Gilbert hospitals as amplifiers - HAI short course 2012.ppt
4
5/8/2012 1 Hotel Dieu – Paris 1500 http://www.nlm.nih.gov/ 1st recorded outbreak of childbed fever - 1746 • Variable incidence – epidemics – higher among women who delivered in hospital • Mortality 20-80% • Pathogenesis – Miasma vs contagion • 1843, Oliver Wendell Holmes –“Contagiousness of puerperal fever” – Doctors should wash their hands Puerperal fever – an 18 th century EID Ignaz Semmelweis, Vienna General Hospital, 1846 • Childbed fever mortality: • Pathologist dies after autopsy! Hand hygiene mandated • Infection rates fell • but Semmelweiss shunned Old Hungarian proverb: “Tell the truth, and people will bash in your head” Fever hospitals – 18 th & 19 th centuries London Smallpox Hospital 1746 • Public demand – to limit spread; research • Built on city outskirts • Variable outbreak activity – smallpox, scarlet fever, diphtheria, typhus
Transcript of Gilbert hospitals as amplifiers - HAI short course 2012.ppt
5/8/2012
1
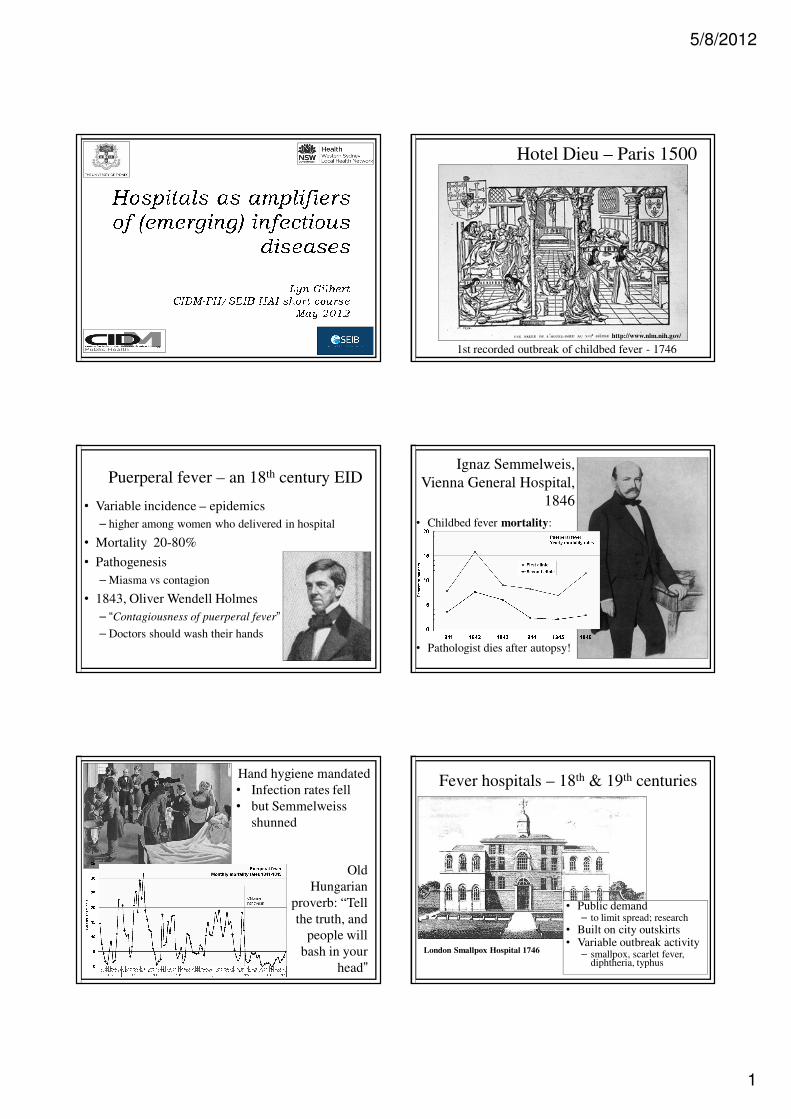
Hotel Dieu – Paris 1500
http://www.nlm.nih.gov/
1st recorded outbreak of childbed fever - 1746
• Variable incidence – epidemics
– higher among women who delivered in hospital
• Mortality 20-80%
• Pathogenesis
– Miasma vs contagion
• 1843, Oliver Wendell Holmes
– “Contagiousness of puerperal fever”
– Doctors should wash their hands
Puerperal fever – an 18th century EIDIgnaz Semmelweis,
Vienna General Hospital,
1846
• Childbed fever mortality:
• Pathologist dies after autopsy!
Hand hygiene mandated
• Infection rates fell
• but Semmelweiss
shunned
Old
Hungarian
proverb: “Tell
the truth, and
people will
bash in your
head”
Fever hospitals – 18th & 19th centuries
London Smallpox Hospital 1746
• Public demand– to limit spread; research
• Built on city outskirts• Variable outbreak activity
– smallpox, scarlet fever, diphtheria, typhus
5/8/2012
2
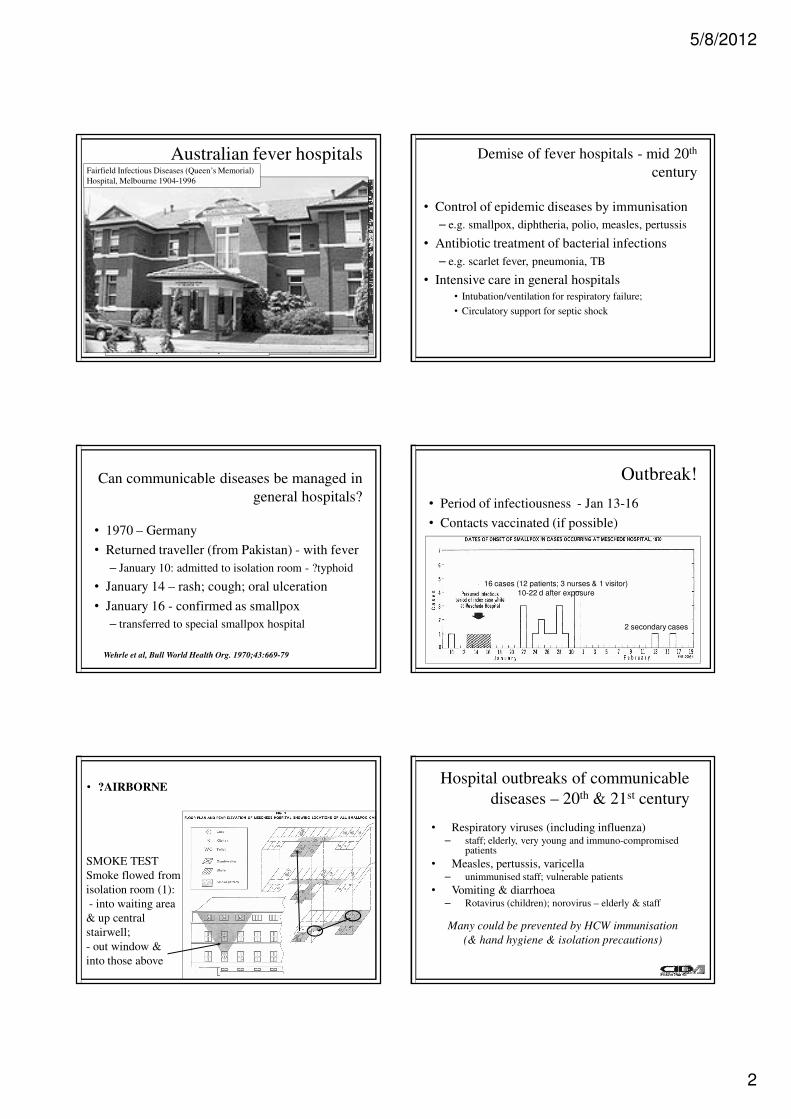
Australian fever hospitals
Prince Henry (The Coast) Hospital 1881 - ??
Fairfield Infectious Diseases (Queen’s Memorial)
Hospital, Melbourne 1904-1996
Demise of fever hospitals - mid 20th
century
• Control of epidemic diseases by immunisation
– e.g. smallpox, diphtheria, polio, measles, pertussis
• Antibiotic treatment of bacterial infections
– e.g. scarlet fever, pneumonia, TB
• Intensive care in general hospitals
• Intubation/ventilation for respiratory failure;
• Circulatory support for septic shock
• 1970 – Germany
• Returned traveller (from Pakistan) - with fever
– January 10: admitted to isolation room - ?typhoid
• January 14 – rash; cough; oral ulceration
• January 16 - confirmed as smallpox
– transferred to special smallpox hospital
Can communicable diseases be managed in
general hospitals?
Wehrle et al, Bull World Health Org. 1970;43:669-79
Outbreak!
• Period of infectiousness - Jan 13-16
• Contacts vaccinated (if possible)
16 cases (12 patients; 3 nurses & 1 visitor)
10-22 d after exposure
2 secondary cases
• ?AIRBORNE
SMOKE TEST
Smoke flowed from
isolation room (1):
- into waiting area
& up central
stairwell;
- out window &
into those above
Hospital outbreaks of communicable
diseases – 20th & 21st century
• Respiratory viruses (including influenza)– staff; elderly, very young and immuno-compromised
patients
• Measles, pertussis, varicella– unimmunised staff; vulnerable patients
• Vomiting & diarrhoea– Rotavirus (children); norovirus – elderly & staff
Many could be prevented by HCW immunisation
(& hand hygiene & isolation precautions)
--

5/8/2012
3
Another (plausible) outbreak –
Sydney 2002
• 35 year old male
– admitted to hospital Feb 2nd
• 24 hour history of:
– fever, rigors, vomiting, confusion, haemoptysis
• Treated empirically for severe pneumonia
– Day 2 – worse; transferred to ICU
– Day 3 – died
--
Biphasic outbreak – 30 cases 5 deaths
--
1st Index case – hospital 1 2nd Index case – hospital 2
10 relatives; 8 HCW infected 2 relatives;
4 neighbours;
3 nurses; 1 nurse’s
relative infected
?Diagnosis
• Index case - no diagnosis
– blood cultures not taken
• Mother and wife - blood cultures Feb 5th
• Gram negative rod isolated - Feb 6th
– Not easily identified
– Sent to reference laboratory
??Yersinia pestis - plague
– Confirmed February 9th
--
?Plague – is this plausible?
• Where has index patient been?
– Indian student; returned from visit to relatives
– Hunting on day before departure; killed and
skinned wild animal!
– Onset of illness 2 days after return (IP 4 days)
• In fact outbreak occurred in India
– Could have happened anywhere!
Joshi et al. Trans Roy Soc Trop Med Hyg 2009;103:455-6
--
SARS, 2003
• Chinese doctor with
SARS – Metropole
Hotel, Hong Kong.
• In 24 hours - 12
people infected.
• Spread to Vietnam,
Canada, Singapore,
USA, Ireland.
30-65% of SARS cases were
HCWsRisk factors for SARS in HCW
Sun Yat-Sen Hospitals, Guangzhou
Odds
ratio
Caring for super-spreaders 3.6
Performing intubation 2.8
Single vs double gloves 4.1
Natural ventilation +/- fan vs air
conditioning
0.4
Avoiding face-to-face contact (always) 0.3
Chen W-Q et al, BMC Public Health 2009, 9:81

5/8/2012
4
Lessons from SARS
• Multiple routes of transmission
– Hands, fomites - excreted in faeces
– Aerosol & droplets - confusion about mask use
• type, need for fit-testing
• Poor compliance with infection control
– Until HCWs died
– Limited knowledge; fatigue
Post SARS (and H1N1) – cough etiquette
How well do we prevent nosocomial
spread of (E)IDs in 2012?
• After 165 years
– HCW hand hygiene compliance ~30-60%
• HCW influenza immunisation uptake - ~40%
• Cough etiquette for patients (?only) before
‘flu season; ??for HCWs, relatives
• HCW still work when symptomatic
• New hospitals built with few isolation rooms
What do we still need to learn?
• Improved, faster diagnosis
• Dynamics of bioaerosols– Masks; airflows; ventilation
• HCW (as well as patients & visitors):– “Victims & vectors” of (E)ID
• Determinants of compliance– behavioural; organisational; environmental;
cultural