Good slide dvt
29
-
Upload
2pawarprashant -
Category
Health & Medicine
-
view
288 -
download
0
Transcript of Good slide dvt


ETIOPATHOGENESIS
• Abnormalities of flow• Abnormalities of vessel wall• Hypercoagulability of blood
ETIOPATHOGENESIS
Objectives/Outline Rationale for thromboprophylaxis
Summary of the 7th ACCP thromboprophylaxis guidelines
Implementation strategies
Rationale for Thromboprophylaxis
I. High prevalence of VTE in certain patient groups
II. Adverse consequences of unprevented VTE
III. Efficacy, effectiveness and cost- effectiveness of thromboprophylaxis

Risk Factors for VTE¨ Previous venous thromboembolism¨ Increased age¨ Surgery¨ Trauma - major, local leg¨ Immobilization - bedrest, stroke, paralysis¨ Malignancy and its Rx (CTX, RTX, hormonal)¨ Heart or respiratory failure¨ Estrogen use, pregnancy, postpartum, SERMs¨ Central venous lines ¨ Thrombophilic abnormalities
Risk Factors for VTE¨ Previous venous thromboembolism¨ Increased age¨ Surgery¨ Trauma - major, local leg¨ Immobilization - ? bedrest, stroke, paralysis¨ Malignancy & its Rx (CTX, RTX, hormonal)¨ Heart or respiratory failure¨ Estrogen use, pregnancy, postpartum, SERMs¨ Central venous lines ¨ Thrombophilic abnormalitiesMost hospitalized patients have at
least one risk factor for VTE
Some Basic Principles of Thromboprophylaxis
• Group prophylaxis rather than individual
• Mechanical prophylaxis only if high risk of bleeding
• No role for aspirin alone as DVT prophylaxis
• Epidural analgesia and anticoagulant thromboprophylaxis are compatible
7th ACCP Conference on Antithrombotic Therapy
DVT Prophylaxis: 3 Patient Groups
Low risk
Moderate risk
High risk

Patient group: Age < 40 years
Medical – fully mobile, brief admission
Surgical – procedure < 30 min, mobile,
no additional risk factors
Recommendations: no specific prophylaxis
mobilization [Grade 1C]
Low risk7th ACCP Conference on Antithrombotic Therapy
Patient group: Age between 40 – 60 years + minor surgery or age < 40 with risk factors Medical – bedrest / sick Surgical – major general, urologic,
gynecologic procedures
Evidence: LDH ~ LMWHOptions: LDH [Grade 1A] 5000 bid
LMWH [Grade 1A] <= 3400 u once daily TEDS, IPC (high bleeding risk) [1C+]
Start: as soon as possibleDuration: until discharge (not “ambulation”)
Moderate risk7th ACCP Conference on Antithrombotic Therapy
Patient group: Major orthopedics (THR, TKA, HFS) Age 40 – 60 years with major surgery (G +U)
Minor surgery, Age > 60, +/- risk factors
Evidence: 1. Venography: fondaparinux > LMWH > OVKA 2. Clinical: LMWH ~ OVKAOptions: LMWH [Grade 1A] > 3400 sc daily
fondaparinux [Grade 1A] oral vitamin K antagonist (INR 2-3) [1A] LDH or LMWH + GCS or IPC
Start: Postop (preop if HFS delayed)
Duration: > 10 days (2-4 weeks)
7th ACCP Conference on Antithrombotic Therapy
High risk

HIT with LDH or LMWH for Prophylaxis
Martel – Blood 2005;106:2710
• meta-analysis of 7 prospective studies comparing prophylactic LDH and LMWH
Prophylactic anticoagulant HIT
Heparin 41/1,730 (2.37 %)
LMWH 1/1,762 (0.06 %)
* NNT=43
Routine Prophylaxis NOT Recommended:• vascular surgery• laparoscopic surgery• knee arthroscopy• spine surgery• isolated lower extremity fractures• long distance travel
7th ACCP Conference on Antithrombotic Therapy
Any additional risk factors will mandate consideration of thromboprophylaxis
Benefit:risk favors routine prophylaxis
• Major orthopedic surgery (THR, TKR, HFS)• Major trauma• Spinal cord injury• Major general, gyne, urologic surgery• Major neurosurgery• Medical patients with additional risk factors• Most ICU patients

Benefit:risk favors routine prophylaxis
• Major orthopedic surgery (THR, TKR, HFS)• Major trauma• Spinal cord injury• Major general, gyne, urologic surgery• Major neurosurgery• Medical patients with additional risk factors• Most ICU patients
Benefit:risk favors no prophylaxis
• Surgical patients: - brief procedure - fully mobile - no additional RFs• Medical patients: - fully mobile - no additional RFs• Long distance travel

Benefit:risk favors routine prophylaxis
• Major orthopedic surgery (THR, TKR, HFS)• Major trauma• Spinal cord injury• Major general, gyne, urologic surgery• Major neurosurgery• Medical patients with additional risk factors• Most ICU patients
Benefit:risk uncertain- local practice or
individual prophyl.
• Laparoscopic surgery• Vascular surgery• Cardiac surgery• Elective spine surgery• Arthroscopic surgery• Burns• Isolated lower extremity fracture
Benefit:risk favors no prophylaxis
• Surgical patients: - brief duration - fully mobile - no additional RFs• Medical patients: - fully mobile - no additional RFs• Long distance travel

Thromboprophylaxis Use in Practice 1992-2002
Prophylaxis Patient Group Studies Patients Use (any)
Orthopedic surgery 4 20,216 90 % (57-98)
General surgery 7 2,473 73 % (38-98)
Critical care 14 3,654 69 % (33-100)
Gynecology 1 456 66 %
Medical patients 5 1,010 23 % (14-62)
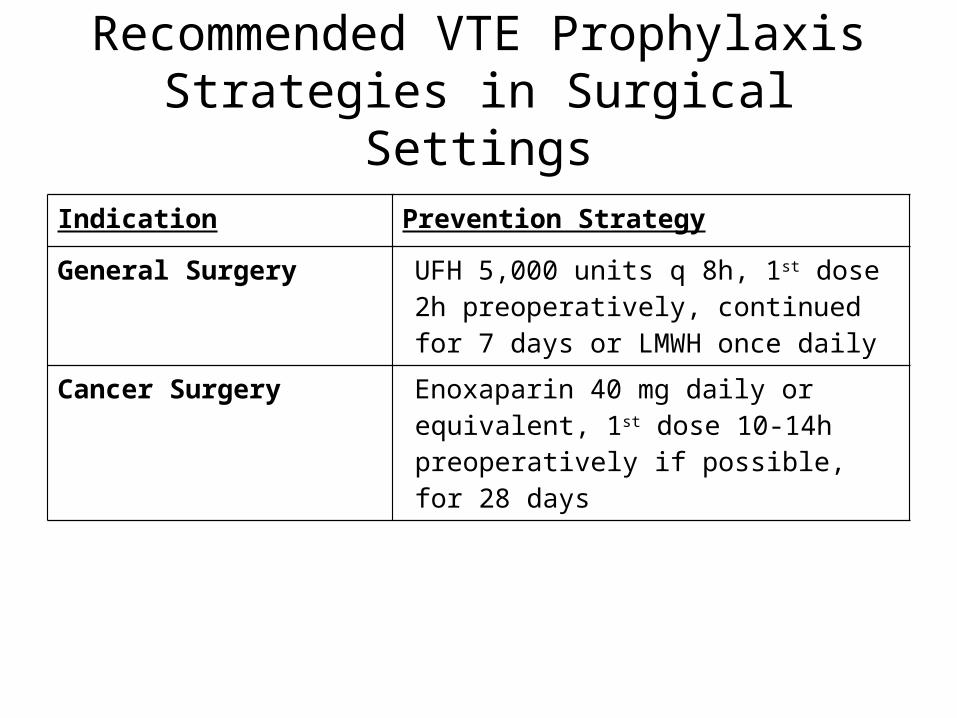
Recommended VTE Prophylaxis Strategies in Surgical Settings
Indication Prevention Strategy
General Surgery UFH 5,000 units q 8h, 1st dose 2h preoperatively, continued for 7 days or LMWH once daily
Cancer Surgery Enoxaparin 40 mg daily or equivalent, 1st dose 10-14h preoperatively if possible, for 28 days
UFH = unfractionated heparinLMWH = low molecular weight heparin

Recommended VTE Prophylaxis Strategies in Surgical Settings (cont.)
Indication Prevention Strategy
Total Hip Replacement
Enoxaparin 40 mg daily or equivalent, beginning preoperative evening, continuing out-of-hospital for 21-28 days
Enoxaparin 30 mg BID or equivalent, 1st dose 12-24h postoperatively, until hospital discharge
Dalteparin 2,500 units ≥ 4h post-op, then 5,000 units daily until hospital discharge or for 35 days

Recommended VTE Prophylaxis Strategies in Surgical Settings (cont.)
Indication Prevention Strategy
Total Hip Replacement (cont.)
Fondaparinux 2.5 mg 4-8h post-op, then ≥ 12h after 1st dose, then daily for 5-9 daysWarfarin daily, 1st dose 7.5 mg 24-48h preoperatively, adjusted to target INR of 2.0-3.0
Warfarin daily, 1st dose 5 mg preoperative evening, adjusted to target INR of 2.0-3.0 and continued 4-6 weeks

Recommended VTE Prophylaxis Strategies in Surgical Settings (cont.)
Indication Prevention StrategyTotal Knee Replacement
Enoxaparin 30 mg BID or equivalent, beginning 12-24h postoperatively, continued for an average of 9 days
Fondaparinux 2.5 mg, 1st dose 4-8h postoperatively, 2nd dose ≥ 12h after 1st dose, then daily for 5-9 days
Hip Fracture Surgery
Fondaparinux 2.5 mg, 1st dose 4-8h postoperatively, 2nd dose ≥ 12h after 1st dose, then daily for 5-9 days. If surgery is delayed > 24-48h after admission, give 1st dose 10-14h preoperatively

Recommended VTE Prophylaxis Strategies in Surgical Settings (cont.)
Indication Prevention StrategyNeurosurgery Enoxaparin 40 mg daily or equivalent, 1st
dose ≤ 24h postoperatively, continued until hospital discharge, plus GCS
Craniotomy for Brain Tumor
Enoxaparin 40 mg daily or UFH 5,000 units BID, 1st dose on 1st postoperative morning, continued until hospital discharge, plus GCS/IPC, plus predischarge venous ultrasonography
GCS = graduated compression stockingsIPC = intermittent pneumatic compression devices
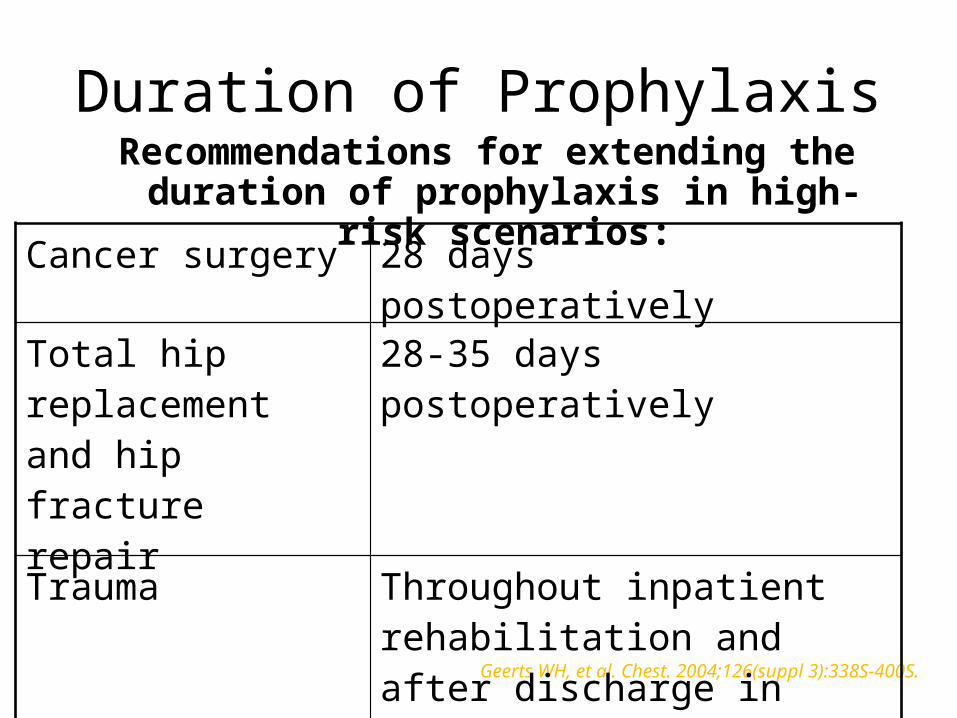
Duration of ProphylaxisRecommendations for extending the duration of
prophylaxis in high-risk scenarios:
Geerts WH, et al. Chest. 2004;126(suppl 3):338S-400S.
Cancer surgery 28 days postoperativelyTotal hip replacement and hip fracture repair
28-35 days postoperatively
Trauma Throughout inpatient rehabilitation and after discharge in patients with significantly impaired mobility

Objectives/Outline Rationale for thromboprophylaxis
Summary of the 7th ACCP thromboprophylaxis guidelines
Implementation strategies
Strategies to Improve Thromboprophylaxis Success
• Excellent quality guidelines• National body endorsement• Hospital accreditation (JCAHO)• Pay for performance (CMS)• Local written policy (care pathway) for the hospital / program / patient care unit• Pharmacist responsibility• Pre-printed orders • Computerized orders
Take-Home Points• Know the common VTE risk factors• Assess VTE risk for each hospitalized patient
individually• Become familiar with the various VTE prophylaxis
regimens for different at-risk patient groups• Apply the current ACCP guidelines to prevent
VTE in hospitalized patients
Prevention of VTE: Summary
1. Thromboprophylaxis is indicated for most hospitalized patients
2. But is under-utilized
3. Not ASA; mechanical rarely; warfarin scary
4. Chest 2004;126(suppl):338S-400S
5. Systems approach / hospital policy
6. Keep it simple, routine: Pre-printed orders
Just do it!

Thank you
http://webmm.ahrq.gov
Bill Geerts, MD, FRCPC, FCCPUniversity of Toronto