Functional Implication of Mitral Annular Disjunction in ......(LV) attachment, is a structural...
10
Functional Implication of Mitral Annular Disjunction in Mitral Valve Prolapse A Quantitative Dynamic 3D Echocardiographic Study Alex Pui-Wai Lee, MD, a Chun-Na Jin, PHD, a Yiting Fan, MM, a,b Randolph H.L. Wong, MBCHB, c Malcolm J. Underwood, MD, b Song Wan, MD b ABSTRACT OBJECTIVES This study aimed to assess the hypothesis that mitral annular disjunction (MAD) is associated with abnormal annular dynamics due to decoupling of annular–ventricular function. BACKGROUND MAD, defined as a separation between the atrial wall–mitral valve (MV) junction and left ventricular (LV) attachment, is a structural abnormality occurring in MV prolapse (MVP). Few data exist on the 3-dimensional (3D) geometry of MAD and its functional implication. METHODS A total of 156 subjects including 101 MVP patients (58 11 years), 30 subjects with normal MV (57 15 years), and 25 heart failure patients with functional mitral regurgitation (66 10 years) were studied using real-time 3D transesophageal echocardiography. The spatial relation between atrial wall, MV, and LV attachment was examined for MAD. The 3D extent of MAD and annular dynamics were quantitatively assessed. The LV global longitudinal strain and basal circumferential strains were measured by speckle tracking echocardiography. RESULTS MAD was evident in 42 MVP patients (42%), measuring 8.9 mm (6.3 to 10.7 mm), circumferentially spanning 87 41 . Dynamically, normal and nondisjunctive annulus contracted and increased in a saddle shape during systole. In heart failure patients with functional mitral regurgitation, mitral annulus was dilated and relatively adynamic, probably related to poor LV function. In contrast, disjunctive annulus displayed paradoxical systolic expansion and flattening (p < 0.0001), despite preserved and comparable LV strains with normal patients. The 3D extent of MAD correlated significantly with abnormal annular dynamics and larger regurgitant orifice (p < 0.0001). In MVP patients without MAD, the LV global longitudinal strain correlated inversely with change in height (r ¼0.61; p < 0.0001), whereas LV basal circumferential strain correlated with change in area (r ¼ 0.61; p < 0.0001), but not in patients with MAD (p > 0.05). CONCLUSIONS MAD is a common anatomic abnormality in MVP. The disjunctive annulus is decoupled functionally from the ventricle, leading to paradoxical annular dynamics with systolic expansion and flattening, and may thus require specific intervention. (J Am Coll Cardiol Img 2017;-:-–-) © 2017 by the American College of Cardiology Foundation. M itral valve (MV) prolapse (MVP) affects 3% of the population, and is the leading surgi- cal indication for mitral regurgitation (1). Although leaflet degeneration has been considered the primary pathology, the importance of intrinsic annular abnormality in the pathogenesis of mitral regurgitation is increasingly recognized (2–5). The mitral annulus is a 3-dimensional (3D), saddle- shaped structure exhibiting dynamic conformational change in the cardiac cycle. The normal annulus From the a Division of Cardiology, Department of Medicine & Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong, China; b Cardiology Department, Renji Hospital, Medical College of Shanghai Jiao Tong University, Shanghai, China; and the c Division of Cardiothoracic Surgery, Department of Surgery, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong, China. This work was partially supported by the General Research Fund of the Research Grant Committee (467812), Hong Kong, China. Dr. Lee has received research equipment support and speaker honorarium from Philips Healthcare. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received July 27, 2016; revised manuscript received November 1, 2016, accepted November 17, 2016. JACC: CARDIOVASCULAR IMAGING VOL. -, NO. -, 2017 ª 2017 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION PUBLISHED BY ELSEVIER ISSN 1936-878X/$36.00 http://dx.doi.org/10.1016/j.jcmg.2016.11.022
Transcript of Functional Implication of Mitral Annular Disjunction in ......(LV) attachment, is a structural...

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . - , N O . - , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 6 . 1 1 . 0 2 2
Functional Implication of Mitral AnnularDisjunction in Mitral Valve ProlapseA Quantitative Dynamic 3D Echocardiographic Study
Alex Pui-Wai Lee, MD,a Chun-Na Jin, PHD,a Yiting Fan, MM,a,b Randolph H.L. Wong, MBCHB,c
Malcolm J. Underwood, MD,b Song Wan, MDb
ABSTRACT
Fro
Ho
Ch
Ho
(46
All
Ma
OBJECTIVES This study aimed to assess the hypothesis that mitral annular disjunction (MAD) is associated with
abnormal annular dynamics due to decoupling of annular–ventricular function.
BACKGROUND MAD, defined as a separation between the atrial wall–mitral valve (MV) junction and left ventricular
(LV) attachment, is a structural abnormality occurring in MV prolapse (MVP). Few data exist on the 3-dimensional (3D)
geometry of MAD and its functional implication.
METHODS A total of 156 subjects including 101 MVP patients (58 � 11 years), 30 subjects with normal MV
(57 � 15 years), and 25 heart failure patients with functional mitral regurgitation (66 � 10 years) were studied using
real-time 3D transesophageal echocardiography. The spatial relation between atrial wall, MV, and LV attachment
was examined for MAD. The 3D extent of MAD and annular dynamics were quantitatively assessed. The LV global
longitudinal strain and basal circumferential strains were measured by speckle tracking echocardiography.
RESULTS MAD was evident in 42 MVP patients (42%), measuring 8.9 mm (6.3 to 10.7 mm), circumferentially
spanning 87 � 41�. Dynamically, normal and nondisjunctive annulus contracted and increased in a saddle shape during
systole. In heart failure patients with functional mitral regurgitation, mitral annulus was dilated and relatively
adynamic, probably related to poor LV function. In contrast, disjunctive annulus displayed paradoxical systolic
expansion and flattening (p < 0.0001), despite preserved and comparable LV strains with normal patients. The 3D
extent of MAD correlated significantly with abnormal annular dynamics and larger regurgitant orifice (p < 0.0001). In
MVP patients without MAD, the LV global longitudinal strain correlated inversely with change in height (r ¼ �0.61;
p < 0.0001), whereas LV basal circumferential strain correlated with change in area (r ¼ 0.61; p < 0.0001), but not in
patients with MAD (p > 0.05).
CONCLUSIONS MAD is a common anatomic abnormality in MVP. The disjunctive annulus is decoupled functionally
from the ventricle, leading to paradoxical annular dynamics with systolic expansion and flattening, and may thus require
specific intervention. (J Am Coll Cardiol Img 2017;-:-–-) © 2017 by the American College of Cardiology Foundation.
M itral valve (MV) prolapse (MVP) affects 3%of the population, and is the leading surgi-cal indication for mitral regurgitation (1).
Although leaflet degeneration has been consideredthe primary pathology, the importance of intrinsic
m the aDivision of Cardiology, Department of Medicine & Therapeutics, T
spital, Hong Kong, China; bCardiology Department, Renji Hospital, Medica
ina; and the cDivision of Cardiothoracic Surgery, Department of Surgery, T
spital, Hong Kong, China. This work was partially supported by the Gene
7812), Hong Kong, China. Dr. Lee has received research equipment suppo
other authors have reported that they have no relationships relevant to
nuscript received July 27, 2016; revised manuscript received November 1
annular abnormality in the pathogenesis of mitralregurgitation is increasingly recognized (2–5). Themitral annulus is a 3-dimensional (3D), saddle-shaped structure exhibiting dynamic conformationalchange in the cardiac cycle. The normal annulus
he Chinese University of Hong Kong, Prince of Wales
l College of Shanghai Jiao Tong University, Shanghai,
he Chinese University of Hong Kong, Prince of Wales
ral Research Fund of the Research Grant Committee
rt and speaker honorarium from Philips Healthcare.
the contents of this paper to disclose.
, 2016, accepted November 17, 2016.

ABBR EV I A T I ON S
AND ACRONYMS
3D = 3-dimensional
ERO = effective regurgitant
orifice
FMR = functional mitral
regurgitation
LA = left atrium
LV = left ventricle
LV-GLS = left ventricular
global longitudinal strain
MAD = mitral annular
disjunction
MV = mitral valve
MVP = mitral valve prolapse
RT3DE = real-time
3-dimensional
echocardiography
Lee et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Annular Disjunction in Mitral Valve Prolapse - 2 0 1 7 :- –-
2
contracts and increases in saddle-shapednonplanarity during systole (6). Such annulardynamics are important for the balanced dis-tribution of mechanical stresses imposed bythe left ventricle (LV) on the MV. We haverecently reported annular flattening in pa-tients with MVP who developed greater mitralregurgitation than those with less regurgita-tion and normal individuals (4). Such annularflattening increases stress on the leaflets (4,7)and chordae (4), which can accelerate thedegenerative processes. Intrinsic annular pa-thology in MVP is also suggested by dynamicstudies (2,3,5). Nevertheless, the anatomicbasis of abnormal annular structure anddynamics in MVP remains unresolved, andthus optimal treatment strategy is uncertain.
Normally, the base of the posterior MV
leaflet joins the left atrial wall and the atrium–MVjunction is connected to the LV on the atrial aspect ofthe ventricular free wall (8). The mitral annulus is infact a tissue plane at the confluence of these struc-tures. Motion of the annulus is, therefore, passivelydetermined by contraction and relaxation of adjacentventricular musculature and by motion of the aorticroot (9). Mitral annular disjunction (MAD) is ananatomic abnormality of the annulus described path-ologically as a wide separation between the atrium–MV junction and the LV attachment (Figure 1) that isappreciable on both gross and histologic examination(8). During MVP repair, surgical inspection may detectMAD as superior displacement or atrialization of theposterior leaflet base (10,11). Both transthoracic (12)and transesophageal (10,11) echocardiography canrecognize MAD with excellent surgical correlation(Figure 1). However, few data exist on the 3D geometryof MAD and its relation with the annular and valvularfunction. Advances in real-time 3-dimensional echo-cardiography (RT3DE) allows quantitative analysis ofthe annular dynamics (2–5,13,14), whereas speckletracking echocardiography can assess deformation ofthe LV musculature. We hypothesized that MAD isassociated with abnormal annular function andmechanistically linked to decoupling of annular dy-namics from ventricular deformation. To test this hy-pothesis, we used transesophageal RT3DE to study the3D annular dynamics and valvemorphology in relationto LV functional analysis assessed by speckle trackingechocardiography. We compared MVP patients withMAD with those without MAD and with normal sub-jects, as well as with patients with functional mitralregurgitation (FMR) due to heart failure. We sought tocharacterize the 3D anatomy of the disjunctiveannulus and define its functional significance.
METHODS
STUDY POPULATION. A total of 156 subjects,including 101 patients with MVP, 25 patients with FMRsecondary to heart failure, and 30 control subjectsreferred for transesophageal echocardiography, werestudied prospectively. MVP was identified on echo-cardiography as systolic displacement (>2 mm) ofeither or both mitral leaflets into the left atrium,beyond the mitral annular plane, as indicated inthe long axis view. FMR was defined as MRsecondary to LV systolic dysfunction (ejectionfraction <40%) and/or annular dilatation withoutintrinsic MV abnormality. The indications for referralfor transesophageal echocardiography includeddetermination of regurgitation severity, evaluation ofsuitability of valve repair, suboptimal transthoracicimages, exclusion of endocarditis, and evaluation of acardiac source of an embolic event. Patients wereexcluded if they had contraindications to trans-esophageal echocardiography, mitral stenosis, aorticvalve disease, pericardial or congenital diseases,endocarditis, or cardiomyopathy. All patients under-went 2-dimensional and 3D transesophageal echocar-diographic examination using a standardized protocolfor the evaluation of the leaflet and annular pathol-ogy. Patients with disjunction of the mitral annulus(MADþ group), as defined below, were compared withthose with no appreciable annular disjunction (MAD�group). Patients found to have no structural heartdiseases on transesophageal echocardiography or ar-rhythmias were included as normal controls. The localinstitutional review board approved this study.
IMAGING. Transesophageal RT3DE of the MV wasperformed with an EPIQ7C ultrasound system (PhilipsHealthcare, Andover, Massachusetts) equipped with afully sampled matrix transducer (X7-2t). ZoomedRT3DE image of the MV apparatus was acquired. Theregion of interest was adjusted to the smallest pyra-midal volume that encompassed the entire MV tomaximize frame rates (>15 Hz). Gated multibeatacquisition was performed carefully with patientbreath-holding to avoid stitching artifact. The effec-tive regurgitant orifice (ERO) of mitral regurgitationwas quantified by the proximal isovelocity surfacearea method (15). For eccentric flow convergence,correction for flow constraint was performed bymultiplying ERO by the ratio of the angle formed bythe walls adjacent to the regurgitant orifice and 180�.
DETECTION AND 3D CHARACTERIZATION OF
ANNULAR DISJUNCTION. The volumetric datasetsof the MV were analyzed offline on an Xcelera work-station (Philips Healthcare). The 3D annular anatomy

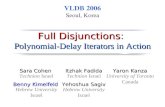
FIGURE 1 Correlation of Histology and Echocardiography of Mitral Annular Disjunction
Histology (A) and transesophageal echocardiography (B) showing the posterior leaflet of the mitral valve (MV), left atrium (LA), and left
ventricle (LV) normally join at the same junction (arrowhead). Histology (C) and echocardiography (D) showing annular disjunction (between
arrowheads) where LA–MV attachment is widely separated from basal LV musculature. Figures 1A and 1C are reprinted with permission from
Hutchins et al. (8).
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7 Lee et al.- 2 0 1 7 :- –- Annular Disjunction in Mitral Valve Prolapse
3
was assessed quantitatively with dedicated software(QLAB 10.3, Philips Healthcare). Three orthogonal im-aging planes were adjusted to ensure that the long axisplanes bisected theMVand the short axis plane parallelto the plane of MV. The spatial relation of the posteriorleaflet attachment to the left atrial wall and the LVbasal myocardium was examined in multiple recon-structed radial planes at 10� intervals rotated aroundthe long axis. MAD was present if there was a wideseparation ($5 mm) between the posterior leafletinsertion into the left atrial wall and the base of the LVfree wall, based on original histologic description byHutchins et al. (8) and echocardiographic descriptionby Eriksson et al. (10). In patients with MAD (MADþgroup), the maximal disjunction distance among allimaging planes and the degree of disjunction arcs weremeasured. We summarized the disjunction extent bycalculating the disjunction index, which was theproduct of the disjunction arc degree and the maximal
disjunction distance (Figure 2). Mitral annular di-mensions and shape were assessed using dedicatedquantification software (Mitral Valve Navigator, Phi-lips Healthcare) at both end-diastole and end-systole.Key annular parameters measured were annularintercommissural width, anteroposterior diameter,circumference, area, and height, as previouslydescribed (4). The ratio of annular height to inter-commissural width was calculated for description ofthe degree of saddle shape of the mitral annulusnormalized to annular size (7). A higher ratio indicatesa deeper saddle shape. Dynamic change of eachannular dimension was calculated by the formula:
Dparameter ¼ end-systolic measurement� end-diastolic measurement:
Leaflet dimensions and papillary muscle tip positionwere assessed quantitatively at end-systole, as pre-viously described (4). Key parameters measured were

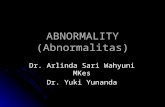
FIGURE 2 RT3DE Datasets of the Annulus
Real time 3-dimensional echocardiography (RT3DE) datasets of the annulus are examined offline on multiple reconstructed radial planes
(red solid lines) at 10� intervals (aortic valve at 0�) rotated around the long axis. There is annular disjunction (doubled arrows) spanning
circumferentially from 210� to 310� (i.e., disjunction arc degree ¼ 100�). The maximal disjunction distance, defined as the maximal separation
between the atrial wall–MV attachment and the basal LV musculature, is 10 mm. The disjunction index, calculated as the product of the
disjunction arc degree and the maximal disjunction distance, is 100� � 10 mm ¼ 1,000� $mm. Yellow line depicts the true atrial–ventricular
junction. Asterisks indicate the fibrous trigones. Abbreviations as in Figure 1.
Lee et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Annular Disjunction in Mitral Valve Prolapse - 2 0 1 7 :- –-
4
leaflet area, billow height and volume, and lengthsfrom papillary muscles to coaptation.
LEFT VENTRICULAR FUNCTION. The LV ejectionfraction, end-systolic and end-diastolic volumes, andleft atrial end-systolic volumes were determined byvolumetric analysis of the 3D datasets obtained bytransthoracic RT3DE following the American Societyof Echocardiography recommendations (16). Two-dimensional speckle tracking echocardiography wasused to evaluate LV strains (17). The left ventricularglobal longitudinal strain (LV-GLS) was analyzedoffline (QLAB 10.3, Philips Healthcare) by averagingthe peak strains derived from apical views, and theleft ventricular basal circumferential strain (LV-BCS)from the basal short axis view.
STATISTICAL METHODS. Data are expressed asmean � SD, median (interquartile range), or numberof patients (percentages) as appropriate. Normality ofcontinuous data was analyzed with the Shapiro–Wilk
test. All continuous variables except ERO, leafletbillow volume, and disjunction distance and indexwere normally distributed. Group comparisons forbaseline characteristics, summarized annular mea-surement (systolic/diastolic average), valve mea-surements at specific time points, and LV strains usedanalysis of variance (ANOVA), Kruskal-Wallis test,chi-square test, or Fisher exact test as appropriate.Pairwise comparisons after a significant ANOVA orKruskal-Wallis test were made by post-hoc Tukeyhonest significant difference or Steel-Dwass tests,respectively. Intragroup comparisons of each annularmeasure between end-systole and end-diastole useda paired Student t test. Repeated-measures ANOVAanalyzed differences in the dynamic changes ofannular measurements from end-diastole to end-systole between groups. Correlations between nor-mally distributed variables were tested by Pearsonanalysis. Correlations of disjunction index with othervariables were tested by Spearman coefficient.

TABLE 1 Patient Characteristics
Normal(n ¼ 30)
MVP
FMR(n ¼ 25) p Value
MAD�(n ¼ 59)
MADþ(n ¼ 42)
Clinical
Age, yrs 57 � 15 60 � 9 56 � 13 66 � 10*‡ 0.007
Men 17 (57) 42 (71) 31 (74) 15 (60) 0.34
Body surface area, m2 1.7 � 0.1 1.7 � 0.2 1.7 � 0.1 1.6 � 0.2 0.12
Heart rate, min-1 71 � 17 76 � 14 73 � 13 78 � 16 0.33
Echocardiography
Left ventricle
Ejection fraction, % 62 � 5 62 � 7 62 � 8 30 � 7*†‡ <0.0001
End-diastolic volume, ml 81 � 18 139 � 42* 133 � 37* 149 � 47* <0.0001
End-systolic volume, ml 31 � 8 53 � 20* 51 � 22* 109 � 30*†‡ <0.0001
Left atrial volume, ml 42 � 9 133 � 64* 132 � 74* 81 � 36†‡ <0.0001
Mitral valve
ERO, mm2 NA 50 (30–64) 56 (32–76) 20 (13–32)†‡ <0.0001
Number of prolapsed segments NA 1.2 � 0.4 3.8 � 2.2† NA <0.0001
Site of lesions† <0.0001
Isolated A1 NA 1 (2) 0 (0) NA
Isolated A2 NA 2 (3) 0 (0) NA
Isolated A3 NA 2 (3) 0 (0) NA
Isolated P1 NA 4 (7) 0 (0) NA
Isolated P2 NA 15 (25) 7 (17) NA
Isolated P3 NA 14 (24) 0 (0) NA
Anterior leaflet (>1 scallop) NA 2 (3) 0 (0) NA
Posterior leaflet (>1 scallop) NA 12 (20) 14 (33) NA
Bileaflet NA 0 (0) 21 (50) NA
Commissural scallops
Anterolateral commissure NA 3 (5) 0 (0) NA
Posteromedial commissure NA 4 (7) 0 (0) NA
Chordal rupture NA 43 (73) 22 (52) NA 0.034
Values are mean � SD, n (%), or median (interquartile range). *p < 0.05 versus normal. †p < 0.05 versus MAD�.‡p < 0.05 versus MADþ.
ERO ¼ effective regurgitant orifice; FMR ¼ functional mitral regurgitation; MAD ¼ mitral annular disjunction;NA ¼ not applicable.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7 Lee et al.- 2 0 1 7 :- –- Annular Disjunction in Mitral Valve Prolapse
5
Intraobserver and interobserver variabilities of 3Dmeasurements of MAD geometry were assessed usingintraclass correlation coefficient of repeated analysisin 10 randomly selected subjects by the same operator1 week apart, and by a different operator. Reproduc-ibility of other 3D MV echocardiographic measure-ments was reported previously (4). Analyses wereperformed with JMP version 12.0 (SAS Institute Inc.,Cary, North Carolina). A value of p < 0.05 wasconsidered significant.
RESULTS
STUDY POPULATION. Table 1 shows patient charac-teristics. Of the 101 subjects with MVP, MAD was seenin 42 patients (42%). A minor degree of annulardisjunction (<5 mm) was seen in 2 normal controlsubjects (one 28-year-old man and one 59-year-oldwoman). MAD was not seen in the FMR group. Thenumber of prolapsed segments was significantlygreater in MADþ than MAD– group (3.8 � 4.3 vs. 1.2 �2.2; p < 0.0001). Segmental distribution of lesions wasdifferent (chi-square ¼ 54.8; p < 0.0001), with isolatedP2 and/or P3 prolapse predominant in MAD– group,and bileaflet prolapse in the MADþ group. Conversely,chordal rupture was more frequent in the MAD– group(chi-square ¼ 4.5; p ¼ 0.034). The LV and left atrialvolumes were increased significantly in both MVPgroups when compared with normal subjects. Therewere no differences between the MADþ and MAD–groups regarding age, sex, LV volumes, ejection frac-tion, left atrial volume, and ERO. The FMR patientswere significantly older (p < 0.05 vs. the other 3groups). The LV volumes of the FMR groups weresignificantly more dilated with lower ejection fraction,but the left atrial volume and the ERO were smallerwhen compared with the MVP groups (all p < 0.05).
LOCATION AND 3D GEOMETRY OF MAD. The intra-class correlation coefficients for intraobserver andinterobserver variability of disjunction distancemeasurement were 0.96 and 0.82, respectively; thatof disjunction arcs measurement were 0.98 and 0.81.In general, MAD is located adjacent to the prolapsedsegments, circumferentially spanning over 87 � 41�
(range 20� to 170�) of the annulus, with the maximaldisjunction distance measuring 8.9 mm (6.3 to 10.7mm). The maximal disjunction was located mostfrequently at P2 (n ¼ 20) and P1 (n ¼ 18), lesscommonly in P3 (n ¼ 4). In the 2 normal subjectsshowing minor MAD, the separation distances were3.4 and 4.9 mm (both <10�) at P2 and P1, respectively.
RELATION OF ANNULAR DISJUNCTION WITH
ANNULAR STRUCTURE AND DYNAMIC FUNCTION.
Averaged measures of annular dimensions are shown
in Table 2. Compared with normal subjects, the mitralannulus of both MVP groups had increased ante-roposterior diameter, intercommissural width, area,and circumference (all p < 0.0001 for both MVP groupsvs. normal). Intercommissural width (p ¼ 0.0083) andarea (p ¼ 0.039) were significantly greater in MADþthan MAD� group, but anteroposterior diameter(p ¼ 0.32) and circumference (p ¼ 0.054) were similar.Annular height was similar in both MADþ andMAD� groups (p ¼ 0.20), but the annular height-to-intercommissural width ratio were significantly lower(p¼0.0058) in theMADþ group. The FMR annulus wasdilated significantly, with increased intercommissuralwidth, anteroposterior diameter, circumference, andarea (all p < 0.05 vs. normal). The intercommissuralwidth and circumference were enlarged to an extentgreater than that of bothMVP groups (all p<0.05). Theannular height of the FMR group was similar tocontrols, but higher than the MADþ group (p ¼ 0.012).

TABLE 2 Mitral Annular Dynamics
Average End-Diastole End-Systole
p Value,End-Systole vs.End-Diastole
Intercommissural width, mm
Normal 33.7 � 2.8 34.9 � 2.9 32.4 � 3.1 <0.0001
MAD� 37.6 � 4.5* 37.6 � 4.9 37.6 � 4.5* 0.91
MADþ 40.4 � 5.5*† 38.8 � 5.2* 42.0 � 6.5*† <0.0001
FMR 41.6 � 4.6*† 43.4 � 5.1*†‡ 39.7 � 4.7* <0.0001
Anteroposterior diameter, mm
Normal 27.9 � 2.7 28.9 � 3.4 26.9 � 2.5 <0.0001
MAD� 35.2 � 4.7* 35.7 � 5.5* 34.8 � 4.4* 0.03
MADþ 36.7 � 6.1* 35.8 � 5.9* 37.5 � 6.8*† 0.0035
FMR 35.8 � 3.1* 36.1 � 4.0* 35.4 � 2.8* 0.29
Circumference, mm
Normal 108 � 8 112 � 10 102 � 9 <0.0001
MAD� 123 � 15* 127 � 16* 120 � 15* <0.0001
MADþ 131 � 18* 129 � 17* 132 � 21*† 0.10
FMR 139 � 15*† 144 � 17*†‡ 135 � 13*† <0.0001
Area, mm2
Normal 751 � 114 802 � 124 697 � 111 <0.0001
MAD� 1,066 � 253* 1,092 � 281* 1,040 � 233* 0.0002
MADþ 1,198 � 340* 1,144 � 306* 1,252 � 390*† 0.0002
FMR 1,244 � 241*† 1,308 � 280*† 1,180 � 216* <0.0001
Height, mm
Normal 7.1 � 1.4 6.3 � 1.6 7.7 � 1.5 <0.0001
MAD� 6.8 � 1.4 6.7 � 1.7 6.9 � 1.6* 0.53
MADþ 6.3 � 1.4 7.5 � 2.1* 5.2 � 1.2*† <0.0001
FMR 7.4 � 0.8‡ 7.2 � 0.8 7.5 � 1.0‡ 0.19
Annular height-to-intercommissural width ratio, %
Normal 21 � 4 18 � 4 24 � 5 <0.0001
MAD� 18 � 4* 18 � 4 18 � 4* 0.52
MADþ 16 � 3*† 19 � 5 13 � 3*† <0.0001
FMR 18 � 3* 17 � 3 19 � 3*‡ 0.0003
Values are mean � SD. *p < 0.05 versus normal. †p < 0.05 versus MAD�. ‡p < 0.05 versus MADþ.
Abbreviations as in Table 1.
Lee et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Annular Disjunction in Mitral Valve Prolapse - 2 0 1 7 :- –-
6
Dynamically, dramatic intergroup differences wereobserved (Table 2, Figure 3). In normal subjects, theannular anteroposterior diameter, intercommissuralwidth, circumference, and area decreased from end-diastole to end-systole (all p < 0.0001). The annularsaddle deepened in systole with increased heightand height-to-intercommissural width ratio (bothp < 0.0001). In MAD� patients, the annular ante-roposterior diameter, circumference, and areadecreased in systole (all p < 0.05), but was lessthan normal (p < 0.05). The intercommissural width(p ¼ 0.91) and height (p ¼ 0.53) remained unchanged,meaning that the annulus did not exhibit significantdeepening of its saddle shape in systole. In contrast,in MADþ patients, the anteroposterior diameter,intercommissural width, and area paradoxicallyincreased in systole (all p < 0.005). In addition, theheight and height-to-intercommissural width ratioparadoxically decreased (both p < 0.0001), resulting
in paradoxical annular “unsaddling” in systole. InFMR patients, the intercommissural width, circum-ference, and area decreased from end-diastole toend-systole (all p < 0.0001); the anteroposteriordiameter (p ¼ 0.29) and annular height (p ¼ 0.19),however, remained unchanged. Systolic increase ofthe annular height-to-intercommissural width ratio(p ¼ 0.0003) was, therefore, contributed mainly bycontraction of the intercommissural width ratherthan an increase in the annular height in FMRpatients. In MADþ patients, the disjunction indexcorrelated significantly with ERO (r ¼ 0.56;p ¼ 0.0001), change in intercommissural width(r ¼ 0.63; p < 0.0001), change in area (r ¼ 0.60;p < 0.0001), change in circumference (r ¼ 0.49;p ¼ 0.001), change in height (r ¼ �0.50; p ¼ 0.0007),and change in height-to-intercommissural widthratio (r ¼ �0.59; p < 0.0001). There is a trend ofcorrelation between disjunction index and change inanteroposterior diameter (r ¼ 0.28; p ¼ 0.07).
RELATION OF ANNULAR DISJUNCTION WITH
VALVULAR STRUCTURE AND FUNCTION. As shownin Table 3, MAD was associated with more severemitral leaflets and chordae tendineae deformity.Compared with normal and MAD� groups, MADþgroup had significantly larger leaflet areas, billowheight and volume, and longer lengths from papillarymuscle to coaptation (all p < 0.05).
RELATION OF ANNULAR DISJUNCTION WITH LEFT
VENTRICULAR FUNCTION. Despite normal LV ejec-tion fraction, the LV-GLS of both MADþ (20.0 � 4.7%[p ¼ 0.014] vs. normal) and MAD� (�19.2 � 3.4%[p ¼ 0.0003] vs. normal) groups was significantly(ANOVA p ¼ 0.0005) reduced when compared withnormal controls (�22.9 � 2.2%). The LV-GLS wascomparable between MADþ and MAD– patients(p ¼ 0.54). The LV-BCS was similar across groups(MADþ vs. MAD– vs. normal ¼ �21.2 � 5.6%vs. �20.9 � 5.3% vs. �20.3% � 4.6%; ANOVA p ¼ 0.81).In MAD– patients, the LV-GLS correlated inverselywith change in height (r ¼�0.61; p < 0.0001), whereasthe LV-BCS correlated with change in area (r ¼ 0.61;p < 0.0001). In contrast, LV strains did not correlatewith any annular dynamics in MADþ patients(p > 0.05).
DISCUSSION
To the best of our knowledge, the current study is thefirst to characterize the 3D structure of MAD and itsfunctional significance. We found that MAD is rela-tively common in MVP. The disjunctive annulus dis-played paradoxical systolic dilatation and flatteningand is associated with more diffuse leaflet deformity.

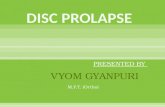
FIGURE 3 Annular Dynamics from End-Diastole to End-Systole
1500
1000
500
Are
a (m
m2 )
End-diastole
p < 0.0001
A
End-Systole
*
**
*
**
§
§
§
§
††
9
8
7
6
5
4
Hei
gh
t (m
m)
End-diastole
p < 0.0001
B
End-Systole
*
*
*
* §
§
†
‡
Normal MAD – MAD + FMR
The p value in each graph denotes that for the interaction time � group for repeated measures ANVOA. *p < 0.05 versus normal control;
†p < 0.05 versus MAD� group; ‡p < 0.05 versus MADþ group; §p < 0.05 versus end-diastolic measurement. Error bars, SEM. MAD�annulus showed systolic contraction of area but, unlike normal annulus, unable to increase its height. FMR annulus, despite significant
enlargement, showed systolic contraction of area; yet annular height was adynamic. In contrast, MADþ annulus showed paradoxical increase
in area and decrease in height in systole. FMR ¼ functional mitral regurgitation; MAD ¼ mitral annular disjunction.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7 Lee et al.- 2 0 1 7 :- –- Annular Disjunction in Mitral Valve Prolapse
7
Such abnormal annular dynamics occur despite rela-tively normal LV systolic function assessed by bothejection fraction and strains, suggesting intrinsicannular abnormalities and a decoupled annularfunction.
NORMAL MITRAL ANNULAR STRUCTURE AND
DYNAMICS. The normal mitral annulus undergoescomplex conformational changes during the cardiaccycle. Such motions are not inherent to the fibrousannulus, but are consequences of external forcesexerted by adjacent ventricular musculature (18).Torrent-Guasp proposed in his helical band modelthat systolic shortening of the circumferential basalloop fibers produces strain to reduce annulus di-mensions like a sphincter (18,19). Systolic deepeningof annular saddle is also a passive motion producedby differential translational annular movements(2,4,7). Longitudinal LV fiber contraction translatesthe posterior annulus apically. The anterior annulus,tethered at the aortic root (9), has to tilt posteriorly,thus folding the annulus into a saddle shape. Inaddition, LV longitudinal contraction pulls the medialand lateral annulus downward and inward, addingcurvature. When the annulus is disjunctive, its
motion no longer follows LV contraction, but exhibitsparadoxical dynamics, conforming to atrial wallmotion. The annulus simply stretches out with leftatrium during systole (Figure 4). Our study providedquantitative evidence of annuloventricular couplingby showing a close relation between the annularconformational dynamics with ventricular strains innormal and nondisjunctive annulus. The absence ofsuch a relation in MVP patients with disjunctiveannulus can be explained by functional decoupling ofthe annular and ventricular motions that entailsanatomic disjunction. These findings support thatMAD has important functional implications.
Patients with FMR have a significantly dilatedannulus. Although the degree of annular enlargementin FMR is comparable with that of MVP patients withMAD, the annular structure and dynamics significantlydiffer between the 2 groups. MAD was not seen in FMRpatients. In contrast with the paradoxical annularexpansion seen in MAD, the FMR annulus contracts insystole. The fractional changes of circumference andarea are lesser than normal; anteroposterior diameterand height are essentially adynamic. These findingsare consistent with previous studies (2,3) and areprobably related to poor ventricular function.

TABLE 3 Measurements of Leaflets and Chordae Tendineae
Control(n ¼ 30)
MVP
ANOVAp Value
MAD�(n ¼ 42)
MADþ(n ¼ 59)
Mitral leaflet areas
Anterior leaflet surface area, mm2 523 � 107 707 � 182* 858 � 296*‡ <0.0001
Posterior leaflet surface area, mm2 363 � 66 549 � 157* 706 � 252*‡ <0.0001
Total leaflet surface area, mm2 886 � 141 1,256 � 291* 1,564 � 474*‡ <0.0001
Leaflet to mitral annular area ratio 1.3 � 0.1 1.2 � 0.1* 1.3 � 0.1† <0.0011
Mitral prolapse measurements
Billow volume, ml 0.0 (0.0–0.1) 0.0 (0.2–0.8)* 1.4 (0.7–1.9)*‡ <0.0001
Billow height, mm 1.7 � 0.9 4.9 � 2.9* 7.3 � 2.8*‡ <0.0001
Chordae tendonae geometry
Length from anterolateral papillarymuscle to coaptation, mm
18.7 � 3.4 21.8 � 4.0* 24.6 � 4.4*‡ <0.0001
Length from posteromedial papillarymuscle to coaptation, mm
19.1 � 3.9 23.4 � 5.2* 26.3 � 5.7*† <0.0001
Values are mean � SD, median (interquartile range), or n (%) as appropriate. *p < 0.005 versus normal.†p < 0.05 versus MAD�. ‡p < 0.005 versus MAD–.
Abbreviations as in Table 1.
FIGURE
(A and B
contract
downwa
posterio
decoupl
Lee et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Annular Disjunction in Mitral Valve Prolapse - 2 0 1 7 :- –-
8
CLINICAL IMPLICATIONS. Our observations supportthe role of annuloplasty in MVP repair; annular ab-normality is common. Recent studies highlighted thepotential advantage of saddle-shaped annuloplasty to
4 Normal and MADþ Annular Dynamics
) In normal subjects, posterior annular (Po) motion is coupled to LV deforma
ion (red arrow), while anterior annulus (An) is fixed by the aortic root. (C and D
rds and inwards (red arrows). These LV motions contract the annulus and “f
r annulus (Po) does not follow LV deformation, but follows instead the motio
ed from LV deformation, resulting in paradoxical systolic expansion and “uns
restore annular shape (20,21). However, our findingsimply that implantation of an annuloplasty ring fromthe atrial side may not restore the function ofdisjunctive annulus fully because annular–ventriculardecoupling may persist (22). Refinement of annulo-plasty techniques by taking into consideration the 3Dgeometry of disjunction and ventricular fiber orien-tation may be important for sustained surgicaloutcome (10,11). Similarly, transcatheter MV repairtechniques that target leaflet pathology (e.g., Mitra-Clip) may not correct fully the annular dysfunctionassociated with disjunction, and thus the long-termoutcome of such therapy in this subset of patientswarrant further investigation.
Our study provides new insights into the patho-physiology of MVP. Autopsy findings of MAD ledHutchins et al. (8) to propose that regional disjunctionpermits hypermobility of atrium–valve junction. Inthe present study, we used 3D echocardiography toconfirm the functional importance of MAD bydemonstrating its association with paradoxicalannular dynamics. Systolic annular dilation mayaccentuate mitral regurgitation. Indeed, the extent ofdisjunction in the MADþ patients correlates with the
tion. Posterior annulus is moved towards LV apex by longitudinal LV
) The anterolateral (AL) and posteromedial (PM) annulus are pulled
old” it into a deeper saddle. (E and F) In contrast, the disjunctive
n of the LA wall (red arrowhead). (G and H) The annular motion is
addling.” AV ¼ aortic valve; other abbreviations as in Figure 1.

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: MAD occurs in
42% of patients with MVP undergoing transesophageal
echocardiography. It represents an intrinsic annular abnormality
that leads to paradoxical annular enlargement and flattening
during systole. The extent of annular disjunction is related
positively to the degree of mitral regurgitation. Such dynamic
abnormalities of the annulus may be related to decoupling of the
annular and ventricular functions.
COMPETENCY IN PATIENT CARE AND PROCEDURAL
SKILLS: Evaluation of the presence and extent of MAD should
become an essential part of pre-procedural planning of surgical
and transcatheter MV repair.
TRANSLATIONAL OUTLOOK: Additional studies are needed
to determine the prognostic importance of MAD in terms of the
progression of primary mitral regurgitation. Further research can
be conducted to explore whether a minor degree of annular
disjunction in otherwise normal MVs may progress and predispose
future valve prolapse. The therapeutic value of treatment stra-
tegies targeting to correct intrinsic annular structural abnormality
such as disjunction can be evaluated in further studies.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7 Lee et al.- 2 0 1 7 :- –- Annular Disjunction in Mitral Valve Prolapse
9
degree of mitral regurgitation. Furthermore, para-doxical systolic annular unsaddling may exaggeratemechanical stresses on the leaflets and chordae, whichmay predispose and perpetuate leaflet/chordaldegeneration. In the MAD� phenotype, despiteannular dilatation, annuloventricular couplingremains intact. Intriguingly, longitudinal LV strain isreduced in MVP and severe mitral regurgitation,possibly due to LV remodeling. This may suggest that,in these patients, the primary pathology lies in leafletand chordal tissue deficiency, whereas annulardysfunction, although present, may only besecondary.
STUDY LIMITATIONS. From our observation, a lesserdegree (<5 mm) of separation between the atrial–valve junction and its ventricular attachment can beseen occasionally in patients with otherwise struc-turally normal MV. Two control subjects were notedto have such minor separation. The separation existsin only 1 imaging plane (i.e., circumferentiallyspanning <10� of the annulus). A minor degree ofannular disjunction has been described in autopsy ofnormal hearts (8). Such minor “disjunction” mayrepresent a normal anatomic variant or an early ormilder form of pathological disjunction. Indeed, itwould be intriguing to understand whether theseminor disjunctions will progress and predisposeleaflet prolapse. However, there are not enough ofthese patients in our study population to draw anyconclusion about such an observation. The clinicalsignificance of minor disjunction warrants furtherlongitudinal follow-up echocardiographic studies.
CONCLUSIONS
The findings of the present study support the preva-lence of intrinsic annular abnormality in patientswith MVP. For the first time in humans, our studyshed lights on the structural basis for this functionalabnormality by demonstrating the decoupling of
annular and ventricular function in relation toanatomic annular disjunction. The comprehensivedescription of MAD geometry in this study has laiddown the framework for future works on new surgicaltechniques and devices. Our results also challengeclinicians to think of the MV as an integrated mech-anism susceptible to valvuloventricular interactions.
ADDRESS FOR CORRESPONDENCE: Dr. Alex Pui-WaiLee, 9/F Lui Che Woo Clinical Sciences Building,Department of Medicine & Therapeutics, Prince ofWales Hospital, 30-32 Ngan Shing Street, Shatin, N.T.,Hong Kong, China. E-mail: [email protected].
RE F E RENCE S
1. Freed LA, Levy D, Levine RA, et al. Prevalenceand clinical outcome of mitral-valve prolapse.N Engl J Med 1999;341:1–7.
2. Grewal J, Suri R, Mankad S, et al. Mitral annulardynamics in myxomatous valve disease: new in-sights with real-time 3-dimensional echocardiog-raphy. Circulation 2010;121:1423–31.
3. Levack MM, Jassar AS, Shang EK, et al.Three-dimensional echocardiographic analysisof mitral annular dynamics: implication forannuloplasty selection. Circulation 2012;126:S183–8.
4. Lee AP, Hsiung MC, Salgo IS, et al. Quanti-tative analysis of mitral valve morphologyin mitral valve prolapse with real-time 3-dimensional echocardiography: importance ofannular saddle shape in the pathogenesis ofmitral regurgitation. Circulation 2013;127:832–41.
5. Clavel MA, Mantovani F, Malouf J, et al.Dynamic phenotypes of degenerative myxomatousmitral valve disease: quantitative 3-dimensionalechocardiographic study. Circulation CardiovascImaging 2015;8:e002989.
6. Levine RA, Hagege AA, Judge DP, et al. Mitralvalve disease–morphology and mechanisms. NatRev Cardiol 2015;12:689–710.
7. Salgo IS, Gorman JH 3rd, Gorman RC, et al.Effect of annular shape on leaflet curvature inreducing mitral leaflet stress. Circulation 2002;106:711–7.
8. Hutchins GM, Moore GW, Skoog DK. The asso-ciation of floppy mitral valve with disjunction ofthe mitral annulus fibrosus. N Engl J Med 1986;314:535–40.

Lee et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 7
Annular Disjunction in Mitral Valve Prolapse - 2 0 1 7 :- –-
10
9. Komoda T, Hetzer R, Oellinger J, et al. Mitralannular flexibility. J Cardiac Surg 1997;12:102–9.
10. Eriksson MJ, Bitkover CY, Omran AS, et al.Mitral annular disjunction in advanced myxoma-tous mitral valve disease: echocardiographicdetection and surgical correction. J Am SocEchocardiogr 2005;18:1014–22.
11. Newcomb AE, David TE, Lad VS, Bobiarski J,Armstrong S, Maganti M. Mitral valve repair foradvanced myxomatous degeneration with poste-rior displacement of the mitral annulus. J ThoracCardiovasc Surg 2008;136:1503–9.
12. Carmo P, Andrade MJ, Aguiar C, Rodrigues R,Gouveia R, Silva JA. Mitral annular disjunction inmyxomatous mitral valve disease: a relevantabnormality recognizable by transthoracic echo-cardiography. Cardiovasc Ultrasound 2010;8:53.
13. Lee AP-W, Fang F, Jin C-N, et al. Quantificationof mitral valve morphology with three-dimensional echocardiography. Circ J 2014;78:1029–37.
14. Lee AP, Acker M, Kubo SH, et al. Mechanismsof recurrent functional mitral regurgitation after
mitral valve repair in nonischemic dilated cardio-myopathy: importance of distal anterior leaflettethering. Circulation 2009;119:2606–14.
15. Zoghbi WA, Enriquez-Sarano M, Foster E, et al.Recommendations for evaluation of the severityof native valvular regurgitation with two-dimensional and Doppler echocardiography. J AmSoc Echocardiogr 2003;16:777–802.
16. Lang RM, Badano LP, Mor-Avi V, et al. Rec-ommendations for cardiac chamber quantificationby echocardiography in adults: an update from theAmerican Society of Echocardiography and theEuropean Association of Cardiovascular Imaging.J Am Soc Echocardiogr 2015;28:1–39.e14.
17. Mor-Avi V, Lang RM, Badano LP, et al. Currentand evolving echocardiographic techniques for thequantitative evaluation of cardiac mechanics:ASE/EAE consensus statement on methodologyand indications endorsed by the Japanese Societyof Echocardiography. J Am Soc Echocardiogr 2011;24:277–313.
18. Ormiston JA, Shah PM, Tei C, Wong M. Sizeand motion of the mitral valve annulus in man. I. A
two-dimensional echocardiographic method andfindings in normal subjects. Circulation 1981;64:113–20.
19. Buckberg G, Hoffman JI, Mahajan A, Saleh S,Coghlan C. Cardiac mechanics revisited: the rela-tionship of cardiac architecture to ventricularfunction. Circulation 2008;118:2571–87.
20. Jensen MO, Jensen H, Levine RA, et al.Saddle-shaped mitral valve annuloplasty ringsimprove leaflet coaptation geometry. J ThoracCardiovasc Surg 2011;142:697–703.
21. Wan S, Lee AP, Jin CN, et al. The choice ofmitral annuloplastic ring-beyond “surgeon’s pref-erence.” Ann Cardiothorac Surg 2015;4:261–5.
22. Shimokawa T, Kasegawa H, Katayama Y,et al. Mechanisms of recurrent regurgitationafter valve repair for prolapsed mitral valvedisease. Ann Thorac Surg 2011;91:1433–8; dis-cussion 1438-9.
KEY WORDS echocardiography, mechanics,mitral valve, surgery