Gastrointestinal Tract Cancer Prevention - CCCUPR 4-13-13.pdf · NCI/DCP/GOCRG • Umar • 2013...
42
NCI/DCP/GOCRG • Umar • 2013 Gastrointestinal Tract Cancer Prevention Asad Umar, DVM, PhD Gastrointestinal & Other Cancers Research Group Division of Cancer Prevention National Cancer Institute, NIH, USA
Transcript of Gastrointestinal Tract Cancer Prevention - CCCUPR 4-13-13.pdf · NCI/DCP/GOCRG • Umar • 2013...

NCI/DCP/GOCRG • Umar • 2013
Gastrointestinal Tract Cancer Prevention
Asad Umar, DVM, PhD Gastrointestinal & Other Cancers Research Group
Division of Cancer Prevention National Cancer Institute, NIH, USA

NCI/DCP/GOCRG • Umar • 2013
BAX
p53
-catenin/
E-cadherin
Chromatin
Remodeling/
Methylation
MSH2/
MLH1
TGF-RII
K-ras
SMAD2/4
AKT
ODC
APC
MMPs
TXNIP
Telomerase
Chronic Disease
Multiple Targets for Intervention
Gastrointestinal Tract:
Colorectal Cancer
NCI/DCP/GOCRG • Umar • 2013
Can
cer
Pro
gre
ssio
n
Time (Years)
Precancer
Carcinoma in situ
Metastasis
Cancer
Normal
Cancer Mortality
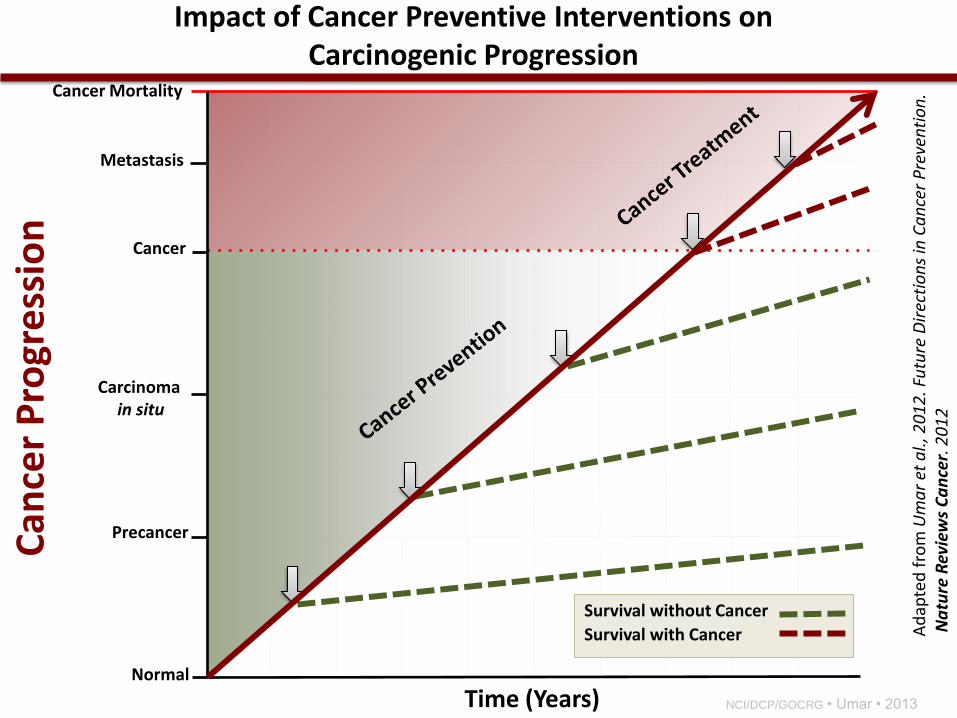
Survival without Cancer
Survival with Cancer Ad
apte
d f
rom
Um
ar
et a
l., 2
01
2. F
utu
re D
irec
tio
ns
in C
an
cer
Pre
ven
tio
n.
Na
ture
Rev
iew
s C
an
cer.
20
12
Impact of Cancer Preventive Interventions on Carcinogenic Progression
NCI/DCP/GOCRG • Umar • 2013
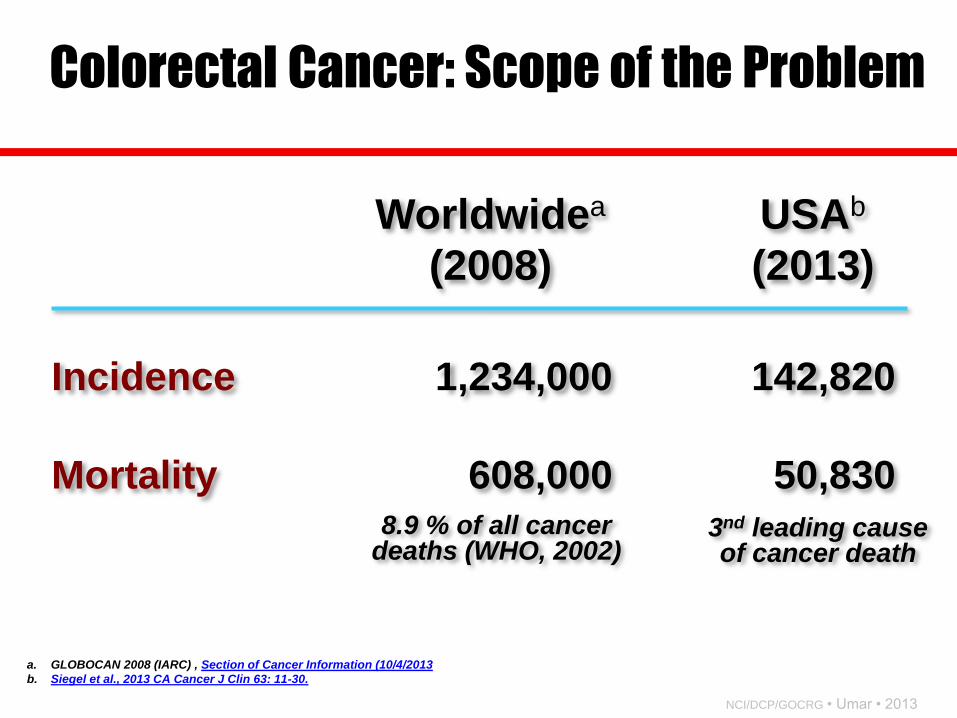
Worldwidea
(2008)
USAb
(2013)
Incidence
Mortality
1,234,000
608,000
142,820
50,830 8.9 % of all cancer
deaths (WHO, 2002) 3nd leading cause of cancer death
Colorectal Cancer: Scope of the Problem
a. GLOBOCAN 2008 (IARC) , Section of Cancer Information (10/4/2013
b. Siegel et al., 2013 CA Cancer J Clin 63: 11-30.
NCI/DCP/GOCRG • Umar • 2013
CRC Trends in Puerto Rico • Annual increases in PR CRC incidence & mortality
(1987-2004)
• In contrast, in US CRC incidence and mortality rates
decreased for NHW, NHB, and USH during the
same time period
• A health disparity that warrants further investigation as well as
better approaches for early detection and cancer prevention in PR
Soto-Salgado et al., Cancer 2009

NCI/DCP/GOCRG • Umar • 2013
Risk Factors – Age > 50 – Unhealthy diet
• Excess caloric intake • Low fruits & vegetables • High-fat, low-fiber diet
– Unhealthy lifestyle • Tobacco use • Low physical activity
– Infectious Agents? • Fusobacterium nucleatum • HPV?
– Hereditary syndromes • FAP • HNPCC
– Chronic inflammatory bowel disease
– Personal history of colorectal neoplasia
– Family history of colorectal neoplasia
– First degree relatives - 2-3x risk
Implications
– Risks are individualized, Must be assessed and discussed
– Healthcare provider
– Family members
Major Risk Factors for Colorectal Cancer

NCI/DCP/GOCRG • Umar • 2013
Alarming Colorectal Cancer Incidence Trends: A Case for Early Detection and Prevention
Umar & Greenwald. Cancer Epi. Biom. Prev. 2009
NCI/DCP/GOCRG • Umar • 2013
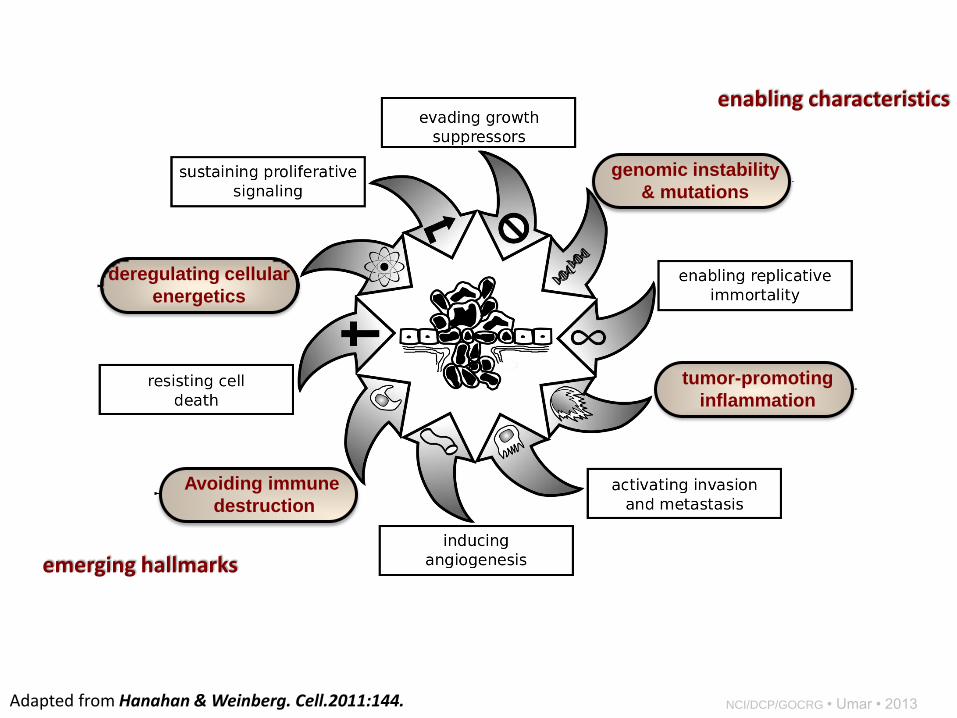
tumor-promoting
inflammation
Avoiding immune
destruction
deregulating cellular
energetics
genomic instability
& mutations
enabling characteristics
emerging hallmarks
Adapted from Hanahan & Weinberg. Cell.2011:144.

NCI/DCP/GOCRG • Umar • 2013
• Analgesic
• Antipyretic
• Anti-inflammatory
Non-steroidal Anti-inflammatory Drugs (NSAIDs)
The term "non-steroidal" distinguishes these drugs from steroids, which, among a broad range of other effects, have a similar eicosanoid-decreasing, anti-inflammatory action

NCI/DCP/GOCRG • Umar • 2013
Common Pharmacological Effects
• Analgesic (CNS and peripheral effect) may involve non-PG related effects
• Antipyretic (CNS effect)
• Anti-inflammatory due mainly to Prostaglandin inhibition

NCI/DCP/GOCRG • Umar • 2013
Pharmacological Effects (cont’d)
• Diverse group of chemicals, but all inhibit cyclooxygenase
• Inhibition of PG synthesis is largely responsible for their therapeutic effects
• But, inhibition of PG synthase in gastric mucosa dyspepsia, gastritis

NCI/DCP/GOCRG • Umar • 2013
Cyclo-oxygenase (COX)
• Constitutively expressed isoform (COX-1)
• At site of inflammation, cytokines stimulate the induction of the 2nd isoform (COX-2)
• Inhibition of COX-1 is responsible for their GI toxicity
• Most currently used NSAIDs are somewhat selective for COX-1, but selective COX-2 inhibitors are available
NCI/DCP/GOCRG • Umar • 2013
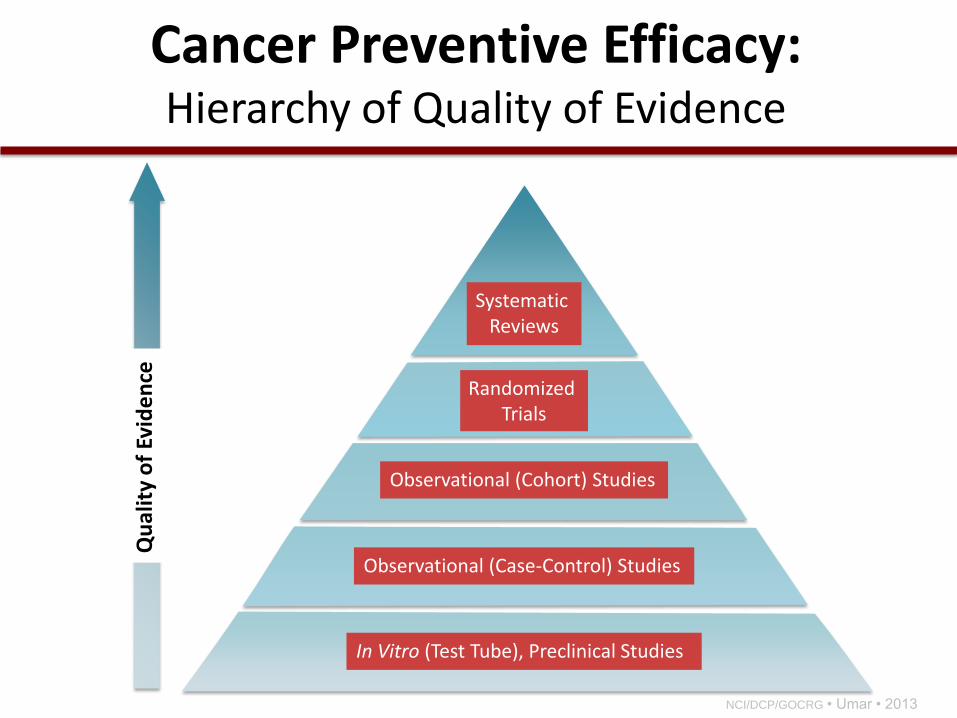
Qu
alit
y o
f Ev
ide
nce
In Vitro (Test Tube), Preclinical Studies
Observational (Case-Control) Studies
Observational (Cohort) Studies
Randomized Trials
Systematic Reviews
Cancer Preventive Efficacy: Hierarchy of Quality of Evidence
NCI/DCP/GOCRG • Umar • 2013
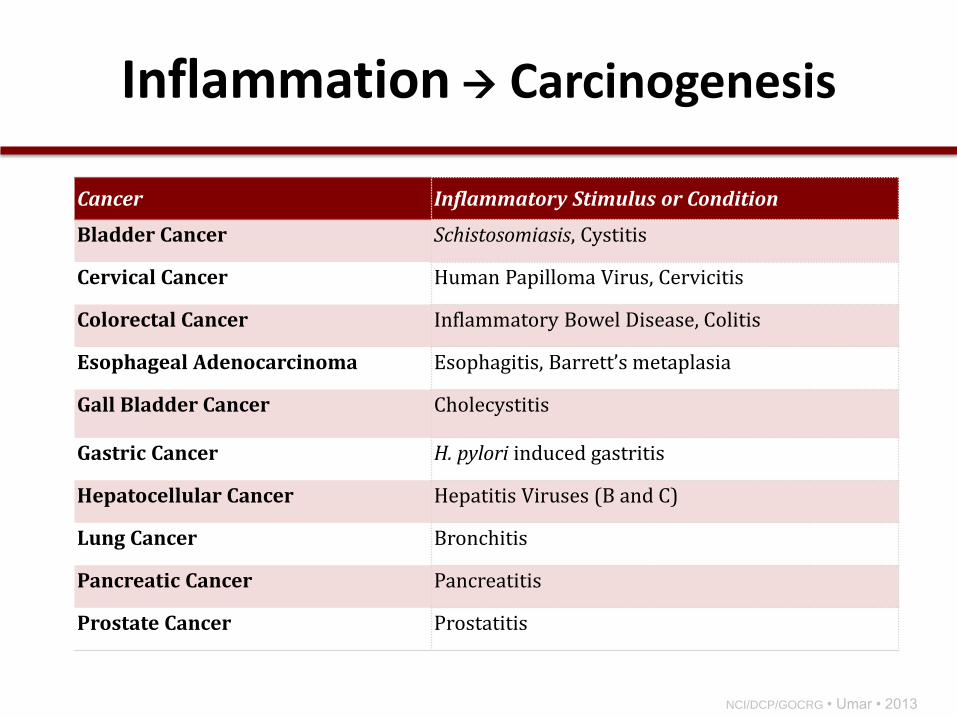
Inflammation Carcinogenesis
Cancer Inflammatory Stimulus or Condition
Bladder Cancer Schistosomiasis, Cystitis
Cervical Cancer Human Papilloma Virus, Cervicitis
Colorectal Cancer Inflammatory Bowel Disease, Colitis
Esophageal Adenocarcinoma Esophagitis, Barrett’s metaplasia
Gall Bladder Cancer Cholecystitis
Gastric Cancer H. pylori induced gastritis
Hepatocellular Cancer Hepatitis Viruses (B and C)
Lung Cancer Bronchitis
Pancreatic Cancer Pancreatitis
Prostate Cancer Prostatitis

NCI/DCP/GOCRG • Umar • 2013
Normal Colorectal Cancer
Inflammation in Colorectal Cancer
Red color indicates upregulation of the COX-2 enzyme.
The COX-2 enzyme is upregulated in human colorectal cancer

NCI/DCP/GOCRG • Umar • 2013
Normal Lung Cancer Red color indicates upregulation of the COX-2 enzyme.
The COX-2 enzyme is upregulated in human lung cancer
Inflammation in Lung Cancer

NCI/DCP/GOCRG • Umar • 2013
Normal Prostate Cancer Red color indicates upregulation of the COX-2 enzyme.
The COX-2 enzyme is upregulated in human prostate cancer
Inflammation in Prostate Cancer
NCI/DCP/GOCRG • Umar • 2013
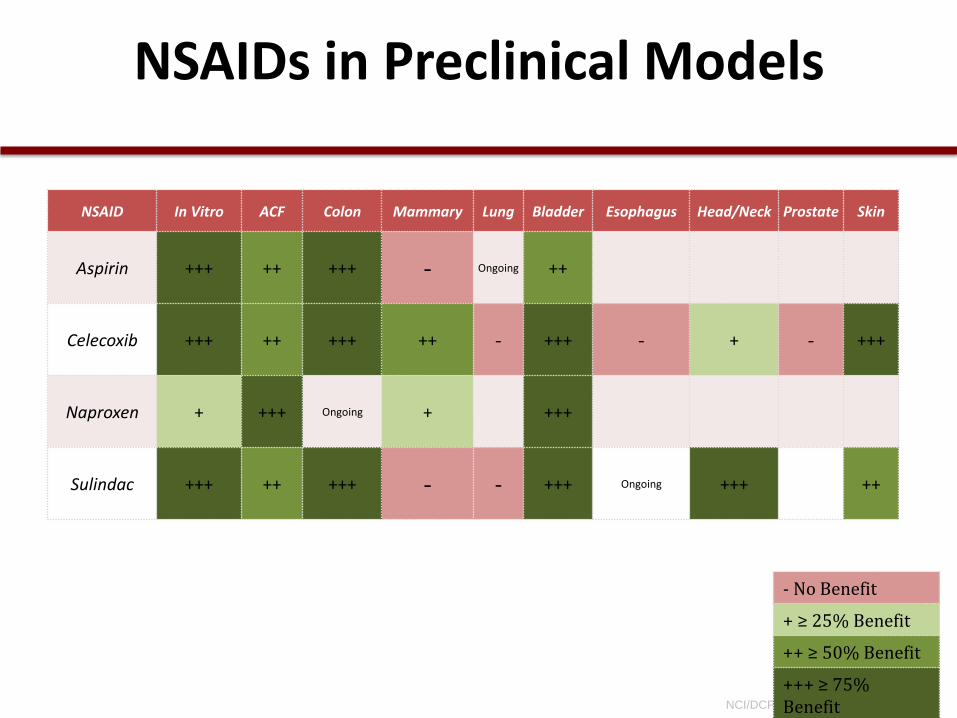
NSAIDs in Preclinical Models
NSAID In Vitro ACF Colon Mammary Lung Bladder Esophagus Head/Neck Prostate Skin
Aspirin +++ ++ +++ - Ongoing ++
Celecoxib +++ ++ +++ ++ - +++ - + - +++
Naproxen + +++ Ongoing + +++
Sulindac +++ ++ +++ - - +++ Ongoing +++ ++
- No Benefit
+ ≥ 25% Benefit
++ ≥ 50% Benefit
+++ ≥ 75% Benefit

NCI/DCP/GOCRG • Umar • 2013
• Retrospective • Prospective
0.58
0.6
0.51
0.68
Thun ‘91 - Women
Thun ‘91 - Men
Giovannucci ’94
Bansal ‘96
NSAIDs Use and Colon Cancer-Associated Mortality
Estimated Relative Risk
0 1 2
Observational Studies:
NCI/DCP/GOCRG • Umar • 2013
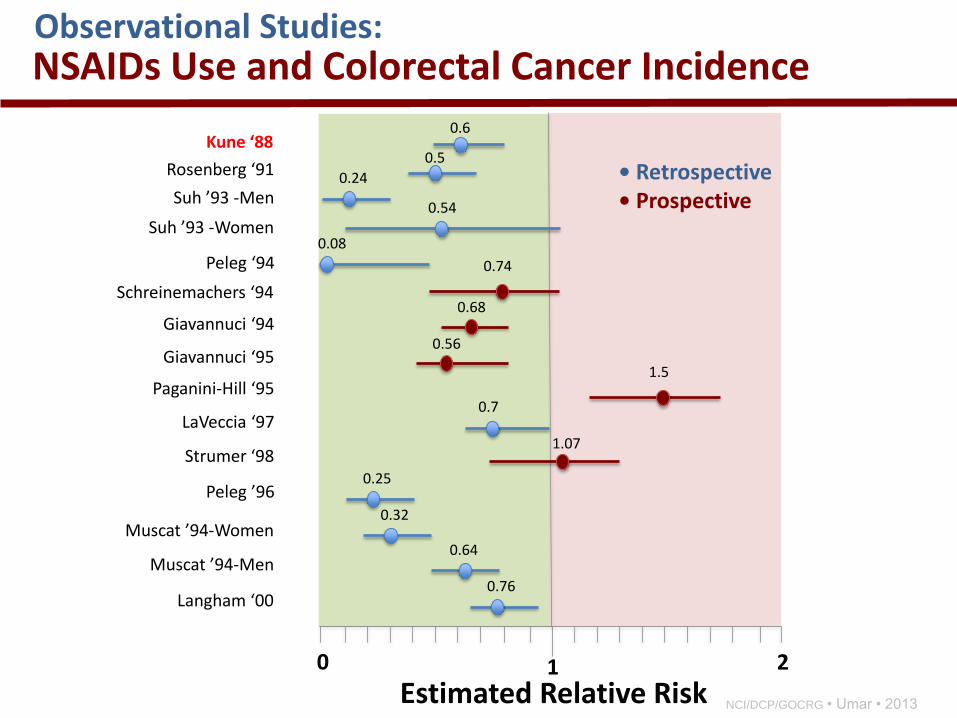
• Retrospective • Prospective
0.6
0.74
Estimated Relative Risk 0 1 2
0.5
0.24
0.08
0.54
0.7
0.68
0.56
1.5
1.07
0.25
0.32
0.64
0.76
Kune ‘88
Rosenberg ‘91
Suh ’93 -Men
Suh ’93 -Women
Peleg ‘94
Schreinemachers ‘94
Giavannuci ‘94
Paganini-Hill ‘95
LaVeccia ‘97
Strumer ‘98
Peleg ’96
Muscat ’94-Women
Muscat ’94-Men
Langham ‘00
Giavannuci ‘95
NSAIDs Use and Colorectal Cancer Incidence Observational Studies:
NCI/DCP/GOCRG • Umar • 2013
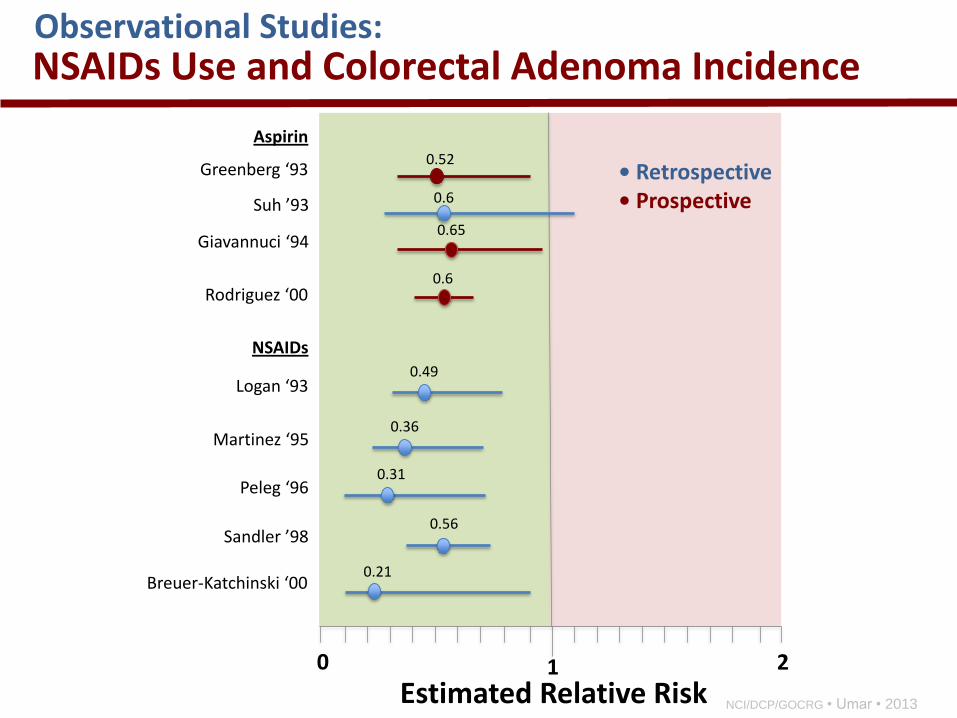
• Retrospective • Prospective
0.52
Estimated Relative Risk 0 1 2
0.6
0.49
0.56
0.65
0.6
0.31
0.21
Aspirin
Greenberg ‘93
Suh ’93
Rodriguez ‘00
NSAIDs
Giavannuci ‘94
Martinez ‘95
Peleg ‘96
Sandler ’98
Breuer-Katchinski ‘00
Logan ‘93
NSAIDs Use and Colorectal Adenoma Incidence Observational Studies:
0.36
NCI/DCP/GOCRG • Umar • 2013
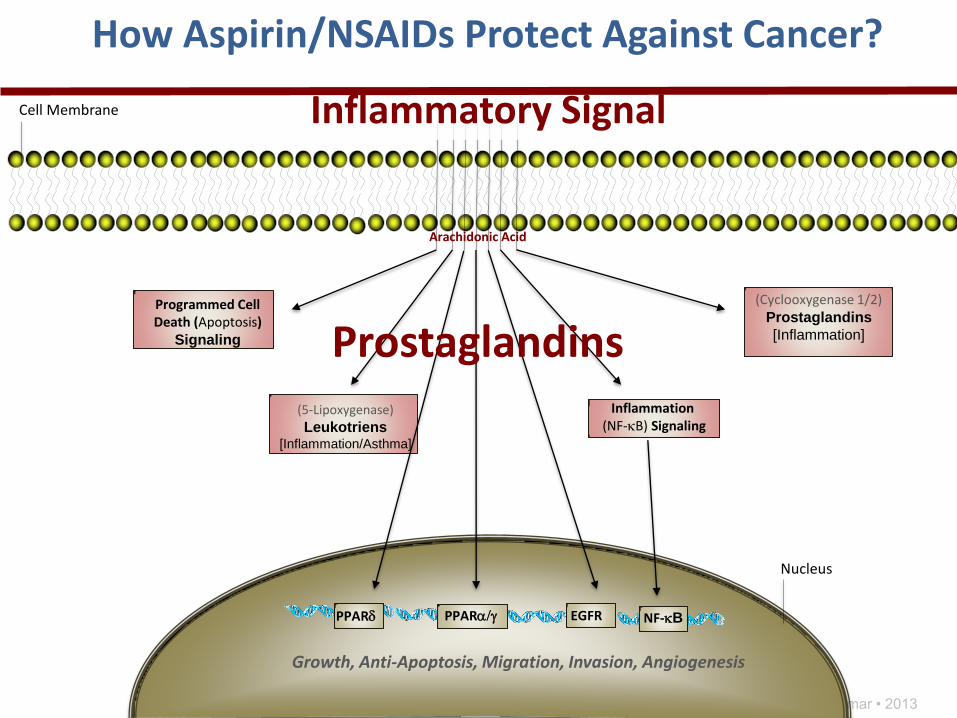
Growth, Anti-Apoptosis, Migration, Invasion, Angiogenesis
(5-Lipoxygenase)
Leukotriens [Inflammation/Asthma]
Inflammation (NF-kB) Signaling
(Cyclooxygenase 1/2) Prostaglandins
[Inflammation]
Cell Membrane
Programmed Cell Death (Apoptosis)
Signaling
Nucleus
PPARa/g PPARd NF-kB EGFR
Arachidonic Acid
Prostaglandins
How Aspirin/NSAIDs Protect Against Cancer?
Inflammatory Signal

NCI/DCP/GOCRG • Umar • 2013
Growth, Anti-Apoptosis, Migration, Invasion, Angiogenesis
(5-Lipoxygenase)
Leukotriens [Inflammation/Asthma]
Inflammation (NF-kB) Signaling
(Cyclooxygenase 1/2) Prostaglandins
[Inflammation]
Cell Membrane
Programmed Cell Death (Apoptosis)
Signaling
Nucleus
PPARa/g PPARd
Non-Steroidal Anti-Inflammatory Drugs
(Aspirin/NSAIDs)
NF-kB EGFR
Arachidonic Acid
Prostaglandins
Inflammatory Signal
How Aspirin/NSAIDs Protect Against Cancer?

NCI/DCP/GOCRG • Umar • 2013
Immune Function
Carcinogenesis
Prostaglandins (PGE2)
Arachidonic
Acid
Free Radical Production Carcinogen Activation
Proliferation
Angiogenesis
Apoptosis
COX-2
COX
inhibitor X COX-1
Sphingomyelin Ceramide
Non-COX Targets: P450s PPAR/g PPARa,g
X
NCI/DCP/GOCRG • Umar • 2013
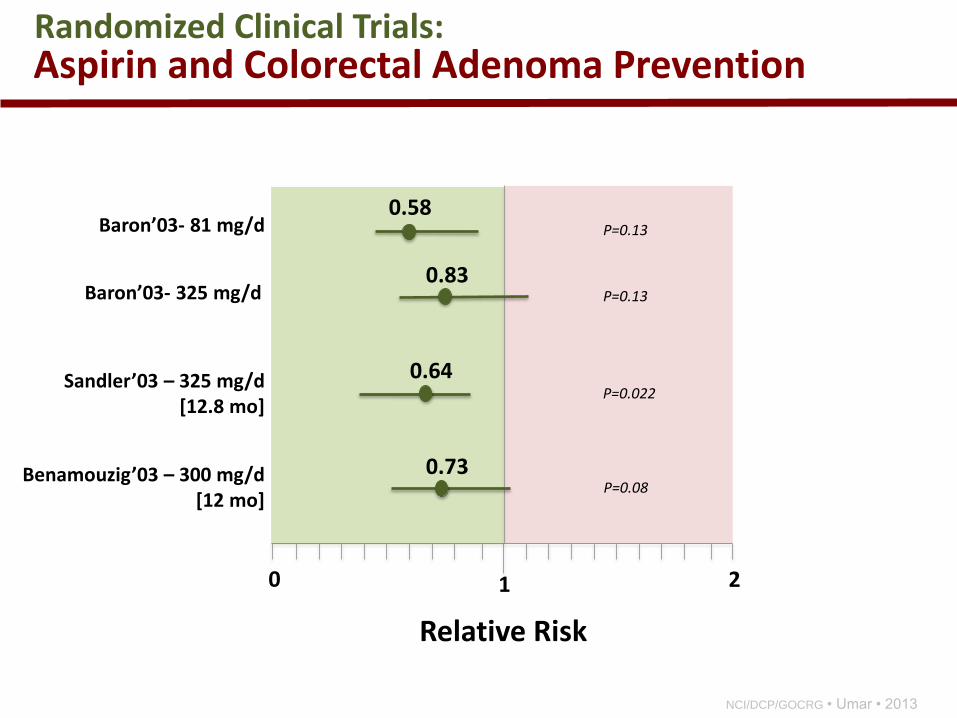
0.58
0.83
0.64
0.73
Baron’03- 81 mg/d
Baron’03- 325 mg/d
Sandler’03 – 325 mg/d [12.8 mo]
Benamouzig’03 – 300 mg/d [12 mo]
Aspirin and Colorectal Adenoma Prevention
Relative Risk
0 1 2
Randomized Clinical Trials:
P=0.022
P=0.13
P=0.13
P=0.08

NCI/DCP/GOCRG • Umar • 2013
NCI/DCP/GOCRG • Umar • 2013
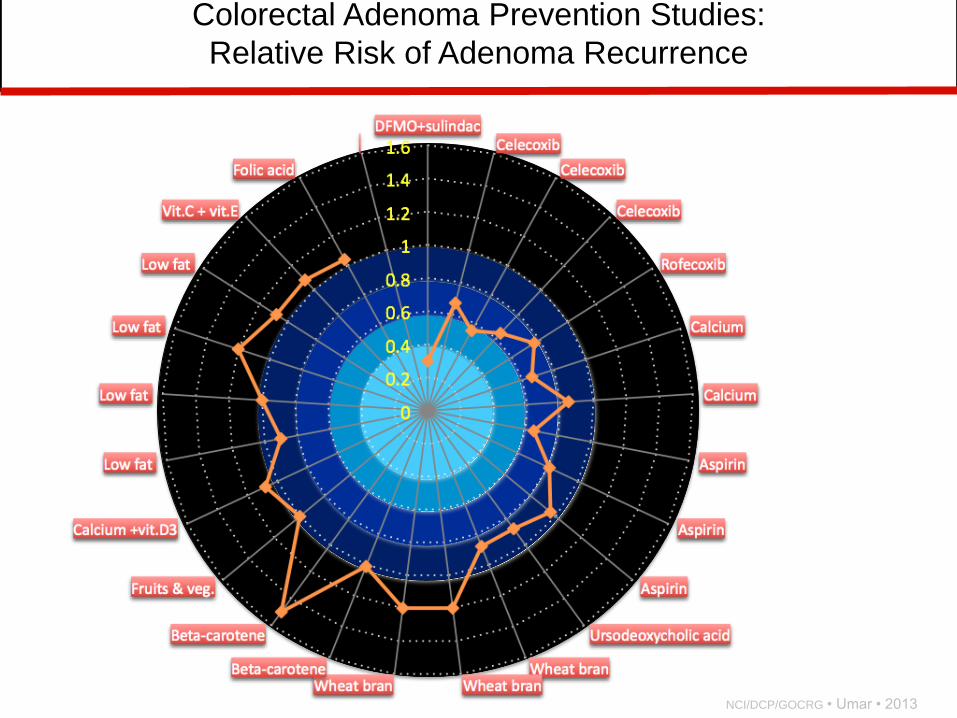
Colorectal Adenoma Prevention Studies:
Relative Risk of Adenoma Recurrence

NCI/DCP/GOCRG • Umar • 2013
Percent Change in Number of Percent Change in Number of Colorectal Polyps with Celecoxib Colorectal Polyps with Celecoxib
(Individual Patients; Median Results)(Individual Patients; Median Results)
Pe
rcen
t C
ha
ng
e f
rom
Ba
se
lin
eP
erc
en
t C
ha
ng
e f
rom
Ba
se
lin
ePlaceboPlacebo
N=15N=15100 mg BID100 mg BID
N=32N=32400 mg BID*400 mg BID*
N=30N=30
--8080
--6060
--4040
--2020
00
2020
4040
6060
8080
0%0% --7%7%
--32%32%
* P = 0.003 versus placebo* P = 0.003 versus placebo Steinbach, et al. NEJM, 2000
Randomized Trials of Celecoxib in Patients with FAP & Sporadic CRC
NCI/DCP/GOCRG • Umar • 2013
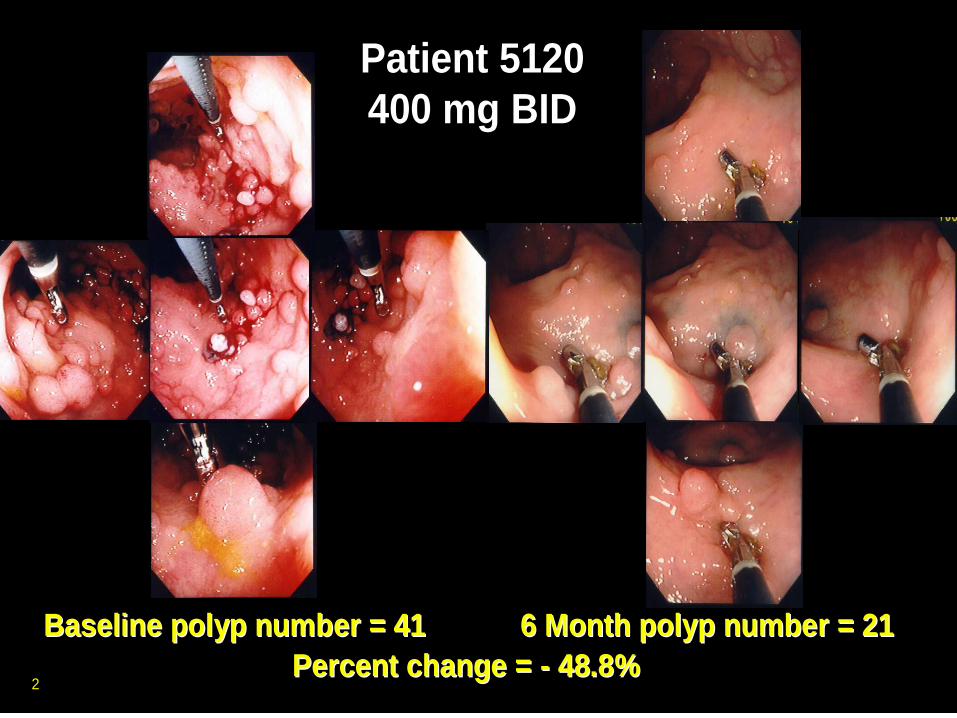
Patient 5120
400 mg BID
Patient 5120
400 mg BID
Baseline polyp number = 41Baseline polyp number = 41 6 Month polyp number = 216 Month polyp number = 21
Percent change = Percent change = -- 48.8%48.8%2
NCI/DCP/GOCRG • Umar • 2013
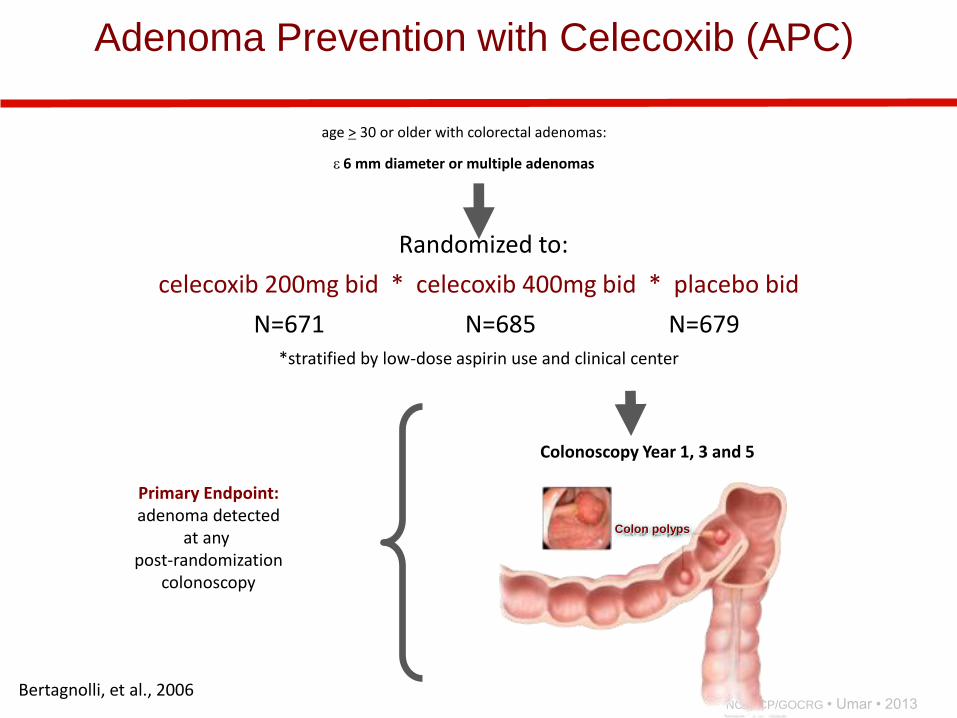
age > 30 or older with colorectal adenomas:
6 mm diameter or multiple adenomas
Randomized to:
celecoxib 200mg bid * celecoxib 400mg bid * placebo bid
N=671 N=685 N=679 *stratified by low-dose aspirin use and clinical center
Primary Endpoint: adenoma detected
at any post-randomization
colonoscopy
Bertagnolli, et al., 2006
Adenoma Prevention with Celecoxib (APC)
Colon polyps
Colonoscopy Year 1, 3 and 5

NCI/DCP/GOCRG • Umar • 2013 Bertagnolli, et al., 2006
Adenoma Prevention with Celecoxib (APC)
0
10
20
30
40
50
60
70
Placebo200 mg BID
400 mg BID
All Adenomas
Advanced Adenomas
Bertagnolli, et al., N Engl J Med 2006; 355:873-884
Randomized Clinical Trials:

NCI/DCP/GOCRG • Umar • 2013
Aspirin Versus Control on Risk of Death Due to Cancer (≥5 Years of Aspirin Treatment by Age at Randomization)
Ro
thw
ell e
t a
l., L
an
cet
20
11
: 37
7, 2
01
1
NCI/DCP/GOCRG • Umar • 2013
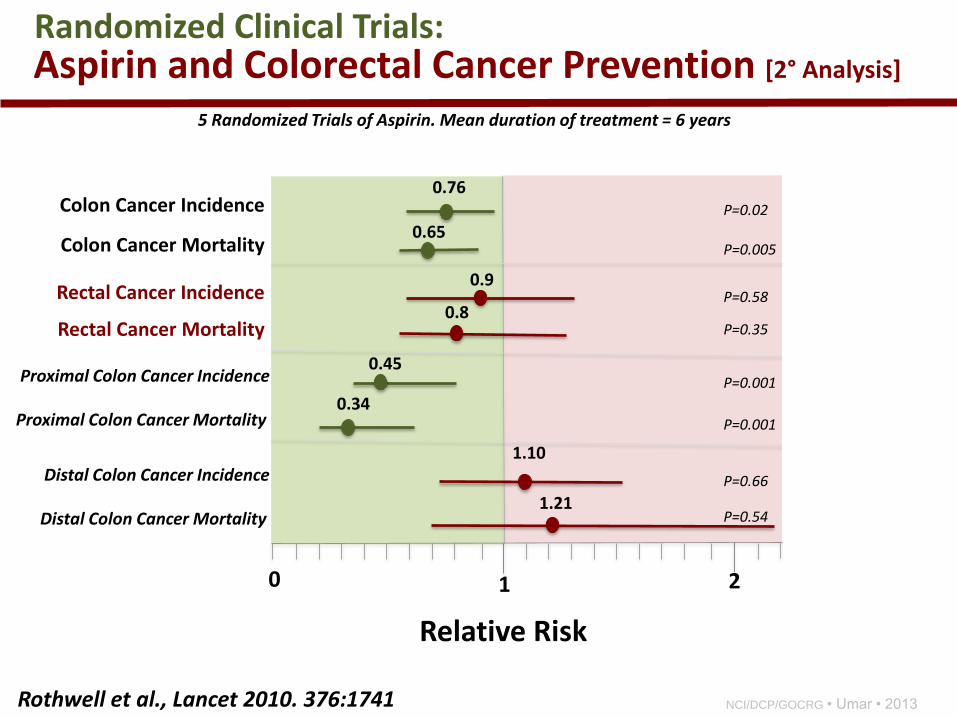
0.76
0.65
0.8
Colon Cancer Incidence
Colon Cancer Mortality
Aspirin and Colorectal Cancer Prevention [2° Analysis]
Relative Risk
0 1 2
Randomized Clinical Trials:
P=0.35
P=0.005
P=0.02
5 Randomized Trials of Aspirin. Mean duration of treatment = 6 years
Rectal Cancer Incidence 0.9
P=0.58
Rectal Cancer Mortality
0.45
0.34
1.21
Proximal Colon Cancer Incidence
P=0.54
P=0.001
P=0.001
1.10
P=0.66
Proximal Colon Cancer Mortality
Distal Colon Cancer Incidence
Distal Colon Cancer Mortality
Rothwell et al., Lancet 2010. 376:1741

NCI/DCP/GOCRG • Umar • 2013
Colorectal Cancer Prevention Agents
Aspirin/
NSAIDs/
Curcumin/
Ca/VitD?
Aspirin/
NSAIDs
Aspirin/COXIBs/
NSAIDs/DFMO

Risk Effects Benefits
Hemorrhage Block Platelet Reduce risk of
aggregation thrombosis
Mask infection Reduce inflammation Treat inflammatory
arthritis/anti-cancer?
Mask tissue injury Reduce pain Treat pain
Impair wound healing Reduce proliferation Abnormal Control
of cell growth
Aspirin: Risk versus Benefits Anti-platelet
Anti-inflammatory
Reduces PGE2

NCI/DCP/GOCRG • Umar • 2013
Aspirin and Colorectal Cancer Prevention [2° Analysis]
Relative Risk
0 1 2
Randomized Clinical Trials:
5 Randomized Trials of Aspirin. Mean duration of treatment = 6 years
Rothwell et al., Lancet 2010. 376:1741
1.01
0.81
0-2.9 years
3-4.9 years 0.7
>5 years
Major Extracranial Bleeds 1.95
1.37
0.63
0-2.9 years
3-4.9 years
>5 years
Cancer Incidence

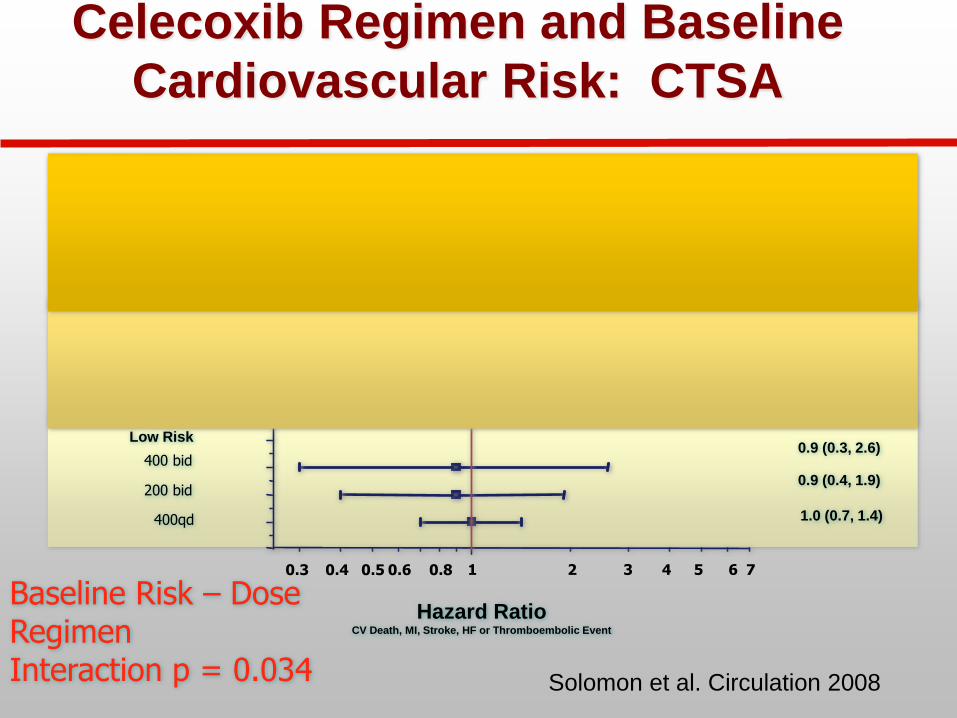
Cross Trials Safety Analysis
• Over 16,000 patient-years of follow-up
• Pooled adjudicated analysis of six randomized trials comparing celecoxib to placebo
• Overall increase in cardiovascular risk identified
• Differences in risk based on the dose and
celecoxib dose-regimen
• Patients at highest baseline cardiovascular risk
had an increased relative risk for celecoxib-
related adverse cardiovascular events
Solomon et al., Circulation 2008

CTSA Trials
• Adenoma Prevention with Celecoxib (APC) Trial
• Prevention of Sporadic Adenomatous Polyps (PreSAP) trial
• Alzheimer’s Disease Anti-inflammatory Prevention Trial (ADAPT)
• MA-27 Breast Cancer Trial
• Celecoxib Diabetic Macular Edema (CDME) trial
• Celecoxib/Selenium Trial
3-category risk score, modified Framingham Risk model – Low: No known risk factor
– Moderate: One of following , age > 75, hypertension, hyperlipidemia, current smoker, low-dose ASA
– High: Diabetes, prior CV disease, or ≥ 2 risk factors in “moderate” category
Solomon et al. Circulation 2008
400qd
200 bid
400 bid
400 qd
200 bid
400 bid
400 qd
200 bid
400 bid
Low Risk
High Risk
400 qd
400 qd
200 bid
400 bid
High Risk 3.5 (1.9,6.4)
1.7 (0.9,3.2)
0.9 (0.3, 2.6)
2.3 (1.5, 3.4)
1.5 (1.2, 1.9)
1.4 (1.0, 2.2)
1.2 (1.0,1.5)
0.9 (0.4, 1.9)
1.0 (0.7, 1.4) 400qd
200 bid
400 bid
400 qd
200 bid
400 bid
400 qd
200 bid
400 bid
Low Risk
Moderate Risk
Hazard Ratio CV Death, MI, Stroke, HF or Thromboembolic Event
High Risk
400 qd
400 qd
200 bid
400 bid
High Risk
Baseline Risk – Dose Regimen Interaction p = 0.034 Solomon et al. Circulation 2008
3.5 (1.9,6.4)
HR (95% CI)
1.7 (0.9,3.2)
0.9 (0.3, 2.6)
2.3 (1.5, 3.4)
1.5 (1.2, 1.9)
1.4 (1.0, 2.2)
1.2 (1.0,1.5)
0.9 (0.4, 1.9)
1.0 (0.7, 1.4)
Pre-Rx CV Risk
Celecoxib Regimen and Baseline
Cardiovascular Risk: CTSA
6 7 5 4 3 2 1 0.3 0.4 0.5 0.6 0.8
NCI/DCP/GOCRG • Umar • 2013
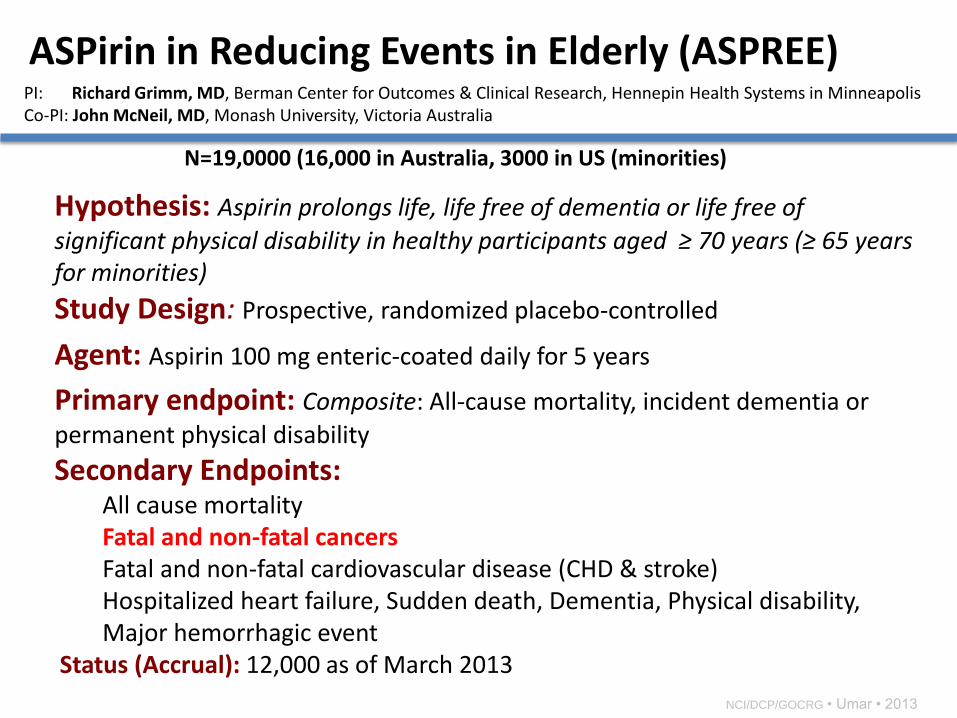
PI: Richard Grimm, MD, Berman Center for Outcomes & Clinical Research, Hennepin Health Systems in Minneapolis Co-PI: John McNeil, MD, Monash University, Victoria Australia
N=19,0000 (16,000 in Australia, 3000 in US (minorities)
Hypothesis: Aspirin prolongs life, life free of dementia or life free of
significant physical disability in healthy participants aged ≥ 70 years (≥ 65 years for minorities)
Study Design: Prospective, randomized placebo-controlled
Agent: Aspirin 100 mg enteric-coated daily for 5 years
Primary endpoint: Composite: All-cause mortality, incident dementia or
permanent physical disability
Secondary Endpoints: All cause mortality Fatal and non-fatal cancers Fatal and non-fatal cardiovascular disease (CHD & stroke) Hospitalized heart failure, Sudden death, Dementia, Physical disability, Major hemorrhagic event
Status (Accrual): 12,000 as of March 2013
ASPirin in Reducing Events in Elderly (ASPREE)
• Aspirin is effective in reducing adenomas at 81/300yr1/300yr3/300
yr4/325 mg daily doses (17/27/21/72/5%)
• Celecoxib significantly reduced colorectal adenoma occurrence
(33/34%), advanced adenomas (57/51%)
• DFMO + sulindac is synergistic in preventing recurrent adenomas (70%)
• CV toxicity gives us a pause for NSAIDs and COXIBs in general population
• Role of Aspirin in cardioprotection and cancer prevention offers hope for
cancer prevention across most Gastrointestinal tract cancers
Summary:
Summary

NCI/DCP/GOCRG • Umar • 2013