GALLSTONES AND PANCREATITIS alex knight. Topics Case Presentation Bile and LFT’s Gallstones ...
34
GALLSTONES AND PANCREATITIS alex knight
-
Upload
lucy-atkinson -
Category
Documents
-
view
225 -
download
0
Transcript of GALLSTONES AND PANCREATITIS alex knight. Topics Case Presentation Bile and LFT’s Gallstones ...
GALLSTONES AND PANCREATITIS
alex knight

Topics
Case Presentation Bile and LFT’s Gallstones Risk Factors Complications +
Presentations

Clinical Scenario
A 45 year old female presents to A&E with an hour long history of severe RUQ pain, and associated vomiting. She has had this in the past few weeks but now its got worse

She has no significant past medical history, is on no regular medication, and has no allergies. She does not smoke, drinks 14 units of alcohol per week and works as a market analyst.

On examination she is febrile at 38.5, tachycardic at 110bpm and her BP is 135/65. On palpation, her abdomen is soft but tender in the RUQ. Murphy’s sign positive

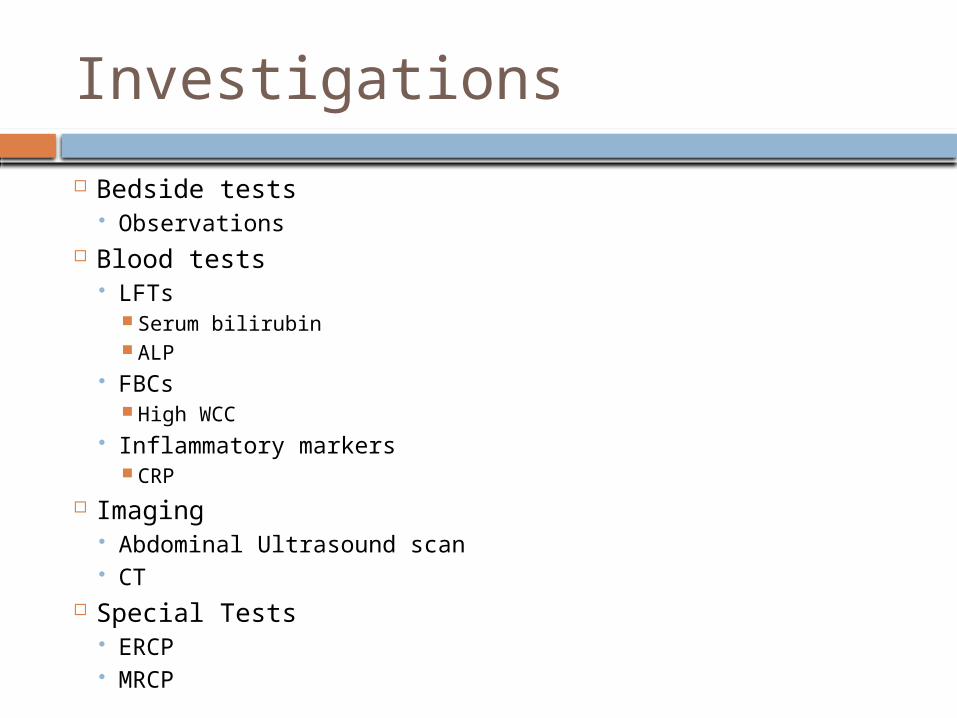
Investigations
Bedside tests Observations
Blood tests LFTs
Serum bilirubin ALP
FBCs High WCC
Inflammatory markers CRP
Imaging Abdominal Ultrasound scan

Management
Conservative NBM IVI fluids Analagesia
Medical Antibiotics?
Surgical Laparascopic +/- open cholecystectomy

Liver Functions
Digestion processing digested food breaking down food and turning it into energy
Homeostasis controlling levels of fats, amino acids and glucose
in the blood storing iron, vitamins and other essential chemicals manufacturing, breaking down and regulating numerous
hormones including sex hormones Immune
combating infections in the body clearing the blood of particles and infections including
bacteria neutralising and destroying drugs and toxins
Blood manufacturing bile Enzymes and proteins - those involved in blood clotting
and tissue repair.

Bile
Water, Electrolytes, Bile acids, Cholesterol, Phospholipids Conjugated Bilirubin

Bile Metabolism

Liver Function Tests and Bile
Albumin General synthetic function + severity of Liver disease
Clotting Also synthetic - Prothrombin time (INR)
Total Bilirubin Processing function
Aminotransferases (AST+ALT) Mitochondrial and cytosolic enzymes – ALT more specific
ALP Enzyme in the cells lining the biliary ducts of the liver
γGlutamyl-transpeptidase (GGT) A rough marker of alcohol consumption if ALP is normal

Gallstones
80% - “Cholesterol” Stones Cholesterol supersaturation of bile
Proportion to bile salts and phospholipids Crystallisation-promoting factors
Bile salt loss in terminal Ileum in Crohn’s Disease Motility of gall bladder
20% - “Pigment” Stones Calcium Bilirubinate
Haemolytic Diseases Cause of recurrent stones post cholecystectomy

Risk Factors
Increasing age Rapid weight loss Drugs – OCP Ileal disease or resection Diabetes


Presentations/Complications
Asymptomatic – Incidental finding In the Gall bladder
Chronic Cholecystitis Biliary Colic Acute Cholecystitis
Empyema of the gallbladder Biliary peritonitis Abcess
Mucocoele Carcinoma of the gallbladder
In the common bile duct Obstructive jaundice Cholangitis Pancreatitis


Chronic Cholecystitis
Abdominal Pain Indigestion Bloating Burping Nausea
Important differentials – peptic ulcer and hiatus hernia

Biliary Colic
Spasm pain when the gallbladder contracts against a stone in the Hartmann’s Pouch
Epigastrium or RUQ Constant, not in waves Extremely severe – sweaty, writhe around
Important Differentials: Perforated peptic ulcer, pancreatitis, ruptured aneurysm

Acute Cholcystitis
Usually progression of biliary colic Increased glandular secretion Distension – possible impeding vascular supply Chemical Inflammation Bacterial Infection Murphy’s sign Patients lie still
Local Peritonitis Important Differentials: Basal Pneumonia,
Intrahepatic Abcess, Perforated peptic ulcer, pancreatitis, ruptured aneurysm

Investigations
Bedside tests Observations
Blood tests LFTs
Serum bilirubin ALP
FBCs High WCC
Inflammatory markers CRP
Imaging Abdominal Ultrasound scan

Management
Conservative NBM IVI fluids Analagesia
Medical Antibiotics?
Surgical Laparascopic +/- open cholecystectomy

Cholecystectomy
Complications General
Bleeding Infection Pneumoperitoneum – vagus nerve – decereased
cardiac output Specific
Bleeding from cystic artery is more difficult to stop haemodynamically
Common Bile Duct Injury or stone movement. Bowel Perforation

Common Bile Duct
RUQ Pain
Fever/Rigors
Jaundice

Triad only present in minority Pain is the most common In comparison to jaundice from
malignancy the Jaundice fluctuates Fever indicates biliary sepsis
Investigations
Bedside tests Observations
Blood tests LFTs
Serum bilirubin ALP
FBCs High WCC
Inflammatory markers CRP
Imaging Abdominal Ultrasound scan CT
Special Tests ERCP MRCP

Management
Conservative NBM IVI fluids Analagesia
Medical Antibiotics
Surgical ERCP

Pancreatitis

Pancreatitis
Mild: Enzymatic spillage Inflammatory cascade activation and Localized oedema. Local exudate may also lead to increased serum
levels of pancreatic enzymes. Moderate:
Increasing local inflammation bleeding, fluid collections and spreading local oedema involving the mesentery and retroperitoneum other organs.
Severe: Necrosis Profound localized bleeding and fluid collections Spread to local structures mesenteric infarction, peritonitis and intra-
abdominal fat ‘saponification’. A persisting accumulation of inflammatory fluid, usually in the
lesser sac, is a pseudocyst, i.e. does not have an epithelial lining.

At admission: Age in years > 55 years White blood cell count > 16x10/l Blood glucose > 11 Serum AST > 200 Serum LDH > 500
Within 48 hours: Calcium < 2 Hematocrit fall > 10% Oxygen PO2 < 8kPa BUN increased by 1.8 or more mmol/L (5 or more mg/dL) after
IV fluid hydration Base deficit (negative base excess) > 4 Sequestration of fluids > 6 L

Ranson Number ITU admission Death
1 (0-2points) 2% 2%
2 (3-4 points) 20% 20%
3 (5-6 points) 50% 40%
4 (7-8 points) 100% 90%

ERCP
Endoscopic Retrograde Cholangio Pancreatography
Diagnostic +/- Therapeutic Stone extraction
Fogarty balloon Basket catheters
Sphincterotomy

ERCP Risks
Bleeding – especially if Sphincterotomy is concerned Infection – cholangitis in the bile duct. Pancreatitis – 5%
Younger patients, Previous post-ERCP pancreatitis Females Procedures that involve cannulation or injection of the pancreatic
duct Patients with sphincter of Oddi dysfunction
Gut perforation Additional risk if a sphincterotomy is performed. D2 is anatomically retroperitoneal, perforations due to
sphincterotomies are also retroperitoneal. Oversedation can result in dangerously low blood pressure,
respiratory depression, nausea, and vomiting. There is also a risk associated with the contrast dye in patients
who are allergic to compounds containing iodine.

MRCP
Magnetic resonance cholangiopancreatography (MRCP) is a medical imaging technique that uses magnetic resonance imaging to visualise the biliary and pancreatic ducts in a non-invasive manner

3 things I want you to take away
123
Complications/Presentations
Investigations
Ranson’s Criteria
![[PPT]Academy of Medicine Farid Jalali - University of … · Web view47 year-old female with recent mild alcohol intake and no history of prior gallstones or acute pancreatitis presents](https://static.fdocuments.in/doc/165x107/5acf74047f8b9a1d328d07c0/pptacademy-of-medicine-farid-jalali-university-of-view47-year-old-female.jpg)