Global inequality in agriculture, nutrition, and health · 39 Humans globally have similar...
33
Page 1 of 19 1 2 3 4 5 6 7 8 9 10 Global inequality in agriculture, nutrition, and health Winnie Bell, MS 1 , Keith Lividini, MS 1,2 , and William A. Masters, PhD* 1 This version last revised 29 June 2020 11 12 13 14 Author affiliations and postal addresses: 15 1. Friedman School of Nutrition Science & Policy, Tufts University, 150 Harrison Ave., Boston MA 16 20111, USA 17 2. HarvestPlus, International Food Policy Research Institute (IFPRI), 1201 Eye St NW, Washington 18 DC 20005, USA 19 Contact author details: 20 * Email: [email protected]; phone: +1.617.636.2751 21 22 Contributions: 23 WB and KL assembled the data and developed the model code. WB prepared the first draft. KL and 24 WAM reviewed and edited the manuscript. WAM conceived the study. 25 26 Acknowledgements: 27 We are grateful to the Wellcome Trust and the London School of Hygiene and Tropical Medicine for 28 their support of this project, and specifically to Alan Dangour and Bhavani Shankar for initiating this 29 work. 30 31 32 33
Transcript of Global inequality in agriculture, nutrition, and health · 39 Humans globally have similar...

Page 1 of 19
1 2 3 4 5 6 7 8 9
10
Global inequality in agriculture, nutrition, and health
Winnie Bell, MS1, Keith Lividini, MS1,2, and William A. Masters, PhD*1
This version last revised 29 June 202011 12 13 14
Author affiliations and postal addresses: 15 1. Friedman School of Nutrition Science & Policy, Tufts University, 150 Harrison Ave., Boston MA16
20111, USA17 2. HarvestPlus, International Food Policy Research Institute (IFPRI), 1201 Eye St NW, Washington18
DC 20005, USA19
Contact author details: 20 * Email: [email protected]; phone: +1.617.636.275121
22 Contributions: 23
WB and KL assembled the data and developed the model code. WB prepared the first draft. KL and 24 WAM reviewed and edited the manuscript. WAM conceived the study. 25
26 Acknowledgements: 27
We are grateful to the Wellcome Trust and the London School of Hygiene and Tropical Medicine for 28 their support of this project, and specifically to Alan Dangour and Bhavani Shankar for initiating this 29 work. 30
31 32 33

Page 2 of 19
34 Global inequality in agriculture, nutrition, and health 35
36 Abstract 37
38 Humans globally have similar nutritional needs but face large differences in natural resource 39 endowments and local food production. This study quantifies food system inequality across 40 countries based on natural resource inputs, food/nutrient outputs, and nutrition/health outcomes, 41 from 1970 to 2010. Animal source foods and overweight/obesity show rapid convergence while 42 availability of selected micronutrients demonstrate slower convergence; however, all variables 43 are more equally distributed than national income per capita, whose Gini coefficient declined 44 from 0·71 to 0·65. Inequalities in total and animal-source dietary energy declined from 0·16 to 45 0·10 and 0·55 to 0·36, respectively. There was convergence in overweight/obesity prevalence 46 from 0·39 to 0·27, while undernutrition and stunting became increasingly concentrated in a few 47 high-burden countries. Characterizing cross-country inequalities in agricultural resources, foods, 48 nutrients, and health can help identify critical opportunities for agriculture and food policies, as 49 well as aid in prioritizing research objectives and donor funding for the coming decade. 50
51 Funding: Wellcome Trust 52
53 54 55

Page 3 of 19
The distribution of agricultural resources and food supplies is a central determinant of human 56 development and health outcomes, because nutritional needs are similar across locations but 57 people live in diverse environments with limited agricultural resources (Rockstrom et al. 2016). 58 Previous research on inequality has found convergence across countries in some aspects of the 59 food system such as dietary patterns (Bentham et al. 2020, Popkin 2017, Khoury et al. 2014), but 60 inequities in other aspects of global food systems have not yet been quantified and may have 61 worsened or improved as conditions change (Hawkes et al. 2009, Baker and Friel 2016). 62 63 This paper quantifies the degree of convergence across countries in food system inputs 64 (agricultural resources), outputs (food and nutrients) and outcomes (nutrition and health), using 65 Lorenz Curves and Gini coefficients to measure inequality in each outcome over the 40-year 66 period from 1970 to 2010. These methods were developed to study inequality of income and 67 wealth, and later applied to other aspects of well-being and human capabilities in general (Sen 68 1979), as well as social epidemiology (Wagstaff et al. 1991, Harper and Lynch 2017), with other 69 applications for example on water use (Seekell et al. 2011, Guragai et al. 2017), industrial goods 70 (Steinberger et al. 2010), carbon emissions and energy use (Groot 2010, Lawrence et al. 2013) 71 and subjective well-being (Gluzmann and Gasparini 2017). 72 73 Previous work on nutrition and health disparities such as Afshin et al. (2019) focuses on average 74 levels of each variable. Our focus on inequality is designed to help visualize and quantify the 75 magnitude of relative deprivation and the location of relative scarcity around the world from 76 1970 to 2010, and thereby reveal the degree to which some countries have caught up while 77 others fall behind changes in other regions. Results reveal whether convergence in availability of 78 harmful dietary components and negative health outcomes occurs faster than convergence in 79 beneficial nutrients and other positive outcomes, and how inequality in nutritional and health 80 outcomes relate to inequalities in national income and natural resources. These findings can help 81 guide agriculture and food policies, as well as prioritize research objectives and donor funding to 82 help achieve the UN Sustainable Development Goals and other targets linked to global food 83 systems. 84
Results 85
Findings for each variable are shown in Lorenz curves and quantile plots to quantify inequality 86 across countries, using a standardized scale for each variable. Each geographic region is color-87 coded to show how countries’ rank in the global distribution differs across variables and changes 88 over time. Lorenz curves show each country’s share of the cumulative proportion of the 89 population on the horizontal axis and the cumulative proportion of the variable of interest on the 90 vertical axis, plotted generally for 1970 and 2010. A 45-degree line indicates the line of perfect 91 equality against which the Gini coefficient of inequality can be calculated. Each country is a line 92 segment whose horizontal run represents the country’s share of the world population. To 93 complement the Lorenz curves, we use quantile plots, also known as Pen’s parade or ‘parade 94 plots’, showing the absolute level of each variable with a bar width that corresponds to the 95 country’s population size. 96 97
Inequality in Gross Domestic Product (GDP), land, and livestock 98 Equality in Gross Domestic Product (GDP) per capita (a measure of total income and 99 expenditure) has changed between 1970 and 2010. The between-country equality of GDP 100

Page 4 of 19
distribution has improved in the past 40 years for the bottom 80 percent of the global population 101 (Figure 1 upper), reflected by the shift of the Lorenz curve towards equality and the decreasing 102 Gini coefficient (from 0·71 to 0·65). This observation is in line with other empirical work that 103 has found that within-country inequality is more concerning than between-country inequality at 104 this stage (Milanovic 2011, 2016). We further observe an increase in the mean GDP rising by 105 ~16% globally and a clear reordering of countries whereby Sub-Saharan African (SSA) countries 106 were in the middle of the distribution in 1970 but by 2010 largely occupy the bottom of the 107 distribution as they have been displaced largely by the rise of China (CH) (Figure 1 lower). 108 109
Figure 1: Gross domestic product per capita 110
111 112 Figure 2 (top-left panel) reveals that 20% of the world's rural population in the most land-scarce 113 countries rely on less than 10% of the world's harvested area with little change between 1970 and 114 2010. In contrast the most land-abundant countries – representing only 20% of the global rural 115 population -- account for almost 60% of the world's harvested area (upper portion of the curve). 116 The Gini coefficient rose slightly from 0·42 to 0·43 between 1970 and 2010. In absolute terms, 117 harvested area has remained essentially the same (bottom left panel) between time periods with 118 only a slight decrease in the global mean (6.16 to 5.98 ln ha/rural capita). 119 120

Page 5 of 19
Figure 2: Area harvested per rural capita and livestock units per rural capita 121
122 123
Figure 2 (right panel) also shows the major livestock units (LSU) per rural capita and indicates 124 the stocks of major livestock types. LSU per capita has increased between 1970 and 2010 for the 125 middle portion of the Lorenz curve while the Gini has decreased from 0·53 to 0·48; however, for 126 the lower 20% and upper 10% of the global population the distribution has remained largely 127 unchanged. About 50% of the LSU are held by the top 15% of the global population. In absolute 128 terms, the global rural per capita LSU has remained essentially the same between time periods 129 increasing slightly from 5.76 to 5.86 LSU/capita. 130
131
Inequality in foods and nutrients 132 To what degree has inequality of income, agricultural land and livestock been overcome to 133 equalize nutrition? Fruit and vegetable consumption has consistently been more equal than 134 income or land distribution, but consumption of animal-source foods had been very unequal in 135 1970 and equalized greatly by 2010 (Figure 3). The worldwide Gini coefficient for ASF/capita 136 plummeted from 0·55 to 0·36 as China (CH) and others moved up in the global ranking, leaving 137 roughly a fifth of the world population with ASF consumption below 10% of dietary energy. 138
139 Dietary energy from fruits and vegetables (F&V) has increased in the past 40 years from 108 to 140 205 kcal/capita, again with significant increases in China. However other countries, particularly 141 in SSA, remain below the mean and for some the amount of energy from F&V has stayed the 142

Page 6 of 19
same or decreased (e.g. Nigeria) (Figure 3, right panel). The Lorenz curve shows that the roughly 143 doubling in available energy from F&V has been generally evenly distributed, reflected in the 144 Gini shifting from 0·35 to 0·27 and only the lowest 15% of the global population not moving 145 towards the line of equality. 146
147
Figure 3: Energy from animal source foods and from fruits and vegetables 148
149 150 Turning to nutrients, vitamin A availability per capita has remained largely unchanged from 151 1970 to 2010, falling slightly from 783 mcg/capita to 719 mcg/capita (Figure 4, panel 1), the 152 vitamin A “poverty” gap decreased as equality increased over that time period (reduction in Gini 153 from 0·35 to 0·28) for the population within the 10th to 80th percentiles. Zinc availability has 154 increased over the past 40 years with the global mean rising from 13·9 mg/capita to 16·3 155 mg/capita (Figure 4, panel 2). Equality of zinc availability across countries has also increased, 156 evidenced by the change in Gini coefficient from 0·19 in 1970 to 0·13 in 2010. The increase in 157 equality has again resulted in redistribution of the global rankings as China has displaced 158 countries such as India, Mexico, Ethiopia and Pakistan backward in the global ranking. 159 160

Page 7 of 19
Figure 4: Micronutrient availability per capita 161
162 163 For dietary iron, mean availability per capita has increased from 17·6 mg/capita to 21·3 164 mg/capita between 1970 and 2010 (Figure 4, panel 3). Equality has increased but only in the 165 upper 50% of the distribution. Of note is that iron availability in China increased significantly, 166 thrusting China from within the lower 35% to the upper 30%. The Gini has decreased slightly 167 from 0·16 to 0·12. These results for dietary iron and zinc may mask inequality in diet quality and 168 nutritionally available minerals, because diets dominated by vegetal foods may be high in 169 compounds such as phytates and oxalates that bind these elements, and . To the extent that 170 bioavailability varies across the distribution based on availability of ASF and other factors, the 171 inequality profile of bioavailable iron and zinc are likely to look different. 172 173 Among other nutrients, availability of protein (g/capita) also increased and became more equal 174 (Supplementary material), evidenced by the Lorenz curve shift toward equality and the lower 175 slope on the Parade graph for 2010. Mean availability increased from 76·4 g/capita in 1970 to 176 92·4 g/capita in 2010; however, countries in SSA have increasingly fallen below the mean as 177 large countries such as China, Brazil and Mexico have increased their protein availability at 178 faster rates. Overall, the Gini coefficient for protein availability decreased from 0·20 in 1970 to 179 0·14 in 2010. Availability of fat in the food supply has also increased (Supplementary material), 180 from 61·2 g/capita in 1970 to 88·1 g/capita in 2010, a 44% increase in per capita fat availability. 181 This change has largely been attributed to increased availability of plant oils (e.g. soybean and 182

Page 8 of 19
palm oil) and ASF (e.g. milk, bovine meat and poultry). Availability has also equalized 183 significantly, as the global Gini fell from 0·38 to 0·24 between 1970 and 2010 and affects all but 184 those countries that comprise the lowest 10% of the global population. 185
186 187
Inequality in anthropometric outcomes 188 Next, we examine health and diet-related nutrition outcomes. Stunting prevalence – an indicator 189 of child development – is measured as the percentage of children under five years of age that are 190 at least two standard deviations below the median height for age. The Parade plot shows a 191 significant decrease in global mean stunting from 35·0% to 22·0%, a change of nearly 15 192 percentage points. Despite these improvements, the advances have not benefited all countries 193 evenly, as those in the upper 40% of the population have remained in a similar position over the 194 40-year period. The bowing in the lower portion of the Lorenz curve demonstrates the increasing195 disparity and concentration of stunting among fewer countries, which is reflected in the Gini 196 coefficient changing from 0·23 to 0·29 (Figure 5, panel 1). 197
198 Prevalence of underweight is defined as body mass index (BMI) <18·5 for men and women over 199 18 years of age. Globally, underweight has decreased 33% from a mean prevalence of 14·5% to 200 9·7% between 1975 and 2010. Countries in South Asia and East Asia carry the burden of 201 underweight, reflected in the Lorenz curve where India and Pakistan remain in the top 20% of 202 the population of underweight in both time periods. Other areas of the world have experienced a 203 decrease in underweight thereby pushing the Lorenz curve further away from equality as the 204 disparity between countries becomes more pronounced (Figure 5, panel 2). 205
206 In parallel with the decrease in underweight, the prevalence of overweight/obesity, defined as a 207 BMI >25 for men and women over 18 years of age, has increased 15 percentage points from a 208 mean prevalence of 21·4% in 1975 to nearly 36·3% in 2010 (Figure 5, panel 3). The global 209 increase is becoming more equalized, indicated by the decreased Gini from 0·39 to 0·27 and 210 demonstrated by the shift in the Lorenz curve toward equality. 211
212 213 214 215 216 217

Page 9 of 19
Figure 5: Stunting per children <5, underweight, and overweight per adult population 218
219 220
Inequality in diet-related diseases 221 Raised blood pressure (RBP) is a diet-related disease whose risk factors include high sodium 222 and/or low potassium intake, low physical activity, stress, etc., and is defined as having blood 223 pressure above 140+ mm Hg (systolic bp) or 90+ mm Hg (diastolic bp). The Lorenz curves for 224 women and men show increasing inequality in the global distribution of RBP with smaller 225 changes for women (0·16 in 1975 and 0·13 in 2010) compared to men (0·17 in 1975 to 0·09 in 226 2010). Over this period, mean RBP prevalence decreased from 25.7% to 21.3% for women and 227 29.0% to 25.0% for men; however, countries have reordered. Figure 6 shows that women and 228 men in higher income regions have shifted from the right to the left-hand side of the distribution 229 between 1975 and 2010. This is particularly striking in the case of women (Figure 6, panel 1), 230 where in 2010, SSA and South Asian countries are now clustered on the right-hand side of the 231 distribution as a result. The lower prevalence in high-incomes countries is likely due to 232 improvements in detection and treatment, in addition to changes in risk factors (NCD RisC, 233 2017b). Other reasons for the decreased prevalence of RBP, particularly in middle-income 234 countries, might include unmeasured improvements in childhood nutrition and year-round 235 availability of fruits and vegetables (NCD RisC, 2017b). 236 237

Page 10 of 19
Figure 6: Raised blood pressure, female and male 238
239 240 The prevalence of diabetes – measured as having either a fasting plasma glucose of 7·0+ 241 mmol/L, a diabetes diagnosis, or using insulin or oral hypoglycemic drugs – is a rising concern 242 worldwide. The Lorenz curve and Gini coefficient show greater inequality for women (Gini: 243 0·12 to 0·15) but greater equality for men (Gini: 0·14 to 0·11) between 1980 and 2010 244 (Supplementary material). In contrast to RBP the mean prevalence of diabetes has increased 245 from 5·0% to 7·7% (or 53·9%) for women and from 4·2% to 8·4% for men (or 98·6%) between 246 1980 and 2010, with countries in South Asia, East Asia and the Pacific, the Middle East and 247 North Africa, and Latin America and the Caribbean carrying most of the increase. In addition, 248 the number of adults affected has also increased, with a higher burden in low- and middle-249 income countries (LMICs) more than in high-income countries (NCD RisC, 2016b). 250 251
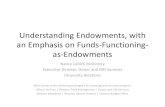
Comparing inequality across domains of agriculture, food and health 252 Figure 7 provides Gini coefficients ordered from the largest to smallest value in 1970. The most 253 uniform distributions around the world are for select foods and nutrients and non-communicable 254 diseases, whereas the most unequal distributions are generally for GDP, agricultural resources, 255 and anthropometric outcomes. 256 257 GDP is the most unequal of the variables shown. Irrigated land, LSU, and area harvested have 258 relatively high and sustained Gini coefficients as well. Despite this observation, equality 259

Page 11 of 19
increased substantially for energy from ASF and to a lesser extent energy from F&V. 260 Correspondingly, inequality in the availability of nutrients has greatly reduced, most 261 significantly for dietary fat. With respect to outcomes we observe increased equality in 262 overweight/obesity. On the other end of the spectrum child stunting and total underweight have 263 become more highly concentrated in a few high-burden countries. 264 265
Figure 7: Levels and changes in Gini coefficients (1970 and 2010) 266
267 268 269 Strengths and limitations 270 This research quantifies the level of inequality across countries in agriculture, food, nutrition, 271 and health, providing a unified view of whether and how the world food system has converged 272 from 1970 to 2010. The work aims to identify patterns whose causes could be investigated in 273 future research. A strength of this approach is that it enables summarizing a large amount of 274
0.00 0.10 0.20 0.30 0.40 0.50 0.60 0.70
Diabetes (pct of women 18+)**
Diabetes (pct of men 18+)**
Raised blood pressure (pct of women 18+)*
Raised blood pressure (pct of men 18+)*
DIET-RELATED DISEASES
Stunting (pct of children <5)#
Overweight & obesity (pct women 18+)*
Overweight & obesity (pct total pop 18+)*
Overweight & obesity (pct men 18+)*
Underweight (pct women 18+)*
Underweight (pct of total pop 18+)*
Underweight (pct of men 18+)*
ANTHROPOMETRIC OUTCOMES
Starchy staples (kcal per capita)
Energy (kcal per capita)
Iron (mg per capita)
Zinc (mg per capita)
Protein (g per capita)
Fruits and vegetables (kcal per capita)
Vitamin A (mcg per capita)
Fat (g per capita)
Animal source food (kcal per capita)
FOODS AND NUTRIENTS
Area harvested (ha per rural person)
Livestock units (units per rural capita)
Irr igated land (ha per rural capita)
Gross domestic product (constant 2010 USD per capita)
GDP AND AGRICULTURAL RESOURCES
2010 1970
Note: Data shown are Gini coefficients, ranging from unity (complete inequality) to zero (perfect equality), constructed as detailed in the text from national totals in 2010 compared to 1970 or the earliest available year, denoted *= 1975, ** =1980, #Years for stunting data vary by country.

Page 12 of 19
information both succinctly (using the quantitative Gini coefficient) and intuitively (by utilizing 275 visualizations that show relative changes between countries). A principal limitation is that we 276 measure inequality between countries only while many observers are additionally interested in 277 inequality within countries and for which different kinds of data would be needed. For national 278 totals, the available data vary, for example regarding the quality and completeness of the 279 underlying Food Balance Sheets (FBS). These data are sourced from estimated production and 280 non-food uses, as well as international trade records for major crops and livestock products with 281 limited information on the diverse items that do not enter commodity markets such as garden 282 produce and wild foods. In addition, data that are included vary in quality as only some estimates 283 come from official national accounts (38% in 2005 and 61% in 2010) while the rest are filled in 284 through additional triangulation methods (FAO, 2013). 285
Discussion 286
We found that despite high and sustained levels of between-country inequality in per capita 287 income and food system resources, food and nutrient availability and health outcomes have 288 become more equally distributed around the world. The largest and most persistent inequalities 289 relate to the agricultural resources used by each country’s rural population. Across Asia and 290 other regions where population growth has slowed rapidly, continued out-migration from rural 291 areas put an end to decades of shrinking farm sizes, allowing the remaining farmers to cultivate 292 increasing land area from year to year. This ‘structural transformation turning point’, when 293 average farm sizes stop shrinking and start expanding, happened around 1914 in the United 294 States, and eventually spread from East Asia in the 1970s across Southeast and South Asia in the 295 2000s (Tomich et al. 2015). For SSA as a whole, that turning point will not occur until after 296 2050, despite rapid growth of cities, due to the continent's very young population and the large 297 fraction of its population whose livelihoods depend on agriculture (Masters et al. 2018). 298 299 Poor diets are one of the leading risk factors for death and disease globally (Forouzanfar et al., 300 2015). Our results show that all foods and nutrients are more equally distributed in 2010 301 compared to 1970. The greatest absolute changes in the Gini were observed for energy from ASF 302 (20 percentage points) followed by total dietary fat (14 percentage points). Increased equality of 303 the global distribution of additional foods and nutrients are observed in the data to a lesser extent 304 in absolute terms (ranging from 2-7 percentage points), though percent reductions ranged from 305 13% in the case of starchy staples to 41% for overall dietary energy. Despite the shift towards 306 greater equality, consumption of most healthy foods remains sub-optimal. For example, findings 307 from the 2002-2003 World Health Survey found that 77·6% of men and 78·4% of women in 52 308 (mostly) LMICs consumed less than the five servings (or 400 g) of F&V per day recommended 309 by the World Health Organization. This is particularly concerning as low intake of fruit is one of 310 the top three contributors -- along with high intake of sodium and low intake of whole grains -- 311 accounting for half of all diet-related deaths and two-thirds of diet related DALYs (Afshin et al., 312 2019). 313 314 We find that convergence of several potentially harmful outcomes has occurred faster than 315 convergence of several beneficial outcomes. Trade and markets have been critical in increasing a 316 more equitable global distribution of food and nutrients, and ultimately health outcomes, given 317 the inherent inequality of agricultural resources and food production across countries (Wood et 318 al., 2018). Yet, trade and well-functioning markets have not benefitted the equitable distribution 319

Page 13 of 19
of all foods and nutrients, and the impact on nutrition and health outcomes is mixed. The equal 320 distribution of potentially unhealthy foods (e.g. ASF) and nutrients (e.g. fat) has increased more 321 rapidly, compared to the distribution of healthy foods and nutrients such as F&V, zinc, iron, and 322 Vitamin A. In addition to trade and functioning markets allowing for increased availability of 323 diverse foods and nutrients, other factors such as consumer preferences, relative prices, and 324 marketing of (unhealthy) foods have further contributed to the observed patterns of convergence. 325 The nutrition and health implications related to these dietary changes have contributed to 326 decreases in stunting and underweight (Black et al. 2013), but also increases in overweight and 327 obesity (NCD RisC, 2016a; NCD RisC, 2017a), and non-communicable diseases like diabetes 328 (NCD RisC, 2016b). 329 330 In sum, our results show that inequality between countries generally declined from 1970 to 2010 331 but did so very differently across the outcomes of interest. Most importantly for nutrition policy, 332 stunting has become increasingly concentrated in a few high-burden countries, allowing 333 interventions aimed at child growth to focus on those locations. Other results identify additional 334 opportunities for agriculture and food policy interventions at global and national levels, as well 335 as provide insight for prioritizing research objectives and donor funding to achieve the UN 336 Sustainable Development Goals and other targets linked to global food systems. 337
Methods 338
Data 339 Data for this paper were drawn from a variety of publicly available sources (Table AX, 340 Supplementary). The variable for Gross Domestic Product (GDP) per capita is reported in 2010 341 dollars and comes from the World Bank World Development Indicators (World Bank, 2019). 342 This variable shows each country’s total production. Variables for area harvested, livestock 343 units, and inputs (irrigated land and fertilizer use) come from the United Nations Food and 344 Agriculture Organization (FAO) FAOSTAT with most data available (FAO, 2019). Livestock 345 units (LSU) are a reference unit that allows for the aggregation of different types and sizes of 346 livestock based on the feed requirements of each species and category. The LSU reference unit is 347 equivalent to the amount grazed by one adult dairy cow producing 3000 kg of milk annually that 348 is not fed any additional foods. 349 350 The food and nutrient supply variables, including overall dietary energy, other macronutrients 351 and micronutrients come from the Nutrient Balance Sheet (NBS) database. NBS is a new dataset 352 which parallels the FAO’s food balance sheets (FBS), matching the 97 food categories in the 353 FBS with the nutritional composition of roughly 1000 foods to track the global flow of 33 354 nutrients through production, international trade, animal feed, seed, manufacturing, waste, and 355 human consumption (publication forthcoming) in terms of the originating primary commodity 356 equivalents1. Data are currently available for 1961-2013. From this dataset dietary energy was 357 further disaggregated into variables for energy from animal source foods, energy from fruits and 358 vegetables, and energy from starchy staples. 359 1 The NBS was developed specifically to examine changes in production, international trade, food system transformations and availability of nutrients over time. While other databases have been developed that provide estimates of nutrient availability based on FBS data (Smith, 2016; Schmidhuber, 2019), these databases do not include additional FBS-related variables.

Page 14 of 19
360 FBS show supply-side variables on the left-hand side of the balance equation (production, 361 imports and exports) and demand-side variables on the right (supply used as seed, feed, food 362 manufacturing, other use, waste, and food) for 97 food categories. In the NBS, FBS food 363 category definitions of primary originating food forms were used to match the FBS categories 364 (which may each include many individual food commodities) to food items in the USDA SR 365 legacy database available at Food Data Central (USDA, 2018). The food composition table 366 (FCT) information for each nutrient including the edible portion of each food item, was then 367 collapsed as an average of the food items corresponding to each FBS food category and 368 multiplied by the FBS food category quantity to standardize the FBS for each macro- and 369 micronutrient. The data were then converted into per capita values using country-specific annual 370 population totals (see below) for 173 countries. 371 372 Data for adult nutrition outcomes and health variables come from the NCD Risk Factor 373 Collaboration (NCD-RisC) comprised of a network of health scientists around the world who 374 work in collaboration with the World Health Organization (WHO). Three different sources of 375 data from the NCD-RisC were used for measuring body mass index (BMI), blood pressure and 376 diabetes. The data on adult underweight and overweight were taken from a pooled analysis of 377 1·698 population-based adult BMI studies with over 19·2 million participants from 189 378 countries. Both the mean BMI and the prevalence were used with standard cut-offs for BMI 379 categories applied in the original analysis (<18·5 kg/m2 [underweight] and >25·0 kg/m2 380 [overweight and obesity] (NCD RisC, 2016a). Stunting data come from the Joint Monitoring 381 Programming, a collaboration between the World Bank, the World Health Organization, and 382 UNICEF. The number of data observations varies by country and the years of data collection are 383 staggered. 384
The variable for blood pressure – defined as systolic blood pressure of 140 mm Hg or higher or 385 diastolic blood pressure of 90 mm Hg or higher -- is based on 1·479 population-based 386 measurement studies with 19·1 million participants (NCD RisC, 2017b). Trends in diabetes 387 prevalence, measured as the fasting plasma glucose of 7·0 mmol/L or higher, or history of 388 diagnosis with diabetes, or use of insulin or oral hypoglycemic drugs, were drawn from a pooled 389 analysis of 751 population-based studies with 4·4 million participants from 146 countries (NCD 390 RisC, 2016b). NCD-RisC uses Bayesian hierarchical models to estimate trends over time in 200 391 countries and all data are age-standardized to the WHO standard population by taking weighted 392 means of age–sex-specific estimates, with use of age weights from the standard population. 393
Demographic information including rural population, total population, women over 18 years of 394 age, men over 18 years of age, and children under five are drawn from the United Nations 395 Population Division (UN DESA), who produce country-level estimates of urban and rural 396 populations by age and sex from 1950 through 2015. For all variables, estimates for rural and 397 urban populations come from the World Urbanization Prospects, 2018 Revision. 398 399
Data cleaning and variable transformation 400 All analyses compare data between 1970 and 2010 or use the closest available years. To provide 401 comparability across years, data are presented for both timepoints based on currently existing 402 territories (e.g. Ethiopia and Eritrea are presented individually for 1970 rather than the combined 403

Page 15 of 19
Ethiopia PDR for 1970). To do so, the per capita value of the “parent” country for the earlier 404 timepoint (e.g. Ethiopia PDR) was applied to each constituent (i.e. Ethiopia and Eritrea) for that 405 year, and the estimated population of each constituent territory was applied using information 406 from UNDESA to avoid under- or double-counting of the applicable population. The UN DESA 407 population estimates use contemporary country borders for past, present, and future estimates 408 (see Supplementary Materials for list of countries with territory changes). 409 410 Several variables required additional cleaning and transformation. Area harvested sums hectares 411 of all crops produced by country and year. Energy from fruits and vegetables and energy from 412 animal source foods sum the energy from fruit and vegetables or animal source foods available 413 by each country and year. Total overweight and obesity and total underweight combine the 414 original NCD RisC data which are presented separately for men and women into a single value. 415 For stunting, given the varied observations per country and the different years available, we 416 selected the earliest data point and the most recent data point for each country. For the earlier 417 time period, most fall between 1983 and 2005; however, there are several countries that first 418 collected stunting prevalence for the first time in 2006 (Belize, South Sudan, Sudan). For the 419 most recent time point, most countries have an observation that falls between 2005 and 2018 but 420 for a few countries the most recent measure comes before 2005 (Bahrain (1995), Mauritius 421 (1995), Czech Republic (2001), Romania (2002), Fiji (2004), Lebanon (2004)). 422 423 All available countries, regardless of population size, were retained in the sample. When 424 considering absolute levels, outliers were included but truncated so as not to affect the optics of 425 the distribution. For several highly skewed variables (e.g. area harvested, livestock units) the 426 natural log was taken. The regional groupings used are based on the World Bank region 427 classification and were separated into seven distinct regions: East Asia and Pacific, Europe and 428 Central Asia, Latin America and the Caribbean, Middle East and North Africa, North America, 429 South Asia, and Sub-Saharan Africa (World Bank, 2018). All countries were matched across 430 datasets using the International Organization for Standardization (ISO) 3166-1 alpha-3 codes 431 (ISO 3) and ISO numeric country codes. 432 433
Data analysis 434 Global inequality can be measured at three different levels, each with varying degrees of nuance. 435 The most basic approach measures unweighted international inequality, where each country 436 counts the same. With this approach, the country is the unit of observation and uses a per capita 437 measure but does not take account of the population. A second approach is population-weighted 438 international inequality in which the mean value of each country is weighted by the population. 439 This approach says nothing about within-country distribution of resources and assumes equal 440 distribution of resources within the country. The third option is to use actual individual level data 441 and calculate inequality across all individuals in the world from poorest to richest (Milanovic 442 2005). 443 444 For our analyses, we use the population-weighted measure of inequality, where the country is the 445 unit of observation, but accounting for population size. Using this method, we are able to draw 446 conclusions about the overall levels of inequality (land, food, nutrients etc.) but cannot draw any 447 conclusions about the within-country distribution of resources. This is an oversimplification of 448 reality in which within-country nutrition and health inequality is a critical concern, and often 449

Page 16 of 19
associated with income, education, and other socio-economic factors, but the objective of this 450 analysis is to show global trends across countries. 451 452 We use techniques borrowed from the field of economics and applied in an innovative way to 453 provide a stylized picture of the distribution of resources. We use Lorenz curves to show how 454 inequality has changed over time. The Lorenz curve is a graphical representation with each 455 country’s share of the cumulative proportion of the population on the horizontal axis and the 456 cumulative proportion of the variable of interest on the vertical axis. The Lorenz curves are 457 plotted for two time points (generally 1970 and 2010, depending on data availability) with a 45-458 degree line indicating the line of perfect equality and the Lorenz curve appearing below it. If the 459 variable on the vertical axis were distributed equally among all countries, then the Lorenz curve 460 would be a diagonal line. The greater the amount of bowing of the Lorenz curve from the line, 461 the greater the inequality across countries. Another feature of the Lorenz curves shown here is 462 that countries are distinguished as segments on the curves (with the horizontal run of the 463 segments based on countries’ relative population sizes), enabling the viewer to see how countries 464 have shifted along the inequality spectrum over time. The Gini coefficient can be derived from 465 the Lorenz curve by taking the ratio of the area between the line of equality and the Lorenz curve 466 as the numerator and the area of the triangle (everything under the line of equality) as the 467 denominator. The Gini coefficient can range from 0-1 with higher numbers indicating greater 468 inequality. In this case we used the Gini index generated by using the fastgini Stata command 469 and applying pweights to account for country population size. 470 471 To complement the Lorenz curves, we present figures of Pen’s parade or parade plots for each 472 variable to provide a more nuanced perspective of the changes over time (1970 and 2010), 473 particularly highlighting the population of the country. This type of data visualization - also 474 known as a quantile plot - was first developed for use in income inequality analysis, where 475 typically the height is proportional to the income and observations are ordered from lowest to 476 greatest (Pen, 1971). The data are arrayed from the lowest per capita value to the highest per 477 capita value with the width of each bar corresponding to the country’s population size (Jann 478 2015). This set of figures provides information on the absolute, per capita values and includes a 479 line for the mean value of each variable in 1970 and 2010. The mean line is shown in order to 480 indicate whether the global level of each outcome is increasing or decreasing and to maintain a 481 link with the Lorenz curve; the ratio of each country mean to the global mean is equal to the 482 slope of the country’s line segment on the Lorenz curve. 483 484 For both the Lorenz curves and parade plots, national level data were used, and per capita values 485 calculated with Stata 15 statistical software. Graphics were designed using the color palette from 486 Color Brewer 2·0 from Pennsylvania State University (Brewer et al. 2013). Additional results for 487 an expanded set of variables can be found in the Supplementary Materials. 488 489 Contributions 490 WB and KL assembled the data and developed the model code. WB prepared the first draft. KL and 491 WAM reviewed and edited the manuscript. WAM conceived the study. 492 493 Funding 494 Wellcome Trust 495 496

Page 17 of 19
References 497
Afshin, A., et al. (2019). "Health effects of dietary risks in 195 countries, 1990--2017: a 498 systematic analysis for the Global Burden of Disease Study 2017." The Lancet 393(10184): 499 1958-1972. 500
Baker, P. and Friel S., (2016). "Food systems transformations, ultra-processed food markets and 501 the nutrition transition in Asia." Globalization and Health 12(1): 80. 502
Bentham, J., Singh, G.M., Danaei, G. et al. (2020) Multidimensional characterization of global 503 food supply from 1961 to 2013. Nature Food 1, 70–75. https://doi.org/10.1038/s43016-019-504 0012-2 505
Black, R. E., et al. (2013). "Maternal and child undernutrition and overweight in low-income and 506 middle-income countries." The Lancet 382(9890): 427-451. 507
Brewer et al. (2013). Color Brewer 2.0: Color advice for cartography. http://colorbrewer2.org/# 508
Food and Agriculture Organization (2013). African Commission on Agricultural Statistics: 509 Issues in the collection of FAO data. 510 http://www.fao.org/fileadmin/templates/ess/documents/afcas23/DOC_-_3f__Eng_.pdf 511
Food and Agriculture Organization. FAOSTAT. Accessed November 2019. 512 http://www.fao.org/faostat/en/ 513
Forouzanfar, M.H. et al. Global Burden of Disease Study 2013 (2015). Global, regional and 514 national comparative risk assessment of 79 behavioural, environmental and occupational 515 and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis 516 for the Global Burden of Disease Study 2013. The Lancet, 386, 2287 323, doi: 517 10.1016/S0140–6736(15)00128-2. 518
Gluzmann, P., & Gasparini, L. (2014). International Inequality in Subjective Welfare: An 519 exploration with the Gallup World Poll, 1–22. https://doi.org/10.1111/rode.12356 520
Groot, L. (2010). Carbon Lorenz curves. Resource and Energy Economics, 32(1), 45-64. 521 https://doi.org/10.1016/j.reseneeco.2009.07.001 522
Guragai, B., Takizawa, S., Hashimoto, T., & Oguma, K. (2017). Science of the Total 523 Environment Effects of inequality of supply hours on consumers’ coping strategies and 524 perceptions of intermittent water supply in Kathmandu Valley, Nepal. Science of the Total 525 Environment, 599–600, 431–441. https://doi.org/10.1016/j.scitotenv.2017.04.182 526
Harper, S., & Lynch, J. (2017). Health inequalities: Measurement and Decomposition. Ch. 5 in 527 Methods in Social Epidemiology, J. M. Oakes & J. Kaufman, eds. (2nd ed.). San Francisco: 528 Jossey-Bass. 529
Hawkes, C., Chopra, M., & Friel, S. (2009). Globalization, Trade, and the Nutrition Transition. 530 Ch. 10 in Globalization and Health: Pathways, evidence and policy, R. Labonté, T. 531 Schrecker, C. Packer, V. Runnel, eds. (1st ed.) New York: Routledge. 532
Jann, B. (2015). Variable bar widths in two-way graphs. The Stata Journal, 15(1), 316-318. 533
Khoury, C.K., Bjorkman, A.D., Dempewolf, H., Ramirez-Villegas, J., Guarino, L., Jarvis, A., 534 Rieseberg, L.H., Struik, P.C. (2014). Increasing homogeneity in global food supplies. 535 Proceedings of the National Academy of Sciences, 111 (11) 4001-4006 536

Page 18 of 19
Lawrence, S., Liu, Q., & Yakovenko, V. M. (2013). Global inequality in energy consumption 537 from 1980 to 2010. Entropy, 15(12), 5565-5579. https://doi.org/10.3390/e15125565 538
Masters, W. A., Rosenblum, N. Z., & Alemu, R. G. (2018). Agricultural Transformation, 539 Nutrition Transition and Food Policy in Africa: Preston Curves Reveal New Stylised Facts. 540 The Journal of Development Studies, 54(5), 788–802. 541 https://doi.org/10.1080/00220388.2018.1430768 542
Milanovic, B. (2005). The Three Concepts of Inequality Defined, from Worlds Apart: Measuring 543 International and Global Inequality. Princeton NJ: University Press. 544
Milanovic, B. (2011). Worlds apart: Measuring international and global inequality. Princeton 545 NJ: University Press. 546
Milanovic, B. (2016). Global Inequality. Cambridge MA: The Belknap Press. 547
NCD RisC. (2016a). Trends in adult body-mass index in 200 countries from 1975 to 2014: a 548 pooled analysis of 1698 population-based measurement studies with 19 · 2 million 549 participants. The Lancet, 387(10026), 1377–1396. https://doi.org/10.1016/S0140-550 6736(16)30054-X 551
NCD RisC. (2016b). Worldwide trends in diabetes since 1980: a pooled analysis of 751 552 population-based studies with 4·4 million participants. The Lancet, 387(10027), 1513–1530. 553 https://doi.org/10.1016/S0140-6736(16)00618-8 554
NCD RisC. (2017a). Worldwide trends in body-mass index, underweight, overweight, and 555 obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement 556 studies in 128 · 9 million children, adolescents, and adults, 2627–2642. 557 https://doi.org/10.1016/S0140-6736(17)32129-3 558
NCD RisC. (2017b). Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis 559 of 1479 population-based measurement studies with 19 · 1 million participants. 560 https://doi.org/10.1016/S0140-6736(16)31919-5 561
Pen, J. (1971). Income Distribution. London: Allen Lane. 562
Popkin, B. M. (2017). "Relationship between shifts in food system dynamics and acceleration of 563 the global nutrition transition." Nutrition Reviews 75(2): 73-82. 564
Rockström, J., Stordalen, G. A., & Horton, R. (2016). Acting in the anthropocene: the EAT–565 Lancet commission. The Lancet, 387(10036), 2364-2365. https://doi.org/10.1016/S0140-566 6736(16)30681-X 567
Schmidhuber, J., Sur, P., Fay, K., Huntley, B., Salama, J., Lee, A., Cornaby, L., Horino, M, 568 Murray, C. & Afshin, A. (2018). The Global Nutrient Database: availability of 569 macronutrients and micronutrients in 195 countries from 1980 to 2013. The Lancet 570 Planetary Health, 2(8), e353-e368. https://doi.org/10.1016/S2542-5196(18)30170-0 571
Seekell, D. A., D’odorico, P., & Pace, M. L. (2011). Virtual water transfers unlikely to redress 572 inequality in global water use. Environmental Research Letters, 6(2), 024017. 573 https://doi.org/10.1088/1748-9326/6/2/024017 574

Page 19 of 19
Smith, Matthew R., Renata Micha, Christopher D. Golden, Dariush Mozaffarian, and Samuel S. 575 Myers. "Global Expanded Nutrient Supply (GENuS) model: a new method for estimating 576 the global dietary supply of nutrients." PLoS One 11, no. 1 (2016): e0146976. 577
Steinberger, J. K., Krausmann, F., & Eisenmenger, N. (2010). Global patterns of materials use: A 578 socioeconomic and geophysical analysis. Ecological Economics, 69(5), 1148-1158. 579 https://doi.org/10.1016/j.ecolecon.2009.12.009 580
Tomich T.P., Kilby P. & Johnston B. (1995). Transforming Agrarian Economies: Opportunities 581 Seized, Opportunities Missed. Ithaca: Cornell University Press. 582
US Department of Agriculture (USDA), Agricultural Research Service, Nutrient Data 583 Laboratory. USDA National Nutrient Database for Standard Reference, Legacy. Version 584 Current: April 2018. Internet: http://www.ars.usda.gov/nutrientdata. 585
Wagstaff, A., Paci, P., & Van Doorslaer, E. (1991). On the measurement of inequalities in 586 health. Social Science & Medicine, 33(5), 545-557. https://doi.org/10.1016/0277-587 9536(91)90212-U 588
Wood, S.A., Smith, M.R., Fanzo, J. et al. (2018). Trade and the equitability of global food 589 nutrient distribution. Nat Sustain 1, 34–37. https://doi.org/10.1038/s41893-017-0008-6 590
World Bank. World Bank Country and Lending Groups. Accessed January 2018. 591 https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-592 and-lending-groups 593
World Bank. World Development Indicators. Accessed November 2019. 594 http://databank.worldbank.org/data/home 595
596
597

Page 1 of 14
Annex of Supplemental Tables and Charts for: 1 2
Global inequality in agriculture, nutrition, and health 3 Winnie Bell, MS, Keith Lividini, MS, and William A. Masters, PhD* 4
5 This version revised 29 June 2020 6
7 8 9
Table A1: Data sources 10 Figure A2: Energy availability 11 Figure A3: Protein and fat availability 12 Figure A4: Starchy staple availability 13 Figure A5: Monounsaturated and Polyunsaturated fat availability 14 Figure A6: Saturated fat and trans fat availability 15 Figure A7: Carbohydrate, fiber and vitamin K availability 16 Figure A8: Sodium, potassium, and magnesium availability 17 Figure A9: Copper and manganese availability 18 Figure A10: Calcium, phosphorous and vitamin D availability 19 Figure A11: Cholesterol, vitamin B12 and folate availability 20 Figure A12: Vitamin B1, vitamin B2 and vitamin B3 availability 21 Figure A13: Vitamin B5, vitamin B6, and choline availability 22 Figure A14: Vitamin E, vitamin C, and selenium availability 23 Figure A15: Underweight, female 24 Figure A16: Overweight, female 25 Figure A17: Underweight, male 26 Figure A18: Overweight, male 27 FigureA19: Diabetes, female and male 28
29 30 31 32 33 34 35
*Contact author: Friedman School of Nutrition, Tufts University ([email protected]).36

Page 2 of 14
Table A1. Data sources 37
Variable Units Reference period used
Number of countries
available in 1970 (or earliest year)
Source
Gross domestic product
Constant 2010 USD per capita; natural log
1970 & 2010 118 World Bank
Area harvested Hectares of all crops produced per rural capita; natural log
1970 & 2010 201 FAOSTAT
Irrigated land Hectares per rural capita 1970 & 2010 201 FAOSTAT
Livestock units Stocks of major livestock types per rural capita; natural log
1970 & 2010 201 FAOSTAT
Fruits and vegetables
Energy per capita 1970 & 2010 173 NBS
Animal source foods
Energy per capita 1970 & 2010 173 NBS
Fat Grams per capita 1970 & 2010 173 NBS
Protein Grams per capita 1970 & 2010 173 NBS
Iron Milligrams per capita 1970 & 2010 173 NBS
Zinc Milligrams per capita 1970 & 2010 173 NBS
Vitamin A Micrograms per capita 1970 & 2010 173 NBS
Stunting 2+ SD below median height for age per capita (children under 5 years old)
Varies by country
131 UNICEF /World
Bank/WHO
Underweight Body Mass Index (kg/m²) <18.5 per capita (adults over 18 years old); age standardized
1975 & 2010 162 NCD RisC
Overweight & obesity
Body Mass Index (kg/m²) >25 per capita (adults over 18 years old); age standardized]
1975 & 2010 162 NCD RisC
Raised blood pressure -- female
140+ mm Hg (systolic bp) or 90+ mm Hg (diastolic bp) per capita (women over 18 years old); age standardized
1975 & 2010 189 NCD RisC

Page 3 of 14
Table A1 (continued)
Raised blood pressure -- male
140+ mm Hg (systolic bp) or 90+ mm Hg (diastolic bp) per capita (men over 18 years old); age standardized
1975 & 2010 189 NCD RisC
Diabetes -- female
Fasting plasma glucose of 7.0+ mmol/L, diabetes diagnosis, use insulin or oral hypoglycaemic drugs per capita (women over 18 years old); age standardized
1980 & 2010 189 NCD RisC
Diabetes -- male
Fasting plasma glucose of 7.0+ mmol/L, diabetes diagnosis, use insulin or oral hypoglycaemic drugs per capita (men over 18 years old); age standardized
1980 & 2010 189 NCD RisC
38 39 40 Figure A2: Energy availability 41
42 43
44
45

Page 4 of 14
Figure A3: Protein and fat availability 46
47
Figure A4: Starchy staple availability 48
49

Page 5 of 14
Figure A5: Monounsaturated fat and Polyunsaturated fat 50
51 52 Figure A6: Saturated fat and Trans fat availability 53
54 55

Page 6 of 14
Figure A7: Carbohydrate, fiber and vitamin K availability 56
57 58 Figure A8: Sodium, potassium, and magnesium availability 59
60 61

Page 7 of 14
Figure A9: Copper and manganese availability 62
63 64 Figure A10: Calcium, phosphorous and vitamin D availability 65
66 67

Page 8 of 14
Figure A11: Cholesterol, vitamin B12 and folate availability 68
69 70 Figure A12: Vitamin B1, vitamin B2, vitamin B3 availability 71
72 73

Page 9 of 14
Figure A13: Vitamin B5, vitamin B6 and choline availability 74
75 76 Figure A14: Vitamin E, vitamin C and selenium availability 77
78 79

Page 10 of 14
Figure A15: Underweight, female 80
81
82
83

Page 11 of 14
84 Figure A16: Overweight, female 85
86
87

Page 12 of 14
Figure A17: Underweight, male 88
89 90
91 92 93

Page 13 of 14
Figure A18: Overweight, male 94
95
96

Page 14 of 14
Figure A19: Diabetes, female and male 97
98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 115 116 117 118