Gastric wall endometriosis in a postmenopausal woman · · 2016-12-13The histopathological...
4
Case Report Gastric wall endometriosis in a postmenopausal woman Abdallah A.A. Mohamed a,⇑ , Yasser A.R.M. Selim a,1 , Mazin A. Arif b,2 , Said A. Albroumi b,2 a Radiology Department, Nizwa Hospital, P.O. Box 1222, Nizwa PC 611, Oman b General Surgery Department, Nizwa Hospital, P.O. Box 1222, Nizwa PC 611, Oman article info Article history: Received 11 July 2016 Accepted 14 August 2016 Available online 8 September 2016 Keywords: Endometriosis Postmenopausal Computed tomography Laparotomy abstract Endometriosis is the presence of endometrial tissue outside of the uterus. It is common in women of childbearing age, and is frequently located in the pelvic cavity. Approximately 10% of endometriosis cases occur in extrapelvic locations. However there are few reports of gastric wall endometriosis. Here, we report a rare case of endometriosis in post- menopausal woman. The patient presented with epigastric pain. The investigations included ultrasound (US) and contrast enhanced computed tomography (CECT) where she was diagnosed with gastric wall neoplasm. She underwent surgery where the mass was excised. The histopathological examination surprisingly came with the diagnosis of gastric wall endometriosis. Ó 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier. This is an open access article under the CC BY-NC-ND license (http://creativecom- mons.org/licenses/by-nc-nd/4.0/). 1. Introduction Endometriosis is identified as the presence of endome- trial tissue in an ectopic location outside of the endome- trial cavity. It is a benign chronic gynaecological disorder which may be associated with infertility. The disease is oestrogen-dependent that usually affects women in repro- ductive age. The prevalence of pelvic endometriosis is approximately 6–10% [1]; however, the presence of extrapelvic endometriosis is seen only in 10% of all diagnosed cases. The prevalence of endometriosis in postmenopausal women can affect 2–5% [2] and usually as a side effect of hormonal therapy and it is rare to present in postmenopausal women without history of hormonal therapy [3]. Extrapelvic endometriosis frequently includes the intestines, kidneys, lungs, skin, and pleura [4]. Gastroin- testinal tract (GIT) endometriosis accounts for almost 5% of cases, with the sigmoid colon and rectum being the most commonly affected locations [5]. Here we report a case of gastric endometriosis that pre- sented as a gastric neoplasm in postmenopausal woman with no history of exogenous hormonal therapy. 2. Case report A 60 year old female patient presented with increasing epigastric pain and left loin pain associated with nausea since long time. She is a known hypertensive on regular medications. She has chronic epigastric pain since long time for which she underwent upper GI endoscopy in February 2014 which revealed diffuse gastritis, and the patient received full regimen proton pump inhibitors with little improvement. No family history of special impor- tance. A physical examination revealed mild epigastric and left loin tenderness, not dyspneic or tachypneic. Chest was clear. BP was 130/80 mm/Hg, temperature was 36.8 °C, and her biochemical and haematological markers http://dx.doi.org/10.1016/j.ejrnm.2016.08.005 0378-603X/Ó 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). Peer review under responsibility of The Egyptian Society of Radiology and Nuclear Medicine. ⇑ Corresponding author. Fax: +968 25211914. E-mail addresses: [email protected] (A.A.A. Mohamed), [email protected] (Y.A.R.M. Selim), [email protected] (M.A. Arif), [email protected] (S.A. Albroumi). 1 Fax: +968 25211914. 2 Fax: +968 25211909. The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1783–1786 Contents lists available at ScienceDirect The Egyptian Journal of Radiology and Nuclear Medicine journal homepage: www.sciencedirect.com/locate/ejrnm
Transcript of Gastric wall endometriosis in a postmenopausal woman · · 2016-12-13The histopathological...

The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1783–1786
Contents lists available at ScienceDirect
The Egyptian Journal of Radiology and Nuclear Medicine
journal homepage: www.sciencedirect .com/ locate /e j rnm
Case Report
Gastric wall endometriosis in a postmenopausal woman
http://dx.doi.org/10.1016/j.ejrnm.2016.08.0050378-603X/� 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Peer review under responsibility of The Egyptian Society of Radiology andNuclear Medicine.⇑ Corresponding author. Fax: +968 25211914.
E-mail addresses: [email protected] (A.A.A. Mohamed),[email protected] (Y.A.R.M. Selim), [email protected](M.A. Arif), [email protected] (S.A. Albroumi).
1 Fax: +968 25211914.2 Fax: +968 25211909.
Abdallah A.A. Mohamed a,⇑, Yasser A.R.M. Selim a,1, Mazin A. Arif b,2, Said A. Albroumi b,2
aRadiology Department, Nizwa Hospital, P.O. Box 1222, Nizwa PC 611, OmanbGeneral Surgery Department, Nizwa Hospital, P.O. Box 1222, Nizwa PC 611, Oman
a r t i c l e i n f o
Article history:Received 11 July 2016Accepted 14 August 2016Available online 8 September 2016
Keywords:EndometriosisPostmenopausalComputed tomographyLaparotomy
a b s t r a c t
Endometriosis is the presence of endometrial tissue outside of the uterus. It is common inwomen of childbearing age, and is frequently located in the pelvic cavity. Approximately10% of endometriosis cases occur in extrapelvic locations. However there are few reportsof gastric wall endometriosis. Here, we report a rare case of endometriosis in post-menopausal woman. The patient presented with epigastric pain. The investigationsincluded ultrasound (US) and contrast enhanced computed tomography (CECT) whereshe was diagnosed with gastric wall neoplasm. She underwent surgery where the masswas excised. The histopathological examination surprisingly came with the diagnosis ofgastric wall endometriosis.� 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting byElsevier. This is an open access article under the CC BY-NC-ND license (http://creativecom-
mons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Endometriosis is identified as the presence of endome-trial tissue in an ectopic location outside of the endome-trial cavity. It is a benign chronic gynaecological disorderwhich may be associated with infertility. The disease isoestrogen-dependent that usually affects women in repro-ductive age. The prevalence of pelvic endometriosis isapproximately 6–10% [1]; however, the presence ofextrapelvic endometriosis is seen only in 10% of alldiagnosed cases. The prevalence of endometriosis inpostmenopausal women can affect 2–5% [2] and usuallyas a side effect of hormonal therapy and it is rare to presentin postmenopausal women without history of hormonaltherapy [3].
Extrapelvic endometriosis frequently includes theintestines, kidneys, lungs, skin, and pleura [4]. Gastroin-testinal tract (GIT) endometriosis accounts for almost 5%of cases, with the sigmoid colon and rectum being the mostcommonly affected locations [5].
Here we report a case of gastric endometriosis that pre-sented as a gastric neoplasm in postmenopausal womanwith no history of exogenous hormonal therapy.
2. Case report
A 60 year old female patient presented with increasingepigastric pain and left loin pain associated with nauseasince long time. She is a known hypertensive on regularmedications. She has chronic epigastric pain since longtime for which she underwent upper GI endoscopy inFebruary 2014 which revealed diffuse gastritis, and thepatient received full regimen proton pump inhibitors withlittle improvement. No family history of special impor-tance. A physical examination revealed mild epigastricand left loin tenderness, not dyspneic or tachypneic. Chestwas clear. BP was 130/80 mm/Hg, temperature was36.8 �C, and her biochemical and haematological markers

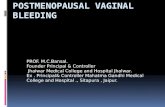
Fig. 1. CECT of the abdomen and pelvis in coronal plan, shows gastricantral wall mass lesion with inhomogeneous enhancement.
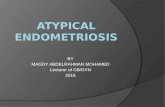
Fig. 2. CECT of the abdomen and pelvis in sagittal plan, shows gastricantral wall mass lesion with inhomogeneous enhancement.
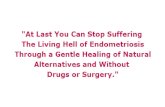
Fig. 3. CECT of the abdomen and pelvis in coronal reformat, shows leftlower ureteric stone with subsequent moderate hydroureteronephrosis.
1784 A.A.A. Mohamed et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1783–1786
were within normal limits. Abdominal ultrasonographyshowed gastric antral mass lesion and left ureteric stoneassociated with moderate hydroureteronephrosis. CECT ofthe abdomen and pelvis was performed which revealed a
large, irregular, inhomogeneously enhancing soft tissuemass involving the inferior wall of the gastric antrum withlarge exophytic component and few satellite nodules withpossible involvement of transverse colon. The mass mea-sures 4.5 cm � 6.5 cm � 4.5 cm. The impression suggestedgastrointestinal stromal tumour (GIST) and Desmoidtumour on top of differential diagnosis [Figs. 1 and 2]. Also,a left lower ureteric stone with subsequent moderatehydroureteronephrosis was noted [Fig. 3].
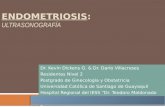
The patient underwent exploratory laparotomy whereexcision of the mass with sleeve gastrectomy of the greatercurvature together with partial transverse colectomy fol-lowed by resection anastomosis of the two colonic ends.The excised surgical specimen was 8 cm � 5 cm. Therewere also three satellite lesions in the greater omentumwhich had been removed with the specimen [Fig. 4].
Histopathological examination revealed extensive areasof haemorrhage and haemorrhagic necrosis. These are sep-arated and bordered by proliferation of spindle cells andadmixture of foamy macrophages and haemosiderin ladenmacrophages. Scanty lymphoid cells are also seen [Fig. 5].The lesion is seen extending up to the serosa of the stom-ach and the colon with serositis. The spindle cells stainpositively with CD 10 and SMA [Fig. 6]. They are negativefor CD 117, desmin, S-100 and CD34. The diagnosis basedon morphological and immunohistochemical featuresfavours endometriosis.
3. Discussion
Endometriosis is the presence of endometrial tissue inan ectopic location outside of the endometrial cavity. It is

Fig. 4. Surgical specimen after resection of the mass lesion.
Fig. 5. H&E stain showing evidence of old and recent haemorrhage.
Fig. 6. Histopathology specimen with CD10 immuno-marker.
A.A.A. Mohamed et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1783–1786 1785
a benign chronic gynaecological disorder which may becomplicated by infertility. The disease is oestrogen-dependent that usually affects women in childbearing
period. The prevalence of pelvic endometriosis isapproximately 6–10% [1]. However the presence ofextrapelvic endometriosis is seen only in 10% of all cases.

1786 A.A.A. Mohamed et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1783–1786
The prevalence of endometriosis in postmenopausalwomen is a rare condition and may affect 2–5% [2] andusually as a side effect of hormonal therapy and it is evenrarer to present in postmenopausal women without his-tory of hormonal therapy [3]. It was first reported in 1950.
Frequent locations of extrapelvic endometriosis includethe intestines, kidneys, lungs, skin, and pleura. GITendometriosis accounts for almost 5% of cases, with thesigmoid colon and rectum being the most commonlyaffected locations [5].
The pathogenesis of endometriosis still unclear, how-ever, several theories to explain the pathogenesis weresuggested which include; coelomic metaplasia whichmay be caused by inflammation and hormonal effect, andthis theory may explain the pathogenesis of the diseasefollowing hysterectomy, in postmenopausal women andin women with uterine agenesis [6,7]. Another theory isendometrial stem cells implantation from vascularendometrial cell transportation, and this theory mayexplain extra pelvic endometriosis [8,9].
The present case is a very rare case of extrapelvic, gas-tric wall endometriosis that occurred in a postmenopausalwoman. The exact pathogenesis of the disease is not clearespecially with no previous history of exogenous hormonaltherapy.
Gastrointestinal endometriosis is usually asymp-tomatic, but may present with abdominal pain, nausea,vomiting, obstruction, or intussusceptions. The most com-mon locations are the sigmoid colon and the rectum. Gas-tric wall endometriosis is the rarest to occur and only fewcases have been reported. In almost all cases of extrapelvicendometriosis, surgical resection of the lesion is the treat-ment of choice [10]. Surgical resection usually results incomplete cure in up to 95% of patients with no recurrence.Only recurrence rate was 4.3% following surgery.
The patient presented here with typical pain of gastritis,especially with her previous medical history of gastritisand upper GI endoscopy.
The case we report endometriosis was not a part of thedifferential diagnosis and the proposed differential wereGIST and desmoid tumour. Surprisingly the postoperativetissue histopathological examination confirmed extrapel-vic gastric wall endometriosis.
4. Conclusion
Extrapelvic endometriosis is rare and can affect unusualsites. Gastric wall endometriosis is extremely rare in apostmenopausal woman, it may mimic gastric wall neo-plasm and it should be included in the differential diagno-sis of gastric masses in women with chronic and cyclicepigastric pain.
Disclosure
We declare no conflict of interests prior and duringpreparation of this paper.
Acknowledgments
We would like to thank the staff of histopathologydepartment at the Royal Hospital, Muscat, Oman for theircontribution.
References
[1] Dabrosin C, Gyorffy S, Margetts P, Ross C, Gauldie J. Therapeuticeffect of angiostatin gene transfer in a murine model ofendometriosis. Am. J. Pathol. 2002;161:909–18.
[2] Punnonen R, Klemi PJ, Nikkanen V. Postmenopausal endometriosis.Eur. J. Obstet. Gynecol. Reprod. Biol. 1980;11:195–200.
[3] Goumenou AG, Chow C, Taylor A, Magos A. Endometriosis arisingduring oestrogen and testosterone treatment 17 years afterabdominal hysterectomy: a case report. Maturitas 2003;46:239–41.
[4] Fernández Vozmediano JM, Armario Hita JC, Cuevas Santos J.Cutaneous endometriosis. Int. J. Dermatol. 2010;49:1410–2.
[5] Kanthimathinathan V, Elakkary E, Bleibel W, Kuwajerwala N,Conjeevaram S, Tootla F. Endometrioma of the large bowel. Dig.Dis. Sci. 2007;52:767–9.
[6] Ridley JH. The histogenesis of endometriosis: a review of facts andfancies. Obstet Gynecol Surv 1968;23:1–35.
[7] Rock JA, Markham SM. Pathogenesis of endometriosis. Lancet1992;340:1264–7.
[8] Douglas C, Rotimi O. Extragenital endometriosis. aclinicopathological review of a Glasgow hospital experience withcase illustrations. J. Obstet. Gynaecol. 2004;24:804–8.
[9] Veeraswamy A, Lewis M, Mann A, Kotikela S, Hajhosseini B, Nezhat C.Extragenital endometriosis. Clin. Obstet. Gynecol. 2010;53:449–66.
[10] Blanco RG, Parithivel VS, Shah AK, Gumbs MA, Schein M, Gerst PH.Abdominal wall endometriomas. Am. J. Surg. 2003;185:596–8.