
Gatos Questionnaire for Early Detection of Suspicious...
17
International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 http://www.sciencepublishinggroup.com/j/ijpbs doi: 10.11648/j.ijpbs.20160103.15 Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results Gregory Tsoucalas * , Stamati Bourelia, Anastasios Markellos, Vasiliki Kalogirou, Styliani Giatsiou, Olga Repana, Presveia Gatou, Ifigeneia Georgousi, Anna Maria Xanthi, Andromachi Korenti, Nikolaos Kosmas, Antonios Antoniou, Konstantinos Gatos Interdisciplinary Study Team, Neurological Clinic-Hellenic Reference for Alzheimer Disease and Dementia Related Syndromes Agios Georgios, Alykes Volou, Greece Email address: [email protected] (G. Tsoucalas) * Corresponding author To cite this article: Gregory Tsoucalas, Stamati Bourelia, Anastasios Markellos, Vasiliki Kalogirou, Styliani Giatsiou, Olga Repana, Presveia Gatou, Ifigeneia Georgousi, Anna Maria Xanthi, Andromachi Korenti, Nikolaos Kosmas, Antonios Antoniou, Konstantinos Gatos. Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results. International Journal of Psychological and Brain Sciences. Vol. 1, No. 3, 2016, pp. 69-85. doi: 10.11648/j.ijpbs.20160103.15 Received: November 9, 2016; Accepted: December 9, 2016; Published: December 20, 2016 Abstract: Dementia presents a cluster of syndromes the effect human brain. It rises various social-economic and health care issues that are difficult to be confronted. Early detection of the possibility of an examinee to be inflicted by a dementia syndrome is an all neurologists quest. Our interdisciplinary team for some year know created a questionnaire that depicts a series of items that could have been changed before the diagnosis of a dementia to be set. Material and Method: More than 180 items were included in the questionnaire. The validation process excluded 26 items. Then n 1 =55 examinees enrolled to our study in order to be watched for 5 years (n 2 =26 were diagnosed with dementia). At the end of this period 26 were inflicted by a dementia (mostly Alzheimer disease and vascular dementia). All answered the GQEDSS - ADRDS Q160 v 1.0 (3 demographic items and 157 Likert scale items), and the MMSE questionnaires. A statistical analysis of the questionnaire was followed. The scree test formed 54 factors, followed by a key item analysis (15 key items) to simplify factors analysis' complexity. Conver- gent or Criterion validity of the GQEDSS - ADRDS questionnaire was determined by establishing its correlation to the MMSE score using the Pearson’s correlation coefficient. Discriminant validity tested whether concepts or measurements that are supposed to be unrelated are, in fact, unrelated. Internal consistency validity of the GQEDSS - ADRDS was determined by calculating Cronbach alpha coefficient. Test-retest reliability (stability) was also performed. Results: The Bartlett Test of Sphericity was 2527.2 and it was significant (p<0.0015). The Kaiser-Meyer-Olkin Measure of Sampling Adequacy was equal to 0.801 showing that the data is suitable for factor analysis. The 160 items were analysed via maximum likelihood extraction method using a Varimax rotation. The correlation coefficients presented p<0.0005. The cut-off points (total summary of 700 scoring points) were set to a: a) < 120, there is a relatively small change, b) 121-180, there is a mediocre change, c) 181-220, there is a relatively good change, and d) >221, there is a relatively high change. Discussion: Although our study presents an intriguing questionnaire, our sample does not meet the Stevens' criteria. Small sample, examiners' subjectivity, non-randomized sample - Convenience, or consecutive sampling (all clients in the outpatient clinic), questionnaire longevity could present a series of BIASes. More study, co-operation with other specialized centres, and a better methodology are required. Keywords: Dementia, Early Detection, Questionnaire 1. Introduction Dementias present a cluster of clinical syndromes characterized of a widespread progressive deterioration of cognitive abilities. This impairment interferes with normal daily functioning posing considerable challenges to patients and their caregivers. Over 70 different causal entities for
Transcript of Gatos Questionnaire for Early Detection of Suspicious...

International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85
http://www.sciencepublishinggroup.com/j/ijpbs
doi: 10.11648/j.ijpbs.20160103.15
Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results
Gregory Tsoucalas*, Stamati Bourelia, Anastasios Markellos, Vasiliki Kalogirou, Styliani Giatsiou,
Olga Repana, Presveia Gatou, Ifigeneia Georgousi, Anna Maria Xanthi, Andromachi Korenti,
Nikolaos Kosmas, Antonios Antoniou, Konstantinos Gatos
Interdisciplinary Study Team, Neurological Clinic-Hellenic Reference for Alzheimer Disease and Dementia Related Syndromes Agios
Georgios, Alykes Volou, Greece
Email address:
[email protected] (G. Tsoucalas) *Corresponding author
To cite this article: Gregory Tsoucalas, Stamati Bourelia, Anastasios Markellos, Vasiliki Kalogirou, Styliani Giatsiou, Olga Repana, Presveia Gatou, Ifigeneia
Georgousi, Anna Maria Xanthi, Andromachi Korenti, Nikolaos Kosmas, Antonios Antoniou, Konstantinos Gatos. Gatos Questionnaire for
Early Detection of Suspicious Signs for Alzheimer Disease and Related Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary
Results. International Journal of Psychological and Brain Sciences. Vol. 1, No. 3, 2016, pp. 69-85. doi: 10.11648/j.ijpbs.20160103.15
Received: November 9, 2016; Accepted: December 9, 2016; Published: December 20, 2016
Abstract: Dementia presents a cluster of syndromes the effect human brain. It rises various social-economic and health care
issues that are difficult to be confronted. Early detection of the possibility of an examinee to be inflicted by a dementia
syndrome is an all neurologists quest. Our interdisciplinary team for some year know created a questionnaire that depicts a
series of items that could have been changed before the diagnosis of a dementia to be set. Material and Method: More than 180
items were included in the questionnaire. The validation process excluded 26 items. Then n1=55 examinees enrolled to our
study in order to be watched for 5 years (n2=26 were diagnosed with dementia). At the end of this period 26 were inflicted by a
dementia (mostly Alzheimer disease and vascular dementia). All answered the GQEDSS - ADRDS Q160 v 1.0 (3 demographic
items and 157 Likert scale items), and the MMSE questionnaires. A statistical analysis of the questionnaire was followed. The
scree test formed 54 factors, followed by a key item analysis (15 key items) to simplify factors analysis' complexity. Conver-
gent or Criterion validity of the GQEDSS - ADRDS questionnaire was determined by establishing its correlation to the MMSE
score using the Pearson’s correlation coefficient. Discriminant validity tested whether concepts or measurements that are
supposed to be unrelated are, in fact, unrelated. Internal consistency validity of the GQEDSS - ADRDS was determined by
calculating Cronbach alpha coefficient. Test-retest reliability (stability) was also performed. Results: The Bartlett Test of
Sphericity was 2527.2 and it was significant (p<0.0015). The Kaiser-Meyer-Olkin Measure of Sampling Adequacy was equal
to 0.801 showing that the data is suitable for factor analysis. The 160 items were analysed via maximum likelihood extraction
method using a Varimax rotation. The correlation coefficients presented p<0.0005. The cut-off points (total summary of 700
scoring points) were set to a: a) < 120, there is a relatively small change, b) 121-180, there is a mediocre change, c) 181-220,
there is a relatively good change, and d) >221, there is a relatively high change. Discussion: Although our study presents an
intriguing questionnaire, our sample does not meet the Stevens' criteria. Small sample, examiners' subjectivity, non-randomized
sample - Convenience, or consecutive sampling (all clients in the outpatient clinic), questionnaire longevity could present a
series of BIASes. More study, co-operation with other specialized centres, and a better methodology are required.
Keywords: Dementia, Early Detection, Questionnaire
1. Introduction
Dementias present a cluster of clinical syndromes
characterized of a widespread progressive deterioration of
cognitive abilities. This impairment interferes with normal
daily functioning posing considerable challenges to patients
and their caregivers. Over 70 different causal entities for

International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 70
dementia have been described. Alzheimer's disease is the
most common cause of dementia but not all dementia is due
to Alzheimer's. Thus vascular dementia has a significant
prevalence among the general population. Despite the
heterogeneity in etiology, dementias affect the mental
competence, memory and learning abilities, speech,
orientation, balance, gait, perception, concentration,
judgment, problem solving ability and social functioning.
Emotions and personality are impaired, the patient
progressively deteriorates and finally becomes incapable
even to complete elementary mental functions. Dementias are
a serious public health problem, with many social and
economic dimensions, as care needs for dementia patients
build up over time [1-2].
It is proven that dementias are not restricted to elderly
only, but they could also attack people younger than 60 years
old. The progressive and mostly irreversible nature of
dementias along with their impact on health system and
society calls for early diagnosis. Early detection of dementia
is essential to guide front-line health care practitioners in
further clinical evaluations and give neurologists time to
develop and implement of preventive and therapeutic
treatments [3].
International medical literature provides a series of shorter
or longer screening tools, batteries combining small cognitive
tests and questions to unveil possible brain fuctional damage.
The most important are: Seven minute neurocognitive
screening battery (7MS), the Memory Impairment Screen
(MIS), the clock drawing test, the cube-copying test, the
DemTect, the AB Cognitive Screen (ABCS), the AD8, the
Montreal Cognitive Assessment (MoCA), the Short
Cognitive Performance Test, the Addenbrooke’s Cognitive
Examination Revised (ACE-R), the Memory Alteration Test
(MAT), the Memory Orientation Screening Test (MOST), the
Mini Mental State Examination severe (MMSE-s), the Severe
Impairment Battery (SIB), and finally the first version of the
worldwide famous Mini Mental State Examination (MMSE)
[4-5].
The MMSE, as a brief mental status examination is a
useful short screening tool, which must be accompanied by a
detailed assessment of individual cognitive and should be
always subject to criticism when it is not aligned with the
patient’s clinical picture. It has been emerged as a useful tool
for physicians regardless of specialty, and allows a gross
approach to the patient's condition, irrelevant of medication
or comorbidities. The MMSE ranges are 30 scoring points for
no, 26-29 for questionable, 21-25 for mild, 11-20 for
moderate, and 0-10 for severe dementia. However, MMSE
does not interfere with quality of life, it is not a prognostic
tool for dementia course, and it does not discriminate
reversible disease, while other conditions, such as delirium,
bipolar disorder, or mental retardation often lead to low
scores in MMSE and patients misclassification [6-7].
This study focuses on the earliest changes in
neuropsychological functioning, hoping to present a new
useful screening questionnaire for the early detection of
impairment by reviewing a plethora of cognitive, functional
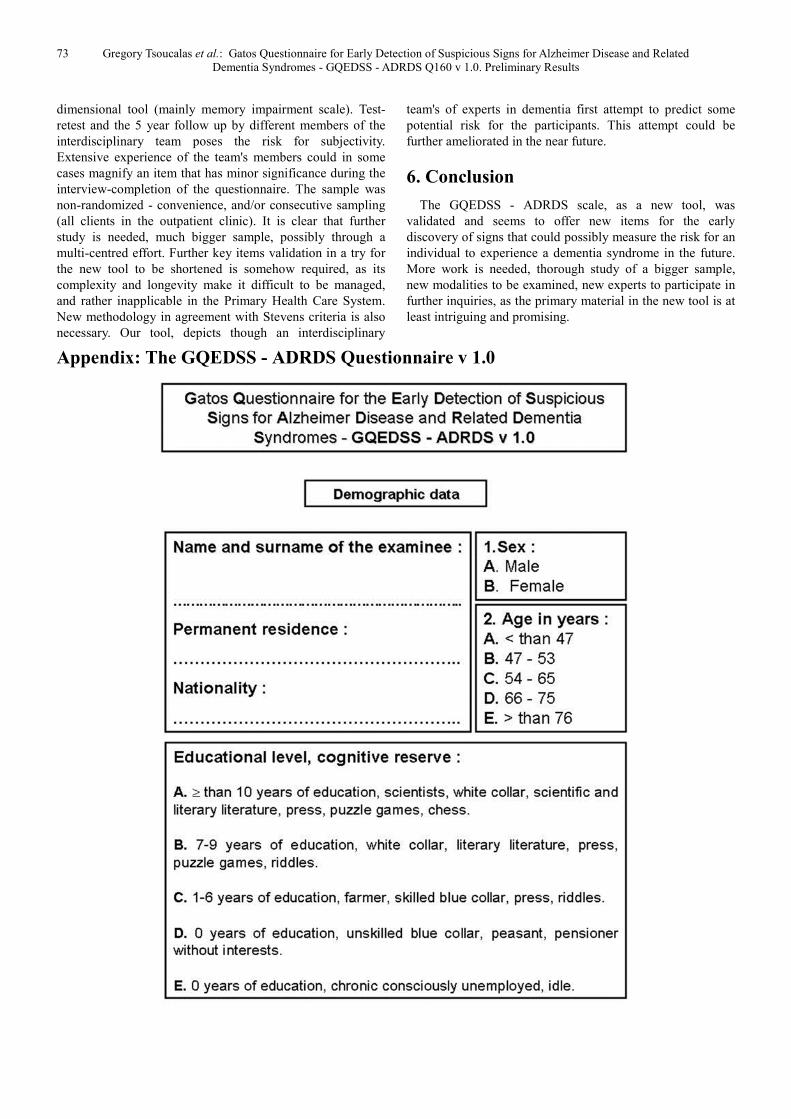
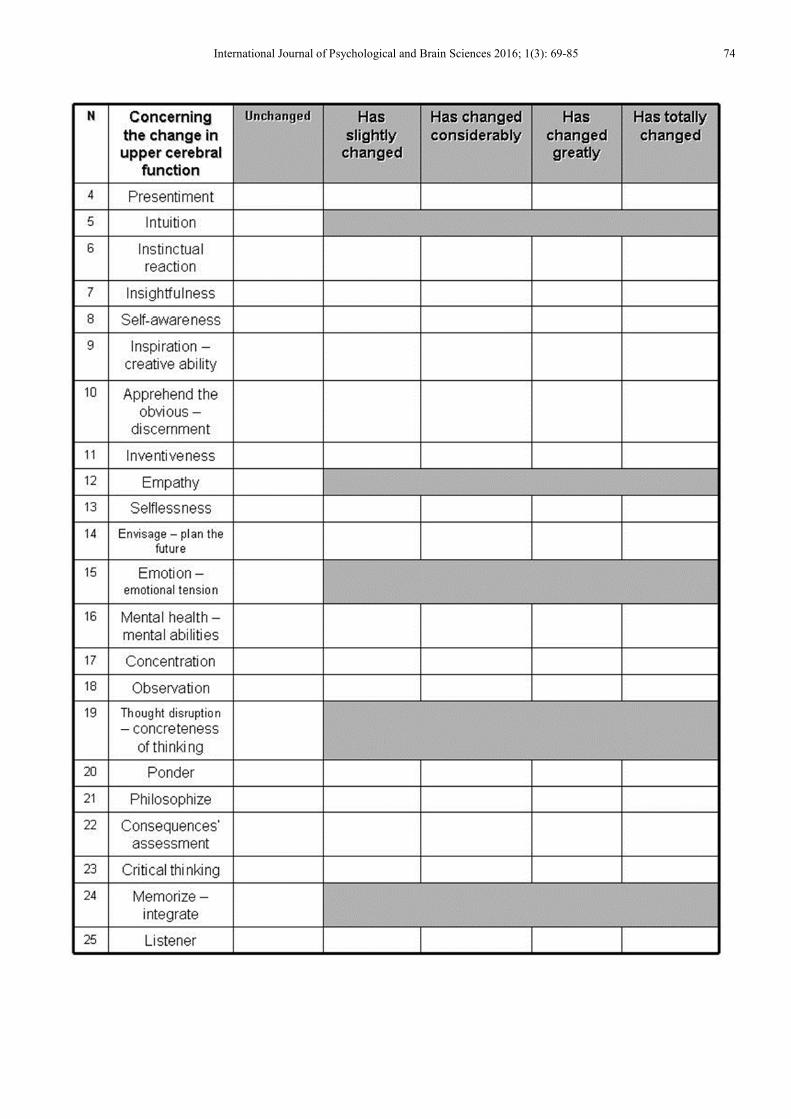
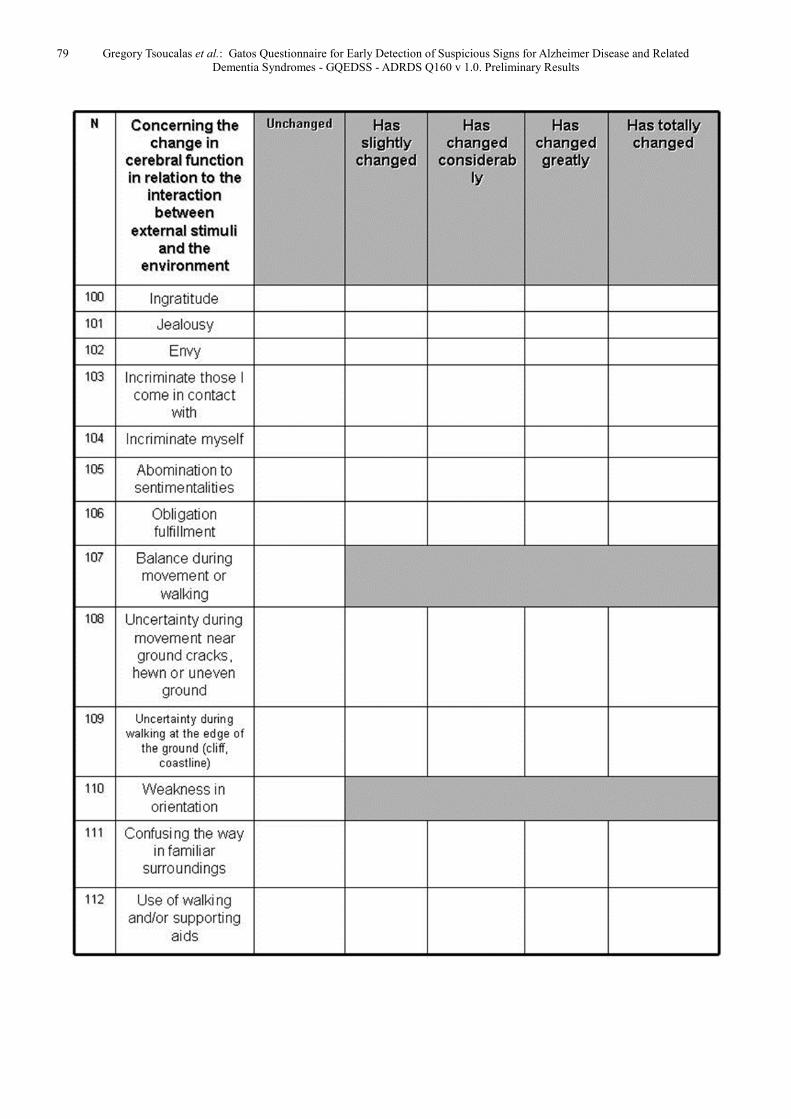
and socializing data. Our questionnaire is separated into 4
sectors: i) demographic data, ii) concerning the change in
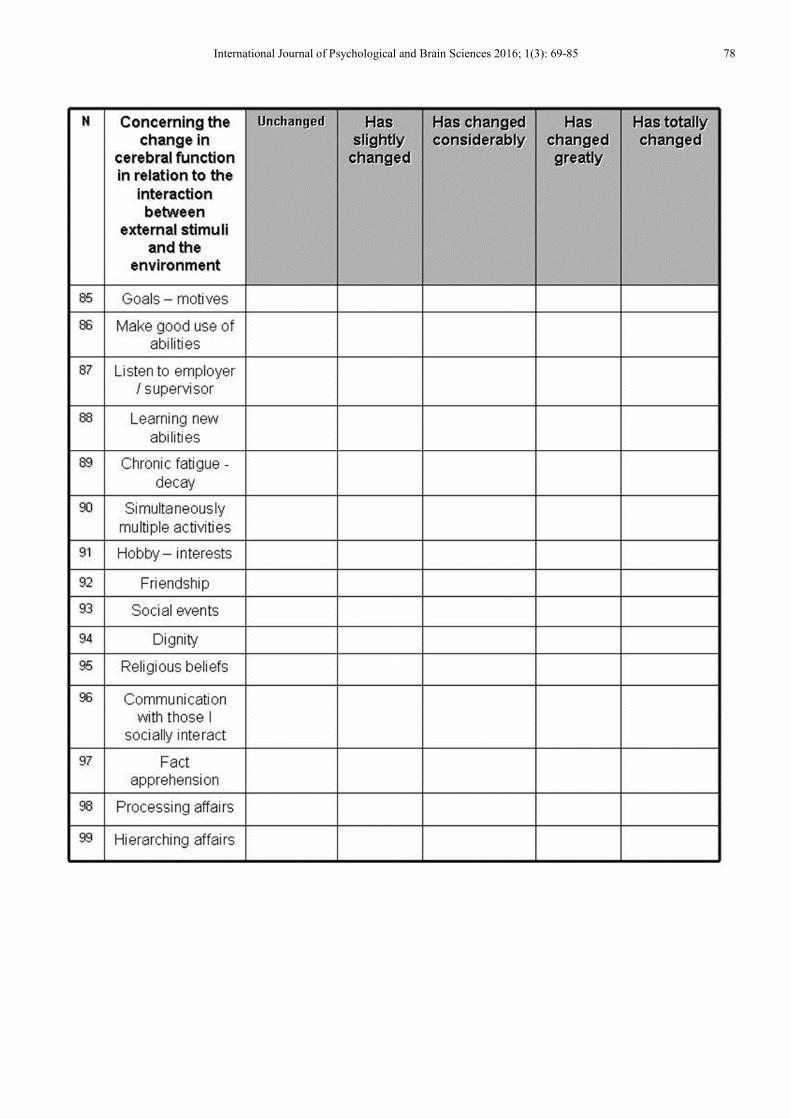
upper cerebral functions, iii) concerning the change in
cerebral function in relation to the interaction between both
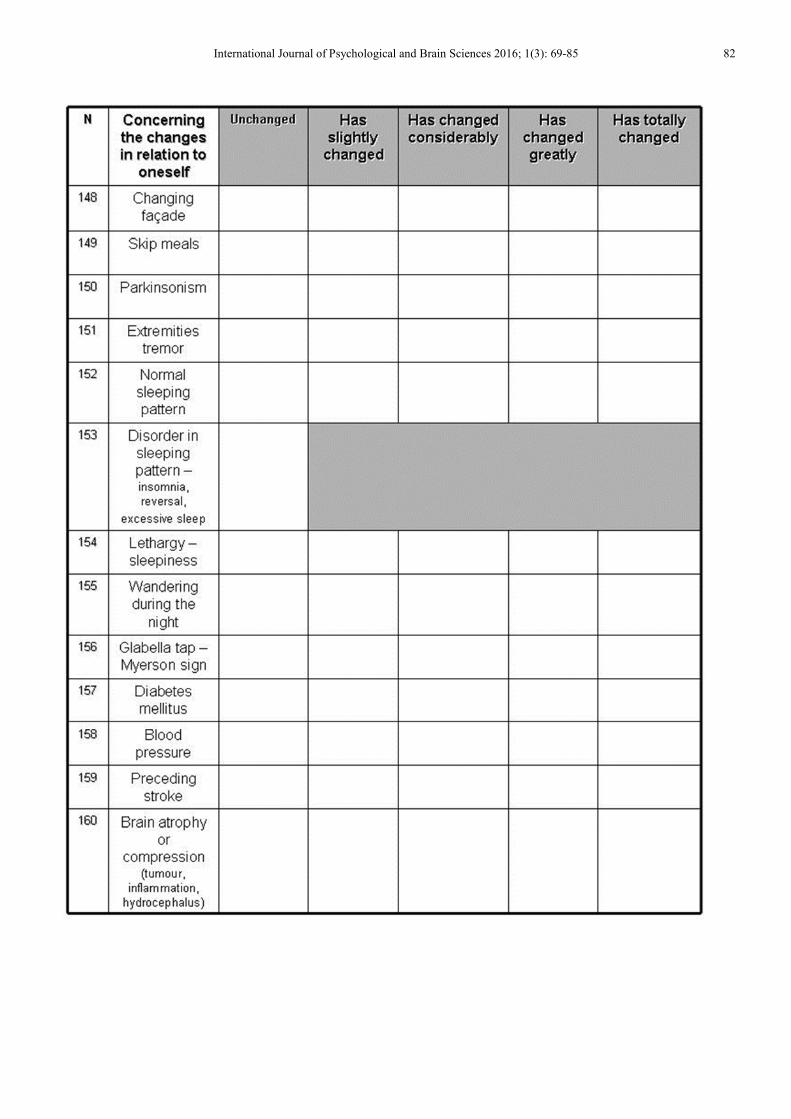
the external stimuli and the environment, and iv) concerning
the changes in relation to oneself, while it contains 160
points-characteristics to be evaluated.
2. Material and Method
A panel of ten, dementia specialized health professionals
were engaged in the validation process. For every item to win
its place in the questionnaire, every team member assessed
the item as “necessary”, “useful but not necessary” and “not
necessary”. Calculating the content validity ratio, all
questions scored between 0.5 and 1 were included in the
questionnaire (26 more items were excluded due to minor
scoring). The final form of the GQEDSS - ADRDS
comprises firstly of a part consisted of 3 domains of general
demographic information related to person in examination
and secondly the main part consisted of 157 items
(questions). This second part questions are rated on a Likert
scale. These 160 items form the GQEDSS - ADRDS scale.
The questionnaire is presented in the appendix section of the
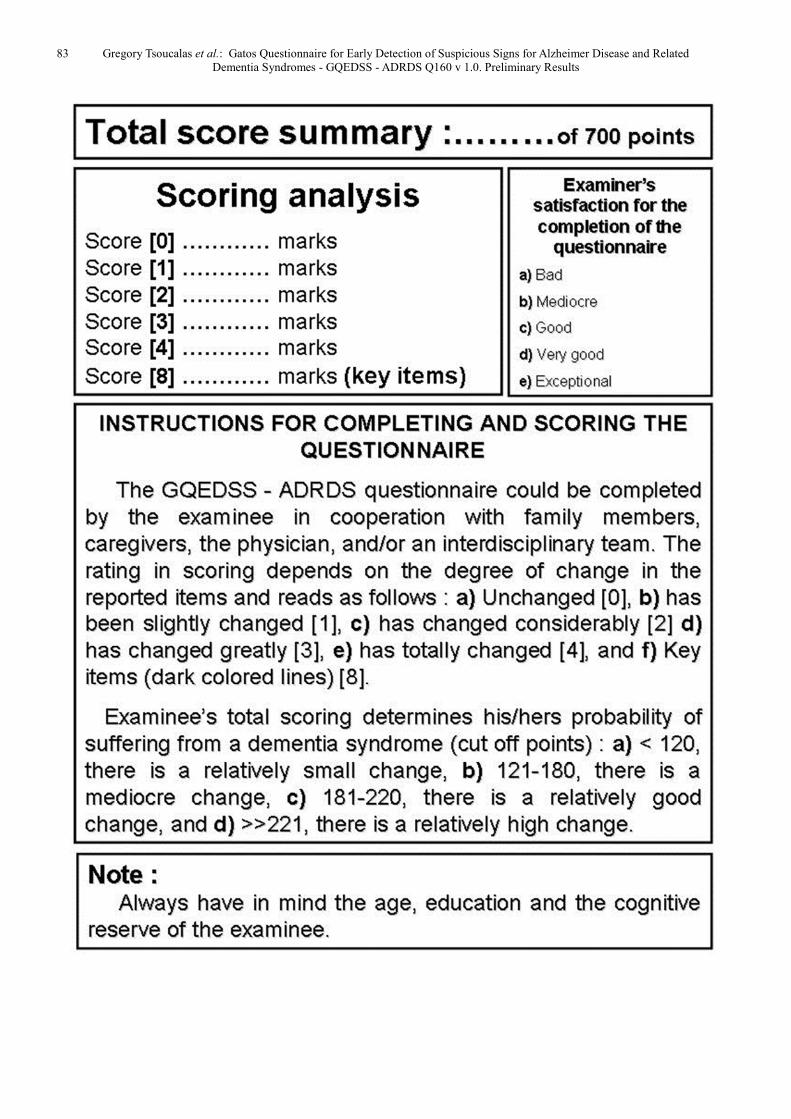
paper. The 160 items total score is used to evaluate person's
probability to experience a dementia syndrome in the future.
For the individualized and holistic clinical assessment of the
patient, however, both parts, should be considered.
Fifty five persons (n1=55) visiting our outpatient sector
were enrolled in the study. The only criterion was an MMSE
score between 0 and 30. Thus relatively "brain healthy"
individuals. Informed consent brochures were administered
and the study was fully conformed with Helsinki declaration
principles and Greek Medical ethics law (Law 3418/2005).
To demonstrate the discriminant validity of the GQEDSS -
ADRDS, the MMSE was also applied. To fill in both
questionnaires, the patient, the relatives, the caregivers and
the specialized personnel cooperation was in some cases
necessary. Both were filled at the same day for every patient,
while for the summary of the fifty five patients to be enrolled
in the study, a time period of five months (January - May
2011) was necessary. For the test-retest validation a period of
48 hours was used for 12 participants to answer both scales
once more. All participants have been under then under
surveillance for the change of a dementia syndrome to inflict
them for further five years (until January 2016). From the
total number of fifty five participants, twenty six (n2=26)
presented dementia. Then, the sample n2 was used for the
significance of various key items to be measured.
3. Statistics
All items were coded and scored and the completed
questionnaires were included in the data set. Individual
unanswered items were excluded from the analysis. All the
data were entered, checked for missing values and analysed
using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA) and

71 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results
SAS version 7.0 (SAS Institute, Cary, NC, USA) statistical
programs. Descriptive statistics, such as the mean, standard
deviation and skewness were used to describe the main
variables. However, due to small study sample, parametric
methods were used to further analyze the data. Statistical
significance was set at p<0,05. Data distribution was tested
with Kolmogorov-Smirnov test και P-P plots.
The validity of a questionnaire is the extent to which the
questionnaire measures the study concept or, otherwise, the
variate that it is supposed to measure. Increase in validity of a
questionnaire is associated with a decrease in systematic
error. However due to the small sample the evaluation of the
validity of the GQEDSS - ADRDS presents a priori
questionable results. The questionnaire validation included
factor analysis, convergent or criterion validity, subscale
validity, discriminant validity, key items analysis, and ROC
analysis.
Exploratory factor analysis (EFA) was conducted to
identify a viable factor structure. EFA, using principal
component extraction method with Varimax rotation, was
conducted for all participants to determine the factor
structure of the 160 items of the GQEDSS - ADRDS
questionnaire. The sample size of 26 patients did not satisfied
the criteria set by Stevens [8] (factors loadings require n
≥300). Factor analyses were repeated until a solution was
attained in which all items included in the analysis met all
Stevens' criteria [9, 10]. The scree test used to determine the
number of factors to retain and rotate. From the analysis 54
factors appeared to be valid. Convergent or Criterion validity
of the GQEDSS - ADRDS questionnaire was determined by
establishing its correlation to the MMSE score using the
Pearson’s correlation coefficient. Subscale validity was
evaluated by examining the subscale correlations.
Discriminant validity tested whether concepts or
measurements that are supposed to be unrelated are, in fact,
unrelated. A successful evaluation of discriminant validity
shows that our questionnaire measuring mental status is not
highly correlated with other questionnaire designed to
measure theoretically different concepts. The discriminant
validity examined using a sample of twelve random persons
(n3=12). Key items evaluation was conducted for the factors'
complexity and variety to be simplified.
A receiver operating curve (ROC) analysis was conducted
to obtain the cut-off level of GQEDSS - ADRDS total score
for differentiation between subgroups of patients formed on
the basis of their disease probability, calculating the
respective areas under the curve (AUC). The areas under the
ROC curve (AUC) with standard error and 95%CI were
calculated using the maximum likelihood estimation method,
which has the advantage of being free of assumption about
the Gaussian distribution of underlying variables.
Furthermore, the sensitivity and specificity of different cut-
off points of GQEDSS - ADRDS total were estimated using
the MMSE score (28 vs 29 or 30) as a gold standard method.
The reliability or precision of a questionnaire concerns the
degree of stability or consistency with which the
questionnaire measures the concept that it is supposed to
measure. The estimation of reliability of the GQEDSS -
ADRDS questionnaire included internal consistency
reliability, test-retest reliability and inter-observer reliability.
Internal consistency validity of the GQEDSS - ADRDS was
determined by calculating Cronbach alpha coefficient. A
Cronbach α coefficient value of 0.7 indicates sufficient
reliability for research purposes and suggests that items are
interdependent and homogeneous in terms of the construct
they measure. For clinical applications a > 0.8 is desirable
[11-13]. Test-retest reliability (stability) (n3 patients)
indicates the stability of patients’ response in time and it was
determined by calculating ICC (intraclass correlation
coefficient: the error in measurements as a proportion of the
total variance) between the total scores of the initial
assessment of the GQEDSS - ADRDS and the total scores of
the reassessment after 3 days. Because this coefficient does
not correct for systematic differences and agreement by
chance, the scores of the 2 assessments were tested for
systematic differences by using the Paired t-test. Inter-
observer reliability is a measure of reliability used to assess
the degree to which different judges or raters agree in their
assessment decisions. Inter-rater reliability is useful because
human observers will not necessarily interpret answers the
same way; raters may disagree as to how well certain
responses or material demonstrate knowledge of the
construct or skill being assessed [14]. The Inter-observer
reliability was examined using the sample of n3 random
patients.
4. Results
Demographics are shown in [Table 1]. The Bartlett Test of
Sphericity was 2527.2 and it was significant (p<0.0015). The
Kaiser-Meyer-Olkin Measure of Sampling Adequacy was
equal to 0.801 showing that the data is suitable for factor
analysis. The 160 items were analysed via maximum
likelihood extraction method using a Varimax rotation. Fifty
four factors with eigenvalues of over 1 were identified. We
used the scree test to determine the number of factors to
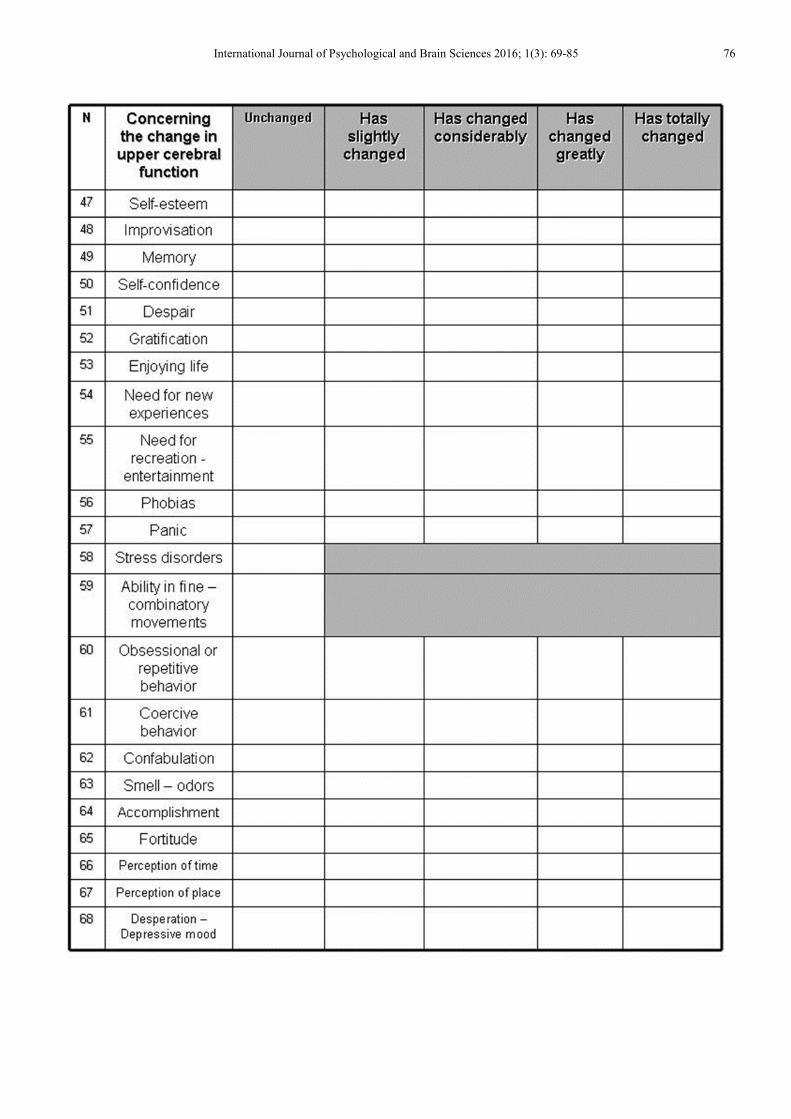
retain and rotate, which suggested a 54 factor solution. Then
a key items evaluation was conducted, naming 15 key items
(dark coloured background in the questionnaire) as most
important after a horizontal statistic analysis (mean value of
n2 items) [Table 2]. The GQEDSS - ADRDS 15 key items
and total score with MMSE score exhibited excellent
correlation. The correlation coefficients presented p<0.0005.
The above result indicated very strong correlation between
the 2 questionnaires and satisfied the criterion validity. The
area under the curve (AUC) of GQEDSS - ADRDS total
score was 0.779 (89%CI 0.82- 0.90 p<0.015), with cut-off
points being set as: a) < 120, there is a relatively small
change, b) 121-180, there is a mediocre change, c) 181-220,
there is a relatively good change, and d) >>221, there is a
relatively high change. The internal consistency of the 160
items of the GQEDSS - ADRDS was measured with
Cronbach's alpha and yielded a value of 0.81, which indicates
excellent internal consistency. All values are higher than 0.62

International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 72
suggesting that items are interdependent and homogeneous in
terms of the construct they measure. The paired samples t-
test between initial assesment and reassesment of
questionnaire indicated no statistically significant
differences. ICC between initial assesment and reassesment
of the test ranged between 0.862-0.959 (p<0.0005). The
above results of stability indicated that GQEDSS - ADRDS
total scores were remarkably consistent between the two
occasions, proving test-retest reliability. The scores of
GQEDSS - ADRDS questionnaire from the two different
specialised doctors were highly correlated (ICC=0.863 to
0.959, p<0.0005) which proved that the raters agreed as to
how well certain responses demonstrate knowledge of the
construct or skill being assessed, proving inter-observer
reliability.
Table 1. Demographic characteristics of the sample.
Sex N Living area Education. In years
Urban Rural Island DS in 5 years 0 1-9 >10
Male (n) 34 9 22 3 15 2 7 6
Female (n) 22 10 11 1 11 7 3 1
Total (n) n1: 56 19 33 4 n2: 26 9 10 7
Table 1. Continue.
Sex Age. Distribution Farmers – Blue. Colars White. Collars Scietists - Business men House keeping
<47 47-53 54-65 66-75 >76
Male (n) 0 0 1 10 4 9 2 4 0
Female (n) 1 1 2 3 4 2 1 1 7
Total (n) 1 1 3 13 8 11 3 5 7
Blue collars: In Greece farmers and peasants should be included.
House keeping: In Greece house keeping is considered a profession, without being paid as such though.
DS: Dementia Syndrome.
Table 2. Key items.
Number Number inside GQEDSS - ADRDS Item
1 Intuition No 5
2 Empathy No 12
3 Emotion - emotional tension No 15
4 Thought disruption – concreteness of thinking No 19
5 Memorize - integrate No 24
6 Stress disorders No 58
7 Ability in fine - combinatory movements No 59
8 Dealing with daily problems / activities No 69
9 Conversation flow - subject flow No 78
10 Action - reaction time, response time No 83
11 Balance during moving or walking No 107
12 Weakness in orientation No 110
13 Isolation - pullback No 122
14 Personal hygiene No 130
15 Disorder in sleeping pattern – insomnia,
reversal, excessive sleep No 153
5. Discussion
An assessment questionnaire in medicine transform
structured information into numerical values [15] and so does
the GQEDSS - ADRDS. Our purpose was not to replace
simpler tools such as MMSE or most modern and
sophisticated as the SIB, or the MMSE-s (Mini Mental State
Examination-severe) [16], the TSI (Test Severe Impairment)
[17], the SCIP (Severe Cognitive Impairment Profile) [18],
the NTG-EDSD Screening Instrument by the American
Academy of Developmental Medicine [19] and the
Addenbrooke's Cognitive Examination-Revised for the Greek
population (ACE-R) [20], but to fill the qualitative gaps in
the assessment of the probability of a person to be inflicted
by a dementia syndrome in the future. Our questionnaire
could also be used as an alternative, or in combination with
the validated tools already in use. The GQEDSS - ADRDS
contributes to a different approach, introducing a
communication pathway between physicians and clients,
assessing some new areas that could be early impaired. It
provides information that medical personnel, relatives and
caregivers can take advantage of, in order to achieve a better
scheduled confrontation against the possibility of an
infliction by dementia syndromes (cognitive exercises,
puzzle games, chess, Sudoku, riddles, socializing, medication
etc). However, the validity of the new scale was based on a
correlation with MMSE scores 28, 29 and 30, which when
standing as unique measurements are generally considered
unreliable. In addition, MMSE measures cognition whereas
GQEDSS - ADRDS scale measures cognitive, functional,
physical, social and personal performance. As MMSE is a
specific and widely available scale, we proceeded with the
comparison between these two scales, despite the
aforementioned differences. A disadvantage of GQEDSS -
ADRDS is that its completion time is estimates between 60
and 75 minutes, depending on the person being examined
(age, education, etc).
The new GQEDSS - ADRDS scale, is a combination of an
extensive experience of about a 30 years battle with
demented patients [21], and items borrowed by predicting
dementia batteries that are availliable for use [19-20, 22-25].
However, GQEDSS - ADRDS could present a series of
statistical biases. The sample was small in comparison with
the number required by the Stevens criteria. All participants
were visitors of the outpatient infirmary, thus somehow all
felt some changes, suspicious for mental diseases. The
MMSE scale which was used for the validation of the
GQEDSS - ADRDS questionnaire is in a way one-
73 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results
dimensional tool (mainly memory impairment scale). Test-
retest and the 5 year follow up by different members of the
interdisciplinary team poses the risk for subjectivity.
Extensive experience of the team's members could in some
cases magnify an item that has minor significance during the
interview-completion of the questionnaire. The sample was
non-randomized - convenience, and/or consecutive sampling
(all clients in the outpatient clinic). It is clear that further
study is needed, much bigger sample, possibly through a
multi-centred effort. Further key items validation in a try for
the new tool to be shortened is somehow required, as its
complexity and longevity make it difficult to be managed,
and rather inapplicable in the Primary Health Care System.
New methodology in agreement with Stevens criteria is also
necessary. Our tool, depicts though an interdisciplinary
team's of experts in dementia first attempt to predict some
potential risk for the participants. This attempt could be
further ameliorated in the near future.
6. Conclusion
The GQEDSS - ADRDS scale, as a new tool, was
validated and seems to offer new items for the early
discovery of signs that could possibly measure the risk for an
individual to experience a dementia syndrome in the future.
More work is needed, thorough study of a bigger sample,
new modalities to be examined, new experts to participate in
further inquiries, as the primary material in the new tool is at
least intriguing and promising.
Appendix: The GQEDSS - ADRDS Questionnaire v 1.0
International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 74

75 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results
International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 76

77 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results
International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 78
79 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results

International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 80

81 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results
International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 82
83 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results

International Journal of Psychological and Brain Sciences 2016; 1(3): 69-85 84
References
[1] Brodaty H. Managing Alzheimer's disease in primary care. London: Science Press (1998).
[2] Gauthier S, Leuzy A, Racine E, Rosa-Neto P. Diagnosis and management of Alzheimer's disease: past, present and future ethical issues. Prog Neurobiol 110 (2013): 102-13.
[3] Schmid NS, Taylor KI, Foldi NS, Berresd M, Monsch AU. Neuropsychological Signs of Alzheimer’s Disease 8 Years Prior to Diagnosis. Journal of Alzheimer’s Disease 34 (2013): 537-546.
85 Gregory Tsoucalas et al.: Gatos Questionnaire for Early Detection of Suspicious Signs for Alzheimer Disease and Related
Dementia Syndromes - GQEDSS - ADRDS Q160 v 1.0. Preliminary Results
[4] Guo Q, Zhou B, Zhao Q, Wang B, Hong Z. Memory and Executive Screening (MES): a brief cognitive test for detecting mild cognitive impairment. BMC Neurology 12 (2012): 119.
[5] Tsoucalas G, Bourelia S, Kalogirou V, Giatsiou S, Mavrogiannaki E, Gatos G, Galanos A, Repana O, Iliadou E, Antoniou A, Sgantzos M, Gatos K. End-stage dementia spark of life: reliability and validity of the "GATOS" questionnaire. Curr Alzheimer Res 12 (2015): 179-188.
[6] Fountoulakis KN, Tsolaki M, Chantzi H, Kazis A. Mini Mental State Examination (MMSE): A validation study in Greece. Am J Alzheimers Dis Other Demen 6 (2000): 342-345.
[7] Tsolaki M, Kounti F (eds). Tests and criteria for the assessment of brain disorders. Thessaloniki: Giachoudis (2010).
[8] Stevens J. Applied Multivariate Statistics for the Social Sciences, 4th Edition, Mahwah New Jersey: Lawrence Erlbaum Associates (2002).
[9] Gorgush RL. Psychometric Theory. New York: McGraw-Hill (1978).
[10] Harman HH. Modern Factor Analysis. Chicago: University of Chicago Press (1967).
[11] Cronbach LJ Coefficient alpha and the internal structure of test. Psychometrica 16 (1951): 297-334.
[12] Nunnally JC Psychometric theory. New York: McGraw-Hill (1978).
[13] Higgins PA, Straub AJ. Understanding the error of our ways: Μapping the concepts of validity and reliability. Nurs Outlook 54 (2006): 23-29.
[14] Bland JM, Altman DG. Statistics notes: Validating scales and indexes. Br Med J 324 (2002): 606-607.
[15] Huber U, Rosli A, Ballmer PE, Rippin SJ. The use of scores in general medicine. Ther Umsch 70 (2013): 559-566.
[16] Wajman JR, Bertolucci PHF. Comparison between neuropsychological evaluation instruments for severe dementia. Arq Neuropsiquiatr 64 (2006): 736-740.
[17] Albert M, Rossor MN. The test for severe impairment: An instrument for the assessment of patients with severe cognitive dysfunction. J Am Geriatr Soc 40 (1992): 449-453.
[18] Peany G, Salmon D, Rice V, Galasko D, Samuel W, Taylor KI, et al. Neuropsychological assessment of severely demented elderly: The Severe Cognitive Impairment Profile. Arch Neurol 53 (1996): 367-372.
[19] American Academy of Developmental Medicine. NTG-EDSD Screening Instrument. http://aadmd.org/ntg/screening. Accessed 07/11/2016.
[20] Konstantinopoulou E, Kosmidis MH, Ioannidis P, Kiosseoglou G, Karacostas D, Taskos N. Adaptation of Addenbrooke's Cognitive Examination-Revised for the Greek population. Eur J Neurol 18 (2011): 442-447.
[21] Gatos K. A test for possibly suspicious signs presented by an elder about 10 years before the appearance of visible dementia signs. Proceedings of the 8th Panhellenic Interdisciplinary Congress for Alzheimer disease and Releted Dementia Syndromes. Thessaloniki, Greece (2003): 61-69.
[22] MS, Moss MB, Tanzi R, Jones K. Preclinical prediction of AD using neuropsychological tests. Journal of the International Neuropsychological Society 7 (2001): 631-639.
[23] Larner AJ. Comparing diagnostic accuracy of cognitive screening instruments: a weighted comparison approach. Dement Geriatr Cogn Dis Extra 3 (2013): 60-65.
[24] Soininen H, Waldemar G. Application of the PredictAD software tool to predict progression in patients with mild cognitive impairment. Dement Geriatr Cogn Disord. 37 (2014): 207-213.
[25] Babacan-Yildiz G, Isik AT, Ur E, Aydemir E, Ertas C, Cebi M, Soysal P, Gursoy E, Kolukisa M, Kocaman G, Celebi A. COST: Cognitive State Test, a brief screening battery for Alzheimer disease in illiterate and literate patients. Int Psychogeriatr 25 (2013): 403-412.

















![INDEX [] · n.r.i questionnaire 3 keyman questionnaire with annexures 5 employer-employee scheme questionnaire 11 personal financial questionnaire 12 general occupation questionnaire](https://static.fdocuments.in/doc/165x107/5e7f0927f331ad3020486c35/index-nri-questionnaire-3-keyman-questionnaire-with-annexures-5-employer-employee.jpg)
