Tjänstens grammatik och retorik - om utvecklingen av Burkes pentad ...
Journal of The Association of Physicians of India ■ Vol. 65 ■ July 201768
Glycemic PentadGlycemic Pentad Forum
Glycemic Pentad Forum (see page no. 79)Received: 29.05.2017; Accepted: 04.06.2017
C O N S E N S U S S T A T E M E N T
AbstractBackground: Conventionally, diabetes management involved targeting the triad of FPG, PPG, and HbA1c. However, several studies have suggested the quintessential need for a paradigm shift to incorporate glycemic variability and quality of life in the holistic diabetes control regimen.
Aim: To generate a consensus and ratify the position of Glycemic Variability (GV) and Quality of Life (QOL), along with the traditional triad, in diabetes management in India. To evaluate whether the triple fixed dose combination of metformin, glimepiride, and voglibose can accomplish the goals of glycemic pentad.
Methodology: Glycemic pentad forum was instituted comprising of 55 experts from different regions of India in the field of diabetology who discussed various evidences related to the topic and shared their experiences and expressed their opinion on the relevance of glycemic pentad in the present diabetes management and whether triple fixed dose combination of metformin, glimepiride, and voglibose is able to achieve glycemic pentad targets.
Results: Forum has come to a consensus that the conglomerate of quintuple elements – FPG, PPG, HbA1c, glycemic variability and quality of life to be termed as glycemic pentad and these milestones to be considered for any antidiabetic therapy. Experts opined that combination therapy is required to achieve the Glycemic Pentad, as monotherapy might not address all the five arms of Glycemic Pentad. Group also agreed that the diabetes management in Indians require separate attention due to their distinct dietary habits (high carbohydrate content) and socio-economic status (economically weak and poorly educated). Therefore, mild adjustments to the standard practices in the western countries are suggested. After evaluating various drugs in the current market to identify candidates that could regulate the elements of Glycemic Pentad, the forum assume that a triple fixed dose combination of metformin, glimepiride, and voglibose could be a better choice in Indians as the combination is safe, affordable and effective in attaining optimal glucose levels and reducing the complications.
Conclusions: Glycemic pentad deserves a prominent position in the diabetes management in India. The triple fixed dose combination of metformin, glimepiride, and voglibose has essential commodities to achieve glycemic pentad targets.
Introduction
Diabetes is one of the lifestyle oriented, metabolic diseases
characterized by decreased insulin sensit ivity and hyperglycemia ultimately causing aberrant glucose homeostasis. Diabetes management
strategies has been recommended in severa l guide l ines a ims a t control l ing the tr iumvirate of FPG, PPG, and HbA1c, which are conventionally referred as glycemic tr iad. 1 The American Diabetes Association recommends targeting HbA1c levels to <7.0% (53mmol/mol), pre-prandial glucose levels to 80 - 130 mg/dl (4.4 – 7.2 mmol/l) and peak postprandial plasma glucose levels to < 180 mg/dl (10.0 mmol/l) in order to achieve better glycemic control.2 However, “one size fits all” concept is NOT suitable for the management of diabetes and therefore individualized treatment based on the patient’s status is recommended.2 For instance, higher HbA1c target might be appropriate in people with co-morbidities and who are prone to hypoglycemia or when there is a high risk associated with possible hypoglycemia.3 Importance of PPG Control in Diabetes
Even though control of fasting h y p e r g l y c e m i a i s e s s e n t i a l , o b t a i n i n g o p t i m a l g l y c e m i c control requires regulat ion of additional parameters.4 Growing body of evidence indicates that reducing postprandial glucose excursions is equally or perhaps more important for achieving HbA1c goals. 1 Contribution of PPG relative to fasting glycemia i s p r e d o m i n a n t w h e n t h e HbA1c levels are approximately below 7.5% in people with non-insulin-treated type 2 diabetes and the contribution decreases progress ively with increasing HbA1c levels.5 Convincing evidence suggest that oxidative stress and

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 2017 69
Fig. 1: Geo mapping of case clusters in neighbouring districts
excessive protein glycation might occur as harmful consequences of sustained chronic hyperglycemia.6 The IDF guidelines on controlling post-meal glucose recommends that postprandial hyperglycemia is harmful and should be lowered by incorporating a variety of both non-pharmacologic and pharmacologic therapies.4
Diet and Postprandial Hyperglycemia in Indian Context
Asian Indian diabetic patients are different from other ethnicities. Carbohydrate content in Indians diet constitutes about 65%, which is more than that is recommended for diabetic patients.7 Of the whole ingredients in an individual’s diet, carbohydrates has the greatest i n f l u e n c e o n b l o o d g l u c o s e level, and both the amount and t y p e o f c a r b o h y d r a t e i n t a k e are the important determinants o f p o s t p r a n d i a l g l u c o s e . 8 Consumption of such imbalanced diet with high carbohydrates could cause increased insulin resistance, metabolic syndrome, and type 2 DM. The amount of carbohydrates consumed affects blood glucose levels and insulin responses and a clear link between carbohydrate intake and post-prandial glucose level exists in diabetic population.9 Since Indians consume diet with high glycemic index and load, postprandial glucose control and overall glycemic control in Indian
diabetic population demands a separate attention.
Glycemic Pentad: Emerging Concept
Traditionally, diabetes control strategies mainly targeted to reduce the triad of fasting and postprandial blood sugars and HbA1c. However, optimal glycemic control in UKPDS and ADVANCE trials failed to prevent macrovascular events and death.10,11 Importance of factors other than average blood glucose in causing diabetes complications have been consistently debated and the advances in research has paved the way to include two more variables, i.e. glycemic variability and quality of life, to the existing components. These five elements are collectively referred as “glycemic pentad”. Different components of glycemic pentad are shown in Figure 1.
Glycemic Variability
It was observed in the Diabetes Control and Complications Trial (DCCT) that in spite of similar HbA1c levels, patients treated with conventional methods showed a r e m a r k a b l e p r o g r e s s i o n t o retinopathy over a period of time when compared to intensively treated subjects.12 Furthermore, controlling glycemic triad does not prevent the occurrence of diabetic
complications and recent studies have shown that mortality rate increased even after maintaining good HbA1c13 and HbA1c derived information is insufficient to explain al l of the risk associated with complications of diabetes.14 High frequency glycemic excursions in conventionally treated patients could be an explanation for this observation.9 Subsequent studies established a relation between osci l la t ing glucose levels and oxidative stress and corroborated t h e h y p o t h e s i s t h a t H b A 1 c together with glycemic variability might be a superior indicator of g lucose control than mean HbA1c alone.6,9 Oscillating blood glucose levels rather than chronic hyperglycemia has been shown to have harmful effects on parameters of cardiovascular (CV) risk such as endothelial dysfunction.15,16 This led to the emergence of new aspect in glycemic control, i.e., glycemic variabil i ty 17 and was included in the concept of the ‘glycemic tetrad.18
G l y c e m i c va r i a b i l i t y ( G V ) can be s imply def ined as the degree of dai ly blood glucose fluctuations (peaks and nadirs) in an individual.19 It comprises of both postprandial glucose spikes a s we l l a s t h e h y p o g l y c e m i c episodes. Glycemic variations are of two types: Variations measured within a day are called as intraday glycemic variations and the glucose variations measured at the same t ime on two consecutive days are called as inter day glucose variat ions. Defect ive glycemic regulation and reduced insulin a va i l a b i l i t y a r e p r e s u m p t i ve etiological factors of GV.20 Even though certain degree of glycemic variations is observed in normal individuals, it increases in people with diabetes and impaired blood glucose tolerance.19
S e v e r a l s t u d i e s a t t r i b u t e hyperglycemia and dysglycemia (peaks and nadirs) to the occurrence of var ious microvascular and m a c r o va s c u l a r c o m p l i c a t i o n s
HbA1C
GlycemicVariability
GLYCEMICPENTAD
Quality ofLife
PPGFPG

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 201770
in diabetes.19 Excessive protein g l y c a t i o n e n d p r o d u c t s a n d ac t ivat ion of ox idat ive s t ress are suggested to be underlying pathophysiological mechanisms c a u s i n g t h e s e v a s c u l a r compl ica t ions . Hypoglycemia along with glycemic variations can influence the onset and progression of diabetes complications and can be troublesome in patients treated in intensive care units (ICUs) for c l inical condit ions other than diabetes.21
Several methods to effectively m e a s u r e p o s t p r a n d i a l h y p e r g l y c e m i a a n d G V a r e available currently. Ambulatory glucose profiling (AGP) is one such technique which retrospectively analyze blood glucose levels from the data collected with flash glucose monitoring (FGM). The FGM and continuous glucose monitoring (CGM) provides information that could not be obtained with periodic capillary blood glucose monitoring, provides all-over the day coverage and alerts and alarms for actual or looming hypo- and hyper-glycemia.22 This information can be used to educate, motivate, and alert people with diabetes. The FGM or CGM is medically recommended for patients with frequent, severe, or nocturnal hypoglycemia, especially in those who are unaware of it.22 Several s tudies indicated that consistent use of CGMS results in better glycemic control. A meta-analysis on fourteen RCTs by Floyd et al. showed a significant reduction in HbA1c and duration of hypoglycemia with CGMS use.23 Similarly, a cochrane review of 22 RCTs revealed a reduction in HbA1c with higher compliance to CGMS when compared to self-monitoring of blood glucose (SMBG).24
In the end, proper biological rationale and enough evidence convince us to endorse the concept of GV as an important risk factor that is directly involved in the p a t h o g e n e s i s o f t h e va s c u l a r complications of diabetes. Overall, it is persuading enough to propose
that regulating glycemic variability is necessary to achieve proper g l y c e m i c c o n t r o l i n d i a b e t e s patients. Collectively, GV and CGMS could help in redefining reasonable interventions in the r e s o u r c e l i m i t e d h e a l t h c a r e environment of countries such as India.
Quality of Life
Of late quality of life (QOL) has emerged as an important parameter in the general disease management routine. The QOL is defined as a multidimensional c o n s t r u c t i n c o r p o r a t i n g a n individual’s subjective perception of physical, emotional, and social wellbeing. 25 I t includes both a cognitive component (satisfaction) and an emot ional component (happiness). In general, QOL is low in diabetes patients and it is positively correlated with duration of the disease.26 Past research on QOL in diabetes has revealed that patients desired to improve the way they feel . 27 Complications associated with diabetes affects the QOL of patients.28 Moreover, acute and bothersome side effects and lifestyle restrictions prevent the patients from motivating to comply with the treatment even though i t promises long-term benefits.27 Therefore therapeutic policies should aim at reducing t h e c o m p l i c a t i o n s a n d a l s o improve t reatment adherence a n d c o m p l i a n c e . B e n e f i t s o f diabetes therapy could be properly reaped through the maximum convenience of the dosing regimen and maximal QOL benef i ts . 27 Martinez et al suggest that QOL in patients could be enhanced by including interventions that could overcome the negative attitude towards treatment adherence and by promoting medical prescription knowledge.29 Furthermore, balance b e t w e e n t r e a t m e n t b u r d e n and health outcomes could be achieved with the wide variety of interventions available in the current market.27
In general patient compliance is poor in diabetes irrespective of the treatment regimen (oral antidiabetic agents or insulin).30 Moreover , phys i c ians should notice that failure to achieve target glycemic levels could be because of inadequate self-management rather than less effectiveness of the prescr ibed medicat ion. In such cases, patient counseling to improve treatment adherence should be preferred rather than increasing the dose or changing the medicat ion. Insul in-based therapy is generally associated with decreased QOL, therefore, it should be carefully considered before various combinations of oral medications are used.31 To sum up, QOL in diabetes is affected by two categories of factors: the disease derived factors such as duration and complications and therapy derived factors such as adverse events, cost, life style restrictions imposed by the treatment . Therapeutic factors generally influence the compl iance to t rea tment and when the compliance is decreased, diabetic complications increase resulting in the deterioration of QOL in a cyclic process. Hence, medications used to treat diabetes should reduce the complications and also contain the features to enhance adherence.
International diabetes guidelines has mentioned the importance o f QOL dur ing the course o f t r e a t m e n t . 2 , 3 T h e A m e r i c a n d i a b e t e s a s s o c i a t i o n ( A D A) recommends to use a pat ient-centered communication style that incorporates active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and financial barriers.2 They also suggest that a successful medical evaluation depends on beneficial interactions between the patient and the care team. Individualization of treatment based on patients’ preferences, values, and goals is also recommended.
Q O L i s g e n e r a l l y a s s e s s e d using a broad questionnaire that

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 2017 71
translates an individual subjective perception into numerical scores. Accuracy and reliability of a QOL tool depends on the extent to which it addresses the factors pertaining to the local population such as language, socio-economic elements, culture, race and religious bel iefs . 32 Several instruments/questionnaires are available to assess QOL. While instruments such as World Health Organization – BREF (WHO-BREF), EuroQol f ive dimensions questionnaire (EQ-5D) and Short Form – 6D (SF – 6D) are used for general QOL assessment, questionnaires such as Diabetes Quality Of Life Measure (DQOL), Diabetes-Specific Quality Of Life Scale (DSQOLS) and Diabetes – 39 (D - 39) are specifically used to measure QOL in diabetes. As India is a diverse country with enormous cultural and socio-economic disparities, QOL assessment tools created for other ethnic populations might not derive complete and proper informat ion . Therefore , India specific QOL measurement tool is the need of the hour. In this regard, Nagpal J et al. has developed Quality Of Life Instrument for Indian Diabetics (QOLID), to assess the QOL of Indian diabetes patients.33 It comprises of eight domains and 34 items (questions) evaluating the physical health, socio-economic and psychological s tatus of a patient. The first three domains role limitation due to physical health, physical endurance, and general health could be classified as health related quality of life (HRQOL); they evaluate the general health and wellbeing of an individual. T h e r e m a i n i n g f i ve d o m a i n s treatment satisfaction, symptom botherness , f inancial worr ies , emotional/mental health and diet advice tolerance reflect the diabetes specific quality of life (DSQOL). Fur ther work i s mandated to validate this instrument across a wider geographical and socio-economic spectrum and in different community settings.
To summarize, QOL should be considered en route to achieve optimal glycemia in a diabetes pat ient . From this v iewpoint , following are some of the important a t t r ibutes of any ant idiabet ic therapy: it should be simple to follow and affordable, it should have convenient dosing regimen and least side effects, it should not impose too many l i festyle restrictions and overall, it should improve the way an individual feels about oneself.
C o l l e c t i ve l y , t h e g l y c e m i c pentad as a new concept deserves to have its position in the diabetes management course. It is imperative that a global antidiabetic strategy should be aimed at reducing the four components o f g lycemic pentad i.e., FPG, PPG, HbA1c, and glucose variability and improving the fifth element, quality of life.
Achieving Goals of Glycemic Pentad with Anti-Diabetic TherapyAnti-diabetic agents
Several varieties of antidiabetic agents are currently available. On the basis of mode of administration, a n t i - d i a b e t i c t h e r a p y c a n b e broadly categorized into injectable and non-injectable or oral therapy. Insulin and i ts analogues and glucagon like peptide 1 (GLP-1) receptor agonists (GLP-1 RAs) belong to the injectable category. Oral antidiabetic (OADs) category is overwhelming, with a variety of drugs that have different modes of action. Insulin secretagogues s u c h a s s u l p h o n y l u r e a s (SU) , megl i t in ides and DPP-4 inhibitors stimulate the β-cells of pancreas to secrete insulin. I n s u l i n s e n s i t i z e r s i n c l u d i n g biguanides, thiazolidinediones, and DPP-4 inhibi tors prevent hepatic glucose production and increase glucose uptake in the peripheral tissues such as muscle and adipose t issue. Two other classes of drugs, alpha-glucosidase inhibi tors (AGIs) and SGLT-2
inhibitors function at the level of glucose absorption and excretion respectively. While AGIs delay the intestinal glucose absorption by inhibiting enzymes responsible for complex carbohydrate breakdown, SGLT-2 inhibitors prevent glucose reabsorption in the kidney by regulating the activity of glucose transporters.
Attaining optimal glucose levels is the foremost objective of any antidiabetic therapy. Decision to begin or alter a therapy is based on the prevailing glycemic levels.34 When monotherapy fails to produce ambient glycemic levels, multiple drugs with different modes of action can be considered.34 Factors such as safety, efficacy, additional benefits in reducing complications, ease of use, and expense are important considerations while choosing an OAD.35 Furthermore, HbA1c levels also provide a direction towards decision making; while high HbA1c levels (≥8.5%) desire to be treated with fast acting agents or combination therapy, levels close to target indicate the use of agents with lesser potential and/or slower onset of action.35 Overall the treatment regimen should be planned in such a way that all of the five goals of glycemic pentad are attained both at the convenience of physician and patient.
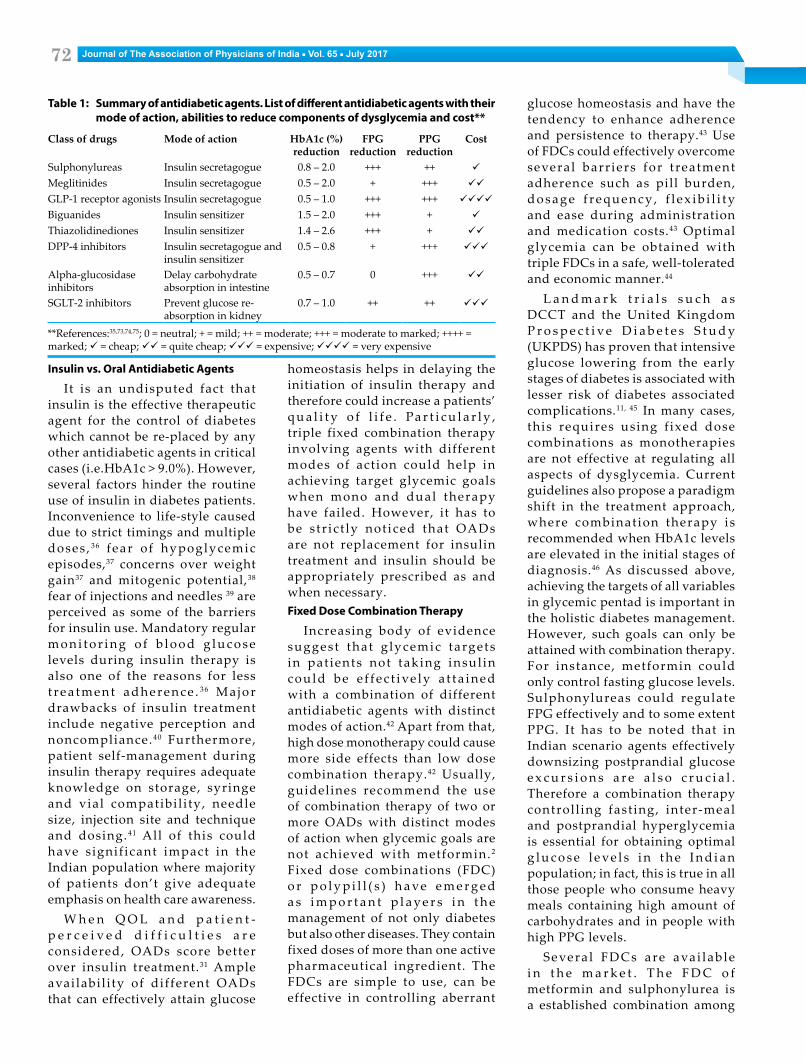
The list of different antidiabetic a g e n t s , t h e i r m o d e o f a c t i o n and ability to reduce different components of glycemic triad is listed in Table 1. Regardless of the mode of administration or action, sole aim of any anti-diabetic therapy is to maintain glucose homeostasis with minimal adverse events and maximal convenience or ease. Since Indians constitute a special category of diabetes population with distinct dietary habits and socio-economic and cultural backgrounds, choice of antidiabetic therapy should not only rely on the effectiveness of the agent but also on the cost, ease of administration and other confounding factors.
Journal of The Association of Physicians of India ■ Vol. 65 ■ July 201772
Insulin vs. Oral Antidiabetic Agents
It is an undisputed fact that insulin is the effective therapeutic agent for the control of diabetes which cannot be re-placed by any other antidiabetic agents in critical cases (i.e.HbA1c > 9.0%). However, several factors hinder the routine use of insulin in diabetes patients. Inconvenience to life-style caused due to strict timings and multiple doses , 36 fear of hypoglycemic episodes,37 concerns over weight gain37 and mitogenic potential,38 fear of injections and needles 39 are perceived as some of the barriers for insulin use. Mandatory regular m o n i t o r i n g o f b l o o d g l u c o s e levels during insulin therapy is also one of the reasons for less t r e a t m e n t a d h e r e n c e . 3 6 M a j o r drawbacks of insulin treatment include negative perception and noncompliance.40 Furthermore, patient self-management during insulin therapy requires adequate knowledge on storage, syringe and vial compatibil i ty, needle size, injection site and technique and dosing.41 All of this could have signif icant impact in the Indian population where majority of patients don’t give adequate emphasis on health care awareness.
W h e n Q O L a n d p a t i e n t -p e r c e i v e d d i f f i c u l t i e s a r e considered, OADs score better over insulin treatment.31 Ample availabil i ty of different OADs that can effectively attain glucose
homeostasis helps in delaying the initiation of insulin therapy and therefore could increase a patients’ q u a l i t y o f l i f e . Pa r t i c u l a r l y , triple fixed combination therapy involving agents with different modes of action could help in achieving target glycemic goals when mono and dual therapy have failed. However, it has to be s tr ic t ly not iced that OADs are not replacement for insulin treatment and insulin should be appropriately prescribed as and when necessary. Fixed Dose Combination Therapy
Increasing body of evidence suggest that g lycemic targets in pat ients not taking insul in could be e f fec t ive ly a t ta ined with a combination of different antidiabetic agents with distinct modes of action.42 Apart from that, high dose monotherapy could cause more side effects than low dose combination therapy.42 Usually, guidelines recommend the use of combination therapy of two or more OADs with distinct modes of action when glycemic goals are not achieved with metformin.2 Fixed dose combinations (FDC) o r p o l y p i l l ( s ) h a ve e m e r g e d a s i m p o r t a n t p l a y e r s i n t h e management of not only diabetes but also other diseases. They contain fixed doses of more than one active pharmaceutical ingredient. The FDCs are simple to use, can be effective in controlling aberrant
glucose homeostasis and have the tendency to enhance adherence and persistence to therapy.43 Use of FDCs could effectively overcome several barr iers for t reatment adherence such as pill burden, d o s a g e f r e q u e n c y , f l e x i b i l i t y and ease during administration and medication costs.43 Optimal glycemia can be obtained with triple FDCs in a safe, well-tolerated and economic manner.44
L a n d m a r k t r i a l s s u c h a s DCCT and the United Kingdom P r o s p e c t i v e D i a b e t e s S t u d y (UKPDS) has proven that intensive glucose lowering from the early stages of diabetes is associated with lesser risk of diabetes associated complications.11, 45 In many cases, this requires using f ixed dose combinations as monotherapies are not effective at regulating all aspects of dysglycemia. Current guidelines also propose a paradigm shift in the treatment approach, where combination therapy is recommended when HbA1c levels are elevated in the initial stages of diagnosis.46 As discussed above, achieving the targets of all variables in glycemic pentad is important in the holistic diabetes management. However, such goals can only be attained with combination therapy. For instance, metformin could only control fasting glucose levels. Sulphonylureas could regulate FPG effectively and to some extent PPG. It has to be noted that in Indian scenario agents effectively downsizing postprandial glucose e x c u r s i o n s a r e a l s o c r u c i a l . Therefore a combination therapy controll ing fast ing, inter-meal and postprandial hyperglycemia is essential for obtaining optimal g l u c o s e l e ve l s i n t h e I n d i a n population; in fact, this is true in all those people who consume heavy meals containing high amount of carbohydrates and in people with high PPG levels.
Severa l FDCs are avai lab le i n t h e m a r k e t . T h e F D C o f metformin and sulphonylurea is a established combination among
Table 1: Summary of antidiabetic agents. List of different antidiabetic agents with their mode of action, abilities to reduce components of dysglycemia and cost**
Class of drugs Mode of action HbA1c (%)reduction
FPG reduction
PPG reduction
Cost
Sulphonylureas Insulin secretagogue 0.8 – 2.0 +++ ++
Meglitinides Insulin secretagogue 0.5 – 2.0 + +++
GLP-1 receptor agonists Insulin secretagogue 0.5 – 1.0 +++ +++
Biguanides Insulin sensitizer 1.5 – 2.0 +++ +
Thiazolidinediones Insulin sensitizer 1.4 – 2.6 +++ +
DPP-4 inhibitors Insulin secretagogue and insulin sensitizer
0.5 – 0.8 + +++
Alpha-glucosidase inhibitors
Delay carbohydrate absorption in intestine
0.5 – 0.7 0 +++
SGLT-2 inhibitors Prevent glucose re-absorption in kidney
0.7 – 1.0 ++ ++
**References:35,73,74,75; 0 = neutral; + = mild; ++ = moderate; +++ = moderate to marked; ++++ = marked; = cheap; = quite cheap; = expensive; = very expensive

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 2017 73
the Indian market . The FDCs of metformin or sulphonylurea with other antidiabetic agents are also routinely available. Of the contextual interest is the triple fixed dose combination of metformin, glimepiride, and voglibose. This combination has different drugs optimizing glucose levels through distinct mechanisms; metformin is an insulin sensitizer, glimepiride is an insulin secretagogue and voglibose delays glucose absorption in intestine. Fixed Dose Combination of Metformin, Glimepiride, and Voglibose Might be Appropriate to Achieve all Goals of Glycemic Pentad
Glycemic pentad acknowledges a multidimensional approach in treating diabetes. It suggests that the therapy should not only aim at clinical features (FPG, PPG, HbA1c, and GV) but also consider the socio-economic and psychological status of the patients. Among the clinical aspects, the major factor that sets Indians (Asians) apart is the postprandial hyperglycemia which is due to intake of high carbohydrate content in the diet. Hence, an antidiabetic agent that could effect ively reduce these excursions and therefore reduce the GV is essential. The antidiabetic therapy has to be affordable and it should be relatively simpler to follow. The FDCs have repeatedly proven the i r e f fec t iveness in attaining these elements of disease management. Therefore, an FDC of metformin, glimepiride, and voglibose appear to have all the necessary characteristics to fulfill this criterion.
Metformin and glimepiride are the most commonly prescribed diabetic agents in India.47 Safety and efficacy of these molecules was proved repeatedly . They are known to reduce the fasting glucose levels and HbA1c and to some extent postprandial glucose. Hypoglycemia and weight gain are the usua l adverse events associated with SUs. However, g l imepir ide use i s assoc ia ted
with less hypoglycemic episodes when compared to o ther SUs except glipizide.48 Furthermore, gl imepiride is associated with weight neutra l iz ing/ reduc ing effects and therefore it might be advantageous.48,49 When compared to various other sulphonylureas, g l imepir ide has highest extra pancreatic activity and lowest ratio of increase in plasma insulin and decrease in blood glucose activity.50 C o m b i n a t i o n o f m e t f o r m i n and gl imepiride was found to be effective when compared to metformin plus DPP-4 inhibitors in a systematic review and meta-analysis of safety and effectiveness variables.51 Efficiency of voglibose is far bigger and its tolerability is also high when compared to other AGIs including acarbose and miglitol.52 Furthermore, voglibose is able to improve insulin sensitivity, increase high-density lipoprotein (HDL) and apolipoprotein A-I levels and reduce insul in and triglyceride levels in the body.53 In addition, voglibose administration elicits changes in the intestinal microbiota and reduces body weight , to ta l cho les tero l and triglyceride levels. 54 Voglibose is also associated with increase in GLP-1 levels in the circulation 55 which could further help in attaining glucose homeostasis. Apart from controlling PPG and h y p e r l i p i d e m i a , v o g l i b o s e i s known to reduce oxidative stress markers and soluble intercellular adhesion molecule 1, which is an inflammatory marker.56 Moreover, voglibose is equally effective as sitagliptin at improving endothelial dysfunction in type 2 diabetes p a t i e n t s . 5 7 P h a r m a c o k i n e t i c p r o p e r t i e s o f m e t f o r m i n , glimepiride, and voglibose are provided in Table 2.
Combined use of voglibose and sulphonylureas might be effective in controlling postprandial plasma glucose and delay the onset of vascular complications in patients with type 2 diabetes.58 Even IDF guidelines suggest that the AGIs
could be effective in combination with metformin or sulphonylurea.3 Therefore, addition of voglibose to metformin and gl imepiride combination would effectively reduce the postprandial glycemic excursions along with FPG and HbA1c. As a result, the overall glycemic variability could also be reduced s ign i f i cant ly . GV parameters such as mean amplitude of glycemic variations (MAGE) and standard deviation (SD) around the mean glucose levels were found to be similar or better with metformin use when compared to insulin or meglitinides.59,60 In an open label prospective study on T2D patients, Matsumoto et al have demonstrated that voglibose is able to effectively reduce the daily glycemic excursions and functional burden of the β cells.61 Furthermore, when compared to sitagliptin, voglibose significantly reduced the slope of postprandial elevation of glucose after every meal and also increased the time taken to at ta in maximal glucose levels post dinner.62 All these evidences clearly suggest that metformin and voglibose are effective at managing glycemic excursions.
T h e D i a b e t e s P r e v e n t i o n Program (DPP) and its Outcomes S tudy (DPPOS) revea led that the investment made on lifestyle interventions and metformin to prevent diabetes in high-risk adults is highly beneficial.63 Long-term use of metformin stabilized body mass index (BMI) and improved body composition in adolescent obese and insulin resistant subjects.64 Evaluation of overall treatment s a t i s f a c t i o n w i t h D i a b e t e s Treatment Specific Questionnaire, status version (DTSQs) revealed no significant differences between combination of metformin plus glimepiride or empagliflozin.65 Furthermore, though a population based mathematical model Zhang et al has found that the use of SUs as second l ine of therapy resulted in similar outcomes such as l i fe years (LYs) and quality

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 201774
adjusted life years (QALYs) as DPP-4 inhibitors or GLP-1 RAs or insulin.66 In addition SU based therapies incurred significantly low cost per QALY and prolonged the t ime required for insul in treatment. Similarly, voglibose along with standard care resulted in cost saving and prolonged life expectancy in glucose intolerant Japanese patients.67 Together these evidences suggest a beneficial role of metformin, glimepiride, a n d v o g l i b o s e i n i m p r o v i n g the QOL. Considering all these facts, it is rationale to put the triple combination of metformin, glimepiride, and voglibose at the forefront of diabetes management in India.
Summary of safety and efficacy studies on the combination of m e t f o r m i n , g l i m e p i r i d e , a n d voglibose is available in Table 3. Availability of l imited number of studies assessing the safety and efficacy of this triple FDC demands the necessity for further high quality studies. However, i t is evident from the already available information that this triple combination is safe to use and effective at reducing FPG, PPG, and HbA1c (Table 2). Pankivn VI et al. also reported a significant weight reduction in the group of patients treated with this FDC when compared to the dual combination of metformin and glimepiride.68 This combination is well tolerated in general,69,70,71 yet, some patients might experience temporary side effects such as abdominal pain,
headache, diarrhea, flatulence, sweating and hot flushes.72
Consensus Statement on the Position of Glycemic Pentad in Diabetes Control and the FDC of Metformin, Glimepiride, and Voglibose in the Management of Diabetes In IndiaObjectives
Research on diabetes has been endorsing the importance of GV and QOL in the management of diabetes along with FPG, PPG, and HbA1c. Even though some guidel ines have been acknowledging the significance of QOL in diabetes contro l , GV has been large ly ignored. Furthermore , Indian diabetes patients are different from western people due to their varied dietary and cultural habits. So diabetes management there r e q u i r e s l i g h t m o d i f i c a t i o n s , p a r t i c u l a r l y i n r e g u l a t i n g p o s t p r a n d i a l h y p e r g l y c e m i a through a cost-effective and easy to follow regimen. Various OADs are available in the market. Even though this g ives quite many opportunities to physicians, often it creates confusion among health care professionals working at primary health care centers where most of the Indian diabetes population is treated. Therefore, there is a need for a simple medication which could offer easy and economical alternative to treat diabetes.Methodology
An expert group, Glycemic
Pentad forum, consisting of 51 leading medical experts f rom different regions of India in the field of diabetology were convened into 5 groups to bring a consensus on the position of glycemic pentad in diabetes control and the FDC of metformin, glimepiride and voglibose in the management of diabetes in India. Each group met independently in different cities of India, reviewed the relevant literature, expressed their opinions o n t h e p o s i t i o n o f g l y c e m i c pentad and shared their personal experiences with the use of triple FDC of metformin, glimepiride, and voglibose in clinical practice. A final consensus statement is generated after the key points in different meetings were shared among the forum and an approval is given by all members of the forum.
Key Points from the Consensus MeetingsConsensus on the position of glycemic pentad in the management of diabetes in Indians
Recent advances in the field of diabetology incited a further leap to diabetes management and added two more dimensions - glycemic variability (GV) and quality of life (QOL) - to already existing glycemic triad and the composite of these 5 elements is now identified as Glycemic Pentad. Glycemic variations are the physiological consequences of circadian rhythms of hormones involved in glucose control and also due to postprandial spikes in glucose levels. Clinical evidences suggest that patients with high GV are prone to high risk of retinopathy. Patients with painful neuropathy had high GV when compared to patients with painless neuropathy. Also, high GV is associated with increased carotid media thickness. Even though the fluctuation reduction with insulin and GLP-1 added together (FLAT-SUGAR) study has provided some evidences on the benefits of controlling GV,
Table 2: Pharmacokinetic parameters of metformin, glimepiride and voglibose
PK Parameters Metformin Glimepiride$ Voglibose@ Half life ~5 hrs* 5-8 hrs 1 to 1.5 hoursMean renal clearance (CLr) 510±130 ml/min* NegligibleTotal clearance (CL) 1140 ± 330 mL/min*** 47.8 mL/min NegligibleOral bioavailability 50–60%** 100% Poorly absorbedPeak plasma concentrations (Cmax) IR- 1-3 hrs
ER- 4-8 hrs#2-3 hrs Undetectable
Plasma protein binding Negligible# > 99.5%.Volume of distribution (Vd) 300–1000 L# 8.8 LElimination half-life 6.2 hrs** 3-6 hrsIR: Immediate release; ER: Extended release; References: *76; **77; ***78; #79; $80; @52

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 2017 75
further high quality research is recommended to strongly establish these facts. GV is of two types: 1. Intra-day variations which are vert ical g lycemic f luctuat ions within a day. 2. Inter-day variations which are observed as time wise glycemic f luctuations between different days. Several evidences suggest that GV is an important predictor of hypoglycemia whereas HbA1c could not provide any such information. Therefore, it is imperative to acknowledge the importance of controlling glycemic variations in diabetes patients.
Of f l a te QOL has emerged as an important element in the m a n a g e m e n t o f d i a b e t e s a n d also in the overall health care of an individual. It predicts an individual’s capacity to manage disease and maintain long-term
health and well-being. Poor QOL worsens the life of an individual in a positive feedback loop. In diabetic patients, poor QOL leads to diminished sel f -care which results in deregulated glycemic control. This leads to increase in the risk of diabetes associated complications which in turn affect the QOL of an individual again. Therefore, it is sensible to address the issue of QOL of a patient during the diabetes treatment.
Considering all these facts, it is convincing to incorporate glycemic variation and quality of life as new dimensions in the overall diabetes management program and therefore glycemic pentad as a fresh concept has utmost significance in the holistic control of diabetes. Hence, it is rational to identify the better combination therapy that
could score well in regulating all five domains of glycemic pentad.Consensus on the role of triple FDC of metformin + glimepiride + voglibose in regulating glycemic variability
P o s t m e a l h y p e r g l y c e m i a , p a r t i c u l a r l y p o s t b r e a k f a s t hyperglycemia is the major factor influencing the glycemic excursions in Indian diabetes patients and a r e i m p o r t a n t i n r e g u l a t i n g glycemic variation and the overall glycemic control and quality of life. Furthermore, for the same amount of carbohydrate intake, Asians have higher postprandial glucose values when compared to Caucasians.
Even though the carbohydrate content in the breakfast is lower than lunch and dinner, post breakfast glucose spikes are observed to be higher in the Indian diabetes patients (personal experience from
Table 3: Efficacy and safety studies on metformin, glimepiride and voglibose combination. A list of safety and efficacy studies that were carried out on the combination of metformin, glimepiride, and voglibose either as FDC or as triple therapy
Author et al., Type of study
No. of subjects (n); duration of study
Drug dosage Efficacy and safety results
Hari K. et al., 2014;69 Non-randomized, open, non-comparative, mono-centric study.
n = 20; 4 months Metformin 500mg (SR#) + Glimepiride 1/2mg + Voglibose 0.2mg OD. (FDC)
Significant reduction in FPG (181±10.2 mg/dl to 116±2.97 mg/ml; P < 0.0001), PPG (239±11.2 mg/dl to 140±4.42 mg/dl; P < 0.0004), and HbA1c (9.07 ±0.346 to 6.51±0.129; p < 0.0001). All of the patients tolerated the drug and no adverse events were reported.
Faruqui AA, 2016;70 Non-randomized, open, non-comparative, mono-centric study.
n = 50; 3 months Metformin 500mg (SR#) + Glimepiride 0.5 mg + Voglibose 0.2mg BD. (FDC)
Significant decrease in HbA1c value 10.6 ± 1.3 vs. 6.6 ± 0.4 (P< 0.0001), FPG levels 208.33mg/dl vs. 118.06 (P< 0.0001), and PPHG levels 360.14 mg/dl vs. 168.36, (P< 0.0001).None of the patients complained about adverse events including nausea, vomiting, and headache at the given doses of medication.
Rao C. et al., 2013;71 Non-randomized, open, non-comparative, mono-centric study.
n = 20; 3 months Metformin 500mg (SR#) + Glimepiride 1/2mg + Voglibose 0.2mg BD. (FDC)
Significant decrease in HbA1c (8.86 ± 0.7111 gm/dl vs. 8.0 ± 0.66 gm/dl), fasting (137±17.64 mg/dl vs. 116.8 ± 6.129 mg/dl, P < 0.0001) and post prandial blood glucose level ((237.8 ± 59.22 mg/dl vs.173.4 ± 27.6 P < 0.0004) was observed from baseline.This triple combination was well tolerated.
Jindal A. et al., 2014;72 Open label study
n = 30; 6 months Metformin 500mg BD + Glimepiride 2mg BD + Voglibose 0.2mg TDS
Significant reduction (p<0.001) in FPG, PPG and HbA1c over a period of 6 months. Side effects such as abdominal pain, headache, diarrhea, flatulence, sweating, and hot flushes are observed.
Murti K. et al., 2016;81
Prospective, open-label, comparative study
n = 75; 10 months Dual therapy group: Metformin 500mg + Glimepiride 1mg Triple therapy group: Metformin 500mg + Glimepiride 1mg + Voglibose 0.3mg
Even though significant reduction in FPG, PPG, and HbA1c was observed from baseline to end of study in both dual and triple therapy groups, it was larger in triple therapy group.
Pankivn VI et al., 201668 Prospective, comparative study
n = 45; 12 weeks Group I: Metformin + Glimepiride + Voglibose 0.2mg TDS.Group II: Metformin + Glimepiride +
Decrease in HbA1c was high in group I (1.5 [1.1; 1.9] % (p < 0.05) than group II (0.1 [0.09; 0.6] % (p > 0.05) after 12 weeks of treatment. Body weight reduced significantly by 2.1 kg in group I while no response was observed in group II. Safety was proven in terms of functional states of liver and kidney.
FDC: Fixed dose combination; # SR: sustained release; OD: Once daily; BD: Twice daily: TDS: Three times in a day

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 201776
experts) than that of post lunch or post dinner.
C o n t i n u o u s g l u c o s e measurement i s important to understand the dynamics of blood glucose levels. Since this technique is expensive to some individuals, 7 point glucose measurements are recommended to be performed routinely with intermittent AGP.
Choice of any antidiabetic drug should be individualized based on the patients’ phenotype, history, affordability, and acceptance.
C h a n g i n g t h e t i m i n g o f medication based on AGP is more beneficial in improving the glycemic control rather than increasing the dosage of the medications.
In the Indian scenario, where consumption of carbohydrates is high, alpha glucosidase inhibitors are the best choice of drugs after metformin and glimepiride.
Alpha glucosidase inhibitors could be preferred over bolus insulin in controlling post meal hyperglycemia when hypoglycemic episodes are considered. This is mainly because it is very difficult t o t h e p a t i e n t t o p l a n t h e i r carbohydrate intake based on the insulin dose on a daily basis.
V o g l i b o s e c o u l d d e c r e a s e glycemic variations by controlling postprandial glucose excursions and also effectively reduce the risk of hypoglycemia. Voglibose (alpha glucosidase inhibitors) is under used in Indian population when compared to other Asian countries.
Voglibose can be prescribed to regulate uncontrolled postprandial glucose peaks in those patients who are already on metformin, glimepiride, and basal insulin. Moreover, addition of voglibose at night could reduce the need for SU or bolus insulin who have the tendency to cause nocturnal hypoglycemia.
In patients who are predisposed to gastroparesis or bloating, start with low dose of voglibose (0.2 mg) and up-titrate it to maximal
dose (0.3 mg) after the patient is acclimatized to the treatment. Voglibose should be restricted in patients with active hepatic disease.
Metformin and glimepiride has been a successful combination in the diabetes management scenario of Indian setup. On the similar note, it is also a well-accepted fact that the effect of this combination reduces after sometime due to various physiological consequences and therefore it compels the inclusion of a new agent.
Triple fixed dose combination (FDC) of metformin, glimepiride, and vog l ibose i s e f f ec t ive in reducing glycemic var iabi l i ty and HbA1c in Indian diabet ic pat ients . The results are very conspicuous when data from triple FDC are compared to metformin + glimepiride dual combination.
In order to control post dinner hyperglycemia in patients who have nocturnal hypoglycemia after sulphonylurea (SUs) use it is recommended to down titrate the SU dose and incorporate voglibose into the treatment regimen. This combination can also be prescribed as up-t i trat ion to the ongoing medication or as a replacement therapy in the patients who are already on a different triple drug combination.
Twice daily dose of this FDC after breakfast and dinner is sufficient to prevent the glycemic excursions in a day. However, as and when required, elevated blood glucose levels post lunch or evening snack could be handled with voglibose alone.
The ideal time to take the triple drug is 15 - 30 minutes before the meal. However, when practical in-convenience is considered, it can also be taken just before the meal, at the time or after the consumption of a meal. Even if the patients miss the appropriate timing, it is recommended that they take it sometime rather than missing the dose completely.
This combination provides an extended temporal window for the patients and the physician before an insulin dose is initiated. However, it is not a substitute for insulin therapy. Patients who have very high HbA1c or PPG levels and require insulin therapy should be given appropriate treatment.
Effective treatment regimens should include GLP-1 receptor agonists and DPP-4 inhibitors along with voglibose in order to achieve over all good glycemic control. Gliptins are a good option when patients have both high FPG and PPG values whereas when only PPG values are more, voglibose is a better choice.
O ve r a l l t h e t r i p l e F D C o f m e t f o r m i n , g l i m e p i r i d e , a n d voglibose is effective in attaining good glycemic control in diabetic patients. While glimepiride controls FPG and to some extent PPG, metformin regulates nocturnal g lucose l eve l s and vog l ibose majorly prevents PPG excursions. As a resul t , th is combinat ion could effectively regulate overall glycemic levels. However, high quality studies comparing the e f f i c a c y o f t r i p l e f i x e d d o s e combination with dual therapy of metformin and glimepiride or any other antidiabetic therapies are recommended so as to fairly demonstrate the additive benefits of this triple combination in the control of diabetes.Consensus on the role of metformin, glimepiride and voglibose FDC in achieving good QOL scores in Indian diabetic patients
Use of the triple drug combination of metformin, glimepiride, and voglibose could result in the overall improvement of QOL in diabetes patients. However, compelling evidences that substantiate this concept has to be generated in the due course through systematically designed QOL studies.
T r i p l e F D C o f m e t f o r m i n , g l imepir ide , and vogl ibose i s associated with improving overall g l y c e m i c c o n t r o l , i n c r e a s i n g

Journal of The Association of Physicians of India ■ Vol. 65 ■ July 2017 77
compliance, reducing pill and cost burden on the patient. Therefore, al l these elements collectively enhance the QOL of an individual.
Generally, Indian population a r e r e l u c t a n t t o r e d u c e h i g h carbohydrate content in their diet. In those people, this FDC provides an excellent option for maintaining ideal glucose levels without compromising much on their food habits. As a result, diet satisfaction is improved and QOL is enhanced.
Since triple therapy reduces the pill and cost burden, it has fairly good chances of increasing the t rea tment adherence and compliance, therefore, it will result in overall good glycemic control and better QOL.
Usually, increase in pill number put a psychological burden on the patient that the disease has worsened. However, with the triple combination therapy, this aspect can be easily circumvented.
Simplified therapy is one of the fundamental characteristics t o i m p r o ve c o m p l i a n c e . T h e FDC of metformin, glimepiride, a n d v o g l i b o s e p r o v i d e s u c h u n c o m p l i c a t e d o p t i o n t o t h e patient, which ultimately leads to improved QOL.
T h e F D C o f m e t f o r m i n , g l i m e p i r i d e , a n d v o g l i b o s e i s assoc iated with decreas ing hypoglycemia episodes and HbA1c levels, which in turn improves the psychosocial behavior of a patient.
Voglibose as a combination with metformin and glimepiride is a better choice drug in comparison to DPP4 inhibitors or SGLT2 inhibitors when compliance, convenience and cost effectiveness are considered.
Compliance to treatment and diet adherence of patients can also be increased by showing their own AGP data.
Patients should be advised on strict diet plan before the onset of any anti-diabetic therapy as f requent changes in d ie t and lifestyle patterns often leads to
confusion in both physicians and patients. In some cases, it might also lead to severe hypoglycemia as well. As a result, the QOL is also affected.Overall consensus on the use of the triple FDC of metformin, glimepiride, and voglibose in attaining goals of glycemic pentad in Indian diabetic patients
Triple combination of metformin, glimepiride, and voglibose is an important armamentarium in the control of glycemic pentad. The drug combinations could effectively r e g u l a t e F P G a n d P P G , a n d therefore the other two elements in glycemic pentad HbA1c and glycemic variations are also well controlled. As the improvement in glycemic control reduces the burden of diabetes associated complications, i t improves the QOL of an individual. Therefore, all objectives of glycemic pentad could be collectively achieved with a single therapy. Hence this combination definitely has a bigger role to perform in the overal l diabetes management of Indian population.
References1. Ceriello A. The glucose triad and its role in
comprehensive glycaemic control: current status, future management. International Journal of Clinical Practice 2010; 64:1705-11.
2. American Diabetes Association. Promoting health and reducing disparities in populations. Standards of Medical Care in Diabetes 2017. Diabetes Care 2017; 40.
3. International Diabetes Federation. Clinical Guidelines Task Force Global Guideline for Type 2 Diabetes, 2012, Available at http://www.idf.org/sites/default/files/IDF-Guideline-for-Type-2-Diabetes.pdf
4. International Diabetes Federation. Guideline for management of post meal glucose in diabetes, 2011, Available at https://www.idf.org/sites/default/files/postmeal%20glucose%20guidelines.pdf
5. Monnier L , Lapinsk i H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients. Diabetes Care 2003; 26:881-5.
6. Monnier L, Colette C. Glycemic Variability Should we and can we prevent it?. Diabetes Care 2008; 31(Supplement 2):S150-4.
7. Joshi SR, Bhansali A, Bajaj S, et al. Results
from a dietary survey in an Indian T2DM population: a STARCH study. BMJ Open 2014; 4:e005138.
8. Sheard NF, Clark NG, Brand-Miller JC, et al. Dietary carbohydrate (amount and type) in the prevention and management of diabetes. Diabetes Care 2004; 27:2266-71.
9. Joshi SR. Glycemic Variabil ity and Ambulatory Glucose Profile in Indian Diabetics. J Assoc Physicians India 2016; 64:11.
10. ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008; 2008:2560-72.
11. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). The Lancet 1998; 352:837-53.
12. Lachin JM, Genuth S, Nathan DM, et al. Effect of glycemic exposure on the risk of microvascular complications in the diabetes control and complications trial—revisited. Diabetes 2008; 57:995-1001.
13. Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008; 2008:2545-59.
14. Hirsch IB. Glycemic variability and diabetes complications: does it matter? Of course it does!. Diabetes Care 2015; 38:1610-4.
15. Piconi L, Quagliaro L, Assaloni R, et al. Constant and intermittent high glucose enhances endothelial cell apoptosis through mitochondrial superoxide overproduction. Diabetes/Metabolism Research and Reviews 2006; 22:198-203.
16. Horvath EM, Benkő R, Kiss L, et al. Rapid ‘glycaemic swings’ induce nitrosative stress, activate poly (ADP-ribose) polymerase and impair endothelial function in a rat model of diabetes mellitus. Diabetologia 2009; 52:952-61.
17. Kalra S, Kalra B. The glycemic pentad: Role of insulin analogues. 2010.
18. Monnier L, Colette C, Owens DR. Integrating glycaemic variability in the glycaemic disorders of type 2 diabetes: a move towards a unified glucose tetrad concept. Diabetes/Metabolism Research and Reviews 2009; 25:393-402.
19. Suh S, Kim JH. Glycemic variability: how do we measure it and why is it important?. Diabetes and Metabolism Journal 2015; 39:273-82.
20. Krishna SV, Kota SK, Modi KD. Glycemic variability: clinical implications. Indian journal of Endocrinology and Metabolism 2013; 17:611.
21. DeVries JH. Glucose variability: where it is important and how to measure it. Diabetes
Journal of The Association of Physicians of India ■ Vol. 65 ■ July 201778
2013; 62:1405-8.
22. Rodbard D. Continuous glucose monitoring: a review of successes, challenges, and opportunities. Diabetes Technology and Therapeutics 2016; 18:S2-3.
23. Floyd B, Chandra P, Hall S, et al. Comparative analysis of the efficacy of continuous glucose monitoring and self-monitoring of blood glucose in type 1 diabetes mellitus. J Diabetes Sci Technol 2012; 6:1094-102.
24. Langendam M, Luijf YM, Hooft L, et al. Continuous glucose monitoring systems for type 1 diabetes mellitus. Cochrane Database Syst Rev 2012; 1:CD008101.
25. Skevington SM, Lotfy M, O’Connell KA. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Quality of Life Research 2004; 13:299-310.
26. Rubin RR, Peyrot M. Quality of life and diabetes. Diabetes/Metabolism Research and Reviews 1999; 15:205-18.
27. Testa MA. Quality-of-life assessment in diabetes research: interpreting the magnitude and meaning of treatment effects. Diabetes Spectrum 2000; 13:29.
28. American Diabetes Association. Quality of life in type 2 diabetic patients is affected by complications but not by intensive policies to improve blood glucose or blood pressure control (UKPDS 37). UK Prospective Diabetes Study Group. Diabetes Care 1999; 22:1125-36.
29. Martínez YV, Prado-Aguilar CA, Rascón-Pacheco RA, et al. Quality of life associated with treatment adherence in patients with type 2 diabetes: a cross-sectional study. BMC Health Services Research 2008; 8:164.
30. Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care 2004; 27:1218-24.
31. Tamir O, Wainstein J, Raz I, et al. Quality of life and patient-perceived difficulties in the treatment of type 2 diabetes. Rev Diabet Stud 2012; 9:46-54.
32. Goh SG, Rusli BN, Khalid BA. Development and validation of the Asian Diabetes Quality of Life (AsianDQOL) Questionnaire. Diabetes Research and Clinical Practice 2015; 108:489-98.
33. Nagpal J, Kumar A, Kakar S, et al. The development of quality of life instrument for Indian diabetes patients (QOLID): a validation and reliability study in middle and higher income groups. J Assoc Physicians India 2010; 58:295-304.
34. Luna B, Feinglos MN. Oral agents in the management of type 2 diabetes mellitus. American Family Physician 2001; 63:1747-56.
35. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in
type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Clinical Diabetes 2009; 27:4-16.
36. Wangnoo SK, Maji D, Das AK, et al. Barriers and solutions to diabetes management: An Indian perspective. Indian J Endocrinol Metabolism 2013; 17:594.
37. Korytkowski M. When oral agents fail: Practical barriers to starting insulin. Int J Obes Relat Metab Disord 2002; 26(Suppl 3):S18–24.
38. Hemkens LG, Grouven U, Bender R, et al. Risk of malignancies in patients with diabetes treated with human insulin or insulin analogues: A cohort study. Diabetologia 2009; 52:1732–44.
39. Nadasen DM, Naidoo M. Patients with type 2 diabetes and difficulties associated with initiation of insulin therapy in a public health clinic in Durban: original research. South African Family Practice 2012; 54:436-40.
40. Kelwade J, Parekh H, Dukle V, et al. How many oral antidiabetic drugs before insulin?. Indian Journal of Endocrinology and Metabolism 2017; 21:249.
41. Kalra S, Balhara YP, Baruah MP, et al. Forum for injection techniques, India: The first Indian recommendations for best practice in insulin injection technique. Indian J Endocrinol Metab 2012; 16:876.
42. Riddle M. Combining sulfonylureas and other oral agents. The American Journal of Medicine 2000; 108:15-22.
43. Kalra S. Aggressive treatment in newly diagnosed diabetes with fixed dose combinations. Medicine 2012; 22:249-53.
44. John M, Gopinath D, Kalra S. Triple fixed drug combinations in type 2 diabetes. Indian Journal of Endocrinology and Metabolism 2015; 19:311.
45. Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 1993:977-86.
46. Bianchi C, Daniele G, Dardano A, et al. Early Combination Therapy with Oral Glucose-Lowering Agents in Type 2 Diabetes. Drugs 2017; 1-8.
47. Sharma S, Tandon VR, Roshi AM. Prescribing Pattern of Oral Antihyperglycaemic Drugs, Rationality and Adherence to American Diabetes Association (ADA) Treatment Guidelines among Type 2 Diabetes Mellitus (T2DM) Postmenopausal Women. Journal of clinical and diagnostic research. JCDR 2016; 10:OC11.
48. Basit A, Riaz M, Fawwad A. Glimepiride: evidence -based facts, trends, and observations. Vasc Health Risk Manag 2012; 8:463-72.
49. Weitgasser R, Lechleitner M, Luger A, et
al. Effects of glimepiride on HbA 1c and body weight in type 2 diabetes: results of a 1.5-year follow-up study. Diabetes research and Clinical Practice 2003; 61:13-9.
50. Müller G, Satoh Y, Geisen K. Extrapancreatic effects of sulfonylureas—a comparison between glimepiride and conventional sulfonylureas. Diabetes Research and Clinical Practice 1995; 28:S115-37.
51. Amate JM, Lopez‐Cuadrado T, Almendro N, et al. Effectiveness and safety of glimepiride and iDPP4, associated with metformin in second line pharmacotherapy of type 2 diabetes mellitus: systematic review and meta‐analysis. International Journal of Clinical Practice 2015; 69:292-304.
52. Dabhi AS, Bhatt NR, Shah MJ. Voglibose: an alpha glucosidase inhibitor. Journal of clinical and diagnostic research. JCDR 2013; 7:3023.
53. Shinozaki K, Suzuki M, Ikebuchi M, et al. Improvement of insulin sensitivity and dyslipidemia with a new α-glucosidase inhibitor, voglibose, in nondiabetic hyperinsulinemic subjects. Metabolism 1996; 45:731-7.
54. Do HJ, Lee YS, Ha MJ, et al. Beneficial effects of voglibose administration on body weight and lipid metabolism via gastrointestinal bile acid modification. Endocrine Journal 2016; 63:691-702.
55. Göke B, Fuder H, Wieckhorst G, et al. Voglibose (AO-128) is an efficient α-glucosidase inhibitor and mobilizes the endogenous GLP-1 reserve. Digestion 1995; 56:493-501.
56. Satoh N, Shimatsu A, Yamada K, et al. An α-glucosidase inhibitor, voglibose, reduces oxidative stress markers and soluble intercellular adhesion molecule 1 in obese type 2 diabetic patients. Metabolism 2006; 55:786-93.
57. Nakamura K, Oe H, Kihara H, et al. DPP-4 inhibitor and alpha-glucosidase inhibitor equally improve endothelial function in patients with type 2 diabetes: EDGE study. Cardiovascular Diabetology 2014; 13:110.
58. Saito N, Sakai H, Suzuki S, et al. Effect of an α-glucosidase inhibitor (voglibose), in combination with sulphonylureas, on glycaemic control in type 2 diabetes patients. Journal of International Medical Research 1998; 26:219-32.
59. Pistrosch F, Köhler C, Schaper F, et al. Effects of insulin glargine versus metformin on glycemic variability, microvascular and beta-cell function in early type 2 diabetes. Acta Diabetologica 2013; 50:587-95.
60. Fang FS, Gong YP, Li CL, et al. Comparison of repaglinide and metformin monotherapy as an initial therapy in Chinese patients with newly diagnosed type 2 diabetes mellitus. Europ J Endocrinol 2014; 170:901.
61. Matsumoto K, Yano M, Miyake S, et al. Effects of Voglibose on Glycemic
Journal of The Association of Physicians of India ■ Vol. 65 ■ July 2017 79
Excursions, Insulin Secretion, and Insulin Sensitivity in Non-lnsulin-ireated NIDDM Patients. Diabetes Care 1998; 21:256-60.
62. Seo C, Sakamoto M, Nishimura R, et al. Comparison of glycemic variability in patients with type 2 diabetes given sitagliptin or voglibose: a continuous glucose monitoring–based pilot study. Diab Technol Therap 2013; 15:378-85.
63. Diabetes Prevention Program Research Group. The 10-year cost-effectiveness of lifestyle intervention or metformin for diabetes prevention. Diabetes Care 2012; 35:723-30.
64. Van Der Aa MP, Elst MA, Van De Garde EM, et al. Long-term treatment with metformin in obese, insulin-resistant adolescents: results of a randomized double-blinded placebo-controlled trial. Nutrition and Diabetes 2016; 6:e228.
65. Chirila C, Zheng Q, Davenport E, et al. Treatment satisfaction in type 2 diabetes patients taking empagliflozin compared with patients taking glimepiride. Quality of Life Research 2016; 25:1199-207.
66. Zhang Y, McCoy RG, Mason JE, et al. Second-line agents for glycemic control for type 2 diabetes: are newer agents better?. Diabetes Care 2014; 37:1338-45.
67. Ikeda S, Kobayashi M, Tajima N. Cost‐effectiveness analysis of voglibose for prevention of type 2 diabetes mellitus in Japanese patients with impaired glucose tolerance. Journal of Diabetes Investigation 2010; 1:252-8.
68. Pankivn VI, Cherniavska IV. Voglibose in Combination of Three Hypoglycemic Agents in the Treatment of Type 2 Diabetes Mellitus. International Journal of Endocrinology. 2016(6.78):37-42.
69. Hari K, Faruqui AA. Efficacy and Tolerability of Ora l Tr ip le Drug Combinat ion (Voglibose, Glimepiride and Metformin) in the Management Type 2 Diabetes Mellitus. JMSCR 2014; 4:746-753.
70. Faruqui AA. Safety and Efficacy of Fixed Dose Combination of Voglibose, Glimepiride and Metformin in Indian Type 2 Diabetes Mellitus Patients. Age (yrs). 2016; 36:78.
71. Rao C, Faruqui AA. Efficacy and safety of oral triple drug combination (voglibose, glimepiride and metformin) in the management of type 2 diabetes mellitus. International Journal of Current Research and Review 2013; 5:20.
72. Jindal A, Jindal M, Kaur M, et al. Efficacy and safety of voglibose as an add-on triple drug in patients of type two diabetes mellitus uncontrolled with glimepiride and metformin in Punjabi population. Indian J Basic Appl Med Res 2014; 3:111-6.
73. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach.
Diabetes Care 2012; 35:1364-79.
74. Evans JL, Balkan B, Chuang E, et al. Oral and injectable (non-insulin) pharmacological agents for type 2 diabetes. 2016.
75. Ceriello A, Gallo M, Candido R, et al. Personalized therapy algorithms for type 2 diabetes: a phenotype-based approach. Pharmgenomics Pers Med 2014; 7:129-36.
76. Gong L, Goswami S, Giacomini KM, et al. Metformin pathways: pharmacokinetics and pharmacodynamics. Pharmacogenetics and Genomics 2012; 22:820-827.
77. Scheen AJ. Clinical pharmacokinetics of metformin. Clin Pharmacokinet 1996; 30:359-71.
78. Graham GG, Punt J, Arora M, et al. Clinical pharmacokinetics of metformin. Clin Pharmacokinet 2011; 50:81-98.
79. Hermann LS. Metformin: a review of its pharmacological properties and therapeutic use. Diabete and metabolisme 1979; 5:233-45.
80. https://www.accessdata.fda.gov/drugsa tfda_docs/label/2009/020496s021lbl.pdf.
81. Murti K, Sethi MK, Dey A, et al. Addition of Voglibose to Glimepiride and Metformin have Better Glucose Control in Diabetics: A Prospective, Parallel-group and Open-label Comparative Study. Internat J Pharmacol 2016; 12:422-8.
Glycemic Pentad Forum: 55 experts
Abhay Sahoo, Kalinga Hospital and SUM Hospital, Bhubaneswar; Abhay Srivastav, Hind Medical College, Lucknow; AH Zargar, Endo care, Advance Centre for Diabetes and Endocrine Care, Srinagar; Altamash Shaikh, Saifee Hospital, Mumbai; Anish Bhel, Apollo Hospital, Mysore; Anuj Maheswari , BBD Medical College, BBD University, Lucknow; Ashish Dengra , Mahi Diabetes T hyr o id Car e Re s ea r ch Ce n t r e , Jabalpur ; Bansi Saboo, Diacare , Ahmedabad; BM Makkar, Diabetes & Obesity Centre, Delhi; Chintan Vyas, SIDS Diabetes Centre, Anand; CR Anand Moses, The Tamilnadu Dr. MGR Medical University, Chennai; Debasis Basu, Apol lo , Kolkata ; Dinesh Agarwal, Caurasiya Nursing Home, Meerut; D Parameswaran, Sri Iswarya Hospital, Coimbatore; GS Kohli, Joy Nursing Home, Delhi; Hemant Thackar, Bhatia Hopspital, Breach Candy Hospital, Mumbai; H Babul Reddy, K I M S Hospital,
Hyderabad; Jagdish Mulchandani, Diabetes & Thyroid Clinic, Delhi; Jejoe Karan Kumar, Abbott, Mumbai; James Sebastian, Maj Hospital , Cochin; Kirti Samudra, Diabetes Care Clinic, New Panvel, Mumbai; KN Manohar , Sharada Medica l Centre, Bangalore; KS Thirupathy, Apollo Hospitals, Karaikudi; Lakshmi L a v a n y a A a l a p a t i , A m e r i c a n Institute of Diabetes & Endocrinolgy, Hyderabad; Manoj Chawla, Lina D i a b e t e s C a r e , M u m b a i ; M K Mukhopadyay, EEFDF Hospital, AMRI Hospital, Kolkata; MK Mohan, MK Nursing Home, Chennai; Mithun Bharatia, Bhartia’s Diabetes Centre, G u w a h a t i ; N a v i n K h i m e s r a , Rajasthan Hospita l , Ahmedabad; Navneet Agarwal, Diabetes Obesity & Thyroid Clinic, Gwalior; Nitin Ranjan Gupta, Integral University, Lucknow; Panneer Selvam, Aruna Diabetes Centre, Chennai; Paramesh, Bangalore Diabetes Centre, Bangalore; PK Goyal, P.K. Goyal Clinic, Delhi; P r a d e e p K a w t r a , D i a b e t e s & Hypertension Clinic, Delhi; Prasanna Kumar, CDEC Hospital, Bengaluru; Prashanth Mappa, Teli Medical Centre, Thalecherry; Praveen Raj, Abbott, Mumbai; Rajesh Agarwal, Diabetes Overweight Thyroid Clinic, Indore; Rajeev Bansal, Heart and Cardiac Centre, Delhi; Rajiv Kovil, Dr. Kovil’s Diabetes Care Centre, Mumbai; Reefa Dsouza, Abbott, Mumbai; RLV Phani Kumar, NRI Hospital, Vi j ayawada ; Roopal Panchani , Aanjaney Endocrine Centre, Baroda; Sanjeev Pathak, Vijayratna Diabetes Diagnost ic & Treatment Centre , Ahmedabad; Shailesh Lodha, EHCC Eternal Heart Care Centre, Jaipur; Sharvil Suresh Gadve, Excel Centre, Kolhapur; Shreeranj Ghodbole, Ruby Hall Clinic, Pune; SM Bandukwala, Lilavati Hospital, Mumbai; Subrata Kundu, Burdwan Critical Care Unit Hosp i ta l , Burdwan ; Sudhindra Kulkarni, Fortis Hospital, Mumbai; Sunil Bansal, Lotus Hospital, Agra; Swapni l Ja in , Yasoda Hospi ta l , Ghaziabad; Vijay Neglur, Jupiter Hospital, Mumbai; Vishal Kastwar, Shreedeep Medica l Care Centre , Jabalpur.