Future directions of ARVs A Pharmacology Perspective...
24
Saye Khoo University of Liverpool, UK Future directions of ARVs A Pharmacology Perspective Declaration of Interests www .hiv-druginteractions.org & www .hep-druginteractions.org Receives sponsorship from AbbVie, Merck, BMS, Janssen, Gilead, ViiV. Editorial content remains independent. Research funding, travel grants, speakers bureau from Gilead, AbbVie, ViiV, Merck, Janssen See https ://www.liverpool.ac.uk/translational-medicine/staff/saye-khoo/external-engagement/
Transcript of Future directions of ARVs A Pharmacology Perspective...
Saye Khoo
University of Liverpool, UK
Future directions of ARVs
A Pharmacology Perspective
Declaration of Interestswww.hiv-druginteractions.org & www.hep-druginteractions.org
Receives sponsorship from AbbVie, Merck, BMS, Janssen, Gilead, ViiV.Editorial content remains independent.
Research funding, travel grants, speakers bureau from Gilead, AbbVie, ViiV, Merck, Janssen
See https://www.liverpool.ac.uk/translational-medicine/staff/saye-khoo/external-engagement/

A Pharmacology Perspective
Smit et al. Lancet ID 2015;15:810-18
▪ >= 50% patients aged over 50
▪ Multiple co-morbidities the norm
▪ Geriatric syndromes

A Pharmacology Perspective
• Liver• Renal• Bone• Metabolic syndrome• Other
Toxicities
• Cardio/cerebrovascular• T2 Diabetes• NAFLD• CKD• Malignancy• Neuropsychiatric
Multiple Morbidities
• Driven by polypharmacy• Not ‘designed out’
DDIs
• Better drugs & formulations• Fewer pills (2DRs? 1DR ??)• LA oral & parenteral• Adjuvant therapies
Burden of Treatment • Dosing Tolerant• Home monitoring • Blips, LLV & sanctuaries• ‘Special’ populations• DDI management
Delivery of Care
Monotherapy
▪ bPI monotherapy (DRVr or LPVr)
virologically inferior, but resistance is unusual, and resuppression expected after re-introduction of NRTIs
may be useful to bridge acute events, eg overdose, post-operatively, ICU (NG feeding), drug toxicity, etc
▪ DTG monotherapy
increased failure WITH high risk of resistance
DOMONO, REDOMO
avoid

2 Drug Regimens
• Pill Size
• Pill number (but FDCs)
• Toxicity (TFV-sparing)
• Interactions (depends)
• Cost saving (depends)
• Preserving options
Why ?
• Less tolerance for missed doses
• Less tolerance for DDI
• More likely to fail with resistance (?)
• Sanctuaries and sterilisation of compartments
Why Not ?
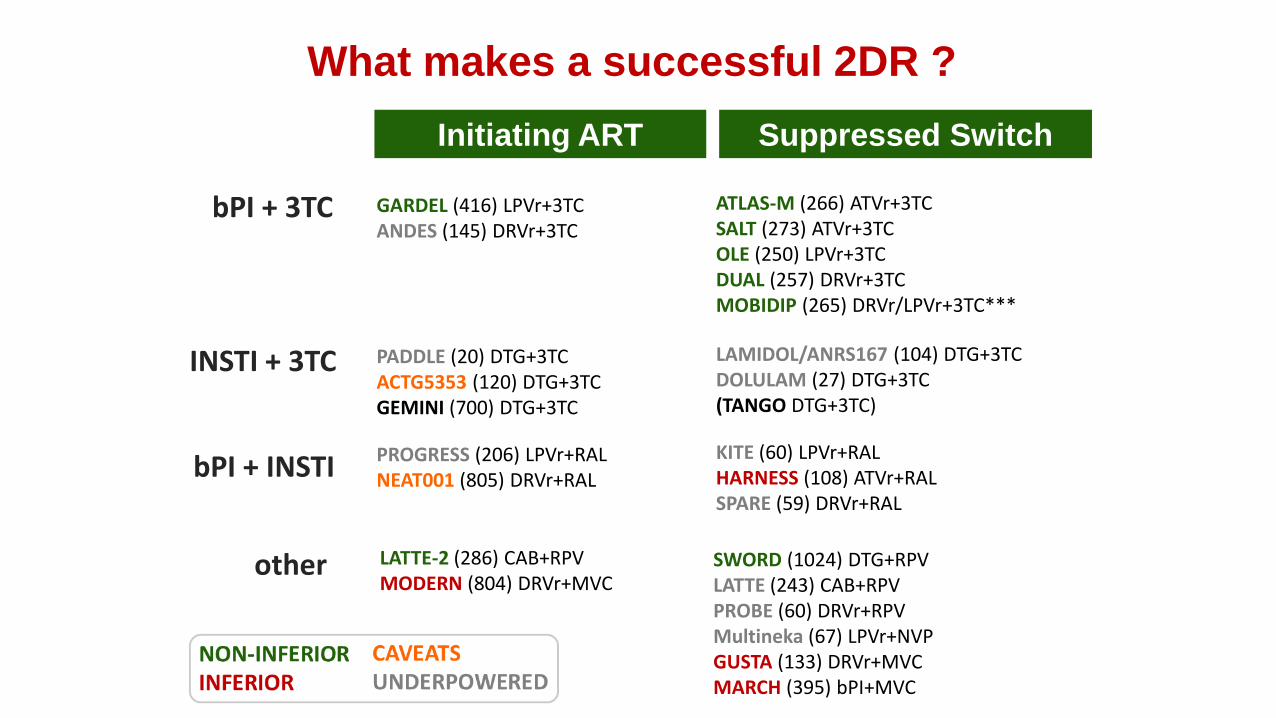
Initiating ART Suppressed Switch
bPI + 3TC
INSTI + 3TC
bPI + INSTI
other
GARDEL (416) LPVr+3TCANDES (145) DRVr+3TC
PROGRESS (206) LPVr+RALNEAT001 (805) DRVr+RAL
PADDLE (20) DTG+3TCACTG5353 (120) DTG+3TCGEMINI (700) DTG+3TC
LATTE-2 (286) CAB+RPVMODERN (804) DRVr+MVC
ATLAS-M (266) ATVr+3TCSALT (273) ATVr+3TCOLE (250) LPVr+3TCDUAL (257) DRVr+3TCMOBIDIP (265) DRVr/LPVr+3TC***
KITE (60) LPVr+RALHARNESS (108) ATVr+RALSPARE (59) DRVr+RAL
LAMIDOL/ANRS167 (104) DTG+3TCDOLULAM (27) DTG+3TC(TANGO DTG+3TC)
SWORD (1024) DTG+RPVLATTE (243) CAB+RPVPROBE (60) DRVr+RPVMultineka (67) LPVr+NVPGUSTA (133) DRVr+MVCMARCH (395) bPI+MVC
What makes a successful 2DR ?

M184V- 92.5% (95% CI 87.2; 97.8)M184V+ 92.5% (95% CI 85.0; 99.9)
p=0.824
Estimated probability of remaining free from VF with dual therapy at 3 years
Gagliardini R 15th EU HIV & Hep Conference, Rome 2017 Abstr 13
ARCA – Virological outcome on dual therapies
Patients suppressed, switch to 2DR (bPI or INI + 3TC) (N=454) vs bPI monotherapy (N=216)Median follow-up: 1.2 years (IQR 0.6-2.4)Overall incidence of VF: 2.35 per 100 PYFU
Dual M184V+ vs monotherapy
Estimated probability of remaining free of VF at 3 yearsDT M184V+ 92.5% (95% CI 85.0; 99.9)
Mono 81.5% (95% CI 73.1; 89.9)p=0.049
Overall dual vs monotherapy
Estimated probability of remaining free of VF at 3 yearsDT 92.5% (95% CI 87.9; 97.0)
Mono 81.5% (95% CI 73.1; 89.9)p<0.001

Initiating ART Suppressed Switch
bPI + 3TC
INSTI + 3TC
bPI + INSTI
other
GARDEL (416) LPVr+3TCANDES (145) DRVr+3TC
PROGRESS (206) LPVr+RALNEAT001 (805) DRVr+RAL
PADDLE (20) DTG+3TCACTG5353 (120) DTG+3TCGEMINI (700) DTG+3TC
LATTE-2 (286) CAB+RPVMODERN (804) DRVr+MVC
ATLAS-M (266) ATVr+3TCSALT (273) ATVr+3TCOLE (250) LPVr+3TCDUAL (257) DRVr+3TCMOBIDIP (265) DRVr/LPVr+3TC***
KITE (60) LPVr+RALHARNESS (108) ATVr+RALSPARE (59) DRVr+RAL
LAMIDOL/ANRS167 (104) DTG+3TCDOLULAM (27) DTG+3TC(TANGO DTG+3TC)
SWORD (1024) DTG+RPVLATTE (243) CAB+RPVPROBE (60) DRVr+RPVMultineka (67) LPVr+NVPGUSTA (133) DRVr+MVCMARCH (395) bPI+MVC
What makes a successful 2DR ?

-3.00
-2.50
-2.00
-1.50
-1.00
-0.50
0.00
DTGRALEVGrETRT20LPVrMVC3TCZDV
- 1.70
- 2.46
- 2.03- 1.99- 1.96- 1.85
- 1.42
- 1.19
- 0.52
ΔV
L (
log
) fr
om
baselin
e
from J Arribas CROI 2017
Lalezari IAS 2009 abst TUAB105;
DeJesus JAIDS 2006;43:1-5;
Markowitz JAIDS 2006;43:509
Sankatsing AIDS 2003;17:2623
Kilby AIDS Res Hum Retroviruses 2002:18:685
Murphy AIDS 2001;15:F1-9
Fatkenhuer Nat Med 2005;11:1170
Eron NEJM 1995;333:1662
Potency of Individual ARVs as Initial Therapy

Rosenbloom et al. Nat Med 2012;18:1378 Laskey & Siliciano. Nat Rev (Microbiol) 2014;12:772
In-vitro, Empirical Assessment of ARVs
Genetic Barrier Synergy/Additivity

• CPE scores do not seem to predict HAND or CSF viral escape
CNS Safety of 2DR
• ATLAS-M (ATVr/3TC)Neurocognitive assessment (N=151)
increase in Global Deficit Score over study
No difference between arms
• Switch to ATVr/3TC (single arm)open label, uncontrolled (N=40)
No change in neurocognitive performance
• SALT (ATVr/3TC)Effect over 96w (N=92)
No difference between 2DR and 3DR
• bPI monotherapy not conclusively shown CNS viral escape
eg LPVr (N=40) monotherapy
Ciccarelli et al CROI 2016
DeLuca et al. IAS 2011
Perez-Valero et al. CROI 2016
Santos et al PLoS ONE 8(7): e70201.

2DRs – Conclusions
• 2DR regimens Not all the same
Need to be individually assessed
Best data for bPI+3TC
Role of 3TC ?
• Reduced covering fire e.g. low adherence, DDIs
… but excluded from trials !
• Compartments Theoretical concern
No actual evidence of harm/benefit
• Not for everyone Special Populations:• Hep B co-infection
• Treatment-experienced ?
• Persistent blips / LLV
• Pregnancy
• DDIs which compromise one/both
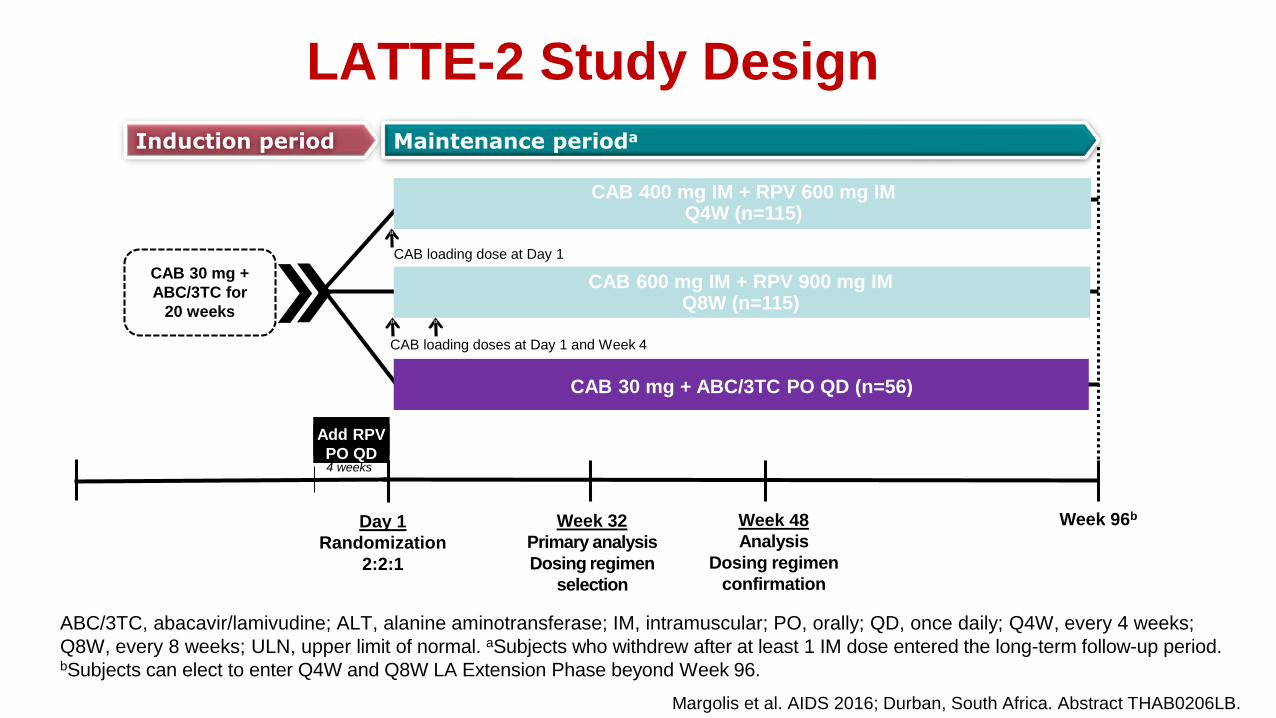
Induction period
LATTE-2 Study Design
Week 32
Primary analysis
Dosing regimen
selection
Day 1
Randomization
2:2:1
Week 48
Analysis
Dosing regimen
confirmation
CAB 400 mg IM + RPV 600 mg IM Q4W (n=115)
CAB 600 mg IM + RPV 900 mg IM Q8W (n=115)
Week 96b
CAB loading dose at Day 1
CAB loading doses at Day 1 and Week 4
CAB 30 mg +
ABC/3TC for
20 weeks
CAB 30 mg + ABC/3TC PO QD (n=56)
Maintenance perioda
Add RPV
PO QD4 weeks
Margolis et al. AIDS 2016; Durban, South Africa. Abstract THAB0206LB.
ABC/3TC, abacavir/lamivudine; ALT, alanine aminotransferase; IM, intramuscular; PO, orally; QD, once daily; Q4W, every 4 weeks;
Q8W, every 8 weeks; ULN, upper limit of normal. aSubjects who withdrew after at least 1 IM dose entered the long-term follow-up period. bSubjects can elect to enter Q4W and Q8W LA Extension Phase beyond Week 96.

LATTE-2 Week 48 Results: HIV-1 RNA <50 c/mL by Snapshot (ITT-ME)
Snapshot success
D1 W32
Q4W 99% 94%
Q8W 95% 95%
Oral 98% 91%
Pro
po
rtio
n o
f p
ati
en
ts w
ith
vir
olo
gic
al
su
pp
ressio
n,
%
BL W-16 W-12 W-8 D1 W4 W8 W12 W16 W20 W24 W28 W32
Study visit
Induction period Maintenance period
W-4 W36 W40 W44 W48
Oral CAB induction (ME population) Oral CAB (n=56) Q4W IM (n=115) Q8W IM (n=115)

High potency underpins the LA approach
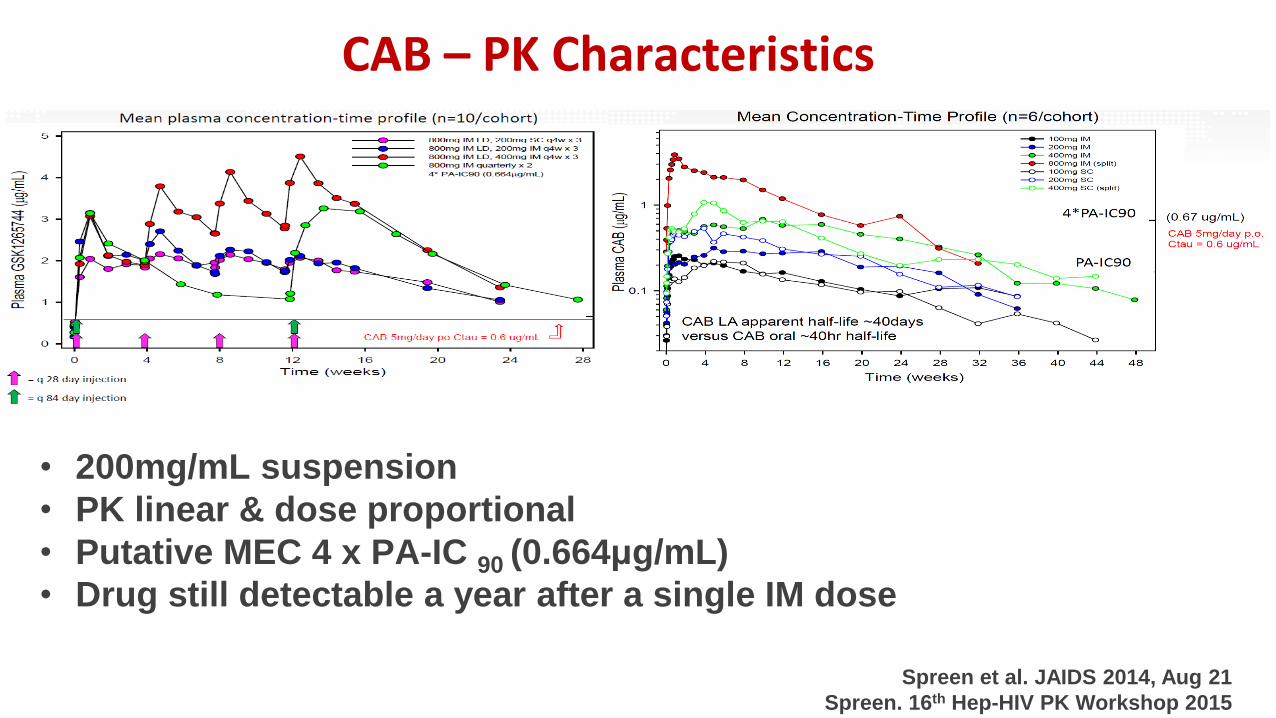
CAB – PK Characteristics
Spreen et al. JAIDS 2014, Aug 21
Spreen. 16th Hep-HIV PK Workshop 2015
• 200mg/mL suspension
• PK linear & dose proportional
• Putative MEC 4 x PA-IC 90 (0.664μg/mL)
• Drug still detectable a year after a single IM dose

Real-life Challenges - injectables
▪ Injection relatedISR, needle fatigue
consistency & reproducibility of injections
children, low BMI
gender-based differences
▪ Pharmaceuticalformulations and co-formulations
variability – BMI, gender, pharmacogenetic
cold chain
scalability, affordability
implementation and health system capacity
alignment with allied interventions (LA contraceptives)
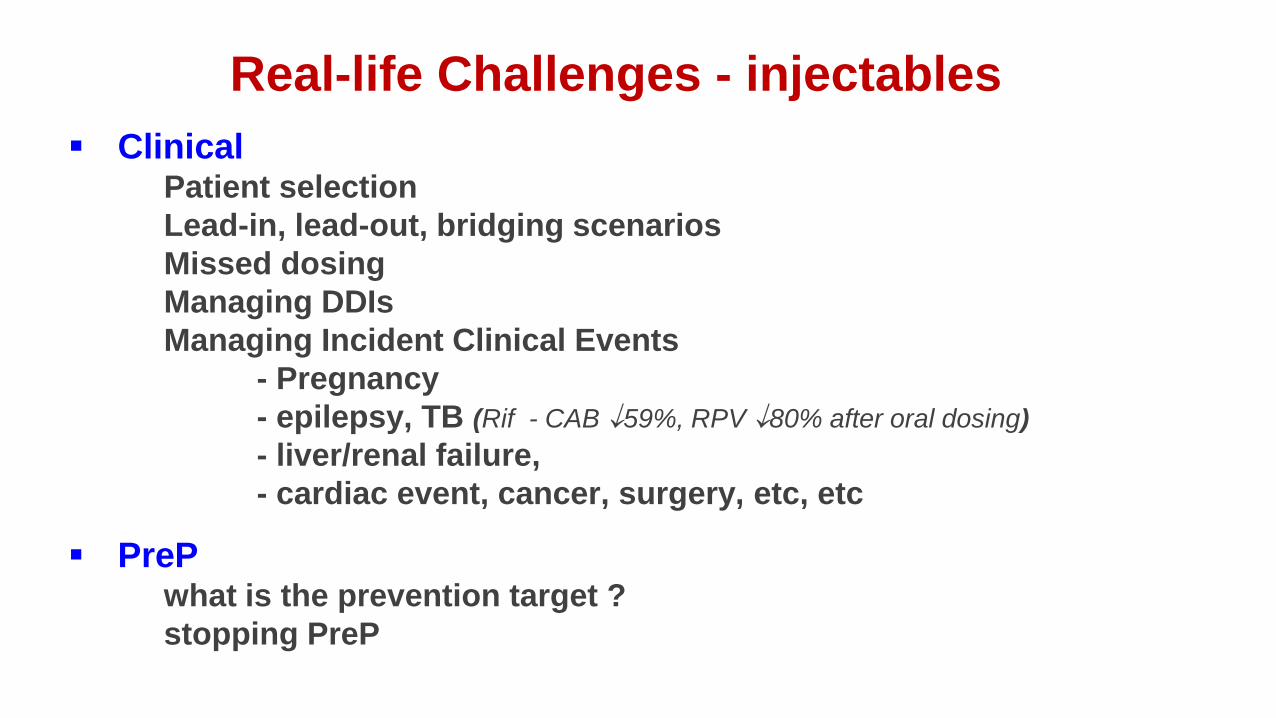
Real-life Challenges - injectables
▪ ClinicalPatient selection
Lead-in, lead-out, bridging scenarios
Missed dosing
Managing DDIs
Managing Incident Clinical Events
- Pregnancy
- epilepsy, TB (Rif - CAB 59%, RPV 80% after oral dosing)
- liver/renal failure,
- cardiac event, cancer, surgery, etc, etc
▪ PrePwhat is the prevention target ?
stopping PreP

Drug-Drug Interactions
• Recognition Take full medication history
Ask about recreational, OTC, herbals
Just too many to remember !

www.hiv-druginteractions.org
www.hep-druginteractions.org
HIV iCharts
Hep iCharts
HIV and Hepatitis DDI Websites

Drug-Drug Interactions
• Recognition Take full medication history
Ask about recreational, OTC, herbals
Just too many to remember !
• Risk assessment Not all DDIs lead to harm
How bad is the harm ? (Therapeutic index)
How likely in this patient ?
• Response Assessing need for drugs
Alternative options ?
Dose modification possible ?
Monitoring safety ?
Discuss with patient and accept risk ?

Guidelines often do not consider Co-morbidities
▪ Survey of NICE Guidelines for T2 Diabetes, Depression, Heart Failure
▪ Compared with recommendations from 12 common co-morbidities
▪ DDI liability assessed
Dumbreck et al. BMJ 2015;350:bmj.h949

Summary
▪ DDIs are frequent and unavoidable
▪ Generally manageable, but only with complete medication recording
▪ Fragmented care - information is lost between teams
▪ Lack of awareness
Increases risk of harm
▪ Good communication and training
▪ Patient involvement
▪ Exploit digital resources for patient safety
Protects against harm
▪ New therapies unlikely to eliminate DDIs (especially with muli-morbidities)
▪ Not all 2DRs are the same
▪ Not all people will benefit from 2DRs
▪ Not all HIV morbidities will be eliminated by virological suppression

Acknowledgements
University of LiverpoolDavid Back
Laura Else
Andrew Hill
Adeneyi Olagunju
Catriona Waitt
Andrew Owen
Marco Siccardi
Kay Seden
Alieu Amara
Sara Gibbons
Sujan Dilly Penchala
Laura Dickinson
Alessandro Schipani
Henry Pertinez
Katie McAllister
St Stephens AIDS TrustMarta Boffito
Infectious Disease Institute, Kampala Mohamed Lamorde