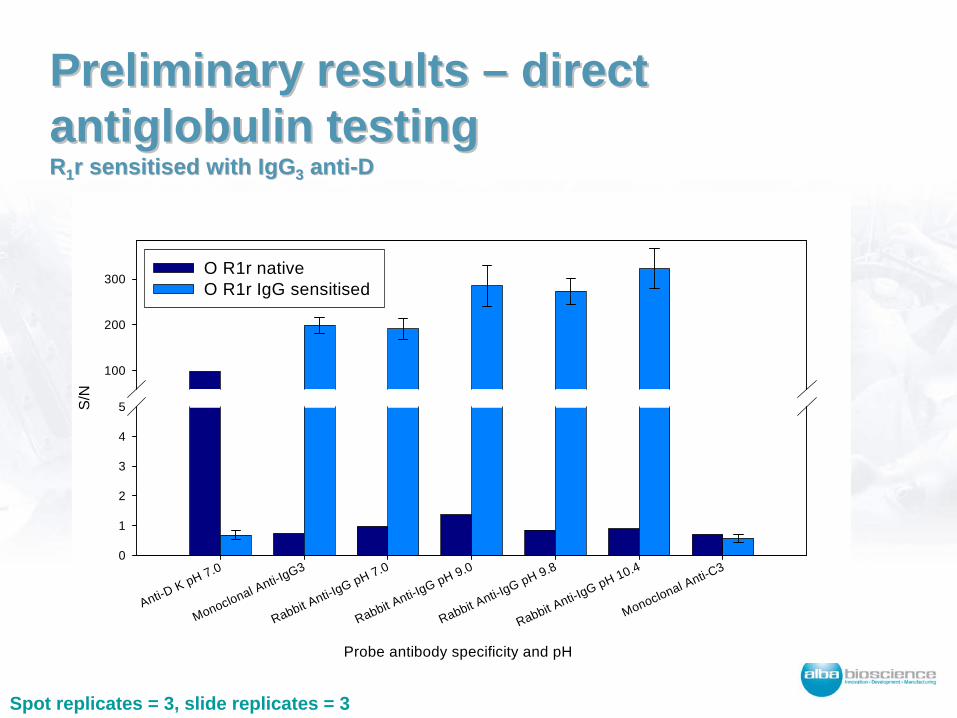
Preliminary results Preliminary results –– direct direct antiglobulinantiglobulin testingtesting RR11 r sensitised with IgGr sensitised with IgG33 antianti--DD
Probe antibody specificity and pH
Anti-D K pH 7.0
Monoclonal Anti-IgG3
Rabbit Anti-IgG pH 7.0
Rabbit Anti-IgG pH 9.0
Rabbit Anti-IgG pH 9.8
Rabbit Anti-IgG pH 10.4
Monoclonal Anti-C3
S/N
0
1
2
3
4
5
100
200
300O R1r native O R1r IgG sensitised
Spot replicates = 3, slide replicates = 3

Preliminary results Preliminary results –– direct direct antiglobulinantiglobulin testingtesting RR11 r sensitised with IgGr sensitised with IgG33 antianti--DD
Probe antibody specificity and pH
Anti-D K pH 7.0
Monoclonal Anti-IgG3
Rabbit Anti-IgG pH 7.0
Rabbit Anti-IgG pH 9.0
Rabbit Anti-IgG pH 9.8
Rabbit Anti-IgG pH 10.4
Monoclonal Anti-C3
S/N
0
1
2
3
4
5
100
200
300O R1r native O R1r IgG sensitised
Spot replicates = 3, slide replicates = 3
AcknowledgementsAcknowledgements
• Alba Bioscience – Product DevelopmentDr Janine Robb, Linda Knowles
• Scottish National Blood Transfusion ServiceDr Juraj Petrik and his Transfusion Transmitted Infection R&D Group
• University of EdinburghDepartment of Pathway Medicine (formerly SCGTI)
• Scottish Enterprise



















