Global and community health--3
14
-
Upload
thelsjm-ltd -
Category
Documents
-
view
212 -
download
0
description
We are taught from day 1 of medical school that the most important tool the physician has to reach a diagnosis is the history.
Transcript of Global and community health--3

256 lsjm 30 april 2010 volume 01

257lsjm 30 april 2010 volume 01
EDITORIAL
Dear Readers
Having explored what is “unhealthy” and how medicine “innovates” constantly in our opening issues, we now sit back (though not on our laurels) for our third offering to “reflect” on health and science.
In my previous piece I spoke about issues that spanned nations and peoples, races and continents. We touched on the changing outlook of multinational pharmaceutical conglomerates and the scale of death due to preventable diseases in the forgotten places of our world.
Today I want to reflect on something as important, but infinitely closer to our daily practicing lives:
Relationships and adviceThe American physician Martin H. Fischer said “In the sick room, ten cents’ worth of human understanding equals ten dollars’ worth of medical science,” and in dynamic 21st century Western healthcare where investigations can be definitive and cures may seem instant, aspiring physicians would do well to keep this in mind.
The first lesson I learnt in clinical school was to always stand up and walk out to greet and receive your waiting patient. The elderly clinician offering these wise words went on to add that by doing so one was afforded an opportunity to asses gait, balance and locomotor functioning instantly, saving precious NHS time. Furthermore he said it would prevent the development of obesity, diabetes, hypertension and all manner of other ailments that accompany our often-sedentary profession. What he failed to mention, was that this simple act allowed us to begin the all important doctor-patient relationship, on an equal footing, echoing Fischer’s words. A footing of kindness and compassion, where as a healer we rise to meet our patients as a manner of respect so that we can both move forward together. There is no cure without a willing patient that complies with our recommendations.
We are taught from day 1 of medical school that the most important tool the physician has to reach a diagnosis is the history. The exchange of between patient and doctor will almost always have within it the offending disease. As important as the initial words spoken by the patient are the recommendations given by the physician. The advice we give, as healthcare professionals is crucial. Doctors remain one of the most trusted professionals in today’s society, and our counsel is often sought and followed.
To this end the interesting discussion piece on previous “gold standard” advice for avoiding skin cancer being perhaps outdated is well worth a read. Vitamin D is now thought to play a vital role in the immune response and keeping out of the sun may indeed prevent us getting melanomas but instead predispose us to M. Tuberculosis! Furthermore the illuminating research article on the effect of the advice on cigarette packaging in helping smokers to quit in Australia further goes to show the immense power of the spoken word and the visual graphic (something doctors and health authorities would do well to remember during a global recession, the spoken word is infinitely less expensive than the manufactured tablet).
Our final piece deals with the sequelae when a doctor-patient relationship goes awry, namely due to the conscientious objection of a clinician with regards to a procedure. It is a significant work as we often find in our daily lives that the course of a consultation and treatment often never runs smooth.
I hope that you find this section challenging, interesting, enjoyable and above all stimulating. I hope that you leave it with the knowledge that for whatever you may prescribe or cut, it is often what you say that heals most.
With best wishes
Vishal [email protected]
258 lsjm 30 april 2010 volume 01
ARTICLE
“Not all sunlight is dangerous, just ultraviolet radiation”Professor JLM Hawk
Shreedhar Krishna, Ajoy BardhanYear 6 Medicine, Imperial College, [email protected]: 10.4201/lsjm.gch.008Dermatologists are human. Therefore, there will be an inherent individual variation in the quality and content of advice provided to the public. However, for the purposes of this essay (as well as being a source of British sunlight policy), the validity of elements comprising the SunSmart message will be examined.
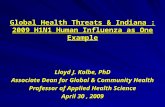
Over the last 25 years, the incidence of malignant melanoma (MM) has increased more than for any other common cancer in the UK.
The SunSmart Message2
Spend time in the shade between 11 and 3Make sure you never burnAim to cover up with a t-shirt, hat and sunglassesRemember to take extra care with childrenThen use factor 15+ sunscreen
In order to examine the efficacy of the advice provided, it is necessary to begin with some statistics.
The FactsTable 1. Age-standardised malignant melanoma incidence rates, Great Britain, 1975-20053
On the face of it, this data seems to support SunSmart’s cautious approach to sun exposure. However, it is not currently known how sun exposure leads to melanoma. Adults who work outdoors as well as children who play outdoors are less likely to develop melanoma than those who work or play indoors.,4 Furthermore, work on a black population showed that melanoma was more common on the lower legs and soles of the feet5 - not prime sun-exposed areas. Clearly, the relationship between melanoma and sunlight is not simple.
The TightropeAdvice on sunshine is aimed at achieving ‘optimum’ sun exposure. However, there is no general consensus on the balance between adverse and beneficial effects.
Physicians walk a precarious tightrope: Prescribe too much sun and there is a greater susceptibility to skin cancers; too little leads to vitamin D deficiency. Complicating matters further, there are large variations in what is considered a sufficient vitamin D level for health. Moreover, proximal factors such a skin pigmentation or traditional dresswear mean that there cannot be one universal optimum exposure for all.
Although UV radiation is prominently associated with the above diseases, it is worthwhile to note that “99 of every 100 British people won’t develop melanoma during their lifetime, and nine of 10 will be free of nonmelanoma skin cancer.”
Conversely, lower intensity UVB exposure is linked to cancers far more prevalent than those affecting the skin. Lending credence to this argument, Giovannucci et al. showed an increase of 17% in total cancer incidence and 29% in mortality with a decrease of 25nmol/L in serum 25(OH)D
3.6 Thus, other than for high skin cancer risk
groups (e.g. individuals with large numbers of melanocytic naevi),7 the benefits of thorough sun exposure far outweigh its dangers.
Vitamin D deficiency has been linked to myriad other conditions, many of which are much commoner than skin cancer. These include multiple sclerosis, schizophrenia, diabetes and cardiovascular disease.
Using the value proposed by Zittermann (100-150 nmol/L), dark-skinned children and the elderly are especially at risk of vitamin D deficiency.
The worryingly low levels reported in the UK elderly population are woefully insufficient for health throughout the year and are associated with osteomalacia, muscle weakness and a tendency to falls and consequent fractures.
Serum 25(OH)D nmol/L Summer Winter
UK children 80 52
Dark-skinned UK children 36-42*
Teenagers 71 21
Young adults 70 30
UK Elderly 35 23

259lsjm 30 april 2010 volume 01
ARTICLE
*(not differentiated by season
Serum 25(OH)D nmol/L Summer Winter
UK children 80 52
Dark-skinned UK children 36-42*
Teenagers 71 21
Young adults 70 30
UK Elderly 35 23
Table 2.
The SunSmart MessageThe UK SunSmart message is derived from an earlier Australian campaign.8 Australia, however, has a considerably greater intensity of sunlight as well as the highest melanoma incidence in the world.9
SunSmart was thus developed in view of Australian objectives to reduce skin cancer; while its message is rational in temperate climates, it is somewhat unsuitable for the UK for a number of reasons:
The British maritime climate produces substantial cloud cover 1. even at the height of summer.People in England and especially Scotland obtain minimal 2. vitamin D from sunlight between October and March.10,
Individual exposure to sunlight demonstrates that Australians 3. are exposed to considerably more UVR than the British.
Thus rather than covering up, we should be opportunistic in obtaining sun exposure, while taking care not to burn.
SUVB exposure causes the provitamin D
3 to be isomerised to pre-
vitamin D3. During continual exposure to sunlight, the pre-vitamin
converts via photo-isomerisation into vitamin D3. Critically, only UVB
exposure initiates vitamin D synthesis. Thus, the recommendation to stay in the shade around midday, may be ensuring that sun exposure is to UVA wavelengths – increasing skin cancer risk with minimal vitamin D synthesis.
MSunburn is especially linked with melanoma and basal cell carcinoma; its avoidance can only be a good thing.
T“While regular sunscreen application can prevent the development of cutaneous dysplasia in sunny countries like Australia without compromising vitamin D levels, daily use of skin products containing UV filters in the UK, which is not known for its sunny climate, is unnecessary and may be potentially harmful.”11
Professor Diffey
The sun protection factor (SPF) is defined as the ratio of the least amount of UV energy required to produce minimal erythema on skin protected by sunscreen to the amount required to produce the same erythema on unprotected skin. Paradoxically, individuals who regularly use high factor (SPF ≥ 15) are more likely to report sunburn than those who do not. This suggests that these individuals have misplaced confidence in their sunscreen and consequently
spend more time in the sun.
It is important to note that the SPF is phototested at an internationally agreed application thickness of 2 mg/cm2. Unfortunately, evidence suggests that consumers apply sunscreen more sparingly, typically between 0.5 – 1.3 mg/cm. Stokes et al. suggest that the actual protection conferred is between 20-50% lower than the SPF on the label. Additionally, there are likely variations in application technique which have not been accounted for.
Therefore for those seeking sun protection, it would be perhaps more prudent to emphasise the generous use of sunscreen rather than a specific SPF. Furthermore, advice on re-application of sunscreen after swimming or significant sweating must be disseminated.
Conclusion
Other than for individuals at high risk of skin cancer, adopting certain behaviours prescribed by SunSmart is unwise and will likely lead to vitamin D deficiency.For the general public, the benefits of thorough sun exposure outweigh the increased risk of skin cancers.Thus, advice should encourage opportunistic sun exposure, while still taking care to avoid sunburn.Due to proximal factors such as skin pigmentation, the ‘one size fits all’ approach of SunSmart is not suitable. Rather, advice should be individualised to fit the patient – not the other way around. Certain groups, such as dark-skinned people and breast-fed babies are at greater risk of vitamin D deficiency and must be advised accordingly.
ReferencesHawk JL. Sunlight and health. Not all sunlight is dangerous, just ultraviolet 1.
radiation. BMJ (Clinical research ed.) 1999; 319(7216): 1066-7; author
reply 1068
http://www.cancerresearchuk.org/sunsmart2.
Statistical Information Team, Cancer Research UK3.
Kaskel P, Sander S, Kron M et al. Outdoor activities in childhood: a 4.
protective factor for cutaneous melanoma? Results of a case-control study
in 271 matched pairs. British Journal of Dermatology 2001; 145(4): 602-
609 doi:10.1046/j.1365-2133.2001.04432.x
Crombie IK. Racial differences in melanoma incidence. British Journal of 5.
Cancer 1979; 40(2): 185-193
Giovannucci E, Liu Y, Rimm EM et al. Prospective study of predictors of 6.
vitamin D status and cancer incidence and mortality in men. Journal of the
For references see thelsjm.co.uk.

260 lsjm 30 april 2010 volume 01
LETTERS
I am a second year medical student, who had the opportunity to get involved and know more about Chagas disease in a studentship last summer. As I looked more into the research, I feel obliged to give you a summary on the development of your disease in the past century and its way forward.
Past For your reference, the American human trypanosomiasis that you discovered has been now named as Chagas disease, paying tribute to your unique triple discovery 101 years ago. As it has been overshadowed by other priorities such as HIV/AIDS (a viral infection causing immunodeficiency reported in 1980s) and Malaria by the media, governments and organizations, it is currently regarded as a Neglected Tropical Disease. To date, Chagas Disease has an incidence of 500,000 per year1 and a prevalence of 1.4%2. It is estimated to infect 8-14 million people in 18 Latin American countries3, with 667000 disability adjusted life years (DALYs)2.
Concerning the pathogenesis, on top of the vectorial transmission of T cruzi via Triatoma infestans you proposed, transfusional, transplacentary transmissions and food and beverage contamination have been the new emerging means4. Through clinical experience, physicians generalized that the acute phase involves pyrexia, swollen lymph glands and inflammation of the eye. Though patients have high parasitaemia during acute phase, they usually go undiagnosed, as it is not uncommon that they are asymptomatic. 10-30 years after initial infection, about 30-40% of the patients develop chronic Chagas disease involving cardiac or gastrointestinal complications. 5
Regarding treatment and management, Uruguay, Chile and Brazil had declared that they are free of T cruzi transmission due to intensive insecticide spraying.6 Benznidazole and Nifurtimox have been the two main drugs prescribed for children, which has up to 62% sero-conversion rate in 3-to-4-year follow-up7. However, they have not been compliant due to long-term treatment (30 to 60 days) and lack of accessibility. They are also reported to have severe gastrointestinal, dermatological, neurological and haematological adverse events limiting the use.8 There are blood bank screenings to monitor and guard against transfusional transmission although vaccination development is at its infancy.
Present One might be delighted to be informed that the World Health Organization (WHO), a specialized agency coordinating authority on international public health started 14 years after your death, proposed a ‘New global effort to eliminate Chagas Disease’ in 20079. It was initially welcomed but received some criticism on the lack of strategic plans6. I have, therefore, tried to investigate three of the ‘five-pillar strategy’ and analyze the situation as a basis for the insights into way forward in the next section.
Monitoring and estimation of burden of disease It was suggested that Chagas disease should be integrated into the health monitoring information systems of Latin American countries. The development of representative, reliable and valid surveys to estimate domestic manifestation, incidence, prevalence, disability, population knowledge, prevention and control was needed6. I have to admit the development of these tools is slow, if not non-existing. However, researchers from Pan American Health Organization (PAHO) had pioneered an estimate of 12755 T. Cruzi-infected Hispanic pregnant women to migrate to the States, with 166 to 638 infected newborns. They also gave information in specific states to monitor, giving a good start for surveillance.10
Identify diagnostic test for screening and diagnosis Prior to the campaign WHO set up, there was a multitude of procedures, including immunosorbent assays, immunofluorescence antibody tests, radioimmune precipitation and PCR based assays serving the purpose of screening and diagnosis. There was an urgent need for a standardized detection. I am happy to inform you that the WHO had looked into it and evaluated the serological assays. They had concluded in the research that radioimmunoprecipitation assays (RIPA) could be considered a gold standard for evaluation of other assays and that the sensitivities and specificities of seven enzyme-linked immunosorbent assays (ELISA) enable them to be used solely for screening and diagnosis.11 Evidence has shown that the reliability of assays is not affected by the origin of samples.12
Letter to Carlos Chagas - Insights into Chagas diseaseJan Man WongYear 2 Medicine, University of East [email protected]:10.4201/lsjm.gch.009
Illu
stra
tion
: Rho
dniu
s pro
lixus
261lsjm 30 april 2010 volume 01
LETTERS
Promote consensus on adequate management As aforementioned, as the two main drugs have high toxicity, short supply and issues regarding efficacy and availability, development of new drug is deemed necessary5. A non-profit product development partnership, Drug for Neglected Diseases initiative (DNDi), tried to link Research and Development to drugs. They have projects in three time phases, ranging from reformulation for children (short-term) to combination treatment (medium-term) to drug discovery (long-term)13.
Regarding the two existing drugs, Marin-Neto and his colleagues outlined a rationale and design and recruiting for a randomized-controlled trial (RCT) assessing Chagas cardiomyopathy, the BENEFIT trial14. Coura had also proposed combination treatment with Allopurinol for new pharmacological regimes15. The All-Party Parlimentary Group on Malaria and Neglected Tropical Diseases from the UK announced in its report that a vaccine has been tested and an antifungal agent has been proposed as a second-line treatment16.
Adding to the good news, the Medecins Sans Frontieres (MSF, aka Doctors without Borders) had published a paper recently, proving the viability, feasibility and necessity of diagnosis and treatment programmes for the disease in four different rural areas in Latin America, given the collaboration between governments and the organization.8
Future Agreeing with Reithinger and colleagues, a clearer strategic plan for new operational activities is crucial6, especially when renewing the ‘New Global Effort to eliminate Chagas Disease’ this year. With the insights from multiple studies, I have suggested the following:
Elimination of vectors As seen from the statistics from Ministry of Health in your home country, Brazil, most of the Chagas cases were transmitted by vectors4, a more stringent and sustainable insecticide spraying is needed. Insecticide spraying is often reported to be irregular if not absent. Insecticide resistance should be monitored and alternatives considered. Insecticide-treated bed nets or dog collars, change of insecticide and expanding spraying areas are other ideas to be considered6. WHO should take the initiative to re-iterate the importance of sustainable spraying and other complimentary practices to governments.
Establish diagnostic and screening protocols As the WHO evaluation on serological assays only included those prior to year 2000 11, they could take a step forward and assess the results from other studies of similar sort. After sufficient data is obtained, it would be best if the WHO or other dedicated research institutes could consolidate the data and develop a meta-analysis, which could serve the basis for a ‘gold standard’ protocol for screening and diagnosis.
Development of treatment / management consensus It is important that an independent agent, such as WHO, ensures that the BENEFIT trial and combination treatment trial is well implemented with sufficient resources. It is also good news that Japanese company Eisai had agreed to develop first new compound, E1224, for Chagas disease with DNDi. This anti-fungal may reduce the non-compliant issues due to its long half-life when come to market earliest in 201417.
The MSF diagnosis and treatment programme had six components including information, education and communication, vector control, health staff training, screening and diagnosis, treatment and compliance and logistics8. Although there are areas that are subject to improvement, such as diagnostic tools, it has a number of advantages. The programme in itself helps training health staff, which compensates for the lack of trained front-line staff due to decentralization of health systems. The component of vector control could, in turn, help the government in surveillance of the disease. With these advantages, it is advised that the WHO, after careful modification, could publicize it as a universally agreed ‘treatment strategy’.
All in all, numerous institutes including DNDi, MSF, PAHO have worked towards the elimination of Chagas Disease, long after your death. A uniting body is needed to ensure these efforts are efficient and meet this goal. At present, the WHO is the defacto lead for such efforts. Let us hope that the renewal of the global effort would not only look good on paper but also practical in implementation.
I sincerely hope to have delivered a succinct but thorough report of progress in this area; with the vigorous input received after this to serve as a stimulus to review the report in the future.
Yours sincerely,
Medical Student
For full references see thelsjm.co.uk.

262 lsjm 30 april 2010 volume 01
PERSPECTIVE
Is Breast cancer prevention a realistic prospect for the future?Katie GriggsYear 3 Medicine, University of [email protected]:10.4201/lsjm.gch.010
Breast cancer is the most common carcinoma affecting women in the UK, making up 31.5% of new female malignancies in 2006.1 It is the leading cause of mortality in women aged 40 to 552, with 11,040 female deaths attributed to the disease in 2005.3 This essay aims to explore the issues surrounding the prevention of breast cancer by reviewing current literature on the topic, and to come to some conclusion as to whether it will ever be possible to completely eradicate the disease. There are some known risk factors which may contribute to a person’s chances of developing breast cancer - although these are by no means definitive indicators of those who will develop the disease. These include genetic4 and hormonal factors5,6,, age7 and various lifestyle factors8,9.
Assessing a person’s riskBased on the risk factors mentioned above, it is possible to work out a woman’s chance of developing cancer, and use this in deciding whether to carry out preventative measures. As some methods of preventing breast cancer have quite severe effects on a woman’s life it is important to decide whether the risks are large enough for
sacrifices to be made elsewhere. In order to calculate a woman’s risk several mathematical models have been created. The Gail model is the most generally applicable, although it does neglect to take into consideration some factors (such as detailed family history) as effectively as others, notably The Claus Model10. The Gail model produces a figure which represents a woman’s five year risk of developing breast cancer, and preventative measures or treatment decisions are often based on that information.
Preventative MeasuresHormone related preventionIt has been found in studies on animals that oestrogens can be involved in the formation and proliferation of breast tumours and that removal of ovaries or administration of anti-oestrogenic drugs has an opposite effect. 11 In pre-menopausal women it is possible to suppress ovarian production of oestrogen. This process is known as ovarian ablation and can be carried out in various ways: oophorectomy, by use of radiation, or treatment with an LHRH (luteinizing hormone-releasing hormone) analogue. It has been proved that bilateral prophylactic oophorectomy offers a protective influence against
Imag
e: Is
tock
xxxx
xxxx
xxxx

263lsjm 30 april 2010 volume 01
PERSPECTIVE
breast cancer – women who had the operation before the age of forty had a 45% reduced risk of developing the disease compared to women with a natural menopause between the ages of 50 to 54.12 There are however downsides to this procedure which need to be carefully considered before the surgery is carried out. Factors associated with an early menopause (hot flushes, anxiety and depression13) may have a significant effect on a woman’s life. There are also long term risks of osteoporosis and decreased libido. A slightly controversial method of breast cancer prevention – but perhaps the most successful - is bilateral prophylactic mastectomy. It has been found that this procedure in women with the BRCA1/2 mutation reduces the risk of breast cancer by approximately 95% in women with prior or concurrent bilateral prophylactic oophorectomy and by approximately 90% in women with intact ovaries10. However, the effects of such a drastic cosmetic procedure can be vast. Women who have had mastectomies without actually having cancer have reported problems with body image, anxiety and depression as well as psychological distress.14 Because of the negative effects associated with such procedures they are currently mainly utilised by those who are considered to be at a high risk of developing breast cancer. If similar successful outcomes could be found in the future through methods which would not have the extreme cosmetic and psychological effects there could be a great uptake of prophylactic treatment in women at low or moderate risk who might otherwise avoid it.
ChemopreventionA more preferable method of breast cancer prevention without such radical effects is chemoprevention; the use of drugs which aim to interrupt carcinogenesis and thus prevent the formation or development of tumours. Selective Oestrogen Receptor Modulators (SERMS) work by blocking the effects of oestrogen on breast tissue. Tamoxifen is the most widely used SERM15 and its use in order to reduce the risk of breast cancer in women with 5 year risk of at least 1.66% (as determined by the GAIL model) has been approved by the FDA16. The NSABP P-1 Study which began in 1992 and recruited 13 388 women who had an increased risk of breast cancer found that tamoxifen in the dose of 20mg per day reduced the risk of invasive breast cancer by 49% after a median follow up of 54.6 months (p<0.0001)17.
There were significant downsides to the use of tamoxifen as a preventative measure; the 6681 women who took tamoxifen as opposed to placebo had 21 additional endometrial cancers (RR 2.53), and were exposed to higher risks of developing pulmonary embolisms (RR3.01) and deep vein thromboses (RR1.60)18. The balance between the benefits and the risk of adverse effect of tamoxifen were different
in each patient depending on their individual risk profile, with younger women benefitting most and experiencing fewer negative effects19. Raloxifene, another SERM which is approved as both a treatment and preventative agent in postmenopausal osteoporosis20, has been found to have a significant effect in reducing breast cancer risk in postmenopausal women. In the MORE study it was found that raloxifene reduced the risk of oestrogen receptor-positive invasive breast cancer by 84%21. In the largest breast cancer trial ever conducted22 on postmenopausal women at high risk of developing breast cancer, raloxifene was found to be as effective as tamoxifen at reducing breast cancer incidence22. Its benefits also included a lower risk of developing uterine cancers and cataracts when compared to tamoxifen23. However, because these results have been so significant only on postmenopausal women, further research is required to ascertain the benefits of Raloxifene on pre-menopausal women, or to find another SERM that is suitable for treating them.In making the decision to use prophylactic treatment for breast cancer it is important to take into consideration the number of people who will have to be treated in order to prevent one case (NNT). The results of the NSABP-P1 trial found that 56 women would have to take tamoxifen for 5 years in order for one person to experience prevention of an invasive carcinoma over that period and the next seven years17. The MORE study found raloxifene had an NNT of 125 over four years24. There is little evidence to suggest that tamoxifen or raloxifene are effective in preventing breast cancer in women at low or moderate risk25. This fact, the NNT values and the negative effects associated with treatment with these drugs imply that it would not be practical for the population as a whole to be treated with either of these SERMS as a preventative measure. In the future, an ideal SERM would have similar or increased ability to reduce breast cancer risk – without the significant downsides that are present in the current SERMs used in prophylactic breast cancer therapy. There are current trials into a ‘new generation’ of SERMs which have the potential to fulfil these requirements, and bazedoxifene, arzoxifene and lasofoxifene have been found to be promising26, although these treatments are not without problems, and further research is required.
Post-menopausal women do not produce oestrogen in the ovaries. Androgens are synthesised in their adrenal glands and converted to oestrone by the aromatase – a cytochrome enzyme.2728 This process can be interrupted by treatment with aromatase inhibitors (AIs). AIs are currently used as a breast cancer treatment, often alongside SERMS like tamoxifen, and have found to be very successful in this role29. There are trials currently underway to investigate the use of AIs as a chemo preventative measure, and data from pre-clinical studies has been promising.30 31Results from the IBIS-2 randomised
For full references see thelsjm.co.uk.
264 lsjm 30 april 2010 volume 01
PERSPECTIVE
References1. Cancer Statistics Registrations 2006 – A National Statistics publication. Series MB1 No.37, 2008 ISSN 0143–4829 (Accessed online on 19/01/09 at www.statistics. gov.uk)2. DEVITA, V.T, HELLMAN S., ROSEBERG S.A., AUSGABE G., Principles and Practice of Oncology (Periodicals) Lippincott Williams & Wilkins, Dec 2000, page 16513. Mortality Statistics- Review of the Registrar General on deaths by cause, sex and age, in England and Wales, 2005. London: Office for national statistics. Series DH2 No.32 ISSN 0140-2587 (Accessed online at 01/02/09 at www.statistics.gov.uk)4. McPHERSON K, STEEL CM, DIXON JM, Breast cancer— epidemiology, risk factors, and genetics British Medical Journal, September 2000: 321(7261) Pages 624-628. 5. HENDERSON BE, FEIGELSON HS. Carcinogenesis, Oxford University Press- March 2000 Vol. 21, No. 3, Pages 427-433, 6. The collaborative group on hormonal factors in breast cancer, breast cancer and hormonal contraceptives: collaborative reanalysis of individual data on 53297 without breast cancer from 54 epidemiological studies. (No authors listed) Lancet 1996, 347 Pages 1713-27.7. Cancer statistics 2005- Cancer Research UK Website. (Accessed online on 01/02/09 at http://www.info.cancerresearchuk.org/ cancerstats/types/breast)8. VAN DEN BRANDT PA, SPIEGELMAN D, YAUN SS et al, Reversal of relation between body mass and endogenous oestrogen concentrations with menopausal status. Journal of the National Cancer Institute 1996; 88: Pages 756-8
For full references see thelsjm.co.uk.
phase III trial – which is a trial of the use of anastrozole in 6000 postmenopausal women with an increased risk of breast cancer - are expected in 201232. Results from this and another major study – the MAP.3 phase III randomised prevention trial33, have the potential to change the methods and success of chemoprevention drastically in the future.
As SERMS and AIs are not without their faults, there has been research into the use of retinoids (derivatives of vitamin A which are known to play a role in cellular and tissue differentiation) as a possible chemoprevention method. Many retinoids produce toxic symptoms that are not acceptable as a risk reduction side effect16, however a less toxic analogue34, fenretinide, has been the subject of several chemoprevention trials. A phase III trial of fenretinide on women with a history of stage I breast cancer found a 35% reduction of contralateral breast cancer in premenopausal women 35. This was found to be linked to levels of plasma insulin-like growth factor-I (IGF-I) levels. Based on these findings, significant research is underway in establishing the role of IGF-I in breast cancer risk36, and the potential implications for retinoid treatment in premenopausal women and those receiving HRT are also areas being researched.
Prevention of ER negative breast cancerAlthough there have been promising results from trials of SERMS and AI in reduction of estrogen receptor positive (ER+) breast cancer, these treatments have no effect on ER- tumour formation37. As around a quarter of breast cancers are ER-38, there is a considerable effort being made to find a way of preventing such malignancies. There are several potential molecular targets that are currently under investigation, and preclinical results have found that rexinoids, tyrosine kinase inhibitors and dual kinase inhibitors, and COX-2 inhibitors prevent the development of ER-negative breast cancer in transgenic mice37. Other targets being investigated include ligands for peroxisome proliferator-activated receptor γ, retinoic acid receptors, vitamin D
3 derivatives, VEGFR, and histone deacetylase inhibitors16. If any of
the methods currently being tested are found to prevent ER- breast cancer, there could be a potential for chemoprevention of both ER- and ER+ cancers by treating patients at risk with a combination of these methods and SERMS/AI. ConclusionBased on the literature reviewed in this essay, it appears that breast cancer will never be absolutely preventable, due to the impossibility of eliminating all methods of carcinogenesis. The fact that not all breast cancers result from the risk factors mentioned earlier in the report38 means that many cases cannot be anticipated and prevented. Prophylactic treatment options that are currently available have fairly severe side effects. These effects would not be willingly tolerated in those who do not consider themselves at a high risk of developing breast cancer and thus by avoiding treatment these people are left unprotected. It does however seem that breast cancer incidence could be considerably reduced through developing techniques of prevention. Preliminary results of studies into several new methods of chemoprevention which may have reduced side effects have been promising. Thus in the future there could be the potential for a virtually harmless preventative measure to be given to everyone, regardless of their risk. This would have a significant effect on breast cancer incidence and mortality.
EM o
f Bre
ast C
ance
r cel
ls- W
ellc
ome
Imag
e


266 lsjm 30 april 2010 volume 01
RESEARCH
Imag
e: W
ellc
ome
Imag
e
Evaluating the impact of cigarette packet graphics on tertiary studentsLing Chen, Courtney Chun Hai Lai, Jessica Tin Yan Lai, Joanna Hong-Meng TaiYear 5 Medicine, Monash University, AustraliaMonash University Medical Students Smoking Reseach [email protected]:10.4201/lsjm.gch.011AbstractObjective: This evaluation measured the initial impact of graphical health warnings within a tertiary student population aged 18---29.Method: A cross-sectional study was conducted in Melbourne, Australia in August 2006 through a self-administered survey. 415 surveys were returned using convenience sampling from a university, a technical college and a suburban shopping centre. Of these, 373 were considered eligible.Results: 81.4% of participants noticed the graphics. Graphics recognition and recall was greater in current smokers compared to past smokers or non-smokers. A greater number of past smokers quit smoking in the six months following the release of the graphics compared with the previous six months. Cost, family/household and friends were the most common factors contributing to attempts or thoughts on smoking cessation.Conclusion: Cigarette packet graphics appeared to encourage smoking cessation within the study population. However, further research is still required into the long term effects of the graphic health warnings and other avenues for smoking cessation. KEY WORDS: Australia; Health knowledge, attitudes, practice; Product labelling; Smoking; Smoking cessation; Students
IntroductionTeenagers and young adults have the highest proportion of current smokers compared to any other age group in Australia. People aged between 18---24 and 25---34 have a smoking prevalence of 23.1% and 27.6% respectively according to the National Health Survey 2007---2008.1 Although this prevalence is slowly declining in Australia,2 this age group has generally been inadequately targeted in anti-smoking interventions.3, 4 Cigarette smoking can cause numerous deleterious health effects, notably within the respiratory and cardiovascular systems.5, 6 Both active and passive smokers face major health risks,7 with smokers having an increased ratio of mortality compared to never-smokers.8 Smoking cessation can reduce the risk of subsequent adverse smoking-related health effects.9, 10Many public health promotion campaigns are aimed at discouraging smoking uptake and encouraging cessation, including text-based cigarette packet warnings and media advertising campaigns within Australia. From 1 March 2006, the Australian Federal Government has mandated graphical health warnings on
new cigarette packets in order to inform, encourage cessation and discourage uptake.11 This follows similar actions in Canada, Brazil, Poland, Singapore and Thailand, with many other countries having implemented these graphics since.12 An evaluation of the graphical warnings in Canada found positive correlations between thoughts regarding the images, quitting intentions, and the increase in quitting attempts.13 Studies in Brazil, Greece and New Zealand showed graphical warnings to encourage cessation and prevent uptake.14---16 In Australia, these health warnings

267lsjm 30 april 2010 volume 01
RESEARCH
had similar effects including deterring school-aged adolescents from smoking and doubling the number of calls to the Australian Quitline.17---19 However, despite the high smoking uptake in the tertiary student population (aged 18---29), no study has been previously undertaken to examine the impact of cigarette packet graphical health warnings on this group.3
ObjectiveThis evaluation measured the initial impact of the graphical health warnings within a population of tertiary students aged 18---29 in Melbourne, Australia, through their reported smoking status, time of cessation and influences on smoking cessation, .
MethodA cross-sectional self-administered survey assessed the impact of the new cigarette packet graphics through 18 multiple choice and four short answer questions (see Appendix 1). The survey elicited participants’ demographic data, smoking status and habits, awareness and thoughts about the new campaign, and changes to beliefs or behaviours. The survey was approved by the Monash University Standing Committee on Ethics in Research Involving Humans and piloted on a small group of young adults before distribution.Smoking status was categorised by “I have never smoked a single cigarette”, “I have previously smoked” or “I currently smoke”. Previous smokers were further classified as having stopped within the last 6 months, between 6---12 months or more than a year. Identification of cigarette packet labelling as an influencing factor in a past smoker’s decision to quit was determined by rating “health warnings on cigarette packets” as having at least “a little” effect.Participants’ written responses were categorised independently by two researchers as either positive (encouraged cessation or continued avoidance of smoking) or non-positive and disagreements were resolved by a third researcher. Convenience sampling of young adults in the vicinity of the researchers were approached and invited to participate in the survey which was carried out during August 2006. An explanatory statement was issued with the self-administered survey, which was returned to a sealed box. Smoking and non-smoking participants were recruited from the Clayton campus of Monash University, the Chadstone and Waverley campuses of Holmesglen Institute of TAFE (Technical and Further Education), and a suburban shopping centre. A total of 415 participants were surveyed of which 373 were considered eligible: 179 from Monash University, 160 from
Holmesglen Institution of TAFE and 34 from The Glen Centro Shopping Centre. Participants were considered eligible if they provided information on smoking status, were aged 18---29 and studying at a tertiary institution. Surveys completed by more than one individual were excluded from analyses. Unanswered questions were excluded from analyses. The data was analysed using SPSS (version 14.0) and Microsoft Excel (version 10.2614.3501).
ResultsThere were a total of 373 eligible participants with 183 non-smokers, 102 past smokers and 88 current smokers. The participants’ recognition and recall of the graphics on cigarette packets are shown in Table 1. Graphics recognition and recall was greater in current smokers compared to non-smokers or past smokers. Amongst the 102 past smokers, a total of 34 people had ceased smoking in the six months after the release of the graphics compared to 13 people who quit in the previous six months.Of these 47 past smokers, those who identified health warnings on cigarette packets as an influencing factor were significantly more likely to have quit in the six months following the release of the graphics compared to the previous six months (odds ratio 7.1, 95% confidence interval 1.31 to 38.8; p=0.023). However, the most common factors contributing to attempts or thoughts on
Non-smoker Past smoker Current smoker TOTAL
Noticed packet change (%)
121 (66.9) 80 (80.0) 73 (85.9) 274 (74.9)
Noticed presence of graphics (%)
139 (76.0) 86 (84.3) 77 (89.5) 302 (81.4)
Mean number of graphics recalled (min, max)
1.82 (0, 6) 1.83 (0, 6) 2.56 (0, 6) 2.01 (0, 6)
Table 1: Graphics recognition and recall by smoking status
Imag
e: W
ellc
ome
Imag
e

268 lsjm 30 april 2010 volume 01
smoking cessation, identified by past and current smokers, were cost (75.2%), family/household (73.3%) and friends (70.5%), with health warnings on cigarette packets at 52.4%. Fifty percent of participants who noticed graphics on cigarette packets wrote a positive remark on the graphics’ effects such as “I have stopped”, “I have decreased in how many I smoke a day” and “[it] reaffirmed my anti-smoking beliefs”. There was no significant correlation between smoking status and whether participants wrote a positive remark (γ2 = 0.468, df = 2, p = 0.791). Non-positive remarks included “I hide the packet”, “the pictures just said what I already knew”, “no change” and non-responses.
DiscussionWhile other studies have compared graphical warnings to text based warnings,20---22 assessed young adults’ perception of the graphics4, 15, 18 and examined the perceived impact of graphical warnings,13---22 they did not focus on the impact of these warnings on tertiary students in Australia. 23.6% of the study participants were current smokers, which is similar to the overall figures for the national smoking rates of 18---24 and 25---34 age groups.1 The limited number of tertiary institutions sampled and the method of selecting participants are potential sources of bias. The high number of people who stopped smoking in the six months following the graphics’ release suggests that cigarette packet graphics could have a significant effect on smoking cessation. However, this result is potentially confounded by the release of television campaigns of a similar nature.23 Although the long term effects of the graphic health warnings could not be ascertained by this study, it has been shown that previous attempts to stop smoking is a predictor for future attempts at cessation and reduced smoking intensity.24, 25While cost is a contributing factor to smoking cessation, it has been consistently increasing since 1993.26 Therefore, its effect on smoking cessation after the introduction of cigarette packet graphics should be minimal. While participants reported family and friends as contributing to thoughts and attempts on smoking cessation, this encouragement may have been motivated by their own viewing of the graphics.Although this study was useful in measuring the possible short-term impact of the graphics, further research is required on the actual long-term effects. A larger sample size of past smokers may allow comparative analyses between predictors of smoking cessation to be conducted. The delay between the official release date and actual sale of cigarette packet graphics in stores was another limitation, resulting in variable initial exposure amongst study participants. Participants who had cigarette packets in view, retrieved cigarette packets or discussed the survey with friends may have also confounded the results.
ConclusionCigarette packet graphics appeared to encourage short-term smoking cessation in the participants surveyed. This pilot study has the potential to contribute to future studies focussing on tertiary students, however, due to the low statistical power and the use of convenience sampling, the generalisation of results to all tertiary students is limited. Future study is required to determine the long-term effects of graphic health warnings and other avenues for smoking cessation in tertiary students.
AcknowledgementsThis study was supervised by Associate Professor Ken Jones, Miss Tsharni Zazryn and Dr Craig Hassed. Assistance for statistical analyses was provided by Miss Tsharni Zazryn. Background information was provided by Julie Taylor and Sally McDonald from Department of Health and Ageing, Canberra. The researchers would also like to acknowledge Ms Victoria Cooper, Ms Bianca Ferrante, Mr Damien Smith and Ms Christina Taitt for allowing the research to be conducted at their respective locations. The researchers received no funding for this study.
Conflicts of InterestTo the best of the researchers’ knowledge, no conflicts of interest could be identified.
References1 Australian Bureau of Statistics. National health survey: Summary of 1. results, 2007---2008 (reissue). Cat. No. 4364.0. Canberra: Australian Bureau of Statistics; 2009. 2 Australian Bureau of Statistics. Tobacco smoking in Australia: A snapshot, 2. 2004---05. Cat. No. 4831.0.55.001. Canberra: Australian Bureau of Statistics; 2006.3 Hammond D. Smoking behaviour among young adults: Beyond youth 3. prevention. Tobacco Control. 2005;14(3):181---5. 4 Koval JJ, Aubut JA, Pederson LL, O’Hegarty M, Chan SS. The 4. potential effectiveness of warning labels on cigarette packages: The perceptions of young adult Canadians. Canadian Journal of Public Health. 2005;96(5):353---6.5 Mucha L, Stephenson J, Morandi N, Dirani R. Meta-analysis of disease 5. risk associated with smoking, by gender and intensity of smoking. Gender Medicine, 2006;3(4):279---91.6 Bjartveit K, Tverdal A. Health consequences of smoking 1---4 cigarettes 6. per day. Tobacco Control. 2005;14(5):315---20. 7 Reardon JZ. Environmental tobacco smoke: respiratory and other health 7. effects. Clinics in Chest Medicine. 2007;28(3):559---73.8 Wang H, Preston SH. Forecasting United States mortality using cohort 8. smoking histories. Proceedings of the National Academy of Sciences of the United States of America. 2009;106(2):393---8. Electronic publication.9 Critchley J, Capewell S. Smoking cessation for the secondary prevention 9.
For full references see thelsjm.co.uk.

269lsjm 30 april 2010 volume 01