
GATA-3 Expression as a Predictor of Hormone Response in Breast Cancer
6
GATA-3 Expression as a Predictor of Hormone Response in Breast Cancer Purvi Parikh, MD, Juan P Palazzo, MD, Lewis J Rose, MD, Constantine Daskalakis, SCD, Ronald J Weigel, MD, PhD, FACS BACKGROUND: Expression of estrogen receptor- (ER) as determined by immunohistochemistry of tumor tissue is currently the most clinically useful test to predict hormone responsiveness of breast cancer. Thirty percent of ER-positive breast cancers do not respond to hormonal therapy. GATA-3 is a transcription factor that is expressed in association with ER and there is evidence that GATA factors influence response to estrogen. In this pilot study, we investigated whether GATA-3 expression is associated with hormone response in breast cancer. STUDY DESIGN: Breast cancer tissue was stained for GATA-3 expression by immunohistochemistry in ER- positive cancers from 28 patients, 14 of whom were defined as hormone unresponsive (cases) and 14 of whom were age-matched controls with hormone-responsive, ER-positive cancers (controls). RESULTS: Comparing cases and controls, there were no differences in expression of ER; progesterone receptor, ErbB2; or tumor grade. Using 20% nuclear staining to characterize tumors as GATA-3 positive or GATA-3 negative, 6 of 14 (43%) cancers in the hormone-unresponsive group and none of the controls were classified as GATA-3 negative (odds ratio, 8.2; 95% confidence interval, 1.2; p 0.031). Using different cut points to characterize GATA-3 positivity yielded very similar results, indicating a positive association between lack of GATA-3 expression and lack of response to hor- monal therapy. CONCLUSIONS: The study suggests that analyzing ER-positive breast tumors for GATA-3 using immunohis- tochemistry might improve prediction of hormone responsiveness. The association between GATA-3 expression and hormone response suggests that GATA-3 may play a role in mecha- nisms controlling response to estrogen. (J Am Coll Surg 2005;200:705–710. © 2005 by the American College of Surgeons) Breast cancer is a heterogeneous disease and current treat- ment options are individualized to the extent possible based on a determination of the biologic character of each tumor. For example, treatment with Trastuzumab (Herceptin) is only indicated for patients with tumors that demonstrate amplification of the protooncogene HER-2/neu (c-ErbB-2). 1 Hormonal therapy has been an important treatment op- tion for many breast cancer patients. Breast cancers that overexpress the estrogen receptor- (ER) protein most often occur in postmenopausal patients, 2 have an im- proved prognosis, 3 and are more likely to respond to hormonal therapy 4 compared with tumors with low or negligible expression of the receptor. Despite recent work using genomics, proteomics, and other diagnostic tests, expression of ER remains the most clinically use- ful method to predict hormone response in breast cancer patients. 5 For many years, expression of ER had been determined by measuring the binding of radiolabeled estrogen to cytosolic proteins using a dextran-coated charcoal assay. 6 The dextran-coated charcoal method re- quired that fresh frozen tumor be saved at the time of resection and the technique was sensitive to the amount and quality of the saved tumor sample. Over the past 20 years, the dextran-coated charcoal method has been re- placed by immunohistochemistry in which ER protein is detected in tumor cells using a monoclonal antibody. Immunohistochemistry has become the preferred Competing interests declared: None. Supported in part by the Kristen Olewine Milke Breast Cancer Research Fund. Received September 2, 2004; Revised December 29, 2004; Accepted Decem- ber 30, 2004. From the Departments of Surgery (Parikh, Weigel), Pathology (Palazzo), and Department of Medicine, Division of Medical Oncology (Rose) and Biosta- tistics Section (Daskalakis),Thomas Jefferson University, Philadelphia, PA. Correspondence address: Ronald J Weigel, MD, PhD, FACS, Department of Surgery, 1025 Walnut St, Ste 605, Philadelphia, PA 19107. 705 © 2005 by the American College of Surgeons ISSN 1072-7515/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jamcollsurg.2004.12.025
-
Upload
purvi-parikh -
Category
Documents
-
view
213 -
download
1
Transcript of GATA-3 Expression as a Predictor of Hormone Response in Breast Cancer

GHPR
BmoFoaHto
C
SF
RbFDtCS
©P
ATA-3 Expression as a Predictor oformone Response in Breast Cancer
urvi Parikh, MD, Juan P Palazzo, MD, Lewis J Rose, MD, Constantine Daskalakis, SCD,onald J Weigel, MD, PhD, FACS
BACKGROUND: Expression of estrogen receptor-� (ER�) as determined by immunohistochemistry of tumortissue is currently the most clinically useful test to predict hormone responsiveness of breastcancer. Thirty percent of ER�-positive breast cancers do not respond to hormonal therapy.GATA-3 is a transcription factor that is expressed in association with ER� and there is evidencethat GATA factors influence response to estrogen. In this pilot study, we investigated whetherGATA-3 expression is associated with hormone response in breast cancer.
STUDY DESIGN: Breast cancer tissue was stained for GATA-3 expression by immunohistochemistry in ER�-positive cancers from 28 patients, 14 of whom were defined as hormone unresponsive (cases)and 14 of whom were age-matched controls with hormone-responsive, ER�-positive cancers(controls).
RESULTS: Comparing cases and controls, there were no differences in expression of ER�; progesteronereceptor, ErbB2; or tumor grade. Using 20% nuclear staining to characterize tumors as GATA-3positive or GATA-3 negative, 6 of 14 (43%) cancers in the hormone-unresponsive group and noneof the controls were classified as GATA-3 negative (odds ratio, 8.2; 95% confidence interval, 1.2��;p � 0.031). Using different cut points to characterize GATA-3 positivity yielded very similar results,indicating a positive association between lack of GATA-3 expression and lack of response to hor-monal therapy.
CONCLUSIONS: The study suggests that analyzing ER�-positive breast tumors for GATA-3 using immunohis-tochemistry might improve prediction of hormone responsiveness. The association betweenGATA-3 expression and hormone response suggests that GATA-3 may play a role in mecha-nisms controlling response to estrogen. (J Am Coll Surg 2005;200:705–710. © 2005 by the
American College of Surgeons)ophnwtfpdecqraypi
reast cancer is a heterogeneous disease and current treat-ent options are individualized to the extent possible based
n a determination of the biologic character of each tumor.or example, treatment with Trastuzumab (Herceptin) isnly indicated for patients with tumors that demonstratemplification of the protooncogene HER-2/neu (c-ErbB-2).1
ormonal therapy has been an important treatment op-ion for many breast cancer patients. Breast cancers thatverexpress the estrogen receptor-� (ER�) protein most
ompeting interests declared: None.
upported in part by the Kristen Olewine Milke Breast Cancer Researchund.
eceived September 2, 2004; Revised December 29, 2004; Accepted Decem-er 30, 2004.rom the Departments of Surgery (Parikh, Weigel), Pathology (Palazzo), andepartment of Medicine, Division of Medical Oncology (Rose) and Biosta-
istics Section (Daskalakis), Thomas Jefferson University, Philadelphia, PA.orrespondence address: Ronald J Weigel, MD, PhD, FACS, Department of
Iurgery, 1025 Walnut St, Ste 605, Philadelphia, PA 19107.
7052005 by the American College of Surgeons
ublished by Elsevier Inc.
ften occur in postmenopausal patients,2 have an im-roved prognosis,3 and are more likely to respond toormonal therapy4 compared with tumors with low oregligible expression of the receptor. Despite recentork using genomics, proteomics, and other diagnostic
ests, expression of ER� remains the most clinically use-ul method to predict hormone response in breast canceratients.5 For many years, expression of ER� had beenetermined by measuring the binding of radiolabeledstrogen to cytosolic proteins using a dextran-coatedharcoal assay.6 The dextran-coated charcoal method re-uired that fresh frozen tumor be saved at the time ofesection and the technique was sensitive to the amountnd quality of the saved tumor sample. Over the past 20ears, the dextran-coated charcoal method has been re-laced by immunohistochemistry in which ER� proteins detected in tumor cells using a monoclonal antibody.
mmunohistochemistry has become the preferredISSN 1072-7515/05/$30.00doi:10.1016/j.jamcollsurg.2004.12.025

mpqt
tpcun27broctp
sEcccsgsresrfiobdh
MPWeawpbba
thiswE
GAoGBtGpi
SPGddfwpviouav(vwtL
RTwttrEpi5
706 Parikh et al GATA-3 Predicts Hormone Response J Am Coll Surg
ethod to determine ER� expression because it can beerformed on formalin-fixed, archival specimens; re-uires minimal tumor tissue; and is based on techniqueshat can be applied to a wide range of antigens.7
Although expression of ER� is the best available predic-or of hormone response, the association between ER� ex-ression and hormone response is not perfect. There is un-ertainty about the optimal cutoff for the percent stainingsed to categorize a tumor as ER�-positive versus ER�-egative. Most pathologists use a value between 10% and0% as the cutoff for positive staining.8-10 Approximately0% of ER�-positive/progesterone receptor (PR)-positivereast cancers respond to hormonal therapy.6 Responseates for ER-positive/PR-negative cancers are in the rangef 30% to 35% and �10% for ER-negative/PR-negativeancers.6,11 Use of additional markers to refine the predic-ion of hormone response could improve the treatmentlan for a significant number of patients.
GATA-3 transcription factor has a pattern of expres-ion in breast cancer that has a striking association withR�.12-14 Approximately 96% of ER�-positive breastancers express GATA-3, but only 22% of ER�-negativeancers express the GATA-3 protein. Studies examininglinical outcomes have concluded that GATA-3 expres-ion, as determined by microarray analysis, can distin-uish tumor subclasses with differences in disease-freeurvival and overall survival.15 It has been shown that aelated GATA factor, GATA-1, is responsible forstrogen-mediated repression of erythropoiesis, and thistudy also demonstrated that ER� binds to GATA-1 in aegion with extensive homology to GATA-3.16 Theseindings have led us to hypothesize that GATA-3 may benvolved in cellular response to estrogen and expressionf GATA-3 might be predictive of hormone response inreast cancer. The purpose of this pilot study was toetermine if expression of GATA-3 is associated withormone response in ER�-positive breast cancers.
ETHODSatient selectione conducted a pilot matched case-control study to
valuate the association between expression of GATA-3nd hormone responsiveness of breast cancer. The studyas carried out at Thomas Jefferson University and allrotocols were IRB approved. Patients were identifiedy the medical oncology service and were determined toe hormone unresponsive on the basis of clinical char-
cteristics of progression of disease or early recurrence on vamoxifen or aromatase inhibitor therapy. All patientsad breast tumors previously determined to be ER� pos-
tive by immunohistochemistry. A control group, con-isting of patients confirmed to be hormone responsive,as individually matched to the case group by age andR� status (ie, all ER�-positive cancers).
ATA-3 immunohistochemistryrchival tumor tissue was collected by the Departmentf Pathology and stained using a 1:250 dilution ofATA-3 monoclonal antibody HG3-31X (Santa Cruziotechnology) with microwave antigen retrieval pre-
reatment in citrate buffer as described previously.12
ATA-3 expression was characterized as to intensity andercent of nuclear staining. Evaluation of GATA-3 stain-ng was done blinded to clinical information.
tatistical analysisreliminary comparisons of cases and controls onATA-3 expression, and other biomarkers, were con-ucted through Wilcoxon’s signed rank test for pairedata. In the main analyses, GATA-3 positivity was de-ined using an a priori value of 20% nuclear staining,hich is the same cut point used to determine ER�ositivity. Data were also analyzed using different cutoffalues for the percent nuclear staining for GATA-3 bymmunohistochemistry (10% through 50%). Becausef the small sample size, exact statistical methods weresed. The proportion of GATA-3�negative patientsmong cases and controls was compared using the exactersion of McNemar’s test for matched data. Odds ratioscomparing the odds of GATA-3 negatives among casesersus controls) and associated 95% confidence intervalsere computed through exact logistic regression. Statis-
ical analyses were carried out with StatXact 6.1 andogXact 5 (Cytel Software Corp).17
ESULTShe population of this pilot study consisted of 14 patientsith ER�-positive breast cancers who failed hormonal
herapy (cases), and an equal number of age-matched pa-ients with ER�-positive cancers who exhibited hormoneesponse (controls).Table 1 presents data for ER�, PR, andrbB2 and reports GATA-3 expression based on percent ofositive tumor cells as determined by immunohistochem-stry. Patients were between 37 and 73 years of age (mean7 years) and because of matching, cases and controls were
ery similar with respect to age (all matched within 2 years).
AcccceptpEp
0cs7gspno
itdThsG
hfgoecs
cpa5ci�i
DAaqchwatr
Tm
P
11111
E ot ava
707Vol. 200, No. 5, May 2005 Parikh et al GATA-3 Predicts Hormone Response
ll breast cancers were determined to be ER� positive (1ase was 32% ER� positive, but the remaining cases andontrols ranged between 60% and 100%; mean 85). Be-ause all cancers were selected to be ER� positive, cases andontrols were similar with regard to ER� positivity (meanxpression of ER� was 82% for cases and 88% for controls,� 0.57). Cases and controls were also similar with respect
o PR expression (mean 55% for cases, 60% for controls,� 0.77). Finally, no major differences were found withrbB2 expression or tumor grade among the case-controlairs for which such information was available.
Percent of nuclei staining with GATA-3 ranged between% and 95% and there was a significant difference whenomparing cases and controls. Average percent nucleartaining was 47% in the hormone-unresponsive group and4% in the age-matched hormone-responsive controlroup (p � 0.039). All cancers that had GATA-3 nucleartaining of � 20% were also noted to have weak staining,ossibly suggesting low levels of protein expression in theuclei of these cells. Figure 1 provides representative imagesf GATA-3 staining.
Clinical evaluation with ER� does not consider stain-ng as a continuous variable, but establishes a cutoff usedo characterize tumors as positive or negative. The stan-ard ER� evaluation by immunohistochemistry athomas Jefferson University’s Department of Pathologyas established that � 20% tumor cell staining is con-idered negative. Applying the same criterion to
able 1. Characteristics (Including GATA-3 Expression) of Cone Responsive)
Casesair ID Age (y) ER� (%) PR (%) ErbB2 GATA-3 (%)
1 61 85 90 � 602 60 90 90 N/A 203 56 95 95 � 954 50 80 50 � 55 63 90 70 � 906 73 90 90 N/A 807 37 80 5 N/A 208 68 60 5 � 709 66 32 5 � 800 48 95 80 � 51 51 70 90 N/A 02 51 90 10 � 203 52 90 85 � 304 57 95 2 � 80
R�, estrogen receptor-�; Hetero, heterogeneity of staining pattern; N/A, n
ATA-3 staining, 6 of 14 (43%) of tumors in the c
ormone-unresponsive group were classified as negativeor GATA-3 expression, and no cancers in the controlroup were classified as negative. This corresponds to andds ratio of 8.2 (ie, GATA-3�negative tumors have anightfold higher risk of being hormone unresponsiveompared with GATA-3�positive tumors), with an as-ociated p value of 0.031 (Table 2).
When introducing a new test using immunohisto-hemistry, the cutoff point to characterize a tumor asositive or negative needs to be established. We evalu-ted data using a range of cutoff values (from 10% to0%, see Table 2). Loss of GATA-3 expression was asso-iated with increased risk of hormone unresponsiveness,rrespective of criterion (ie, odds ratios were consistently
1). Cut points between 20% and 40% performed sim-larly, although 30% seemed to yield the strongest result.
ISCUSSIONpproximately 200,000 women are diagnosed annu-lly in the US with invasive breast cancer and three-uarters of these cancers will be ER� positive.18 Be-ause 30% of ER� positive cancers will not beormone responsive, it is estimated that 45,000omen will be treated with hormone therapy on an
nnual basis but will not respond to this form ofherapy. Improving the ability to predict hormoneesponse will have a significant impact on breast can-
(Hormone Unresponsive) and Age-Matched Controls (Hor-
Controls-3 notes Age (y) ER� (%) PR (%) ErbB2 GATA-3 (%)
— 60 90 80 � 50eak 60 90 0 � 95— 56 80 60 � 60eak 48 70 85 � 75— 63 80 20 � 80— 73 100 35 � 90etero 37 70 80 � 40— 68 100 75 � 90etero 66 90 95 � 90eak 48 90 90 � 60— 51 90 95 � 80eak 53 90 50 � 95— 52 100 5 � 80— 55 90 65 � 50
ilable; PR, progesterone receptor; Weak, staining was weak nuclear.
ases
GATA
W
W
H
HW
W
er treatment by avoiding costs related to ineffective

tm
eE
ssurl1iohTsih
osGswpmwGtli
tcorrEgcpmghEaasupms
Fta(s
708 Parikh et al GATA-3 Predicts Hormone Response J Am Coll Surg
reatment and by eliminating the delay of initiatingore-effective therapy.Results from this pilot study suggest that GATA-3
xpression may be associated with hormone response in
igure 1. Immunohistochemistry of GATA-3 staining. Examples ofhree different invasive ductal carcinomas stained with the GATA-3ntibody. (A) Shows 95% of tumor cells with strong nuclear staining;B) 20% of tumor cells staining; and (C) �5% of the tumor cellstaining (immunohistochemistry, �150 and �250).
R�-positive breast cancers. Using a cutoff for nuclear r
taining of � 20% to define negative GATA-3 expres-ion, we would estimate that 43% of hormone-nresponsive, ER�-positive breast cancers could be cor-ectly predicted to be hormone insensitive based on theack of GATA-3 expression (sensitivity). Approximately9,350 women who are diagnosed with an ER�-positivenvasive breast cancer annually and who are currentlyffered hormonal therapy could be correctly defined asormone unresponsive using expression of GATA-3.he fact that none of the age-matched controls was clas-
ified as GATA-3 negative suggests a low probability ofncorrectly predicting that an ER�-positive tumor isormone unresponsive (high specificity).These findings should be viewed with caution because
f the study’s limitations as a result of its small sampleize. First, the strength of the association betweenATA-3 expression and hormone response, and the sen-
itivity and specificity of this marker, were estimatedith very limited precision. Second, no adjustment forossible differences between cases and controls on otherarkers of hormone response was possible. And, third, itas not possible to formally determine an optimalATA-3�positivity cut point. Despite these limita-
ions, the study’s findings can now guide the design of aarger, more definitive study that can address thesessues.
A number of methods have been pursued as a meanso improve the prediction of hormone response in breastancer. One recent study attempted to use methylationf the ER� gene as a clinical test to predict hormoneesponse and suggested an improvement over hormoneeceptor evaluation.19 Attempts to use expression ofR�-regulated genes to improve the prediction of estro-en response have been reported but results have notonsistently indicated that this approach improves therediction of endocrine responsiveness beyond hor-one receptor status.20-22 Use of a radiolabeled ER� li-
and has demonstrated a promising method to predictormone responsiveness of metastatic breast cancers.23
xpression of ER� has been evaluated but there does notppear to be a clear correlation between ER� expressionnd hormone response of breast cancer.24,25 A recenttudy suggested that expression of PR isoforms might besed to identify a subgroup of patients with ER�-ositive tumors that are less likely to respond to hor-onal therapy.26 Another study suggested that expres-
ion of the cdk inhibitor p27Kip1 might be predictive of
esponse to antiestrogens.27 Although there is active in-
thhtogtthiceeG
bcspcoahhttctmwmtGmmcc
bwc
ASAA
DCSOS
Ads
R
Ts
Pf
�
�
�
�
�
9
709Vol. 200, No. 5, May 2005 Parikh et al GATA-3 Predicts Hormone Response
erest in this area of investigation, none of these studiesas been definitive and expression of ER� by immuno-istochemistry remains the most clinically useful predic-or of hormone response. Many of the tests being devel-ped use polymerase chain reaction amplification,enome array hybridization, or more complex molecularests that require the use of fresh frozen tissue. A predic-ive test that is based on immunohistochemistry wouldave the advantage of being rapidly adopted in the clin-
cal setting. We hope that a future study will be able toonfirm the strength of the predictive utility of GATA-3xpression in patients with ER�-positive cancers and tovaluate the optimal positivity cut point for such aATA-3 test.Expression of GATA-3 has been shown to predict a
reast cancer subtype, defined as luminal A, whicharries an improved disease-free survival and overallurvival when compared with tumors that do not ex-ress GATA-3.15 The method used to define a breastancer as hormone responsive or unresponsive basedn clinical outcomes is open to debate. If a patient hasrecurrence or develops metastatic disease while onormonal therapy, we tend to classify the cancer asormone unresponsive. On the other hand, if a pa-ient remains disease free on hormonal therapy, weend to classify her as hormone responsive. But thelinical course of the patient may not be directly at-ributable to the hormone responsiveness of the tu-or. Hence, GATA-3 may be a marker for a cancerith a more favorable biology independent of hor-one response and may control differentiation of the
umor as suggested by a recent study examiningATA-3 mutations.28 An additional question that re-ains to be addressed is whether GATA-3 expressionay also be used to predict hormone response or out-
omes among patients with ER�-negative breast can-
able 2. Comparison of GATA-3 Expression in Cases (Hormoive), Using Various Definitions of GATA-3 Positivity (Cut Poi
ositive cut pointor GATA-3�
Negative casesNc
n % n
10% 3 21 020% 6 43 030% 7 50 040% 7 50 150% 7 50 3
5% CI, 95% confidence interval; OR, odds ratio.
ers. Additional work on the action of GATA-3 in
reast cancer will be needed to define mechanisms byhich this transcription factor may alter the clinical
ourse of breast cancers.
uthor Contributionstudy conception and design: Rose, Daskalakis, Weigelcquisition of data: Parikh, Palazzo, Weigelnalysis and interpretation of data: Parikh, Palazzo,Daskalakis, Weigelrafting of manuscript: Parikh, Weigelritical revision: Palazzo, Rose, Daskalakis, Weigeltatistical expertise: Daskalakisbtaining funding: Weigel
upervision: Palazzo, Rose, Weigel
cknowledgment: We wish to thank Kathy Califano and Mag-alena Potoczek for performing the immunohistochemicaltains.
EFERENCES
1. Pegram MD, Pienkowski T, Northfelt DW, et al. Results of twoopen-label, multicenter phase II studies of docetaxel, platinumsalts, and trastuzumab in HER2-positive advanced breast can-cer. J Natl Cancer Inst 2004;96:759–769.
2. Fisher ER, Redmond CK, Liu H, et al. Correlation of estrogenreceptor and pathologic characteristics of invasive breast cancer.Cancer 1980;45:349–353.
3. Knight WA, Livingston RB, Gregory EJ, McGuire WL. Estro-gen receptor as an independent prognostic factor for early recur-rence in breast cancer. Cancer Res 1977;37:4669–4671.
4. Heuson JC, Longeval E, Mattheiem WH, et al. Significance ofquantitative assessment of estrogen receptors for endocrine ther-apy in advanced breast cancer. Cancer 1977;39:1971–1977.
5. Buzdar AU, Vergote I, Sainsbury R. The impact of hormonereceptor status on the clinical efficacy of the new-generationaromatase inhibitors: a review of data from first-line metastaticdisease trials in postmenopausal women. Breast J 2004;10:211–217.
nresponsive) and Age-Matched Controls (Hormone Respon-
vels
OR 95% CI p Value%
0 3.85 0.41, � 0.2500 8.17 1.18, � 0.0310 9.61 1.44, � 0.0167 8.17 1.18, � 0.031
21 3.00 0.54, 30.39 0.289
ne Unts)egationtro
6. Jordan VC, Wolf MF, Mirecki DM, et al. Hormone receptor

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
710 Parikh et al GATA-3 Predicts Hormone Response J Am Coll Surg
assays: clinical usefulness in the management of carcinoma ofthe breast. Crit Rev Clin Lab Sci 1988;26:97–152.
7. Harvey JM, Clark GM, Osborne CK, Allred DC. Estrogen recep-tor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapyin breast cancer. J Clin Oncol 1999;17:1474–1481.
8. Diaz LK, Sahin A, Sneige N. Interobserver agreement for estro-gen receptor immunohistochemical analysis in breast cancer: acomparison of manual and computer-assisted scoring methods.Ann Diagn Pathol 2004;8:23–27.
9. Regitnig P, Reiner A, Dinges HP, et al. Quality assurance fordetection of estrogen and progesterone receptors by immuno-histochemistry in Austrian pathology laboratories. VirchowsArch 2002;441:328–34. Epub September 17, 2002.
0. Wishart GC, Gaston M, Poultsidis AA, Purushotham AD. Hor-mone receptor status in primary breast cancer—time for a con-sensus? Eur J Cancer 2002;38:1201–1203.
1. McGuire WL, Horwitz KB, Pearson OH, Segaloff A. Currentstatus of estrogen and progesterone receptors in breast cancer.Cancer 1977;39:2934–2947.
2. Hoch RV, Thompson DA, Baker RJ, Weigel RJ. GATA-3 isexpressed in association with estrogen receptor in breast cancer.Int J Cancer 1999;84:122–128.
3. Schaner ME, Ross DT, Ciaravino G, et al. Gene expressionpatterns in ovarian carcinomas. Mol Biol Cell 5,2003;14:4376–4386. Epub September 5, 2003.
4. Yang GP, Ross DT, Kuang WW, et al. Combining SSH andcDNA microarrays for rapid identification of differentially ex-pressed genes. Nucleic Acids Res 1999;27:1517–1523.
5. SorlieT, Perou CM,Tibshirani R, et al. Gene expression patternsof breast carcinomas distinguish tumor subclasses with clinicalimplications. Proc Natl Acad Sci USA 2001;98:10869–10874.
6. Blobel GA, Sieff CA, Orkin SH. Ligand-dependent repressionof the erythroid transcription factor GATA-1 by the estrogenreceptor. Mol Cell Biol 1995;15:3147–3153.
7. Hirji KF, Mehta CR, Patel NR. Exact inference for matched
case-control studies. Biometrics 1988;44:803–814.8. Ghafoor A, Jemal A, Ward E, et al. Trends in breast cancer byrace and ethnicity. CA Cancer J Clin 2003;53:342–355.
9. Widschwendter M, Siegmund KD, Muller HM, et al. Associa-tion of breast cancer DNA methylation profiles with hormonereceptor status and response to tamoxifen. Cancer Res 2004;64:3807–3813.
0. Hayashi S. Prediction of hormone sensitivity by DNA microar-ray. Biomed Pharmacother 2004;58:1–9.
1. Yoshida N, Omoto Y, Inoue A, et al. Prediction of prognosis ofestrogen receptor-positive breast cancer with combination ofselected estrogen-regulated genes. Cancer Sci 2004;95:496–502.
2. Luqmani YA, Ricketts D, Ryall G, et al. Prediction of responseto endocrine therapy in breast cancer using immunocytochem-ical assays for pS2, oestrogen receptor and progesterone receptor.Int J Cancer 1993;54:619–623.
3. Bennink RJ, van Tienhoven G, Rijks LJ, et al. In vivo predictionof response to antiestrogen treatment in estrogen receptor-positive breast cancer. J Nucl Med 2004;45:1–7.
4. de Cremoux P, Tran-Perennou C, Elie C, et al. Quantitation ofestradiol receptors alpha and beta and progesterone receptors inhuman breast tumors by real-time reverse transcription-polymerase chain reaction. Correlation with protein assays. Bio-chem Pharmacol 2002;64:507–515.
5. Iwase H, Zhang Z, Omoto Y, et al. Clinical significance of theexpression of estrogen receptors alpha and beta for endocrinetherapy of breast cancer. Cancer Chemother Pharmacol 2003;52[Suppl 1]:S34–S38. Epub June 19, 2003.
6. Hopp TA, Weiss HL, Hilsenbeck SG, et al. Breast cancer pa-tients with progesterone receptor PR-A-Rich tumors havepoorer disease-free survival rates. Clin Cancer Res 2004;10:2751–2760.
7. Arteaga CL. Cdk inhibitor p27Kip1 and hormone dependencein breast cancer. Clin Cancer Res 2004;10:368S–371S.
8. Usary J, Llaca V, Karaca G, et al. Mutation of GATA3 in human
breast tumors. Oncogene 2004;23:7669–7678.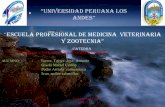














![Henri Bergson - Gandirea si miscarea [gata]](https://static.fdocuments.in/doc/165x107/568bd8411a28ab2034a2b625/henri-bergson-gandirea-si-miscarea-gata.jpg)


