Gemelli ART - Session 8...ORR, % 61 71 (including 2 CRs) Disease-control rate, % -- 92 at 6 wks...
66
Session 8 Special focus on hormon, target and immunotherapies Take home messages
Transcript of Gemelli ART - Session 8...ORR, % 61 71 (including 2 CRs) Disease-control rate, % -- 92 at 6 wks...

Session 8
Special focus on hormon, target and immunotherapies
Take home messages

Lung Cancer Remains a Major Global Health Burden
§ One of the most common cancers and leading cause of cancer deaths in US and worldwide[1,2]
– New cases, 2017 (estimated): global, 1.8 million (ITALY 40.000)
– Deaths, 2017 (estimated): US, 155,870; global, 1.6 million
§ ~ 80% to 85% of cases are NSCLC (~ 184,000)
– Stage IV at diagnosis: ~ 57%
– Represented by multiple disease subtypes
§ Standard of care for stage IV NSCLC: systemic therapy
§ GLOBOCAN Cancer Fact Sheets. 2012. 2. Siegel RL, et al. CA Cancer J Clin. 2016;66:7-30. § American Cancer Society. Non-small-cell Lung Cancer. 4. SEER Cancer Statistics Review,
1975-2002. 5. Li T, et al. J Clin Oncol. 2013;31:1039-1049.

Therapeutic Decision Making
Histo-typing Geno-typing (Predictive Biomarkers)
These factors are interlinked and not independent
Adapted from Gandara DR, et al. Clin Lung Cancer. 2009;10:392-394.
Therapeutic Decision Making for Advanced NSCLC
“Immunopheno-typing” (Predictive
Biomarkers?)
Clinico-typing

Treating Stage IV NSCLC
NSCLC M+ NOT ONCOGENE ADDICTED
NSCLC M+ NOT ONCOGENE ADDICTED
NSCLC M+ ONCOGENE ADDICTED
§ EGFR (18,19,20,21) § ALK § ROS1, BRAF, Others
PD-L1 (TPS) ≥50%
• PD-L1 (TPS) <50% • PD-L1 NEGATIVE • Controindications
to immunotherapy

NSCLC M+ ONCOGENE ADDICTED
§ EGFR (18,19,20,21) § ALK § ROS1, BRAF, Others
LiT,etal.JClinOncol.2013;31:1039-1049.
NSCLCasonedisease
Histology-BasedSubtyping
Squamous34%
Other11%
Adenoca55%
Adenocarcinoma
SquamousCellCancer
ALKHER2BRAFPIK3CAAKT1MAP2K1NRASROS1RETEGFRKRASUnknown
EGFRvIIIPI3KCAEGFRDDR2FGFR1AmpUnknown
First-targetedtxALKEGFR
25-30 %

EGFR Mutations: Context
§ Found in 10% to 30% of NSCLC pts
§ More common in never-smokers, adenocarcinomas, females, Asians[1,2]
§ Predominantly located in EGFR exons 18, 19, 21
– ~ 85% of EGFR mutations are either deletions in exon 19 or a single-point mutation in exon 21 (L858R)
§ Specific EGFR mutation identified is important – There are sensitive mutations, primary resistance mutations (often exon
20), and acquired resistance mutations (T790M)
• Pao W, et al. J Clin Oncol. 2005;23:2556-2568. 2. Wu YL, et al. J Thorac Oncol. 2007;2:430-439. • Gazdar AF. Oncogene. 2009;28:S24-S31.

First-line Treatment With EGFR TKIs vs Chemotherapy in EGFR-Mutated NSCLC
Study Treatment N Median PFS, Mos ORR, % Median OS, Mos
Maemondo[1] Gefitinib vs carboplatin/ paclitaxel 230 10.8 vs 5.4
(P < .001) 74 vs 31 30.5 vs 23.6 (P = .31)
Mitsudomi[2,3] Gefitinib vs cisplatin/docetaxel 172 9.2 vs 6.3
(P < .0001) 62 vs 32 34.8 vs 37.3 (HR: 1.25)
OPTIMAL[4,5] Erlotinib vs carboplatin/gemcitabine 165 13.1 vs 4.6
(P < .0001) 83 vs 36 22.8 vs 27.2 (HR: 1.19)
EURTAC[6] Erlotinib vs platinum-based chemotherapy 173 9.7 vs 5.2
(P < .0001) 58 vs 15 19.3 vs 19.5 (P = .87)
LUX-Lung 3[7,8] Afatinib vs cisplatin/pemetrexed 345 11.1 vs 6.9
(P = .001) 56 vs 23 28.2 vs 28.2 (P = .39)
LUX-Lung 6[8,9] Afatinib vs cisplatin/gemcitabine 364 11.0 vs 5.6
(P < .0001) 67 vs 23 23.1 vs 23.5 (P = .61)
1. Maemondo M, et al. N Engl J Med. 2010;362:2380-2388. 2. Mitsudomi T, et al. Lancet Oncol. 2010;11:121-128. 3. Yoshioka H, et al. ASCO 2014. Abstract 8117. 4. Zhou C, et al. Lancet Oncol. 2011;12:735-742. 5. Zhou C, et al. Ann Oncol. 2015;26:1877-1883. 6. Rosell R, et al. Lancet Oncol. 2012;13:239-246. 7. Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334. 8. Yang JC, et al. Lancet Oncol. 2015;16:141-151. 9. Wu YL, et al. Lancet Oncol. 2014;15:213-222.

EGFR TKI: gefitinib, afatinib, erlotinib
19del
L858R
Uncommon Mutations
EGFR TKI: gefitinib, afatinib, erlotinib
EGFR TKI: gefitinib, afatinib, erlotinib 1st Line
NSCLC EGFR M+

60
Phase III WJOG 5108L Study: Erlotinib vs Gefitinib in Previously Treated NSCLC
Urata Y, et al. J Clin Oncol. 2016;[Epub ahead of print].
EGFR Mutation–Positive 100
80
40
20
0 0 48 42 36 30 24 18 12 6
Mos
PFS
(%)
198 203
0 0
3 0
5 1
11 4
17 15
31 38
74 72
143 136
No. at risk Erlotinib Gefitinib
Erlotinib Gefitinib
10.0 (95% CI; 8.5-11.2) 8.3 (95% CI;7.2-9.7)
HR 1.093 (95% CI; 0.879-1.358) P = .424
Median (mos)

LUX-Lung 7 (Phase IIb Study) : PFS With First-line Afatinib vs
Gefitinib in EGFR-Mutated NSCLC
*Estimated using exploratory Kaplan-Meier analyses.
Park K, et al. Lancet Oncol. 2016;17:577-589.
Afatinib (n = 160) Gefitinib (n = 159)
HR: 0.73 (95% CI: 0.57-0.95; P = .017)
Median PFS, Mos (95% CI)
11.0 (10.6-12.9) 10.9 (9.1-11.5)
12-Mo PFS*, % (95% CI)
47.4 (39.2-55.2) 41.3 (33.0-49.5)
24-Mo PFS*, % (95% CI)
17.6 (11.7-24.6) 7.6 (3.5-13.8)
100
80
60
40
20
0 0 6 12 18 24 30 36 42
Mos
Pts
(%)

First-line Dacomitinib vs Gefitinib in EGFR-Mutant Advanced NSCLC: Background § Dacomitinib: second-generation ErbB family TKI[1]
– Irreversible inhibitor of EGFR/HER1, HER2, HER4
§ ARCHER 1017: previous single-arm phase II examination of first-line dacomitinib in pts with EGFR-mutant NSCLC[2] – ORR: 75.6%, median PFS: 18.2 mos
§ ARCHER 1050: current phase III analysis evaluating safety, efficacy of first-line dacomitinib vs gefitinib for pts with advanced NSCLC and an EGFR-activating mutation[3]
1. Engelman JA, et al. Cancer Res. 2007;67:11924-11932. 2. Jänne PA, et al. Lancet Oncol. 2014;15:1433-1441. 3. Mok T, et al. ASCO 2017. Abstract LBA9007.

ARCHER 1050: Study Design
§ Multicenter, randomized, open-label phase III study
§ Primary endpoint: PFS by blinded independent review
§ Secondary endpoints: PFS by investigator assessment, ORR, DoR, TTF, OS, safety, pt-reported outcomes
Treatment-naive pts with advanced NSCLC, EGFR-activating mutation(s),
and ECOG PS 0/1; no CNS metastases or prior TKIs
(N = 452)
Dacomitinib 45 mg PO QD (n = 227)
Gefitinib 250 mg PO QD (n = 225)
Mok T, et al. ASCO 2017. Abstract LBA9007.
Stratified by race (Asian vs non-Asian), EGFR mutation (exon 19 vs 21)

ARCHER 1050: PFS by Independent Review
§ Median follow-up for PFS: 22.1 mos
Outcome Dacomitinib (n = 227)
Gefitinib (n = 225)
Median PFS, mos (95% CI)*
14.7 (11.1-16.6)
9.2 (9.1-11.0)
24-mo PFS, % 30.6 9.6 *HR: 0.59 (95% CI: 0.47-0.74; P < .0001)
Wu, Yi-Long et al. The Lancet Oncology 2017 Sep 25

ARCHER 1050: Adverse Events
Mok T, et al. ASCO 2017. Abstract LBA9007.
AE Occurring in ≥ 15% in Either Arm, %
Dacomitinib (n = 227) Gefitinib (n = 224) Any Gr 1 Gr 2 Gr 3 Any Gr 1 Gr 2 Gr 3
Diarrhea* 87.2 49.8 28.6 8.4 55.8 46.0 8.9 0.9 Paronychia 61.7 20.3 33.9 7.5 20.1 13.4 5.4 1.3 Dermatitis acneiform 48.9 16.3 18.9 13.7 28.6 19.2 9.4 0 Stomatitis 43.6 22.5 17.6 3.5 17.9 14.7 2.7 0.4 Decreased appetite 30.8 17.6 10.1 3.1 24.6 21.4 2.7 0.4 Dry skin 27.8 18.5 7.9 1.3 17.0 15.6 1.3 0 Weight decrease 25.6 13.7 9.7 2.2 16.5 9.8 6.3 0.4 Alopecia 23.3 18.1 4.8 0.4 12.5 11.6 0.9 0 Cough 21.1 17.2 4.0 0 18.8 16.1 2.2 0.4 Pruritis 19.8 11.9 7.5 0.4 13.8 10.7 1.8 1.3 ALT increase 19.4 16.3 2.2 0.9 39.3 20.1 10.7 8.5 *Gr 5 diarrhea, n = 1. Otherwise, no listed AE with severity above grade 3 in either arm.

19del
L858R
Uncommon Mutations
EGFR TKI: DACOMITINIB 1st Line
Non-squamous NSCLC EGFR M+ Where are we going?
Study investigators conclude that dacomitinib represents new option for treatment-naive pts with advanced EGFR-mutant NSCLC
Mok T, et al. ASCO 2017. Abstract LBA9007.

EGFR TKI: afatinib preferred
19del
L858R
Uncommon Mutations
EGFR TKI: afatinib, gefitinib,erlotinib
EGFR TKI: afatinib preferred
Progressive disease
1st Line
Non-squamous NSCLC EGFR M+
≃ 10-12 months

Disease Progression on EGFR TKI in NSCLC With EGFR-Sensitizing Mutations
PD: Clinical characteristics
§ Rapid global progression
§ Slow growth globally
§ Growth in several areas, but not all
PD: Molecular characteristics
§ Unknown (other pathways)
§ EGFR T790M (exon 20)
§ MET amplification
§ PIK3CA
Camidge DR, et al. Nat Rev Clin Oncol. 2014;11:473-481.
T790M ~ 40% to 55%
T790M + EGFR amp
~ 10% Other
EGFR mut 1% to 2%
SCLC with PI3K ~ 4%
SCLC ~ 6%
PIK3CA ~ 1% to 2%
MET amp ~ 5%
BRAF ~ 1%
HER2 amp ~ 8% to 13%
EMT ~ 1% to 2%
Unknown ~ 15% to 20%

EGFR TKI: afatinib preferred
19del
L858R
Uncommon Mutations
EGFR TKI: afatinib, gefitinib,erlotinib
EGFR TKI: afatinib preferred
Progressive disease
plasma Cf DNA
T790M- T790M+
Tumor rebiopsy
Third gereration EGFR TKI: Osimertinib
T790M- T790M+
Chemiotherapy doublet
1st Line
2nd Line
3rd Line
Non-squamous NSCLC EGFR M+

Osimertinib (AZD9291): Novel EGFR TKI in EGFR-Mutated NSCLC § Osimertinib FDA approved (November 2015) for advanced
EGFR T790M–positive NSCLC after PD on prior EGFR TKI
– Approval based on AURA and AURA2 single-arm phase II studies of osimertinib in advanced/metastatic NSCLC with EGFR T790M
– Companion diagnostic test for EGFR mutation also approved
AURA (N = 201)
AURA2 (N = 210)
ORR, % 61 71 (including 2 CRs) Disease-control rate, % -- 92 at 6 wks Median PFS, mos Not reached 8.6 Median DoR, mos Not reached 7.8
1. Mitsudomi T, et al. WCLC 2015. Abstract 1406. 2. Yang JC, et al. WCLC 2015. Abstract 943.

AURA3: Osimertinib vs Platinum/Pemetrexed in EGFR T790M–Positive Advanced NSCLC
§ Primary endpoint: PFS (investigator assessed)
§ Additional endpoints: ORR, DoR, DCR, OS, safety
Locally advanced or metastatic NSCLC with
disease progression and EGFR T790M mutation after first-line EGFR TKI therapy; ≤ 1 line of therapy for
advanced NSCLC (N = 419)
Osimertinib 80 mg QD
(n = 279)
Platinum/Pemetrexed Chemotherapy Q3W for up to 6 cycles
(n = 140)
Mok TS, et al. N Engl J Med. 2017;376:629-640. ClinicalTrials.gov. NCT02151981.

AURA3: PFS by Investigator Assessment
Mok TS, et al. N Engl J Med. 2017;376:629-640.
§ Median PFS significantly improved in all evaluated subgroups (age, sex, sensitizing EGFR mutation, CNS disease, and smoking history)
100
80
60
40
20
0
PFS
(%)
Osimertinib Platinum/pemetrexed
0 3 6 9 12 15 18 Mos
Outcome Osimertinib (n = 279)
Plt/pem (n = 140) HR (95% CI)
Median PFS, mos 10.1 4.4 0.30 (0.23-0.41) P < .001 (95% CI) (8.3-12.3) (4.2-5.6)

AURA3: Treatment-Related Adverse Events
N (%), ≥ 10% incidence in either arm
Osimertinib (n = 279) Platinum/Pemetrexed (n = 136) Any Grade Grade ≥ 3 Any grade Grade ≥ 3
Any adverse event 231 (83) 16 (6) 121 (89) 46 (34) Diarrhea 82 (29) 2 (1) 8 (6) 1 (1) Rash 79 (28) 1 (< 1) 6 (4) 0 Paronychia 57 (20) 0 1 (1) 0 Dry skin 52 (19) 0 2 (1) 0 Stomatitis 34 (12) 0 19 (14) 2 (1) Pruritus 30 (11) 0 4 (3) 0 Nausea 21 (8) 0 64 (47) 4 (3) Decreased appetite 20 (7) 1 (< 1) 43 (32) 4 (3) Anemia 9 (3) 1 (< 1) 35 (26) 13 (10) Fatigue 19 (7) 0 32 (24) 1 (1) Neutropenia 15 (5) 0 27 (20) 15 (11) Vomiting 11 (4) 0 25 (18) 3 (2)
Select Adverse Events Interstitial lung disease 9 (3) 1 (< 1) 1 (1) 1 (1) QT prolongation 7 (3) 0 1 (1) 0
Mok TS, et al. N Engl J Med. 2017;376:629-640.

EGFR TKI: afatinib preferred
19del
L858R
Uncommon Mutations
EGFR TKI: afatinib, gefitinib,erlotinib
EGFR TKI: afatinib preferred
Progressive disease
plasma Cf DNA
T790M- T790M+
Tumor rebiopsy
Chemiotherapy doublet Third gereration EGFR TKI: Osimertinib
T790M- T790M+
Chemiotherapy doublet
1st Line
2nd Line
3rd Line
Non-squamous NSCLC EGFR M+

T790M-Negative EGFR TKI-Resistant NSCLC
To date, there are no specific guidelines for the treatment of this subgroup and, outside of clinical trials, platinum-doublet chemotherapy represents the principal treatment option.

Non-squamous NSCLC EGFR M+
“Osimertinib: The Winner Takes It All?”
cit. Tony Mok

First-line Osimertinib vs SoC for EGFR Mutant Advanced NSCLC (FLAURA)
§ Primary endpoint: PFS
§ Secondary endpoints including: ORR, DoR, OS, safety
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
Treatment-naive pts with advanced NSCLC
adenocarcinoma with an EGFR exon 19 or 21 mutation,
WHO PS 0/1, stable CNS mets permitted
(N = 556)
Osimertinib 80 mg PO daily (n = 279)
Erlotinib 150 mg or Gefitinib 250 mg PO daily (n = 277)
Until disease progression or unacceptable
toxicity
EGFR mutation (del19 vs L858R) and race (Asian vs non-Asian)

FLAURA: Survival and Response Outcomes
Outcome Osimertinib (n = 279)
SoC (n = 277)
HR/OR (95% CI) P Value
Median PFS, mos § No CNS mets (n = 440) § With CNS mets (n = 116)
18.9 19.1 15.2
10.2 10.9 9.6
0.46 (0.37-0.57) 0.46 (0.36-0.59) 0.47 (0.30-0.74)
< .0001 <. 0001 .0009
ORR, % § CR § PR
80 3
77
76 1
74
1.28 (0.85-1.93) .2335
Median DoR, mos 17.2 8.5 NR
§ Median OS not reached in either arm
─ Interim analysis at 25% maturity suggests 37% reduced risk of death with osimertinib vs SoC (P = .0068, not significant)
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.

18.9 (15.2, 21.4) 10.2 (9.6, 11.1)
Prob
abilit
y of p
rogr
essio
n-fre
e sur
vival
0.2
0.4
0.6
0.8
0.0
0 3 6 21 24 27 9 12 15 18 Time from randomisation (months) No. at risk
Osimertinib 279 262 233 210 178 139 71 26 4 0 SoC 277 239 197 152 107 78 37 10 2 0
Osimertinib SoC
Prob
abilit
y of o
vera
ll sur
vival
0.2
0.4
0.6
0.8
0.0
0 3 6 9 27
No. at risk
30 12 15 18 21 24 Time from randomisation (months)
Osimertinib 279 276 269 253 243 232 154 87 29 4 0 SoC 277 263 252 237 218 200 126 64 24 1 0
HR 0.63 (95% CI 0.45, 0.88)
p=0.0068ǂ
Median overall survival Osimertinib Not reached
SoC Not reached
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
PFS OS interim analysis
FLAURA: Survival and Response Outcomes

Non-squamous NSCLC EGFR M+
Osimertinib: Where are we going?
19del
L858R
Uncommon Mutations
EGFR TKI: OSIMERTINIB 1st Line
2nd Line Chemiotherapy doublet
3rd Line Chemiotherapy

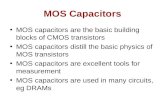
Treatment Based on ALK Translocation and ROS1 Fusion

ALK Fusion Gene
Adapted from Soda et al. Nature; 2007.

ALK Fusion Variants
Sasaki, European Journal of Cancer; 2010.

ALK Gene Rearrangements
§ Most common in younger nonsmokers with adenocarcinoma, adenosquamous carcinoma, and rarely SCC
§ Frequency: 4% overall, 33% in EGFR-negative never-smokers
§ Several ALK variants identified in NSCLC; clinical significance of each is unknown
§ Testing
– Vysis break apart FISH (> 15% cells with split signal in 50 nuclei scored)
– ALK IHC
§ 3 agents now approved for ALK-positive NSCLC (first-line and/or after progression)
Shaw AT, et al. J Clin Oncol. 2009;27:4247-4253. Soda M, et al. Nature. 2007;448:561-566.

PROFILE 1014: First-line Crizotinib vs Pemetrexed/Platinum* in Advanced NSCLC § Phase III trial (N = 343) ALK-positive pts with nonsquamous NSCLC
and no prior systemic treatment for advanced disease Crizotinib
(n = 172) Chemotherapy
(n = 171)
Median PFS, mos 10.9 7.0
HR (95% CI) 0.45 (0.35-0.60)
P value < .001
ORR, % 74 45
P value < .001
Solomon BJ, et al. N Engl J Med. 2014;371:2167-2177.
*Carboplatin or cisplatin.
100
80
60
40
0
20
0 5 10 15 20 25 30 35
PFS
(%)
172 171
120 105
65 36
38 12
19 2
7 1
1 0
0 0
Crizotinib
Chemotherapy
Mos Pts at Risk, n Crizotinib
Chemotherapy

Crizotinib
NO-squamous NSCLC ALK rearrangement
1st Line
Treating Stage IV NSCLC EML4/ALK +

Crizotinib Resistance
§ L1196M
§ L1152R
§ C1156Y
§ F1174L
Sasaki Clinical Cancer Research. Epub 2011.

ALK Mutations With Reported Clinical Resistance to ALK Inhibitors
ALK Version Crizotinib Ceritinib Alectinib Brigatinib/Lorlatinib Wild-type
T1151TIns X
L1152R X X
C1156Y X
I1171N X X
F1174C X
F1174L X
F1174V X X
L1196M X
G1202R X X X
D1203N X
S1206F X
S1206Y X
G1269A X
Kim D-W, et al. ASCO 2016. Abstract 9008.

Next-Generation ALK Inhibitor CNS Activity
Kim DW, et al. Lancet Oncol. 2016;17:452-463. Mok T, et al. ASCO 2015. Abstract 8059. Felip E, et al. ASCO 2015. Abstract 8060. Shaw AT, et al. Lancet Oncol. 2016;17:234-242. Ou S, et al. J Clin Oncol. 2016;34:661-668. Kim DW, et al. ASCO 2016. Abstract 9007. Solomon BJ, et al. ASCO 2016. Abstract 9009. Reckamp K, et al. ELCC 2017. Abstract 88O.
Bra
in O
RR
(%)
(n = 8) (n = 28) (n = 33) (n = 17) (n = 16) (n = 35) (n = 25) (n = 18) (n = 18)
*No previous ALK inhibitor.
Ceritinib (750 mg/day)
Alectinib (600 mg BID)
Brigatinib (90 or 180 mg QD)
Lorlatinib (Various)
63%*
36% 39.4%
58.8%*
75%
57%
36%
67%
39%
0
10
20
30
40
50
60
70
80
90
100
(n = 13)
69%
Ensartinib (Various)

Crizotinib
Ceritinib or Alectinib
Chemotherapy Doublet
Pemetrexed based preferred
NO-squamous NSCLC ALK rearrangement
1st Line
2nd Line
3rd Line
Treating Stage IV NSCLC EML4/ALK +

ASCEND-4: First-line Ceritinib vs Pemetrexed/Platinum* in Advanced NSCLC § Phase III trial (N = 376) ALK-positive pts with nonsquamous
NSCLC and no prior systemic treatment for advanced disease Ceritinib
(n = 189) Chemotherapy
(n = 187)
Median PFS, mos 16.6 8.1
HR (95% CI) 0.55 (0.42-0.73)
P value < .00001
ORR, % 72.5 26.7
Soria JC, et al. Lancet. 2017;389:917-929.
*Carboplatin or cisplatin.
100
80
60
40
0
20
0 2 4 6 8 10 12 14
PFS
(%)
189 187
155 136
139 114
125 82
116 71
105 60
98 53
76 35
Mos Pts at Risk, n Ceritinib
Chemotherapy
16 18 20 22 24 26 28 30 32 34
59 24
43 16
32 11
23 5
16 3
11 1
1 1
1 0
1 0
0 0
Ceritinib
Chemotherapy

CERITINIB
LORLATINIB(GI202R)
ChemotherapyDoublet
Pemetrexedbasedpreferred
NO-squamousNSCLCALKrearrangement
1stLine
2ndLine
3rdLine
Wherearewegoing?

§ Primary endpoint: PFS by independent review facility
§ Secondary endpoint: OS, ORR, PK, QoL, CNS PFS, safety
J-ALEX: Study Design
Alectinib 300 mg twice daily PO
28-day cycle (n = 103)
Crizotinib 250 mg twice daily PO
28-day cycle (n = 104)
Stage IIIB/IV or recurrent ALK+ NSCLC
(by IHC/FISH or RT-PCR) ECOG PS ≤ 2
≥ 1 measurable lesion (investigator assessed)
≤ 1 previous chemotherapy Treated/asymptomatic
brain metastasis permitted (N = 207)
Stratified by clinical stage (IIIB/IV vs recurrent), previous chemotherapy,
ECOG PS (≤ 1 vs 2)
1:1
Nokihara H, et al. ASCO 2016. Abstract 9008.
3 preplanned interim analyses
for efficacy: 33%, 50%, 75% of final events (current report: second interim
analysis)

§ Primary endpoint: PFS
§ Secondary endpoint: HRQoL, ORR, CNS PFS, DoR, OS, safety
ALEX: Study Design
Alectinib 600 mg twice daily PO
28-day cycle (n = 103)
Crizotinib 250 mg twice daily PO
28-day cycle (n = 104)
Stage IIIB/IV or recurrent ALK+ NSCLC
(by IHC) ECOG PS ≤ 2
No previous systemic therapy for advanced disease
Asymptomatic brain metastasis permitted
(N = 303)
1:1
ClinicalTrials.gov. NCT02075840.
Until PD, unacceptable
toxicity, or withdrawal

ALEX: Survival Outcomes
Peters S, et al. N Engl J Med. 2017;[Epub ahead of print].
Investigator-Assessed PFS
Mos
PFS
(%)
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30
11.1 mos
Alectinib
NR
Crizotinib
IRC-assessed PFS: 25.7 vs 10.4 mos; HR: 0.50 (95% CI: 0.36-0.70; P < .001)
HR: 0.47 (95% CI: 0.34-0.65; P < .001)
Mos
OS
(%)
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30
HR: 0.76 (95% CI: 0.48-1.20; P = .24)
Alectinib
Crizotinib
OS

ALEX: PFS According to Pt Subgroups (Investigator Assessed)
Peters S, et al. N Engl J Med. 2017;[Epub ahead of print].
Subgroup Overall Age, Yrs
< 65 ≥ 65
Sex Female Male
Ethnicity Asian Non-Asian
Smoking status Active smoker Nonsmoker Past smoker
ECOG PS 0 1 2
CNS Mets at baseline Yes No
Prior Brain Radiation Yes No
Events/Pts, n 164/303
125/233 39/70
91/171 73/132
72/138 92/165
12/17
103/190 49/96
44/97
105/186 15/20
78/122 86/181
26/47
138/256
HR (95% CI) .48 (0.35-0.66)
.48 (0.34-0.70) .45 (0.24-0.87)
.39 (0.25-0.60) .61 (0.38-0.98)
.46 (0.28-0.75) .49 (0.32-0.75)
1.16 (0.35-3.90) .44 (0.29-0.66) .42 (0.23-0.77)
.40 (0.21-0.77) .48 (0.32-0.71) .74 (0.25-2.15)
.40 (0.25-0.64) .51 (0.33-0.80)
.33 (0.14-0.74) .52 (0.36-0.73)
0.1 1 10
Alectinib better Crizotinib better

ALEX: Time to CNS Progression
Peters S, et al. N Engl J Med. 2017;[Epub ahead of print].
CNS Progression, no Previous Systemic PD
Alectinib (n = 152)
Crizotinib (n = 151)
Pts with event, n (%) 18 (12) 68 (45) Cause-specific HR (95% CI) P value
0.16 (0.10-0.28) < .001
Cumulative Incidence of CNS Progression § Competing risk of CNS progression, non-CNS progression, and death based on first event was analyzed
Mos
Cum
ulat
ive
Inci
denc
e (%
)
0
10
20
30
40
50
0 6 12 18 24 30
60 Crizotinib, 12-mo cumulative incidence rate: 41.4% (95% CI: 33.2-49.4)
Alectinib, 12-mo cumulative incidence rate: 9.4% (95% CI: 5.4-14.7)

ALEX: AEs (≥ 10% Difference Between Arms)
Peters S, et al. N Engl J Med. 2017;[Epub ahead of print].
Crizotinib Alectinib (n = 152)
Crizotinib (n = 151)
Any Grade Grade 3-5 Any Grade Grade 3-5
Nausea 21 (14) 1 (1) 72 (48) 5 (3)
Diarrhea 18 (12) 0 68 (45) 3 (2)
Vomiting 11 (7) 0 58 (38) 5 (3)
Peripheral edema 26 (17) 0 42 (28) 1 (1)
Dysgeusia 4 (3) 0 29 (19) 0
Increased ALT 23 (15) 7 (5) 45 (30) 22 (15)
Increased AST 21 (14) 8 (5) 37 (25) 16 (11)
Visual impairment 2 (1) 0 18 (12) 0
Increased blood bilirubin 23 (15) 3 (2) 2 (1) 0
Myalgia 24 (16) 0 3 (2) 0
Anemia 30 (20) 7 (5) 7 (5) 1 (1)
Increased weight 15 (10) 1 (1) 0 0

ALECTINIB
BRIGANTINIB? LORLATINIB?
Chemotherapy Doublet
Pemetrexed based preferred
NO-squamous NSCLC ALK rearrangement
1st Line
2nd Line
3rd Line
Wherearewegoing?

Treatment Algorithm for Advanced NSCLC: Molecular Biomarker Positive
ALK positive
Progression
First line Second line and beyond
EGFR mutation positive
Advanced NSCLC (Molecular Biomarker Positive)
ROS1 positive
Crizotinib
Follow treatment options for adenocarcinoma or squamous cell carcinoma without actionable biomarker
Osimertinib
EGFR T790M mutation negative
Alectinib, brigatinib, or
ceritinib dependent on
previous therapy
Alectinib, ceritinib, or crizotinib
Erlotinib, afatinib, or gefitinib
EGFR T790M mutation positive
BRAF V600E positive
Dabrafenib/ trametinib

NSCLC M+ NON-ONCOGENE ADDICTED
PD-L1 (TPS) ≥50%
25-30%

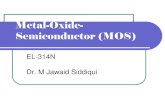
Ribas A. N Engl J Med. 2012;366:2517-2519.
CTLA-4 and PD-1/PD-L1 Checkpoint Blockade for Cancer Treatment
CTLA-4 mAbs: Ipilimumab Tremelimumab
PD-1 mAbs: Nivolumab Pembrolizumab PD-L1 mAbs: Atezolizumab Avelumab Durvalumab
Priming phase (lymph node)
Effector phase (peripheral tissue)
T-cell migration
Dendritic cell T-cell
MHC TCR
B7
CD28
CTLA-4
T-cell Cancer cell
MHC TCR
PD-1
PD-L1
T-cell Cancer
cell Dendritic
cell T-cell

Pembrolizumab* (Anti–PD-1)
Nivolumab* (Anti–PD-1)
Atezolizumab (Anti–PD-L1)
Durvalumab (Anti–PD-L1)
Diagnostic partner Dako Dako Ventana Ventana
Clone 22C3[1] 28-8[2] SP142[3] SP263
Machine utilized Link 48 Link 48 BenchMark ULTRA
BenchMark ULTRA
Compartment TC TC TC/IC TC
Variables % of cells % of cells % of cells % of cells
Definition of positive
PD-L1(+): ≥ 50%
PD-L1(+): ≥ 1%
PD-L1(+): TC3/IC3 (≥ 50% / ≥ 10%)
TC2/IC2 (5% - 49% / 5% - 9%)
TC1/IC1 (1% - 4%)
PD-L1(+): ≥ 25%
PD-L1 IHC Assays
*FDA-approved assays.
1. Garon EB, et al. N Engl J Med. 2015;372:2018-2028. 2. Phillips T, et al. Appl Immunohistochem Mol Morphol. 2015;23:541-549. 3. Fehrenbacher L, et al. Lancet. 2016;387:1837-1847.
Tumor mutational burden (TMB)
Tumor infiltrating lymphocyte
?

KEYNOTE-024: Pembrolizumab vs CT as First-line Therapy for Advanced NSCLC § Open-label phase III trial
§ Primary endpoint: PFS
§ Secondary and exploratory endpoints: ORR, OS, DoR, and safety
Pts with stage IV NSCLC and ECOG PS 0/1, no previous systemic therapy, no actionable EGFR/ALK mutations,
and PD-L1 TPS ≥ 50%* (N = 305)
Pembrolizumab 200 mg IV Q3W for up to 35 cycles
(n = 154)
Chemotherapy (histology based) for up to 6 cycles
(n = 151)
Stratified by ECOG PS (0 vs 1), histology (squamous vs nonsquamous), and
enrollment region
Until PD (crossover to pembrolizumab allowed)
*≥ 50% tumor cell staining using 22C3 companion diagnostic IHC assay.
Until PD or unacceptable toxicity
Reck M, et al. N Engl J Med. 2016;375:1823-1833.

KEYNOTE-024: ORR and Survival Outcomes
§ ORR: 44.8% (pembrolizumab) vs 27.8% (chemotherapy)
§ FDA approval October 2016 § Now SoC to test for PD-L1 at initial diagnosis (22c3 assay) § Approximately 25% to 28% of NSCLC cases have PD-L1 ≥ 50%
100
80
60
40
20
0
OS
Mos
OS
(%)
21 0 3 6 9 12 15
Pembrolizumab Chemotherapy
HR for OS: 0.60 (95% CI: 0.41-0.89; P = .005)
18
PFS
Mos
PFS
(%)
100
80
60
40
20
0 18 0 3 6 9 12 15
HR for PFS: 0.50 (95% CI: 0.37-0.68; P < .001)
6.0 10.3
Reck M, et al. N Engl J Med. 2016;375:1823-1833.

KEYNOTE-024: Treatment-Related AEs With Incidence ≥ 10%
1/2 Grade
3/4 Pembrolizumab Chemotherapy
Reck M, et al. N Engl J Med. 2016;375:1823-1833.
Inci
denc
e (%
)
50 45 40 35 30 25 20 15 10
5 0

First-line NSCLC M+
EGFR and ALK wild type
PD-L1 ≥ 50%
Pembrolizumab
Platinum Doublet
Chemotherapy
1st Line
2st Line
3st Line
Optimal duration of immune checkpoint therapy is yet to be defined
Treating Stage IV NSCLC PD-L1 (TPS) >50%

§ Anti-PD-L1 vs CT: Avelumab, Atezolizumab, Durvalumab
§ Dual checkpoint blockade
§ Checkpoint blockade plus chemotherapy and/or radiation
§ Checkpoint blockade plus vaccines
§ Checkpoint blockade plus oncolytic viruses
§ Checkpoint blockade plus HDAC inhibitors (Epacatostat, etc.)
§ Checkpoint blockade plus . . .
Wherearewegoing?

NSCLC M+ NON-ONCOGENE ADDICTED
PD-L1 (TPS) < 50%
PD-L1 NEGATIVE
Controindications to immunotherapy
40/50 %

Treating Stage IV NSCLC: 1st line

Immune Checkpoint Inhibitors in Pretreated Advanced NSCLC
CheckMate 017 CheckMate 057
KEYNOTE-010 OAK
Nonsquamous Stage IIIB/IV
(N = 582)
Nivolumab
Docetaxel
Squamous Stage IIIB/IV
(N = 272)
Nivolumab
Docetaxel
Advanced NSCLC with ≥ 1% PD-L1+
tumor cells (N = 1034)
Pembrolizumab (2 mg/kg)
Docetaxel
Pembrolizumab (10 mg/kg)
Advanced NSCLC (2L/3L)
(N = 1225)
Atezolizumab
Docetaxel

Phase III Studies of Second-line Immunotherapy in NSCLC
1. Brahmer J, et al. N Engl J Med. 2015;373:123-135. 2. Herbst RS, et al. Lancet. 2016;387:1540-1550. 3. Rittmeyer A, et al. Lancet. 2017;389:255-265.
Agent/Phase III Study ISTO
PD-L1
TPS Treatment Arms Median OS, Mos
HR for OS Benefit in SqNSCLC
(95% CI)
Nivo/CheckMate 017[1] Squam Any Nivo vs docetaxel 9.2 vs 6.0 (P < .001) 0.59 (0.44-0.79)
(P < .001)
Nivo/CheckMate 057[1] Nonsquam Any Nivo vs docetaxel
12.2 vs 9.4 (P < .002)
0.73 (0.59 to 0.89)
(P=0.002)
Pembro/KEYNOTE-010[2] NSCLC ≥ 1%
§ Pembro 2 mg/kg vs docetaxel
§ Pembro 10 mg/kg
vs docetaxel
§ PD-L1 ≥ 1%: 10.4 vs 8.5 (P = .0008) § PD-L1 ≥ 50%: 14.9 vs 8.2 (P = .0002) § PD-L1 ≥ 1%: 12.7 vs 8.5 (P < .0001)
§ PD-L1 ≥ 50%: 17.3 vs 8.2 (P < .0001)
0.74 (0.50-1.09) (NS)*
Atezo/OAK[3] NSCLC Any Atezo vs docetaxel § ITT: 13.8 vs 9.6 (P = .0003)
§ PD-L1 ≥ 50%: 15.7 vs 10.3 (P = .0102) 0.73 (0.54-0.98)
(P = .0383)
*For pooled pembrolizumab doses vs docetaxel in total population.

REVEL: Ramucirumab + Docetaxel vs Docetaxel in Pts With PD After Chemotherapy: OS
Garon EB, et al. Lancet. 2014;384:665-673.
0 3 6 9 12 15 18 21 24 27 30 33 36 0
20
40
60
80
100 O
S (%
)
Mos
Ram + doc Pbo + doc Censored
Ram + doc Pbo + doc Ram + doc vs pbo + doc HR: 0.86 (95% CI: 0.75-0.98; P = .023)
10.5 (9.5-11.2) 9.1 (8.4-10.0)
Median OS, Mos (95% CI)
Ramucirumab in combination with docetaxel is approved for metastatic NSCLC with disease progression on or after platinum-based chemotherapy

LUME-Lung 1 Nintedanib + Docetaxel vs Docetaxel in Pts With PD After
Chemotherapy: OS by Histology
Adenocarcinoma subset
Nintedanib+docetaxel(n=655)
Placebo+docetaxel(n=659)
Median,mo 10.1 9.1
HR(95%CI) 0.94(0.83to1.05)
P .2720
Nintedanib+docetaxel(n=322)
Placebo+docetaxel(n=336)
Median,mo 12.6 10.3
HR(95%CI) 0.83(0.70to0.99)
P .0359
All patients
100
80
60
40
20
0 0 4 8 12 16 20 24 28 32 36
0 4 8 12 16 20 24 28 32 36
Reck M, et al. ASCO 2013.

“Old Agents”
Docetaxel, Pemetrexed*, Erlotinib
New Immunotherapy Agents
Nivolumab, Pembrolizumab (PD-L1>1%),
New Antiangiogenic Agents
Ramucirumab + Docetaxel (only USA) Nindetanib + Docetaxel (only EU)*
* only adenocarcinoma

Selecting Second-Line Therapy
PatientFactors
• PS• Tabagism• Comorbidities• Patientpreference
TreatmentHistory
• First-lineregimen• Durationofresponsetofirst-linetreatment
TumorCharacteristics
• Histology• Molecularprofile

D’Argento E, et al. Curr. Treat. Options in Oncol. (2016)
nonsquamous NSCLC squamous NSCLC
2nd line
1
1