Functional Manual Therapy for the Lower Quarter · Functional Manual Therapy for the Lower Quarter...
21
7/19/2013 Jack Miller 1 Functional Manual Therapy for the Lower Quarter Dr. Jack Miller, Western Univ., London, Canada Case history #1 • 25 y/o male auto plant worker • Wanting to train for weight lifting • C/O upper/mid back symptoms with doing weighted squats • Wants personal trainer advise on how to strengthen his upper back • What would you do? 2 Deep squat movement pattern 3 What do you observe? 4
-
Upload
trinhtuyen -
Category
Documents
-
view
221 -
download
4
Transcript of Functional Manual Therapy for the Lower Quarter · Functional Manual Therapy for the Lower Quarter...

7/19/2013
Jack Miller 1
Functional Manual Therapy for the Lower Quarter
Dr. Jack Miller, Western Univ., London, Canada
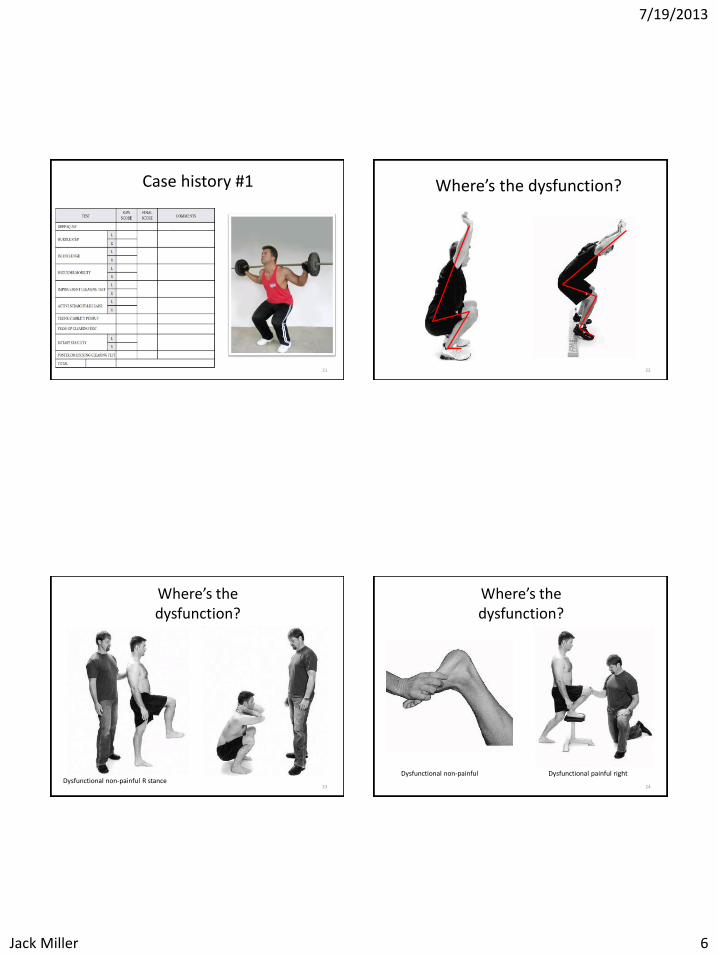
Case history #1
• 25 y/o male auto plant worker
• Wanting to train for weight lifting
• C/O upper/mid back symptoms with doing weighted squats
• Wants personal trainer advise on how to strengthen his upper back
• What would you do?
2
Deep squat movement pattern
3
What do you observe?
4
7/19/2013
Jack Miller 2
What do you observe?
5
Case history #2
• 23 year old university student
• 6 months increasing anterior knee pain
• No history of: injury, locking, giving way
• Worse after step aerobic class
• Wants personal trainer to help strengthen quadriceps muscles
• What would you do?
6
Hurdle step movement pattern
7
What do you observe?
8
7/19/2013
Jack Miller 3
What do you observe?
9
Case history #3
• 50 year old male accountant
• One year history increasing right-sided low back pain
• Described as general ache
• Worse with standing, walking, eased by sitting
• Wants personal trainer to work trunk core muscles
• What would you do?
10
In-line lunge movement pattern
11
What do you observe?
12

7/19/2013
Jack Miller 4
What do you observe?
13
With each of these cases
Functional movement loss 14
Functional Movement Loss
Tissue extensibility dysfunction
15
Tissue extensibility dysfunction resets
• Muscle shortening
• Trigger point activity
• Scarring and fibrosis
• Neural tissue
16
7/19/2013
Jack Miller 5
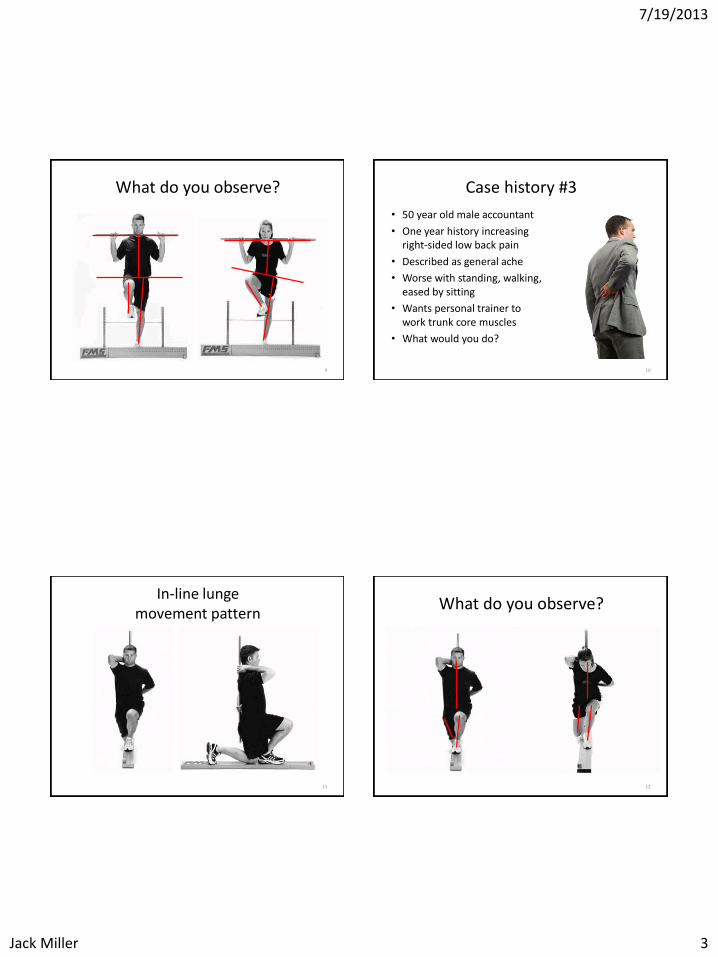
Functional movement loss
Tissue extensibility dysfunction
17
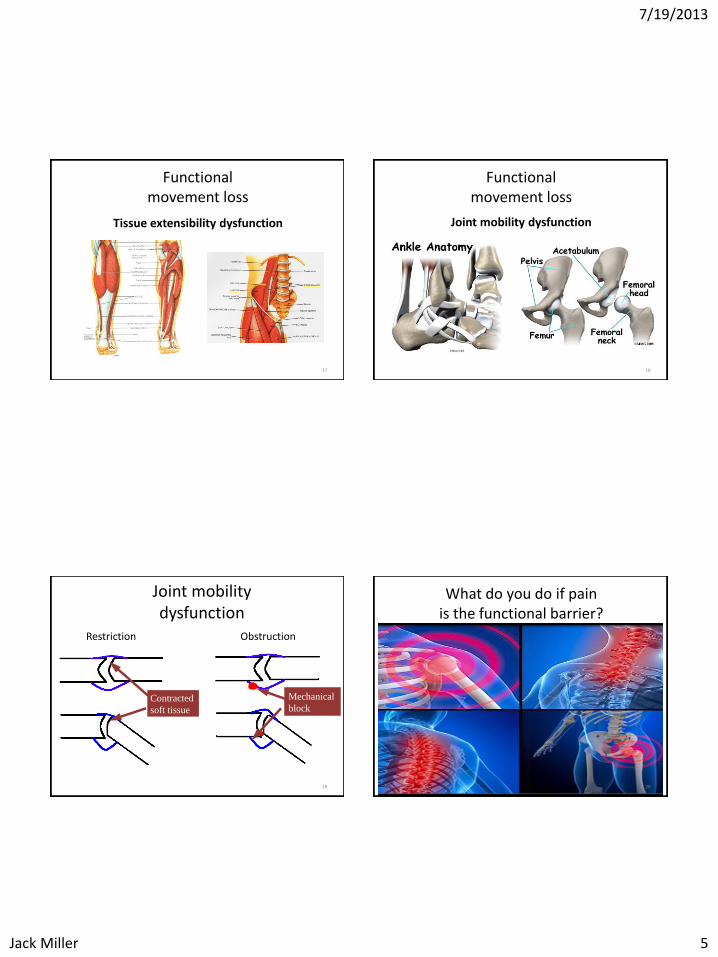
Functional movement loss
Joint mobility dysfunction
18
Joint mobility dysfunction
Obstruction
Mechanical
block
Restriction
Contracted
soft tissue
19
What do you do if pain is the functional barrier?
20
7/19/2013
Jack Miller 6
Case history #1
0 Right ankle pain 0
3
2
2
Poor control right stance
3 Poor control right ankle stance
2
2
3
3 3
- -
-
-
3
3
3
3
3
-
3
-
-
3
3
16
21
Where’s the dysfunction?
22
Where’s the dysfunction?
Dysfunctional non-painful R stance 23
Where’s the dysfunction?
Dysfunctional non-painful
Dysfunctional painful right
24

7/19/2013
Jack Miller 7
Analysis
• Dysfunctional and painful right ankle WB dorsiflexion
• Inability to squat due to loss of ankle dorsiflexion
• Mid-thoracic pain with weight lifting secondary to increased trunk flexion
25
Predicting short-term response to thrust and non-thrust manipulation and exercise
in patients post inversion ankle sprain
• Whitman, Cleland, Mintken, Keirns, Bieniek, Albin, Magel, McPoil
• JOSPT, Vol 39, No 3, March 2009
• Step-wise logistic regression to determine the most accurate set of variable for prediction of treatment success
26
Accuracy statistics with 95% CI for individual predictors
Variable Sensitivity
(95% CI)
Specificity
(95% CI)
+ve likelihood ratio
(95% CI)
Post-test
Probability
Worse when
standing
0.75 0.50 1.5 82%
Worse in
evening
0.46 0.75 1.8 84%
Navicular
drop 5.0
mm
0.77 0.48 1.4 81%
Distal tib-fib
joint
hypomobility
0.68 0.62 1.8 84%
27
MWM Ankle Dorsi-flexion (NWB)
• Mobilization
• Anterior glide distal tibia, talus fixated
• Movement
• Passive dorsiflexion
• Tips
• Useful in irritable cases
• Treatment plane is oblique med-lat.
28

7/19/2013
Jack Miller 8
The Initial Effects of a Mulligan’s Mobilization with Movement Technique on
Dorsiflexion and Pain in Sub acute Ankle Sprains
• Collins, N., Teys, P., Vincenzino B. • University of Queensland • Manual Therapy 9 (2004) • Double blind, randomized controlled trial • Incorporated • Repeated measures • Cross over design • Subjects acted as their own control
29
Study Subjects
• 16 participants, 8 male, 8 female
• Recruited from: Queensland University sports medicine clinic
• Average age 28.25 yrs (SD 9.33 yrs)
• Grade II lateral ankle sprain
• “Incomplete tear of the ATFL with mild laxity and instability and reduced function”
• Average duration 40 days (SD +/- 24 days)
30
Weight bearing ankle dorsi-flexion “lunge” mesurement
31
Outcome measures
Mobility function • Weight bearing dorsiflexion range Pain • Pressure pain threshold (PPT)
• Over proximal 1/3 of tibialis anterior muscle belly • Directly distal to the lateral maleolus over the CFL • Directly anterior to the lateral maleolus over the ATFL
• Thermal Pain Threshold (TPT) • Over the proximal 1/3 of tibialis anterior muscle belly • Directly anterior to the lateral maleolus over the ATFL
32

7/19/2013
Jack Miller 9
Study Results: Dorsiflexion
• MWM Treatment group • A significant interaction treatment
effect demonstrated for the MWM technique P=0.002
• Average increase from 57.27 to 68.93 cm.
• Placebo group • Average increase from 60.17 to
62.07 cm.
• Control group
• Average decrease from 58.29 to 56.42 cm.
0
10
20
30
40
50
60
70
80
Treatment Placebo Control
pre Rx
post Rx
33
Study Results: Pain
• Pressure Pain Threshold
• No significant interactive effects demonstrated
• Thermal Pain Threshold
• No significant effects demonstrated
34
Study Discussion
“MWM technique to patients with sub-acute lateral ankle sprains produced a significant immediate improvement in dorsiflexion but no initial effect on mechanical or thermal pain threshold”
“Current and previous research findings suggest the predominant mechanism of action for the dorsiflexion MWM technique is most likely mechanical rather that a direct hypoalgesic effect”
35
Talar subluxation
36

7/19/2013
Jack Miller 10
Initial changes in Posterior Talar Glide and Dorsi flexion of the Ankle After Mobilization with
Movement In Individuals with Recurrent ankle sprain
• JOSPT Vol 36 No 7 July 2006
• Vincenzino B., Branjerdporn M., et. al.
• University of Queensland St. Lucia
• Double –blind randomized crossover study with repeat measures including a no-treatment control condition
37
Outcome measures (dependent Variables)
• Posterior Glide • Method described by Denegar (JOSPT, 32: 166-173, 2002)
• Manual glide of talus with firm capsular end-feel • Measurement of tibial angulation measured with
inclinometer at end feel point
• Weight Bearing ankle Dorsi-flexion • Method described by Bennell (AJP 44(3): - 175-80 1998)
• Distance from tip of great toe to wall
• All measures taken prior to and following intervention
• All measures repeated 3 times
38
39
Independent variables
Weight bearing MWM (WB-MWM) • Subject in standing • Mobilization belt produced posterior glide of talus • 10 sec. hold at ERL • 4 repetitions with 20 sec rest between • 4 sets of 4 performed at each treatment session
Non-Weight bearing MWM (NWB-MWM) • Mobilization applied manually, subjects in supine • 10 sec. hold at ERL • 4 sets of 4 performed at each treatment session
No treatment group (control) • Standing in relaxed posture with no manual contact • Same time as per treatment groups
40
7/19/2013
Jack Miller 11
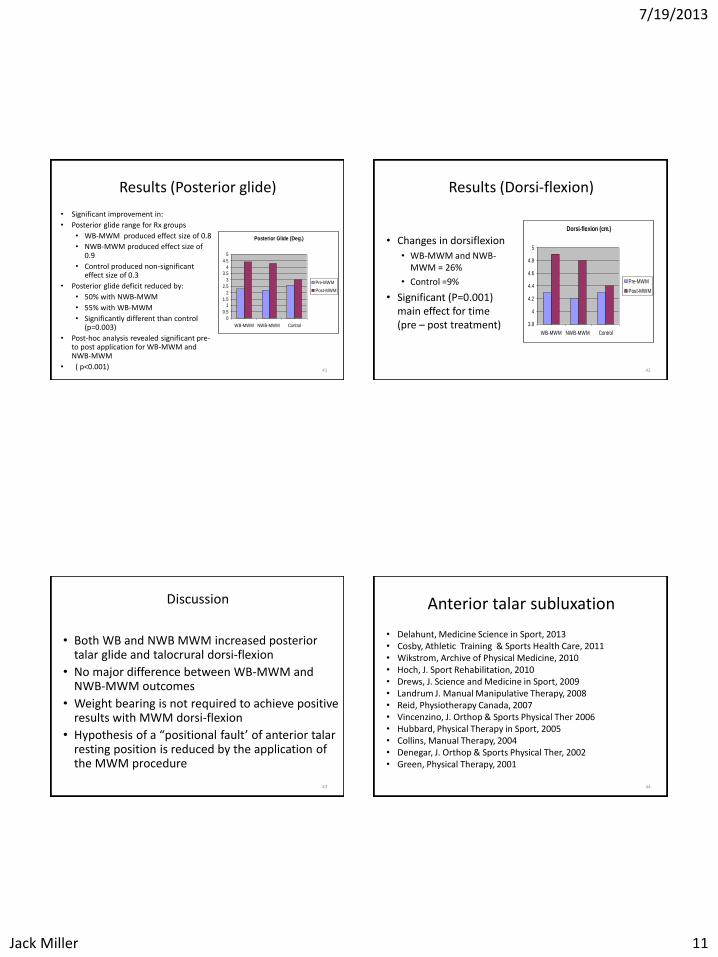
Results (Posterior glide)
• Significant improvement in:
• Posterior glide range for Rx groups
• WB-MWM produced effect size of 0.8
• NWB-MWM produced effect size of 0.9
• Control produced non-significant effect size of 0.3
• Posterior glide deficit reduced by:
• 50% with NWB-MWM
• 55% with WB-MWM
• Significantly different than control (p=0.003)
• Post-hoc analysis revealed significant pre-to post application for WB-MWM and NWB-MWM
• ( p<0.001)
Posterior Glide (Deg.)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
WB-MWM NWB-MWM Control
Pre-MWM
Post-MWM
41
Results (Dorsi-flexion)
• Changes in dorsiflexion
• WB-MWM and NWB-MWM = 26%
• Control =9%
• Significant (P=0.001) main effect for time (pre – post treatment)
Dorsi-flexion (cm.)
3.8
4
4.2
4.4
4.6
4.8
5
WB-MWM NWB-MWM Control
Pre-MWM
Post-MWM
42
Discussion
• Both WB and NWB MWM increased posterior talar glide and talocrural dorsi-flexion
• No major difference between WB-MWM and NWB-MWM outcomes
• Weight bearing is not required to achieve positive results with MWM dorsi-flexion
• Hypothesis of a “positional fault’ of anterior talar resting position is reduced by the application of the MWM procedure
43
Anterior talar subluxation
• Delahunt, Medicine Science in Sport, 2013 • Cosby, Athletic Training & Sports Health Care, 2011 • Wikstrom, Archive of Physical Medicine, 2010 • Hoch, J. Sport Rehabilitation, 2010 • Drews, J. Science and Medicine in Sport, 2009 • Landrum J. Manual Manipulative Therapy, 2008 • Reid, Physiotherapy Canada, 2007 • Vincenzino, J. Orthop & Sports Physical Ther 2006 • Hubbard, Physical Therapy in Sport, 2005 • Collins, Manual Therapy, 2004 • Denegar, J. Orthop & Sports Physical Ther, 2002 • Green, Physical Therapy, 2001
44

7/19/2013
Jack Miller 12
MWM Ankle Dorsi-flexion (WB)
• Mobilization
• Anterior glide distal tibia, talus fixated
• Movement
• Patient lunges forward
• Tips
• Progress from non to partial to full W/B
• Track with dynamic treatment plane
45
Cleland J, Mintken P et. al., JOSPT 2013;43 (7)July:443-455.
Manual Physical Therapy and Exercise Versus Supervised Home Exercise in the Management of Patients With Inversion Ankle Sprain: A Multicenter Randomized Clinical Trial
• 74 subjects grade I, II inversion sprain
• No time limits, 3:10 NPRS, -ve Ottawa rules
• Home exercise program only (4 PT visits)
• MTEX + 4 OMT procedures (4 PT visits)
46
Functional Ankle Activity Measure
47
Lower Extremity Function Scale
48

7/19/2013
Jack Miller 13
Case history #2
03
03
0
3
2
3
3
3
2
0
-
-
3
3
-
3
3
3
-
3
-
3
3
3
Rotates right leg externally
20
Right ant. knee pain
Right ant. knee pain
49
Where’s the dysfunction?
50
Where’s the dysfunction?
Dysfunctional painful Functional pain free 51
Where’s the dysfunction?
Functional non-painful 52

7/19/2013
Jack Miller 14
Analysis
• Dysfunctional and painful right hip
• Loss of hip internal rotation
• Increased mechanical stress on knee during step ups in aerobic class
53
Altman R. et. al., The American College of Rheumatology criteria for the classification and reporting of osteoarthritis
of the hip, Arthritis and Rheumatology, 1991;34:505-14.
• Cluster one: • Hip internal rotation < 15º • Hip flexion < 115º • Age > 50 years
• Cluster two: • If Hip internal rotation >/= 15º
• Pain with hip internal rotation • Duration of AM stiffness of hip </= 60 min. • Age > 50 years
54
Hip internal rotation and knee OA and/or Pain
Knee OA
• Deyle An In Med 2000
• Deyle Phys ther 2005
• Cliborne JOSPT 2004
• Currier JOSPT 2007
Anterior knee pain
• Lowry JOSPT 2008
• Iverson Phys Ther 2008
• Mascal JOSPT 2003
• Cibulka JOSPT 2005
• Vaughn JOSPT 2000
• Powers JOSPT 2000
• Powers JOSPT 2003
• Powers JOSPT 2010
55
Hip internal rotation and knee OA and/or Pain
CPR Currier JOSPT 2007,
• Hip groin pain or paresthesia
• Anterior thigh pain
• Passive knee flexion <122 degrees
• Pain with hip distraction
• Passive hip internal rotation < 17 degrees.
• +ve LR if 1 variable = 5.1
56

7/19/2013
Jack Miller 15
Hip internal rotation and knee OA and/or Pain
CPR Currier JOSPT 2007,
• Hip groin pain or paresthesia
• Anterior thigh pain
• Passive knee flexion <122 degrees
• Pain with hip distraction
• Passive hip internal rotation < 17 degrees.
• +ve LR if 1 variable = 5.1
• +ve LR if 2 variables = 12.9
57
Hip Pain and Mobility Deficits Altman R, Delitto A. et. al., 2009, Hip Osteoarthritis:
Clinical Practice Guidelines, JOSPT,;39(4), A1-A25.
• Interventions - Manual Therapy “Clinicians should consider the use of manual therapy procedures to provide short-term pain relief and improve hip mobility and function in patients with mild-hip osteoarthritis.”
• Based on moderate level evidence.
58
Clinical Practice Guidelines
Orthopaedic Section of APTA Cibulka 2009
“Clinicians should consider the use of manual therapy procedures to provide short term relief and improve hip mobility and function in patients with mild hip osteo-arthritis”
American College of Rheumatology Hockberg 2012
“Patients with hip OA should . . . Use manual therapy in combination with exercise under the supervision of a Physical Therapist”
59
Hip Internal rotation MWM
Mobilization
• Lateral glide femur
Movement
• Internal hip rotation
Tips
• May need anterior+/-inferior vector
• Control pelvis
• Ensure knee stable
60

7/19/2013
Jack Miller 16
Netherlands
MCID = 4 POINTS
61 62
63
USA
64

7/19/2013
Jack Miller 17
Hip internal rotation MWM (closed chain)
Mobilization
• Lateral glide of hip via belt
• Fixate pelvis
Movement
• Internal rotation via patient twisting
Tips
• Control pelvis
• Ensure client is stabilized by holding a chair back or bed
65
Case history #3
2
-
0
3
3
2
-
3
0
3
0
2
-
3
0
1
Right low back pain
+ + Low back pain
1
2
-
1
1
12
1
2
Right low back pain
Hamstring tension
66
Where’s the dysfunction?
67
Hip Extension
Dysfunctional and non-painful Dysfunctional and non-painful 68

7/19/2013
Jack Miller 18
Thomas test +/- modifications
Dysfunctional and non-painful Dysfunctional and non-painful 69
Bilateral lumbar extension
Functional and painful Functional and painful 70
Unilateral lumbar extension
Functional and painful (Right) Functional and painful (Right) 71
Analysis
• Functional painful lumbar extension
• Dysfunctional, non-painful loss of hip extension
• Increased stress on lumbar spine related to loss of hip extension in standing / walking
72
7/19/2013
Jack Miller 19
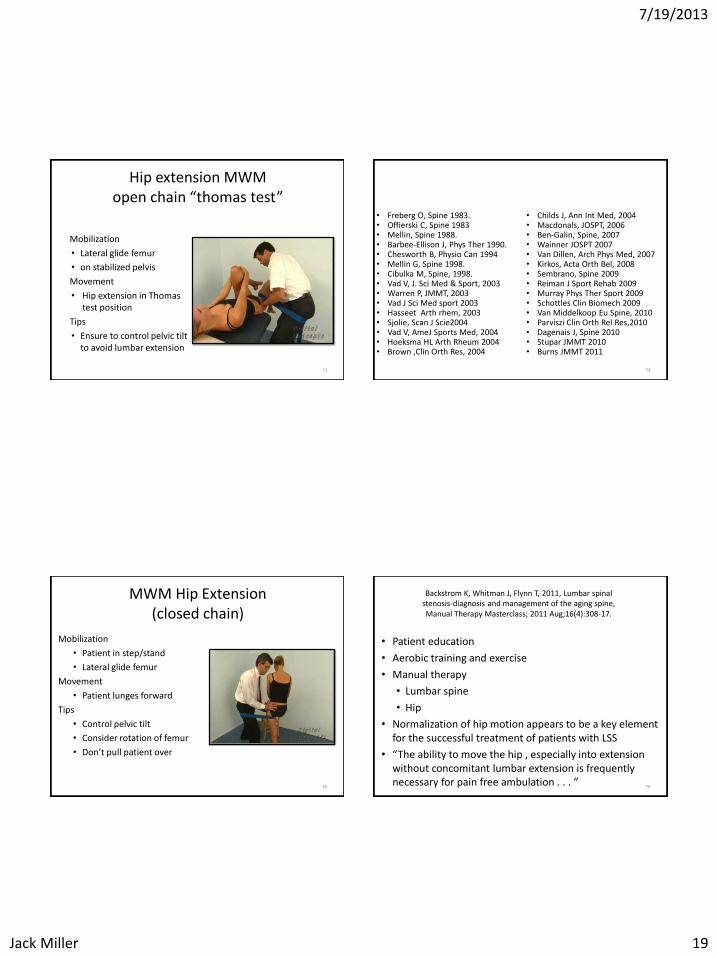
Hip extension MWM open chain “thomas test”
Mobilization
• Lateral glide femur
• on stabilized pelvis
Movement
• Hip extension in Thomas test position
Tips
• Ensure to control pelvic tilt to avoid lumbar extension
73
Loss of hip range of motion and mechanical low back pain
• Freberg O, Spine 1983. • Offierski C, Spine 1983 • Mellin, Spine 1988. • Barbee-Ellison J, Phys Ther 1990. • Chesworth B, Physio Can 1994 • Mellin G, Spine 1998. • Cibulka M, Spine, 1998. • Vad V, J. Sci Med & Sport, 2003 • Warren P, JMMT, 2003 • Vad J Sci Med sport 2003 • Hasseet Arth rhem, 2003 • Sjolie, Scan J Scie2004 • Vad V, AmeJ Sports Med, 2004 • Hoeksma HL Arth Rheum 2004 • Brown ,Clin Orth Res, 2004
• Childs J, Ann Int Med, 2004 • Macdonals, JOSPT, 2006 • Ben-Galin, Spine, 2007 • Wainner JOSPT 2007 • Van Dillen, Arch Phys Med, 2007 • Kirkos, Acta Orth Bel, 2008 • Sembrano, Spine 2009 • Reiman J Sport Rehab 2009 • Murray Phys Ther Sport 2009 • Schottles Clin Biomech 2009 • Van Middelkoop Eu Spine, 2010 • Parviszi Clin Orth Rel Res,2010 • Dagenais J, Spine 2010 • Stupar JMMT 2010 • Burns JMMT 2011
74
MWM Hip Extension (closed chain)
Mobilization
• Patient in step/stand
• Lateral glide femur
Movement
• Patient lunges forward
Tips
• Control pelvic tilt
• Consider rotation of femur
• Don’t pull patient over
75
Backstrom K, Whitman J, Flynn T, 2011, Lumbar spinal stenosis-diagnosis and management of the aging spine, Manual Therapy Masterclass; 2011 Aug;16(4):308-17.
• Patient education
• Aerobic training and exercise
• Manual therapy
• Lumbar spine
• Hip
• Normalization of hip motion appears to be a key element for the successful treatment of patients with LSS
• “The ability to move the hip , especially into extension without concomitant lumbar extension is frequently necessary for pain free ambulation . . . “
76

7/19/2013
Jack Miller 20
The 2 X 2 function matrix
Non-painful
Painful
Functional FN
FP
Dysfunctional DN
DP
77
The 2 X 2 function matrix
Non-painful
Painful
Functional Continue with wellness program
Dysfunctional
78
The 2 X 2 function matrix
Non-painful
Painful
Functional
Specific motor control training
Dysfunctional
79
The 2 X 2 function matrix
Non-painful
Painful
Functional
Dysfunctional Soft tissue resets • Needling • ASTYM • Neural mobilization
80
7/19/2013
Jack Miller 21
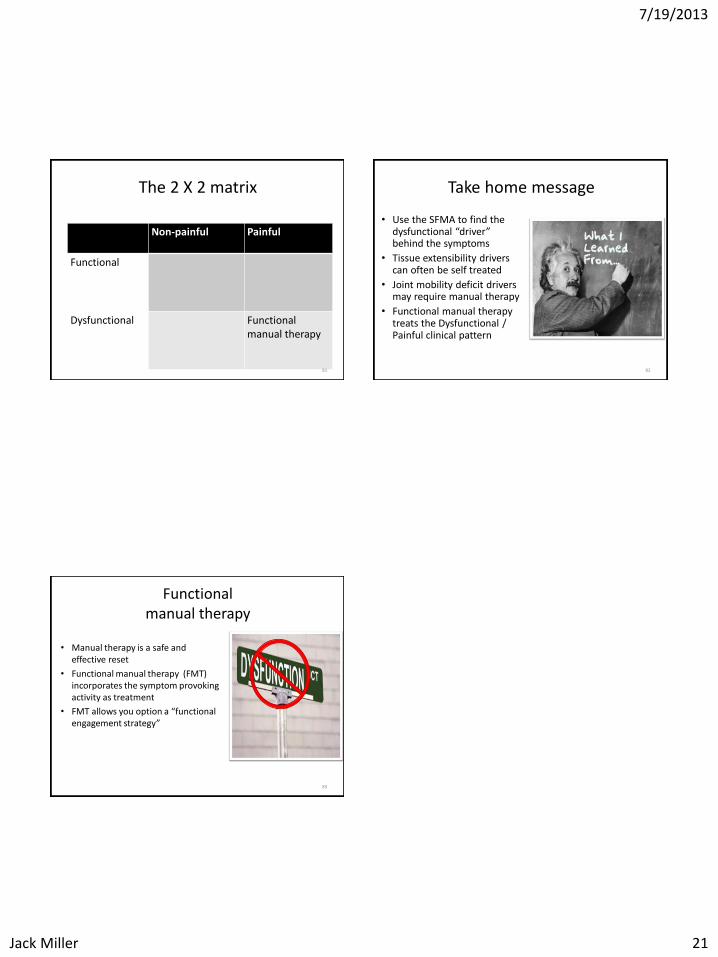
The 2 X 2 matrix
Non-painful
Painful
Functional
Dysfunctional
Functional manual therapy
81
Take home message
• Use the SFMA to find the dysfunctional “driver” behind the symptoms
• Tissue extensibility drivers can often be self treated
• Joint mobility deficit drivers may require manual therapy
• Functional manual therapy treats the Dysfunctional / Painful clinical pattern
82
Functional manual therapy
• Manual therapy is a safe and effective reset
• Functional manual therapy (FMT) incorporates the symptom provoking activity as treatment
• FMT allows you option a “functional engagement strategy”
83