Fungus Danielle Hansen, DO Internal Medicine Lecture Series April 4, 2007.
59
Fungus Fungus Danielle Hansen, DO Danielle Hansen, DO Internal Medicine Lecture Internal Medicine Lecture Series Series April 4, 2007 April 4, 2007
-
Upload
edmund-farmer -
Category
Documents
-
view
214 -
download
0
Transcript of Fungus Danielle Hansen, DO Internal Medicine Lecture Series April 4, 2007.

FungusFungus
Danielle Hansen, DODanielle Hansen, DO
Internal Medicine Lecture SeriesInternal Medicine Lecture Series
April 4, 2007April 4, 2007

Predisposing FactorsPredisposing Factors ImmunosuppressedImmunosuppressed Broad-Spectrum AntibioticsBroad-Spectrum Antibiotics Central Venous CathetersCentral Venous Catheters TraumaTrauma BurnsBurns Total Parenteral NutritionTotal Parenteral Nutrition Hemodialysis or Peritoneal DialysisHemodialysis or Peritoneal Dialysis Abdominal SurgeryAbdominal Surgery GI Tract Perforations and Anastomotic LeaksGI Tract Perforations and Anastomotic Leaks Gradual OnsetGradual Onset

DermatophytesDermatophytes
RingwormRingworm 5 Million DO Visits Annually5 Million DO Visits Annually >$200 Million>$200 Million TypesTypes
EpidermophytonEpidermophyton TrichophytonTrichophyton MicrosporumMicrosporum
DiagnosisDiagnosis KOH TestKOH Test CultureCulture
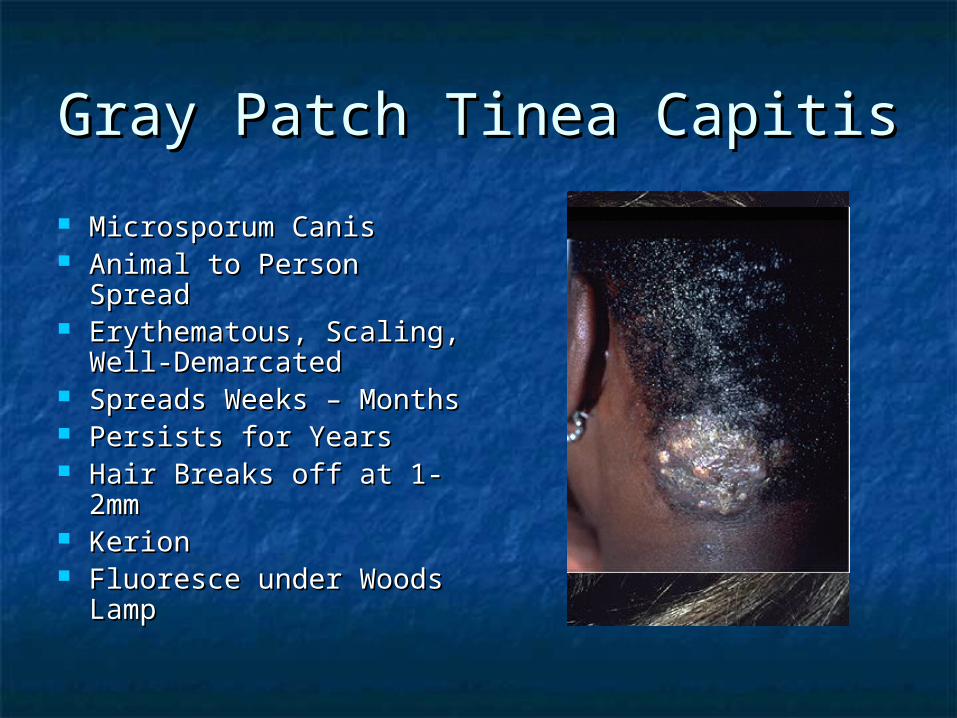
Gray Patch Tinea CapitisGray Patch Tinea Capitis
Microsporum CanisMicrosporum Canis Animal to Person SpreadAnimal to Person Spread Erythematous, Scaling, Erythematous, Scaling,
Well-DemarcatedWell-Demarcated Spreads Weeks – MonthsSpreads Weeks – Months Persists for YearsPersists for Years Hair Breaks off at 1-2mmHair Breaks off at 1-2mm KerionKerion Fluoresce under Woods Fluoresce under Woods
LampLamp

Black Dot Tinea CapititsBlack Dot Tinea Capitits
African AmericansAfrican Americans Person to Person Person to Person
SpreadSpread Erythematous, Erythematous,
ScalingScaling Slowly EnlargesSlowly Enlarges Hair Breaks off FlushHair Breaks off Flush KerionKerion Do Not FluoresceDo Not Fluoresce

Tinea Capitis TreatmentTinea Capitis Treatment
GriseofulvinGriseofulvin 250mg PO BID x 6-12 250mg PO BID x 6-12 weeksweeks
Terbinafine 250mg PO QD x 4 weeksTerbinafine 250mg PO QD x 4 weeks ItraconazoleItraconazole FluconazoleFluconazole
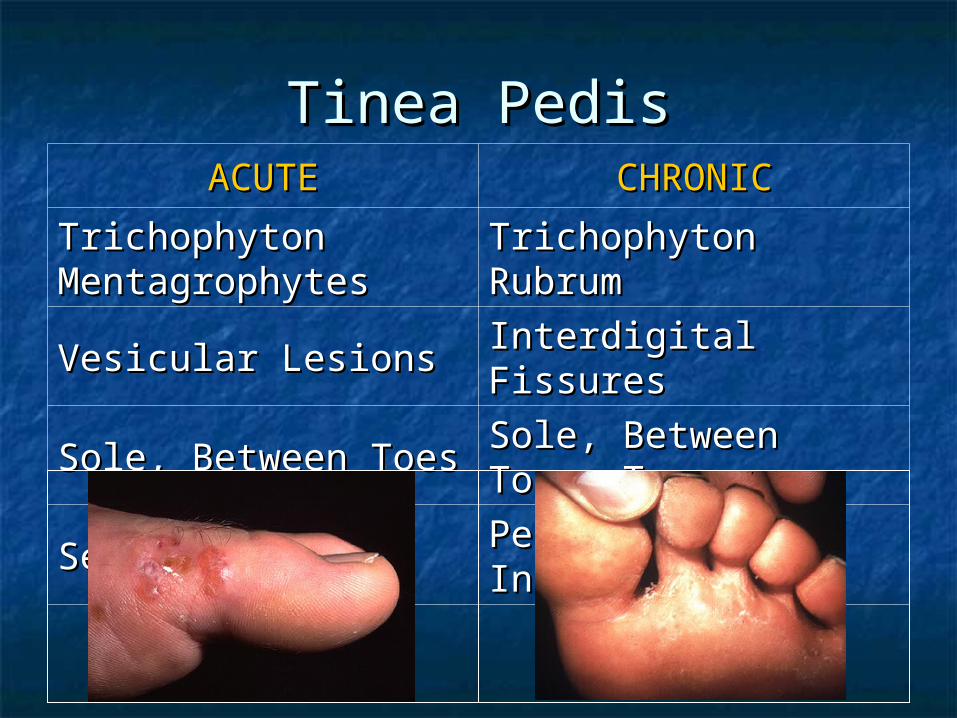
Tinea PedisTinea PedisACUTEACUTE CHRONICCHRONIC
Trichophyton Trichophyton MentagrophytesMentagrophytes Trichophyton RubrumTrichophyton Rubrum
Vesicular LesionsVesicular Lesions Interdigital FissuresInterdigital Fissures
Sole, Between ToesSole, Between Toes Sole, Between Toes, Sole, Between Toes, TopTop
Self-LimitedSelf-Limited Persists IndefinitelyPersists Indefinitely

Tinea Pedis TreatmentTinea Pedis Treatment
Topical Antifungal x 4 weeksTopical Antifungal x 4 weeks Oral AntifungalOral Antifungal
Griseofluvin 250 – 500mg BIDGriseofluvin 250 – 500mg BID Terbinafine 250mg QDTerbinafine 250mg QD Itraconazole 200mg QDItraconazole 200mg QD
Foot PowderFoot Powder Non-occlusive FootwearNon-occlusive Footwear
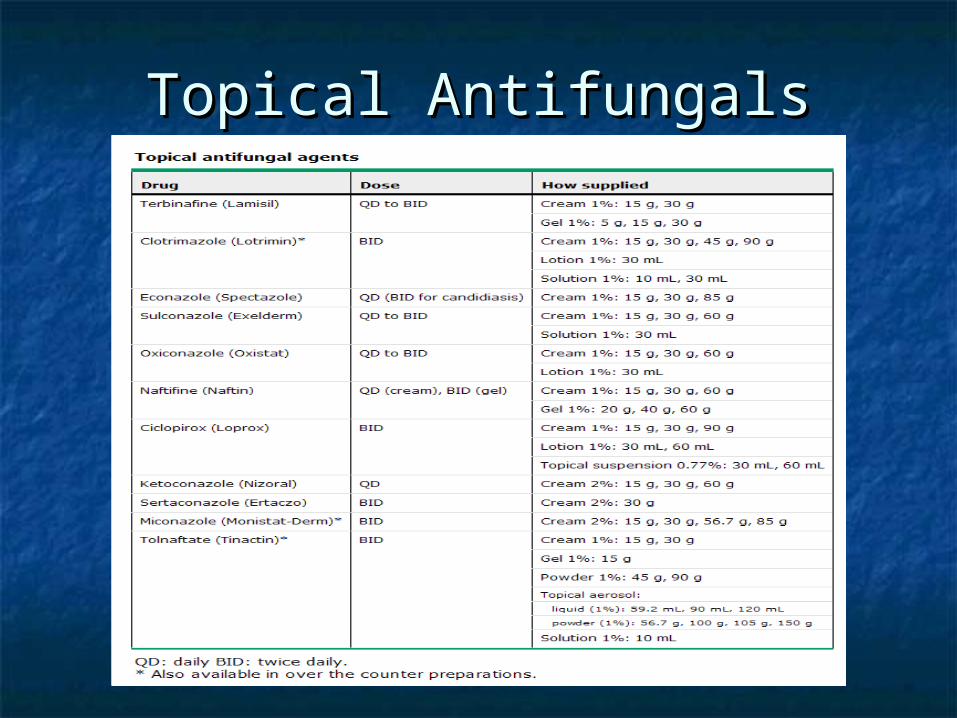
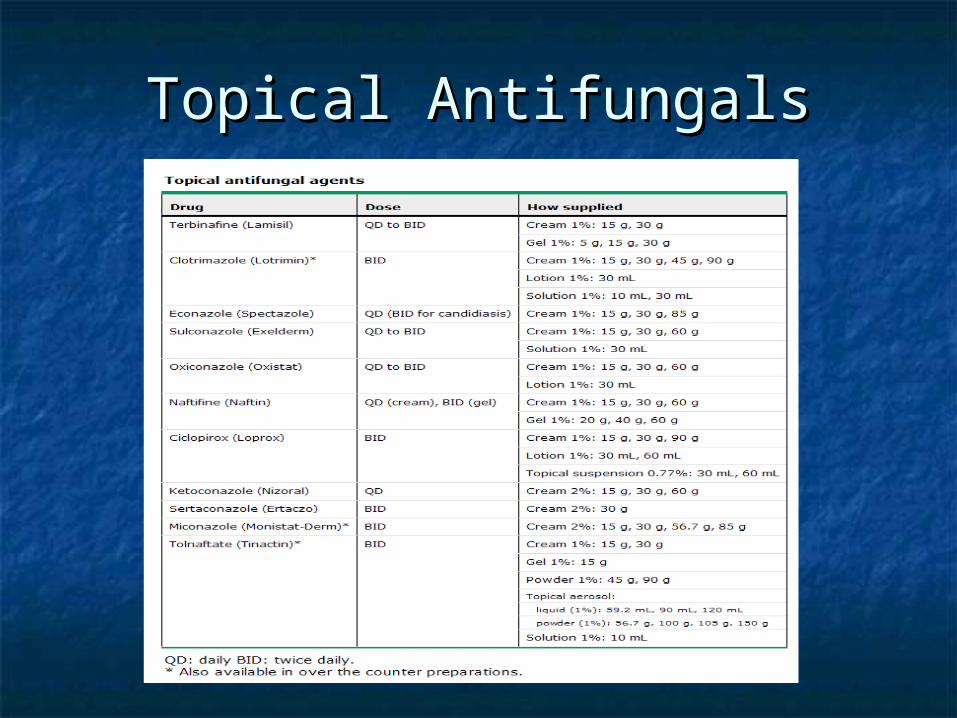
Topical AntifungalsTopical Antifungals
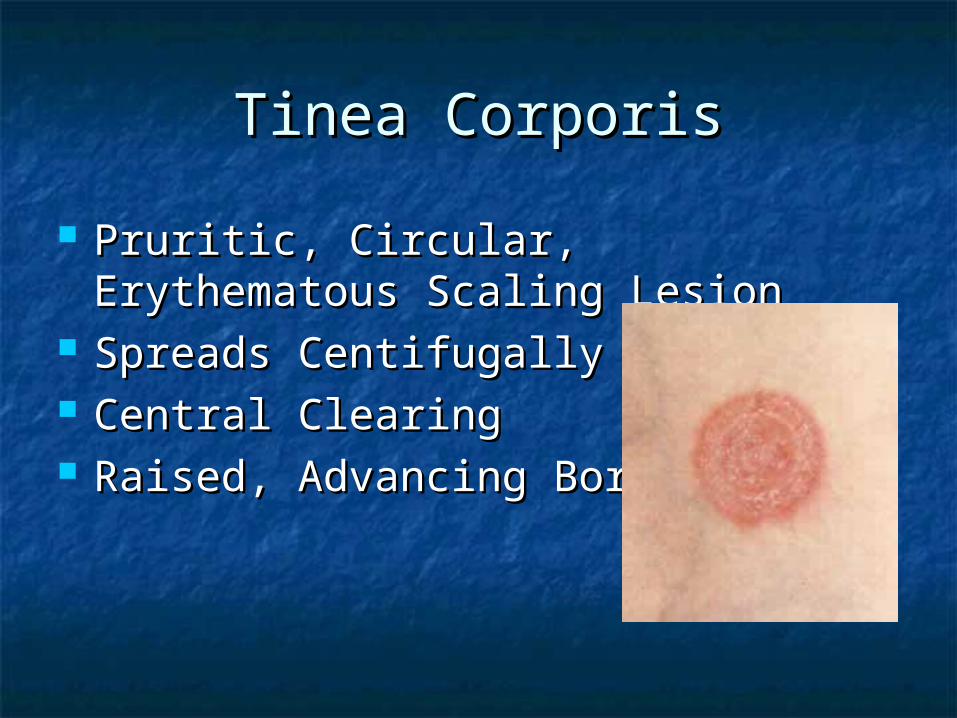
Tinea CorporisTinea Corporis
Pruritic, Circular, Erythematous Pruritic, Circular, Erythematous Scaling LesionScaling Lesion
Spreads CentifugallySpreads Centifugally Central ClearingCentral Clearing Raised, Advancing BorderRaised, Advancing Border

Tinea Corporis TreatmentTinea Corporis Treatment
Topical AntifungalsTopical Antifungals
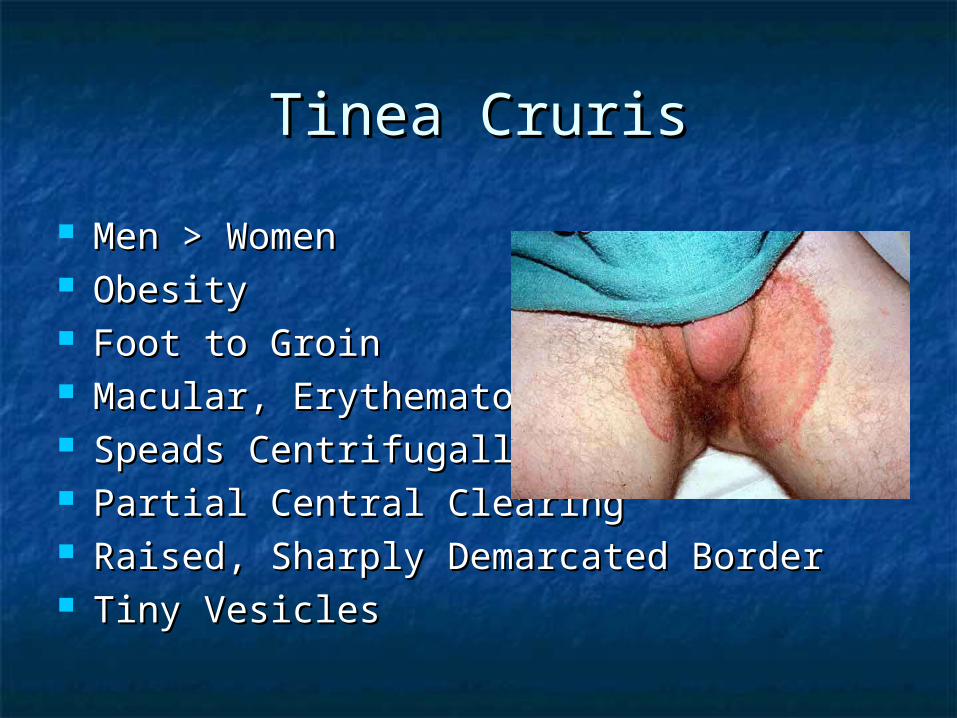
Tinea CrurisTinea Cruris
Men > WomenMen > Women ObesityObesity Foot to GroinFoot to Groin Macular, ErythematousMacular, Erythematous Speads CentrifugallySpeads Centrifugally Partial Central ClearingPartial Central Clearing Raised, Sharply Demarcated BorderRaised, Sharply Demarcated Border Tiny VesiclesTiny Vesicles

Tinea Cruris TreatmentTinea Cruris Treatment
Topical AntifungalsTopical Antifungals Systemic Antifungals if Resistant to Systemic Antifungals if Resistant to
TopicalsTopicals Recurs if Fail to Treat Tinea PedisRecurs if Fail to Treat Tinea Pedis Talcum or Desiccant PowderTalcum or Desiccant Powder No Hot BathsNo Hot Baths Loose Fitting ClothingLoose Fitting Clothing
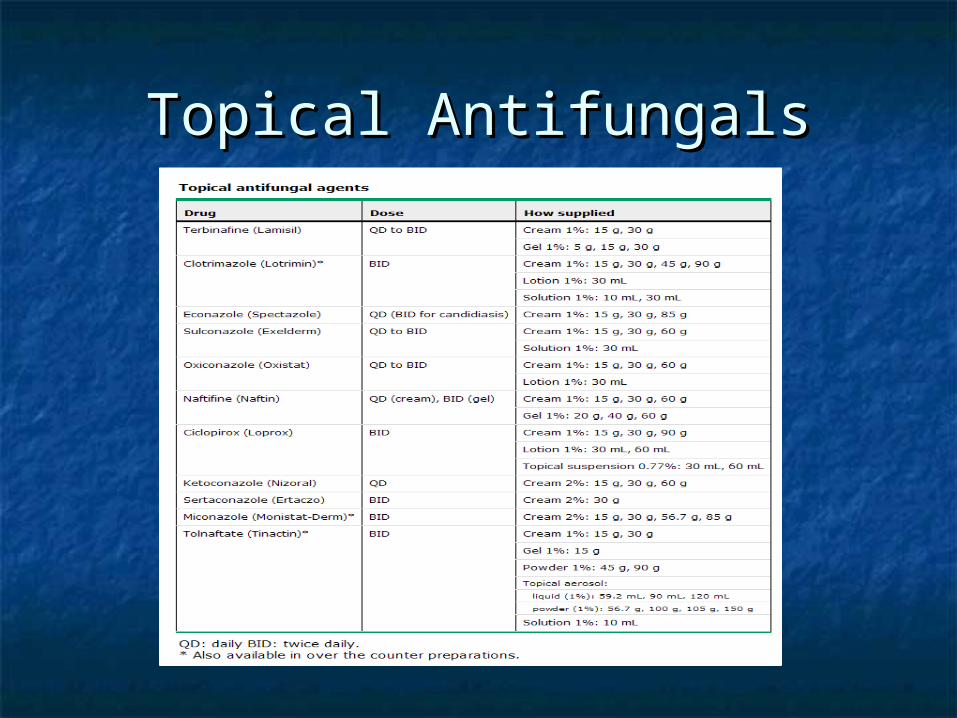
Topical AntifungalsTopical Antifungals

Candidal IntertrigoCandidal Intertrigo
Skin FrictionSkin Friction ObesityObesity Chafing ClothingChafing Clothing Rubbing ActivitiesRubbing Activities
MoistureMoisture ObesityObesity Occlusive ClothingOcclusive Clothing HyperhidrosisHyperhidrosis
DMDM CorticosteroidsCorticosteroids ABXABX HIVHIV ChemotherapyChemotherapy ImmunosuppresantsImmunosuppresants Occupational Occupational
Exposure to SugarExposure to Sugar

Candidal IntertrigoCandidal Intertrigo
Erythematous, Erythematous, Macerated Plaques Macerated Plaques and Erosionsand Erosions
Peripheral ScalingPeripheral Scaling Satelite Satelite
PapulopustulesPapulopustules PruriticPruritic KOH TestKOH Test CultureCulture
Candidal Intertrigo Candidal Intertrigo TreatmentTreatment
Topical AntifungalTopical Antifungal Drying AgentsDrying Agents
Antifungal PowdersAntifungal Powders Aluminum Acetate SolutionAluminum Acetate Solution Gentian VioletGentian Violet Talcum PowderTalcum Powder
Systemic AntifungalsSystemic Antifungals
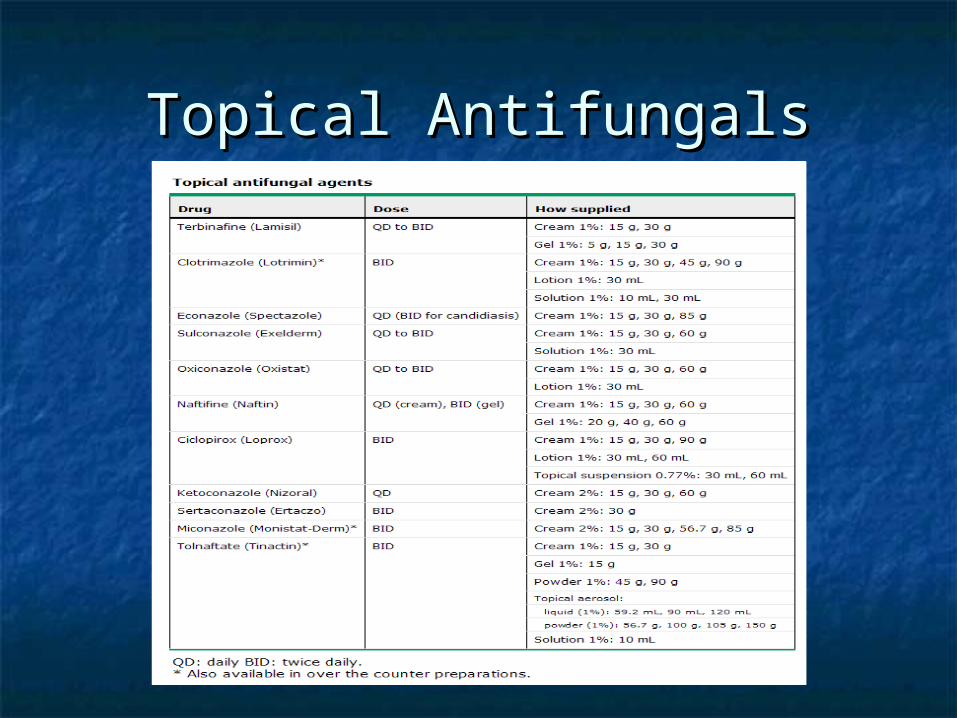
Topical AntifungalsTopical Antifungals

OnychomycosisOnychomycosis
Distal Distal SubungualSubungual
Proximal Proximal SubungualSubungual
White White SuperficialSuperficial
YeastYeast
Great ToeGreat Toe HIVHIV Fingernails, Fingernails, ImmunodeficieImmunodeficie
ntnt
White/Brown/White/Brown/
YellowYellowDull White Dull White
SpotsSpotsThick, Thick,
Yellow/BrownYellow/Brown
Distal to Distal to CuticleCuticle
Proximal to Proximal to DistalDistal
CentrifugallyCentrifugally

Onychomycosis TreatmentOnychomycosis Treatment
Indications for TreatmentIndications for Treatment Cellulitis in LECellulitis in LE Diabetics with Additional Risk Factor for CellulitisDiabetics with Additional Risk Factor for Cellulitis PainPain CosmeticsCosmetics
Terbinafine 250mg/day x 6-12wks Terbinafine 250mg/day x 6-12wks Itraconazole 200mg/day x 6-12wks or Itraconazole 200mg/day x 6-12wks or
200mg/day x 7days/month x 2 mo200mg/day x 7days/month x 2 mo SurgerySurgery
OtomycosisOtomycosis
External Auditory CanalExternal Auditory Canal 6.5 – 12.5% of Otitis Externa6.5 – 12.5% of Otitis Externa 61+ Species of 28 Genera61+ Species of 28 Genera
Aspergillus NigerAspergillus Niger CandidaCandida
Tropical and Subtropical RegionsTropical and Subtropical Regions Swimming, Canal CleaningSwimming, Canal Cleaning Antibiotic Ear DropsAntibiotic Ear Drops

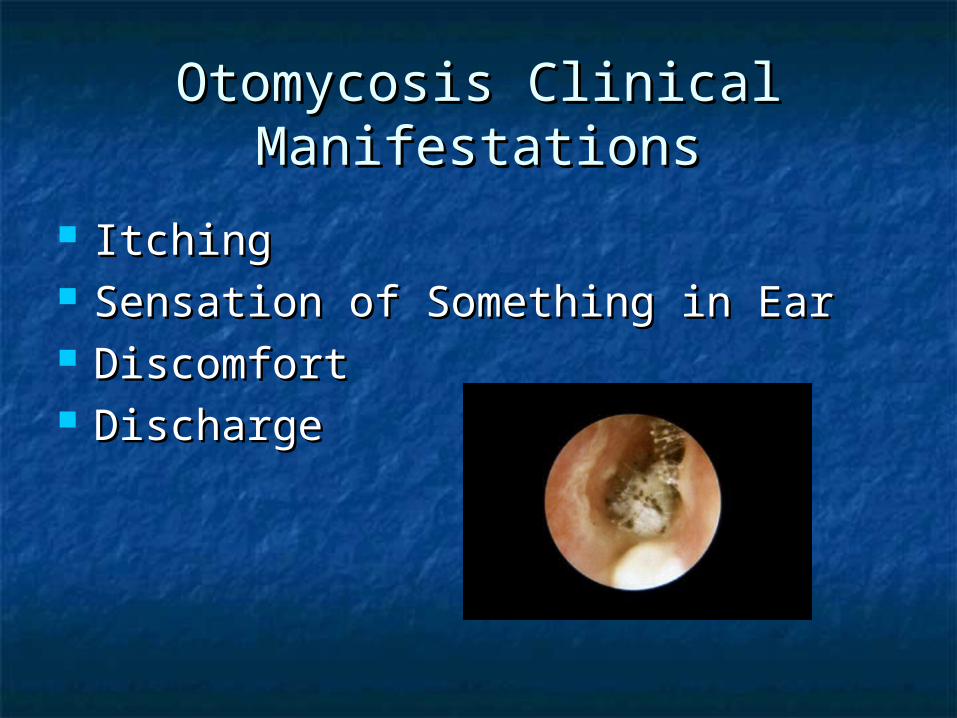
Otomycosis Clinical Otomycosis Clinical ManifestationsManifestations
ItchingItching Sensation of Something in EarSensation of Something in Ear DiscomfortDiscomfort DischargeDischarge

Otomycosis TreatmentOtomycosis Treatment
Clean CanalClean Canal SteroidsSteroids AntisepticsAntiseptics
Gentian VioletGentian Violet CresylateCresylate MerthiolateMerthiolate
Acidifying SolutionsAcidifying Solutions VoSolVoSol Otic DomeboroOtic Domeboro
AntifungalsAntifungals Drying AgentsDrying Agents
A. NigerA. Niger C. C. AlbicansAlbicans
C. C. ParapsilosisParapsilosis
Amphotericin BAmphotericin B ++ ++++ ++++
ClotrimoazoleClotrimoazole ++++ ++++ ++++
FlucytosineFlucytosine 00 00 00
MiconazoleMiconazole ++ ++++ ++++
NatamycinNatamycin ++++ ++ ++
NystatinNystatin ++ ++++ ++++
TolnaftateTolnaftate 00 00 00

Fungal EndophthalmitisFungal Endophthalmitis
EpidemiologyEpidemiology Trauma Trauma SurgerySurgery Hematogenous Seeding Hematogenous Seeding
of Retina and Choroidof Retina and Choroid
Clinical ManifestationsClinical Manifestations Eye PainEye Pain Gradual Decrease in Gradual Decrease in
Visual AcuityVisual Acuity Focal, Glistening, White, Focal, Glistening, White,
Infiltrative, Mound-like Infiltrative, Mound-like Lesion on RetinaLesion on Retina
Vitreal HazeVitreal Haze Fluffy, White Balls in Fluffy, White Balls in
VitreousVitreous

Fungal EndophthalmitisFungal Endophthalmitis
IV AntifungalIV Antifungal Intravitreal AntifungalIntravitreal Antifungal Surgical Removal of Vitreous and Surgical Removal of Vitreous and
Foreign MaterialForeign Material

Oropharyngeal CandidiasisOropharyngeal Candidiasis
EpidemiologyEpidemiology Elderly with DenturesElderly with Dentures AntibioticsAntibiotics Inhaled CorticosteroidsInhaled Corticosteroids ChemotherapyChemotherapy Radiation of Head and NeckRadiation of Head and Neck Cellular Immune DeficiencyCellular Immune Deficiency XerostomiaXerostomia
Clinical ManifestationsClinical Manifestations Cotton MouthCotton Mouth Loss of TasteLoss of Taste OdynophagiaOdynophagia Pain with DenturesPain with Dentures

Oropharyngeal CandidiasisOropharyngeal Candidiasis Diagnosis Diagnosis
White Plaques on White Plaques on Buccal Mucosa, Buccal Mucosa, Palate, Tongue, Palate, Tongue, Oropharynx, under Oropharynx, under DenturesDentures
Budding Yeast with Budding Yeast with or without or without Pseudohyphae from Pseudohyphae from ScrapingScraping
TreatmentTreatment Nystatin Swish and Nystatin Swish and
Swallow 5x/day Swallow 5x/day Fluconazole 200mg Fluconazole 200mg
x1, then 100mg QD x1, then 100mg QD Chlorhexidine Chlorhexidine
Gluconate Soak for Gluconate Soak for DenturesDentures
Duration of Duration of Treatment 7-14 daysTreatment 7-14 days

Candida EsophagitisCandida Esophagitis EpidemiologyEpidemiology
HIVHIV Hematologic Hematologic
MalignaniesMalignanies ThrushThrush
Clinical ManifestationsClinical Manifestations OdynophagiaOdynophagia
DiagnosisDiagnosis White Mucosal Plaque-White Mucosal Plaque-
like Lesions on EGDlike Lesions on EGD Biopsy Shows Yeast and Biopsy Shows Yeast and
Pseudohyphae Invading Pseudohyphae Invading Mucosal CellsMucosal Cells
Culture + CandidaCulture + Candida TreatmentTreatment
Fluconazole 100-200mg Fluconazole 100-200mg QD x 14-21 daysQD x 14-21 days

Candida PneumoniaCandida Pneumonia
EpidemiologyEpidemiology Infection vs Colonization vs Infection vs Colonization vs
ContaminationContamination Primary Candida Pneumonia < 1%Primary Candida Pneumonia < 1% Aspiration of Oropharyngeal ContentsAspiration of Oropharyngeal Contents
Clinical ManifestationsClinical Manifestations FeverFever TachypneaTachypnea Nonspecific Patchy Infiltrates on CXRNonspecific Patchy Infiltrates on CXR

Candida PneumoniaCandida Pneumonia
DiagnosisDiagnosis Sputum CultureSputum Culture
Sensitivity 85%Sensitivity 85% Specificity 60%Specificity 60%
Bronchoalveolar Bronchoalveolar LavageLavage
Sensitivity 71%Sensitivity 71% Specificity 57%Specificity 57%
TreatmentTreatment No TreatmentNo Treatment
Immunocompetent Immunocompetent with + Sputumwith + Sputum
Amphotericin B 0.7-Amphotericin B 0.7-1.0 mg/kg daily1.0 mg/kg daily
Isolated Pneumonia Isolated Pneumonia Treatment for Treatment for
Disseminated Disseminated DiseaseDisease
Secondary PneumoniaSecondary Pneumonia
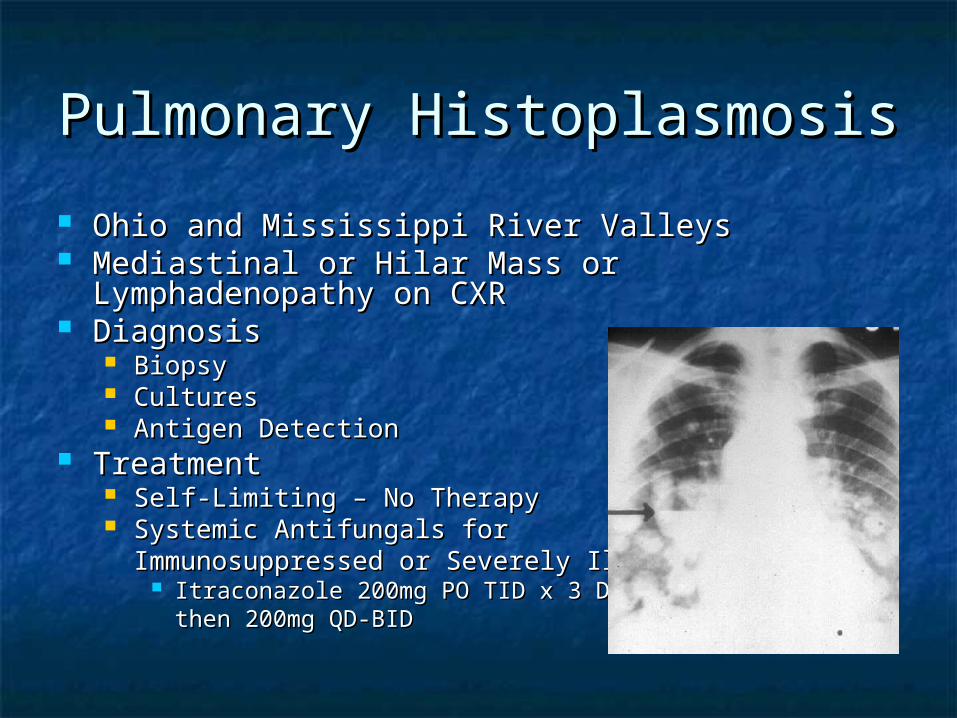
Pulmonary HistoplasmosisPulmonary Histoplasmosis
Ohio and Mississippi River ValleysOhio and Mississippi River Valleys Mediastinal or Hilar Mass or Lymphadenopathy on Mediastinal or Hilar Mass or Lymphadenopathy on
CXRCXR Diagnosis Diagnosis
BiopsyBiopsy CulturesCultures Antigen DetectionAntigen Detection
TreatmentTreatment Self-Limiting – No TherapySelf-Limiting – No Therapy Systemic Antifungals for Systemic Antifungals for
Immunosuppressed or Severely IllImmunosuppressed or Severely Ill Itraconazole 200mg PO TID x 3 Days, Itraconazole 200mg PO TID x 3 Days,
then 200mg QD-BIDthen 200mg QD-BID
Fungal EndocarditisFungal Endocarditis
EpidemiologyEpidemiology Prosthetic Heart Prosthetic Heart
ValvesValves IV Drug UsersIV Drug Users Central Venous Central Venous
CathetersCatheters Prolonged Prolonged
FungemiaFungemia
Clinical Clinical ManifestationsManifestations FeverFever MurmurMurmur Signs and Signs and
Symptoms of Heart Symptoms of Heart FailureFailure
Peripheral Peripheral EmbolismEmbolism50-100% Mortality

Candida EndocarditisCandida Endocarditis
DiagnosisDiagnosis Persistent Persistent
CandidemiaCandidemia Vegetations on Vegetations on
EchocardiographyEchocardiography
TreatmentTreatment Amphotericin B +/- Amphotericin B +/-
Flucytosine x 6 Flucytosine x 6 weeksweeks
Surgical ResectionSurgical Resection
Fungal PeritonitisFungal Peritonitis
EpidemiologyEpidemiology Gut PerforationGut Perforation Anastomotic LeaksAnastomotic Leaks Acute Necrotizing Acute Necrotizing
PancreatitisPancreatitis Peritoneal DialysisPeritoneal Dialysis Gangrenous Gangrenous
CholecystitisCholecystitis C. Albicans > C. C. Albicans > C.
Galbrata > OthersGalbrata > Others
Clinical ManifestationsClinical Manifestations Fevers/ChillsFevers/Chills Abdominal PainAbdominal Pain
DiagnosisDiagnosis Culture of AspirateCulture of Aspirate
CT guidedCT guided U/S GuidedU/S Guided
Culture at time of Culture at time of SurgerySurgery
Culture from Drain Culture from Drain InadequateInadequate

Fungal Peritonitis TreatmentFungal Peritonitis Treatment
Fluconazole 400mg dailyFluconazole 400mg daily Preferred unless C. GalbrataPreferred unless C. Galbrata
Amphotericin B 0.7mg/kg dailyAmphotericin B 0.7mg/kg daily C. GalbrataC. Galbrata
CaspofunginCaspofungin C. GalbrataC. Galbrata
Duration of Therapy at Least 2 WeeksDuration of Therapy at Least 2 Weeks Surgical InterventionSurgical Intervention
Fungal Infection of Fungal Infection of Bladder and KidneysBladder and Kidneys
CandidaCandida AspergillusAspergillus TrichosporonTrichosporon ZygomycetesZygomycetes Dematiaceous MoldsDematiaceous Molds Cryptococcus NeoformansCryptococcus Neoformans Dimorphic FungiDimorphic Fungi
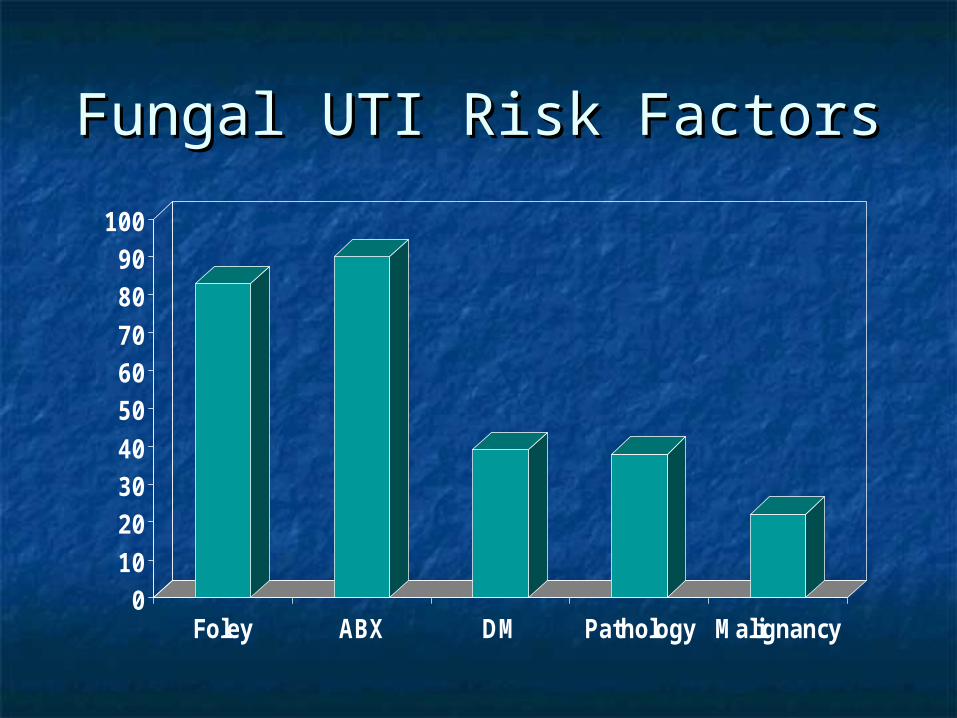
Fungal UTI Risk FactorsFungal UTI Risk Factors
0102030405060708090
100
Foley ABX DM Pathology Malignancy
CharacteristicsCharacteristics
Bladder Infection Vs. ColonizationBladder Infection Vs. Colonization Acute Renal InfectionAcute Renal Infection
Hematogenous SeedingHematogenous Seeding Multiple Micro-abscessesMultiple Micro-abscesses
Chronic Renal InfectionChronic Renal Infection Unilateral, Ascending SeedingUnilateral, Ascending Seeding Perinephric Abscess or BezoarPerinephric Abscess or Bezoar
Efficacy of Funguria Efficacy of Funguria TreatmentTreatment
No Affect on MortalityNo Affect on Mortality Resolution of FunguriaResolution of Funguria
No Treatment 76%No Treatment 76% Catheter Removal 35%Catheter Removal 35% Fluconazole or Amphotericin B 50%Fluconazole or Amphotericin B 50%

Fungal UTI Treatment Fungal UTI Treatment GuidelinesGuidelines
Symptomatic UTISymptomatic UTI Fluconazole 400mg x 1, then 200mg/day x Fluconazole 400mg x 1, then 200mg/day x
1313 Amphotericin B 0.3-0.7 mg/kg/day IV x 1-7Amphotericin B 0.3-0.7 mg/kg/day IV x 1-7 Flucytosine 25mg/kg/day PO x 5-7Flucytosine 25mg/kg/day PO x 5-7
Asymptomatic UTIAsymptomatic UTI Only Treat if NeutropenicOnly Treat if Neutropenic
Perinephric AbscessPerinephric Abscess Surgical Drainage + Systemic AntifungalSurgical Drainage + Systemic Antifungal

Candida VulvovaginitisCandida Vulvovaginitis
EpidemiologyEpidemiology Increased Estrogen Increased Estrogen
LevelsLevels AntibioticsAntibiotics CorticosteroidsCorticosteroids Diabetes MellitusDiabetes Mellitus HIVHIV IUDIUD DiaphragmDiaphragm
Clinical Clinical ManifestationsManifestations ItchItch DischargeDischarge DyspareuniaDyspareunia DysuriaDysuria Vaginal IrritationVaginal Irritation

Candida Vulvovaginitis Candida Vulvovaginitis DiagnosisDiagnosis
Vulvar Erythema and SwellingVulvar Erythema and Swelling Vaginal Erythema and White, Curd-like Vaginal Erythema and White, Curd-like
DischargeDischarge Budding Yeast with or without Budding Yeast with or without
Pseudohyphae on Wet Mount or KOH Pseudohyphae on Wet Mount or KOH Prep of Vaginal SecretionsPrep of Vaginal Secretions
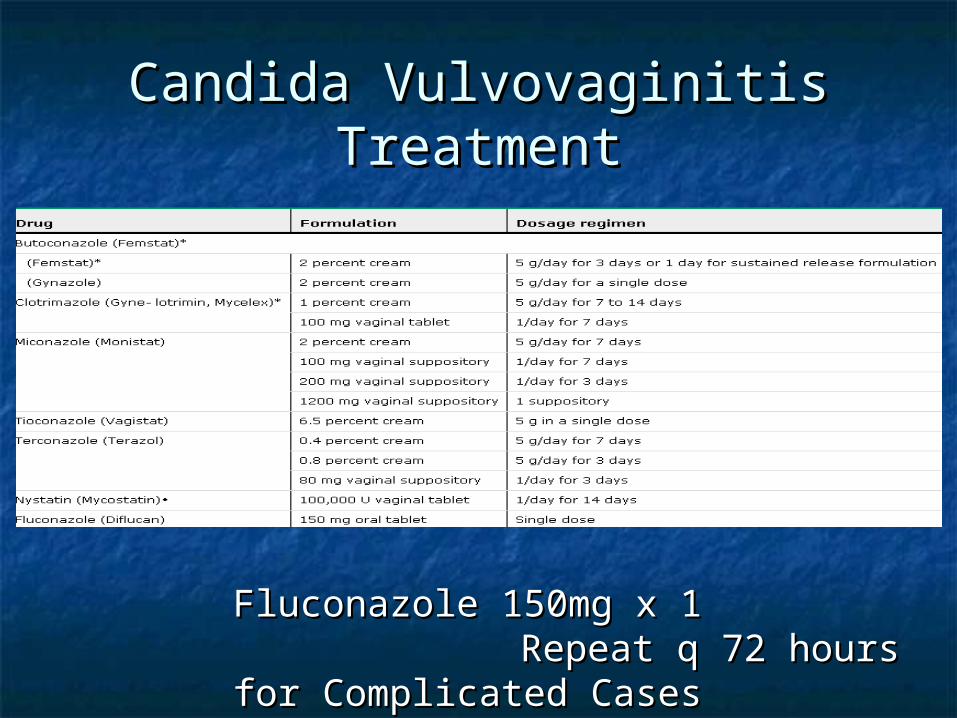
Candida Vulvovaginitis Candida Vulvovaginitis TreatmentTreatment
Fluconazole 150mg x 1Fluconazole 150mg x 1Repeat q 72 hours Repeat q 72 hours
for Complicated Casesfor Complicated Cases
Candida Osteoarticular Candida Osteoarticular InfectionsInfections
EpidemiologyEpidemiology Hematogenous Hematogenous
SpreadSpread TraumaTrauma Intraarticular InjectionIntraarticular Injection SurgerySurgery Injection Drug UseInjection Drug Use Native > Prosthetic Native > Prosthetic
JointsJoints Months-Years after Months-Years after
InsultInsult
Clinical Clinical Manifestations Manifestations PainPain Decreased Range of Decreased Range of
MotionMotion

Candida Osteoarticular Candida Osteoarticular InfectionsInfections
DiagnosisDiagnosis Candidemia in 50-Candidemia in 50-
60%60% WBC WNLWBC WNL ESRESR Erosion on Xray or Erosion on Xray or
MRIMRI Culture of Infected Culture of Infected
SiteSite
TreatmentTreatment Systemic TherapySystemic Therapy
Amphotericin B 0.5-Amphotericin B 0.5-1mg/kg/day x 2-3 1mg/kg/day x 2-3 weeksweeks
then then Fluconazole Fluconazole 400mg/day x 6-12 400mg/day x 6-12 monthsmonths
I & DI & D Remove ProsthesisRemove Prosthesis

Candida MediastinitisCandida Mediastinitis EpidemiologyEpidemiology
Thoracic SurgeryThoracic Surgery Prior Antibiotic Prior Antibiotic
TherapyTherapy Time from Insult to Time from Insult to
Infection 11 DaysInfection 11 Days Range 6 - 100Range 6 - 100
Hematogenous Hematogenous SpreadSpread
Mortality Rate 55%Mortality Rate 55%
Clinical Clinical ManifestationsManifestations Chest Wall Chest Wall
ErythemaErythema Chest Wall Chest Wall
DrainageDrainage FeverFever Sternal InstabilitySternal Instability
TreatmentTreatmentAmphotericin B 0.7 – 1.0 mg/kg dailyAmphotericin B 0.7 – 1.0 mg/kg daily
Fluconazole 400mg dailyFluconazole 400mg dailySurgical DrainageSurgical Drainage

Fungal MeningitisFungal Meningitis
Ventricular Drainage DevicesVentricular Drainage Devices Ventriculoperitoneal ShuntVentriculoperitoneal Shunt Ventriculoatrial ShuntVentriculoatrial Shunt
CraniotomyCraniotomy Hematogenous SpreadHematogenous Spread CSFCSF
Low GlucoseLow Glucose High ProteinHigh Protein

Candidal MeningitisCandidal Meningitis
C. Albicans > C. Paraspilosis > C. TropicalisC. Albicans > C. Paraspilosis > C. Tropicalis ImmunosuppressedImmunosuppressed Fever, Nuchal Rigidity, Altered MS, Fever, Nuchal Rigidity, Altered MS,
HeadacheHeadache Culture CSFCulture CSF Micro-abscesses on MRIMicro-abscesses on MRI Amphotericin B + FlucytosineAmphotericin B + Flucytosine Follow up LP in 1 WeekFollow up LP in 1 Week

Coccidiodal MeningitisCoccidiodal Meningitis
C. Immitis > C. PosadasiiC. Immitis > C. Posadasii Southwestern USSouthwestern US HeadacheHeadache
Persistent or Progressively WorseningPersistent or Progressively Worsening Unusual SeverityUnusual Severity Nausea/VomittingNausea/Vomitting Blurred VisionBlurred Vision Mental Status ChangeMental Status Change
+Culture or Anti-Coccidioidal Antibodies in CSF+Culture or Anti-Coccidioidal Antibodies in CSF Untreated 95% MortalityUntreated 95% Mortality Fluconazole 400-1000mg/day PO IndefinitelyFluconazole 400-1000mg/day PO Indefinitely Intrathecal Amphotericin B for NonrespondersIntrathecal Amphotericin B for Nonresponders

Cryptococcal MeningitisCryptococcal Meningitis
C. NeoformansC. Neoformans InhalationInhalation ImmunosuppressedImmunosuppressed Headache, Fever, Lethargy, Mental Status Headache, Fever, Lethargy, Mental Status
Changes, Memory LossChanges, Memory Loss CSF Culture, India Ink, Cryptococcal Antigen CSF Culture, India Ink, Cryptococcal Antigen
AssayAssay Fatal if UntreatedFatal if Untreated Amphotericin B + Flucytosine x 2 WeeksAmphotericin B + Flucytosine x 2 Weeks
Followed with 3 – 6 months of Fluconazole POFollowed with 3 – 6 months of Fluconazole PO Intrathecal for NonrespondersIntrathecal for Nonresponders
Follow up LP in 2 WeeksFollow up LP in 2 Weeks

FungemiaFungemia ImmunosuppressedImmunosuppressed
Hematologic Hematologic MalignanciesMalignancies
Transplant RecipientsTransplant Recipients ChemotherapyChemotherapy
ICUICU TraumaTrauma BurnsBurns Central LinesCentral Lines TPNTPN ABXABX HemodialysisHemodialysis Abdominal Surgical Abdominal Surgical
ProceduresProcedures GI Tract Perforations GI Tract Perforations
and Anastomotic Leaksand Anastomotic Leaks
Hematogenous SpreadHematogenous Spread C. Albicans C. Albicans
C. Galbrata C. Galbrata C. Parapsilosis C. Parapsilosis C. TropicalisC. TropicalisC. KruseiC. Krusei

Candidemia Clinical Candidemia Clinical ManifestationsManifestations
FeverFever SepsisSepsis Skin LesionsSkin Lesions Eye LesionsEye Lesions Muscle AbscessesMuscle Abscesses Multiorgan System FailureMultiorgan System Failure

Candidemia Diagnosis and Candidemia Diagnosis and TreatmentTreatment
DiagnosisDiagnosis + Blood Cultures+ Blood Cultures Biopsy of Involved Biopsy of Involved
SitesSites
TreatmentTreatment Ophthalmologic Ophthalmologic
ExamExam Catheter RemovalCatheter Removal Systemic AntifungalSystemic Antifungal
Fluconazole 800mg Fluconazole 800mg x1, then 400mg QD x1, then 400mg QD x 14 Days after -BCx 14 Days after -BC
Caspofungin for C. Caspofungin for C. Krusei and C. Krusei and C. GalbrataGalbrata

QuestionsQuestions
1.1. The mortality rate associated with The mortality rate associated with fungal endocarditis is:fungal endocarditis is:
a) < 10%a) < 10%
b) 20-30%b) 20-30%
c) 30-40%c) 30-40%
d) > 50%d) > 50%
QuestionsQuestions
2.2. 67y/o female admitted to the ICU with 67y/o female admitted to the ICU with sepsis. Broad spectrum antibiotics were sepsis. Broad spectrum antibiotics were initiated. She continues to decline. Blood initiated. She continues to decline. Blood cultures finally grow Candida Albicans. cultures finally grow Candida Albicans. After initiating the appropriate After initiating the appropriate antifungal, you:antifungal, you:a) Consult Opthalmologya) Consult Opthalmologyb) Consult GIb) Consult GIc) Consult Orthopedicsc) Consult Orthopedicsd) Consult Psychiatryd) Consult Psychiatry

QuestionsQuestions
3.3. All of the following are susceptible All of the following are susceptible to Fluconazole except:to Fluconazole except:
a) C. Albicansa) C. Albicans
b) C. Kruseib) C. Krusei
c) C. Parapsilosisc) C. Parapsilosis
d) C. Tropicalisd) C. Tropicalis