gastrointestinal tract and abdomen SPLENECTOMY · PDF filegastrointestinal tract and abdomen...
26
Scientific American Surgery DOI 10.2310/7800.2082 10/14 © 2014 Decker Intellectual Properties Inc gastrointestinal tract and abdomen SPLENECTOMY Bindhu Oommen, MD, MPH, Kent W. Kercher, MD, FACS, B. Todd Heniford, MD, FACS, and Ian A. Villanueva, MD, FACS* Most early splenectomies were done in patients who had undergone penetrating trauma. The first reported splenec- tomy in the Western world was performed by Zacarello in 1549, although the veracity of his operative description has been questioned. Between this initial report and the 1800s, very few cases were recorded. In 1816, the first recounted splenectomy in North America was performed by O’Brien; the patient was in the act of committing a rape when his victim plunged a large knife into his left side. The spleen was protruding from the wound, and the surgeon performed an en masse ligation. Initial attempts at elective splenectomy were associated with significant mortality, and these were done for sequelae of portal hypertension (Quittenbaum in 1826). Shortly there- after, when Wells performed one of the first splenectomies using general anesthesia, both patients died. In 1866, Bryant was the first to attempt splenectomy in a patient with leuke- mia. Over the following 15 years, 14 splenectomies were attempted as therapy for leukemia; none of the patients survived. In a 1908 review of 49 similar cases, Johnston reported a mortality of 87.7%. 1 These dismal results led to the abandonment of splenectomy for leukemia and other hematologic malignancies until the modern era. In 1916, Kaznelson, of Prague, was the first to report good results from splenectomy in patients with idiopathic thrombocyto- penic purpura (ITP). 2 As the 20th century progressed, splenectomy became more common in direct proportion to the increase in the use of motor vehicles. The eventual recognition of the syndrome known as overwhelming postsplenectomy infection (OPSI) made splenic conservation an important consideration. Par- tial splenectomy had initially been described by the French surgeon Péan in the 19th century. This procedure received little further study until almost 100 years later, when the Brazilian surgeon Campos Cristo reevaluated Péan’s tech- nique in his report of eight trauma patients treated with partial splenectomy. 3 Upadhyaya and Simpson’s report on 16 children admitted for splenic trauma to The Hospital for Sick Children in Toronto between 1948 and 1955 was instru- mental in establishing the validity of nonoperative treatment of splenic trauma. 4 In late 1991 and early 1992, four groups working indepen- dently—Delaître and Maignien in Paris, Carroll and col- leagues in Los Angeles, Cushieri in the United Kingdom, and Thibault and colleagues in Canada—published the first reports of laparoscopic splenectomy in patients with hematologic disorders. 5–8 Since then, the development of operative techniques for laparoscopic partial splenectomy has tested the limits of minimally invasive surgery and encouraged clinical research into methods of simplifying the execution of the operation. 9–11 Now in the 21st century, laparoscopic splenectomy has become an established stand- ard of care in the management of surgical diseases of the spleen, 12 except in the hemodynamically unstable trauma patient requiring splenectomy. 13 Although adoption of min- imally invasive splenectomy has led to a gradual decrease in the indications for open splenectomy, both procedures are still essential components of spleen surgery. Indications and Contraindications for Procedure indications In the current era of predominantly nonoperative man- agement of traumatic splenic injuries, with splenic salvage rates over 90%, 14 medical indications now represent the most common reason for splenectomy. 13,15–18 These nontraumatic indications include, but are not limited to, symptomatic relief of splenomegaly, hypersplenism secondary to chronic illnesses, blood dyscrasias, hematologic malignancies, splenic tumors and cysts, and infection [see Table 1]. 13,15,19–24 Additionally, approximately one fifth of splenectomies are performed for iatrogenic or incidental reasons, which can be * The authors and editors gratefully acknowledge the contribu- tions of the previous authors, Eric C. Poulin, MD, MSc, FACS, FRCSC, Christopher M. Schlachta, MDCM, FACS, FRSCS, and Joseph Mamazza, MDCM, FRSC, to the development and writing of this topic review. Red text is tied to a SCORE learning objective. Table 1 Clinical Indications for Splenectomy Medical indications (43%) Benign hematologic disease (56%) Idiopathic thrombocytopenic purpura (ITP) Thrombotic thrombocytopenic purpura (TTP) Hereditary spherocytosis (HS) Autoimmune hemolytic anemia (AHA) Sickle cell disease (SCD) Thalassemia Systemic erythematous lupus (SLE) Hematologic malignancy (34%) Lymphoma (Hodgkin and non-Hodgkin) Hairy cell leukemia (HCL) Splenic marginal zone lymphoma (SMZL) Chronic lymphocytic leukemia (CLL) Chronic myelogenous leukemia (CML) Acute lymphocytic leukemia (ALL) Acute myelogenous leukemia (AML) Myelodysplastic syndrome (MDS) Idiopathic myelofibrosis Solid tumors and cysts Hemangiomas Hemangiosarcoma Infection Splenic abscess Tuberculosis Trauma (37%) Iatrogenic/incidental (20%) Esophageal/gastric surgery (32%) Colon surgery (30%)
Transcript of gastrointestinal tract and abdomen SPLENECTOMY · PDF filegastrointestinal tract and abdomen...

Scientific American Surgery DOI 10.2310/7800.2082
10/14
© 2014 Decker Intellectual Properties Inc
gastrointestinal tract and abdomen
S P L E N E C T O M Y
Bindhu Oommen, MD, MPH, Kent W. Kercher, MD, FACS, B. Todd Heniford, MD, FACS, and Ian A. Villanueva, MD, FACS*
Most early splenectomies were done in patients who had undergone penetrating trauma. The first reported splenectomy in the Western world was performed by Zacarello in 1549, although the veracity of his operative description has been questioned. Between this initial report and the 1800s, very few cases were recorded. In 1816, the first recounted splenectomy in North America was performed by O’Brien; the patient was in the act of committing a rape when his victim plunged a large knife into his left side. The spleen was protruding from the wound, and the surgeon performed an en masse ligation.
Initial attempts at elective splenectomy were associated with significant mortality, and these were done for sequelae of portal hypertension (Quittenbaum in 1826). Shortly thereafter, when Wells performed one of the first splenectomies using general anesthesia, both patients died. In 1866, Bryant was the first to attempt splenectomy in a patient with leukemia. Over the following 15 years, 14 splenectomies were attempted as therapy for leukemia; none of the patients survived. In a 1908 review of 49 similar cases, Johnston reported a mortality of 87.7%.1 These dismal results led to the abandonment of splenectomy for leukemia and other hematologic malignancies until the modern era. In 1916, Kaznelson, of Prague, was the first to report good results from splenectomy in patients with idiopathic thrombocytopenic purpura (ITP).2
As the 20th century progressed, splenectomy became more common in direct proportion to the increase in the use of motor vehicles. The eventual recognition of the syndrome known as overwhelming postsplenectomy infection (OPSI) made splenic conservation an important consideration. Partial splenectomy had initially been described by the French surgeon Péan in the 19th century. This procedure received little further study until almost 100 years later, when the Brazilian surgeon Campos Cristo reevaluated Péan’s technique in his report of eight trauma patients treated with partial splenectomy.3 Upadhyaya and Simpson’s report on 16 children admitted for splenic trauma to The Hospital for Sick Children in Toronto between 1948 and 1955 was instrumental in establishing the validity of nonoperative treatment of splenic trauma.4
In late 1991 and early 1992, four groups working independently—Delaître and Maignien in Paris, Carroll and colleagues in Los Angeles, Cushieri in the United Kingdom, and Thibault and colleagues in Canada—published the first reports of laparoscopic splenectomy in patients with hematologic disorders.5–8 Since then, the development of
operative techniques for laparoscopic partial splenectomy has tested the limits of minimally invasive surgery and encouraged clinical research into methods of simplifying the execution of the operation.9–11 Now in the 21st century, laparoscopic splenectomy has become an established standard of care in the management of surgical diseases of the spleen,12 except in the hemodynamically unstable trauma patient requiring splenectomy.13 Although adoption of minimally invasive splenectomy has led to a gradual decrease in the indications for open splenectomy, both procedures are still essential components of spleen surgery.
Indications and Contraindications for Procedure
indications
In the current era of predominantly nonoperative management of traumatic splenic injuries, with splenic salvage rates over 90%,14 medical indications now represent the most common reason for splenectomy.13,15–18 These nontraumatic indications include, but are not limited to, symptomatic relief of splenomegaly, hypersplenism secondary to chronic illnesses, blood dyscrasias, hematologic malignancies, splenic tumors and cysts, and infection [see Table 1].13,15,19–24 Additionally, approximately one fifth of splenectomies are performed for iatrogenic or incidental reasons, which can be
* The authors and editors gratefully acknowledge the contributions of the previous authors, Eric C. Poulin, MD, MSc, FACS, FRCSC, Christopher M. Schlachta, MDCM, FACS, FRSCS, and Joseph Mamazza, MDCM, FRSC, to the development and writing of this topic review.
Red text is tied to a SCORE learning objective.
Table 1 Clinical Indications for SplenectomyMedical indications (43%)
Benign hematologic disease (56%)Idiopathic thrombocytopenic purpura (ITP)Thrombotic thrombocytopenic purpura (TTP)Hereditary spherocytosis (HS)Autoimmune hemolytic anemia (AHA)Sickle cell disease (SCD)ThalassemiaSystemic erythematous lupus (SLE)
Hematologic malignancy (34%)Lymphoma (Hodgkin and nonHodgkin)Hairy cell leukemia (HCL)Splenic marginal zone lymphoma (SMZL)Chronic lymphocytic leukemia (CLL)Chronic myelogenous leukemia (CML)Acute lymphocytic leukemia (ALL)Acute myelogenous leukemia (AML)Myelodysplastic syndrome (MDS)Idiopathic myelofibrosis
Solid tumors and cystsHemangiomasHemangiosarcoma
InfectionSplenic abscessTuberculosis
Trauma (37%)Iatrogenic/incidental (20%)
Esophageal/gastric surgery (32%) Colon surgery (30%)

Scientific American Surgery
10/14
gastro splenectomy — 2
either malignant (e.g., organ resection for cancers of the stomach, pancreas, colon, adrenal gland, or kidney) or nonmalignant.15,18 Although it is not within the scope of this topic review to present full, detailed descriptions of all of these indications, we touch on each to describe the evolving surgical role of splenectomy in these disease processes.
Splenomegaly and Hypersplenism
Splenomegaly and hypersplenism are clinical entities that are often the symptomatic manifestations of various hematologic conditions. Splenomegaly refers to an enlargement of the spleen and can be classified based on weight or craniocaudal length [see Figure 1 and Table 2].25 Hypersplenism, not to be confused with splenomegaly, is a nonspecific term indicating that the intrinsic activities of the spleen go unregulated, with subsequent sequestration and destruction of blood cells with or without an associated increase in splenic size.20,26 A significant reduction in one or more cellular elements of the blood then results in anemia, thrombocytopenia, or pancytopenia, in the presence of normocellular or hypercellular bone marrow and/or splenomegaly.20,26,27
Hypersplenism can be primary or secondary in etiology. Primary hypersplenism is thought to be related to congenita l or acquired alteration in blood cell membrane or structure (e.g., ITP, hemolytic anemias).20 Secondary hypersplenism is associated with certain acute and chronic infections, autoimmune states (e.g., Felty syndrome, systemic lupus erythematosus), infiltrative and neoplastic conditions involving the spleen (e.g., sarcoidosis, Gaucher disease, certain myeloproliferative disorders, and lymphomas), and occasionally “congestive splenomegaly,” brought about by portal hypertension or splenic vein thrombosis.20
The decision to perform splenectomy for either splenomegaly and/or hypersplenism should be based on well defined, welldocumented, and often strictly limited indications. For example, in some instances of refractory cytopenias manifesting with massive splenomegaly or clinically significant bleeding disorders, splenectomy can be palliative and is the treatment of choice in reducing transfusion requirements and improving blood counts. In this setting, splenectomy usually does not alter the overall disease
progression, but it can aid in controlling pressurerelated symptoms in the majority of patients and help achieve durable remission in at least half of cases.27,28 Patients with cirrhosis and portal hypertension have a higher incidence of hypersplenism,27 and recent evidence suggests that splenectomy may also have a role in these patients with liver disease (i.e., cirrhosis, hepatocellular carcinoma, etc.) and hypersplenism, particularly with regard to improving liver function and expanding the indication of liver resection if postoperative management is conducted conservatively.29–32 Thus, for both splenomegaly and hypersplenism, especially in the setting of hematologic malignancy or hematopoietic disorder, the potential for palliation and known mean duration of expected response must be weighed against the increased morbidity and mortality of splenectomy in this subset of patients.20,33
Benign Hematologic Disease
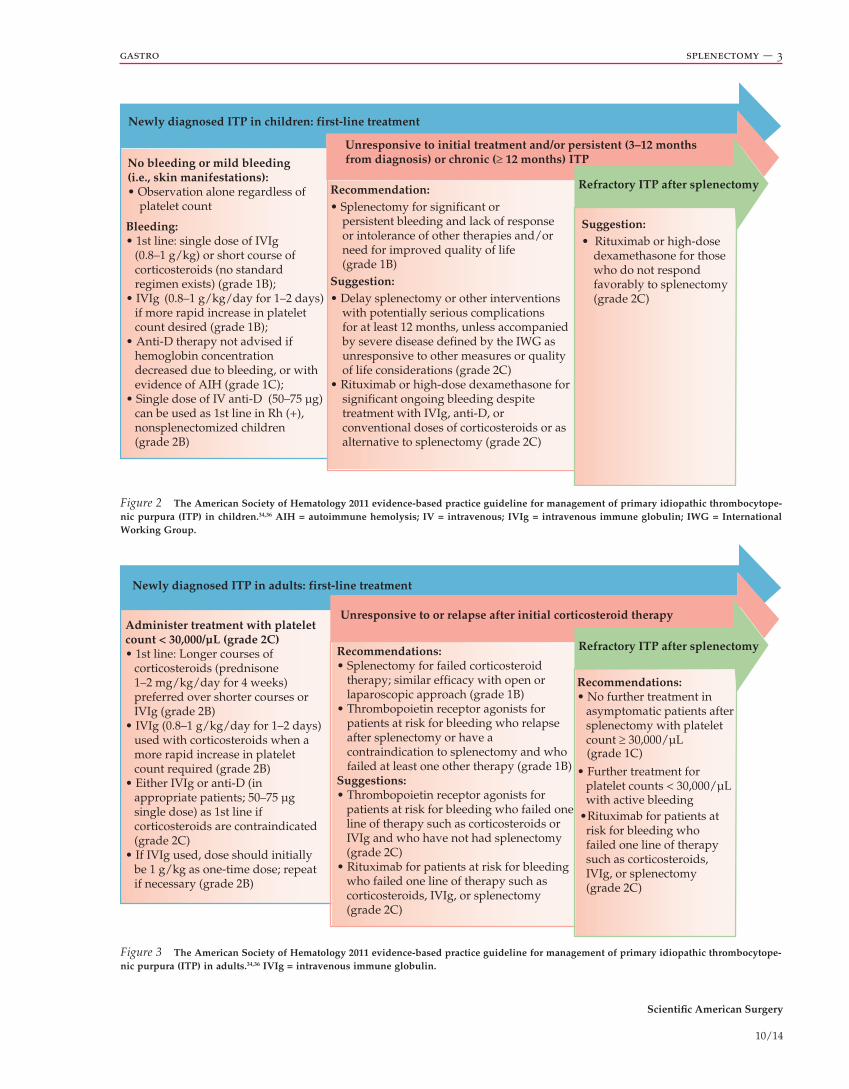
Idiopathic thrombocytopenic purpura This autoimmune disorder has a variable clinical course and is characterized by thrombocytopenia secondary to antiplatelet antibodymediated destruction of platelets.34 ITP can occur in both adults and children and can be either acute (occurrin g less than 6 months and usually resolving spontaneously), persistent (3 to 12 months from diagnosis), or chronic (lasting more than 12 months).34,35 The American Society of Hematology evidencebased practice guidelines for the management of ITP in both children and adults are provided here [see Figure 2 and Figure 3].34,36 Medical therapy is considered firstline treatment for ITP and includes corticosteroids, intravenous immune globulin (IVIg), or intravenous antiD (i.e., Rho(D) immunoglobulin).37 Splenectomy, on the other hand, is generally recommended for chronic or persistent ITP associated with significant or persistent bleeding, a lack of responsiveness or intolerance to other therapies, and/or a need for improved quality of life.34 Patients who respond to steroids usually have a curative response (over 90%) to splenectomy.38 However, splenectom y or other interventions with potentially serious complications should be delayed for at least 12 months after initiation of medical therapy, unless accompanied by severe disease that is unresponsive to other measures or other quality of life considerations.34,39
A recent analysis of outcomes and treatment costs for children undergoing splenectomy for chronic ITP proposed that early surgical consultation may be justified given the high success rate and low morbidity, particularly given the significant complication rate and cost of continued medical treatment. In this series of 22 patients, from the time of diagnosis to splenectomy, patients were administered a Figure 1 Splenomegaly.
Table 2 Classification of SplenomegalySpleen Size Weight (g) Craniocaudal Length (cm)
Normal 150–200 < 12
Nonmassive < 600 < 17
Massive 600–1,600 17–22
Supermassive > 1,600 > 22
Scientific American Surgery
10/14
gastro splenectomy — 3
Figure 2 The American Society of Hematology 2011 evidence-based practice guideline for management of primary idiopathic thrombocytope-nic purpura (ITP) in children.34,36 AIH = autoimmune hemolysis; IV = intravenous; IVIg = intravenous immune globulin; IWG = International Working Group.
Figure 3 The American Society of Hematology 2011 evidence-based practice guideline for management of primary idiopathic thrombocytope-nic purpura (ITP) in adults.34,36 IVIg = intravenous immune globulin.
Newly diagnosed ITP in children: first-line treatment
Unresponsive to initial treatment and/or persistent (3–12 monthsfrom diagnosis) or chronic (≥ 12 months) ITP
Refractory ITP after splenectomy
No bleeding or mild bleeding (i.e., skin manifestations):• Observation alone regardless of platelet count
Bleeding:• 1st line: single dose of IVIg (0.8–1 g/kg) or short course of corticosteroids (no standard regimen exists) (grade 1B);• IVIg (0.8–1 g/kg/day for 1–2 days) if more rapid increase in platelet count desired (grade 1B);• Anti-D therapy not advised if hemoglobin concentration decreased due to bleeding, or with evidence of AIH (grade 1C);• Single dose of IV anti-D (50–75 µg) can be used as 1st line in Rh (+), nonsplenectomized children (grade 2B)
Recommendation:• Splenectomy for significant or persistent bleeding and lack of response or intolerance of other therapies and/or need for improved quality of life (grade 1B)Suggestion:• Delay splenectomy or other interventions with potentially serious complications for at least 12 months, unless accompanied by severe disease defined by the IWG as unresponsive to other measures or quality of life considerations (grade 2C)• Rituximab or high-dose dexamethasone for significant ongoing bleeding despite treatment with IVIg, anti-D, or conventional doses of corticosteroids or as alternative to splenectomy (grade 2C)
Suggestion:• Rituximab or high-dose dexamethasone for those who do not respond favorably to splenectomy (grade 2C)
Newly diagnosed ITP in adults: first-line treatment
Unresponsive to or relapse after initial corticosteroid therapy
Refractory ITP after splenectomy
Administer treatment with platelet count < 30,000/µL (grade 2C)• 1st line: Longer courses of
corticosteroids (prednisone 1–2 mg/kg/day for 4 weeks) preferred over shorter courses or IVIg (grade 2B)• IVIg (0.8–1 g/kg/day for 1–2 days) used with corticosteroids when a more rapid increase in platelet count required (grade 2B)• Either IVIg or anti-D (in appropriate patients; 50–75 µg single dose) as 1st line if corticosteroids are contraindicated (grade 2C)• If IVIg used, dose should initially be 1 g/kg as one-time dose; repeat if necessary (grade 2B)
Recommendations:• Splenectomy for failed corticosteroid therapy; similar efficacy with open or laparoscopic approach (grade 1B)• Thrombopoietin receptor agonists for
patients at risk for bleeding who relapseafter splenectomy or have a contraindication to splenectomy and whofailed at least one other therapy (grade 1B)
Suggestions:• Thrombopoietin receptor agonists for
patients at risk for bleeding who failed oneline of therapy such as corticosteroids or IVIg and who have not had splenectomy(grade 2C)
• Rituximab for patients at risk for bleedingwho failed one line of therapy such as corticosteroids, IVIg, or splenectomy(grade 2C)
Recommendations:• No further treatment in asymptomatic patients after splenectomy with platelet count ≥ 30,000/µL
• Further treatment for platelet counts < 30,000/µL with active bleeding•Rituximab for patients at risk for bleeding who failed one line of therapy such as corticosteroids, IVIg, or splenectomy (grade 2C)
(grade 1C)

Scientific American Surgery
10/14
gastro splenectomy — 4
median of six (range 0 to 60) doses of IVIg and a median of one dose of antiD antibody, in addition to concomitant steroid therapy.37 The only reported complication was OPSI after a dog bite with a median followup of 15 months (range 1 to 79), and the group found that the median cost of splenectomy was significantly less than the cost of medical therapy ($20,803 versus $146,284; p < .05).37 With 30day and longterm complication rates of 10% and 5%, respectively, low mortality, and favorable response rates (complete response rates of 77 to 85%), splenectomy is considered definitive therapy and an effective adjunct in the management course of patients failing to achieve or sustain response s to medical therapy.37,40
Autoimmune hemolytic anemia (AHA) This group of diseases is characterized by autoantibodymediated red blood cell (RBC) destruction; it is divided into warm and cold autoantibody types and by the presence of an underlying or associated disorder into primary and secondary. As with ITP, AHA should be treated medically, and most patients do respond, although relapses can occur, requiring maintenance therapy. Splenectomy is an effective secondline treatment, with low morbidity, and can provide longterm remission without medication.40 For those patients who require high maintenance doses or are unfavorable candidates for surgery, rituximab, a monoclonal antibody against protein CD20, which is primarily found on the surface of immune B cells, is useful and is the best therapeutic alternative for steroidrefractory patients.41
Hereditary spherocytosis (HS) HS is characterized by hemolytic anemia and splenomegaly, with retention and damage of abnormal RBCs, caused by an intrinsic erythrocyte membrane defect.42 Splenectomy is considered the treatment of choice for patients with symptomatic HS as it removes the primary spherocytes,42 reducing the intraspleni c hemolytic process of the disease and therefore correcting the anemia.43 Partial splenectomy can decrease hemolysis; however, total splenectomy is more effective. Partial splenectom y, advocated for children in particular, has been associated with longer operative times and length of stay; these disadvantages should be balanced by retained immunity.44
Thrombotic thrombocytopenic purpura (TTP) Whether by inherited or acquired deficiency of a metalloproteinase (i.e., ADAMTS13) that cleaves large multimers of von Willebrand factor, TTP is characterized by thrombocytopenia and microangiopathic hemolytic anemia.45 It is further manifested by elevated lactate dehydrogenase (LDH) concentration and RBC fragments.45
TTP is one of the few hematologic emergencies, with almost inevitable death if left untreated. The role of splenectomy in the treatment of TTP has evolved.45 Historically, splenectomy with corticosteroids was considered firstline therapy for TTP, but this had response rates of only around 50%, with mortality of up to 40%.4650 Subsequent advent of plasma exchange improved prognosis with TTP, with remission rates of 70 to 80%.51,52 Today, plasma exchange remains firstline therapy for patients with TTP, and the role of splenectomy in treatment of this disease remains controversial.45,53
For the 20 to 30% of patients who are either resistant to plasma exchange or have repeated relapses requiring frequent plasma exchange therapy to maintain remission, immunosuppression and splenectomy are treatment options.19,51,52,54 Splenectomy, by eliminating a source of pathogenic autoantibody production, can be a successful treatment for patients with relapsing or plasmarefractory acquired TTP. However, data supporting splenectomy for TTP are limited to case series, with no control group and variable followup data to report to estimate relapse rates.19
Sickle cell disease (SCD) The primary role of splenectomy with SCD is after an acute splenic sequestration crisis. An acute splenic sequestration crisis is a medical emergency, requiring immediate restoration of blood volume, usually with RBC transfusions, to counteract the rapid entrapment, pooling, and destruction of RBCs in the spleen.21 Acute splenic sequestration is characterized by rapid onset of abdominal pain and distention, pallor, weakness, dyspnea, and tachycardia; it is defined clinically as splenomegaly and a fall in hemoglobin concentration by 2 g/dL or more from the person’s normal levels.21,55,56
Approximately 50% of patients have recurrence of acute splenic sequestration after the first attack, with decreasing intervals between subsequent crises and an associated 20% mortality with recurrence.55,57 Both longterm blood transfusions and splenectomy are options for preventing further episodes of acute splenic sequestration or death. However, transfusions are wrought with their own complications and are expensive and time consuming. In this regard, splenectomy may reduce recurrence (partial splenectomy) or prevent further sequestration crisis (total splenectomy).21,57 Still, there is a lack of evidence showing that splenectomy improves survival or decreases morbidity from acute spleni c sequestration.21
Hematologic Malignancies
Although certain benign platelet disorders and anemias respond well to surgical intervention, splenectomy for hematologic malignancies has commenced only in the last decade.26 In a study of 134 patients with hematologic malignancies at MD Anderson Cancer Center, splenectomy was associated with a perioperative mortality of 5% and a major morbidity rate of 4%. Moreover, splenectomy produced a significant and longlasting restoration of platelet levels with a decrease in transfusion requirements, as well as symptomatic relief (e.g., early satiety, fullness, or pain).26 These benefits were demonstrated for the most profoundly thrombocytopenic patients as well. The group concluded that although surgery may not serve as an independent singlemodality therapeutic intervention for patients with hematologic malignancies, it does serve an adjunct role.
Hairy cell leukemia (HCL) Over the last five decades, treatment of HCL, a rare adult B cell lymphoid leukemia characterized by pancytopenia, splenomegaly, and absolute monocytopenia,58 has progressed from splenectomy to interferon alfa to purine nucleoside analogues. Splenectomy was associated with a good response but a 5year survival rate of only 68%, whereas interferona was associated with much lower complete response rates. However, the introduction of

Scientific American Surgery
10/14
gastro splenectomy — 5
cell lung cancer, and malignant pheochromocytoma. Generally, a history of malignancy and a splenic mass warrant high suspicion and further workup. In selected cases of isolated metastasis to the spleen, splenectomy may improve diseasefree and/or overall survival.
Splenic Abscesses and Cysts
Splenic abscesses and parasitic cysts Infectious or parasitic splenic cysts are rare but can be life threatening.66,67 Pyogenic abscesses are a common result of splenic trauma and/or hematogenous or contiguous bacterial spread and usually present as isolated, heterogeneous, hypodense lesions with smooth or irregular borders and show variable enhancement.64,67 In contrast, mycobacterial and fungal involvement of the spleen, usually seen in the immunocompromised patient, is suspected when multiple small 5 to 10 mm nodules are seen diffusely involving the spleen.64 Although there is a role for medical therapy with infectious splenic cysts (parasitic or abscess), total splenectomy combined with antibiotics remains the treatment of choice for splenic abscesses, particularly if there are multiple abscesses.66,67 Carbonell and colleagues demonstrated in the first published series that laparoscopic splenectomy for splenic abscess is both safe and effective.68 More recently, depending on abscess size and patient conditions, antibiotics with a spleenpreserving approach are advocated, particularly in immunocompetent children. This has been accomplished with both partial splenectomy and percutaneous drainage. With regard to parasitic cysts (e.g., hydatid cysts) of the spleen, although antihelminthic medications are used in addition to surgery, most of these drugs do not reach adequate concentrations within the cyst cavity to kill the parasites; therefore, the standard treatment of hydatid cyst disease remains surgery.66 Both the open or laparoscopic approach is acceptable, but total splenectomy is preferred, especially for larger cysts, due to the high risk of intraoperative rupture when a conservative approach is adapted during surgery.66
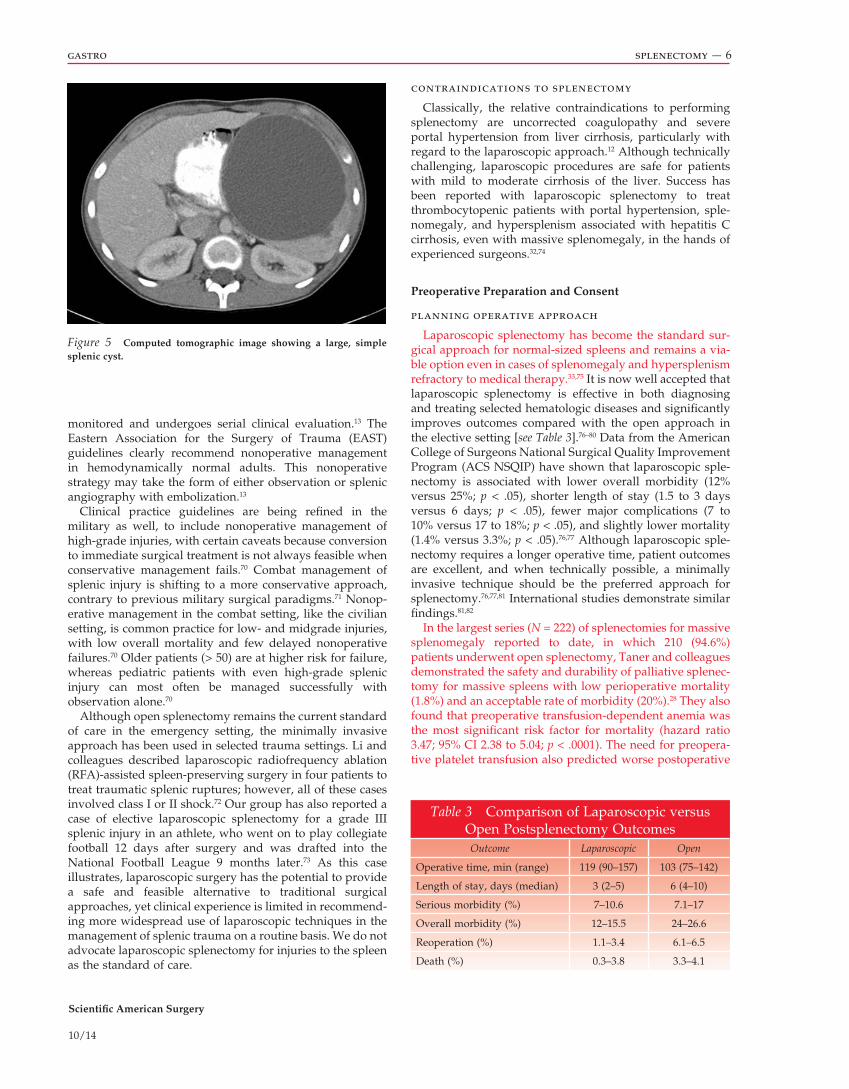
With regard to nonparasitic splenic cysts, congenital cysts are the most common (82%), followed by posttraumatic cysts (15%) [see Figure 5].69 Minimally invasive, spleen preserving surgery is the preferred treatment in selected patients, although total splenectomy is optimal and provides definitive treatment. Small cysts (< 5 cm) may be managed conservatively with computed tomography (CT) or ultrasound followup. Larger cysts, and cysts that progress in size or are symptomatic, should be treated by open or laparoscopic splenectomy. Due to unacceptably high recurrence rates, laparoscopic cystectomy/partial decapsulation/unroofing is not recommended.69
Trauma
The management of splenic trauma has evolved over the past three decades. Exploratory laparotomy with splenectomy remains the mainstay of treatment for patients with diffuse peritonitis or who are hemodynamically unstable after blunt abdominal trauma. However, selective nonoperative management supersedes splenectomy for the hemodynamically stable patient, irrespective of the grade of injury, age of the patient, or presence of associated injuries, in favor of splenic preservation, assuming that the patient is closely
purine nucleoside analogues (e.g., pentostatin59 and cladribine60) has changed the course of this rare disease, with a high rate of complete and durable remissions. Purine analogues are now the mainstay of treatment for HCL.58,61–63 Patients who relapse are generally retreated with a purine analogue, with or without a monoclonal antibody, rituximab.58,61,63 Currently, the principal indication for splenectomy in patients with HCL is symptomatic splenomegaly in the presence of lowlevel bone marrow infiltration.63 The British Journal of Haematology guidelines emphasize the importance of waiting at least 6 months for the full benefits of splenectomy to be apparent before starting any other therapy.63
Splenic Neoplasms
Primary splenic neoplasms Primary benign splenic neoplasms include hemangioma [see Figure 4], hamartoma, littoral cell angioma, and inflammatory pseudotumor.64 Primary malignant neoplasms involving the spleen are lymphoma, arising from the white pulp, and angiosarcoma, arising from the red pulp. NonHodgkin lymphoma of B cell origin is the most common primary splenic lymphoma.64 Angiosarcoma, although rare, is the most common primary nonhematopoietic malignant tumor of the spleen.64 It is a highly aggressive tumor with a poor prognosis and is associated with splenomegaly and spontaneous splenic rupture in about 25% of patients.64 Primary malignant splenic neoplasms should be treated with splenectomy. Benign neoplasms causing significant mass effect should also be treated with splenectomy; partial splenectomy should be considered when feasible.
Metastatic lesions The spleen is an uncommon site of metastatic disease. In one of the largest series (n = 148) of splenectomies for suspicious splenic masses identified on imaging, the authors at Memorial SloanKettering Cancer Center demonstrated that a previous history of cancer was an independent predictor of malignancy in splenic lesions (OR 6.3; 95% CI 2.32 to 16.97; p = .001); the most common pathologies included ovarian cancer, melanoma, and colorectal cancer.65 There are also case reports of splenic metastasis from squamous cell carcinoma of the esophagus, non–small
Figure 4 A splenic mass.
Scientific American Surgery
10/14
gastro splenectomy — 6
Figure 5 Computed tomographic image showing a large, simple splenic cyst.
monitored and undergoes serial clinical evaluation.13 The Eastern Association for the Surgery of Trauma (EAST) guidelines clearly recommend nonoperative management in hemodynamically normal adults. This nonoperative strategy may take the form of either observation or splenic angiography with embolization.13
Clinical practice guidelines are being refined in the military as well, to include nonoperative management of highgrade injuries, with certain caveats because conversion to immediate surgical treatment is not always feasible when conservative management fails.70 Combat management of splenic injury is shifting to a more conservative approach, contrary to previous military surgical paradigms.71 Nonoperative management in the combat setting, like the civilian setting, is common practice for low and midgrade injuries, with low overall mortality and few delayed nonoperative failures.70 Older patients (> 50) are at higher risk for failure, whereas pediatric patients with even highgrade splenic injury can most often be managed successfully with observation alone.70
Although open splenectomy remains the current standard of care in the emergency setting, the minimally invasive approach has been used in selected trauma settings. Li and colleagues described laparoscopic radiofrequency ablation (RFA)assisted spleenpreserving surgery in four patients to treat traumatic splenic ruptures; however, all of these cases involved class I or II shock.72 Our group has also reported a case of elective laparoscopic splenectomy for a grade III splenic injury in an athlete, who went on to play collegiate football 12 days after surgery and was drafted into the National Football League 9 months later.73 As this case illustrates, laparoscopic surgery has the potential to provide a safe and feasible alternative to traditional surgical approaches, yet clinical experience is limited in recommending more widespread use of laparoscopic techniques in the management of splenic trauma on a routine basis. We do not advocate laparoscopic splenectomy for injuries to the spleen as the standard of care.
contraindications to splenectomy
Classically, the relative contraindications to performing splenectomy are uncorrected coagulopathy and severe portal hypertension from liver cirrhosis, particularly with regard to the laparoscopic approach.12 Although technically challenging, laparoscopic procedures are safe for patients with mild to moderate cirrhosis of the liver. Success has been reported with laparoscopic splenectomy to treat thrombocytopenic patients with portal hypertension, splenomegaly, and hypersplenism associated with hepatitis C cirrhosis, even with massive splenomegaly, in the hands of experienced surgeons.32,74
Preoperative Preparation and Consent
planning operative approach
Laparoscopic splenectomy has become the standard surgical approach for normalsized spleens and remains a viable option even in cases of splenomegaly and hypersplenism refractory to medical therapy.33,75 It is now well accepted that laparoscopic splenectomy is effective in both diagnosing and treating selected hematologic diseases and significantly improves outcomes compared with the open approach in the elective setting [see Table 3].76–80 Data from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) have shown that laparoscopic splenectomy is associated with lower overall morbidity (12% versus 25%; p < .05), shorter length of stay (1.5 to 3 days versus 6 days; p < .05), fewer major complications (7 to 10% versus 17 to 18%; p < .05), and slightly lower mortality (1.4% versus 3.3%; p < .05).76,77 Although laparoscopic splenectomy requires a longer operative time, patient outcomes are excellent, and when technically possible, a minimally invasive technique should be the preferred approach for splenectomy.76,77,81 International studies demonstrate similar findings.81,82
In the largest series (N = 222) of splenectomies for massive splenomegaly reported to date, in which 210 (94.6%) patients underwent open splenectomy, Taner and colleagues demonstrated the safety and durability of palliative splenectomy for massive spleens with low perioperative mortality (1.8%) and an acceptable rate of morbidity (20%).28 They also found that preoperative transfusiondependent anemia was the most significant risk factor for mortality (hazard ratio 3.47; 95% CI 2.38 to 5.04; p < .0001). The need for preoperative platelet transfusion also predicted worse postoperative
Table 3 Comparison of Laparoscopic versus Open Postsplenectomy OutcomesOutcome Laparoscopic Open
Operative time, min (range) 119 (90–157) 103 (75–142)
Length of stay, days (median) 3 (2–5) 6 (4–10)
Serious morbidity (%) 7–10.6 7.1–17
Overall morbidity (%) 12–15.5 24–26.6
Reoperation (%) 1.1–3.4 6.1–6.5
Death (%) 0.3–3.8 3.3–4.1

Scientific American Surgery
10/14
gastro splenectomy — 7
survival (hazard ratio 2.19; 95% CI 1.35 to 3.57; p = .0015).28 Although open splenectomy has historically been the preferred approach for splenomegaly and hypersplenism,28,75 the minimally invasive approach has pushed the limits in this setting. A recent ACS NSQIP study of 639 patients with splenomegaly and/or hypersplenism, as well as other case series, demonstrated the advantages of laparoscopy for both normalsized and large spleens, even though larger spleens were associated with longer operative times and lengths of stay compared with normalsized spleens. When looking specifically at large spleens, open splenectomy was associated with more transfusion requirements, longer length of stay, and higher morbidity compared with those with laparoscopic splenectomy.75 Grahn and colleagues also showed that the laparoscopic approach is safe, shortens length of stay, and improves mortality.83 Wu and colleagues also showed that, despite previous thoughts that massive splenomegaly increased the likelihood of conversion to open splenectomy,83 conversion rates are currently reasonably low as skills have improved and as long as the surgeon realizes that there is a learning curve and accepts longer operative times.84
Our group showed in a series of 142 patients that, on average, laparoscopic removal of an enlarged spleen required an additional 45 minutes of operating room time compared with spleens of normal size.33 With supermassive splenomegaly, the handassisted approach markedly reduced operative time, with no difference in length of stay or convalescence compared with purely laparoscopic management.25 Although mean operative time and estimated blood loss are lower for patients with normalsized spleens, there were no differences in conversion rates, length of stay, or complications between the two groups.32,33 Moreover, compared with standard laparoscopic splenectomy, handassisted laparoscopic splenectomy (HALS) allows comparable estimates of blood loss and length of stay but decrease s operative time even with supermassive spleens.25,33
Despite the above data, many still advocate the open approach in the setting of trauma, splenomegaly, and hypersplenism and with iatrogenic injuries.13,75 Even with the expanding use of laparoscopic splenectomy, a recent ACS NSQIP study demonstrated that the rate of laparoscopic splenectomy was only 41.8% (annual range 20 to 47%) for splenomegaly and hypersplenism compared with 84.2% for normalsized spleens.75 Thus, open splenectomy remains within the armamentarium of many practicing surgeons.
Even though immunization has nearly eliminated postsplenectomy sepsis, concerns regarding it have encouraged the practice of preserving splenic tissue and function. For this reason, partial splenectomy is occasionally used for the treatment of benign tumors of the spleen and for excision of cystic lesions.83 The indications and contraindications for partial splenectomy are listed here [see Table 4].33,84 Partial splenectomy has also been an option in the management of splenic trauma when the patient’s condition is stable enough to permit the meticulous dissection required for the operation.25,32
imaging
One of the key steps to preoperative planning and approach, along with the history and physical examination,
Table 4 Indications and Contraindications for Partial Splenectomy
IndicationsSelected grade II–IV splenic injuries with the following:
Hemodynamic stabilityNo evidence of other intraabdominal organ injuryNo associated head injuryNo coagulopathyCT confirmation of isolated splenic injury
Selective elective indicationsResection of nonparasitic cystsHamartomas and other benign splenic tumorsInflammatory pseudotumor of the spleenType I Gaucher diseaseCholesteryl ester storage diseaseChronic myelogenous leukemiaThalassemia majorSpherocytosisStaging of Hodgkin disease in children
Absolute/relative contraindications in traumaInadequate exposureInability to mobilize spleen and tail of pancreas to midlineInability to leave > 25% of splenic mass for complete splenic
function
CT = computed tomography
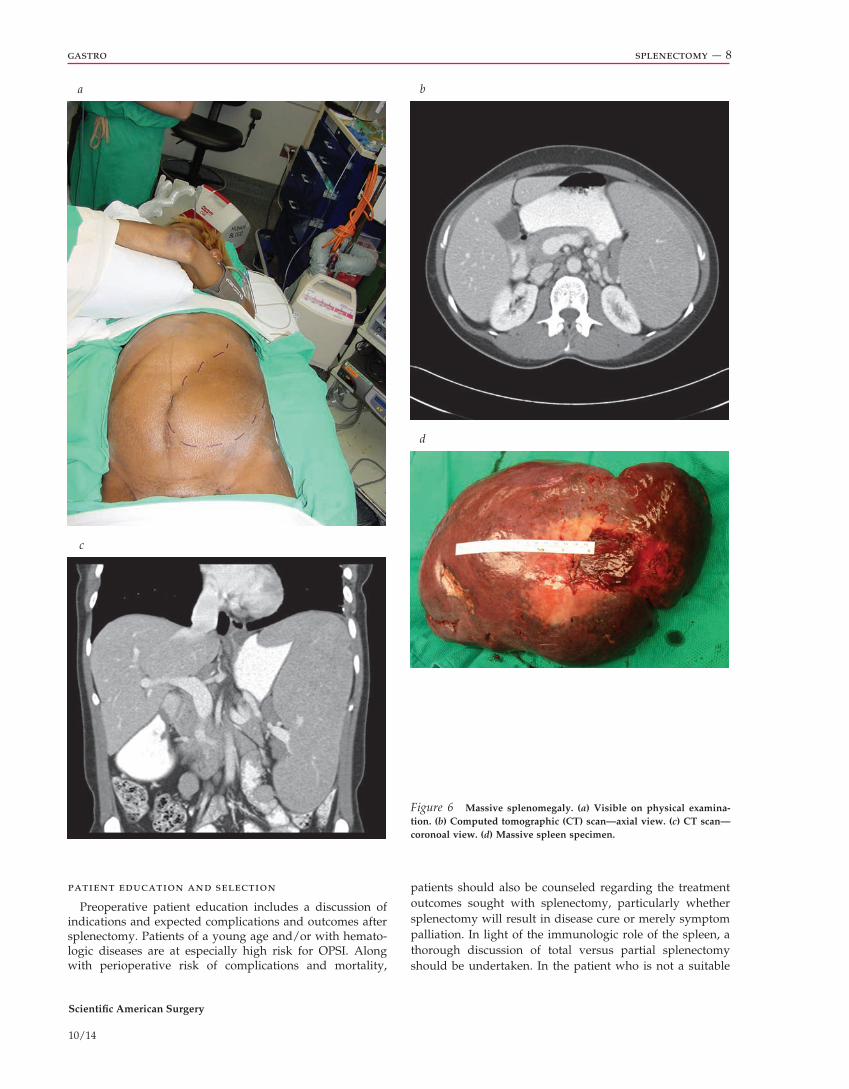
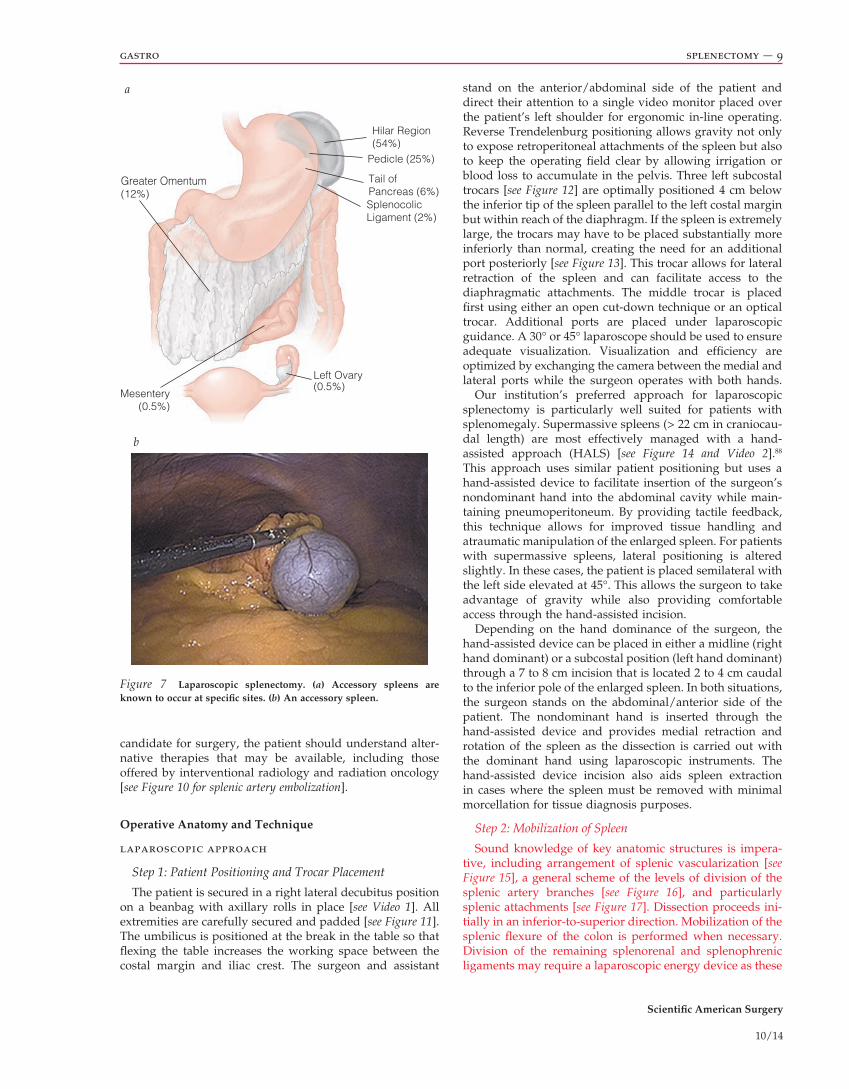
is review of imaging studies, most frequently CT or ultrasonography [see Figure 6]. Preoperative imaging will aid in the identification and characterization of critical anatomy, particularly the size and volume of the spleen; vascularity; splenic abscesses, cysts, or tumors; and accessory splenic tissue. Even with preoperative imaging, it is important to explore the abdomen for accessory spleens at the time of splenectomy as the sensitivity and specificity of CT for detecting accessory spleens are 60% and 95.6%, respectively; laparoscopic detection is 93.3% and 100%, respectively.12 We believe that the most thorough way to locate accessory spleens is through a combination of focused review of preoperative imaging (CT scan) and a careful intraoperative search for accessory splenic tissue. The most common locations of accessory spleens are shown here [see Figure 7].
preoperative vaccination
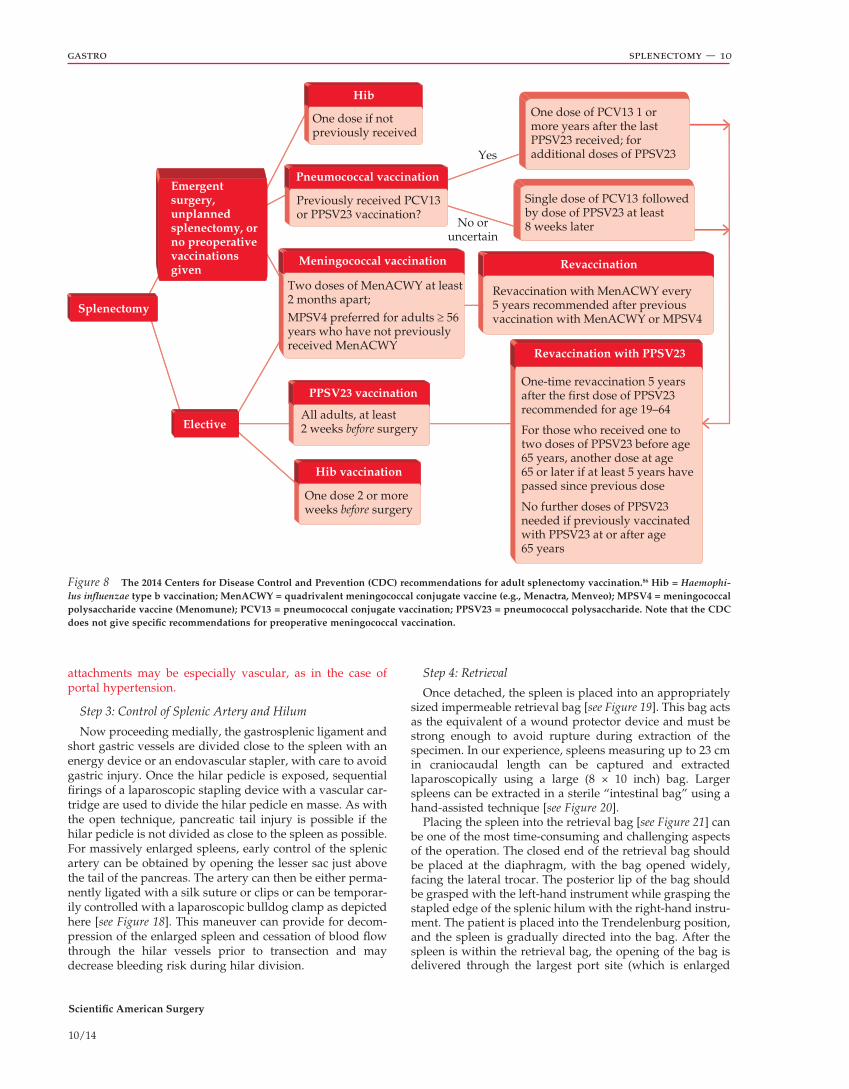
Once the decision to pursue splenectomy has been made, preoperative preparation requires preimmunization to cover encapsulated organisms (i.e., Streptococcus pneumoniae, Haemophilus influenzae type B, Neisseria meningitidis) 2 to 6 weeks prior to surgery.85 When vaccines cannot be administered before surgery, such as in the case of emergent splenectomy for trauma, they should be given within 2 weeks after surgery. The 2014 Centers for Disease Control and Prevention (CDC) recommendations for splenectomy vaccinations are provided here [see Figure 8 and Figure 9].86 However, the timing of postsplenectomy vaccination is a subject of some controversy. In one study of trauma patients, better functional antibody responses were seen with delayed (14day) vaccination as opposed to administration at 24 hours or even at 7 days.87 Still, many surgeons will immunize within 24 hours after trauma splenectomy to avoid losing the patient to followup.
Scientific American Surgery
10/14
gastro splenectomy — 8
a b
c
d
Figure 6 Massive splenomegaly. (a) Visible on physical examina-tion. (b) Computed tomographic (CT) scan—axial view. (c) CT scan—coronoal view. (d) Massive spleen specimen.
patients should also be counseled regarding the treatment outcomes sought with splenectomy, particularly whether splenectomy will result in disease cure or merely symptom palliation. In light of the immunologic role of the spleen, a thorough discussion of total versus partial splenectomy should be undertaken. In the patient who is not a suitable
patient education and selection
Preoperative patient education includes a discussion of indications and expected complications and outcomes after splenectomy. Patients of a young age and/or with hematologic diseases are at especially high risk for OPSI. Along with perioperative risk of complications and mortality,
Scientific American Surgery
10/14
gastro splenectomy — 9
a
Greater Omentum(12%)
Mesentery(0.5%)
Left Ovary(0.5%)
Hilar Region (54%)
Pedicle (25%)
Tail of Pancreas (6%)SplenocolicLigament (2%)
b
Figure 7 Laparoscopic splenectomy. (a) Accessory spleens are known to occur at specific sites. (b) An accessory spleen.
candidate for surgery, the patient should understand alternative therapies that may be available, including those offered by interventional radiology and radiation oncology [see Figure 10 for splenic artery embolization].
Operative Anatomy and Technique
laparoscopic approach
Step 1: Patient Positioning and Trocar Placement
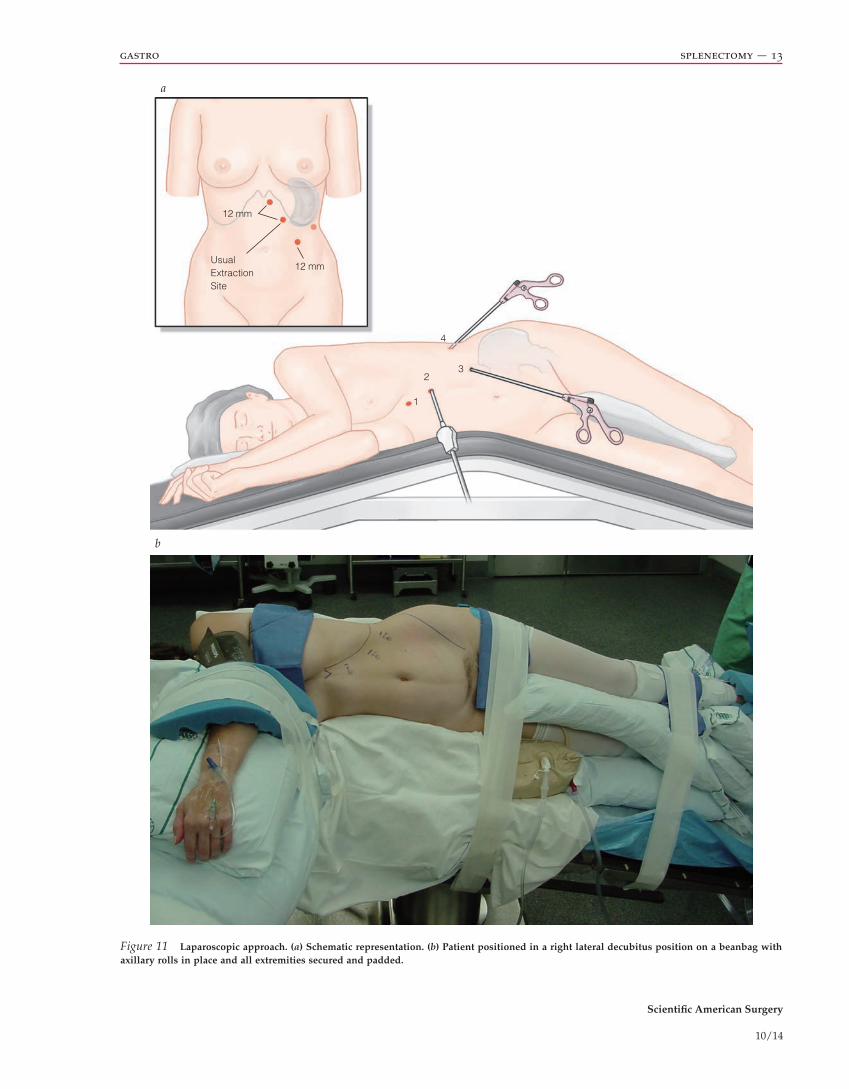
The patient is secured in a right lateral decubitus position on a beanbag with axillary rolls in place [see Video 1]. All extremities are carefully secured and padded [see Figure 11]. The umbilicus is positioned at the break in the table so that flexing the table increases the working space between the costal margin and iliac crest. The surgeon and assistant
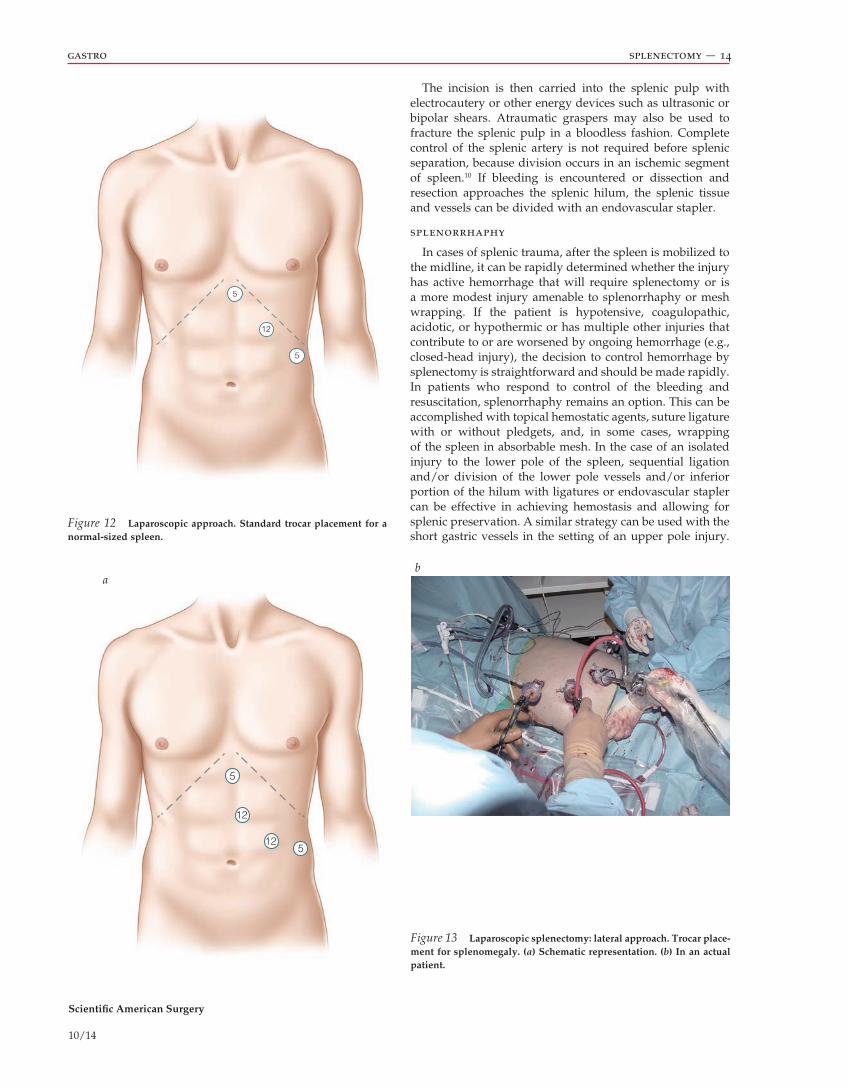
stand on the anterior/abdominal side of the patient and direct their attention to a single video monitor placed over the patient’s left shoulder for ergonomic inline operating. Reverse Trendelenburg positioning allows gravity not only to expose retroperitoneal attachments of the spleen but also to keep the operating field clear by allowing irrigation or blood loss to accumulate in the pelvis. Three left subcostal trocars [see Figure 12] are optimally positioned 4 cm below the inferior tip of the spleen parallel to the left costal margin but within reach of the diaphragm. If the spleen is extremel y large, the trocars may have to be placed substantially more inferiorly than normal, creating the need for an additional port posteriorly [see Figure 13]. This trocar allows for lateral retraction of the spleen and can facilitate access to the diaphragmatic attachments. The middle trocar is placed first using either an open cutdown technique or an optical trocar. Additional ports are placed under laparoscopic guidance. A 30° or 45° laparoscope should be used to ensure adequate visualization. Visualization and efficiency are optimized by exchanging the camera between the medial and lateral ports while the surgeon operates with both hands.
Our institution’s preferred approach for laparoscopic splenectomy is particularly well suited for patients with splenomegaly. Supermassive spleens (> 22 cm in craniocaudal length) are most effectively managed with a hand assisted approach (HALS) [see Figure 14 and Video 2].88 This approach uses similar patient positioning but uses a handassisted device to facilitate insertion of the surgeon’s nondominant hand into the abdominal cavity while maintaining pneumoperitoneum. By providing tactile feedback, this technique allows for improved tissue handling and atraumatic manipulation of the enlarged spleen. For patients with supermassive spleens, lateral positioning is altered slightly. In these cases, the patient is placed semilateral with the left side elevated at 45°. This allows the surgeon to take advantage of gravity while also providing comfortable access through the handassisted incision.
Depending on the hand dominance of the surgeon, the handassisted device can be placed in either a midline (right hand dominant) or a subcostal position (left hand dominant) through a 7 to 8 cm incision that is located 2 to 4 cm caudal to the inferior pole of the enlarged spleen. In both situations, the surgeon stands on the abdominal/anterior side of the patient. The nondominant hand is inserted through the handassisted device and provides medial retraction and rotation of the spleen as the dissection is carried out with the dominant hand using laparoscopic instruments. The handassisted device incision also aids spleen extraction in cases where the spleen must be removed with minimal morcellation for tissue diagnosis purposes.
Step 2: Mobilization of Spleen
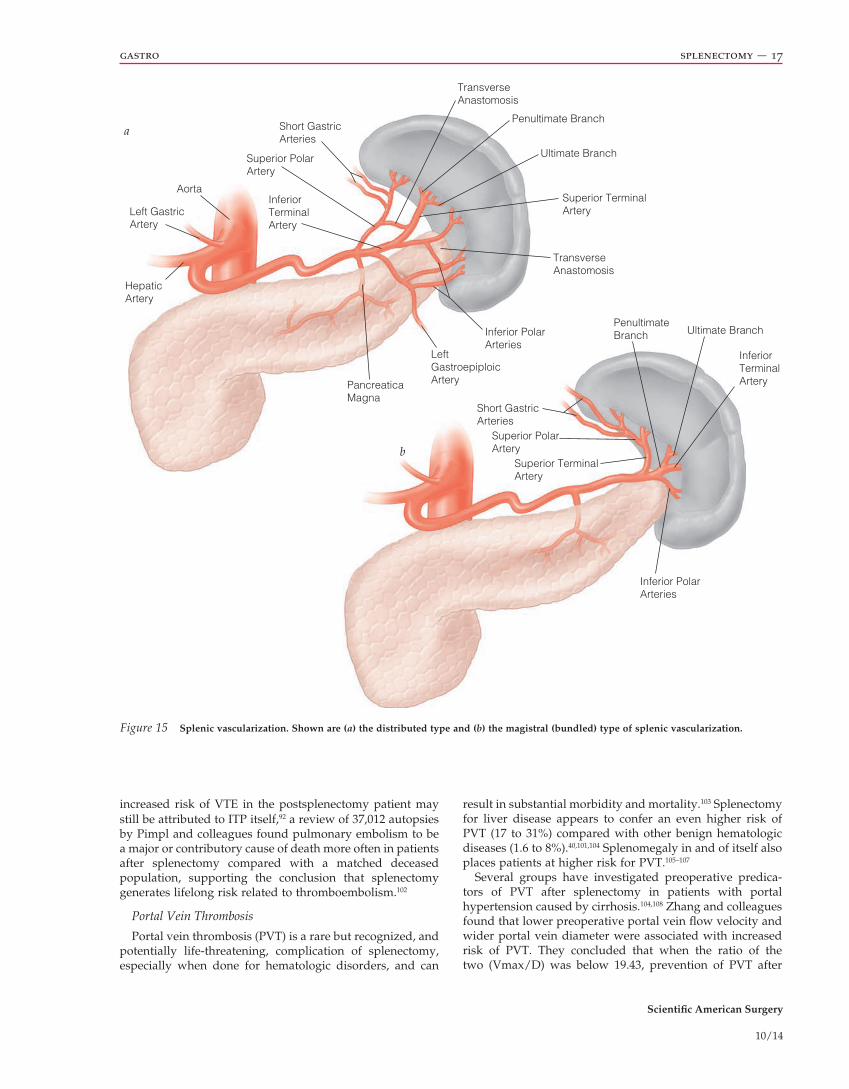
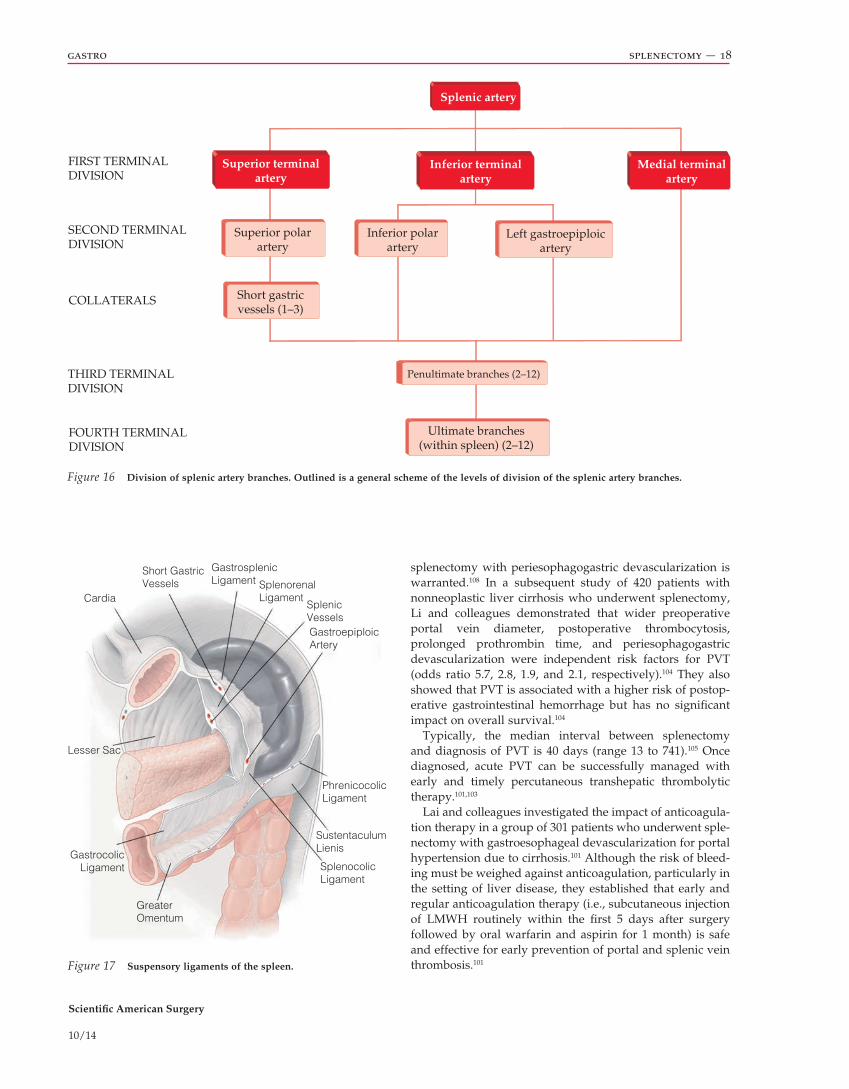
Sound knowledge of key anatomic structures is imperative, including arrangement of splenic vascularization [see Figure 15], a general scheme of the levels of division of the splenic artery branches [see Figure 16], and particularly splenic attachments [see Figure 17]. Dissection proceeds initially in an inferiortosuperior direction. Mobilization of the splenic flexure of the colon is performed when necessary. Division of the remaining splenorenal and splenophrenic ligaments may require a laparoscopic energy device as these
Scientific American Surgery
10/14
gastro splenectomy — 10
Figure 8 The 2014 Centers for Disease Control and Prevention (CDC) recommendations for adult splenectomy vaccination.86 Hib = Haemophi-lus influenzae type b vaccination; MenACWY = quadrivalent meningococcal conjugate vaccine (e.g., Menactra, Menveo); MPSV4 = meningococcal polysaccharide vaccine (Menomune); PCV13 = pneumococcal conjugate vaccination; PPSV23 = pneumococcal polysaccharide. Note that the CDC does not give specific recommendations for preoperative meningococcal vaccination.
Step 4: Retrieval
Once detached, the spleen is placed into an appropriately sized impermeable retrieval bag [see Figure 19]. This bag acts as the equivalent of a wound protector device and must be strong enough to avoid rupture during extraction of the specimen. In our experience, spleens measuring up to 23 cm in craniocaudal length can be captured and extracted laparoscopically using a large (8 × 10 inch) bag. Larger spleens can be extracted in a sterile “intestinal bag” using a handassisted technique [see Figure 20].
Placing the spleen into the retrieval bag [see Figure 21] can be one of the most timeconsuming and challenging aspects of the operation. The closed end of the retrieval bag should be placed at the diaphragm, with the bag opened widely, facing the lateral trocar. The posterior lip of the bag should be grasped with the lefthand instrument while grasping the stapled edge of the splenic hilum with the righthand instrument. The patient is placed into the Trendelenburg position, and the spleen is gradually directed into the bag. After the spleen is within the retrieval bag, the opening of the bag is delivered through the largest port site (which is enlarged
attachments may be especially vascular, as in the case of portal hypertension.
Step 3: Control of Splenic Artery and Hilum
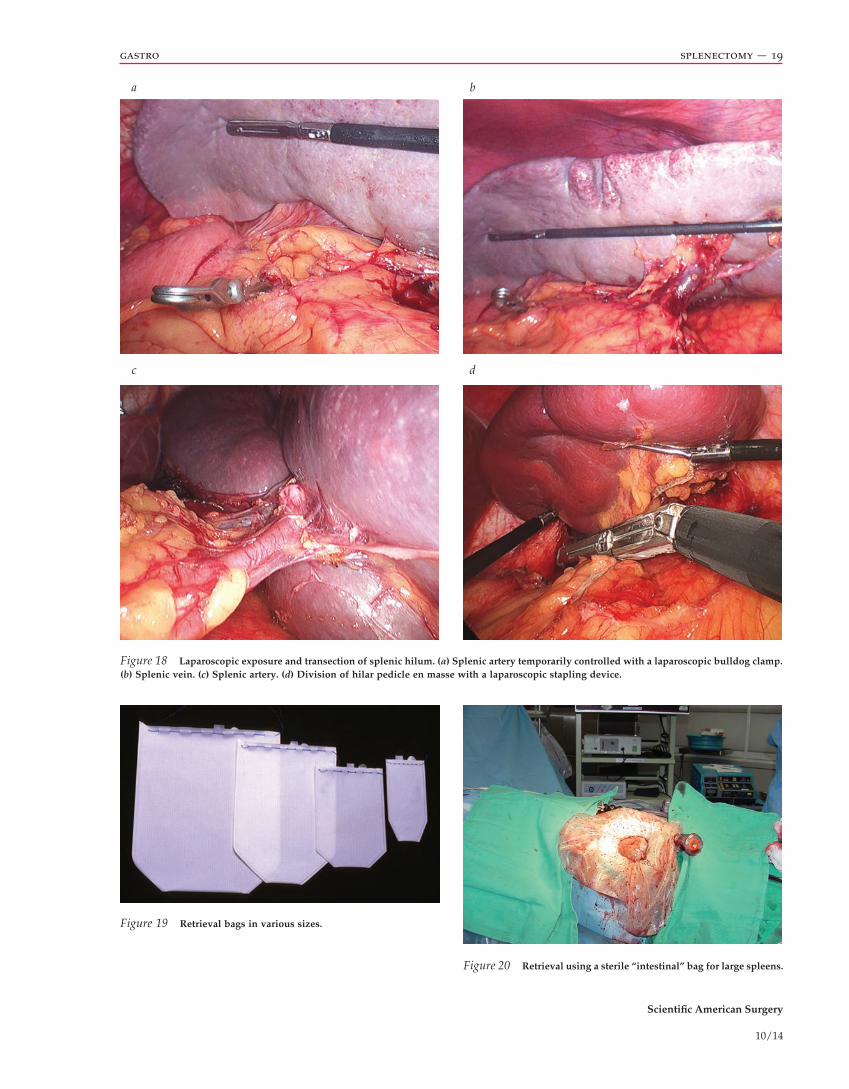
Now proceeding medially, the gastrosplenic ligament and short gastric vessels are divided close to the spleen with an energy device or an endovascular stapler, with care to avoid gastric injury. Once the hilar pedicle is exposed, sequential firings of a laparoscopic stapling device with a vascular cartridge are used to divide the hilar pedicle en masse. As with the open technique, pancreatic tail injury is possible if the hilar pedicle is not divided as close to the spleen as possible. For massively enlarged spleens, early control of the splenic artery can be obtained by opening the lesser sac just above the tail of the pancreas. The artery can then be either permanently ligated with a silk suture or clips or can be temporarily controlled with a laparoscopic bulldog clamp as depicted here [see Figure 18]. This maneuver can provide for decompression of the enlarged spleen and cessation of blood flow through the hilar vessels prior to transection and may decrease bleeding risk during hilar division.
Yes
No oruncertain
One dose if notpreviously received
Hib
Pneumococcal vaccination
Previously received PCV13 or PPSV23 vaccination?
Meningococcal vaccination
Two doses of MenACWY at least 2 months apart;MPSV4 preferred for adults ≥ 56years who have not previouslyreceived MenACWY
All adults, at least 2 weeks before surgery
PPSV23 vaccination
Hib vaccination
One dose 2 or moreweeks before surgery
Revaccination with PPSV23
One-time revaccination 5 yearsafter the first dose of PPSV23recommended for age 19–64
For those who received one to two doses of PPSV23 before age 65 years, another dose at age 65 or later if at least 5 years havepassed since previous dose
No further doses of PPSV23needed if previously vaccinatedwith PPSV23 at or after age65 years
Revaccination
Revaccination with MenACWY every 5 years recommended after previousvaccination with MenACWY or MPSV4
One dose of PCV13 1 or more years after the last PPSV23 received; for additional doses of PPSV23
Single dose of PCV13 followed by dose of PPSV23 at least 8 weeks later
Emergentsurgery,unplannedsplenectomy, orno preoperativevaccinationsgiven
Splenectomy
Elective

Scientific American Surgery
10/14
gastro splenectomy — 11
Figure 9 The 2014 Centers for Disease Control and Prevention recommendations for pediatric splenectomy vaccination.86
when necessary) or the handassisted incision. Depending on tissue diagnostic needs, the spleen may then be removed intact, manually avulsed into retrievable portions, or morcellated with ring forceps.25
open approach
Step 1: Incision
In the supine position, a left subcostal incision may suffice for small to normalsized spleens, such as in ITP. A generous midline incision may be necessary in cases of splenomegaly or depending on the patient’s body habitus [see Figure 22]. The left costal margin must be retracted cephalad and laterally either by an assistant or a selfretaining retractor. Verify gastric decompression before proceeding.
Step 2: Early Ligation of the Splenic Artery
With hypersplenism and splenomegaly, preliminary control of the splenic artery in the lesser sac is possible. In a patient undergoing splenectomy for ITP, plans should be made for platelet transfusion after splenic artery ligation. The splenic artery can be ligated near the tail of the pancreas by incising the gastrocolic and gastrosplenic ligaments lateral to the gastroepiploic arcade. Ligating the lower short gastric vessels may also aid visualization, although care must be taken to avoid incorporating the gastric wall during this maneuver as it may increase the risk of postoperative gastric fistula. Imbricating the greater curvature over the ligated short gastric vessels is a reasonable maneuver if gastric injury is in question.89
Minimum age for vaccines:• Pneumococcal vaccines–6 weeks for PCV13; 2 years for PPSV23
• Haemophilus influenzae type b (Hib) conjugate vaccines–6 weeks for PRP-T [ACTHIB, DTaP-IPV/Hib(pentacel)] & Hib-MenCY [Menhibrix], PRP-CMP (PedyaxHIB or COMVAX); 12 months for PRP-T [Hiberix]
• Meningococcal conjugate vaccines–6 weeks for HibMenCY[MenHibrix], 9 months for MenACWY-D [Menactra], 2 months for MenACWY-CRM [Menveo]
Hib vaccine
Age < 15 months: routine schedule
Age ≥ 15 months: a single dose 2 or more weeks before surgery
Pneumococcal vaccine
Previously received PCV13 or PPSV23 vaccination?
Meningococcal vaccine
Age < 19 months: a four-dose infant series of MenHibrix or Menveo at 2, 4, 6, and 12–15 months Age 19–23 months: if not completed a series of MenHibrix or Menveo, administer two primary doses of Menveo at least 3 months apartAge ≥ 24 months: if not completed series of MenHibrix or Menveo or Menactra, administer two primary doses of either Menactra or Menveo
Pneumococcal vaccine
As above
Yes
No oruncertain
Pneumococcal vaccine
Age < 24 months: routine vaccination with PCV13Age 24–71 months: (1) one dose of PCV13 if three doses of PCV previously, (2) two doses of PCV13 at least 8 weeks apart if < three doses of PCV previously, (3) one supplemental dose of PCV13 if four doses of PCV7 or other age-appropriated PCV7 series completed previously; Age 6–18 years: If no history of PPSV23but has received PCV13, administerPPSV23 at least 8 weeks after the mostrecent dose of PCV13; if PPSV23received but not PCV13, then one doseof PCV13 at least 8 weeks after mostrecent dose of PPSV23
Age 2–5 years: one dose of PCV13 followed by one dose PPSV23 at least 8 weeks later
Revaccination with PPSV23
Age 6–18 years: one-timerevaccination 5 years after thefirst dose of PPSV23recommended
Age < 12 months: routine schedule
Age 12–59 months: if no doses or only one dose before 12 months of age, administer two additional doses 8 weeks apart; if two or more doses before 12 months received, administer one additional dose;
Age ≥ 5 years: one dose of Hib vaccine
Hib Vaccine
Splenectomy
Elective
Emergentsurgery,unplannedsplenectomy, orno preoperativevaccinationsgiven

Scientific American Surgery
10/14
gastro splenectomy — 12
Figure 10 Splenic artery embolization. Shown are splenic angio-grams of a patient with thrombotic thrombocytopenic purpura before (left) and after (right) splenic artery embolization.
Video 1 Purely laparoscopic splenectomy.
pancreas. Meticulous dissection must be undertaken here to avoid ligating portions of the tail of the pancreas and producing a subsequent pancreatic fistula. The splenic artery, vein, and other branching vasculature can then be ligated and divided safely at the hilum to allow for removal of the spleen [see Figure 24]. Although clamps, ties, and/or suture ligatures are appropriate for open splenectomy, the use of endovascular linear gastrointestinal anastomosis (GIA) staplers (as used in laparoscopic splenectomy) can provide for rapid and reliable hilar division even in the open setting [see Figure 25]. These devices are particularly useful in obese patients and with splenomegaly, when exposure of the hilum can be challenging.
partial splenectomy
Patient positioning and instrument placement are similar to the surgeon’s preferred open or laparoscopic technique. The targeted superior or inferior pole is mobilized as described previously. Branches of the short gastric and branching hilar vessels supplying the desired pole are dissected and ligated close to the parenchyma. An appropriate number of penultimate branches of the short gastric and branching hilar vessels are taken in such a way as to create a clear line of demarcation between normal spleen and devascularized spleen. This process is continued until the desired number of splenic segments is devascularized.
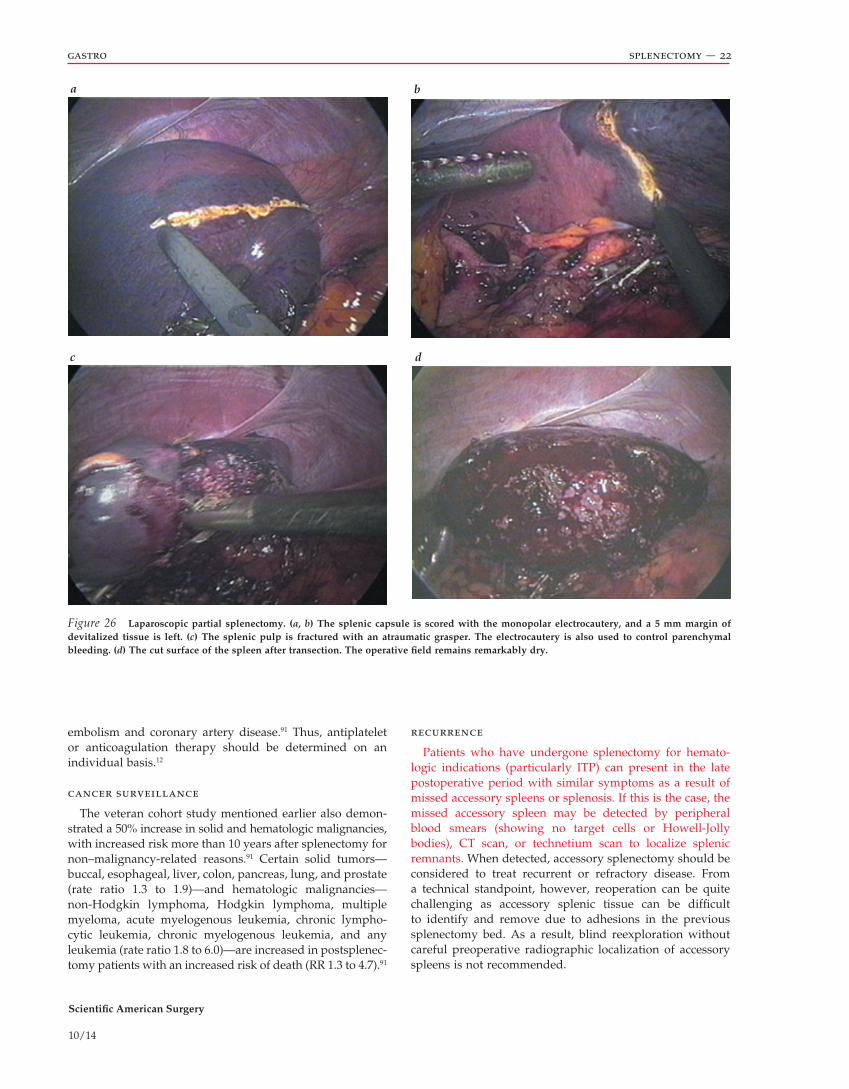
Next, a standard monopolar electrocautery is used to score the splenic capsule circumferentially, with care taken to ensure that a 5 to 10 mm rim of devascularized splenic tissue remains in situ [see Figure 26]. This is the most important technical point for this procedure as bleeding from vascularized splenic tissue is the primary risk of partial splenectomy. Once the spleen has been allowed to demarcate, resection is remarkably bloodless, provided that an adequate rim of ischemic tissue is left in place. The feasibility of leaving portions of ischemic spleen in situ has been demonstrated in a large prospective, randomized trial involving partial splenic embolization as primary treatment of hematologic disorders.34
Step 3: Mobilization of the Spleen
With the spleen retracted medially [see Figure 23] by the surgeon’s left hand, divide the splenocolic, splenorenal, and splenophrenic ligaments without injury to adjacent structures. Allow the spleen to be retracted anteriorly and medially into midline incision by dissecting in a retropancreatic/prenephric plane. At this point, the spleen can be freely mobilized along with the tail of the pancreas into the midline. Active bleeding can be controlled with manual compression of the splenic hilum or careful application of vascular clamps to the hilum. If clamps are used, it is important to exercise care to avoid injury to the tail of the pancreas. Laparotomy pads may be packed behind the spleen to tamponade bleeding and support the spleen.
Step 4: Ligation of the Splenic Hilum
With the spleen and tail of the pancreas elevated, carefully dissect the splenic artery and vein from the tail of the
Scientific American Surgery
10/14
gastro splenectomy — 13
12 mm
12 mm
1
23
4
UsualExtractionSite
a
b
Figure 11 Laparoscopic approach. (a) Schematic representation. (b) Patient positioned in a right lateral decubitus position on a beanbag with axillary rolls in place and all extremities secured and padded.
Scientific American Surgery
10/14
gastro splenectomy — 14
5
5
12
5
5
12
12
ab
Figure 12 Laparoscopic approach. Standard trocar placement for a normal-sized spleen.
Figure 13 Laparoscopic splenectomy: lateral approach. Trocar place-ment for splenomegaly. (a) Schematic representation. (b) In an actual patient.
The incision is then carried into the splenic pulp with electrocautery or other energy devices such as ultrasonic or bipolar shears. Atraumatic graspers may also be used to fracture the splenic pulp in a bloodless fashion. Complete control of the splenic artery is not required before splenic separation, because division occurs in an ischemic segment of spleen.10 If bleeding is encountered or dissection and resection approaches the splenic hilum, the splenic tissue and vessels can be divided with an endovascular stapler.
splenorrhaphy
In cases of splenic trauma, after the spleen is mobilized to the midline, it can be rapidly determined whether the injury has active hemorrhage that will require splenectomy or is a more modest injury amenable to splenorrhaphy or mesh wrapping. If the patient is hypotensive, coagulopathic, acidotic, or hypothermic or has multiple other injuries that contribute to or are worsened by ongoing hemorrhage (e.g., closedhead injury), the decision to control hemorrhage by splenectomy is straightforward and should be made rapidly. In patients who respond to control of the bleeding and resuscitation, splenorrhaphy remains an option. This can be accomplished with topical hemostatic agents, suture ligature with or without pledgets, and, in some cases, wrapping of the spleen in absorbable mesh. In the case of an isolated injury to the lower pole of the spleen, sequential ligation and/or division of the lower pole vessels and/or inferior portion of the hilum with ligatures or endovascular stapler can be effective in achieving hemostasis and allowing for splenic preservation. A similar strategy can be used with the short gastric vessels in the setting of an upper pole injury.

Scientific American Surgery
10/14
gastro splenectomy — 15
a b
d
Figure 14 Hand-assisted laparoscopic splenectomy. (a) A hand port with trocar inserted to allow insufflation. (b) A large spleen is visible through the hand port. (c) Use of a hand port to facilitate laparoscopic splenectomy in a patient with a large spleen. (d) Hand port in the left lower quadrant.
The splenic fossa should be carefully examined for hemorrhage and possible injury to the stomach or pancreas before closing. If there is evidence of or reasonable concern for possible injury to the pancreas, a closedsuction drain should be left in the splenic bed.
Postoperative Complications and Their Management
Both operative approach and indications for splenectomy have evolved over the past two decades. Overall morbidity and mortality after splenectomy remain low; common complications include pancreatitis, postoperative hemorrhage, and atelectasis, although the most cited major complications are infectious and thrombotic complications.12 The incidences of common complications related to splenectomy, as
reported in the literature, are presented here [see Table 5].76,77,79,80,90 Of note, in a series of 94 laparoscopic splenectomies at the Cleveland Clinic, the most common morbidity associated with laparoscopic splenectomy was pancreatic injury (16%).78 In this series, six patients had pancreatic fluid collections and one a pancreatic fistula.78 In our experience, pancreatic complications are exceedingly rare, although the potential for pancreatic injury underscores the need to carefully identify and avoid the pancreatic tail when dividing the splenic hilum. In some cases, this requires meticulous dissection of the pancreatic tail away from the hilar vessels and splenic capsule. Gastric fistulas are also a rare but serious occurrence, with only a handful of case reports published.89
c

Scientific American Surgery
10/14
gastro splenectomy — 16
Video 2 Hand-assisted laparoscopic splenectomy (HALS).
overwhelming postsplenectomy infection
In general, postsplenectomy patients are at increased risk for being hospitalized for pneumonia, meningitis, and septicemia (rate ratios 1.9 to 3.4).91 Mortality from pneumonia and septicemia is also increased (rate ratio 1.6 to 3.0).92 OPSI is a rare (occurring in up to 0.5% of patients) but serious condition associated with mortality as high as 50 to 80%.12,93 An Italian study found that patients without a spleen or with diminished splenic function are at 10 to 15 times higher risk than the normal population of developing lifethreatening infections (OPSI),93 and rapid progression to fulminant infection and death can occur within 48 hours.85 It most often occurs in the first 2 years after splenectomy, but rare instances of OPSI in the immediate postsplenectomy period and up to 47 years after operation have been described.94 In general, the incidence of severe infection after splenectomy is highest among children and those with malignancy and lowest among trauma patients.18 It is important to treat OPSI empirically with antibiotics before culture data are available. With reported mortality as high as 70% in children with OPSI compared with adult counterparts, postoperative immunization directed at encapsulated organisms, if not administered preoperatively, is crucial to avoiding these dire statistics and can reduce mortality to 10 to 40%.18 For these reasons, partial splenectomy should also be considered in children when feasible.
reactive thrombocytosis and vascular events
Thrombocytosis
Splenectomy alone accounts for 19% of all possible causes of extreme thrombocytosis, and secondary (reactive) thrombocytosis after splenectomy is predictable, with a cited incidence of 75 to 82%.95–97 Platelet counts usually peak at 1 to 3 weeks and return to normal within weeks, months, and,
rarely, years, without postoperative thrombosis.97,98 In most patients with secondary thrombocytosis, plateletlowering treatment is not required because their abnormal platelet count itself does not place them at risk for thromboembolic or vascular events.99
However, unlike the average trauma patient with postsplenectomy thrombocytosis, patients with underlying systemic diseases, which may contribute to elevated platelet counts, are more prone to thrombotic, vascular, and bleedin g complications. Venous thromboembolism (VTE) usually occur s with platelet counts greater than 600,000 to 800,000/µL, with an incidence of about 5%.97 In this group of patients at high risk for vascular events, prophylactic plateletlowering therapy and aspirin are indicated if bleeding does not pose a greater risk.99,100 Management of extreme thrombocytosis and its associated adverse effects include acetylsalicylic acid (ASA), anagrelide (a plateletlowering agent), interferon alfa, ticlopidine, lowmolecular weight heparin (LMWH), and plasmapharesis, but hydroxyurea has been the treatment of choice in many studies.95–97,101
Venous Thromboembolism
In one of the largest populationbased studies (N = 9,976) examining the effect of splenectomy on complications in ITP patients, Boyle and colleagues demonstrated an approximately fivefold increased risk of early abdominal venous thromboembolism (AbVTE) and VTE (deep vein thrombosis [DVT] and pulmonary embolism), with a threefold higher risk of late VTE, after splenectomy.92 The cumulative incidence of AbVTE after splenectomy in this population was reported as 1.6% postsplenectomy compared with 1% in those who did not undergo splenectomy; VTE after splenectomy was 4.3% versus 1.7%.92 Additionally, AbVTE was associated with increased odds ratio for death (OR 3.3; 95% CI 2.1 to 5.1).92 Although this group acknowledged that the
Scientific American Surgery
10/14
gastro splenectomy — 17
a
b
Aorta
Left GastricArtery
LeftGastroepiploicArtery
HepaticArtery
Inferior PolarArteries
Inferior PolarArteries
PancreaticaMagna
InferiorTerminalArtery
InferiorTerminalArtery
Superior PolarArtery
Superior PolarArtery
TransverseAnastomosis
TransverseAnastomosis
Short GastricArteries
Superior TerminalArtery
Superior TerminalArtery
Ultimate Branch
Ultimate Branch
Penultimate Branch
PenultimateBranch
Short GastricArteries
Figure 15 Splenic vascularization. Shown are (a) the distributed type and (b) the magistral (bundled) type of splenic vascularization.
increased risk of VTE in the postsplenectomy patient may still be attributed to ITP itself,92 a review of 37,012 autopsies by Pimpl and colleagues found pulmonary embolism to be a major or contributory cause of death more often in patients after splenectomy compared with a matched deceased population, supporting the conclusion that splenectomy generates lifelong risk related to thromboembolism.102
Portal Vein Thrombosis
Portal vein thrombosis (PVT) is a rare but recognized, and potentially lifethreatening, complication of splenectomy, especially when done for hematologic disorders, and can
result in substantial morbidity and mortality.103 Splenectomy for liver disease appears to confer an even higher risk of PVT (17 to 31%) compared with other benign hematologic diseases (1.6 to 8%).40,101,104 Splenomegaly in and of itself also places patients at higher risk for PVT.105–107
Several groups have investigated preoperative predicators of PVT after splenectomy in patients with portal hypertension caused by cirrhosis.104,108 Zhang and colleagues found that lower preoperative portal vein flow velocity and wider portal vein diameter were associated with increased risk of PVT. They concluded that when the ratio of the two (Vmax/D) was below 19.43, prevention of PVT after
Scientific American Surgery
10/14
gastro splenectomy — 18
FIRST TERMINALDIVISION
SECOND TERMINALDIVISION
COLLATERALS
THIRD TERMINALDIVISION
FOURTH TERMINALDIVISION
Short gastricvessels (1–3)
Superior polarartery
Inferior polarartery
Left gastroepiploicartery
Ultimate branches(within spleen) (2–12)
Penultimate branches (2–12)
Splenic artery
Superior terminalartery
Inferior terminalartery
Medial terminalartery
Cardia
Short GastricVessels
GastrosplenicLigament Splenorenal
LigamentSplenicVesselsGastroepiploicArtery
PhrenicocolicLigament
SustentaculumLienis
SplenocolicLigament
GreaterOmentum
GastrocolicLigament
Lesser Sac
Figure 16 Division of splenic artery branches. Outlined is a general scheme of the levels of division of the splenic artery branches.
Figure 17 Suspensory ligaments of the spleen.
splenectomy with periesophagogastric devascularization is warranted.108 In a subsequent study of 420 patients with nonneoplastic liver cirrhosis who underwent splenectomy, Li and colleagues demonstrated that wider preoperative portal vein diameter, postoperative thrombocytosis, pro longe d prothrombin time, and periesophagogastric devascularization were independent risk factors for PVT (odds ratio 5.7, 2.8, 1.9, and 2.1, respectively).104 They also showed that PVT is associated with a higher risk of postoperative gastrointestinal hemorrhage but has no significant impact on overall survival.104
Typically, the median interval between splenectomy and diagnosis of PVT is 40 days (range 13 to 741).105 Once diagnosed, acute PVT can be successfully managed with early and timely percutaneous transhepatic thrombolytic therapy.101,103
Lai and colleagues investigated the impact of anticoagulation therapy in a group of 301 patients who underwent splenectomy with gastroesophageal devascularization for portal hypertension due to cirrhosis.101 Although the risk of bleeding must be weighed against anticoagulation, particularly in the setting of liver disease, they established that early and regular anticoagulation therapy (i.e., subcutaneous injection of LMWH routinely within the first 5 days after surgery followed by oral warfarin and aspirin for 1 month) is safe and effective for early prevention of portal and splenic vein thrombosis.101
Scientific American Surgery
10/14
gastro splenectomy — 19
a b
c d
Figure 18 Laparoscopic exposure and transection of splenic hilum. (a) Splenic artery temporarily controlled with a laparoscopic bulldog clamp. (b) Splenic vein. (c) Splenic artery. (d) Division of hilar pedicle en masse with a laparoscopic stapling device.
Figure 19 Retrieval bags in various sizes.
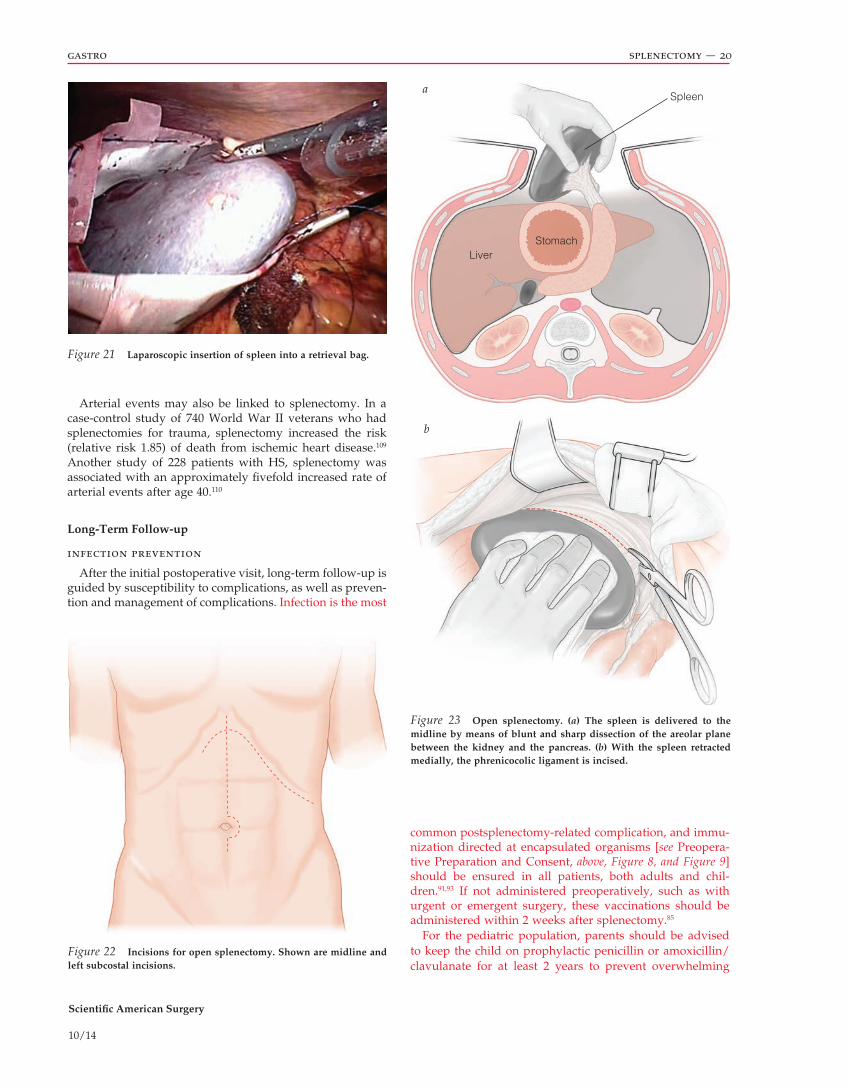
Figure 20 Retrieval using a sterile “intestinal” bag for large spleens.
Scientific American Surgery
10/14
gastro splenectomy — 20
StomachLiver
Spleena
b
Figure 21 Laparoscopic insertion of spleen into a retrieval bag.
Figure 22 Incisions for open splenectomy. Shown are midline and left subcostal incisions.
Figure 23 Open splenectomy. (a) The spleen is delivered to the midline by means of blunt and sharp dissection of the areolar plane between the kidney and the pancreas. (b) With the spleen retracted medially, the phrenicocolic ligament is incised.
Arterial events may also be linked to splenectomy. In a casecontrol study of 740 World War II veterans who had splenectomies for trauma, splenectomy increased the risk (relative risk 1.85) of death from ischemic heart disease.109 Another study of 228 patients with HS, splenectomy was associated with an approximately fivefold increased rate of arterial events after age 40.110
Long-Term Follow-up
infection prevention
After the initial postoperative visit, longterm followup is guided by susceptibility to complications, as well as prevention and management of complications. Infection is the most
common postsplenectomyrelated complication, and immunization directed at encapsulated organisms [see Preoperative Preparation and Consent, above, Figure 8, and Figure 9] should be ensured in all patients, both adults and children.91,93 If not administered preoperatively, such as with urgent or emergent surgery, these vaccinations should be administered within 2 weeks after splenectomy.85
For the pediatric population, parents should be advised to keep the child on prophylactic penicillin or amoxicillin/clavulanate for at least 2 years to prevent overwhelming
Scientific American Surgery
10/14
gastro splenectomy — 21
a
b
c
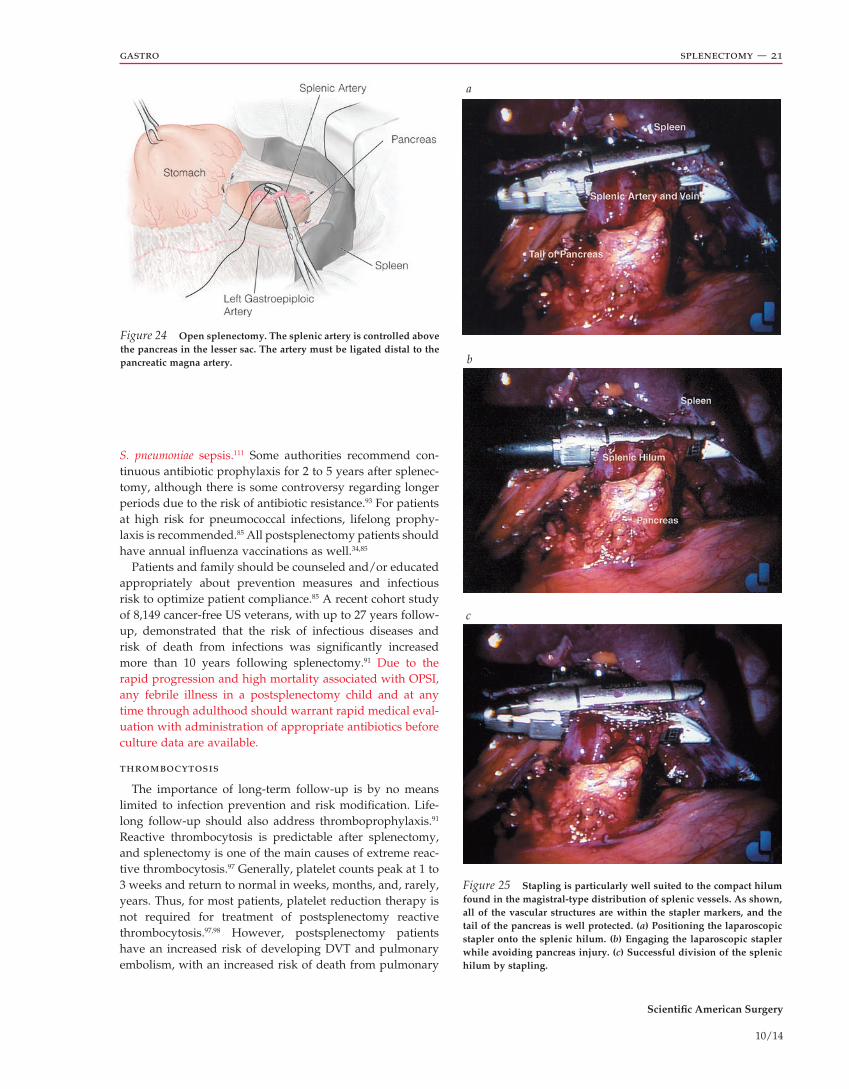
Figure 24 Open splenectomy. The splenic artery is controlled above the pancreas in the lesser sac. The artery must be ligated distal to the pancreatic magna artery.
Figure 25 Stapling is particularly well suited to the compact hilum found in the magistral-type distribution of splenic vessels. As shown, all of the vascular structures are within the stapler markers, and the tail of the pancreas is well protected. (a) Positioning the laparoscopic stapler onto the splenic hilum. (b) Engaging the laparoscopic stapler while avoiding pancreas injury. (c) Successful division of the splenic hilum by stapling.
S. pneumoniae sepsis.111 Some authorities recommend continuous antibiotic prophylaxis for 2 to 5 years after splenectomy, although there is some controversy regarding longer periods due to the risk of antibiotic resistance.93 For patients at high risk for pneumococcal infections, lifelong prophylaxis is recommended.85 All postsplenectomy patients should have annual influenza vaccinations as well.34,85
Patients and family should be counseled and/or educated appropriately about prevention measures and infectious risk to optimize patient compliance.85 A recent cohort study of 8,149 cancerfree US veterans, with up to 27 years followup, demonstrated that the risk of infectious diseases and risk of death from infections was significantly increased more than 10 years following splenectomy.91 Due to the rapid progression and high mortality associated with OPSI, any febrile illness in a postsplenectomy child and at any time through adulthood should warrant rapid medical evaluation with administration of appropriate antibiotics before culture data are available.
thrombocytosis
The importance of longterm followup is by no means limited to infection prevention and risk modification. Lifelong followup should also address thromboprophylaxis.91 Reactive thrombocytosis is predictable after splenectomy, and splenectomy is one of the main causes of extreme reactive thrombocytosis.97 Generally, platelet counts peak at 1 to 3 weeks and return to normal in weeks, months, and, rarely, years. Thus, for most patients, platelet reduction therapy is not required for treatment of postsplenectomy reactive thrombocytosis.97,98 However, postsplenectomy patients have an increased risk of developing DVT and pulmonary embolism, with an increased risk of death from pulmonary
Scientific American Surgery
10/14
gastro splenectomy — 22
embolism and coronary artery disease.91 Thus, antiplatelet or anticoagulation therapy should be determined on an individual basis.12
cancer surveillance
The veteran cohort study mentioned earlier also demonstrated a 50% increase in solid and hematologic mali gnancies, with increased risk more than 10 years after splenectomy for non–malignancyrelated reasons.91 Certain solid tumors—buccal, esophageal, liver, colon, pancreas, lung, and prostate (rate ratio 1.3 to 1.9)—and hematologic malignancies— nonHodgkin lymphoma, Hodgkin lymphoma, multiple myeloma, acute myelogenous leukemia, chronic lymphocytic leukemia, chronic myelogenous leukemia, and any leukemia (rate ratio 1.8 to 6.0)—are increased in postsplenectomy patients with an increased risk of death (RR 1.3 to 4.7).91
recurrence
Patients who have undergone splenectomy for hematologic indications (particularly ITP) can present in the late postoperative period with similar symptoms as a result of missed accessory spleens or splenosis. If this is the case, the missed accessory spleen may be detected by peripheral blood smears (showing no target cells or HowellJolly bodies), CT scan, or technetium scan to localize splenic remnants. When detected, accessory splenectomy should be considered to treat recurrent or refractory disease. From a technical standpoint, however, reoperation can be quite challenging as accessory splenic tissue can be difficult to identify and remove due to adhesions in the previous splenectomy bed. As a result, blind reexploration without careful preoperative radiographic localization of accessory spleens is not recommended.
a b
c d
Figure 26 Laparoscopic partial splenectomy. (a, b) The splenic capsule is scored with the monopolar electrocautery, and a 5 mm margin of devitalized tissue is left. (c) The splenic pulp is fractured with an atraumatic grasper. The electrocautery is also used to control parenchymal bleeding. (d) The cut surface of the spleen after transection. The operative field remains remarkably dry.
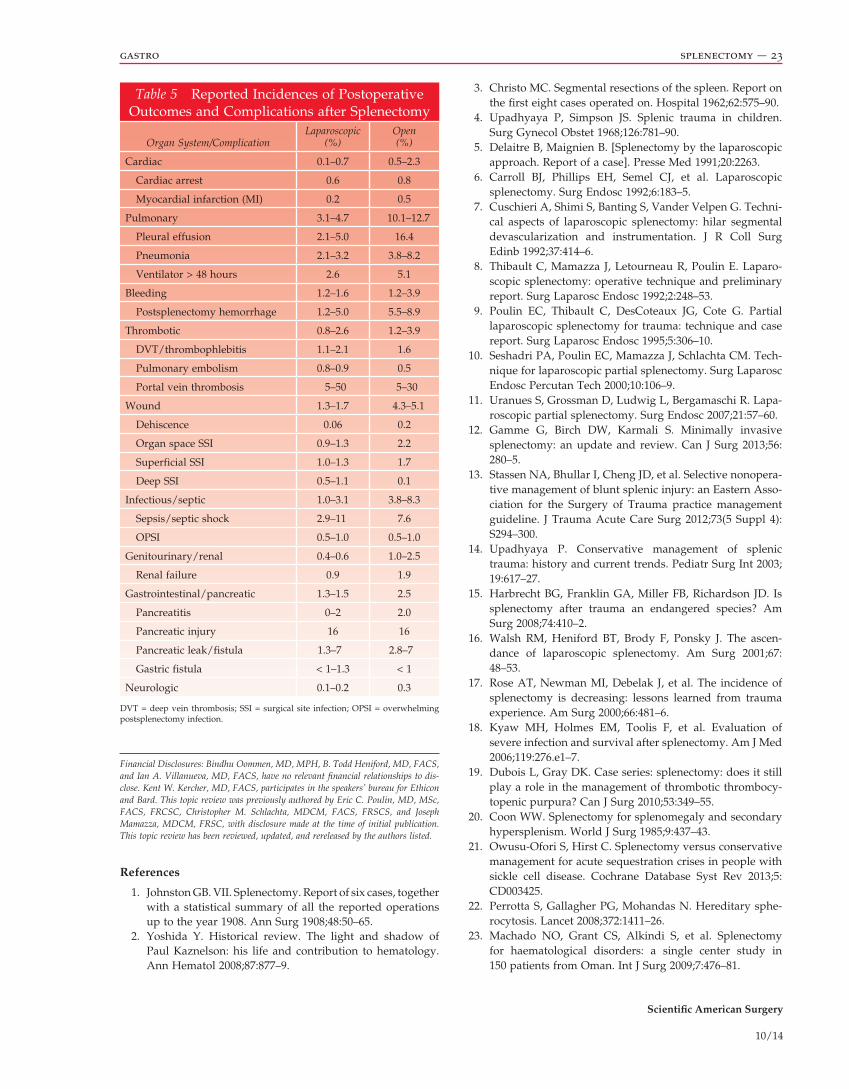
Scientific American Surgery
10/14
gastro splenectomy — 23
Financial Disclosures: Bindhu Oommen, MD, MPH, B. Todd Heniford, MD, FACS, and Ian A. Villanueva, MD, FACS, have no relevant financial relationships to dis-close. Kent W. Kercher, MD, FACS, participates in the speakers’ bureau for Ethicon and Bard. This topic review was previously authored by Eric C. Poulin, MD, MSc, FACS, FRCSC, Christopher M. Schlachta, MDCM, FACS, FRSCS, and Joseph Mamazza, MDCM, FRSC, with disclosure made at the time of initial publication. This topic review has been reviewed, updated, and rereleased by the authors listed.
References
1. Johnston GB. VII. Splenectomy. Report of six cases, together with a statistical summary of all the reported operations up to the year 1908. Ann Surg 1908;48:50–65.
2. Yoshida Y. Historical review. The light and shadow of Paul Kaznelson: his life and contribution to hematology. Ann Hematol 2008;87:877–9.
3. Christo MC. Segmental resections of the spleen. Report on the first eight cases operated on. Hospital 1962;62:575–90.
4. Upadhyaya P, Simpson JS. Splenic trauma in children. Surg Gynecol Obstet 1968;126:781–90.
5. Delaitre B, Maignien B. [Splenectomy by the laparoscopic approach. Report of a case]. Presse Med 1991;20:2263.
6. Carroll BJ, Phillips EH, Semel CJ, et al. Laparoscopic splenectomy. Surg Endosc 1992;6:183–5.
7. Cuschieri A, Shimi S, Banting S, Vander Velpen G. Technical aspects of laparoscopic splenectomy: hilar segmental devascularization and instrumentation. J R Coll Surg Edinb 1992;37:414–6.
8. Thibault C, Mamazza J, Letourneau R, Poulin E. Laparoscopic splenectomy: operative technique and preliminary report. Surg Laparosc Endosc 1992;2:248–53.
9. Poulin EC, Thibault C, DesCoteaux JG, Cote G. Partial laparoscopic splenectomy for trauma: technique and case report. Surg Laparosc Endosc 1995;5:306–10.
10. Seshadri PA, Poulin EC, Mamazza J, Schlachta CM. Technique for laparoscopic partial splenectomy. Surg Laparosc Endosc Percutan Tech 2000;10:106–9.
11. Uranues S, Grossman D, Ludwig L, Bergamaschi R. Laparoscopic partial splenectomy. Surg Endosc 2007;21:57–60.
12. Gamme G, Birch DW, Karmali S. Minimally invasive splenectomy: an update and review. Can J Surg 2013;56: 280–5.
13. Stassen NA, Bhullar I, Cheng JD, et al. Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg 2012;73(5 Suppl 4):S294–300.
14. Upadhyaya P. Conservative management of splenic trauma: history and current trends. Pediatr Surg Int 2003; 19:617–27.
15. Harbrecht BG, Franklin GA, Miller FB, Richardson JD. Is splenectomy after trauma an endangered species? Am Surg 2008;74:410–2.
16. Walsh RM, Heniford BT, Brody F, Ponsky J. The ascendance of laparoscopic splenectomy. Am Surg 2001;67: 48–53.
17. Rose AT, Newman MI, Debelak J, et al. The incidence of splenectomy is decreasing: lessons learned from trauma experience. Am Surg 2000;66:481–6.
18. Kyaw MH, Holmes EM, Toolis F, et al. Evaluation of severe infection and survival after splenectomy. Am J Med 2006;119:276.e1–7.
19. Dubois L, Gray DK. Case series: splenectomy: does it still play a role in the management of thrombotic thrombocytopenic purpura? Can J Surg 2010;53:349–55.
20. Coon WW. Splenectomy for splenomegaly and secondary hypersplenism. World J Surg 1985;9:437–43.
21. OwusuOfori S, Hirst C. Splenectomy versus conservative management for acute sequestration crises in people with sickle cell disease. Cochrane Database Syst Rev 2013;5:CD003425.
22. Perrotta S, Gallagher PG, Mohandas N. Hereditary spherocytosis. Lancet 2008;372:1411–26.
23. Machado NO, Grant CS, Alkindi S, et al. Splenectomy for haematological disorders: a single center study in 150 patients from Oman. Int J Surg 2009;7:476–81.
Table 5 Reported Incidences of Postoperative Outcomes and Complications after Splenectomy
Organ System/ComplicationLaparoscopic
(%)Open (%)
Cardiac 0.1–0.7 0.5–2.3
Cardiac arrest 0.6 0.8
Myocardial infarction (MI) 0.2 0.5
Pulmonary 3.1–4.7 10.1–12.7
Pleural effusion 2.1–5.0 16.4
Pneumonia 2.1–3.2 3.8–8.2
Ventilator > 48 hours 2.6 5.1
Bleeding 1.2–1.6 1.2–3.9
Postsplenectomy hemorrhage 1.2–5.0 5.5–8.9
Thrombotic 0.8–2.6 1.2–3.9
DVT/thrombophlebitis 1.1–2.1 1.6
Pulmonary embolism 0.8–0.9 0.5
Portal vein thrombosis 5–50 5–30
Wound 1.3–1.7 4.3–5.1
Dehiscence 0.06 0.2
Organ space SSI 0.9–1.3 2.2
Superficial SSI 1.0–1.3 1.7
Deep SSI 0.5–1.1 0.1
Infectious/septic 1.0–3.1 3.8–8.3
Sepsis/septic shock 2.9–11 7.6
OPSI 0.5–1.0 0.5–1.0
Genitourinary/renal 0.4–0.6 1.0–2.5
Renal failure 0.9 1.9
Gastrointestinal/pancreatic 1.3–1.5 2.5
Pancreatitis 0–2 2.0
Pancreatic injury 16 16
Pancreatic leak/fistula 1.3–7 2.8–7
Gastric fistula < 1–1.3 < 1
Neurologic 0.1–0.2 0.3
DVT = deep vein thrombosis; SSI = surgical site infection; OPSI = overwhelming postsplenectomy infection.

Scientific American Surgery
10/14
gastro splenectomy — 24
42. Casale M, Perrotta S. Splenectomy for hereditary spherocytosis: complete, partial or not at all? Expert Rev Hematol 2011;4:627–35.
43. Vecchio R, Intagliata E, Ferla F, et al. Laparoscopic splenectomy in patients with hereditary spherocytosis: report on 12 consecutive cases. Updates Surg 2013;65:277–81. DOI: 10.1007/s133040130236x. [Epub 2013 Oct 16]
44. Seims AD, Breckler FD, Hardacker KD, Rescorla FJ. Partial versus total splenectomy in children with hereditary spherocytosis. Surgery 2013;154:849–53; discussion 853–845.
45. Crowther MA, George JN. Thrombotic thrombocytopenic purpura: 2008 update. Cleve Clin J Med 2008;75:369–75.
46. Cuttner J. Splenectomy, steroids, and dextran 70 in thrombotic thrombocytopenic purpura. JAMA 1974;227:397–402.
47. Rutkow IM. Thrombotic thrombocytopenic purpura (TTP) and splenectomy: a current appraisal. Ann Surg 1978;188: 701–5.
48. Cuttner J. Thrombotic thrombocytopenic purpura: a tenyear experience. Blood 1980;56:302–6.
49. Bukowski RM, Hewlett JS, Reimer RR, et al. Therapy of thrombotic thrombocytopenic purpura: an overview. Semin Thromb Hemostasis 1981;7(1):1–8.
50. Bernard RP, Bauman AW, Schwartz SI. Splenectomy for thrombotic thrombocytopenic purpura. Ann Surg 1969;169: 616–24.
51. Rock GA, Shumak KH, Buskard NA, et al. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. Canadian Apheresis Study Group. N Engl J Med 1991;325:393–7.
52. Bell WR, Braine HG, Ness PM, Kickler TS. Improved survival in thrombotic thrombocytopenic purpurahemolytic uremic syndrome. Clinical experience in 108 patients. N Engl J Med 1991;325:398–403.
53. Tsai HM. Thrombotic thrombocytopenic purpura and the atypical hemolytic uremic syndrome: an update. Hematol Oncol Clin North Am 2013;27:565–84.
54. Onundarson PT, Rowe JM, Heal JM, Francis CW. Response to plasma exchange and splenectomy in thrombotic thrombocytopenic purpura. A 10year experience at a single institution. Arch Intern Med 1992;152:791–6.
55. Topley JM, Rogers DW, Stevens MC, Serjeant GR. Acute splenic sequestration and hypersplenism in the first five years in homozygous sickle cell disease. Arch Dis Child 1981;56:765–9.
56. AlSalem AH, Naserullah Z, Qaisaruddin S, et al. Splenic complications of the sickling syndromes and the role of splenectomy. J Pediatr Hematol Oncol 1999;21:401–6.
57. Emond AM, Collis R, Darvill D, et al. Acute splenic sequestration in homozygous sickle cell disease: natural history and management. J Pediatr 1985;107:201–6.
58. Naik RR, Saven A. My treatment approach to hairy cell leukemia. Mayo Clin Proc 2012;87:67–76.
59. Spiers AS, Parekh SJ, Bishop MB. Hairycell leukemia: induction of complete remission with pentostatin (2’deoxycoformycin). J Clin Oncol 1984;2:1336–42.
60. Piro LD, Carrera CJ, Carson DA, Beutler E. Lasting remissions in hairycell leukemia induced by a single infusion of 2chlorodeoxyadenosine. N Engl J Med 1990;322:1117–21.
61. Grever MR, Lozanski G. Modern strategies for hairy cell leukemia. J Clin Oncol 2011;29:583–90.
24. Zhou J, Wu Z, Zhou Z, et al. Efficacy and safety of laparoscopic splenectomy in thrombocytopenia secondary to systemic lupus erythematosus. Clin Rheumatol 2013;32: 1131–8.
25. Kercher KW, Matthews BD, Walsh RM, et al. Laparoscopic splenectomy for massive splenomegaly. Am J Surg 2002; 183:192–6.
26. Berman RS, Feig BW, Hunt KK, et al. Platelet kinetics and decreased transfusion requirements after splenectomy for hematologic malignancy. Ann Surg 2004;240:852–7.
27. Jeker R. [Hypersplenism]. Ther Umsch 2013;70:152–6. 28. Taner T, Nagorney DM, Tefferi A, et al. Splenectomy for
massive splenomegaly: longterm results and risks for mortality. Ann Surg 2013;258:1034–9.
29. Kim SH, Kim DY, Lim JH, et al. Role of splenectomy in patients with hepatocellular carcinoma and hypersplenism. Aust N Z J Surg 2013;83:865–70. DOI: 10.1111/j.14452197.2012.06241.x. [Epub 2012 Sep 17]
30. Zhu JH, Wang YD, Ye ZY, et al. Laparoscopic versus open splenectomy for hypersplenism secondary to liver cirrhosis. Surg Laparosc Endosc Percutan Tech 2009;19:258–62.
31. Kedia S, Goyal R, Mangla V, et al. Splenectomy in cirrhosis with hypersplenism: improvement in cytopenias, Child’s status and institution of specific treatment for hepatitis C with success. Ann Hepatol 2012;11:921–9.
32. Kercher KW, Carbonell AM, Heniford BT, et al. Laparoscopic splenectomy reverses thrombocytopenia in patients with hepatitis C cirrhosis and portal hypertension. J Gastrointest Surg 2004;8:120–6.
33. Heniford BT, Park A, Walsh RM, et al. Laparoscopic splenectomy in patients with normalsized spleens versus splenomegaly: does size matter? Am Surg 2001;67:854–7; discussion 857–8.
34. Neunert C, Lim W, Crowther M, et al. The American Society of Hematology 2011 evidencebased practice guideline for immune thrombocytopenia. Blood 2011;117:4190–207.
35. Zeng Y, Duan X, Xu J, Ni X. TPO receptor agonist for chronic idiopathic thrombocytopenic purpura. Cochrane Database Syst Rev 2011;(7):CD008235.
36. Neunert CE. Current management of immune thrombocytopenia. Hematology Am Soc Hematol Educ Program 2013;2013:276–82.
37. Gwilliam NR, Lazar DA, Brandt ML, et al. An analysis of outcomes and treatment costs for children undergoing splenectomy for chronic immune thrombocytopenia purpura. J Pediatr Surg 2012;47:1537–41.
38. Liu EH, Dilip CK, Yeh TS, et al. Longterm relapsefree rurvival rate and predictive factors of idiopathic thrombocytopenic purpura in adults undergoing splenectomy. Biomed J 2013;36:23–7.
39. Provan D, Stasi R, Newland AC, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood 2010;115: 168–86.
40. Patel NY, Chilsen AM, Mathiason MA, et al. Outcomes and complications after splenectomy for hematologic disorders. Am J Surg 2012;204:1014–9; discussion 1019–20.
41. JaimePerez JC, RodriguezMartinez M, GomezdeLeon A, et al. Current approaches for the treatment of autoimmune hemolytic anemia. Arch Immunol Ther Exp (Warsz) 2013;61:385–95.

Scientific American Surgery
10/14
gastro splenectomy — 25
62. Golomb HM. Fifty years of hairy cell leukemia treatments. Leuk Lymphoma 2011;52 Suppl 2:3–5.
63. Jones G, ParryJones N, Wilkins B, et al, British Committee for Standards in Haematology. Revised guidelines for the diagnosis and management of hairy cell leukaemia and hairy cell leukaemia variant. Br J Haematol 2012;156: 186–95.
64. Kaza RK, Azar S, AlHawary MM, Francis IR. Primary and secondary neoplasms of the spleen. Cancer Imaging 2010; 10:173–82.
65. Pugalenthi A, Bradley C, Gonen M, et al. Splenectomy to treat splenic lesions: an analysis of 148 cases at a cancer center. J Surg Oncol 2013;108:521–5. DOI: 10.1002/jso.23433. [Epub 2013 Sep 16]
66. Rasheed K, Zargar SA, Telwani AA. Hydatid cyst of spleen: a diagnostic challenge. N Am J Med Sci 2013;5: 10–20.
67. Sreekar H, Saraf V, Pangi AC, et al. A retrospective study of 75 cases of splenic abscess. Indian J Surg 2011;73:398–402.
68. Carbonell AM, Kercher KW, Matthews BD, et al. Laparoscopic splenectomy for splenic abscess. Surg Laparosc Endoscpercutan Tech 2004;14:289–91.
69. Sinha CK, Agrawal M. Nonparasitic splenic cysts in children: current status. Surgeon 2011;9:49–53.
70. Zonies D, Eastridge B. Combat management of splenic injury: trends during a decade of conflict. J Trauma Acute Care Surg 2012;73(2 Suppl 1):S71–4.
71. Mossadegh S, Midwinter M, Sapsford W, Tai N. Military treatment of splenic injury in the era of nonoperative management. J R Army Med Corps 2013;159:110–3.
72. Li Y, Cui L, Zhang W, et al. Laparoscopic radiofrequency ablation for traumatic splenic rupture. J Surg Res 2013;185: 711–6. DOI: 10.1016/j.jss.2013.06.018. [Epub 2013 Jul 1]
73. Mostafa G, Matthews BD, Sing RF, et al. Elective laparoscopic splenectomy for grade III splenic injury in an athlete. Surg Laparosc Endosc Percutan Tech 2002;12:283–6; discussion 286–8.
74. Cobb WS, Heniford BT, Burns JM, et al. Cirrhosis is not a contraindication to laparoscopic surgery. Surg Endosc 2005;19:418–23.
75. Ardestani A, Tavakkoli A. Laparoscopic versus open splenectomy: the impact of spleen size on outcomes. J Laparoendosc Adv Surg Tech A 2013;23:760–4.
76. Ahad S, Gonczy C, Advani V, et al. True benefit or selection bias: an analysis of laparoscopic versus open splenectomy from the ACSNSQIP. Surg Endosc 2013;27:1865–71.
77. Deeb AP, Kim MJ, Fleming FJ, et al. The impact of operative approach in elective splenectomy: a multivariate analysis of outcomes from the NSQIP database. Surg Laparosc Endoscpercutan Tech 2012;22:415–9.
78. Chand B, Walsh RM, Ponsky J, Brody F. Pancreatic complications following laparoscopic splenectomy. Surg Endosc 2001;15:1273–6.
79. Qu Y, Ren S, Li C, et al. Management of postoperative complications following splenectomy. Int Surg 2013;98:55–60.
80. Winslow ER, Brunt LM. Perioperative outcomes of laparoscopic versus open splenectomy: a metaanalysis with an emphasis on complications. Surgery 2003;134:647–53; discussion 654–645.
81. Ray U, Gupta S, Chatterjee S, et al. Laparoscopic versus open splenectomy in the treatment of idiopathic thrombocytopenic purpura: an Indian experience. J Indian Med Assoc 2012;110:889–93.
82. Nyilas A, Paszt A, Simonka Z, et al. [Comparison of laparoscopic and open splenectomy]. Magy Seb 2013;66(1): 14–20.
83. Grahn SW, Alvarez J 3rd, Kirkwood K. Trends in laparoscopic splenectomy for massive splenomegaly. Arch Surg 2006;141:755–61; discussion 761–752.
84. Wu Z, Zhou J, Cai YQ, et al. The learning curve for laparoscopic splenectomy for massive splenomegaly: a single surgeon’s experience. Chin Med J (Engl) 2013;126:2103–8.
85. DahyotFizelier C, Debaene B, Mimoz O. [Management of infection risk in asplenic patients]. Ann Fr Anesth Reanim 2013;32:251–6.
86. Centers for Disease Control and Prevention. Immunization schedules. Available at: http://www.cdc.gov/ vaccines/schedules/hcp/imz/adultshell.html (accessed April 2014).
87. Shatz DV, Schinsky MF, Pais LB, et al. Immune responses of splenectomized trauma patients to the 23valent pneumococcal polysaccharide vaccine at 1 versus 7 versus 14 days after splenectomy. J Trauma 1998;44:760–5; discussio n 765–6.
88. Wang X, Li Y, Zhou J, et al. Handassisted laparoscopic splenectomy is a better choice for patients with supramassive splenomegaly due to liver cirrhosis. J Laparoendosc Adv Surg Tech A 2012;22:962–7.
89. Harrison BJ, Glanges E, Sparkman RS. Gastric fistula following splenectomy: its cause and prevention. Ann Surg 1977;185:210–3.
90. Zhe C, Jianwei L, Jian C, et al. Laparoscopic versus open splenectomy and esophagogastric devascularization for bleeding varices or severe hypersplenism: a comparative study. J Gastrointest Surg 2013;17:654–9.
91. Kristinsson SY, Gridley G, Hoover RN, et al. Longterm risks after splenectomy among 8,149 cancerfree U.S. veterans: a cohort study with up to 27 years followup. Haematologica 2014;99:392–8. DOI: 10.3324/haematol. 2013.092460. [Epub 2013 Sep 20]
92. Boyle S, White RH, Brunson A, Wun T. Splenectomy and the incidence of venous thromboembolism and sepsis in patients with immune thrombocytopenia. Blood 2013;121: 4782–90.
93. Miniero R, Barretta M, Dolceamore TR, et al. [Update on prevention of infections in patients without spleen or with diminished splenic function]. Minerva Pediatr 2013;65: 427–45.
94. Waldron DJ, Harding B, Duignan J. Overwhelming infection occurring in the immediate postsplenectomy period. Br J Clin Pract 1989;43:421–2.
95. Das SS, Bhattacharya S, Sen S. Managing uncontrolled postsplenectomy reactive thrombocytosis in idiopathic thrombocytopenic purpura: role of thrombocytapheresis. Transfus Apher Sci 2013;49:171–3. DOI: 10.1016/j.transci. 2012.09.009. [Epub 2013 Jul 16]
96. Raval JS, Redner RL, Kiss JE. Plateletpheresis for postsplenectomy rebound thrombocytosis in a patient with chronic immune thrombocytopenic purpura on romiplostim. J Clin Apher 2013;28:321–4.

Scientific American Surgery
10/14
gastro splenectomy — 26
97. Khan PN, Nair RJ, Olivares J, et al. Postsplenectomy reactive thrombocytosis. Proc (Bayl Univ Med Cent) 2009;22(1): 9–12.
98. Oida T, Kano H, Mimatsu K, et al. Thrombocytosis following splenectomy: with or without additional organ resection. Hepatogastroenterology 2012;59:1033–5.
99. Schafer AI. Thrombocytosis. N Engl J Med 2004;350: 1211–9.
100. Stamou KM, Toutouzas KG, Kekis PB, et al. Prospective study of the incidence and risk factors of postsplenectomy thrombosis of the portal, mesenteric, and splenic veins. Arch Surg 2006;141:663–9.
101. Lai W, Lu SC, Li GY, et al. Anticoagulation therapy prevents portalsplenic vein thrombosis after splenectomy with gastroesophageal devascularization. World J Gastroenterol 2012;18:3443–50.
102. Pimpl W, Dapunt O, Kaindl H, Thalhamer J. Incidence of septic and thromboembolicrelated deaths after splenectomy in adults. Br J Surg 1989;76:517–21.
103. Kercher KW, Sing RF, Watson KW, et al. Transhepatic thrombolysis in acute portal vein thrombosis after laparoscopic splenectomy. Surg Laparosc Endosc Percutan Tech 2002;12:131–6.
104. Li MX, Zhang XF, Liu ZW, Lv Y. Risk factors and clinical characteristics of portal vein thrombosis after splenectomy in patients with liver cirrhosis. Hepatobiliary Pancreat Dis Int 2013;12:512–9.
105. Fujita F, Lyass S, Otsuka K, et al. Portal vein thrombosis following splenectomy: identification of risk factors. Am Surg 2003;69:951–6.
106. Tran T, Demyttenaere SV, Polyhronopoulos G, et al. Recommended timing for surveillance ultrasonography to diagnose portal splenic vein thrombosis after laparoscopic splenectomy. Surg Endosc 2010;24:1670–8.
107. Harris W, Marcaccio M. Incidence of portal vein thrombosis after laparoscopic splenectomy. Can J Surg 2005;48: 352–4.
108. Zhang Y, Wen TF, Yan LN, et al. Preoperative predictors of portal vein thrombosis after splenectomy with periesophagogastric devascularization. World J Gastroenterol 2012;18:1834–9.
109. Robinette CD, Fraumeni JF Jr. Splenectomy and subsequent mortality in veterans of the 193945 war. Lancet 1977;2:127–9.
110. Schilling RF. Spherocytosis, splenectomy, strokes, and heat attacks. Lancet 1997;350:1677–8.
111. Enzler MJ, Berbari E, Osmon DR. Antimicrobial prophylaxis in adults. Mayo Clin Proc 2011;86:686–701.
Acknowledgments
Figures 1 and 4 Courtesy of Taylor S. Riall, MD, PhD, FACS.Figures 7a, 11a, 15, 17, 22, 23, and 24 Tom MooreFigures 12 and 13a Christine Kenney