Galveston Area Ambulance Authority Medical Protocols
163
Galveston Area Ambulance Authority Medical Protocols
Transcript of Galveston Area Ambulance Authority Medical Protocols
Galveston Area Ambulance Authority
Medical Protocols

James Vincent M.D. Page 1
Medical Protocols
The Galveston Area Ambulance Authority(GAAA) Treatment Protocols are for the sole use of providers
that are providing care under the authority of GAAA or while deployed by GAAA in a disaster situation.
These protocols are valid from March 1, 2017 through March 31, 2018.
The GAAA protocols were written using the guidance of medical research and following accepted
national standards. The protocols were written by a committee of practicing paramedics at GAAA after
lengthy research and debate. The protocols were approved by Dr. James Vincent, medical director for
GAAA. This document is based upon current accepted medical practice and evidence. Due to the
evolving nature of medical standards this document is not a static piece of paper but is expected to be
used and revised as a dynamic document.
These protocols are a tool that providers will use with their assessment, knowledge, and experience to
provide exceptional patient care. Protocols are not meant to be blindly followed; instead providers
should understand the rationale behind the protocol pathways. All pathways are to be utilized only to
the degree that the patient requires. The pathways in the flowchart are used to facilitate the most
appropriate level of care for the patient. If a patient’s status does not require a certain pathway, it is
acceptable to omit or skip the treatment. Protocols are written for specific sets of symptoms and
conditions and can be combined in order to address the patient’s needs and complaints. The committee
and the medical director at GAAA recognize that in certain circumstances deviation from the protocols is
in the best interest of the patient. Protocol deviations should be a rare event and require detailed
documentation.
GAAA services a large area of Galveston County with multiple providers of various certification and
licensure levels. GAAA also utilizes first responders in the majority of our response districts and provides
non-emergency and emergency transfers originating in Galveston County and surrounding areas. With
the exception of Beach Patrol providers who are trained in the use of blind airway devices and basic first
aid, these protocols are not meant to provide authorization for providers outside of the GAAA system.
Any questions regarding who can practice under these guidelines should be referred to GAAA SOGs.
James Stephen Vincent M.D.
Medical Director

James Vincent M.D. Page 2
Medical Protocols
January 1, 2017
GAAA Field Staff:
I have been made aware of impending shortages of normal saline supplies, due to national shortages. In
the setting of limited supplies:
1. Do not give IV fluids indiscriminately or “reflexively” for any patient.
Consider holding IV fluids EXCEEPT for patients with a known or suspected volume-depleted
state.
2. Lactated Ringers (LR) may be used as a substitute for NS throughout the protocols when
indicated. As LR may be detrimental to patients in a shock or hypoperfusion state, carefully
weigh the risks of aggressive LR use, versus holding fluids and/or optimizing transport time to
the hospital, in these patients.
James Vincent, MD
Medical Director, GAAA
James Stephen Vincent M.D.
Medical Director
James Vincent M.D. Page 3
Medical Protocols
Fundamentals of Care
Patient Assessment 8
Documentation Guidelines 11
General System Guidelines 13
Air Medical Activation Guidelines 15
Specialty Care 17
On-Scene Medical Providers 18
Selected Age Definitions, Competency 19
Types of Consent 20
Treatment of Minors 21
Restraint / Transport against Patient Will 22
Refusals 23
Termination of CPR 24
Out of Hospital DNR 26
Hospice Patients 28
Scope of Practice 29
Inter-Facility Transfers 31
Expired Medications and Medication Shortages 34
Ebola Preparedness 35
Universal Treatment
Universal Treatment Guidelines 40
Rapid Sequence Induction 41
Failed Airway 42
James Vincent M.D. Page 4
Medical Protocols
Pain Management 43
Police Custody 44
Medical
Allergic Reaction 45
Anxiety 46
Behavioral Emergencies 47
Excited Delirium 48
COPD / Asthma 49
Diabetic Emergency 50
Hypotension 51
Nausea / Vomiting 52
Overdose 53
Respiratory Distress 54
Seizure 55
Stroke / CVA 56
Syncope 57
Cardiac
Acute Coronary Syndrome 58
Supra-Ventricular Tachycardia 60
A-Fib with RVR 61
Ventricular Tachycardia with a Pulse 62
Symptomatic Bradycardia 63
Adult Cardiac Arrest 64
Post Resuscitation 65
Post Resuscitation Induced Hypothermia 66

James Vincent M.D. Page 5
Medical Protocols
Hypertension 67
Congestive Heart Failure 68
Trauma
Selective Spinal Immobilization 69
Crush Injury 70
Major Trauma 71
Extremity Trauma 72
Extremity Hemorrhage or Amputation 73
Burns – Electrical / Chemical 74
Burns – Thermal 75
Marine Life Envenomation 76
Snake Bite 77
Drowning / Near Drowning 78
Pediatric
Active Labor 79
OB Emergencies 80
Neonatal Resuscitation 82
Pediatric Cardiac Arrest 83
Pediatric Diabetic Emergencies 84
Pediatric Pain Management 85
Pediatric Allergic Reaction 86
Pediatric Seizure 87
Pediatric Respiratory Distress 88
Pediatric Bradycardia 89
Pediatric Supra-Ventricular Tachycardia 90

James Vincent M.D. Page 6
Medical Protocols
Procedures
Capnography 91
Child Birth 94
CPAP 95
EZ-IO Intraosseous Infusion 96
Infection Control 98
Kendrick Extrication Device 99
King LTS Airway 100
Nasogastric / Orogastric Tube Insertion 101
Oral Tracheal Intubation 102
Needle Decompression 103
Spinal Immobilization 105
Taser Barb Removal 106
Injection: Subcutaneous / Intramuscular 107
Surgical Airway: Cricothyrotomy 109
Surgical Airway: Quick Trach 110
Tourniquet 111
Traction Splint 112
Transfers – Air Medical 113
Transfers – Trauma 114
Venti-Pac 117
Appendix A – Medication Formulary 118
Appendix B – Equipment List 159
James Vincent M.D. Page 7
Medical Protocols
EMT Basic Procedure-
EMT Basic Drug Administration-
EMT Intermediate Procedure-
EMT Intermediate Drug Administration-
Paramedic Procedure-
Paramedic Drug Administration-
See Protocol-
Important Note Regarding Protocol-
Pediatric Protocol Note-
James Vincent M.D. Page 8
Medical Protocols
Patient Assessment
A systematic approach to patient assessment allows for high quality and safe care that will be consistent
between providers and across a wide variety of patient encounters. The following outlines the expected
framework for the assessment, treatment, and communication which should occur for EVERY patient
encounter:
Primary Survey
1. Airway - is it patent? Identify and correct existing or potential obstruction, inclusive of advanced airway management as indicated.
2. Breathing - rate and quality. Identify and correct existing or potential compromising factors 3. Circulation – pulse, rate, quality, and location. Control external bleeding.
4. Determine level of consciousness (use AVPU system, Glasgow Coma Scale, or other system as indicated).
Secondary Survey
1. Reassure the patient and keep him/her informed about treatment. 2. Obtain a brief history from the patient, family and bystanders. Check for medical identification. 3. Perform a head-to-toe assessment.
4. Obtain and record vital signs as indicated by patient condition, to include heart rate, blood pressure (indicating patient’s position), respiratory rate, temperature (measured in degrees Celsius), skin color, cardiac monitor, blood glucose, SaO2 and ETCO2.
Treatment
Treat appropriately in order of priority. Refer to specific protocol.
Communications
1. Radio or telephone information protocol during transport. a. Identify transporting unit. b. Patient's age and sex. c. Chief complaint or problem. d. Pertinent history as needed to clarify problem (medications, illnesses, allergies, mechanism
of injury, etc.). e. Physical assessment findings. f. Vital signs and level of consciousness. g. Treatment given and patient's response. h. Estimated time of arrival (ETA).
2. Advise ED of changes in patient's condition during transportation.
3. Give a verbal report to ED nurse and/or physician on arrival.
4. Complete electronic patient care report (e-PCR). See following section for further details.

James Vincent M.D. Page 9
Medical Protocols
Cardiac Monitoring
1. Patients experiencing possible cardiac symptoms must have a 12 lead EKG within 5 minutes of patient contact whenever possible. Refer to the appropriate protocol for specific treatment. (12 lead EKG is appropriate prior to and post administration of medications, tracings should be
attached to the e-PCR)
Indications for 12 Lead Monitoring
Chest Pain or discomfort (radiating or non-radiating)
Congestive Heart Failure (CHF)
Syncope or near Syncope
Unconscious
Respiratory distress in patients >18 years of age
Chest Trauma (blunt or penetrating)
Non Traumatic GI bleeding
Overdose
CVA and or HTN
Female >50 years presenting with abdominal arm or neck pain.
Hypertension or Hypotension
Altered Mental Status
Post Resuscitation
2. Rhythms, dysrhythmias and 12-lead EKG's are to be documented and recorded as part of the patient’s record. A hard copy of the 12-lead EKG shall be made:
a. The 12 Lead ECG must be uploaded and attached to the patients ESO e-PCR when possible.
b. If/when electronic attachment is not possible due to technology failure, a paper copy must be made and routed to the Mid County Annex EMS office and filed in patient records.
c. The 12 lead must include;
i. The call run number
ii. Patient name
iii. Age
iv. Date of service
v. Receiving hospital

James Vincent M.D. Page 10
Medical Protocols
Respiratory Status Monitoring
Patients presenting with respiratory distress of any etiology should be assessed treated and monitored
throughout treatment and transport. End Tidal CO2 (ETCO2) monitoring is the gold standard and should
be utilized with these patients when available. SaO2 monitoring may be substituted when ETCO2
monitoring is not available.
The goal is to maintain ETCO2 between 35 - 45 mm/Hg and SaO2 at 97% or more.
Guidelines for Treatment of Respiratory Distress:
1. Oxygen Therapy. Consider limiting to 3 liters per minute in COPD or be prepared to actively support ventilation.
2. Consider intubation, CPAP, or bag valve mask/ventilation as indicated by the patient’s condition.
3. Obtain IV/IO access.
4. Position of comfort, generally sitting if adequate blood pressure.
5. See specific protocols for further details and interventions.
6. Special Considerations:
1. Rule out obstruction.
2. Listen to lung sounds for presence of:
a. Rales, rhonchi, or wheezes.
b. Accentuated or diminished lung sounds.
3. Obtain pre and post treatment ETCO2 and or SaO2 and document in e-PCR.

James Vincent M.D. Page 11
Medical Protocols
Documentation Guidelines
While our first and most important job is to provide patient care, all patient care and assessments must
be accurately recorded. This includes the patient s primary complaint; the patient’s presenting signs
and symptoms (assessment); and all treatments and interventions, both attempted and successful.
Deviations from protocol must also be documented, to include the reason the deviation occurred.
Protocol deviation narrative should also include the method used to notify supervising staff and/or the
medical director.
High-risk medicolegal situations require additional and thorough narrative, such as cases involving: an
unexpected death in the field or death of a young person; a prolonged resuscitation; a complex multi-
casualty incident with multiple patients and involvement of outside services; situations where law
enforcement personnel are also on scene due to violence or other civil disturbances; or cases when the
patient or family are visibly displeased with care provided. Additional details are useful to hospital-
based providers, are important during quality reviews, and may confer protection in the case of a
lawsuit.
All patient care reports (PCR’s) must be completed by the end of shift.
There are 5 main reasons to document EMS call Clinical, Legal, Operational, Financial, and Compliance.
10 items that must be in ePCRs
1. Times and dates: Make sure that all times and dates are recorded and correct.
2. Addresses of scene and destination: should include city and county.
3. Patient’s complaint on arrival: What was the patient’s primary complaint? Use patients own
words to describe the complaint when possible. Patient describes pain as “Crushing sensation in
the center of chest”.
4. Patient assessment: A primary assessment, including vital signs, must be completed on every
patient contact. This includes transports and patient refusals. All refusals’ need to 2 sets of vital
signs.
5. Patient demographics: Accurately record patient’s name, mailing address, DOB, SSN, and
telephone number. If unable to ascertain the patient’s name, state is requiring that UNKNOWN,
UNKNOWN for both last and first name.
6. Patient history, medications, and allergies: Obtain a list of the patient’s past medical history, all
medications taken by patients and list any allergies.
7. Treatments: A complete listing of all interventions and medications including time given. How
did patient response to treatment? Be sure to include both successful and unsuccessful
attempts. Including movement of patient. ( draw sheet, S.L.I.P., or bariatric equipment used)
8. Billing information: Every attempt should be made to obtain the patients insurance
information. Ask for a face sheet at the ER or get a copy made of insurance card.
9. Mileage: Total loaded mileage must be documented on every transport.

James Vincent M.D. Page 12
Medical Protocols
10. Signatures: A signature is required for all patients. If patient is unable to sign, a family member
of care giver can sign for patient. If a family member or care giver is not available, you will need
to note why patient is unable to sign, for example “patient is unable to sign due to AMS”.
ePCRs Specialty Patient Section
The following six sub-sections forward important data to GAAA QA and DSHS:
1. Cincinnati Stroke Scale 2. Obstetrical 3. Spinal Immobilization 4. Burns 5. CPR 6. Motor Vehicle Collision
Non-Emergency Transfers
In addition to the above guidelines, non-emergency transfers require additional documentation
specifying why the patient requires a stretcher. Relevant history, exam, and past medical history items
which support the patient’s condition as being bed-confined or non-ambulatory should be included. All
of the following must be attested and documented:
1. Unable to get up from bed without assistance, and
2. Unable to ambulate, and
3. Unable to sit in a chair or wheel chair,
4. Unable to maintain oxygenation without assistance.
Common Documentation Errors
Spelling and grammar (i.e. capital letters, punctuations, and complete sentences) are extremely
important components of the patient care narrative, both for professionalism and medicolegal reasons.
Do not use unapproved abbreviations. Most abbreviations are upper and lower case sensitive. If you are not sure whether an abbreviation is acceptable or not, write it out. Unacceptable Acceptable Abbreviation for PT Pt. Patient CC Write out Chief complaint AOS Write out Arrived on scene Cp CP Chest pain MSO MSO4 Morphine Sulfate
If you give treatment to a patient like a public assist, or bandage a wound you must fill out an ePCR.
All refusals must have 2 sets of vital signs, and document that you have explained the possible
consequences of the patient not seeking medical attention.

James Vincent M.D. Page 13
Medical Protocols
General System Guidelines
Transfer of Care to a Provider of a lower skill level
Leaving patients on-scene should not be a routine procedure. It is to be considered only when a patient requires immediate transport in order to maximize potential outcome.
The transport provider may transfer patient care to a provider of a lower skill level while
awaiting additional transport resources when transfer of established care is not beyond the
scope and/or training of the provider.
When a patient presents without need for MICU level care and a BLS/ALS unit is available,
patient care may be transferred at the discretion of the on-duty shift supervisor.
Mass and multi-casualty incident transport decisions will be made by the transport officer.
Cancellation or Alteration of a Response
Units may not respond non-emergency to a call for service for the sole reason that the caller
requests “No Lights and Sirens.”
Police, fire and other first responders can disregard responding units, but may not do so in order
to contact another transport provider.
Off-duty GAAA providers may downgrade or disregard responding units.
Dispatch may not disregard units when a caller requests EMS cancel their response; the
responding units must continue to the scene.
Mutual Aid:
When providers are requested to respond through an official channel for mutual aid; these
protocols remain in effect.
If a provider is dispatched on a radio channel separate from GAAA’s primary radio channel, the
responding unit must advise GAAA dispatch and the on-duty supervisor that they are responding
to a mutual aid request.
Level of Response to 9-11 Calls
Emergency traffic is the use of lights and sirens to respond to a location.
Non-emergency traffic is traveling without the use of emergency lighting or warning devices.
GAAA does not operate utilizing a tiered or EMD system.
When responding to emergency calls responders should use emergency traffic unless
downgraded or otherwise directed.
Providers may respond non-emergency to certain types of calls:
o Calls that are dispatched as a public assist without injuries
o Calls that require staging for scene safety and the provider can make the location in less
than 7 minutes driving non-emergency.
o Calls that are requested to incoming vessels or aircraft that have a known ETA that is

James Vincent M.D. Page 14
Medical Protocols
provided by dispatch and that the crew can make location prior to the arrival of the
vessel or aircraft.
o When directed to do so by the on duty supervisor.
On-Line Medical Consultation (OLMC): Providers have several options for OLMC:
Contact the receiving facility where the patient is being transported and speak with an ER
physician.
Contact the GAAA medical director, Dr. James Vincent.
At certain times it may be appropriate to contact the patient’s regular treating physician.
For inter-facility transports the provider should obtain written orders specific to the patient for
any treatments that are outside the provider’s standard scope of practice.
Nurses and other ancillary staff may not give providers treatment orders.
Once OLMC has been established the provider should follow the orders given by the physician that is
assuming care of the patient. However in cases that the provider feels the prescribed treatment would
violate accepted medical standards, supervisory guidance should be requested and the provider should
not follow those directives that may cause harm to the patient. In the event of a disaster situation or
other extreme circumstance, even if expressly directed by an OLMC physician, providers are prohibited
from performing field C-sections or field amputations.
Flight Operations: GAAA responds when dispatched to PHI out of Scholes field to provide medical care
to offshore locations such as ships and oil-rigs in the Gulf of Mexico. Providers may transport to a
variety of facilities along the US Gulf Coast.
For safety, GAAA providers are required to wear long pants and boots on all flights.
Additional equipment is located in the supply lockers at Scholes field in the PHI terminal.
Flight physiology will affect patient’s condition and require differing techniques to care for the
patient than ground based transport.
o Patients may require supplemental oxygen
o IV fluids will not flow in the absence of pressure infusers
o Entrapped air may expand in the patient’s body cavities.
OLMC is typically not available for providers responding off-shore; so Team Captains are
required on all flights.
If the shift supervisor is required to maintain system status by sending a non-team captain
paramedic on an offshore flight, that provider is permitted to utilize all treatment pathways,
including those at Team Captain level skills.

James Vincent M.D. Page 15
Medical Protocols
Air Medical Activation Guidelines
Overview: Air medical transport is an important adjunct to the overall care of the severely ill or injured patient. Air medical provider (AMP) resources should be utilized in accordance with the regional trauma plan. Purpose: These AMP activation guidelines are intended to provide a framework for each RAC to develop a standardized method for ground emergency medical service providers to request a scene response by an AMP, to reduce delays in providing optimal care for severely ill or injured patients, and to decrease mortality and morbidity. Decision Criteria: AMP activation/scene response should be considered when it can reduce transportation time for severely ill or injured patients meeting activation criteria. Should there be any question whether or not to activate regional AMP resources, on-line or receiving facility medical control should be consulted for a final decision. Guidelines for Activation:
1. The ground emergency medical service provider may, when one or more of the elements of the activation criteria exist, request a scene response by an AMP and assist with transportation to an appropriate acute care facility.
2. Ground emergency medical service providers should not remain on scene awaiting AMP arrival if ground transport time will be less than the combined arrival and return time of the AMP.
3. Ground emergency medical service providers should activate the AMP as early as possible, including prior to their arrival at the scene if the mechanism of injury or scene report meets criteria.
4. The EMS provider should comply with RAC-approved triage criteria (such as that listed below) to activate AMP transport.
5. Other factors that should be considered are: a) Location of incident b) Number of patients c) Age of patients d) The total AMP response time (response time+ scene time +transport time) will
result in delivery of the patient(s) to the most appropriate facility faster than transport by ground ambulance.
e) Weight of patients f) AMP activation will provide access to advanced life support interventions critical for
patient survival that are not available on scene (and more quickly than ground EMS can arrive at the nearest hospital).
g) Special circumstances & patient injuries (transport of suspected spinal injury over rough terrain) where patient outcome would be improved by AMP transport.
6. In all instances the available AMP that best meets the needs of the patient will be utilized.
Other considerations: Trauma patients meeting criteria for AMP dispatch should be transported to a Level I, II, or III Trauma Center. Severely ill medical patients should be transported to the nearest appropriate acute care facility.

James Vincent M.D. Page 16
Medical Protocols
Air Medical Activation Criteria:
1. Severely injured or ill patients located in a remote or off-road area not readily accessible to ground ambulance.
2. Ground resources with acceptable response time exhausted or exceeded in the region. 3. Reduction in transport time to a trauma center compared to ground transport for the
seriously injured trauma patient. 4. Motor vehicle collisions involving:
a. Ejection b. Rollover c. Death in same patient compartment d. Patient extrication of 20 minutes or greater
5. Falls from a distance of greater than 20 feet 6. Auto-pedestrian injury with significant impact (> 20 mph) 7. Physiologic:
a. Glasgow Coma Scale of less than 10 b. Systolic blood pressure of < 90 with signs/symptoms of shock
8. Anatomic: a) All penetrating injuries to the head, neck, torso, and/or extremities proximal to the
elbow and knee b) All penetrating injuries to the head, neck, torso, and/or extremities proximal to the
elbow and knee c) Flail chest d) Combination trauma with burns of 20% involving face or inhalation injuries e) Major burns including:
i. Inhalation ii. 2nd or 3rd degree burns > 20% BSA iii. Combination trauma with burns
f) Two or more proximal long-bone fractures g) Pelvic fractures h) Traumatic paralysis i) Amputation proximal to the wrist or elbow j) Depressed or open skull fractures
9. Multiple severely injured patients on scene 10. No available trauma center within one hour of ground transportation.
James Vincent M.D. Page 17
Medical Protocols
Specialty Care:
T r a n s p o r t decisions for specialty problems such as Trauma, Stroke, ACS/STEMI, Pediatric Care
and Burns will be made with attention to local hospital and regional protocols. Evidence-based
support fueling national quality initiatives to bring a patient to a certified/accredited specialty
center will be weighed against the need to bring a critically unstable patient to the closest
available facility.
Trauma: Patients with acute traumatic injuries will be transported to an appropriate
Trauma Center per RAC guidelines. (See “Transfers – Trauma” under Procedures Section).
Local Stroke Resources: Patients presenting with acute stroke symptoms less than 6 hours
in onset will be preferentially taken to a stroke center when possible. Air medical
transport may be considered for select patients with symptom onset less than 2 hours in
order to facilitate time-dependent lytic therapy.
ACS/STEMI: Patients experiencing acute STEMI are best managed in facilities with active
cath lab programs and should be preferentially taken to these centers. The receiving
hospital emergency department physician should be notified while en route. The field EKG
demonstrating the STEMI should be transmitted electronically to the receiving hospital
when possible, in order to facilitate activation of the cath lab before arrival when
appropriate.
Pediatric Care: Children with critical illness or injury and children with chronic underlying
medical conditions should be preferentially transported to a facility capable of caring for
the child’s critical illness or special needs. The parents should be enlisted to assist with
destination decisions whenever possible.
Burn Care: Patients fulfilling criteria for major burns (see burn care protocol) should be
transported to a burn center whenever possible.

James Vincent M.D. Page 18
Medical Protocols
On-Scene Medical Providers:
(Per the Texas State Board of Medical Examiners (TSBME), the licensing body for physicians in Texas.)
Control at the scene of a medical emergency shall be the responsibility of the individual in attendance
who is most appropriately trained and knowledgeable in providing prehospital emergency stabilization
and transport.
Physician On-Scene/General Guidelines The credentialed provider on-scene is responsible for management of the
patient(s) and acts as the agent of the medical director or OLMC. In order to participate in care physicians must present a valid Texas Board of
Medical Examiner’s License (all physicians are issued a wallet card) or be recognized as a physician by the provider.
Patient’s Personal Physician On-Scene If the patient's personal physician is present and assumes care, the provider
should defer to the patient’s personal physician. That physician shall provide the provider with written orders if they deviate from this document.
If there is a serious disagreement between the patient’s personal physician and
the system SOGs, the physician shall be placed in direct communication with
OLMC. If the patient’s personal physician and the on-line physician disagree on
treatment, the patient’s personal physician must either continue to provide
direct patient care and accompany the patient to the hospital, or must defer all
remaining care to the on-line physician. Intervener Physician On-Scene
If an intervener physician is present at the scene, has been satisfactorily identified as a licensed physician (by showing a valid copy of his/her Texas medical license), and expressed willingness to assume responsibility for care of the patient, OLMC should be contacted. The on-line physician has the option to:
manage the case exclusively work with the intervener physician allow the intervener physician to assume complete responsibility for the
patient If there is a disagreement between the intervener physician and OLMC, the
provider will take direction from the on-line physician and place the intervener physician in contact with the on-line physician.
The intervener physician must document his or her interventions and/or orders on the EMS patient care record.
The decision of the intervener physician to not accompany the patient to the hospital shall be made with the approval of the on-line physician.
James Vincent M.D. Page 19
Medical Protocols
Selected Age Definitions:
Adult: A patient that is over the age of 18 years of age.
Minor: A patient under the age of 18.
Pediatric patient: For treatment purposes only. Any patient that has not reached puberty or is able to fit on a Broselow tape
Competency: Mental competency: This is a legal definition and refers to the presumption that a patient is legally mentally competent unless a court of law has judged them to be incompetent. Present mental capacity: refers to a patient’s current mental ability to understand and appreciate the nature and consequences of his/her condition and to make rational treatment decisions. Determination of competency involves consideration of the following:
Adult patients.
Alert, able to communicate, and demonstrates appropriate cognitive skills for the circumstances of the situation.
Showing no indication of impairment by alcohol or drug use.
Showing no current evidence of suicidal ideations, suicide attempts or any indication that they may be a danger to themselves or others. Law enforcement must be requested for this patient population.
A law enforcement officer may arrest a patient who threatens or attempts suicide under Texas Health and Safety Code Section 573.001. The statute also covers other mentally ill patients and a similar statute allows an arrest for chemical dependency. Remember though, only a law enforcement officer can make these arrests.
Showing no current evidence of bizarre/psychotic thoughts and/or behavior, or displaying behavior that is inconsistent with the circumstances of the situation.
No physical finding or evidence of illness or injury that may impair their ability to understand and evaluate their current situation (for example, a patient with a head injury and an abnormal GCS, a patient with significant hypoxia or hypotension, etc.).
A patient that has NOT been declared legally incompetent by a court of law.
If a patient has been declared legally incompetent, his/her court appointed guardian has the right to consent to or refuse evaluation, treatment, and/or transportation for the patient.

James Vincent M.D. Page 20
Medical Protocols
Types of Consent
Informed Consent: This is the legal standard regarding the process in which the patient refuses or consents to medical care.
o The patient is competent and able to make a decision about their medical care. o The patient is given all the necessary information a reasonable person would require to
make the decision including: risks, benefits and alternatives o The patient is capable of deliberating and communicating their choice.
Implied Consent: This type of consent regards the legal standard for consent during a life-threatening emergency. Patients must be:
o Unable to communicate because of an injury, accident, illness, or unconsciousness and suffering from what reasonably appears to be a life-threatening injury or illness
o OR suffering from impaired present mental capacity o OR a minor who is suffering from what appears to be a life-threatening injury or illness
and whose parents, guardians or managing or possessory conservator are not present. o Patients who are not mentally competent or have an impaired present mental capacity.
The latter case will generally require law enforcement assistance.
Substituted Consent: When another person consents for the patient such as for minors, incapacitated patients, incarcerated patients and those who have been deemed by a court of law to be legally incompetent.

James Vincent M.D. Page 21
Medical Protocols
Consent and Treatment of Minors
A minor is able to consent or refuse medical care in a limited set of circumstances in Texas.
Emancipation: This requires a court order in the state of Texas.
Minors who are on active military duty with the US Military
When consenting to the diagnosis and treatment of an infectious, contagious, or communicable disease that is required by law or rule to be reported by the licensed physician or dentist to a local health officer or the Texas Department of State Health Services
Is consenting to examination and treatment for drug or chemical addiction, drug or chemical dependency, or any other condition directly related to drug or chemical use
A minor can consent to counseling for suicide prevention, chemical addiction or
dependency, or sexual, physical or emotional abuse Minors who are married are considered emancipated
Pregnancy:
Minors may consent or refuse medical care related to the care of their unborn child or for their pregnancy.
Minors may also consent or refuse medical care and treatment of their child if they have custody of that child.
Who other than the parents of a minor can consent to or refuse medical treatment? Per Texas Statutes- Family Code §32.001
Grandparent Adult brother or sister Adult aunt or uncle Any educational institution in which the minor is enrolled and has written
authorization from persons having power to consent Any adult who has actual care, control and possession of the minor and has written
authorization to consent for medical treatment. A court having jurisdiction over a suit affecting the parent-child relationship of which the child is
the subject
A peace officer who has lawfully taken custody of minor, if the peace officer has reasonable grounds to believe the minor is in need of immediate medical treatment.
A managing or possessory conservator or guardian.
A provider may be denied access to minor children by a parent or guardian if there is no obvious
immediate life threat to the patient. However, in general, parents or guardians cannot refuse
life-saving therapy for a child based on religious or other grounds.
If the provider feels that the child is in immediate danger of a life threatening illness or injury
and the parent or guardian is refusing medical care, contact law enforcement for assistance in
treatment and transport.
In the event of an unaccompanied minor that requests refusal of medical care, consent may be obtained
via telephone by contacting the parent or guardian of the minor.

James Vincent M.D. Page 22
Medical Protocols
Restraint /Transport Against Patient Will:
Texas Penal Code § 573.001 and 573.002 places responsibility for management of patients with
psychiatric problems with local law enforcement. Pursuant to this law EMS crews will assess patients
with psychiatric problems for any medical problems which they may have. Patients with acute medical
issues will be treated and transported as appropriate for their medical condition. Persons with
psychiatric problems that have no acute medical problem will be left under the supervision of local law
enforcement authorities.
Patients who are mentally competent have the ability to refuse medical care even if the patient may
potentially suffer increased illness, injury, disability or death. However patients who do not meet the
definition for competency require treatment and transport to an Emergency Department.
1. Assess scene safety. Attempts to physically restrain a patient should be made (when possible) with law enforcement assistance.
2. Determine if the patient is mentally competent and able to consent to or refuse medical care.
3. Patients should never be restrained if they are legally able to refuse care in order to force medical care upon them.
4. If the patient is not mentally competent and the patient has a potentially significant injury or illness that requires medical care, GAAA providers will provide care when safe to do so.
5. Providers should attempt to de-escalate the situation with verbal techniques.
6. If verbal techniques fail or scene safety degrades in a way that becomes potentially dangerous for the providers, first responders, general public or the patient, then additional methods should be implemented.
7. Physical restraints should be safe & humane. At NO TIME should a patient be struck or managed in such a way as to impose pain. Restrain in a position of comfort and safety.
8. Inhumane or dangerous techniques of physical restraint including prone positioning, placing the patient between backboards or hogtieing are expressly prohibited.
9. Document the reason for restraint, the mental status exam, options attempted, and method of restraint on all patients.
10. Patients that are combative and who have been restrained should have chemical restraint unless contraindicated.
11. If chemical restraint is used; refer to the “Behavioral Emergency” protocol (page 47). Patients should be continuously monitored after implementing any degree of restraint.
12. At no time should the patient be left alone.

James Vincent M.D. Page 23
Medical Protocols
Refusals:
Any person, eighteen years of age or older, that is deemed to have the legal competency and present
mental capacity to consent, may consent to, or refuse evaluation, treatment, and/or transportation.
A provider may be denied access to personal property (land and home) by the property owner or
patient, if there is no obvious immediate life threat to a patient.
Patients that do not require transport by an Emergency ambulance:
Adult patients with less than <40BSA mild sunburn
Jellyfish envenomation successfully treated with first aid and in the absence of other complaints.
Patients who request transport for medication refills or doctor’s office visits, in the absence of any
complaints.

James Vincent M.D. Page 24
Medical Protocols
Termination of CPR
Termination of CPR is a difficult decision for clinicians. Termination of CPR should not be performed in public locations with the exceptions of hospitals, nursing home, assisted living facilities and other healthcare facilities. Termination may be performed in private residences and where the deceased and family’s privacy can be respected. Termination efforts involve the entire family if present and after a field termination care and guidance should be redirected to the family and friends present at the resuscitation.
Resuscitation should not be initiated when any of the following is noted:
Obvious appearance of death
Decomposition
Rigor mortis
Obvious mortal wounds (massive burn injuries, severe traumatic injuries with obvious signs of organ destruction such as brain, thoracic contents, etc.)
Severe extremity damage, including amputation, should not be considered an obvious mortal wound without coexistent injury/illness
Other circumstances
Patient submersion greater than 15 minutes after the arrival of first responders.
Patients who are submersed in cold water do not have a definitive time that resuscitation is futile and resuscitation should be initiated in the absence of other obvious signs of death.
Valid Out-Of-Hospital Do Not Resuscitate written order or device from any US State.
A valid licensed physician on scene or by telephone orders no resuscitation efforts.
Traumatic Cardiac Arrest:
o Arrival to the hospital time is greater than 10 minutes from time of arrest
o Asystole or PEA with a rate less than <40/minute. (Paramedic)
o This does not apply to isolated blunt traumatic arrest such as sudden blows to the chest
such as caused by a baseball or a strike with a fist. It does apply to severe crush injuries
to the torso.
o No evidence of signs of life
Any provider, in the following circumstances, may discontinue resuscitation efforts without OLMC:
Resuscitation efforts were inappropriately initiated when criteria to not resuscitate were present.
A valid OOH-DNR or advanced directive was discovered after resuscitative efforts were initiated.
As per the limited termination of resuscitation(TOR) protocol (see below)
For traumatic arrest only: when an EKG is applied after resuscitation is initiated and a PEA <40 or asytole is noted. (Paramedic)
James Vincent M.D. Page 25
Medical Protocols
Termination of appropriate Resuscitation Efforts Utilizing OLMC: There are instances when a provider
must contact OLMC when considering discontinuation of resuscitation efforts. These include but are not
limited to the following circumstances:
Attempts of 15 minutes or more using ACLS/PALS interventions with no return of spontaneous circulation (ROSC).
Patients who are found with presumed natural death and whose family request no interventions be performed but do not have a DNR.
If the decision to terminate resuscitation efforts is made:
Continue resuscitation while requesting an order to discontinue the resuscitative efforts.
Contact OLMC (recorded line preferred).
Document thoroughly per system and agency protocols.
Termination of appropriate Resuscitation Efforts without OLMC
This is permitted only by a Team Captain or higher level. This should not be performed if family is not able to accept the death. Prior to initiating this protocol the provider should speak with the family regarding the failed resuscitation efforts.
Team Captain or higher only
Adult patients
Cardiac arrests that were not witnessed by GAAA providers or first responders.
No bystander CPR
15 minutes or more of continued asystole
No defibrillation delivered during resuscitation and the patient is in asystole.
For offshore flights and no OLMC are available providers are permitted to cease resuscitation efforts when:
15 minutes of ACLS has been delivered without ROSC and in the presence of asystole
Provider fatigue
When the extrication time of the patient to the aircraft or to the provider would exceed 15 minutes and no bystander CPR has been delivered and the patient is confirmed to be pulseless and apneic.

James Vincent M.D. Page 26
Medical Protocols
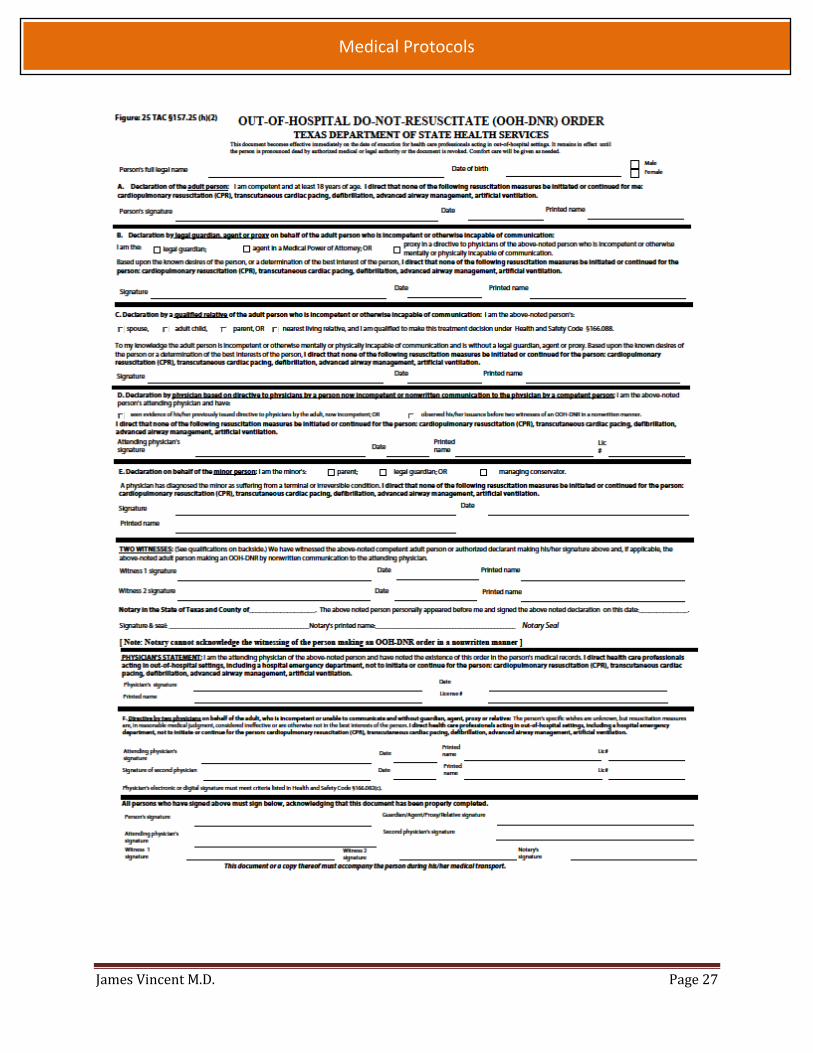
Out of Hospital Do NOT Resuscitate (OOH DNR)
Patients have a legal right to consent to, or refuse, recommended medical procedures, including
resuscitative efforts. The decision to honor, or not to honor, an OOH DNR must be made quickly and
accurately. Remember, it is our obligation to carry out the patient’s appropriately designated medical
choices.
An OOH DNR order should NOT be honored and resuscitative efforts should be initiated in the
following circumstances:
o The patient or person who executed the order destroys the form and/or removes the identification device.
o The patient or person who executed the order directs someone in their presence to destroy the form and/or removes the identification device.
o The patient or person who executed the order tells the EMS providers or attending physician that it is his/her intent to revoke the order.
o The attending physician or physician’s designee, if present at the time of revocation, has recorded in the patient’s medical record the time, date, and place of the revocation and enters “VOID” on each page of the DNR order.
o The patient is known to be pregnant.
o In the event that there is a question as whether to honor or not honor an OOH DNR or
Advanced Directive, contact OLMC as needed.
Important Points to Remember
o Always rule out a non-traumatic etiology for what may be perceived as a traumatic arrest (for example, primary ventricular fibrillation resulting in a minor car crash).
o Anytime a DNR is not honored, the reason must be documented in the patient care record (PCR).
o An advanced directive does not imply that a patient refuses palliative and/or supportive care. Care intended for the comfort of the patient should not be withheld based on a medical power of attorney.
When an EMS provider honors an appropriately executed DNR order, the law provides protection against any charges of aiding in suicide 9Section 22.08 of the Penal Code -TAC 166.047.
When in doubt, always initiate resuscitative efforts. Later termination can be implemented if appropriate.
James Vincent M.D. Page 27
Medical Protocols

James Vincent M.D. Page 28
Medical Protocols
Hospice Patients
When a patient with a severe illness decides that curative measures are no longer appropriate or effective, the option of hospice care is a compassionate, dignified and cost-effective end-of-life care option. The address where a hospice patient resides will ideally be flagged from dispatch to allow for appropriate identification of these patients. While a patient or legal surrogate may reverse a hospice decision at any time, transport of these patients inappropriately to the hospital emergency room generally will trigger loss of funding for the patient. Our role when caring for a hospice patient includes:
Confirming hospice status
Providing comfort measures
Addressing family concerns
Coordinating care with the Hospice Team, which may include transport to the hospital as a direct admission
As end-of-life issues are difficult for patients and healthcare professionals alike, the shift Supervisor or Medical Director should be contacted immediately for assistance should any questions or concerns arise during the care of these patients.

James Vincent M.D. Page 29
Medical Protocols
Scope of Practice
The State of Texas does not have a state-mandated scope of practice. Each system determines the
providers’ scope of practice.
The following skills/interventions are authorized by credential level in our system:
Emergency Medical Technician- Basic (EMT-B) Credentials
Patient assessment
Spinal motion restriction
CPR/AED application
OPA/NPA
Oropharyngeal suction
Pulse Oximetry
BVM ventilations
Blood glucose assessment
Oral glucose administration
Bandaging/Splinting
Emergency Childbirth
Mark 1 Auto injector kits if available
Medication administration: all medications and routes as outlined in ECA and EMT-B level Patient Care Guidelines
12-lead acquisition if appropriately trained
Small volume nebulizer Members of Galveston Beach Patrol
CPAP
Combitube
Assist patient with prescribed medications
Oxygen administration: Titrate to an oxygen saturation of 92% or patient improvement by the use of NC, NRB, and BVM oxygen administration.
End-tidal CO2 monitoring and interpretation
CPAP

James Vincent M.D. Page 30
Medical Protocols
Emergency Medical Technician- Intermediate (EMT-I) Credentials
All EMT-B skills/interventions plus:
Medication administration: all medications and routes as outlined in EMT-B, and IM, PO, IV, IN, SQ, nebulized medications as directed in the protocols.
Peripheral intravenous access
Intraosseous access
Orotracheal intubation
Nasotracheal intubation
Tracheal suctioning
External jugular cannulation
EZ-IO
Non Team Captain Paramedics
All EMT-B, and EMT-I skills/interventions plus:
All routes of medication administration
(IV, IO, ET, SQ, SL, PR, IM and IN)
Obtaining and interpreting ECG &
12-leads.
All cardiac related medications in a
cardiac arrest situation.
Vagal maneuvers
Defibrillation / Cardioversion
External cardiac pacing
Gastric tube insertion
Any other skill as directed by Team
Captain.
Team Captain Paramedics
All skills listed above
Chest decompression
Surgical airway
Pharmacologically Assisted Intubation
Supervisor
All skills listed above
All Therapies within the protocols including extended medical authorization and other special procedural skills as developed.

James Vincent M.D. Page 31
Medical Protocols
Inter-facility Transfers:
When transferring a patient who requires transport to a higher level of care or for specialty services not available at the sending facility the following guidelines should be used:
Consult with the on-duty shift supervisor for any patient care issues that cannot be resolved through this document. If called to transport a patient that is potentially unstable for transport, assess and consult with the treating physician.
Consistent with the intent of EMTALA, the transfer of a patient not stabilized for transport may be preferable to keeping that patient at a facility incapable of providing stabilizing care. If the patient requires advanced treatment or interventions that are beyond the scope of prehospital providers the facility should provide appropriately trained staff to accompany the patient.
Additional staffing:
If the staff member is an RN, he or she will maintain patient care responsibility and function within his or her scope of practice and under the orders of the transferring physician. The GAAA provider(s) and the RN will work together to provide patient care. If the patient deteriorates en route the Paramedic will assume care outside the RN’s scope of practice.
If the additional staff member is an RT, he or she will manage ventilator settings and all treatment under his or her scope of practice. The paramedic will assist as needed and manage the comprehensive patient care.
If the additional staff member is a physician, then that physician will remain in charge of patient care. The GAAA provider will assist as required.
If the additional staff member is a flight paramedic, GAAA providers will assist as required and, unless requested, the patient will remain in the care of the flight paramedic.
Due to the unique nature of inter-facility transports, providers will encounter medications and invasive procedures that are not typically utilized in pre-hospital treatment. Providers should not monitor medications or devices that they are not familiar with. Providers should not take possession of any medication that is not from GAAA formulary to administer to the patient en route. Providers may monitor and transport an extended formulary but should not institute or titrate any medications or infusions not stated in this document. Limited titration can be performed by paramedics with written orders.
Dial-a-flows are not appropriate for medication and infusion monitoring on inter-facility transfers.
EMT- Basics are permitted to transport and monitor all patients as noted in GAAA protocols and:
Monitor only:
Peripheral lines with a saline lock.
Personal Insulin infusion pumps that are maintained by the patient.
Feeding tubes and TPN solutions on an infusion pump.
Established (greater than 2 week placement) of tracheostomy patients on home ventilators with
pre-set ventilator settings.

James Vincent M.D. Page 32
Medical Protocols
NG/OG tubes.
Internal pacemakers.
Spinal stimulators.
Foley catheters.
Central venous access lines without infusions excepting patient controlled devices.
EMT-Intermediates: All skills and medications listed above and:
Peripheral lines containing plain isotonic or glucose solutions without medications added. May
adjust per the patient’s condition and/or written orders from the sending facility.
IV antibiotics running at a KVO rate or on an infusion pump if the medication has been initiated
by the sending facility.
Ventilator patients that do not require sedation, paralysis, EKG monitoring or other advanced
procedure.
EMT-Paramedics: All skills and medications listed above
Non-Team captain Paramedics will require written orders to administer sedation or paralysis
for intubated patients on ventilators.
Administer but not initiate glucose or isotonic IV fluids that are not standard GAAA formulary.
May monitor and adjust IV solutions containing potassium less than 20mEq/L.
Medications that GAAA providers may monitor without titration and administered through an
infusion pump. In the event of an infusion pump malfunction, the infusion should be stopped
and the appropriate facility contacted for guidance.
Heparin Magnesium
Anticoagulants or Antiplatelet agents Solutions with >20mEq/L of KCL
Electrolyte preparations Insulin
Antibiotics Mannitol
Sedatives in an infusion dose Paralytics as a continuous infusion
Sodium Bicarbonate infusions TPN/PPN
Anesthetic infusions IV steroids

James Vincent M.D. Page 33
Medical Protocols
The following medications may be titrated with written orders from the sending facility :
Insulin Propranolol and other beta-blockers
IV Nitrates Anti-dysrhythmics
Vasopressors Anti-hypertensive continuous infusions
Lidocaine
NOTE: Although the sending facility may have initiated medication(s), Paramedics MUST be familiar with
the medications that the patient may be receiving at the time of transfer. Reminder: interfacility
medications are not to be initiated by Paramedics.
Paramedics may monitor:
Ventilators
PIC Lines
Bladder Irrigation
Chest tubes
Femoral lines
ICP monitoring devices that are not in active use.
Blood products may be monitored by providers.
Paramedics may transport patients with femoral sheaths that are not currently accessed. Patients that
have arterial line monitoring, active ICP monitoring devices or Intra-aortic balloon pumps require
additional trained personnel from the sending facility to monitor and manage those devices.

James Vincent M.D. Page 34
Medical Protocols
Expired Medications and Medication Shortages
In the setting of national medication shortages, when it is deemed to be in the patient’s best interest to
use an expired medication, as opposed to either an inferior alternative or no medication, an expired
medication may be used. Additionally, providers will not be responsible for giving medications in any
protocol in which the medicine is unavailable due to national shortages or supply issues. Clinically
appropriate pharmacologic substitutions may be authorized on a case-by-case basis and communicated
directly to field staff by the medical director.

James Vincent M.D. Page 35
Medical Protocols
Ebola Preparedness Procedure
Dispatch Decision Tree for Ebola Screening
Does the
patient have a
fever > 38*C or
100.4*F
NO Proceed with normal
call process
YES
Does the patient have severe
headache, muscle pain, vomiting,
diarrhea, abdominal pain or
unexplained bleeding?
NO Proceed with normal
call process
YES
In the past 21 days
has the patient been
in contact with blood
or body fluids of a
patient known to
have or suspected to
have Ebola?
In the past 21 days
handled bats or
nonhuman primates
from a disease
endemic area?
In the past 21 days
been in residence or
traveled to a country
where an Ebola
outbreak is
occurring?
Western Africa Countries:
Guinea, Liberia, Nigeria, Sierra Leone
If the answer to any of these questions is
YES notify the crew immediately for Person
under Investigation of Ebola

James Vincent M.D. Page 36
Medical Protocols
4.2 – Guidance for Emergency Medical Services (EMS) Systems for 9-1-1 Public Safety Answering Points (PSAPs) for Management of Patients with Known or suspected Ebola Virus Disease (EVD) Purpose To provide an integrated plan of operations between the University of Texas Medical
Branch (UTMB) Health System and any Emergency Medical Service in the safe transport and healthcare for patients with diagnosed or possible Ebola Virus Disease.
Audience Healthcare personnel in the UTMB Emergency Department (ED) and personnel in the EMS.
Policy and Procedures
I. Transport of patients with possible EVD based on 9-1-1 calls to the EMS A. When calls come in to the dispatcher requesting Transport of a patient with possible
EVD, the dispatcher should ask the following questions: 1. Do they or someone else with them have a fever of greater than 38*C or
101.5*F and if they have additional symptoms such as severe headache, muscle pain, vomiting diarrhea, abdominal pain or unexplained bleeding?
2. If the patient has symptoms of Ebola, then ask the patient about risk factors within the past 3 weeks before the onset of symptoms, including:
a. Has the patient had contact with blood or body fluids of a patient known to have or suspected to have EVD?
b. Has the patient had residence in-or traveled to a country where an Ebola outbreak is occurring?
a. Guinea b. Sierra Leone c. Liberia d. Nigeria
c. Has the patient handled bats or non-humans primates from the disease-endemic areas?
d. If the dispatcher has information from the above queries suggesting that the person may possibly have EVD, they should make sure that the EMS personnel are made confidentially aware of the potential for EVD so that responders can don appropriate PPE before they arrive at the scene.
II. Transport of cases of possible EVD from UTMB outlying Clinics to the UTMB ED A. Cases that present to UTMB Clinics with possible EVD will be screened using the
same screening protocol as that used by the UTMB ED.
Section: UTMB On-Line Documentation
Subject: Healthcare Epidemiology Policies and Procedures
Topic: 4.02 – Guidance for Emergency Medical Services (EMS) Systems for 9-
1-1 Public safety Answering Points (PSAPs) for Management of Patients with
Known or suspected Ebola Virus Disease (EVD)
4.02 – Policy
10.21.14
2014 - Author
James Vincent M.D. Page 37
Medical Protocols
B. When a patient in an outlying UTMB clinic meets the screening criteria for EVD or possible EVD, the clinic will call the EMS and request transfer to the UTMB ED. The clinic will notify the UTMB ED that the patient is being transferred.
III. PPE for EMS when transporting a case of EVD or possible EVD A. KleenGard suit B. Three pairs of gloves
1. Latex gloves 2. Middle pair of long puncture-resistant gloves taped to gown cuffs 3. Outer pair of latex or nitrile gloves 4. Surgical mask 5. Goggles or face shield 6. Shoe-leg covers
IV. Use caution when approaching a patient with Ebola. Illness can cause delirium, with erratic behavior that can place EMS personnel at risk of infection, e.g., flailing or staggering.
V. Pre-hospital resuscitation procedures such as endotracheal intubation, open suctioning of airways, and cardiopulmonary resuscitation frequently result in a large amount of body fluids, such as saliva and vomit. Performing these procedures in a less controlled environment (e.g., moving vehicle) increases risk of exposure for EMS personnel. If conducted, perform these procedures under safer circumstances (e.g. stopped vehicle, hospital destination).
A. During pre-hospital resuscitation procedures (intubation, open suctioning of airways, cardiopulmonary resuscitation).
1. In addition to recommended PPE above, respiratory protection that is at least as protective as a NIOSH-certified, fit-tested N95 filtering face piece respirator or higher should be worn (instead of a facemask).
2. Activities should be limited, especially during transport that increase the risk of exposure to infectious material (e.g., airway management, cardiopulmonary resuscitation, use of needles).
B. Limit the use of needles and other sharps as much as possible. All needles and sharps should be handled with extreme care and disposed in puncture-proof, sealed containers.
C. Phlebotomy procedures and laboratory testing should be limited to the minimum necessary for essential diagnostic evaluation and medical care.
D. If blood, body fluids, secretions, or excretions from a patient with suspected Ebola come into direct contact with the EMS provider’s skin or mucous membranes, then the EMS provider should immediately stop working. If eyes are involved, the EMS provider should flush eyes with large amounts of water. The EMS provider should wash the affected skin surfaces with soap and water and report exposure to an occupational health provider or supervisor for follow-up.
E. PPE should be worn upon entry into the scene and continue to be worn until personnel are no longer in contact with the patient.
F. PPE should be carefully removed without contaminating one’s eyes, mucous membranes, or clothing with potentially infectious materials.
G. Re-useable PPE should be cleaned and disinfected according to the manufacturer’s reprocessing instructions and EMS agency policies.
H. Refer to all figures for instructions for putting on and removing PPE. I. Hand hygiene should be performed immediately after removal of PPE.

James Vincent M.D. Page 38
Medical Protocols
VI. Cleaning EMS transport vehicles after transporting a patient with suspected or confirmed Ebola.
A. EMS personnel performing cleaning and disinfection should wear recommended PPE (described above) and consider use of additional barriers (e.g., rubber boots or shoe and leg coverings) if needed.
B. Face protection (face mask with googles or face shield) should be worn since tasks such as liquid waste disposal can generate splashes.
C. Patient-care surfaces (including stretchers, railings, medical equipment, control panels and adjacent flooring, walls and work surfaces) are likely to become contaminated and should be cleaned and disinfected after transport.
D. A blood spill or spill of other body fluid or substance (e.g., feces or vomit) should be managed through removal of bulk spill matter, cleaning the site, and then disinfecting the site. For large spills, a chemical disinfectant with sufficient potency is needed to overcome the tendency of proteins in blood and other body substances to neutralize the disinfectant’s active ingredient.
E. An EPA-registered hospital disinfectant with instructions for cleaning and decontaminating surfaces or objects soiled with blood or body fluids should be used according to those instructions. After the bulk waste is wiped up, the surface should be disinfected as described in D. above.
F. Contaminated reusable patient care equipment should be placed in biohazard bags and labeled for cleaning and disinfection according to agency policies. Reusable equipment should be cleaned and disinfected according to manufacturer’s instructions by trained personnel wearing correct PPE. Avoid contamination of reusable porous surfaces that cannot be made single use.
G. Use only a mattress and pillow with plastic or other covering that fluids cannot get through. To reduce exposure among staff to potentially contaminated textiles (cloth products) while laundering, discard all linens, non-fluid-impermeable pillows or mattresses as a regulated medical waste.
DONNING AND REMOVAL OF PERSONAL PROTECTIVE EQUIPMENT
PPE for EMS when transporting a case of EVD or possible EVD includes all of the items below:
Disposable KleenGard coverall
Three pairs of gloves o Latex gloves o Middle pair of long puncture-resistant o Outer pair of latex or nitrile gloves
Surgical mask
Goggles or face shield
Waterproof shoe-leg covers
For multiple pairs of gloves , (i.e. for EMS), carefully pull second puncture resistant gloves over first pair and tape cuffs of KleenGard coverall, sealing completely. Carefully pull third pair of gloves over the taped pair.

James Vincent M.D. Page 39
Medical Protocols
How to don a KleenGard suit:
Unfasten times/unzip zipper
Scrunch up the legs of the suit, making a space for your feet to go through to touch the ground
Step into the suit one leg at a time
Gently pull the suit over your legs and to your waist
One arm at a time, put on the upper portion of the suit
Zip the zipper
How to don shoe covers/leg covers:
Ensure that foot and leg protectors are fastened carefully outside the KleenGard suit legs
How to remove KleenGard suit:
Undo ties on foot-leg protectors and remove and discard in contaminated trash
Unfasten ties/unzip zipper on KleenGard suit
Peel suit away from neck and shoulder
Outer pair of gloves and middle pair of gloves taped to cuffs of KleenGard suit will be removed with the suit
Turn contaminated outside of suit toward the inside
Fold or roll into a bundle
Discard
REFERENCES
1. Centers for Disease Control and Prevention. Ebola Hemorrhagic Fever. Case Definition for Ebola Virus Disease (EVD). September 10, 2014.
2. Centers for Disease Control and Prevention. Ebola Hemorrhagic Fever. Safe Management of Patients with Ebola Virus Disease (EVD) in U.S. Hospitals. August 27, 2014.
3. Centers for Disease Control and Prevention. Ebola Hemorrhagic Fever. Infection Prevention and Control Recommendations for Hospitalized Patients with Known or Suspected Ebola Hemorrhagic Fever in U.S. Hospitals. August 30, 2014.
4. Centers for Diseases Control and Prevention. Ebola Hemorrhagic Fever. Interim Guidance for Emergency Medical Services (EMS) Systems and 9-1-1 Public Safety Answering Points (PSARs) for Management of Patients with Known or Suspected Ebola Virus Disease in the United States. September 10, 2014.
James Vincent M.D. Page 40
Medical Protocols
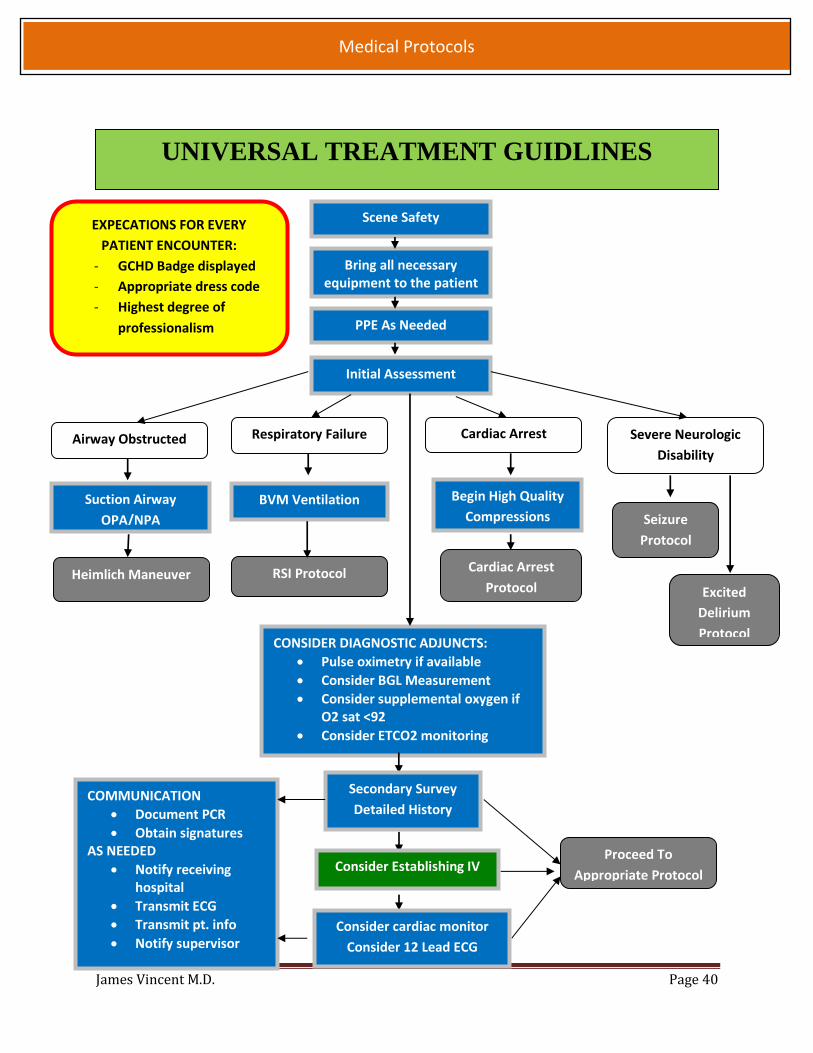
UNIVERSAL TREATMENT GUIDLINES
Scene Safety
PPE As Needed
Initial Assessment
Cardiac Arrest
Cardiac Arrest
Protocol
CONSIDER DIAGNOSTIC ADJUNCTS:
Pulse oximetry if available
Consider BGL Measurement
Consider supplemental oxygen if O2 sat <92
Consider ETCO2 monitoring
RSI Protocol
Bring all necessary equipment to the patient
Heimlich Maneuver
Respiratory Failure
BVM Ventilation
Airway Obstructed Severe Neurologic
Disability
Suction Airway
OPA/NPA
Begin High Quality
Compressions
Excited
Delirium
Protocol
Seizure
Protocol
Secondary Survey
Detailed History
Proceed To
Appropriate Protocol Consider Establishing IV
COMMUNICATION
Document PCR
Obtain signatures AS NEEDED
Notify receiving hospital
Transmit ECG
Transmit pt. info
Notify supervisor
EXPECATIONS FOR EVERY
PATIENT ENCOUNTER:
- GCHD Badge displayed
- Appropriate dress code
- Highest degree of
professionalism
Consider cardiac monitor
Consider 12 Lead ECG
James Vincent M.D. Page 41
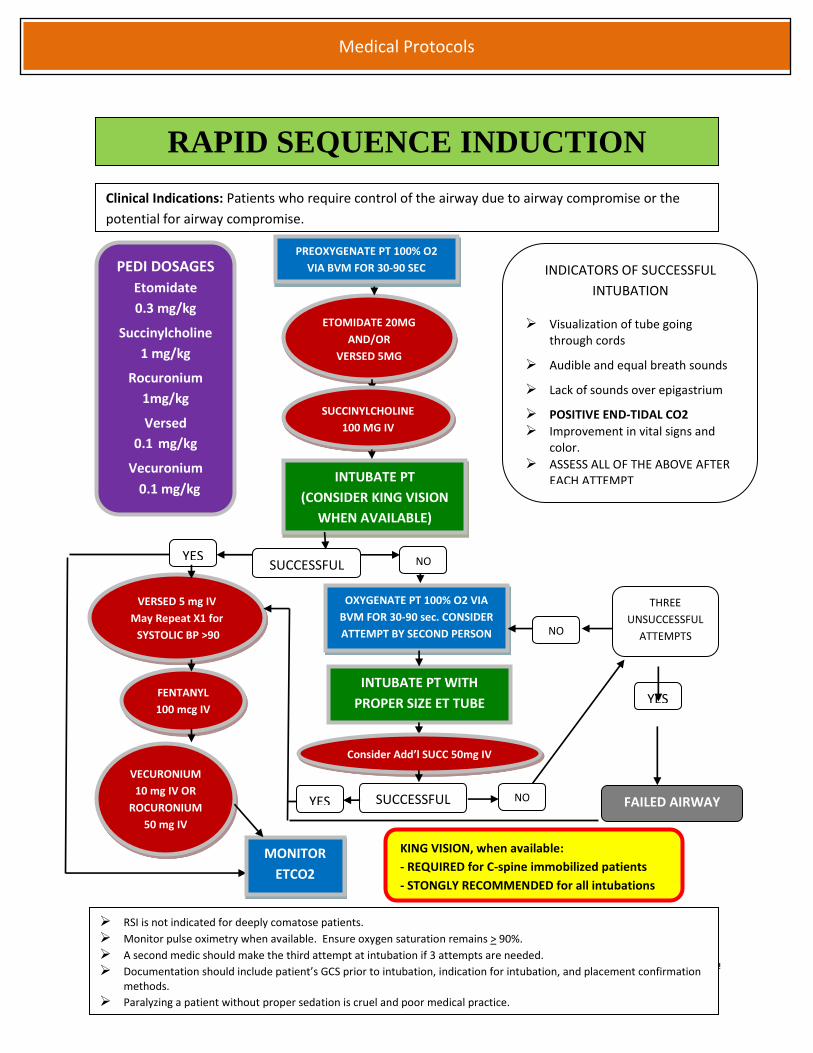
Medical Protocols
PREOXYGENATE PT 100% O2
VIA BVM FOR 30-90 SEC
ETOMIDATE 20MG
AND/OR
VERSED 5MG
INTUBATE PT
(CONSIDER KING VISION
WHEN AVAILABLE)
SUCCESSFUL
SUCCINYLCHOLINE
100 MG IV
YES
NO
OXYGENATE PT 100% O2 VIA
BVM FOR 30-90 sec. CONSIDER
ATTEMPT BY SECOND PERSON
INTUBATE PT WITH
PROPER SIZE ET TUBE
VERSED 5 mg IV
May Repeat X1 for
SYSTOLIC BP >90
FENTANYL
100 mcg IV
SUCCESSFUL NO YES
THREE
UNSUCCESSFUL
ATTEMPTS
NO
YES
Clinical Indications: Patients who require control of the airway due to airway compromise or the
potential for airway compromise.
RAPID SEQUENCE INDUCTION
RSI is not indicated for deeply comatose patients.
Monitor pulse oximetry when available. Ensure oxygen saturation remains > 90%.
A second medic should make the third attempt at intubation if 3 attempts are needed.
Documentation should include patient’s GCS prior to intubation, indication for intubation, and placement confirmation methods.
Paralyzing a patient without proper sedation is cruel and poor medical practice.
VECURONIUM
10 mg IV OR
ROCURONIUM
50 mg IV
INDICATORS OF SUCCESSFUL
INTUBATION
Visualization of tube going through cords
Audible and equal breath sounds
Lack of sounds over epigastrium
POSITIVE END-TIDAL CO2
Improvement in vital signs and color.
ASSESS ALL OF THE ABOVE AFTER EACH ATTEMPT
FAILED AIRWAY
Consider Add’l SUCC 50mg IV
PEDI DOSAGES
Etomidate
0.3 mg/kg
Succinylcholine
1 mg/kg
Rocuronium
1mg/kg
Versed
0.1 mg/kg
Vecuronium
0.1 mg/kg
KING VISION, when available:
- REQUIRED for C-spine immobilized patients
- STONGLY RECOMMENDED for all intubations
Yes to any item?
Patient will require spinal motion
restriction
MONITOR
ETCO2

James Vincent M.D. Page 42
Medical Protocols
FAILED AIRWAY Indications:
BVM fails to maintain SpO2 >90% or becomes difficult to ventilate.
Three failed total attempts at oral-tracheal intubation
Continuous pulse oximetry when available and ETCO2 monitoring should be used in all
patients with inadequate respiratory function.
Notify receiving Emergency Department ASAP about patients with failed air-way.
Place King Tube Surgical Airway
Facial Trauma or Swelling
NO YES
Announce over the Radio “Medic
______ Failed Air-way Protocol”
SpO2 <90%
YES NO
Continue To
ventilate with
BVM
SpO2 drops below <90% or
becomes difficult to ventilate
with BVM
Ventilate PT at a ≤ 12 / min,
keeping SpO2 above 90% SpO2 <90%
QuickTrach
YES

James Vincent M.D. Page 43
Medical Protocols
PAIN MANAGEMENT Clinical Indications:
Patients that need pain management and are unable to obtain adequate relief with non-
pharmaceutical measures
AND / OR
For sickle cell patients, also consider 1 liter of Normal saline.
For hemodynamically unstable patients, Fentanyl should be the first line treatment.
Morphine should be administered only with systolic pressure >90 and when the pt is not
presenting with signs of imminent circulatory collapse.
Morphine should not be used during active child birth.
Consider administration of Zofran early when administering Morphine.
(See Nausea Protocol)
In the elderly, patients with renal or severe liver disease reduce dosage by half.
Our goal is not complete cessation of pain, aim for 50% reduction of pain.
Fentanyl may be administered IV, IM, or IN.
This is not the necessarily the order of administration, use patient needs and presentation
as a guideline.
Consider 25 mcg IV dosages for elderly patients.
General Pain
Management
Morphine 2-5mg IV
May repeat X1
Fentanyl 50 – 100 mcg
IV/IM/IN May repeat X1

James Vincent M.D. Page 44
Medical Protocols
History:
Trauma
Drug Abuse
Foot Pursuit
Pepper Spray
Taser Evaluation
POLICE CUSTODY Signs and Symptoms:
External Trauma
Taser Barbs
Wheezing, SOB
AMS
Palpitations
Intoxication/Substance abuse
Differential:
Agitated Delirium
Traumatic Injury
Substance Abuse
Psychiatric Emergency
Traumatic brain injury
Asthma Exacerbation
Cardiac
Universal Treatment Guidelines
Suspected Traumatic Injury or
medical condition.
Pepper Spray Minor Laceration
or Abrasions?
Taser
Appropriate
Protocol
Irrigate Eyes and Face
w/ water. Remove
contaminated clothing
Wheezing
Appropriate wound
care.
YES
NO
Taser Barb
Removal Protocol
COPD/Asthma
Protocol & Transport
Coordinate disposition with LEO
and if necessary medical control
and the on-duty Supervisor.
Excited Delirium is a distinct syndrome that is marked by restlessness, combativeness, and hyperthermia. These patients are at high risk and should be transported by an ALS unit.
Patients who are in police custody retain their rights to medical care. This should be coordinated with the law enforcement officer (LEO). If any questions occurs whether the patient requires transport, contact the on-duty supervisor for guidance.
Sutures have a 6-8 hour window. Advise LEO and patient to obtain a Tetanus shot if the patient has not received one in more
than 10 years. If an asthmatic pt is exposed to pepper spray and is released to LEO or EMS care is refused
by LEO: all parties should be advised to contact EMS if wheezing or difficulty breathing occurs.

James Vincent M.D. Page 45
Medical Protocols
ALLERGIC REACTION Signs and Symptoms:
Stable: o Rash/ Hives / Urticaria o Stable Vital Signs
Unstable: Two or more of the following o Dyspnea o Wheezing o Cyanosis o Excessive Salvation o Edema to Eyelids, Lips, Hands,
Tongue
Differential:
Niacin Overdose
Angioedema due to ACE Inhibitors
Heat rash
Pulmonary Embolism
Foreign body obstruction
Unstable Stable
Benadryl 25-50 mg
SIVP or IM
Epinephrine 1:1000
0.3mg IM
May repeat X1 in 5 min
If Wheezing develops see
COPD/Asthma Protocol
The shorter the time from the patients exposure to the onset of symptoms, the more severe the reaction.
Apply cold packs. May be applied to bites and stings in order to reduce the swelling and slow blood flow from the affected are.
Famotidine is an antacid with H2 antagonist properties that has been shown to work well for hives and other allergic reactions.
Universal Treatment Guidelines
Solumedrol 125mg
IV/IM
NS Bolus 1000 cc IV

James Vincent M.D. Page 46
Medical Protocols
History:
Behavioral or
psychiatric disorder
History of Anxiety
Recent trauma or
emotional distress
Differential:
Hypoxia
Head Trauma
Pulmonary Embolism
Signs and Symptoms:
Hyperventilation
Sensation of panic
Agitation
ANXIETY
Verbal Calming
Versed 1-2mg
IN/IM/IV may repeat
once
This Protocol is NOT to be implemented for patients who are refusing EMS care and are
legally mentally competent and able to refuse care.
The majority of patients that present with uncomplicated anxiety will not require
pharmacological management. Verbal calming and empathy is generally effective.
Consider midazolam 0.5 mg IV for elderly patients.
For pediatric patients < 13 y.o. contact medical control.
Universal Treatment Guidelines

James Vincent M.D. Page 47
Medical Protocols
History:
Psychiatric Illness
Injury to self or
threats against others
Substance abuse or
Overdose
Diabetes
Differential Diagnosis:
Excessive Heat or Cold
Substance Abuse or
Intoxication
Head Trauma
Hypoxia
Hypoglycemia
CVA / Brain Tumor
CNS infection
Signs and Symptoms:
Anxious, tense, restless,
fidgeting
Hallucinations, or
delusional thoughts
Labile mood,
unpredictable, excitable
Combative or violent
Expression of suicidal or
homicidal ideation
BEHAVIORAL EMERGENCY
Verbal Calming
BGL, Any vital signs that can be
safely obtained.
Physical Restraints (see p.12)
Suspected Stimulant Overdose should be treated with Valium / Versed until pt is calmed or
systolic blood pressure of 100 is reached.
Do not restrain in the prone position. Physical restraints without chemical restraint can
increase the risk of Excited Delirium in susceptible patients.
For agitated or very combative patients do not restrain without adequate sedation to reduce
the risk of excited delirium.
Patients restrained using handcuffs in police custody must be transported with law
enforcement’s assistance.
This Protocol is NOT to be implemented for patients who are refusing EMS care and are
legally able to do so.
If the patient is suspected of excited delirium and cardiac arrest ensues, Sodium Bicarbonate
and fluid bolus should be administered early in the arrest. If available cooled IV fluids should
be used. Consider passive cooling.
After restraint procedures are used the patient will require continuous monitoring.
For pediatric patients
< 13 y.o. contact
medical control.
Universal Treatment Guidelines
Versed 5mg IN/IM
may repeat X 1
Valium 10mg IM
One dose OR

James Vincent M.D. Page 48
Medical Protocols
History:
Use of Bath Salts
Use of Synthetic
Marijuana
Use of LSD
Use of Cocaine
Signs and Symptoms:
Agitation
Aggressive or
threatening behavior
Amazing strength
Dilated Pupils
Sweating
Hot to the touch
Tachypnea
Differential Diagnosis:
Excessive Heat or Cold
Substance Abuse or
Intoxication
Head Trauma
Hypoxia
Hypoglycemia
CVA / Brain Tumor
CNS infection
If Geodon is given IV, immediacy contact the medical director and notify the Clinical
Coordinator ASAP.
Do not restrain in the prone position. Physical restraints without chemical restraint can
increase the effects of Excited Delirium and are inhumane.
Patients restrained using handcuffs in police custody must be transported with law
enforcement’s assistance.
This Protocol is NOT to be implemented for patients who are refusing EMS care and are
legally able to do so.
If the patient is suspected of excited delirium and cardiac arrest ensues Sodium Bicarbonate
and fluid bolus should be administered early in the arrest. If available cooled IV fluids should
be used. Consider passive cooling.
Universal Treatment Guidelines
Cardiac Monitoring, 12 Lead EKG
Verbal Calming
Versed
5 mg IV/IM/IN
For pediatric patients
contact medical
control.
Benadryl 25-50 mg
IV/IM
FOR IMMINENT LIFE THREAT
TO PATIENT OR HARM TO
STAFF
CARDIAC ARREST
Sodium Bicarb
50-100 mEq IV Geodon
20 mg IM
GEODON SHALL ONLY
BE GIVEN IM
EXCITED DELIRIUM

James Vincent M.D. Page 49
Medical Protocols
COPD / ASTHMA
Universal Treatment Guidelines
Cardiac Monitoring, 12 Lead EKG
Albuterol 2.5mg / Atrovent 0.5 mg
may repeat x2
Epinephrine (1:1000) 0.3mg IM
may repeat X1 in 5 min
Consider C-PAP
5cm H20
Solumedrol 125mg IV
Differential:
Pneumonia
Congestive Heart Failure
Anaphylaxis
Tuberculosis
Signs and symptoms:
Pursed Lips
Audible Wheezing
Decreased Breath Sounds
Inability to Complete Sentences
Prolonged Expiratory Phase
Magnesium Sulfate is recommended after 1 hour of treatment or for life-threatening asthma and should be given over 20 minutes. It should be used infrequently.
RSI Protocol
Albuterol 2.5mg nebs
continuously
Respiratory Distress Protocol
Bronchospasm most likely cause of distress
Life Threatening Asthma
Magnesium SO4 2G IV over 20 min
Apply ETCO2 Device
Obtain EKG
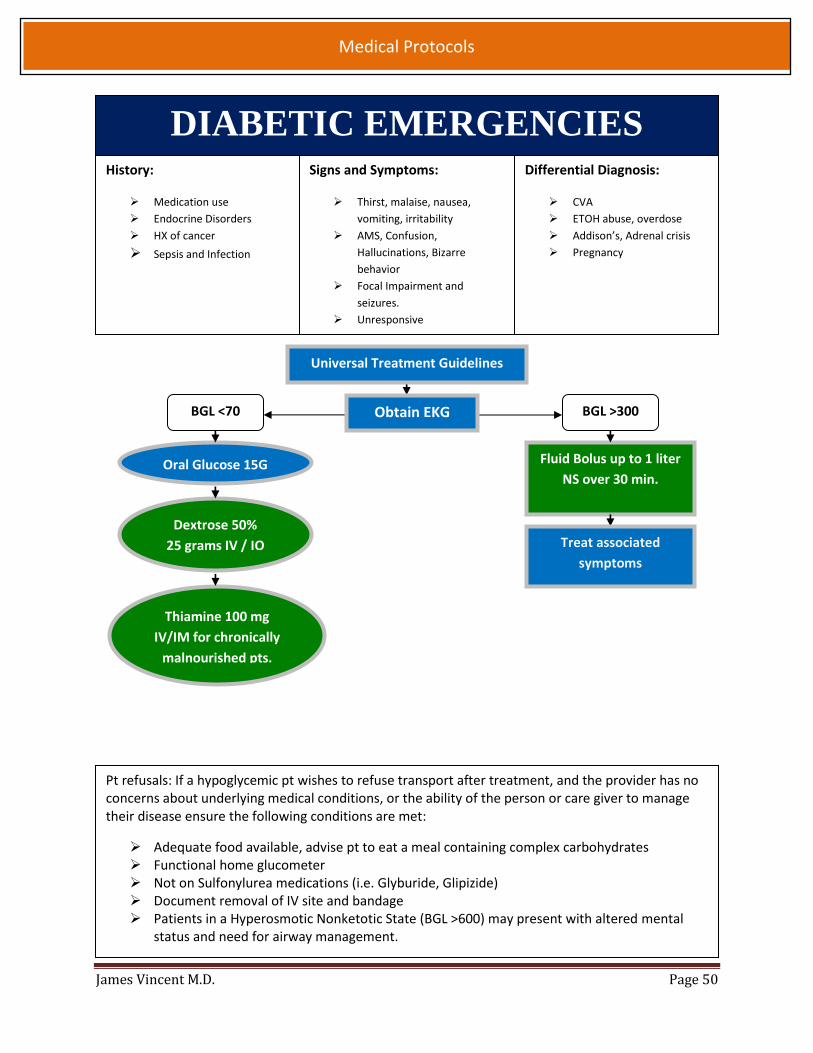
James Vincent M.D. Page 50
Medical Protocols
DIABETIC EMERGENCIES History:
Medication use
Endocrine Disorders
HX of cancer
Sepsis and Infection
Differential Diagnosis:
CVA
ETOH abuse, overdose
Addison’s, Adrenal crisis
Pregnancy
Signs and Symptoms:
Thirst, malaise, nausea,
vomiting, irritability
AMS, Confusion,
Hallucinations, Bizarre
behavior
Focal Impairment and
seizures.
Unresponsive
BGL <70
Dextrose 50%
25 grams IV / IO
Thiamine 100 mg
IV/IM for chronically
malnourished pts.
Oral Glucose 15G
Obtain EKG
Pt refusals: If a hypoglycemic pt wishes to refuse transport after treatment, and the provider has no concerns about underlying medical conditions, or the ability of the person or care giver to manage their disease ensure the following conditions are met:
Adequate food available, advise pt to eat a meal containing complex carbohydrates Functional home glucometer Not on Sulfonylurea medications (i.e. Glyburide, Glipizide) Document removal of IV site and bandage Patients in a Hyperosmotic Nonketotic State (BGL >600) may present with altered mental
status and need for airway management.
Fluid Bolus up to 1 liter
NS over 30 min.
BGL >300
Treat associated
symptoms
Universal Treatment Guidelines

James Vincent M.D. Page 51
Medical Protocols
HYPOTENSION Signs and Symptoms:
SYSTOLIC BP < 90 WITH SYMPTOMS Lightheaded, Dizziness Positive Tilt test Altered Mental Status Restlessness, Confusion Weak, rapid pulse Pale, cool, clammy skin Coffee ground emesis, Tarry Stool
Differential Diagnosis:
Shock- Carcinogenic, Septic, Neurogenic, Anaphylactic
Pregnancy Ectopic Pregnancy Dysrhythmias Pulmonary Embolus Tension Pneumothorax Medication Effect / Overdose Vasovagal
Universal Treatment Guidelines
CONSIDER SEPSIS IF ANY TWO ARE MET
1. Temperature >100.9 F or < 96.8
2. Heart rate > 90 Beats per minute;
3. Respiratory rate > 20 Breaths per min
4. Acutely altered mental status; or
5. Serum glucose < 120 mg/dL
(The Robson screening tool)
NON-TRAUMA NON-CARDIAC
(ex.: dehydration, GI bleed,
heat exhaustion, vagal event)
CARDIAC
(ex.: STEMI, CHF,
dysrhythmias,
bradycardia)
NS Bolus 500cc
repeat x 3
NS Bolus 500cc X1
Epinephrine 10 mcg = 1mL
Q 2-5 minutes
OR 5-20 mcg/min IV infusion
Titrate to SBP >90
Go to appropriate
protocol once etiology
determined
EPINEPHRINE FOR HYPOTENSION
Draw up 9 mL of NS in a 10mL syringe
Add 1 mL of cardiac Epi (1:10,000)
1 mL = 10 mcg = 1:100,000 epinephrine
Cardiac Monitor, 12 Lead EKG
NS Bolus 500cc,
Repeat until
30mL/kg given
Notify receiving hospital of
suspicion of sepsis (“Sepsis Alert”)
if hospital has a sepsis program
Norepinephrine
2-12 mcg/min IV
Target MAP 65

James Vincent M.D. Page 52
Medical Protocols
NAUSEA / VOMITING Signs and Symptoms:
Nausea Vomiting Dry lips, sunken eyes Tachycardia, hypotension
Differential:
Infection (viral, food-borne) Toxin, overdose, drugs, alcohol Increased intracranial pressure (stroke,
hemorrhage, trauma) Acute coronary syndrome
Universal Treatment Guidelines
Zofran 4mg IV/IM
May repeat X1
Patients should be placed in an upright lateral recumbent position. Patients experiencing nausea or vomiting should not be allowed to ingest anything
by mouth while in EMS care. ALL nausea and vomiting patients should have a Blood Glucose Assessment.
6 mo to 4 yo:
Zofran 2 mg IV or IM
>4 yo:
Zofran 4 mg IV or IM
ADULT PEDIATRIC >6
months

James Vincent M.D. Page 53
Medical Protocols
Activated Charcoal
OVERDOSE
Signs and Symptoms:
Irregular or rapid respirations. Shallow respirations or apnea. Bradycardia Tachycardia Altered mental status.
Differential:
Head trauma Hypoglycemia Hyperglycemia Hypoxia
Universal Treatment Guidelines
Cardiac Monitoring , 12 Lead EKG
Consider Activated
Charcoal 50 Grams
Sodium Bicarb
50 -100 mEq IV
For all medications / drugs contact Poison Control 1-800-764-7661
Max dose of Narcan 2mg.
Narcan is NOT to be given to conscious or breathing patients unless a decreasing LOC or decreasing
respiratory drive is noted.
Narcan is not to be used for diagnostic purposes.
Narcan is to be administered in 0.4 mg doses titrated to respiratory drive.
Activated Charcoal can be administered up to 2 hours after ingestion.
DO NOT administer Activated Charcoal for acids, alkali, or petroleum base products.
Signs of a Dystonic Reaction include: o Protruding or pulling sensation of tongue o Twisted neck, or facial muscle spasm o Roving or deviated gaze o Abdominal rigidity and pain o Spasm of the entire body
Calcium Channel Blocker
with symptomatic
hypotension
Known TCA & Wide QRS
Suspected
Stimulant Calcium Gluconate 10%
1 -2 grams IV over 10 min
= 10 -20 mL Behavioral Emergency Protocol
Suspected Opiate and apneic
Narcan 0.4 mg IV/IM/IN
May repeat X4 until
breathing
Max dose 2mg
Dystonic Reaction
Benadryl 25-50 mg
IV / IM

James Vincent M.D. Page 54
Medical Protocols
RESPIRATORY DISTRESS
Sign and Symptoms
Dyspnea / pursed breathing
Unable to speak full sentences
Increased respiratory rate and effort
Wheezing, stridor
Rales, rhonchi
Use of accessory muscles
Fever, cough
Tachycardia
Differential Diagnosis
Asthma
COPD / Chronic Bronchitis
Anaphylaxis
Pleural effusion
Pneumonia
Pulmonary embolus
Pneumothorax
Cardiac (ACS or CHF)
Pericardial tamponade
Anxiety / hyperventilation
Universal Treatment Guidelines
12 Lead ECG / Cardiac monitor
Pulse Oximeter and ETCO2
Bronchospasm suggested by:
- History of asthma / COPD
- Use of inhalers chronically
- Smoking history
- wheezing on exam
Other Causes:
- Anxiety
- Allergic Reaction
- ACS
- Pain
- Pneumothorax
- Other
Pulmonary edema suspected:
- History of CHF
- Use of Lasix chronically
- Cardiac disease history
- Rales and leg edema on
exam
COPD / Asthma Protocol
Proceed to Appropriate Protocol
CHF Protocol
Apply Oxygen

James Vincent M.D. Page 55
Medical Protocols
SEIZURE History:
Reported / Witnessed Seizure activity.
Previous Seizure History
Medical alert tag Information
History of trauma
History of diabetes
History of pregnancy
Differential:
Head Trauma
Tumor
Metabolic, Hepatic, or Renal failure
Hypoxia
Medication non-compliance
Infection / Fever
Alcohol withdrawal
Eclampsia
Stroke
Hyperthermia
Hypoglycemia
Signs and Symptoms:
Decreased mental status
Sleepiness
Incontinence
Observed seizure activity
Evidence of trauma
Unconscious
Status Epilepticus Post-ictal
Blood Glucose
Diabetic Protocol
BGL < 60
Seizure Reoccurs
Universal Treatment Guidelines
OR
Initial dose of IN Versed 5mg in 1 ml each nostril. Status Epilepticus is defined as 2 or more successive seizures without a period of consciousness or recovery. This
is a true emergency requiring rapid airway control, treatment, and transport. Grand mal seizures are associated with loss of consciousness, incontinence, and tongue trauma. Petit mal seizures effect only a part of the body and are not usually associated with a loss of consciousness. Jacksonian seizures are seizures which start as focal seizure and become generalized. Be prepared for airway problems and continued seizures. INTUBATION IS USUALLY NOT NEEDED. Attempt airway
positioning and nasopharyngeal airway during immediate post-ictal phase. Assess possibility of occult trauma and substance abuse. For any seizures in pregnant patient, follow the OB emergency protocols. Valium (Diazepam) is not effective when administered IM. It should be given IV or PR only.
Valium 10mg IV
Versed 5 mg
IN / IV / IM
May repeat X1
RSI Protocol Airway Positioning,
Nasopharyngeal airway, O2,
BVM Ventilations as needed
Consider ETCO2 Monitoring
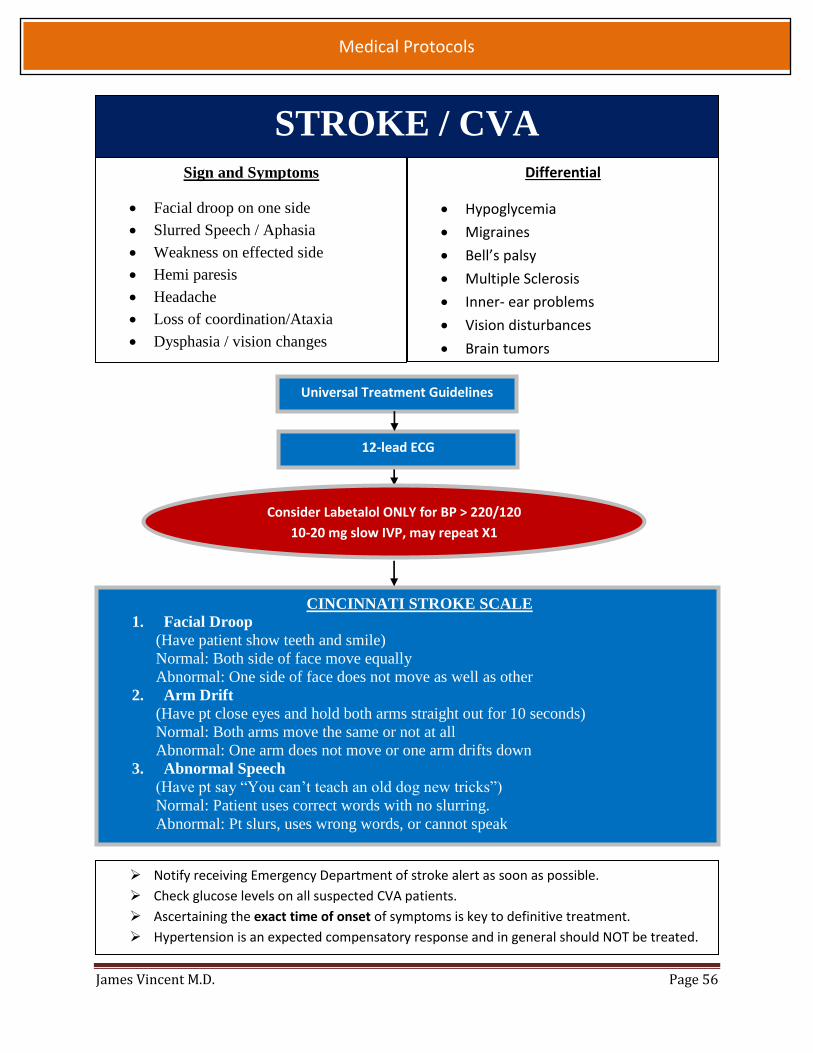
James Vincent M.D. Page 56
Medical Protocols
CINCINNATI STROKE SCALE
1. Facial Droop
(Have patient show teeth and smile)
Normal: Both side of face move equally
Abnormal: One side of face does not move as well as other
2. Arm Drift
(Have pt close eyes and hold both arms straight out for 10 seconds)
Normal: Both arms move the same or not at all
Abnormal: One arm does not move or one arm drifts down
3. Abnormal Speech
(Have pt say “You can’t teach an old dog new tricks”)
Normal: Patient uses correct words with no slurring.
Abnormal: Pt slurs, uses wrong words, or cannot speak
Notify receiving Emergency Department of stroke alert as soon as possible.
Check glucose levels on all suspected CVA patients.
Ascertaining the exact time of onset of symptoms is key to definitive treatment.
Hypertension is an expected compensatory response and in general should NOT be treated.
Universal Treatment Guidelines
Consider Labetalol ONLY for BP > 220/120
10-20 mg slow IVP, may repeat X1
12-lead ECG
Sign and Symptoms
Facial droop on one side
Slurred Speech / Aphasia
Weakness on effected side
Hemi paresis
Headache
Loss of coordination/Ataxia
Dysphasia / vision changes
Differential
Hypoglycemia
Migraines
Bell’s palsy
Multiple Sclerosis
Inner- ear problems
Vision disturbances
Brain tumors
STROKE / CVA
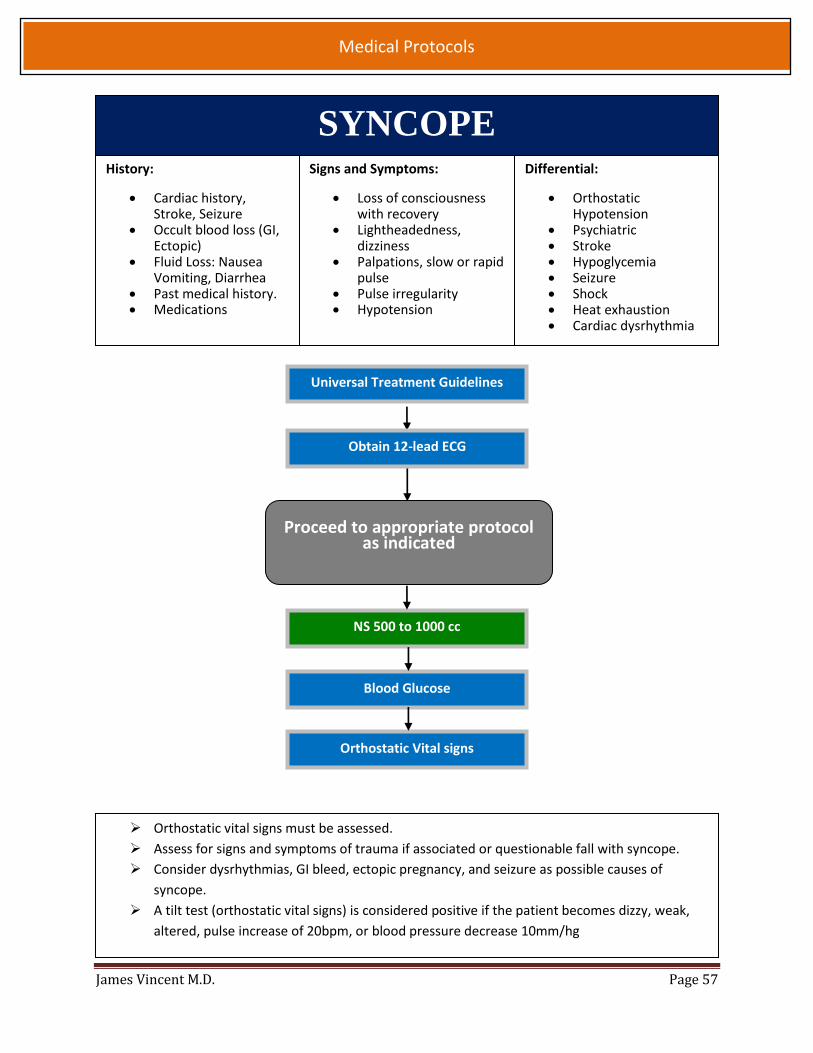
James Vincent M.D. Page 57
Medical Protocols
SYNCOPE Signs and Symptoms:
Loss of consciousness with recovery
Lightheadedness, dizziness
Palpations, slow or rapid pulse
Pulse irregularity Hypotension
Differential:
Orthostatic Hypotension
Psychiatric Stroke Hypoglycemia Seizure Shock Heat exhaustion Cardiac dysrhythmia
History:
Cardiac history, Stroke, Seizure
Occult blood loss (GI, Ectopic)
Fluid Loss: Nausea Vomiting, Diarrhea
Past medical history. Medications
Universal Treatment Guidelines
Proceed to appropriate protocol as indicated
NS 500 to 1000 cc
Blood Glucose
Orthostatic Vital signs
Orthostatic vital signs must be assessed.
Assess for signs and symptoms of trauma if associated or questionable fall with syncope.
Consider dysrhythmias, GI bleed, ectopic pregnancy, and seizure as possible causes of
syncope.
A tilt test (orthostatic vital signs) is considered positive if the patient becomes dizzy, weak,
altered, pulse increase of 20bpm, or blood pressure decrease 10mm/hg
Obtain 12-lead ECG

James Vincent M.D. Page 58
Medical Protocols
ACUTE CORONARY SYNDROME Signs and Symptoms:
Non-Reproducible chest pain History of cardiac events Location (Substernal, Epigastric, Arm,
Neck, Shoulder) Radiation of pain Nausea, vomiting, or dizziness Dyspnea
Differential Diagnosis:
Trauma vs. Medical Pulmonary Embolism Asthma / COPD Pneumothorax Aortic dissection or aneurysm Chest wall injury or pain GE reflux or Hiatal Hernia Overdose of Cocaine or
Methamphetamine
Universal Treatment Guidelines
STEMI
NON-STEMI
Keep scene time <15 min.
Consider NS Bolus of 250-500cc
for suspected Inferior MI
Establish 2nd IV of at least 18
gauge while transporting
For continued pain see pain
management protocol
Consider Protocols as needed for, Hypotension,
HTN, Nausea / Vomiting, Dysrhythmias
Notify receiving Emergency Department as soon as possible for suspected STEMI. Patients with marginal Blood Pressure and concern for inferior Right sided STEMI, IV access is
preferred before the administration of Nitroglycerin. Avoid Nitroglycerin in any patient who has used Viagra or Levitra in the past 24 hours, or
Cialis in the past 36 hours. Diabetics, geriatric patients, and females may have atypical pain or only generalized
complaints. An IV is not required for administration of Nitroglycerin. BP drop is expected after receiving Nitro. Do not hold further doses unless SBP < 90.
Aspirin 324 mg PO chewed
12 lead EKG
Nitroglycerin Spray every
5 min X3 with SBP of >90
Transmit EKG to receiving hospital

James Vincent M.D. Page 59
Medical Protocols
ACUTE CORONARY SYNDROME

James Vincent M.D. Page 60
Medical Protocols
SUPRA-VENTRICULAR TACHYCARDIA
Adenosine 6mg
fast IVP
IV, NS Bolus 250-500 cc
Adenosine 12mg
fast IVP, may repeat X1
Synchronized cardioversion
50 joules
Synchronized cardioversion
100 joules
Synchronized cardioversion
150 joules
Signs and Symptoms:
Rapid Regular Pulse >150, palpitations
Feeling weak, light headed, or dizzy
Differential Diagnosis:
Ventricular Tachycardia
A-Fib W/ RVR
Unstable is defined by severe hypotension, altered mental status and/or weak or absent
radial pulses.
Sedation should not be used with hemodynamically unstable pts.
SVT refractory to Adenosine can be treated with Diltiazem if not contra-indicated.
Vagal maneuvers are contraindicated if pt has a HX of CVA, carotid surgery or carotid bruits.
CONTINUOUS PRINT-OUT OF MONITOR TRACING DURING CONVERSION IS VERY HELPFUL
FOR RECEIVING HOSPITAL’S CARDIOLOGIST.
Universal Treatment Guidelines
Diltiazem 10-20 mg
Repeat 25mg X1 in
10 min.
Consider Pain Management
and/or Anxiety Protocols
12 Lead EKG
STABLE
Amiodarone 150 mg
over 10 min
YES NO
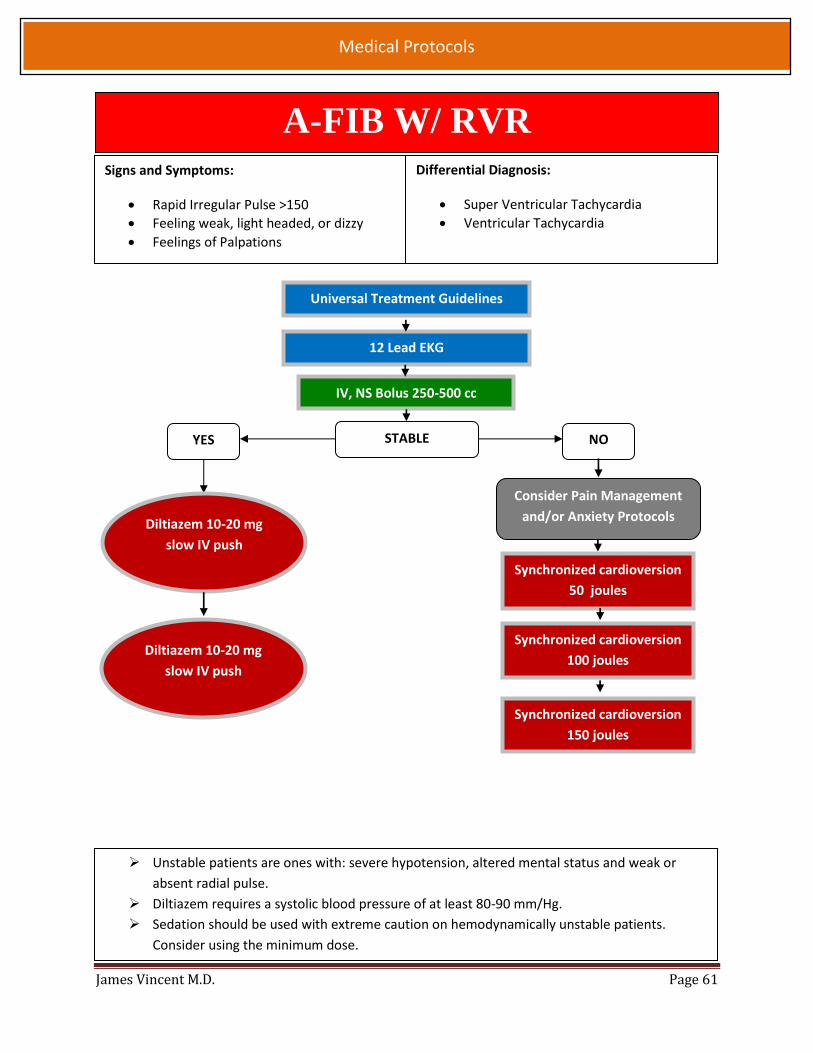
James Vincent M.D. Page 61
Medical Protocols
A-FIB W/ RVR
Signs and Symptoms:
Rapid Irregular Pulse >150
Feeling weak, light headed, or dizzy
Feelings of Palpations
Differential Diagnosis:
Super Ventricular Tachycardia
Ventricular Tachycardia
Universal Treatment Guidelines
12 Lead EKG
IV, NS Bolus 250-500 cc
STABLE NO
Consider Pain Management
and/or Anxiety Protocols
Synchronized cardioversion
50 joules
Synchronized cardioversion
100 joules
Synchronized cardioversion
150 joules
YES
Diltiazem 10-20 mg
slow IV push
Diltiazem 10-20 mg
slow IV push
Unstable patients are ones with: severe hypotension, altered mental status and weak or
absent radial pulse.
Diltiazem requires a systolic blood pressure of at least 80-90 mm/Hg.
Sedation should be used with extreme caution on hemodynamically unstable patients.
Consider using the minimum dose.

James Vincent M.D. Page 62
Medical Protocols
VENTRICULAR TACHYCARDIA W/ PULSE
Signs and symptoms:
Runs or sustained Ventricular Tachycardia.
Conscious, rapid pulse
Chest Pain, Shortness of breath
Dizziness
QRS >0.12 sec.
Differential:
Artifact / Device Failure
Drugs
Pulmonary
Universal Treatment Guidelines
Wide, regular rhythm with QRS >0.12 sec?
No
Pulse
YES
Cardiac
Arrest
Protocol
STABLE UNSTABLE
Synchronized Cardioversion
150 joules
May repeat as needed
Consider Pain Management
and/or Anxiety Protocols
For witnessed / monitored ventricular tachycardia try having the patient cough.
Polymorphic V-Tach (Torsade’s de Pointes) consider Magnesium Sulfate 2grams IVP
Notify receiving Emergency Department as soon as possible of the patient’s condition.
Brief episodes of ventricular ectopy do not require treatment (Formerly “Ventricular Ectopy”
protocol, which has been removed.)
Amiodarone 150mg
over 10 min
may repeat x1
SVT
Protocol
Narrow
Complex
Amiodarone 150mg
over 10 min
may repeat x1
12 Lead EKG

James Vincent M.D. Page 63
Medical Protocols
SYMPTOMATIC BRADYCARDIA Signs and Symptoms
Heart rate <60
Chest Pain
Hypotension (systolic >90)
Ventricular ectopy
Dyspnea
Altered Mental Status
Seizures
Differential Diagnosis
Beta-blocker Overdose
Hypothermia
Digoxin Toxicity
Calcium Channel Overdose
Malnutrition
Increased ICP
TRANSCUTANEOUS PACING AT A RATE
OF 60 AT LOWEST MILLIAMP SETTING
THAT OBTAINS CAPTURE.
ATROPINE 0.5MG-1MG
MAY REPEAT q 3-5 MIN
MAX DOSE 3mg
IF HEART RATE >60 AND BP REMAINS <90 SYSTOLIC
SEE HYPOTENSION PROTOCOL
USE CAUTION: Atropine should be omitted for second degree Type ll or Third Degree AV
Heart blocks
DO NOT TREAT BRADYCARDIA IF PT HAS NORMAL BLOOD PRESSURE AND NO SYMPTOMS.
Universal Treatment Guidelines
Consider Pain Management
and/or Anxiety Protocols
12 Lead EKG

James Vincent M.D. Page 64
Medical Protocols
ADULT CARDIAC ARREST
EMT B/I to use AED
for rhythm analysis
and shocks
EMT-I may use
Epinephrine 1mg
q3-5 min as in
diagram
EMT-I may
establish IO when
indicated

James Vincent M.D. Page 65
Medical Protocols
POST RESUSCITATION Signs and Symptoms:
Return of spontaneous circulation.
Differential Diagnosis:
Continue to address specific differentials
associated with the original
dysrhythmia.
Universal Treatment Guidelines
Hypotension
Normal Saline Fluid
Bolus 500cc
Significant Ectopy
Bradycardia
Ventricular
Tachycardia with a
pulse Protocol
Bradycardia
Protocol
Notify receiving emergency department as soon as possible.
Hyperventilation leads to negative patient outcomes and should be avoided.
Immediately post resuscitation patients should be treated conservatively. Remember the
negative side effects of cardiac drugs such as increasing myocardial oxygen demand.
Hypotension can be caused by injuries resulting from CPR, hypovolemia, pneumothorax and
medication reactions to ALS drugs.
PVC’s that present after resuscitation should rarely be treated until other causes have been
addressed. Remember that an anti-arrhythmic may suppress the ventricular response.
12 Lead EKG
Hypotension
Protocol If cardiac arrest reoccurs
resume appropriate
protocol
Watch for a drop in ETCO2
as an indicator of loss of
pulse

James Vincent M.D. Page 66
Medical Protocols
POST-RESUSCITATION INDUCED HYPOTHERMIA
Criteria
Post Cardiac Arrest with ROSC
Patient Comatose
Non-traumatic etiology
Transport to a facility that will continue procedure
Differential:
Continue to address specific differentials associated with the original dysrhythmia.
Arrests caused by drowning, hanging or asphyxiation can use this protocol.
Return of Spontaneous
Circulation
Criteria for Induced
Hypothermia and initial
temp >34c
Post Resuscitation
Protocol
NO
Advanced Airway NO RSI Protocol
Successful
Expose Patient, Apply Ice Packs
if available to Axilla and groin.
Reassess Temperature >34c and
Shivering <33C
Etomidate 20mg IV/IO Discontinue Cooling Measures
If no advanced airway can be obtained, cooling may only be initiated with online medical direction.
Do not delay transport to initiate cooling patient. Patients may develop metabolic alkalosis with cooling. Do not hyperventilate. Take care to protect patient’s modesty. Undergarments may remain in place during cooling.
Do not use in
Pediatric patients. If patients goes
into cardiac
arrest STOP
procedure and
resume
appropriate
protocol
Cold Saline Bolus 1-2 liters
(if available)
12 Lead EKG ACS Protocol as
needed.
Notify receiving
hospital if STEMI
present.

James Vincent M.D. Page 67
Medical Protocols
HYPERTENSION
History:
Hypertension
Stroke
Medication
Compliance
Pregnancy
Signs and Symptoms:
Systolic BP >180
OR Diastolic BP >110
With one of the following
Headache
Nausea / Vomiting
Chest Pain
Vertigo
Nose Bleed
Shortness of breath
Differential Diagnosis:
Myocardial Infarction
Cushing’s Response-
Bradycardia with
Hypertension
Pre-eclampsia /
Eclampsia
Asymptomatic hypertension does not require treatment regardless of how high the blood
pressure is. Treatment may interfere with compensatory mechanisms and cause harm.
Target Systolic blood pressure should be two thirds of the initial blood pressure.
Do not use labetalol if HR < 60
Labetalol onset 5-10 min with a peak effect of 30 min.
Never treat Blood pressure based on one set of vitals.
Avoid Nitroglycerin in pt who has taken erectile dysfunction drugs in the past 48 hrs
Universal Treatment Guidelines
Nitroglycerin 0.4 mg
spray
may be repeated X2 Labetalol 10-20mg
Slow IV push
Repeat q10 min X2
Neurologic or Other
(OB, renal, nosebleed)
Cardiac (angina, CHF) or
labetalol contraindicated
Enalapril 1.25 mg
Slow IV push
May repeat X1
12 Lead EKG
Nitro spray q5 min
for continued HTN
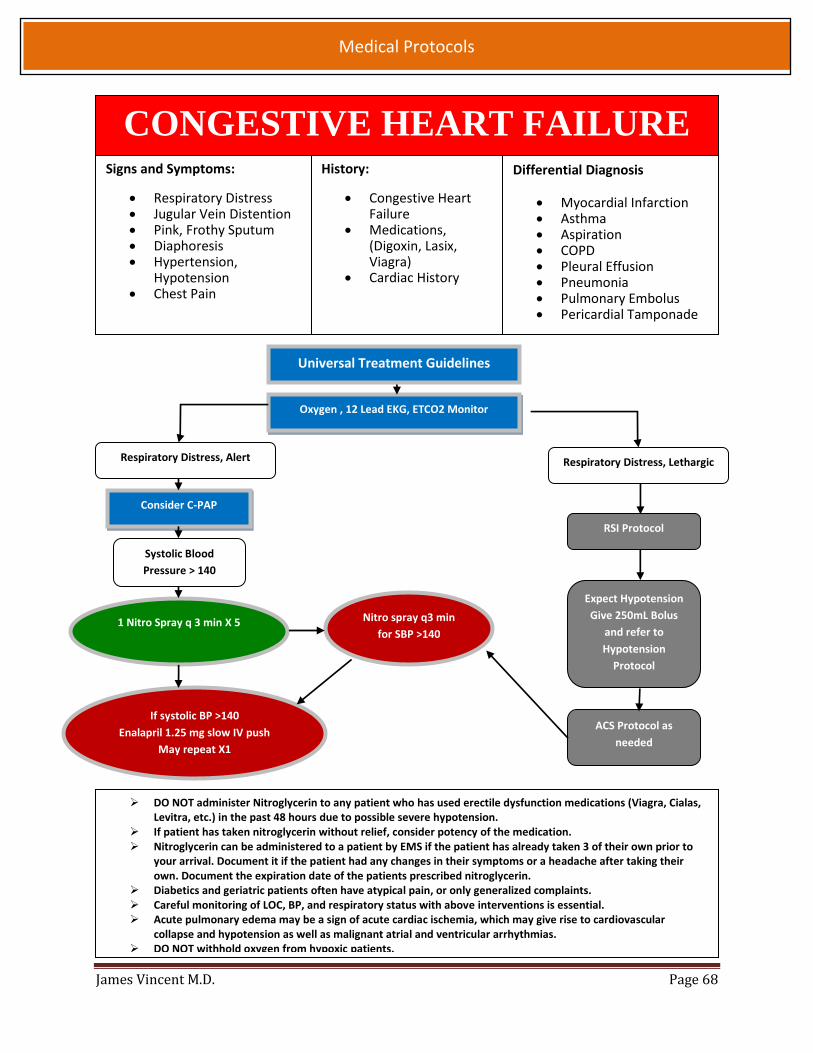
James Vincent M.D. Page 68
Medical Protocols
CONGESTIVE HEART FAILURE Signs and Symptoms:
Respiratory Distress Jugular Vein Distention Pink, Frothy Sputum Diaphoresis Hypertension,
Hypotension Chest Pain
History:
Congestive Heart Failure
Medications, (Digoxin, Lasix, Viagra)
Cardiac History
Differential Diagnosis
Myocardial Infarction Asthma Aspiration COPD Pleural Effusion Pneumonia Pulmonary Embolus Pericardial Tamponade
Respiratory Distress, Alert
Oxygen , 12 Lead EKG, ETCO2 Monitor
Consider C-PAP
Systolic Blood
Pressure > 140
1 Nitro Spray q 3 min X 5
If systolic BP >140
Enalapril 1.25 mg slow IV push
May repeat X1
RSI Protocol
DO NOT administer Nitroglycerin to any patient who has used erectile dysfunction medications (Viagra, Cialas, Levitra, etc.) in the past 48 hours due to possible severe hypotension.
If patient has taken nitroglycerin without relief, consider potency of the medication. Nitroglycerin can be administered to a patient by EMS if the patient has already taken 3 of their own prior to
your arrival. Document it if the patient had any changes in their symptoms or a headache after taking their own. Document the expiration date of the patients prescribed nitroglycerin.
Diabetics and geriatric patients often have atypical pain, or only generalized complaints. Careful monitoring of LOC, BP, and respiratory status with above interventions is essential. Acute pulmonary edema may be a sign of acute cardiac ischemia, which may give rise to cardiovascular
collapse and hypotension as well as malignant atrial and ventricular arrhythmias. DO NOT withhold oxygen from hypoxic patients.
Universal Treatment Guidelines
Respiratory Distress, Lethargic
Expect Hypotension
Give 250mL Bolus
and refer to
Hypotension
Protocol
ACS Protocol as
needed
Nitro spray q3 min
for SBP >140

James Vincent M.D. Page 69
Medical Protocols
Taser barb removal Taser barb rem Taser barb removal oval
VENTRICULAR ECTOPY SELECTIVE SPINAL IMMOBILIZATION
History:
Mechanism of injury Fall height Drugs or alcohol use Auto Pedestrian / Bicycle Accident Diving incidents
Signs and Symptoms:
Focal neurological deficit Any spinal tenderness.
The patient must be able to
look up, touch chin to the
chest and from side, to side
without spinal process pain.
Yes to any item?
Patient will require spinal
motion restriction
Focal Deficit?
Age <5 or >65?
Does the patient have altered
alertness?
Suspected or Known
Intoxication?
Distracting injury?
Spinal Exam: any point
tenderness to spine or with
range of motion?
The decision not to immobilize must be fully documented and include all of the above
historical and exam findings.
Palpate each spinous process to assess for tenderness. Only if no tenderness was elicited,
perform a range of motion exam.
Partial Immobilizations:
o At times securing a patient to a rigid spine board may worsen a spinal injury if
present or may otherwise harm the patient. These patients may be transported in
semi-recumbent position with a c-collar.
o Examples of patients who may not tolerate supine positioning: agitated patients and
patients with decompensated CHF or with kyphosis.
Dangerous mechanism? Ex: Fall > 3feet, mod to high speed MVA,
diving accident, ATV crash, auto-ped?

James Vincent M.D. Page 70
Medical Protocols
calcium gluconate 10% 10cc
CRUSH INJURY Signs and Symptoms:
Pain
Pallor
Pulselessness
Paralysis
Skin cool to the touch
History:
Entrapment of extremity or torso for prolonged
period of times.
Universal Treatment Guidelines
Consider RSI Protocol
Sodium Bicarb 50-100 mEq IV to be administered immediately after removal from entrapment
Observe all crush injuries, even those who look well. Administer intravenous fluids before releasing the crushed body part. This step is especially
important in cases of prolonged crush >4 hours. Crush syndrome can occur in crush scenarios of <1 hour. Sodium Bicarbonate should only be given in instances of entrapment > 2hrs. Suspect hyperkalemia if T waves become peaked, QRS>.12seconds, and / or hypotension
develops. If cardiac arrest occurs after release of entrapment, give Sodium Bicarbonate 1mEq/kg
immediately and every 10 min during CPR.
Extremity Trauma or Amputation Protocols as needed
1-2 L NS
Consider Pain Management
and/or Anxiety Protocols
Calcium Gluconate 10%
1 -2 grams IV over 10 min =
10 -20 mL for arrhythmias

James Vincent M.D. Page 71
Medical Protocols
MAJOR TRAUMA SIGNS AND SYMPTOMS:
DETERMINE EVENTS LEADING TO TRAUMA AND MECHANISM OF INJURY
PAIN, SWELLING, DEFORMITY, BLEEDING, LESIONS
ALTERED MENTAL STATUS, UNCONSCIOUS
HYPOTENSION, SHOCK
DIFFERENTIAL:
TENSION PNEUMOTHORAX / HEMOTHORAX
FLAIL CHEST
PERICARDIAL TAMPONADE
OPEN CHEST WOUND
OPEN / CLOSED HEAD INJURY
SPINAL INJURY
PELVIC / HIP FRACTURE
Universal Treatment Guidelines
CONTROL ALL
MAJOR
BLEEDING
VITAL SIGNS
TITRATE BLOOD
PRESSURE TO AT
LEAST 90 SYSTOLIC
with small NS
boluses 250mL
Consider RSI
Protocol
Consider Tourniquet
Protocol
SPLINT SUSPECTED
FRACTURES
Consider Pain
Management Protocol
GERIATIC PT SHOULD BE EVALUATED WITH A HIGH INDEX OF SUSPENSION.
MECHANISM IS THE BEST INDICATOR OF SERIOUS INJURY.
SCENE TIMES SHOULD NOT BE DELAYED FOR PROCEDURES; THESE SHOULD BE PERFORMED
DURING TRANSPORT WHEN POSSIBLE.
ON SCENE TIME OF 10 MIN OR LESS FOR THE UNSTABLE TRAUMA PT IS THE GOAL.
ALLOW PERMISSIVE HYPOTENSION TO PREVENT FURTHER HEMORRHAGE.
BILATERAL IV OR
IO ACCESS
Consider Needle
Decompression
O2 AS NEEDED DETERMINE
GCS
UNSTABLE
PATIENTS MUST
BE TRANSPORTED
IMMEDIATELY.
Goal Scene Time
< 10 minutes
CONTINUALLY REASSESS
ASSESS FOR
FOCAL NEURO
DEFICITS
AIRWAY AND
CERVICAL SPINE
CONTROL
BREATHING AND
OXYGENATION
CIRCULATION AND
HEMORRHAGE
CONTROL
DISABILITY
ASSESSMENT
EXPOSURE
Consider Antibiotic
Therapy for open long
bone fractures
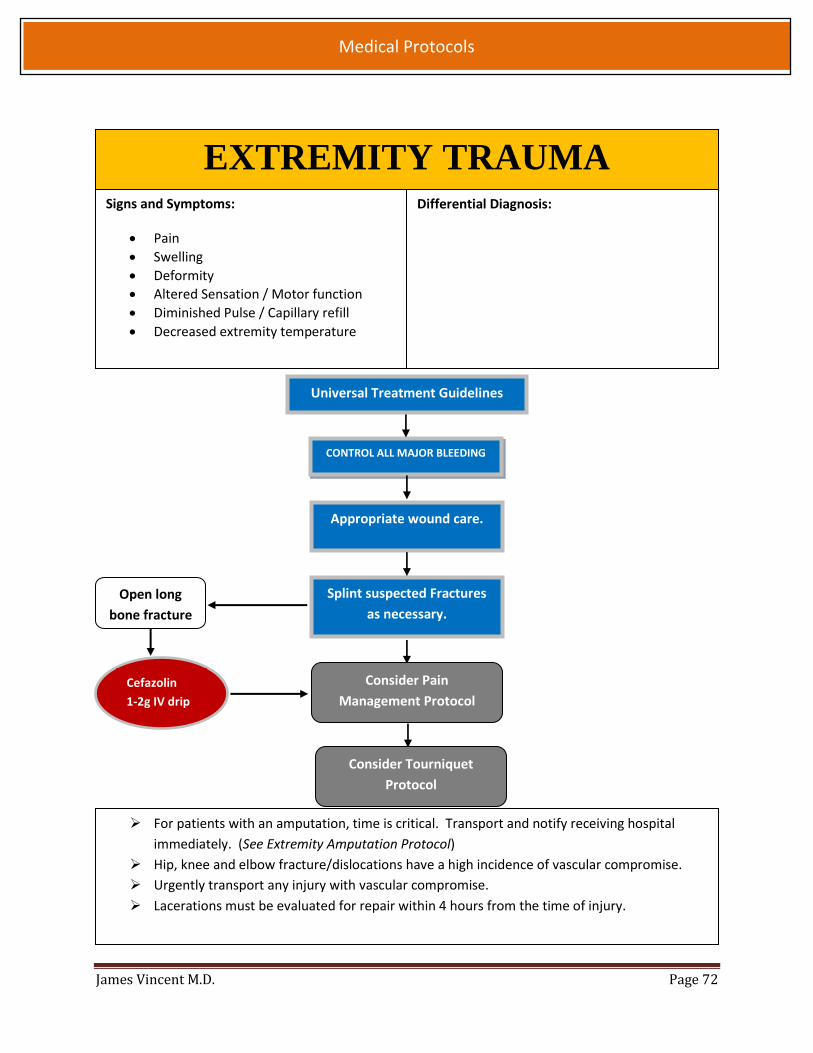
James Vincent M.D. Page 72
Medical Protocols
Open long
bone fracture
EXTREMITY TRAUMA Signs and Symptoms:
Pain
Swelling
Deformity
Altered Sensation / Motor function
Diminished Pulse / Capillary refill
Decreased extremity temperature
Appropriate wound care.
Splint suspected Fractures
as necessary.
CONTROL ALL MAJOR BLEEDING
Differential Diagnosis:
For patients with an amputation, time is critical. Transport and notify receiving hospital
immediately. (See Extremity Amputation Protocol)
Hip, knee and elbow fracture/dislocations have a high incidence of vascular compromise.
Urgently transport any injury with vascular compromise.
Lacerations must be evaluated for repair within 4 hours from the time of injury.
Consider Pain
Management Protocol
Universal Treatment Guidelines
Consider Tourniquet
Protocol
Cefazolin
1-2g IV drip
1-2g IV
1

James Vincent M.D. Page 73
Medical Protocols
EXTREMITY HEMORRHAGE / AMPUTATION
Signs and Symptoms:
Amputation / Partial Amputation
Pain and Swelling
Deformity
Altered Sensations / Motor Function
Differential Diagnosis:
Abrasion
Amputation
Contusion
Dislocation
Fracture
Laceration
Universal Treatment Guidelines
Apply direct pressure to control hemorrhaging.
If unable to control with direct pressure, apply
indirect pressure using arterial pressure points and
elevating the affected limb if possible.
Consider Pain Management
Protocol
If hemorrhage cannot be controlled by direct
pressure and the injury is life threatening consider
tourniquet application
Consider Tourniquet
Transport amputation victims rapidly, as successful replantation is time-dependent.
Hip dislocations, knee and elbow fracture / dislocations have a high chance of vascular
compromise.
Blood loss may be concealed or not apparent with extremity injuries.
Lacerations must be evaluated for repair within 4 hours.
Incomplete Amputation: Splint affected digit / limb in a physiological position.
Amputation:
o All retrievable tissue should be transported. (DO NOT DELAY TRANSPORT for tissue retrieval) o Rinse amputation with normal saline or sterile water. o Wrap amputation in sterile gauze that has been moistened with normal saline or sterile water. o Place in plastic bag or container; place container in separate container filled with ice. (if available) o DO NOT PLACE AMPUTATED PART IN DIRECT CONTACT WITH ICE.
Consider Antibiotic
Therapy for any open long
bone fractures without
amputation
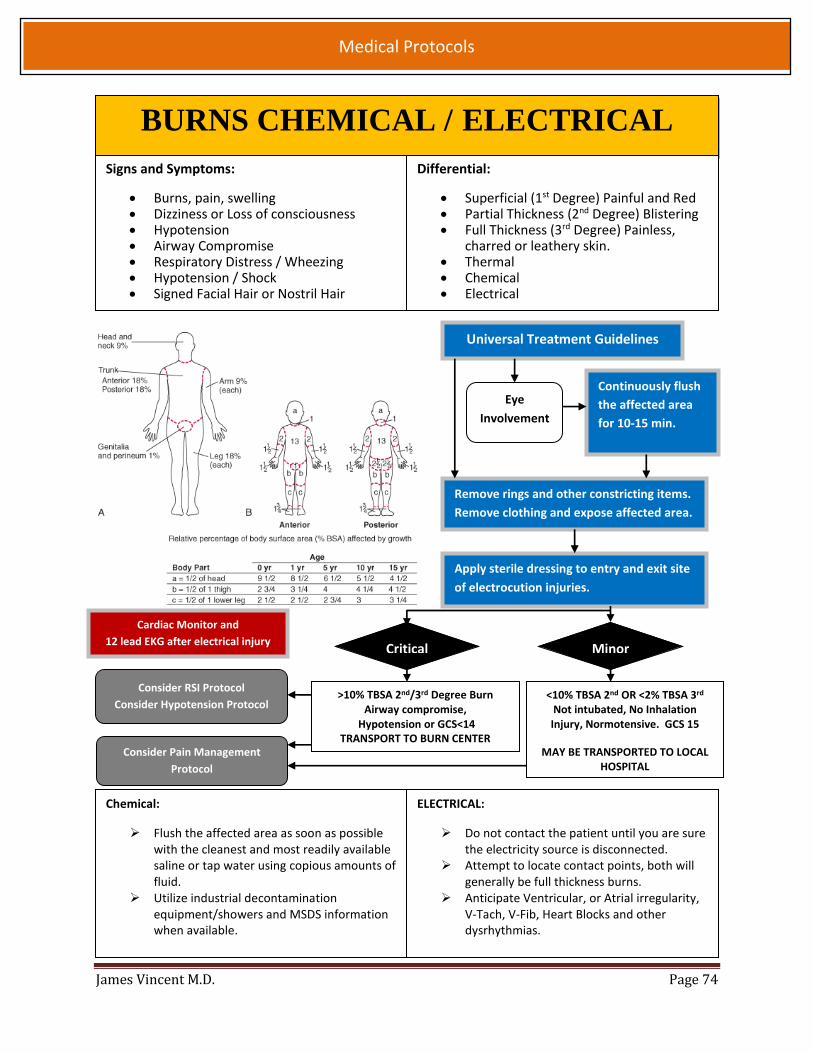
James Vincent M.D. Page 74
Medical Protocols
BURNS CHEMICAL / ELECTRICAL
Signs and Symptoms:
Burns, pain, swelling Dizziness or Loss of consciousness Hypotension Airway Compromise Respiratory Distress / Wheezing Hypotension / Shock Signed Facial Hair or Nostril Hair
Differential:
Superficial (1st Degree) Painful and Red Partial Thickness (2nd Degree) Blistering Full Thickness (3rd Degree) Painless,
charred or leathery skin. Thermal Chemical Electrical
Chemical:
Flush the affected area as soon as possible with the cleanest and most readily available saline or tap water using copious amounts of fluid.
Utilize industrial decontamination equipment/showers and MSDS information when available.
ELECTRICAL:
Do not contact the patient until you are sure the electricity source is disconnected.
Attempt to locate contact points, both will generally be full thickness burns.
Anticipate Ventricular, or Atrial irregularity, V-Tach, V-Fib, Heart Blocks and other dysrhythmias.
Universal Treatment Guidelines
Eye
Involvement
Continuously flush
the affected area
for 10-15 min.
Remove rings and other constricting items.
Remove clothing and expose affected area.
Apply sterile dressing to entry and exit site
of electrocution injuries.
Critical Minor
>10% TBSA 2nd/3rd Degree Burn Airway compromise,
Hypotension or GCS<14 TRANSPORT TO BURN CENTER
<10% TBSA 2nd OR <2% TBSA 3rd Not intubated, No Inhalation Injury, Normotensive. GCS 15
MAY BE TRANSPORTED TO LOCAL HOSPITAL
Consider RSI Protocol
Consider Hypotension Protocol
Consider Pain Management
Protocol
Cardiac Monitor and
12 lead EKG after electrical injury

James Vincent M.D. Page 75
Medical Protocols
BURNS - THERMAL Signs and Symptoms:
Burns, pain, swelling Dizziness or Loss of consciousness Hypotension Airway Compromise Respiratory Distress / Wheezing Hypotension / Shock Signed Facial Hair or Nostril Hair
Differential:
Superficial (1st Degree) Painful and Red Partial Thickness (2nd Degree) Blistering Full Thickness (3rd Degree) Painless,
charred or leathery skin. Thermal Chemical Electrical
Assure whatever caused the burn is no longer contacting the skin.
Early intubation is necessary for patients with significant inhalation injuries.
Burn patients are prone to hypothermia – NEVER cool or apply ice to the burned area.
Other burns ideally treated at a Burn Center: - Feet, hands, face, genital burns - Circumferential burns (due to
possible vascular compromise) - Any 3rd degree burn >2% TBSA - Burns with associated trauma - Nontrivial Pediatric burns - Burns in adults > 50, esp. with
underlying comorbid conditions
Universal Treatment Guidelines
Critical Minor
>10% TBSA 2nd/3rd Degree Burn Airway compromise,
Hypotension or GCS<14 TRANSPORT TO BURN CENTER
<10% TBSA 2nd OR <2% TBSA 3rd Not intubated, No Inhalation Injury, Normotensive. GCS 15
MAY BE TRANSPORTED TO LOCAL HOSPITAL
Pain Management Protocol
Cool the wound with normal saline, cover burn with dry sterile dressing.
Remove rings, bracelets, and other constricting articles.
Consider RSI Protocol
Assess Airway
Determine TBSA/depth of Burn
NS infusion < 6 yo 125 mL/hour IV 6-13 yo 250 mL/hour IV 14 + yo 500 mL/hour IV

James Vincent M.D. Page 76
Medical Protocols
MARINE LIFE ENVENOMATIONS History:
Type of bite or sting
Time, location and size of bite or sting.
Any prior reaction
Rabies and tetanus risk & status
Immunocompromised
Differential:
Snake Bite
Skin Infections
Infection risk
Rabies
Tetanus
Marine Life
Cellulitis
Transport patients with severe systemic response or allergic reaction to jellyfish stings. Jellyfish stings in the Galveston area are rarely serious despite the amount of pain. Rarely
toxic varieties can drift into the area and the patient will present in imminent collapse. Stingray envenomation require medical attention due to the high risk of infection and risk of
retained barbs or foreign mater in the wound. Transport and treat patients with high BSA % of jellyfish stings or patients with stings to the
mucosa due to the risk for infection, severe pain and cosmetic damage.
Signs and Symptoms:
Description of the injury
Rash: local or generalized
Hypotension
Respiratory Distress
Vomiting
Headache
JELLYFISH STINGRAY
Irrigate with copious
amounts of saline over
the wound.
Advise the Pt that if they
have mild pain after
treatment a topical
antihistamine may help.
If able immerse the
affected site in very hot
water or place hot packs
to the affected area.
Advise pt to allow EMS to
transport PT. for proper
wound care and to
ensure no foreign
material remains in the
wound.
Consider Pain
Management
Protocol
NOTE: Vinegar irrigation of jellyfish wounds is no longer recommended, (except in cases of Pacific box jellyfish or Atlantic Portuguese man-of-war stings, which are not endemic to Galveston.)

James Vincent M.D. Page 77
Medical Protocols
Consider Anaphylaxis and
Hypotension Protocols
SNAKE BITE History:
Type of bite or sting.
Time location and size of bite or sting.
Any prior reaction.
Rabies and tetanus risk & status.
Immunocompromised
Differential:
Animal or Human Bite
Skin Infections
Infection Risk
Rabies Risk
Tetanus Risk
Insect Bite
Marine Life
Signs and Symptoms:
Swelling
Allergic reaction
Hypotension or Shock
Difficulty Breathing
Signs of Systemic Response
Universal Treatment Guidelines
Immediate transport to a trauma
center.
Keep pt movement to a minimum. Remove items that may constrict swelling tissue. Document size and time of edema near the injury site. When transporting from Moody Gardens bring anti-venin if available with the patient
and all the snake identification card and all records sent by Moody Gardens. If the patient is from Moody Gardens then choose the transport destination
requested by Moody Gardens staff based upon their training and knowledge.
Consider Pain
Management Protocol
DO NOT BRING DEAD OR LIVE SNAKES TO THE ER
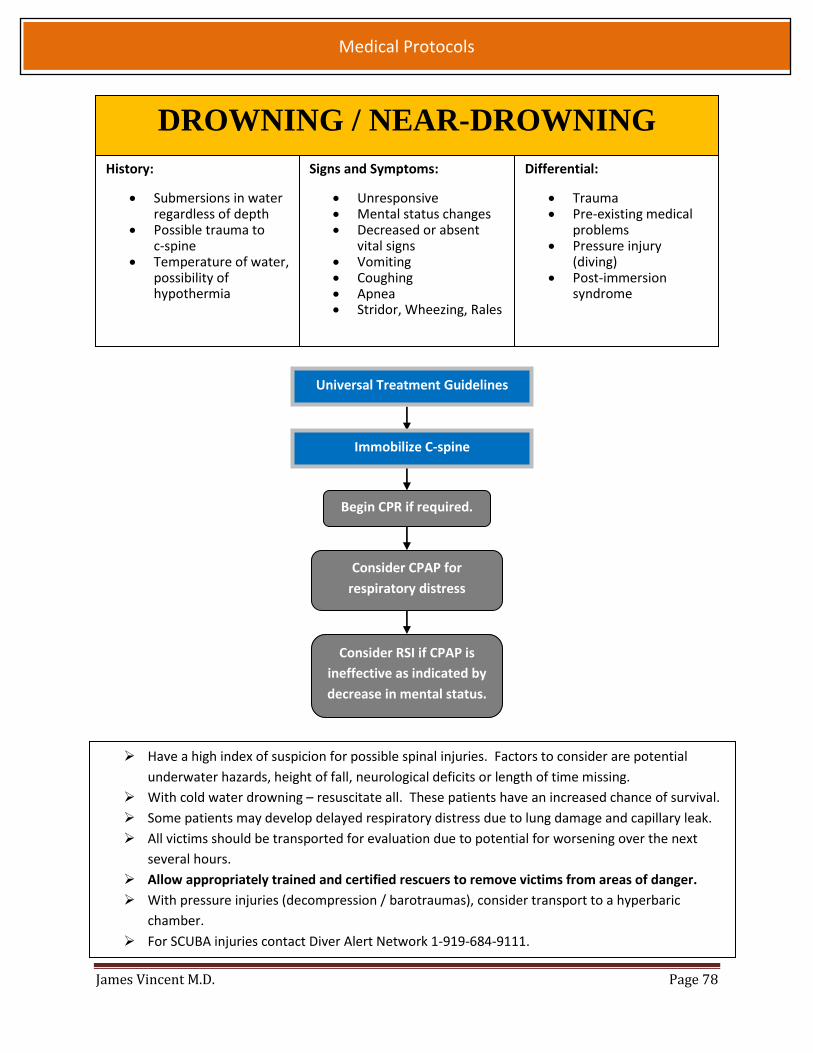
James Vincent M.D. Page 78
Medical Protocols
DROWNING / NEAR-DROWNING
History:
Submersions in water regardless of depth
Possible trauma to c-spine
Temperature of water, possibility of hypothermia
Differential:
Trauma Pre-existing medical
problems Pressure injury
(diving) Post-immersion
syndrome
Signs and Symptoms:
Unresponsive Mental status changes Decreased or absent
vital signs Vomiting Coughing Apnea Stridor, Wheezing, Rales
Begin CPR if required.
Consider CPAP for
respiratory distress
Consider RSI if CPAP is
ineffective as indicated by
decrease in mental status.
Have a high index of suspicion for possible spinal injuries. Factors to consider are potential
underwater hazards, height of fall, neurological deficits or length of time missing.
With cold water drowning – resuscitate all. These patients have an increased chance of survival.
Some patients may develop delayed respiratory distress due to lung damage and capillary leak.
All victims should be transported for evaluation due to potential for worsening over the next
several hours.
Allow appropriately trained and certified rescuers to remove victims from areas of danger.
With pressure injuries (decompression / barotraumas), consider transport to a hyperbaric
chamber.
For SCUBA injuries contact Diver Alert Network 1-919-684-9111.
Universal Treatment Guidelines
Immobilize C-spine

James Vincent M.D. Page 79
Medical Protocols
NO Crowing
ACTIVE LABOR Signs and Symptoms
Evident gravid uterus
Spasmodic pain
Vaginal discharge or bleeding
Crowning or the urge to push
Meconium
Differential Diagnosis:
Prolapsed cord
Placenta Previa
Abruptio Placenta
Abnormal Presentation o Buttock o Hand o Foot
Universal Treatment Guidelines
Left Lateral Position
Hypotension or Vaginal
Bleeding;
Abnormal Presentation
YES
OB Emergency
Protocol or
Difficult Child
Birth Protocol
NO Crowning
Crowning >36 Weeks
Crowning <36 Weeks,
or Multiple Gestation
Rapid Transport
Child Birth
Procedure
NO
Document all times. (Delivery, Contraction Frequency, and Length)
If Maternal Seizures occur, refer to OB Emergencies Protocol.
After delivery, massaging the uterus (lower abdomen) will promote uterine contractions and
help control post-partum bleeding.
Some perineal bleeding is normal with any child birth, large quintiles of blood or free
bleeding are not.
Record APGAR at 1 min. and 5 minutes after child birth.
Transport

James Vincent M.D. Page 80
Medical Protocols
Ectopic Pregnancy
Should be considered as a
possibility for patients with severe
abdominal/pelvic pain with known
pregnancy
Normal Saline 500-1000cc NS Bolus
Consider Pain Management Protocol
All of the following are considered priority symptoms and should be
transport to UTMB or CLRMC due to possible need for emergency surgery.
Abrupto Placenta
Should be considered for pregnant
patients complaining of severe
“ripping” pain with possible
hypotension.
High flow O2, position on left side
w/ padding;
NS Bolus 500-1000cc to maintain
SBP >100
OB EMERGENCIES
Eclampsia
Magnesium Sulfate 50% 2 gm
in 50 mL NS IV saline wide
open max 4 grams
Universal Treatment Guidelines
Diazepam 5 mg IV for active
seizures refractory to
magnesium sulfate
Eclampsia is described as
seizures in a pregnant woman
that are not related to a
preexisting brain condition.
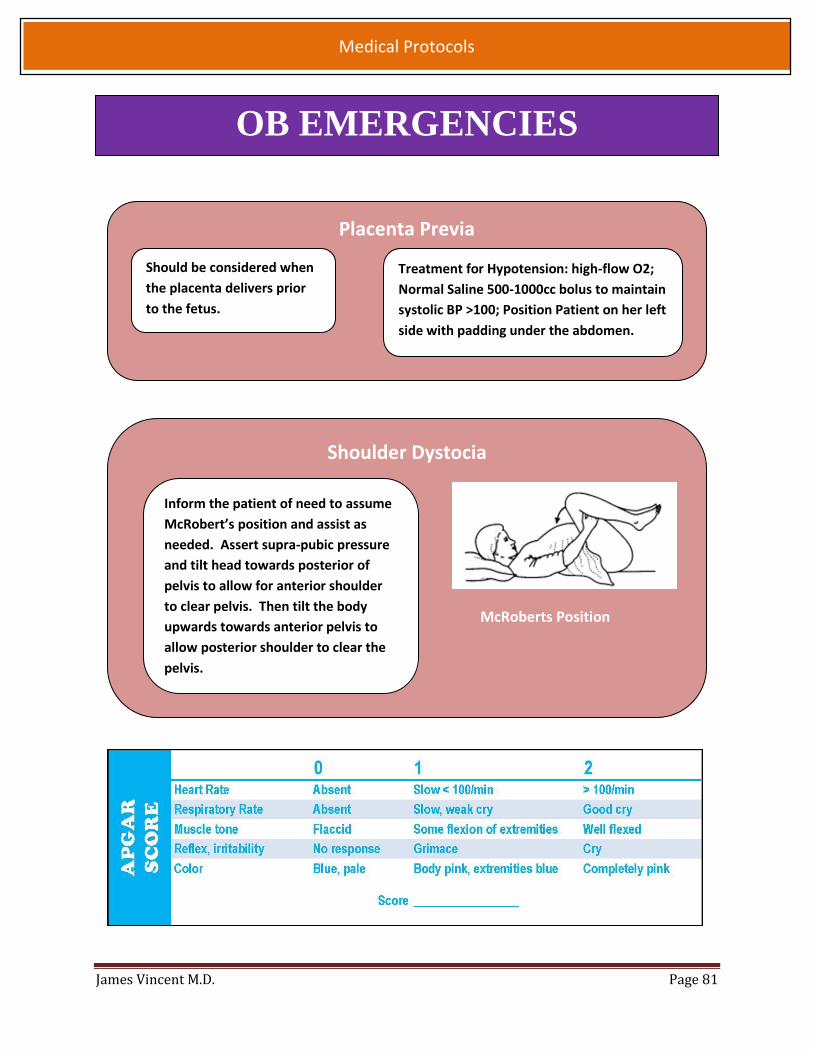
James Vincent M.D. Page 81
Medical Protocols
Placenta Previa
Should be considered when
the placenta delivers prior
to the fetus.
Treatment for Hypotension: high-flow O2;
Normal Saline 500-1000cc bolus to maintain
systolic BP >100; Position Patient on her left
side with padding under the abdomen.
Shoulder Dystocia
McRoberts Position
Inform the patient of need to assume
McRobert’s position and assist as
needed. Assert supra-pubic pressure
and tilt head towards posterior of
pelvis to allow for anterior shoulder
to clear pelvis. Then tilt the body
upwards towards anterior pelvis to
allow posterior shoulder to clear the
pelvis.
OB EMERGENCIES

James Vincent M.D. Page 82
Medical Protocols
NEONATAL RESUSCITATION
Universal Treatment Guidelines
Delivery of Newborn
Term gestation?
Breathing or crying?
Good muscle tone?
Good color?
Breathing, HR >100,
but cyanotic
O2 By Mask or Blow-by
Persistent
Cyanosis
Apneic, Gasping
or HR <100
HR<60
Chest Compressions
Pediatric Cardiac
Arrest Protocol &
Transport
Prepare for RSI
Protocol if
apnea/cyanosis
persist
Observational Care &
Transport
Routine Care
Provide warmth
Clear airway if needed
Dry
Ongoing evaluation
Provide warmth
Position and clear the airway
Dry, stimulate, reposition
Evaluate HR, Respiration, Color
YES
10-15 rapid
ventilations with
BVM will often
stimulate
spontaneous
breathing
NO
Ventilate with PPV

James Vincent M.D. Page 83
Medical Protocols
Insert IO
EMT-I
may use
Epinephr
ine
ET Tube size Uncuffed Cuffed
0-1yr 3.5 3.0
1-2yr 4.0 3.5
>2yr 4+(age/4) 3.5+age/4)
Consider
advanced
airway
PEDIATRIC CARDIAC ARREST
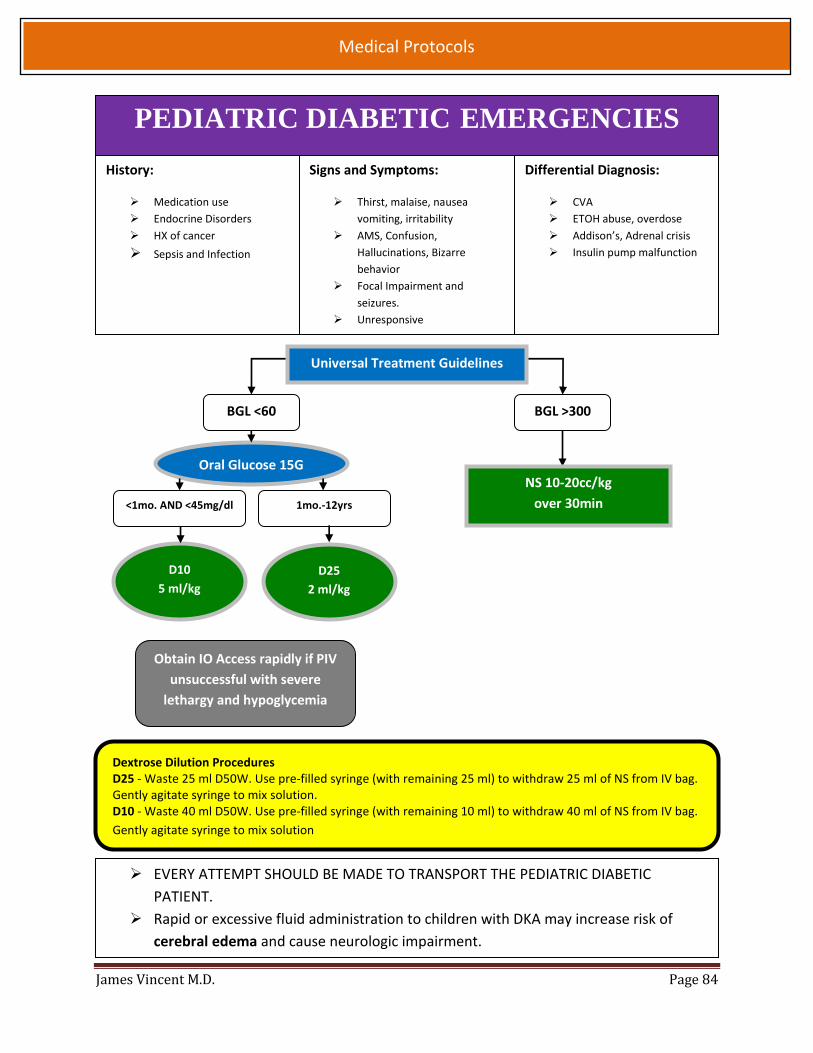
James Vincent M.D. Page 84
Medical Protocols
PEDIATRIC DIABETIC EMERGENCIES
Dextrose Dilution Procedures D25 - Waste 25 ml D50W. Use pre-filled syringe (with remaining 25 ml) to withdraw 25 ml of NS from IV bag. Gently agitate syringe to mix solution. D10 - Waste 40 ml D50W. Use pre-filled syringe (with remaining 10 ml) to withdraw 40 ml of NS from IV bag.
Gently agitate syringe to mix solution
History:
Medication use
Endocrine Disorders
HX of cancer
Sepsis and Infection
Signs and Symptoms:
Thirst, malaise, nausea
vomiting, irritability
AMS, Confusion,
Hallucinations, Bizarre
behavior
Focal Impairment and
seizures.
Unresponsive
Differential Diagnosis:
CVA
ETOH abuse, overdose
Addison’s, Adrenal crisis
Insulin pump malfunction
Oral Glucose 15G
BGL <60 BGL >300
D25
2 ml/kg
D10
5 ml/kg
1mo.-12yrs
EVERY ATTEMPT SHOULD BE MADE TO TRANSPORT THE PEDIATRIC DIABETIC
PATIENT.
Rapid or excessive fluid administration to children with DKA may increase risk of
cerebral edema and cause neurologic impairment.
Universal Treatment Guidelines
NS 10-20cc/kg
over 30min <1mo. AND <45mg/dl
Obtain IO Access rapidly if PIV
unsuccessful with severe
lethargy and hypoglycemia

James Vincent M.D. Page 85
Medical Protocols
PEDIATRIC PAIN MANAGEMENT Clinical Indications:
Patients that need pain management and are unable to obtain adequate relief with non-
pharmaceutical measures
For sickle cell Patients also consider 5cc/kg bolus of Normal saline.
For hemodynamically unstable patients Fentanyl should be first line treatment.
Morphine should be administered only with systolic pressure >90 and pt is not presenting
with signs of imminent circulatory collapse.
Consider administration of Zofran early when administering Morphine.
Our goal is not complete cessation of pain, aim for 50% reduction of pain.
Monitor for respiratory depression.
Morphine 0.1 mg/kg
IV/IM
max dose of 5mg
General Pain
Management
OR
Fentanyl 1 mcg/kg
IV/IN/IM
May repeat X1

James Vincent M.D. Page 86
Medical Protocols
PEDIATRIC ALLERGIC REACTION
Signs and Symptoms:
Stable: o Rash/ Hives / Urticaria o Normal Vital Signs
Unstable: Two or more of the following o Dyspnea or wheezing o Cyanosis o Nausea, vomiting o Excessive Salvation o Edema to Eyelids, Lips, Hands,
Tongue
Differential:
Niacin Overdose
Angioedema due to ACE Inhibitors
Heat rash
Pulmonary Embolism
Foreign body obstruction
Unstable Stable
If Wheezing present see
Respiratory Distress Protocol
Universal Treatment Guidelines
The shorter the time from the patients exposure to the onset of symptoms, the more severe the reaction.
Apply Cold Packs may be applied to bites and stings, in order to reduce the swelling and slow blood flow from the affected are.
Famotidine is an antacid with H2 antagonist properties that has been shown to work well for hives and other allergic reactions.
Epinepherine 1:1000
0.01 mg/kg IM
Max dose 0.3mg
may repeat 1 in 5 min
Benadryl 1mg/kg IV/ IM
Max dose 25mg
Solumedrol 2mg/kg IV/IM
Max dose 125mg
NS Bolus 20cc/kg
Max 1000cc

James Vincent M.D. Page 87
Medical Protocols
PEDIATRIC SEIZURE History:
Reported / Witnessed Seizure activity.
Previous Seizure History
Medical alert tag Information
History of trauma
History of diabetes
History of fever
Differential:
Head Trauma
Tumor
Metabolic, Hepatic, or Renal failure
Hypoxia
Drug medication, non-compliance
Infection / Fever
Alcohol withdrawal
Eclampsia
Stroke
Hyperthermia
Hypoglycemia
Signs and Symptoms:
Decreased mental status
Sleepiness
Incontinence
Observed seizure activity
Evidence of trauma
Unconscious
Status Epilepticus Post-ictal
Blood Glucose
Consider RSI Protocol
Diabetic Protocol
BGL < 60
Seizure Reoccurs
OR
Initial dose of IN Versed should be divided evenly between each nostril. Status Epilepticus is defined as 2 or more successive seizures without a period of consciousness or recovery. This
is a true emergency requiring rapid airway control, treatment, and transport. Grand mal seizures are associated with loss of consciousness, incontinence, and tongue trauma. Petit mal seizures effect only a part of the body and are not usually associated with a loss of consciousness. Jacksonian seizures are seizures which start as focal seizure and become generalized. Be prepared for airway problems and continued seizures. Assess possibility of occult trauma and substance abuse. For any seizures in pregnant patient, follow the OB emergency protocols. Valium (Diazepam) is not effective when administered IM. It should be given IV or rectally only.
Valium 0.2mg/kg
IV Max dose 10mg
Versed 0.1mg/kg
IN/ IV/IM/buccal
Max dose 5 mg
May repeat X1
in 5 min
Universal Treatment Guidelines
Airway Positioning,
Nasopharyngeal airway, O2,
BVM Ventilations as needed
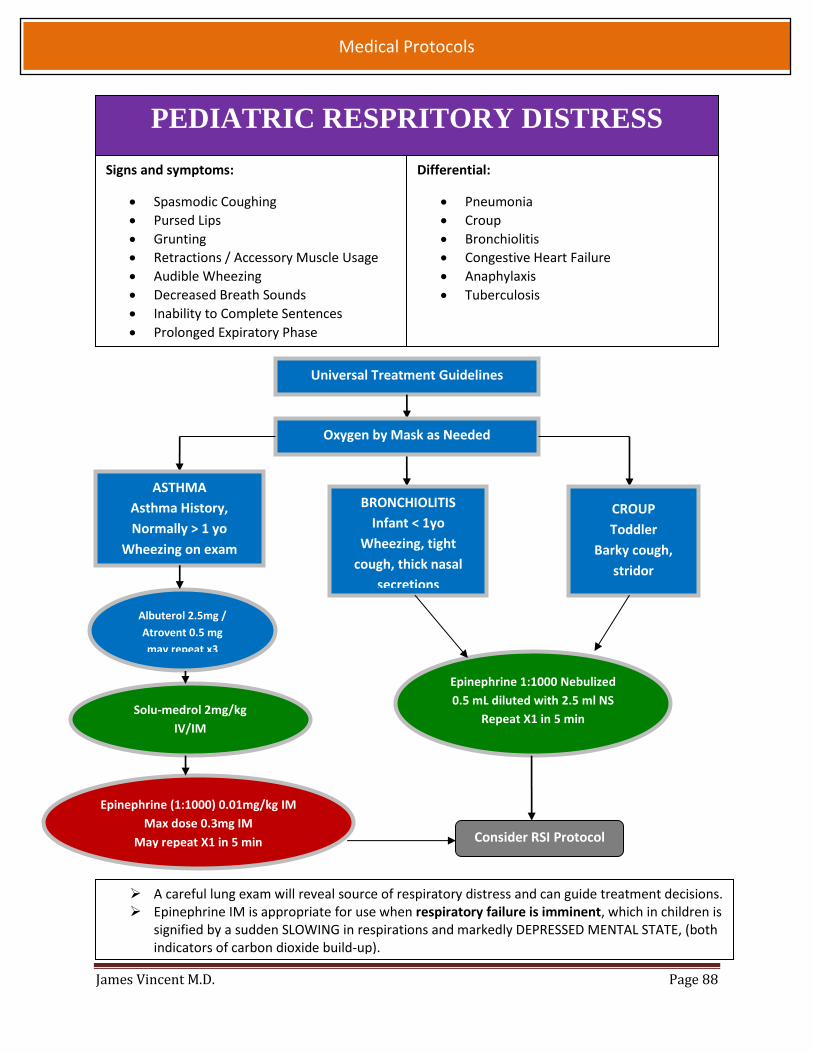
James Vincent M.D. Page 88
Medical Protocols
PEDIATRIC RESPRITORY DISTRESS
Signs and symptoms:
Spasmodic Coughing
Pursed Lips
Grunting
Retractions / Accessory Muscle Usage
Audible Wheezing
Decreased Breath Sounds
Inability to Complete Sentences
Prolonged Expiratory Phase
Differential:
Pneumonia
Croup
Bronchiolitis
Congestive Heart Failure
Anaphylaxis
Tuberculosis
A careful lung exam will reveal source of respiratory distress and can guide treatment decisions. Epinephrine IM is appropriate for use when respiratory failure is imminent, which in children is
signified by a sudden SLOWING in respirations and markedly DEPRESSED MENTAL STATE, (both indicators of carbon dioxide build-up).
Universal Treatment Guidelines
Epinephrine 1:1000 Nebulized
0.5 mL diluted with 2.5 ml NS
Repeat X1 in 5 min
ASTHMA
Asthma History,
Normally > 1 yo
Wheezing on exam
Albuterol 2.5mg /
Atrovent 0.5 mg
may repeat x3
Solu-medrol 2mg/kg
IV/IM
Max Dose 125MG
Epinephrine (1:1000) 0.01mg/kg IM
Max dose 0.3mg IM
May repeat X1 in 5 min
BRONCHIOLITIS
Infant < 1yo
Wheezing, tight
cough, thick nasal
secretions
CROUP
Toddler
Barky cough,
stridor
Oxygen by Mask as Needed
Consider RSI Protocol

James Vincent M.D. Page 89
Medical Protocols
PEDIATRIC BRADYCARDIA Signs and Symptoms
Heart rate <60
Chest Pain
Hypotension
Ventricular ectopy
Dyspnea
Altered Mental Status
Seizures
Differential Diagnosis
Beta-blocker Overdose
Hypothermia
Digoxin Toxicity
Calcium Channel Overdose
Malnutrition
Increased ICP
Universal Treatment Guidelines Definition of Hypotension by Systolic Blood Pressure and Age.
Neonate 0 – 28 days <60 mm Hg
Infants 1 – 12 months <70 mm Hg
Children 1-10 years <70mm Hg + (age in years x2)
Children >10 years <90 mm Hg
Heart rates in pediatric patients.
AGE Awake Rate Sleeping Rate
Newborn to
3months 85 to 205 80 to 160
3 months to
2 years 100 to 190 75 to 160
2 to 10 years 60 to 140 60 to 90
>10 years 60 to 100 50 to 90
Respiratory rates in pediatric patients.
Age Rate
Infant 30-60
Toddler 24-40
Preschooler 22-34
School-age child 18-30
Adolescent 12-16
Epinephrine 1:10 000
0.01mg/kg q 3-5 min.
Assess respirations. Apply O2 and
assist with BVM as necessary.
IF CARDIAC ARREST OCCURS SEE
PEDIATRIC ARREST PROTOCOL
Respiratory Compromise is the
leading cause of pediatric
bradycardia.
Respiratory care should be number
one priority in all pediatric patients.
Start compressions if pulse weak or
signs of lethargy present
Insert IO

James Vincent M.D. Page 90
Medical Protocols
Attempt Vagal maneuver
Adenosine 0.1 mg/kg
fast IVP max 6 mg
IV or Intraosseous Access
STABLE NO YES
Adenosine 0.2 mg/kg
max 12 mg
Synchronized cardioversion
0.5 to 1 joule / kg
Synchronized cardioversion
2 joules/ kg
Synchronized cardioversion
2 joules/ kg
Signs and Symptoms:
Rapid Regular Pulse >180
Feeling weak, light headed, or dizzy
Feelings of Palpations
Differential Diagnosis:
Ventricular Tachycardia
A-Fib W/ RVR
Unstable is defined absence of a radial pulse, feeling light headed or dizzy.
Sedation should not be used on hemodynamically unstable pts.
Print a monitor strip during conversion if patient condition allows.
While a 12-lead EKG is ideal, a 3-lead tracing is adequate for small children, toddlers and infants
Amiodarone 5mg/kg
over 10 min
Universal Treatment Guidelines
Adenosine 0.2 mg/kg
max 12 mg
PEDIATRIC SUPRAVENTRICULAR TACHYCARDIA
Consider Sedation with
Versed 0.1 mg/kg (max 2mg)
OR fentanyl 1mcg/kg

James Vincent M.D. Page 91
Medical Protocols
CAPNOGRAPHY (ETCO2) Indications:
Verification of ET tube placement
Continuous monitoring of ET tube during transport
Shortness of breath / hyperventilation
Status epilepticus
Unconsciousness / poor arousability
Pre and post treatment for asthma / COPD
Indicator of Return of Spontaneous Circulation during cardiac arrest
TECHNIQUE
For Verification of ET tube placement:
1. Visualize the ET tube passing through cords with King Vision (when available)
2. Assess for breath sounds high in the axilla, on the anterior chest, and over the
epigastrium
3. Apply the ETCO2 monitor. REQUIRED WITH ALL INTUBATED PATIENTS
4. Note the following ETCO2 information on the ePCR:
a. The initial ETCO2 value and presence or absence of a good waveform
b. A repeat ETCO2 value one minute or so later and quality of waveform
c. Successful intubation is indicated by:
i. ETCO2 of 5 or greater
ii. Good waveform
5. Continuously monitor waveform and ETCO2 value during transport as a sign of tube
dislodgement or loss of pulse.
For assessment of patients who are short of breath:
1. Apply nasal ETCO2 device
2. Document findings on the ePCR
For all patients, consider the following when ETCO2 is outside the normal range (35-45):
1. Tube dislodgement
2. Poor perfusion
3. Hyperventilation / Hypoventilation

James Vincent M.D. Page 92
Medical Protocols
CAPNOGRAPHY WAVE FORMS
Normal Capnography: A wave form is present; the wave form begins at the base line, raises steeply,
plateaus with a gradual upslope, and quickly returns to the baseline.
End Tidal CO2 normal range: 35-45 mmHg
Hyperventilation
Hypoventilation, Stroke, Seizure, Head Injury, CNS Depression
Asthma, COPD, CHF
ET CO2 monitoring on non-intubated patients - assess severity & effectiveness of treatment.
Bronchospasm will produce a “shark fin” wave form.
CPR with Return of Circulation (ROSC)
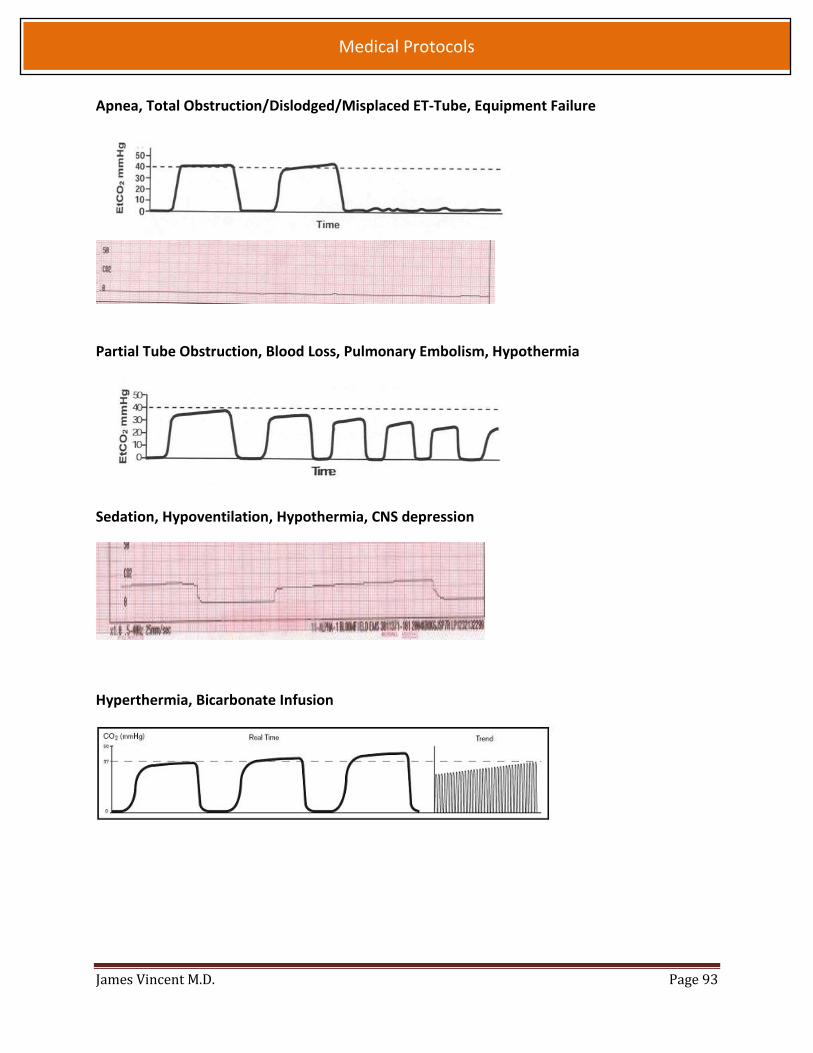
James Vincent M.D. Page 93
Medical Protocols
Apnea, Total Obstruction/Dislodged/Misplaced ET-Tube, Equipment Failure
Partial Tube Obstruction, Blood Loss, Pulmonary Embolism, Hypothermia
Sedation, Hypoventilation, Hypothermia, CNS depression
Hyperthermia, Bicarbonate Infusion

James Vincent M.D. Page 94
Medical Protocols
CHILD BIRTH
NORMAL DELIVERY PROCEDURES
1. Attempt to prevent explosive delivery 2. As delivery of head occurs, suction mouth then nose. 3. If membranes are still intact, instruct the mother to stop pushing and
gently tear the membrane and immediately suction mouth, then nose.
4. Keep newborn warm and dry. 5. Keep newborn at the level of the vagina until the cord is clamped and
cut. 6. Once cord pulsations cease, place one clamp 6 inches from the
newborn and another clamp 9 inches from the newborn. Cut cord between the clamps.
7. Allow newborn to nurse. If multiple births, do not allow nursing until all have been delivered.
8. APGAR score at 1st minute and 5th minute after birth.
Indications:
Imminent Child Birth

James Vincent M.D. Page 95
Medical Protocols
CPAP
Clinical indications:
CPAP is indicated in patients for whom inadequate ventilation is suspected. This could be as
a result of pulmonary edema, pneumonia, COPD, asthma, etc.
PATIENT MUST BE BREATHING FOR PROPER USE OF CPAP.
In asthmatic patients, continuous monitoring is required to reduce the risk of respiratory
depression.
1. Ensure adequate oxygen supply to ventilation device.
2. Explain procedure to Pt.
3. Place the delivery mask over the nose and mouth. Oxygen
should be flowing through the device at this point.
4. Secure the mask with the provided straps starting with the
lower straps until minimal air leak occurs.
5. Adjust Positive End Expiratory Pressure (PEEP) on CPAP device
slowly starting at 0cmH2O until desired pressure is reached.
6. Evaluate the response of patient assessing breath sounds,
general appearance and oxygen saturation if possible.
7. Encourage patient to allow forced ventilation to occur.
8. Document time and response on patient care report.

James Vincent M.D. Page 96
Medical Protocols
EZ-IO INTRAOSSEOUS INFUSION
Indications:
First-line access for all cardiac arrests
Any ALS patient from whom immediate fluid or
medication treatment is indicated. In addition,
patients must have at least one of the following
1. Altered mental status
2. Respiratory compromise
3. Hemodynamic instability
Flow Rate may appear to be slower than those achieved with an IV catheter Ensure the administration of appropriate syringe bolus prior to infusion. NO FLUSH =NO FLOW Pain control for EZ-IO Insertion should be performed prior to initial syringe flush or infusion. Allow to work for
30-60 seconds prior to Syringe flush o For adults administer 40mg of Lidocaine = 2ml of 2% lidocaine for cardiac use. o For pediatric s administer 0.5 MG/KG= 0.05 ml/kg of 2% lidocaine for cardiac use. (20 kg child = 1 mL)
Be cautious of potential air embolism, subcutaneous infiltration, fracture, or osteomyelitis.
1. Prepare Equipment
2. Select insertion site
a. Adult proximal humerus (PREFERRED SITE)
b. Adult proximal tibia: Measure one finger width distal to tibial tuberosity, along,
along the flat aspect of the medial tibia.
c. Pediatric proximal tibia: One finger width distal to the tibial tuberosity OR if unable
to palpate tibial tuberosity; two fingers below the patella along the flat aspect of
the medial tibia.
d. Adult distal tibia: Two finger widths proximal to the medial malleolus and midline
on the medial shaft.
e. Pediatric distal tibia. One finger width proximal to the medial malleolus along the
flat aspect of the medial distal tibia.
3. Prepare the skin with alcohol and/or betadine.
4. Prepare IO driver and needle set; load needle set onto driver.
5. Hold the IO driver in one hand and stabilize the leg near the insertion site with the opposite
hand.
6. Position the driver at the insertion site with the needle at a 90 Degree angle to the surface of
the bone.
7. Before powering the driver, insert the needle through the skin. When you feel the needle is
hitting resistance from the bone, make sure the 5mm line is still visible above the skin.
Power the driver on while applying minimal pressure. Insert the needle until a change in
resistance is noted. Remove the driver from the needle set and the stylet from the catheter.
Attach the connection tubing.
8. Use syringe to rapidly infuse 10ml of NS. If no infiltration is seen, attach the IV line and infuse
fluids or medications as usual. (For adults the IV bag will need to be under pressure.) 9. Secure the needle by looping the tubing and taping it back to the skin.
Contraindications:
Pt with an available secure IV line adequate for
necessary treatment or in whom an IV line can be
placed in a timely fashion.
Pt’s that do not require immediate fluid or
medication therapy. IO SHALL NOT BE
PERFORMED FOR PROPHYLAXIS.
Fracture of bone selected for IO infusion.
Inability to identify landmarks for procedure.
Known previous orthopedic procedure or
preexisting medical disease (such as tumor of the
bone selected for IO infusion.
Severe Burn or infection at the site of insertion.
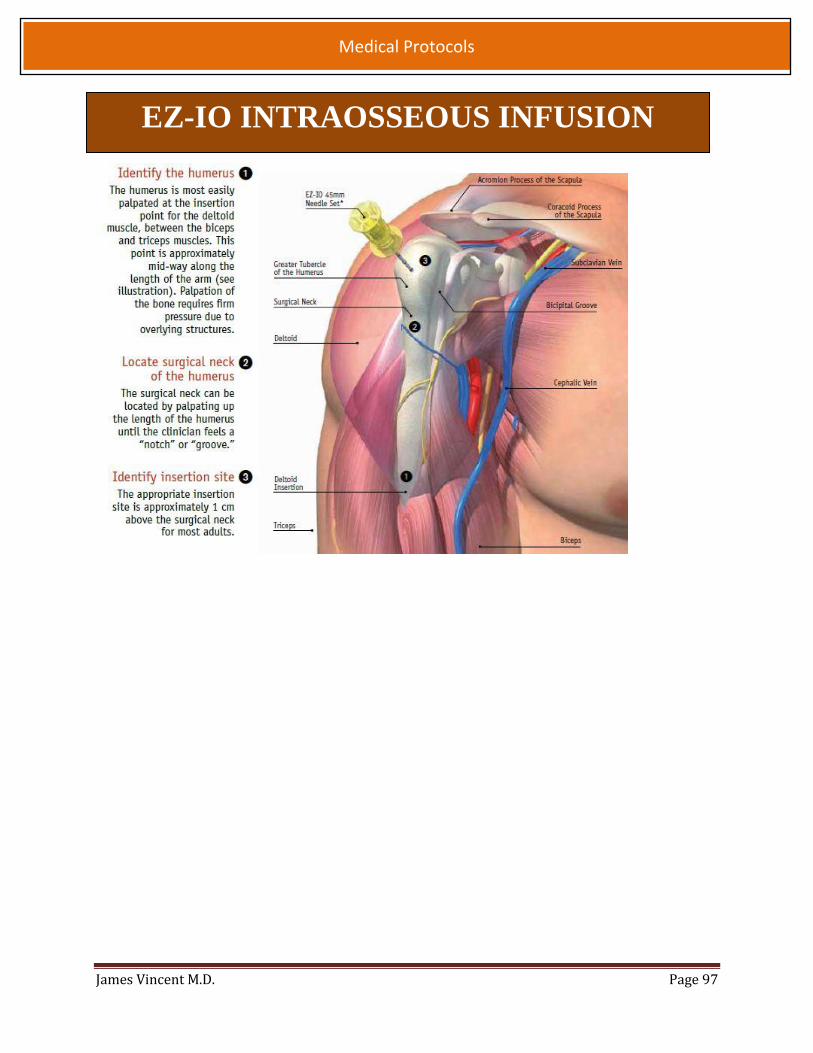
James Vincent M.D. Page 97
Medical Protocols
EZ-IO INTRAOSSEOUS INFUSION

James Vincent M.D. Page 98
Medical Protocols
ontact Droplet and Airborne Precautions
INFECTION CONTROL History:
Febrile Rash, Discharge or
Potential Exposure Immunocompromised Generalized vs. focal
seizure (toddlers)
Differential:
Sepsis Medication Reaction Hyperthyroid Heat Stroke Meningitis Simple febrile seizure
Signs and Symptoms:
Warm, flushed, sweaty Rash Headache Abdominal Pain Seizure type, duration
(for febrile seizures)
Universal Treatment Guidelines
Droplet Precautions
PPE + HEPA Mask for Provider;
Surgical Mask for Patient
Airborne Precautions
Suspect TB, SARS, or drug
resistant pneumonia (MRSA/VRE)
Suspect Influenza, Mumps or
Meningitis
PPE + Surgical Mask for
Provider and Patient
For suspected Ebola Virus Disease patient, see dedicated
section under Fundamentals of Care, p 33

James Vincent M.D. Page 99
Medical Protocols
KENDRICK EXTRICATION DEVICE INDICATIONS:
Used to prepare patients with suspected spinal fracture for extrication and / or movement from a sitting to a supine position.
When a short spine board could not be used.
Application of patients into KED
1. Open KED and place it between the patient’s buttocks and the seat the
patient is sitting on.
2. Center the KED on the patient and position the KED snugly under the
patient’s armpits.
3. Fasten the chest straps, snug up the bottom and the middle straps.
4. Slide the leg straps under the patient’s legs, and around the tops.
5. Secure the leg straps to the same side of the KED.
Movement of the patient in the KED
1. Both rescuers grasp the side handles on opposite sides of the KED. Place other arms under the patient’s legs.
2. Locking their arms together under the patient, the rescuers lift the patient up (keeping the patients legs at a 45 degree angle).
3. Lower the patient onto the long spine board. 4. Undo the leg straps.
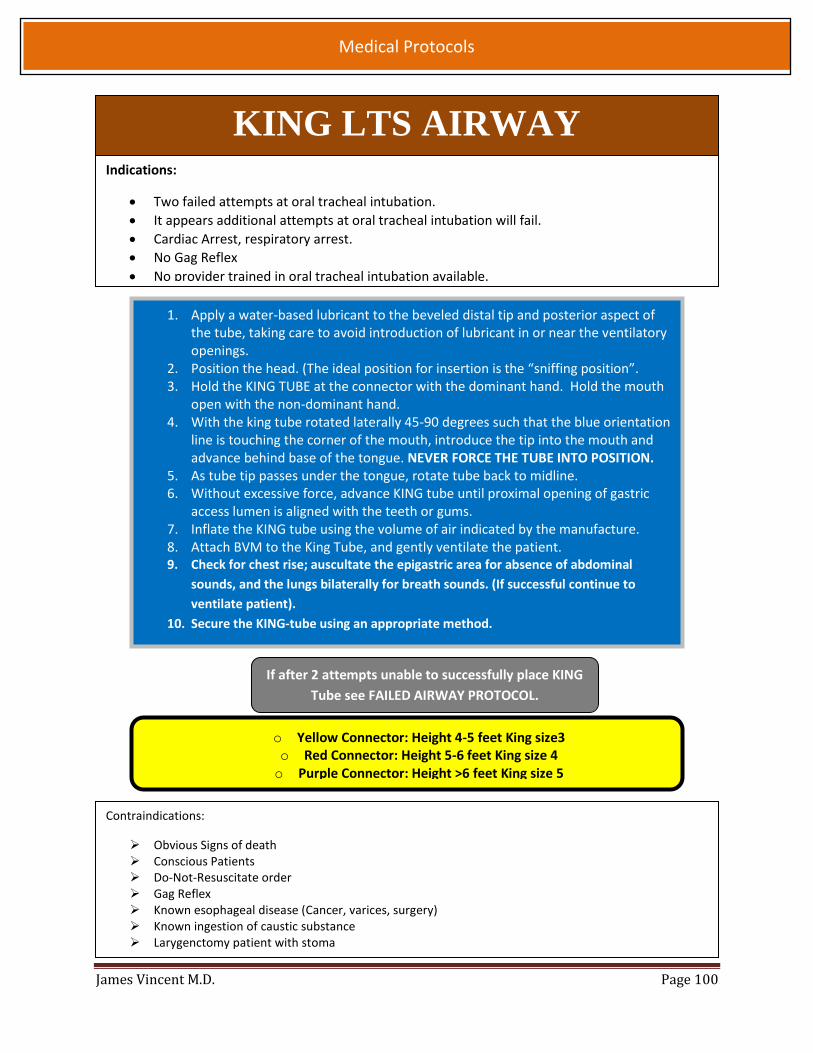
James Vincent M.D. Page 100
Medical Protocols
Indications:
Two failed attempts at oral tracheal intubation.
It appears additional attempts at oral tracheal intubation will fail.
Cardiac Arrest, respiratory arrest.
No Gag Reflex
No provider trained in oral tracheal intubation available.
KING LTS AIRWAY
1. Apply a water-based lubricant to the beveled distal tip and posterior aspect of the tube, taking care to avoid introduction of lubricant in or near the ventilatory openings.
2. Position the head. (The ideal position for insertion is the “sniffing position”. 3. Hold the KING TUBE at the connector with the dominant hand. Hold the mouth
open with the non-dominant hand. 4. With the king tube rotated laterally 45-90 degrees such that the blue orientation
line is touching the corner of the mouth, introduce the tip into the mouth and advance behind base of the tongue. NEVER FORCE THE TUBE INTO POSITION.
5. As tube tip passes under the tongue, rotate tube back to midline. 6. Without excessive force, advance KING tube until proximal opening of gastric
access lumen is aligned with the teeth or gums. 7. Inflate the KING tube using the volume of air indicated by the manufacture. 8. Attach BVM to the King Tube, and gently ventilate the patient. 9. Check for chest rise; auscultate the epigastric area for absence of abdominal
sounds, and the lungs bilaterally for breath sounds. (If successful continue to
ventilate patient).
10. Secure the KING-tube using an appropriate method.
Contraindications:
Obvious Signs of death Conscious Patients Do-Not-Resuscitate order Gag Reflex Known esophageal disease (Cancer, varices, surgery) Known ingestion of caustic substance Larygenctomy patient with stoma
If after 2 attempts unable to successfully place KING
Tube see FAILED AIRWAY PROTOCOL.
o Yellow Connector: Height 4-5 feet King size3 o Red Connector: Height 5-6 feet King size 4 o Purple Connector: Height >6 feet King size 5
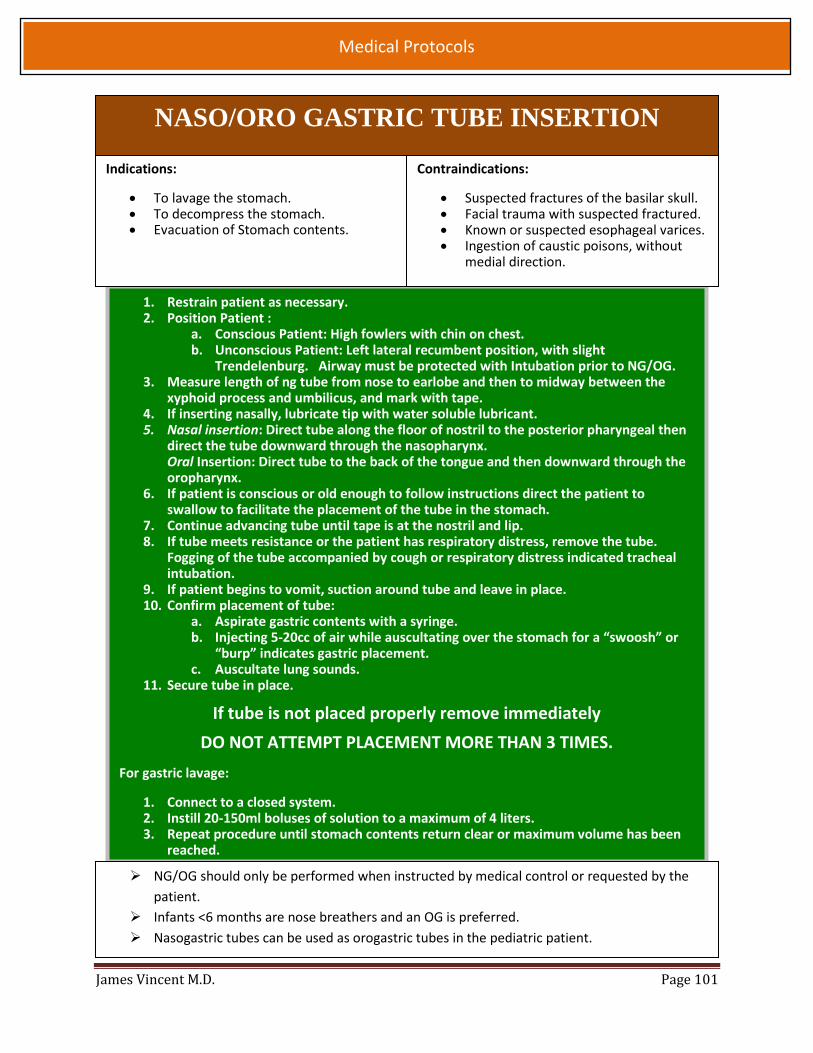
James Vincent M.D. Page 101
Medical Protocols
NASO/ORO GASTRIC TUBE INSERTION
1. Restrain patient as necessary. 2. Position Patient :
a. Conscious Patient: High fowlers with chin on chest. b. Unconscious Patient: Left lateral recumbent position, with slight
Trendelenburg. Airway must be protected with Intubation prior to NG/OG. 3. Measure length of ng tube from nose to earlobe and then to midway between the
xyphoid process and umbilicus, and mark with tape. 4. If inserting nasally, lubricate tip with water soluble lubricant. 5. Nasal insertion: Direct tube along the floor of nostril to the posterior pharyngeal then
direct the tube downward through the nasopharynx. Oral Insertion: Direct tube to the back of the tongue and then downward through the oropharynx.
6. If patient is conscious or old enough to follow instructions direct the patient to swallow to facilitate the placement of the tube in the stomach.
7. Continue advancing tube until tape is at the nostril and lip. 8. If tube meets resistance or the patient has respiratory distress, remove the tube.
Fogging of the tube accompanied by cough or respiratory distress indicated tracheal intubation.
9. If patient begins to vomit, suction around tube and leave in place. 10. Confirm placement of tube:
a. Aspirate gastric contents with a syringe. b. Injecting 5-20cc of air while auscultating over the stomach for a “swoosh” or
“burp” indicates gastric placement. c. Auscultate lung sounds.
11. Secure tube in place.
If tube is not placed properly remove immediately
DO NOT ATTEMPT PLACEMENT MORE THAN 3 TIMES.
For gastric lavage:
1. Connect to a closed system. 2. Instill 20-150ml boluses of solution to a maximum of 4 liters. 3. Repeat procedure until stomach contents return clear or maximum volume has been
reached.
NG/OG should only be performed when instructed by medical control or requested by the
patient.
Infants <6 months are nose breathers and an OG is preferred.
Nasogastric tubes can be used as orogastric tubes in the pediatric patient.
Contraindications:
Suspected fractures of the basilar skull. Facial trauma with suspected fractured. Known or suspected esophageal varices. Ingestion of caustic poisons, without
medial direction.
Indications:
To lavage the stomach. To decompress the stomach. Evacuation of Stomach contents.

James Vincent M.D. Page 102
Medical Protocols
OROTRACHEAL INTUBATION
Clinical indications:
Inability to adequately ventilate a patient with a Bag Valve Mask or longer EMS transport
distances requiring a more secure airway.
An unconscious patient without a gag reflex who is apneic or is demonstrating inadequate
respiratory effort.
1. Assemble appropriate equipment (to include): o BVM o Oxygen with regulator o Suction o Appropriate size ETT and stylet o ETT securing device o Gas exchange indicator o Magill forceps o 10cc syringe o Laryngoscope with appropriate size blade o Cardiac monitor, ETCO2 monitor
2. Properly position the patient in the supine position and ventilate adequately as indicated by the
patient treatment protocol you are following.
3. With suction standing by and proper manpower to provide Slicks maneuver if indicated, take
the laryngoscope in your LEFT hand and insert into the RIGHT side of the patients mouth. In a
forward abducting motion pull the lower jaw up and away from the patient while moving the
laryngoscope blade to the LEFT in an attempt to visualize the glottic opening. When you see the glottic opening and can identify the landmarks of the glottic opening, insert the ETT through the
glottic opening and into the trachea until you are at approximately at 23-26cm at the lip line. 4. Ventilate the patient while checking for the standard "Earmarks" of a successful intubation,
those being: o Good waveform on ETCO2 monitor (MOST RELIABLE INDICATOR) o Condensation in the ETT o Chest rise and fall o Good BVM compliance o Good positive and equal breath sounds o Good gas exchange as indicated by the color change on the gas indicator o Negative gastric sounds
5. Advise the receiving ER of an intubated patient and transport A.S.A.P. during protocol. 6. Secure ET Tube to the patients face, using “tube tamer”, tape, or string. Do not be put off task by vomitus, in the absence of suction sometimes if you lift a little
higher you can see over the top of the vomit into the back of the oropharynx. If at all possible the patient should be placed on cardiac monitor at all times, to monitor for
bradycardia and cardiac rhythm. Limit attempts to 10sec each.
James Vincent M.D. Page 103
Medical Protocols
NEEDLE DECOMPRESSION
Indications:
Tension Pneumothorax
1. Asses Chest and respiratory exertion.
2. Apply O2 per non-rebreather mask or BVM with 100%
supplemental O2.
3. Identify second intercostal space, midclavicular line on the
affected side.
4. Prep the area.
5. Snugly attach a 14 or 16 gauge angiocath to a 10ml syringe or
use arrow kit.
6. Insert the needle into the skin over the rib into the 2nd
intercostal space in mid-clavicular line directly above the 3rd
rib.
7. Puncture the parietal pleura.
8. Aspirate air as necessary to relieve patient’s symptoms.
9. Leave the plastic catheter remaining but remove the needle.
10. Secure the catheter.
11. Connect the catheter to a one way valve.
12. Reassess ventilator status, jugular veins, tracheal position,
pulse, and blood pressure.
13. Document procedure and responses.
Contraindications:
No apparent signs and symptoms of a tension pneumothorax.
Indications of Tension Pneumothorax
Hemodynamic Compromise, Systolic BP < 90 with any of the following: o JVD o Asymmetrical Chest Movement o Tracheal Deviation o Absent/Decreased Breath Sounds o Increase Resistance with Ventilation

James Vincent M.D. Page 104
Medical Protocols
NEEDLE DECOMPRESSION

James Vincent M.D. Page 105
Medical Protocols
SPINAL IMMOBILIZATION INDICATIONS:
Possible C-Spine FX
Motor Vehicle Collision
Fall from greater than patient’s height.
Fall from standing with pt age >65.
Unconscious patients with high possibility of traumatic spine injury.
Combative patients with high possibility of traumatic spine injury.
Auto-pedestrian accident
Bicycle accident
Traumatic Injury for patients with osteoporosis.
Contraindications:
Some patients due to size or age will not be able to be immobilized through in-line
stabilization with standard backboards and c-collars.
See the spinal motion restriction protocol for alternate methods of partial immobilization.
1. Place the patient in the appropriately sized c-collar
2. Once the collar is secure a second rescuer should still maintain their
position to ensure stabilization.
3. Log roll the patient to one side, maintain c-spine control.
4. Check the back, legs and back of head for injuries.
5. Place the long spine board under the patient.
6. Roll the patient onto long spine board while still maintaining s-spine
control.
7. Place head blocks next to the patients head.
8. Secure the torso and legs to the long spine board using straps, webbing
or tape.
9. Secure the patients head to the long spine board.
NOTE: for the patients in a vehicle or otherwise unable to be place in the prone
or supine position, place them on a backboard by the safest method available
that maximizes maintenance of in-line spinal stability.
Never force a patient into a non-neutral position to immobilize them. Padding
below the neck may be necessary. The patient may also require alternate
means of neck immobilization, in these cases a “horse collar” made of a towel
may be necessary.

James Vincent M.D. Page 106
Medical Protocols
TASER BARB REMOVAL
Disposition:
Transport PT if: 1. The barb lodged in a high risk area. 2. Patient falls under another protocol. 3. Pt meets signs and symptoms of
excited delirium and requires chemical restraint.
Assess and Treat:
Psychosis Hypoxia Hypoglycemia Overdose Central Nervous System Infection Trauma or Seizure
Remove only one barb at a time. DO NOT attempt to remove barbs in the face, genitalia, neck, women’s breast, or any site
that your clinical judgment deems high risk. Patients that have been fighting and/or who have taken stimulant medications are at a risk
for excited delirium and may require treatment and transport if symptoms present. Ensure that the wires are disconnected from the Taser device. Obtain vital signs when safe to do so.
1. Stabilize the skin around the barb and use one hard jerk
to pull the barb out of the patient’s skin.
2. Ensure that the barb tips are intact.
3. Return Barbs to LEO. IF LEO does not take custody of the
barbs, dispose of them in a sharps container.
4. Provide proper wound care, clean and cover with a
bandage.
5. Inform patient and LEO that the patient will need to seek
medical attention if signs of infection later develop.
6. The subject will need a tetanus shot if they have not had
one in the last 10 years.
James Vincent M.D. Page 107
Medical Protocols
INJECTION: SUBCUTANEOUS
INTRAMUSCLAR Clinical Indications:
When medication is necessary and the medication is necessary and the medication must be
given via SQ (not auto –injector) or IM route or as an alternative route in selected
medications
1. Receive and confirm medication order, or perform according to
standing order.
2. Prepare equipment and medication, expelling air from the syringe.
3. Explain the procedure to the patient and reconfirm patient
allergies.
4. Expose the selected area and cleanse the injection site with
alcohol.
5. Insert the needle into the skin with a smooth, steady motion.
SQ:45-degree angle skin pinched
IM:90- degree angle skin flat
6. Aspirate for blood.
7. Inject the medication.
8. Withdraw the needle quickly, dispose of needle properly.
9. Apply pressure to the site.
10. Monitor the patient therapeutic effects as well as any possible
side effects.
11. Document the medication, dose, route, and time on/with the
Patient care report.
The thigh should be used for injections in pediatric patients and injection volume should not
exceed 1cc.
The most common site for subcutaneous injection is the arm
o Injection volume should not exceed 1cc.
The possible injection sites for subcutaneous injection include the arm, buttock, and thigh.
o Injection volume should not exceed 1cc for the arm.
o Injection volume should not exceed 2 cc for the thigh or buttock
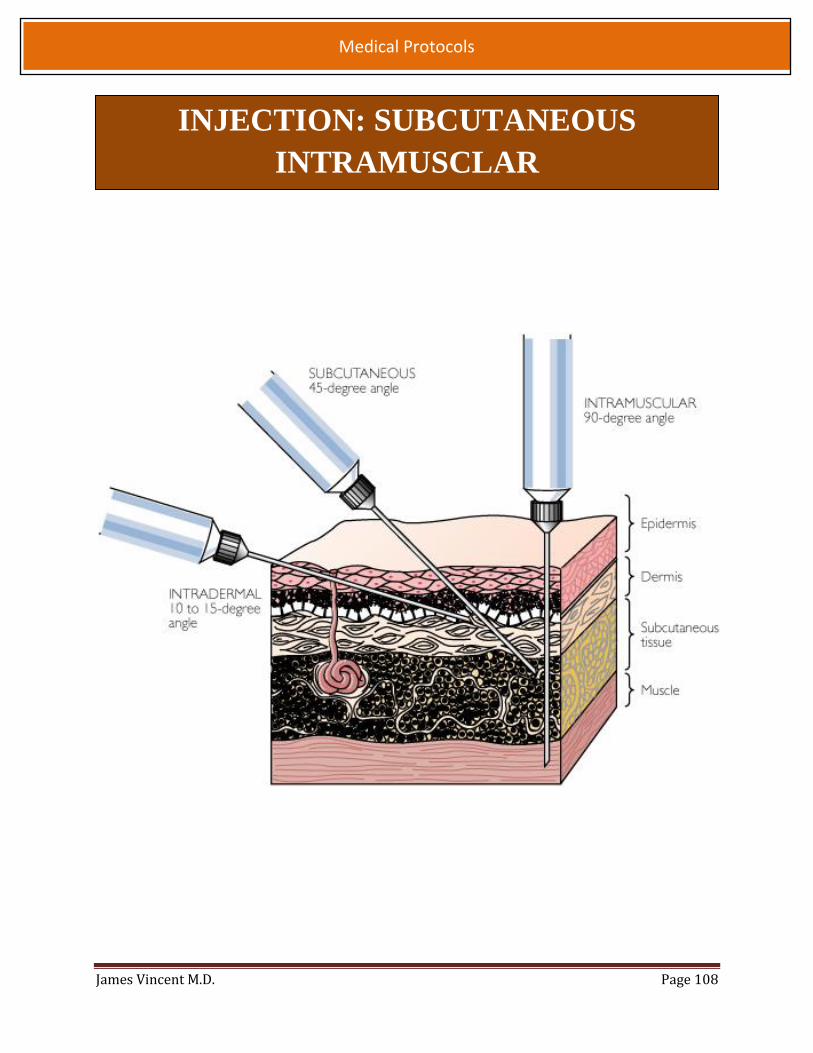
James Vincent M.D. Page 108
Medical Protocols
INJECTION: SUBCUTANEOUS
INTRAMUSCLAR

James Vincent M.D. Page 109
Medical Protocols
SURGICAL AIRWAY: CRICOTHYROTOMY
Indications:
Unable to ventilate. Unable to intubate. Unable to ventilate with rescue airway. Severe Facial or nasal injuries that
prevent successful ventilation or airway placement.
Severe mid-tracheal injuries or anatomy that prevents intubation / ventilation.
Sever uncontrolled angioedema, anaphylaxis and certain types of inhalation injures.
Contraindications:
Inability to identify landmarks. Not trained in this procedure. Able to ventilate with less invasive
techniques Able to intubate
Notify the receiving Emergency Department of procedure as soon as possible during
protocol.
If bleeding occurs, use suction and proceed. Insertion and inflation of endotracheal tube
through the cricothyotomy site will protect the patient from blood entering the airway.
If using an endotracheal tube only advance 2 - 2.5cm to avoid right main stem intubation.
1. Assemble equipment a. Betadine prep swabs b. Scalpel c. Large curved hemostat, Bougie Tube, or Extra scalpel handle d. Tracheostomy or endotracheal tube e. Tape
2. Expose the neck. 3. Identify the thyroid cartilage. The space between the cricothyroid notch and the
thyroid cartilage is the location of the cricothyroid membrane. 4. Prep the area. 5. Stabilize the trachea by holding the thyroid cartilage between the thumb and
fingers. 6. Make a horizontal incision approximately ½ inch through the skin and cricothyroid
membrane. 7. Insert hemostat to dilate the incision. (Never remove scalpel or hemostat without
something in the incision space; the small incision will close.) 8. Turn the hemostat or scalpel handle until the opening is sufficient to allow the
passing of a small endotracheal tube. (6.0-7.0 mm 9. Pass the endotracheal tube about 1 – 1.5 inches into the trachea. 10. Inflate the cuff if using a cuffed tube and ventilate the pt with high flow oxygen. 11. Check breath sounds bilaterally and secure with tape. 12. Monitor patient condition and reassess frequently. 13. Control any bleeding and dress the wound.

James Vincent M.D. Page 110
Medical Protocols
SURGICAL AIRWAY: QUICK TRACH
Clinical Indications:
Surgical Airway as indicated by the failed airway protocol.
1. Pre-oxygenate patient when possible. 2. Assemble all available equipment. 3. Locate cricothyroid membrane at the inferior portion of the thyroid cartilage
(with the head in the neutral position, membrane is approx. 3 finger widths above the sterna notch).
4. Have assistant hold skin taunt over membrane and locate midline. 5. Prepare the area with betadine if possible. 6. Hold the needle bevel up at a 90 degree angle, aimed inferiorly as you
approach the skin. 7. Puncture the skin with the needle and continue with firm steady pressure
while aspirating for air with a syringe. 8. As soon as air is aspirated freely stop advancing the needle airway assembly. 9. Modify the angle to 60 degrees from the head and advance to level of the
stopper. 10. Remove the stopper while holding the needle /airway assembly firmly in
place. Do not advance the needle further. (NOTE: if the patient is obese and no air can be aspirated with the stopper in place you may remove the stopper and continue advancing until air is aspirated. Be aware that without the stopper, risk of perforating the posterior aspect of the trachea is greatly increased).
11. Hold the needle and syringe firmly and slide only the plastic cannula along the needle into the trachea until the flange rests on the neck. Carefully remove the needle and syringe.
12. Secure the cannula with the neck strap. 13. Apply the EtCO2 detector and to the tube and the bvm. 14. Confirm placement with the use of breath sounds, pulse ox, and Color-metric
change. 15. Ensure 100% supplemental Oxygen via BVM.
Notify the receiving Emergency Department of procedure as soon as possible during
protocol.
James Vincent M.D. Page 111
Medical Protocols
Contraindications:
Non-extremity hemorrhage
Proximal extremity location where tourniquet application is not practical.
1. Place tourniquet proximal to wound.
2. Tighten per manufacturer instructions until hemorrhage stops
and/or distal pulses in affected extremity disappear.
3. Secure tourniquet per manufacturer instructions.
4. Note Time of tourniquet application and communicate this to
receiving care providers.
5. Dress wounds appropriately.
6. If Delayed or prolonged transport and tourniquet application
time is more than 5 hours contact medical control.
Clinical Indications:
Life threatening extremity hemorrhage that cannot be controlled by other means.
Tourniquets should be used extremely infrequently
TOURNIQUET
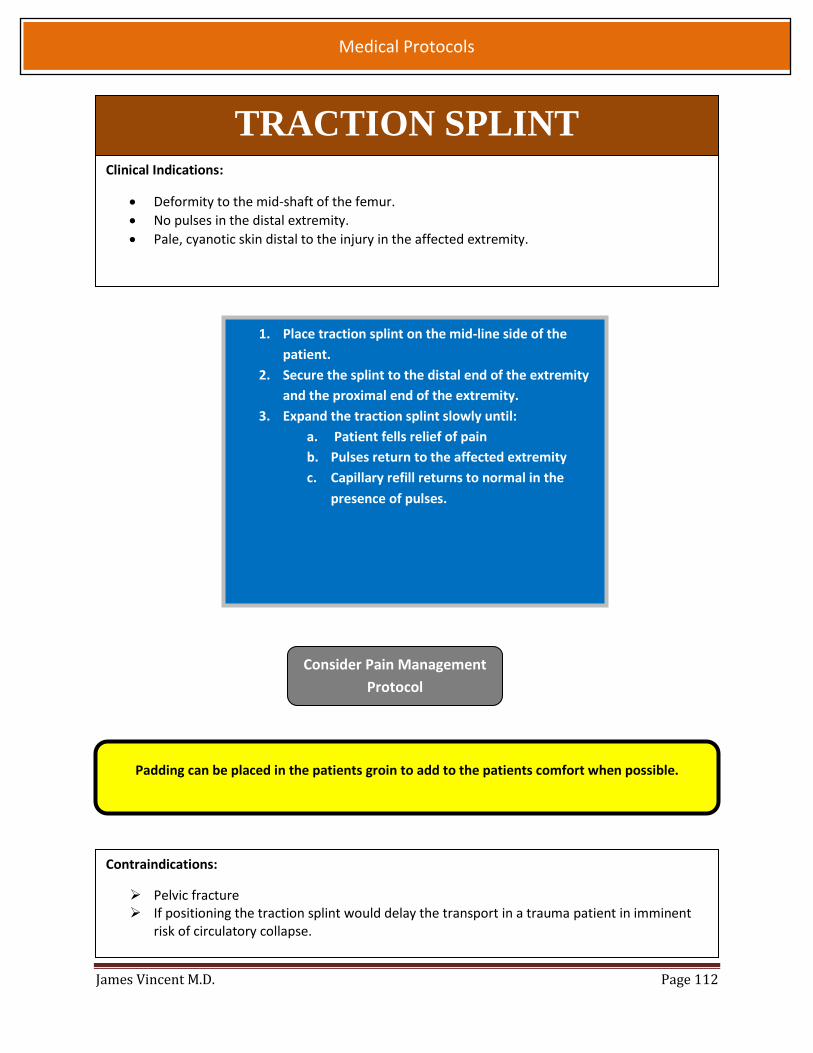
James Vincent M.D. Page 112
Medical Protocols
TRACTION SPLINT Clinical Indications:
Deformity to the mid-shaft of the femur.
No pulses in the distal extremity.
Pale, cyanotic skin distal to the injury in the affected extremity.
Contraindications:
Pelvic fracture If positioning the traction splint would delay the transport in a trauma patient in imminent
risk of circulatory collapse.
Padding can be placed in the patients groin to add to the patients comfort when possible.
1. Place traction splint on the mid-line side of the
patient.
2. Secure the splint to the distal end of the extremity
and the proximal end of the extremity.
3. Expand the traction splint slowly until:
a. Patient fells relief of pain
b. Pulses return to the affected extremity
c. Capillary refill returns to normal in the
presence of pulses.
Consider Pain Management
Protocol
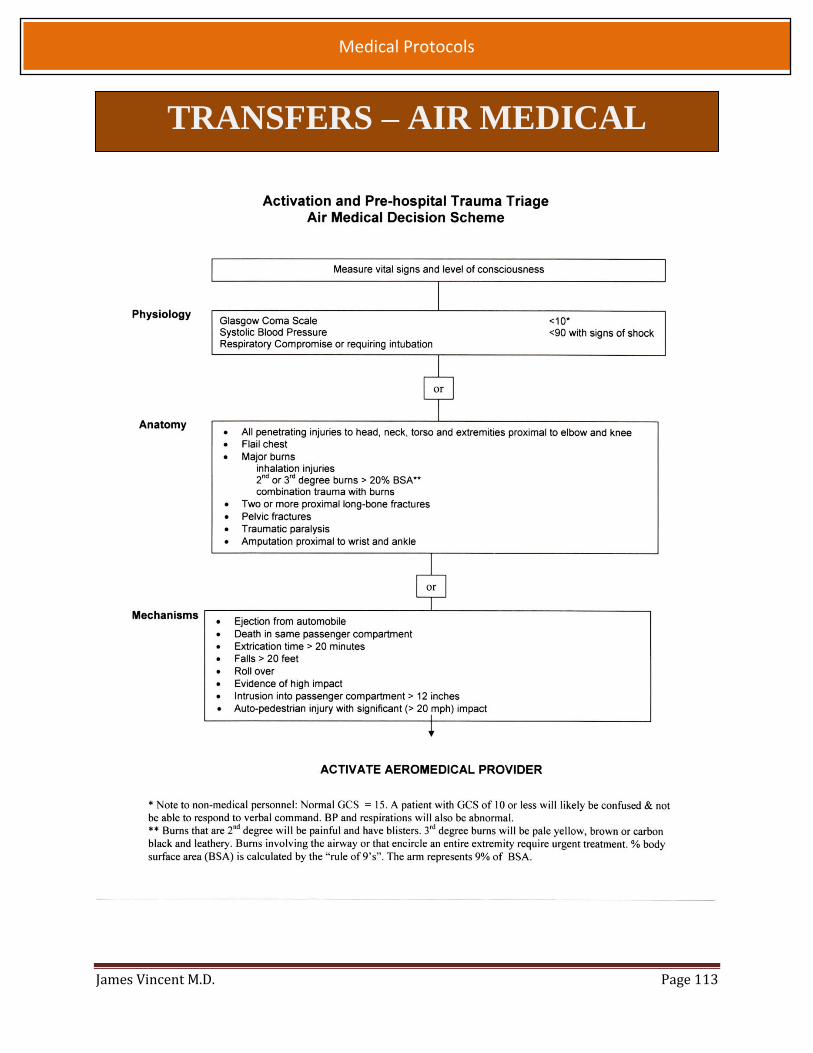
James Vincent M.D. Page 113
Medical Protocols
TRANSFERS – AIR MEDICAL
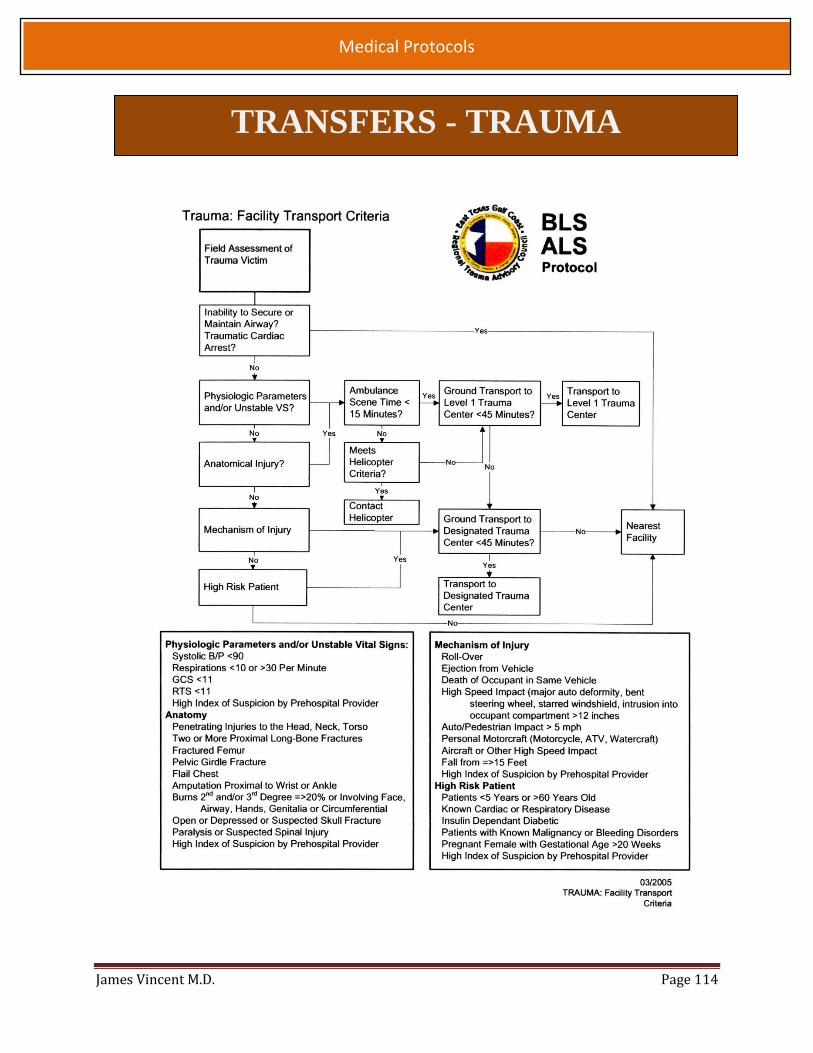
James Vincent M.D. Page 114
Medical Protocols
TRANSFERS - TRAUMA

James Vincent M.D. Page 115
Medical Protocols
TRANSFERS - TRAUMA

James Vincent M.D. Page 116
Medical Protocols
TRANSFERS - TRAUMA

James Vincent M.D. Page 117
Medical Protocols
VentiPAC PORTABLE VENTILATOR
1. Connect the ventilator to the oxygen supply
2. Switch the ventilator on/off switch to on (you should hear the ventilator
begin to cycle)
3. Set the breathing parameters to suite the pt (obtain from the facilities
respiratory therapist when available)
4. Set air mix switch to 100% for
A CPR
B Respiratory arrest
C. Contaminated environments
5. Connect tubing to the patient
6. Ensure the settings are adequate for the patient by,
A. Monitoring the patient’s vital signs and physical condition (remember to
treat the patient not the monitor)
B. Confirm airway placement prior to and after each movement, suctioning,
when connecting or discounting the tubing from the patients airway device,
and when checking vital signs
7. If the ventilator fails to work properly at any point during the transport of a
patient, IMMEDIATELY DISCONNECT THE VENTILATOR FORM THE PATIENT
AND SWITCH TO A BVM
Typical Ventilator Settings for an Adult Patient
On/off (On), X100Pa (40)
Inspiratory Time (1.5)
Expiratory Time (3.0)
Air Mix (=50% O2)
Inspiratory Flow L/sec (0.50)

James Vincent M.D. Page 118
Medical Protocols
APPENDIX A: MEDICATION FORMULARY
Medication Quick Reference Dosage Page
Acetylsalicylic Acid 324 mg PO 121
Activated Charcoal 50 grams PO 122
Adenosine (Adenocard) 6/12/12 mg 123
Pedi 0.1/0.2/0.2 mg/kg
Albuterol 2.5 mg per neb 125
Amiodarone 300 then 150 mg for arrest 126
150 mg over 10 min for dysrhythmias
Pedi 5 mg/kg
Anectine (Succinylcholine) 100 mg IV/IO 127
3-4 mg/kg IM, (Max 150 mg)
Pedi 1 mg/kg IV/IO, (Max 100 mg)
Atropine 0.5 to 1 mg 128
Calcium gluconate 1 gram IV = 10ml 129
Cefazolin (Ancef) 1-2 gram(s) IV infusion in 50-250 mL 130
Diltiazem (Cardizem) 10-20 mg, then 25mg 131
Diphenhydramine (Benadryl) 25-50 mg IV/IM 132
Pedi 1 mg/kg IV, (Max 25mg)
Dextrose 50% 25 grams = “1 amp” 133
Pedi D10 5mL/kg, D25 2 mL/kg
Diazepam (Valium) 5-10 mg IV 134
Pedi 0.2 mg/kg
Enalaprilat (Vasotec) 1.25 mg IV 135
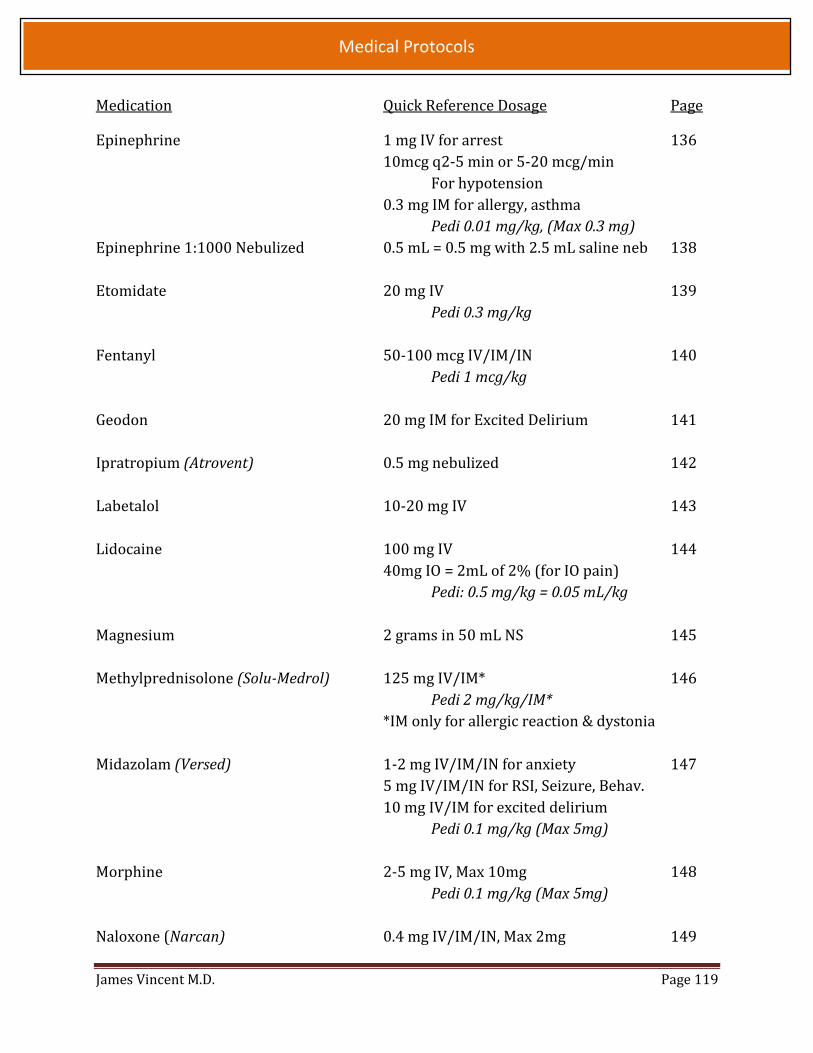
James Vincent M.D. Page 119
Medical Protocols
Medication Quick Reference Dosage Page
Epinephrine 1 mg IV for arrest 136
10mcg q2-5 min or 5-20 mcg/min
For hypotension
0.3 mg IM for allergy, asthma
Pedi 0.01 mg/kg, (Max 0.3 mg)
Epinephrine 1:1000 Nebulized 0.5 mL = 0.5 mg with 2.5 mL saline neb 138
Etomidate 20 mg IV 139
Pedi 0.3 mg/kg
Fentanyl 50-100 mcg IV/IM/IN 140
Pedi 1 mcg/kg
Geodon 20 mg IM for Excited Delirium 141
Ipratropium (Atrovent) 0.5 mg nebulized 142
Labetalol 10-20 mg IV 143
Lidocaine 100 mg IV 144
40mg IO = 2mL of 2% (for IO pain)
Pedi: 0.5 mg/kg = 0.05 mL/kg
Magnesium 2 grams in 50 mL NS 145
Methylprednisolone (Solu-Medrol) 125 mg IV/IM* 146
Pedi 2 mg/kg/IM*
*IM only for allergic reaction & dystonia
Midazolam (Versed) 1-2 mg IV/IM/IN for anxiety 147
5 mg IV/IM/IN for RSI, Seizure, Behav.
10 mg IV/IM for excited delirium
Pedi 0.1 mg/kg (Max 5mg)
Morphine 2-5 mg IV, Max 10mg 148
Pedi 0.1 mg/kg (Max 5mg)
Naloxone (Narcan) 0.4 mg IV/IM/IN, Max 2mg 149

James Vincent M.D. Page 120
Medical Protocols
Medication Quick Reference Dosage Page
Nitroglycerin 0.4 mg SL q5 min for ACS or HTN 150
0.4 mg SL q3 min for CHF
Norepinephrine (Levophed) 2-12 mcg/minute IV for hypotension 151
Pedi: not indicated
Ondansetron (Zofran) 4 mg IV/IM 152
Pedi 6mo to 4yr 2mg, >4 yr 4 mg
Oral Glucose 15 grams PO 153
Oxygen NC: 1-4 L, Neb: 8 L, Mask 10-15L/min 154
Rocuronium 50 mg IV 155
Pedi 1 mg/kg
Sodium Bicarbonate 50-100 mEq IV 156
Thiamine 100 mg IV/IM 157
Vecuronium 10 mg IV 158
Pedi 0.1 mg/kg

James Vincent M.D. Page 121
Medical Protocols
ACETYLSALICYLIC ACID (ASPRIN, ASA)
Class Platelet inhibitor, anti-inflammatory agent
Mechanism of Action Prostaglandin inhibition, prevents platelet aggregation
Indications Chest pain suggestive of acute myocardial infarction
Protocol: Acute Coronary Syndrome
Contraindications Hypersensitivity to ASA or nonsteroidal anti-inflammatory drugs (NSAIDS)
Gastrointestinal bleeding
Adverse Reactions Heartburn
Gastrointestinal bleeding
Nausea, vomiting
Wheezing in allergic patients
Prolonged bleeding
Dosage and Administrations Adult :
324mg PO
Pediatric: not recommended in pediatric population
Duration of Action Onset: 30-45 minutes
Duration: life of platelet (7-10 day)
Special Considerations/Drug Interactions Pregnancy safety: category D

James Vincent M.D. Page 122
Medical Protocols
ACTIVATED CHARCOAL (ACTIDOSE-AQUA) Class
Poison antidote
Mechanism of Action Binds and absorbs ingested toxins and inhibits the absorption of poisons
Indications Many oral poisonings, medication overdoses
Protocol: Overdose
Contraindications Ingestion of: turpentine, corrosives (lye and strong acids), caustics, or
petroleum distillates (kerosene, gasoline, paint thinner, cleaning fluid, furniture polish)
Adverse Reactions May indirectly induce nausea and vomiting May cause constipation
Dosage and Administrations Adult:
50 grams PO or NGT
Duration of Action Onset: Immediate
Duration: Continual while in GI tract
Special Considerations/Drug Interactions Is relatively insoluble in water May blacken feces Does not adsorb all drugs and toxic substances (for example, cyanide, lithium,
iron, lead and arsenic) Overdoses such as Phenobarbital, Carbamazepine, Theophylline, Phonation
and Digitalis, multiple doses of charcoal may be required to be effective Syrup of Ipecac is adsorbed by activated charcoal

James Vincent M.D. Page 123
Medical Protocols
ADENOSINE (ADENOCARD) Class
Antiarrhythmic
Mechanism of Action An endogenous purine nucleotide that slows conduction through the AV node,
interrupts the reentry pathways to the AV node and can restore normal sinus
rhythm in PSVT via modulation of K+ currents and blunting of catecholamine
response
Indications Conversion to sinus rhythm of Paroxysmal Supraventricular Tachycardia
(PSVT), including that associated (Wolff-Parkinson-White syndrome) To aid in the diagnosis of broad or narrow complex supraventricular
tachycardia Protocol: Supraventricular Tachycardia
Contraindications
Hypersensitivity to the medication 2nd or 3rd degree AV block (except in patients with a functioning artificial
pacemaker) Sick Sinus Syndrome where you see the accessory pathway conduct the atrial
impulses at rates > 220) Adverse Reactions
Non-cardiac: facial flushing, chest pain, dyspnea, headache, lightheadedness Cardiac: 1st, 2nd or 3rd degree heart block; transient asystole; varied atrial
and ventricular arrhythmias 1/2 life is 10 seconds. A brief period of asystole (up to 15 seconds) following
conversion, followed by resumption of NSR is common after rapid administration
Adverse reactions are generally transient, resolve within 1 minute of drug administration, and do not require intervention, nor are they an indication to not attempt a subsequent administration of a higher dose of the same medication.
Adult:
6mg FIVP with 10cc NS flush, wait 1-2 min if no conversion 12mg FIVP with
10cc NS flush , wait 1-2 minutes if no conversion 12mg FIVP with 10cc NS
flush (Max of 30mg)
Pediatric:
0.1 mg/kg (to a max of 6 mg) IV/IO with 10cc NS flush, wait 1-2 minutes.
If no conversion, 0.2 mg/kg (to a maximum of 12 mg) with a NS 10 ml flush.
Wait 1-2 minutes; if no conversion, 0.2 mg/kg (to a max of 12 mg) with a 10cc NS flush
(Total Max of 30mg)

James Vincent M.D. Page 124
Medical Protocols
Duration of Action Onset: < 60seconds
Peak : 60 seconds
Duration: 1-2 minutes
Special Considerations/Drug Interactions The effects of Adenosine are antagonized by methylxanthines, caffeine,
Theophylline (larger doses may be required to be effective) Direct IV rapid bolus (1 - 2 seconds), preferably via large bore EJ or AC site due
to short half-life and followed by NS 10 - 20 ml flush Must be administered quickly, preferably via large bore IV in the AC or EJ, may be
administered via IO.
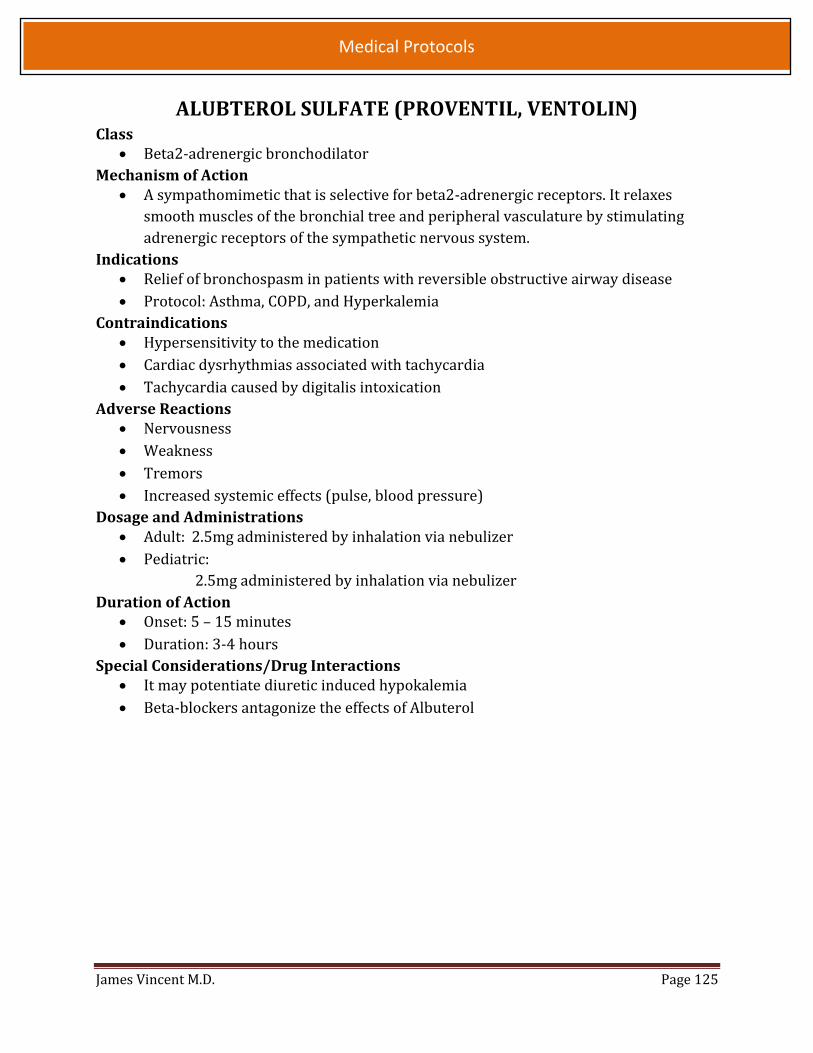
James Vincent M.D. Page 125
Medical Protocols
ALUBTEROL SULFATE (PROVENTIL, VENTOLIN) Class
Beta2-adrenergic bronchodilator
Mechanism of Action A sympathomimetic that is selective for beta2-adrenergic receptors. It relaxes
smooth muscles of the bronchial tree and peripheral vasculature by stimulating
adrenergic receptors of the sympathetic nervous system.
Indications Relief of bronchospasm in patients with reversible obstructive airway disease
Protocol: Asthma, COPD, and Hyperkalemia
Contraindications Hypersensitivity to the medication
Cardiac dysrhythmias associated with tachycardia
Tachycardia caused by digitalis intoxication
Adverse Reactions Nervousness
Weakness
Tremors
Increased systemic effects (pulse, blood pressure)
Dosage and Administrations Adult: 2.5mg administered by inhalation via nebulizer
Pediatric:
2.5mg administered by inhalation via nebulizer
Duration of Action Onset: 5 – 15 minutes
Duration: 3-4 hours
Special Considerations/Drug Interactions It may potentiate diuretic induced hypokalemia
Beta-blockers antagonize the effects of Albuterol

James Vincent M.D. Page 126
Medical Protocols
AMIODARONE (CORDARONE) Class
Antidysrhtythmic
Mechanism of Action Prolongation of action potential
Non-competitive alpha and beta sympathetic blocking effects
Calcium channel block effects
Indications Ventricular fibrillation, ventricular tachycardia with or without a pulse
Protocol: Ventricular fibrillation, ventricular tachycardia with or without a pulse,
and A-fib/SVT refractory to Adenocard and Diltiazem
Contraindications Hypersensitivity to the medication
Bradycardia
Cardiogenic shock
Adverse Reactions Hypotension
Bradycardia
CHF
Dosage and Administrations Adult:
V-fib and pulseless V-tach- 300mg in 50cc’s of NS- initial dose wait ten
minutes, then administer 150mg in 50cc’s of NS x 3;
V-tach with a pulse or refractory A-fib/SVT – 150mg in 50ccs over 10
minutes.
Pediatric:
V-fib and pulseless V-tach- 5mg/kg (Max dose of 300mg);
SVT- 5mg/kg over 10 minutes
Duration of Action Onset: 5-15 minutes
Peak effect: variable
Duration: long and variable
Special Considerations/Drug Interactions Incompatible with Sodium Bicarbonate- can precipitate
Caution with Beta Blockers- may increase hypotension and Bradycardia
Caution with Calcium Channel Blockers- hypotension and increase
inotropic/dromotropic effects
Hypotension associated with slow infusion rate

James Vincent M.D. Page 127
Medical Protocols
ANECTINE (SUCCINYLCHOLINE) Class
Depolarizing neuromuscular blocker; skeletal muscle relaxant Mechanism of Action
Ultra-short acting depolarizing agent that mimics acetylcholine as it binds with the
cholinergic receptors on the motor end plate, producing a phase I block as
manifested by fasciculations.
Indications Rapid Sequence Intubation
Contraindications Penetrating eye injuries Acute narrow angle glaucoma Malignant hyperthermia – personal of familial history After the acute phase of major burn or extensive trauma Muscular Myopathies (i.e.: Muscular dystrophy)
Adverse Reactions Anaphylaxis Hyperkalemia Malignant Hyperthermia Cardiac Dysrhythmias Bradycardia which may progress to asystole Rhabdomyolysis Increased intraocular pressure
Dosage and Administrations Adult:
100mg IV/IO
3-4mg/kg IM to max dose to 150mg
Pediatric:
1mg/kg to a max dose of 100mg IV/IO
Duration of Action Onset: 1 minute Duration: 5-10 minutes
Special Considerations/Drug Interactions Pregnancy Category C
Diazepam may reduce duration of action
Beta blockers and organophosphates may potentiate effects
Use with caution in hyperkalemic or possible hyperkalemic patients
Consider premedication with atropine, particularly in pediatric patients
Use with caution in pediatric patients
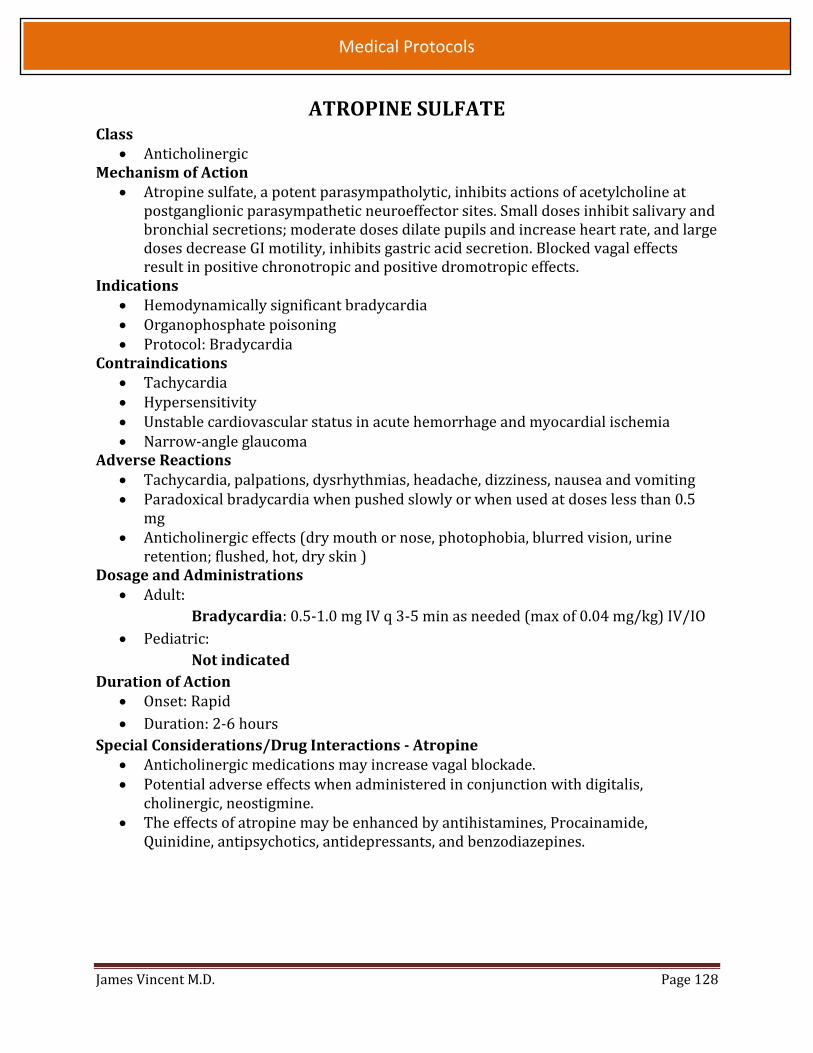
James Vincent M.D. Page 128
Medical Protocols
ATROPINE SULFATE Class
Anticholinergic Mechanism of Action
Atropine sulfate, a potent parasympatholytic, inhibits actions of acetylcholine at postganglionic parasympathetic neuroeffector sites. Small doses inhibit salivary and bronchial secretions; moderate doses dilate pupils and increase heart rate, and large doses decrease GI motility, inhibits gastric acid secretion. Blocked vagal effects result in positive chronotropic and positive dromotropic effects.
Indications Hemodynamically significant bradycardia Organophosphate poisoning Protocol: Bradycardia
Contraindications Tachycardia Hypersensitivity Unstable cardiovascular status in acute hemorrhage and myocardial ischemia Narrow-angle glaucoma
Adverse Reactions Tachycardia, palpations, dysrhythmias, headache, dizziness, nausea and vomiting Paradoxical bradycardia when pushed slowly or when used at doses less than 0.5
mg Anticholinergic effects (dry mouth or nose, photophobia, blurred vision, urine
retention; flushed, hot, dry skin ) Dosage and Administrations
Adult:
Bradycardia: 0.5-1.0 mg IV q 3-5 min as needed (max of 0.04 mg/kg) IV/IO
Pediatric:
Not indicated
Duration of Action Onset: Rapid
Duration: 2-6 hours
Special Considerations/Drug Interactions - Atropine Anticholinergic medications may increase vagal blockade. Potential adverse effects when administered in conjunction with digitalis,
cholinergic, neostigmine. The effects of atropine may be enhanced by antihistamines, Procainamide,
Quinidine, antipsychotics, antidepressants, and benzodiazepines.

James Vincent M.D. Page 129
Medical Protocols
CALCIUM GLUCONATE 10% Class
Minerals and electrolytes Mechanism of Action
Calcium is a positive inotrope Variable effect on systemic vascular resistance When used to prevent or treat negative calcium balance (e.g., osteoporosis), the
calcium in calcium salts moderates nerve and muscle performance and allows normal cardiac function
Indications Suspected Hyperkalemia in adult PEA/Asystole associated with renal patients
Antidote for calcium channel blocker overdose and magnesium sulfate toxicity
Hyperkalemia associated with adult crush injury
Protocol: Overdose, crush injury
Contraindications Patients with digitalis toxicity
Caution should be used with dehydrated patients
Adverse Reactions When given too rapidly or to someone on digitalis, can cause sudden death from
ventricular fibrillation
Dosage and Administrations Adult:
1 gram (= 10mL) over 10 minutes. May repeat X1
Duration of Action Onset: Immediate
Duration: 30 minute to 2 hours
Special Considerations/Drug Interactions Incompatible with Sodium Bicarbonate- IV line must be flushed with copious
amounts of saline Calcium may decrease the bioavailability of tetracycline’s, fluoroquinolones, iron
salts and salicylates, Atenolol, and sodium polystyrene sulfonate I.V. calcium may antagonize the effects of Verapamil; large intakes of dietary fiber
may decrease calcium absorption due to a decreased GI transit time and the formation of fiber-calcium complexes
Increased effect: I.V. calcium may increase the effects of Quinidine and digitalis

James Vincent M.D. Page 130
Medical Protocols
Cefazolin (Ancef) Class
Antibiotic - cephalosporin Mechanism of Action
Bactericidal agent that acts by inhibition of bacterial cell wall synthesis Indications
Open Skeletal fracture A break in the skin over a fracture site
Contraindications History of anaphylaxis (not a simple rash) to penicillin Known allergy to the cephalosporin group of antibiotics <1 year of age
Adverse Reactions Diarrhea Anaphylaxis Itching Skin rash
Dosage and Administration Adult:
1-2 gram IV infusion over 10-30 minutes Can administer 1 gram for patient <70kg Can administer 2grams for patients >70kg
After reconstituting medication, mix into a 50ml, 100ml or 250ml bag of Normal Saline
Preferred mixing dose is 50ml Normal saline for each 1mg of antibiotic
Duration of Action Duration unknown
Special Considerations/Drug Interactions Be alert for hypersensitivity reaction Pregnancy Category B Renal Impairment may require reduced dosage IV incompatible with Amiodarone Parenteral drug products should be shaken well when reconstituted and inspected
for particulate matter prior to administration Note that reconstituted solutions may range in color from pale yellow to yellow
without a change in potency.

James Vincent M.D. Page 131
Medical Protocols
DILTIAZEM (CARDIZEM) Class
Benzothiazepine, Calcium Channel Blocker, Cardiovascular agent
Mechanism of Action A slow calcium channel blocker that blocks calcium ion influx during depolarization
of cardiac and vascular smooth muscle. It decreases peripheral vascular resistance
and caused relaxation of the vascular smooth muscle resulting in a decrease of both
systolic and diastolic blood pressure
Indications Atrial arrhythmia
Protocol: Atrial Fibrillation
Contraindications Administration of intravenous beta-blockers within a few hours of intravenous
Diltiazem
Atrial fibrillation or flutter associated with an accessory bypass tract (Wolff-
Parkinson- White or short PR syndromes)
Hypotension
Sick sinus syndrome without a pacemaker
Adverse Reactions Bradyarrhythmia
Peripheral edema
CHF
Heart block
Myocardial infarction
Dosage and Administrations Adult:
10-20mg SIVP over 2 min
May repeat with a dose of 25mg SIVP over 2 min
Duration of Action Onset: 2-5 minutes
Special Considerations/Drug Interactions Renal impairment can cause an increased risk of toxicity
Ventricular function, impaired
Hepatic or renal impairment, heart failure

James Vincent M.D. Page 132
Medical Protocols
DIPHENHYDRAMINE (BENADRYL) Class
Antihistamine
Mechanism of Action Antihistamines prevent histamines from reaching H1- and H2-receptor sites.
Antihistamine is specific for conditions in which histamine excess is present (for example, acute urticaria) but is adjunctive therapy in the treatment of anaphylactic shock because epinephrine is more effective.
Indications Allergic reactions
Anaphylaxis
Acute dystonic reactions
Protocol: Overdose, anaphylaxis, excited delirium
Contraindications Lower respiratory diseases such as asthma attacks Patients taking MAOIs Hypersensitivity Narrow-angle glaucoma
Adverse Reactions Dose-related drowsiness
Disrupted coordination
Hypotension
Palpitations
Tachycardia, bradycardia
Thickening of bronchial secretions
Dosage and Administrations Adult:
25-50 mg SIVP/ IM Pediatric:
1mg/kg SIVP/IM Max 25mg
Duration of Action - Diphenhydramine Peak: 1-3 hours Duration:6-12 hours
Special Considerations/Drug Interactions CNS depressants may increase depressant effects.
MAOIs may prolong and intensify Anticholinergic effects of antihistamines.
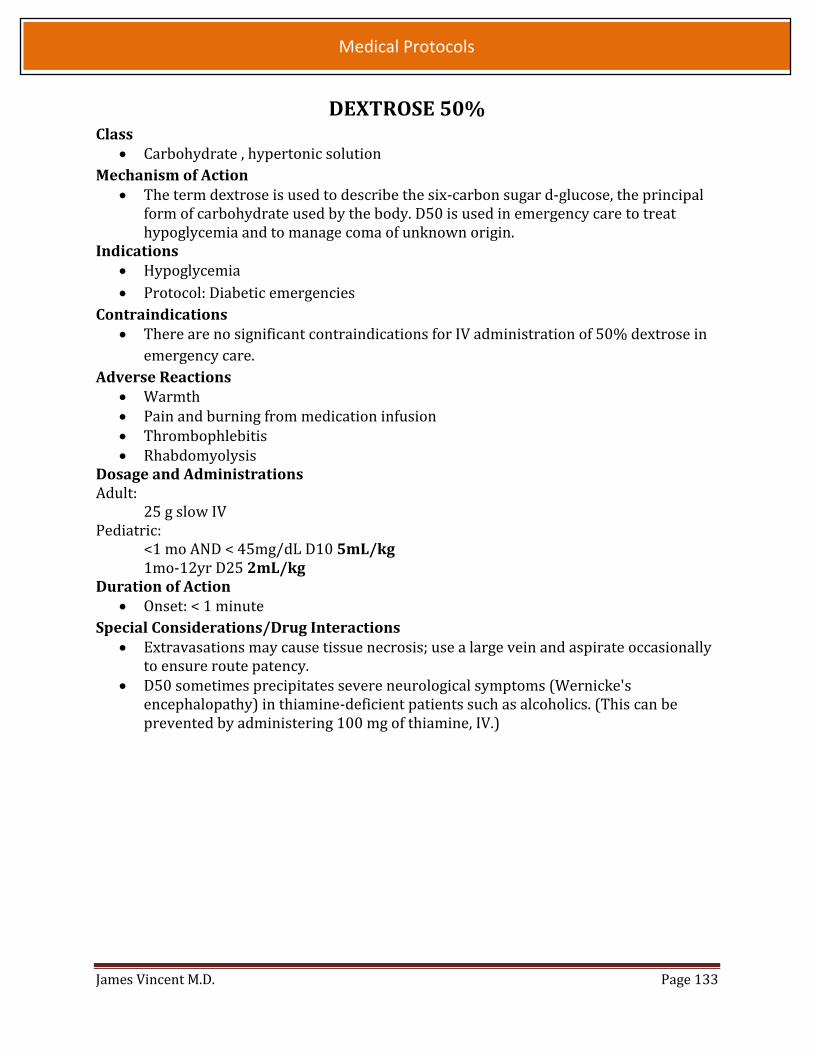
James Vincent M.D. Page 133
Medical Protocols
DEXTROSE 50% Class
Carbohydrate , hypertonic solution
Mechanism of Action The term dextrose is used to describe the six-carbon sugar d-glucose, the principal
form of carbohydrate used by the body. D50 is used in emergency care to treat hypoglycemia and to manage coma of unknown origin.
Indications Hypoglycemia
Protocol: Diabetic emergencies
Contraindications There are no significant contraindications for IV administration of 50% dextrose in
emergency care.
Adverse Reactions Warmth Pain and burning from medication infusion Thrombophlebitis Rhabdomyolysis
Dosage and Administrations Adult:
25 g slow IV Pediatric:
<1 mo AND < 45mg/dL D10 5mL/kg 1mo-12yr D25 2mL/kg
Duration of Action Onset: < 1 minute
Special Considerations/Drug Interactions Extravasations may cause tissue necrosis; use a large vein and aspirate occasionally
to ensure route patency. D50 sometimes precipitates severe neurological symptoms (Wernicke's
encephalopathy) in thiamine-deficient patients such as alcoholics. (This can be prevented by administering 100 mg of thiamine, IV.)

James Vincent M.D. Page 134
Medical Protocols
DIAZEPAM (VALIUM) Class
Benzodiazepine sedative-hypnotic, anticonvulsant Mechanism of Action
Diazepam acts on the limbic, thalamic, and hypothalamic regions of the CNS to potentiate the effects of inhibitory neurotransmitters, raising the seizure threshold in the motor cortex.
Indications Acute anxiety states Acute alcohol withdrawal Muscle relaxant Seizure activity Preoperative sedation Protocol: Behavioral emergencies, Seizures, Eclampsia
Contraindications Hypersensitivity to the drug Shock
Adverse Reactions Hypotension Reflex tachycardia Respiratory depression Ataxia Psychomotor impairment Confusion Nausea
Dosage and Administrations Adult:
Eclampsia: 5mg SIVP
Seizures/Behavioral: 10mg SIVP
Pediatric:
Seizures: 0.2 mg/kg IV; Max dosage of 10mg
Duration of Action Onset: (IV) 1-5 min (IM) 15-30 min
Duration: (IV) 15 min-1 hr (IM) 15 min-1 hr Special Considerations/Drug Interactions
May cause local venous irritation. Resuscitation equipment should be readily available
Rapid IV administration may be followed by respiratory depression and excessive sedation.
Though the drug is still widely used as an anticonvulsant, it is relatively weak and of short duration.
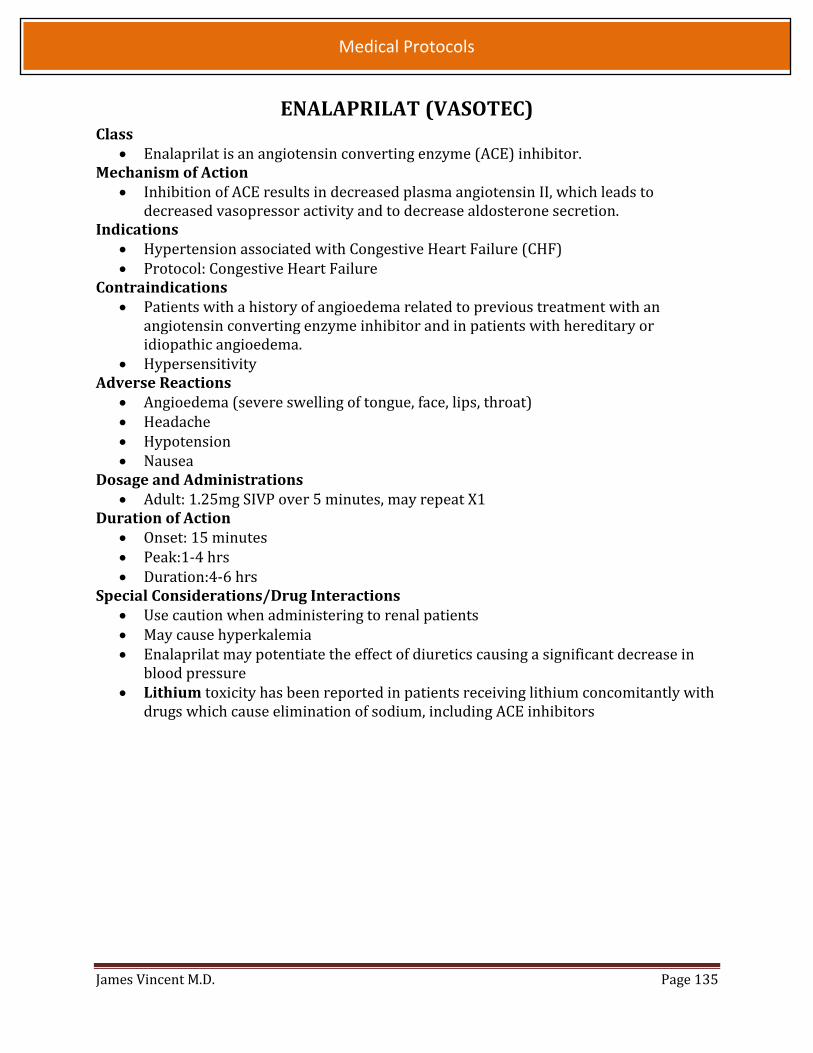
James Vincent M.D. Page 135
Medical Protocols
ENALAPRILAT (VASOTEC) Class
Enalaprilat is an angiotensin converting enzyme (ACE) inhibitor. Mechanism of Action
Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decrease aldosterone secretion.
Indications Hypertension associated with Congestive Heart Failure (CHF) Protocol: Congestive Heart Failure
Contraindications Patients with a history of angioedema related to previous treatment with an
angiotensin converting enzyme inhibitor and in patients with hereditary or idiopathic angioedema.
Hypersensitivity Adverse Reactions
Angioedema (severe swelling of tongue, face, lips, throat) Headache Hypotension Nausea
Dosage and Administrations Adult: 1.25mg SIVP over 5 minutes, may repeat X1
Duration of Action Onset: 15 minutes Peak:1-4 hrs Duration:4-6 hrs
Special Considerations/Drug Interactions Use caution when administering to renal patients May cause hyperkalemia Enalaprilat may potentiate the effect of diuretics causing a significant decrease in
blood pressure Lithium toxicity has been reported in patients receiving lithium concomitantly with
drugs which cause elimination of sodium, including ACE inhibitors

James Vincent M.D. Page 136
Medical Protocols
EPINEPHRINE (ADRENALINE) Class
Sympathomimetic
Mechanism of Action Epinephrine stimulates alpha-, beta1-, and beta2-adrenergic receptors in dose-
related fashion. It is the initial drug of choice for treating bronchoconstriction and hypotension resulting from anaphylaxis as well as all forms of cardiac arrest. Rapid injection produces a rapid increase in systolic pressure, ventricular contractility, and heart rate. In addition, epinephrine causes vasoconstriction in the arterioles of the skin, mucosa, and splanchnic areas and antagonizes the effects of histamine.
Indications Bronchial asthma Acute allergic reaction Cardiac arrest Anaphylaxis Protocol: V-Fib/Pulseless V-Tach, Asystole/PEA, Anaphylaxis, COPD/Asthma,
Bradycardia Contraindications
Hypersensitivity Hypovolemic shock Coronary insufficiency Hypertension
Adverse Reactions
Headache, nausea, restlessness, weakness, dysrhythmias, hypertension Dosage and Administrations Adult:
V-Fib/Pulseless V-Tach, Asystole/PEA – 1mg (1:10,000) IV/IO every 3-5 minutes Anaphylaxis – 0.3mg (1:1,000) IM every 5 minutes. May repeat x 1
COPD/Asthma - 0.3mg (1:1,000) IM. May repeat x 1 in 5 minutes. Hypotension – 10 mcg q 3 minutes, or 5-20 mcg/min (calculated from normal Dosage of 0.1-0.4 mcg/kg/min Pediatric:
V-Fib/Pulseless V-Tach, Asystole/PEA – 0.01mg/kg (1:10,000) IV/IO every 3-5 minutes Anaphylaxis – 0.01mg/kg (1:1,000) IM every 5 minutes, Max dose 0.3 mg. May repeat x 2
Asthma - 0.01mg/kg (1:1,000) IM every 5 minutes. May repeat x 1 Bradycardia - 0.01mg/kg (1:10,000) IV/IO every 3-5 minutes Duration of Action
Onset: (SQ) 5-10 min (IV) 1-2 min
Duration: 5-10 min

James Vincent M.D. Page 137
Medical Protocols
Special Considerations/Drug Interactions MAOI’s and Bretylium may potentiate the effect of Epinephrine.
Beta-adrenergic antagonists may blunt inotropic response.
Sympathomimetics and phosphodiesterase inhibitors may exacerbate dysrhythmia
response.
May be deactivated by alkaline solutions (Sodium Bicarbonate, Furosemide).
Syncope has occurred after epinephrine administration to asthmatic children.
May increase myocardial oxygen demand.

James Vincent M.D. Page 138
Medical Protocols
EPINEPHRINE NEBULIZED Class
Sympathomimetic
Mechanism of Action Acts as a bronchodilator that stimulates beta2 receptors in the lungs, resulting in
relaxation of bronchial smooth muscle. It alleviates bronchospasm, increases vital
capacity, and reduces airway resistance. It inhibits the release of histamine and is
useful in treating laryngeal edema.
Indications Bronchial asthma Prevention of bronchospasm Croup (laryngotracheobronchitis) Laryngeal edema Protocol: Pediatric Respiratory Distress : Brochiolitis and Croup
Contraindications Hypertension
Cardiovascular disease
Epiglottitis
Adverse Reactions Tachycardia
Dysrhythmia
Dosage and Administrations Pediatric:
Dilute 0.5ml of Epinephrine (1:1000) in 2.5ml of saline. Administer by
aerosolization
May repeat x 1 in 5 minutes.
Duration of Action Onset : within 5 minutes
Duration : 1-3 hours
Special Considerations/Drug Interactions - Epinephrine
May produce tachycardia and other dysrhythmias
Monitor vital signs closely
Excessive use may cause bronchospasm
MAOI’s and Bretylium may potentiate the effect of Epinephrine.
Beta-adrenergic antagonists may blunt inotropic response.
Sympathomimetics and phosphodiesterase inhibitors may exacerbate dysrhythmia
response.

James Vincent M.D. Page 139
Medical Protocols
ETOMIDATE (AMIDATE) Class
Etomidate is a hypnotic drug without analgesic activity Mechanism of Action
Etomidate is a hypnotic drug without analgesic activity Etomidate is a short-acting hypnotic, which appears to have gamma-aminobutyric acid (GABA)–like effects. Unlike the barbiturates, etomidate reduces subcortical inhibition at the onset of hypnosis while inducing neocortical sleep. Studies in animals suggest that a part of the action of etomidate consists of a depression of the activity and reactivity of the brain stem reticular formation.
Indications Induction of general anesthesia Protocol: Rapid sequence intubation, and post resuscitation induced hypothermia
Contraindications Patients who have known hypersensitivity
Adverse Reactions Etomidate may induce cardiac depression in elderly patients, particularly those with
hypertension Transient venous pain on injection and transient skeletal muscle movements,
including myoclonus Hyperventilation, hypoventilation, apnea of short duration (5 to 90 seconds with
spontaneous recovery), laryngospasm, hiccup and snoring. These conditions were managed by conventional countermeasures.
Hypertension, hypotension, tachycardia, bradycardia and other arrhythmias have occasionally been observed
Dosage and Administrations Adult:
20 mg IV/IO Pediatric:
0.3 mg/kg IV/IO, Max dose 20mg Duration of Action - Etomidate
Onset: within 1 minute Duration: 3 to 5 minutes
Special Considerations/Drug Interactions Risk benefit should be considered with Immunosuppression, sepsis or
Transplantation (potential effects on adrenal function) Etomidate can block the adrenal gland's production of cortisol and other steroid
hormones, possibly resulting in temporary adrenal gland failure. This may cause abnormal salt and water balance, lowered blood pressure, and, ultimately, shock.

James Vincent M.D. Page 140
Medical Protocols
FENTANYL Class
Synthetic narcotic Mechanism of Action
A potent, short-acting, rapid-onset opioid agonist that relieves pain by stimulating opioid receptors in CNS; also causes respiratory depression and peripheral vasodilation; inhibits intestinal peristalsis and sphincter of Oddi spasm; stimulates chemoreceptors that cause vomiting; increases bladder tone.
Indications Traumatic and Cardiac pain management, rapid sequence intubation Protocol: rapid sequence intubation, pain management,
Contraindications Hypersensitivity
Adverse Reactions
Bradycardia, more rapid and significant ventilation impairment in patients with
COPD and prolonged clinical effects in patients with hepatic or renal impairment. Severe muscular rigidity develops in patients if administered rapidly.
Dosage and Administrations Adult:
50-100mcg SIVP over 1-2 minutes; Max dose of 200mcg, May repeat X1 May be administered via IV/IM/IN
Pediatric: 1 mcg/kg SIVP over 1-2 minutes May repeat 1 mcg/kg X1
Duration of Action Onset: Immediately (IV); 7 to 8 min (IM). Duration: 30 to 60 min (IV); 1 to 2 h (IM).
Special Considerations/Drug Interactions Amiodarone: Profound bradycardia, sinus arrest, and hypotension may occur. Barbiturate anesthetics (e.g., thiopental) May have additive effects. Reduce
dosage of one or both agents. CNS depressants (e.g., alcohol, benzodiazepines [e.g., diazepam], general
anesthetics, hypnotics, other opioid, phenothiazines, sedating antihistamines, sedatives, skeletal muscle relaxants, tranquilizers) Concomitant use may produce increased depressant effects (e.g., hypotension, profound sedation, respiratory depression).
MAOIs (e.g., phenelzine) Fentanyl is not recommended for use in patients who have received MAOIs within 14 days.

James Vincent M.D. Page 141
Medical Protocols
Geodon Class
Antipsychotropic Mechanism of Action
It has been proposed that Geodon’s beneficial effects are achieved by blocking dopamine and serotonin receptors. Geodon also inhibits reuptake of serotonin and epinephrine in the brain.
Indications Psychosis where Excited Delirium is suspected.
Contraindications
Hypersensitivity to Geodon Adverse Reactions
Prolonged Q-T Interval Dosage and Administrations
Adult: Excited Delirium: 10-20mg IM
Duration of Action
Onset: Within 1 min Duration: 9-17 min
Special Considerations/Drug Interactions
Should not be given to patients with recent acute myocardial infarction, or known
history of QT prolongation.
Geodon should never be given intravenously.

James Vincent M.D. Page 142
Medical Protocols
IPRATROPIUM (ATROVENT) Class
Anticholinergic (parasympatholytic) agent Mechanism of Action
Atrovent inhibits interaction of acetylcholine at receptor sites on the bronchial smooth muscle, resulting in bronchodilation
Indications Patients with bronchospasm (asthma and COPD) may benefit from this medication.
Patients will typically present with wheezing or persistent cough. Remember with severe bronchospasm, the patient may not be moving enough air to have lung sounds auscultated
Protocol: COPD/Asthma Contraindications
The solution that is used for nebulization can be safely used in patients with a soy product allergy, but not if there is a known hypersensitivity to Ipratropium or atropine.
Adverse Reactions Palpitations Dizziness Anxiety Tremors Headache Nervousness Dry mouth
Dosage and Administrations Adult:
0.5mg mixed with Albuterol via aerosolization x 3 Pediatric:
0.5mg mixed with Albuterol via aerosolization x 3 Duration of Action
Onset:5-15 minutes Duration: 2-8 hrs
Special Considerations/Drug Interactions Can cause a paradoxical bronchospasm increasing the patient's respiratory
difficulties. Nebulizers can be attached to the ET tube and ventilated into patient with BVM.

James Vincent M.D. Page 143
Medical Protocols
LABETALOL Class
Alpha- and beta-adrenergic blocker Mechanism of Action
Labetalol is a competitive alpha1-receptor blocker as well as a nonselective beta-receptor blocker used to lower blood pressure in a hypertensive crisis. Because of alpha- and beta-blocking properties, blood pressure is reduced without reflex tachycardia, and total peripheral resistance is decreased without a significant alteration in cardiac output.
Indications Hypertension Protocol: Hypertension
Contraindications Bronchial asthma Congestive heart failure Second- and third-degree heart block Bradycardia Cardiogenic shock
Adverse Reactions Headache and facial flushing Ventricular dysrhythmias Hypotension and dizziness Dyspnea Diaphoresis
Dosage and Administrations Adult:
10-20 mg SIVP over 2 min. Repeat X2 q 10 min Duration of Action
Onset: Within 5 min Duration: 3-6 hr
Special Considerations/Drug Interactions Bronchodilator effects of beta-adrenergic agonists may be blunted by Labetalol.
Nitroglycerin may augment hypotensive effects. Observe for signs of congestive heart failure, bradycardia, and bronchospasm.
Labetalol should only be administered with the patient in a supine position.

James Vincent M.D. Page 144
Medical Protocols
LIDOCAINE (XYLOCAINE) Class
Antidysrhtythmic Mechanism of Action
Lidocaine decreases phase-4 diastolic depolarization and suppresses premature ventricular contractions. In addition, it is used to treat ventricular tachycardia and some cases of ventricular fibrillation. Lidocaine also raises the ventricular fibrillation threshold
Indications Protocol: IO pain management
Contraindications Hypersensitivity Stokes-Adams syndrome Second- or third-degree heart block in the absence of an artificial pacemaker
Adverse Reactions Lightheadedness, hypotension, confusion, blurred vision, cardiovascular collapse,
bradycardia CNS depression (altered level of consciousness, irritability, muscle twitching,
seizures) with high doses Dosage and Administrations
Adult: Intraosseous pain: 40 mg IV = 2 mL of 2% cardiac lidocaine
Pediatric: Intraosseous pain: 0.5 mg/kg of 2% cardiac lidocaine = 0.05 mL/kg,
10 kg = 0.5 mL, 20 kg = 1 mL, 30 kg = 1.5mL
Duration of Action Onset: 30-90 sec
Duration: 2-4 hr Special Considerations/Drug Interactions
Since Lidocaine is metabolized in the liver, elderly patients, patients with hepatic diseases, shock or congestive heart failure will not break down the drug rapidly. Consider one-half dose for boluses and drip rate in these patients.
Apnea induced with succinylcholine may be prolonged with large doses of Lidocaine.
If bradycardia occurs in conjunction with PVCs, always treat the bradycardia first with atropine or TCP. Exceedingly high doses of Lidocaine can result in coma or death.

James Vincent M.D. Page 145
Medical Protocols
MAGNESIUM SULFATE Class
CNS depressant Mechanism of Action
Magnesium sulfate reduces striated muscle contractions and blocks peripheral neuromuscular transmission by reducing acetylcholine release at the myoneural junction.
Indications Seizures of eclampsia (toxemia of pregnancy) Torsade’s de pointes Severe asthma Protocol: Asthma, Eclamptic pregnancy
Contraindications Heart block
Adverse Reactions Diaphoresis Facial flushing Hypotension Depressed reflexes Hypothermia Reduced heart rate Circulatory collapse Respiratory depression
Dosage and Administrations Adult:
2 grams in 50 cc of NS over 10 minutes Duration of Action
Onset: Immediate Duration: 3-4 hr
Special Considerations/Drug Interactions CNS depressant effects may be enhanced if the patient is taking other CNS
depressants. Serious changes in cardiac function may occur with cardiac glycosides.
IV calcium gluconate or calcium chloride should be available as an antagonist to magnesium if needed.
Magnesium must be used with caution in patients with renal failure, since it is cleared by the kidneys and can reach toxic levels easily in those patients.
James Vincent M.D. Page 146
Medical Protocols
METHYLPREDNISOLONE (SOLU-MEDROL) Class
Glucocorticoid Mechanism of Action
Methylprednisolone is a synthetic steroid that suppresses acute and chronic
inflammation. In addition, it potentiates vascular smooth muscle relaxation by beta-
adrenergic agonists and may alter airway hyperactivity. A newer usage is for
reduction of posttraumatic spinal cord edema
Indications Anaphylaxis Bronchodilator for unresponsive asthma Shock (controversial) Acute spinal cord injury Protocol: COPD/Asthma, Anaphylaxis
Contraindications Use with caution in patients with, immuno-suppressed systems, GI bleeding and
diabetes mellitus. Adverse Reactions
Headache Hypertension Sodium and water retention Hypokalemia Alkalosis
Dosage and Administrations Adult:
125mg IV/IM
Pediatric:
2mg/kg IV/IM Max dose of 125 mg
Duration of Action Onset: 1-2 hrs Duration: 8-24 hr
Special Considerations/Drug Interactions Crosses the placenta and may cause fetal harm.
Ensure that the patient is not currently ill (pneumonia) or is currently taking
steroids.
James Vincent M.D. Page 147
Medical Protocols
MIDAZOLAM (VERSED) Class
Short-acting benzodiazepine CNS depressant Mechanism of Action
Midazolam HCl is a water-soluble benzodiazepine that may be administered for conscious sedation to relieve apprehension or impair memory before endotracheal or nasotracheal intubation.
Indications Premedication for tracheal intubation Seizures Protocols: Rapid sequence intubation, seizures, anxiety, behavioral, sedation prior
to cardioversion Contraindications
Hypersensitivity to Midazolam Glaucoma Shock Depressed vital signs Concomitant use of barbiturates, alcohol, narcotics, or other CNS depressants
Adverse Reactions Cough and/or hiccups Over-sedation Nausea and vomiting Headache and/or blurred vision Fluctuations in vital signs including hypotension Respiratory depression and/ or arrest
Dosage and Administrations Adult:
Anxiety: 1-2 mg IV/IM/IN RSI: 5mg IV/IM/IN, May Repeat X 1 Seizures, behavioral: 5mg IN/IV/IM, May repeat x 1 Excited Delirium: 10 mg/IV/IM
Pediatric: Seizures: 0.1 mg/kg IN/IV/IM Max 5mg Sedation: 0.1mg/kg Max 2mg
Duration of Action Onset: 1-3 min (IV); dose dependent Duration: 2-6 hr; dose dependent
Special Considerations/Drug Interactions Sedative effect of midazolam may be accentuated by concomitant use of
barbiturates, alcohol, or narcotics (it should therefore not be used in patients who have taken CNS depressants).
Administer immediately before the intubation procedure.
James Vincent M.D. Page 148
Medical Protocols
MORPHINE SULFATE Class
Opioid analgesic Mechanism of Action
Morphine sulfate is a natural opium alkaloid that increases peripheral venous capacitance and decreases venous return ("chemical phlebotomy"). It promotes analgesia, euphoria, and respiratory and physical depression. Secondary pharmacological effects of morphine include depressed responsiveness of alpha-adrenergic receptors (producing peripheral vasodilation) and baroreceptor inhibition. In addition, because morphine decreases both preload and afterload, it may decrease myocardial oxygen demand.
Indications Moderate to severe acute and chronic pain
Should be used with caution with pulmonary edema Protocol: pain management
Contraindications Hypersensitivity to narcotics Diarrhea caused by poisoning Hypovolemia Hypotension
Adverse Reactions Hypotension, tachycardia, bradycardia, palpitations, syncope, facial flushing,
respiratory depression, euphoria, bronchospasm, dry mouth Dosage and Administrations
Adult: 2-5 mg every 5 minutes Max 10 mg
Pediatric 0.1 mg/kg Max 5mg
Duration of Action Onset: Immediate Duration: 2-7 hr
Special Considerations/Drug Interactions CNS depressants may potentiate effects of morphine (respiratory depression,
hypotension, sedation). MAOl’s may cause paradoxical excitation. Narcotics rapidly cross the placenta. Use with caution in older adults, those with
asthma, and those susceptible to CNS depression. May worsen bradycardia or heart block in inferior myocardial infarction (vagotonic effect). Naloxone should be readily available.

James Vincent M.D. Page 149
Medical Protocols
NALOXONE (NARCAN) Class
Synthetic opioid antagonist Mechanism of Action
Naloxone is a competitive narcotic antagonist used in the management and reversal of overdoses caused by narcotics and synthetic narcotic agents. Unlike other narcotic antagonists, which do not completely inhibit the analgesic properties of opiates, naloxone antagonizes all actions of morphine.
Indications Decreased level of consciousness Coma of unknown origin For the complete or partial reversal of CNS and respiratory depression induced by
opioids: Narcotic agonist : Morphine sulfate, Heroin, Hydromorphone (Dilaudid), Methadone , Meperidine (Demerol) , Paregoric, Fentanyl citrate (Sublimaze), Oxycodone (Percodan), Codeine, Propoxyphene (Darvon)
Narcotic agonist and antagonist: Butorphanol tartrate (Stadol), Pentazocine (Talwin), Nalbuphine (Nubain)
Protocol: Overdose Contraindications
Hypersensitivity Adverse Reactions
Tachycardia and/or dysrhythmias Hypertension Nausea and vomiting Diaphoresis
Dosage and Administrations Adult:
0.4mg IV/IM/IN, Max of 2 mg Duration of Action
Onset: Within 2 min Duration: 30-60 min
Special Considerations/Drug Interactions Seizures have been reported (no causal relationship established). May not reverse hypotension. Caution should be exercised when administering
naloxone to narcotic addicts (may precipitate withdrawal with hypertension, tachycardia, and violent behavior).
James Vincent M.D. Page 150
Medical Protocols
NITROGLYCERIN Class
Vasodilator Mechanism of Action
It is now believed that atherosclerosis limits coronary dilation and that the benefits of nitrates and nitrites result from dilation of arterioles and veins in the periphery. The resulting reduction in preload and to a lesser extent in afterload decreases the work load of the heart and lowers myocardial oxygen demand. Nitroglycerin is very lipid soluble and is thought to enter the body from the GI tract through the lymphatics rather than the portal blood.
Indications Ischemic chest pain Congestive heart failure(CHF) Protocol: Acute coronary syndrome(ACS) , CHF
Contraindications Hypersensitivity Hypotension Do not administer NTG to male patients who have taken medication for erectile
dysfunction in the previous 48 hours. The combination of these meds with NTG may produce profound hypotension or cardiac arrest.
Adverse Reactions Transient headache Postural syncope Reflex tachycardia Hypotension Nausea and vomiting Muscle twitching Diaphoresis
Dosage and Administrations Adult:
ACS: 0.4 mg metered dose every 5 minutes until systolic BP of > 90 CHF: 0.4mg every 3 minutes x 5 Hypertension: 0.4mg X3
Duration of Action Onset:1-3 min Duration:20-30 min
Special Considerations/Drug Interactions Nitroglycerin decomposes when exposed to light or heat.
James Vincent M.D. Page 151
Medical Protocols
NOREPINEPHRINE (LEVOPHED) Class
Sympathomimetic
Mechanism of Action Norepinephrine alpha- and beta1-adrenergic receptors in dose-related fashion. It is
the initial drug of choice for treating hypotension refractory to IV fluids in the setting of sepsis. Continuous IV infusion results in increased contractility and heart rate as well as vasoconstriction, thereby increasing systemic blood pressure and coronary blood flow. Clinically, alpha effects (vasoconstriction) are greater than beta effects (inotropic and chronotropic effects).
Indications Hypotension refractory to 2L of IV fluids in the setting of sepsis Protocol: Hypotension
Contraindications Hypersensitivity Hypertension
Adverse Reactions
Headache, nausea, restlessness, weakness, dysrhythmias, hypertension Dosage and Administrations
Adult: Hypotension – 2-12 mcg/min NOTE: NOT WEIGHT BASED INFUSION Pediatric: Not used in prehospital setting due to need for extremely low
weight-based dose (0.05-0.1 mcg/kg/min) Special Considerations/Drug Interactions
Now considered first line vasoactive agent for septic shock, as dopamine was found
in a large clinical trial to have an unacceptably high occurrence of dysrhythmias
Large doses have been described in clinical trials 0.01-3 mcg/kg/minute
(0.7 to 200 mcg/min)
James Vincent M.D. Page 152
Medical Protocols
ONDANSETRON (ZOFRAN) Class
Antiemetic, Serotonin Receptor Antagonist, 5-HT3 Mechanism of Action
Antiemetic - The mechanism by which ondansetron works to control nausea and vomiting is not fully understood; it is believed that the antiemetic properties occur as a result of serotonin receptor antagonism.
Indications Nausea and vomiting due to chemotherapy. Prophylactic use prior to administration of pain management medication. Nausea and vomiting with moderate to severe dehydration or electrolyte imbalance. Protocol: nausea including nausea in a CVA patient
Contraindications History of allergic reaction to ondansetron or to any medicine similar to ondansetron,
including dolasetron (Anzemet), granisetron (Kytril), or palonosetron (Aloxi). Adverse Reactions
Constipation, diarrhea, dry mouth Headache, dizziness, drowsiness/sedation Anaphylaxis (rare) Fatigue, malaise, chills Cardiac dysrhythmia (rare), hypotension Bronchospasm Muscle pain
Dosage and Administrations Adult:
4mg IV/IM, may repeat X1 Pediatric:
6 months to 4 years: 2 mg IV/IM Greater than 4 years: 4 mg IV/IM
Duration of Action Onset: Immediate Duration 4-6 hours
Special Considerations/Drug Interactions Patients with a history, or family history, of Long QT syndrome; transient EKG changes
have been seen with IV administration including QT interval prolongation.

James Vincent M.D. Page 153
Medical Protocols
ORAL GLUCOSE Class
Monosaccharide Carbohydrate Mechanism of Action
After absorption of glucose in the GI tract, glucose is distributed in the tissues and provides a prompt increase in circulating blood sugar
Indications Hypoglycemic conscious pt w/ altered mental status
Protocol: Diabetic emergencies Contraindications
Unconscious
Patient hasn't taken insulin for days Adverse Reactions
Nausea Dosage and Administrations
Adult and Pediatric: 15 grams PO SL Preferred method of administration is between the cheek and gums
Duration of Action Onset: 15 minutes
Special Considerations/Drug Interactions Assure patient has the capabilities of swallowing and maintaining an airway Ensure that a BGL is checked prior to administration of Glucose in all patients,
especially ones that may have a suspected head injury Reassess BGL after administration of Glucose

James Vincent M.D. Page 154
Medical Protocols
OXYGEN Class
Naturally occurring atmospheric gas Mechanism of Action
Oxygen is odorless, tasteless, colorless gas that is present in room air at a concentration of about 21%. It helps oxidize glucose to produce ATP (Adenosine triphosphate).
Indications Confirmed or suspected hypoxia Ischemic chest pain Respiratory insufficiency Prophylatically during air transport Confirmed or suspected carbon monoxide poisoning and other causes of decreased
tissue oxygenation Protocol: Universal treatment guidelines
Contraindications Oxygen should not be withheld from any patients, even those with COPD.
Adverse Reactions High flow oxygen may cause decreased LOC and respiratory depression in patients
with COPD Dosage and Administrations
Adult and Pediatric: High concentration: 10-15 lpm via nonrebreather mask Low concentration: 1-4 lpm via nasal cannula Nebulizer: 8 lpm
Duration of Action Onset: Immediate Duration: less than 2 minutes
Special Considerations/Drug Interactions Oxygen vigorously supports combustion

James Vincent M.D. Page 155
Medical Protocols
ROCURONIUM
Class Non depolarizing neuromuscular blocker
Mechanism of Action Rocuronium bromide is a non-depolarizing skeletal muscle relaxant. Binding with
cholinergic receptor sites inhibits transmission of nerve impulses, antagonizing the action of acetylcholine. Has no analgesic properties and the patient maybe conscious, but unable to communicate by any means.
Indications
To maintain complete muscle relaxation with an intubated patient Protocol: rapid sequence intubation
Contraindications Hypersensitivity
Adverse Reactions Causes respiratory paralysis; supportive airway control must be continuous and under
direct observation at all times. Dosage and Administrations
Adult: 50mg IV
Pediatric: 1mg/kg (max 50mg)
Duration of Action Onset: 1-2 minutes Peak: 4 minutes Duration: 30 minutes
Special Considerations/Drug Interactions Myasthenia gravis and other neuromuscular diseases increase sensitivity to the drug.
James Vincent M.D. Page 156
Medical Protocols
SODIUM BICARBONATE Class
Buffer Mechanism of Action
Sodium bicarbonate reacts with hydrogen ions to form water and carbon dioxide and thereby can act to buffer metabolic acidosis. Increasing the plasma concentration of bicarbonate causes blood pH to rise.
Indications Tricyclic antidepressant (TCA) overdose Alkalinization for treatment of specific intoxications Protocol: Hyperkalemia, Crush injury
Contraindications In patients with chloride loss from vomiting and Gl suction Metabolic and respiratory alkalosis Hypocalcemia Hypokalemia
Adverse Reactions Metabolic alkalosis Hypoxia Rise in intracellular Pco2 and increased tissue acidosis Electrolyte imbalance (tetany) Seizures Tissue sloughing at injection site
Dosage and Administrations Adult:
Hyperkalemia/Crush injury: 50- 100mEq TCA: 50-100 mEq
Duration of Action Onset: 2-10 min Duration: 30-60 min
Special Considerations/Drug Interactions May precipitate in calcium solutions. Vasopressors may be deactivated. Bicarbonate administration produces carbon dioxide, which crosses cell membranes
more rapidly than bicarbonate, potentially worsening intracellular acidosis. May increase edematous or sodium-retaining states. May worsen congestive heart failure.

James Vincent M.D. Page 157
Medical Protocols
THIAMINE Class
Vitamin (B1) Mechanism of Action
Thiamine combines with ATP to form thiamine pyrophosphate coenzyme, a necessary component for carbohydrate metabolism. Most vitamins required by the body are obtained through diet, but certain states, such as alcoholism and malnourishment, may affect the intake, absorption, and use of thiamine. The brain is extremely sensitive to thiamine deficiency.
Indications Coma of unknown origin (before the administration of dextrose 50%, or Naloxone) Delirium tremens Beriberi (rare) / Wernicke's encephalopathy Protocol: Diabetic emergencies
Contraindications There are no significant drug interactions with other emergency medications
Adverse Reactions Hypotension (from rapid injection or large dose) Anxiety Diaphoresis Nausea and vomiting Allergic reaction (usually from IV injection; very rare)
Dosage and Administrations Adult: 100mg IV/IM
Duration of Action Onset: Rapid Duration: variable
Special Considerations/Drug Interactions Large IV doses may cause respiratory difficulties. Anaphylactic reactions have been reported.
James Vincent M.D. Page 158
Medical Protocols
VECURONIUM Class
Non depolarizing neuromuscular blocker Mechanism of Action
Vecuronium bromide is a non-depolarizing skeletal muscle relaxant. Binding with cholinergic receptor sites inhibits transmission of nerve impulses, antagonizing the action of acetylcholine. Has no analgesic properties and the patient maybe conscious, but unable to communicate by any means. First muscles affected include eyes, face, neck; followed by limbs, abdomen, chest; diaphragm affected last. Recovery usually occurs in the reverse order and may take longer than 60 minutes.
Indications
To maintain general anesthesia with an intubated patient Protocol: rapid sequence intubation
Contraindications Hypersensitivity
Adverse Reactions Causes respiratory paralysis; supportive airway control must be continuous and under
direct observation at all times. Dosage and Administrations
Adult: 10mg IV
Pediatric: 0.1mg/kg (max 10mg)
Duration of Action Onset: 30-60 seconds Peak: 3-5 minutes Duration: 30-60 minutes
Special Considerations/Drug Interactions Myasthenia gravis and other neuromuscular diseases increase sensitivity to the drug.

GAAA DAILY AMBULANCE CHECK LIST
James Vincent M.D. Page 159
911 Date __________________________
Truck # ________________________
Medic # ________________________
Personnel Printed Name
_______________________________
Personnel Printed Name
_______________________________
Supervisor _____________________
Tough Book # __________________
( ) Engine Oil Level
( ) Radiator Level
( ) Transmission Fluid
( ) Tires
Safety Sticker Expiration ________
Insurance Card Expiration________
DHSH Cert. Expiration __________
( ) GAAA Protocols - 1
( ) Emergency Response Guide - 1
( ) Triage Tags - 25
( ) Mounted Fire Extinguisher - 1
( ) Key Map Book – 1
( ) Flashlight - 1
EKG Monitor#__________ (MICU)
( ) Data Cable – (E-series) - 1
( ) USB thumb drive – (X-series) - 1
( ) V-Leads - 1
( ) Limb Leads - 1
( ) Electrodes - 1 pack
( ) Multi-function Pads Adult - 1
( ) Multi-function Pads Pedi – 1
( ) Capnography NC (Adult and Pedi ) –
1ea
Capnography ETT (Adult & Pedi) – 1ea
( ) Additional Battery - 1
NarcKit – MICU’s / M10
[ ] Diazepam 20mg x 1
[ ] Fentanyl 100mcg x 2
[ ] Versed 5 mg x 4
[ ] Morphine 10mg x 1
[ ] Geodon 20mg x 1
( ) Carpujet - 1
( ) MADD Nasal Atomizer – 1
( ) Knocks box key-1 (M-1,2,3,4 only)
( ) CPAP # _____________________
( ) CPAP Circuit - 1
( ) Portable Suction # ____________
( ) Disposable Canister - 1
( ) Suction Tubing – 1
( ) Yankuer – 1
( ) Suction Cath (6fr & 14fr) – 1ea
( ) ET Roll
( ) Laryngoscope Handle – 1
( ) Mac Blades-(1, 2, 3, 4) - 1ea
( ) Miller Blades-(0, 1, 2, 3, 4) -1ea
( ) ET Tubes-(2.5, 3, 3.5, 4, 5, 6, 6. 5, 9) -
1 ea
( ) ET Tubes (7.0, 7.5, 8.0) – 2 ea
( ) Stylet – (6fr, 10fr, 14fr) -1 ea
( ) ET Tube Holder / Ties – 1
( ) Capnography ETT (Adult & Pedi) – 1ea
( ) OPA’s (5 sizes) – 1 set
( ) Adult Magill Forceps – 1
( ) Pediatric Magill Forceps – 1
( ) Bougie ETT Introducer – 1
( ) ETT Tamer/Ties (Adult and Pedi) –
1 ea
( ) Surgilube - 1
( ) Syringe 10cc – 1
( ) Syringe 30cc – 1
( ) C Batteries – 2
( ) Airway Bag
Oxygen Cylinder _____________psi
( ) CPAP Quick Connect – 1
( ) BVM (Adult, Child, Infant) - 1 ea
( ) ET Roll – 1
( ) King Tube (Sizes 3, 4, 5) – 1ea
( ) Quick Tach – 1
( ) Needle Decompression Kit - 1
( ) NRB Adult – 2
( ) NRB Pediatric - 1
( ) Nasal Cannula – 2
( ) Nebulizer - 1
( ) Hemostat – 1
( ) BP Cuff (Lg & Reg Adult, Child) 1ea
King Vision # ___________________
( ) King Vision Blade - 1
( ) Stethoscope – 1
( ) Pen Light - 1
( ) Trauma Shears – 1
( ) Kerlix Roll – 2
( ) Ace Wrap - 1
( ) Occlusive Dressing – 2
( ) 4 x 4 sterile – 4
( ) Triangular Bandage - 2
( ) Sam Splint - 1
( ) N95 Mask – 3
( ) Medication Kit
EZ IO Drill #___________________
( ) IO Needles (15, 25, 45mm) - 1ea
( ) Broselow Tape - 1
( ) IV Caths (16, 18, 20,22,24ga) 2ea
( ) Needles (20ga) - 2
( ) Syringe 1cc – 1
( ) Syringe 3cc – 3
( ) Syringe 10cc –3
( ) Tape 1” – 2
( ) Paper tape 1” - 1
( ) Alcohol Preps – 5
( ) Beta Dine Preps - 2
( ) Non sterile 4x4 - 10
( ) Saline Locks – 5
( ) Saline 10cc vial/syringe – 5
( ) Saline Bags (250 & 500 or 1000cc) –
1ea
( ) Select 3 Drip Sets – 1
( ) Glucometer – 1
( ) Strips and Lancets – 6 ea
Unit Equipment
Main O2 Cylinder ____________psi
Stretcher # _____________________
Stair chair # ____________________
Combi-Board or Scoop #-____________
( ) KED
( ) Sager Splint
( ) Air Splint(Sm, Med, Lg, & Torso)
( ) Air Splint Pump - 1
( ) Portable O2 - 3
( ) Traffic Safety Vest – 3
( ) Reflector Kit - 1
( ) Child seat (optional) – 1
( ) Back boards – 2
( ) Backboard webbing - 1
( ) C-Collars Adult – 6
( ) C-Collars (Pedi & Infant) – 4 ea
( ) Head Rolls – 6
( ) 2inch backboard tape – 1
( ) BP Cuff (Thigh, Lg. Adult, Reg.
Adult, Child, Infant) – 1ea
( ) Stethoscope – 1
( ) ET Roll – 1
( ) AAA Batteries – 3
( ) King Vision Blade - 1
( ) ETT holder/Tie – 1
( ) ETCO2 detector ET tube -1
( ) ETCO2 detector ET tube -1
( ) Capnography NC Adult – 4
( ) BVM (Adult, Child, Infant) - 1 ea
( ) NRB- Adult –5
( ) NRB – Pedi & Infant – 2 ea
( ) NC – 5
( ) Nebulizer – 5
( ) Yankuer/Suction Tubing - 3
( ) Suction Canister – 1 wall & 1 extra
( ) NGT- 18fr – 2
( ) Suction catheters (14fr & 6fr) 2ea
( ) EKG Electrodes - 1 pk
( ) Multi-function Pads Adult - 1
( ) Multi-function Pads Pedi - 1
( ) ECG Paper - 1
( ) OB Kit – 2

GAAA DAILY AMBULANCE CHECK LIST
James Vincent M.D. Page 160
911 Unit Equipment Continued…
( ) Foil Blanket - 1
( ) Burn Sheet - 2
( ) Trauma Dressing – 2
( ) Abdominal Pads - 2
( ) Alcohol Preps – 1 bx
( ) Iodine Preps – 3
( ) Band Aids – 1 bx
( ) Bacitracin – 5 pk
( ) Tape – 1” – 4
( ) Paper Tape - 1
( ) Sterile Water - 2
( ) Rubbing Alcohol - 1
( ) Triangular Bandages - 4
( ) Kerlix – 4
( ) Ace Wrap – 2
( ) Commercial Tourniquet - 1
( ) Occlusive Dressing - 4
( ) 4x4 Sterile – 1 bx
( ) 4x4 Non sterile – 1 pk
( ) Cold packs- 5
( ) Hot Packs – 5
( ) Trauma Shears – 1
( ) Ring Cutter - 1
( ) Glucometer Strips – 10
( ) Lancets – 6
( ) Ammonia Inhalants – 5
( ) Select 3 – 6
( ) Buretrol set – 1
( ) Dial-a-flow-1
( ) Saline 10cc vial/syringe – 10
( ) Saline 50cc bag – 2
( ) Saline 250cc bag – 2
( ) Saline 500 or 1000cc bag – 6
( ) IV catheter (16, 18, 20) -6 ea
( ) IV catheter (22, 24) – 2 ea
( ) Needle 20ga – 5
( ) IO 15ga – 1
( ) Syringe 1cc- 2
( ) Syringe 3 cc – 5
( ) Syringe 10cc – 10
( ) Syringe 30cc – 2
( ) Sharps Container Lg – 1
( ) Sharps Container Sm – 1
( ) Biohazard Bags – 2
( ) Trash Bags – 2
( ) N95 Mask – 4
( ) Gowns- 4
( ) Safety Glasses- 3
( ) Gloves (Sm, Med, Lg, X-Lg) -1bx
( ) Hand Sanitizer – 1
( ) Cavicide Wipes/Spray- 1
( ) Thermometer
( ) Peroxide-1 btl
( ) stuffed animal x2
( ) odor neutralizer x1
MEDICATIONS
KIT UNIT
Activated Charcoal 50g [ ] x 1
[ ] x 5 Adenosine 6mg [ ] x 5
[ ] x 3 Albuterol 2.5mg [ ] x 6
[ ] x 2 Amiodarone 150mg [ ] x 4
Ancef (Cefazolin) 1g [ ] x 2
[ ] x 1 Aspirin 81mg - 1 btl [ ] x 1
[ ] x 3 Atropine 1mg [ ] x 3
[ ] x 1 Dextrose 50% 25g [ ] x 1
[ ] x 1 Diltiazem 25mg [ ] x 2
(Keep in cooler if available)________
[ ] x 1 Diphenhydramine 50mg [ ] x 1
[ ] x 1 Calcium Gluc. 10ml [ ] x 1
[ ] x 1 Enalaprilat 2.5mg [ ] x 1
[ ] x 1 Epinephrine (1:1) 1mg [ ] x 1
[ ] x 6 Epinephrine (1:10) 1mg [ ] x 6
[ ] x 1 Etomidate 20mg [ ] x 1
[ ] x 1 Glucose Oral 15g [ ] x 1
[ ] x 2 Ipratropium 0.5 mg [ ] x 3
[ ] x 1 Labetalol 40mg [ ] x 1
[ ] x 1 Lidocaine 2% 100mg [ ] x 1
[ ] x 2 Magnesium Sulfate 1g [ ] x 2
[ ] x 1 Narcan 2mg [ ] x 1
[ ] x 1 Nitroglycerin Spray Btl [ ] x 1
[ ] Norepinephrine 4mg [ ] x2
[ ] x 1 Ondansetron 4mg [ ] x 2
[ ] x 2 Sodium Bicarb 50mEq [ ] x 2
MEDICATIONS
KIT UNIT
[ ] x 1 Solu-Medrol 125mg [ ] x 1
[ ] x 1 Succinylcholine 200mg [ ] x 1
(Keep in cooler if available)________
[ ] x 1 Thiamine 200mg [ ] x 1
[ ] x 1 Vecuronium 10mg or [ ] x 1 Rocuronium 100mcg [ ] x1
(Keep In cooler if available_________)

GAAA DAILY AMBULANCE CHECK LIST
James Vincent M.D. Page 161
NET Date __________________________
Truck # ________________________
Medic # ________________________
Personnel Printed Name
_______________________________
Personnel Printed Name
_______________________________
Supervisor _____________________
( ) Tough Book # ________________
( ) Engine Oil Level
( ) Radiator Level
( ) Transmission Fluid
( ) Tires
Safety Sticker Expiration ________
Insurance Card Expiration________
DHSH Cert. Expiration __________
( ) GAAA Protocols -1
( ) Emergency Response Guide - 1
( ) Triage Tags - 25
( ) Mounted Fire Extinguisher -1
( ) Key Map Book – 1
( ) Flashlight - 1
EKG Monitor/AED#_____________
( ) Data Cable - 1
( ) V-Leads - 1
( ) Limb Leads - 1
( ) Electrodes - 1 pack
( ) Multi-function Pads Adult - 1
( ) Multi-function Pads Pedi - 1
( ) Additional Battery - 1
NarcKit – MICU’s / M10
[ ] Diazepam 10mg x 1
[ ] Fentanyl 100mcg x 2
[ ] Versed 5 mg x 4
[ ] Morphine 10mg x 1
[ ] Geodon 20mg x 1
( ) Carpujet - 1
( ) MADD Nasal Atomizer – 1
( ) Knoks box key1 (medic 10 only)
( ) CPAP # _____________________
( ) CPAP Circuit - 1
( ) Portable Suction # ____________
( ) Disposable Canister - 1
( ) Suction Tubing – 1
( ) Yankuer – 1
( ) Suction Cath (6fr & 14fr) – 1ea
( ) ET Roll
( ) Laryngoscope Handle – 1
( ) Mac Blades-(1, 2, 3, 4) - 1ea
( ) Miller Blades-(0, 1, 2, 3, 4) -1ea
( ) ET Tubes-(2.5, 3, 3.5, 4, 5, 6, 6.5, 9) - 1
ea
( ) ET Tubes (7.0, 7.5, 8.0) – 2 ea
( ) Stylet – (6fr, 10fr, 14fr) -1 ea
( ) ET Tube Holder / Ties – 1
( ) CO2 detector (Adult & Pedi) – 1ea
( ) OPA’s (5 sizes) – 1 set
( ) Adult Magill Forceps – 1
( ) Pediatric Magill Forceps – 1
( ) Bougie ETT Introducer - 1
( ) Surgilube - 1
( ) Syringe 10cc – 1
( ) Syringe 30cc – 1
( ) C Batteries – 2
( ) Airway Bag
Oxygen Cylinder _____________psi
( ) CPAP Quick Connect – 1
( ) BVM (Adult, Child, Infant) - 1 ea
( ) ET Roll – 1
( ) King Tube (Sizes 3, 4, 5) -1
( ) Quick Trach - 1
( ) Needle Decompression Kit - 1
( ) NRB Adult – 1
( ) NRB Pediatric - 1
( ) Nasal Cannula – 2
( ) Nebulizer - 1
( ) BP Cuff (Lg & Reg. Adult) 1ea
( ) Stethoscope – 1
( ) Pen Light - 1
( ) Trauma Shears – 1
( ) Kerlix Roll – 1
( ) Occlusive Dressing – 2
( ) 4 x 4 sterile – 2
( ) Triangular Bandage -2
( ) Sam Splint - 1
( ) N95 Mask – 3
( ) Medication Kit
EZ IO Drill #_________________
( ) IO Needles (15, 25, 45mm) - 1ea
( ) Broselow Tape - 1
( ) IV Caths (16, 18, 20, 22,24ga) 2ea
( ) Needles (20ga) – 2 ea
( ) Syringe 1cc – 1
( ) Syringe 3cc – 2
( ) Syringe 10cc – 2
( ) Tape 1” – 2
( ) Paper Tape 1” - 1
( ) Alcohol Preps – 5
( ) Beta Dine Preps - 2
( ) Non sterile 4x4 - 5
( ) Saline Locks – 2
( ) Saline 10cc vial/syringe – 2
( ) Saline Bags (250cc & 500 or 1000cc)
1ea
( ) Select 3 Drip Sets – 1
( ) Glucometer – 1
( ) Strips and Lancets – 4 ea
Unit Equipment
Main O2 Cylinder ____________psi
Unit Equipment Continued…
Stretcher # _______________________
Stair chair # _______________________
Combi-Board or Scoop #____________
( ) KED
( ) Sager Splint
( ) Air Splint(Sm, Med, Lg, & Torso)
( ) Air Splint Pump - 1
( ) Portable O2 - 2
( ) Traffic Safety Vest – 3
( ) Reflector Kit - 1
( ) Child seat (optional) – 1
( ) Back boards – 1
( ) Backboard webbing - 1
( ) C-Collars Adult – 4
( ) C-Collars (Pedi and Infant) – 2 ea
( ) Head Rolls – 4
( ) 2inch backboard tape – 1
( ) BP Cuff (Thigh, Lg. Adult, Reg. Adult,
Child, Infant) – 1ea
( ) Stethoscope – 1
( ) BVM (Adult, Child, Infant) - 1 ea
( ) NRB- Adult – 3
( ) NRB – Pedi & Infant – 2 ea
( ) NC –3
( ) Nebulizer – 2
( ) Yankuer/Suction Tubing - 1
( ) Suction Canister – 1 wall
( ) NGT- 18fr – 1
( ) Suction catheters (14fr & 6fr) 1ea
( ) EKG Electrodes - 1 pk
( ) Multi-function Pads Adult - 1
( ) Multi-function Pads Pedi - 1
( ) ECG Paper - 1
( ) OB Kit – 1
( ) Foil Blanket - 1
( ) Burn Sheet - 1
( ) Trauma Dressing – 1
( ) Abdominal Pads - 2
( ) Alcohol Preps – 1 bx
( ) Iodine Preps – 3
( ) Band Aids – 1 bx
( ) Bacitracin – 5 pk
( ) Tape – 1” – 2
( ) Paper Tape - 1
( ) Sterile Water - 1
( ) Rubbing Alcohol - 1
( ) Triangular Bandages - 2
( ) Kerlix –2
( ) Ace Wrap – 1
( ) Commercial Tourniquet - 1
( ) Occlusive Dressing - 2
( ) 4x4 Sterile – 1 bx

GAAA DAILY AMBULANCE CHECK LIST
James Vincent M.D. Page 162
NET Unit Equipment Continued…
( ) 4x4 Non sterile – 1 pk
( ) Cold packs- 5
( ) Hot Packs – 5
( ) Trauma Shears – 1
( ) Ring Cutter - 1
( ) Thermometer -1
( ) Glucometer Strips – 5
( ) Lancets – 5
( ) Ammonia Inhalants – 2
( ) Select 3 – 2
( ) Buretrol set – 1
( ) Dial a Flow-1
( ) Saline 10cc vial/syringe – 5
( ) Saline 50cc bag –1
( ) Saline 250cc bag – 1
( ) Saline – 500 or 1000cc bag –2
( ) IV cath (16, 18, 20, 22, 24) -2 ea
( ) Needle 20ga –2
( ) IO 15ga – 1
( ) Syringe 1cc- 1
( ) Syringe 3 cc – 1
( ) Syringe 10cc – 5
( ) Syringe 30cc –1
( ) Sharps Container Lg – 1
( ) Sharps Container Sm – 1
( ) Biohazard Bags – 2
( ) Trash Bags – 2
( ) N95 Mask – 4
( ) Gowns- 4
( ) Safety Glasses- 3
( ) Gloves (Sm, Med, Lg, X-Lg) -1bx
( ) Hand Sanitizer – 1
( ) Cavicide Wipes/Spray- 1
( ) SLIPP
( ) Peroxide-1 btl
( ) Stuffed animal x2
( ) odor neutralizer x1
MEDICATIONS- KIT ONLY
[ ] Activated Charcoal 50g x 1
[ ] Adenosine 6mg x 6
[ ] Albuterol 2.5mg x 6
[ ] Amiodarone 150mg x 4
[ ] Ancef (Cefazolin) 1g x 2
[ ] Aspirin 81mg - 1 bottle
[ ] Atropine 1mg x 3
[ ] Dextrose 50% 25g x 2
[ ] Diltiazem 25mg x 2
(Keep in cooler if available)
[ ] Diphenhydramine 50mg x 1
[ ] Calcium Gluconate 10ml x 2
MEDICATIONS - KIT ONLY
[ ] Enalaprilat 2.5mg x 1
[ ] Epinephrine (1:1) 1mg x 1
[ ] Epinephrine (1:10) 1mg x 6
[ ] Etomidate 20mg x 2
[ ] Glucagon 1mg – 10 x 2
[ ] Glucose Oral 15g x 2
[ ] Ipratropium 0.5 mg x 3
[ ] Labetalol 40mg x 1
[ ] Lidocaine 2% 100mg x 1
[ ] Magnesium Sulfate 1g x 4
[ ] Narcan 2mg x 1
[ ] Nitroglycerin Spray Btl x 1
[ ] Ondansetron 4mg x 2
[ ] Sodium Bicarb 50mEq x 2
[ ] Solu-Medrol 125mg x 1
[ ] Succinylcholine 200mg x 1
(Keep In cooler if available)
[ ] Thiamine 200mg x 1
[ ] Vecuronium 10mg x 1