
the association of glutathione transferase a1, m1, p1 and t1 gene ...
Upload
anjali-mishraCategory
view
212download
0
Surg Today (2011) 41:471–476DOI 10.1007/s00595-009-4310-4
Reprint requests to: A. MishraReceived: July 9, 2009 / Accepted: October 14, 2009
Original Article
Glutathione S-Transferase M1 and T1 Polymorphism and Response to Neoadjuvant Chemotherapy (CAF) in Breast Cancer Patients
ANJALI MISHRA1, RICHA CHANDRA
2, PRATEEK KUMAR MEHROTRA1, PRACHI BAJPAI
2, and DEEPA AGRAWAL2
1 Department of Endocrine Surgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Raebareli Road, Lucknow 226014, India2 Cardiovascular Toxicology Division, Indian Institute of Toxicology Research (IITR), Lucknow, India
AbstractPurpose. Response to neoadjuvant chemotherapy (NACT) for breast cancer patients cannot be predicted; however, polymorphism of the glutathione S-transfer-ase genes GSTM1 and GSTT1 can modify the response to chemotherapy. The aim of this study was to establish whether there is an association between the polymor-phism of GSTM1 and GSTT1 and response to NACT.Methods. The subjects of this study were 45 patients with locally advanced breast cancer (LABC), who received the cyclophosphamide, adriamycin, and 5-fl uorouracil (CAF) regimen as NACT. We analyzed the relationship between the genotypes and responses to chemotherapy.Results. The response rates to chemotherapy were better, although not signifi cantly so, in patients with the GSTM1 and GSTT1 null genotypes (odds ratio [OR] 2.06 and 1.45). Similar fi ndings were noted in patients with either or both of the null genotypes (OR 2.67 and 1.16). Among the responders, patients with the GSTM1 and GSTT1 null genotypes had higher rates of complete response following chemotherapy than those with one or more active allele (OR 1.8 and 1.3), although the difference was not signifi cant.Conclusions. There was an association between the polymorphism of glutathione S-transferases and responses to chemotherapy, but the differences were not signifi cant. However, larger studies are needed to investigate the role and effi ciency of GST polymor-phism in predicting response to chemotherapy.
Key words Neoadjuvant chemotherapy · Predicted re-sponse to chemotherapy
Introduction
Breast cancer is one of the most common cancers of women around the world1 and chemotherapy is an inte-gral part of its management. Neoadjuvant chemother-apy (NACT) is currently part of the standard treatment for locally advanced breast cancer (LABC), and anthra-cycline-based chemotherapy regimens are preferred for downstaging breast cancer tumors.2 Response to che-motherapy cannot be predicted,3–5 but polymorphism in genes encoding for metabolizing enzymes and drug transporters can affect drug effi cacy and toxicity.6 Glu-tathione S-transferases (GSTs) are a family of multi-functional enzymes involved in the conjugation reaction between reduced glutathione and a variety of electro-philes. DNA-reactive metabolites of cyclophosphamide and adriamycin, the two most commonly used chemo-therapeutic agents in the treatment of breast carcinoma, are substrates for GST-mediated glutathione conjuga-tion.7 Glutathione S-transferases are divided into four classes: alpha, mu, pi, and theta (α, μ, π, θ), based on amino acid sequence similarity and antibody cross-reac-tivity. Allelic deletions in GSTM1 (μ) and GSTT1 (θ) genotypes result in polymorphism, and complete dele-tion of both the alleles (null-type) is associated with reduced enzyme activity. Few studies have investigated the association between GSTM1 and GSTT1 polymor-phism and the survival of breast cancer patients treated with adjuvant chemotherapy. While some documented a survival benefi t in patients with null genotype, others did not corroborate these fi ndings.8,9 Response to NACT is considered a surrogate marker of long overall survival (OS) and disease-free survival (DFS).10,11 Therefore, if there is a relationship between GST polymorphism and the survival of breast cancer patients, a similar relation-ship should exist between GST polymorphism and response to chemotherapy. Selected studies have inves-tigated the association of GSTM1 and GSTT1 polymor-phism and tumor response to NACT.12,13 This is an

472 A. Mishra et al.: GST and Neoadjuvant Chemotherapy
important association to study, not only for its prognos-tic value, but to determine whether the response to NACT can be predicted, so that an alternative regimen can be offered to patients unlikely to respond to che-motherapy at fi rst instance, rather than to offer it as salvage therapy. This approach will thus help to opti-mize treatment and avoid the sequela of noneffective chemotherapy regimens. We conducted this study to investigate the association between the polymorphism of GSTM1 and GSTT1 genes and the response to NACT.
Patients and Methods
The subjects of this study were 45 patients with locally advanced breast cancer (Stage III as per the 2004 Union Internationale Contre le Cancer or American Joint Committee on Cancer system classifi cation). These patients had received chemotherapy between January 2004 and December 2008, and were being followed up at our outpatient clinic. All patients had pathological documentation of cancer and had staging workup, according to the standard clinical practice at our center. This included fi ne-needle aspiration cytology (FNAC), chest X-ray, abdominal ultrasonography, and bone scan. All patients had a Tru-cut biopsy performed prior to the fi rst cycle of chemotherapy to obtain tissue for study of estrogen receptor (ER), progesterone receptor (PgR), and HER2/neu. The receptor status was ascertained immunohistochemically. All patients received CAF che-motherapy, comprising cyclophosphamide 600 mg/m2, adriamycin 60 mg/m2, and 5-fl uorouracil (5- FU) 600 mg/m2, at 3-weekly intervals. No patients had received radiotherapy or hormonal treatment prior to the che-motherapy. The Ethical Committee of our institution approved the study protocol and informed consent was obtained from all patients. Demographic, clinical, radiological, operative, and histology details, including hormone receptor status and HER2/neu status, of all patients were noted. The response to chemotherapy was clinically assessed 3 weeks after the completion of three cycles of chemotherapy as per the RECIST criteria (Response Evaluation Criteria in Solid Tumors) and was reassessed 3 weeks after the completion of last cycle of chemotherapy.14 Patients were subsequently grouped as responders (complete+partial response) or nonre-sponders (stable+progressive disease). Nonresponders usually received four cycles of docetaxel (100 mg/m2) followed by surgery, while responders usually received six cycles of the CAF regimen followed by surgery.
Genomic DNA was extracted from 5 ml peripheral blood collected in ethylenediamine tetraacetic acid vials using the standard Proteinase K phenol–chloroform method. Polymerase chain reaction (PCR) amplifi cation
was done using a modifi cation of the PCR method for exons 6–7, as described by Bell et al., to establish the presence or absence of the GSTM1 gene.15 GSTT1 gen-otype was determined using a modifi cation of the pro-tocol of Pemble.16 The presence or deletion of GSTM1 and GSTT1 were determined using primer pairs, 5′-GAA CTC CCT GAA AAG CTA AAG C-3′, 5′-GTT GGG CTC AAA TAT ACG GTG G-3′ and 5′-TTC CTT ACT GGT CCT CAC ATC TC-3′, 5′-TCA CCG GAT CAT GGC CAG CA-3′, to synthesize 215 and 480 base pairs, respectively. β-Globin was coamplifi ed as an internal standard, using the primers 5′-CAA CTT CAT CCA CGT TCA CC-3′ and 5′-GAA GAG CCA AGG ACA GGT AC-3′ to synthesize the 268 base pairs. Mul-tiplex PCR was performed in a volume of 25 μl contain-ing 4 dNTP at 200 μM each, 1.5 mM MgCl2, 20 pmol of each primer, 100 ng DNA, and 0.5 units of Taq poly-merase and the reaction buffer. Reaction was initiated by denaturation for 5 min at 94°C. The PCR reaction was set as 35 cycles: at 94°C for 1 min, 58°C for 1 min, and 72°C for 1 min, with a fi nal elongation of 10 min at 72°C. The presence of at least one GSTT1 or GSTM1 allele (non-null genotype) or its complete deletion (null genotype) was confi rmed by running the amplifi ed product on 2% agarose gel. The gel was stained with ethidium bromide and then photographed.
The presence or absence of non-null or null geno-types of GSTM1 and GSTT1 was correlated with the response to NACT (CAF). Pearson’s chi-square test and Fisher’s exact test were done to look for proportions, and the Student t-test was used to establish signifi cant differences in mean values. Overall signifi cance of the null genotype was determined by calculating the odds ratios (OR). The odds ratio was expressed with a cor-responding 95% confi dence interval (CI).
Results
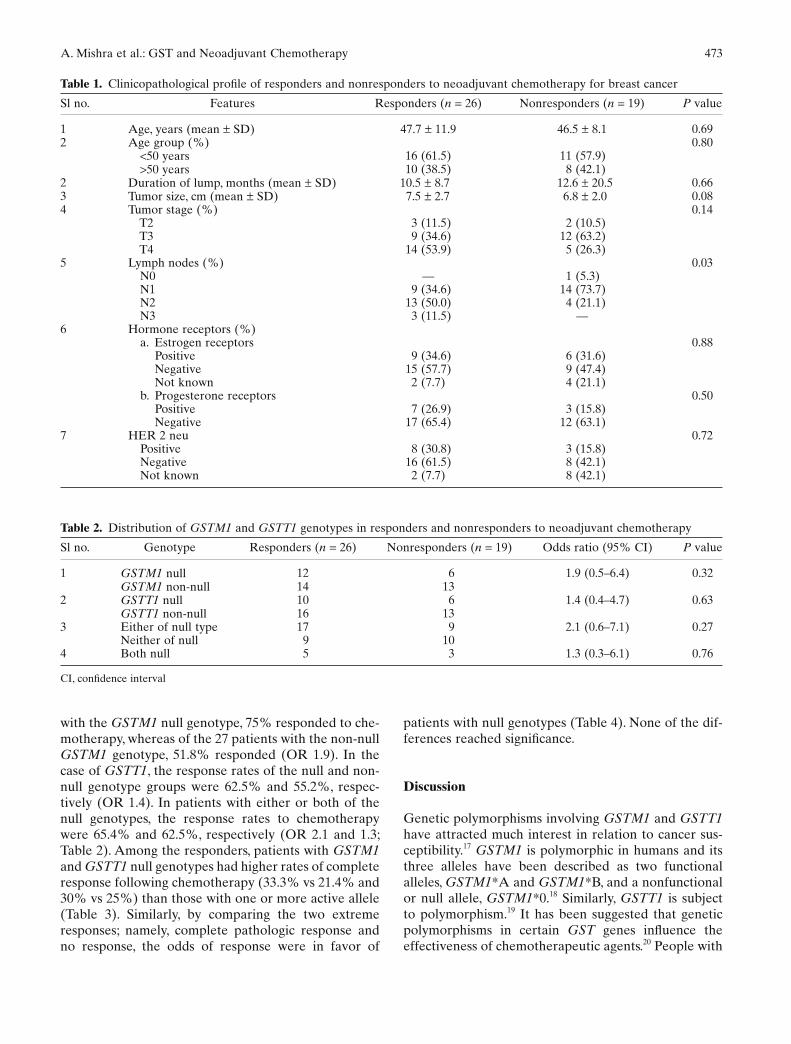
The patients comprised 44 women and 1 man, with a mean age of 47.2 ± 10.4 years (range, 28–75 years). The mean duration of the disease was 11.4 ± 14.2 months (20–84 months) and the mean tumor size prechemo-therapy was 7.1 ± 2.4 cm (2–14 cm). We classifi ed 26 tumors as responsive and 19 as nonresponsive to NACT. Among the responders, 7 showed a complete response and 19 showed a partial response. The clinicopathologi-cal features of the patients were comparable in both groups (Table 1). The overall prevalence of GSTM1 and GSTT1 null genotype in this study was 40% and 35.6%, respectively. Overall, either GSTM1 or GSTT1 was of the null type in 57.81% of patients and both genotypes were of the null type in 17.8%. More of the GSTM1 null-genotype patients than the non-null-genotype patients responded to chemotherapy. Of the 18 patients
A. Mishra et al.: GST and Neoadjuvant Chemotherapy 473
with the GSTM1 null genotype, 75% responded to che-motherapy, whereas of the 27 patients with the non-null GSTM1 genotype, 51.8% responded (OR 1.9). In the case of GSTT1, the response rates of the null and non-null genotype groups were 62.5% and 55.2%, respec-tively (OR 1.4). In patients with either or both of the null genotypes, the response rates to chemotherapy were 65.4% and 62.5%, respectively (OR 2.1 and 1.3; Table 2). Among the responders, patients with GSTM1 and GSTT1 null genotypes had higher rates of complete response following chemotherapy (33.3% vs 21.4% and 30% vs 25%) than those with one or more active allele (Table 3). Similarly, by comparing the two extreme responses; namely, complete pathologic response and no response, the odds of response were in favor of
patients with null genotypes (Table 4). None of the dif-ferences reached signifi cance.
Discussion
Genetic polymorphisms involving GSTM1 and GSTT1 have attracted much interest in relation to cancer sus-ceptibility.17 GSTM1 is polymorphic in humans and its three alleles have been described as two functional alleles, GSTM1*A and GSTM1*B, and a nonfunctional or null allele, GSTM1*0.18 Similarly, GSTT1 is subject to polymorphism.19 It has been suggested that genetic polymorphisms in certain GST genes infl uence the effectiveness of chemotherapeutic agents.20 People with
Table 1. Clinicopathological profi le of responders and nonresponders to neoadjuvant chemotherapy for breast cancer
Sl no. Features Responders (n = 26) Nonresponders (n = 19) P value
1 Age, years (mean ± SD) 47.7 ± 11.9 46.5 ± 8.1 0.692 Age group (%) 0.80
<50 years 16 (61.5) 11 (57.9) >50 years 10 (38.5) 8 (42.1)
2 Duration of lump, months (mean ± SD) 10.5 ± 8.7 12.6 ± 20.5 0.663 Tumor size, cm (mean ± SD) 7.5 ± 2.7 6.8 ± 2.0 0.084 Tumor stage (%) 0.14
T2 3 (11.5) 2 (10.5) T3 9 (34.6) 12 (63.2) T4 14 (53.9) 5 (26.3)
5 Lymph nodes (%) 0.03 N0 — 1 (5.3) N1 9 (34.6) 14 (73.7) N2 13 (50.0) 4 (21.1) N3 3 (11.5) —
6 Hormone receptors (%) a. Estrogen receptors 0.88 Positive 9 (34.6) 6 (31.6) Negative 15 (57.7) 9 (47.4) Not known 2 (7.7) 4 (21.1) b. Progesterone receptors 0.50 Positive 7 (26.9) 3 (15.8) Negative 17 (65.4) 12 (63.1)
7 HER 2 neu 0.72 Positive 8 (30.8) 3 (15.8) Negative 16 (61.5) 8 (42.1) Not known 2 (7.7) 8 (42.1)
Table 2. Distribution of GSTM1 and GSTT1 genotypes in responders and nonresponders to neoadjuvant chemotherapy
Sl no. Genotype Responders (n = 26) Nonresponders (n = 19) Odds ratio (95% CI) P value
1 GSTM1 null 12 6 1.9 (0.5–6.4) 0.32GSTM1 non-null 14 13
2 GSTT1 null 10 6 1.4 (0.4–4.7) 0.63GSTT1 non-null 16 13
3 Either of null type 17 9 2.1 (0.6–7.1) 0.27Neither of null 9 10
4 Both null 5 3 1.3 (0.3–6.1) 0.76
CI, confi dence interval

474 A. Mishra et al.: GST and Neoadjuvant Chemotherapy
the null genotype are less able to detoxify the metabo-lites of several drugs, chemicals, and carcinogens. As a result, they are more susceptible to the development of certain cancers, including breast cancer. On the other hand, because of the same property of these metaboliz-ing enzymes, these people are likely to respond better to chemotherapeutic drugs, resulting in a survival advan-tage.6 The prevalence of GSTM1 and GSTT1 null geno-types varies in different ethnic populations. Various Indian studies have quoted prevalence rates ranging from 22% to 33% for the GSTM1 null genotype and from 17.6% to 18.4% for the GSTT1 genotypes in the normal healthy population.21,22 In a study from south India, breast cancer patients had a high rate of the GSTM1 and GSTT1 null genotype.23 The prevalence of GSTM1 (47.7%) and GSTT1 (36.1%) in this study is similar to that of other published reports.
Recent studies have investigated the association of GST polymorphism and survival in breast cancer patients receiving adjuvant chemotherapy. In a series of 85 patients with metastatic or infl ammatory breast cancer treated with AFM (doxorubicin, fl uorouracil, and methotrexate) chemotherapy followed by high-dose cyclophosphamide, cisplatin, and carmustine, the median survival of patients with null GSTM1 was higher than that of those with one or both copies of the gene (3.5 years vs 1.5 years).8 However, Lizard-Nacol et al. did not fi nd any effect of the GSTM1 genotype on DFS or OS in 92 patients who received primary chemother-apy (CAF).12 Similarly, in another study of 1034 Chinese patients with breast cancers treated by adjuvant chemo-therapy, Yang et al. did not fi nd any relationship between
OS and GSTM1 and GSTT1 polymorphism, but noted the potential role of GSTP1 polymorphism in predict-ing clinical outcome. In their series, patients who carried the low-activity allozyme of GSTP1 had an improved therapeutic outcome, in the form of a 60% reduction in overall mortality. They concluded that genetic polymor-phism might modulate the response to chemotherapy in patients with breast carcinoma. However, since there were no details of chemotherapy regimens in their study, they could not evaluate the association between specifi c chemotherapy and GST polymorphism.9
The results of studies reporting an association between GST polymorphism and the outcome of breast cancer patients receiving adjuvant chemotherapy are signifi cant in prognostication, but cannot be utilized for clinical decision-making. However, the ability to reli-ably predict a patient’s response based on genotype will improve therapeutic decision-making remarkably and save patients from being subjected to unnecessary side effects, which is particularly important for those with LABC. The introduction of NACT has resulted in improved survival and those whose cancers respond well to chemotherapy gain most.10,11 Considering that people with the null genotype have a survival advan-tage, they are more likely to show better response to chemotherapy, despite which very few studies have looked into this association. The authors of one such study of 44 breast cancer patients attempted to predict the response to docetaxel by studying the gene profi les of responders and nonresponders to chemotherapy. They found that nonresponders had elevated expres-sion of genes controlling cellular redox-enzymes, GST
Table 3. Comparison of GSTM1 and GSTT1 null genotype between complete responders and partial responders
Sl no. Genotype Complete response (n = 7) Partial response (n = 19) Odds ratio (95% CI) P value
1 GSTM1 null 4 8 1.8 (0.3–10.5) 0.49GSTM1 non-null 3 11
2 GSTT1 null 3 7 1.3 (0.2–7.5) 0.78GSTT1 non-null 4 12
3 Either of null 6 11 4.3 (0.4–43.7) 0.19Neither of null 1 8
4 Both null 1 4 0.6 (0.1–8.5) 0.69
Table 4. Comparison of GSTM1 and GSTT1 null genotype between complete responders and nonresponders
Sl no. Genotype Complete responders (n = 7) Nonresponders (n = 19) Odds ratio (95% CI) P value
1 GSTM1 null 4 6 2.9 (0.5–17.2) 0.24GSTM1 non-null 3 13
2 GSTT1 null 3 6 1.6 (0.3–9.7) 0.59GSTT1 non-null 4 13
3 Either of null 6 9 6.6 (0.7–66.5) 0.08Neither of null 1 10
4 Both null 1 3 0.9 (0.1–10.3) 0.92

A. Mishra et al.: GST and Neoadjuvant Chemotherapy 475
being one of them, and suggested that administration of chemicals inhibiting redox enzymes to nonresponders might improve their response to chemotherapy.13 In another study consisting of 92 patients who received CAF, Lizard-Nacol et al. did not observe any relation-ship between the GSTM1 genotype and response to chemotherapy, although they noted that no response to chemotherapy was associated with signifi cantly poor DFS and OS.12 These fi ndings seem paradoxical, con-sidering that response to chemotherapy is a surrogate marker for survival, although obviously not out of context because response to chemotherapy may be modulated by many genetic and nongenetic factors.
As previously mentioned, the ultimate goal of these studies is to predict the regimen-specifi c sensitivity of an individual before the initiation of chemotherapy, to optimize the therapy and avoid unnecessary exposure to the side effects of a noneffective chemotherapeutic regimen. One of the members of GST family of genes, GST-π, has been widely studied in this regard. Elevated expression of GST-π has been correlated with resis-tance to cisplatin in lung cancer, and in head and neck cancer.13,24,25 The same gene, with other genes controlling cellular redox-enzymes, was also found to be a predictor of resistance to docetaxel in breast cancer patients.13 Similarly, GSTA1 polymorphism was shown to affect busulfan elimination signifi cantly, suggesting that it could help optimize high-dose therapy by GSTA1 geno-typing in advance.26 GSTM1 and GSTT1 polymorphism might help to predict the response to doxorubicin and alkylating agents.7,27 Moreover, polymorphism of GSTM1, GSTT1, and GST-π has been correlated with toxicities of various cytotoxic agents, including doxoru-bicin, alkylating compounds, cytosine arabinoside, and cisplatin.27–29 In future, as more data become available, we might have more substantial information for predict-ing response and adverse reaction to chemotherapy based on GST polymorphism.
In this series of Indian breast cancer patients, we observed a positive albeit insignifi cant relationship between response to chemotherapy and null genotype of GSTM1 (OR: 1.9) and GSTT1 (OR: 1.4). Breast cancer patients carrying the null genotype showed a better response to chemotherapy, and a complete response was achieved in more of these patients than in those with the non-null genotype. Thus, we conclude that GSTM1 and GSTT1 play a role in modulating response to chemotherapy, although this may not be an individually important factor. However, as there is vari-ability in the prevalence of GST polymorphism across various ethnic groups, and this study has a power of 80% and Alpha 0.05 for detecting signifi cant differences, by assuming that signifi cant difference would be that 90% patients carrying null genotype should be responders and only 10% would be nonresponders. Therefore,
although our fi ndings were not signifi cant, there was still an association between GST polymorphism and the response to chemotherapy. Larger clinical studies are needed to establish the exact signifi cance of GST poly-morphism in predicting responses to chemotherapy.
References
1. Hortobagyi GN, de la Garza Salazar J, Pritchard K, Amadori D, Haidinger R, Hudis CA, et al. The global breast cancer burden: variations in epidemiology and survival. Clin Breast Cancer 2005;6:391–401.
2. Bafaloukos D. Neo-adjuvant therapy in breast cancer. Ann Oncol 2005;16(s-2):174–81.
3. Pusztai L, Symmans FW, Hortobagyi GN. Development of phar-macogenomic markers to select preoperative chemotherapy for breast cancer. Breast Cancer 2005;12:73–85.
4. Vyzula R, Dusek L, Zaloudík J, Demlová R, Klimes D, Selve-kerová S. Breast cancer and neoadjuvant therapy: any predictive marker? Neoplasma 2004;51:471–80.
5. Faneyte IF, Schrama JG, Peterse JL, Remijnse PL, Rodenhuis S, van de Vijver MJ. Breast cancer response to neoadjuvant chemo-therapy: predictive markers and relation with outcome. Br J Cancer 2003;88:406–12.
6. Bosh TM, Meijerman I, Beijnen JH, Schellens JH. Genetic poly-morphisms of drug-metabolizing enzymes and drug transporters in the chemotherapeutic treatment of cancer. Clin Pharmacokinet 2006;45:253–85.
7. Stearns V, Davisson NE, Flockhart DA. Pharmacogenetics in the treatment of breast cancer. Pharmacogenenomics J 2004;4:143–53.
8. Petros WP, Hopkins PJ, Spruill S, Broadwater G, Vredenburgh JJ, Colvin OM, et al. Association between drug metabolism genotype, chemotherapy pharmacokinetics and overall survival in patient with breast cancer. J Clin Oncol 2005;23:6117–25.
9. Yang G, Shu X-O, Ruan Z-X, Cai QY, Jin F, Gao Y-T, et al. Genetic polymorphism in glutathione-S-transferase genes (GSTM1, GSTT1, GSTP1) and survival after chemotherapy for invasive breast carcinomas. Cancer 2005;103:52–8.
10. Fisher B, Bryant J, Wolmark N, Mamounas E, Brown A, Fisher ER, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer J Clin Oncol 1998;16:2672–85.
11. Pierga JY, Mouret E, Laurence V, Diéras V, Savigioni A, Beuzeboc P, et al. Prognostic factors for survival after neoadjuvant chemo-therapy in operable breast cancer. the role of clinical response Eur J Cancer 2003;39:1089–96.
12. Lizard-Nacol S, Coudert B, Colosetti P, Riedinger J-M, Fargeot P, Brunet-Lecome P. Glutathione S transferase M1 null genotype: lack of association with tumour characteristics and survival in advanced breast cancer. Breast Cancer Res 1999;1:81–7.
13. Iwao-Koizumi K, Matoba R, Ueno N, Kim SJ, Ando A, Miyoshi Y, et al. Prediction of docetaxel response in human breast cancer by gene expression profi ling. J Clin Oncol 2005;23:422–31.
14. Therasse P, ArbucSG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst 2000;92:205–16.
15. Bell DA, Taylor JA, Paulson DF, Robertson CN, Mohler JL, Lucier GW. Genetic risk and carcinogen exposure: a common inherited defect of the carcinogen-metabolic gene glutathione-S-transferase M1 (GSTM1) that increases the susceptibility to bladder cancer. J Natl Cancer Inst 1993;85:1159–64.
16. Pemble TR. Molecular epidemiology of the human glutathione-S-transferase genotypes GSTM1 and GSTT1 in cancer susceptibil-ity. Cancer Epidemiol Biomarkers Prev 1997;6:733–43.

476 A. Mishra et al.: GST and Neoadjuvant Chemotherapy
17. Helzlsouer KJ, Selmin O, Huang HY, Strickland PT, Hoffman S, Alberg AJ, et al. Association between glutathione S-transferase M1, P1, and T1 genetic polymorphisms and development of breast cancer. J Natl Cancer Inst 1998;90:512–8.
18. Board PG. Gene deletion and partial defi ciency of the glutathione S-transferase (ligandin) system in man. FEBS Lett 1981;135:2–4.
19. Pemble S, Schroeder KR, Spencer SR, Meyer DJ, Hallier E, Bolt HM, et al. Human glutathione-S-transferase (GSTT1) cDNA cloning and the characterization of a genetic polymorphism. Biochem J 1994;300:271–6.
20. Hayes JD, Pulford DJ. The glutathione-S-transferase supergene family: regulation of GST and the contribution of the isoenzymes to cancer chemoprotection and drug resistance. Crit Rev Biochem Mol Biol 1995;30:445–600.
21. Mishra DK, Kumar A, Srivastava DS, Mittal RD. Allelic variation of GSTT1, GSTM1 and GSTP1 genes in North Indian population. Asian Pac J Cancer Prev 2004;5:362–5.
22. Vettriselvi V, Vijayalakshmi K, Paul SF, Venkatachalam P. Genetic variation of GSTT1, GSTM1 and GSTP1 genes in a South Indian population Asian Pac J Cancer Prev2006;7:325–8.
23. Syamala VS, Sreeja L, Syamala V, Raveendran PB, Balakrishnan R, Kuttan R, et al. Infl uence of germline polymorphisms of GSTT1, GSTM1, and GSTP1 in familial versus sporadic breast cancer susceptibility and survival. Fam Cancer 2008;7:213–20.
24. Bai F, Nakanishi Y, Kawasaki M, Takayama K, Yatsunami J, Pei XH, et al. Immunohistochemical expression of glutathione S-transferase-Pi can predict chemotherapy response in patients with nonsmall cell lung carcinoma. Cancer 1996 1;78:416–21.
25. Shiga H, Heath EI, Rasmussen AA, Trock B, Johnston PG, Foras-tiere AA, et al. Prognostic value of p53, glutathione S-transferase pi, and thymidylate synthase for neoadjuvant cisplatin-based chemotherapy in head and neck cancer. Clin Cancer Res 1999;5:4097–104.
26. Kusama M, Kubota T, Matsukura Y, Matsuno K, Ogawa S, Kanda Y, et al. Infl uence of glutathione S-transferase A1 polymorphism on the pharmacokinetics of busulfan. Clin Chim Acta 2006;368:93–8.
27. Mossallam GI, Abdel Hamid TM, Samra MA. Glutathione S-transferase GSTM1 and GSTT1 polymorphisms in adult acute myeloid leukemia; its impact on toxicity and response to chemo-therapy. J Egypt Natl Cancer Inst 2006;18:264–73.
28. Barahmani N, Carpentieri S, Li XN, Wang T, Cao Y, Howe L, et al. Glutathione S-transferase M1 and T1 polymorphisms may predict adverse effects after therapy in children with medulloblas-toma. NeuroOncology 2009;11:292–300.
29. Oldenburg J, Kraggerud SM, Brydøy M, Cvancarova M, Lothe RA, Fossa SD. Association between long-term neuro-toxicities in testicular cancer survivors and polymorphisms in glutathione-s-transferase-P1 and -M1, a retrospective cross sectional study. J Transl Med 2007;5:70.


















