GASTROINTESTINAL. Common GI disorders in Children Obesity Anorexia Nervosa Bulimia Cleft lip/Cleft...
84
GASTROINTESTINAL
-
Upload
kathlyn-may -
Category
Documents
-
view
222 -
download
1
Transcript of GASTROINTESTINAL. Common GI disorders in Children Obesity Anorexia Nervosa Bulimia Cleft lip/Cleft...

GASTROINTESTINAL
Common GI disorders in Children
• Obesity• Anorexia Nervosa• Bulimia• Cleft lip/Cleft palate• GER• Pyloric Stenosis
• Intussusception• Hirschprung’s Disease• Celiac disease• Giardiasis• Pin worm• Diarrhea

EATING DISORDERS

Overweight and Obesity• Many reasons the increase in overweight children in the US.
• Calories consumed is not the issue• Lack of exercise is believed to be the main cause:
• convenience of driving • unsafe neighborhoods
• Television viewing and screen time accompanied by ingestion of high-calorie foods

Childhood Obesity
• Both immediate and long term side effects • Low Self-esteem
• Can be a precursor of• hyperlipidemia,• sleep apnea• gall stones• orthopedic problems• HTN• DM
Nursing Consideration• Identify risk and prevent new cases of overweight children
• How much screen time per day?• TV, computer in bedroom?• Video games (unless Wii-fit or Kinect)• I-pods, I-pads, Smart phone?
• Genetic factors and common lifestyles are also a risk • Overweight parents

Nursing Considerations• Identify overweight children and support to establish
healthy lifestyles• Screen time should be limited to 2 hours a day• Family exercise 30-60 minutes a day• Healthy snacking• Avoid ‘supersizing’ fast food portions• Limit eating out• Teach MyPyramid

Nursing Considerations• Add fiber to prolong stomach emptying time• Teach methods to manage stress• Set short term, reachable goals (5lbs. over 1 month, not
50 for the year)• For school age obese children, formal weight loss
programs are available

Nursing Considerations• Teach children how to prepare food within developmental
limits
• Parental education plays a very important part in success.
Anorexia Nervosa
• A potentially life-threatening type of disordered eating • 95% of cases are girls age 12-18• A voluntary refusal to eat b/c of an intense fear of gaining
weight leads to:• Preoccupation with food and body weight• Excessive weight loss
Causes of Anorexia Nervosa• Cultural overemphasis on thinness
• May have existing “Perfectionist” personality
• Possible biological cause
• Life stress or loss
• Conflict in the family• the child is not encouraged to be independent, and
never develops autonomy…feelings of loss of control, poor self esteem
Anorexia Nervosa• Poor self-esteem leads to a pronounced disturbed body
image
• Excessive dieting leads to a feeling of control over body
Symptoms
• Lengthy and vigorous exercise(up to 4 hours daily) to prevent weight gain.
• Laxatives or diuretics to induce weight loss.• Intense and irrational fear of becoming obese (although underweight)
• Fear does not decrease as weight is lost• Perceive food as revolting• Refuse to eat or vomit immediately after eating

Symptoms
• Girls can find support of anorexia on internet
• Share information on weight loss techniques
• View anorexia as beautiful

Physical Characteristics• Excessive weight loss (25% less than normal body
weight)• Hypokalemia• Dysthymias• Dependent edema• Hypotension• Hypothermia• Bradycardia• Lanugo formation• Amenorrhea• Can lead to death

Treatment Goals• Address the physiologic problems associated with
malnutrition• Local Hospital 2-3 days admission• Enteral feedings or TPN• replace lost fluid, protein, and nutrients
• Address the behavioral and cognitive components of the disorder• Specialized Treatment Center-long term

Long Term Out-Patient Treatment
• Establish realistic goals• Build rapport, trusting relationship• Need to gain weight to reach 90-95 lbs. • 3 lbs per week, only weigh once a week.• Individual, group, and family therapy• Need continued follow-up, 2-3 years of counseling to be sure that self-image is being maintained

BulimiaBinge eating followed by depression and activities to
control weight gain
• Also occurs primarily in adolescent females• Food is eaten secretly, high in calories• Abdominal pain from overfull stomach• Vomit to relieve the pain• Laxatives and diuretics• Affects older adolescents, college age

Cause of Bulimia• Adolescent may be unable to express feelings• Has an existing low self esteem or depression• Lacks impulse control• Poor body image
• Purging leads to increased sense of control and decreased anxiety
Symptoms• Easily concealed• Usually average body weight
• Physical Findings depend on amount of purging• Electrolyte imbalances• Tooth erosion, gum recession• Esophagitis• Abdominal distension

Treatment• Hospitalization is usually not needed• Focus is on changing behavior• Treating depression• Teaching to recognize connections between emotional
states and stress and the impulse to binge or purge

STRUCTURAL DISORDERS

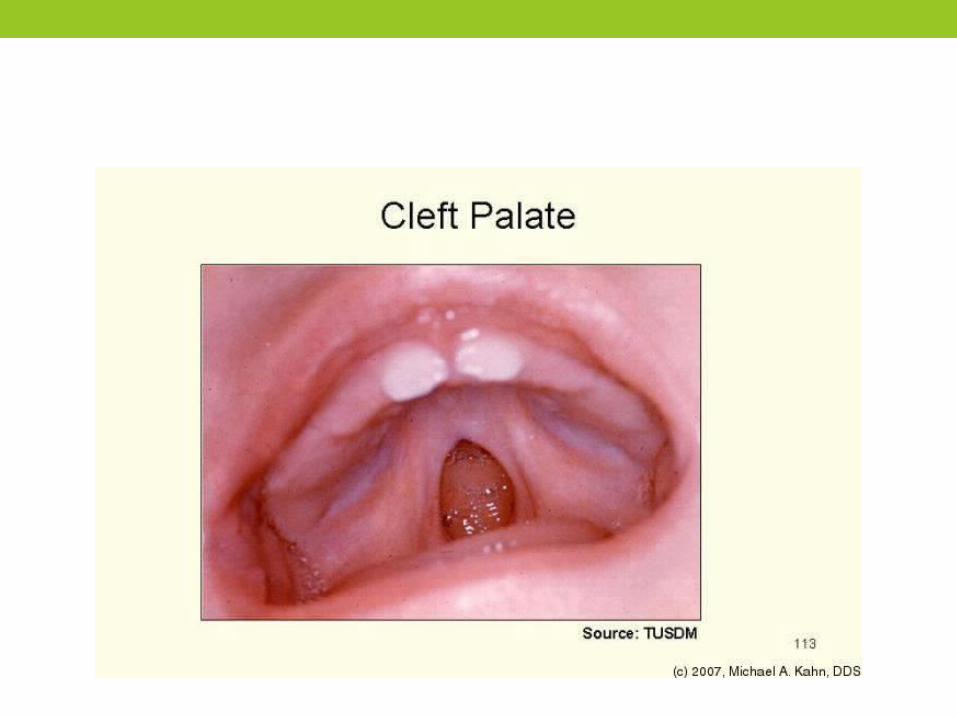
Cleft lip/Cleft palate
• Cleft Lip: failure of maxillary and median nasal processes to fuse
• Cleft Palate: midline fissure of palate
• Cause is believed to be multifactorial
environmental and genetic
• Apparent at birth => severe emotional reaction by parents


Unilateral Cleft Lip

Cleft Lip: Immediate nursing challenges birth until surgery
Keep upright during feedingCannot use a normal nipple (can’t generate suction)Use large soft nipple with large hole or a “gravity flow”
nipple (deposits formula in mouth)Needs breaks during feedings


Cleft Palate: Immediate nursing challenges birth until surgery
Nipple must be positioned so that it is compressed by infant’s tongue and existing palate
Swallow excessive air, burp frequently
Immediate nursing challenges
Emphasize positive aspects of childHold infant close (modeling behavior), infant is special
Explanation of immediate and long-range problems assoc. with CL/CP

Surgical Repair• Cleft Lip age 6-12 wks
• Z-plasty: staggered suture line minimizes scar tissue formation• May need more than one operation
• Cleft Palate 12-18 months

Post-operatively: Cleft Lip Repair
• # 1 Priority-Protect operative site!
• Logan Bar: thin arched metal device taped or butterflied to cheeks, protects suture line from tension & trauma
• Arms restrained at elbows x 2 weeks
Post-operatively: Cleft Lip Repair
Clear liquids first => formulaBreck feeder (syringe with rubber tubing), prevents infant from sucking on tubing until lip heals
Meticulous care to suture line, carefully cleanse after feeding by gently wiping with saline
Position on side or back

Breck Feeder

Post-operatively: Cleft Palate Repair
• Can lie on abdomen• Fluids from a cup• Still needs restraint at elbow• No: pacifiers, tongue depressors, thermometers, straws,
spoons• Blended diet => soft (no food harder than mashed
potatoes)
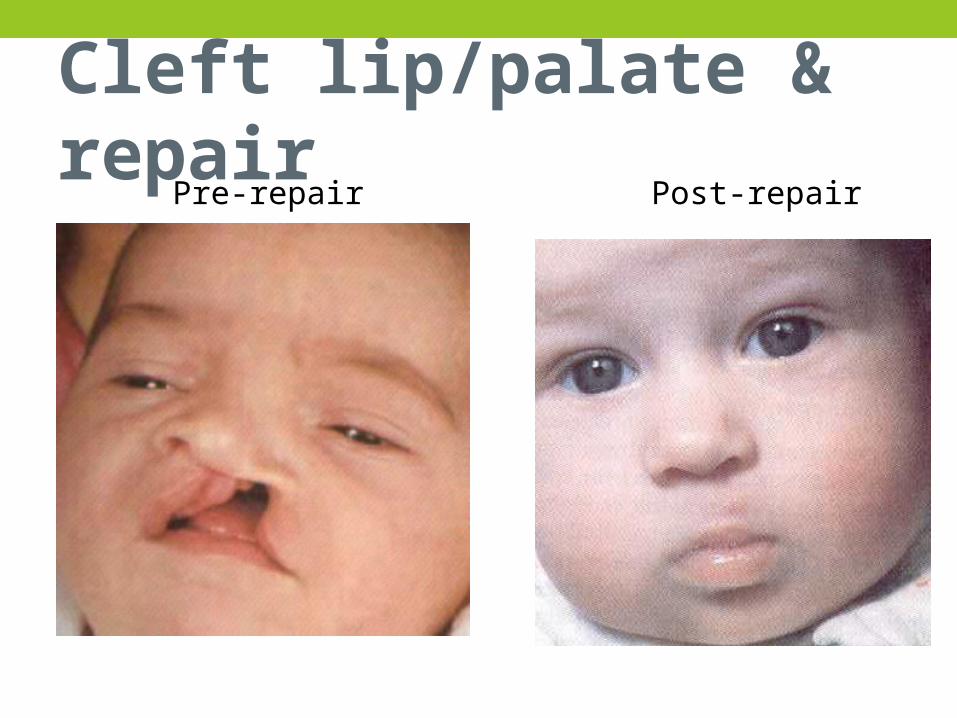
Cleft lip/palate & repairPre-repair Post-repair

Prognosis: good, BUT
• Speech impairment • Improper tooth alignment• Varying degree of hearing loss• Improper drainage of middle ear => recurrent otitis
media
• Therefore upper respiratory infections need prompt
treatment

Gastroesophageal Reflux (GER)• LE sphincter & lower portion of esophagus are lax
• Regurgitation of gastric contents into esophagus
• Usually begins 1 week after birth
• Regurgitation immediately after feeding

Gastroesophageal RefluxTreatment•Upright position for feeding & 1h after feeding•Formula thickened with rice cereal or special formula•Enfamil AR (contains added rice)•Semi-elemental formula (Pregestimil, Nutramigen, Alimentum)•Zantac or Prilosec (decrease irritation)

Pyloric Stenosis
hypertrophied muscle of the pylorus is grossly enlarged leads to delayed stomach emptying
Symptoms
•Begins a few weeks after birth• regurgitation, occasional non-projectile vomiting 4-6 weeks after birth
•progresses to projectile vomiting (3-4 feet) shortly after feeding

Symptoms
• Emesis contains stale milk, sour smell, no bile• Chronic hunger• Visible gastric peristalsis moves from left to right across
the epigastrium• Dehydration, lethargic, weight loss
Treatment
•Pylorotomy• longitudinal incision through muscle fibers of the pyloris
• Incision is in the periumbical area

Pyloric Stenosis
Post-op• High risk for infection-location of incision• Small, frequent feedings • “Down’s Regimen
• NPO x 4 hrs, then Glucose and H2O q 2-3 hrs, then ½ strength formula/breast milk q 2-3 hrs, then full strength
• Burp well to prevent air in stomach• Position right side
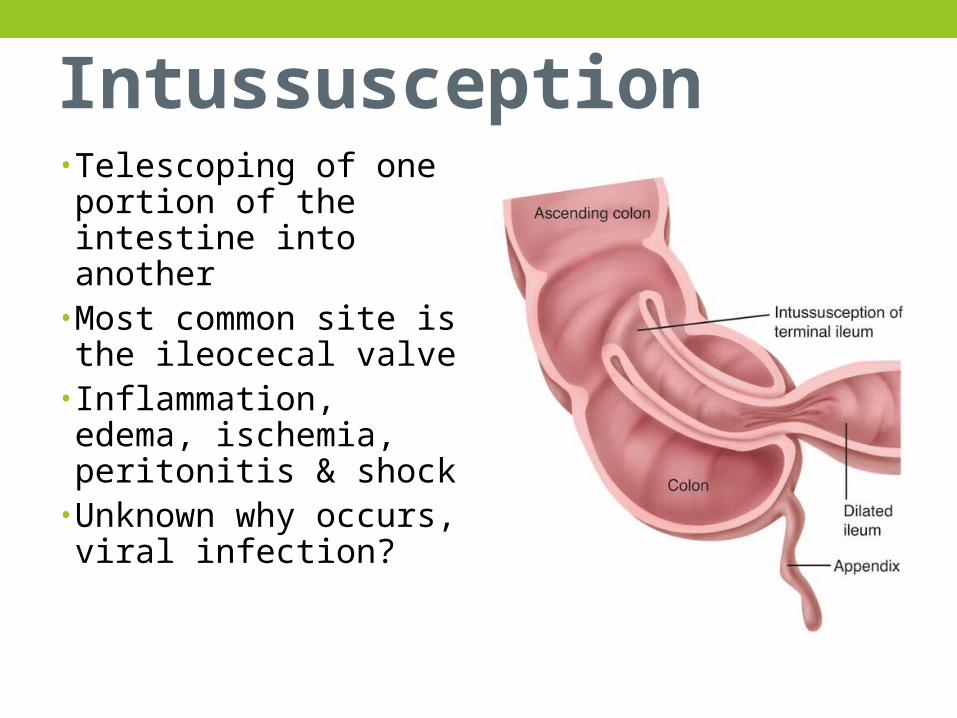
Intussusception• Telescoping of one portion of the intestine into another
• Most common site is the ileocecal valve
• Inflammation, edema, ischemia, peritonitis & shock
• Unknown why occurs, viral infection?

Symptoms
• Affects children (3mos to 5 years, usually occurs in first year of life)
• Sudden acute abdominal pain q 15minutes • Vomiting (contains bile)• Lethargy• Tender, distended abdomen• Stools contain blood and mucus (“currant jelly”)
Management• nonsurgical hydrostatic reduction (barium enema)• force is exerted by flowing barium via enema to push
bowel back into place• surgery if unsuccessful• if positive bowel sounds (oral feedings)• watch for passage of normal brown stool

MOTILITY DISORDERS
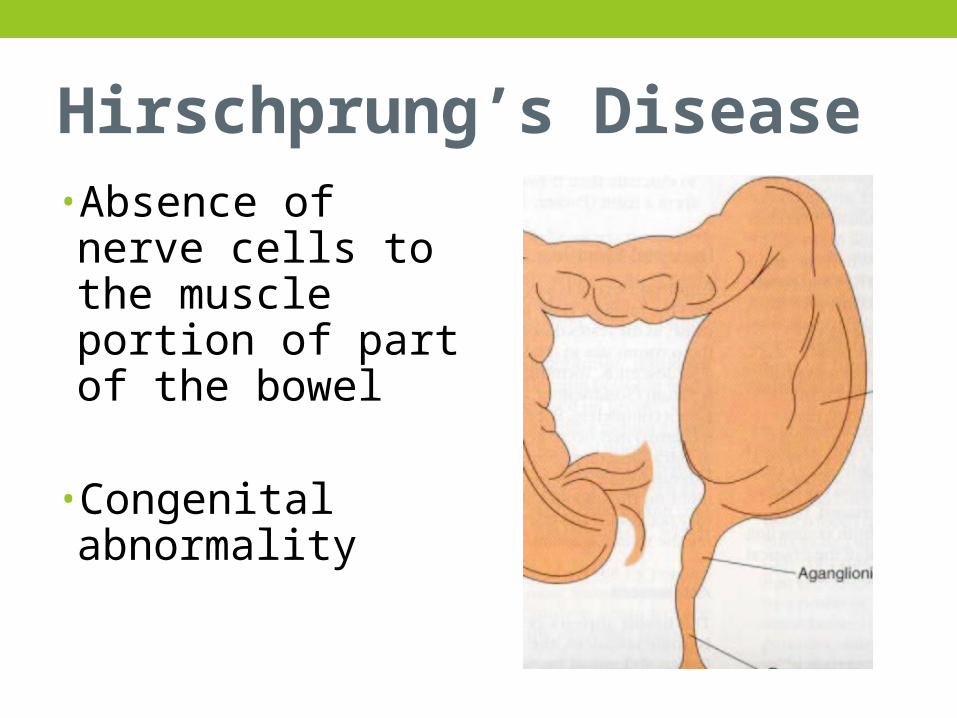
Hirschprung’s Disease• Absence of nerve cells to the muscle portion of part of the bowel
• Congenital abnormality
Symptoms• Symptoms vary according to severity of aganglionic bowel• Severe-symptoms present in newborn• Mild-may not be detected until childhood

Newborns
•Failure to pass meconium•Spitting up, poor feeding•Bile-stained vomit•Abdominal distention

Infancy
•Failure to thrive•Abdominal distention•Constipation and may have
episodes of vomiting and
explosive, watery diarrhea with fever

Childhood
•Chronic constipation•May alternate with diarrhea•Ribbon-like stools•Abdominal distention•Poorly nourished, anemic
Diagnosis•Barium enema, x-ray•Biopsy of intestine (will show lack of nerve enervation)

Treatment• Bowel repair at 12-18 months• Surgery to remove the agaglionic portion of the bowel, 2
parts• Temporary colostomy

Post Op
• NG tube, IV, Foley• Abdominal distention• Assess bowel status• Assess stoma• Small, frequent feedings

Closure of Colostomy• Perineal area is not accustomed to contact with stool. • Provide meticulous skin care, breakdown is very likely. • Teach parents
• change diapers frequently• clean the perineal area carefully• apply a protective barrier at each diaper change.
MALABSORPTION DISORDERS

Celiac disease• Malabsorption syndrome
• Inability to digest gluten leads to toxic levels that damage mucosal cells of small intestine

Signs and Symptoms
• Usually noticed at 9-18 months of age
• Impaired fat absorption (Steatorrhea)
• Behavioral changes (irritability, apathy)
• Impaired absorption of nutrients (malnutrition, abdominal distention, anemia, anorexia, muscle wasting)

Celiac Crisis•Acute, severe, profuse watery diarrhea and vomiting
•May be precipitated by: infections, prolonged fluid and electrolyte depletion, emotional distress
•Corn and rice are the dietary substitutes
•Avoid oats, barley, rye, wheat

Nursing Considerations• Supporting the parents in maintaining a gluten-free diet for
the child for life even when symptom free• Watch for hidden sources of gluten• Assist in maintaining diet in school• Discontinuation of the diet
• risk for growth retardation • Risk of gastrointestinal cancers
INFECTIONS

Intestinal parasites
• Occur most frequently in tropical regions. • Outbreaks take place where:
• Water is not treated• Food is incorrectly prepared• People live in crowded conditions with poor sanitation• Camping• Pets• Sandboxes
Most Common Parasites in Children• Giardiasis• Pinworms

Giardiasis• Transmitted hand-to-mouth
• Cysts are ingested• Passed into the duodenum where they begin actively feeding.• excreted in the stool.
GiardiasisInfants & young children:• Diarrhea, vomiting, anorexia, poor weight gain
Children • Abdominal cramps, intermittent loose stools
(malodorous, watery, pale, greasy), constipation
Treatment Flagyl x 7 days)

Pin Worms• Eggs float in air (easily inhaled)• Worms move on skin and mucous membranes cause intense itching
• As child scratches eggs are deposited under fingernails
• Hand to mouth activity leads to continual reinfection
• Can live on toilet seats, doorknobs, bed linen, underwear, food
Symptoms• Intense rectal itching• Nonspecific symptoms of irritability, poor sleep, bed-wetting, distractibility
• Tape test loop of transparent tape pressed to perianal area for microscopic exam
• Treated with (Vermox) mebendazole

Intestinal parasites
Provide preventative education• good hygiene and health habits.• appropriate sanitation practices I• wash hands after diaper changes, toilet use• deposit soiled diaper in closed receptacle
Acute Gastroenteritis (Diarrhea)• Reabsorption of too little water• Produces diarrhea • Can lead to fluid and electrolyte alterations.• Inflammation of the stomach and intestines• Caused by viral, bacterial, or parasitic infections, or a
chronic problem. • Rotavirus is the leading cause

Symptoms
Mild• A few loose stools each day without evidence of illness
Moderate• Several loose or watery stools daily• Normal or elevated temp• Vomiting• Irritability• No signs of dehydration

DiarrheaSevere•Numerous to continuous stools•Flat affect, lethargic• Irritability•Weak cry• Increased temperature (103-104)•Pulse & respirations weak & rapid

Severe•Depressed fontanels•Sunken eyes, no tears•Poor skin turgor•Pale, cold skin•Urine output decreased• Increased specific gravity•5-15% body weight loss•Metabolic acidosis

Mild to moderate is managed at home
• Assess fluid & electrolyte balance• Rehydration• Maintenance of fluid therapy• Reintroduction of adequate diet (BRAT) Bananas,
Rice, Applesauce, Toast/Tea
Oral rehydration therapy: (Pedialyte)

Severe: requires hospitalization
• Prevent spread to other patients/personnel • Admission weight and daily weight• IV replacement therapyAccurate I&O• Count frequency of bedding & clothing changes
• Weigh diapers (1g = 1ml of fluid)• Monitor specific gravity of urine

Nursing Interventions
•Rest GI tract (NPO)•Assess skin turgor, mucous membranes, fontanel, sensory alterations
•Maintain skin integrity•Stool samples•No rectal temps
PRACTICE QUESTIONS!

The nurse has completed discharge teaching on the dietary regimen of a child with celiac disease. The nurse recognized that client education has been successful when the mother states that the child must comply with the gluten-free diet:
1. Throughout life
2. Until the child achieved developmental milestones
3. Only until symptoms resolved
4. Until child reaches adolescence
An 18-month child with a history of cleft lip and palate has been admitted for palate surgery. The nurse would provide which explanation about why a toothbrush should not be used immediately after surgery?
1. The toothbrush would frighten the child2. The child no longer has deciduous teeth3. The suture line could be interrupted4. The child will be NPO

While gathering admission data on a 2 year old child, the nurse notes all the following abnormal findings. Which finding is related to a diagnosis of Hirschsprung’s disease? (Select all that apply)
1. Bile-stained vomit2. Decreased urine output3. Poor weight gain since birth4. Intermittent sharp pain5. Alternating constipation and diarrhea

A 6-week-old infant is brought to the pediatrician’s office with a history of frequent vomiting after feeding and failure to gain weight. The diagnosis of GER is made and discharge instructions are planned. The nurse should include to teach the parents to:
1. Dilute the formula2. Delay burping3. Change to soy formula4. Position the baby 30-45 degree angle after
feeding

A child who underwent cleft palate repair has just returned form surgery with elbow restraints in place. The parents question why their child must have the restraints. The nurse would give which of the following as the best explanation to the parents?
1. “This device is frequently used postoperatively to protect the IV site”
2. “The restraints will help us maintain proper body alignment”3. “Elbow restraints are used postoperatively to keep the child’s
hand away form the surgical site”4. “The restraints help maintain the child’s NPO status”

The nurse is caring for an infant vomiting secondary to pyloric stenosis. The mother questions why the vomitus of this child’s looks different from that of her other children when they are ill. The nurse would best explain that the emesis of an infant with pyloric stenosis does not contain bile b/c:
1. The GI system is still immature in newborns and infants
2. The obstruction is above the bile duct3. The emesis is from passive regurgitation4. The bile duct is obstructed