Gi Gallbladder & Pancreas
72
1 Pascale Gehy-Andre PA-C Diseases of Gallbladder & Bile Ducts
-
Upload
miami-dade -
Category
Health & Medicine
-
view
4.856 -
download
3
description
Transcript of Gi Gallbladder & Pancreas

1
Pascale Gehy-Andre PA-C
Diseases of Gallbladder & Bile Ducts

2
Anatomy of the Gallbladder• A. A pickle shaped sac
that is 8-10 cm long c a capacity of about 50 ml.
• B. Divided into:− Neck: (has a small
pouch called Hartmann’s pouch. This is the location of most of the pathology)
− Body− Fundus
• C. Contracts after a fatty meal is ingested.
Add a picture here.

3
Biliary Anatomy• Hepatocytes
canaliculi biliary ductules
L & R hepatic ducts common hepatic duct
• Common hepatic ducts & Cystic Duct Common Bile Duct (CBD)

4
Bile Production
• A. Bile is an isotonic mixture consisting of −1. electrolytes−2. Protein−3. bile salts−4. cholesterol−5. phospholipids- (phospholipids: contain
phos. & on hydrolysis yield fatty acids, glycerol, lethicin, & cephalins. Phospholipase is the enzyme found in liver & pancrease)
−6. bile pigment

5
Bile Production• B. Cholate & chenodeoycholate which are bile salts are
synthesized by hepatocytes from cholesterol in a multi-step procedure.
• C. Cholecystokinin (pancreatic enzyme) is released from the small bowel after a fatty meal, stimulates the GB to contract & sphincter of oddi to relax
• D. Bile acids aid in the absorption of fat forming micelles which are absorbed in the small bowel.
• E. The bile salts are reabsorbed in the small bowel & transported back to the liver. Averaging 9x’s/day.

6
Bile Acid Insufficiency• 1. Insufficient bile acids can result from a
disorder at any step in enteropathic circulation− A. liver disease with decreased production of
acids− B. obstruction of the duct− C. Bacterial overgrowth
• (bile acids are conjugated before they can participate in fat absorption)
− D. Disorders of the terminal ileum which decrease the absorption of the bile salts.

7
Bile Acid Insufficiency (cont)• 2. Bile acids facilitate the absorption of dietary fat
by the formation of intraluminal micelles.
• Therefore if absent will result in malabsorption of fat.
• Treatment−A. Tetracycline for small bowel overgrowth−B. Terminal ileum disorders should be treated −C. Use of medium chain triglycerides are helpfulNote: failure to correct allows bile acids to enter
the large bowel producing diarrhea.

8
Cholelithiasis (Gallstones)Cholelithiasis (Gallstones)• Definition: presence of concretions in the
gallbladder or bile ducts.• 1. Affects 20 million people/year• 2. Stone type
– A. Cholesterol (70%) (most common)• All ages• Mostly women• Use of estrogen• Obesity• Diabetes• Disease of small bowel & sphincter
• Definition: presence of concretions in the gallbladder or bile ducts.
• 1. Affects 20 million people/year• 2. Stone type
– A. Cholesterol (70%) (most common)• All ages• Mostly women• Use of estrogen• Obesity• Diabetes• Disease of small bowel & sphincter

9
GallStones (Cholelithiasis)GallStones (Cholelithiasis)• 2. Stone type (cont):
– B. pigment 30%• (calcium bilirubinate)• Mostly bilirubin• Hemolytic states,
cirrhosis & elderly
• 3. Mixed
• 2. Stone type (cont):– B. pigment 30%
• (calcium bilirubinate)• Mostly bilirubin• Hemolytic states,
cirrhosis & elderly
• 3. Mixed

10
Interrelation of gallbladder diseaseInterrelation of gallbladder disease• 1. Cholecystitis is associated with cholelithiasis
in 85%-90% of cases• 2. Regurgitation of pancreatic acid causes non-
bacterial cholecystitis• 3. Bile stasis due to sphincter of oddi spasm or
obstruction is a cause of inflammation• 4. Gangrene of GB is due to chronic cholecystitis• 5. A porcelain GB (heavily calcified) should be
removed surgically because of increased risk of GB cancer
• 1. Cholecystitis is associated with cholelithiasis in 85%-90% of cases
• 2. Regurgitation of pancreatic acid causes non-bacterial cholecystitis
• 3. Bile stasis due to sphincter of oddi spasm or obstruction is a cause of inflammation
• 4. Gangrene of GB is due to chronic cholecystitis• 5. A porcelain GB (heavily calcified) should be
removed surgically because of increased risk of GB cancer

11
Diagnostic StudiesDiagnostic Studies• A. Chemistry, CBC, LFT’s, amylase
– 1. CBC elevated in cholecystitis c slight elevation of LFT’s
– 2. Biliary obstruction: bilirubin, alk phos & amylase may be elvated.
• B. Plain film of the abdomen is of poor value.
• Only 15-20% of stones are radiopaque.• C. Oral Cholecystogram:
– Requires patient to take pills
• A. Chemistry, CBC, LFT’s, amylase– 1. CBC elevated in cholecystitis c slight
elevation of LFT’s– 2. Biliary obstruction: bilirubin, alk phos &
amylase may be elvated.• B. Plain film of the abdomen is of poor
value. • Only 15-20% of stones are radiopaque.• C. Oral Cholecystogram:
– Requires patient to take pills

12
Diagnostic Studies (cont)Diagnostic Studies (cont)
• D. Ultrasound:– Most sensitive and specific test for the detection of gallstones– Limited in obese patients– Simple to do & safe– No preparation needed– May show thinkened wall in acute cholecystitis
• E. HIDA scan:– Used if acute cholecystitis is suspected. The nuclear material is
normally taken up in the GB. If obstructed no GB will be seen.
• F. CT scan
• D. Ultrasound:– Most sensitive and specific test for the detection of gallstones– Limited in obese patients– Simple to do & safe– No preparation needed– May show thinkened wall in acute cholecystitis
• E. HIDA scan:– Used if acute cholecystitis is suspected. The nuclear material is
normally taken up in the GB. If obstructed no GB will be seen.
• F. CT scan

13
Treatment of Cholelithiasis (Gallstones)
Treatment of Cholelithiasis (Gallstones)• 1. Pain relief
• 2. Cholecystectomy– Emergent for cholecystitis– Scheduled if symptomatic cholelithiasis s/ cholecystitis
• 3. Dissolution with – Ursidiol, – chenodeoxycholic acid (actigall)– Contraindicated in:
• Liver ds• large stones• Pregnant women• Severe sx**It takes 2 yrs to work
– Indications: elderly?• 4. Lithotripsy
• 1. Pain relief• 2. Cholecystectomy
– Emergent for cholecystitis– Scheduled if symptomatic cholelithiasis s/ cholecystitis
• 3. Dissolution with – Ursidiol, – chenodeoxycholic acid (actigall)– Contraindicated in:
• Liver ds• large stones• Pregnant women• Severe sx**It takes 2 yrs to work
– Indications: elderly?• 4. Lithotripsy

14
Complications of Cholelithiasis (Gallstones)
Complications of Cholelithiasis (Gallstones)
• Colic• Acute cholecystitis• Cholangitis• Perforation• Fistulization• Gallstone ileus
• Colic• Acute cholecystitis• Cholangitis• Perforation• Fistulization• Gallstone ileus

15
Acute Cholecystitis
• Types:– 1. Acute calculus cholecystitis
• Inflammation of GB in association with stones
• Stones are in the GB, cystic duct, or in CBD
– 2. Acute Acalculus cholecystitis• Acute inflammation of the GB without the presence of
stones
• High incidence of gangrene, necrosis, & perforation
• High mortality rate because more common in elderly & debilitated c absence of oral intake & GB stasis
• Early intervention (consider drainage first)
• Large doses of IV antibiotics

16
Acute Cholecystitis• 1. Key Symptoms:
– Pain in RUQ or epigastric area– Possible radiation to shoulder, back, tip of R scapula, or flank– Nausea & vomiting– Fever, tachycardia, tachypnea– Jaundice (represents obstruction)
• Urine turns dark (acolic stool-Bilirubin)
• 2. Key Signs:– RUQ (or epigastric) tenderness– +Murphy’s sign
• 3. Laboratory:– Leukocytosis– Alk Phos & bilirubin
• (c obstruction & pathology of GB)– SGOT ^, SGPT ^ (if cholangitis present)

17
Acute Cholecystitis (cont)
• 4. Common in:– Fat
– Fertile• (OCP use)
– Forty
– Females
• 5. Differential Diagnosis:– Peptic ulcer
– Appendicitis
– Hepatitis
– Pyelonephritis
– Pneumonia
– MI
– Renal colic
– Pancreatitis
– Cholangitis

18
Acute Cholecystitis
• 6. Key Diagnostic Tests:– Ultrasound
• Most sensitive and specific test for the detection of gallstones
• GB wall thickening and the presence of pericholecystic fluid are radiographic signs of acute cholecystitis
– HIDA Scan (dimethyl iminodiacetic acid) • great when bilirubin elevated
• Does not detect gallstones
• Identifies an obstructed GB
• The most sensitive and specific test for cholecystitis (especially acalculus cholecystitis)

19
Acute Cholecystitis
• Key Diagnostic Tests: (continued)– Oral cholecystogram (limited)– CT scan
• most accurate for differential of intra- & extrahepatic obstruction with 95% accuracy.
• Often used in the workup of abdominal pain without specific localizing signs & symptoms
• CT scan is not a first line study for detection of gallstones because of greater cost & invasive nature of the test
• When present gallstones usually are observed on CT

20

21
Acute Cholecystitis (cont)
• Treatment:– IV fluids– Antibiotics– Analgesics
• (No morphine- theories of sphincter of Oddi spasm)
– Cholecystectomy• Open vs.
laparoscopic surgery

22
Acute Cholecystitis (cont)• Complications:
– Perforation– GB ileus– Biliary colic– Biliary Dyskinesia– Choledocholithiasis– Chronic
Cholecystitis– Tumors of GB

23
Gallbladder disease (cont)
• Biliary colic:– Usually due to stones– Pain due to GB distention– Nausea/ Vomiting– Relief of pain suddenly
• Biliary Dyskinesia:– Symptoms without stones– GB doesn’t empty properly

24
Choledocholithiasis• Stones in the common duct which may
cause the following symptoms:– Biliary colic– Obstructive jaundice– Intermittent jaundice– Pancreatitis
– Cholangitis (inflammation of CBD)
– Hemobilia• Fever • Pain• Blood (in the intrahepatic system)

25
Cholangitis
• inflammation of CBD
• Charcot’sTriad:– RUQ pain (biliary pain)
– Jaundice
– Fever

26
Cholangitis Mneumonic
Charcot's triad/ Conjugated bilirubin increaseHepatic abscesses/ Hepatic (intra/extra) bile ductsObstructionLeukocytosisAlkaline phosphatase increaseNeoplasmsGallstonesInflammatory bowel disease (ulcerative colitis)Transaminase increaseInfectionSclerosing

27
Chronic Cholecystitis
• Associated c GB stones in 95% of cases
• Frequent attacks & GB empties poorly
• Fever unusual
• Pain usually several hrs after eating
• Bloating, belching, and flatus
• Murphy’s sign absent
• Labs: CBC, Amylase, bilirubin, enzymes normal
• HIDA scan positive

28
Tumors of the Gallbladder• Polyps: are rare
• Carcinoma of GB:– Uncommon– Mostly women– Usually diagnosed too late– Spread by direct invasion– Adenocarcinoma– Courvoisier’s sign
(palpable GB)
• Carcinoma of Bile Duct:– Usually adenocarcinoma– Symptoms:
• Painless jaundice• Mass palpable

2929
Review GallbladderReview Gallbladder GallstonesGallstones~ 70% cholesterol & ~ 70% cholesterol &
30% pigment stones30% pigment stones• May be asymptomatic (70%)May be asymptomatic (70%)• May cause biliary colic (20%)May cause biliary colic (20%)• May cause cholecystitis (10%)May cause cholecystitis (10%)
Biliary colic-Biliary colic- steady cramplike pain in steady cramplike pain in epigastrium (RUQ) epigastrium (RUQ) • Pain subsides over 30-60 minPain subsides over 30-60 min
CholecystitisCholecystitis- steady cramplike pain in - steady cramplike pain in epigastrium (RUQ) & + Murphy’s signepigastrium (RUQ) & + Murphy’s sign• Pain does not subside spontaneouslyPain does not subside spontaneously
CholangitisCholangitis- triad= - triad= • 1. biliary pain (RUQ) 2. jaundice 3. fever1. biliary pain (RUQ) 2. jaundice 3. fever• Sclerosing cholangitis- autoimmune inflammation of the bile Sclerosing cholangitis- autoimmune inflammation of the bile
ducts. A rare complication of ulcerative colitisducts. A rare complication of ulcerative colitis

30
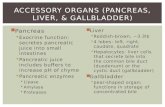
Pancreas
• Anatomy• Head: embraces the duodenal curve• Body: crosses the vertebral column• Tail: in the hilum of the spleen

31

32

33

34
Pancreas Physiology
• 1. Islets of Langerhans: responsible for the production of:• A. Insulin• B. Glucagon:
• A hormone that is produced by the alpha cells of langerhan that produces glucose from glycogen.
• C. Gastrin• D. Somatostatin
• Gastrin and somatostatin are mostly in stomach, but also in pancreas, stimulates HCL stopping agents.

35
Pancreas Physiology (cont)
• 2. Enzymes secreted from ducts:• Amylase (CHO)• Lipase (Fats)• Trypsinogen (Protein)
• Is converted to trypsin in the duodenum so as not to cause autodigestion
NOTE: Liver produces alpha trypsin to protect against autodigestion

36
Pancreas Physiology (cont)
• 3. Pancreatic secretion stimulated by two hormones:• Secretin:
• Produced in the duodenum & stimulated by acid
• Inhibits gastric acid• Stimulates pancreas to produce bicarb &
chloride
• Cholecystokinin:• A pancreozymin which is released in response
to fat & amino acids in the duodenum• Stimulates pancreas to produce amylase,
lipase, & trypsin

37
Pancreas Physiology (cont)
• 4. The pancreas secrets 1-4 Liters of fluid per day
• 5. The pancreatic juice is usually alkaline.• Food in duodenum causes secretion of secretin
(due to high acid content). Secretin releases H2O & bicarb.
• 6. In pancreatitis we use foods low in fat & protein because they stimulate secretion from the pancreas. CHO is a weaker stimulant.
• 7. Pancreatic enzymes inhibit gastric secretion of its enzymes.

3838
Acute PancreatitisAcute Pancreatitis
Etiology:Etiology:Alcohol & Gallstones Alcohol & Gallstones = 80-90%= 80-90%• Other causes:Other causes:
Complications of ERCP Complications of ERCP (endoscopic retrograde (endoscopic retrograde cholangiopancreatography)cholangiopancreatography)
TraumaTrauma Infections (mumps/ viral)Infections (mumps/ viral) Hyperlipidemia: TG > 1000 mgHyperlipidemia: TG > 1000 mg HypercalemiaHypercalemia Drugs (thiazides, lasix)Drugs (thiazides, lasix) IdiopathicIdiopathic

3939
Pancreatitis Causes MneumonicPancreatitis Causes Mneumonic I GET SMASHEDI GET SMASHED::
IIdiopathiticdiopathiticGGallstonesallstonesEEthanolthanolTTraumaraumaSSteroidsteroidsMMumpsumpsAAutoimmune (PAN)utoimmune (PAN)SScorpion stingscorpion stingsHHyperlipidemia/ yperlipidemia/ HHypercalcemiaypercalcemiaEERCPRCPDDrugs (including azathioprine and diuretics)rugs (including azathioprine and diuretics)
Note: 'Get Smashed' is slang in some countries for drinking, Note: 'Get Smashed' is slang in some countries for drinking, and ethanol is an important pancreatitis cause.and ethanol is an important pancreatitis cause.
Note: Shortest answer is gallstones for women, and ethanol Note: Shortest answer is gallstones for women, and ethanol for men. for men.

4040

4141

4242

4343

4444
Acute PancreatitisAcute Pancreatitis
Symptoms:Symptoms:• Epigastric pain severe, boring in natureEpigastric pain severe, boring in nature• Radiation to backRadiation to back• Nausea & vomitingNausea & vomiting• Aggravated by eatingAggravated by eating• Feels better leaning forwardFeels better leaning forward• Possible + peritoneal signsPossible + peritoneal signs

4545
Acute PancreatitisAcute Pancreatitis Key Signs:Key Signs:
• Low grade fever, tachycardia, tachypneaLow grade fever, tachycardia, tachypnea• Pleural effusions or basal consolidation of lung (left)Pleural effusions or basal consolidation of lung (left)• Bowel sounds are feeble or absentBowel sounds are feeble or absent• Low blood pressure, thready pulse, diaphoretic Low blood pressure, thready pulse, diaphoretic
(shock)(shock)• Rare findings are:Rare findings are:
Jaundice due to common bile duct compressionJaundice due to common bile duct compression Cullen signCullen sign: discoloration of the periumbilical : discoloration of the periumbilical
areaarea Grey turner signGrey turner sign: flank discoloration: flank discoloration
• These two are specific for pancreatitisThese two are specific for pancreatitis

4646
Acute pancreatitisAcute pancreatitis Laboratory tests:Laboratory tests:
• Elevated serum amylase (>4x’s normal)Elevated serum amylase (>4x’s normal) Goes down within 48 hrsGoes down within 48 hrs UrineUrine amylase neither specific nor sensitive amylase neither specific nor sensitive If normal needs to be confirmed by CTIf normal needs to be confirmed by CT
• Serum lipaseSerum lipase delayed but delayed but more specificmore specific
• CBC usually abnormalCBC usually abnormal Elevated WBCElevated WBC If hgb/hct fall means poor prognosisIf hgb/hct fall means poor prognosis
• ChemistryChemistry HyperglycemiaHyperglycemia hypocalcemiahypocalcemia
• LFT’sLFT’s Abnormal if biliary tree involvedAbnormal if biliary tree involved
**Excessive fluid loss**Excessive fluid loss

4747
Ranson’s criteria Ranson’s criteria on admissionon admission 1. Age greater than 55 on admission?1. Age greater than 55 on admission?
Yes Yes (1 points) (1 points) No No (0 points)(0 points) 2. WBC greater than 16K on admission?2. WBC greater than 16K on admission?
Yes Yes (1 points) (1 points) No No (0 points)(0 points) 3. Blood glucose greater than 200 mg% 3. Blood glucose greater than 200 mg%
on admission?on admission?Yes Yes (1 points) (1 points) No No (0 points)(0 points)
4. Serum LDH greater than 350 IU/L on 4. Serum LDH greater than 350 IU/L on admission?admission?
Yes Yes (1 points) (1 points) No No (0 points)(0 points) 5. Serum SGOT (AST) greater than 250 SF 5. Serum SGOT (AST) greater than 250 SF
units on admission?units on admission?Yes Yes (1 points) (1 points) No No (0 points)(0 points)

4848
Ranson’s criteria Ranson’s criteria within 48 hrswithin 48 hrs 1. Hematocrit fall more than 10% within 48 hrs 1. Hematocrit fall more than 10% within 48 hrs
of admission?of admission?Yes Yes (1 points) (1 points) No No (0 points)(0 points)
2. BUN rise more than 5 mg/dl within 48 hrs of 2. BUN rise more than 5 mg/dl within 48 hrs of admission?admission?
Yes Yes (1 points) (1 points) No No (0 points)(0 points) 3. Serum calcium less than 8 mg% within 48 3. Serum calcium less than 8 mg% within 48
hrs of admission?hrs of admission?Yes Yes (1 points) (1 points) No No (0 points)(0 points)
4. Arterial pO2 less than 60 mmHg within 48 4. Arterial pO2 less than 60 mmHg within 48 hrs of admission?hrs of admission?
Yes Yes (1 points) (1 points) No No (0 points)(0 points) 5. Base deficit less than 4 mEq/L within 48 hrs 5. Base deficit less than 4 mEq/L within 48 hrs
of admission?of admission?Yes Yes (1 points) (1 points) No No (0 points)(0 points)
6. Fluid sequestration more than 6L 6. Fluid sequestration more than 6L within 48 hrs of admission?within 48 hrs of admission?
Yes Yes (1 points) (1 points) No No (0 points)(0 points)

4949
Ranson's criteria for pancreatitis Ranson's criteria for pancreatitis mortality predictionmortality prediction
Score Interpretation Score Interpretation under 3 Predicted mortality about 1%under 3 Predicted mortality about 1%
3-4 Predicted mortality of 15%3-4 Predicted mortality of 15%
5-6 Predicted mortality of 40%5-6 Predicted mortality of 40%
> 6 Predicted mortality of 100%> 6 Predicted mortality of 100%


5151
Pancreatitis Ranson’s CriteriaPancreatitis Ranson’s Criteria On Admission On Admission MneumonicMneumonic
""GAGA LAWLAW" (GA is abbreviation for Georgia):" (GA is abbreviation for Georgia):GGlucose >200lucose >200AAST >250ST >250LLDH >350DH >350AAge >55 y.o.ge >55 y.o.WWBC >16000BC >16000
OrOr LEGALLEGAL::
LLeukocytes > 16.000eukocytes > 16.000EEnzyme AST > 250nzyme AST > 250GGlucose > 200lucose > 200AAge > 55ge > 55LLDH > 350DH > 350

5252
Pancreatitis Ranson’s CriteriaPancreatitis Ranson’s CriteriaInitial 48 hrsInitial 48 hrs Mneumonic Mneumonic
""CC & & HOBBSHOBBS" (" (CCalvin and alvin and HobbHobbeess):):CCalcium < 8alcium < 8HHct drop > 10%ct drop > 10%OOxygen < 60 mmxygen < 60 mmBBUN rise > 5UN rise > 5BBase deficit > 4ase deficit > 4SSequestration of fluid > 6Lequestration of fluid > 6L

5353
Acute PancreatitisAcute Pancreatitis
Radiology studies:Radiology studies:• Plain films of abdomen (upright)Plain films of abdomen (upright)
Helps r/o perforation (free air) or intestinal Helps r/o perforation (free air) or intestinal obstructionobstruction
• Abdominal sonogram identifies:Abdominal sonogram identifies: GB, CBD size, stonesGB, CBD size, stones
• CT scanCT scan Size of pancreasSize of pancreas Extent of necrosisExtent of necrosis Fluid collectionFluid collection
Prognosis: most recover within 48-72 hrsPrognosis: most recover within 48-72 hrs• Mortality average is about 10%Mortality average is about 10%

5454
Acute PancreatitisAcute Pancreatitis
Treatment:Treatment:• NPONPO• Nasogastric tube (rids acid)Nasogastric tube (rids acid)• IV fluids (electrolytes, calcium)IV fluids (electrolytes, calcium)• Parenteral analgesics (Demerol)Parenteral analgesics (Demerol)• Antibiotics in severe biliary pancreatitisAntibiotics in severe biliary pancreatitis• Removal of stones from ampulla if Removal of stones from ampulla if
needed.needed.• High CHO, low fat & proteinHigh CHO, low fat & protein

5555
Pancreatitis: TreatmentPancreatitis: TreatmentMneumonicMneumonic
MACHINESMACHINES::MMonitor vital signsonitor vital signsAAnalgesia/ nalgesia/ AAntibioticsntibioticsCCalcium gluconate (if necessary)alcium gluconate (if necessary)HH2 blockers2 blockersIIV access/ V access/ IIV fluidsV fluidsNNil by mouthil by mouthEEmpty gastric contentsmpty gastric contentsSSurgery if required/ urgery if required/ SSenior reviewenior review

5656
Acute pancreatitisAcute pancreatitis Complications of pancreatitisComplications of pancreatitis
• 1. 1. PseudocystsPseudocysts Due to necrosis of cells causing accumulation of Due to necrosis of cells causing accumulation of
blood, pancreatic juices, fatblood, pancreatic juices, fat Resolve spontaneouslyResolve spontaneously
• 2. 2. Pancreatic AbscessPancreatic Abscess Infected cystsInfected cysts
• 3. 3. OthersOthers Fat necrosisFat necrosis ARDS (respiratory distress syndrome)ARDS (respiratory distress syndrome) Acute tubular necrosisAcute tubular necrosis DIC, hemorrhageDIC, hemorrhage Pancreatic insufficiency Pancreatic insufficiency

5757
Acute PancreatitisAcute Pancreatitis
Differential diagnosisDifferential diagnosis• Acute cholecystitisAcute cholecystitis• Biliary colicBiliary colic• CholangitisCholangitis• Peptic ulcerPeptic ulcer• HepatitisHepatitis• Intestinal obstructionIntestinal obstruction• MIMI• PneumoniaPneumonia

5858
Chronic PancreatitisChronic Pancreatitis
Defined:Defined:• Episodes of acute inflammation in a Episodes of acute inflammation in a
previously injured pancreaspreviously injured pancreas Causes:Causes:
• Alcoholic abuseAlcoholic abuse• TraumaTrauma• Pancreas divisum: failure of the ventral Pancreas divisum: failure of the ventral
& dorsal pancreatic ducts to fuse& dorsal pancreatic ducts to fuse• Most common cause in children is cystic Most common cause in children is cystic
fibrosisfibrosis

5959

6060
Chronic PancreatitisChronic Pancreatitis
Key Symptoms:Key Symptoms:• 1. Recurrent abdominal pain radiating to back, 1. Recurrent abdominal pain radiating to back,
lasting hrs to days, lasting hrs to days, precipitated by alcohol.precipitated by alcohol.• 2. Steatorrhea when 90% of pancreas is 2. Steatorrhea when 90% of pancreas is
destroyed. Increase protein in diet without destroyed. Increase protein in diet without complications. Increased fat intake will cause complications. Increased fat intake will cause further increase in diarrhea.further increase in diarrhea.
• 3. CHO malabsorption is rare3. CHO malabsorption is rare• 4. Vitamin B12 malabsorption: 4. Vitamin B12 malabsorption: due to decreased due to decreased
secretion of trypsin. B12 combines with a R-protein in secretion of trypsin. B12 combines with a R-protein in the stomach. If not cleaved by trypsin, it will not bind the stomach. If not cleaved by trypsin, it will not bind with IF. Then can not be absorbed in the terminal ileumwith IF. Then can not be absorbed in the terminal ileum
• 5. Diabetes mellitus5. Diabetes mellitus

6161
Chronic PancreatitisChronic Pancreatitis Key Sign:Key Sign:
• Epigastric tendernessEpigastric tenderness Laboratory:Laboratory:
• Blood tests not useful: Blood tests not useful: serum amylase often serum amylase often normalnormal; amylase & lipase only ^ in acute states; amylase & lipase only ^ in acute states
• Secretin test: to estimate the volume of fluid & Secretin test: to estimate the volume of fluid & bicarb.bicarb.
• Radiology tests:Radiology tests: Flat plate (AXR) may reveal calcificationsFlat plate (AXR) may reveal calcifications ERCP showing a dilated CBDERCP showing a dilated CBD CT scan showingCT scan showing calcificationscalcifications, ,
pseudocysts, ductal abnormalitiespseudocysts, ductal abnormalities

6262

6363

6464
Chronic PancreatitisChronic Pancreatitis Treatment:Treatment:
• 1. pain relief:1. pain relief: No alcoholNo alcohol Analgesics (narcotics- careful c addicts)Analgesics (narcotics- careful c addicts) Pancreatic extractsPancreatic extracts
• 2. Steatorrhea: 2. Steatorrhea: use of oral enzymes with meals, low fat diet, use of oral enzymes with meals, low fat diet,
low protein, medium chain triglycerides.low protein, medium chain triglycerides.
• Diabetes: Diabetes: Calorie restrictionCalorie restriction Small doses of insulinSmall doses of insulin

6565
Pancreatic CarcinomaPancreatic Carcinoma Most common is Ductal carcinoma Most common is Ductal carcinoma
accounts for more than 90% of all accounts for more than 90% of all pancreatic carcinomas. This is exocrine.pancreatic carcinomas. This is exocrine.
Most are adenocarcinoma of ampulla Most are adenocarcinoma of ampulla area = no curearea = no cure
More frequent in males over 40 yoMore frequent in males over 40 yo Smoking increases incidenceSmoking increases incidence Top ranked cancers:Top ranked cancers:
MenMen WomenWomenLungLung breastbreastColonColon coloncolonProstateProstate lunglungPancreasPancreas ovaryovary
pancreaspancreas

6666
Pancreatic CarcinomaPancreatic Carcinoma
Less common: Endocrine causesLess common: Endocrine causes• 1. insulinoma1. insulinoma• 2. gastrinoma2. gastrinoma• 3. glucagonoma3. glucagonoma• 4. somatostatinoma 4. somatostatinoma inhibits all islet cell fxninhibits all islet cell fxn
• 5. VIPoma 5. VIPoma (pancreatic polypeptide) causes severe (pancreatic polypeptide) causes severe diarrhea & hypokalemia (pancreatic diarrhea)diarrhea & hypokalemia (pancreatic diarrhea)

6767
Pancreatic CarcinomaPancreatic Carcinoma About About 2/3 occur in the head2/3 occur in the head & usually & usually
spreads to the contiguous structuresspreads to the contiguous structures Symptoms:Symptoms:
• Vague discomfortVague discomfort• More toward backMore toward back• Worse on lying downWorse on lying down• Weight lossWeight loss• Jaundice is characteristicJaundice is characteristic• Glucose intolerance can be an early signGlucose intolerance can be an early sign• N/V weakness on occasionN/V weakness on occasion• PruritisPruritis• Pain can be early if the tail is involved because of splanchnic Pain can be early if the tail is involved because of splanchnic
nerve nerve Note: painless, non-pruritic, jaundice if head involvedNote: painless, non-pruritic, jaundice if head involved
but painful if tail is involved but painful if tail is involved

6868
Pancreatic CarcinomaPancreatic Carcinoma Classic findings:Classic findings:
• None in early stagesNone in early stages• If common duct obstructed due to head If common duct obstructed due to head
tumor = jaundice & icterus tumor = jaundice & icterus • GB can be palpable (Courvoisier’s sign)GB can be palpable (Courvoisier’s sign)• Ascites & peripheral edema may be a sign of Ascites & peripheral edema may be a sign of
portal hypertensionportal hypertension• Superficial thrombophlebitis Superficial thrombophlebitis (Trousseau’s (Trousseau’s
sign)sign) occurs. occurs.

6969
Pancreatic CarcinomaPancreatic Carcinoma Laboratory Tests:Laboratory Tests:
• Routine tests in early stages normalRoutine tests in early stages normal• Alk phos & transaminases (AST/ALT) are Alk phos & transaminases (AST/ALT) are
slightly elevatedslightly elevated• Ultrasound: the best in the initial diagnosisUltrasound: the best in the initial diagnosis• CT scan is better at staging the tumorCT scan is better at staging the tumor• Angiography (helpful if tumor is resectable)Angiography (helpful if tumor is resectable)
Stages:Stages:• I. Confined to pancreasI. Confined to pancreas• II. Involving only the neighboring structuresII. Involving only the neighboring structures• III. Involving regional lymph nodesIII. Involving regional lymph nodes• IV. Metastatic to liver & distant spreadIV. Metastatic to liver & distant spread

7070

7171
Pancreatic CarcinomaPancreatic Carcinoma
Differential Diagnosis:Differential Diagnosis:• Chronic pancreatitisChronic pancreatitis• CholecystitisCholecystitis• Causes of jaundice: hepatitisCauses of jaundice: hepatitis• Irritable bowel syndromeIrritable bowel syndrome• Carcinoma of duodenumCarcinoma of duodenum• Common bile duct stonesCommon bile duct stones• Peptic ulcer diseasePeptic ulcer disease• DepressionDepression• Ampulla carcinomaAmpulla carcinoma• Metastatic disease to the pancreasMetastatic disease to the pancreas

7272
Pancreatic CarcinomaPancreatic Carcinoma Treatment:Treatment:
• Prognosis is poor, with no survivors to 5 yrsPrognosis is poor, with no survivors to 5 yrs
• 10-15% are resectable10-15% are resectable
• If resectable 30% survive less than 2 yrsIf resectable 30% survive less than 2 yrs
• Chemotherapy gives poor responseChemotherapy gives poor response
• A whipple procedure for temporary reliefA whipple procedure for temporary relief Includes removal of small portion of duodenum, Includes removal of small portion of duodenum,
distal stomach, GB, CBD, regional nodes, some distal stomach, GB, CBD, regional nodes, some jejunum & pancreasjejunum & pancreas