Gastrointestinal Stromal Tumors - Department of Surgery … · of gastric gastrointestinal stromal...
51
Gastrointestinal Stromal Tumors Grand Rounds Sept 9, 2010 www.downstatesurgery.org
Transcript of Gastrointestinal Stromal Tumors - Department of Surgery … · of gastric gastrointestinal stromal...

Gastrointestinal Stromal Tumors
Grand Rounds
Sept 9, 2010
www.downstatesurgery.org

Outline
• Case• Epidemiology• Pathology• Clinical presentation• Treatment for primary/recurrent/metastatic
disease• Adjuvant / Neoadjuvant therapy• Laparoscopic resection
www.downstatesurgery.org

Case - History
• HPI: – 61 yo M, recent h/o bilat inguinal hernia repair.– Abdominal CT for post-op pain revealed gastric
mass.– Endoscopic bx consistent with GIST.– At presentation, denied GI symptoms (bleeding,
dysphagia, N/V, fullness, hematochezia).
• PMH: neg• PSH: per HPI
www.downstatesurgery.org

Case - Exam
• AF, 76, 108/74
• WNWD male; appearance consistent with age
• NC, neck supple, no LA
• RRR
• CTAB
• SNTND, no organomegaly; well-healed bilat inguinal hernia scars
www.downstatesurgery.org

Case – Labs
• Na 143
• K 4.0
• Cl 107
• BUN 15
• Cr 0.78
• Ca 9.1
• Alb 4.5
• T Bili 0.6
• AP 53
• AST 17
• ALT 16
• WBC 3.9
• Hgb 14.2
• Hct 42.4
• Plt 149
www.downstatesurgery.org

Case – CT Scanwww.downstatesurgery.org

Case – CT Scanwww.downstatesurgery.org

Case – Tumor Locationwww.downstatesurgery.org

Case – Tumor Locationwww.downstatesurgery.org

Case – Operation
• Laparoscopic approach.
• 4x4cm tumor freed from lesser omentum using harmonic scalpel taking care to identify L gastric and hepatic arteries.
• Gastric wall abutting mass was resected with endoGIA ensuring 1 cm margin.
• Concurrent endoscopy to visualize gastric lumen.
www.downstatesurgery.org

Case – Pathology
• GIST tumor – 3 x 4 cm.
• CD117 immunostain positive.
• Tumor arises within gastric wall.
• Negative margins.
• Low mitotic rate.
• Stage – pT4 Nx Mx.
• Prognosis – low risk.
www.downstatesurgery.org

Case – Postop
• Tolerating diet, discharged on POD 2.
• FU:– Followed by oncology.
– Started on Gleevec.
– Pt doing well; without complaints.
www.downstatesurgery.org

Epidemiology
– Most common sarcoma of GI tract
– Only 0.2% of all GI tumors
– 7-20 cases per 1 million persons per year in the US
www.downstatesurgery.org

History
• The term ‘GIST’ first used in early 1980s.• Referred to spindle and epithelioid tumors
arising from stromal/mesenchymalcomponents of GI tract.
• True GISTs lacked complete muscle or neural differentiation.
• Up to 2/3 of GISTs were CD34 positive.– Initially used as marker for GISTs.– Neither selective or specific.
www.downstatesurgery.org

History
• CD117 antigen identified– Near-universally expressed in GISTs
– Not expressed in leiomyomas, true leiomyosarcomas, and other spindle-cell tumors
www.downstatesurgery.org

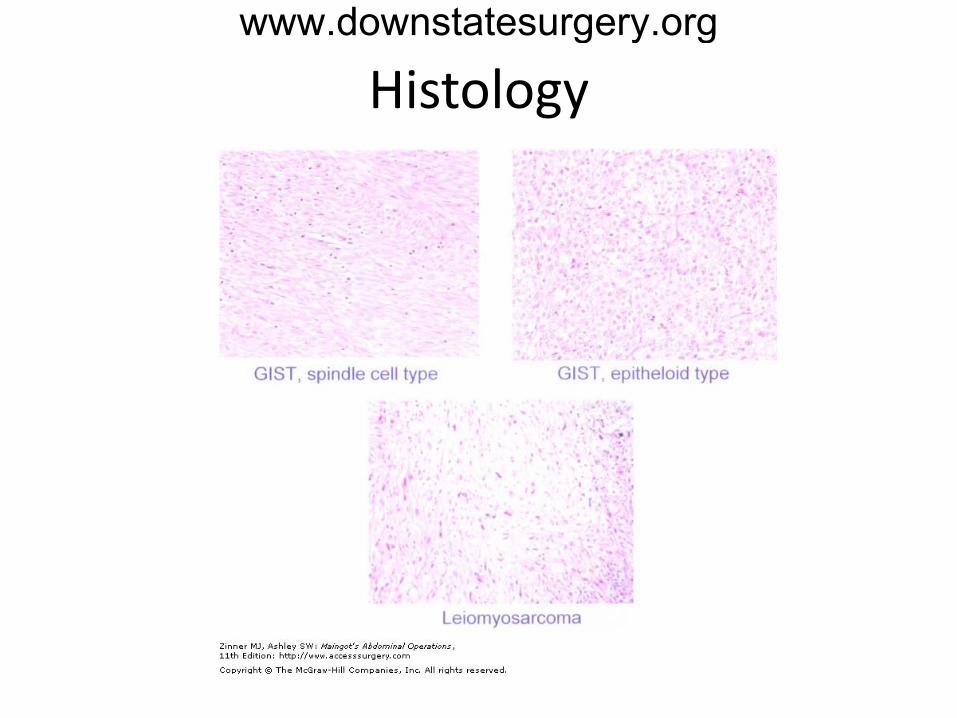
Histology
• Heterogeneous
• Long fascicles of bland spindle cells
• Occasionally epithelioid with eosinophilic cytoplasma and nuclear atypia
• Based on immunohistology, GIST cells thought to arise from Interstitial Cells of Cajal, which are components of intestinal autonomic nervous system that serve as pacemaker cells.
www.downstatesurgery.org
Histologywww.downstatesurgery.org
Molecular Biology
• Molecular basis for GIST is gain of function of KIT proto-oncogene.
• KIT receptor is a Tyrosine Kinase, which is activated when bound to a ligand known as steel factor or stem cell factor.
www.downstatesurgery.org

Molecular Biology
• KIT is important in the development and maintenance of components of hematopoesis, gametogenesis, and intestinal pacemaker cells.
• KIT mutation identified in neoplasms involving:– Mast cell tumors
– Myelofibrosis
– CML
– Germ cell tumors
– GIST
www.downstatesurgery.org

Molecular Biologywww.downstatesurgery.org

Molecular Biology
• 68% - mutation at exon 11
• 11% - mutation at exon 9
• 0.6-4% - mutation at exon 13 or 17
• 7% - gain of function mutation at PDGFRA
www.downstatesurgery.org

Immunohistochemistry
Type CD117 CD34 SMA S100 Desmin
GIST + (>95%) + (60-70%) ± (30-40%) − rare
Leiomyoma − + (10-15%) + − +
Leiomyosarcoma − − + − +
Schwannoma − − − + −
www.downstatesurgery.org

Clinical Presentation
• 40-60 years of age (described in children as young as 10)
• Equal sex distribution
• No racial predilection
www.downstatesurgery.org

Presenting Symptoms
• Most asymptomatic.– Discovered incidentally on imaging or laparotomy
for other reasons.
• Symptoms– Bleeding – MC
– Vague abdominal pain
– Bowel obstruction
– Perforation
www.downstatesurgery.org

DDx of Submucosal Tumors of Intestine
• GIST• Leiomyoma• Leiomyosarcoma• Schwannoma• Malignant peripheral nerve sheath tumor• Solitary fibrous tumor• Inflammatory myofibroblastic tumor• Desmoid tumor• Metastatic melanoma
www.downstatesurgery.org

Evaluation
• Endoscopy
• EUS with FNA
• CT
• PET– Important when assessing chemotherapy
response.
www.downstatesurgery.org

Anatomic Presentation
• Primary GIST can arise throughout GI tract
• Stomach (40-70%)
• Small bowel (20-40%)
• Colorectum (5-15%)
• Esophagus (<5%)
www.downstatesurgery.org

Metastasis
• 15-50% present with overt metastatic disease
• Almost entirely intra-abdominal– Liver and peritoneum MC met sites
– In diffuse disease, may stud omentum, diaphragm, bowel serosa
– Can develop tumor-associated ascites
• Pulmonary metastasis – 5%
www.downstatesurgery.org

Prognostic Features
• Poor prognosis associated with– Large size
– Increased mitotic rate
– Location in SB
www.downstatesurgery.org

Risk Classification for Metastasis
Risk category Size Mitotic Count
Very low < 2 cm < 5 per 50 HPF
Low 2-5 cm < 5 per 50 HPF
Intermediate < 5 cm 6-10 per 50 HPF
5-10 cm < 5 per HPF
High > 5 cm > 5 per 50 HPF
> 10 cm Any mitotic rate
Any size > 10 per 50 HPF
www.downstatesurgery.org

Rates of Progression-free Survival
Tumorsize [cm]
Mitotic rate [HPF]
Gastric Jejunum/ileum
Duodenum Rectum
≤ 2 ≤5/50 100 100 100 100
2 to 5 ≤5/50 98.1 95.7 91.7 91.5
5 to 10 ≤5/50 96.4 7666 43
> 10 ≤5/50 88 48
≤ 2 >5/50 100 50 - 46
2 to 5 >5/50 84 27 50 48
5 to 10 >5/50 45 1514 29
> 10 >5/50 14 10
www.downstatesurgery.org
Presenter
Presentation Notes
Based on long-term follow-up studies on 1055 gastric, 629 small intestinal, 144 duodenal, and 111 rectal cancers. * Data are combined for tumors >5 cm. • Small number of cases. Adapted from: Miettinen, M, et al. Semin Diagn Pathol 2006; 23:70.

Imatinib (Gleevec)www.downstatesurgery.org

Imatinib (Gleevec)
• Imatinib mesylate - Glivic in Europe
• Originally developed to treat CML
• Oral
• Inhibits KIT and PDGFRA protein kinases– Lodges in an ATP-binding pocket that forms upon
receptor dimerization.
www.downstatesurgery.org
Imatinib (Gleevec)
• Effective use in GIST patients first reported in 2001.
• Initially approved for use in US and Europe for advanced or metastatic disease.
www.downstatesurgery.org

Imatinib – Side Effects
• SE– Edema– Nausea– Muscle cramps– Diarrhea– Headache– Dermatitis– Fatigue– Anemia– Neutropenia
• Most SE mild to moderate and tend to resolve with ongoing therapy
www.downstatesurgery.org

Imatinib – KIT Mutation
• Response depends on mutation location– Exon 11 – 72% response
– Exon 9 – 32% response
• Survival dependent on mutation location– Exon 11 – 22.5 months event free
– Exon 9 – 6.6 months
– No mutation – 2.7 months
www.downstatesurgery.org

Surgical Management of Localized Primary Disease
• Surgery is standard therapy for all resectable nonmetastatic tumors.
• Resectable in 70-80% of patients.
• Tumor rupture or violation of tumor pseudocapsule associated with increased risk of recurrence, including disseminated disease.
• If adjacent organs are involved, en bloc resection recommended.
www.downstatesurgery.org

Surgical Management of Localized Primary Disease
• Optimal resection margin has not been established.– As GIST generally do not exhibit infiltrative spread,
a 1 cm margin is usually sought.
• Wider resection of uninvolved tissue confers no additional benefit.
• Routine lymphadenectomy is unnecessary because nodal metastases are rare.
www.downstatesurgery.org

Management of Primary Diseasewww.downstatesurgery.org

Postop Surveillance
• Typical sites of tumor recurrence following resection include:– Resection bed.– Liver.– Peritoneum.
• Timing variable; has been seen as early as 3 months.
• Because more recurrences occur within the first 5 years, imaging every 6 months are routine.
• No serum markers.
www.downstatesurgery.org

Recurrence
• Recurrence rates vary:– 2-15% for low risk
– 70-90% for high risk
• Without adjuvant therapy, at 5 years:– Appx 50% of pts with curative surgery will develop
local or metastatic disease.
– Only 40-55% will survive.
www.downstatesurgery.org

Management of Metastatic Disease
• All unresectable, recurrent, and metastatic GIST are considered for life-long imatinib therapy.
• Median time to response is 3 months.
• Complete response rare.
• 2 year survival for responders – 85-90%.
www.downstatesurgery.org

Adjuvant Therapy
Placebo-Controlled Randomized Trial of Adjuvant Imatinib Mesylate Following the Resection of Localized, Primary Gastrointestinal Stromal Tumor (GIST). Lancet, Mar 2009.
• ACOSOG – sponsored.• Randomized phase 3, double-blind, placebo-
controlled, multicenter trial.• Study period: 2002-2007.
www.downstatesurgery.org

Adjuvant Therapy
• 713 pts randomized to receive imatinib or placebo for 1 year successful primary GIST resection.
• Pts stratified by tumor size.• Pts were allowed to cross over with disease recurrence.• Accrual stopped early based on interim analysis.• Imatinib significantly prolonged RFS compared to
placebo (98% vs 83% at 1 year; HR 0.66; p < 0.0001).• Overall 1 year survival was similar (99.2% vs 99.7%; HR
0.66; p = 0.47).
www.downstatesurgery.org

Recurrence Free Survivalwww.downstatesurgery.org

Overall Survivalwww.downstatesurgery.org

Adjuvant Therapy
• Study addressed questions regarding:– Rx efficicacy vs placebo.– Rx efficicacy stratified by tumor size.
• Study did not address:– Optimal dosing.– Optimal duration of therapy (EORTC, SSG studies
ongoing)
• FDA approved Imatinib for adjuvant therapy for GIST > 3 cm.
www.downstatesurgery.org

Neoadjuvant Therapy
• Surgery is the only potentially curative option for GIST.
• Setting where neoadjuvant therapy may be beneficial:– Unresectable or borderline resectable primary tumor.
– Resectable tumor that requires extensive organ disruption.
• Goal: to facilitate surgery and/or preserve surrounding organs.
www.downstatesurgery.org

Neoadjuvant Therapy
• No randomized trials.• Multicenter RTOG/ACRIN prospective phase II
trial.– Rx for 8-12 weeks preop.– For primary disease, 7% response, 83% stable disease.– For metastatic disease, 5% response, 91% stable
disease.– At median FU of 3 years, 2 year:
• Primary disease – PFS: 83%, OS: 93%.• Met disease – PFS: 77%, OS: 91%.
www.downstatesurgery.org

Long-term Outcomes of Laparoscopic Resection
Long-term outcomes of laparoscopic resection of gastric gastrointestinal stromal tumors. Carolinas Medical Center. Annals of Surgery, 2006.
• Case series of 50 pts over 10 years.
• Laparoscopic resections of gastric GISTs.
www.downstatesurgery.org

Long-term Outcomes of Laparoscopic Resection
• Patient Characteristics– Mean age 60 years (range 34-84 years)– Mean size 4.4 cm (range 1.0 – 8.5 cm)– 9 pts had 10 or more mitotic figures on HPF
• Outcomes at mean follow-up of 36 months– 46 pts (92%) were disease free– 1 pt alive with metastatic disease– 1 pt with met dz, died of cardiac reasons– 2 pt died due to met dz
www.downstatesurgery.org