Fundamentals of Phototherapy for Neonatal Jaundice · Neonatal jaundice expert Maisels suggests...
12
S10 Advances in Neonatal Care • Vol. 11, No. 5S • pp. S10-S21 Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited. Fundamentals of Phototherapy for Neonatal Jaundice Laura A. Stokowski, MS, RN Dr R. H. Dobbs asked her if she had painted the baby’s skin with iodine. She denied having done so, telling him that what she held in her arms was a jaun- diced infant whose color had faded except in an area that had been covered by the corner of a sheet. 2 Subsequently, physicians and scientists at Rochford Hospital discovered that the levels of bilirubin pig- ment in tubes of blood left sitting in the sun also dropped dramatically. Putting these observations together, the idea of phototherapy for neonatal jaun- dice was born. The very first phototherapy unit incor- porating an artificial light source instead of natural sunlight was devised and tested by Cremer et al 3 at Rochford Hospital, and the results were reported in The Lancet, in 1958 (Figure 2). Phototherapy was not used in the United States until the landmark study of Lucey et al 4 was pub- lished in Pediatrics a full decade later. This random- ized controlled trial demonstrating the effectiveness of phototherapy led to its acceptance as a simple, inexpensive, and relatively safe way to prevent hyperbilirubinemia in premature infants. NORMAL BILIRUBIN METABOLISM Humans continuously form bilirubin, and newborn infants produce relatively more bilirubin than any Author Affiliations: Inova Fairfax Hospital for Children, Falls Church, Virginia Correspondence: Laura A. Stokowski, MS, RN, 8317 Argent Circle, Fairfax Station, VA 22039 ([email protected]). Copyright © 2011 by The National Association of Neonatal Nurses DOI: 10.1097/ANC.0b013e31822ee62c ABSTRACT Phototherapy is the use of visible light for the treatment of hyperbilirubinemia in the newborn. This relatively common therapy lowers the serum bilirubin level by transforming bilirubin into water-soluble isomers that can be eliminated without conjugation in the liver. The dose of phototherapy is a key factor in how quickly it works; dose in turn is deter- mined by the wavelength of the light, the intensity of the light (irradiance), the distance between the light and the baby, and the body surface area exposed to the light. Commercially available phototherapy systems include those that deliver light via fluorescent bulbs, halogen quartz lamps, light-emitting diodes, and fiberoptic mattresses. Proper nursing care enhances the effectiveness of phototherapy and minimizes complications. Caregiver responsibilities include ensuring effective irradiance delivery, maximizing skin exposure, providing eye protection and eye care, careful attention to thermoregulation, maintaining adequate hydration, promoting elimination, and supporting parent-infant interaction. KEY WORDS: bilirubin, hyperbilirubinemia, jaundice, neonatal intensive care, newborn, phototherapy, premature infant P hototherapy is the use of visible light for the treatment of hyperbilirubinemia, or jaundice, in the newborn. 1 It is perhaps the most com- mon nonroutine therapy applied in the newborn population. How phototherapy came to be is a fasci- nating story, with a nurse at its center. 2 Sister Ward, the nurse in charge of the Premature Unit at Rochford General Hospital in Essex, England, firmly believed in the restorative powers of fresh air and sunshine (Figure 1). On sunny days, she would wheel the infants outdoors into the hospital court- yard, returning them to the nursery just before the doctors—who were not as keen on this practice— arrived for ward rounds. One day in 1956, Sister Ward showed the physicians an undressed infant whose skin was pale except for a triangular area that appeared much yellower than the rest of its body. Originally published in the December 2006 issue of Advances in Neonatal Care. This version has been revised and updated August 2011 by the author.
Transcript of Fundamentals of Phototherapy for Neonatal Jaundice · Neonatal jaundice expert Maisels suggests...

S10 Advances in Neonatal Care • Vol. 11, No. 5S • pp. S10-S21
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
Fundamentals of Phototherapy forNeonatal Jaundice
Laura A. Stokowski, MS, RN
Dr R. H. Dobbs asked her if she had painted thebaby’s skin with iodine. She denied having done so,telling him that what she held in her arms was a jaun-diced infant whose color had faded except in an areathat had been covered by the corner of a sheet.2
Subsequently, physicians and scientists at RochfordHospital discovered that the levels of bilirubin pig-ment in tubes of blood left sitting in the sun alsodropped dramatically. Putting these observationstogether, the idea of phototherapy for neonatal jaun-dice was born. The very first phototherapy unit incor-porating an artificial light source instead of naturalsunlight was devised and tested by Cremer et al3 atRochford Hospital, and the results were reported inThe Lancet, in 1958 (Figure 2).
Phototherapy was not used in the United Statesuntil the landmark study of Lucey et al4 was pub-lished in Pediatrics a full decade later. This random-ized controlled trial demonstrating the effectivenessof phototherapy led to its acceptance as a simple,inexpensive, and relatively safe way to preventhyperbilirubinemia in premature infants.
NORMAL BILIRUBIN METABOLISM
Humans continuously form bilirubin, and newborninfants produce relatively more bilirubin than any
AAuutthhoorr AAffffiilliiaattiioonnss:: Inova Fairfax Hospital for Children, FallsChurch, VirginiaCCoorrrreessppoonnddeennccee:: Laura A. Stokowski, MS, RN, 8317 ArgentCircle, Fairfax Station, VA 22039 ([email protected]).
Copyright © 2011 by The National Association of Neonatal Nurses
DOI: 10.1097/ANC.0b013e31822ee62c
ABSTRACTPhototherapy is the use of visible light for the treatment of hyperbilirubinemia in the newborn. This relatively commontherapy lowers the serum bilirubin level by transforming bilirubin into water-soluble isomers that can be eliminatedwithout conjugation in the liver. The dose of phototherapy is a key factor in how quickly it works; dose in turn is deter-mined by the wavelength of the light, the intensity of the light (irradiance), the distance between the light and the baby,and the body surface area exposed to the light. Commercially available phototherapy systems include those that deliverlight via fluorescent bulbs, halogen quartz lamps, light-emitting diodes, and fiberoptic mattresses. Proper nursing careenhances the effectiveness of phototherapy and minimizes complications. Caregiver responsibilities include ensuringeffective irradiance delivery, maximizing skin exposure, providing eye protection and eye care, careful attention tothermoregulation, maintaining adequate hydration, promoting elimination, and supporting parent-infant interaction.KEY WORDS: bilirubin, hyperbilirubinemia, jaundice, neonatal intensive care, newborn, phototherapy, premature infant
Phototherapy is the use of visible light for thetreatment of hyperbilirubinemia, or jaundice,in the newborn.1 It is perhaps the most com-
mon nonroutine therapy applied in the newbornpopulation. How phototherapy came to be is a fasci-nating story, with a nurse at its center.2
Sister Ward, the nurse in charge of the PrematureUnit at Rochford General Hospital in Essex, England,firmly believed in the restorative powers of fresh airand sunshine (Figure 1). On sunny days, she wouldwheel the infants outdoors into the hospital court-yard, returning them to the nursery just before thedoctors—who were not as keen on this practice—arrived for ward rounds. One day in 1956, SisterWard showed the physicians an undressed infantwhose skin was pale except for a triangular area thatappeared much yellower than the rest of its body.
Originally published in the December 2006 issue of Advances in Neonatal Care. This version has been revised and updated August 2011 by the author.
ANC200224.qxp 8/24/11 3:03 AM Page 10

Advances in Neonatal Care • Vol. 11, No. 5S
Fundamentals of Phototherapy for Neonatal Jaundice S11
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
other age group. The typical bilirubin load of thenewborn is quite high, 2 to 3 times that of an adult.Bilirubin is a product of the normal destruction of cir-culating erythrocytes (which have a shortened lifes-pan in the newborn infant) and increased turnover ofcytochromes.5 Some infants have excessive bilirubinproduction, and a correspondingly elevated load ofunconjugated bilirubin (Table 1).
Unconjugated bilirubin is lipid-soluble and mustbe transported to the liver in the plasma, boundreversibly to albumin.6 In the liver, bilirubin is trans-ported across hepatic cell membranes, where it bindsto ligandin for conjugation. A liver enzyme, uridinediphosphoglucuronate glucuronosyltransferase, con-jugates bilirubin, converting it to water-soluble biliru-bin pigments that can be excreted into the bile andexit the body via the intestines, or, to a lesser degree,filtered through the kidneys (Figure 3). Bilirubin pig-ments in the gut that are not eliminated can be reab-sorbed into the circulation as unconjugated bilirubin,
essentially recycling the bilirubin load, a processcalled enterohepatic recirculation. Thus, babies withreduced conjugation or elimination of bilirubin arealso at risk for hyperbilirubinemia (Table 1). A moredetailed explanation of newborn bilirubin metabo-lism can be found in an article in the April 2002 issueof this journal.7
HOW PHOTOTHERAPY WORKS
Phototherapy converts bilirubin that is present in thesuperficial capillaries and interstitial spaces of theskin and subcutaneous tissues to water-soluble iso-mers that are excretable without further metabolismby the liver (Figure 4). Neonatal jaundice expertMaisels suggests that phototherapy is much like apercutaneous drug.6,8 When phototherapy illumi-nates the skin, an infusion of discrete photons ofenergy are absorbed by bilirubin much like a drugmolecule binds to a receptor. Bilirubin molecules inlight-exposed skin undergo relatively quick photo-chemical reactions—configurational isomerization,
FIGURE 1.
Miss Jean Ward, in 1956, with one of the earliest
infants given phototherapy at Rochford General
Hospital. Courtesy of BMJ Publishing Group.
FIGURE 2.
The first artificial light apparatus devised for cradle
illumination of infants at Rochford General Hospital.
The hemicylindrical stainless steel reflector, suspended
on a height-adjustable moveable gantry, contains
eight 24-in light blue 40-W fluorescent tubes spaced
2 in apart. A cot can be wheeled underneath the
reflector, and the lights can be switched on separately
to vary the amount of power delivered.3 Reprinted
with permission.
ANC200224.qxp 8/24/11 3:03 AM Page 11
www.advancesinneonatalcare.org
S12 Stokowski
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
structural isomerization, and photooxidation—toform nontoxic, excretable isomers. These bilirubinisomers have different shapes than the native isomer,are more polar, and can be excreted from the liverinto the bile without undergoing conjugation orrequiring special transport for their excretion.9Urinary and gastrointestinal elimination remainimportant to the process of reducing the bilirubinload.
WHEN IS PHOTOTHERAPY PRESCRIBED?
The aim of phototherapy is to curtail rising serumbilirubin and prevent its toxic accumulation in thebrain, where it can cause the serious, permanentneurological complication known as kernicterus.Where the technology is readily available, pho-totherapy has nearly abolished the need for
exchange transfusion to treat hyperbilirubinemia.Phototherapy is typically used either prophylacti-cally or therapeutically.
• In preterm infants or those with a knownhemolytic process, it is often used prophylacti-cally, to prevent a significant rise in serumbilirubin.
• In late-preterm and full-term infants, it is admin-istered at therapeutic doses to reduce excessivebilirubin levels and avoid development ofbilirubin encephalopathy.
The photoisomerization of bilirubin begins almostinstantaneously when the skin is exposed to light.8Unlike unconjugated bilirubin, the photoproducts ofthese processes are not neurotoxic.8 Therefore, the mostimportant intervention for the severely hyperbilirubine-mic infant is to initiate phototherapy without delay.
TABLE 1. Mechanisms of Hyperbilirubinemia
(1a) Increased Bilirubin Production (1b) Impaired Conjugation or Excretion
Hemolytic disease of the newborn Inadequate or poor feeding intake
• Rh isoimmunization • Prematurity (�39 weeks)
• ABO incompatibility • Delayed or impaired lactogenesis
• Minor blood group incompatibility • Inadequate milk transfer
• Other feeding disorders
Polycythemia Increased enterohepatic circulation
• Intestinal obstruction
• Meconium ileus
• Meconium plugging
• Cystic fibrosis
Red blood cell enzyme disorders Hormonal deficiencies
• G6PD deficiency • Hypothyroidism
• Pyruvate kinase deficiency • Hypopituitarism
Red blood cell membrane defects Disorders of bilirubin metabolism
• Hereditary spherocytosis • Crigler-Najjar syndrome I and II
• Gilbert disease
• Lucey-Driscoll syndrome
Birth trauma
• Vacuum or instrumented delivery
• Bruising
• Cephalohematoma or subgaleal bleed
Neonatal infection
• Urinary tract infection
• Sepsis
Ethnicity
• Asian ethnic background
ANC200224.qxp 8/24/11 3:03 AM Page 12

Advances in Neonatal Care • Vol. 11, No. 5S
THE IMPORTANCE OF DOSE
A robust relationship exists between the dose of pho-totherapy and the rate of decline in serum bilirubinlevel.8 Dose of phototherapy is determined by severalkey factors:
• Spectral qualities of the light source used (wave-length range and peak);
• Intensity of the light (irradiance);• Distance between the light and the infant’s skin;• Body surface area exposed by the irradiated
field or “footprint.”
Spectral QualitiesThe most effective light sources for degrading biliru-bin emit light in a relatively narrow wavelengthrange (400 to 520 nanometers, or nm), with a peak of460 � 10 nm.1 At these wavelengths, light penetratesthe skin well and is maximally absorbed by biliru-bin.8 Blue, green, and turquoise light (the blue-greenspectrum) are considered the most effective, andsome evidences suggest that given equal irradiancelevels, the turquoise spectral range is more efficientin reducing bilirubin than blue because of greaterskin penetration.9
FIGURE 3.
Neonatal bilirubin metabolism. From Stokowski.7 Reprinted with permission.
Fundamentals of Phototherapy for Neonatal Jaundice S13
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
ANC200224.qxp 8/24/11 3:03 AM Page 13

www.advancesinneonatalcare.org
S14 Stokowski
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
A popular, but mistaken belief holds that pho-totherapy delivers ultraviolet light. The phototherapysystems currently used for newborn infants do notemit significant amounts of ultraviolet radiation.8
IrradianceIrradiance is the light intensity, or number of photonsdelivered per square centimeter of exposed body sur-face. The delivered irradiance determines the effec-tiveness of phototherapy; the higher the irradiance,the faster the decline in serum bilirubin level.10
Spectral irradiance, quantified as �W/cm2/nm,varies with the design of the light source. It can bemeasured with a spectral radiometer sensitive to theeffective wavelength of light. Intensive phototherapyrequires a spectral irradiance of 30 �W/cm2/nm,delivered over as much of the body surface aspossible.
Distance From LightLight intensity is inversely related to the distancebetween the light and the body surface. A simple
way to increase irradiance is to move the light closerto the infant. Caution must be exerted when posi-tioning halogen phototherapy lamps, which cannotbe positioned closer to the infant than recommendedby their manufacturers without incurring the risk fora burn.11
Exposed Body Surface AreaThe greater the body surface area exposed to light,the faster the decline in serum bilirubin. Many lightsources used in neonatal care do not expose a suffi-cient area of skin to the light. The light source mayhave an adequate spectral irradiance in the center ofthe light’s footprint; however, irradiance decays sig-nificantly at the periphery of the light.12 The result isthat only an insufficient proportion of the infant’sbody surface area receives effective treatment. Thisproblem can be solved by positioning the infantproperly within the footprint of the light or usingmultiple light sources for coverage of at least 80% ofthe body surface13 (Figure 5).
The size of the exposed body surface area, alongwith the level of irradiance, determines the spectralpower of the phototherapy application, which in turninfluences its effectiveness.14 The larger the exposedbody surface and stronger the light, the higher thespectral power.
COMPARING AND CONTRASTINGPHOTOTHERAPY DELIVERY SYSTEMS
A number of different light sources are commer-cially available for neonatal phototherapy. Each hasits own advantages and disadvantages. Different
FIGURE 4.
The mechanism of phototherapy. When bilirubin mol-
ecules absorb light, 2 main photochemical reactions
occur: Native 4Z, 15Z-bilirubin converts to 4Z, 15E
bilirubin (also known as photobilirubin) and to lumiru-
bin. Unlike 4Z, 15Z bilirubin, photobilirubin can be
excreted via the liver without conjugation, but its
clearance is very slow and its conversion is reversible.
In the bowel (away from the light), photobilirubin is
converted back to native bilirubin. Lumirubin is not
reversible. So, although much less lumirubin than
photobilirubin is formed, lumirubin is cleared from the
serum much more rapidly, and it is likely that lumirubin
formation is primarily responsible for the decline in
serum bilirubin that results from phototherapy. Small
amounts of native bilirubin are also oxidized to
monopyrroles and dipyrroles that can be excreted in
the urine. This is a slow process and only a minor
contributor to the elimination of bilirubin during
phototherapy. Diagram courtesy of Mary Puchalski.
FIGURE 5.
Two halogen spotlight are used to provide more
complete coverage. Note that the lights are not
superimposed over the same area of skin but are
used to provide coverage over different body surface
areas on this large infant.
ANC200224.qxp 8/24/11 3:03 AM Page 14
Advances in Neonatal Care • Vol. 11, No. 5S
Fundamentals of Phototherapy for Neonatal Jaundice S15
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
neonatal phototherapy systems achieve vastly differ-ent irradiance levels, and this can influence their clin-ical effectiveness.12
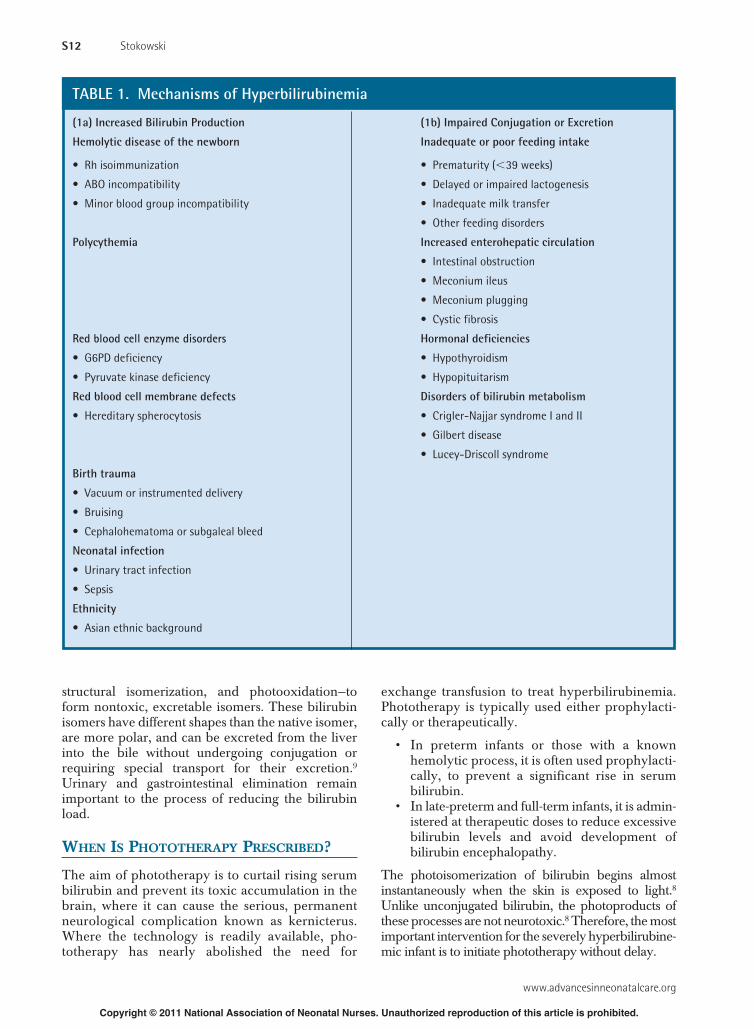
Combined phototherapy is often the treatment ofchoice for very preterm infants with hyperbilirubine-mia, because it has been shown to achieve lower serumbilirubin levels with a shorter duration of treatment, andto significantly reduce exchange transfusions.15 Onemethod frequently employed to provide combinationphototherapy is to use an overhead unit above the infant(fluorescent bank light, gallium nitride light-emittingdiode [LED], or halogen lamp) and a fiberoptic mattress
underneath the infant. A commercially available systemcombines banks of fluorescent tubes on each side, witha transparent mattress containing fan-cooled fluorescentbulbs (Bili-Bassinet, Natus Medical Incorporated, SanCarlos, California) (Figure 6).
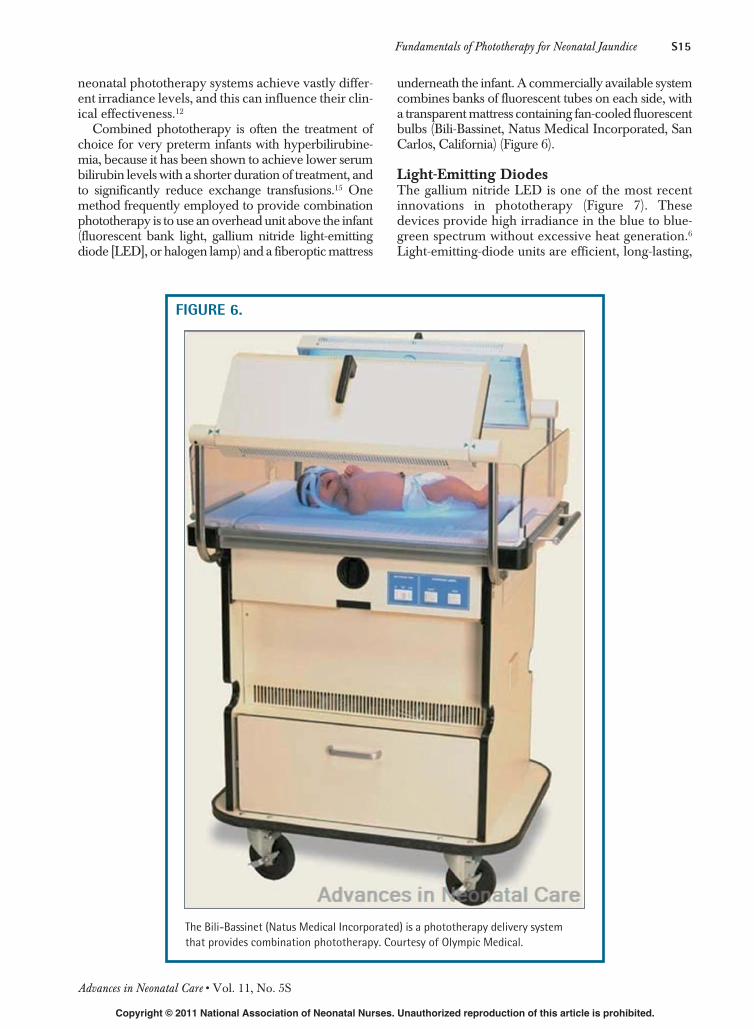
Light-Emitting DiodesThe gallium nitride LED is one of the most recentinnovations in phototherapy (Figure 7). Thesedevices provide high irradiance in the blue to blue-green spectrum without excessive heat generation.6Light-emitting-diode units are efficient, long-lasting,
FIGURE 6.
The Bili-Bassinet (Natus Medical Incorporated) is a phototherapy delivery system
that provides combination phototherapy. Courtesy of Olympic Medical.
ANC200224.qxp 8/24/11 3:03 AM Page 15
www.advancesinneonatalcare.org
S16 Stokowski
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
and cost-effective.1 The latest models incorporateamber LEDs to counteract the “blue hue” effect thatcan irritate caregivers.1
Halogen Spot LightsHalogen lamp sources deliver phototherapy using 1 ormore quartz halogen bulbs (Figure 8). It is possible toachieve sufficient irradiance with halogen light sources;however, devices designed with a single lamp produce acircle of light with high irradiance only in the center.Halogen systems are compact and caregiver-friendly;however, quartz halogen bulbs carry the disadvantage ofgenerating significant amounts of heat. Manufacturer’srecommendations for safe maximal distance should befollowed.11 A newer device that incorporates a metalhalide bulb (Giraffe SPOT PT Lite, GE Healthcare,Waukesha, Wisconsin) is an improvement over earlierhalogen spotlights. The light source is located in a lightbox, away from the infant, resulting in a cooler light sur-rounding the infant. This high-intensity light is transmit-ted through a light pipe in a flexible gooseneck that canbe adjusted for maximum light footprint.
Fluorescent TubesOften referred to as “bank lights,” fluorescent tubephototherapy devices have been around the longest(Figure 9). It is vital to realize, however, that not allfluorescent tubes are the same. Dramatic differencesexist in the irradiance produced by different types offluorescent tubes, even within the same 425- to 475-nmwavelength.11 Bulbs used in this type of phototherapyunit include daylight, cool-white, blue, “special blue”(the most effective), or a combination of these. Onesystem contains 6 blue tubes and 2 white tubes withan optional on/off switch. Caregivers are often both-ered by the blue-hue effect produced by all bluetubes, and the blue light can impair assessment ofinfant skin color. The white light tubes in this unit canbe switched on to minimize the blue-hue effect with-out hindering the effectiveness of the phototherapytreatment.
Fluorescent tube units are often positioned toofar away from the infant to be effective. They shouldbe positioned as close to the infant as possible.8Maisels recommends that these units be placed 10 cm
FIGURE 7.
Phototherapy system that comprises a light-emitting diode and the option to
switch between single or double phototherapy at the touch of a button (NeoBlue,
Natus Medical Inc, San Carlos, California). Courtesy of Natus Medical Inc.
ANC200224.qxp 8/24/11 3:03 AM Page 16

Advances in Neonatal Care • Vol. 11, No. 5S
Fundamentals of Phototherapy for Neonatal Jaundice S17
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
above nude full-term infants in bassinets for effectivephototherapy. This method achieves an irradiance of50 �W/cm2 while maintaining normal body temper-ature8 and has been successfully implemented injaundiced infants 37 or more weeks’ gestation.16
Fiberoptic BlanketsFiberoptic devices contain a tungsten-halogen bulbthat delivers light via a cable into a plastic pad con-taining fiberoptic fibers (Figure 10). The padremains cool and can be placed directly under aninfant to increase the skin surface area that isexposed. The pad can also be wrapped around theinfant’s midsection to provide phototherapy whilethe infant is being held. Because the spectral powerof the pad alone is low, it is commonly used in con-junction with overhead lights to provide doublephototherapy.
NURSING CARE OF THE INFANTRECEIVING PHOTOTHERAPY
Phototherapy is much more than just switching on alight. The efficiency with which phototherapy achievesa decline in serum bilirubin level is in large part deter-mined by nursing care. Appropriate nursing care alsominimizes the potential side effects and complicationsof phototherapy.
Ensure Effective IrradiancePosition phototherapy lamps or mattresses to providethe most complete skin exposure possible. Lightsources should be as close to the infant as possible,with the exception of halogen-lamp phototherapyunits. Overhead units that incorporate rubberized feetto rest on the incubator surface should be lowereduntil they are in contact with the top of the incubator.
Periodic checks of spectral irradiance produced bydifferent phototherapy units should be conducted toensure adequate irradiance delivery.11 Irradiance ismeasured with a radiometer, an instrument that
FIGURE 8.
Halogen spot light phototherapy system. Courtesy of
GE Healthcare. Reprinted with permission.
FIGURE 9.
Phototherapy systems that incorporate fluorescent
tubes. Conventional bank lights (A) can be positioned
over an infant in a bassinet or incubator. Courtesy of
Olympic Medical. An overhead system that combines
blue and white tubes is both effective and caregiver
friendly (B). Courtesy of Draeger Medical. With the
BiliBed (C), the infant lays on a soft mattress of fluo-
rescent tubes, receiving high-intensity phototherapy
from below. Courtesy of Medela, Inc.
A
B
ANC200224.qxp 8/24/11 3:03 AM Page 17

www.advancesinneonatalcare.org
S18 Stokowski
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
gauges light in the effective wavelength for pho-totherapy (Figure 11). Measurements do vary amongdifferent radiometers; use the instrument recom-mended by the manufacturer of the correspondingphototherapy system.
Measured irradiance can vary widely dependingon where the measurement is taken.11 Irradiance inthe center of the illuminated area can be double thatof the periphery.11 It is preferable to take severalmeasurements in the illuminated area at infant skinlevel and average them for a determination of overalleffective irradiance.8
It is fairly common to see terms such as “single,”“double,” and “triple” used in orders prescribingphototherapy. Such terms refer only to how manypieces of equipment should be used to deliver pho-totherapy, and not to a specific target dose, or irradi-ance level. In other words, “single phototherapy” is1 phototherapy unit, “double” is 2 units, and so forth.Naturally, it is hoped that 2 phototherapy units will
deliver more efficient phototherapy than a singleunit, probably through improved skin coverage.However, no standard definitions of “single,” “dou-ble,” and “triple” phototherapy describe photother-apy dosages in terms of target irradiance levels.
Provide Eye ProtectionOpaque eye shields must be used during photother-apy to protect the infant’s eyes from retinal damage(Figure 12). To adequately block the transmission oflight, carefully apply eye coverings by first closing theinfant’s eyes and then applying shields securely.Avoid eye patches that are too tight, as they mayapply undue pressure to the infant’s delicate eye. Turnoff the phototherapy unit and remove eye patchesperiodically to assess eyes for drainage, edema, andevidence of infection, to provide visual stimulation,and to encourage parent-infant interaction as appro-priate on the basis of the infant’s clinical status.
Complications of using eye patches include apnea(from displaced eye patches obstructing the nares),eye irritation, corneal abrasion, blocked tears ducts,and conjunctivitis.17 Proper eye care is essential.Gently clean the infant’s eyes with sterile cotton orsoft gauze moistened with sterile water or saline, start-ing with the inner canthus of the eye and moving out-ward in a single, smooth stroke. A separate cleansingpad should be used for each eye. Gloves should beworn when providing eye care. A clean internal layershould be inserted or patches should be changed atregular intervals.
Assess Skin ExposureThe largest surface area of the infant’s body, thetrunk, should be positioned in the center of the light,where irradiance is highest. In most cases, it is notnecessary to remove diapers or boundary materialsused for postural support while providing photother-apy. Removing diapers and nesting materials around
FIGURE 10.
Fiberoptic blanket phototherapy system. Courtesy of
GE Healthcare.
FIGURE 12.
Properly positioned phototherapy eye shields.
FIGURE 11.
Using a radiometer to measure irradiance level during
phototherapy.
ANC200224.qxp 8/24/11 3:03 AM Page 18

Advances in Neonatal Care • Vol. 11, No. 5S
Fundamentals of Phototherapy for Neonatal Jaundice S19
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
jaundiced, low-risk preterm infants weighing morethan 1500 g at birth does not shorten the length oftreatment.18 It is not known, however, whether dia-pers and/or boundary materials affect the bilirubindecline in smaller, less mature infants or in larger,more mature infants with severe hyperbilirubinemia.
The American Academy of Pediatrics recom-mends removing diapers for intensive phototherapy,when the serum bilirubin is approaching exchangetransfusion level.11 Light-permeable diapers are alsocommercially available (BiliBottoms, CAS MedicalSystems, Inc, Branford, Connecticut).
Proper PositioningFrequent turning to expose different areas of skin hasnot been shown to improve the effectiveness of con-ventional (single) phototherapy.19-21
One study actually reported that the serum biliru-bin levels of infants maintained in a supine positionwithout turning declined significantly faster thanthose of infants who were turned prone/supine every2 to 3 hours.20
Assess and Adjust Thermoregulation DevicesSome phototherapy units can cause a significantincrease in the infant’s body temperature.22 Whenphototherapy is directed over an incubator, immedi-ate and sustained fluctuations can occur in the thermalenvironment.23 Thermal instability can occur whenusing either the skin- or air-control mode of the incu-bator. With inadequate monitoring, vigilance, andadjustments to the thermal environment, the infantcan easily develop hypothermia or hyperthermiaduring phototherapy.
When phototherapy is initiated during air controlmode, a rapid rise in body temperature usually neces-sitates a downward adjustment in the air temperatureset point. When phototherapy is discontinued, the airtemperature set point may require an upward read-justment to compensate for the loss of heat from thephototherapy lights.
During skin control mode, the air temperature usu-ally drops when phototherapy is initiated because theadditional heat warms the infant, and less environmen-tal heat support is required. Using skin control modeis generally preferred during phototherapy becausethis automatic compensatory mechanism keeps theinfant’s body temperature within normal limits as longas the lights remain on. However, if the lights areturned off abruptly, the infant’s temperature can alsodrop precipitously. It will then take some time for theair temperature to rise again and rewarm the infant.
Promoting Elimination and Skin IntegrityThe photoproducts of bilirubin require eliminationfrom the body in the stool or urine. Some of the pho-tochemical reactions induced by phototherapy arereversible, meaning that the isomers can be con-
verted back to unconjugated bilirubin if they are noteliminated in the stool.6 Enteral feeding is essentialto promote stooling in hyperbilirubinemic infants.Lumirubin, an irreversible product of structural iso-merization of bilirubin, is excreted in the urine aswell as in the bile, so an adequate urine output is alsoimportant. An ongoing assessment of the infant’surine output is an important measure not only ofhydration but also of elimination of bilirubin. Theinfant’s urine may appear dark in color as bilirubinelimination increases.
Watery stools and diarrhea have been observed ininfants undergoing phototherapy. These characteris-tic dark greenish stools are related to the increasedexcretion of unconjugated bilirubin from the intes-tines.6 Protective skin care is necessary to preventperianal skin breakdown from watery stools.
HydrationSeveral studies have documented an increase intransepidermal water loss during phototherapy.24,25
Excessive fluid losses via the skin are of particularconcern in the smallest, most immature infants dur-ing the first week of life. These losses can be exacer-bated by phototherapy, although insensible waterlosses are not as high with fiberoptic or LED pho-totherapy devices.5 Increasing fluid intake has beenshown to shorten the duration of phototherapy infull-term neonates.26 Some infants may experienceintestinal fluid losses from a high volume of loosestools during phototherapy. Although it is importantto maintain adequate hydration, routine supplemen-tation with intravenous fluids is not recommended.6For breastfed infants with evidence of dehydration,supplementation with a milk-based formula inhibitsthe enterohepatic circulation of bilirubin and mayimprove the efficacy of phototherapy.6
Maintaining fluid balance by increasing incubatorhumidity might also be counterproductive, especiallyif high levels of humidity are used. A recent study27
found that when humidification was set at more than90%, irradiance delivery from an LED phototherapyunit was reduced by 15% and that from a halogenphototherapy unit by 45%. The mist and water con-densation within the incubator are postulated tointerfere with irradiance delivery.
Promoting Parent-Infant InteractionsPhototherapy necessarily separates the neonate fromits mother and may interfere with the process of estab-lishing lactation. Unless jaundice is severe, photother-apy can be safely be interrupted at feeding time toallow continuation of breastfeeding, parental visits,and skin-to-skin care.6 Remove the eye patches duringthese visits. If the serum bilirubin level is approachingthe exchange transfusion threshold, and/or if theinfant has escalating pathologic jaundice, photother-apy should be continuously maintained.6
ANC200224.qxp 8/24/11 3:03 AM Page 19

www.advancesinneonatalcare.org
S20 Stokowski
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
Monitoring Bilirubin LevelsThe most significant decline in bilirubin level occursin the first 4 to 6 hours after initiating phototherapy.Conventional (single) phototherapy can decrease theserum bilirubin by up to 22% in the first 24 hours oftreatment. Double phototherapy can produce a fall ofas much as 29% in the first 24 hours,28 and intensivephototherapy can lower the bilirubin level by asmuch as 5 mg/dL/h (85 �mol/L/h) In infants withrapidly rising bilirubin levels, stabilizing the bilirubinlevel or slowing its rate of rise should be consideredvalid measures of the success of therapy.29
Phototherapy lamps must be turned off whiledrawing blood samples for serum bilirubin testing,because the lights will act on the bilirubin pigmentsin the blood sample, causing the bilirubin level todecline, thereby providing erroneous data to the careteam.3 Transcutaneous bilirubinometry can also beused for the evaluation of bilirubin levels in infantsreceiving phototherapy by using the unexposed skinof the forehead, under the infant’s eye patches, forthese measurements.30
After discontinuing phototherapy the bilirubinlevel often rises slightly, a phenomenon known as“rebound.” Rebound hyperbilirubinemia is usually anelevation of no more than 1 to 2 mg/dL31,32; however,postphototherapy rebound to clinically significantlevels can occur.33 Infants at greatest risk of significantpostphototherapy rebound in serum bilirubin levelsrequiring closer follow-up include the following:
• Premature infants;• Infants with ongoing hemolysis (ie, positive
direct Coombs tests);• Infants treated before 72 hours of age.33
A serum bilirubin measurement obtained 24 hoursafter discontinuation of phototherapy will detectrebound hyperbilirubinemia.32
INDICATIONS FOR INTENSIVEPHOTOTHERAPY
When an infant’s serum bilirubin is rising rapidly orapproaching exchange transfusion level, intensivephototherapy must be instituted at maximal spectralpower. This entails delivering high levels of irradi-ance (usually 30 �W/cm2/nm or higher) to as muchof the infant’s surface area as possible.1 The most effi-cient phototherapy units available should be used,and they should be positioned for maximum skincoverage. In these situations, additional surface-areaexposure can be achieved by removing the infant’sdiaper and lining the sides of the bassinet, incubator,or radiant warmer with light-reflecting material suchaluminum foil or white linens.34 Intensive photother-apy can produce a decline in serum bilirubin of asmuch as 10 mg/dL within a few hours in severelyhyperbilirubinemic infants.35
Intensive phototherapy may have another, evenmore important benefit in an infant with a bilirubinlevel high enough to increase the risk for neurologi-cal damage.36 Almost as soon as the lights areswitched on, the process of isomerization of bilitubinbegins, converting bilirubin molecules into morepolar photoisomers, that are unable to cross theblood-brain barrier independently to gain access tothe neurons.35 Well before a measurable decline inserum bilirubin occurs, the effects of phototherapyare believed to protect the brain from the neurotoxiceffects of bilirubin, although no studies have yetproved this hypothesis.
LIMITATIONS OF HOME PHOTOTHERAPYAND SUNLIGHT
The irradiance and surface area exposure producedby home phototherapy units are lower than those pro-duced by typical hospital units11 making them less effi-cient at lowering the serum bilirubin level. Whether avalid indication for home phototherapy exists is ques-tionable; current guidelines state that a bilirubin highenough to warrant treatment should be managed inthe hospital.11 In the past, parents have sometimesbeen told to expose their jaundiced infants to sunlight.Notwithstanding phototherapy’s beginnings in thesunny courtyard of an English hospital, this practice isnot considered a safe or reliable way to treat jaun-dice.11 There are reports in the literature of infantsdeveloping kernicterus after their parents wereinstructed to treat their infants’ jaundice at home byexposing them to sunlight, in some cases for as little as15 minutes per day.37 Not only was this very likely tobe ineffective but also it probably contributed todelays in recognition of the severity of the hyperbiliru-binemia as well as delays in proper treatment.
ADVERSE EFFECTS OF PHOTOTHERAPY
The most noticeable clinical complication of pho-totherapy is “bronze baby syndrome,” a grayish-browndiscoloration of the skin that occurs exclusively ininfants with cholestatic jaundice.11 Bronze babysyndrome is believed to occur when the brown pho-toproducts of porphyrins, especially copper por-phyrins, accumulate in the skin and their excretion isimpaired by cholestasis.5 Phototherapy can damagered-blood-cell membranes, increasing their suscepti-bility to lipid peroxidation and hemolysis.1 Theseeffects may contribute to the pathogenesis of disor-ders common in the very low-birth-weight infant,including bronchopulmonary dysplasia, retinopathyof prematurity, and necrotizing enterocolitis.1Phototherapy has been associated with patency of theductus arteriosus38 and ileus in very low-birth-weightinfants,39 as well as retinopahty of prematurity.40
Recent evidence also suggests that phototherapy
ANC200224.qxp 8/24/11 3:03 AM Page 20

Advances in Neonatal Care • Vol. 11, No. 5S
Fundamentals of Phototherapy for Neonatal Jaundice S21
Copyright © 2011 National Association of Neonatal Nurses. Unauthorized reproduction of this article is prohibited.
impairs immune system function through alterationsof cytokine production.41 Phototherapy has beenlinked to the development of abnormal melanocyticnevi when the children become older. The evidencefor this association is not definitive and has beendebated, but at this time, this possible effect cannot beruled out.42 Although it is not always possible to sepa-rate the effects of phototherapy from the effects ofhyperbilirubinemia itself, recent research has impli-cated phototherapy as a risk factor for childhoodasthma.43 Other rare side effects include purpura andbulbous eruptions, which can occur in infants with ele-vated direct bilirubin. Phototherapy is contraindicatedin infants with congenital erythropoietic porphyria,because blistering and photosensitivity can result.5
CONCLUSION
For more than 40 years, phototherapy has been thestandard of care for the treatment of hyperbilirubine-mia in the newborn. In retrospect, phototherapy mayhave prevented nearly as much morbidity and mor-tality in neonatal care as the use of oxygen and hascertainly done so with fewer complications. Becausewe have become so comfortable with this simpletherapy, however, we must guard against becomingcomplacent about the disorder that we are treating.Hyperbilirubinemia in term and preterm infants can,in rare instances, lead to serious complications. It isessential that neonatal caregivers utilize photother-apy to its fullest potential when treating the commonbut not always benign problem of neonatal hyper-bilirubinemia.
References1. Vreman HJ, Wong RJ, Stevenson DK. Phototherapy: current methods and future
directions. Semi Perinatol. 2004;28:326-333.
2. Dobbs RH, Cremer RJ. Phototherapy. Arch Dis Child. 1975;50:833-836.
3. Cremer RJ, Perryman PW, Richards DH. Influence of light on the hyperbilirubinemia
of infants. Lancet 1958;1:1094-1097.
4. Lucey J, Ferriero M, Hewitt J. Prevention of hyperbilirubinemia of prematurity by
phototherapy. Pediatrics. 1968;41:1047-1054.
5. Wong RJ, DeSandre GH, Sibley E, Stevenson DK. Neonatal jaundice and liver
disease. In: Fanaroff AA, Martin RJ, Walsh MC, eds. Fanaroff and Martin’sNeonatal-Perinatal Medicine: Diseases of the Fetus and Infant. Philadelphia, PA:
Mosby; 2006:1419-1452.
6. Maisels MJ. Jaundice. In: MacDonald MG, Mullett MD, Seshia MMK, eds. Avery’sNeonatology. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:768-846.
7. Stokowski LA. Early recognition of neonatal jaundice and kernicterus. AdvNeonatal Care. 2002;2:101-114.
8. Maisels MJ, McDonagh AF. Phototherapy for neonatal jaundice. N Engl J Med.
2008;358:920-928.
9. Ebbesen F, Madsen P, Støvring S, Hundborg H, Agati G. Therapeutic effect of
turquoise versus blue light with equal irradiance in preterm infants with jaundice.
Acta Paediatr. 2007;96:837-841.
10. Tan KL. The pattern of bilirubin response to phototherapy for neonatal hyper-
bilirubinemia. Pediatr Res. 1982;16:670-674.
11. American Academy of Pediatrics, Subcommittee on Hyperbilirubinemia.
Management of hyperbilirubinemia in the newborn infant 35 or more weeks of
gestation. Pediatrics. 2004;114:297-316.
12. Hart G, Cameron R. The importance of irradiance and area in neonatal pho-
totherapy. Arch Dis Childhood Fetal Neonatal Ed. 2005;90:F437-F440.
13. Buhatin VK. Performance evaluation for neonatal phototherapy. Indian Pediatr.2009;46:19-21.
14. Hansen TW. Twists and turns in phototherapy for neonatal jaundice. ActaPaediatr. 2010;99:1117-1118
15. Romagnoli C, Zecca E, Pappaci P, Vento G, Girlando P, Latella C. Which pho-
totherapy system is most effective in lowering serum bilirubin in very preterm
infants? Fetal Diagn Ther. 2006;21:204-209.
16. Walker L, Vroman L, Becker J, Anderson F. Open crib phototherapy: using
evidence to change practice. Nurs Womens Health. 2007;11:402-404.
17. Fok TF, Wong W, Cheng AF. Use of eye patches in phototherapy: effects on
conjunctival bacterial pathogens and conjunctivitis. Pediatr Infect Dis J.1995;14:1091-1094.
18. Pritchard MA, Beller EM, Norton B. Skin exposure during conventional
phototherapy: a randomized controlled trial. J Paediatr Child Health. 2004;
40:270-274.
19. Chen C, Liu S, Lai C, Hwang C, Hsu H. Changing position does not improve
the efficacy of conventional phototherapy. Acta Paediatr Tw. 2002;43:255-
258.
20. Shinwell ES, Sciaky Y, Karplus M. Effect of position changing on bilirubin levels
during phototherapy. J Perinatol. 2002;22:226-229.
21. Donneborg ML, Knudsen KB, Ebbesen F. Effect of infants’ position on serum
bilirubin level during conventional phototherapy. Acta Paediatr. 2010;99:
1131-1134.
22. Pezzati M, Fusi F, Dani C, Piva D, Bertini G, Rubaltelli FF. Changes in skin temper-
ature of hyperbilirubinemic newborns under phototherapy: conventional versus
fiberoptic device. Am J Perinatol. 2002;19:439-444.
23. Dollberg S, Atherton HB, Hoath SB. Effect of different phototherapy lights on
incubator characteristics and dynamics under three modes of servocontrol. AmJ Perinatol. 1995;12:55-60.
24. Maayan-Metzger A, Yosipovitch G, Hadad E, Sirota L. Transepidermal water loss
and skin hydration in preterm infants during phototherapy. Am J Perinatol.2001;18:393-396.
25. Grunhagen DJ, De Boer MGJ, De Beaufort AJ, Walther FJ. Transepidermal water
loss during halogen spotlight phototherapy in preterm infants. Pediatr Res.
2002;51:402-405.
26. Mehta S, Kumar P, Narang A. A randomized controlled trial of fluid supplemen-
tation in term neonates with severe hyperbilirubinemia. J Pediatr. 2005;147:
781-785.
27. de Carvalho M, Torrao CT, Moreira ME. Mist and water condensation inside incu-
bators reduce the efficacy of phototherapy. Arch Dis Child Fetal Neonatal Ed.
2011;96:F138-F140.
28. Tan KL. Comparison of the efficacy of fiberoptic and conventional phototherapy
for neonatal hyperbilirubinemia. J Pediatr. 1994;125:607-612.
29. Hansen TW. Acute management of extreme neonatal jaundice—the potential
benefits of intensified phototherapy and interruption of enterohepatic bilirubin
circulation. Acta Paediatr. 1997;86:843-846.
30. Nanjundaswamy S, Petrova A, Mehta R, Hegyi T. Transcutaneous bilirubinom-
etry in preterm infants receiving phototherapy. Am J Perinatol. 2005;22:
127-131.
31. Maisels MJ, Kring E. Bilirubin rebound following intensive phototherapy. ArchPediatr Adolesc Med. 2002;156:669-672
32. Lazar L, Litwin A, Merlob P. Phototherapy for neonatal nonhemolytic hyper-
bilirubinemia. Analysis of rebound and indications for discontinuing therapy.
Clin Pediatr (Phila). 1993;32:264-267.
33. Kaplan M, Kaplan E, Hammerman C, et al. Post-phototherapy neonatal bilirubin
rebound: a potential cause of significant hyperbilirubinemia. Arch Dis Child.2006;91:31-34
34. Djokomuljanto S, Quah BS, Surini Y, et al. Efficacy of phototherapy for neonatal
jaundice is increased by the use of low-cost white reflecting curtains. Arch DisChild. 2006;91:F439-F442.
35. Hansen TW. The role of phototherapy in the crash-cart approach to extreme
neonatal jaundice. Semin Perinatol. 2011;35:171-174.
36. Ruud Hansen TW. Phototherapy for neonatal jaundice—therapeutic effects on
more than one level? Semin Perinatol. 2010;34:231-234
37. Centers for Disease Control and Prevention. Kernicterus in full-term infants—
United States, 1994-1998. Morbid Mortal Wkly Rep. 2001;50:491-494.
38. Barefield ES, Dwyer MD, Cassady G. Association of patent ductus arteriosus and
phototherapy in infants weighing less than 1000 grams. J Perinatol. 1993;13:
376-380.
39. Raghavan K, Thomas E, Patole S, Muller R. Is phototherapy a risk factor for ileus
in high-risk neonates? J Matern Fetal Neonat Med. 2005;18:129-131.
40. Xiong T, Qu Y, Cambier S, Mu D. The side effects of phototherapy for neonatal
jaundice: what do we know? What should we do? [published online ahead of
print April 1, 2011]. Eur J Pediatr. DOI: 10.1007/s00431-011-1454-1.
41. Kurt A, Aygun AD, Kurt AN, Godekmerdan A, Akarsu S, Yilmaz E. Use of
phototherapy for neonatal hyperbilirubinemia affects cytokine production and
lymphocyte subsets. Neonatology. 2009;95:262-266.
42. Brewster DH, Tucker JS, Fleming M, et al. Risk of skin cancer after neonatal
phototherapy: retrospective cohort study. Arch Dis Child. 2010;95:826-831.
43. Aspberg S, Dahlquist G, Kahan T, Källén B. Confirmed association between neona-
tal phototherapy or neonatal icterus and risk of childhood asthma. PediatrAllergy Immunol. 2010;24(4 part 2):733-739.
ANC200224.qxp 8/24/11 3:03 AM Page 21