Gestatinal trophoblastic diseases by Dr ekram
42
By: Ekramuddin Final year MBBS ROLL 08-050
-
Upload
ayub-medical-college -
Category
Health & Medicine
-
view
119 -
download
0
Transcript of Gestatinal trophoblastic diseases by Dr ekram

By:
EkramuddinFinal year MBBS
ROLL 08-050

INTRODUCTION TO NORMAL PLACENTATION
1. Trophoblast is the tissue that forms the fetal part of the placenta.
2. Its first appears as the outer most layer of the implanted blastocyst (a ball of cells with cavitation formed in the 3rd week of gestation from feltilized ovum.
3. Primary chorionic villi are formed from trophoblast tissue cords which then converts into secondary villi by acquiring central mesenchymal core from extra mesenchymal mesoderm.

IMPLANTED BLASTOCYST 4TH WEEK

IMPLANTED BLASTOCYST
4TH WEEK 5TH WEEK

DEFINITION OF GESTATIONAL TROPHOBLASTIC DISEASES
GTDs are group of tumors and tumor like conditions arising from the trophoblastic tissue of malignant potential.
where this malignant or uncontrolled proliferative potential comes from??

1..abnormal fertilization as in hydatiform mole
2..pure epithelial malignant neoplasms as in uterine choriocarcinoma
3..normal pregnancy as in most cases of placental site trophoblastic tumors

GTDs include:Hydatidiform Mole:(Benign)1..Complete 2..Partial
Gestational Trophoblastic Neoplasia (GTN):(malignant)1..Persistent/Invasive Mole2..Choriocarcinoma3..Placental-Site Trophoblastic Tumor (PSTT)

Hydatidiform Mole
INCIDENCE: Asia: complete mole 2- per 1000.
Partial mole 1 per 700 pregnancies.
3 fold more in western countries.

HYDATIFORM MOLE AETIOPATHOLOGY

Hydatidiform Mole
Risk Factors: History of previous GTD
If one previous mole, 1% chance of recurrence . If 2 previous moles, risk of recurrence increases
to 16-28% Smoking Vitamin A deficiency Maternal age extremes.

Hydatidiform MoleClinical Presentations:
SYMPTOMS
First trimester Vaginal bleeding (most common) Pelvic pain Hyperemesis gravidarum Hyperthyroidism Vaginal passage of hydropic vesicles

HYDATIFORM MOLE SIGNS
Large for dates Soft uterus No fetal parts palpable ,no lie,no
presentation. No fetal movements No fetal heart sounds

DEFERENTIALS
Ectopic pregnancy PROM Ovarian cyst Multiple pregnancy Appendicitis Missed miscariage

INVESTIGATIONS
1. ROUTINE: blood CP, grouping,cross matching,chest x-ray,RBS,and urine RE.
2. SPECIFIC: BhCG levels, USG (TVS),”snow storm appearance” REMEMBER: fast accurate BhCG levels and
TVS combinely are the best diagnostic tools a gyneacologist and obtetrecian can offer a women with early pregnancy disorders.
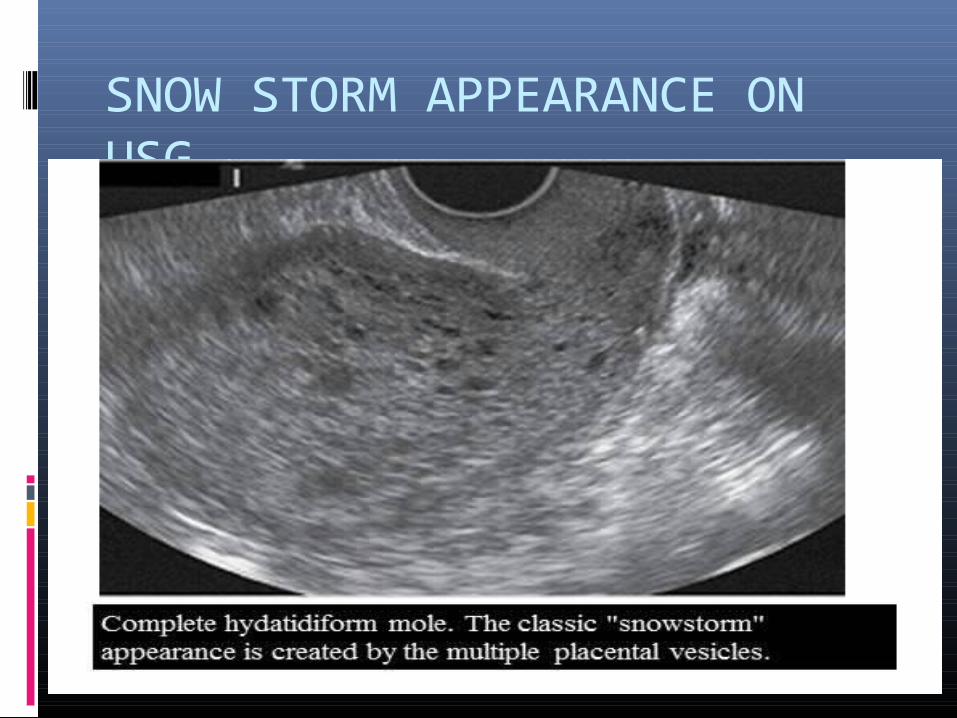
SNOW STORM APPEARANCE ON USG

MOLAR PREGNANCY (GROSS)
COMPLETE MOLE PARTIAL MOLE

Hydatidiform Mole Treatment 1. Counsel the couples2. Suction and curretage for complete mole3. Hysterectomy if completed childbearing4. Give anti D antibodies if mother O-IVE5. FOLLOW UP….. Weekly BhCG titers until negative for
consecutive 3 wks Monthly titers until negative for 6 consecutive
months If still high titers encountered after D&C then
treat chemotheraputically for remaining tissue.
Contrception by barrier method until hcg normal for 6 months.then can concieve


Gestational Trophoblastic Neoplasia (GTN)
Persistent/Invasive Mole Choriocarcinoma Placental-Site Trophoblastic Tumor (PSTT)
** Malignant

Risk Factors for GTN After Mole
Preevacuation uterine size greater than gestationl age or larger than 20 weeks gestation
Theca-lutein cysts larger than 6 cm Age > 40 years Serum hCG levels > 100,000 mIU/mL Medical complications of molar pregnancy Previous hydatidiform mole

Invasive Mole
Myometrial invasion by hydatidiform mole 1 in 15,000 pregnancies 10-17% of hydatidiform moles will progress
to invasive moles Mets to lungs and brain. Treated by chemotherapy and hysterectomy.

Persistent Mole
Definition of persistent molar disease and need for chemotherapy (at least one of the following): B-hCG plateau for ≥ 4 values for ≥ 3 weeks B-hCG increase of ≥ 10% for ≥ 3 values for ≥ 2
weeks B-hCG persistence 6 months after molar
evacuation Histopathologic diagnosis of choriocarcinoma Presence of metastatic disease

Choriocarcinoma
It is a pure epithelial malignant neoplasm of trophoblast cells
Most aggressive type of GTN Abnormal trophoblastic hyperplasia Absence of chorionic villi Direct invasion of myometrium Vascular spread to distant sites:
Lungs Brain Liver Pelvis and vagina Spleen, intestines, and kidney Presents as acute abdomen,cough,hemoptisis,blurring of
vision,headache and seizures.

Choriocarcinoma (con’d)
May come from any type of pregnancy- 25% follow abortion or tubal pregnancy- 25% with term gestation- 50% from hydatidiform moles
2-3% of moles progress to choriocarcinoma Incidence 1 in 40,000 pregnancies

Placental-Site Trophoblastic Tumor (PSTT)
Originate from intermediate cytotrophoblast cells along with blood vessels and syncitiotrophoblast.
Secrete human placental lactogen (hPL) B-hCG often normal Less vascular invasion, necrosis and
hemorrhage than choriocarcinoma Lymphatic spread Arise months to years after term pregnancy in
most cases but can occur after spontaneous abortion or molar pregnancy

Placental-Site Trophoblastic Tumor (PSTT)
Most common symptom is vaginal bleeding Tend to:
- Remain in uterus- Disseminate late- Produce low levels of B-hCG compared to other GTN- Be resistant to chemotherapy (treat with surgery)

Signs & Symptoms GTN
Continued uterine bleeding, uterine perforation, enlarged irregular uterus, persistent bilateral ovarian enlargement
From metastatic lesions: abdominal pain, hemoptysis, melena, increased intracranial pressure (headaches, seizures, hemiplegia), dyspnea, cough, chest pain

Diagnosis of GTN
Increase or plateau in B-hCG after molar pregnancy
Pathologic diagnosis by D&C or biopsy of metastatic lesions
WARNING: biopsy of metastatic lesions can result in massive hemorrhage
Metastatic workup: CXR (or CT chest), CT abdomen/pelvis +/- CT/MR of brain

Classification & Staging of GTD
FIGO Staging Describes anatomic distribution of disease
World Health Organization (WHO) Scoring Index Describes prognosis

FIGO Staging
Stage Description
I Disease confined to the uterus
II Disease extends outside the uterus but limited to genital structures (adnexa, vagina, and broad ligament)
III Disease extends to the lungs with or without genital tract involvement
IV Disease involves any other metastatic sites

WHO Prognostic Score Index
Score
Characteristic 0 1 2 4
Age <40 ≥40 - -
Antecedent preg Mole Abortion Term -
Interval from index pregnancy
<4 months
4-6 months
7-12 months >12 months
Pretreatment hCG <103 103- 104 104-105 >105
Largest tumor size (including uterus)
< 3cm 3-4 cm ≥5cm -
Site of metastases Lung Spleen, kidney
GI tract Liver, brain
Number of metastases - 1-4 5-8 >8
Previous failed chemotherapy
- - Single drug ≥2 drugs

Therapy for GTN
Low-risk = score ≤6 High-risk = score ≥7 Single agent therapy for nonmetastatic
(stage I) or low-risk metastatic (stage II and III) with score <7 survival rates ~ 100%
Combination chemotherapy +/- adjuvant radiation and/or surgery for high-risk metastatic disease or score ≥7

Therapy: Nonmetastatic GTN
Single-agent with either methotrexate or dactinomycin
Chemotherapy continued until hCG values normal and then 2-3 cycles beyond
Change to alternative single-agent for hCG plateaus above normal or toxicities
If significant elevation of hCG or new metastases, switch to multiagent
85-90% cured with initial regimen, <5% will require hysterectomy for cure

Therapy: Low-risk Metastatic GTN
Low-risk metastatic disease can be treated with single-agent therapy with 5-day regimens
Cure rates ~100% but 30-50% will be develop resistance to first agent
If resistance to sequential single-agent chemotherapy (5-10% of patients), switch to multiagent chemotherapy

Therapy: High-risk Metastatic GTN Stage IV Stage II/III with score > 7 Disease refractory to single-agent chemotherapy
Combination Chemotherapy: EMACO:
Day 1: Etoposide, Methotrexate and Dactinomycin Day 8: Cyclophosphamide and Vincristine
(Oncovorin) Repeat q2 weeks until remission Continue for at least 2-3 cycles beyond first normal
hCG MAC (Methotrexate, Dactinomycin,
Cyclophosphamide) EMA/EP – EMA + Etoposide and Cisplatin

Therapy: High-risk Metastatic GTN Cure rates 80-90% Hysterectomy and/or thoracotomy may be
useful in resistant setting or symptomatic management
Poorer prognosis with choriocarcinoma, metastases to places other than lung and/or vagina, number of metastases, and failure of previous chemotherapy

Pacental Site Ttrophoblastic Tumor Therapy
Hysterectomy Chemotherapy for metastatic disease or
nonmetastatic disease with poor prognosis:- Interval from index pregnancy > 2 years- Deep myometrial invasion- Tumor necrosis- Mitotic count > 6 per 10 high-power fields
Survival rates: ~100% for nonmetastatic disease 50-60% for metastatic disease

Follow-up Care
After completion of chemotherapy, follow serial hCG every 2 weeks for three months, then monthly for one year
Physical examinations every 6-12 months and imaging as indicated

Reproductive Performance
Most women resume normal ovarian function
No increase risk of stillbirths, abortions, congenital anomalies, prematurity, or major obstetric complications
No evidence of reactivation At increased risk for development of second
episode

False Positive Serum hCG
Phantom hCG syndrome/ phantom choriocarcinoma
3-4% of healthy individuals have human-antimouse antibodies that can mimic hCG immunoreactivity
To verify: Urine hCG should be negative Should not show parallel decrease with serial
dilutions Test at national B-hCG reference lab

Summary
Hydatidiform mole is a benign condition, 80% cured with suction D&C
Malignant GTN: Persistent or invasive mole Choriocarcinoma PSTT
WHO score > 7 represents high-risk disease GTN very sensitive to chemotherapy

Thank You...Thank You...

![[Ekram hossain, dusit_niyato,_zhu_han]_dynamic_spe(book_fi.org)](https://static.fdocuments.in/doc/165x107/54c25f594a795924248b46a5/ekram-hossain-dusitniyatozhuhandynamicspebookfiorg.jpg)