
Global child and adolescent mental ... - Harvard University
13
Global child and adolescent mental health: The orphan of development assistance for health The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Lu, Chunling, Zhihui Li, and Vikram Patel. 2018. “Global child and adolescent mental health: The orphan of development assistance for health.” PLoS Medicine 15 (3): e1002524. doi:10.1371/journal.pmed.1002524. http://dx.doi.org/10.1371/ journal.pmed.1002524. Published Version doi:10.1371/journal.pmed.1002524 Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:35982160 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA
Transcript of Global child and adolescent mental ... - Harvard University

Global child and adolescentmental health: The orphan of
development assistance for healthThe Harvard community has made this
article openly available. Please share howthis access benefits you. Your story matters
Citation Lu, Chunling, Zhihui Li, and Vikram Patel. 2018. “Global childand adolescent mental health: The orphan of developmentassistance for health.” PLoS Medicine 15 (3): e1002524.doi:10.1371/journal.pmed.1002524. http://dx.doi.org/10.1371/journal.pmed.1002524.
Published Version doi:10.1371/journal.pmed.1002524
Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:35982160
Terms of Use This article was downloaded from Harvard University’s DASHrepository, and is made available under the terms and conditionsapplicable to Other Posted Material, as set forth at http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#LAA

POLICY FORUM
Global child and adolescent mental health:
The orphan of development assistance for
health
Chunling Lu1,2,3*, Zhihui Li4, Vikram Patel2
1 Division of Global Health Equity, Brigham and Women’s Hospital, Boston, Massachusetts, United States of
America, 2 Department of Global Health and Social Medicine, Harvard Medical School, Boston,
Massachusetts, United States of America, 3 Department of Science and Technology-National Research
Foundation (DST-NRF) Center of Excellence in Human Development, University of Witwatersrand,
Johannesburg, South Africa, 4 Department of Global Health and Population, Harvard T.H. Chan School of
Public Health, Boston, Massachusetts, United States of America
Summary points
• One-quarter of disability-adjusted life years (DALYs) for mental disorders and sub-
stance abuse is borne by those 24 years old or younger, the age group that accounted for
more than 40% of the world population. Using the aid activities database from the Cred-
itor Reporting System (CRS), we estimated the level of development assistance for child
and adolescent mental health (DAMH_CA) in 132 developing countries between 2007
and 2015.
• The total amount of DAMH_CA with a primary target on child and adolescent mental
health was US$190.3 million over the 8 years, accounting for 12.5% of total development
assistance for mental health (DAMH) and 0.1% of development assistance for health
(DAH).
• The largest investments in DAMH_CA over this 8-year period were disbursed to the
humanitarian assistance sector for children and adolescents in disasters or conflicts (US
$77.2 million [41% of DAMH_CA]), followed by the sector of government and civil ser-
vices (US$58.6 million [31%]), the health sector (US$38.0 million [20%]), and the edu-
cation sector (US$15.6 million [8%]).
• Donors invested little in child and adolescent mental health, in both absolute amount
and fraction.
• The donor community should substantially increase DAMH_CA to establish and
enhance the capacity for delivering mental health care to this demographic group.
Background
More than 40% of the world population is 24 years old or younger, the vast majority of whom
live in low- and lower middle–income countries [1]. Globally, a quarter of disability-adjusted
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 1 / 12
a1111111111
a1111111111
a1111111111
a1111111111
a1111111111
OPENACCESS
Citation: Lu C, Li Z, Patel V (2018) Global child and
adolescent mental health: The orphan of
development assistance for health. PLoS Med 15
(3): e1002524. https://doi.org/10.1371/journal.
pmed.1002524
Published: March 9, 2018
Copyright: © 2018 Lu et al. This is an open access
article distributed under the terms of the Creative
Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in
any medium, provided the original author and
source are credited.
Data Availability Statement: All aid data files are
available from the Creditor Reporting System
database. The link is https://stats.oecd.org/Index.
aspx?DataSetCode=CRS1. All population data are
available from the United Nation Population
Division. The link is https://esa.un.org/unpd/wpp/.
Funding: This study was funded by NIH 1K0HD07
1929-01 https://www.nih.gov The funders had no
role in study design, data collection and analysis,
decision to publish, or preparation of the
manuscript.
Competing interests: VP is a member of the
Editorial Board of PLOS Medicine.
Abbreviations: BMGF, Bill & Melinda Gates
Foundation; CRS, Creditor Reporting System; DAC,
Development Assistance Committee; DAH,
development assistance for health; DALY,

life years (DALYs) for mental disorders and substance abuse is borne by this age group [2],
and about 75% of mental disorders diagnosed in adulthood have their onset before the age of
24 years [3]. Most children and young people in developing countries, however, do not have
access to mental health care.
Lack of financial commitment is amongst the major barriers for improving access to mental
health interventions in developing countries. Unsurprisingly, the least resourced regions and
countries in the world rely heavily on development assistance, typically from high-income
countries or foundations, to support the health sector. Our previous study on development
assistance for mental health (DAMH) demonstrated that DAMH remained low both in abso-
lute terms and as a proportion of development assistance for health (DAH) between 2007 and
2013 [4].
This analysis extends our previous analysis by investigating development assistance for
child (below age 10) and adolescent (between age 10 and 24) mental health (DAMH_CA). We
tracked the level of DAMH_CA in 132 countries between 2007 and 2015 (S1 Table).
Estimating DAMH_CA between 2007 and 2015
Data sources
We used the Organization for Economic Co-operation and Development (OECD) Creditor
Reporting System (CRS) aid activity database [5], which was downloaded in May 2017. The
CRS database is publicly accessible and provides information on aid activities reported directly
by the governments of the 26 members of the Development Assistance Committee (DAC),
multilateral organizations (e.g., World Bank), global health initiatives (e.g., GAVI, the Vaccine
Alliance), non-DAC countries (e.g., United Arab Emirates), and private donors (the Bill &
Melinda Gates Foundation [BMGF]) [5,6]. See S1 Text for more details on data sources. Our
analysis included 132 countries (S1 Table) founded by 44 donors.
Identifying projects on child and adolescent mental health
We defined DAMH_CA as aid disbursed to projects that either primarily or partially targeted
the promotion of mental health or the prevention and treatment of mental disorders for chil-
dren or adolescents. We adopted a multi-sectoral perspective [4,7] and included mental health
projects in non-health sectors such as education, government and civil services, and humani-
tarian assistance.
CRS data do not have a variable to indicate mental health projects for children and adoles-
cents but has three variables (project title, short description, and long description) that allowed
us to identify such projects with a list of key words (S2 Table) used in the previous studies
[4,8]. Key word searches were performed for projects in the sectors listed in Table 1. The defi-
nition of these sectors in the CRS can be found in S1 Box. Details on identification strategy are
presented in S1 Text.
Analyzing DAMH_CA
We followed the approach from an earlier study [7] and constructed two sets of estimates: one
including the full disbursements of multi-target projects (the upper bound of estimated aid for
DAMH_CA, presented in the Supporting information and the other (the lower bound of esti-
mated aid for DAMH_CA, presented in the text), which included only projects with a primary
target of promoting mental health for children and adolescents. We used actual disbursements
(grants and loans) rather than commitments to estimate DAMH_CA. The time frame allowed
us to both track changes in DAMH_CA since The Lancet published its first series on mental
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 2 / 12
disability-adjusted life year; DAMH, development
assistance for mental health; DAMH_CA,
development assistance for child and adolescent
mental health; EU, European Union; GFATM, Global
Fund to Fight AIDS, Tuberculosis and Malaria;
LMIC, low- and middle-income country; NGO,
nongovernmental organization; OECD, Organization
for Economic Co-operation and Development;
USD, US dollar.
Provenance: Not commissioned; externally peer
reviewed.

Table 1. Sectors for identifying DAMH_CA projects: Frequency and the two most common themes.
Sectors
Projects with the primary purpose on DAMH_CA (lower
bound), N = 1,384
Projects primarily or partially on DAMH_CA (upper bound), N = 4,009
Frequency
(Percentage) of
Total Projects
Two most common themes Frequency
(Percentage) of Total
Projects,
Two most common themes
Education
Basic Education 65 (4.70%) Establish psycho-pedagogical
research center for special
educational needs;
Educate and train students with
mental disabilities
423 (10.55%) Help teenagers grow and enhance their mental and
physical health;
Increase parents’ knowledge of early childhood
development, including cognitive, socio-emotional,
linguistic, and physical aspects
Secondary Education 16 (4.70%) Provide special assistance to
traumatized children;
Provide support to young children
to treat or prevent traumatizing
92 (2.29%) Emotional service for children, along with education,
effort, medical service, and cultural exchange;
Raise awareness of children’s reaction to violence and
war, prevent/minimize the long-term effects of trauma
Postsecondary
Education
22 (1.59%) Project targeting disruptive behavior
and attention disorders of childhood
and adolescence;
Provide primary care for youth with
mental illness
39 (0.97%) Improve school performance to favor the harmonic
physical and psychological development of
disadvantaged children;
Support public institutions to provide youth with
appropriate psychological and social expertise
Education, Level
Unspecified
36 (2.60%) Construction of a center for children
with autism;
Psychological intervention and
development project for poor
university students
148 (3.69%) Provide activities to help enhance youths’ mental and
physical health;
Provide school-based interventions to improve child
cognitive and psychosocial development and physical
and nutritional health and increase school enrollment
rate
Health
General Health 225 (16.26%) Improving psychological healthcare
for children;
Address negative effects of alcohol
and drug use among children and
youth
384 (9.58%) Provide treatment and psychological support for HIV/
AIDS patients;
Improve physical, nutritional, and psychological
services for preschool-aged children
Basic Health 88 (6.36%) Provide psychosocial care for young
children;
Support a therapy and support
center for children with autism
338 (8.43%) Improve growth and development of children under 6
years old in terms of nutrition, health, psychosocial,
and cognitive aspects;
Seek to reach children who have both physical and
mental disabilities
Population and
Reproductive Health
35 (2.53%) Monitor and promote psychosocial
care among young children;
Provide psychosocial care for
children and orphans living with
chronic illness
497 (12.40%) Address the HIV- and AIDS-related needs of high-risk
populations, including drug users, sex workers, and
orphans;
Provide psychosocial and medical support for people to
live with HIV/AIDS
Government and Civil
Service
Government and Civil
Society
149 (10.77%) Control tobacco and alcohol use
among children and young people;
Improve well-being of children and
youth traumatized by displacement
and war
482 (12.02%) Address educational and psychosocial impact of armed
conflict, build child protection network, promote
rights-based work;
Improve physical and mental health of women victims
of domestic violence and their children
Conflict, Peace, and
Security
44 (3.18%) Improve psychological healthcare
for children;
Ensure psychological and social
support in reintegration in home
communities
126 (3.14%) Provide interventions (psychosocial and medical, and
vocational training) for women and child soldiers;
Provide jobs, training, funding for income generation
and offer remedial schooling, trauma counseling, and
family reintegration
Other Social
Infrastructure and
Services
(Continued)
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 3 / 12
health and adolescent health [9,10] and to avoid the issue of missing disbursement data in the
CRS [6].
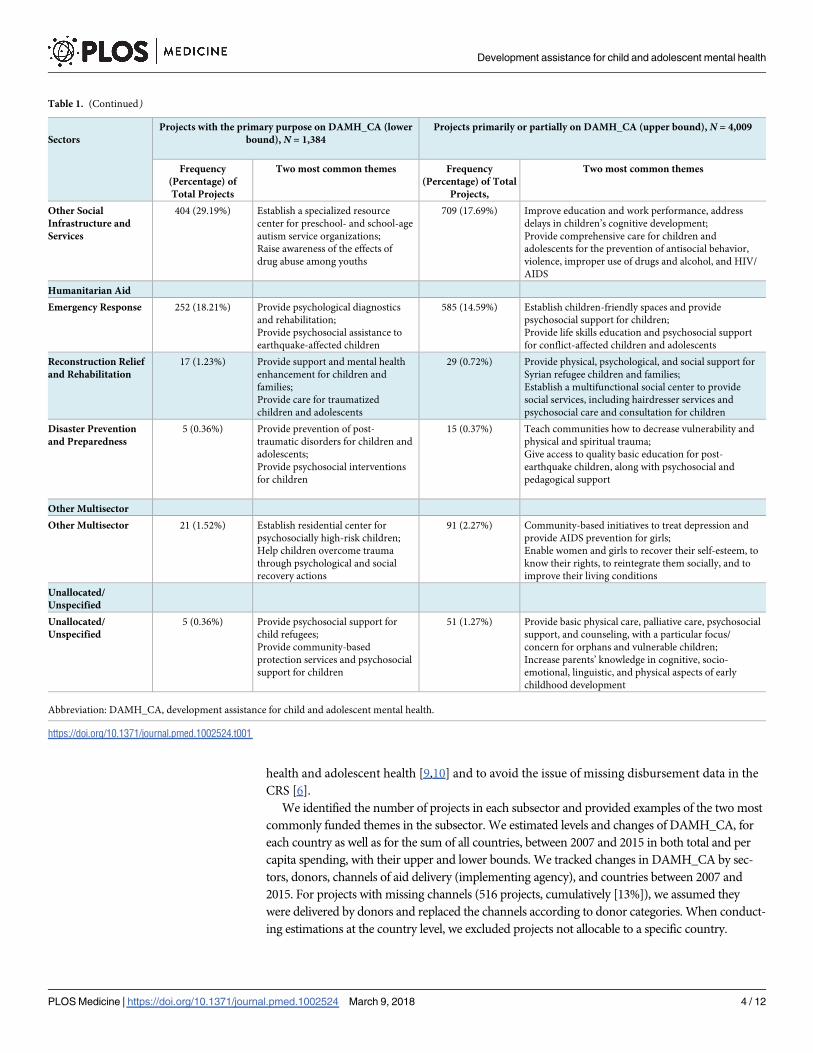
We identified the number of projects in each subsector and provided examples of the two most
commonly funded themes in the subsector. We estimated levels and changes of DAMH_CA, for
each country as well as for the sum of all countries, between 2007 and 2015 in both total and per
capita spending, with their upper and lower bounds. We tracked changes in DAMH_CA by sec-
tors, donors, channels of aid delivery (implementing agency), and countries between 2007 and
2015. For projects with missing channels (516 projects, cumulatively [13%]), we assumed they
were delivered by donors and replaced the channels according to donor categories. When conduct-
ing estimations at the country level, we excluded projects not allocable to a specific country.
Table 1. (Continued)
Sectors
Projects with the primary purpose on DAMH_CA (lower
bound), N = 1,384
Projects primarily or partially on DAMH_CA (upper bound), N = 4,009
Frequency
(Percentage) of
Total Projects
Two most common themes Frequency
(Percentage) of Total
Projects,
Two most common themes
Other Social
Infrastructure and
Services
404 (29.19%) Establish a specialized resource
center for preschool- and school-age
autism service organizations;
Raise awareness of the effects of
drug abuse among youths
709 (17.69%) Improve education and work performance, address
delays in children’s cognitive development;
Provide comprehensive care for children and
adolescents for the prevention of antisocial behavior,
violence, improper use of drugs and alcohol, and HIV/
AIDS
Humanitarian Aid
Emergency Response 252 (18.21%) Provide psychological diagnostics
and rehabilitation;
Provide psychosocial assistance to
earthquake-affected children
585 (14.59%) Establish children-friendly spaces and provide
psychosocial support for children;
Provide life skills education and psychosocial support
for conflict-affected children and adolescents
Reconstruction Relief
and Rehabilitation
17 (1.23%) Provide support and mental health
enhancement for children and
families;
Provide care for traumatized
children and adolescents
29 (0.72%) Provide physical, psychological, and social support for
Syrian refugee children and families;
Establish a multifunctional social center to provide
social services, including hairdresser services and
psychosocial care and consultation for children
Disaster Prevention
and Preparedness
5 (0.36%) Provide prevention of post-
traumatic disorders for children and
adolescents;
Provide psychosocial interventions
for children
15 (0.37%) Teach communities how to decrease vulnerability and
physical and spiritual trauma;
Give access to quality basic education for post-
earthquake children, along with psychosocial and
pedagogical support
Other Multisector
Other Multisector 21 (1.52%) Establish residential center for
psychosocially high-risk children;
Help children overcome trauma
through psychological and social
recovery actions
91 (2.27%) Community-based initiatives to treat depression and
provide AIDS prevention for girls;
Enable women and girls to recover their self-esteem, to
know their rights, to reintegrate them socially, and to
improve their living conditions
Unallocated/
Unspecified
Unallocated/
Unspecified
5 (0.36%) Provide psychosocial support for
child refugees;
Provide community-based
protection services and psychosocial
support for children
51 (1.27%) Provide basic physical care, palliative care, psychosocial
support, and counseling, with a particular focus/
concern for orphans and vulnerable children;
Increase parents’ knowledge in cognitive, socio-
emotional, linguistic, and physical aspects of early
childhood development
Abbreviation: DAMH_CA, development assistance for child and adolescent mental health.
https://doi.org/10.1371/journal.pmed.1002524.t001
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 4 / 12

We paid special attention to DAMH_CA that targeted suicide and the five types of mental
disorders that are the leading causes for disability or death among the children and adolescents
group: (1) anxiety, (2) autism, (3) depression, (4) substance abuse, and (5) trauma [11,12].
All disbursements are in 2013 US dollars (USDs). STATA 14 was used in analysis.
Themes supported by DAMH_CA
We identified 1,384 DAMH_CA projects with primary targets on child and adolescent men-
tal health (lower bound). Among them, 404 were allocated to “Other Social Infrastructure
and Services,” and the most common themes were in providing special care for children
with autism and raising awareness of drug abuse among youths. There were 252 projects for
“Emergency Response,” with the most common themes being providing psychosocial assis-
tance and care to children in disasters or conflict areas. There were 225 projects for “Gen-
eral Health,” with the most common themes being improving psychological healthcare for
children and addressing alcohol and drug use among adolescents. There were 149 projects
for “Government and Civil Society,” with the most common themes being controlling
tobacco and alcohol use and improving well-being for children and youth affected by wars
(Table 1).
Absolute and relative DAMH_CA, lower-bound estimates
Between 2007 and 2015, a total of US$190.3 million was disbursed to projects with the primary
purpose of improving the mental health of children and adolescents, accounting for 12.5% of
DAMH and 0.10% of the total DAH disbursed over this period. The DAMH_CA increased
from US$6.6 million in 2007 to US$30.2 million in 2015, with fluctuations over time. The per-
centages of DAMH_CA in total DAMH increased from 10% in 2007 to 17% in 2008 and
dropped to 6% in 2013. In 2015, 14% of DAMH was for child and adolescent mental health
(Fig 1).
Fig 1. DAMH_CA by year (million, 2013 USD) and DAMH_CA disbursements as percentages of total DAMH,
lower-bound estimates. DAMH, development assistance for mental health; DAMH_CA, development assistance for
child and adolescent mental health, USD, US dollar.
https://doi.org/10.1371/journal.pmed.1002524.g001
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 5 / 12

Sectors receiving DAMH_CA, lower-bound estimates
The humanitarian aid sector received the largest cumulative DAMH_CA, with a total amount
of US$77.2 million (40.5% of total DAMH_CA), followed by the government and civil society
sector (US$58.6 million [30.8%]), the health sector (US$38.0 million [20.0%]), and the educa-
tion sector (US$15.6 million [8.2%]) (Fig 2). In terms of each sector’s proportion in
DAMH_CA, government and civil services had the largest proportion in 2007 and 2008. It was
then replaced by humanitarian assistance between 2009 and 2014 and returned to the leading
position in 2015 (38.4% in total DAMH_CA in 2015), followed closely by “Humanitarian Aid”
(37.9%), “Health” (18.3%), and “Education” (5.4%).
DAMH_CA channels and donors, lower-bound estimates
In terms of channel of delivery, from 2007 to 2015, nongovernmental organizations (NGOs)
and civil society received the largest cumulative DAMH_CA of US$110.6 million (58.1% of
total DAMH_CA), followed by UN organizations and WHO (US$46.4 million [24.4%]); the
public sector in recipient countries received a relatively small fraction (US$23.1 million
[12.1%]) (see S2 Fig).
The top three donors were European Union (EU) institutions (US$44.8 million), Germany
(US$21.8 million), and Switzerland (US$18.6 million). During the analysis period, they
together provided between 32.1% and 71.7% of total DAMH_CA each year, with a mean of
51.5% (S3 Fig). Even for the top 10 donors, their percentage of total DAH on DAMH_CA
over the 8 years is pitifully small, from 0.03% in Canada to 2.69% in Finland (S3 Table). When
using the upper-bound estimates, the Global Fund to Fight AIDS, Tuberculosis and Malaria
(GFATM) appeared to be the largest donor (cumulatively US$551.3 million), with most of its
investments in providing psychological support and other medical and social care for high-
risk populations of HIV/AIDS, including drug users (S4 Fig).
Fig 2. DAMH_CA by year and sector (million, 2013 USD), lower-bound estimates. In this figure, we combined the
sectors “General Health” and “Population Program and Reproductive Health” in the original CRS dataset as “Health,”
the sectors “Humanitarian Aid” and “Multisector/Crosscutting” as “Humanitarian Aid,” and the sectors “Government
and Civil Society” and “Other Social Infrastructure and Services” as “Government and Civil Society.” CRS, Creditor
Reporting System; DAMH_CA, development assistance for child and adolescent mental health; USD, US dollar.
https://doi.org/10.1371/journal.pmed.1002524.g002
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 6 / 12

DAMH_CA per capita at the recipient country level, lower-bound
estimates
Fig 3 presents the world map of average annual per capita DAMH_CA for 132 countries.
Throughout the analysis period, 21 countries did not receive any funding on DAMH_CA,
including 3 low-income countries (Guinea-Bissau, Gambia, and Comoros), 8 lower middle–
income countries (e.g., Lesotho, Tonga, and Djibouti), and 10 upper middle–income countries
(e.g., Gabon, Namibia, and Botswana). Per capita, 69 countries received less than US$0.01
DAMH_CA, including 20 low-income countries (e.g. Rwanda, Mozambique, and Guinea), 26
lower middle–income countries (e.g., India, Senegal, and Nigeria), and 23 upper middle–
income countries (e.g., China, Mexico, and Chile). Only 14 countries received more than US
$0.05 DAMH_CA per capita, with 4 of them receiving more than US$0.2 per capita: West
Bank and Gaza Strip (US$2.9 per capita), Kiribati (US$1.3), Lebanon (US$0.4), and Bosnia
and Herzegovina (US$0.2). Numerical values of annual DAMH_CA per capita for each coun-
try (in both upper and lower bounds) are reported in S4 Table and S5 Table.
In different regions, projects that received a large amount of DAMH_CA often had differ-
ent targets. For example, in the Eastern Mediterranean and Europe, DAMH_CA projects with
a large amount of disbursements usually focused on alcohol addiction. DAMH_CA projects in
Middle Eastern countries (e.g., West Bank and Gaza Strip, Lebanon) were usually focused on
coping with trauma and providing psychological support to children and adolescents in con-
flicts. In Africa, a large amount of DAMH_CA was related to HIV/AIDS projects, which
included components addressing drug addiction and psychological care for children and ado-
lescents living with HIV.
Fig 3. Average annual per capita DAMH_CA disbursement between 2007 and 2015 in each country (2013 USD), lower-bound estimates. (1) The top 10 countries
with the highest average annual per capita DAMH_CA disbursement are West Bank and Gaza Strip (US$2.88), Kiribati (US$1.33), Lebanon (US$0.37), Bosnia and
Herzegovina (US$0.23), Samoa (US$0.16), Georgia (US$0.15), Jordan (US$0.13), Sri Lanka (US$0.11), Libya (US$0.11), and Central African Republic (US$0.11). (2)
We did not include unallocable or regional DAMH_CA projects. DAMH_CA, development assistance for child and adolescent mental health; USD, US dollar.
https://doi.org/10.1371/journal.pmed.1002524.g003
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 7 / 12

DAMH_CA to suicide and five mental disorders, lower-bound
estimates
Interventions targeting the five leading causes for disability or death among children and ado-
lescents received relatively small disbursements. The lower-bound estimates show that the
cumulative amount of disbursements to trauma-related mental disorders accounted for 1.13%
of total DAMH_CA, followed by substance abuse (0.76%), autism (0.19%), suicide (0.02%),
depression (0.02%), and anxiety (0.01%) (see S9 Fig). Findings on investments in these disor-
ders remain similar when using upper-bound estimates (S5 Fig).
Discussion
Using the CRS data with a multi-sectoral perspective, we tracked 44 donors’ aid disbursements
to DAMH_CA projects implemented in 132 developing countries between 2007 and 2015.
The total amount of DAMH_CA with a primary target on the mental health of children and
adolescents was US$190.3 million over the 8 years, accounting for 12.5% of total DAMH and
0.1% of total DAH. Per capita, 90 developing countries received either 0 or less than US$0.01
average DAMH_CA, including 23 low-income countries (out of 36 total low-income countries
[64%]). Global child and adolescent mental health is truly the orphan of DAH. Our findings
are consistent with a recent publication on DAMH_CA [13].
Additional concerns we observed are related to volatility and poor targeting of assistance.
DAMH_CA experienced marked fluctuations over the 8-year period, mainly driven by the
investments from two donors. This poses challenges for effective long-term budgeting and
planning for recipient countries with high dependence on external sources for mental health
financing. Furthermore, it is alarming that both the total amount and proportion of
DAMH_CA for the public sectors has been comparatively very low (12.1% over the 8-year
period), with most DAMH_CA targeting temporary or short-term humanitarian assistance to
children and adolescents in disasters or conflicts and channeling the assistance through
NGOs. This is consistent with our previous study on DAMH, in which we also observed that
the share of DAMH channeled to public health sectors, the key player in delivering basic men-
tal health care, was small. Though there is mounting evidence that mental health services for
children and adolescents can be effectively delivered by community health workers [14], only
a tiny fraction of aid has been invested (US$14.2 million over the 8-year period) in delivering
mental health care to children and adolescents with priority mental health conditions.
This analysis has the following limitations. (1) Due to a lack of details of aid projects at the
recipient country level, our estimates did not include aid to developing countries from emerg-
ing economies (e.g., China), NGOs, or foundations (with the exception of the BMGF). (2) The
identification strategy was not able to capture all projects on DAMH_CA or those with typo-
graphical errors and solely relied on project descriptions provided by donors, which could be
subject to unreliable quality. (3) When estimating DAMH_CA at the country level, data that
could not be allocated to a specific recipient country were not included. (4) The estimates of
DAMH_CA for the specific mental disorders (e.g., depression) in the analysis could be under-
estimated, as projects with general mental health terms as key words (e.g., projects of “mental
health”) could also provide care to patients with depression but not be included in the current
estimates due to lack of information regarding separate funds for depression. (5) Our estima-
tion only focused on projects that either primarily or partially targeted mental health for chil-
dren and adolescents. We did not include projects that targeted socioeconomic determinants
of child and adolescent mental health, such as nutrition or maternal education; thus, our esti-
mates may largely reflect investments in selective prevention (e.g., children in humanitarian
contexts) or treatment and care.
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 8 / 12

Despite these limitations, this analysis is the first to report on the financing of mental health
care for children and adolescents in low- and middle-income countries (LMICs) between 2007
and 2015. We consider a number of key lessons to be drawn from this analysis. First, given the
evidence that much of the burden of mental disorders has its origins in childhood or adoles-
cence and early interventions are potentially the key to prevention and recovery [15,16], there
should be an increase, at least a doubling, in DAMH_CA so as to enable developing countries
to strengthen their capacity by investing in mental health infrastructure and training provid-
ers, including community health workers and specialists, to deliver cost-effective interven-
tions. We believe that challenging the stigma associated with mental disorders, providing
accurate information about the prevalence and impact of mental disorders in children and
adolescents, and cost-effectiveness of interventions will raise interest in investing in mental
health among the donor community. Second, investments should be based on scientific evi-
dence of the patterns of the burden of disease, cost-effective interventions, and a recipient
country’s own sociocultural context. For example, as community-based delivery of psychoso-
cial interventions by frontline workers has been shown to be cost-effective in LMICs, more
funds should be directed to this approach. Third, while it is important for donors to continue
supporting humanitarian assistance for those living in conflict areas, there should be more
donor investments, with more stability and better targeting for building and sustaining mental
health programs to achieve universal mental health coverage in the long term. In particular,
funding should target the public system to ensure that the goals of integrating mental health
interventions (promotional, preventive, or curative) into appropriate platforms for delivery,
including health, education, and social sectors, are achieved [17].
Supporting information
S1 Text. Data sources and identification strategy.
(DOCX)
S1 Table. One hundred thirty-two recipients in the CRS (according to the World Bank
income classification in 2010). CRS, Creditor Reporting System.
(XLSX)
S2 Table. Key words used to search DAMH_CA projects in the CRS, 2007–2015. CRS,
Creditor Reporting System; DAMH_CA, development assistance for child and adolescent
mental health.
(XLSX)
S3 Table. Top 10 DAMH_CA donors: DAMH_CA (lower bound) as a percentage of their
DAH over the 8 years. DAH, development assistance for health; DAMH_CA, development
assistance for child and adolescent mental health.
(XLSX)
S4 Table. Annual DAMH_CA disbursements per capita (2013 USD) to each recipient
country between 2007 and 2015, lower-bound estimates. DAMH_CA, development assis-
tance for child and adolescent mental health; USD, US dollar.
(XLSX)
S5 Table. Annual DAMH_CA disbursements per capita (2013 USD) to each recipient
country between 2007 and 2015, upper-bound estimates. DAMH_CA, development assis-
tance for child and adolescent mental health; USD, US dollar.
(XLSX)
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 9 / 12
S1 Box. Definition of sectors in CRS data. CRS, Creditor Reporting System.
(DOCX)
S1 Fig. Annual proportion of DAMH_CA in total DAH between 2007 and 2015, lower-
bound estimates. DAH, development assistance for health; DAMH_CA, development assis-
tance for child and adolescent mental health.
(TIFF)
S2 Fig. Annual DAMH_CA (million, 2013 USD) by channel between 2007 and 2015,
lower-bound estimates. UN organizations include UN, UNFPA, UNICEF, UNDP, UNAIDS,
and UNECE. DAMH_CA, development assistance for child and adolescent mental health; EU,
European Union; UN, United Nations; UNAIDS, the Joint United Nations Programme on
HIV and AIDS; UNDP, United Nations Development Programme; UNECE: United Nations
Economic Commission for Europe; UNFPA, United Nations Population Fund; UNICEF,
United Nations Children’s Fund; USD, US dollar.
(TIFF)
S3 Fig. Annual DAMH_CA (million, 2013 USD) by donor between 2007 and 2015, lower-
bound estimates. DAMH_CA, development assistance for child and adolescent mental health;
USD, US dollar.
(TIFF)
S4 Fig. Annual DAMH_CA (million, 2013 USD) by donor between 2007 and 2015, upper-
bound estimates. DAMH_CA, development assistance for child and adolescent mental health;
USD, US dollar.
(TIFF)
S5 Fig. Cumulative DAMH_CA disbursement (million, 2013 USD) of suicide and mental
disorders and their percentages in total DAMH_CA between 2007 and 2015, lower-bound
estimates. The DAH to each health focus shown in this figure is not mutually exclusive. For
example, if a project is for both anxiety and depression, we included this project in the estima-
tion of both health focuses. DAH, development assistance for health; DAMH_CA, develop-
ment assistance for child and adolescent mental health; USD, US dollar.
(TIFF)
S6 Fig. DAMH_CA by year (million, 2013 USD) and DAMH_CA disbursements as per-
centages of total DAMH between 2007 and 2015, upper-bound estimates. DAMH, develop-
ment assistance for mental health; DAMH_CA, development assistance for child and
adolescent mental health; USD, US dollar.
(TIFF)
S7 Fig. Annual DAMH_CA (million, 2013 USD) by sector (combined) between 2007 and
2015, upper-bound estimates. In this figure, we combined the sectors of “General Health”
and “Population Program and Reproductive Health” in the original CRS dataset as “Health,”
the sectors of “Humanitarian Aid” and “Multisector/Crosscutting” as “Humanitarian Aid,”
and the sectors of “Government and Civil Society” and “Other Social Infrastructure and Ser-
vices” as “Government and Civil Society.” CRS, Creditor Reporting System; DAMH_CA,
development assistance for child and adolescent mental health; USD, US dollar.
(TIFF)
S8 Fig. Annual DAMH_CA (million, 2013 USD) by channel between 2007 and 2015,
upper-bound estimates. UN organizations include UN, UNFPA, UNICEF, UNDP, UNAIDS,
and UNECE. DAMH_CA, development assistance for child and adolescent mental health; EU,
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 10 / 12
European Union; UN; United Nations; UNAIDS, the Joint United Nations Programme on
HIV and AIDS; UNDP, United Nations Development Programme; UNECE, United Nations
Economic Commission for Europe; UNFPA; United Nations Population Fund; UNICEF,
United Nations Children’s Fund; USD, US dollar.
(TIFF)
S9 Fig. Per capita DAMH_CA disbursement (2013 USD) between 2007 and 2015 in each
country, upper-bound estimates. We did not include unallocable or regional DAMH_CA
projects. DAMH_CA, development assistance for child and adolescent mental health; USD,
US dollar.
(TIF)
S10 Fig. Cumulative DAMH_CA disbursement (million, 2013 USD) between 2007 and
2015 by health focus, upper-bound estimates. DAMH_CA, development assistance for child
and adolescent mental health; USD, US dollar.
(TIF)
References1. Mundi Index. World Demographics Profile 2017 [Internet]. [cited 2017 Oct 4]. Available from: http://
www.indexmundi.com/world/demographics_profile.html
2. Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2016 (GBD 2016)
Results. [Internet]. Seattle, United States: Institute for Health Metrics and Evaluation (IHME). 2017
[cited 2017 Dec 19]. Available from: http://ghdx.healthdata.org/gbd-results-tool
3. Ruiz P, Primm A. Disparities in psychiatric care: Clinical and cross-cultural perspectives. Lippincott Wil-
liams & Wilkins; 2010.
4. Gilbert BJ, Patel V, Farmer PE, Lu C. Assessing Development Assistance for Mental Health in Develop-
ing Countries: 2007–2013. PLoS Med. 2015; 12(6):e1001834. https://doi.org/10.1371/journal.pmed.
1001834 PMID: 26035429
5. OECD. Creditor Reporting System (CRS) [Internet]. [cited 2017 Aug 2]. Available from: https://stats.
oecd.org/Index.aspx?DataSetCode = CRS1
6. OECD. Technical Guide to terms and data in the Creditor Reporting System (CRS) Aid Activities data-
base—OECD [Internet]. [cited 2017 Aug 2]. Available from: http://www.oecd.org/dac/stats/crsguide.htm
7. Lu C, Chu A, Li Z, Shen J, Subramanian S, Hill K. Assessing development assistance for child survival
between 2000 and 2014: A multi-sectoral perspective. Fan VY, editor. PLoS ONE. 2017; 12(7):
e0178887. https://doi.org/10.1371/journal.pone.0178887 PMID: 28700612
8. Charlson FJ, Dieleman J, Singh L, Whiteford HA. Donor Financing of Global Mental Health, 1995–
2015: An Assessment of Trends, Channels, and Alignment with the Disease Burden. Maulik PK, editor.
PLoS ONE. 2017; 12(1):e0169384. https://doi.org/10.1371/journal.pone.0169384 PMID: 28046059
9. Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR, et al. No health without mental health. Lancet.
2007 Sep; 370(9590):859–77. https://doi.org/10.1016/S0140-6736(07)61238-0 PMID: 17804063
10. Patel V, Flisher AJ, Hetrick S, McGorry P. Mental health of young people: a global public-health chal-
lenge. Lancet (London, England). 2007 Apr 14; 369(9569):1302–13.
11. Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. The Lancet Psychia-
try. 2016 Feb; 3(2):171–8. https://doi.org/10.1016/S2215-0366(15)00505-2 PMID: 26851330
12. World Health Organization. Adolescent health epidemiology. WHO [Internet]. 2014 [cited 2017 Aug 2];
Available from: http://www.who.int/maternal_child_adolescent/epidemiology/adolescence/en/
13. Turner J, Pigott H, Tomlinson M, Jordans MJ. Developmental assistance for child and adolescent men-
tal health in low- and middle-income countries (2007–2014): Annual trends and allocation by sector,
project type, donors and recipients. J Glob Health. 2017 Dec; 7(2):20901.
14. Kieling C, Baker-Henningham H, Belfer M, Conti G, Ertem I, Omigbodun O, et al. Child and adolescent
mental health worldwide: evidence for action. Lancet (London, England). 2011 Oct 22; 378
(9801):1515–25.
15. Erskine HE, Moffitt TE, Copeland WE, Costello EJ, Ferrari AJ, Patton G, et al. A heavy burden on
young minds: the global burden of mental and substance use disorders in children and youth. Psychol
Med. 2015 May 23; 45(7):1551–63. https://doi.org/10.1017/S0033291714002888 PMID: 25534496
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 11 / 12

16. World Health Organization. WHO | Comprehensive mental health action plan 2013–2020. WHO [Inter-
net]. 2015 [cited 2017 Oct 4]; Available from: http://www.who.int/mental_health/action_plan_2013/en/
17. Patel V, Chisholm D, Parikh R, Charlson FJ, Degenhardt L, Dua T, et al. Addressing the burden of men-
tal, neurological, and substance use disorders: key messages from Disease Control Priorities, 3rd edi-
tion. Lancet (London, England). 2016 Apr 16; 387(10028):1672–85.
Development assistance for child and adolescent mental health
PLOS Medicine | https://doi.org/10.1371/journal.pmed.1002524 March 9, 2018 12 / 12


















