Giulio Draetta, PhD, MD, Professor, Genomic … Draetta, PhD, MD, Professor, Genomic Medicine...
62
Keynote Address Giulio Draetta, PhD, MD, Professor, Genomic Medicine Director, Institute for Applied Cancer Science, MD Anderson Cancer Center
-
Upload
duongtuyen -
Category
Documents
-
view
214 -
download
0
Transcript of Giulio Draetta, PhD, MD, Professor, Genomic … Draetta, PhD, MD, Professor, Genomic Medicine...

Keynote Address
Giulio Draetta, PhD, MD, Professor, Genomic Medicine Director, Institute for Applied Cancer Science, MD Anderson Cancer Center

Waterfall plot of best percent change in target lesions from baseline for 133* patients on the basis of investigator assessment *Excludes patients with early death before re-imaging, non-measurable non-target disease, or indeterminate r...
Camidge et al., Activity and safety of crizotinib in patients with ALK-positive non-small-cell lung cancer: updated results from a phase 1 study The Lancet Oncology Volume 13, Issue 10 2012 1011 - 1019
When something works you notice it!!
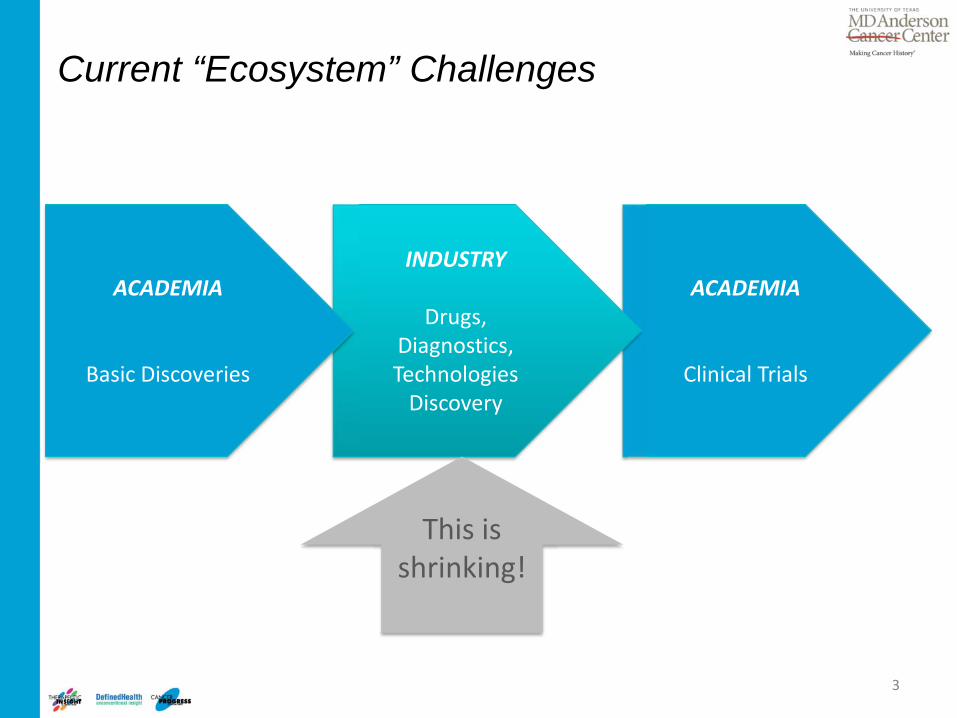
ACADEMIA
Clinical Trials
Current “Ecosystem” Challenges
INDUSTRY
Drugs, Diagnostics, Technologies
Discovery
ACADEMIA
Basic Discoveries
This is shrinking!
3

Percentage entering next stage
0
10
20
30
40
50
60
70
80
90
100
Entering Phase 1 Entering Phase 2 Entering Phase 3 Entering preregistration
Targeted therapy
Chemotherapy
Other
B. Pagliara, MedNous, 2011
Analysis conducted on 529 new chemical or biological entities that entered clinical trials between November 2004 and November 2005, followed through April 2011

Barriers to overall progress in cancer treatment
• Limited insights into factors driving cancer • Elemental knowledge of the cancer genome • Poor understanding of the target’s “biology”
– In what context (genetic, micro-environmental, host and macro-environmental) is the target rate-limiting?
• Lack of insight on appropriate combinations – Tumor will find a way to bypass a single-point intervention – Co-extinction is required to shut down a complex highly-redundant
network • Challenged cancer drug development ecosystem
5

Cancer signaling is not linear…. It is a highly inter-connected and redundant network
• Greater than 90% of cancer drugs fail approval • E ven approved ones are not s ubs tantially effective and provide benefit
only in a s ubs et of patients


New era of cancer genomics
OLD NEW
100
1,000
10,000
100,000
1,000,000
Sep-
01
Sep-
02
Sep-
03
Sep-
04
Sep-
05
Sep-
06
Sep-
07
Sep-
08
Sep-
09
Sep-
10
NHGRI Large-Scale Sequencing Program: Cumulative Sequence Production (Gb)
~5 million bases (2000) ~250 billion bases (CURRENT) Per week:

Comprehensive analysis
Common standards
Public data release
Coordination & comparison
International Cancer Genome Consortium Projects 38 project teams in 13 jurisdictions 16,000 tumor genomes in 5 years
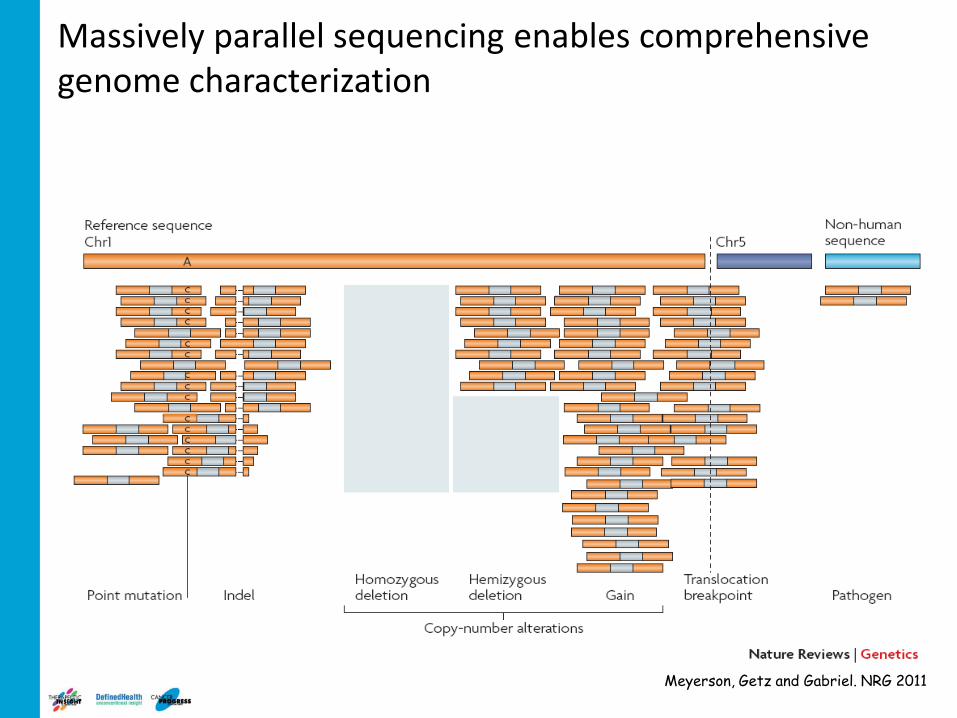
Massively parallel sequencing enables comprehensive genome characterization
Meyerson, Getz and Gabriel. NRG 2011

Translate cancer genome into actionable drug development endpoints
11
Need to functionalize the cancer genome
• Hundreds of candidates
• Drivers vs. passengers
• Context-specificity
• Deep biology to inform on mechanism of action
Analysis
Insight
Function
Cancer Genomics
The genome will inform the right targets and the right patients for the right drugs, ONLY when interpreted in context of the biology

Barriers to overall progress in cancer treatment
• Limited insights into factors driving cancer • Elemental knowledge of the cancer genome • Poor understanding of the target’s “biology”
– In what context (genetic, micro-environmental, host and macro-environmental) is the target rate-limiting?
• Lack of insight on appropriate combinations – Tumor will find a way to bypass a single-point intervention – Co-extinction is required to shut down a complex highly-redundant network
• Challenged cancer drug development ecosystem
12

Primary Tumor-Derived Cells Primary Engineered Cell Lines
ORF Libraries shRNA Libraries
In vivo Tumorigenicity
Metastasis
Anchorage Independent
growth
Invasion Migration
Proliferation Apoptosis
Cancer Phenotypes in the Context of Resistant Disease
Drug Resistance
Functional interrogation of cancer genomes
13 Tim Heffernan

Primary Melanocyte hTERT, p53DD, R24C, BRAFV600E
Focused “Driver Kinase” Lib. 110 WT Human
Kinases
Genetically-defined Tumor Target Cells
Orthotopic Injection Library of GEOIs
Multiple in vivo hits in JNK-pathway Clinical path hypothesis
Phenotype: in vivo tumorigenicity
Tumor Latency - Control: 28 weeks - Drivers: 10 -18 weeks
Proof of concept: In vivo screen to identify kinases that cooperate with BRAF to accelerate melanoma growth
14 T Heffernan, L Chin
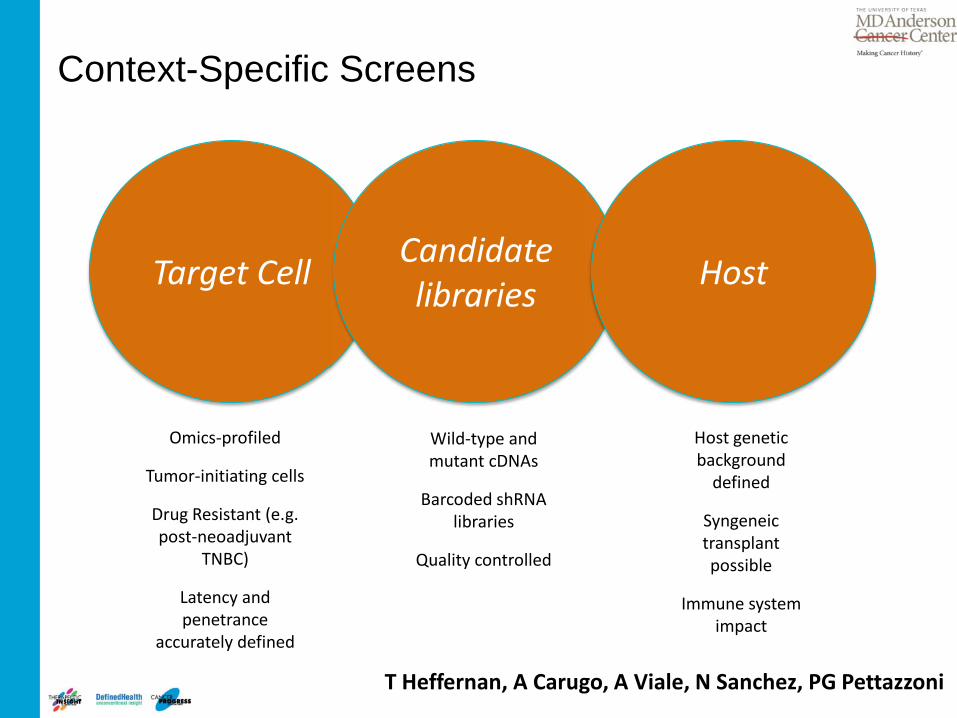
Context-Specific Screens
Target Cell
Omics-profiled
Tumor-initiating cells
Drug Resistant (e.g. post-neoadjuvant
TNBC)
Latency and penetrance
accurately defined
Candidate libraries
Wild-type and mutant cDNAs
Barcoded shRNA libraries
Quality controlled
Host
Host genetic background
defined
Syngeneic transplant possible
Immune system impact
T Heffernan, A Carugo, A Viale, N Sanchez, PG Pettazzoni
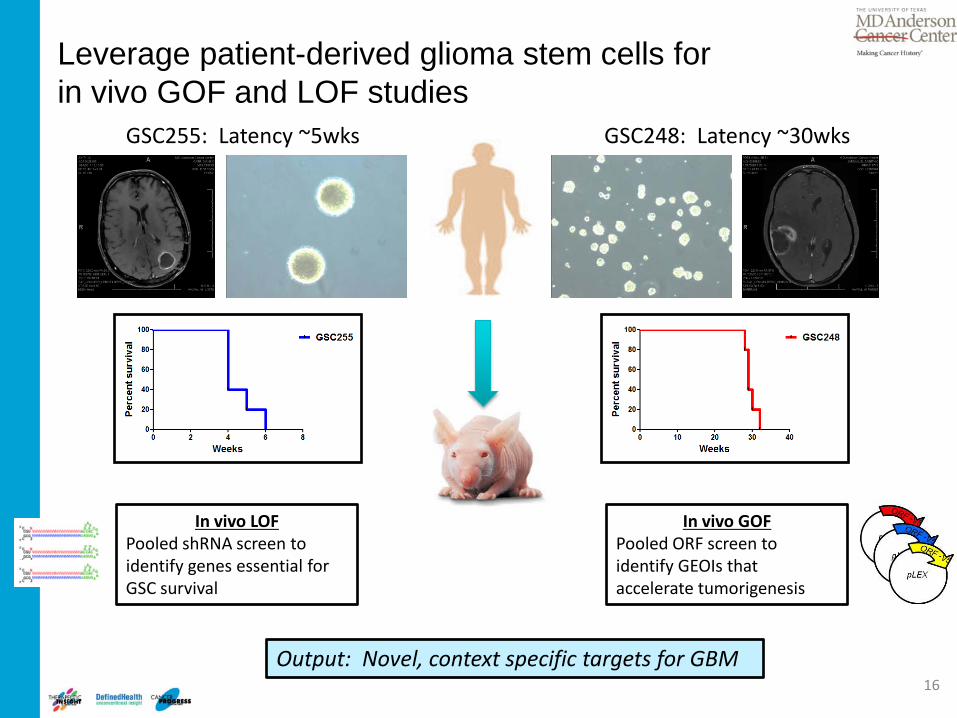
Leverage patient-derived glioma stem cells for in vivo GOF and LOF studies
16
GSC255: Latency ~5wks GSC248: Latency ~30wks
In vivo LOF Pooled shRNA screen to identify genes essential for GSC survival
In vivo GOF Pooled ORF screen to identify GEOIs that accelerate tumorigenesis
Output: Novel, context specific targets for GBM
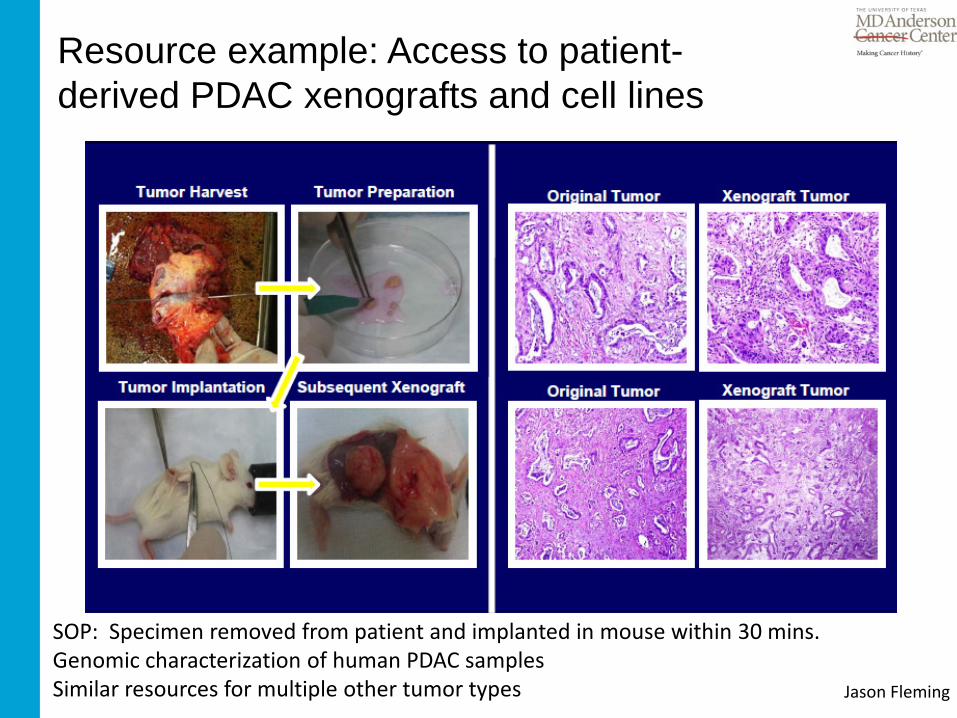
Resource example: Access to patient-derived PDAC xenografts and cell lines
SOP: Specimen removed from patient and implanted in mouse within 30 mins. Genomic characterization of human PDAC samples Similar resources for multiple other tumor types Jason Fleming
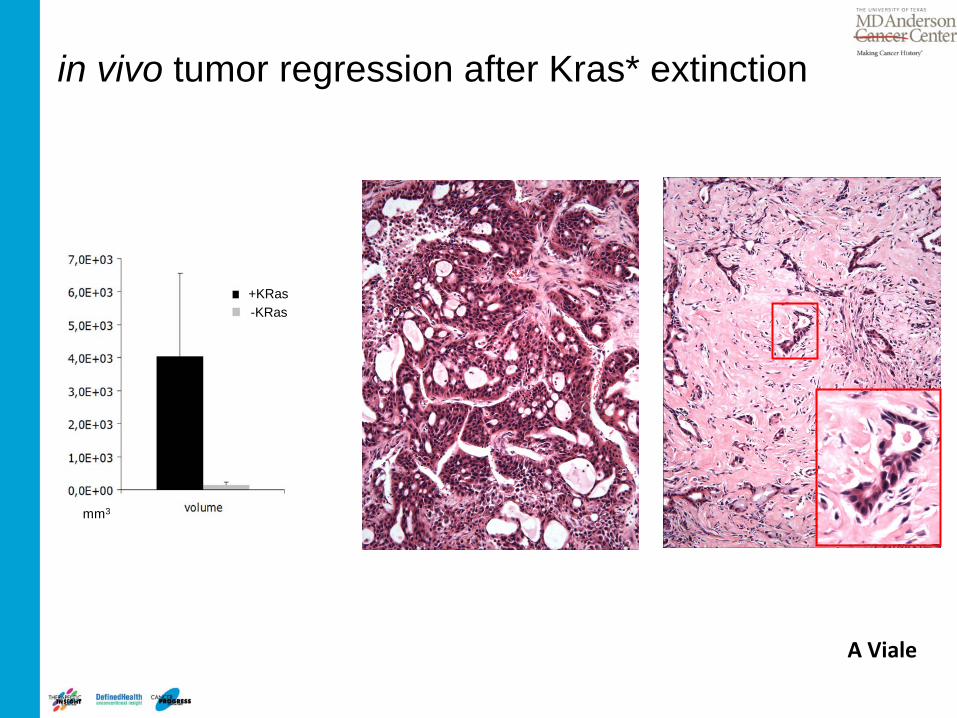
After 2 weeks
mm3
+KRas -KRas
KRas* expressing Tumor
EE 20X EE 20X
Tumor after Kras* extinction
in vivo tumor regression after Kras* extinction
A Viale

Ald+
CD133
CD133
+KR
as*
-KR
as* A
ld+
Tumor cells surviving KRas* extinction are all triple positive
IHC
40X αCD44 αCD133
Remaining tumor cells express stem cell markers
A Viale

αBrdU αCD44 20X
BrdU incorporation 48hs after KRas* reactivation
Upon KRas*re-expression residual cells enter massively into cell cycle and tumors relapse
A Viale
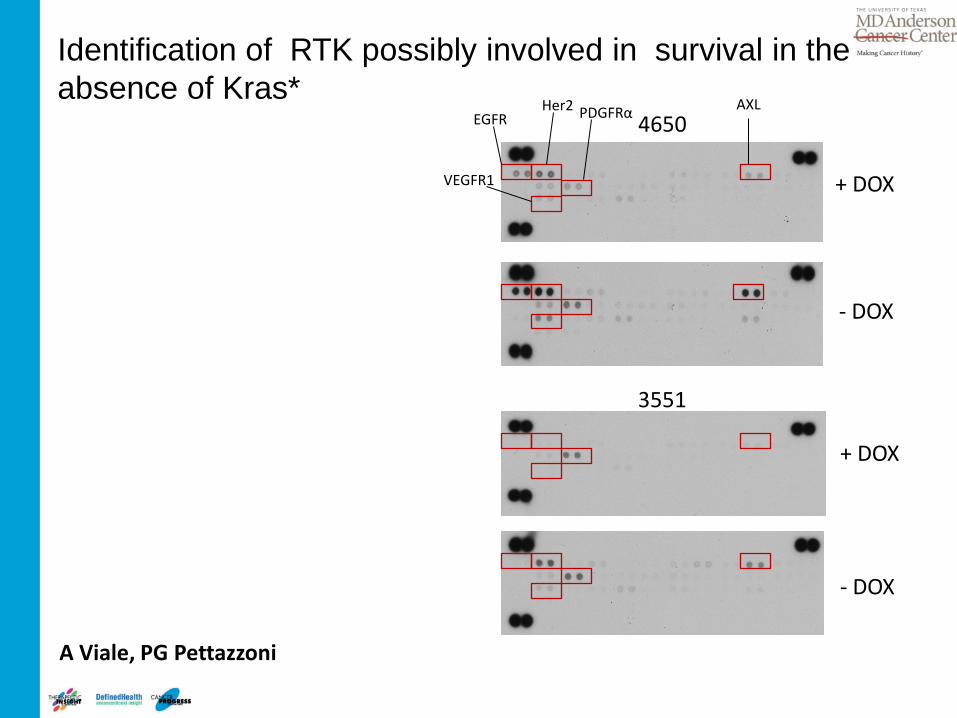
- DOX
- DOX
+ DOX
+ DOX
Her2 AXL EGFR 4650
3551
PDGFRα
VEGFR1
A Viale, PG Pettazzoni
Identification of RTK possibly involved in survival in the absence of Kras*
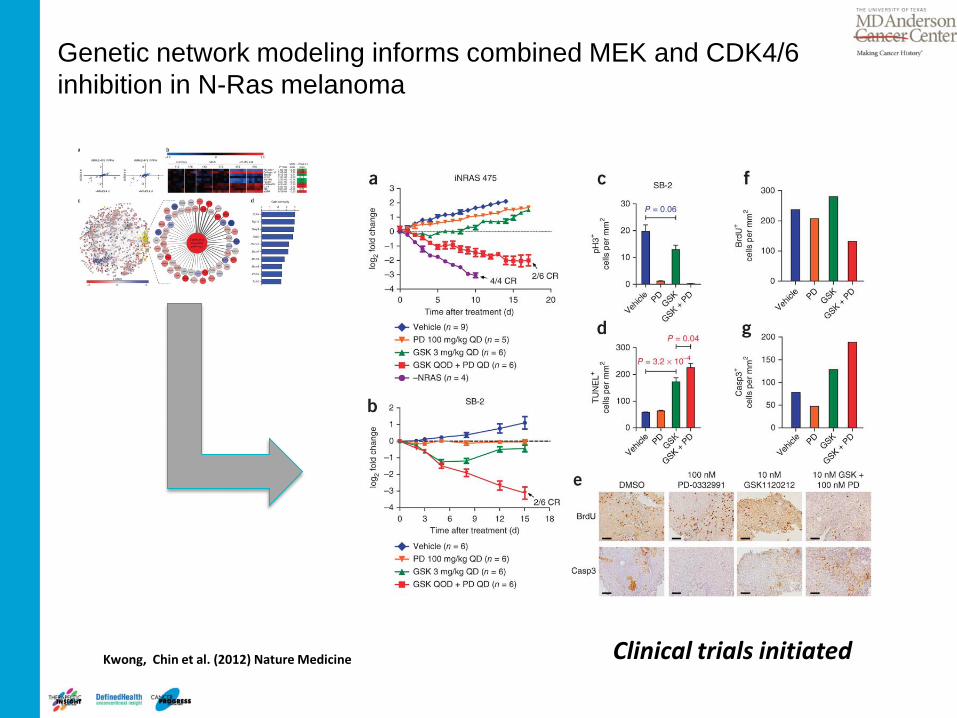
Genetic network modeling informs combined MEK and CDK4/6 inhibition in N-Ras melanoma
Kwong, Chin et al. (2012) Nature Medicine Clinical trials initiated

Barriers to overall progress in cancer treatment
• Limited insights into factors driving cancer • Elemental knowledge of the cancer genome • Poor understanding of the target’s “biology”
– In what context (genetic, micro-environmental, host and macro-environmental) is the target rate-limiting?
• Lack of insight on appropriate combinations – Tumor will find a way to bypass a single-point intervention – Co-extinction is required to shut down a complex highly-redundant
network • Challenged cancer drug development ecosystem
23

Make a deal before it’s too late!
Phase III Phase II Phase I IND Clinical Candidate
Drug discovery Target
Academia > Biotech Biotech > Pharma Pharma Research > Pharma Development Start company > Sell Company VCs > IPOs

Oncology Drug Development: gap between Academy and Industry
25
Academia Industry
Culture
Creativity
Personal Eminence
Perseverance
Risky projects, long term commitment
Publication driven culture
Culture
Focus
Team work
Flexibility
Risk mitigation, quick Go-NoGo decision
Product & patent driven culture
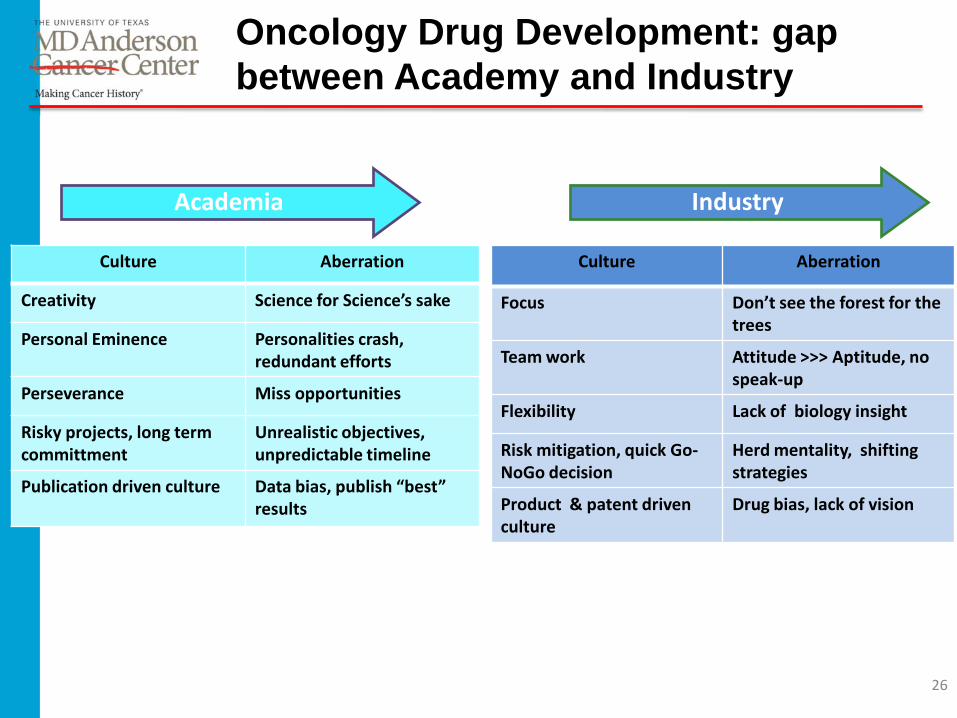
Oncology Drug Development: gap between Academy and Industry
26
Academia Industry
Culture Aberration
Creativity Science for Science’s sake
Personal Eminence Personalities crash, redundant efforts
Perseverance Miss opportunities
Risky projects, long term committment
Unrealistic objectives, unpredictable timeline
Publication driven culture Data bias, publish “best” results
Culture Aberration
Focus Don’t see the forest for the trees
Team work Attitude >>> Aptitude, no speak-up
Flexibility Lack of biology insight
Risk mitigation, quick Go-NoGo decision
Herd mentality, shifting strategies
Product & patent driven culture
Drug bias, lack of vision

Oncology Drug Development: gap between Academy and Industry
27
Academia Industry
Physiology
Creativity
Personal Eminence
Perseverance
Risky projects, long term committment
Publication driven culture
Physiology
Focus
Team work
Flexibility
Risk mitigation, quick Go-NoGo decision
Product & patent driven culture
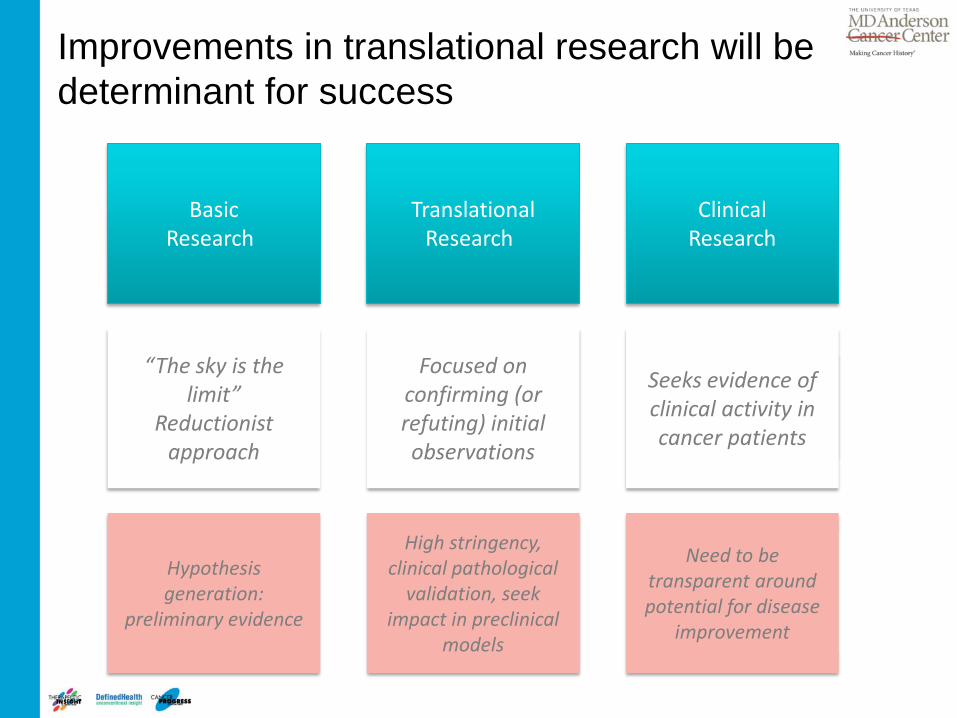
Improvements in translational research will be determinant for success
Basic Research
“The sky is the limit”
Reductionist approach
Hypothesis generation:
preliminary evidence
Translational Research
Focused on confirming (or refuting) initial observations
High stringency, clinical pathological
validation, seek impact in preclinical
models
Clinical Research
Seeks evidence of clinical activity in cancer patients
Need to be transparent around potential for disease
improvement
Cytotoxic vs. targeted agents – both validated therapies – different paradigms
Conventional cytotoxic agent Targeted agents
Proven modality: e. g. childhood ALL, testicular cancer
Proven curative modality: e. g. CML,
Undefined molecular target in most cases
Primary target defined
Broad anti-proliferative activity Anti-tumor activity limited to specific genetic context
DNA damage, e.g. alkylating and intercalating agents
No evidence of DNA damage or other “permanent” damage
Mutagenic in in vitro and in vivo tests No evidence of mutagenic activity
Narrow therapeutic window Higher therapeutic window
Testing in healthy volunteers considered unethical
Testing in healthy volunteers possible
Administer at maximum-tolerated dose Administer at biologically effective dose

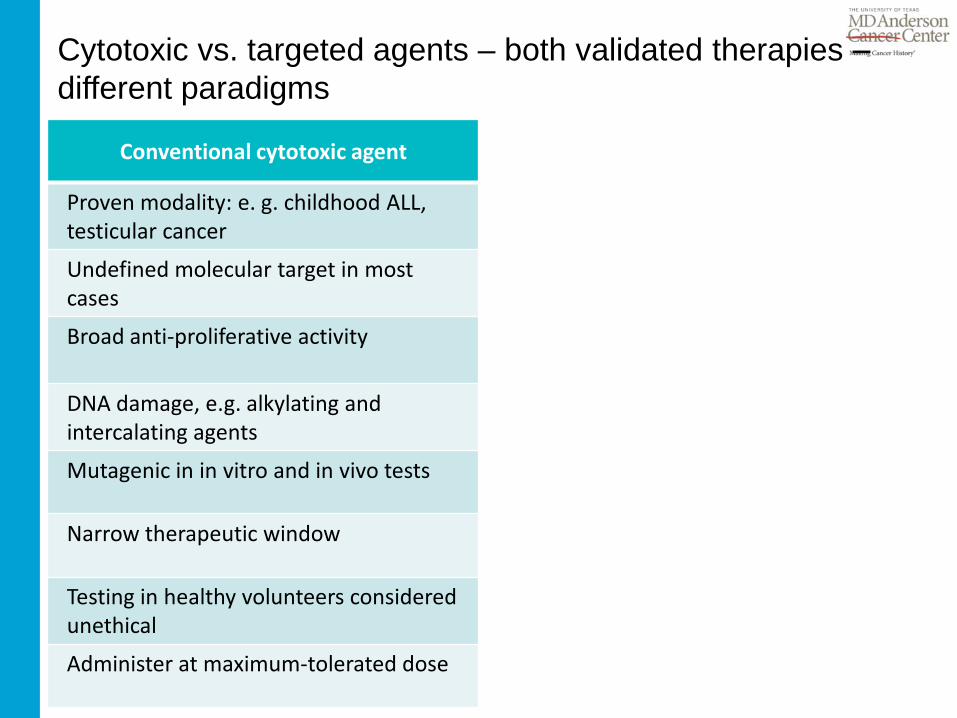
Cytotoxic vs. targeted agents – both validated therapies – different paradigms
Conventional cytotoxic agent Targeted agents
Proven modality: e. g. childhood ALL, testicular cancer
Proven modality: e. g. CML, BRAFm melanoma, EGFRm NSCLC
Undefined molecular target Primary target defined
Broad anti-proliferative activity Anti-tumor activity limited to specific genetic context
DNA damage, e.g. alkylating and intercalating agents
No evidence of DNA damage or other “permanent” damage
Mutagenic in in vitro and in vivo tests No evidence of mutagenic activity
Narrow therapeutic window Higher therapeutic window
Testing in healthy volunteers considered unethical
Testing in healthy volunteers possible
Administer at maximum-tolerated dose Administer at biologically effective dose
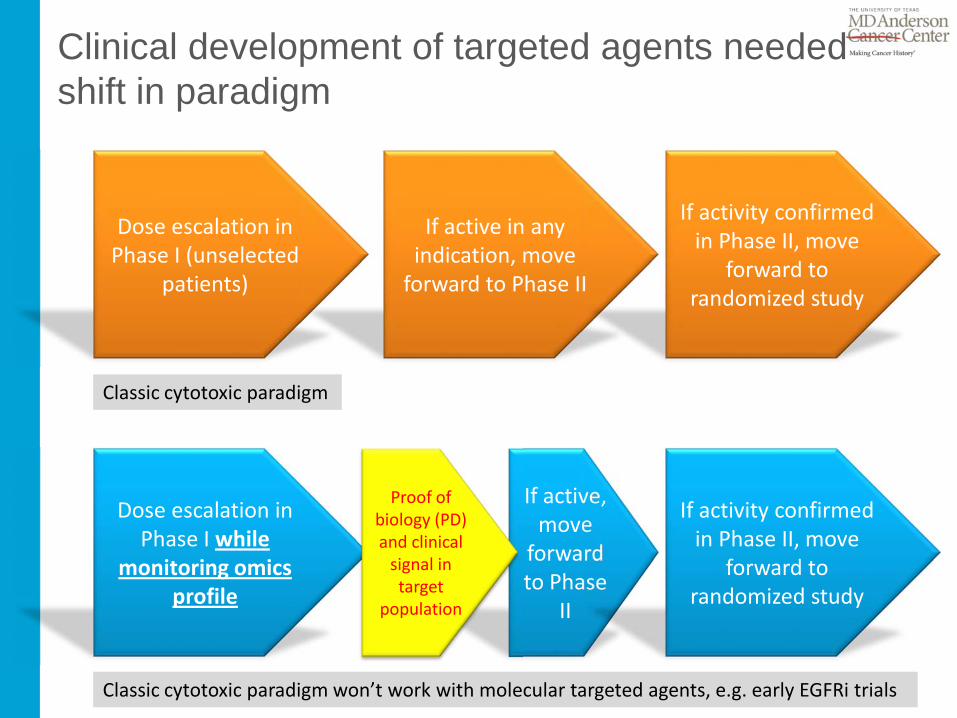
Clinical development of targeted agents needed shift in paradigm
Dose escalation in Phase I (unselected
patients)
If active in any indication, move
forward to Phase II
If activity confirmed in Phase II, move
forward to randomized study
Classic cytotoxic paradigm
Dose escalation in Phase I while
monitoring omics profile
If active, move
forward to Phase
II
If activity confirmed in Phase II, move
forward to randomized study
Classic cytotoxic paradigm won’t work with molecular targeted agents, e.g. early EGFRi trials
Proof of biology (PD) and clinical
signal in target
population

Where will improvements come from
• Eliminate “cytotoxic” development culture when dealing with targeted therapies • Should be able to utilize healthy volunteers for PK and PD analysis in early Phase I • Avoid subjecting patients to useless treatments • Access to early stage patients rather than late stage disease • Mandatory patient biopsies
Pharmacokinetics, biodistribution, safety adequate for testing in
healthy volunteers
High quality agents (small molecules,
antibodies, vaccines, other)
Tumor genetic fingerprinting at time of
treatment Patient stratification Tailored combination
strategies
Improved understanding of
disease state at time of treatment (molecular and
physiopathology)
Early proof of biology and activity response
read-out (imaging, others)
Allows trial interruption and
potential to evaluate alternative

The MD Anderson Moon Shot Initiative
“By applying today’s knowledge and game-changing technologies, MD Anderson’s Moon Shots Program will dramatically accelerate improved survival in the next five to ten years, beyond the 1% to 2% annual declines in cancer mortality that we’ve seen in the past decade. The expertise and team science behind our selected cancer moon shots also will lay the foundation for ultimate cure of these diseases in the years to follow.” Ronald DePinho, M.D., MD Anderson president

Cancer Prevention and Early Detection
Prevention Early Detection Treatment
NO
W
Prevention Early Detection Treatment
FUTU
RE

How to drive a comprehensive plan of attack
– Prevention – Early detection: imaging, tissue markers – Diagnostics: integrate genomic profiling into clinical practice – Drug discovery expertise
• Internal effort justification: need to have internal expertise to better integrate with the external world – importance of scouting and triaging
• Small molecules • Biologics and immunotherapeutics
– Clinical development • Evaluating therapies of true potential
– Early access to new, high quality treatments • Streamlining regulatory reviews and operations • Imaging and other modalities to monitor response • Immuno-monitoring

The Initial Moon Shots at MD Anderson
Acute myeloid leukemia and myelodysplastic syndrome
Breast and ovarian cancers – two cancers with a shared genetic pathway
Chronic lymphocytic leukemia
Lung cancer
Melanoma
Prostate cancer
Current state of scientific knowledge Strength and breadth of the MD Anderson team Potential for measurable near-term success Potential for cure in long term
37
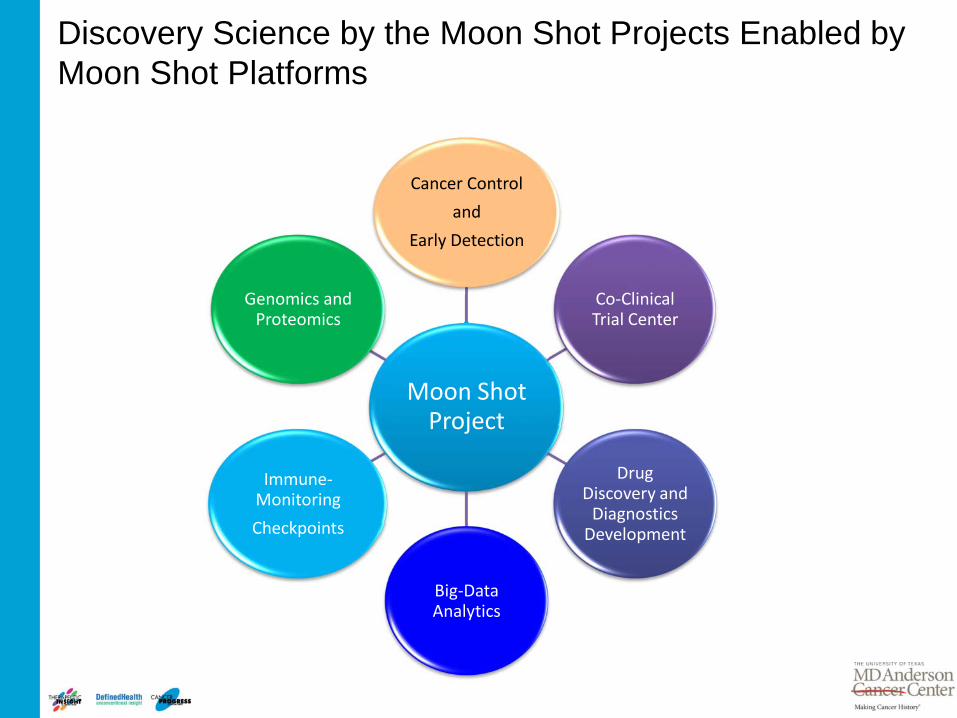
Moon Shot Project
Cancer Control and
Early Detection
Genomics and Proteomics
Immune-Monitoring Checkpoints
Big-Data Analytics
Drug Discovery and
Diagnostics Development
Co-Clinical Trial Center
Discovery Science by the Moon Shot Projects Enabled by Moon Shot Platforms

Institute for Applied Cancer Science
• Singular focus on the rapid discovery of new drugs that are clinically relevant: small molecules and biotherapeutics
• Operational since January 2012: currently 60 scientists; will grow to 75 at full capacity
• More than 200 years’ collective industry drug discovery experience
• Thorough evaluation of more than 50 potential programs: 3 inaugural programs and several in exploratory pipeline
– Disease relevance – Ease of therapeutic attack – Defined clinical trial path
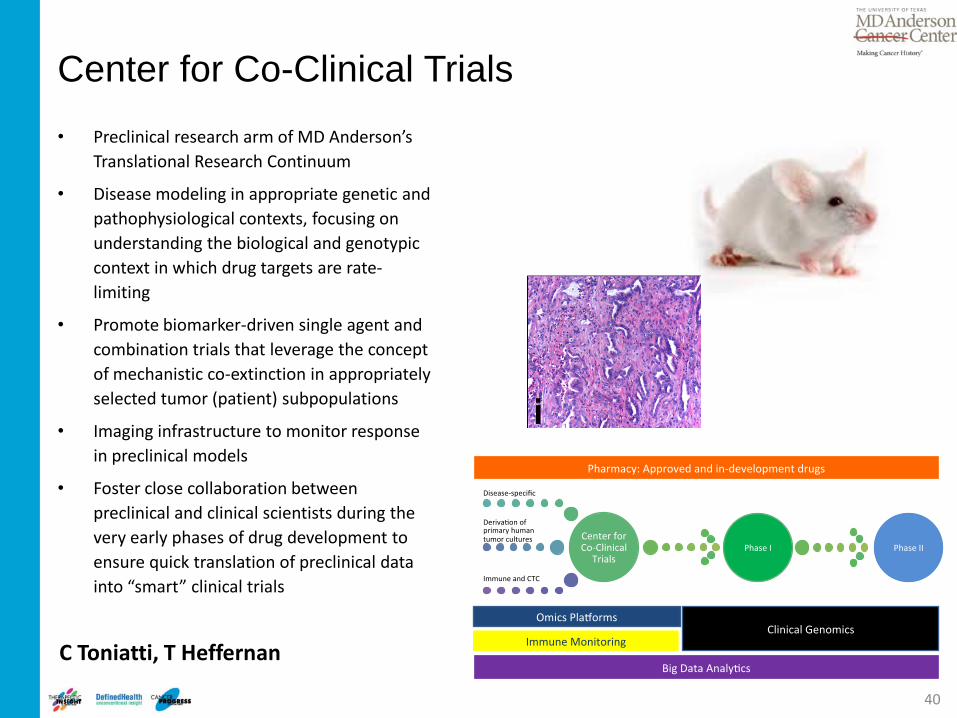
Center for Co-Clinical Trials • Preclinical research arm of MD Anderson’s
Translational Research Continuum
• Disease modeling in appropriate genetic and pathophysiological contexts, focusing on understanding the biological and genotypic context in which drug targets are rate-limiting
• Promote biomarker-driven single agent and combination trials that leverage the concept of mechanistic co-extinction in appropriately selected tumor (patient) subpopulations
• Imaging infrastructure to monitor response in preclinical models
• Foster close collaboration between preclinical and clinical scientists during the very early phases of drug development to ensure quick translation of preclinical data into “smart” clinical trials
40
C Toniatti, T Heffernan
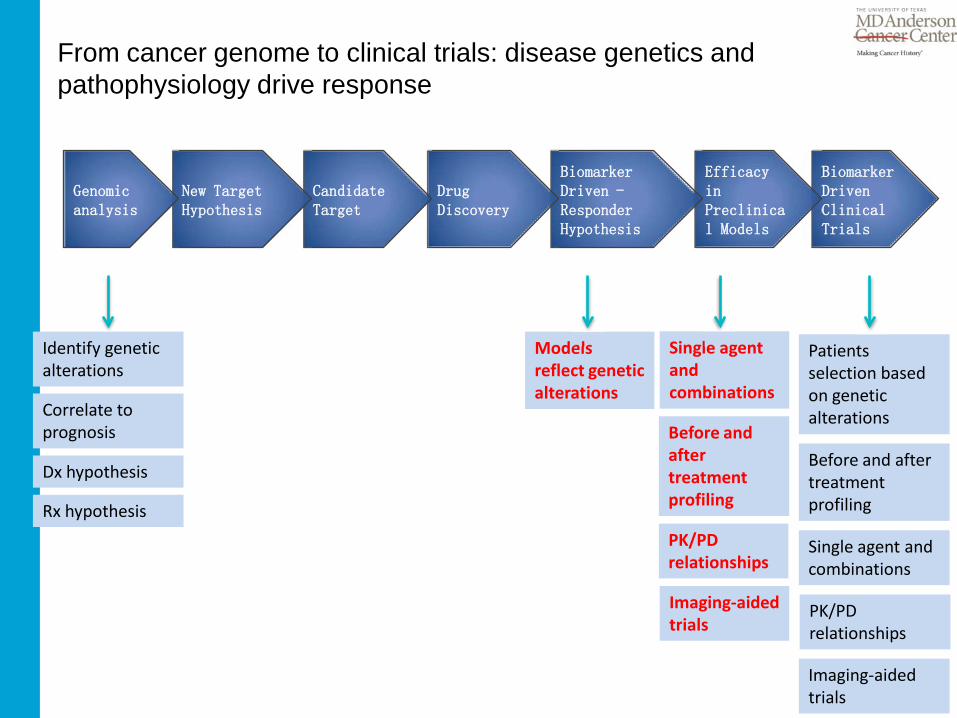
From cancer genome to clinical trials: disease genetics and pathophysiology drive response
Biomarker Driven Clinical Trials
Identify genetic alterations
Correlate to prognosis
Dx hypothesis
Rx hypothesis
Models reflect genetic alterations
Before and after treatment profiling
Patients selection based on genetic alterations
Single agent and combinations
PK/PD relationships
Imaging-aided trials
Single agent and combinations
PK/PD relationships
Imaging-aided trials
Before and after treatment profiling
Efficacy in Preclinical Models
Biomarker Driven -Responder Hypothesis
Drug Discovery
Candidate Target
New Target Hypothesis
Genomic analysis

Clinical information
and data
Treatment Decisions
& Response
Assessment
Patient Consent, Biospecimen Collection, QC, Banking , Biomolecule Processing
Omics & Research Data Big Data Platform
TCGA/ICGC Pubmed Patent db Social media Other
Longitudinal Patient Data Warehouse
Massive Data Analytics Massive Data Analytics
Watson Solutions
Research & Operations
Adaptive Learning in Cancer Care
Lynda Chin, Andy Futreal

Develop minimal Assay funnel
POC Cmpds (Selectivity)
Stringent/broad Loss of function studies
Comprehensive Target Validation
Context-specific Gain of function studies
Go/No-Go
Cmpd Efficacy Study in vivo
Lead Optimization
Clinical pathological validation
Prec
linic
al C
andi
date
Basic
and
tran
slatio
nal r
esea
rch
in a
cade
mia
Clinical Path
Human Relevance; clinical path hypothesis
Pharmacological Target Validation
Biomarker discovery Biomarker dev
Relevant MOA to define biomarkers for target engagement; pathway modulation; efficacy, etc.
Assays in human
Parallel and integrated target and drug discovery biology

Cancer Biology
Drug Discovery
Clinical Research
Drug Discovery Project at IACS – Metabolic target
44
nM cellular activity 3 Patents filed 08/12 Multiple chemotypes In vivo PoC in 3 models
On-track to select clinical candidate in 2H13
Treatment Period
Working with MDACC physician scientists to translate findings into clinical impact
Explored opportunities with eleven disease centers
Robust responses in patient samples for specific indication
Establishing PK/PD/Efficacy relationship
Potential phase 1b population identified
Comprehensive understanding of MOA
Fully enabled research operating plan
Identified tumors dependent on pathway
Exploring additional synthetic lethality opportunities

Right target, right drug, right patients
Selection of targets
• Unbiased target selection based on disease relevance
Quality of compounds identified
• Critical assessment
• Wait for right compound to be developed
• Implement industry standard stage gate - optimized for:
• Potency and cellular activity
• lack of off-target activity/ancillary pharmacology
• benign safety/toxicity profile
• pharmacokinetics, tissue distribution, efflux
• understand dosing regimes and exposure required for maximal efficacy
• appropriate physicochemical characteristics and formulation

46
Rapalog
mTOR ATP competitive Inhibitors
Protein translation is critical for malignant transformation
V Giuliani, T Heffernan

Protein synthesis is required for PI3K-AKT dependent transformation
47
Increased cap-dependent translation is required for AKT-induced lymphoma
Hsieh et al. Cancer Cell 2010
V Giuliani, T Heffernan

EIF4E knockdown inhibits growth in vitro and in vivo
48
eIF4E KD induces apoptosis IV dosing of eIF4E ASO inhibits xenograft growth
KD of eIF4E expression with antisense oligos inhibits expression of eIF4E-regulated proteins
Graff et al. JCI 2007
V Giuliani, T Heffernan
49
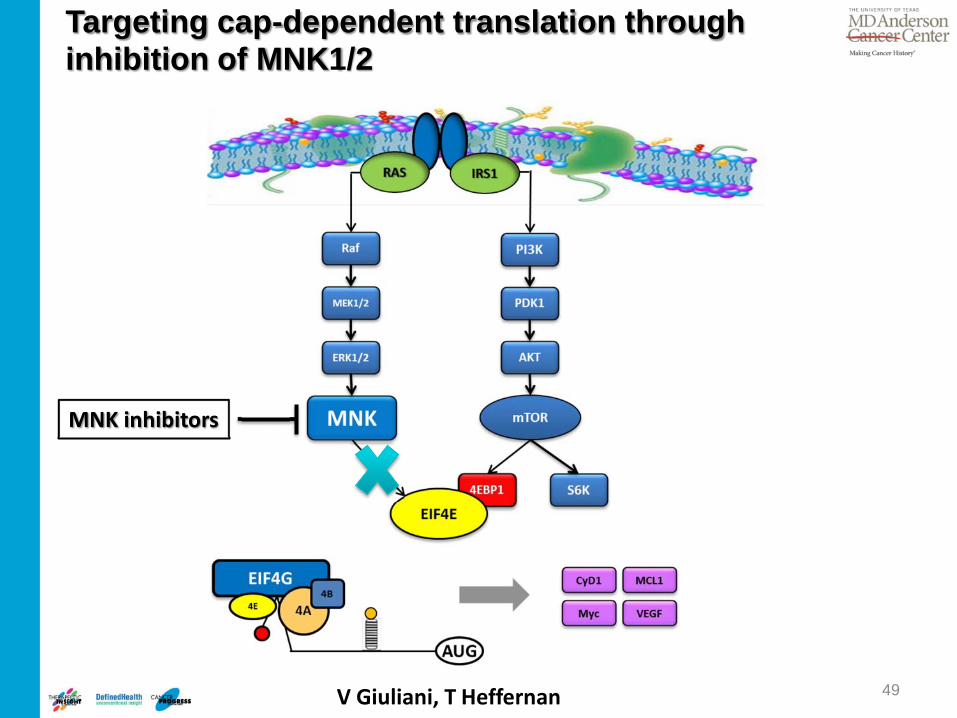
Targeting cap-dependent translation through inhibition of MNK1/2
MNK inhibitors
V Giuliani, T Heffernan
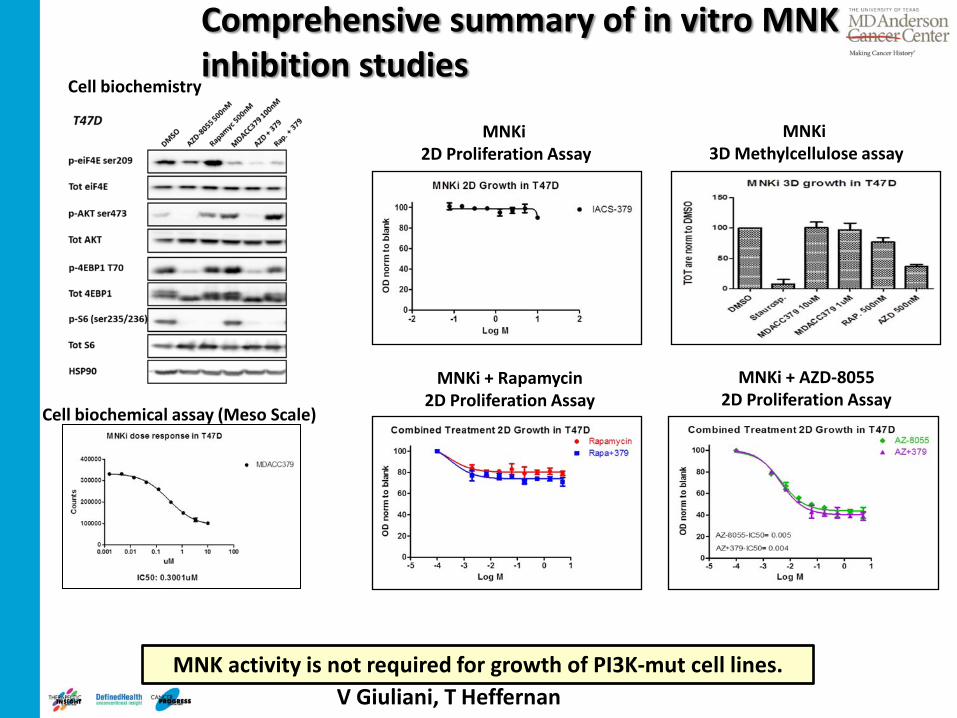
Comprehensive summary of in vitro MNK inhibition studies
MNK activity is not required for growth of PI3K-mut cell lines.
MNKi + Rapamycin 2D Proliferation Assay
MNKi + AZD-8055 2D Proliferation Assay
MNKi 3D Methylcellulose assay
MNKi 2D Proliferation Assay
Cell biochemical assay (Meso Scale)
Cell biochemistry
V Giuliani, T Heffernan

Proprietary and Confidential 51
pHAGE-dsRED-IRES-GFP (in house)
MNK inhibition does not reduce protein translation
CAP Dependent
CAP Independent
DMSO
MNK inhibitor
• MNK inhibition failed to decrease CAP-dependent translation
Analysis by Harmony (blue Hoechst; Green GFP; Red dsRED)
24h
MASCIA

From disconnected sequential process to fully integrated approach: only at MD Anderson!
Cancer Biology
Drug Discovery
Clinical Research
Clinical Trials
Drug Discovery
Cancer Biology

Providing access to technology vs. project financing?
European Lead Factory opens for business
Who is going to lead and integrate projects?
Not convinced this is the best option

Highlights The Karyopharm Story – born October 2010!
• Karyopharm is the leader in the science and chemistry of SINE – Selective Inhibitors of Nuclear Export – for cancer, inflammation, viral, and other proliferative disorders
• A family of closely related, oral SINEs show potent and selective anti-cancer
and anti-inflammatory activities in multiple preclinical models • KPT-330 oral SINE Phase 1 human clinical trials in solid tumors and
hematologic malignancies initiated in June 2012 – proceeding well
• KPT-335 oral SINE in Phase 1 dogs with non-Hodgkin’s lymphoma with clear activity and good tolerability – pivotal study start November 2012
• KPT-355 oral SINE for inflammatory disorders and viral infections in
preclinical development with potential for 2013 IND with partnership

Sharon Shacham, PhD, MBA – Founder, Chief Scientific Officer, Head of R&D, SAB Co-Chairman Former Sr. Vice President of Drug Development, Epix Pharmaceuticals Founding scientist, Predix Pharmaceuticals Led discovery and development from target identification through development of NCEs across multiple therapeutic areas to proof of concept studies in human (PhIIb)
Michael Kauffman, MD, PhD – Co-Founder, Chief Executive Officer and Board Member Former Chief Medical Officer, Onyx Pharmaceuticals Inc (ONXX), Proteolix Inc. Former VP, Clinical (Millenium): Led clinical development team leading to accelerated approval of Velcade® Former CEO, Epix Pharmaceuticals and Predix Pharmaceuticals - raising >$215M in 5 years Director, Zalicus (ZLCS) and former Chairman, Proteolix Inc.
Ron DePinho, M.D. – Co-Founder and Oncology Advisor President, MD Anderson Cancer Center Member, National Academy of Sciences and Institute of Medicine Former Director, Belfer Institute for Applied Cancer Science at the Dana-Farber Cancer Institute Founder & Director: Aveo Pharmaceuticals, Eden Therapeutics, and Metamark Genetics, Inc.
Mansoor Raza Mirza, M.D. – Board Member and Clinical Oncology Advisor Chief Oncologist at the Department of Oncology, Rigshospitalet, Copenhagen University Hospital National representative in the European Network of Gynecologic Oncology Trials (ENGOT) and in the Gynecologic Cancer Inter-Group (GCIG) Director: Metamark Genetics, Inc. Giulio Draetta, MD PhD – Co-Founder, Chairman of SAB and Oncology Advisor Director, Applied Cancer Genetics, MD Anderson Cancer Center Former Chief Research Business Development Officer, Dana Farber Cancer Institute; Formerly head of oncology drug discovery at Pharmacia and Merck. Scientific Advisor: Epitherapeutics, Daiichi-Sankyo, Genzyme. Former Advisor: Mitotix, Inc.
Leadership Team People

Nuclear Export Machinery

KPT-330 SINE Forces Nuclear Retention and Increases Levels of Many TSPs
DMSO
KPT- 330
p53 pRB PP2A p21 IκB p27
KPT-330 on U2OS osteosarcoma for 4-24 hours @ 1 µM (~400 ng/mL)
Forced Nuclear Retention & Activation by Blocking Nuclear Export
CRM1 Inhibition

Solid Tumor Patient 1 (3 mg/m2): p53
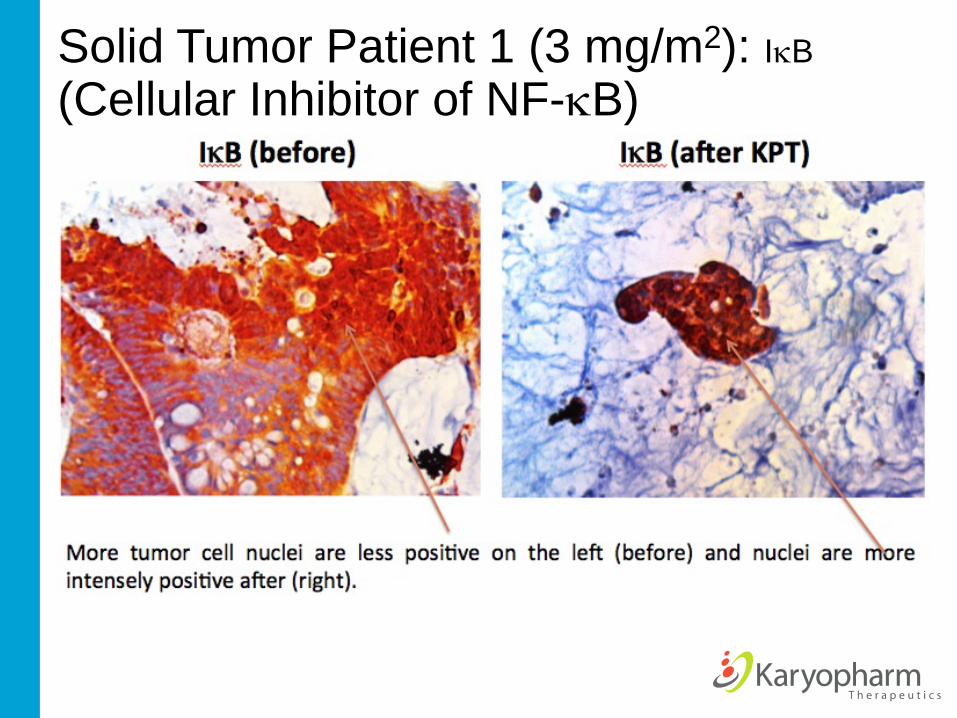
Solid Tumor Patient 1 (3 mg/m2): IκB (Cellular Inhibitor of NF-κB)

Summary Summary
• KPT-SINE, CRM1 Antagonists, irreversibly block the nuclear export of multiple tumor suppressor & growth regulatory proteins countering multiple oncogenic signals across a variety of tumor types
• SINE show selective tumoricidal toxicity
– Potent killing of CLL, lymphoma, MM, acute leukemia, pancreatic, HCC, and other malignant cells
– Minimal effects on normal cells which have an intact genome
• SINE are well tolerated in vivo, with oral bioavailability
– Main toxicity is weight loss (0-15%) at doses highly active across multiple xenograft experiments in mice and in dogs; mitigated with high caloric foods; No significant effects on clinical chemistry or hematologic parameters (except reticulocyte counts) at anti-cancer doses in several species
• KPT-335 oral shows clear activity in dogs with spontaneous NHL at well tolerated doses with planned FDA CVM approval in 2H 2014
• KTP-330 oral up to 12 mg/m2 well tolerated to date with clear biomarker effects, stable long-term disease control in both solid and heme malignancies, nuclear localization of tumor suppressor proteins in human K-ras colon cancer; dose escalation progressing well

Institute for Applied Cancer Science: Building team science to conquer cancer!
61

Keynote Address
Giulio Draetta, PhD, MD, Professor, Genomic Medicine Director, Institute for Applied Cancer Science, MD Anderson Cancer Center