Gait analysis may help to distinguish hereditary spastic paraplegia from cerebral palsy
6
Gait analysis may help to distinguish hereditary spastic paraplegia from cerebral palsy Sebastian I. Wolf a, *, Frank Braatz a , Dimitrios Metaxiotis a,b , Petra Armbrust a , Thomas Dreher a , Leonhard Do ¨ derlein a,c , Ralf Mikut d a Department of Orthopaedic Surgery, University of Heidelberg, Schlierbacher Landstr. 200a, 69118 Heidelberg, Germany b Orthopaedic Department, Papageorgiou Hospital, Thessaloniki, Greece c Behandlungszentrum Aschau, Germany d Institute for Applied Computer Science, Karlsruhe Institute of Technology (KIT), Germany 1. Introduction Hereditary spastic paraplegia (HSP) designates a heterogeneous group of genetic disorders of which not all can yet be diagnosed by routine genetic testing [1]. In its ‘‘pure’’ form, HSP leads to progressive spasticity in the lower limbs due to pyramidal tract degeneration [2]. HSP is classified as complex when complicated by other neurological signs such as ataxia, mental retardation, dementia, extrapyramidal signs, visual dysfunction, or epilepsy [3]. Pure HSP represents around 70% of the cases and is typically inherited in an autosomal dominant manner [3,4]. In most cases, the phenotype includes slowly progressive spasticity in the lower limbs, resulting in gait deficiencies and loss of mobility starting in the second decade after the onset of symptoms. Clinically, the onset of this type of HSP can be from childhood through to late adult life, whereas more than half of mutation carriers do not develop symptoms until after the age of 30 years [5]. Although the clinical findings may vary, two groups of clinical types have been described based on the age at presentation: type I before and type II after 35 years of age [6]. With an onset in the first few years of life, combined with delayed motor milestones, the diagnosis is more suggestive of cerebral palsy (CP), particularly if the clinical picture is relatively static [5]. However, due to the progressive nature of the clinical symptoms in HSP, these patients are typically treated differently to patients with CP. Since genetic testing is not always possible and both the clinical status and the patients’ history may not always be sufficient to establish the diagnosis, a detailed analysis of the gait pattern may help in the decision for an appropriate treatment. Unlike CP, where gait has been studied in detail using 3D motion capture, only few studies have objectively described gait function in HSP. Braschinsky et al. [7] reported on reduced walking speed in 46 patients set in the context of reduced active hip flexion and abduction ROM as well as reduced ankle dorsiflexion ROM, which were determined clinically. Earlier, the group of Klebe found a reduced ROM in knee flexion and reduced walking speed due to reduced stride length and cadence along with an increase in step width in 22 adult patients (age 35–61 years) when compared to Gait & Posture 33 (2011) 556–561 ARTICLE INFO Article history: Received 27 July 2010 Received in revised form 13 January 2011 Accepted 15 January 2011 Keywords: Hereditary spastic paraplegia Gait analysis Automated methods Classification Feature extraction Pattern recognition ABSTRACT Hereditary spastic paraplegia (HSP) designates a group of genetic disorders typically leading to spasticity in the lower limbs and consequently to gait disorders. Although the symptoms are similar to those of cerebral palsy (CP), the correct diagnosis is important for treatment recommendations as one condition is progressive in nature whereas the other is not. Due to the heterogeneity of HSP, genetic testing is complex and in some genetic forms still not possible. The aim of this study was, therefore, to investigate if instrumented 3D-gait analysis could help distinguish between these two conditions. The gait pattern of 29 patients with HSP was compared with that of 29 patients with CP who were matched in age, sex, and the extent of gait disturbance and also to 29 typically developing subjects for reference. More than 3000 gait parameters were evaluated for their relevance to classify patients into diagnostic groups. Cluster analysis revealed that these gait features may classify only subgroups of symptoms as the gait pattern is very heterogeneous within each diagnosis group. However, prolonged hip extension, knee extension, and ankle plantar flexion were identified as indicators for HSP. In addition, large trunk tilt velocities appear unique in some cases of HSP. These indicators in gait pattern may contribute in establishing the diagnosis of HSP, which is important in predicting outcome when planning surgical treatment for functional improvements in these patients. ß 2011 Elsevier B.V. All rights reserved. * Corresponding author. Tel.: +49 6221 966724. E-mail address: [email protected] (S.I. Wolf). Contents lists available at ScienceDirect Gait & Posture journal homepage: www.elsevier.com/locate/gaitpost 0966-6362/$ – see front matter ß 2011 Elsevier B.V. All rights reserved. doi:10.1016/j.gaitpost.2011.01.009
-
Upload
rufaida-hussain -
Category
Documents
-
view
213 -
download
1
description
Hereditary spastic paraplegia (HSP) designates a group of genetic disorders typically leading to spasticityin the lower limbs and consequently to gait disorders. Although the symptoms are similar to those ofcerebral palsy (CP), the correct diagnosis is important for treatment recommendations as one conditionis progressive in nature whereas the other is not. Due to the heterogeneity of HSP, genetic testing iscomplex and in some genetic forms still not possible. The aim of this study was, therefore, to investigateif instrumented 3D-gait analysis could help distinguish between these two conditions.The gait pattern of 29 patients with HSP was compared with that of 29 patients with CP who werematched in age, sex, and the extent of gait disturbance and also to 29 typically developing subjects forreference. More than 3000 gait parameters were evaluated for their relevance to classify patients intodiagnostic groups. Cluster analysis revealed that these gait features may classify only subgroups ofsymptoms as the gait pattern is very heterogeneous within each diagnosis group. However, prolongedhip extension, knee extension, and ankle plantar flexion were identified as indicators forHSP. In addition,large trunk tilt velocities appear unique in some cases of HSP. These indicators in gait pattern maycontribute in establishing the diagnosis of HSP, which is important inpredicting outcomewhen planningsurgical treatment for functional improvements in these patients
Transcript of Gait analysis may help to distinguish hereditary spastic paraplegia from cerebral palsy
-
ri
0a
y
Gait & Posture 33 (2011) 556561
Contents lists available at ScienceDirect
Gait & P
l s1. Introduction
Hereditary spastic paraplegia (HSP) designates a heterogeneousgroup of genetic disorders of which not all can yet be diagnosed byroutine genetic testing [1]. In its pure form, HSP leads toprogressive spasticity in the lower limbs due to pyramidal tractdegeneration [2]. HSP is classied as complex when complicatedby other neurological signs such as ataxia, mental retardation,dementia, extrapyramidal signs, visual dysfunction, or epilepsy [3].Pure HSP represents around 70% of the cases and is typicallyinherited in an autosomal dominant manner [3,4]. In most cases,the phenotype includes slowly progressive spasticity in the lowerlimbs, resulting in gait deciencies and loss of mobility starting inthe second decade after the onset of symptoms. Clinically, theonset of this type of HSP can be from childhood through to lateadult life, whereas more than half of mutation carriers do notdevelop symptoms until after the age of 30 years [5]. Although the
clinical ndings may vary, two groups of clinical types have beendescribed based on the age at presentation: type I before and type IIafter 35 years of age [6]. With an onset in the rst few years of life,combined with delayed motor milestones, the diagnosis is moresuggestive of cerebral palsy (CP), particularly if the clinical pictureis relatively static [5]. However, due to the progressive nature ofthe clinical symptoms in HSP, these patients are typically treateddifferently to patients with CP. Since genetic testing is not alwayspossible and both the clinical status and the patients history maynot always be sufcient to establish the diagnosis, a detailedanalysis of the gait pattern may help in the decision for anappropriate treatment.
Unlike CP, where gait has been studied in detail using 3Dmotion capture, only few studies have objectively described gaitfunction in HSP. Braschinsky et al. [7] reported on reduced walkingspeed in 46 patients set in the context of reduced active hip exionand abduction ROM as well as reduced ankle dorsiexion ROM,whichwere determined clinically. Earlier, the group of Klebe founda reduced ROM in knee exion and reduced walking speed due toreduced stride length and cadence along with an increase in stepwidth in 22 adult patients (age 3561 years) when compared to
A R T I C L E I N F O
Article history:
Received 27 July 2010
Received in revised form 13 January 2011
Accepted 15 January 2011
Keywords:
Hereditary spastic paraplegia
Gait analysis
Automated methods
Classication
Feature extraction
Pattern recognition
A B S T R A C T
Hereditary spastic paraplegia (HSP) designates a group of genetic disorders typically leading to spasticity
in the lower limbs and consequently to gait disorders. Although the symptoms are similar to those of
cerebral palsy (CP), the correct diagnosis is important for treatment recommendations as one condition
is progressive in nature whereas the other is not. Due to the heterogeneity of HSP, genetic testing is
complex and in some genetic forms still not possible. The aim of this study was, therefore, to investigate
if instrumented 3D-gait analysis could help distinguish between these two conditions.
The gait pattern of 29 patients with HSP was compared with that of 29 patients with CP who were
matched in age, sex, and the extent of gait disturbance and also to 29 typically developing subjects for
reference. More than 3000 gait parameters were evaluated for their relevance to classify patients into
diagnostic groups. Cluster analysis revealed that these gait features may classify only subgroups of
symptoms as the gait pattern is very heterogeneous within each diagnosis group. However, prolonged
hip extension, knee extension, and ankle plantar exionwere identied as indicators for HSP. In addition,
large trunk tilt velocities appear unique in some cases of HSP. These indicators in gait pattern may
contribute in establishing the diagnosis of HSP, which is important in predicting outcomewhen planning
surgical treatment for functional improvements in these patients.
2011 Elsevier B.V. All rights reserved.
* Corresponding author. Tel.: +49 6221 966724.
E-mail address: [email protected] (S.I. Wolf).
0966-6362/$ see front matter 2011 Elsevier B.V. All rights reserved.doi:10.1016/j.gaitpost.2011.01.009Gait analysis may help to distinguish hecerebral palsy
Sebastian I. Wolf a,*, Frank Braatz a, Dimitrios MetaxLeonhard Doderlein a,c, Ralf Mikut d
aDepartment of Orthopaedic Surgery, University of Heidelberg, Schlierbacher Landstr. 20bOrthopaedic Department, Papageorgiou Hospital, Thessaloniki, GreececBehandlungszentrum Aschau, Germanyd Institute for Applied Computer Science, Karlsruhe Institute of Technology (KIT), German
journal homepage: www.eeditary spastic paraplegia from
otis a,b, Petra Armbrust a, Thomas Dreher a,
, 69118 Heidelberg, Germany
osture
evier .com/ locate /ga i tpost
-
healthy controls [8]. The most detailed ndings so far werereported in 15 children with HSP (aged 615 years) by comparingtheir gait to that of 40 patients with CP and 20 healthy controlsubjects with the aim to quantitatively assess differences in gaitbetween the two conditions [9]. Temporospatial and kinematicparameters were found to be similar in the two patient groups butknee exion at initial contact was particularly increased whencompared to the CP group. Both groups tended to hyperextend theknee in mid-stance, however, a longer duration of hyperextensionwas observed in patients with HSP.
These rst objective ndings on gait characteristics in HSP andthe clinical observation that some patients show a gait patternatypical for CP suggest that objective gait observation may help indistinguishing the two conditions. Therefore, the aim of thisretrospective study was to identify pathology-related gait patternsor characteristic features irrespective of the patient history. Forthis, a systematic approach based on both gait feature computationas described in [10] and on the use cluster analysis was employed.Instrumented gait analysis could then be used both for a betterdiagnostic work-up and for determining the best treatmentoptions for the patient.
2. Patients
Thirty-ve patients with clinical symptoms of HSP were seenbetween 1996 and 2008 at the outpatient clinics of our hospital.Instrumented 3D-clinical gait analysis (CGA) based on a conven-tional gait model [11] was conducted to establish furthertreatment recommendations. Of these patients, 29 (aged 563years, 8f/21m) were included in the study since (a) gait data were
classied as GMFCS 1, in another 18 patients as GMFCS 2, and inthree patients as GMFCS 3. On their rst visit, 24 subjects had notpreviously had any operations whereas ve had received soft-tissue operations (calf muscles), among them two who alsoreceived proximal procedures (adductors, hamstrings, rectusfemoris). More details about the subjects are given in Table 1.
Further, a group of 385 patients diagnosedwith diplegic type CPwho presented for their rst visit in our hospital and who had alsoundergone CGA were scanned for the same inclusion criteria as inthe HSP group. Sorted by age and sex, best matches to the HSPgroup were manually picked in a blinded manner only by theinformation on age, sex, and Gillette Gait Index (GGI) [13]. In thisgroup seven cases were classied as GMFCS 1, in another 16patients as GMFCS 2, and in six patients as GMFCS 3. It turned out(by accident) that, similarly to the HSP group, ve of these 29patients had also undergone soft-tissue operations (calf muscles),among them three who had also had proximal procedures,including one case of bony correction.
Hence the two groups showed very similar clinical backgroundsbut with different diagnoses. For reference and testing reasons, athird group of typically developing subjects (NORM) was selectedretrospectively out of the gait data base, aiming for bestmatches inage and sex.
3. Methods
For the instrumented gait analyses a Vicon 370motion capture systemwas used
during the years 19962001 andwas then replaced by a Vicon 612 system applying
a conventional gait model [11]. For each patient, the data of at least ve strides of
different trials were averaged. To assess gait patterns, a previously developed
methodological modular framework was applied [10]. This framework formalizes
pe
S.I. Wolf et al. / Gait & Posture 33 (2011) 556561 557reasonably reliable, i.e., data from ve or more trials weremeasured and averaged, (b) video documentation was available,and (c) the diagnosis of HSPwas conrmed by either a documentedfamily history or by late age of onset (for HSP type II cases). Thegross motor function score (GMFCS, [12]) in eight cases was
Table 1Subject characteristics.
Triple HSP group
Sex Age GGI Walking aid Previous surgeries HSP ty
1 m 5.6 72 No No I
2 f 6.2 132 No No I
3 m 8.2 131 No No I
4 m 8.7 360 No No I
5 m 9.0 305 No No I
6 f 9.1 277 No No I
7 m 9.5 1511 No No I
8 m 9.9 45 No No I
9 f 11.9 606 No No I
10 f 12.1 271 No Yes I
11 m 14.0 100 No No I
12 m 14.2 118 No No I
13 m 14.5 149 No No I
14 m 15.3 545 No No I
15 m 15.7 994 No No I
16 m 16.4 398 No Yes I
17 m 17.6 299 No No I
18 m 19.9 1135 Yes No I
19 m 21.2 235 No No I
20 f 29.0 182 No Yes I
21 f 34.9 148 No No I
22 m 36.4 408 No No I
23 m 36.6 220 No No II
24 m 37.5 169 No Yes I
25 m 37.7 260 No No II
26 m 38.7 326 No Yes I
27 m 46.7 505 Yes No II
28 f 52.3 990 Yes No II
29 f 63.5 180 No No IIthe processing steps of data selection, gait parameter calculation, and evaluation, as
well as classication according to the clinical problem. For these steps, several
mathematicalmethodswere selected and the validity of the approachwas tested by
applying it to the clinical problem of Botulinum Toxin-A treatment for spastic
equinus [10]. The methodology is only briey described here. An extended
summary can be found in the electronic appendix. Original time series, i.e., 3D
CP group Reference
Sex Age GGI Walking aid Previous surgeries Sex Age
m 4.8 89 No No m 5.0
f 6.0 111 No No f 5.9
m 7.7 98 No No m 7.9
m 8.7 303 No No m 8.7
m 9.3 304 No No m 9.1
f 8.8 266 No No f 9.4
m 9.6 1584 No No m 9.1
m 10.3 137 No No m 10.2
f 11.7 581 No No f 11.4
f 11.7 279 No No f 11.7
m 13.3 128 No No m 11.7
m 14.4 189 No Yes m 12.7
m 14.4 235 No No m 13.5
m 15.5 526 No No m 15.5
m 16.0 1101 No No m 15.7
m 15.8 419 No No m 23.9
m 17.7 233 No No m 24.7
m 22.6 853 Yes No m 25.8
m 21.5 240 No No m 27.2
f 29.6 252 No No f 29.3
f 32.1 228 No No f 33.0
m 35.3 528 No No m 35.6
m 35.1 244 No Yes m 35.7
m 38.0 122 No Yes m 37.8
m 38.3 543 Yes Yes m 41.4
m 46.1 423 No No m 43.2
m 55.3 415 No No m 51.0
f 49.1 626 Yes Yes f 50.4
f 46.2 186 Yes No f 51.7
-
Table 2List of the 10most relevant gait parameters to distinguish the gait pattern of patients with HSP from the NORM using mutual information. TDP, time distance parameter; Str,
stride; St, stance; Sw, swing; MSw, mid swing.
Rank Value Time
series
Gait
phase
NORM HSP CP Relevance
NORMHSP
p-Value
NORMHSP
Relevance
NORMCP
p-Value
NORMCP
1 ROM Knee FlexExt Sw 54.2 (4.5) 26.1 (11.0) 23.4 (10.1) 0.587 1.89E19 0.628 2.72E202 ROM PelvicTilt Str 2.8 (0.8) 8.9 (3.8) 9.3 (3.4) 0.580 7.70E16 0.745 1.33E193 TDP Double Support 20.7 (2.8) 31.6 (12.1) 33.5 (10.8) 0.519 1.19E13 0.561 1.98E174 ROM Knee FlexExt MSw 29.4 (3.8) 10.0 (5.5) 8.0 (5.0) 0.485 2.58E20 0.540 1.71E205 ROM PelvicTilt Vel Str 0.4 (0.1) 1.2 (0.6) 1.1 (0.4) 0.476 3.49E14 0.524 7.64E196 ROM Knee FlexExt Str 55.5 (4.2) 38.4 (13.7) 34.9 (13.2) 0.456 3.65E11 0.500 1.84E147 MIN Knee FlexExt Sw 3.9 (3.4) 21.4 (13.5) 27.7 (11.6) 0.454 2.36E15 0.603 8.39E208 ROM PelvicTilt St 2.5 (0.8) 8.1 (3.7) 8.5 (3.2) 0.454 5.46E15 0.606 6.18E209 TDP Walking Speed 1.3 (0.2) 0.9 (0.3) 0.8 (0.3) 0.453 4.78E13 0.560 7.91E1810 ROM Knee FlexExt Vel Str 6.6 (0.7) 4.1 (1.4) 3.8 (1.5) 0.445 3.90E16 0.476 3.33E17
S.I. Wolf et al. / Gait & Posture 33 (2011) 556561558joint angles of pelvis, hip, knee, and ankle obtained by conventional, instrumented
3D gait analysis [11] and three derived time series, i.e., joint angle velocities, norm
distances, and norm distances for joint angle velocities to calculate single
features, i.e., scalar quantities of gait parameters. These parameters included range
of motion, mean, maximum, and minimum values of time series as well as the
temporal position of maximum and minimum values in the gait cycle or in
functional sub phases as dened by Perry [14]. In total, 3187 gait parameters,
including 19 additional scalar time distance parameters such as cadence and
walking speed, are generated. The feature set is very similar to [10], but without the
features from the stride-to-stride kinematic variance and with nine additional
time-distance parameters. To cover prolonged knee extension, the most successful
feature found in [9], the duration in the gait cycle with values smaller than zero (in
this case knee hyperextension) was systematically added as an additional
parameter for all joint angle and joint angle velocity time series. Driven by the
subjective clinical impression that trunk movement in some HSP patients appears
unique and distinct, 3D-data on trunk movements available in 18 (out of 29)
patients with HSP and 25 (out of 29) patients with CPwere also analyzed via single-
feature computation in the same manner as described above.
The features were then ranked for relevance between zero (unable to separate
the different groups) and one (unique assignment) of the patient groups in question
using mutual information and a priori relevance. In other words, we assessed the
extent to which each parameter could suitably distinguish between gait patterns of
HSP and CP (and physiologic gait). Finally, when also taking cross correlations
between parameters into account by subsequently excluding variables when they
are less relevant than another highly correlated one, a ranking list with a set of
largely independent gait parameters is produced, characterizing the given clinical
(classication) problem. In this contribution, these lists were produced pairwise for
the groups HSP, CP, and NORM. Statistical signicance with a signicance level of
p < 0.05 was determined for each parameter using the non-parametric Wilcoxon
rank-sum test and Bonferroni correction for multiple testing.
Furthermore, unsupervised cluster analysis methodswere applied to account for
heterogeneous gait patterns within each patient group. Here, a standard Fuzzy C-
Means algorithmwith raw data-based time series, a normalization of time series to
mean values of zero and a standard deviation of one, a fuzzier m = 1, and a xed
number of clusters C = 4, 5, and 6 were chosen [15]. Sagittal plane kinematics
including joint angles and joint angle velocities of pelvis, hip, knee, and ankle was
used to classify the sets of 4, 5, and 6 clusters across patient groups. The analysiswas
done with the open-source Matlab toolbox Gait-CAD [19,20].
4. Results
In Table 2, a ranking list is given for the 10 most relevant gaitparameters classifying the group of patients with HSP from age-
matched reference normal subjects (NORM), corresponding values
Table 3List of the 10 most relevant gait parameters distinguishing the gait patterns of patient
duration in which the parameter is smaller then 0; ROM, range of motion. Gait phases
Rank Value Time series Gait phase NORM
1 TDP Stride Time 1.0 (0.1)
2 TDP Step Time 0.6 (0.1)
3 Mean PelvicTilt Str 11.1 (4.3)
4 T
-
0 50 100
0
20
40Crouch
Pe
lvic
Tilt
0 50 100-20
020
4060
Hip
Fle
xE
xt
0
2040
60
80
Kn
ee
Fle
xE
xt
0 50 100
0
20
40Recurvatum
0 50 100-20
020
4060
0
2040
60
80
0 5
0
20
40Stiff
0 5-20
020
4060
5
0
2040
60
80
5
it cy
ound
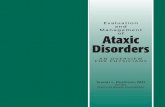
S.I. Wolf et al. / Gait & Posture 33 (2011) 556561 559abnormalities in CP and which were therefore used for naming theclusters. Type 1 is characterized by excessive knee exionthroughout the gait cycle, known as crouch gait. Type 2 showsprominent knee extension or hyperextension in mid-stance(recurvatum gait) whereas type 3 shows insufcient kneeextension with limited knee range of motion (stiff knee gait).
0 50 100
0 50 100
-80-60-40-20
020
Do
rsiP
lan
Fle
x
Gait cycle [%]
0 50 100
0 50 100
-80-60-40-20
020
Gait cycle [%]
0
0
-80-60-40-20
020
Ga
Fig. 1. Clusters of sagittal gait kinematics fFinally, type 4 (jump knee gait) is characterized by increased kneeexion at loading response and almost normal knee function laterin the gait cycle as in type 5 (norm like gait). It should be stressedthat the results shown in Fig. 1 were received independently of anyclinical knowledge by taking all sagittal plane kinematics intoaccount. Interestingly, the classication did not change/improvesignicantly when using only knee exion or ankle kinematics forclassication (not shown).
The relative distribution of each diagnosis group into each gaitpattern cluster (Fig. 2) was unique only for the reference groupwith a perfect classication for normal (58/58). In pathological
Norm like Norm like
Norm like
CrouchCrouch
Recurvatum
Stiff Knee
Stiff Knee
Jump KneeJump Knee
0
5
10
15
20
25
30
35
40
45
50
55
60
NormCPHSP
num
ber
of le
gs
Fig. 2. Relative distribution of each patient group into gait pattern clusters.conditions, cases contributed to any of the ve gait patternsregardless of the type of pathology (HSP or CP). However, thecontribution of each pathological condition to the norm-likecluster was very small (3 and 4 of 58, respectively) and comprisedthe mildest cases. Hence, HSP showed in principle the samephenotypes as CP, the only noticeable difference being that only
0 100
Knee
0 100
0 100
0 100
cle [%]
0 50 100
0
20
40Jump Knee
0 50 100-20
020
4060
0 50 100
0
2040
60
80
0 50 100
-80-60-40-20
020
Gait cycle [%]
0 50 100
0
20
40Norm like
0 50 100-20
020
4060
0 50 100
0
2040
60
80
0 50 100
-80-60-40-20
020
Gait cycle [%]
across all subjects (HSP, CP, and NORM).one leg of the CP group shows a recurvatum knee as compared to14 legs in the HSP group.
The analysis of 3D-data of the trunk revealed that highermaximum trunk tilt velocities found in patients with HSP mostsignicantly (p = 2.3E005) differed between diagnosis groupsHSP and CP.
5. Discussion
HSP is associated with progressive impairment of gait;however, information on functional ability and especially the gaitpattern in these patients is still limited and mainly derived fromsubjective observational gait analysis. Nevertheless, a number ofresearchers have attempted to describe the gait problems inpatients with HSP [7,17]. The largest cross-sectional study wasperformed by Erichsen et al. [18], who reported on 194 subjectswith HSP in southeast Norway. Among these, 31% were classiedas walkers with mild symptoms, 32% as walkers but unable to run,25% as walkers restricted to walking aids, and 11% as wheel-chair-dependent. Unfortunately, none of the studies provide anyinformation about specic gait deviations.
To our knowledge the only two studies that examined gaitpatterns objectively are the ones by Klebe et al. [8], comparing 22adult patients with healthy controls, and Cimolin et al. [9], whocompared 15 children with HSP to a group of 40 patients with CPand to 20 healthy controls. The latter study reports on prolongedknee hyperextension in stance, a gait feature also found to besignicantly different between diagnosis groups in our patients(p < 0.002 without Bonferroni correction; feature not shown inTable 3 since it is ranked 32with relevance 0.047).More prominent
-
S.I. Wolf et al. / Gait & Posture 33 (2011) 556561560and relevant, however, are the differences with respect toprolonged times of hip extension and ankle plantar exion (comp.Table 3 features ranked 46). Cimolin and co-workers speculatedthat a motor strategy different to that in CP, a compensatory kneestabilization strategy, was responsible for prolonged kneehyperextension in HSP. Knee hyperextension would not beaccompanied by ankle plantar exion and hence without thepresence of a plantar exion/knee extension couple. In contrast, wefound knee hyperextension linked to plantar exion in HSP (comp.Fig. 1; second column recurvatum).We suspect that this linkwasoverlooked when only group mean averages were examined andthus the presence of functional phenotypeswithin the pathologicalcondition was neglected. Instead, the relative distribution of eachpatient group into gait pattern clusters with only one out of 58 legsclassied as recurvatum (comp. Fig. 2) reects the clinical ndingthat patients with CP who have not previously received surgicaltreatment are unlikely to show knee hyperextension. It has to benoted that some HSP patients in this recurvatum cluster did notshow true knee hyperextension but a rather increased kneeextension to be described by almost full extension in stance incombination with reduced knee exion in swing. Hence, the merending of knee hyperextension or increased knee extension assuch in patients with no history of surgical treatment wouldindicate a high probability of HSP. The cause for this nding in HSPmay primarily represent weakness rather than spasticity. This is incontrast to (typically post-surgical) patients with CP who showdominance of quadriceps spasticity rather than weakness. Thisreasoning is corroborated by the nding of extended time of hipextension (comp. Table 3, feature ranked 5). The predominance ofeither weakness or spasticity may indeed relate to the differentcause of the twopathologies, i.e., the lesion of the immature centralnervous system in CP and the group of genetic conditions leadingto problems with axonal transport (HSP). However, since anyrigorous evidence about the interdependency of spasticity andweakness is still missing this reasoning remains speculative. Moredetailed investigations of other rare diseases with similarfunctional ndings such as the Segawa-Syndrome (idiopathicdystony) or the Curschmann-Steinert-Syndrome (myotonic dys-trophy) may help in elucidating the relation of weakness andspasticity with the primary cause.
Furthermore, we tried to assess the subjective impression of aunique pelvistrunk coordination pattern in HSP observed onvideo. By adding trunk motion to the formalized algorithmdeveloped for classifying lower limb kinematics [10], we foundsignicantly increased peak trunk tilt velocities in HSP ascompared to CP. Four patients with HSP showed a noticeable,quick forward and backward movement of the trunk at the end ofloading response and at stance-swing transition which was notpresent to this extent in any of our patients with CP. There mightalso be a link between this nding in trunk motion and prolongedknee extension in stance. However, this was not examined infurther statistical detail because it only applied to a minority ofsubjects within this group and because trunk data were notavailable for all of them.
The cluster analysis revealed that the gait pattern alone couldnot fully classify the patients into diagnosis groups as the gaitpattern was heterogeneous within each diagnosis group.However, for subgroups of symptoms, namely for recurvatumgait, specic characteristics can be found which indicate thepresence of HSP. These are prolonged hip extension in stance,knee hyperextension, and ankle plantar exion in the lower limbfollowed by large trunk tilt velocities in loading response andstance/swing transition. Clinically these may be importantndings when other diagnostic factors, i.e., familial historyand genetic testing are not reassuring enough for the diagnosisof HSP.As HSP is a rare group of diseases, sample sizes are typicallysmall. With a sample size of 29 subjects, we are far from claimingto present a complete clinical picture but with an age range from5 to 63 years a large variety of subject characteristicswas denitelycovered. Effort has been spent in generating adequate samples forcomparing HSP to CP and to physiologic gait. By scanning the gaitdatabase for diplegic patients with CP with the same inclusioncriteria except for diagnosis, we expect to have an adequatecomparison.We tried tominimize the number of limiting factors inthis comparison, such as inhomogeneity between groups due todifferent functional levels, age, sex, and previous surgeries, bypicking matched pairs. None of these factors differed signicantlybetween the groups. However, the inclusion of a wide age rangeand a wide spectrum of involvement in each group in what arealready heterogeneous conditions may have introduced anadditional and possibly even articial challenge in differentiatingbetween these groups. The comparison of more homogenoussubgroups would be possible but with limited statistical powerand the risk of additional bias effects. Namely, age and body heightmight be inuencing factors as with increasing age and bodyheight weakness becomes an increasing disadvantage for thebiomechanics of walking.
6. Conclusion
The clinical resemblance of HSP and CP is reected on the strongsimilarity of gait patterns found by using a rigorous CGA approachin the largest sample of HSP in the literature. The gait pattern alonecannot fully classify the patients into diagnosis groups as eachgroup is heterogeneous. However, prolonged hip extension instance, knee hyperextension, and ankle plantar exion as well aslarge trunk tilt velocities in loading response and stance/swingtransition are indicative of HSP. These diagnostic indicators maywell be clinically relevantwhen surgical treatment is in question asHSP is progressive in nature whereas CP is not. A further studymonitoring the factor of time both with and without orthopaedicintervention in this patient group is underway.
Conict of interest statement
None of the authors had any nancial or personal relationshipswith other people or organizations that could inappropriately biastheir work.
Appendix A. Supplementary data
Supplementary data associatedwith this article can be found, inthe online version, at doi:10.1016/j.gaitpost.2011.01.009.
References
[1] Fink JK. Hereditary spastic paraplegia. Curr Neurol Neurosci Rep2006;6(1):6576.
[2] Depienne C, Stevanin G, Brice A, Durr A. Hereditary spastic paraplegias: anupdate. Curr Opin Neurol 2007;20(6):67480.
[3] Harding AE. Classication of the hereditary ataxias and paraplegias. Lancet1983;1(8334):11515.
[4] Fink JK. Advances in the hereditary spastic paraplegias. Exp Neurol2003;184(Suppl. 1):S10610.
[5] Salinas S, Proukakis C, Crosby A, Warner TT. Hereditary spastic paraplegia:clinical features and pathogenetic mechanisms. Lancet Neurol2008;7(12):112738.
[6] Harding AE. Hereditary pure spastic paraplegia: a clinical and genetic studyof 22 families. J Neurol Neurosurg Psychiatry 1981;44(10):87183.
[7] Braschinsky M, Parts K, Maamagi H, Gross-Paju K, Haldre S. Functionalassessment of lower extremities in hereditary spastic paraplegia. Arch PhysMed Rehabil 2009;90(11):188790.
[8] Klebe S, Stolze H, Kopper F, Lorenz D, Wenzelburger R, Volkmann J, et al. Gaitanalysis of sporadic and hereditary spastic paraplegia. J Neurol2004;251(5):5718.
-
[9] Cimolin V, Piccinini L, DAngelo MG, Turconi AC, Berti M, Crivellini M, et al. Arepatients with hereditary spastic paraplegia different from patients with spas-tic diplegia during walking? Gait evaluation using 3D gait analysis. FunctNeurol 2007;22(1):238.
[10] Wolf S, Loose T, Schablowski M, Doderlein L, Rupp R, Gerner HJ, et al.Automated feature assessment in instrumented gait analysis. Gait Posture2006;23(3):3318.
[11] KadabaMP, Ramakrishnan HK,WoottenME. Measurement of lower extremitykinematics during level walking. J Orthop Res 1990;8(3):38392.
[12] Palisano RJ, Hanna SE, Rosenbaum PL, Russell DJ, Walter SD, Wood EP, et al.Validation of a model of gross motor function for children with cerebral palsy.Phys Ther 2000;80(10):97485.
[13] Schutte LM, Narayanan U, Stout JL, Selber P, Gage JR, Schwartz MH. An indexfor quantifying deviations from normal gait. Gait Posture 2000;11(1):2531.
[14] Perry JP. Gait analysis: normal and pathological function. Thorofare, NJ:Slack; 1992 .
[15] Rozumalski A, Schwartz MH. Crouch gait patterns dened using k-meanscluster analysis are related to underlying clinical pathology. Gait Posture2009;30(2):15560.
[16] Sutherland DH, Davids JR. Common gait abnormalities of the knee in cerebralpalsy. Clin Orthop Relat Res 1993;288:13947.
[17] von Fellenberg J, Paternotte C, Prudhomme JF, Weissenbach J, Hazan J,Burgunder JM. Klinische und molekulargenetische Analyse bei vier schweit-zerischen Familien mit der reinen Form der hereditaren spastischen Spinal-paralyse. Schweiz Med Wochenschr 1998;128(26):104350.
[18] Erichsen AK, Koht J, Stray-Pedersen A, Abdelnoor M, Tallaksen CM. Prevalenceof hereditary ataxia and spastic paraplegia in southeast Norway: a population-based study. Brain 2009;132(Pt 6):157788.
[19] Mikut R, Burmeister O, Braun S, Reischl M. The open source Matlab toolboxGait-CAD and its application to bioelectric signal processing. In: Proceedings ofDGBMT-Workshop Biosignal Analysis, Potsdam; 2008. p. 10911.
[20] http://sourceforge.net/projects/gait-cad/.
S.I. Wolf et al. / Gait & Posture 33 (2011) 556561 561
Gait analysis may help to distinguish hereditary spastic paraplegia from cerebral palsyIntroductionPatientsMethodsResultsDiscussionConclusionConflict of interest statementSupplementary dataReferences