Gonioscopy
80
GONIOSCOP Y WHAT WHO (people and evolution ) WHY (Purpose) HOW (Principl e and method) WHERE
-
Upload
meenank -
Category
Health & Medicine
-
view
2.514 -
download
2
Transcript of Gonioscopy

GONIOSCOPY
WHAT
WHO (people and evolution)
WHY (Purpose)
HOW (Principle and
method)
WHERE

What is Gonioscopy
• Gonioscopy is an examination of the eye to look at the anterior chamber from the ant. part of iris to the post. part of cornea using the help of gonio-lens and slit lamp.

The Who of Gonioscopy

Pioneer
• Alexios Trantas : The first person to examine angle in the Anterior chamber in a living eye.
• In 1900 with the aid of direct ophthalmoscopy and stimulating digital pressure on corneo-scleral capsule he examined – ciliary body, ora serrata and , the anterior chamber .
1901 – Gazette Medicale d’Orient.

• Maximilian Salzmann: He reported that light that emanates from the angle undergoes ‘total internal reflection’ and thus, cannot be intercepted by ophthalmoscope due to change in medium
• He indicated that indirect ophthalmoscopy give’s a better view of angle than that of direct ophthalmoscopy.
• He later calculated that the lens with smaller radius of that of cornea would facilitate Gonioscopy (Zeiss scleral contact lens 7mm).

Impact Of Slitlamp Biomicroscopy
• 1920- Zeiss perfected the first slitlamp basing on principle of Noble laureate Allvar Gullstrand (Sweden) and Czapski’s corneal microscope.
• Koeppe (Germany) : Mathematically calculated the most adv. Contact lens and gave the method biomicroscopy of angle of ant. Chamber with slit lamp (magni. – 40 dia)

• He could see the nasal and temporal aspects of angle in sitting position of patient with the help of new more convex and thicker lens.
• Koeppe’s method improvised by Ascher and used on recumbent patients made it possible to visualizing inferior and superior angles
• Koeppe’s method is still been used for direct gonioscopy without reflecting surface

The American Pioneer• Manuel Uribe Troncoso: Involved in Gonioscopy
due to interest in glaucoma • 1925-Discribed self illuminating mono-ocular
Gonioscopy with its complex arrangment of reflecting prisms ( mag: 30 dia)
• 1941- Discribed chamber angles in various glaucoma’s
• 1947 – Wrote first comprehensive book on Gonioscopy
• Clarified the anatomical terminology of structures of angle seen in Gonioscopy.

Otto Barkan
• He combined Koeppe’s contact lens, the light powerful Vogt carbon-arc slit lamp and Zeiss binocular microscope which gave 40x mag.
• He coined the term ‘open angle glaucoma’ and suggested that, sclerosis of trabecular meshwork was the cause for raise in IOP
• He devised internal trebeculectomy under microscopy which spurned to todays external trebeculectomy and trebeculectomy

Contd…• He was able to correlate the raise of IOP in
eyes with narrow angle glaucoma with closure of angle by root of iris naming ‘narrow angle glaucoma’ and advocated peripheral iridectomy as a cure.
• Barkan and Maisler studied the exact topography of angle structures .

Goldmann’s Gonioscopy
• It was Goldmann a Swizz Ophthalmologist in Prague who popularised gonioscopy in Europe, not only by introducing a simple and superior method of examination but, also through his papers which confirmed Barkan’s observations.
• Allen, Braley and Thorpe (1945) with four reflecting surfaces gave a miter shaped gonioscope where external curvature of koeppe lens was replaced by a prism which stayed on the cornea by capillary attraction.

Why do we need Gonioscopy
• As the recesses of the angle of anterior chamber are difficult to visualize since this region is covered by projecting shelf of sclera at the limbus and all the emergent light is subjected to total internal reflection.

Why do we need Gonioscopy
• Fundamental part of comprehensive exam• Most important factor in correct diagnosis• Done initially for all glaucoma patients and
suspects• Repeated periodically for all angle – closure
glaucoma patients

Purpose of Gonioscopy
• Visualization of anterior chamber angle • View of peripheral iris• Difference between angle – closure,
occludable, and secondary glaucomas

Other ways to evaluate the angle
Scheimpflup photography Ultrasound biomicroscopy

Anterior Segment optical coherence tomography

Principle of Gonioscopy

Criticle angle
• When light is passing from a medium with greater refractive index to one with lesser refractive index angle of refraction (r)will be larger than angle of incidence(i)
• Critical angle is where ‘r’ = 90⁰• When ‘I’ exceeds critical angle the light is
reflected back into the medium • Critical angle for corneal-air interface = 46⁰• Light from A.C. angle as exceeds the critical angle
is reflected back into the anterior chamber leading to ‘ Total internal reflection’

Critical angle, cornel and goniolens

Principle of Gonioscopy

Method of Gonioscopy

Common Goniolens and Typeslens description
1. Indirect goniolens
• goldmann single mirror Mirror inclined at 62⁰
• Zeiss four mirror All mirrors at 64⁰ , no fluid bridge requried
• Posner four mirror Modified Zeiss with handel
• Sussman four mirror Hand held Zeiss model
• Ritch Trabeculoplasty lens Four mirror’s : 2 at 59⁰ and 2 at 62⁰ , with a convex lens over two of the mirror’s
2. Direct goniolens
• Koeppe Dome shaped lens
• Barkan Quarter sphere, surgical and diagnostic lens
• Swan-Jacob Surgical goniolens for children

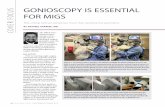
Direct Gonioscopy
Instruments : goniolens , gonioscope or hand bio-microscope (15-20x) and a light source

Direct Gonioscopy• Advantages– Observer’s height can be changed
to look deep or get a better look at the angle structre’s
– As done in supine position it can be used for sedated, comatosed, or in children
– Useful in examining the fundus with small pupil with D.O
– Straight on the view– Panoramic view of the angle
structure’s– Comparison of angle recession– Causes less distortion of A.C.

Direct Gonioscopy
• Disadvantages – Inconvenient– Special equipment needed

Indirect Gonioscopy• Instrument's used : gonioprism and a slitlamp• Most widely used gonioprisum : Goldmann
– Goldman single mirror• Height of the mirror : 12 mm• Angle of the mirror : 62 ⁰• Central well diameter : 12mm• Posterior radius of curvature : 7.38 mm
– Goldmann three mirror• One mirror for examination of anterior chamber : 59⁰• Two mirror’s for examination of fundus.
• The posterior radius of curvature is such that both the lens need viscous material to fill the space

• Contd…• Modified Goldmann lens have been
developed – One with a posterior curvature of 8.4 mm
eliminating the need of a viscous material– Another with a anti-reflecting coat used in laser
trabeculoplasty

Indirect Gonioscopy

Indirect Gonioscopy

Indirect Gonioscopy

Four mirror lens
• Zeiss four mirror lens, all at an angle of 64⁰ eliminating the need for rotating
• Original four mirror is on a Unger Holder• Posner has a fixed holder• Sussman is held directly• Posterior curvature of all these lens is equal to
that of cornea which allows the patien’s own tears to form the fluid bridge

Indirect Gonioscopy

Indirect Gonioscopy

Indirect Gonioscopy

Indirect Gonioscopy

Slit lamp technique

Slit lamp technique

Indirect Gonioscopy

Indirect Gonioscopy

What to see
• While performing a direct or an indirect Gonioscopy and starting from the root of the iris and moving anteriorly to cornea the structure’s to be identified and examined are1) Ciliary body band2) Scleral spur3) Functional trabecular meshwork 4) Schwalbe’s line5) Normal blood vessels

Normal Angle Structures

Pupil • It is best to start at the pupil for rapid
orientation • Anterior lens surface is observed for focal
opacification and posterior synechiae• This position is also good for examining
dandruff flake's like exfoliations on the pigment at the posterior edge of pupil – Exfoliation syndrome
• Iridodonesis – to a small extent seen in normal eye and easily observed in pathognomic one

Angle Structures : Iris
• Contour– flat – deep A.C– Convex – shallow A.C. ,
hyperopia
– Concave – high myopia, pigment dispersion synd.
– Abnormal last rolling – plateau iris

Angle Structures : Iris• Site of insertion : while examining the iris care
should be taken in distinguishing the apparent and actual juncture
• This is established by the use of indentation Gonioscopy
• Angulation : It is the angle between iris insertion and slope of the inner cornea in the A.C .( 10⁰)
• Abnormalities : neovascularization, hypoplasia, atrophy

Angle Recess
• Is seen beyond the final roll of iris • At birth – incomplete• 1sr yr of life it firms a concavity into the
anterior surface of the ciliary body

Angle Structures : Ciliary Body band
• This structural portion of ciliary body is visible in the A.C. as a result of iris insertion
• Width depends on level of iris insertion
• Wider in myopes and narrow in hyperopia
• Color: grey to dark brown

Angle Structures : Scleral Spur
• This is the post. Lip of scleral sulcus which is attached to the ciliary body posteriorly and corneo-scleral meshwork anteriorly
• Color : prominent white line

Angle Structures : Scleral Spur
• May be obscured by– Iris process– iris bombe– Peripheral anterior synechiae– pigments

Angle Structures : Trabecular Meshwork
• Pigmented band anterior to scleral spur• Although extent of TMW is from root of iris to
schwalbe’s line it is considered as 2 portionsa) Anterior - between schwalbe’s line and ant. Edge
of schlemm’s cannal• Involved in lesser degree of aqueous out flow
b) Posterior – Functional part , primary site of aqueous out flow• Appearance of funtional TMW depends on
amount of pigmant deposition

Angle Structures : Trabecular Meshwork
• At birth no pigment and with age from faint to dark brown
• Pigment deposition may be homogeneous or irregular
• When lightly pigmented blood reflex in schlemm’s cannal may be seen as a red band

Angle Structures : Schwalbe’s line
• Junction between anterior chamber angle structures and cornea where the descement’s membrane terminates
• Fine ridge ant. to TMW identified by a small built up of pigment
• Landmark for TMW in narrow angle

Angle Structures : Schwalbe’s line


Angle Blood vessels

Differentiating between iris processes and synechiae

Manipulation's
• Sometimes the iridocorneal angle is quite confusing
• Often the angle is difficult to interpret because there is too much or too little angle pigmentation
• In such cases manipulation’s are used for better viewing and diagnosis

Technique for examining difficult angle’s
• Looking over the hill• Corneal wedging• Indentation• Van-Hericks test

Look over the hill
• WHAT ? Sometimes the iris is bowed forward making visualization of the iridocorneal angle quite challenging
• WHERE ? Open angle with iris bowing , cholinergic agents such as pilocarpine
• WHY ? To know weather the angle is occluded or not

Over the Hill Gonioscopy

Corneal Wedge
• WHAT ? When a thin slit of light hits the irido-corneal angle at an angle of 10⁰-15⁰, two light reflections are seen from the external and internal corneal surfaces which pipe down at the sclero-corneal junction (Schwalbe’s line) marking the anterior border of trabecular meshwork

• WHY ? corneal wedge is a useful technique to identify the trabecular meshwork in eyes that are either nonpigmented or excessively pigmented its diff. to mark trabecular meshwork begins
• WHERE ? Young patients where the trabecular meshwork has not yet developed any pigmentation
• WHY ? To diff. wide-open and nonpigmented angle or a totally closed angle where one is looking at the internal cornea.

The Corneal Wedge

The Corneal Wedge

Indentation Gonioscopy
• When iris covers the trabecular meshwork (TM) its easy to mistake:– The non-pigmented TM for scleral spur– Pigmented Schwalbe’s line for TM– Apposition from synechiae
• Indentation Gonioscopy is particularly useful in these cases

Indentation Gonioscopy
• Useful when iris surface is convex– Done when recognition of angle structures is
difficult• Performed in all glaucoma cases– Differentiates appositional vs synechial closure in
pupillary block– Measures extent of angle closure– Identifies plateau iris config.– Identifies lens induced angle closure

Recognition of sites of blockage in angle closure
Pupil block Plateau iris

Indentation Gonioscopy


Indentation Gonioscopy:Synechial closure

Plateau iris configuration
large or anteriorly positioned ciliary processes that push the peripheral iris forward

Indentation : plateau iris

Indentation : cilicary body pseudo-plateau iris


VAN HERICK’S method of cornael thickness as a unit of measure
• WHAT ? The Van Herick test is a slit lamp estimation of the angle depth
• WHY ? To estimate the angle width• WHERE ? In nonpigmented angles it can be
difficult to determine whether the angle is open or closed

Thin bright slit 60⁰ from temporally is brought into cornea until A.C. is located compared with depth of peripheral A.C. If the
depth of the A.C = corneal thickness then it’s a wide open angle
5% 15% 25%
40% 75% 100%

The Speath method


Grading of Angle Width : Shaffer’s


Difficulties in gonioscopy
• Koeppe’s lens: Scleral lip pressing on outer sclera causing narrowing of angle
• Zeiss lens: excessive pressure on central cornea causes angle widening and descement’s folds
• Air or methylcellulose collected on inner surface removed with soap water
• All lenses cleaned with dil.bleach or hydrogen peroxide after use