
General Surgery Resident Handbook 2017-2018€¦ · 9 NOSM General Surgery Resident Handbook...
28
General Surgery Resident Handbook 2017-2018
Transcript of General Surgery Resident Handbook 2017-2018€¦ · 9 NOSM General Surgery Resident Handbook...

1 NOSM Genera l Surger y Res ident Handbook 2017-2018
General Surgery Resident Handbook 2017-2018

2 NOSM Genera l Surger y Res ident Handbook 2017-2018
ContentsWelcome to Your Residency .................................................................... 3
Welcome Letter from Dr. Pankaj Bhatia ................................................. 4
Introduction to NOSM General Surgery Program Roles ...................... 5
Program Contacts .................................................................................... 6Hospital Contact Information .....................................................................................................7
Ethics, Professional Responsibility and Standards of Conduct .......... 8
Core PGY1 Curriculum ............................................................................. 9Leave Process .....................................................................................................................................13
Retreats .................................................................................................. 15Program Specific Retreats ..........................................................................................................15
General Surgery Program Funded Courses ....................................... 15
Exams and Certifications ...................................................................... 16
Absenteeism .......................................................................................... 16
Communication .................................................................................... 17
Surgical Resident Orientation Checklist ............................................. 17
SURGICAL RESIDENT ORIENTATION CHECKLIST ................................. 18
Guidelines for Giving Feedback ........................................................... 19
Assessment in General Surgery ........................................................... 19Point-of-Care Clinical Encounter Trainee Assessment (POCCE) .........................22Surgical Competency Assessment of Resident (SCAR) ............................................22
How to Become Involved with the General Surgery Program ........... 24Teaching Opportunities ..............................................................................................................24Committees and Program Administration ......................................................................24Job Description of a Chief Resident.....................................................................................24
Program Resources ................................................................................ 26
General Surgery Resident To-Do List ................................................... 26

3 NOSM Genera l Surger y Res ident Handbook 2017-2018
Welcome to Your ResidencyWelcome to your residency at NOSM! Residency is an adventure and you are fortunate to be embarking on this new phase of your life in beautiful Northern Ontario. If you are not from here, we trust you will feel at home quickly as people across the North will welcome and appreciate you.
We are looking forward to meeting you and are delighted that you have chosen Northern Ontario for this crucial stage of your education. We are here to help you achieve your goals during your residency.
NOSM residency programs embrace resident-centered approaches with a balance of high support and high expectations. The clinical and academic work will be demanding, you will learn quickly and there will be support, back up and teaching. You will develop clinical independence with a safety net.
Throughout your residency, NOSM staff, program directors, preceptors and your resident colleagues, as well as the NOSM Postgraduate Office are there to answer question, give guidance and provide the support you need.
As you begin your residency, which will offer unique and diverse learning experiences across the North, I encourage you to be ambitious and self-directed so you can make the most of every clinical encounter and conversation with your preceptors, to hone your clinical skills and knowledge.
Residency is complicated and challenging. Please read this manual carefully as it is designed to make life in residency go smoothly and help you to avoid pitfalls and problems. Your success in residency depends in large part on your motivation, your ability to be organized, and your attention to important details, in addition to your clinical know-how.
I wish you the all the best in your residency training and look forward to getting to know you.
Sincerely,
Dr. Catherine Cervin

4 NOSM Genera l Surger y Res ident Handbook 2017-2018
Welcome Letter from Dr. Pankaj BhatiaWelcome to Northern Ontario and congratulations on joining the Northern Ontario School of Medicine Specialty General Surgery Program. We’re delighted to have you. This document is designed to help you navigate the transition to residency and help answer some questions you may have about starting residency at NOSM. Another important resource about being a Surgery resident can be found in the Canadian Association of General Surgeons Residents Committee Residency Survival guide. I strongly recommend that you read and utilize this resource in addition to this handbook. This document outlines all items listed below:
1. CAGS and the ResidentsCommittee
2. MakingYour Life (and Learning) Easier
3. Nuts and Bolts of Every New Rotation
4. On Call
5. Onthe Wards
6. Teaching as a Resident
7. Well Being
8. Textbooks We Like
9. Websites and Apps We Like
10. Giving Rounds
11. National Exams
12. A Note on Loupes
13. Research
14. Mentors and Professional Development
15. Milestones in General Surgery Residency
16. International Surgery
17. Professional Resources and Resident Associations
If you have questions about the program as the year goes by, do not hesitate to ask.
Sincerely,
Dr. Pankaj Bhatia

5 NOSM Genera l Surger y Res ident Handbook 2017-2018
Introduction to NOSM General Surgery Program Roles
Program Coordinators
Program Coordinators act as manager of information flowing to, from, and within the residency program. They are the main point of contact for the program; performing complex administrative duties in support of the program. For instance, they engage in coordination, planning, information management, communication, and project development. Program Coordinators provide assistance and support throughout residency.
Site Directors
Site Directors are responsible for communicating with preceptors in their district in order to coordinate all training activities, acting as a liaison for the residents’ rotations in their district. Should problems arise, they should be available as a resource, representing the Royal College General Surgery program and NOSM, for residents and preceptors.
Preceptors (Clinical Preceptors)
Preceptors are responsible for the regular assessment of residents. Generally, preceptors guide and teach residents daily, on a one-on-one basis. Where a resident identifies a specific area of interest, the program will strive to match the resident to preceptors who may better suit their interest.

6 NOSM Genera l Surger y Res ident Handbook 2017-2018
Program Contacts
General Surgery, Program DirectorDr. P. Bhatia Telephone: c/o Cyndy MacKenzie (807) 766-7444Fax: c/o Cyndy MacKenzie (807) 766-7483Email: [email protected]
Surgical Foundations, Director Dr. Claude CullinanEmail: [email protected]
Program CoordinatorCyndy MacKenzieTelephone: (807) 766-7444Fax: (807) 766-7483Email: [email protected]
Thunder Bay Site, DirectorDr. Andrew SmithEmail: [email protected]
North Bay Site, DirectorDr. Pawan Kuma Email: [email protected]
Sault Ste. Marie Site, DirectorDr. S. AllenEmail: [email protected]
Timmins Site, DirectorDr. H. VoogjarvEmail: [email protected]
Sudbury Site, DirectorDr. R. BenedictEmail: [email protected]
Huntsville Site Coordinator Dr. R. Kirkpatrick Email: [email protected]
Research CoordinatorDr. Shona SmithEmail: [email protected]
Academics, Director Dr. Pankaj BhatiaEmail: [email protected]
Administrative Assistant Connie MerendaTelephone: (807) 766-7446Fax: (807) 766-7483Email: [email protected]
Co-Chief ResidentsDr. Henry Jiang PGY5 Email: [email protected]
Dr. Justin Poling PGY5 Email: [email protected]

7 NOSM Genera l Surger y Res ident Handbook 2017-2018
Hospital Contact Information
Thunder Bay Regional Hospital: (807)684-6000980 Oliver RoadThunder Bay, ON P7B 6V4
Ambulatory Care 684-6550Orthopedic Clinic 684-6363Emergency Department 684-6100ICU 684-6366MCU Intermediate 684-6365Karen Anderson (Academic Liaison Coordinator) 684-6416OR / Endo Bookings 684-6188
Health Sciences North: (705) 523-710041 Ramsey Lake RoadSudbury, ON P3E 5J1
Ambulatory Care/Minor procedures ext. 5155Emergency Department ext. 1050ICU – Cardiology ext. 5473ICU – Medical ext. 4722Resident Liaison - Line Ferris ext. 4483
North Bay Regional Health Centre: (705) 474-860050 College Drive North Bay, ON P1B 5A4
Resident Liaison - Ashley Foreman ext 2518Timmins and District Hospital: (705) 267-2131700 Ross Avenue Timmins, ON P4N 8P2
Resident Liaison -Fran Zimmerman ext. 6370
Muskoka Algonquin Health Centre: (705) 789-2311100 Frank Miller Drive Huntsville, ON P1H 1H7
Resident Liaison -Sue Featherston ext. 2705
Sault Ste. Marie Hospital 750 Great Northern Road Sault Ste. Marie ON P6B 0A8 Resident Liason - Carrie Jones 759-3725
8 NOSM Genera l Surger y Res ident Handbook 2017-2018
Ethics, Professional Responsibility and Standards of Conduct Professionalism is a core value for all health professionals and it is at the heart of your study and practice. Professionalism will be highlighted throughout your residency, in both academic and clinical settings, and embedded in the evaluation process as one of the fundamental roles in the CanMEDS framework. The NOSM professionalism policy and code of conduct is in development and will be circulated when complete.
The Canadian Medical Association Code of Ethics should be reviewed and kept at the forefront of your mind when practicing.
Here in the Royal College General Surgery Program, we believe that residents are responsible for a large portion of their postgraduate medical education. Taking control and ownership of your residency training will maximize your motivation to seek out the highest quality educational opportunities and experiences. The opportunity to achieve a level of training equal to, or greater than, any postgraduate General Surgery program in Canada, is yours for the taking.
As a self-directed learner, you will experience a lifetime of professional rewards, shared with your patients. As a modern health professional, you must continually monitor your knowledge, skills and attitudes, seek out new knowledge, and improve on areas of weakness in order to maintain the highest standard of care. Your patients deserve this care and you owe it to them and yourself.
As an adult learner, you are an active participant in your own education. During your residency, you will refine your skills in setting learning objectives, choosing learning strategies, understanding your preferred learning style, and evaluating your own progress. You will have the opportunity to make suggestions both to individual preceptors, and to the program, to improve the training process. This cooperative effort is in mutual agreement between the College and the certificant.
In our preceptor-based learning environment, you must always remember to respect all of your preceptors` patients as if they were your own. As a professional learner, you should maintain and respect the code of ethics and conduct of the profession itself in all of your personal and professional activities. As you assume an ever-increasing role as a physician with authority, trust and respect, you must accept the responsibilities that are a condition of these privileges.
This program was created for you by the people of Ontario with whom you are entering into a social contract to provide both leadership and service in health care. The treatment of illness, the monitoring of wellness, the creation and promotion of preventative health measures, research and professional development are all factors of this contract.

9 NOSM Genera l Surger y Res ident Handbook 2017-2018
Core PGY1 CurriculumThe Postgraduate Education Office offers all programs the opportunity to participate in a core curriculum. First year postgraduate medical trainees will be notified about the sessions held throughout the year in Sudbury and Thunder Bay. Special guest lecturers/facilitators will guide residents through topics related to the CanMEDS roles as well as practicing in Northern Ontario. Sessions aim to combine didactic components with interactive discussion and exercises to build skills for all postgraduate trainees.
Acute Critical Event Simulation (ACES)
All PGY1 residents at NOSM are required to take an ACES course. ACES is an established 2 day, simulation based, educational course, sponsored by the Royal College to train physicians (residents and practicing physicians) in practical hands on approaches to crises management. Evidence has shown that physicians who have taken this course are more confident and comfortable practicing in rural settings. To prepare for the course, you will be provided with pre-course materials sent from the Royal College. A certificate from the College will also be issued upon completion. The Special Projects Coordinator will email you regarding booking your ACES course. Courses are held throughout the year in both Sudbury and Thunder Bay.

10 NOSM Genera l Surger y Res ident Handbook 2017-2018
NOSM GENERAL SURGERY ROTATION TEMPLATEPg
Year Sample Content and Sequence of Rotations/Number of 4-week Blocks
1 2 3 4 5 6 7 8 9 10 11 12 13
First Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Endo Endo Select ERGen Surg Comm
Gen Surg Comm
SecondGen Surg Comm
Gen Surg Comm
Vasc Surg
Vasc Surg
ICU ICU ICU Research Trauma TraumaACS / Gen
SurgACS / Gen
SurgACS / Gen
Surg
ThirdElect /Select
Elect /Select
Elect /Select
Elect /Select
Elect /Select
Elect/Select
Peds Sx Peds SxGen Surg Comm
Gen Surg Comm
ACS / Gen Surg
ACS / Gen Surg
ACS / Gen Surg
FourthGen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Gen Surg or Select
Fifth Chf Chf Chf Chf Chf Chf Chf Chf Chf Chf Chf Chf Chf
Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg Gen Surg
Select = Selective (relevant and approved) Gen Surg Comm = General Surgery - Community
Elect = Electives (RPC approved) ER=Emergency Medicine Vasc Surg = Vascular Surgery
ACS = Acute Care Service
Content of Training–sample structure (PGY1&2 can be redistributed with approval of Program Director)
PGY-17 Blocks Gen Sx (Tbay/Sudbury)
1 Block Emergency Medicine
2 Blocks endoscopy (surgery call)
1 Block Selective (Internal Medicine or Anesthesia or Plastics)
2 Blocks Gen Sx (community)
PGY-22 Blocks Gen Sx (community)
2 Blocks Trauma
3 Blocks ICU
3 Blocks ACS/Gen Sx (Sudbury/Tbay)
1 Block Research
2 Blocks Vascular Surgery
LMCC II should be completed in PGY-2 Year

11 NOSM Genera l Surger y Res ident Handbook 2017-2018
PGY-36 Blocks of selectives/electives (plan to be approved by RPC 6 blocks prior to beginning of academic year)
2 Blocks Pediatric Sx (Ottawa)
2 Blocks Gen Sx (Community)
3 Blocks Acute Care Sx
Resident must have passed Surgical Foundations exam prior to progressing on to PGY-4****
PGY-413 Blocks in Gen Sx or relevant surgical disciplines
• Pediatric Surgery
• Vascular Surgery
• Surgical Oncology
• Transplantation
• Thoracic Surgery
• Community Surgical Rotation
**Maximum of 4 blocks outside of Gen Sx
**Maximum of 4 blocks away from NOSM
**Alternate sites between chiefs
PGY-513 Blocks in Gen Sx alternating between Tbay and Sudbury (7 and 6 blocks)

12 NOSM Genera l Surger y Res ident Handbook 2017-2018
Rotation InformationThe rotation schedule is difficult to change but we try to be accommodating. In general, It is planned that residents will rotate at various northern sites in our distributed education model.
For all rotations, you will receive in PANDA an orientation package attached to your rotation, outlining who to meet, where, and on what date/time. Prior to the start of any out-of-town rotation, you will be provided with maps, keys, important addresses and phone numbers, etc. for your destination.
Expectations for General Surgery Rotations:
1. In Thunder Bay, residents start call Monday through Fridays at 1700h (if daily duties are completed prior, residents are expected to contact the staff and start call earlier), and at 0800 Saturdays and Sundays. Call ends at 2359 from Sundays through Thursdays and at 0800 on Fridays and Saturdays. All call is home call.
2. In Sudbury, off-service residents (family, anesthesia) take call from 0700 to 2359 Sunday through Thursday and 0700 to 0700 Friday and Saturday. Surgery residents are on call for the full 24 hours any day of the week. Unless residents are performing consults or operations after midnight, they are expected to work the next day. All call is home call but a call room is available for the on call surgery resident if desired. Senior resident/Chief call may begin later in the day (ie. 1600h) to protect elective OR time.
3. Weekend call for scheduling purposes will be Fri/Sun one week, and Saturday on a separate, nonconsecutive weekend, in accordance with PARO regulations. Consecutive weekends may be scheduled only at the resident’s request or to accommodate the resident’s request for certain weekends off.
4. Call is based on a 28 day rotation. As per PARO, home call is 1 in 3 which works out to maximum 9 calls per 28 day schedule.
5. When the resident has scheduled absences (conferences, vacations, etc.) those days will be subtracted from the total days and the call adjusted so as not to exceed 1 in 3.
6. Off-service residents will be treated as general surgery residents for the purposes of call expectations. Call will be preferably established to cover all days during the month but if there are an excess of residents, they will be assigned to buddy call with a more senior general surgery resident.
7. Residents are expected to round on their team’s patients on the weekends they are on call. Rounding post call, within PARO limits, is expected.
8. Handover of overnight issues is the responsibility of the overnight resident to the appropriate attending surgeon or resident(s) on their service. Similarly, residents not on call should be handing over their lists (and especially the sicker patients) to the one on call at or before 17:00 each weekday.
13 NOSM Genera l Surger y Res ident Handbook 2017-2018
Leave ProcessAll leave requests are submitted to [email protected]
• Dr. Bhatia is the lead preceptor for any call concerns or final decisions
• leave requests are initially directed by clinical scheduling to the Program coordinator for tracking, then the call scheduler, to ensure call coverage is met; the call scheduler makes every effort to ensure full coverage; if full coverage is not possible, call scheduler is to consult with Dr. Bhatia or the Site Director
• the call scheduler will reply to clinical scheduling, approving or declining the leave request (IMP so that call is covered....only the call scheduler will receive all leave requests / the big picture)
• if the request is approved, clinical scheduling then includes the approved leave in the block notice for the preceptors awareness.
For Ottawa - the process is similar as your NOSM Program Coordinator will track all your leave and facilitate getting the leave request to the Ottawa schedulers for their approval / decline.
Academic Sessions:
Academic sessions occur bimonthly throughout the year during protected time from clinical duties and will be hosted by various teaching site/city locations. The sessions are mandatory and will be 2-3 full days in length and in some cases will require travel. Your preceptor will be notified about these sessions when reminded of your rotation. Where necessary, travel will be covered and you can use the [email protected] resource to aid in your travel plans.
Schedule July 2017 - June 2018; sites alternating between Thunder Bay and Sudbury, depending on resident distribution
July 17,18,19, 2017 Sudbury — pgy5’s
October or November-TBD. 2017 Sault Ste. Marie — pgy4’s
Feb 5, 6, 7, (whenever is after CARMS) 2018 Sudbury —pgy 3’s
April 9, 10, 11, 2018 Thunder Bay — pgy2’s
June 18, 19, 20, 2018 Sudbury — pgy 1’s
Journal clubs - held as part of the Academic Days
Depending on the site, journal clubs are held on a monthly/bi monthly basis on which two articles are discussed and critiqued. Journal club is led by one resident and one staff member. The journal club sessions enable residents to learn and practice their critical appraisal skills as well as increase their awareness of articles relevant to the practice of general surgery. They also allow staff to evaluate the resident as a med expert as well as communicator and scholar, covering three of the seven standards.
Other Academic Sessions:
Residents will also have the opportunity to participate in local community educational rounds, presentations, journal clubs and rounds through the Ontario Telemedicine Network, Teleconference or Webex when stationed in Northern Ontario. In addition to academic days and subspecialty rounds, videoconferencing and local academic seminars will be utilized as educational opportunities while on community rotations.
14 NOSM Genera l Surger y Res ident Handbook 2017-2018
Surgical Foundations:
Residents in the first two years of training will attend the Surgical Foundations Program. Upon successful completion of the Surgical Foundations program there is a final exam.
Begininng August 22, 2017, these sessions are on site in Thunder Bay, usually in the Medical Professional Building, beside TBRHSC, NOSM Teaching rooms 202 a/b and videoconferenced to HSN in Sudbury. Sessions will occur weekly on Tuesday afternoons from 1400 – 1700h. On scheduled dates, there will be technical skill labs in place of the videoconference.
Thunder Bay Teaching Rounds, Wednesdays 1700h
Sudbury Teaching Rounds, Thursdays 0730h.
Friday Resident Led Rounds – Friday 0700h – 0800h
Residents take turn leading resident rounds on various topics. Please be in contact with your Chief Residents for more information on the schedule and topic list. Sessions are conducted via web ex online meeting rooms.
Procedure Logging
You are expected to keep accurate and up-to-date logs of procedures performed during your training. This is important to identify deficient areas, but also to provide procedure counts for fellowship applications. They may also be required in the future for endoscopy privileges.
All residents have access to T-res and should use this program to log cases. The most efficient way to log procedures is daily, and using the smartphone app. Collecting stickers and inputing them weeks later only increases the chance of missing procedures or breaching patient confidentiality.
There are many headings in the T-res system but at minimum residents should log:
1) procedure date, location, site, preceptor
2) procedure type and whether it is MIS, Open, or Converted
3) patient MRN
4) your role in the surgery (Primary, first assist, etc)
If using the app, remember to sync regularly

15 NOSM Genera l Surger y Res ident Handbook 2017-2018
RetreatsProgram Specific RetreatsEach year, the PGY-1’s through PGY-5’s are encouraged to come together to discuss many aspects of the program to improve the quality of our residency training. Retreats are funded and provide an opportunity for junior and senior residents to spend time together in an informal setting and lay the foundation for a working relationship in the years to come.
Retreats provide opportunities to focus on specific areas of interest that affect the resident body directly. Example topics include: On-call policy, budget allocation and participation in research activities. Residents may choose to review their respective portfolios, join committees and provide feedback on various aspects of the program. This is also an opportunity to combine academic work and social networking activities and team building.
General Surgery Program Funded Courses (Resident responsibility to register and submit leave approval well in advance)
Basic Laparoscopic Surgery - ALS BASIC (PGY1-2) Hamilton August https://www.cmas.ca/events
Advanced Laparoscopic Surgery - ALS ADVANCE (PGY3-5) Hamilton November https://www.cmas.ca/events
Fundamentals of Laparoscopic Surgery FLS – SAGES (PGY3-4) web based education module http://www.flsprogram.org/contents-2/
Advanced Trauma Operative Management - ATOM (PGY4) Toronto http://www.atomcourse.com/
CANADIAN GENERAL SURGERY REVIEW PROGRAM – CAGS (PGY5) Toronto http://generalsurgeryreview.ca/
AMERICAN COLLEGE OF SURGEONS – Annual Clinical Congress (PGY5) various US locations https://www.facs.org/events
Canadian Surgery Forum - (PGY2 & 4)
CAGS Conference
**January 2014 RPC, program approved funding resident travel and accommodation to conferences within North America where they are presenting**
Resident Conference Grant
The Residency Program Committee will respectively consider each individual residents request to utilize the programs allotted Resident Conference Grant ($1500.00 per academic year), on an as required basis, when a resident submits a request to utilize. Requests are to be submitted via email to the Program Coordinator who will bring to the attention of the committee.

16 NOSM Genera l Surger y Res ident Handbook 2017-2018
Exams and CertificationsCAGS: The Canadian Association of General Surgeons (CAGS) Exam happens every February. All residents take this CAGS exam in every year of their residency. The exam is multiple choice and is proctored on site in either Thunder Bay or Sudbury.
SF: In the spring of PGY2, residents take the Surgical Foundations exam. Registration is the residents responsibility, one year in advance. Please refer to the link below for more information:
http://www.royalcollege.ca/portal/page/portal/rc/credentials/start/exams
FLS: Foundations of Laparoscopic Surgery (FLS) certification is to be achieved usually within the PGY3/4 year. http://www.flsprogram.org/
FINAL: The General Surgery final certification exam occurs in the spring of the PGY5 year. Registration is the residents’ responsibility, on e year in advance. Please refer to the link below for more information:
http://www.royalcollege.ca/portal/page/portal/rc/credentials/start/exams
Absenteeism Reliability is a cornerstone of professional behavior – coming to work on time, every day for patient care is critical to a surgeon’s ability to practice. The clear expectations of the program are that residents come to work every day and arrive on time for clinical responsibilities and academic sessions.
All planned absences – vacation, professional leave, lieu days, scheduled appointments over two hours in length with health care providers etc. must have the appropriate leave form completed and submitted in advance as required by the NOSM Postgraduate Office process to ensure accountability.
All planned absences – vacation, professional leave, lieu days, scheduled appointments over two hours in length with health care providers etc. must have the appropriate leave form completed and submitted in advance as required by the NOSM Postgraduate Office process to ensure accountability.
Competence needs to be demonstrated consistently, over a period of time and in a variety of settings so that preceptors and the program are confident that our residents will be able to undertake independent practice safely. Thus, in order to ensure that our residents develop the needed skills and competencies for the orthopedic surgical program, adequate time must be spent in clinics, the operating room and other clinical environments. The expectation and goal for all residents is 100% attendance at all clinical and academic sessions. Multiple absences, whatever the reason, interfere with the ability to develop skills, to be viewed as a contributing team member, to improve knowledge and to demonstrate competence.
In order to fulfill this requirement the following minimum attendance is necessary during a rotation, outside of mandatory courses and formally approved leave:
85% of all clinics; 85% of all scheduled operating room experiences; 85% of all on-call duties
If this level of attendance is not achieved for a given rotation, the rotation will be considered incomplete and make up time will need to be undertaken. This may delay completion of the postgraduate year and promotion to the next level. If there are repeated incomplete rotations due to the above, probation and subsequent dismissal from the program may be the result.

17 NOSM Genera l Surger y Res ident Handbook 2017-2018
It is understandable that occasional unplanned absence may arise due to illness or other emergency. However, absence without notification as per the NOSM Postgraduate Office process outlined in the PGE Office Resident Handbook, is a serious breach of professional conduct. Repeated absences, or late arrivals that occur without notification or that are undocumented demonstrate that the core professional responsibility of reliability has not been achieved and will result in probation and possible dismissal.
Communication The act of notifying the program and communicating with preceptors regarding an absence is a well established tenet of professional behaviour. The following steps must be taken in order to properly communicate an absence, as per the NOSM Postgraduate Office policy and process:
For absence from clinical duties:
• as soon as possible and before 0800, notify the supervising preceptor by directly contacting him or her by phone or text as per the Leave of Absence process outlined in the PGE Office Resident Handbook;
• email the program coordinator the completed leave of absence form capturing all absence detail within 24 hours (There is no need to provide any confidential detail related to any health issue).
For absence from academic sessions:
• notify the program coordinator as soon as possible and before the start of the academic session;
• email the program coordinator the completed leave of absence form capturing all absence detail within 24 hours.
PARO regulated leave e.g. post call day, etc. does not constitute an absence and hence does not require the above mentioned process to be followed.
Surgical Resident Orientation Checklist Surgical Rotation Checklist: Residents will take the initiative to book a meeting with their preceptor in the first week of the rotation in order to complete the Surgical Rotation Checklist (SRC). The SRC will ensure the goals and objectives for the rotation are reviewed, make a plan for the rotation and set times for meetings to complete midterm and final evaluations. The SRC is available from the program coordinator and on My Curriculum along with other important forms Guidelines for Giving Feedback

18 NOSM Genera l Surger y Res ident Handbook 2017-2018
SURGICAL RESIDENT ORIENTATION CHECKLIST At the beginning of each rotation, it is required that the preceptor and resident find a moment to brief each other on the goals, objectives and expectations for the upcoming rotation. A checklist has been created to aid in this discussion.
Rotation: ___________________________________ Date(s): _________________________________
Rotation Schedule
❍ Daily schedule has been provided to the resident including expected start times
❍ Reviewed vacation or academic leave scheduled during rotation
❍ Call schedule has been provided
❍ Rounds that the resident are expected to attend and location
Contact
❍ Exchange of contact information between resident and preceptor (e.g. cell number, email)
Expectations:
❍ Review office and clinic environment i.e. dress code, patient encounters, EMR, etc.
❍ Review OR environment i.e. preparation, participation, dictation, etc.
❍ Review on-call responsibilities e.g. ER, consult dictation, consult log sheet, etc.
Evaluation
❍ In Training Assessment Report(s) and rotation specific evaluations e.g. 360, SCARS, etc. will be introduced
❍ Tentative mid-term evaluation date: ____________________________________
❍Tentative final evaluation date: ________________________________________
Goals/Objectives
❍ Rotation specific and resident goals and objectives reviewed
Preceptor Resident Date
RETURN SIGNED CHECKLIST TO PROGRAM COORDINATOR
19 NOSM Genera l Surger y Res ident Handbook 2017-2018
Guidelines for Giving FeedbackWhen giving feedback to faculty members, in person or in writing, try to be descriptive and provide examples. Rather than focusing on what went wrong, describe how things could be improved. For example, stating, “That was the most boring seminar I’ve ever attended,” is not constructive or professional. A more constructive and descriptive feedback statement might be, “I would have appreciated specific clinical questions directed at the audience to help us think through the case.”
When submitting feedback in writing, it is advisable to consider how comfortable one might be with providing the same feedback in person. In short, it is very important to always remain respectful and professional.
Communication, feedback and assessment are essential to learning. Ideally, feedback should be expected, given and received by resident and preceptor on a daily basis.
Feedback is intended to be formative and can be given and/or solicited verbally and in writing. The feedback process is paramount in navigating a resident’s way to becoming a competent, independent practitioner.
Assessment in General Surgery Regular assessment and feedback to support developing competence and document that competence has been achieved is a core requirement of the program for all residents. In addition to the In Training Assessments (ITARs) within the one45 online evaluation system, residents on surgical rotations are expected to complete and submit to the Program Coordinator, one Point of care clinical encounter form (POCCE) and one Surgical Competency evaluation of resident form (SCAR) per week. Completed POCCEs and SCAR forms are submitted to the Program Coordinator for saving in residents files, to be considered at each 6m resident review with the Program Director. These forms are available from the Program Coordinator. The program expects all these forms to be completed on time as required to successfully fulfill the requirements of the training year. Should you choose to request preceptors to complete SCAR and POCCE forms more frequently this would be considered a demonstration of exemplary professional behavior, self directed learning and engagement in the program.
The assessment process determines if residents have achieved certain milestones (passing a rotation, passing an exam, being promoted to the next PGY level).
Assessments are based on the program, and take into account a resident’s own specific goals, objectives and competencies.

20 NOSM Genera l Surger y Res ident Handbook 2017-2018
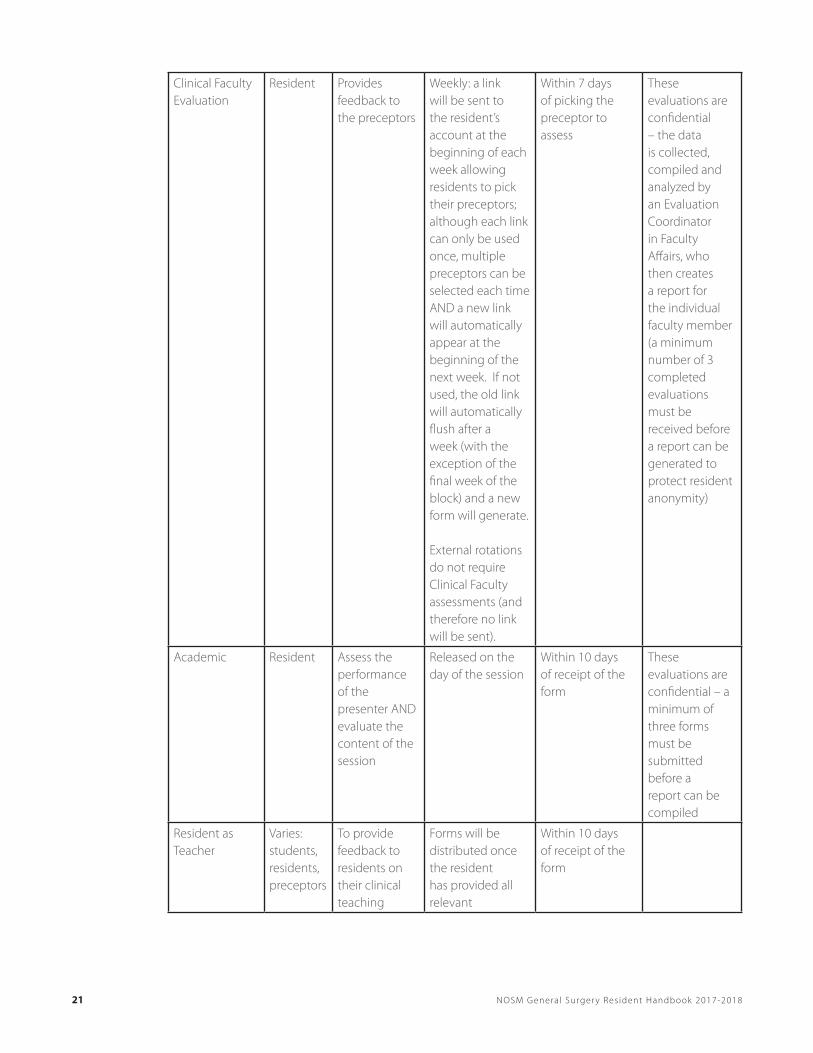
Assessment & Evaluation Summary:
Evaluation Evaluator Purpose Availability DeadlinesAdditional Comments
In-Training Assessment Report(ITAR) and/or In-Training Evaluation Report (ITER)
Preceptor Assesses the performance of the resident
12 days before the end of the rotation
10 days after the end of rotation; mid rotation if the rotation is longer than 4 weeks
*it is expected that the resident will meet with the preceptor before the end of the rotation to discuss the evaluation and ensure its completion
Resident will receive notice when the preceptor has completed the final evaluation online but will not be able to review it until they have completed all of their evaluations for that specific rotation
Rotation Evaluation
Resident Evaluates the learning experience
12 days before the end of the rotation
10 days after the end of the rotation
These evaluations are confidential – a minimum of three forms must be submitted before a report can be compiled
21 NOSM Genera l Surger y Res ident Handbook 2017-2018
Clinical Faculty Evaluation
Resident Provides feedback to the preceptors
Weekly: a link will be sent to the resident’s account at the beginning of each week allowing residents to pick their preceptors; although each link can only be used once, multiple preceptors can be selected each time AND a new link will automatically appear at the beginning of the next week. If not used, the old link will automatically flush after a week (with the exception of the final week of the block) and a new form will generate.
External rotations do not require Clinical Faculty assessments (and therefore no link will be sent).
Within 7 days of picking the preceptor to assess
These evaluations are confidential – the data is collected, compiled and analyzed by an Evaluation Coordinator in Faculty Affairs, who then creates a report for the individual faculty member (a minimum number of 3 completed evaluations must be received before a report can be generated to protect resident anonymity)
Academic Resident Assess the performance of the presenter AND evaluate the content of the session
Released on the day of the session
Within 10 days of receipt of the form
These evaluations are confidential – a minimum of three forms must be submitted before a report can be compiled
Resident as Teacher
Varies: students, residents, preceptors
To provide feedback to residents on their clinical teaching
Forms will be distributed once the resident has provided all relevant
Within 10 days of receipt of the form
22 NOSM Genera l Surger y Res ident Handbook 2017-2018
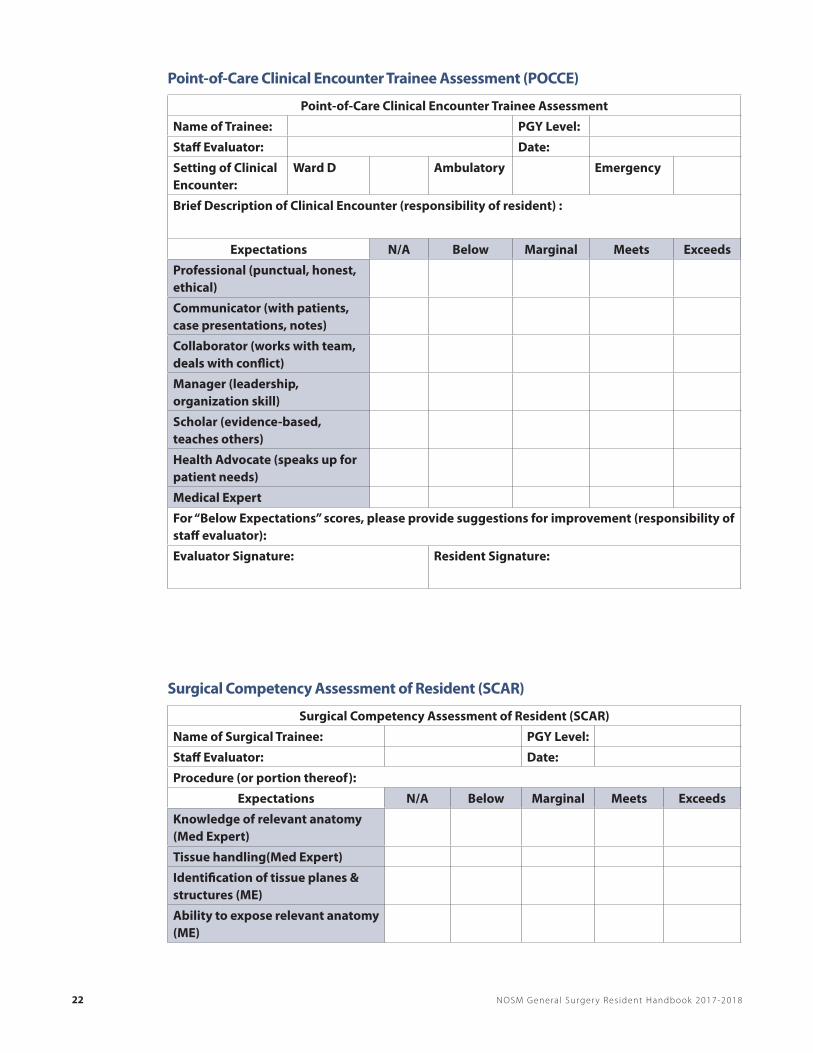
Point-of-Care Clinical Encounter Trainee Assessment (POCCE)
Point-of-Care Clinical Encounter Trainee Assessment
Name of Trainee: PGY Level:
Staff Evaluator: Date:
Setting of Clinical Encounter:
Ward D Ambulatory Emergency
Brief Description of Clinical Encounter (responsibility of resident) :
Expectations N/A Below Marginal Meets Exceeds
Professional (punctual, honest, ethical)
Communicator (with patients, case presentations, notes)
Collaborator (works with team, deals with conflict)
Manager (leadership, organization skill)
Scholar (evidence-based, teaches others)
Health Advocate (speaks up for patient needs)
Medical Expert
For “Below Expectations” scores, please provide suggestions for improvement (responsibility of staff evaluator):
Evaluator Signature: Resident Signature:
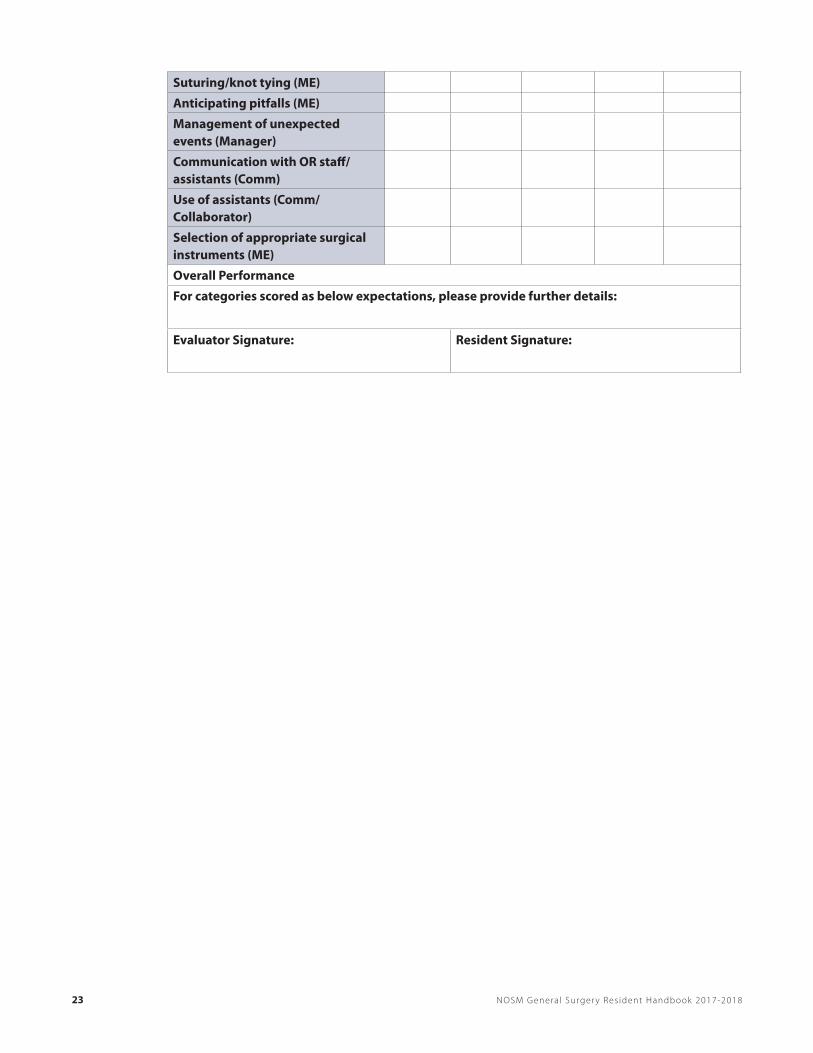
Surgical Competency Assessment of Resident (SCAR)
Surgical Competency Assessment of Resident (SCAR)
Name of Surgical Trainee: PGY Level:
Staff Evaluator: Date:
Procedure (or portion thereof):
Expectations N/A Below Marginal Meets Exceeds
Knowledge of relevant anatomy (Med Expert)
Tissue handling(Med Expert)
Identification of tissue planes & structures (ME)
Ability to expose relevant anatomy (ME)
23 NOSM Genera l Surger y Res ident Handbook 2017-2018
Suturing/knot tying (ME)
Anticipating pitfalls (ME)
Management of unexpected events (Manager)
Communication with OR staff/assistants (Comm)
Use of assistants (Comm/Collaborator)
Selection of appropriate surgical instruments (ME)
Overall Performance
For categories scored as below expectations, please provide further details:
Evaluator Signature: Resident Signature:

24 NOSM Genera l Surger y Res ident Handbook 2017-2018
How to Become Involved with the General Surgery ProgramTeaching OpportunitiesThere will be a number of opportunities to participate in informal and formal teaching activities.
Friday Morning Resident Rounds:
Resident presentations are teleconferenced for audio and slide shows are done over Webex. This is a 45 min presentation + 15 min for questions/discussion on a topic of your choice and should be evidence- based. Medical students can be involved for the first 5-10 min of the presentation. Off-service residents are required to present.
Scheduling and discussion of topics will organized by the residents at either the summer resident retreat or by the Chief Resident(s)
User Information for the sessions is as follows: When: 7:00am - 8:00am
RaTS (Residents as Teachers):
The purpose of RaTS is to assist residents in enhancing their teaching skills as medical educators. The curriculum is presented by experts in medical education and is available to PGY1’s on dates to be announced.
Evaluation of residents as teachers resides in one45. It is the teaching residents responsibility to convey to their program coordinator the details of the teaching encounter in order for feedback to be gathered in one45.
Committees and Program AdministrationChief Resident Description:
The PGY5 year consists of 12 months of General Surgery in which the resident is expected to perform at the level of a Junior Attending. The chief resident’s primary responsibilities are to liaise with residents, faculty, unit and departmental administrative staff and office personnel to assist in the effective running of the Program.
Chief Resident Creed:
I am a consultant General Surgeon. I am going to pass my exams. I am going to help my colleagues pass the exams. For today, this is all there is.
Job Description of a Chief ResidentClinical Responsibilities
Ward: The Chief resident will assist and supervise the junior residents in daily ward care of patients. The Chief resident will round with the junior residents and provide them with direction in carrying our management plans for all patients. The Chief resident is expected to be directly familiar with those patients he/she has operated on and also provide supervision of the care of the remaining patients. The Chief resident will ensure that adequate chart documentation occurs on all patients, and that residents complete dictations.

25 NOSM Genera l Surger y Res ident Handbook 2017-2018
Clinic: Attendance to at least one clinic per week is required. The Chief resident is expected to evaluate both new consultations and follow-up patients in the clinic.
Operating Room: Attendance at the majority of the teams cases is expected. The Chief resident’s role will vary according to the case and the learning requirements of the junior members. There may be opportunity for the chief resident to act as the teaching assistant to the junior resident on the smaller cases. All residents are expected to attend the OR in a timely fashion to help with patient positioning and to become familiar with the chart if the case is being done on an outpatient basis.
Emergency Room: The Chief resident will provide backup for the junior residents who are assigned to the emergency room both during the day and at night. If manpower is limited the chief resident may be the primary provider of surgical consultation in the emergency room.
Other: Attendance at the site teaching rounds, grand rounds, and whole group academic half day is mandatory.
Teaching Responsibilities
Resident Rounds: The Chief resident is expected to present teaching rounds on a regular basis.
Ward teaching: It is expected that part of attending ward rounds with the residents is that the chief residents will use case examples as starting points for educational discussion with the junior residents, including the assigning of mini-projects for the junior residents to explore and research clinical issues.
Teaching of other health care professionals: When rounding with other health care professionals, the chief resident is expected to explain and teach all those in attendance for the education of all involved.
Teaching of medical students: It is expected that chief residents will take the time to provide teaching to the clinical clerks in a variety of clinical settings.
Administrative Responsibilities
Call Schedule: The Chief resident must make the on call schedule and publish it according to PARO guidelines.
Rounds Schedule: The chief resident will assign the teaching rounds to the junior residents and provide a schedule to the Program Coordinator.
Committees
The Residency Program Committee: Two residents sit on this committee. One being a Chief/Senior resident and another resident elected by his or her peers. Terms of this position are one year in duration.
Appeals Committee: You may be asked to sit on an Appeals Committee in the event that a resident fails a rotation and decides to appeal the decision. This would be a rare occurrence but the presence of a relatively unbiased resident on such a committee may be necessary.
CaRMS: Residents may be asked to sit on the Interview team to help select incoming residents. Those chosen to participate will be relieved of clinical duties for the event and will have any necessary travel covered by the program.
26 NOSM Genera l Surger y Res ident Handbook 2017-2018
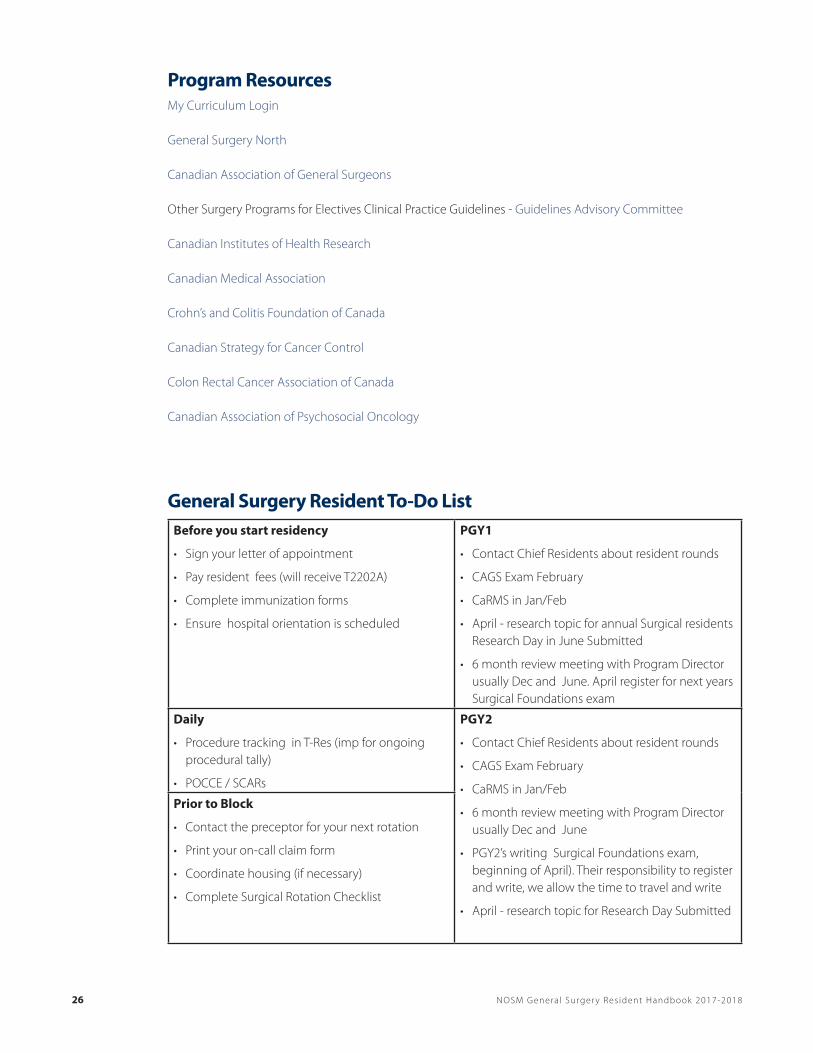
Program ResourcesMy Curriculum Login
General Surgery North
Canadian Association of General Surgeons
Other Surgery Programs for Electives Clinical Practice Guidelines - Guidelines Advisory Committee
Canadian Institutes of Health Research
Canadian Medical Association
Crohn’s and Colitis Foundation of Canada
Canadian Strategy for Cancer Control
Colon Rectal Cancer Association of Canada
Canadian Association of Psychosocial Oncology
General Surgery Resident To-Do ListBefore you start residency
• Sign your letter of appointment
• Pay resident fees (will receive T2202A)
• Complete immunization forms
• Ensure hospital orientation is scheduled
PGY1
• Contact Chief Residents about resident rounds
• CAGS Exam February
• CaRMS in Jan/Feb
• April - research topic for annual Surgical residents Research Day in June Submitted
• 6 month review meeting with Program Director usually Dec and June. April register for next years Surgical Foundations exam
Daily
• Procedure tracking in T-Res (imp for ongoing procedural tally)
• POCCE / SCARs
PGY2
• Contact Chief Residents about resident rounds
• CAGS Exam February
• CaRMS in Jan/Feb
• 6 month review meeting with Program Director usually Dec and June
• PGY2’s writing Surgical Foundations exam, beginning of April). Their responsibility to register and write, we allow the time to travel and write
• April - research topic for Research Day Submitted
Prior to Block
• Contact the preceptor for your next rotation
• Print your on-call claim form
• Coordinate housing (if necessary)
• Complete Surgical Rotation Checklist

27 NOSM Genera l Surger y Res ident Handbook 2017-2018
End of Block
• Complete rotation and preceptor assessments
• Review your rotation assessment
• Complete travel reimbursement form
• Submit on-call claim form ([email protected])
PGY3
• Contact Chief Residents about resident rounds
• CAGS Exam February
• CaRMS in Jan/Feb
• April research topics for Research Day Submitted
• 6 month review meeting with Program Director usually Dec and June
PGY4
• Create and maintain Friday resident led rounds schedule
• Register for ATOM course
• Contact Chief Residents about resident rounds
• ALL PGY4’S MUST REGISTER FOR THEIR ROYAL COLLEGE ASSESSMENT http://rcpsc.medical.org/ residency/certification(exam is written in Y5 but they must register for assessment now)
• CAGS Exam February
• CaRMS in Jan/Feb
• April research topics for Research Day Submitted
• 6 month review meeting with Program Director usually Dec and June
PGY5
• ALL PGY5’S MUST REGISTER FOR THEIR ROYAL COLLEGE EXAM http://rcpsc.medical.org/residency/certification/ (exam is written in Y5)
• Register for Review Course
• CAGS Exam February
• CaRMS in Jan/Feb
• 6 month review meeting with Program Director usually Dec

28 NOSM Genera l Surger y Res ident Handbook 2017-2018











![New Years Poster [Peds] 8 - FFF Enterprises · Title: New Years Poster [Peds] 8.5x11 Subject: New Years Poster [Peds] 8.5x11 Keywords: New Years Poster [Peds] 8.5x11 Created Date:](https://static.fdocuments.in/doc/165x107/5fd6db4c8a000945d6684aca/new-years-poster-peds-8-fff-title-new-years-poster-peds-85x11-subject-new.jpg)






