
Gem ox panitumumab
30
-
Upload
chandan-krushna-das -
Category
Health & Medicine
-
view
41 -
download
4
Transcript of Gem ox panitumumab
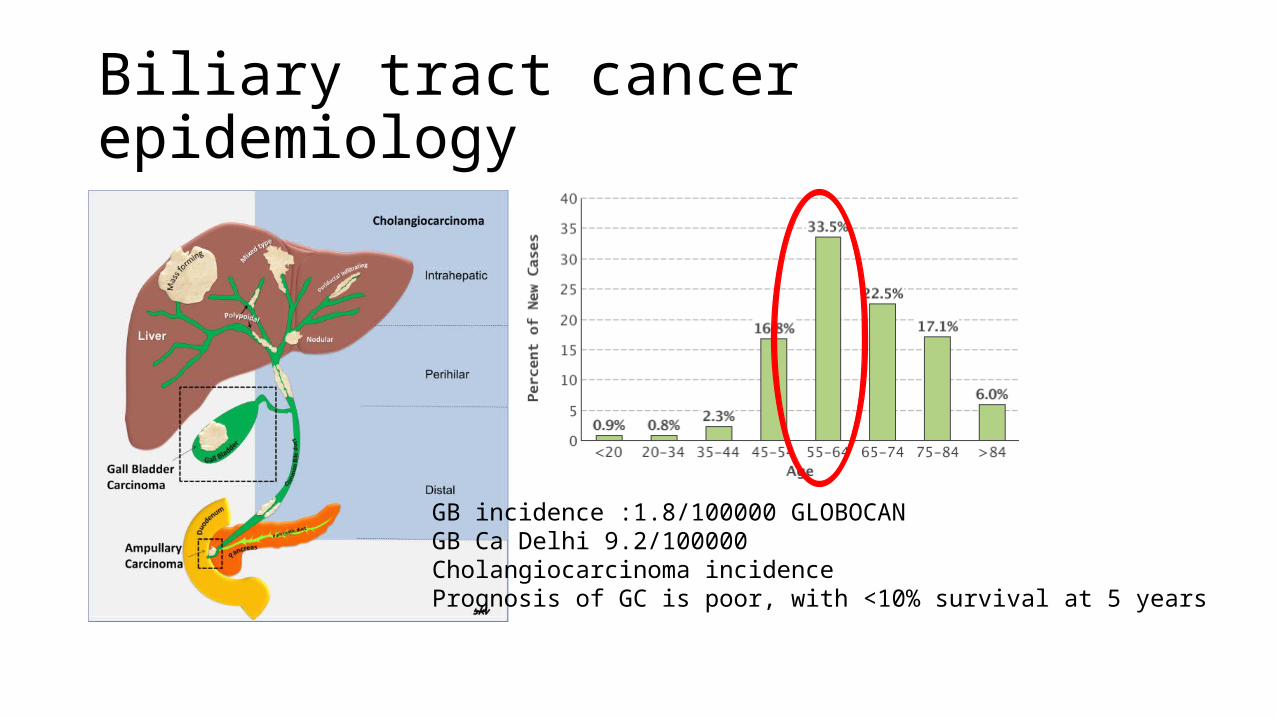
Biliary tract cancer epidemiology
GB incidence :1.8/100000 GLOBOCANGB Ca Delhi 9.2/100000 Cholangiocarcinoma incidencePrognosis of GC is poor, with <10% survival at 5 years
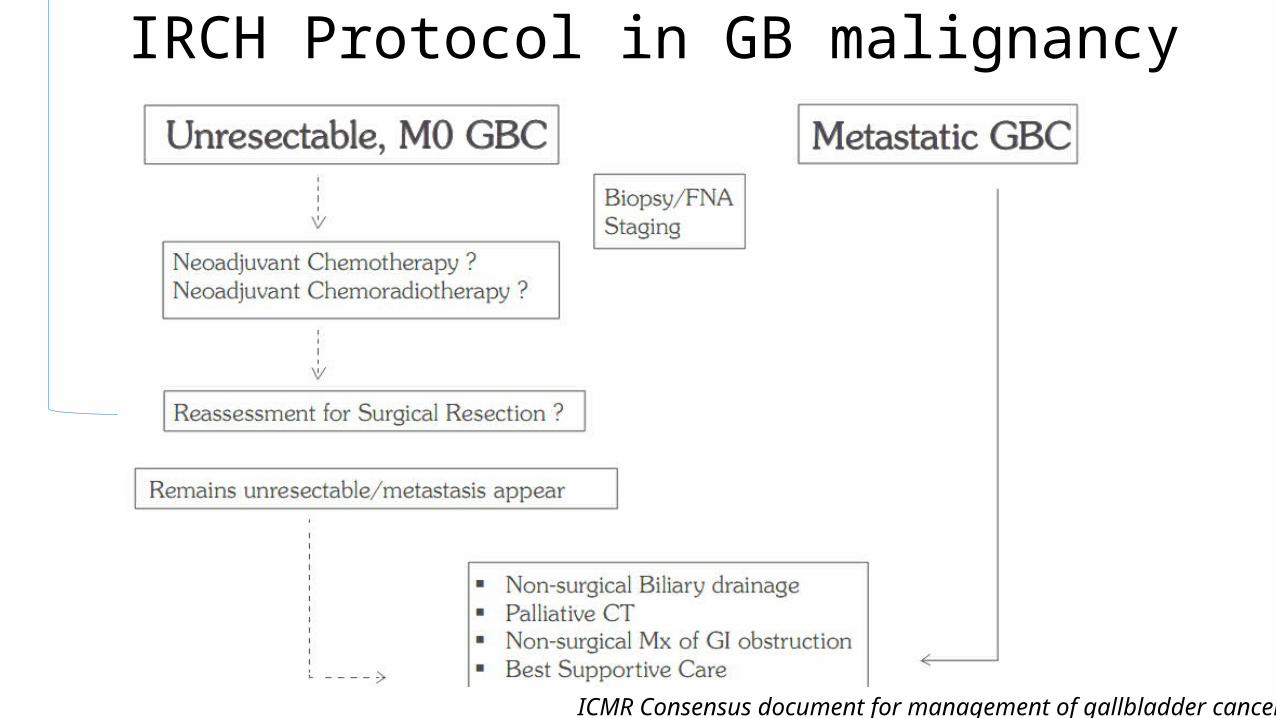
IRCH Protocol in GB malignancy
ICMR Consensus document for management of gallbladder cancer 2014
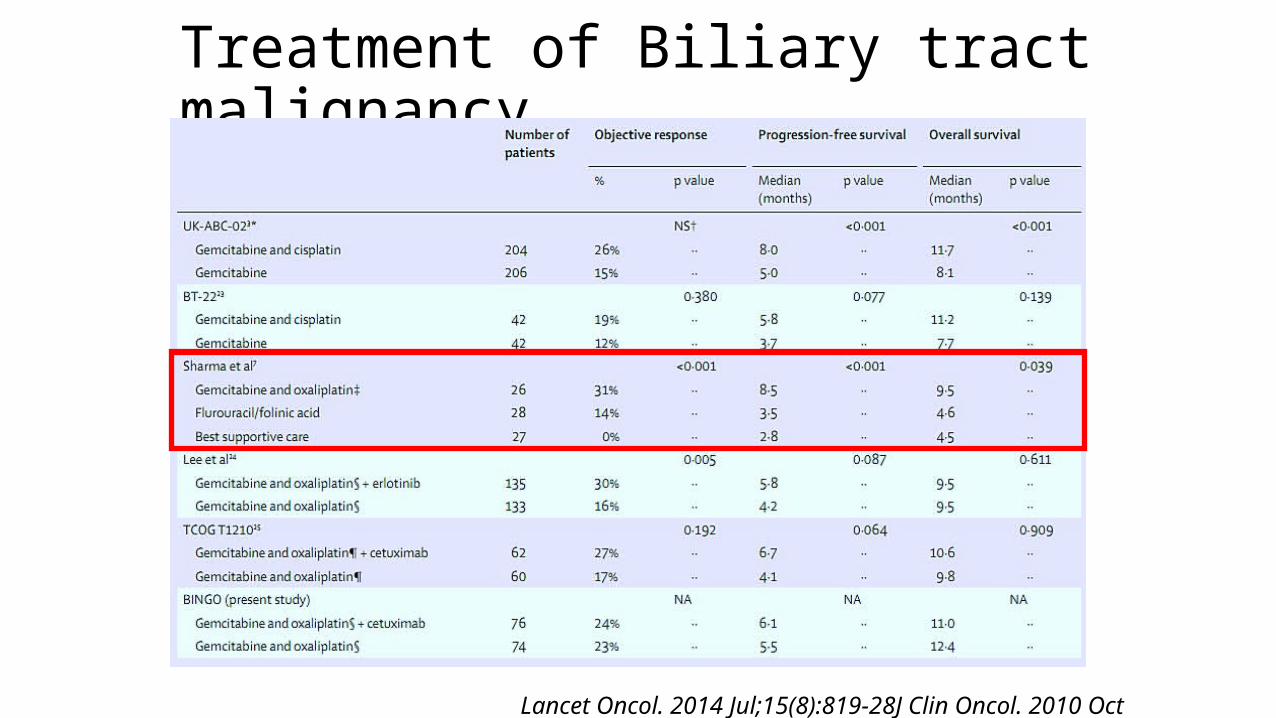
Treatment of Biliary tract malignancy
Lancet Oncol. 2014 Jul;15(8):819-28J Clin Oncol. 2010 Oct 20;28(30):4581-6.
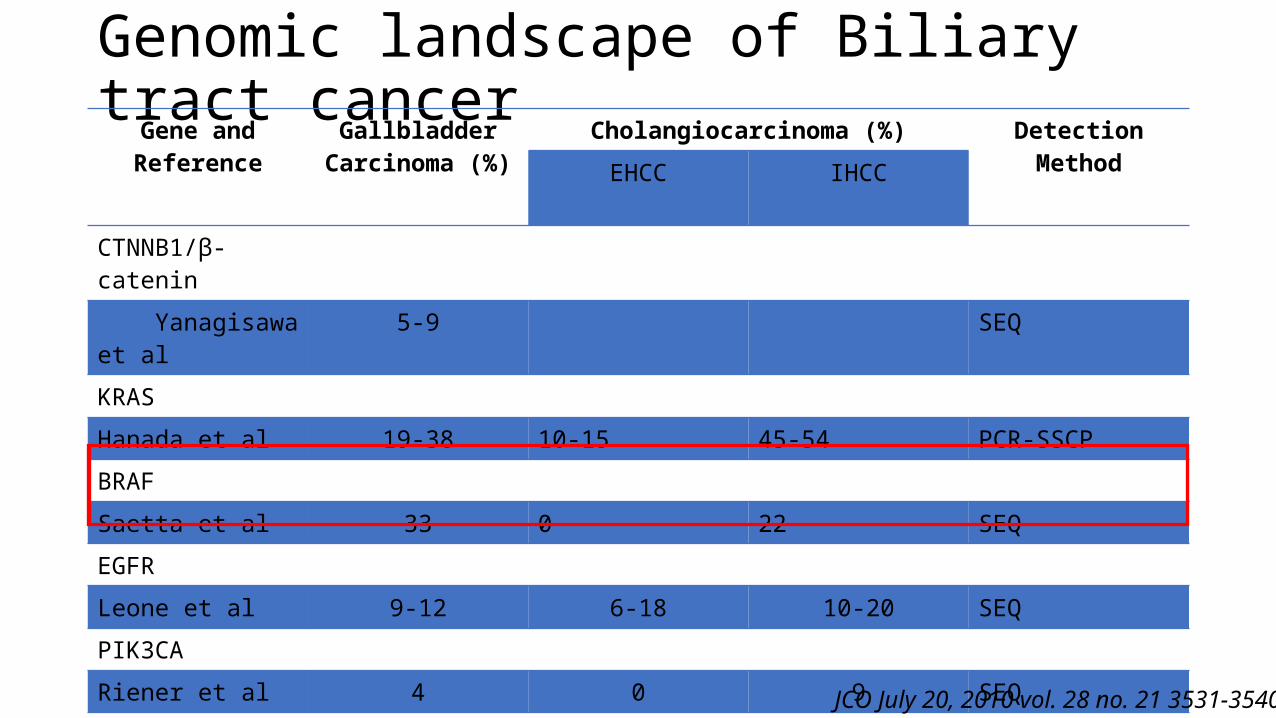
Genomic landscape of Biliary tract cancer Gene and Reference Gallbladder
Carcinoma (%)Cholangiocarcinoma (%) Detection Method
EHCC IHCC
CTNNB1/β-catenin
Yanagisawa et al
5-9 SEQ
KRAS
Hanada et al 19-38 10-15 45-54 PCR-SSCP
BRAF
Saetta et al 33 0 22 SEQ
EGFR
Leone et al 9-12 6-18 10-20 SEQ
PIK3CA
Riener et al 4 0 9 SEQ
ERBB2/HER2
Nakazawa et al 16 5 0 IHC and FISHJCO July 20, 2010 vol. 28 no. 21 3531-3540
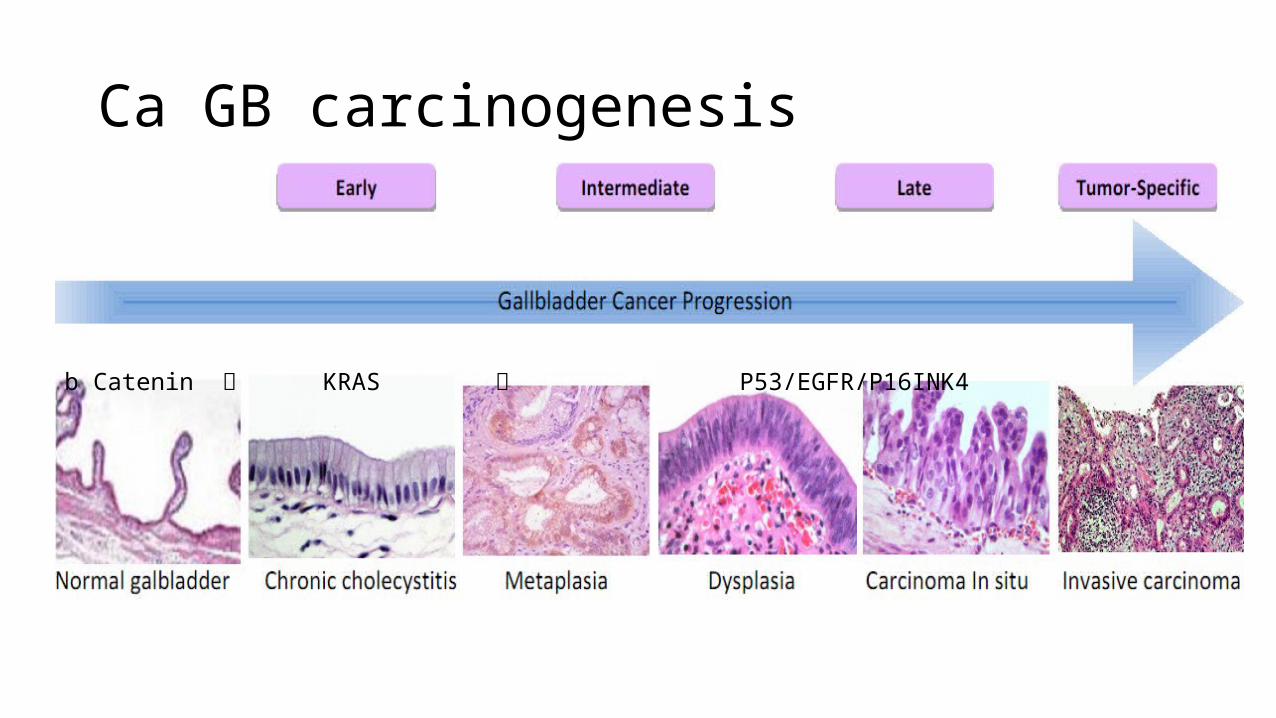
Ca GB carcinogenesis
• GB Ca Cholangiocarcinoma
b Catenin KRAS P53/EGFR/P16INK4
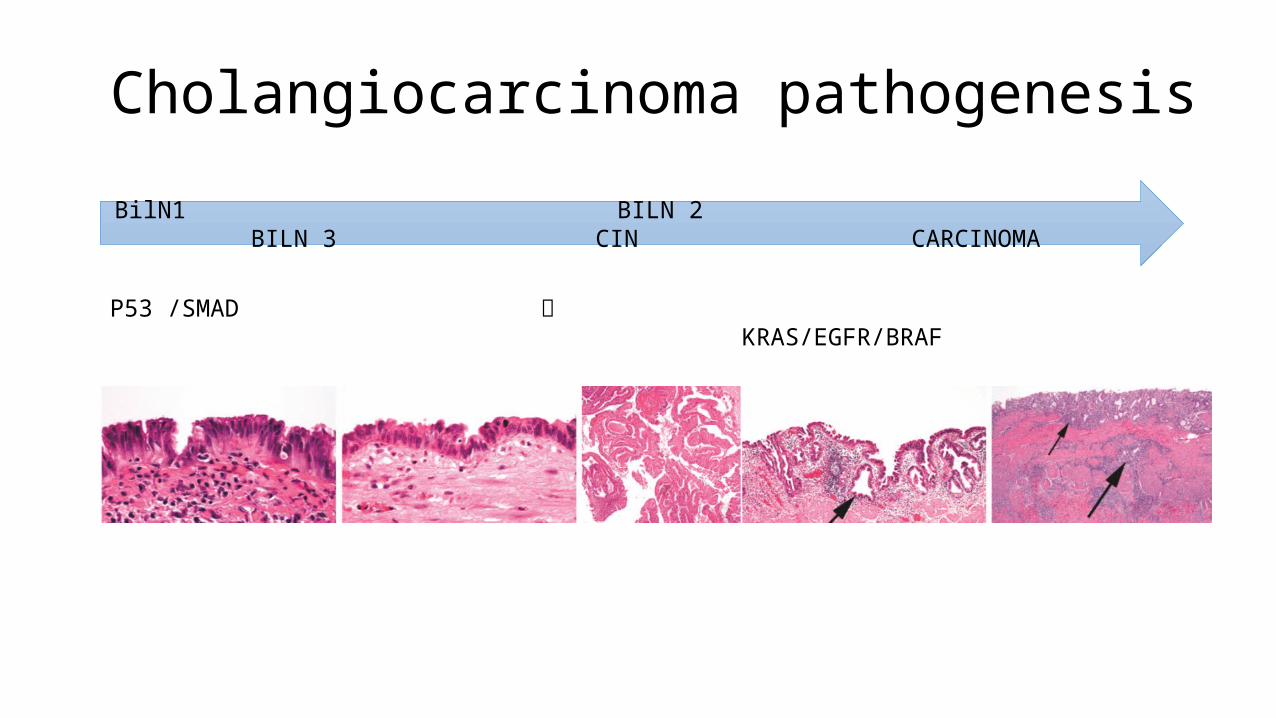
Cholangiocarcinoma pathogenesis
BilN1 BILN 2 BILN 3 CIN CARCINOMA
P53 /SMAD KRAS/EGFR/BRAF
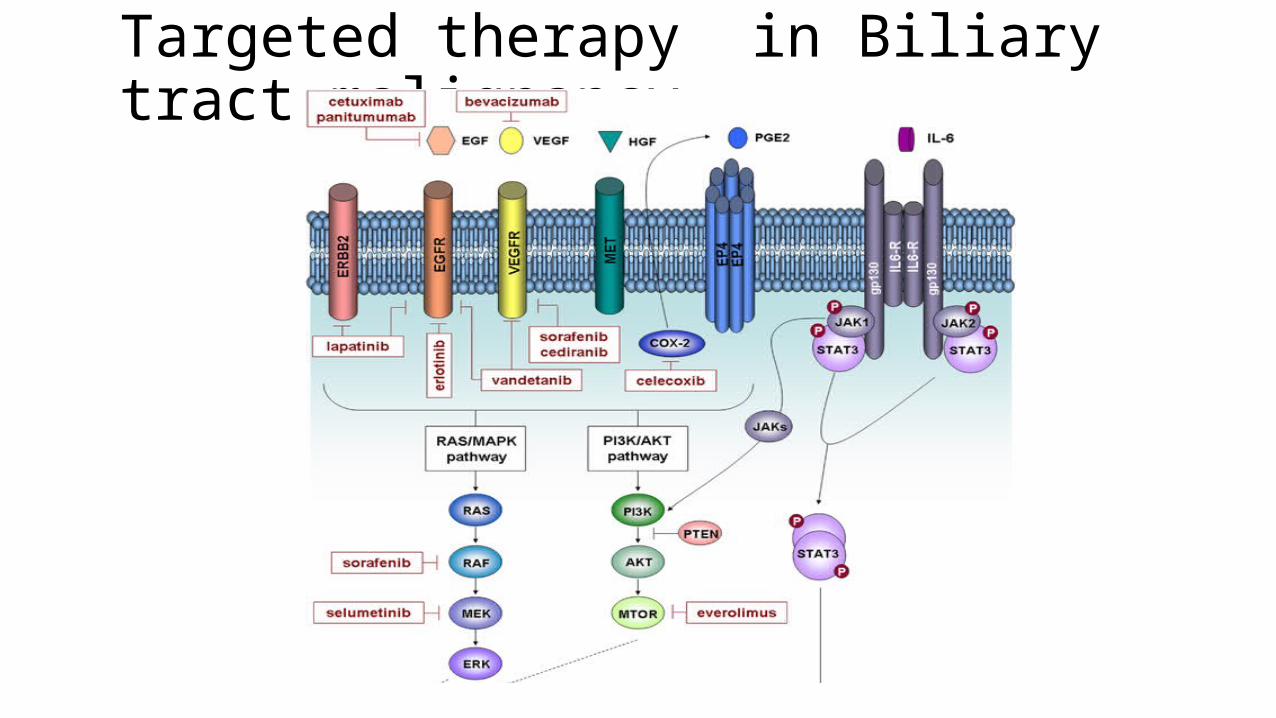
Targeted therapy in Biliary tract malignancy

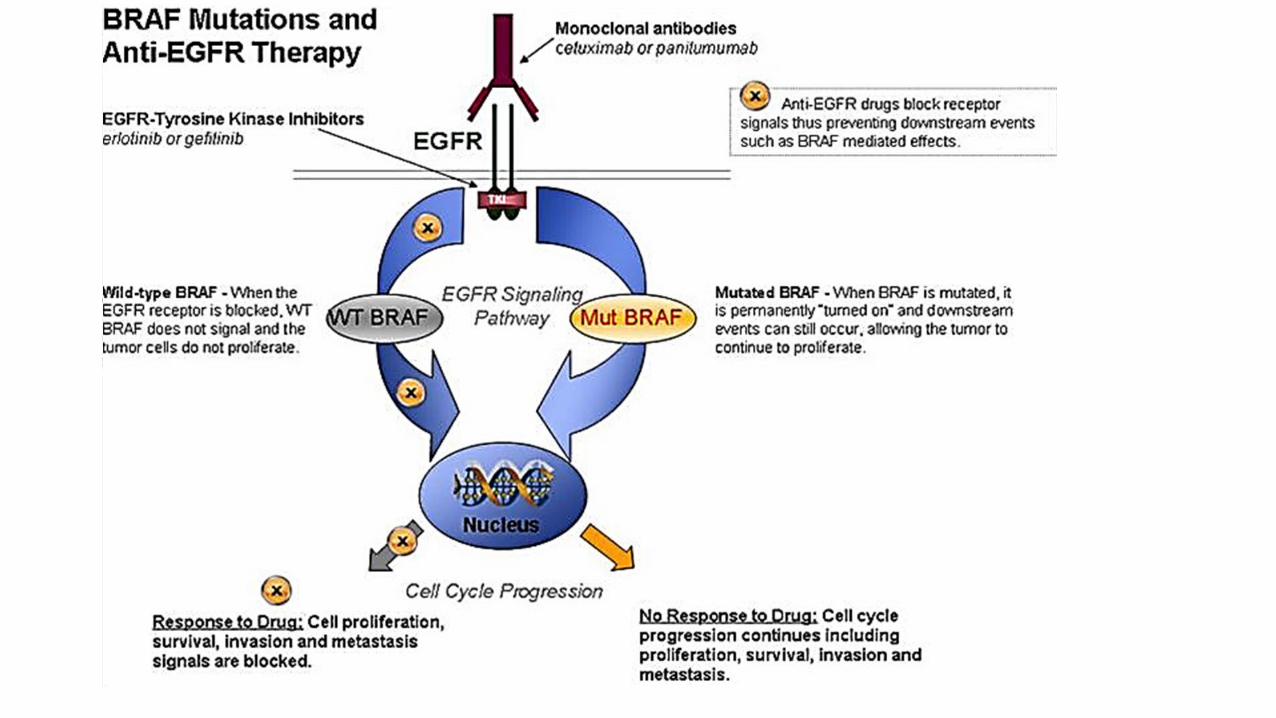
EGFR-MAb and Chemotherapy
• blocks EGFR nuclear import
EGFR Mab
• DNA Repair enzyme
Inhibits
• Oxaliplatin induced DNA damage
Augments
EGFR Mab+Chemotherapy
Synergism
Mahtani R.The Oncologist January 2008 vol. 13 no. 1 39-50
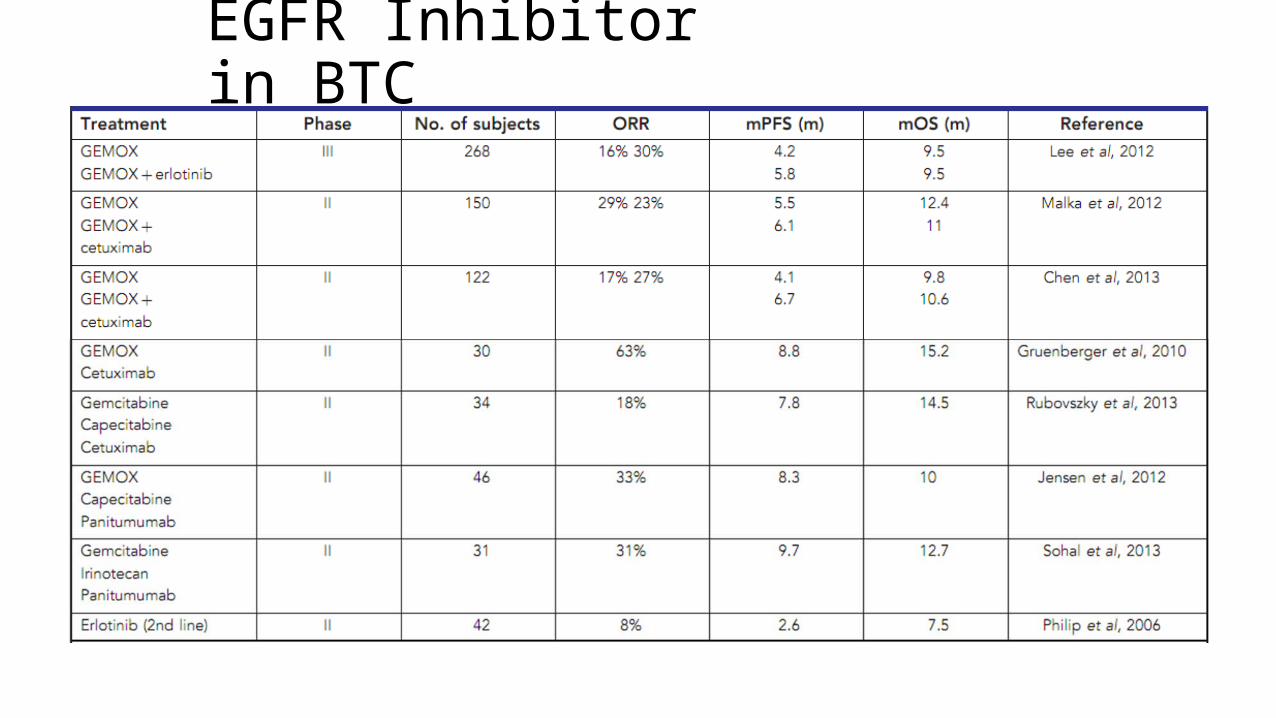
EGFR Inhibitor in BTC
Study Methodology
Open labelsingle-arm phase II studyMulticentric 7 center in USA
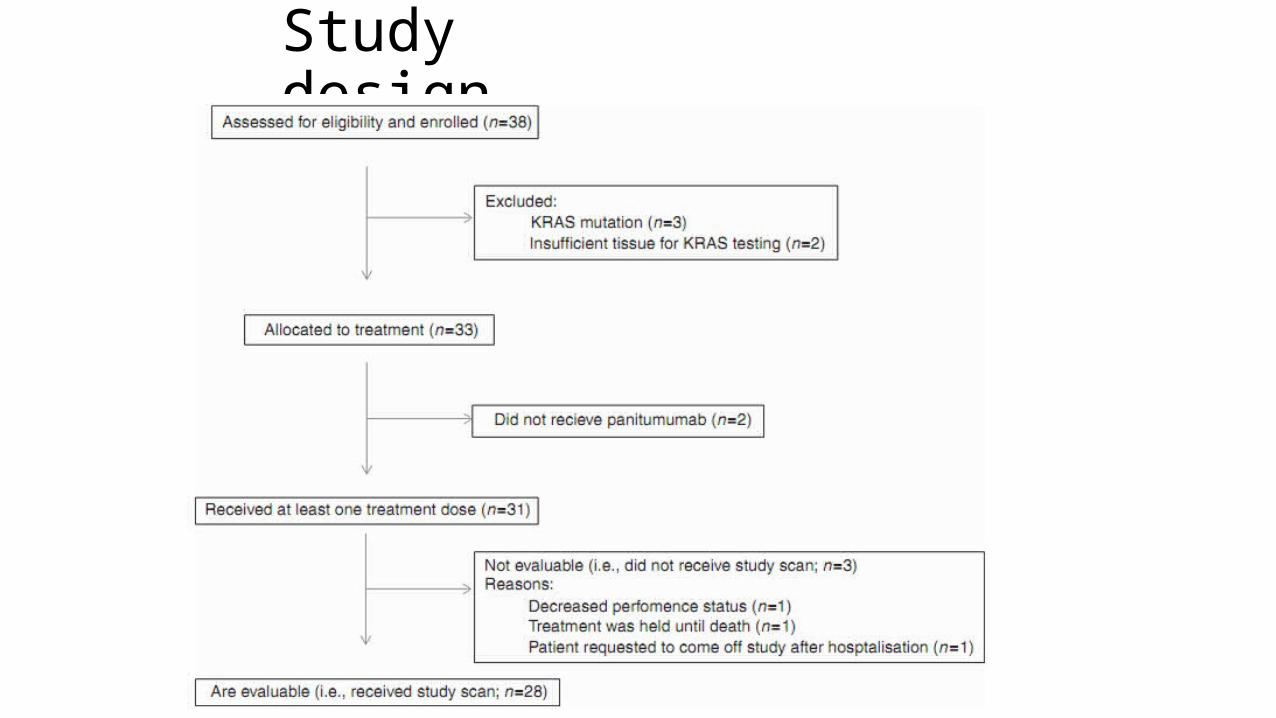
Study design
Inclusion criteria
Metastatic or unresectable KRAS WT biliary tract adenocarcinoma(bile ducts, hepatic duct, cystic duct, common bile duct, ampulla of Vater or gallbladder adenocarcinoma)
>18 yearNo history of chemotherapy or anti-EGFR therapy ECOG performance status of 0 or 1 Adequate hepatic, renal and hematologic function
Exclusion criteria
Patients with concurrent malignancies Patients with known brain metastasis Pre-existing grade 2 or higher peripheral neuropathy
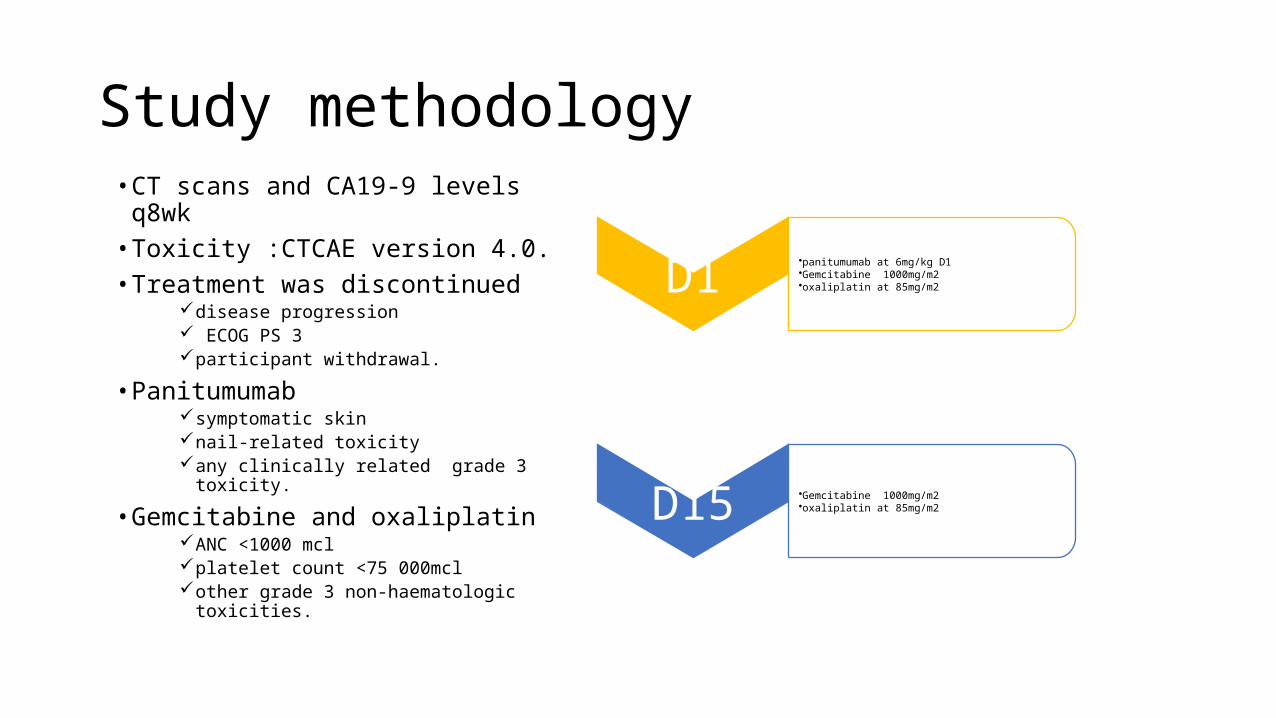
Study methodology• CT scans and CA19-9 levels q8wk • Toxicity :CTCAE version 4.0. • Treatment was discontinued
disease progression ECOG PS 3 participant withdrawal.
• Panitumumab symptomatic skin nail-related toxicity any clinically related grade 3 toxicity.
• Gemcitabine and oxaliplatin ANC <1000 mcl platelet count <75 000mcl other grade 3 non-haematologic
toxicities.
D1•panitumumab at 6mg/kg D1•Gemcitabine 1000mg/m2•oxaliplatin at 85mg/m2
D15 •Gemcitabine 1000mg/m2•oxaliplatin at 85mg/m2
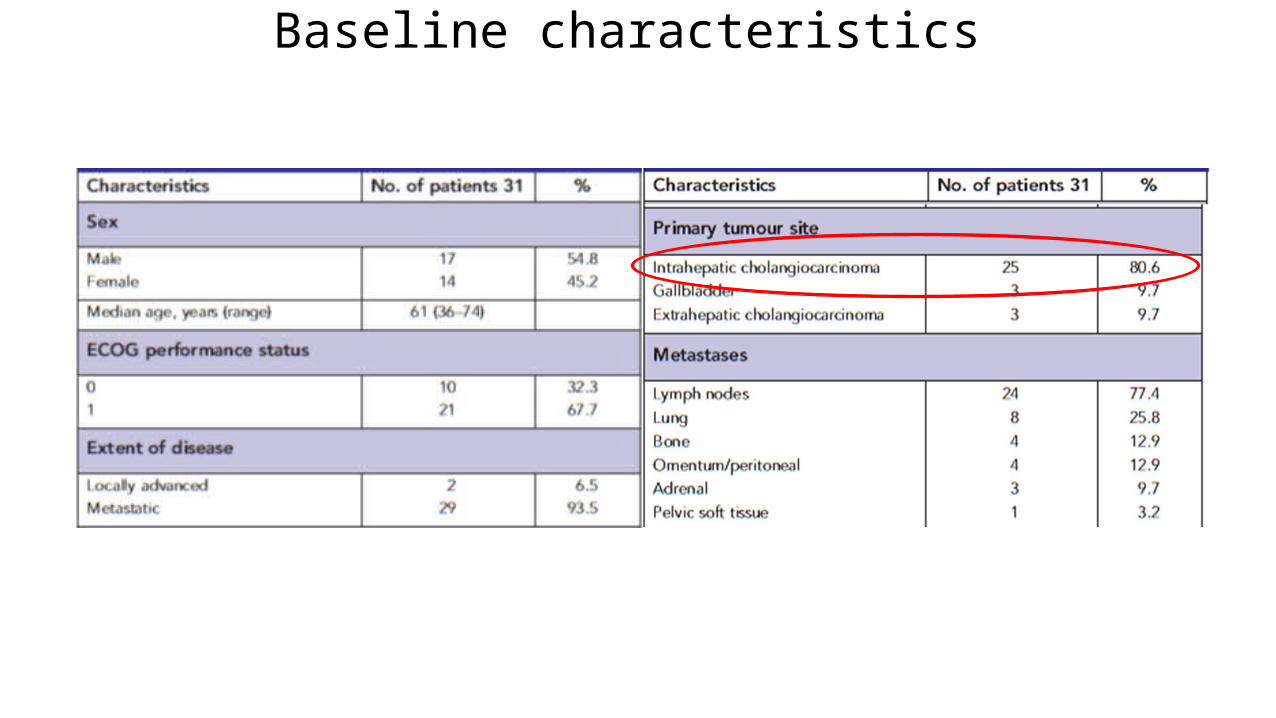
Baseline characteristics
Statistical analysis• Intention-to-treat (ITT) principles• The primary endpoint :radiographic response rate by RECIST • secondary endpoints :PFS, OS and toxicity. • sample size of 30 • power of 80% with a type 1 error set at 0.10.• PFS:The time from study enrolment to date of cancer progression or
death, whichever occurred first• OS : the time of enrolment in the study until the date of death from
any cause. The survival analysis calculated by Kaplan–Meier. • SAS software (v9.3; SAS Institute, Cary,NC, USA)
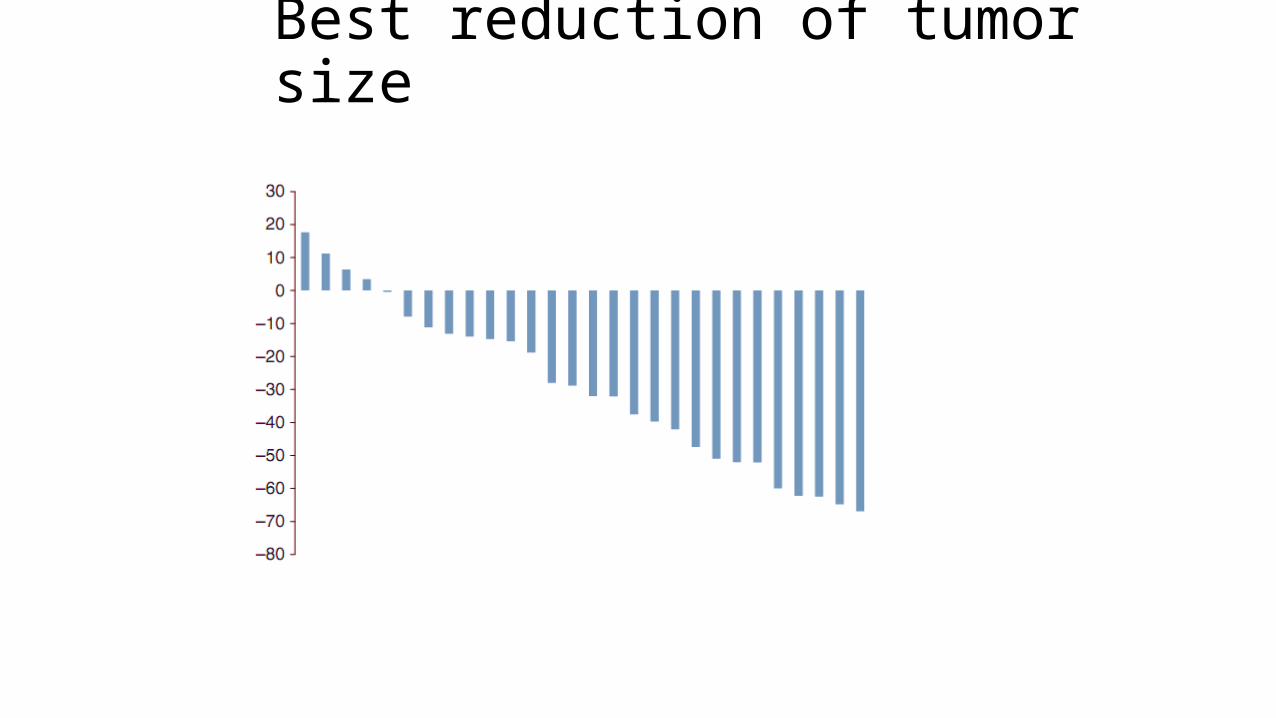
Best reduction of tumor size
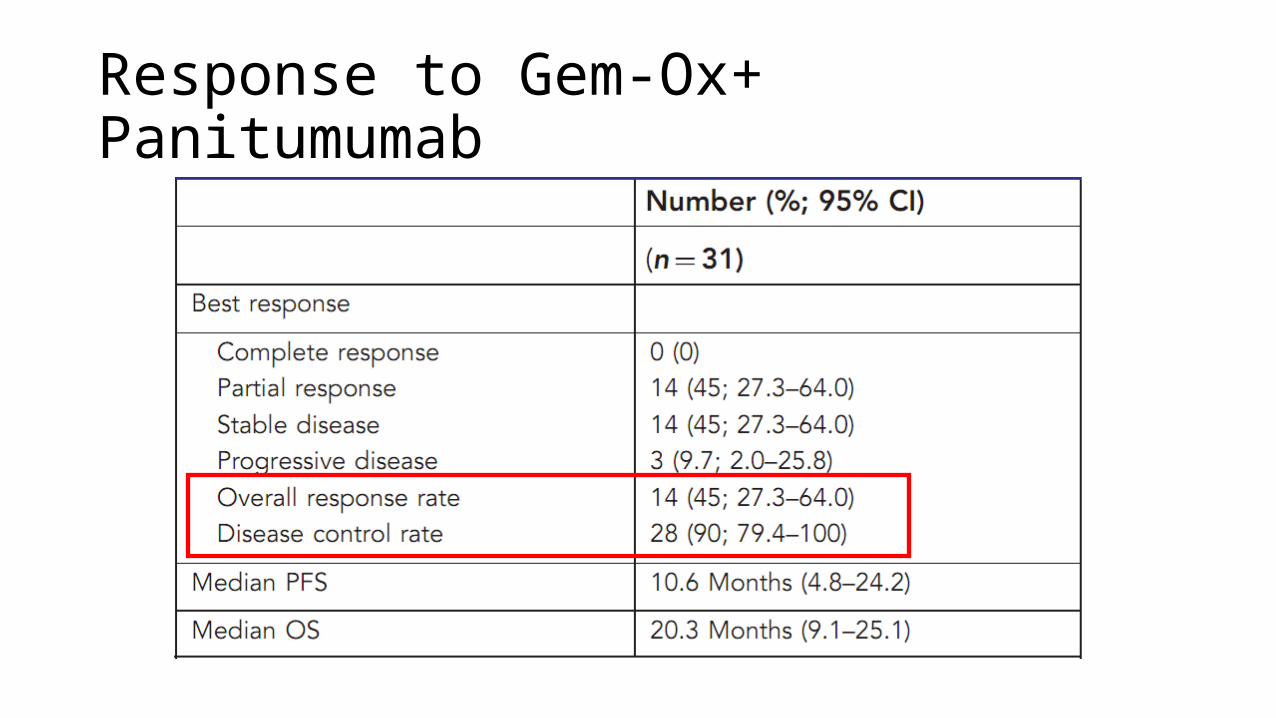
Response to Gem-Ox+ Panitumumab
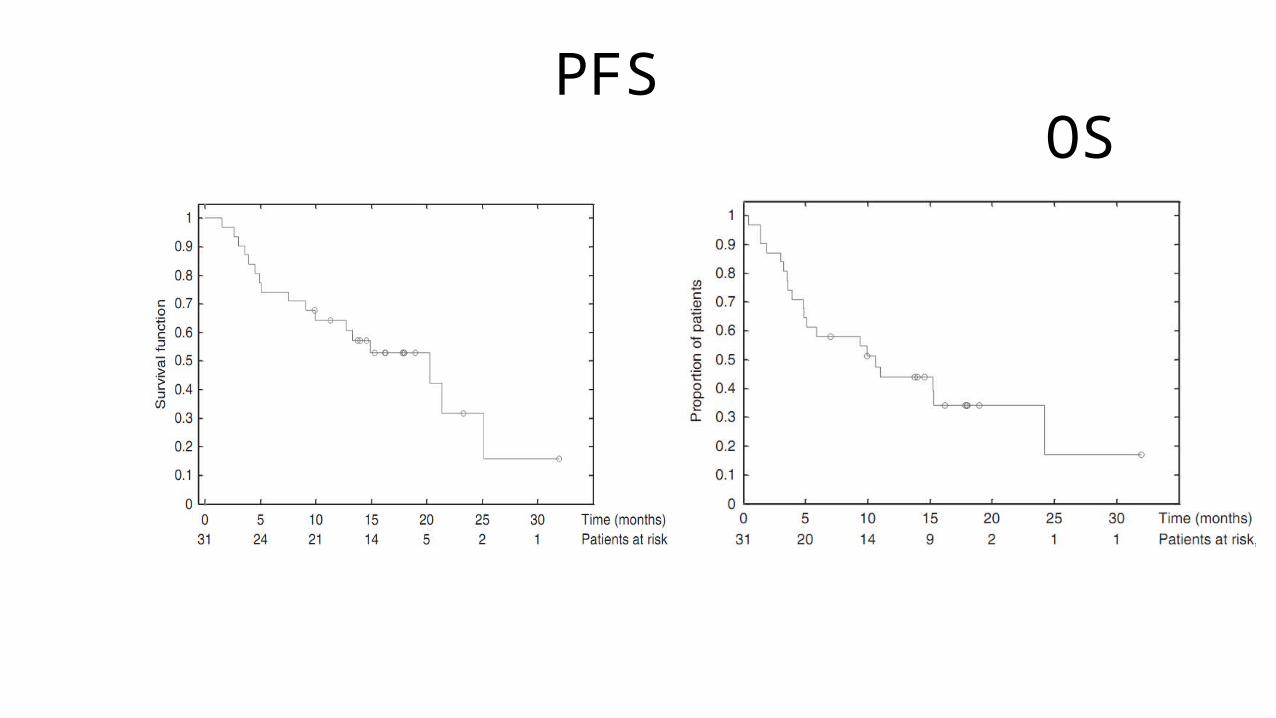
PFS OS
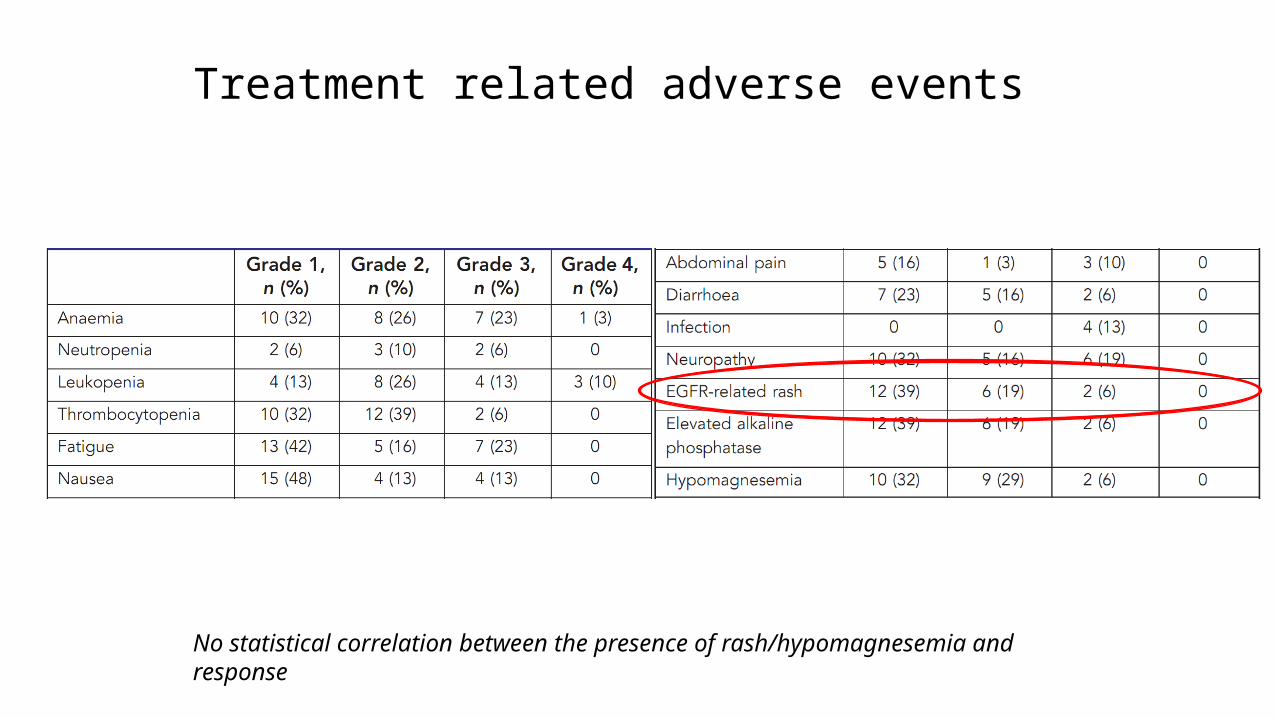
Treatment related adverse events
No statistical correlation between the presence of rash/hypomagnesemia and response
Discussion
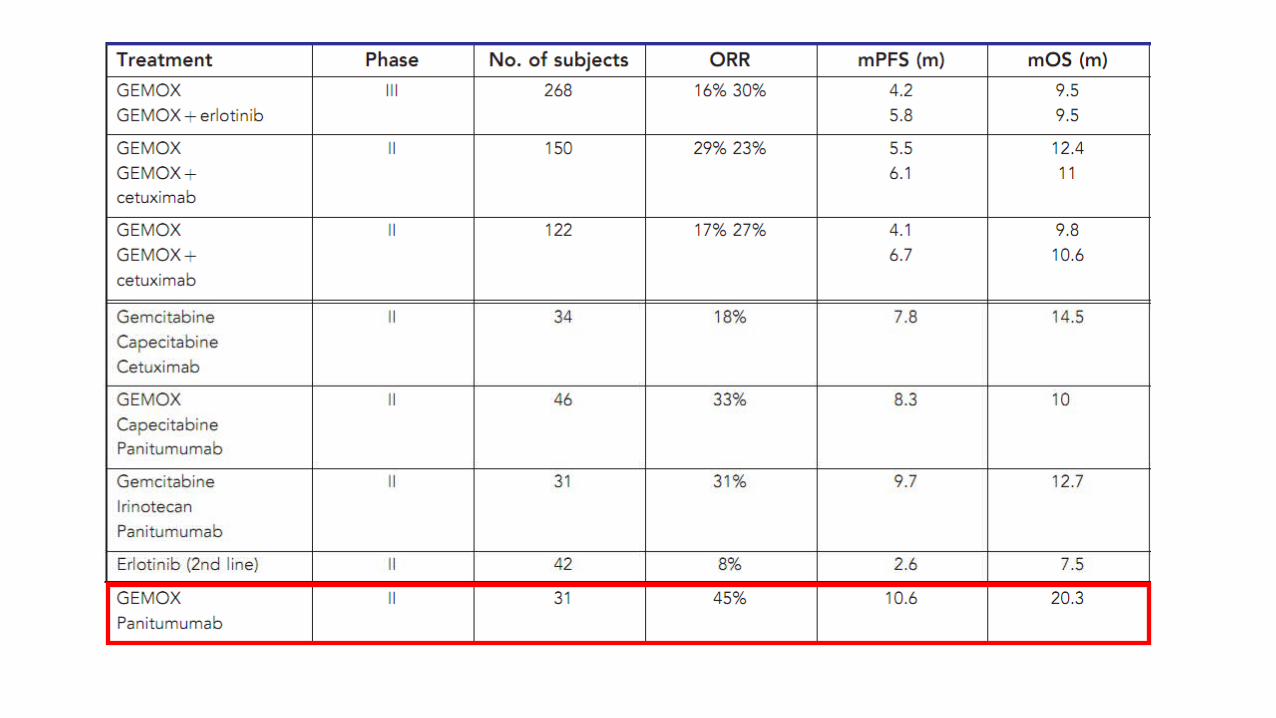
• This open-label phase II trial was designed to evaluate the efficacy of panitumumab to GemOx among selected patients with a KRAS WT allele.• Response rate of 50%, in evaluable patients and 45% in patients who
received at least one dose of study drug.• The median PFS was 10.6 months and median OS 20.3 months.• The combination of gemcitabine, oxaliplatin and panitumumab was
well tolerated with manageable grade 3 and 4 toxicities
Critical appraisal
Sample size Adequate :30 patients was required to achieve with power of 80% to detect an absolute difference in response rate of20% (50% vs 30%) using a one-sided binomial test with a type 1error set at 0.102. Statistics well defined
Combinations regimen chosen: A large effect demonstrated Preclinical synergy
Pre specified improvement in response rate compared to historical data :Done
Journal of Clinical Oncology, Vol 27, No 19 (July 1), 2009: pp 3073-3076
Critical appraisal
Sample size adequate
Statistics well defined yes
Novel single agent tested yes
Pre specified improvement in response rate compared to historical data
yes
Ongoing phase 3 trial on basis of this trial yes
End point tailored to drug’s mechanism of action
ORR
Appropriate criteria for assessment yes
In the sea of pessimism about Ca GBstill there is hope……
Thank You












![Chapter 22 – Introduction to Electroanalytical Chemistry 22 – Introduction to... · Indicator Electrode Reference Electrode Ox Ox Ox log[ ] 0.0592 ( . ) Ox z E ind vsref L No](https://static.fdocuments.in/doc/165x107/614862c82918e2056c22a781/chapter-22-a-introduction-to-electroanalytical-chemistry-22-a-introduction-to.jpg)





