
German national case collection for familial pancreatic cancer (FaPaCa): ten years experience
8
German national case collection for familial pancreatic cancer (FaPaCa): ten years experience Ralph Schneider • Emily P. Slater • Mercede Sina • Nils Habbe • Volker Fendrich • Elvira Mattha ¨i • Peter Langer • Detlef K. Bartsch Published online: 5 January 2011 Ó Springer Science+Business Media B.V. 2011 Abstract Familial pancreatic cancer (FPC) is a rare hereditary tumor syndrome. The 10-years experience of the national case collection for familial pancreatic cancer of Germany (FaPaCa) is reported. Since 1999 FaPaCa has collected families with at least two first-degree relatives with confirmed pancreatic cancer (PC), who did not fulfill the criteria of other hereditary tumor syndromes. Histopa- thological verification of tumor diagnoses, and genetic counseling were prerequisites for enrollment of families in FaPaCa. 94 of 452 evaluated families fulfilled the criteria for partaking in FaPaCa. PC represented the sole tumor entity in 38 (40%) families. In 56 families additional tumor types occurred, including breast cancer (n = 28), colon cancer (n = 20) and lung cancer (n = 11). In 70 (74%) families the pattern of inheritance was consistent with an autosomal dominant trait. Compared to the preceding generation, a younger age of onset was observed in the offspring of PC patients (median: 57 vs. 69 years), indi- cating anticipation. Mutation analyses of BRCA2, PALB2, CDKN2a, RNASEL, STK11, NOD2, CHEK2 and PALLD, revealed deleterious causative germline mutations of BRCA2 and PALB2 in 2 of 70 (3%) and 2 of 41 (4.9%) German FPC families, respectively. Prospective PC screening with EUS, MRI and MRCP detected precancer- ous lesions (IPMN, multifocal PanIN2/3) or carcinoma in 5.5% (4 of 72) to 12.5% (9 of 72) of individuals at risk, depending on histological verification. Appropriate inclu- sion of families at high risk for PC in registries, such as FaPaCa, provides a unique and excellent tool to gain clinical and genetic knowledge of FPC. Focused research projects can be conducted most efficiently, when data of different FPC registries are combined. Keywords Familial pancreatic cancer Á Genetic susceptibility Á Screening Á Hereditary tumor syndrome Introduction Pancreatic Cancer (PC) is a challenging tumor entity with an increasing incidence and a dismal prognosis. The overall five-year-survival rate is less than 5% attributed to late clinical symptoms, low resection rates and poor response to radio- and chemotherapy [1]. Long-time survivors are observed, but only if the tumor is diagnosed in its early stage [2]. An inherited predisposition to PC is currently believed to occur in three distinct clinical settings. First, it occurs in hereditary tumor predisposition syndromes such as Peutz- Jeghers-Syndrome (PJS), pancreatic-melanoma cancer- syndrome (PCMS) or familial-atypical multiple mole melanoma (FAMMM), hereditary breast and ovarian can- cer, Li-Fraumeni-syndrome and others. These syndromes are characterized by a clinical phenotype other than PC, but are known to be associated with an increased risk of PC. Hereditary pancreatitis and cystic fibrosis are the second setting; here genetically determined early changes of the pancreas can predispose to the development of PC. The risk for the development of PC in these diseases/syndromes, whose underlying gene defects are largely known, varies from \ 5% to up to 40% (Table 1). The third setting is R. Schneider Á E. P. Slater Á N. Habbe Á V. Fendrich Á E. Mattha ¨i Á P. Langer (&) Á D. K. Bartsch Department of Visceral, Thoracic and Vascular Surgery, Philipps University Marburg, Baldingerstrasse, 35043 Marburg, Germany e-mail: [email protected] M. Sina Institute of Clinical Genetics, Philipps University Marburg, Marburg, Germany 123 Familial Cancer (2011) 10:323–330 DOI 10.1007/s10689-010-9414-x
-
Upload
ralph-schneider -
Category
Documents
-
view
213 -
download
0
Transcript of German national case collection for familial pancreatic cancer (FaPaCa): ten years experience

German national case collection for familial pancreatic cancer(FaPaCa): ten years experience
Ralph Schneider • Emily P. Slater •
Mercede Sina • Nils Habbe • Volker Fendrich •
Elvira Matthai • Peter Langer • Detlef K. Bartsch
Published online: 5 January 2011
� Springer Science+Business Media B.V. 2011
Abstract Familial pancreatic cancer (FPC) is a rare
hereditary tumor syndrome. The 10-years experience of the
national case collection for familial pancreatic cancer of
Germany (FaPaCa) is reported. Since 1999 FaPaCa has
collected families with at least two first-degree relatives
with confirmed pancreatic cancer (PC), who did not fulfill
the criteria of other hereditary tumor syndromes. Histopa-
thological verification of tumor diagnoses, and genetic
counseling were prerequisites for enrollment of families in
FaPaCa. 94 of 452 evaluated families fulfilled the criteria
for partaking in FaPaCa. PC represented the sole tumor
entity in 38 (40%) families. In 56 families additional tumor
types occurred, including breast cancer (n = 28), colon
cancer (n = 20) and lung cancer (n = 11). In 70 (74%)
families the pattern of inheritance was consistent with an
autosomal dominant trait. Compared to the preceding
generation, a younger age of onset was observed in the
offspring of PC patients (median: 57 vs. 69 years), indi-
cating anticipation. Mutation analyses of BRCA2, PALB2,
CDKN2a, RNASEL, STK11, NOD2, CHEK2 and PALLD,
revealed deleterious causative germline mutations of
BRCA2 and PALB2 in 2 of 70 (3%) and 2 of 41 (4.9%)
German FPC families, respectively. Prospective PC
screening with EUS, MRI and MRCP detected precancer-
ous lesions (IPMN, multifocal PanIN2/3) or carcinoma in
5.5% (4 of 72) to 12.5% (9 of 72) of individuals at risk,
depending on histological verification. Appropriate inclu-
sion of families at high risk for PC in registries, such as
FaPaCa, provides a unique and excellent tool to gain
clinical and genetic knowledge of FPC. Focused research
projects can be conducted most efficiently, when data of
different FPC registries are combined.
Keywords Familial pancreatic cancer � Genetic
susceptibility � Screening � Hereditary tumor syndrome
Introduction
Pancreatic Cancer (PC) is a challenging tumor entity with
an increasing incidence and a dismal prognosis. The overall
five-year-survival rate is less than 5% attributed to late
clinical symptoms, low resection rates and poor response to
radio- and chemotherapy [1]. Long-time survivors are
observed, but only if the tumor is diagnosed in its early
stage [2].
An inherited predisposition to PC is currently believed
to occur in three distinct clinical settings. First, it occurs in
hereditary tumor predisposition syndromes such as Peutz-
Jeghers-Syndrome (PJS), pancreatic-melanoma cancer-
syndrome (PCMS) or familial-atypical multiple mole
melanoma (FAMMM), hereditary breast and ovarian can-
cer, Li-Fraumeni-syndrome and others. These syndromes
are characterized by a clinical phenotype other than PC, but
are known to be associated with an increased risk of PC.
Hereditary pancreatitis and cystic fibrosis are the second
setting; here genetically determined early changes of the
pancreas can predispose to the development of PC. The risk
for the development of PC in these diseases/syndromes,
whose underlying gene defects are largely known, varies
from \5% to up to 40% (Table 1). The third setting is
R. Schneider � E. P. Slater � N. Habbe � V. Fendrich �E. Matthai � P. Langer (&) � D. K. Bartsch
Department of Visceral, Thoracic and Vascular Surgery, Philipps
University Marburg, Baldingerstrasse, 35043 Marburg, Germany
e-mail: [email protected]
M. Sina
Institute of Clinical Genetics, Philipps University Marburg,
Marburg, Germany
123
Familial Cancer (2011) 10:323–330
DOI 10.1007/s10689-010-9414-x

familial pancreatic cancer (FPC) which is applied to fam-
ilies with two or more first-degree relatives with PC that do
not fulfill the criteria for another inherited tumor syndrome
[3]. Some groups also use the term FPC for families with
PC in three or more relatives of any degree [4, 5].
Initially, several case reports of familial aggregation of
PC suggested the existence of hereditary pancreatic cancer
[6–8]. In 1989, Lynch was the first to publish a systematic
study of a larger cohort of 18 families with PC [9]. Sub-
sequently, national and international tumor registries such
as the North American National Familial Pancreatic Tumor
Registry (NFPTR), the German National Case Collection
of Familial Pancreatic Cancer (FaPaCa) and the European
Registry of Hereditary Pancreatitis and Familial Pancreatic
Cancer (EUROPAC) were established to collect data on
FPC families [5, 10–12]. Based on the strict inclusion
criteria of confirmation of the PC diagnosis by histopa-
thology and medical reports, a familial aggregation of PC
was reported to be only 2.7 and 1.9% in two prospective
studies from Sweden and Germany, respectively [13, 14].
In order to investigate the clinical and genetic charac-
teristics of FPC, the German national case collection for
familial pancreatic cancer (FaPaCa) was established in
1999. Here, we report the 10-years experience of this
collection and the concept of genetic and clinical screening
of family members at risk.
Patients and methods
The FaPaCa registry is a national case collection for
familial pancreatic cancer families funded by the Deutsche
Krebshilfe (Grant 106 925). Families with two or more
first-degree relatives with a confirmed diagnosis of PC and
without evidence of any other inherited tumor syndrome
were collected. Families with an occurrence of melanoma
or PC in two first-degree relatives representing the FAM-
MM or PCMS-syndrome, were also collected in FaPaCa,
but not analyzed in this report.
Multiple centers contributed to the establishment of
FaPaCa which is coordinated by the Philipps University of
Marburg in Germany and has been described in detail in
previous publications [10, 13]. Members from FPC fami-
lies were recruited between July 1999 and July 2009 by
direct referral via their physicians or by personal contact to
the FaPaCa study-office based on information about the
study, e.g. via the internet (http://www.fapaca.de). All
eligible persons and families were genetically counseled by
a genetic counselor (M.S.) and a three-generation family
pedigree was constructed. All participating persons
underwent a physical examination. All cancer diagnoses
were confirmed by review of medical and pathological
records, deaths certificates and by examination of the
pathology slides whenever available.
All diseased index patients of FPC families were sub-
jected to mutation analysis of the genes BRCA2, CDKN2a,
PALB2, PLLD, CHEK2, RNASEL, NOD2 and STK11 as
described previously [15–22]. If a germline mutation was
identified in the index patient, predictive genetic testing of
this mutation was offered to all family members after
genetic counseling. The result of the predictive testing was
revealed to the family members during another interdisci-
plinary counseling, involving a geneticist, a psychologist, a
surgeon and gastroenterologist.
Individuals at risk (IAR) older than 18 years were
encouraged to participate in a prospective screening pro-
gram that was conducted at our institution. The screening
started 10 years before the earliest age of onset of PC in the
family or at age 40 years, whichever was first. The fol-
lowing individuals from families registered in FaPaCa
were classified as IAR and encouraged to participate in the
study:
Table 1 Cumulative lifetime
risk of PC in the different
settings of inherited PC
FAMMM-syndrome familial
atypical multiple mole-
melanoma syndrome
Setting of inherited PC Gene PC-risk (%)
until 70 years
1. Hereditary tumor predisposition syndromes
Peutz-Jeghers syndrome LKB1 36
FAMMM syndrome CDKN2a 17
Hereditary breast and ovarian cancer BRCA1, BRCA2 3–8
Li-Fraumeni TP53 \5
Hereditary nonpolyposis colorectal carcinoma MLH1, MSH2 \5
Familial adenomatous polyposis APC \5
Ataxia telangiectasia ATM \5
2. Tumor syndromes with chronic inflammation/dysfunction of the gland
Hereditary Pancreatitis PRSS1, SPINK1 40
Cystic fibrosis CFTR \5
3. FPC-syndrome BRCA2, PALB2,…? *40
324 R. Schneider et al.
123

– first-degree relative of an affected patient of a FPC
family;
– members of a FPC-family carrying a predisposing
mutation such as BRCA2, PALB2 or CDKN2a, inde-
pendent of the degree of relationship.
The FaPaCa registry was approved by the Ethics Com-
mittee of the Philipps-University of Marburg (36/1997, last
amendment 2009) and all participants provided written
informed consent.
Results
In a 10-year period, 452 potential FPC families were
admitted to the study office of FaPaCa. After genetic
counseling of the index patient, it was possible to obtain
contact with 284 families. More than half (58%, n = 167)
of potential FPC families were not included in FaPaCa for
different reasons: a, family members denied participation in
the project, so that anamnestic data could not be confirmed
(n = 57, 34%); b, histological verification of the diagnosis
was not possible due to the lack of medical records of
family members deceased for more than 20 years (n = 48,
29%); c, pedigree evaluation showed that affected family
members were not first-degree relatives (n = 42, 25%), d,
examination of histological reports revealed a pathology
other than ductal pancreatic adenocarcinoma (n = 20,
12%). Five families are still under evaluation. Eighteen
pancreatic cancer/melanoma-prone (PCMS) families were
not analyzed in the current study, since these were recently
published as a separate disease entity [23].
So far, 94 FPC families fulfilled the inclusion criteria
and underwent genetic counseling, including the prepara-
tion of a three-generation pedigree. A representative family
is shown in Fig. 1. All families were Caucasian with none
reporting Ashkenazi Jewish heritage. A total of 442 family
members underwent genetic counseling and physical
examination with median 4 (range 1–29) family members
counseled. Blood was collected from 421 family members,
of whom 67 were affected with PC. Pancreatic tumor tissue
could be collected from 40 FPC patients.
Of the 94 verified FPC families, 38 (40%) revealed only
PC. Twenty-eight (30%) families showed both PC and
breast cancer. In two of these families 3 female patients
developed both tumors, synchronous and metachronous.
PC and colon cancer occurred in 20 (21%) families, PC and
lung cancer in 11 (12%) families, PC and prostate cancer in
6 (6%) families, and PC and other tumor types in 7 (7%)
families, respectively (Table 2). Four (4%) families
revealed an accumulation of family members with insulin-
dependent diabetes mellitus and five families (5%) had a
history of pancreatitis. Of the 94 FPC families, 1 family
had 5 affected members with PC, 11 families had 4, 9
families had 3 and 73 families had two affected members.
Three generations were affected in 3 families, two gener-
ations in 67 families and 1 generation was affected in 24
families. Among patients affected with PC were 116 males
and 106 females. The median age of diagnosis of PC was
63 years (range 31–91). Thirty-five (16%) of the affected
PC patients had a young age of onset of the disease
Fig. 1 Representative FPC
family with an isolated
accumulation of PC. Four
patients in two generations are
affected (y years of age; dg age
at diagnosis)
Table 2 Tumor combinations reported in our 94 FPC families
Tumor combinations Number of affected families
PC only 38/94 40.4%
PC ? breast cancer 28/94 29.8%
PC ? colorectal cancer 20/94 21.3%
PC ? lung cancer 11/94 11.7%
PC ? prostate cancer 6/94 6.4%
PC ? other tumor types 7/94 7.5%
PC pancreatic cancer; other tumor types include: endometrial, tes-
ticular and gastric cancer; lymphoma, melanoma and brain tumor
German national case collection for familial pancreatic cancer (FaPaCa) 325
123

(\50 years). In 70 families with 2 or more affected gen-
erations the age at onset revealed a shift towards an earlier
age in the younger generations (median 69 years, range
42–91 years vs. median 57 years, range 31–81 years). An
analysis of 80 parent/child pairs from EUROPAC and
FaPaCa registries had already demonstrated a significant
shift towards an earlier age of death of about 10 years
(70 years vs. 64 years vs. 49 years) in the younger gener-
ations, indicating anticipation in 85% of families [24].
We performed mutation analyses of potential causative
candidate genes, either in our cohort of families or by
pooling families with the EUROPAC registries or the
Polish case collection (Szczecin registry) [20]. In a first
step only affected patients were screened for germline
mutations. Initially, we identified BRCA2 mutations in 5 of
26 (15%) of European FPC families [15]. The current
status of 70 analyzed German families showed deleterious
BRCA2 mutations in only 3% (2 families) and unclassified
variants of unknown clinical importance in 8.6% (6 fami-
lies) [25]. PALB2 mutations have been detected in 2 of 41
(5%) analyzed German families [22]. CDKN2a mutations
were only identified in 2 of 18 PC/melanoma-prone fami-
lies, so called PCMS or FAMMM-PC families [23], but in
none of the FPC families without melanoma. None or non
deleterious germline alterations could be identified in
PALLD [21], RNASEL [16], STK11 [19], CHEK2 [17] and
NOD2 [20] genes. In total, 4 (2/70 BRCA2 and 2/41
PALB2) of the FPC families carried deleterious causative
germline mutations and another 6 families had unclassified
variants of BRCA2, that might have clinical importance.
Eighty-eight family members of these 10 families under-
went predictive genetic testing after genetic counseling and
35 mutation carriers were identified.
The participation in a clinical screening program for the
early detection of PC was recommended to 207 IAR of
FPC families. The screening program was restricted to
mutation carriers, if the underlying gene defect was known
in the family. The screening program as outlined in
Algorithm 1 started 10 years before the earliest age of
onset in the family, at the latest by the age of 40 years. The
results of the first 5 years of prospective screening in FPC
and PCMS families from July 2002 until December 2007
were previously published [26]. After a 24 month extended
screening period (until December 2009, median follow-up
44 months) 72 IAR of FPC families participated in the
screening program with a total of 210 examination visits
(median 2, range 1–11). Forty-six IAR (63.9%) had a
normal pancreas based on the evaluation by endoscopic
ultrasound (EUS) and magnetic resonance imaging (MRI)
with MRCP. Twenty-six (36.1%) IAR showed lesions and/
or abnormalities in the pancreas, of whom 10 were oper-
ated on and 16 IAR, including 5 with potential side branch
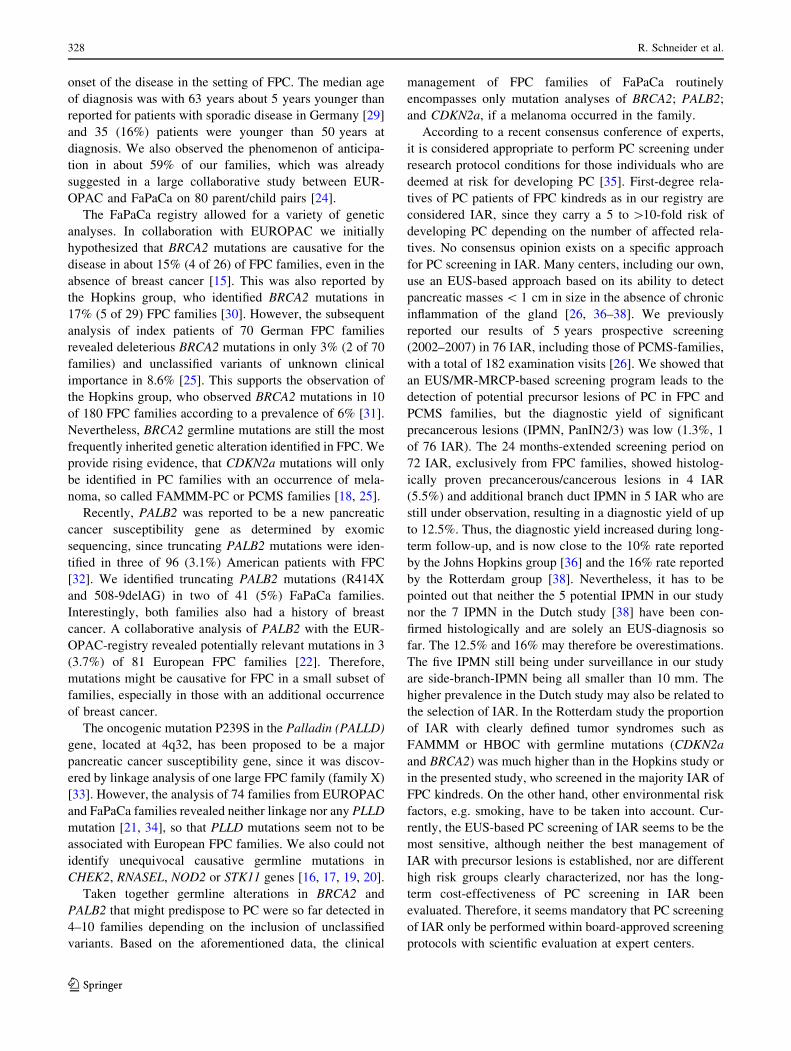
IPMN (Fig. 2), are under close observation. In one patient
surgical exploration could not confirm the small hypoech-
oic lesion seen in EUS, therefore no pancreatic resection
was carried out. Nine IAR underwent pancreatic resection
and had the following pathologies: PC (n = 1), serous
cystadenoma (n = 3), PanIN3 (n = 1), IPMN (n = 2),
PanIN1/2 lesions (n = 2). Interestingly, one patient with
IPMN also revealed multifocal PanIN2 lesions (Table 3).
These resulted in a diagnostic yield of malignant (PC) or
potentially malignant precursor lesions of PC (IPMN, Pa-
nIN3, multifocal PanIN2) between 5.5% (4 of 72) to 12.5%
(9 of 72), depending on inclusion of the 5 IAR with branch
duct IPMNs on imaging.
Algorithm 1 Screening-algorithm of the FaPaCa prospective
screening program for PC
Fig. 2 MRI image of an IAR showing suspicious lesions for IPMN
(arrows). The postoperative histopathological examination of the
resected pancreatic specimen revealed IPMN and multifocal PanIN2
lesions
326 R. Schneider et al.
123

Discussion
A registry for FPC allows for the testing and refining of
assumptions on the epidemiology of the disease. Moreover,
the registry may be used to test novel screening modalities
to identify early, resectable tumors providing tissue sam-
ples that can reveal vital features of the early stages of the
disease, or even better, its precursor lesions. Finally, reg-
istries allow for linkage and association studies to identify
novel mutations or polymorphisms that predispose to PC.
These motives for establishing a registry for FPC have
ensured that many have been created, most of which have
remained small. However, size is critical if the registry is
intended to supply solid epidemiological and genetic data.
The National Familial Pancreas Tumor Registry (NFPTR)
based at Johns Hopkins University is the largest and reg-
istered up until December 2008 2,505 FPC families with at
least 2 first-degree relatives (http://pathology.jhu.edu.
pancreas/PartNFPTR.php). The European Registry of
Familial Pancreatic Cancer and Hereditary Pancreatitis
(EUROPAC), coordinated in Liverpool, UK and Greifs-
wald, Germany) had collected 233 FPC families with two
or more PC cases by February 2008. FaPaCa is the third
largest FPC collection and collaborates closely with the
EUROPAC registry regarding epidemiological and genetic
data [15, 16, 19, 21, 24] to strengthen the results and
conclusions of the respective studies.
Over a 10 year period, FaPaCa evaluated 452 potential
FPC families, but only 94 could be enrolled in the registry.
It is a major effort in Germany to obtain contact with the
family and the permission to verify the tumor diagnosis of
family members by pathology and medical reports. More
than 30% of eligible families did not want to participate in
the registry. Furthermore, about 41% of families could not
be included, because the PC diagnosis either could not be
confirmed as pathological reports were no longer available
(29%) or the PC diagnosis was incorrect (12%). However,
we insisted on verification of the PC diagnosis to ensure
that the families were true FPC families, whereas other
groups do not require histological confirmation or first-
degree relationship [12, 27]. We strongly believe that
verification of the PC diagnosis is important for any epi-
demiologic or genetic analysis, as well as for the risk
adjustment and screening recommendations of family
members.
The phenotypic appearance of our FPC families fits well
into the concept that FPC generally can be divided into
groups, namely pure PC families and those associated with
other tumor types. The three most frequent other tumor
types were breast cancer (30%), colon cancer (21%) and
lung cancer (12%). This observation is similar to the
reports from other groups [9, 12]. Whether this is a hint for
a common predisposing gene defect (e.g. BRCA2,
CDKN2a) or just chance, given the high prevalence of
these tumors in the German population, remains specula-
tive. The pattern of inheritance was consistent with an
autosomal dominant trait in 70 families (74%), comple-
mentary to that reported by the EUROPAC registry (58%,
125/233) [28]. In contrast to previous studies from the
United States [3, 4] there seems to be an earlier age of
Table 3 Characteristics of IAR operated on for pancreatic lesions
ID, age at surgery Sex Surgery Pathology Morbidity Follow-up F-up
[mo]
25-4-25-204, 44 f Exploration, liver-
wedge
No pancreatic tumor, FNH in specimen of the liver None Incisional
hernia
118
25-2-28-204, 61 f DP ? SE Serous oligocystic adenoma Fistula No pathologies 76
25-7-85-2, 61 f DP ? SE Serous oligocystic adenoma,
lobular fibrosis with PanIN1
None Cystic lesion
pancreatic head
(prev. known)
85
25-7-41-109, 54 m SPDP Focal fibrosis with
PanIN1/2 lesions
Fistula No pathologies 69
25-4-5-2, 42 f SPDP Serous oligocystic adenoma None No pathologies 40
25-1-91-1, 54 m DP ? SE Lobular Fibrosis with PanIN1 ? sqamous
metaplasia
None No pathologies 37
25-5-67-24, 53 f SPDP Lobular fibrosis with PanIN1 ? gastric type IPMN None NIDDM 30
25-5-67-26, 52 f TP Pancreatic cancer Diabetes Lung metastasis 12
25-4-48-206, 58 f TP Multifocal PanIN2 ? IPMN Diabetes No pathologies 4
25-5-67-28, 51 f TP PanIN3 ? multifocal PanIN1/2 Diabetes No pathologies 3
F-up follow-up time, liver-wedge liver-wedge-resection, FNH focal nodular hyperplasia, DP ? SE distal pancreatectomy ? splenectomy, SPDPspleen preserving distal pancreatectomy, TP total pancreatectomy, IPMN intraductal pancreatic mucinous neoplasia, NIDDM non insulin
dependent diabetes mellitus, fistula postoperative pancreatic fistula (conservatively treated), prev. known previously known
German national case collection for familial pancreatic cancer (FaPaCa) 327
123
onset of the disease in the setting of FPC. The median age
of diagnosis was with 63 years about 5 years younger than
reported for patients with sporadic disease in Germany [29]
and 35 (16%) patients were younger than 50 years at
diagnosis. We also observed the phenomenon of anticipa-
tion in about 59% of our families, which was already
suggested in a large collaborative study between EUR-
OPAC and FaPaCa on 80 parent/child pairs [24].
The FaPaCa registry allowed for a variety of genetic
analyses. In collaboration with EUROPAC we initially
hypothesized that BRCA2 mutations are causative for the
disease in about 15% (4 of 26) of FPC families, even in the
absence of breast cancer [15]. This was also reported by
the Hopkins group, who identified BRCA2 mutations in
17% (5 of 29) FPC families [30]. However, the subsequent
analysis of index patients of 70 German FPC families
revealed deleterious BRCA2 mutations in only 3% (2 of 70
families) and unclassified variants of unknown clinical
importance in 8.6% [25]. This supports the observation of
the Hopkins group, who observed BRCA2 mutations in 10
of 180 FPC families according to a prevalence of 6% [31].
Nevertheless, BRCA2 germline mutations are still the most
frequently inherited genetic alteration identified in FPC. We
provide rising evidence, that CDKN2a mutations will only
be identified in PC families with an occurrence of mela-
noma, so called FAMMM-PC or PCMS families [18, 25].
Recently, PALB2 was reported to be a new pancreatic
cancer susceptibility gene as determined by exomic
sequencing, since truncating PALB2 mutations were iden-
tified in three of 96 (3.1%) American patients with FPC
[32]. We identified truncating PALB2 mutations (R414X
and 508-9delAG) in two of 41 (5%) FaPaCa families.
Interestingly, both families also had a history of breast
cancer. A collaborative analysis of PALB2 with the EUR-
OPAC-registry revealed potentially relevant mutations in 3
(3.7%) of 81 European FPC families [22]. Therefore,
mutations might be causative for FPC in a small subset of
families, especially in those with an additional occurrence
of breast cancer.
The oncogenic mutation P239S in the Palladin (PALLD)
gene, located at 4q32, has been proposed to be a major
pancreatic cancer susceptibility gene, since it was discov-
ered by linkage analysis of one large FPC family (family X)
[33]. However, the analysis of 74 families from EUROPAC
and FaPaCa families revealed neither linkage nor any PLLD
mutation [21, 34], so that PLLD mutations seem not to be
associated with European FPC families. We also could not
identify unequivocal causative germline mutations in
CHEK2, RNASEL, NOD2 or STK11 genes [16, 17, 19, 20].
Taken together germline alterations in BRCA2 and
PALB2 that might predispose to PC were so far detected in
4–10 families depending on the inclusion of unclassified
variants. Based on the aforementioned data, the clinical
management of FPC families of FaPaCa routinely
encompasses only mutation analyses of BRCA2; PALB2;
and CDKN2a, if a melanoma occurred in the family.
According to a recent consensus conference of experts,
it is considered appropriate to perform PC screening under
research protocol conditions for those individuals who are
deemed at risk for developing PC [35]. First-degree rela-
tives of PC patients of FPC kindreds as in our registry are
considered IAR, since they carry a 5 to [10-fold risk of
developing PC depending on the number of affected rela-
tives. No consensus opinion exists on a specific approach
for PC screening in IAR. Many centers, including our own,
use an EUS-based approach based on its ability to detect
pancreatic masses \ 1 cm in size in the absence of chronic
inflammation of the gland [26, 36–38]. We previously
reported our results of 5 years prospective screening
(2002–2007) in 76 IAR, including those of PCMS-families,
with a total of 182 examination visits [26]. We showed that
an EUS/MR-MRCP-based screening program leads to the
detection of potential precursor lesions of PC in FPC and
PCMS families, but the diagnostic yield of significant
precancerous lesions (IPMN, PanIN2/3) was low (1.3%, 1
of 76 IAR). The 24 months-extended screening period on
72 IAR, exclusively from FPC families, showed histolog-
ically proven precancerous/cancerous lesions in 4 IAR
(5.5%) and additional branch duct IPMN in 5 IAR who are
still under observation, resulting in a diagnostic yield of up
to 12.5%. Thus, the diagnostic yield increased during long-
term follow-up, and is now close to the 10% rate reported
by the Johns Hopkins group [36] and the 16% rate reported
by the Rotterdam group [38]. Nevertheless, it has to be
pointed out that neither the 5 potential IPMN in our study
nor the 7 IPMN in the Dutch study [38] have been con-
firmed histologically and are solely an EUS-diagnosis so
far. The 12.5% and 16% may therefore be overestimations.
The five IPMN still being under surveillance in our study
are side-branch-IPMN being all smaller than 10 mm. The
higher prevalence in the Dutch study may also be related to
the selection of IAR. In the Rotterdam study the proportion
of IAR with clearly defined tumor syndromes such as
FAMMM or HBOC with germline mutations (CDKN2a
and BRCA2) was much higher than in the Hopkins study or
in the presented study, who screened in the majority IAR of
FPC kindreds. On the other hand, other environmental risk
factors, e.g. smoking, have to be taken into account. Cur-
rently, the EUS-based PC screening of IAR seems to be the
most sensitive, although neither the best management of
IAR with precursor lesions is established, nor are different
high risk groups clearly characterized, nor has the long-
term cost-effectiveness of PC screening in IAR been
evaluated. Therefore, it seems mandatory that PC screening
of IAR only be performed within board-approved screening
protocols with scientific evaluation at expert centers.
328 R. Schneider et al.
123

The question as to which surgical procedure should be
used once a reproducible pancreatic lesion is diagnosed in
an asymptomatic IAR also remains unresolved. Some
centers advocate total pancreatectomy, if the imaginable
lesions were intraoperatively confirmed as preneoplastic or
cancerous lesion by frozen section [39]. The rationale for
this approach is that IAR often have multifocal precursor
lesions or neoplasia. This excludes any type of operation
that would leave behind pancreatic tissue [13]. Based on
the available screening data, we and others [37, 38] offer
IAR partial pancreatectomy to avoid both, overtreatment
and the significant drawbacks of total pancreatectomy such
as brittle diabetes. We first resect the part of the pancreas
that contains the suspicious lesion(s) and only proceed to
total pancreatectomy, if the frozen section diagnoses a PC
or multifocal high grade PanIN or IPMN.
In summary, the collection and careful clinical investi-
gation of FPC families, as in FaPaCa, provide the basis for
identifying the underlying gene defect(s) and the assess-
ment of the PC risk of family members. Screening and
potentially future chemoprevention strategies for IAR can
be evaluated in a board approved clinical research setting.
In addition, IAR from FPC families can be investigated for
a variety of environmental factors that may modulate the
deleterious cancer-prone phenotype. Most importantly,
focused research projects can be conducted most efficiently
and profoundly when data from the various FPC registries,
as demonstrated by EUROPAC and FaPaCa, are combined.
Acknowledgments We are grateful to all FPC families for partic-
ipating in the registry. This study was supported by grants 70-2362-
Ba2, 70-2828-Ba3 and 103709 of the Deutsche Krebshilfe.
References
1. Cooperman AM (2001) Pancreatic cancer: the bigger picture.
Surg Clin North Am 81:557–574
2. Cleary SP, Gryfe R, Guindi M et al (2004) Prognostic factors in
resected pancreatic adenocarcinoma: analysis of actual 5-year
survivors. J Am Coll Surg 198:722–731
3. Hruban RH, Petersen GM, Ha PK et al (1998) Genetics of pan-
creatic cancer. From genes to families. Surg Oncol Clin N Am
7:1–23
4. Lynch HT, Brand RE, Deters CA et al (2001) Hereditary pan-
creatic cancer. Pancreatology 1:466–471
5. Applebaum SE, Kant JA, Whitcomb DC et al (2000) Genetic
testing. Counseling, laboratory, and regulatory issues and the
EUROPAC protocol for ethical research in multicenter studies of
inherited pancreatic diseases. Med Clin North Am 84:575–588
viii
6. Ehrenthal D, Haeger L, Griffin T et al (1987) Familial pancreatic
adenocarcinoma in three generations. A case report and a review
of the literature. Cancer 59:1661–1664
7. MacDermott RP, Kramer P (1973) Adenocarcinoma of the pan-
creas in four siblings. Gastroenterology 65:137–139
8. Reimer RR, Fraumeni JF Jr, Ozols RF et al (1977) Pancreatic
cancer in father and son. Lancet 1:911
9. Lynch HT, Lanspa SJ, Fitzgibbons RJ Jr et al (1989) Familial
pancreatic cancer (part 1): genetic pathology review. Nebr Med J
74:109–112
10. Bartsch DK, Sina-Frey M, Ziegler A et al (2001) Update of
familial pancreatic cancer in Germany. Pancreatology 1:510–516
11. Tersmette AC, Petersen GM, Offerhaus GJ et al (2001) Increased
risk of incident pancreatic cancer among first-degree relatives of
patients with familial pancreatic cancer. Clin Cancer Res
7:738–744
12. Hruban RH, Petersen GM, Goggins M et al (1999) Familial
pancreatic cancer. Ann Oncol 10(Suppl 4):69–73
13. Bartsch DK, Kress R, Sina-Frey M et al (2004) Prevalence of
familial pancreatic cancer in Germany. Int J Cancer 110:902–906
14. Hemminki K, Li X (2003) Familial and second primary pancre-
atic cancers: a nationwide epidemiologic study from Sweden. Int
J Cancer 103:525–530
15. Hahn SA, Greenhalf B, Ellis I et al (2003) BRCA2 germline
mutations in familial pancreatic carcinoma. J Natl Cancer Inst
95:214–221
16. Bartsch DK, Fendrich V, Slater EP et al (2005) RNASEL
germline variants are associated with pancreatic cancer. Int J
Cancer 117:718–722
17. Bartsch DK, Krysewski K, Sina-Frey M et al (2006) Low fre-
quency of CHEK2 mutations in familial pancreatic cancer. Fam
Cancer 5:305–308
18. Bartsch DK, Sina-Frey M, Lang S et al (2002) CDKN2A germ-
line mutations in familial pancreatic cancer. Ann Surg
236:730–737
19. Grutzmann R, McFaul C, Bartsch DK et al (2004) No evidence
for germline mutations of the LKB1/STK11 gene in familial
pancreatic carcinoma. Cancer Lett 214:63–68
20. Nej K, Bartsch DK, Sina-Frey M et al (2004) The
NOD23020insC mutation and the risk of familial pancreatic
cancer? Hered Cancer Clin Pract 2:149–150
21. Slater E, Amrillaeva V, Fendrich V et al (2007) Palladin mutation
causes familial pancreatic cancer: absence in European families.
PLoS Med 4:e164
22. Slater EP, Langer P, Habbe N et al. (2010) Prevalence of PALB2
mutations in familial pancreatic cancer. Clin Genet (in press)
23. Bartsch DK, Langer P, Habbe N et al. (2009) Clinical and genetic
analysis of 18 pancreatic carcinoma/melanoma-prone families.
Clin Genet 77:333–341
24. McFaul CD, Greenhalf W, Earl J et al (2006) Anticipation in
familial pancreatic cancer. Gut 55:252–258
25. Slater EP, Langer P, Fendrich V et al. (2010) Prevalence of
BRCA2 and CDKN2a mutations in German familial pancreatic
cancer families. Fam Cancer 9:335–343
26. Langer P, Kann PH, Fendrich V et al (2009) Five years of pro-
spective screening of high-risk individuals from families with
familial pancreatic cancer. Gut 58:1410–1418
27. Lynch HT, Fusaro L, Smyrk TC et al (1995) Medical genetic
study of eight pancreatic cancer-prone families. Cancer Invest
13:141–149
28. Greenhalf W, Malats N, Nilsson M et al (2008) International
registries of families at high risk of pancreatic cancer. Pancrea-
tology 8:558–565
29. Schuz J, Schon D, Batzler W et al (2000) Cancer registration in
Germany: current status, perspectives and trends in cancer inci-
dence 1973–93. J Epidemiol Biostat 5:99–107
30. Murphy KM, Brune KA, Griffin C et al (2002) Evaluation of
candidate genes MAP2K4, MADH4, ACVR1B, and BRCA2 in
familial pancreatic cancer: deleterious BRCA2 mutations in 17%.
Cancer Res 62:3789–3793
31. Couch FJ, Johnson MR, Rabe KG et al (2007) The prevalence of
BRCA2 mutations in familial pancreatic cancer. Cancer Epi-
demiol Biomark Prev 16:342–346
German national case collection for familial pancreatic cancer (FaPaCa) 329
123

32. Jones S, Hruban RH, Kamiyama M et al (2009) Exomic
sequencing identifies PALB2 as a pancreatic cancer susceptibility
gene. Science 324:217
33. Pogue-Geile KL, Chen R, Bronner MP et al (2006) Palladin
mutation causes familial pancreatic cancer and suggests a new
cancer mechanism. PLoS Med 3:e516
34. Earl J, Yan L, Vitone LJ et al (2006) Evaluation of the 4q32–34
locus in European familial pancreatic cancer. Cancer Epidemiol
Biomark Prev 15:1948–1955
35. Brand RE (2009) Screening for familial pancreatic cancer: is
doing something better than doing nothing? Gut 58:1321–1322
36. Canto MI, Goggins M, Yeo CJ et al (2004) Screening for pan-
creatic neoplasia in high-risk individuals: an EUS-based
approach. Clin Gastroenterol Hepatol 2:606–621
37. Canto MI, Goggins M, Hruban RH et al (2006) Screening for
early pancreatic neoplasia in high-risk individuals: a prospective
controlled study. Clin Gastroenterol Hepatol 4:766–781
38. Poley JW, Kluijt I, Gouma DJ et al (2009) The yield of first-time
endoscopic ultrasonography in screening individuals at a high
risk of developing pancreatic cancer. Am J Gastroenterol
104:2175–2181
39. Brentnall TA (2005) Management strategies for patients with
hereditary pancreatic cancer. Curr Treat Options Oncol
6:437–445
330 R. Schneider et al.
123


















