Go ren,Ole oiteaokiyoaucii sckkc unioelo,aiie,ekui ru ... · Go ren,Ole oiteaokiyoaucii sckkc...
11
Go Green, Go Online to take your course Earn 4 CE credits This course was written for dentists, dental hygienists, and assistants. Methacrylate Based Resin Endodontic Sealers: A Paradigm Shift in Endodontics? A Peer-Reviewed Publication Written by Cornelis H. Pameijer DMD, DSc, PhD; Frederic Barnett DMD; Osvaldo Zmener DDS, Dr Odont and Benjamin Schein DDS, MS This course has been made possible through an unrestricted educational grant from Ultradent Products Inc. The cost of this CE course is $59.00 for 4 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing. PennWell is an ADA CERP recognized provider ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns of complaints about a CE provider may be directed to the provider or to ADA CERP at www.ada.org/goto/cerp.
Transcript of Go ren,Ole oiteaokiyoaucii sckkc unioelo,aiie,ekui ru ... · Go ren,Ole oiteaokiyoaucii sckkc...
Go Green, Go Online to take your course
Earn
4 CE creditsThis course was
written for dentists, dental hygienists,
and assistants.
Methacrylate Based Resin Endodontic Sealers: A Paradigm Shift in Endodontics?A Peer-Reviewed Publication Written by Cornelis H. Pameijer DMD, DSc, PhD; Frederic Barnett DMD; Osvaldo Zmener DDS, Dr Odont and Benjamin Schein DDS, MS
This course has been made possible through an unrestricted educational grant from Ultradent Products Inc. The cost of this CE course is $59.00 for 4 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
PennWell is an ADA CERP Recognized Provider
PennWell is an ADA CERP recognized provider ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.Concerns of complaints about a CE provider may be directed to the provider or to ADA CERP at www.ada.org/goto/cerp.

2 www.ineedce.com
Educational ObjectivesUpon completion of this course, the clinician will be able to do the following:1. Be knowledgeable concerning the introduction of
methacrylate based resin sealers2. Be knowledgeable about leakage studies conducted
on methacrylate based resin sealers and the factors that influence the outcomes of these tests
3. Understand the advantages that methacrylate based resin sealers may offer over other endodontic obturation materials
4. Be knowledgeable about the clinical technique used to place methacrylate based resin sealers
AbstractBonding materials and techniques have completely changed the way dentistry is practiced. Since their in-troduction, techniques have evolved such that it is now possible to bond materials to dentin, and hydrophobic resins have been replaced by hydrophilic resins. In recent years several methacrylate resin-based root canal seal-ers (MBRSs) have been introduced as an alternative to conventional gutta-percha and zinc oxide-eugenol-based techniques. Efforts to introduce a simplified obturation technique based on dentin bonding principles coupled with favorable physical properties have contributed to an increase in interest in using this approach. It is the intent of the authors to critically review the published literature and to arrive at an opinion as to the current status and future of methacrylate based resin sealers. This will be followed by presentations of cases in which methacrylate based resin sealers were used.
IntroductionThe acid etch bonding technique was introduced to dentistry in the mid-1950s by Buonocore1 and was based on resin technology developed by Hagger.2 Bonding materials and techniques have completely changed the way dentistry is practiced. Hydrophobic resins were replaced by hydrophilic materials, and about 30 years of research resulted in a change from using 85% phosphoric acid liquid for 60 seconds to etch enamel to using 35% phosphoric acid gels for 15 seconds for both dentin and enamel. Later, resin-based sealers and different obtura-tion materials were introduced into endodontics.
Before a newly developed material should be used clinically, a series of tests needs to be performed to de-termine its biocompatibility. The currently used meth-acrylate based resin sealers that will be discussed have been tested rigorously, with the exception of clinical prospective studies. They did, however, undergo user evaluation tests. There is a legitimate concern on the part of manufacturers that if a prospective study were to be done — and in endodontics ideally with at least a
5-year postoperative follow-up — the time elapsed from initiation of the project until the final results are obtained would be excessive and counterproductive. Frequently, improvements in materials and changes in techniques are introduced after materials are on the market and are based on clinical feedback from practitioners and data from researchers. The ultimate success can only be determined when a material or technique is used success-fully in clinical practice. Based on their long track record, gutta-percha and zinc oxide-eugenol and other conven-tional sealers should serve as the “gold standard” for a meaningful comparison.
Methacrylate based resin sealersMethacrylate based resin sealers are based on polymer chemistry technology, initially developed for adhesive restorative dentistry. Attention will be focused on two systems: 1. EndoREZ (Ultradent Products Inc. South
Jordan, UT) 2. Epiphany (Pentron Clinical, Wallingford,
CT)/ Resilon
EndoREZ is a hydrophilic, two-component, chemical or dual-curing sealer and contains zinc oxide, barium sul-fate, resins, and pigments in a matrix of urethane dimeth-acrylate. The sealer can be used with gutta-percha or with resin-coated gutta-percha, the latter with the objective of forming a monoblock (Figure 1).
Figure 1. EndoREZ
Early publications, including those of Becce and Pameijer, reported on the biocompatibility and adhesive-ness of EndoREZ, the latter based on its hydrophilic properties.3,4 Subsequently, publications appeared testing the different MBRSs using a variety of techniques, which to a large extent have caused more controversy than that they solved concerns regarding safety and efficacy, and whether they are long-lasting and will ultimately replace gutta-percha and conventional sealers.
Products such as RealSeal (Sybron Dental Specialties, Orange, CA), SimpliFill (LightSpeed Technology Inc., San Antonio, TX) and Resinate (Obtura Spartan, Fenton, MO) are all categorized under Epiphany/Resilon.
Resilon is composed of polymer-based resin (polycap-rolactone), bioactive glass, bismuth oxide, barium sul-fate, and coloring agents. Epiphany contains a dual cure sealer, UDMA, PEGDMA, EBPADMA and BISGMA, barium-borosilicate, BaSO4, bi oxychloride, calcium

www.ineedce.com 3
hydroxide, photo initiators, and a thinning resin. In ad-dition, the system comes with a self-etching primer. The premise behind the material is the formation of a “mono-block” (the primer forms a hybrid layer that bonds to the sealer, which in turn bonds to the Resilon core).
Methacrylate based resins sealers enable obturation in a slightly moist root canal because they are hydrophilic. This hydrophilicity, combined with advanced bonding techniques and a user-friendly methodology (EndoREZ), encourages the formation of deep resin tags extending into the dentinal tubules from the root canals. Deep resin tags help enhance bonding and the clinical success of obturation.
Figure 2. Epiphany/Resilon
Leakage studiesIt is well established that selection of an appropriate sealer will influence the outcome of endodontic therapy.5,6 For that reason many investigators have focused on this im-portant aspect, using techniques such as fluid filtration, dye penetration, and bacterial leakage to test coronal and apical leakage of MBRS. Frequently, AH Plus or AH 26 are used as control materials.
In one of the first published leakage tests using India ink, Zmener and Banegas7 in 2004 reported no statisti-cally significant difference between EndoREZ and AH Plus. Orucoglu et al.,8 using the fluid filtration method, reported that Diaket with cold lateral condensation leaked less apically than EndoREZ and AH Plus did. Neto et al.9 reported that AH Plus leaked less than EndoREZ and AH 26 when using a single cone technique. Adanir et al.10 found that resin-based sealers were more effective than zinc oxide-eugenol in sealing root canals, again using the fluid filtration method. Using similar techniques, Onay et al.11 found that the apical seal of Epiphany and Resilon was not different from those of AH Plus and gutta-percha, AH Plus and Resilon, or Epiphany and gutta-percha. In contrast, Tunga and Bodrumlu12 concluded by means of a fluid-transport method that Epiphany and Resilon leaked significantly less (p<0.05) than gutta-percha and AH 26 did. Stratton et al.13 reached a similar conclusion compar-ing Resilon with gutta-percha and AH Plus. Shipper et
al.14 and Maltezos et al.15 drew similar conclusions using a bacterial leakage test and found that Epiphany and Resilon were superior to gutta-percha and various other sealers. On the other hand, Pitout et al.,16 using bacterial leakage tests as well as a dye penetration method, and Biggs et al.17 did not observe a difference between Resilon and gutta-percha. In summary, there has been no general agreement as to whether or not there is reduced leakage when using MBRSs.
Several authors have used dye penetration to de-termine whether MBRSs are superior to conventional materials. Gernhard et al.18 and Sevimay and Kalayci19 established more dye leakage for EndoREZ than for AH Plus and gutta-percha. Resilon as the main obturation material consistently resulted in less microleakage than gutta-percha at all 3 time intervals — 10 days and 1 and 3 months.20 An explanation for this difference between the two materials will follow later.
Toxicology studies Dental materials must be biocompatible. Cytotoxicity studies have been conducted by numerous investigators. As in the leakage studies, the results of in vitro studies vary among investigators. Huang et al.21 showed that the elution compounds from MBRS, zinc oxide-eugenol, and calcium hydroxide-based sealers were cytotoxic to pri-mary human PDL cultures and V79 cells, with calcium hydroxide being the least toxic. Also, according to Huang and co-workers,22 the highest level of DNA damage was induced by MBRSs, in this case Topseal, AH 26, and AH Plus. Koulaouzidou et al.23 demonstrated similar results — AH 26 had a severe cytotoxic effect, while Topseal and AH Plus had a markedly lower effect. This was further supported by Bouillaguet et al.24 who reported that “most materials pose significant cytotoxic risks and that cytotoxicity generally increased with time.” At 72 hours, GuttaFlow became significantly less toxic than AH Plus, Epiphany sealer, and Resilon. Key et al.25 determined Epiphany to be less toxic than Grossman’s sealer, while Epiphany was more cytotoxic than Sealapex after 1 hour, but less after 24 hours. Epiphany was more cytotoxic than conventional materials were. Eldeniz et al.26 reported similar findings. Based on the findings of these authors, it appears that not one sealer is universally accepted as being non-toxic. Controversy regarding the reaction of materials exposed to certain test conditions is not new. With the introduction of glass ionomer cements, tissue culture tests reported toxicity when they were placed in direct contact with the medium.27,28,29 However, after elution of irritating chemicals, the reaction subsided over time.
The early toxicology studies of EndoREZ by Louw, Becce, and Pameijer reported that EndoREZ was mildly irritating, yet within acceptable standards. This has been

4 www.ineedce.com
supported by more recent studies by Pameijer, Zmener, and Banegas.
Based on testing, EndoREZ was determined to be bio-compatible and was introduced to the dental profession.
The role of moistureThe data from several of the leakage studies are most likely the result of the ingrained belief that after a final rinse root canals need to be dried thoroughly. Statements in materials and methods sections of papers such as “the canals were dried”17,30 set the stage for a hydrophobic environment while a hydrophilic material is being used. For methacrylate based resin sealers, whether EndoREZ or to a lesser extent Epiphany, to establish a proper seal the dentin needs to be moist to allow for the penetration of resin tags in the opened dentinal tubules, thus taking advantage of the hydrophilicity of the bonding agent or sealer. In the case of EndoREZ, this allows for deep penetration of resin tags, up to 500 µm or more, and for Epiphany allows bonding of the adhesive by means of a hybrid layer to the dentin.
Zmener et al.31 studied four scenarios of dentin wetness/dryness for apical and coronal dye leakage us-ing methylene blue. In Group 1, 95% ethanol was used followed by paper points to dry the canals. In Group 2, the canals were blot dried with several paper points. In Group 3, a luer vacuum adaptor with low vacuum for 5 seconds followed by one paper point for only 1–2 seconds was used. In Group 4, the root canal remained flooded, and no effort was made to remove excess distilled water. It was theorized that perhaps the hydrophilic properties of EndoREZ with the scenario in Group 4 would dis-place excess water. EndoREZ and Epiphany/Resilon in Groups 2 and 3 exhibited significantly less coronal and apical leakage (p<0.05) than was seen in Groups 1 and 4. The method with a low vacuum luer adaptor and 1–2 s paper point drying (Group 3) scored the lowest leakage. There was no statistically significant difference between EndoREZ and Epiphany/Resilon.
One of the reasons that Epiphany/Resilon has per-haps scored better results in leakage studies is based on the Epiphany/Resilon system’s use of a dentin bonding agent, which makes the moisture condition of root dentin less critical. This statement can be underscored by the study of Gillespie et al. They reported less leakage for EndoREZ when a dual-cured two-step self-etch adhesive was used,32 and statistically significant differences in fill-ing techniques. EndoREZ alone exhibited significantly higher overall leakage, while no difference was found between AH Plus and the EndoREZ modified technique using a dentin bonding agent. Leakage studies that state in their materials and methods sections that “the canals were dried with paper points” have generated data with questionable validity, as the methodology is flawed. Field
Emission Scanning Electron Microscopy (FESEM) and scanning electron microscopy (SEM) demonstrate the potential of EndoREZ when proper moist conditions are adhered to and the recommended insertion technique is followed, as well as what happens when the canal is dried according to well-established endodontic techniques us-ing paper points.
Work by Lambrechts et al.33 in 2006 using FESEM showed convincingly the excellent hydrophilic penetra-tion potential of EndoREZ when applied to moist dentin. They placed teeth in HCl for 30 hours followed by 2% NaOCl for 10 minutes and a distilled water rinse to dis-solve the dentin. Resin tag bundles protruding from the root canal filling surface and extending from 400 to 600 µm or more were seen using FESEM (Figure 3). Due to their length and weight these bundles bent parallel to the root filling surface. In view of the ability to penetrate the dentinal tubules to the extent shown in this study, a bonding agent in conjunction with EndoREZ does not seem to offer any benefits. It may actually be detrimental, as the sealer can only bond to the resin of the bonding agent without resin tag bundle formations.
Figure 3. FESEMicrograph of extruded resin tags
The foreground shows fractured resin tags (due to polymerization shrinkage) or resin tags that have partially entered the dentinal tubules. Image courtesy of Lambrechts et al.
In contrast, inserting EndoREZ with a gutta-percha point into a dried root canal produces poor adaptation of the sealer to dentin with a lack of resin tag formation.
The resin will simply not be able to penetrate the dentinal tubules, setting the stage for excessive leakage, which is solely operator induced. This explains the con-siderable leakage reported in leakage studies in which the dentin was dried before insertion of the sealer.
Oxygen inhibited layer During biocompatibility studies, specimen preparation of methacrylate based resin sealers can result in the for-mation of an “oxygen inhibited layer.” Resin, whether chemical, light, or dual cured, does not polymerize when in contact with air. That is not to say that polymerized

www.ineedce.com 5
sealers cannot cause irritation. Conversion of monomer in a typical polymerization reaction is at best less than 50–70%.34 Oxygen left behind from NaOCL inhibits po-lymerization. Therefore, it is of importance to thoroughly flush the root canal with EDTA after the use of NaOCL, followed by sterile saline or 2% chlorhexidine (Consepsis, Ultradent Products Inc.).
Clinical evidenceOne long-term study on EndoREZ has been reported (Zmener and Pameijer35,36) and one intermediate clinical study on Epiphany/Resilon (Debelian37). In a retrospec-tive study on 180 patients,35 a total of 295 root canals were treated with laterally condensed gutta-percha cones in conjunction with EndoREZ. Root canal therapy was carried out in one visit using standardized techniques. The results were assessed clinically and radiographi-cally 14 to 24 months postoperatively and compared to baseline radiographs. Parameters for success were based on absence of clinical symptoms, a normal or slightly widened periodontal ligament, and reduction of periapi-cal radiolucencies with an absence of pain in patients who had pre-existing lesions associated with pain. After 2 years, the overall success rate was 91.03%. In a subse-quent 5-year follow-up,36 129 of the patients responded to a recall request. Root canals had been adequately filled to the working length in 92 teeth (76.66%) and short in 13 (10.83%). Fifteen cases (12.50%), filled flush at the initiation of the experiment, showed slight resorption of the filling material at the apex within the lumen of the root canal. Of the 10 roots with extrusion, none had ra-diographic evidence of sealer in the periradicular tissues after 5 years. All patients were free of clinical symptoms. A life table analysis revealed a cumulative probability of success of 86.3% at the 5-year recall with a 95% confi-dence interval of 79.7%–91.0%. This percentage compares well with what has been reported in the literature for other sealers.38,39
In a 2-year prospective study on Resilon/Epiphany re-ported by Debelian,37 a total of 67 vital teeth were treated in one visit and 53 necrotic pulps in 2 visits (n=120). Af-ter 2 years, 108 cases were evaluated. Using the mean of the Periapical Index Scores (PAI) of three evaluators, the results can be interpreted as follows. When the PAI 1 and 2 were combined (1=healed; 2=healing), success after 24 months was 91.6%. It is of interest to note that the results reported by Zmener and Pameijer35 after 24 months using EndoREZ were almost the same, 91.3%. It appears that after 2 years the materials performed similarly in spite of different clinical protocols and different operators. If we exclude all experiments that have a flawed specimen preparation technique, in particular the drying of dentin, then MBRSs appear to perform like conventional root canal sealers.
Do methacrylate based resin sealers reinforce roots?A comparison of intraradicular dentin bond strength between Epiphany/Resilon and gutta-percha/Kerr Pulp Canal Sealer EWT, using a push-out test, demonstrated that the mean bond strength of the Epiphany/Resilon group was significantly higher (p<0.05) (Skidmore et al.40). Teixeira et al.41 also reported higher fracture loads for MBRS than gutta-percha; however, no statistical significance was established. The lack of reinforcement was further refuted by Ungor et al.42 by testing dentin root cylinders with AH Plus + gutta-percha, AH Plus + Resilon, Epiphany + Resilon, Epiphany + gutta-percha, and gutta-percha alone. They concluded that the Epiph-any-Resilon combination was not superior to that of the AH Plus/gutta-percha. Using a similar dentin cylinder protocol to optimize standardization, Grande et al.48 ar-rived at a similar conclusion. The flexural properties of Resilon and gutta-percha are too low to reinforce roots. Although supportive of the results of Grande et al.,43 the data of Gesi et al.44 cannot be accepted as valid since these researchers dried the debrided root canals with multiple paper points. Also, for Epiphany/Resilon the manufac-turer’s instructions for use clearly recommend the dentin be moist. Additional criticism has been leveled at the choice of the push-through test, variation in specimen thickness, analysis of the data, etc. (Leinfelder45).
Retreatment of methacrylate based resin sealersThe ability to retreat endodontically treated teeth is one of the requirements of a root canal sealer. According to de Oliveira et al.46 and Ezzie and co-workers,47 compared to gutta-percha and AH Plus, Epiphany/Resilon could be removed faster and demonstrated less residual filling material when K3 files46 or ProFile 0.06 combined with heat and chloroform47 were used.
Methacrylate based resin sealers: Clinical techniqueSeveral methacrylate based resin sealers available to the dental profession. The product used for the technique in the cases that are presented is EndoREZ, which is one of these. EndoREZ is a suitable endodontic sealer for most obturation techniques.
After canal instrumentation and disinfection, all anti-microbial rinses and agents should be thoroughly removed and rinsed from the canal. Do not desiccate the canal with multiple paper points. The hydrophilic nature of EndoREZ allows the clinician to use just 1–2 paper points, which leaves a small amount of moisture inside the canal. This small amount of moisture is actually ben-eficial when using EndoREZ since the material actively seeks the moisture deep into dentinal tubules and lateral
6 www.ineedce.com
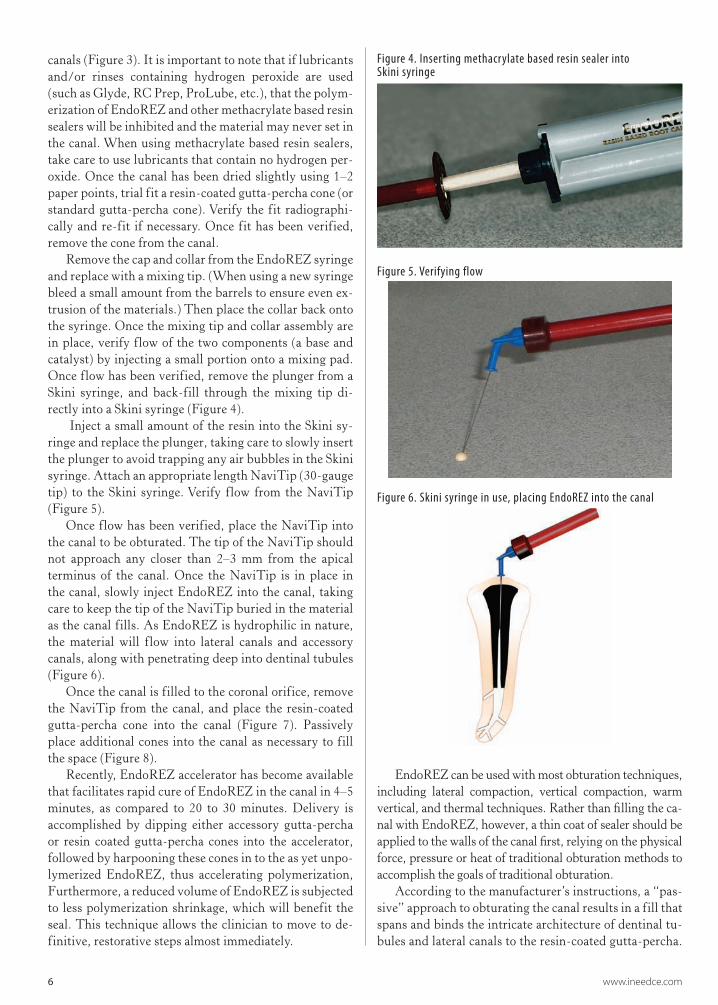
canals (Figure 3). It is important to note that if lubricants and/or rinses containing hydrogen peroxide are used (such as Glyde, RC Prep, ProLube, etc.), that the polym-erization of EndoREZ and other methacrylate based resin sealers will be inhibited and the material may never set in the canal. When using methacrylate based resin sealers, take care to use lubricants that contain no hydrogen per-oxide. Once the canal has been dried slightly using 1–2 paper points, trial fit a resin-coated gutta-percha cone (or standard gutta-percha cone). Verify the fit radiographi-cally and re-fit if necessary. Once fit has been verified, remove the cone from the canal.
Remove the cap and collar from the EndoREZ syringe and replace with a mixing tip. (When using a new syringe bleed a small amount from the barrels to ensure even ex-trusion of the materials.) Then place the collar back onto the syringe. Once the mixing tip and collar assembly are in place, verify flow of the two components (a base and catalyst) by injecting a small portion onto a mixing pad. Once flow has been verified, remove the plunger from a Skini syringe, and back-fill through the mixing tip di-rectly into a Skini syringe (Figure 4).
Inject a small amount of the resin into the Skini sy-ringe and replace the plunger, taking care to slowly insert the plunger to avoid trapping any air bubbles in the Skini syringe. Attach an appropriate length NaviTip (30-gauge tip) to the Skini syringe. Verify flow from the NaviTip (Figure 5).
Once flow has been verified, place the NaviTip into the canal to be obturated. The tip of the NaviTip should not approach any closer than 2–3 mm from the apical terminus of the canal. Once the NaviTip is in place in the canal, slowly inject EndoREZ into the canal, taking care to keep the tip of the NaviTip buried in the material as the canal fills. As EndoREZ is hydrophilic in nature, the material will flow into lateral canals and accessory canals, along with penetrating deep into dentinal tubules (Figure 6).
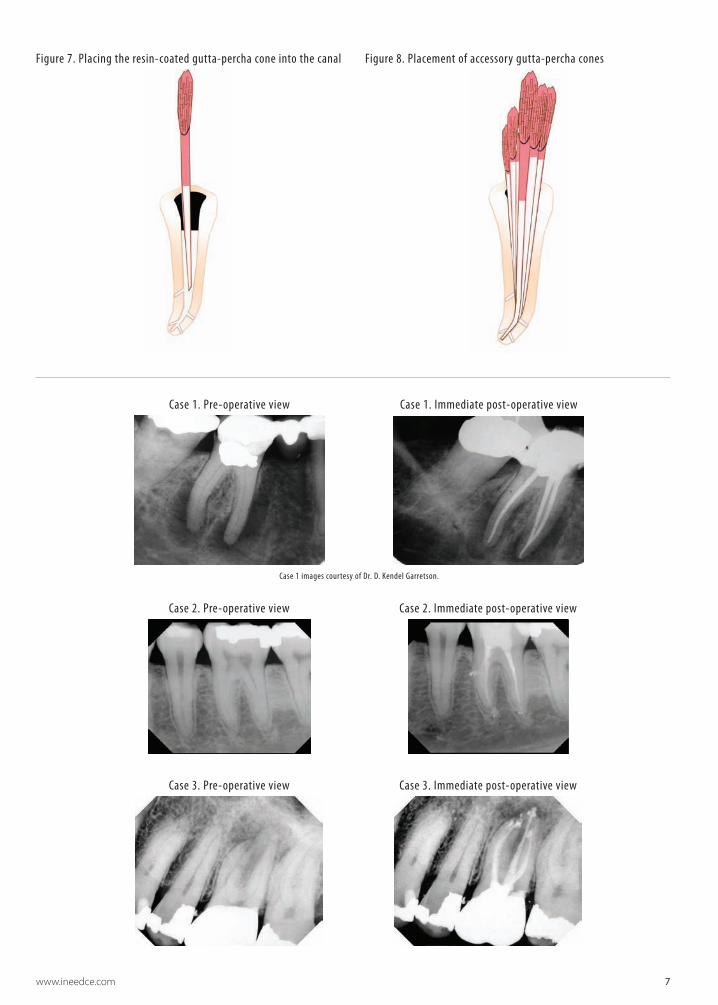
Once the canal is filled to the coronal orifice, remove the NaviTip from the canal, and place the resin-coated gutta-percha cone into the canal (Figure 7). Passively place additional cones into the canal as necessary to fill the space (Figure 8).
Recently, EndoREZ accelerator has become available that facilitates rapid cure of EndoREZ in the canal in 4–5 minutes, as compared to 20 to 30 minutes. Delivery is accomplished by dipping either accessory gutta-percha or resin coated gutta-percha cones into the accelerator, followed by harpooning these cones in to the as yet unpo-lymerized EndoREZ, thus accelerating polymerization, Furthermore, a reduced volume of EndoREZ is subjected to less polymerization shrinkage, which will benefit the seal. This technique allows the clinician to move to de-finitive, restorative steps almost immediately.
EndoREZ can be used with most obturation techniques, including lateral compaction, vertical compaction, warm vertical, and thermal techniques. Rather than filling the ca-nal with EndoREZ, however, a thin coat of sealer should be applied to the walls of the canal first, relying on the physical force, pressure or heat of traditional obturation methods to accomplish the goals of traditional obturation.
According to the manufacturer’s instructions, a “pas-sive” approach to obturating the canal results in a fill that spans and binds the intricate architecture of dentinal tu-bules and lateral canals to the resin-coated gutta-percha.
Figure 4. Inserting methacrylate based resin sealer into Skini syringe
Figure 5. Verifying flow
Figure 6. Skini syringe in use, placing EndoREZ into the canal
www.ineedce.com 7
Case 2. Pre-operative view Case 2. Immediate post-operative view
Case 3. Pre-operative view Case 3. Immediate post-operative view
Case 1. Pre-operative view Case 1. Immediate post-operative view
Case 1 images courtesy of Dr. D. Kendel Garretson.
Figure 7. Placing the resin-coated gutta-percha cone into the canal Figure 8. Placement of accessory gutta-percha cones

8 www.ineedce.com
After the gutta-percha cones have been placed, use a heat element to sear off any loose ends.
Successful obturation is obtained using the above technique, as demonstrated by the cases.
Discussion and future expectationsThe clinical success rates that have been reported for both EndoREZ and Epiphany/Resilon are in agreement with success rates in previous studies using conventional sealers and gutta-percha (Ørstavik et al.48; Ausburger and Peters49; Friedman et al.50).
In addition, EndoREZ and Epiphany are well toler-ated and can be considered biocompatible. Extensive use by the dental profession has proven this to be true.
Technique modifications and new techniques will continue to be developed, and new sealers, currently under development, will appear on the market within a few years. It can be anticipated that methacrylate based resin sealers will continue to improve their appeal to the dental profession.
References1. Buonocore MG. A simple method of increasing the
adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955 Dec;34(6):849–53.
2. Hagger, O.3. Becce C and Pameijer CH. SEM study of a new
endodontic root canal sealer. J Dent Res. AADR Issue 79, Abstract #866, 2001.
4, Becce C and Pameijer CH. Biocompatibility of a new endodontic sealer. J Dent Res. 81, IADR Special Issue, Abstract #2483, page B-321, 2003.
5. Spangberg LSW. In vitro assessment of the toxicity of endodontic materials. Int Endod J. 1981;14:27–34.
6. Ørstavik D, Kerekes K, Eriksen HM. Clinical performance of three endodontic sealers. Endod Dent Traumatol. 1987;3:178–186.
7. Zmener O, Banegas G. Apical leakage of endodontic sealers. Endod Pract. 2004;7:31–23.
8. Orucoglu H, Sengun A, Yilmaz N. Apical leakage of resin based root canal sealers with a new computerized fluid filtration meter. J Endod. 2005 Dec;31(12):886–90.
9. Neto UX, de Moraes IG, Westphalen VP, Menezes R, Carneiro E, Fariniuk LF. Leakage of 4 resin-based root-canal sealers used with a single-cone technique. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007 May 22.
10. Adanir N, Cobankara FK, Belli S. Sealing properties of different resin-based root canal sealers. J Biomed Mater Res B Appl Biomater. 2006 Apr;77(1):1–4.
11. Onay EO, Ungor M, Orucoglu H. An in vitro evaluation of the apical sealing ability of a new resin-based root canal obturation system. J Endod. 2006 Oct;32(10):976–8. Epub 2006 Jul 10.
12. Tunga U, Bodrumlu E. Assessment of the sealing ability of a new root canal obturation material. J Endod. 2006 Sep;32(9):876–8.
13. Stratton RK, Apicella MJ, Mines P. A fluid filtration comparison of gutta-percha versus Resilon, a new soft resin endodontic obturation system. J Endod. 2006 Jul;32(7):642–5.
14. Shipper G, Ørstavik D, Teixeira FB, Trope M. An evaluation of microbial leakage in roots filled with a
thermoplastic synthetic polymer-based root canal filling material (Resilon). J Endod. 2004 May;30(5):342–7.
15. Maltezos C, Glickman GN, Ezzo P, He J. Comparison of the sealing of Resilon, Pro Root MTA, and Super-EBA as root-end filling materials: a bacterial leakage study. J Endod. 2006 Apr;32(4):324–7.
16. Pitout E, Oberholzer TG, Blignaut E, Molepo J. Coronal leakage of teeth root-filled with gutta-percha or Resilon root canal filling material. J Endod. 2006 Sep;32(9):879–81.
17. Biggs SG, Knowles KI, Ibarrola JL, Pashley DH. An in vitro assessment of the sealing ability of Resilon/Epiphany using fluid filtration. J Endod. 2006 Aug;32(8):759–61.
18. Gernhardt CR, Kruger T, Bekes K, Schaller HG. Apical sealing ability of 2 epoxy resin-based sealers used with root canal obturation techniques based on warm gutta-percha compared to cold lateral condensation. Quintessence Int. 2007 Mar;38(3):229–34.
19. Sevimay S, Kalayci A. Evaluation of apical sealing ability and adaptation to dentine of two resin-based sealers. J Oral Rehabil. 2005 Feb;32(2):105–10.
20. Aptekar A, Ginnan K. Comparative analysis of microleakage and seal for 2 obturation materials: Resilon/Epiphany and gutta-percha. J Can Dent Assoc. 2006 Apr;72(3):245.
21. Huang FM, Tai KW, Chou MY, Chang YC. Cytotoxicity of resin-, zinc oxide-eugenol-, and calcium hydroxide-based root canal sealers on human periodontal ligament cells and permanent V79 cells. Int Endod J. 2002 Feb;35(2):153–8.
22. Huang TH, Lee H, Kao CT. Evaluation of the genotoxicity of zinc oxide eugenol-based, calcium hydroxide-based, and epoxy resin-based root canal sealers by comet assay. J Endod. 2001 Dec;27(12):744–8.
23. Koulaouzidou EA, Papazisis KT, Beltes P, Geromichalos GD, Kortsaris AH. Cytotoxicity of three resin-based root canal sealers: an in vitro evaluation. Endod Dent Traumatol. 1998 Aug;14(4):182–5.
24. Bouillaguet S, Wataha JC, Tay FR, Brackett MG, Lockwood PE. Initial in vitro biological response to contemporary endodontic sealers. J Endod. 2006 Oct;32(10):989–92. Epub 2006 Jul 26
25. Key JE, Rahemtulla FG, Eleazer PD. Cytotoxicity of a new root canal filling material on human gingival fibroblasts. J Endod. 2006 Aug;32(8):756–8.
26. Eldeniz AU, Mustafa K, Ørstavik D, Dahl JE. Cytotoxicity of new resin-, calcium hydroxide- and silicone-based root canal sealers on fibroblasts derived from human gingiva and L929 cell lines. Int Endod J. 2007 May;40(5):329–37.
27. Hume WR, Mount GJ. In vitro studies on the potential for pulpal cytotoxicity of glass-ionomer cements. J Dent Res. 1988 Jun;67(6):915–8.
28. Doherty PJ. Biocompatibility evaluation of glass ionomer cement using cell culture techniques. Clin Mater. 1991;7(4):335–40.
29. Schedle A, Franz A, Rausch-Fan X, Spittler A, Lucas T, Samorapoompichit P, Sperr W, Boltz-Nitulescu G. Cytotoxic effects of dental composites, adhesive substances, compomers and cements. Dent Mater. 1998 Nov;14(6):429–40.
30. Kardon BP, Kuttler S, Hardigan P, Dorn SO. An in vitro evaluation of the sealing ability of a new root-canal-obturation system. J Endod. 2003;29(10);658–61.
31. Zmener O, Alvarez Serrano S, Vidueira M, Macchi R, Pameijer CH. Coronal and apical leakage with two resin-based sealers under different root canal moisture conditions. Submitted for publication 2007.
32. Gillespie WT, Loushine RJ, Weller RN, Mazzoni A, et al. Improving the performance of EndoREZ root canal
www.ineedce.com 9
sealer with a dual-cured two-step self-etch adhesive. II. Apical and coronal seal. J Endod. 2006;32:771–5.
33. Lambrechts P, Van Meerbeek B, Bergmasn L, Moisiadsis P. Unpublished data, 2006.
34. Kildal KK, Ruyter IE. How different curing methods affect the degree of conversion of resin-based inlay/onlay materials. Acta Odontol Scand. 1994 Oct;52(5):315–22.
35. Zmener O and Pameijer CH. Clinical and radiographic evaluation of a Resin-based root canal sealer. Am J Dent. 2004;17:19–22.
36. Zmener O and Pameijer CH. Clinical and radiographical evaluation of a resin-based root canal sealer: A 5-year follow-up. J Endod. 2007;33:676–9.
37. Debelian G. Treatment outcome of teeth treated with an evidence-based disinfection protocol and filled with Resilon. J Endod. 2006;32: Abstract #PR4.
38. Swartz DB, Skidmore AE, Griffin JA. Twenty years of endodontic success and failure. J Endod. 1983;9:198–202.
39. Ørstavik D, Kerekes K, Eriksen HM. Clinical performance of three endodontic sealers. Endod Dent Traumatol. 1987;3:178–86.
40. Skidmore LJ, Berzins DW, Bahcall JK. An in vitro comparison of the intraradicular dentin bond strength of Resilon and gutta-percha. J Endod. 2006 Oct;32(10):963–6.
41. Teixeira FB, Teixeira EC, Thompson JY, Trope M. Fracture resistance of roots endodontically treated with a new resin filling material. J Am Dent Assoc. 2004 May;135(5):646–52.
42. Ungor M, Onay EO, Orucoglu H. Push-out bond strengths: the Epiphany-Resilon endodontic obturation system compared with different pairings of Epiphany, Resilon, AH Plus and gutta-percha. Int Endod J. 2006 Aug;39(8):643–7.
43. Grande NM, Lavorgna L, Ioppolo P, Bedini R, Pameijer CH, Somma F. Influence of different root canal filling materials on the mechanical properties of root canal dentin. J Endod. 2007;33:859–64.
44. Gesi A, Raffaelli O, Goracci C, Pashley DH, Tay FR, Ferrari M. Interfacial strength of Resilon and gutta-percha to intraradicular dentin. J Endod. 2005 Nov;31(11):809–13.
45. Leinfelder KF. A critical analysis of recent research on Resilon obturation material.
46. de Oliveira DP, Barbizam JV, Trope M, Teixeira FB. Comparison between gutta-percha and Resilon removal using two different techniques in endodontic retreatment. J Endod. 2006 Apr;32(4):362–4.
47. Ezzie E, Fleury A, Solomon E, Spears R, He J. Efficacy of retreatment techniques for a resin-based root canal obturation material. J Endod. 2006 Apr;32(4):341–4.
48. Ørstavik D, Kerekes K, Eriksen HM. Clinical performance of three endodontic sealers. Endod Dent Traumatol. 1987;3:178–86.
49. Ausburger RA, Peters DD. Radiographic evaluation of extruded obturation materials. J Endod 1990;16:492–7.
50. Friedman S, Lost C, Zarrabian M, Trope M. Evaluation of success and failure after endodontic therapy using a glass ionomer cement sealer. J Endod. 1995;21:384–90.
Author Profiles
Cornelis H. Pameijer, DMD, MScD, DSc, PhDDr. Pameijer earned his dental degrees from the University of Utrecht in The Netherlands and Boston University, Boston, MA. In addition, he holds a PhD from the University of Lund in Sweden, as well as an MScD, DSc, and Certificate of Advanced Graduate
studies in Prosthodontics, from Boston University. Dr. Pameijer is currently Professor Emeritus at the Univer-sity of Connecticut, Farmington, CT. Dr. Pameijer has published over 200 publications in mostly peer reviewed journals and is on the editorial board of many scientific journals. He has lectured extensively nationally and in-ternationally in Europe, Asia, North and South America and Africa. Dr.Pameijer is currently a consultant for sev-eral American and European companies and spends his time doing research, writing publications, lecturing and one day private practice.
Dr. Frederic BarnettDr. Frederic Barnett, DMD is the Chairman and Direc-tor, IB Bender Division of Postdoctoral Endodontics at the Albert Einstein Medical Center in Philadelphia, PA.
Dr. Osvaldo Zmener DDSDr. Osvaldo Zmener DDS, Dr Odont is Head Professor of the Post Graduate Program for Specialized Endodontics, Faculty of Medical Sciences at the School of Dentistry, University of El Salvador, Buenos Aires, Argentina.
Dr. Benjamin Schein, DDS, MSDr. Benjamin Schein, DDS, MS is an endodontist in pri-vate practice in Las Vegas, NV.
DisclaimerThe authors of this course have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
Reader FeedbackWe encourage your comments on this or any PennWell course. For your convenience, an online feedback form is available at www.ineedce.com.
10 www.ineedce.com
Questions
1. The acid-etch bonding technique was based on resin technology developed by _______. a. Haggerb. Blackc. Simonsend. none of the above
2. Hydrophobic resins have been replaced by hydrophilic materials.a. Trueb. False
3. When acid-etch bonding techniques were first used in dentistry, they used _____ for _____ to etch _____. a. 35% phosphoric acid; 60 seconds; enamel
and dentinb. 35% phosphoric acid; 60 seconds; enamelc. 85% phosphoric acid; 60 seconds; enameld. none of the above
4. Frequently, improvements in materials and changes in techniques are intro-duced after materials are on the market and are based on clinical feedback from practitioners and data from researchers.a. Trueb. False
5. The primer used with Epiphany _____. a. is self-etchingb. forms a hybrid layer that bonds to the sealer c. is a pure white color upon visual examinationd. a and b
6. EndoREZ _____.a. is hydrophilicb. contains zinc oxidec. can be used with gutta-percha or resin-coated
gutta-perchad. all of the above
7. Resilon’s composition includes _____.a. barium sulfateb. polymer-based resinc. calcium hydroxided. all of the above
8. Many investigators have focused on the selection of a sealer because _____.a. this is an easy thing to studyb. manufacturers of gutta-percha have
mandated thisc. selection of an appropriate sealer will influence
the outcome of endodontic therapyd. all of the above
9. Techniques used to investigate sealers, and addressed in this paper, have included iontophoresis.a. Trueb. False
10. Using fluid filtration methods, Orucoglu et al. as well as Adanir et al. reported that EndoREZ leaked more than zinc oxide–eugenol did. a. Trueb. False
11. Huang et al. found in cytotoxicity tests that _____ was the least toxic.a. calcium hydroxideb. calcium sulfitec. sodium perborated. none of the above
12. Early toxicology studies by Louw, Becce, and Pameijer and later studies by Pameijer, Zmener, and Banegas have found EndoREZ to be mildly irritating and within acceptable standards. a. Trueb. False
13. The data from several of the leakage studies discussed in this article are most likely the result of the ingrained belief that _____.a. after a final rinse, root canals must be treated
with EDTAb. after a final rinse, root canals need to be
dried thoroughlyc. before a final rinse, root canals need to be etchedd. a and c
14. For methacrylate based resin sealers, to establish a proper seal the dentin needs to be _____ to allow for the _____. a. dry; penetration of resin tags in the closed
dentinal tubulesb. moist; penetration of resin tags in the closed
dentinal tubulesc. moist; penetration of resin tags in the opened
dentinal tubulesd. none of the above
15. Leaving dentin moist prior to using EndoREZ sealer _____.a. allows for permutation of resin tagsb. enables deep penetration of resin tags up to 50 μmc. enables deep penetration of resin tags up to
500 μmd. a and c
16. Leaving dentin moist prior to using Epiphany _____.a. enables deep penetration of resin tags into
the cementumb. enables bonding of the adhesive by means of a
hybrid layer to the dentinc. enables bonding of the adhesive by means of a
hybrid later to the cementumd. a and c
17. EndoREZ and Epiphany both use a dentin bonding agent.a. Trueb. False
18. According to the article, the meth-odology of leakage studies that state in their materials and methods sections that “the canals were dried with paper points” is _____ .a. appropriateb. correctc. flawedd. a and b
19. Using FESEM, Lambrechts et al. showed resin tag bundles protruding from the root canal filling surface and extending _____ after EndoREZ was used as a sealer.a. from 200 to 400 μm b. from 400 to 600 μmc. from 500 to 700 μm d. none of the above
20. Resin does not polymerize when in contact with air.a. Trueb. False
21. It is important to thoroughly flush the root canal with EDTA after the use of NaOCl, followed by sterile saline or 2% chlorhexidine because_____.a. this helps EDTA form a bond with the resinb. oxygen left behind from NaOCL promotes
polymerization, thus forming an oxygen-inhibited layer
c. oxygen left behind from NaOCL inhibits polym-erization, thus forming an oxygen-inhibited layer
d. a and b
22. In a retrospective study on 180 patients, where EndoREZ was used as the root canal sealer, _____.a. after 2 years, the overall success rate was 91.03%b. after 5 years, all patients evaluated were free of
clinical symptoms c. a and bd. none of the above
23. The ability to re-treat endodontically treated teeth is one of the requirements of a root canal sealer.a. Trueb. False
24. Compared to gutta-percha and AH Plus, one study found that a methacry-late based resin sealer (Epiphany/Resi-lon) could be removed faster and with less residual filling material.a. Trueb. False
25. Leaving a small amount of moisture in root canals after final rinsing is ben-eficial for methacrylate resin–based sealers _____.a. due to the hydrophobic nature of the sealerb. due to the hydrophilic nature of the sealerc. due to the poor porosity of dentind. none of the above
26. Use of lubricants and/or rinses contain-ing hydrogen peroxide will _______.a. promote demineralizationb. promote polymerization of methacrylate based
resin sealersc. inhibit polymerization of methacrylate based
resin sealersd. a and c
27. EndoREZ will flow into lateral canals and accessory canals because it is _____.a. hydrophobicb. hydrophilicc. thinner in viscosity than waterd. a and c
28. A resin-coated gutta-percha point should be placed in the root canal prior to placing any methacrylate based resin sealer in the canal.a. Trueb. False
29. An accelerator is available and _____.a. speeds up setting of EndoREZb. should be placed in the canal prior to
placing sealerc. should be coated on accessory gutta-percha points
prior to placing these in the canald. a and c
30. Both EndoREZ and Epiphany/Resilon _____.a. are well-tolerated and biocompatibleb. have been extensively used by the
dental professionc. have been studied and found to have clinical
success rates in agreement with success rates using conventional sealers and gutta-percha
d. all of the above
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
For immediate results, go to www.ineedce.com and click on the button “take tests Online.” answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
�Payment of $59.00 is enclosed. (Checks and credit cards are accepted.)
If paying by credit card, please complete the following: MC Visa AmEx Discover
Acct. Number: _______________________________
Exp. Date: _____________________
Charges on your statement will show up as PennWell
Mail completed answer sheet to
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O. Box 116, Chesterland, OH 44026 or fax to: (440) 845-3447
Educational Objectives1. Be knowledgeable concerning the introduction of resin-based sealers
2. Be knowledgeable about leakage studies conducted on resin-based sealers and the factors that influence the outcomes
of these tests
3. Understand the advantages that resin-based sealers may offer over other endodontic obturation materials
4. Be knowledgeable about the clinical technique used to place resin-based sealers
Course EvaluationPlease evaluate this course by responding to the following statements, using a scale of Excellent = 5 to Poor = 0.
1. Were the individual course objectives met? Objective #1: Yes No Objective #3: Yes No
Objective #2: Yes No Objective #4: Yes No
2. To what extent were the course objectives accomplished overall? 5 4 3 2 1 0
3. Please rate your personal mastery of the course objectives. 5 4 3 2 1 0
4. How would you rate the objectives and educational methods? 5 4 3 2 1 0
5. How do you rate the author’s grasp of the topic? 5 4 3 2 1 0
6. Please rate the instructor’s effectiveness. 5 4 3 2 1 0
7. Was the overall administration of the course effective? 5 4 3 2 1 0
8. Do you feel that the references were adequate? Yes No
9. Would you participate in a similar program on a different topic? Yes No
10. If any of the continuing education questions were unclear or ambiguous, please list them.
___________________________________________________________________
11. Was there any subject matter you found confusing? Please describe.
___________________________________________________________________
___________________________________________________________________
12. What additional continuing dental education topics would you like to see?
___________________________________________________________________
___________________________________________________________________
ANSWER SHEET
Methacrylate Based Resin Endodontic Sealers: A Paradigm Shift in Endodontics?
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP:
Telephone: Home ( ) Office ( )
Requirements for successful completion of the course and to obtain dental continuing education credits: 1) Read the entire course. 2) Complete all information above. 3) Complete answer sheets in either pen or pencil. 4) Mark only one answer for each question. 5) A score of 70% on this test will earn you 4 CE credits. 6) Complete the Course Evaluation below. 7) Make check payable to PennWell Corp.
AGD Code 074
AUTHOR DISCLAIMERThe authors of this course have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
SPONSOR/PROVIDERThis course was made possible through an unrestricted educational grant from Ultradent Products Inc. No manufacturer or third party has had any input into the development of course content. All content has been derived from references listed, and or the opinions of clinicians. Please direct all questions pertaining to PennWell or the administration of this course to Machele Galloway, 1421 S. Sheridan Rd., Tulsa, OK 74112 or [email protected].
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification forms will be mailed within two weeks after taking an examination.
EDUCATIONAL DISCLAIMERThe opinions of efficacy or perceived value of any products or companies mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of PennWell.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
COURSE CREDITS/COSTAll participants scoring at least 70% (answering 21 or more questions correctly) on the examination will receive a verification form verifying 4 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 3274. The cost for courses ranges from $49.00 to $110.00.
Many PennWell self-study courses have been approved by the Dental Assisting National Board, Inc. (DANB) and can be used by dental assistants who are DANB Certified to meet DANB’s annual continuing education requirements. To find out if this course or any other PennWell course has been approved by DANB, please contact DANB’s Recertification Department at 1-800-FOR-DANB, ext. 445.
RECORD KEEPINGPennWell maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
© 2008 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
www.ineedce.com 11