
Git3
62
1 Small Intestine and Large Intestine Function & Motility
Transcript of Git3

1
Small Intestine and Large Intestine Function & Motility

SMALL INTESTINE
Is part of GIT extending from pyloric sphincter of stomach to ileocecal valve.
Major site for digestion & absorption of carbohydrates, proteins & fats.
Length around 4-5 mts.3 parts – Duodenum, jejunum & ileum.Secretion from small intestine called as succus
entericus.

Mucous membrane of SI is covered by Intestinal villi of height 1 mm. The villi are lined by columnar cells called enterocytes.
Each enterocyte gives hair like projection called microvilli, increases surface area for absorption.
Simple tubular glands lined by columnar cells in intestine called Crypts of Lieberkuhn.
These columnar cells show active mitosis.Brunner’s glands seen majorly in duodenum
region.
Crypts of Lieberkuhn – secrete the intestinal juice
1. Enterocytes : digestive Enzymes2. Goblet cell : Mucus3. Paneth cell : Glycoproteins , Immunoglobulin,
Lysozymes (defensins)4. Enterochromaffin cells : Seretonin , 5HT
Endocrine cells: GI hormones, e.g. Secretin, CCK, VIP, GIP

Volume 1800ml/day Alkaline, 8.3 pHisotonic with plasma S.G : 1010composed of water (about 98%)Solids
inorganic salts Cations - K+, Na+, Ca++ Anions - Cl-, HCO3-
jejunal secretions : Cl-, K+ is ileal secretions : Na+, Ca++
SUCCUS ENTERICUS

Organic constituents: ProteinsMucinAlbuminImmunoglobulin A numerous shed epithelial cells of the intestinal
mucous membraneDigestive enzymes - present in the shed
epithelial cells & little role in digestion

Functions of succus entericus
1) Digestive functionBy Proteolytic enzymesBy Amylolytic enzymes
By Lipolytic enzymes
.
2). Protective function. Mucus protects lining of small intestine.Paneth cells of intestinal glands secrete defensins .
3) Enterokinase present in intestinal juice activates trypsinogen into trypsin

Intestinal Enzymes:
I. Activating Enzyme
Enteropeptidase or enterokinase is a brush border enzyme of the duodenum and jejunum.
released in response to secretin, CCK or bile acids
converts inactive trypsinogen into active trypsin.

II. Digestive Enzymes
(a) Proteolytic Enzymes. Break down polypeptide into aminoacids
CarboxypeptidasesEndopeptidasesDipeptidases
(b) Enzymes Acting on Nucleic AcidsNuclease. Nucleotidase Nucleosidase
Fat Splitting (Lipolytic) Enzyme: Intestinal lipase present in the brush border of epithelial cell
its action is much weaker than that of pancreatic lipase.
Enzymes Acting on Carbohydrates: important amylolytic enzymes are the
disaccharidases Maltase Sucrase Lactase. Isomaltase Trehlase Amylase
Regulation of Small Intestinal Secretion Local ; Neural ; Hormonal ;
Local Stimuli: Presence of chyme in the intestine increases
intestinal secretion. Distention of intestine stimulate secretion,
probably by local nervous reflexes.

2. Extrinsic Nerves- Vagal stimulation - increases secretion of
glands Sympathetic stimulation inhibits secretion.
Inhibition helps to prevent loss of fluid & electrolyte help absorptive process

3. Hormones:
GIT hormones: VIP, GIP & Gastrin – stimulates intestinal secretion
Acetylcholine – increases & noradrenaline inhibits secretion

14
Small intestinal movements
FunctionMixing AbsorptionPropulsion
Types: BER MMC
Mixing - segmentation
- pendular movement
propulsive -peristalsis

15
Types of movements
Segmentation contractionsRhythmic contractions Intestine is divided into segments of 1-2cmsCircular muscle contractionEach contraction lasts for 1 – 3 secondFunction
• mixing
• absorption

16
Segmentation
CommonestAlternating
contractionMixing
17
Pendular movementsSome times seen Simple constrictions of the intestinal wall
which moves up & down for short distancesCauses to & fro movements of chymeAids mixing & exposure to greater area of
mucosa
Tonic contractionsProlonged contraction of segments of
intestineOne segment – isolated from another

18
Peristalsis
Distended bowel, causes contraction behind the stimulus (proximal) & relaxation in front (distal)
Velocity of peristaltic wave – 0.5 – 2.0 cms/secMovement of chyme – 1 cm/minDepends on the integrity of myentric plexus.

19
Acetylcholine & substance P - cause contraction behind stimulus
VIP & Nitric oxide - cause relaxation in front of stimulus
LAW OF GUT.

20
Peristalsis
Function Rapid propulsion
of intestinal content
‘clearing’

21
Peristaltic rush – strong / rapid peristaltic waves –
travel long distance & quickly sweep the intestinal
content into colon e.g. intestinal irritation
(catharitics) or excess distension
Antiperistalsis - vomiting
Peristalsis
For peristalsis,intact nerve supply has to be there.
Do not occur in denervated intestine.The extrinsic hormones also influence. As parasympathetic system- stimulate &
sympathetic nerves- inhibit the peristalsis. Gastrin, CCK-PZ, serotonin, etc ↑, whereas
secretin,etc ↓ peristalsis. But the presence of food in intestine is an
important stimulus.

23
Movement of intestinal villi
Fasting – villi ~ inactive & lie flatContact with food
To & fro Lashing or swaying movementsShorten & elongate alternatelyStirring of fluids – help in absorption, expulsion of
lymph from lactealsDependent on intact submucosal plexusStimulation
Vagal – increases movementsSympathetic – pale & motionless

24
Regulation of intestinal motility
Coordinated & regulated by – Local , Neural & Hormonal mechanisms
Segmental & pendular movements – myogenic , occurs in denervated loop.
Peristalsis is an intrinsic neural reflex
25
Extrinsic influence & regulation Parasympathetic - Vagus – increases – tone & intestinal
motilitySympathetic – inhibits
Humoral factors - Motility & Tone
Increased by Decreased byAcetylcholine NoradrenalinSerotonin SecretinMotilin Glucagon CCK VIPGastrin NOInsulinHistamineSubstance P

Applied physiology1) Malabsorption syndrome:
Causes- a} Resection of small intestine
b} Gastro-colic fistula
c} Sprue
d} Coeliac disease
Sprue : a intestinal disorder multiple causes leading to damaged intestinal mucosa.

3) Coeliac disease: characterised by congenital absence of enzyme gluten hydrolase in intestinal mucosal cells, results in formation of a toxic polypeptide ‘Gliadin’ from Gluten (protein in barley,rye,wheat,etc).
Gliadin causes intestinal T cells to produce an inflammatory allergic response that flattens & disrupts the formation of microvilli.
27

clinical features : Indigestion, diarrhoea, anorexia & weight loss,
abdominal cramps Nutritional defieciancy ,macrocytic anemia.Vit B, Folic acid and Vit k defieciency. Osteomalcia ,
Steatorrhea .etc.
28

Adynamic ileus: (Paralytic ileus)
Intestines are traumatised, smooth muscles are directly inhibited.→ motility↓
Peritoneal irritation.—reflex inhibition due to ↑ noradrenergic dischrage.
Intestines will be irregularly distended by pockets of gas and fluid.
Treatment :obstruction relieved by aspiration of gas and fluid by Ryle’s tube till peristalsis returns.
29

30
Large Intestine

31
Functions of large intestine
Secretions - Goblet cells secrete mucus – protective
lubricant layer. Helps in stool formation. (adherent medium for holding fecal matter together). Protects wall from bacterial activity.
- Secretion of bicarbonate to fight acidity caused in stool due to bacterial action.
- Secretion of potassium. Digestion none except by bacteria
32
Functions of large intestine (contd.)Absorption water & electrolytes, sodium & chlorides are absorbed.
Bile salts, certain products of bacterial action (indole) also absorbed.
90% fluid removed , 1000-2000ml of chyme converted to 200-250ml of semisolid feaces
ExcretionHeavy metals, metabolites, drugs e.g.. Emetine.
Fluids for transfusion purposes & drugs (anesthetics) maybe given through large gut.
Also used to transplant ureters after removal of a pathological urinary bladder.

33
Large Intestine Absorption

34
Bacterial Flora
consist of:Bacteria surviving the small intestine that enter the cecum
and Those entering via the anus
(pathogens,symbionts,commensals )
These bacteria: Colonize the colonFerment indigestible carbohydratesRelease irritating acids and gases (flatus)Synthesize B complex vitamins ,vitamin K,
folic acid ,short chain fatty acid

35
Movements of large intestineColonic transit time
Food enters caecum – 4 hrs after meal
Ileum empty – 8hrs
Caecum & ascending colon empty – 13 to 17 hrs
Distal colon - 18 hrs
Rectum – 24 hrs
Some remnants of meal are present in rectum ~ 72 hrs

36
Types of movement
Similar to SI
Segmentation contraction – present in
proximal region of colon (i.e, ascending &
transverse region)
Haustral contractions or churning in which
colonic wall roll back & forth
Kneading movements - alternate contraction
& relaxation of large segments of colon
37
Pendular type of movement – peristalsis cum
anti peristalsis causing mixing of colonic content
Peristalsis – wave of contraction sweeping down LI
Frequency less than SI

38
Mass movement or mass peristalsis
1-3 times/day
Forceful contractions
Involve contraction of large segment of colon
Propel contents into rectum & induce desire
for defecation
Mass movement can occur after meal
• Gastro colic reflex
• Duodeno colic reflexMediated by ANSMediated by ANS

39
Defecation
A spinal reflex under voluntary control.
Rectum usually (almost) empty (retrograde contractions return content to sigmoid, until there is too much of it)
Just before defecation mass movement fills rectum → ↑ pressure → reflex relaxation of inner sphincter (smooth muscle) via parasympathetic fibers in pelvic nerves & contraction of outer sph. (skeletal muscle controlled intentionally via pudendal nerves)

40
Defecation
Pelvic Nerve
Pudendal Nerve

41
DefecationStretch receptors in rectal wall can adapt - urge
to defecate can temporarily subside if suppressed
Reflex controlled from sacral spinal cord, modulated from higher levels
Voluntary signals stimulate relaxation of the external anal sphincter and defecation occurs

42
Applied aspectConstipation: commonest disorder of large bowel motility
Cause :
Irregular bowel habits
Hypothyroidism
Anal strictures
Colon cancer
Diarrhoea: increase in frequency of passage of stools, due to large bowel irritation
Cause:
Infection
Emotional tension (psychogenic diarrhoea)

43
Adynamic or Paralytic ileus : trauma to intestine cause
inhibition of smooth muscle
Hirschsprung`s disease or aganglionic megacolon :
congenital absence of both myentric & submucous
plexus
Blind loop syndrome –excessive bacterial growth due
to stasis

Digestion of carbohydrates
The different carbohydrates in diet are Polysaccharides like glycogen,amylose,amylopectin,etc
The disaccharides in the diet are sucrose, lactose, starch,etc. , whereas monosaccharides are mostly glucose & fructose.
Other carbohydrates in diet include Alcohol, Lactic acid, pyruvic acid,pectins,dextrins and of course cellulose.
The end products of carbohydrates is monosaccharides.

I. Carbohydrate
Starch amylase Disaccharide (salivary, pancreatic, intestinal) (Maltose, Isomaltose, maltotriose)
+
dietary disaccharide
Sucrose + Lactose
Monosaccharide(Glucose, fructose, galactose)
Intestinal disaccharidases. Maltase, sucrase, lactase
Digestion
In the mouth: The salivary amylase present. In the stomach: The salivary amylase act here for a
longer time. As such less enzymes (weak amylase) present in stomach region.
In the intestine: Along with enzymes in stomach from pancreas like pancreatic amylase & succus entericus enzymes like maltase, sucrase, lactase,dextrinase, trehalase,etc act on the carbohydrates in food to break it down into m.s.
The pancreatic amylase can act both on boiled & unboiled starch but salivary amylase acts on boiled starch only.

Brokendown products (glucose) transported from lumen of S.I. into epithelial cells in the mucus membrane of S.I by means of sodium co-transport.
From epithelial cell, glucose is absorbed into portal vein by facilitated diffusion.
Utilization of carbohydrates occurs mainly by oxidative process in which the carbohydrates are burnt down slowly to release energy. This process is called catabolism.
The part of released energy is utilized by the tissues for the physiological actions & rest of the energy is stored as rich energy phosphate bonds and in the form of proteins, carbohydrates & lipids in the tissues. This process is called anabolism.

Carbohydrates: Hydrolyzed into Monosaccharides
Glucose is transported to cells requiring energy; insulin influences rate of transport

Absorption of CHO

DIGESTION, ABSORPTION AND METABOLISM OF PROTEINS.
Proteins: Food containing high protein are- meat,fish egg & milk and the various proteins in them are collagen, albumin,casein,lactalbumin, vitellin,etc.
Digestion of proteins: (by proteolytic enzymes)
A) Mouth- No protein digestion occurs.
B) Stomach- By pepsin & rennin
C) Small intestine- By pancreatic enzymes like trypsin, chymotrypsin in duodenum & jejunum as well as succus entericus which contains dipeptidases,tripeptidases & aminopeptidases.
The final products of protein digestion are amino acids absorbed from intestine.

II. Proteins & Nucleoproteins
Proteins
Proteases, peptones, large polypeptides
also digest collagen
Smaller peptides & some free a.a.
Amino acids (98% of dietary protein)
(polypeptide chains composed of a.a. bound by peptide linkage)STOMACH
Pepsin
DUODENUM
Pancreatic trypsin & chymotrypsin (endopeptidase),
Carboxypeptidase (exopeptidase)
Intestinal exopeptidase (aminopeptidase, dipeptidase, amino-tripeptidase)
Digestion

Absorption: in form of amino acids from small intestine. The levo a.a actively absorbed by sodium co-transport. Whereas
dextro a.a. by facilitated diffusion.
Area Juice Enzyme Substrate Endproduct
Mouth Saliva NO proteolytic enzyme present
Stomach Gastric juice Pepsin Proteins Proteoses,Peptones,etc
Small intestine
Pancreatic juice
Trypsin Proteosuspeptones
Amino acids
Chymotrypsin
Carboxy peptidases A&B
DipeptidasesTripeptidasesPolypeptides
Succus entericus
Dipeptidases DipeptidesAmino acids
Tripeptidases Tripeptides
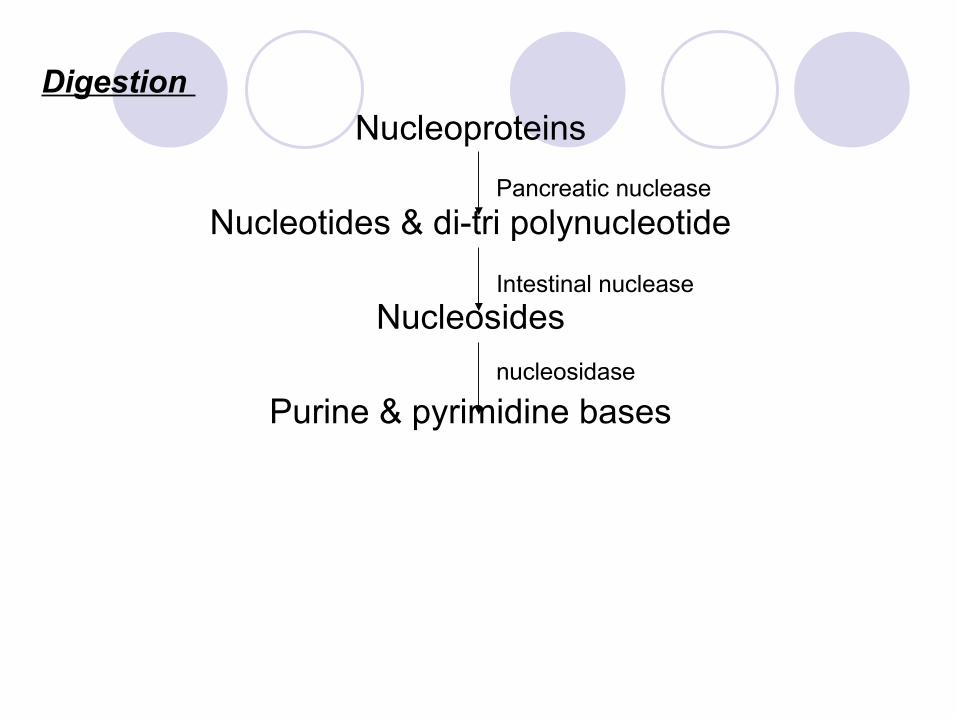
Nucleoproteins
Nucleotides & di-tri polynucleotide
Nucleosides
Purine & pyrimidine bases
Pancreatic nuclease
Intestinal nuclease
nucleosidase
Digestion

Protein & Amino Acid Transport

Absorption of proteins
Sources of digested proteins50% - ingested food25% - digested juices25% - desquamated mucosal cells
7 different transport system transport a.a into enterocytes 5 – co-transport a.a & Na+ 2 – independent of Na+

protein absorption - jejunum & some in upper ileum Proteins with mol wt > 200 – 300 are poorly absorbedIntestine of newborn can absorb intact protein by
pinocytosis.
This enables absorption of antibodies from colostrum.minute amount of native proteins is absorbed in
M – cells overlying peyer’s patches is responsible for food allergies

DIGESTION OF LIPIDSLipids are consumed in form of neutral fats (triglycerides)The different types of fat available are Saturated,
monounsaturated,polyunsaturated fats, etc.The various sources are milk,cheese,butter,oils,fish,
meats,nuts,etc.
Digestion:
a) Mouth- By lingual lipase, But digestion does not occur.
b) Stomach- By Gastric lipase in gastric juice.
c) Intestine- By bile salts, pancreatic enzymes,intestinal lipase,etc.
FINAL PRODUCTS OF FAT DIGESTION are fatty acids, cholesterol & monoglycerides.

Absorption: Monoglycerides,cholesterol,etc form miscelles and enter the enterocytes by simple diffusion.
In mucosal cells, most of monoglycerides are converted into triglycerides. These are coated with a layer of protein,cholesterol & phospholipids to form particles called chylomicrons. These chylomicrons being larger in size cannot pass through membrane of blood capillaries.Hence these are transported through lymph vessels and finally into blood.
Storage: The lipids are stored in adipose tissue & liver. When the above chylomicrons are travelling through capillaries of adipose tissue or liver, enzyme called lipoprotein lipase present in capillary endothelium hydrolyses triglycerides of chylomicrons into free fatty acids (FFA) & glycerol.

FFA & glycerol enter fat cells of adipose tissue or liver cells (i.e. storage points). Here again the FFA & glycerol is converted into triglycerides and stored in these cells.
Other contents of chylomicrons such as cholesterol & phopholipids which are released into the blood combine with proteins to form lipoproteins.
When tissues of body need energy,the triglycerides stored in this adipose tissue is hydrolyzed into FFA & glycerol. The FFA are transported to the body tissues through blood.
These lipids (FFAs) are transported in blood in combination with albumin or in form of lipoproteins.

Transport of Lipids Across Intestinal Epithelium

Water & Vitamin absorption
Out of 10 liters, only 100-200 ml of water is excreted out.Osmotic difference is the driving force for water
absorption.Plenty of water is absorbed in large intestine.All vitamins except vitamin D which is mostly formed in
the skin are absorbed in diet. Fat soluble vitamins absorbed along with lipids require presence of bile salts.
Vitamin B12 is majorly absorbed from ileum. Other vitamins from jejunum..

Water and Ions
Water: can move in either direction across wall of small intestine depending on osmotic gradients
Ions: sodium, potassium, calcium, magnesium, phosphate are actively transported


















