
Generalized herpes simplex in malnourished children · to have generalized oedema and skin rash...
6
J. clin. Path., 1970, 23, 24-30 Generalized herpes simplex in malnourished children A. C. TEMPLETON From the Department of Pathology, Makerere University College, Kampala, Uganda SYNOPSIS Five cases of fatal generalized herpes simplex infection in malnourished children are described. This is almost certainly a much more common disease in underdeveloped communities than is at present appreciated. Only a greater awareness of the disease, coupled with full use of histological and cultural methods of diagnosis, will lead to knowledge of its true frequency. A case of neonatal infection, the first recorded in an African, is also described. Reasons are suggested as to why this disease should be seen in malnourished infants in Africa but only very rarely in neonates. Although infection with herpes simplex virus is very common, fatal generalized disease is apparently a rare phenomenon, and the first description of a case is usually accredited to Hass (1935). In cases reported from Europe and America it has occurred most frequently in the neonatal period, but in a few instances older children have been affected (Zuelzer and Stuhlberg, 1952). In Africa, however, most cases seem to occur in children between the ages of 2 and 26 months, and are most frequently associated with kwashior- kor or other forms of malnutrition. Many of these children have also had some other viral infection, such as measles, in the recent past. McKenzie and his coworkers (Becker, Naud6, Kipps, and MacKenzie, 1963; Kipps, Becker, Wainwright, and MacKenzie, 1967) have seen many cases at necropsy in Durban and Cape Town and state Received for publication 23 April 1969. that this disease has been seen frequently by their colleagues in South Africa. They record that generalized herpes in association with meas- les has been noted in Dakar, Senegal, but apparent- ly not elsewhere. The South African group ex- press the view 'we do not believe that these are the only cities where this disease is to be found'. Six cases seen in Kampala, Uganda, are here recorded. Materials and Methods A case of generalized herpes virus infection (case 6) was seen at necropsy at Mulago Hospital, Kampala, in March 1968. The diagnosis was confirmed by virus isolation. Since the histo- logical features of the disease are often sufficiently on June 29, 2020 by guest. Protected by copyright. http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.23.1.24 on 1 February 1970. Downloaded from
Transcript of Generalized herpes simplex in malnourished children · to have generalized oedema and skin rash...

J. clin. Path., 1970, 23, 24-30
Generalized herpes simplex inmalnourished children
A. C. TEMPLETONFrom the Department of Pathology, Makerere University College, Kampala, Uganda
SYNOPSIS Five cases of fatal generalized herpes simplex infection in malnourished childrenare described. This is almost certainly a much more common disease in underdevelopedcommunities than is at present appreciated. Only a greater awareness of the disease, coupledwith full use of histological and cultural methods of diagnosis, will lead to knowledge of itstrue frequency.A case of neonatal infection, the first recorded in an African, is also described. Reasons are
suggested as to why this disease should be seen in malnourished infants in Africa but onlyvery rarely in neonates.
Although infection with herpes simplex virusis very common, fatal generalized disease isapparently a rare phenomenon, and the firstdescription of a case is usually accredited to Hass(1935). In cases reportedfrom Europe and Americait has occurred most frequently in the neonatalperiod, but in a few instances older children havebeen affected (Zuelzer and Stuhlberg, 1952). InAfrica, however, most cases seem to occur inchildren between the ages of 2 and 26 months,and are most frequently associated with kwashior-kor or other forms of malnutrition. Many of thesechildren have also had some other viral infection,such as measles, in the recent past. McKenzieand his coworkers (Becker, Naud6, Kipps, andMacKenzie, 1963; Kipps, Becker, Wainwright,and MacKenzie, 1967) have seen many cases atnecropsy in Durban and Cape Town and stateReceived for publication 23 April 1969.
that this disease has been seen frequently bytheir colleagues in South Africa. They recordthat generalized herpes in association with meas-les has been noted in Dakar, Senegal, but apparent-ly not elsewhere. The South African group ex-press the view 'we do not believe that these arethe only cities where this disease is to be found'.Six cases seen in Kampala, Uganda, are hererecorded.
Materials and Methods
A case of generalized herpes virus infection(case 6) was seen at necropsy at Mulago Hospital,Kampala, in March 1968. The diagnosis wasconfirmed by virus isolation. Since the histo-logical features of the disease are often sufficiently
on June 29, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.23.1.24 on 1 F
ebruary 1970. Dow
nloaded from

Generalized herpes simplex in malnourished children
distinctive to make a firm diagnosis withoutculture, a search was made of the records of post-mortem examinations performed in the Depart-ment of Pathology, Makerere University MedicalSchool, from 1962 to 1967. A total of 5,300 casereports was scrutinized and any in which necrosisof, or haemorrhage into, the liver or adrenal wasmentioned, were re-examined. Fresh slides fromthese cases were cut and stained with haematoxy-lin and eosin, PAS, Feulgen, and methyl greenpyronin methods. In those cases in which a firmdiagnosis was possible, the clinical notes wereexamined. A total of six cases was found by thesemeans.
Case Reports
Brief details of the history
necropsy are given below.
and findings at
CASE 1
A 4-year-old African male child was admittedwith a history of two weeks' generalized oedema.On examination he was noted to have the classicalsigns of kwashiorkor. Haemoglobin on admissionwas noted as 9 2g %. He was treated withaspecialdiet rich in protein. He appeared to be improvingbut after three weeks in hospital suddenly devel-oped a sore mouth which was followed two dayslater by a generalized skin rash which appearedvesicular. He developed a high temperature andsigns of pneumonia were noted and the haemo-globin had fallen to 6-0g %. He died two dayslater.Postmortem examination showed an under-
nourished child with generalized oedema. Alarge number of small round ulcers were seenon arms, legs, scalp, and back. These were mostlylocated in the flexures. Ulcers were also foundin the mouth and throat. Numerous small ulcerswere seen in the small and large intestines butall the other organs were as usually found in achild with kwashiorkor. Microscopy showedtypical lesions of herpes simplex in the mouth,tongue, small and large intestines and in the liver,spleen, and adrenals. The lungs showed the chan-ges of bronchopneumonia. The brain was essen-tially normal.
CASE 2An 18-month-old male infant from Burundi wasadmitted with severe kwashiorkor. He was notedto have generalized oedema and skin rash withulceration, most marked in the flexures. His mouthwas noted to be sore and after three days inhospital he was found to have ulcers on the lipsand tongue. On the fourth hospital day, the tem-perature rose to 103°F and he had a convulsion;lumbar puncture was done and the cerebro-
spinal fluid was normal. The child died the nextday.At necropsy, the skin rash was found to have
healed but ulcers were noted on the lips andtongue. The liver was pale and greasy and numer-ous small haemorrhages were seen under thecapsule. Other organs appeared macroscopicallynormal. Microscopically typical lesions werefound in the mouth and liver. The brain, lungs,and adrenal were normal.
CASE 3A 20-month-old Banyaruanda child was ad-mitted with signs of kwashiorkor. Three monthspreviously he had been treated in hospital forkwashiorkor and hookworm anaemia. He wastreated with a high-protein diet and oral ironand appeared to be improving.On the eighth dayin hospital be became dyspnoeic and developed acough; tuberculosis was suspected and the childwas started on antituberculous therapy. The nextday a vesicular rash developed in the groin andrapidly spread to involve the rest of the body.This was clinically diagnosed as chickenpox.The child died two days later as a result ofpneumonia.At necropsy the rash was found to be resolving
but ulcers were noted in the mouth and throat.The lungs showed extensive tuberculosis and theliver contained fat. Microscopically, lesions highlysuggestive of herpes simplex were found in themouth, lung, liver, spleen, and adrenal. Extensivenon-reactive caseating tuberculous broncho-pneumonia was seen although organisms werescanty.
CASE 4A 7-day-old Batoro infant, who had been bornat home, was admitted with a history of twodays of vomiting of blood and convulsions.The child died shortly after admission.At necropsy there was no skin rash. Numerous
small haemorrhages were found in the liver,kidney, bowel, and lung. A presumptive diagnosisof thrombocytopenia was made on the macro-scopic appearances. In addition to the petecheae,ring-like haemorrhages, 3 or 4 mm in diameter,were noted under the capsule of the liver.Microscopically, areas of necrosis surrounded bycells containing the typical inclusions of herpessimplex were found in the liver parenchyma.The adrenals and spleen showed essentiallysimilar lesions scattered through their substance.Petecheal haemorrhages were seen in these organs,and also in the lung, bowel, and kidney.
CASE 5A 12-month-old female Banyaruanda infant wasadmitted with severekwashiorkor. Onexaminationthe child was pyrexial (100°F) and signs of bron-
on June 29, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.23.1.24 on 1 F
ebruary 1970. Dow
nloaded from

26 A. C. Templeton
chopneumonia were present. A few hours afteradmission the child had a convulsion and lumbarpuncture showed a normal cerebrospinal fluid.She died two days later as a result of the pneu-monia.At necropsy no ulcers were found on the skin
or in the mouth. The lungs showed extensivebronchitis and bronchopneumonia. The liverwas fatty and pale in colour, and numerous smallcircular haemorrhages were seen on the cutsurface. Microscopic examination showed inhala-tion pneumonia with no evidence of viral infec-tion. The brain appeared normal but character-istic patches of necrosis were found in liver andadrenal.
CASE 6A 14-month-old Ankole female infant was ad-mitted with signs of kwashiorkor. She had numer-
_"-AP
... 1.... v ~~~~~~~~.w^S,...... . l...i
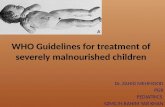
Fig. 1 Section of the adrenal (case 4) to showrounded areas of necrosis in the cortex (haematoxylinand eosin, x 50).
ous ulcers all over the skin which had beenpresent for two months. These were found mainlyin the flexures of the groin, knee, and elbow. Onadmission the child was irritable and apathetic.Haemoglobin was 8 0g% and blood glucose was100 mg%. During the next three days the rashbecame more ulcerated and on the sixth hospitalday she had a convulsion. Lumbar punctureshowed a normal cerebrospinal fluid and theblood glucose level was 19 mg%.The child diedshortly afterwards.At necropsy there were huge numbers of ulcers
of the skin, most marked in the flexures, but nolesions were found in the mouth or pharynx.Culture of the skin ulcers grew a mixed bacterialflora, including staphylococci and E. coli. Thebrain appeared normal. The lungs were consoli-datedandthebronchi injected. The bowel appearednormal. The liver was generally pale and fattybut showed innumerable small circular haemor-rhages throughout the parenchyma but best seenunder the capsule. Minute spots could be seenin the cortex of the adrenals but other organsappeared normal. A portion of liver grew herpessimplex virus in tissue culture.
Microscopically typical necrotic lesions wereseen in the liver and adrenal. The lung showedbronchopneumonia with none of the stigmataof viral infection. The spleen appeared normal.The skin rash was difficult to interpret becauseof the secondary infection but in a biopsy fromthe flexure of the elbow a few inclusion bodieswere seen in the margin of an ulcer. The brainappeared normal microscopically, apart fromminor changes in the neurones suggestive ofhypoglycaemia, which was presumed to be aresult of the extensive hepatic necrosis.
Microscopical Appearances
Histological diagnosis in generalized herpessimplex is usually straightforward. The organsfrequently affected are the liver and adrenalthough necrotic areas in the adrenal may besmall and few in number (Fig. 1). The cortex isaffected exclusively and the medulla is alwaysnormal. The areas of necrosis are spherical andseem to spare the outermost and innermostzones of the cortex. It is in the liver, however,that the most characteristic changes are seen.Macroscopically the capsular surface and crosssections of the organ show innumerable, tiny,whitish spheres each surrounded by a 'halo'of haemorrhage(Fig. 2). In kwashiorkor, when theremaining liver cells are distended with fat, theappearance is very striking. Microscopically theseareas show a central zone of complete necrosissurrounded by an area in which the cells showthe various stages of infection by herpes virus.Surrounding this is a zone of dilated vessels andextruded red cells; the absence of inflammatory
on June 29, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.23.1.24 on 1 F
ebruary 1970. Dow
nloaded from

Generalized herpes simplex in malnourished children
Fig. 2 Surface of the liver (case 6) showing howsharply the areas of necrosis and haemorrhagestand out in the fatty background ( x 1-6).
....
Fig. 3 Liver cells illustrating the development ofthe inclusion body: (left) a large nucleolus and Bbodies; (centre) two nuclei filled with homogeneousA bodies; (right) the shrunken eosinophilic inclusionsurrounded by clumped chromatin (H and E, x 1,200).
cells in all areas is a striking feature. Thesepatches of necrosis do not bear any constantrelationship to the liver lobule. In the olderchildren, the size of each area was considerablysmaller than in the neonatal case and the descrip-tions and illustrations in published reports indi-cate that this is generally true. The characteristicfeature of this infection is the change which occursin the nuclei with the formation of an inclusionbody. Similar changes take place in the nucleiof cells from different tissues from differentspecies so that it is a property of the virus ratherthan the host cells that determines their formation.Most of ths descriptions of the development andhistochemistry of the the changes in the nucleushave been on cells of tissue culture or eggs.However, the same changes may be seen in post-mortem material using haematoxylin and eosin,Feulgen, and methyl green pyronin stains (Fig. 3).The first change noted is an enlargement of the
nucleoli. In tissue culture, this has been shown tooccur within 30 minutes of infection by virus(Love and Wildy, 1963). A little later, small,dark, circumscribed B bodies may be seen in thenucleoplasm, and these stain positively withhaematoxylin and methyl green but not withFeulgen. After a few hours, large masses developand coalesce until they entirely fill the nucleus(A bodies). These A bodies stain positivelywith both Feulgen and haematoxylin at firstbut as they become older they lose their affinity forboth these stains and, becoming smaller, tend toshrink away from the nuclear membrane, eventu-ally showing all the characteristics of the centraleosinophilic Cowdry typeA inclusions. During theearly stage of the development of the A body,the B bodies migrate to the edge of the nucleusand on rare occasions may be seen in the cyto-plasm of the cell. As the development of theseinclusion bodies progresses, the nucleoli dis-appear and the chromatin material of the nucleusbecomes progressively more clumped and isarranged around the periphery of the nucleus.Giant cell formation is rarely observed in theliver but appears more commonly in the adrenalcortex.
Epidemiology
It has recently been shown that two distinctantigenic types of herpes simplex virus exist:type 2 includes most of the viruses producinggenital infections (Dowdle, Nahmias, Harwell,and Pauls, 1967) and type 1 produces many of thecases of herpes labialis. Serum raised againsttype 1 strain only partially neutralizes type 2virus; this fact explains the apparent anomalyof neonatal herpes infection occurring in infantswith circulating antibody. Most surveys of theincidence of herpes infection have been conductedusing type 1 strains and serum, so that very little
on June 29, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.23.1.24 on 1 F
ebruary 1970. Dow
nloaded from

28 A. C. Templeton
information is as yet available as to the incidenceof type 2 strains, especially in Africa.Neonatal infection may occur in the infant
of a non-immune mother as a result of contactwith a person with herpes infection or perhapsfrom a primary infection in the mother. Infectionmay occur as a result of contact with type 2strain even if the mother has circulating anti-type 1 antibody. This is particularly liable tohappen if the mother has a primary genital herpesinfection. In Africa neonatal infection is extremelyrare, in fact case 4 in the present series appearsto be the first recorded instance. The possibleexplanations of this are that all mothers areimmune or that the causative virus is very rare.
Coetzee (1955) found circulating antibody in100% of the adult Bantu population of Pretoria.A survey in Cape Town showed the Bantu popula-tion to have the highest incidence of antibody,the white the lowest, and the Cape coloured groupoccupied an intermediate position (Becker, 1966).It is therefore of interest to note that the onlyfatal neonatal case seen by the South Africanworkers was a white infant (Kipps et al, 1967). InKampala 126 out of 130 adults were found to havecirculating antibody (Woodall, Williams, Simp-son, and Haddow, 1965) but it is likely that inrural districts the prevalence of antibody islower; it may be significant that the mother ofthe infant with neonatal infection (case 4) hadonly recently arrived from a country district.There is no information available as to the inci-dence of type 2 strains in Uganda, but one couldperhaps infer that they are not frequent becauseof the paucity of generalized disease in neonates.The rarity of neonatal infection with type 1
strains is probably a result of the universalpresence of antibody in the adult populationwhich would ensure protection during the earlyweeks of life.
In South Africa the incidence of fatal general-ized herpes seems to be higher than elsewhere andit is interesting to speculate why this should be.It is possible that different strains of virus occurin these areas but experience suggests that thisis not so (Becker et al, 1963). In Durban 38 casesof the disease were found in two years duringwhich time 'well over a thousand postmortemswere performed each year' (Kipps et al, 1967).In Kampala only six were found in a total of5,300 necropsies. Although it is possible thatcases were missed in Kampala the difference is astriking one. The Bantu population of Durbanis urbanized and children tend to live with theirparents in the town. In Kampala it is usual tosend children home to the family shamba wherethey remain until they go to school, by whichtime malnutrition is no longer a problem. Theonly families actually living in crowded circum-stances in the town are recent immigrants. It isof interest therefore that all five children withinfection associated with malnutrition came fromimmigrant families and none were of the indigen-
ous Baganda tribe who show just as high anincidence of kwashiorkor.
Relation to Malnutrition
Infection with herpes simplex virus is an extremelycommon event. It has been estimated that 90%of infections are subclinical(Scott, 1957). Althoughviraemia occurring at the time of primary infec-tion has only rarely been demonstrated (Dudgeon,1950); Ruchman and Dodd, 1950), it probablyoccurs quite frequently. In the vast majority ofcases this is ofno significance apart fromproducinga transient malaise, but in some circumstancesviraemia progresses to fatal generalized infection.Since the majority of such cases occur in mal-nourished children and neonates it has beenassumed that there is some form of deficientimmunological response in these subjects. Anti-body production, serum levels of antibody, andturnover rates appear to be normal in kwashior-kor (Cohen and Hansen, 1962). It has beenstated that interferon production is normal (WHOExpert Committee, 1965). It would seem likely,therefore, that delayed hypersensitivity might bedeficient in same way. In support of this conceptreaction to BCG is frequently defective (Harlandand Brown, 1965) and Mantoux testing is unreli-able in malnourished children (Lloyd, 1968).These reactions are mediated by thymic-depend-ent lymphocytes and certainly thymic atrophy isextreme in children dying from kwashiorkor.
In some cases reported fatal generalized infec-tions occur in apparently well nourished children.For example, in children with eczema it has longbeen known that fatal generalized infection is adistinct hazard (Kaposi, 1895). Five of the 13cases of generalized herpes infection occurringafter measles seen in Senegal occurred in wellnourished children (Armengoud quoted by Kippset al, 1967). Chickenpox appeared to be associatedin case 3. It is possible that in these cases thedeficiency in response is a result of abnormality inthe skin. Kwashiorkor is associated with grossalterations in the skin which is thinner than nor-mal and flakes over the flexures. Local interferonproduction in the skin has been shown to be im-portant in the healing of experimental herpesinfection in mice (Sydiskis and Schultz, 1966)and it could be that this is a contributory factorto the sensitivity of children with kwashiorkor.
I should like to thank the clinicians and pathologistsconcerned with these patients for access to theirrecords, and to Professor F. 0. MacCallum of OxfordUniversity, England; Professor D. MacKenzie of CapeTown, South Africa; and Professor M. S. R. Hutt,of Makerere, Uganda, for their help and advice.Dr B. Henderson, of the East African Virus ResearchInstitute, Entebbe, Uganda, did the tissue culture.
on June 29, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.23.1.24 on 1 F
ebruary 1970. Dow
nloaded from

Generalized herpes simplex in malnourished children
References
Becker, W. B. (1966). The epidemiology of herpes virus infectionin three racial communities in Cape Town. S. Afr. med. J.,40, 109-111.
Becker, W. B., Naud6, L. du T., Kipps, A., and MacKenzie, D.(1963). Virus studies in disseminated herpes simplexinfections. S. Afr. med. J., 37, 74-76.
Coetzee, J. N. (1955). The epidemiology of herpes simplex in thePretoria Bantu population. S. Afr. J. Lab. clin. Med., 1,52-56.
Cohen, S., and Hansen, J. D. L. (1962). Metabolism of albumiaand v globulin in Kwashiorkor. Proc. Nutr. Soc. 5th. Afr.,3, 26-31.
Dowdle, W. R., Nahmias, A. J., Harwell, R. W., and Pauls, F. P.(1967). Association ofantigenic type of herpesvirus hominiswith site of viral recovery. J. Immunol., 99, 974-980.
Dudgeon, J. A. (1950). A complement fixation test for herpessimplex infections. J. clin. Path., 3, 239-247.
Harland, P. S. E. G., and Brown, R. E. (1965). Tuberculin sensi-tivity following B.C.G. vaccination in undernourishedchildren. E. Afr. med. J., 42, 233-238.
Hass, G. M. (1935). Hepato-adrenal necrosis with intranuclearinclusion bodies. Amer. J. Path., 11, 127-142.
Kaposi, M. (1895). Pathology and Treatment of Disease of theSkin, p. 346. Wood, New York.
Kipps, A. Becker, W., Wainwright, J., and MacKenzie, D. (1967).Fatal disseminated primary herpes virus infection inchildren: epidemiology based on 93 non-neonatal cases.S. Afr. med. J., 41, 647-651.
Lloyd, A. P. C. (1968). Tuberculin test in malnourished children.Brit. med. J., 3, 529-531.
Love, R., and Wildy, P. (1963). Cytochemical studies of thenucleo-proteins of HeLa cells infected with herpes virus.J. cell. Biol., 17, 237-254.
Ruchman, I., and Dodd, K. (1950). Recovery of herpes simplexvirus from the blood of a patient with herpetic rhinitis.J. Lab. clin. Med., 35, 434-439.
Scott, T. F. McN. (1957). Epidemiology of herpetic infections.Amer. J. Ophthal., 43, April, Part 2, 134-147.
Sydiskis, R. J., and Schultz, I. (1966). Interferon and antibodyproduction in mice with herpes simplex skin infections.J. infect. Dis., 116, 455-460.
Woodall, J. P., Williams, M. C., Simpson, D. I. H., and Haddow,A. J. (1965).The isolation in mice of strains of herpes virusfrom Burkitt tumours. Europ. J. Cancer, 1, 137-140.
World Health Organisation Expert Committee (1965). Nutritionand infection. Wld. Hlth. Org. Techn. Rep. Ser., 314, 16.
Zuelzer, W. W., and Stuhlberg, C. S. (1952). Herpes simplexvirus as the cause of fulminating visceral disease andhepatitis in infancy. Amer. J. dis. Child., 83, 421-439.
Addendum
DEMONSTRATION OF HERPES SIMPLEX VIRALANTIGEN BY IMMUNOFLUORESCENCEAs Sabin and Messore (1961) showed that indirectimmunofluorescence will detect the antigen ofherpes simplex virus in formalin-fixed tissue, thistechnique was applied to material from thecases described above, in the hope of getting
additional confirmation of the diagnosis. Sincethere is little information on stability of theantigen under prolonged storage, particularly inthe tropics, the presence of herpes infection wouldnot be excluded by a failure to show specificfluorescence in tissues which had been fixed forone to six years.
MATERIALS AND METHOD
Rabbit seraRabbits were immunized by repeated injectionsof RK 13 cells infected with a type 1 herpessimplex virus. Normal rabbit serum was used forthe control staining. As a check on specificityfurther sections were stained with antiherpesrabbit serum which had been absorbed with eithernormal BHK 21 cells or herpes-infected BHK 21cells. This latter absorption abolished the specificstaining. Sera diluted 1:20 were applied to sectionsfor one hour.
Anti-rabbit globulinThis, conjugated with fluorescein (Nordic Diag-nostics, Holland), diluted 1:80, was applied for20 minutes.
MicroscopyThe preparations were examined on a VickersPatholette microscope, with iodine-quartz lamp,Barr & Stroud interference filter as primary andSchott OG.515 as secondary filter.
RESULTSStaining was considered specific if a cell, or groupof cells, fluoresced with immune serum in themiddle layer and did not fluoresce with normalserum, or antigen-adsorbed immune serum.
Case INo specific staining was seen in liver. In skinthere were numerous vesicles, but no specificstaining was observed.
Case 2In liver scattered groups of cells showing specificstaining, and in adrenal there were areas ofdiffuse specific staining in the cortex.
Case 3No specific staining was seen in liver or adrenal.
Case 4Many patches of liver cells showed specificstaining, and in adrenal there were areas ofnecrosis with specifically stained cells at theiredges in the cortex.
Case S
In liver there were scattered groups of cellsshowing specific staining, mostly in portal tracts.In adrenal there were patches of clearly de-
29 on June 29, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.23.1.24 on 1 February 1970. D
ownloaded from





![Refractory Oedema of Nephrotic Syndrome in a Resource Poor ... · in oedema formation in NS [4]. The mechanism causing the oedema of NS of various aetiologies is critical to the management](https://static.fdocuments.in/doc/165x107/5f09f57a7e708231d42953ed/refractory-oedema-of-nephrotic-syndrome-in-a-resource-poor-in-oedema-formation.jpg)











