Front Lines June 2009
20
THE MEMBERS’ PUBLICATION OF THE ONTARIO NURSES’ ASSOCIATION AIN THIS ISSUE… E4 From ONA President Linda Haslam-Stroud, RN E5 From ONA CEO Lesley Bell, RN, MBA E16 From ONA First Vice-President Vicki McKenna, RN JUNE 2009 Vol. 9 • No. 3 Just as ONA prepares our members for anoth- er flu pandemic, the class action suit brought by registered nurses following the SARS out- break in 2003 has been thrown out. On May 7, 2009, just a few weeks aſter E continues on page 3 E continues on page 3 SARS Lawsuit Dismissed as H1N1 Hits AFEATURES IAC Recommendations ............................ 6 Nursing Week Photospread ............ 10-11 ADEPARTMENTS Member News.......................................... 6 ONA News ............................................. 12 Queen’s Park Update ............................. 17 OHC News .............................................. 17 Human Rights and Equity .................... 18 Awards and Decisions ........................... 19 OFL News ............................................... 20 members in the nursing homes sector have overwhelmingly ratified an agreement reached between our Nursing Homes Central Negotiating Team and the employer group, which will see wage and premium increases, and gains in workload, staffing, and health and safety issues. “ONA is very pleased that we’ve been able to reach this agreement for our nursing homes members, who provide quality care to the province’s most vulnerable people,” said ONA Presi- dent Linda Haslam-Stroud. “is tentative settlement provides approximately six to seven per cent increases over its two-year period, and language that improves occupational health and safety, which is a priority for ONA.” Following several days of negotiations, which began on March 30, 2009 and continued on April 20, 2009, the tentative agreement was reached in early May with the assistance of mediator Gerry Lee. e deal, which runs from July 1, 2009 to June 30, 2011, the H1N1 virus hit our province, the Ontario Court of Appeal ruled that the provincial government does not owe a “private law duty of care” to front-line registered nurses and ONA Nursing Homes Settlement Ratified INSIDE: Nursing Homes Central Agreement Highlights!
-
Upload
ontario-nurses-association -
Category
Documents
-
view
217 -
download
2
description
The members’ publication of the Ontario Nurses’ Association. Vol. 9, No. 3 - Nursing homes settlement ratified; SARS lawsuit dismissed as H1N1 hits.
Transcript of Front Lines June 2009

The MeMbers’ publicaTion oF The onTario nurses’ associaTion
AIN thIs Issue…
E4From ONA President
Linda Haslam-Stroud, RN
E5From ONA CEO
Lesley Bell, RN, MBA
E16From ONA First Vice-President
Vicki McKenna, RN
JuNe 2009 Vol. 9 • No. 3
Just as ONA prepares our members for anoth-er flu pandemic, the class action suit brought by registered nurses following the SARS out-break in 2003 has been thrown out.
On May 7, 2009, just a few weeks after E continues on page 3
E continues on page 3
SARS Lawsuit Dismissed as H1N1 Hits
AFeaTures
IAC Recommendations............................ 6Nursing Week Photospread............ 10-11
ADeparTMenTs
Member News.......................................... 6ONA News .............................................12Queen’s Park Update.............................17OHC News..............................................17Human Rights and Equity ....................18Awards and Decisions...........................19OFL News...............................................20
members in the nursing homes sector have overwhelmingly ratified an agreement reached between our Nursing Homes Central Negotiating Team and the employer
group, which will see wage and premium increases, and gains in workload, staffing, and health and safety issues.
“ONA is very pleased that we’ve been able to reach this agreement for our nursing homes members, who provide quality care to the province’s most vulnerable people,” said ONA Presi-dent Linda Haslam-Stroud. “This tentative settlement provides approximately six to seven per cent increases over its two-year period, and language that improves occupational health and safety, which is a priority for ONA.”
Following several days of negotiations, which began on March 30, 2009 and continued on April 20, 2009, the tentative agreement was reached in early May with the assistance of mediator Gerry Lee. The deal, which runs from July 1, 2009 to June 30, 2011,
the H1N1 virus hit our province, the Ontario Court of Appeal ruled that the provincial government does not owe a “private law duty of care” to front-line registered nurses and
ona
Nursing homes settlement Ratified
INsIde: Nursing Homes Central Agreement Highlights!
62324-2_ONA Front Line V9.indd 1 6/19/09 2:48:09 PM

JUNE 20092
Linda Haslam-Stroud, RNPresident, VM #2254
Communications & Public
Relations
Vicki McKenna, RNFirst VP, VM #2314
Political Action & Professional
Issues
Diane Parker, RNVP Region 1, VM #7710
Occupational Health & Safety
Anne Clark, RNVP Region 2, VM #7758
Labour Relations
Andy Summers, RNVP Region 3, VM #7754
Human Rights & Equity
Dianne Leclair, RNVP Region 4, VM #7752
Finance
Karen Bertrand, RNVP Region 5, VM #7702
Education
Lesley Bell, RNChief Executive Officer,
VM #2255
How to contact your 2009 ONA Board of Directors
Call ONA toll-free at 1-800-387-5580 (press 0)
or (416) 964-1979 in Toronto and follow the
operator’s prompts to access board members’
voice-mail. Voice-mail numbers (VM) for Board
members in the Toronto office are listed below.
Tel: (416) 964-8833
Toll free: 1-800-387-5580
ONA Provincial Office85 Grenville St., Ste. 400
Toronto ON M5S 3A2
ONA is the union representing 54,000 registered nurses and allied health
professionals and more than 10,000 nursing students providing care in
hospitals, long-term care facilities, public health, the community, clinics
and industry.
Fax: (416) 964-8864
e-mail: [email protected]
www.ona.org
Design: Artifact graphic design
Printed by union labour: Thistle Printing Limited
Copyright © 2009 Ontario Nurses’ Association
All rights reserved. No part of this publication may be reproduced or transmitted in
any form or by any means, including electronic, mechanical, photocopy, recording,
or by any information storage or retrieval system, without permission in writing
from the publisher.
ISSN: 0834-9088
ThE MEMbErs’ pUblicaTioN oF ThE oNTario NUrsEs’ associaTioN
Editor: Ruth Featherstone
Features Editor: Melanie Levenson
Send submissions to: The editor at [email protected]
Contributors: Sheree Bond, Brooke Burns, Nancy Johnson, Mary Lou King, David
Nicholson, Lawrence Walter, WSIB Team.
E Hamilton2 King St., W., 2nd Floor Rear
Dundas, ON L9H 6Z1
Tel: (905) 628-0850
Fax: (905) 628-2557
E Kingston4 Cataraqui St., Ste. 306
Kingston ON K7K 1Z7
Tel: (613) 545-1110
Fax: (613) 531-9043
E London750 Baseline Rd. E., Ste. 204
London ON N6C 2R5
Tel: (519) 438-2153
Fax: (519) 433-2050
E Orillia210 Memorial Ave.,
Unit 126A
Orillia ON L3V 7V1
Tel: (705) 327-0404
Fax: (705) 327-0511
E Ottawa1400 Clyde Ave., Ste. 211
Nepean ON K2G 3J2
Tel: (613) 226-3733
Fax: (613) 723-0947
E Sudbury764 Notre Dame Ave., Unit 3
Sudbury ON P3A 2T4
Tel: (705) 560-2610
Fax: (705) 560-1411
E Thunder Bay#214, Woodgate Centre,
1139 Alloy Dr.
Thunder Bay ON P7B 6M8
Tel: (807) 344-9115
Fax: (807) 344-8850
E TimminsCanadian Mental Health
Association Building
330 Second Ave, Ste. 203
Timmins ON P4N 8A4
Tel: (705) 264-2294
Fax: (705) 268-4355
E Windsor3155 Howard Ave., Ste. 220
Windsor ON N8X 3Y9
Tel: (519) 966-6350
Fax: (519) 972-0814
ONA Regional Offices
JUNE 2009 Vol. 9 • No. 3
ON OUR COVER: ONA President Linda Haslam-Stroud holds up the nursing homes settlement highlights document,
included with this issue of Front Lines, as members of our Nursing Homes Central Negotiating Team look on at an
all-sector meeting in downtown Toronto on May 26, 2009.
that the “interest of nurses cannot be prioritized over the general public interest.”
“The message to front-line registered nurses is that government is not accountable for their safety or their lives,” said ONA President Linda Haslam-Stroud. “The government is not required to pass laws that provide RNs with safe working conditions and equipment, and they don’t have to take responsibility for keeping us safe. It’s a de-plorable and outrageous situation.”
ONA had launched an action against the Ontario government in 2005 on behalf of ONA member Tecla Lin, who tragically lost her life in the second SARS outbreak, and 52 other nurses for negli-gence in the handling of the SARS outbreak, arguing officials failed to provide adequate and timely information alerting nurses on how to protect themselves. The government brought a motion to strike out the claim, stating they did not owe nurses infected with SARS a duty to take reasonable steps to protect them. The government lost this motion and appealed the decision.
“ONA will not take this lying down when so many of our mem-bers risked their health and lives,” added Haslam-Stroud.
“ONA will continue to push for safe conditions for our mem-bers. We will be even more aggressive in ensuring that our members are properly armed with information and protective equipment, as no one else will do it for us. This is particularly critical as we face the H1N1 virus.”
Now that the virus has been declared a pandemic by the World Health Organization, ONA is well prepared, thanks to the lessons learned from the SARS crisis. We immediately launched a Pandemic Steering Committee to review current information from the Ministry of Health and Long-Term Care and disseminate it to our members.
When facing infectious disease outbreaks, the Campbell SARS Commission advised the government and employers to enact the precautionary principle, meaning that action to reduce risk should not await scientific certainty. While the government has been slow to act on this advice, we recommend that members work with their facility’s Joint Health and Safety Committee to demand that your employer, in consultation with your committee, conducts risk as-sessments; identifies health care workers who may be exposed to this influenza; equips any health care workers at risk of exposure with proper personal protective equipment; and develops measures and procedures for limiting exposure.
The home page of the ONA website at www.ona.org contains fre-quently updated information on the H1N1 virus and additional tips on what you can do to protect yourself. A policy directive from the Canadian Federation of Nurses Unions on the outbreak and person-al protective equipment can also be found on our home page. BFL
Econt. from cover
SARS Lawsuit Dismissed as H1N1 Hits
Up fRONt
62324-2_ONA Front Line V9.indd 2 6/19/09 4:06:02 PM
3June 2009
ONA is the union representing 54,000 registered nurses and allied health
professionals and more than 10,000 nursing students providing care in
hospitals, long-term care facilities, public health, the community, clinics
and industry.
Fax: (416) 964-8864
e-mail: [email protected]
Design: Artifact graphic design
Printed by union labour: Thistle Printing Limited
Copyright © 2009 Ontario Nurses’ Association
All rights reserved. No part of this publication may be reproduced or transmitted in
any form or by any means, including electronic, mechanical, photocopy, recording,
or by any information storage or retrieval system, without permission in writing
from the publisher.
ISSN: 0834-9088
Editor: Ruth Featherstone
Features Editor: Melanie Levenson
Send submissions to: Communications and Government Relations Intake at [email protected]
Contributors: Sheree Bond, Brooke Burns, Nancy Johnson, Mary Lou King, David
Nicholson, Lawrence Walter, WSIB Team.
E Thunder Bay#214, Woodgate Centre,
1139 Alloy Dr.
Thunder Bay ON P7B 6M8
Tel: (807) 344-9115
Fax: (807) 344-8850
E TimminsCanadian Mental Health
Association Building
330 Second Ave, Ste. 203
Timmins ON P4N 8A4
Tel: (705) 264-2294
Fax: (705) 268-4355
E Windsor3155 Howard Ave., Ste. 220
Windsor ON N8X 3Y9
Tel: (519) 966-6350
Fax: (519) 972-0814
affects approximately 2,200 ONA members employed in 151 partici-pating nursing homes throughout the province.
Details were released to ONA leaders at a nursing homes sector meeting in Toronto on May 26, 2009 and posted on the members’ sec-tion of our website at www.ona.org. Ratification meetings took place in late May and early June, and the results were released on June 12, 2009.
Highlights of the settlement are included with this issue of Front Lines. Questions and concerns can be e-mailed to Haslam-Stroud at [email protected]. BFL
Econt. from cover
ON OUR COVER: ONA President Linda Haslam-Stroud holds up the nursing homes settlement highlights document,
included with this issue of Front Lines, as members of our Nursing Homes Central Negotiating Team look on at an
all-sector meeting in downtown Toronto on May 26, 2009.
Nursing homes settlement Ratified
April Board HighlightsThe following are key highlights from the most recent Board of Direc-tors meeting, held April 15-17, 2009 at the ONA provincial office.
A Recommendations for the 2010 Treasurers Workshop were approved including: maintaining the workshop as a two-day event; continuing to bring in new Treasurers for two days of training; exploring options for providing new Treasurers with education on governance and ONA structure; including an extra half-day for technology training in new Local Coordinator Workshops; and suspending the Treasurer/Local Coordinator Day based on member feedback.
A ONA will provide $2,000 to the Ontario Federation of Labour, of which we are a member, for the production of a DVD on sexual harassment.
A A DVD for the Friends and Allies breakout session of the Human Rights and Equity Caucus will be created, including real stories of members on the Human Rights and Equity Team.
Complete highlights of the Board of Directors meeting are available on the members’ section of the ONA website at www.ona.org. The next Board meeting will be held at the provincial office on June 17-18, 2009 and highlights will appear in the next issue of Front Lines.
that the “interest of nurses cannot be prioritized over the general public interest.”
“The message to front-line registered nurses is that government is not accountable for their safety or their lives,” said ONA President Linda Haslam-Stroud. “The government is not required to pass laws that provide RNs with safe working conditions and equipment, and they don’t have to take responsibility for keeping us safe. It’s a de-plorable and outrageous situation.”
ONA had launched an action against the Ontario government in 2005 on behalf of ONA member Tecla Lin, who tragically lost her life in the second SARS outbreak, and 52 other nurses for negli-gence in the handling of the SARS outbreak, arguing officials failed to provide adequate and timely information alerting nurses on how to protect themselves. The government brought a motion to strike out the claim, stating they did not owe nurses infected with SARS a duty to take reasonable steps to protect them. The government lost this motion and appealed the decision.
“ONA will not take this lying down when so many of our mem-bers risked their health and lives,” added Haslam-Stroud.
“ONA will continue to push for safe conditions for our mem-bers. We will be even more aggressive in ensuring that our members are properly armed with information and protective equipment, as no one else will do it for us. This is particularly critical as we face the H1N1 virus.”
Now that the virus has been declared a pandemic by the World Health Organization, ONA is well prepared, thanks to the lessons learned from the SARS crisis. We immediately launched a Pandemic Steering Committee to review current information from the Ministry of Health and Long-Term Care and disseminate it to our members.
When facing infectious disease outbreaks, the Campbell SARS Commission advised the government and employers to enact the precautionary principle, meaning that action to reduce risk should not await scientific certainty. While the government has been slow to act on this advice, we recommend that members work with their facility’s Joint Health and Safety Committee to demand that your employer, in consultation with your committee, conducts risk as-sessments; identifies health care workers who may be exposed to this influenza; equips any health care workers at risk of exposure with proper personal protective equipment; and develops measures and procedures for limiting exposure.
The home page of the ONA website at www.ona.org contains fre-quently updated information on the H1N1 virus and additional tips on what you can do to protect yourself. A policy directive from the Canadian Federation of Nurses Unions on the outbreak and person-al protective equipment can also be found on our home page. BFL
Econt. from cover
SARS Lawsuit Dismissed as H1N1 Hits
Ontario Minister of Health and Long-Term Care David Caplan (pictured with ONA President Linda Haslam-Stroud) and his Policy Advisor Shabnum Durani attend the ONA Board of Directors meeting on April 15, 2009 at ONA’s provincial office to discuss Ontario’s health care priorities and our concerns about nursing layoffs, position/hour reductions in all sectors and the need to stabilize the nursing workforce. Minister Caplan said his government is committed to the nursing workforce.
Up fRONt
62324-2_ONA Front Line V9.indd 3 6/19/09 2:48:19 PM

June 20094
From ONA President / Présidente, AIIO
Linda Haslam-Stroud, RN
From ONA Chief Executive Officer / Directrice générale, AIIO
Lesley Bell, RN, MBA
personal stories hit home with publicfew weeks ago I came across a letter to the editor written by two of our hospital members that really struck a chord with me.
The letter describes a typical night in the life of a nurse. It talks about the conflicting priorities they face throughout the shift: provid-ing constant care to too many patients, processing doctors’ orders, checking computerized medication records, and charting. Through-out it all, a phone is ringing in the background, but there is no one to answer it because the nurses are too busy. The authors conclude the letter by reflecting on the shift on the drive home and wondering if they forgot to do something.
What is so poignant about this letter is not just how eloquently it is written, or that it accurately describes the working realities of today’s nurses. It is the anguish that we, as the reader, can actually feel behind the words. It is the authors’ enormous sense of conflict, torment and guilt that leaps from the page. It allows us into the minds of nurses struggling in an ailing health care system. A system that permits nurses to be laid off as a means for hospitals to balance their books. A system where a devastating nursing shortage has yet to be appropriately ad-dressed. A system where those nurses who remain are stressed, burned out, frustrated and questioning if they could have done more on their shift.
It is these kinds of firsthand accounts that really resonate with the public. It is all very well and good for ONA and our allies to push the government and employers for needed changes to the health care system– and we will continue to do so – and educate the public on the facts, but it is these personal tales of despair published in local news-papers, where people are most likely to read them, that will have the biggest impact. The public may not always understand statistics, but this they get. After all, these are their nurses in their community caring for their citizens. And that may be our most powerful ammunition in getting them to help us in our fight.
So I urge you to take advantage of any opportunity you have to tell your personal stories to the public. Send a letter to the editor, as these ONA members, talk to your family, friends and neighbours. It need not be an overwhelming or daunting task. Discuss what you do, what you know, and what you are faced with on the job each and every shift and you can’t possibly go wrong.
The letter is available on the homepage of the ONA website at www.ona.org under “Health Care News.”
a isars ruling sends the Wrong Message
s another flu pandemic is upon us and the public relies on the government to keep them safe, it is ironic that the Ontario Court of Appeal has ruled that very government is not accountable for
their inaction during the SARS crisis of 2003.I don’t have to remind you that our lives were turned upside down
by SARS. We were scared. We were quarantined. We got sick. And tragically, we lost two of our fellow members. We did everything that was asked of us and then some. All that we expected in return was for the government, which sends directives to hospitals, to ensure our safety. They let us down.
Their directives were inadequate, too late and put our members at risk of contracting SARS. They didn’t tell us the risks and they man-dated supposedly appropriate protections, which were simply not good enough. We sounded the alarm bells, but we were ignored. Expecting that the government be held accountable for their lack of action is the least we could ask for. But we have been let down again.
The Court ruled that this is risk incurred by virtue of our calling. We don’t believe that dying should be part of the job! In fact, it is in every-one’s best interest to know that the government is taking steps to avoid harm to nurses and others who risk their lives and health every day.
Every nurse in this province should be outraged by this ruling. It says the government is not accountable for providing RNs with safe working conditions and equipment. This is the wrong message to be sending at a time when the World Health Organization has declared a H1N1 influenza pandemic.
While the government has come leaps and bounds in terms of be-ing prepared, we are left to wonder if some facilities are well enough prepared, if proper screening programs are in place, if there are enough masks and proper isolation to protect workers, and if planning is in place for the surge of potential people that will require care with fewer registered nurses in our system. After all, the government is not legally responsible for keeping us safe.
If there’s one thing this ruling proved, it’s that you need your union more than ever. If we can’t depend on the government and our employ-ers to protect us, we will have to do so ourselves. I can assure you that ONA will be watching with a critical eye to ensure our workplaces are safe. We will aggressively fight to ensure that you are armed with infor-mation and protective equipment. We must err on the side of caution because we can never allow another preventable nurse’s death.
aDes témoignages personnels qui touchent le public
l y a quelques semaines, je suis tombée sur une lettre d’une tribune libre écrite par deux de nos membres du personnel hospitalier qui m’a vraiment touchée.
La lettre décrit une nuit typique dans la vie d’une infirmière. Elle parle des priorités concurrentes que les infirmières doivent gérer tout au long de leur quart de travail : les soins constants à donner à un trop grand nombre de patients, les ordonnances à traiter, les fiches infor-matisées de médicaments à vérifier et la consignation des notes au dos-sier. Au milieu de tout cela, un téléphone qui sonne quelque part, mais personne pour y répondre, car les infirmières sont trop occupées. Les auteures concluent leur lettre en évoquant leur retour en auto à la mai-son pendant lequel elles reviennent sur les tâches accomplies pendant leur quart, se demandant si elles ont oublié de faire quelque chose.
Ce qui me frappe le plus dans cette lettre, ce n’est pas l’éloquence avec laquelle elle a été rédigée ni l’exactitude avec laquelle elle décrit la réalité quotidienne du travail des infirmières, c’est l’angoisse présente derrière les mots que le lecteur peut réellement ressentir. C’est le ter-rible sentiment de conflit, d’inquiétude et de culpabilité éprouvé par les auteures qui se dégage de leur lettre. Il nous fait comprendre l’état d’esprit d’infirmières qui font un travail difficile dans un système de santé mal en point.
C’est ce genre de témoignage direct qui trouve un écho dans la population. C’est très bien pour l’AIIO et ses alliés de faire pression auprès du gouvernement et des employeurs pour obtenir des change-ments nécessaires dans le système de santé, et nous continuerons d’agir ainsi, et d’informer le public sur les faits, mais ce sont des témoignages de désespoir personnel de ce genre publié dans la presse locale, que les gens risquent le plus de lire, qui auront le plus gros effet. La population peut parfois ne pas comprendre les statistiques, mais elle sera sensi-ble à ce genre de message. Après tout, il s’agit de leurs infirmières qui soignent leur monde dans leur communauté. Et c’est peut-être notre atout le plus puissant pour amener les gens à nous aider dans notre combat.
Je vous demande donc de saisir toutes les occasions qui s’offrent à vous pour livrer vos témoignages personnels au public. Envoyez une lettre à une tribune libre, comme l’ont fait ces membres de l’AIIO, parlez à votre famille, à vos amis et à vos voisins. Il n’est pas nécessaire d’en faire une tâche compliquée et exigeante. Parlez simplement de ce que vous faites, de ce que vous savez, de ce à quoi vous devez faire face au travail pendant chacun de vos quarts et vous ne pouvez pas vous tromper.
62324-2_ONA Front Line V9.indd 4 6/19/09 2:48:21 PM

5June 2009
From ONA Chief Executive Officer / Directrice générale, AIIO
Lesley Bell, RN, MBA
sars ruling sends the Wrong Messages another flu pandemic is upon us and the public relies on the government to keep them safe, it is ironic that the Ontario Court of Appeal has ruled that very government is not accountable for
their inaction during the SARS crisis of 2003.I don’t have to remind you that our lives were turned upside down
by SARS. We were scared. We were quarantined. We got sick. And tragically, we lost two of our fellow members. We did everything that was asked of us and then some. All that we expected in return was for the government, which sends directives to hospitals, to ensure our safety. They let us down.
Their directives were inadequate, too late and put our members at risk of contracting SARS. They didn’t tell us the risks and they man-dated supposedly appropriate protections, which were simply not good enough. We sounded the alarm bells, but we were ignored. Expecting that the government be held accountable for their lack of action is the least we could ask for. But we have been let down again.
The Court ruled that this is risk incurred by virtue of our calling. We don’t believe that dying should be part of the job! In fact, it is in every-one’s best interest to know that the government is taking steps to avoid harm to nurses and others who risk their lives and health every day.
Every nurse in this province should be outraged by this ruling. It says the government is not accountable for providing RNs with safe working conditions and equipment. This is the wrong message to be sending at a time when the World Health Organization has declared a H1N1 influenza pandemic.
While the government has come leaps and bounds in terms of be-ing prepared, we are left to wonder if some facilities are well enough prepared, if proper screening programs are in place, if there are enough masks and proper isolation to protect workers, and if planning is in place for the surge of potential people that will require care with fewer registered nurses in our system. After all, the government is not legally responsible for keeping us safe.
If there’s one thing this ruling proved, it’s that you need your union more than ever. If we can’t depend on the government and our employ-ers to protect us, we will have to do so ourselves. I can assure you that ONA will be watching with a critical eye to ensure our workplaces are safe. We will aggressively fight to ensure that you are armed with infor-mation and protective equipment. We must err on the side of caution because we can never allow another preventable nurse’s death.
a aDes témoignages personnels qui touchent le public
l y a quelques semaines, je suis tombée sur une lettre d’une tribune libre écrite par deux de nos membres du personnel hospitalier qui m’a vraiment touchée.
La lettre décrit une nuit typique dans la vie d’une infirmière. Elle parle des priorités concurrentes que les infirmières doivent gérer tout au long de leur quart de travail : les soins constants à donner à un trop grand nombre de patients, les ordonnances à traiter, les fiches infor-matisées de médicaments à vérifier et la consignation des notes au dos-sier. Au milieu de tout cela, un téléphone qui sonne quelque part, mais personne pour y répondre, car les infirmières sont trop occupées. Les auteures concluent leur lettre en évoquant leur retour en auto à la mai-son pendant lequel elles reviennent sur les tâches accomplies pendant leur quart, se demandant si elles ont oublié de faire quelque chose.
Ce qui me frappe le plus dans cette lettre, ce n’est pas l’éloquence avec laquelle elle a été rédigée ni l’exactitude avec laquelle elle décrit la réalité quotidienne du travail des infirmières, c’est l’angoisse présente derrière les mots que le lecteur peut réellement ressentir. C’est le ter-rible sentiment de conflit, d’inquiétude et de culpabilité éprouvé par les auteures qui se dégage de leur lettre. Il nous fait comprendre l’état d’esprit d’infirmières qui font un travail difficile dans un système de santé mal en point.
C’est ce genre de témoignage direct qui trouve un écho dans la population. C’est très bien pour l’AIIO et ses alliés de faire pression auprès du gouvernement et des employeurs pour obtenir des change-ments nécessaires dans le système de santé, et nous continuerons d’agir ainsi, et d’informer le public sur les faits, mais ce sont des témoignages de désespoir personnel de ce genre publié dans la presse locale, que les gens risquent le plus de lire, qui auront le plus gros effet. La population peut parfois ne pas comprendre les statistiques, mais elle sera sensi-ble à ce genre de message. Après tout, il s’agit de leurs infirmières qui soignent leur monde dans leur communauté. Et c’est peut-être notre atout le plus puissant pour amener les gens à nous aider dans notre combat.
Je vous demande donc de saisir toutes les occasions qui s’offrent à vous pour livrer vos témoignages personnels au public. Envoyez une lettre à une tribune libre, comme l’ont fait ces membres de l’AIIO, parlez à votre famille, à vos amis et à vos voisins. Il n’est pas nécessaire d’en faire une tâche compliquée et exigeante. Parlez simplement de ce que vous faites, de ce que vous savez, de ce à quoi vous devez faire face au travail pendant chacun de vos quarts et vous ne pouvez pas vous tromper.
un jugement à propos du sras envoie le mauvais message
lors qu’une autre pandémie de grippe menace et que le public se fie au gouvernement pour le protéger, il est ironique d’apprendre que la Cour d’appel de l’Ontario a jugé que le gouvernement ne
répondra pas de son inaction pendant la crise du SRAS en 2003.Je n’ai pas besoin de vous rappeler que nos vies ont été bouleversées
par le SRAS. Nous avons eu peur. Nous avons été mises en quarantaine. Nous avons été malades. De plus, nous avons malheureusement perdu deux de nos collègues. Nous avons fait tout ce qui a été demandé et plus encore. Tout ce que nous attendions en retour du gouvernement, c’était qu’il donne des directives aux hôpitaux pour assurer notre sécu-rité. Ils nous ont laissé tomber.
Leurs directives étaient inadéquates, elles sont arrivées trop tard et ont fait courir à nos membres le risque de contracter le SRAS. Ils ne nous ont pas informées des risques et ils ont prescrit des mesures de protection censées être appropriées, mais qui n’étaient tout simplement pas suffisantes. Nous avons sonné l’alarme, mais on nous a ignorées.
La Cour a jugé que le risque encouru faisait partie des risques du métier. Nous ne croyons pas que la mort devrait faire partie de notre travail! En fait, c’est dans le meilleur intérêt de tous de savoir que le gouvernement prend des mesures pour protéger les infirmières et les autres personnes qui risquent leur vie et leur santé chaque jour.
Chaque infirmière de cette province doit éprouver de l’indignation à la suite de ce jugement. Il dit que le gouvernement n’a pas la respon-sabilité d’offrir des conditions de travail et du matériel sécuritaires aux infirmières autorisées. C’est un mauvais message qu’il envoie, surtout en ce moment.
Bien que le gouvernement ait fait de grands progrès pour ce qui est des préparatifs, nous demandons si certains établissements sont assez bien préparés, si des programmes de dépistage adéquats sont en place, s’il y a assez de masques et d’équipement de protection approprié pour les travailleurs, si des plans sont en place pour faire face à une augmen-tation subite de personnes qui auront besoin de soins alors qu’il y a moins d’infirmières autorisées dans notre système de santé.
S’il y a une chose que cette décision a prouvée, c’est bien que vous avez plus que jamais besoin de votre syndicat. Si nous ne pouvons nous fier à notre gouvernement et à nos employeurs pour nous protéger, nous devrons le faire nous-mêmes. Je peux vous assurer que l’AIIO surveillera les choses d’un œil critique pour vous garantir des lieux de travail sécuritaires.
62324-2_ONA Front Line V9.indd 5 6/19/09 2:48:22 PM

6
ona MeMbers across onTario
FebruarY 2009
Improvements to ER Staffing, Thanks to IAC
ONA members take advantage of the day that commemorates the
struggles and gains of workers and the labour movement by taking their
concerns straight to the streets. On May 1, 2009 (May Day) members
from Region 3, including Shannon DaCunha (left photo), hand out ONA’s
Cutting Nurses, Cutting Care campaign flyers to downtown Toronto
commuters. On the same day, approximately 20 members from Quinte
Health Care in Belleville, Local 31, demonstrate outside of the offices
of the Southeast Local Health Integration Network and meet with their
Members Issue an SOS!What started out as a call to action from the Town of Fort Erie to protect
local hospital services turned into a mass protest of almost 4,000 con-
cerned citizens, including dozens of ONA members, at Queen’s Park.
Approximately 50 busloads of people from communities across On-
tario where local hospitals are threatened with major cuts or closures
joined together on April 29, 2009 at the Ontario legislature to send
an urgent SOS – Save Our Services – to the provincial government
and outline a strategy to protect local hospitals and save health care
services in the province.
Registered nurses at the St. Catharine’s site of
the Niagara Health System have been required
to perform more work than is consistent with
safe patient care because the ER has not been
staffed with the approved complement of
RNs, an Independent Assessment Committee
(IAC) has determined.
The IAC was engaged in 2008 following
four years of attempts by the hospital and the
Bargaining Unit of Local 26 to address pro-
fessional workload issues in the emergency
department of the St. Catharine’s site. Our
members did not feel that sufficient progress
was being made.
In its report released in March 2009, the
IAC concluded that the impact of the large
number of vacant RN positions on staff has
been exacerbated by high levels of sick time
and required overtime. The hospital attempted
to address the RN shortage by hiring regis-
tered practical nurses and registered respi-
ratory therapists (RRTs) into RN positions on
a temporary basis, and by the extensive use
of agency nurses. While RPNs and RRTs pro-
vide a value-added role to the ER, they can-
not replicate the level, nature, and complexity
of care provided by RNs, the IAC stated. The
difficulties resulting from consistent under-
staffing were further increased by the gap in
trust, confidence and respectful communica-
tion between the RNs and nursing leaders at
all levels.
Among the IAC’s 30 recommendations in
the areas of staffing and scheduling; commu-
nication and culture; and leadership are:
• TheChiefNursingExecutivepersonallyleads
discussion with the ER, RNs, clinical manag-
er, health program director and allied health
director to achieve consensus on how the
RNs and RRTs will practice together, and on
criteria for RN and RPN patient assignment.
• The hospital staffs the ER with 10 RNs
around the clock.
• The one-year RPN-Health Care Aide posi-
tions not be renewed after July 2009 and
revert to RN positions.
• The hospital develops a plan to decrease
nursing agency use in the ER.
• The hospital and ONA jointly undertake a
comprehensive evaluation of staffing, pa-
tient care needs and workload in September
2010 to determine whether additional staff
resources are required.
• Thehospitalimplementsastrategytoeval-
uate the impact of the IAC recommended
changes one year following implementa-
tion. BFL
“Health care is not a luxury to be enjoyed by people in large ur-
ban areas only,” said Local 35 Coordinator Shirley Roebuck, one of the
speakers at the event, whose local emergency room (the Sydenham
campus of the Chatham-Kent Health Alliance) is threatened. “The small
emergency departments across rural communities in all of Ontario play
a vital role in health care.”
Just hours after the protestors returned home, the Liberal government
voted to kill a motion by Progressive Conservative MPP Elizabeth Witmer
that the government “admits there’s a hospital funding crisis” and devel-
ops a plan to stop the firing of nurses and erase hospital deficits. BFL
Protestors converge on Queen’s Park on April 29, 2009 for a mass rally to decry threatened cuts to and closures of local hospitals. Local 35 Coordinator Shirley Roebuck (left), whose own emergency room faces closure and has been very active in this fight, was one of the passionate speakers at the event.
Members from Local 35 increase efforts to prevent the closure of their local emergency department by holding a rally outside of their MPP’s constituency office in Wallaceburg on April 18, 2009. A February 2009 report retained by the Local Health Integration Network recommended the closure of the emergency department of the Sydenham campus of the Chatham-Kent Alliance, and since that time, the Local has joined with community groups to try and stop the closure. This demonstration was part of a series of cross-province protests to stop the cuts to our hospitals, spearheaded by the Ontario Health Coalition.
62324-2_ONA Front Line V9.indd 6 6/19/09 2:48:25 PM

7June 2009
ONA members take advantage of the day that commemorates the
struggles and gains of workers and the labour movement by taking their
concerns straight to the streets. On May 1, 2009 (May Day) members
from Region 3, including Shannon DaCunha (left photo), hand out ONA’s
Cutting Nurses, Cutting Care campaign flyers to downtown Toronto
commuters. On the same day, approximately 20 members from Quinte
Health Care in Belleville, Local 31, demonstrate outside of the offices
of the Southeast Local Health Integration Network and meet with their
director to achieve consensus on how the
RNs and RRTs will practice together, and on
criteria for RN and RPN patient assignment.
• The hospital staffs the ER with 10 RNs
around the clock.
• The one-year RPN-Health Care Aide posi-
tions not be renewed after July 2009 and
revert to RN positions.
• The hospital develops a plan to decrease
nursing agency use in the ER.
• The hospital and ONA jointly undertake a
comprehensive evaluation of staffing, pa-
tient care needs and workload in September
2010 to determine whether additional staff
resources are required.
• Thehospitalimplementsastrategytoeval-
uate the impact of the IAC recommended
changes one year following implementa-
tion. BFL
“Health care is not a luxury to be enjoyed by people in large ur-
ban areas only,” said Local 35 Coordinator Shirley Roebuck, one of the
speakers at the event, whose local emergency room (the Sydenham
campus of the Chatham-Kent Health Alliance) is threatened. “The small
emergency departments across rural communities in all of Ontario play
a vital role in health care.”
Just hours after the protestors returned home, the Liberal government
voted to kill a motion by Progressive Conservative MPP Elizabeth Witmer
that the government “admits there’s a hospital funding crisis” and devel-
ops a plan to stop the firing of nurses and erase hospital deficits. BFL
RNs Take Complaints Straight to OLRBIn a precedent-setting move, ONA members
from Hamilton Health Sciences Centre, Local
70, St. Joseph’s Healthcare, Local 75, and To-
ronto’s University Health Network, Local 97,
are taking their fight against layoffs straight
to the Ontario Labour Relations Board (OLRB).
RNs are being cut and there will be de-
creases to hours of other positions at the hos-
pitals. The majority of nurses will be moved to
other areas, which may be out of their spe-
cialty. ONA is concerned that the transfers will
remove our members’ rights to take early re-
tirement, compensation packages or to bump
less senior nurses, which are available under
layoff language.
“The hospitals are not respecting the col-
lective agreement,” said ONA President Linda
Haslam-Stroud, “We are not going to give up
this fight and we are going to continue to ag-
gressively pursue any avenues we can.”
No date has been set for our hearing
against the hospitals, which also includes the
Ontario Hospital Association. Grievances have
also been filed. BFL
Not Going Down without a Fight!
Members from Local 35 increase efforts to prevent the closure of their local emergency department by holding a rally outside of their MPP’s constituency office in Wallaceburg on April 18, 2009. A February 2009 report retained by the Local Health Integration Network recommended the closure of the emergency department of the Sydenham campus of the Chatham-Kent Alliance, and since that time, the Local has joined with community groups to try and stop the closure. This demonstration was part of a series of cross-province protests to stop the cuts to our hospitals, spearheaded by the Ontario Health Coalition.
MPP for 20 minutes to discuss their working conditions, disrespect by
management and violation of rights (right photo). “I am happy we are
making some noise and are being heard,” said Local 31 Coordinator
Bernice MacCormack. Pictured are (left to right): Kim Beaugrand, Danni
Lynn Boyer, Kathy Cummings, Debbie Reed, Perry Simard.
May Day! May Day!
62324-2_ONA Front Line V9.indd 7 6/19/09 2:48:28 PM

June 20098
ona MeMbers across onTario
An ONA member has received 10,000 Aeroplan
miles for helping a distressed passenger on a
flight from Vancouver to Toronto.
Janet Arnold (pictured), a psychiatric nurse
at Sault Area Hospital, Local 46, was returning
to Toronto earlier this year when she saw a man
pacing around shortly after her Air Canada flight
departed. Noting that the flight attendants were
having a hard time with the man, who wouldn’t
sit in his seat, she offered to speak to him, and
did so for approximately an hour in a galley.
“He was very unpredictable and a little bit hard to understand,” she
said of the man whose final destination was Tunisia. “He didn’t really
threaten violence. He was so confused talking about where the plane
should be going – and that was the scary part.”
Arnold offered some relaxation tips, encouraging him to focus on com-
pleting the flight to Toronto. It did the trick and the man took his seat.
“I considered it a good Samaritan act, preventing the plane from
making an unscheduled landing to deal with the situation,” Arnold
said. “I was happy to help.”
For her successful intervention, Arnold was sent an e-mail of thanks
from Air Canada and credited with 10,000 miles in her Aeroplan ac-
count.
ONA sends our kudos to this very caring member! BFL
ONA leaders and members from Region 3 join ONA Vice-President Andy Summers for a Stewards Assembly, organized by the Toronto and York Region Labour Council on May 7, 2009 in Toronto. Solidarity in a Time of Crisis brought together stewards, staff and leaders from all unions in greater Toronto to discuss the looming challenges the economic crisis will put on wage levels, benefits, pensions and basic labour rights, and map out a united defence of our collective agreements and the standard of living of members. Pictured are (left to right): Local 95 member Michael Shiravand, Summers, Local 6 Coordinator Carolyn Edgar, Local 80 Bargaining Unit President Judie Surridge and Local 125 Coordinator Sandra Bearzot.
Our MeMBerS WrITe…
SARS LawsuitI am one of the nurses you represented in the SARS lawsuit. Thank you for the years of hard work and dedication that you and your staff devoted to our cause.
I was in court for day two of the hearing. I felt disappointed that the judges appeared disengaged and apathetic – needless to say, not well versed in the details of the case, when compared to the previous judge from the lower court.
My take away from the hearing related to Judge Sharpe alluding to the fact that we had signed up for this based on our professional choice. I feel there is a system in place to protect vulnerable workers, much like the security system in his lobby. When the system fails, resulting in death and life changing illness, there must be some sort of accountability.
The outcome of this hearing reflects an erosion of the judicial system, democracy and humanity. This is a slap in the face for ALL health care professionals, which unfortunately may very well manifest itself in the wake of another pandemic.
I trust that we will be able to continue our pursuit of justice.Kind regards,Sylvia Gordon, RNRegion 3
Violence Against NursesI am truly appalled at what I read in regards to the government not being responsible for nurses. We are the front lines. Shame, shame on the government! This is what makes all nurses cringe if they have daughters. My daughters, unfortunately or fortunately, chose not to go into nursing because of the actual abuse they saw that I, as an RN, have been through. I chose to be a nurse because of a passion to help others. I love people and love my nursing career. I am a dedicated, knowledgeable and hard working nurse, but I did not sign up to be a nurse knowing that I would or could die on the job. Yes, I am aware that there are perils in the front lines, especially nurses working in the emergency departments.
When firemen die of cancer, (the government) has given compensation for the firefighters because it was in the line of duty. How can the government not stand behind and beside us? Shame on the government at all levels.
Rosalinda Leo, RN, BScN, CDE Region 3
Showing Solidarity
ONA Welcomes New MembersONA has had a successful certification vote at the Wellington
Health Nursing Home in Prescott. As a result, we welcome seven
registered nurses to our organization.
Injured Workers Take Note!ONA is issuing an important notice to our injured members that the Workplace Safety and Insurance Board (WSIB), employers and insur-ance companies can and often do use video surveillance as evidence.
In many cases, the surveillance, which is legal, is used to try to show members performing functions that WSIB, employers and insurance companies don’t believe they should be able to do to qualify for benefits. That information may be used against them in different proceedings.
However, the use of this material and how it was obtained can be subject to a legal challenge by ONA.
YOu ASKeD uS . . .
What is ONA’s Position on Mandatory Flu Vaccines?With the H1N1 virus making daily headlines, many of you have asked
ONA for our position on mandatory influenza immunizations.
ONA’s All-Sector Strategic Bargaining Project Team recently de-
cided to delve into this issue further by examining collective agree-
ment language, relevant legislation, standards of nursing practice
and case law.
The team concluded that ONA will not issue an official position
on the benefits or detriments of the influenza vaccine. ONA mem-
bers have individual rights subject to particular collective agree-
ment language, which provides parameters. Please check your col-
lective agreement for particular language.
ONA believes that exposure to influenza is a hazard in all work-
places for all workers and reasonable controls should be applied
everywhere.
The College of Nurses of Ontario (CNO) has no immunization
requirements for nurses, and neither the CNO nor the Occupational Health and Safety Act require nurses to report their personal im-
munization status to the employer. However, some collective agree-
ments require that, at the time of an outbreak, members disclose
their status to employer health services. In a decision reported in
the winter 2009 issue of the CNO’s Standard, a director of Occu-
pational Health and Infection Control was disciplined for sending
an e-mail to staff on two units, listing the names of 14 staff she
believed had not received the influenza vaccine and who would not
be able to work in the event of an outbreak.
The CNO states that all nurses are accountable for knowing their
personal status relevant to their practice setting, and taking appro-
priate action to ensure client protection. In deciding whether to get
the influenza vaccine, the CNO suggests a nurse needs to examine
how contracting the flu could affect clients. BFL
ONA Member (soon to be) Flying high!
62324-2_ONA Front Line V9.indd 8 6/19/09 2:48:28 PM
9June 2009
Our MeMBerS WrITe…
SARS LawsuitI am one of the nurses you represented in the SARS lawsuit. Thank you for the years of hard work and dedication that you and your staff devoted to our cause.
I was in court for day two of the hearing. I felt disappointed that the judges appeared disengaged and apathetic – needless to say, not well versed in the details of the case, when compared to the previous judge from the lower court.
My take away from the hearing related to Judge Sharpe alluding to the fact that we had signed up for this based on our professional choice. I feel there is a system in place to protect vulnerable workers, much like the security system in his lobby. When the system fails, resulting in death and life changing illness, there must be some sort of accountability.
The outcome of this hearing reflects an erosion of the judicial system, democracy and humanity. This is a slap in the face for ALL health care professionals, which unfortunately may very well manifest itself in the wake of another pandemic.
I trust that we will be able to continue our pursuit of justice.Kind regards,Sylvia Gordon, RNRegion 3
Violence Against NursesI am truly appalled at what I read in regards to the government not being responsible for nurses. We are the front lines. Shame, shame on the government! This is what makes all nurses cringe if they have daughters. My daughters, unfortunately or fortunately, chose not to go into nursing because of the actual abuse they saw that I, as an RN, have been through. I chose to be a nurse because of a passion to help others. I love people and love my nursing career. I am a dedicated, knowledgeable and hard working nurse, but I did not sign up to be a nurse knowing that I would or could die on the job. Yes, I am aware that there are perils in the front lines, especially nurses working in the emergency departments.
When firemen die of cancer, (the government) has given compensation for the firefighters because it was in the line of duty. How can the government not stand behind and beside us? Shame on the government at all levels.
Rosalinda Leo, RN, BScN, CDE Region 3
ONA Welcomes New MembersONA has had a successful certification vote at the Wellington
Health Nursing Home in Prescott. As a result, we welcome seven
registered nurses to our organization.
Injured Workers Take Note!ONA is issuing an important notice to our injured members that the Workplace Safety and Insurance Board (WSIB), employers and insur-ance companies can and often do use video surveillance as evidence.
In many cases, the surveillance, which is legal, is used to try to show members performing functions that WSIB, employers and insurance companies don’t believe they should be able to do to qualify for benefits. That information may be used against them in different proceedings.
However, the use of this material and how it was obtained can be subject to a legal challenge by ONA.
YOu ASKeD uS . . .
What is ONA’s Position on Mandatory Flu Vaccines?With the H1N1 virus making daily headlines, many of you have asked
ONA for our position on mandatory influenza immunizations.
ONA’s All-Sector Strategic Bargaining Project Team recently de-
cided to delve into this issue further by examining collective agree-
ment language, relevant legislation, standards of nursing practice
and case law.
The team concluded that ONA will not issue an official position
on the benefits or detriments of the influenza vaccine. ONA mem-
bers have individual rights subject to particular collective agree-
ment language, which provides parameters. Please check your col-
lective agreement for particular language.
ONA believes that exposure to influenza is a hazard in all work-
places for all workers and reasonable controls should be applied
everywhere.
The College of Nurses of Ontario (CNO) has no immunization
requirements for nurses, and neither the CNO nor the Occupational Health and Safety Act require nurses to report their personal im-
munization status to the employer. However, some collective agree-
ments require that, at the time of an outbreak, members disclose
their status to employer health services. In a decision reported in
the winter 2009 issue of the CNO’s Standard, a director of Occu-
pational Health and Infection Control was disciplined for sending
an e-mail to staff on two units, listing the names of 14 staff she
believed had not received the influenza vaccine and who would not
be able to work in the event of an outbreak.
The CNO states that all nurses are accountable for knowing their
personal status relevant to their practice setting, and taking appro-
priate action to ensure client protection. In deciding whether to get
the influenza vaccine, the CNO suggests a nurse needs to examine
how contracting the flu could affect clients. BFL
ONA provincial and Local leaders, members and staff join our allies and other concerned citizens at a Canadian Auto Workers rally on April 23, 2009 at Queen’s Park in Toronto, demanding stronger pension protections from government and corporations. The global financial crisis and economic recession has put Canadian pension plans in an increasingly precarious state, calling into question their ongoing viability. Pictured are (left to right): Local 125 Coordinator Sandra Bearzot, Region 3 Vice-President Andy Summers, Region 5 Vice-President Karen Bertrand, ONA President Linda Haslam-Stroud.
Local leaders from Region 2, flanked by their Vice-President Anne Clark (in lime green), receive media training at their spring Area Coordinators Conference (ACC) in Cornwall on May 20, 2009. ACCs provide Local Coordinators and Bargaining Unit Presidents with an opportunity to discuss the business of their Local, current trends and concerns, upcoming events and other important issues, and receive education on key issues.
Fighting for Pension Protection
Managing the Media
62324-2_ONA Front Line V9.indd 9 6/19/09 2:48:30 PM
June 200910
NursiNg Week 2009
Our Nurses. Respected, Vital Professionals. Caring for You.
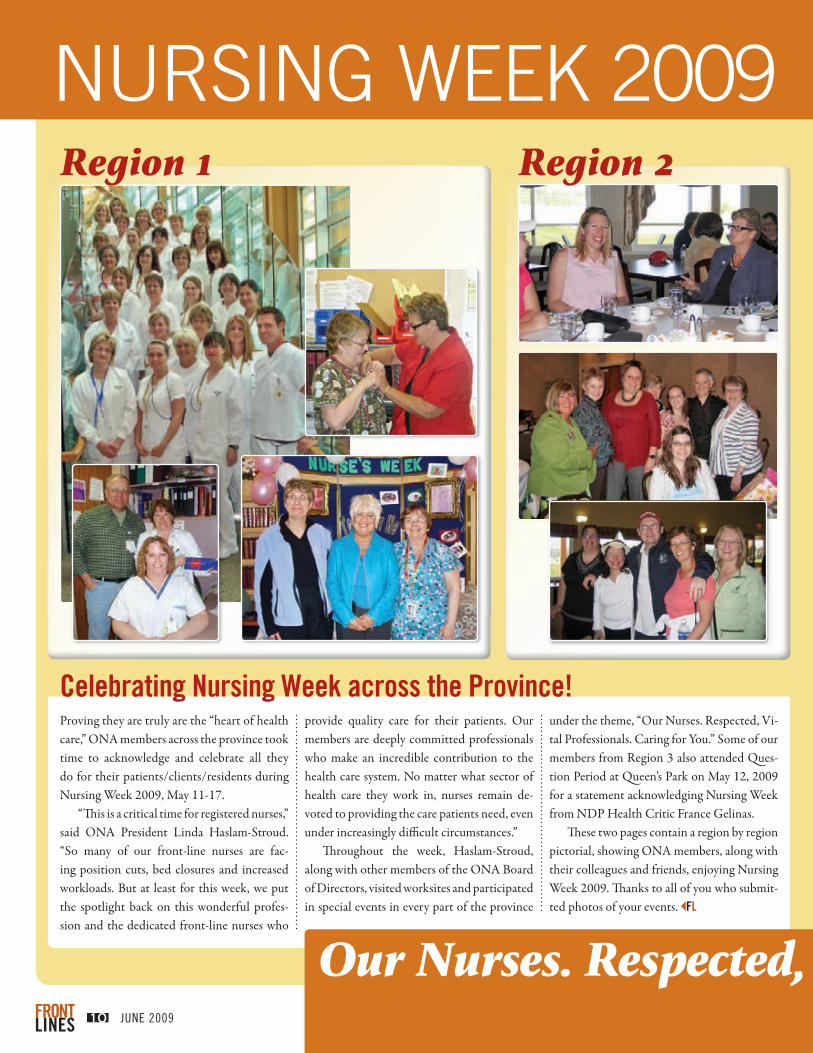
Celebrating Nursing Week across the Province!Proving they are truly are the “heart of health care,” ONA members across the province took time to acknowledge and celebrate all they do for their patients/clients/residents during Nursing Week 2009, May 11-17.
“This is a critical time for registered nurses,” said ONA President Linda Haslam-Stroud. “So many of our front-line nurses are fac-ing position cuts, bed closures and increased workloads. But at least for this week, we put the spotlight back on this wonderful profes-sion and the dedicated front-line nurses who
provide quality care for their patients. Our members are deeply committed professionals who make an incredible contribution to the health care system. No matter what sector of health care they work in, nurses remain de-voted to providing the care patients need, even under increasingly difficult circumstances.”
Throughout the week, Haslam-Stroud, along with other members of the ONA Board of Directors, visited worksites and participated in special events in every part of the province
under the theme, “Our Nurses. Respected, Vi-tal Professionals. Caring for You.” Some of our members from Region 3 also attended Ques-tion Period at Queen’s Park on May 12, 2009 for a statement acknowledging Nursing Week from NDP Health Critic France Gelinas.
These two pages contain a region by region pictorial, showing ONA members, along with their colleagues and friends, enjoying Nursing Week 2009. Thanks to all of you who submit-ted photos of your events. BFL
Region 2
Region 5
Region 3Region 1
62324-2_ONA Front Line V9.indd 10 6/19/09 2:48:33 PM

NursiNg Week 2009
Our Nurses. Respected, Vital Professionals. Caring for You.
under the theme, “Our Nurses. Respected, Vi-tal Professionals. Caring for You.” Some of our members from Region 3 also attended Ques-tion Period at Queen’s Park on May 12, 2009 for a statement acknowledging Nursing Week from NDP Health Critic France Gelinas.
These two pages contain a region by region pictorial, showing ONA members, along with their colleagues and friends, enjoying Nursing Week 2009. Thanks to all of you who submit-ted photos of your events. BFL
Region 5
June 2009 11
Region 4Region 3
62324-2_ONA Front Line V9.indd 11 6/19/09 2:48:38 PM

June 20091212
ona neWs
survey of Nurse Abuse no shock to ONAA Statistics Canada study revealing that one-third of all nurses
polled in Canada were physically assaulted by a patient in 2005 is
not shocking to ONA.
The report, which included new details in a 2005 study on
workplace risks originally released the following year, found that
34 per cent of nurses polled who worked in hospitals and long-
term care in 2005 reported being physically assaulted by patients
over the previous 12 months. Forty-seven per cent reported psy-
chological abuse. Psychiatric nurses and male nurses appeared
particularly at risk in the study of responses from 12,200 nurses,
part of a larger study involving 218,000 nurses. The odds that
nurses would report physical assault or emotional abuse tended to
be high among those who thought there wasn’t enough staffing at
their facility, the authors noted.
“Sadly, this report was not a shock to me at all and will not
by any means be a shock to front-line nurses,” said ONA Presi-
dent Linda Haslam-Stroud. “In fact, the numbers may actually be
higher because nurses generally underreport violence in the work-
place. We’re living it each and every day. We will continue to lobby
the government to ensure appropriate safety laws are in place.
These statistics can only help with that fight.”
To view the entire survey, log onto the StatsCanada website
at www.statcan.gc.ca. BFL
Ohs Act Amendments Need Work, ONA saysWhile amendments to the province’s Occupational Health and Safety Act (Bill 168) to protect workers from workplace violence and harass-
ment are a step in the right direction, ONA is concerned that they don’t
go far enough.
The proposed legislation, Bill 168, will require employers to develop
a framework that would include policies and programs to help prevent
workplace violence and harassment; will require employers to take rea-
sonable precautions to protect an employee from domestic violence
in the workplace; and will allow workers to remove themselves from
harmful situations if they have reason to believe that they are at risk
of imminent danger due to workplace violence.
“We are pleased to see that the government is finally taking steps
to address long-standing issues of violence and harassment that nurs-
es face in their workplaces,” said ONA President Linda Haslam-Stroud.
“However, we are concerned that issues raised in the Lori Dupont inquest
will not be adequately covered under Bill 168 as currently written.”
The Ministry of Health and Long-Term Care has also appointed two
Healthy Work Environment Champions – Rob Devitt, President and CEO
of Toronto East General Hospital, and Dr. Heather Laschinger, a uni-
versity professor and Associate Director of Nursing Research at the
University of Western Ontario – to provide advice on implementation
of the government’s strategy to prevent workplace violence and create
safe work environments for health care workers.
ONA has been lobbying for improvements to the Act for several
years and will be proposing amendments to the revised Act. BFL
ONA President Linda Haslam-Stroud fields media questions during a scrum follow-ing the reading of the Ontario budget at Queen’s Park on March 26, 2009.
ONA President Linda Haslam-Stroud (right) chats with a CTV reporter on the StatsCanada survey on violence against RNs in her office at the ONA provincial office in downtown Toronto on April 15, 2009.
shortage Can be eliminated, CNA Report showsCanada could have a shortfall of 60,000 regis-
tered nurses by the year 2022, but the short-
ages could be averted and care bolstered by
instituting a series of simple policy mea-
sures that would make nurses more efficient,
healthier, happier and on the job longer,” a
study commissioned by the Canadian Nurses
Association (CNA) says.
Tested Solutions for Eliminating Canada’s Registered Nurse Shortage reports there are
currently 217,000 registered nurses in Canada,
the single largest group of health care provid-
ers, but that work force is aging and, increas-
ingly, nurses are leaving the profession early
because of the physical and mental strain, and
lack of flexibility in their work schedules and
time for education and research.
However, if six policy scenarios were un-
dertaken collectively and immediately, the
nursing shortage could be eliminated in 15
years while halving existing levels of in-mi-
gration and recruitment, the report states. The
scenarios are:
• IncreasingRNproductivity.
• Increasingenrolmentinnursing
programs.
• Reducingabsenteeism.
• Improvingretentionofpracticing
nurses.
• Gettingmorenursestoworkto
retirement age.
• Reducingtherecruitmentofnurses
from developing countries.
“Nurses are burning out earlier or getting
injured on the job more than other workers,”
Canadian Federation of Nurses Unions Presi-
dent Linda Silas said. “Nurses’ unions across
Canada are looking to work with government,
employers and the nursing professional asso-
ciations to improve the health and wellbeing
of nurses to retain them longer in the work-
force.”
To read the full report, log onto the CNA’s
website at www.cna-nurses.ca. BFL
62324-2_ONA Front Line V9.indd 12 6/19/09 2:48:40 PM

13June 2009
shortage Can be eliminated, CNA Report showsCanada could have a shortfall of 60,000 regis-
tered nurses by the year 2022, but the short-
ages could be averted and care bolstered by
instituting a series of simple policy mea-
sures that would make nurses more efficient,
healthier, happier and on the job longer,” a
study commissioned by the Canadian Nurses
Association (CNA) says.
Tested Solutions for Eliminating Canada’s Registered Nurse Shortage reports there are
currently 217,000 registered nurses in Canada,
the single largest group of health care provid-
ers, but that work force is aging and, increas-
ingly, nurses are leaving the profession early
because of the physical and mental strain, and
lack of flexibility in their work schedules and
time for education and research.
However, if six policy scenarios were un-
dertaken collectively and immediately, the
nursing shortage could be eliminated in 15
years while halving existing levels of in-mi-
gration and recruitment, the report states. The
scenarios are:
• IncreasingRNproductivity.
• Increasingenrolmentinnursing
programs.
• Reducingabsenteeism.
• Improvingretentionofpracticing
nurses.
• Gettingmorenursestoworkto
retirement age.
• Reducingtherecruitmentofnurses
from developing countries.
“Nurses are burning out earlier or getting
injured on the job more than other workers,”
Canadian Federation of Nurses Unions Presi-
dent Linda Silas said. “Nurses’ unions across
Canada are looking to work with government,
employers and the nursing professional asso-
ciations to improve the health and wellbeing
of nurses to retain them longer in the work-
force.”
To read the full report, log onto the CNA’s
website at www.cna-nurses.ca. BFL
ONA Mourns Fallen, Injured WorkersThe sky was grey and the mood somber as
ONA, our union allies and politicians re-
membered those who have fallen or been
injured while on the job, and called for ac-
tion to eliminate hazardous working condi-
tions at the annual Day of Mourning ser-
vices in Toronto.
On April 28, 2009, ONA Region 3 Vice-
President Andy Summers (pictured) told the
gathering outside of City Hall that in addi-
tion to threats posed by infectious diseases
and registered nursing position cuts, front-
line nurses continue to face workplace vio-
lence and abuse in record numbers.
“Being a front-line nurse is a dangerous
business right now,” he said. “Nurses suffer
some of the highest rates of injury, sickness
and burnout due to stress, workload, under-
staffing and job conditions. We are here to-
day to commemorate our colleagues and also
acknowledge the challenges our health care
workers face on the front lines.”
The overall statistics are grim: 488 On-
tario workers died last year because of their
work, and 317,000 injuries and occupational
diseases were reported to the Workplace
Safety and Insurance Board. These totals do
not cover the thousands of workers who die
each year of cancer, lung disease and other ill-
nesses caused by exposure to toxic substances
on the job that have gone unreported or mis-
diagnosed.
More than 100 countries participate in
Day of Mourning activities. BFL
ONA President Heads EastFollowing her presentation to the Health Boards Association of Newfoundland and Labrador in St. John’s on April 2, 2009, ONA President Linda Haslam-Stroud poses with conference organizer Mark Gill. Haslam-Stroud spoke about the No-vember 2005 murder of ONA member Lori Du-pont, the coroner’s jury recommendations into her death, workplace safety, and ONA action.
62324-2_ONA Front Line V9.indd 13 6/19/09 2:48:42 PM
June 200914
ona neWs
NeWS IN BrIef
E Ontario’s push to shorten ER wait times is having an unintended consequence for some
patients, ONA President Linda Haslam-Stroud
has told the media. “There is no surge capac-
ity in the system,” she said, adding that On-
tario hospitals aren’t prepared for the poten-
tial crush of patients that would occur during
a flu pandemic. Shipping patients out of the
ER quickly is resulting in “hallway nursing” –
patients being cared for in the hallways or
other units, identified by a sticky note - with
insufficient numbers of nurses to provide
care and no privacy. ONA continues to warn
Minister of Health and Long-Term Care David
Caplan of the dangers of hallway nursing, but
our concerns have largely been dismissed.
E The Canadian Health Coalition has launched a national campaign to save pub-
lic health care because it says Canadians are
being misled about the benefits of privatized
care in hopes of lulling them into accepting
for-profit services. The national campaign,
launched in New Brunswick in May, will
travel to communities throughout Canada
to hold townhall meetings on the threat of
privatized for-profit services. A new website
– www.medicare.ca – encourages Canadians
to get involved in the fight.
E The Ontario Hospital Association has launched a website to present and explain
current hospital information to the gen-
eral public. The website allows users to
learn more about how their hospitals are
performing by location, type of care or one
of 39 health indicators, including hospital
death rates and C. difficile infection rates.
The website’s address is myhospitalcare.ca.
NAMeS IN THe NeWS
E A registered nurse from Sudbury is president-elect of the Registered Nurses As-
sociation of Ontario. DAVID MCNEIL, who
will assume the presidency next April, is
Vice-President of Clinical Programs and Chief
Nursing Officer of Sudbury Regional Hospital.
on a sample of 3,650 health care workers,
including 941 nurses, in Texas. American
researchers found a range of chemicals in
hospitals could irritate the lungs, including
cleansers and antiseptics used on patients’
skin, chemicals used for sterilizing equip-
ment and all-purpose cleaners.
E Careers in the health care sector are in high demand, topping the list of occupa-
tions showing signs of shortages at the na-
tional level, a new report reveals. “Through-
out the 1990s, growth in the health and
social assistance sector was minimal as
governments in Canada cut back signifi-
cantly on health care spending in order
to bring deficits under control,” the report
Looking Ahead: A 10-Year Outlook for the Canadian Labour Market states.
E Nurses are second only to mothers on a list of the hardest working Canadians,
a Workopolis survey of 4,000 Canadians
finds. The survey shows that employees
are averaging an extra three hours a week
on the job and feel they are working “too
hard.” Half said they work harder because
it’s expected of them and is the nature of
their job.
E The shortage of nurses and doctors topped the list of concerns Ontarians have with
our health care system, a Toronto Star poll
reveals. Seventy-two per cent of Ontarians
said they are confident they would receive
the help needed, but 43 per cent would
consider travelling abroad to avoid long
wait times for certain services.
E Canadian nursing homes use restraints on elderly residents more than most coun-
tries in the world, a new study finds. Ca-
nadian homes use restraints or belts on
almost one-third of residents, despite
years of evidence suggesting that their use
brings negative side effects, the study says,
adding that Canada should adopt strict
nursing home legislation, such as the U.S.
Ontario has new legislation that imposes
guidelines on nursing homes.
COuNTerpArTS
E The Newfoundland and Labrador Nurses Union has ratified a four-year
deal that raises wages and provides in-
creases to shift differential and standby
rates, and education leaves. The contract
was reached with the province only
hours before the nurses were scheduled
to hit the picket lines on May 20, 2009.
E The British Columbia Nurses Union has reached an agreement with the
province to extend its contract by two
years. The agreement comes with a 3 per
cent labour market adjustment in 2010
and 2011 and a scheduled 4.2 per cent
wage increase this past April. The deal is
intended to retain nurses in the province
as the nursing shortage worsens.
E The New Brunswick Nurses Union (NBNU) is concerned that the govern-
ment’s new interest in physician assis-
tants may drain resources from nurse
practitioners. A report from the prov-
ince’s Department of Health on how to
introduce physician assistants is being
studied by the government. “I hoped
that as the years go on, we would ed-
ucate more nurse practitioners,” said
NBNU President Marilyn Quinn. “I think
there are many more places they could
be practising that we haven’t explored
yet.” She added that the province should
commit sufficient resources to make
sure nurse practitioners are used to their
potential.
E The Manitoba Nurses Union is criticizing the province’s practice of
publishing the names of nurses who re-
peatedly abuse drugs or alcohol in the
magazine and website of the Manitoba
College of Nurses. Union President San-
di Mowat said the public should know
about serious offences such as patient
abuse, but people who are addicted to
drugs or alcohol should not have their
names broadcast for all to see.
E A partnership between the Saskatchewan Union of Nurses and the provincial govern-
ment 14 months ago has resulted in 159 more
registered nurses and registered practical
nurses than last year, achieving 20 per cent
of the 800 target, the two groups say. Nursing
vacancies have also declined, from 793 last
fall to 617 in December. Under the agreement,
the province committed $60-million to the
Saskatchewan Association of Health Organi-
zations to cover the first year’s salary for the
additional nurses.
E In a dramatic move to unite the power and influence of America’s leading RN organiza-
tions, the United American Nurses, California
Nurses Association/National Nurses Orga-
nizing Committee, and the Massachusetts
Nurses Association have announced they’re
joining together to form a new 150,000 mem-
ber association. The new union of nurse-led
organizations, the United American Nurses-
National Nurses Organization Committee,
resolves to build an RN movement to defend
and advance the interest of front-line nurses;
organize all non-union front-line nurses; pro-
vide a powerful voice for RN rights and safe
practice; provide a vehicle for solidarity with
sister nurse and allied organizations around
the world; and create a national pension for
union RNs.
E The California Nurses Association and the
Service Employees International Union – two
of the fastest growing unions in the U.S. –
have agreed to work together to unionize
hospital workers and push for universal health
care. While the two unions were once rivals,
they said now is the time to unite to push for
a better health care system.
reCeNT STuDIeS
E Nurses who are exposed to cleaning products, antiseptics and disinfectants in hos-
pitals have an increased risk of contracting
asthma by 70 per cent, research has discovered.
The findings, published in the journal Occupa-tional and Environmental Medicine, are based
62324-2_ONA Front Line V9.indd 14 6/19/09 2:48:43 PM
15June 2009
JI_ONA_Apr09_FINAL.eps 1 21/04/09 3:52 PM
on a sample of 3,650 health care workers,
including 941 nurses, in Texas. American
researchers found a range of chemicals in
hospitals could irritate the lungs, including
cleansers and antiseptics used on patients’
skin, chemicals used for sterilizing equip-
ment and all-purpose cleaners.
E Careers in the health care sector are in high demand, topping the list of occupa-
tions showing signs of shortages at the na-
tional level, a new report reveals. “Through-
out the 1990s, growth in the health and
social assistance sector was minimal as
governments in Canada cut back signifi-
cantly on health care spending in order
to bring deficits under control,” the report
Looking Ahead: A 10-Year Outlook for the Canadian Labour Market states.
E Nurses are second only to mothers on a list of the hardest working Canadians,
a Workopolis survey of 4,000 Canadians
finds. The survey shows that employees
are averaging an extra three hours a week
on the job and feel they are working “too
hard.” Half said they work harder because
it’s expected of them and is the nature of
their job.
E The shortage of nurses and doctors topped the list of concerns Ontarians have with
our health care system, a Toronto Star poll
reveals. Seventy-two per cent of Ontarians
said they are confident they would receive
the help needed, but 43 per cent would
consider travelling abroad to avoid long
wait times for certain services.
E Canadian nursing homes use restraints on elderly residents more than most coun-
tries in the world, a new study finds. Ca-
nadian homes use restraints or belts on
almost one-third of residents, despite
years of evidence suggesting that their use
brings negative side effects, the study says,
adding that Canada should adopt strict
nursing home legislation, such as the U.S.
Ontario has new legislation that imposes
guidelines on nursing homes.
E A partnership between the Saskatchewan Union of Nurses and the provincial govern-
ment 14 months ago has resulted in 159 more
registered nurses and registered practical
nurses than last year, achieving 20 per cent
of the 800 target, the two groups say. Nursing
vacancies have also declined, from 793 last
fall to 617 in December. Under the agreement,
the province committed $60-million to the
Saskatchewan Association of Health Organi-
zations to cover the first year’s salary for the
additional nurses.
E In a dramatic move to unite the power and influence of America’s leading RN organiza-
tions, the United American Nurses, California
Nurses Association/National Nurses Orga-
nizing Committee, and the Massachusetts
Nurses Association have announced they’re
joining together to form a new 150,000 mem-
ber association. The new union of nurse-led
organizations, the United American Nurses-
National Nurses Organization Committee,
resolves to build an RN movement to defend
and advance the interest of front-line nurses;
organize all non-union front-line nurses; pro-
vide a powerful voice for RN rights and safe
practice; provide a vehicle for solidarity with
sister nurse and allied organizations around
the world; and create a national pension for
union RNs.
E The California Nurses Association and the
Service Employees International Union – two
of the fastest growing unions in the U.S. –
have agreed to work together to unionize
hospital workers and push for universal health
care. While the two unions were once rivals,
they said now is the time to unite to push for
a better health care system.
reCeNT STuDIeS
E Nurses who are exposed to cleaning products, antiseptics and disinfectants in hos-
pitals have an increased risk of contracting
asthma by 70 per cent, research has discovered.
The findings, published in the journal Occupa-tional and Environmental Medicine, are based
62324-2_ONA Front Line V9.indd 15 6/19/09 2:48:43 PM

June 200916
Fight to save local hospitals Must continuelip through the pages of this issue of Front Lines and you will see photo after photo of members throughout Ontario engaging in political action to preserve something very close to their hearts:
services at their local hospitals. But with more hospitals on the chop-ping block, never has this fight been so important.
While it’s true that some of these local hospitals may be small and seemingly unimportant to the government, the care they provide is just as critical to their citizens as their urban counterparts, which are also facing serious cuts of their own. These local hospitals ensure their communities have access to the lifesaving care that every Ontarian has the right to expect.
The government has responded to our lobbying efforts by imple-menting a task force to look into rural health. But there is no promise to save the services that have been or are being cut and it is not at all clear who is on this task force, nor its mandate and timelines. We need the cuts to stop and we need them to stop now!
We are also concerned about recent comments in the media from Premier McGuinty, who said he received advice that cutting local emergency departments and creating so-called “centres of excellence,” where resources are consolidated, would provide better care. But this doesn’t take into account problems that seem obvious to us, such as in-adequate transportation to these centres, impassable rural roads in se-vere weather, the risk to patients who have to travel further for urgent care, and thousands of patients descending on these centres without the funding or staff to provide them with care. I’d say the term “centres of excellence” is rather ironic and misleading.
I hope you will be inspired by the stories of your colleagues in this issue and join the fight. Please call, fax or e-mail Premier McGuinty and your local MPP and demand a moratorium on hospital cuts and closures, and policy to protect small and rural hospitals across On-tario. The Ontario Health Coalition is intensifying its campaigns to save these services, and I encourage you to check out its website at www.ontariohealthcoalition.ca for information on how you can get involved. If we don’t, I fear health care may become a luxury only af-forded to those who live in urban centres.
From First Vice-President
Vicki McKenna, RN
F e
E The Ministry of Health and Long-Term Care is redesigning the compliance inspection program for long-term care (LTC) homes to comply with the new Long-Term Care Homes Act, 2007. New regulations to support the implementation of the legislation are also being developed. The compliance inspection redesign is in-tended to provide a more accountable and risk-focused program. Enhancements to the program will include the implementation of risk indicators linked with new technology. This is intended to result in early detection of compliance issues and timely resolu-tion of potential issues. Planning for the Compliance Transfor-mation Project began in late 2007 and formally launched in April 2008. By 2010, each LTC resident will be assessed upon admis-sion to a LTC home using a software tool called the Resident As-sessment Instrument (RAI), and then every three months (each quarter) or when there is a significant change in condition. Cur-rently, the RAI is rolled out to 35 per cent (217) of LTC homes. As of January 2009, RAI-MDS has rolled out to all LTC homes in Ontario in three phases over nine to 12 months. Critical Inci-dent System software that allows LTC homes to securely report “unusual occurrences” online to Ministry compliance staff has been implemented across all LTC homes in Ontario as of April 2008. The inspection and appeals process is being redesigned to focus on a LTC resident’s quality of care and quality of life, with input from the risk indicators to be published on the Ministry website in spring 2009.
E Dr. Arlene King has been named the province’s new Chief Medi-cal Officer of Health, effective June 15, 2009. Dr. King is formerly Director General of the Centre for Immunization and Respira-tory Infectious Diseases at the Public Health Agency of Canada. She has been working in the field of public health since 1992 and has held various positions in communicable disease control at the British Columbia Centre for Disease Control, and served as a Medical Officer of Health in Burnaby and Vancouver. B.C. Act-ing Chief Medical Officer of Health Dr. David Williams will re-assume his position as Associate Chief Medical Officer of Health, Health Protection and Prevention this month.
E Graham Scott has been appointed supervisor of Quinte Health-care Corporation (QHC) to address governance and financial is-sues. Scott, a former Deputy Minister of Health, will oversee the implementation of recommendations from a 2006 assessment on governance and related matters at QHC. He will also be fol-lowing up on steps recommended in a 2008 review of a system performance report by Ken Tremblay. As supervisor, Scott will assume full powers of the hospital board, the corporation, its of-ficers and members of the corporation. Scott will report directly to the Minister of Health and Long-Term Care.
Queen’s park upDaTe
nous devons continuer de nous battre pour sauver les hôpitaux locaux
n feuilletant les pages de ce numéro de Front Lines, vous aper-cevrez les nombreuses photos de nos membres qui, d’un bout à l’autre de l’Ontario, se lancent dans l’action politique dans l’es-
poir de préserver une chose qui leur tient particulièrement à cœur : les services des hôpitaux de leur localité.
Bien que certains hôpitaux locaux soient petits et puissent sembler insignifiants pour le gouvernement, les soins qu’ils offrent aux rési-dants de ces régions sont aussi essentiels que les soins fournis par les établissements urbains, qui sont également aux prises avec d’impor-tantes compressions. Les hôpitaux locaux assurent à leurs collectivités l’accès aux soins vitaux auxquels tous les Ontariens ont droit.
Le gouvernement a répondu aux efforts déployés par nos groupes de pression en mettant sur pied un groupe de travail qui se penchera sur les soins de santé en milieu rural. Cependant, aucune promesse n’a été faite concernant les services qui ont été éliminés ou qui sont en voie de l’être, et nous ne savons rien des membres de ce groupe de travail, ni de leur mandat et de leur échéancier.
Nous nous inquiétons également des récents commentaires du pre-mier ministre McGuinty dans les médias. M. McGuinty a déclaré qu’on lui a conseillé d’éliminer les services d’urgence locaux et de créer de soi-disant « centres d’excellence » où les ressources sont regroupées afin d’améliorer les soins. Ces conseils ne tiennent toutefois pas compte de certains problèmes qui nous paraissent évidents : les moyens de transport inadéquats vers ces centres, les routes rurales impraticables en cas d’in-tempérie, le risque pour les patients qui doivent franchir de plus grandes distances pour obtenir des soins d’urgence et le fait que des milliers de patients se retrouvent dans des centres qui ne disposent pas du finance-ment ou du personnel nécessaire pour leur offrir des soins. À mon avis, l’expression « centres d’excellence » est plutôt ironique et trompeuse.
J’espère que les histoires de vos collègues qui sont présentées dans ce numéro vous inspireront et que vous vous rallierez à notre combat. Je vous invite à communiquer avec le premier ministre McGuinty et votre député, que ce soit par téléphone, télécopieur ou courrier électro-nique, et à réclamer un moratoire sur les compressions et les fermetures dans les hôpitaux, ainsi qu’une politique visant à protéger les petits établissements ruraux partout en Ontario. L’Ontario Health Coali-tion intensifie actuellement les campagnes qu’elle mène pour sauver ces services, et je vous encourage à aller consulter son site Web, à www.ontariohealthcoalition.ca, pour savoir comment vous pouvez y prendre part. Si nous ne faisons rien, j’ai bien peur que les soins de santé devien-nent un luxe uniquement accessible aux résidants des centres urbains.
62324-2_ONA Front Line V9.indd 16 6/19/09 2:48:44 PM

17June 2009
E The Ministry of Health and Long-Term Care is redesigning the compliance inspection program for long-term care (LTC) homes to comply with the new Long-Term Care Homes Act, 2007. New regulations to support the implementation of the legislation are also being developed. The compliance inspection redesign is in-tended to provide a more accountable and risk-focused program. Enhancements to the program will include the implementation of risk indicators linked with new technology. This is intended to result in early detection of compliance issues and timely resolu-tion of potential issues. Planning for the Compliance Transfor-mation Project began in late 2007 and formally launched in April 2008. By 2010, each LTC resident will be assessed upon admis-sion to a LTC home using a software tool called the Resident As-sessment Instrument (RAI), and then every three months (each quarter) or when there is a significant change in condition. Cur-rently, the RAI is rolled out to 35 per cent (217) of LTC homes. As of January 2009, RAI-MDS has rolled out to all LTC homes in Ontario in three phases over nine to 12 months. Critical Inci-dent System software that allows LTC homes to securely report “unusual occurrences” online to Ministry compliance staff has been implemented across all LTC homes in Ontario as of April 2008. The inspection and appeals process is being redesigned to focus on a LTC resident’s quality of care and quality of life, with input from the risk indicators to be published on the Ministry website in spring 2009.
E Dr. Arlene King has been named the province’s new Chief Medi-cal Officer of Health, effective June 15, 2009. Dr. King is formerly Director General of the Centre for Immunization and Respira-tory Infectious Diseases at the Public Health Agency of Canada. She has been working in the field of public health since 1992 and has held various positions in communicable disease control at the British Columbia Centre for Disease Control, and served as a Medical Officer of Health in Burnaby and Vancouver. B.C. Act-ing Chief Medical Officer of Health Dr. David Williams will re-assume his position as Associate Chief Medical Officer of Health, Health Protection and Prevention this month.
E Graham Scott has been appointed supervisor of Quinte Health-care Corporation (QHC) to address governance and financial is-sues. Scott, a former Deputy Minister of Health, will oversee the implementation of recommendations from a 2006 assessment on governance and related matters at QHC. He will also be fol-lowing up on steps recommended in a 2008 review of a system performance report by Ken Tremblay. As supervisor, Scott will assume full powers of the hospital board, the corporation, its of-ficers and members of the corporation. Scott will report directly to the Minister of Health and Long-Term Care.
Queen’s park upDaTe
nous devons continuer de nous battre pour sauver les hôpitaux locaux
n feuilletant les pages de ce numéro de Front Lines, vous aper-cevrez les nombreuses photos de nos membres qui, d’un bout à l’autre de l’Ontario, se lancent dans l’action politique dans l’es-
poir de préserver une chose qui leur tient particulièrement à cœur : les services des hôpitaux de leur localité.
Bien que certains hôpitaux locaux soient petits et puissent sembler insignifiants pour le gouvernement, les soins qu’ils offrent aux rési-dants de ces régions sont aussi essentiels que les soins fournis par les établissements urbains, qui sont également aux prises avec d’impor-tantes compressions. Les hôpitaux locaux assurent à leurs collectivités l’accès aux soins vitaux auxquels tous les Ontariens ont droit.
Le gouvernement a répondu aux efforts déployés par nos groupes de pression en mettant sur pied un groupe de travail qui se penchera sur les soins de santé en milieu rural. Cependant, aucune promesse n’a été faite concernant les services qui ont été éliminés ou qui sont en voie de l’être, et nous ne savons rien des membres de ce groupe de travail, ni de leur mandat et de leur échéancier.
Nous nous inquiétons également des récents commentaires du pre-mier ministre McGuinty dans les médias. M. McGuinty a déclaré qu’on lui a conseillé d’éliminer les services d’urgence locaux et de créer de soi-disant « centres d’excellence » où les ressources sont regroupées afin d’améliorer les soins. Ces conseils ne tiennent toutefois pas compte de certains problèmes qui nous paraissent évidents : les moyens de transport inadéquats vers ces centres, les routes rurales impraticables en cas d’in-tempérie, le risque pour les patients qui doivent franchir de plus grandes distances pour obtenir des soins d’urgence et le fait que des milliers de patients se retrouvent dans des centres qui ne disposent pas du finance-ment ou du personnel nécessaire pour leur offrir des soins. À mon avis, l’expression « centres d’excellence » est plutôt ironique et trompeuse.
J’espère que les histoires de vos collègues qui sont présentées dans ce numéro vous inspireront et que vous vous rallierez à notre combat. Je vous invite à communiquer avec le premier ministre McGuinty et votre député, que ce soit par téléphone, télécopieur ou courrier électro-nique, et à réclamer un moratoire sur les compressions et les fermetures dans les hôpitaux, ainsi qu’une politique visant à protéger les petits établissements ruraux partout en Ontario. L’Ontario Health Coali-tion intensifie actuellement les campagnes qu’elle mène pour sauver ces services, et je vous encourage à aller consulter son site Web, à www.ontariohealthcoalition.ca, pour savoir comment vous pouvez y prendre part. Si nous ne faisons rien, j’ai bien peur que les soins de santé devien-nent un luxe uniquement accessible aux résidants des centres urbains.
E As PARt OF Its “Hospital Cuts Threaten our Health” campaign,
the OHC is holding a series of townhall meetings across the
province on the hospital cuts happening throughout Ontario.
The meetings will raise community awareness about the cuts
and ask for support in the fight back. Cutting nursing staff is
very serious and is affecting patient care, and we need to be
cautious about “downloading patients out of hospital beds into
very inappropriate care settings or not providing enough care
for them,” said OHC Director Natalie Mehra. Members of the
ONA Board of Directors, Local leaders, members and staff have
attended several of the townhalls, distributing information on
and material from our Cutting Nurses, Cutting Care campaign.
E the stAted gOALs of the Ministry of Health and Long-Term Care
to provide effective whistleblower protection, zero-tolerance of
abuse and neglect, and improve important care and quality of
life issues are not met in the draft regulations under Bill 140, the
Long-Term Care Homes Act, 2007, the OHC says. In its submission
to the Ministry, the OHC concluded there are no requirements or
standards for most care and programs in the draft regulations;
no staffing standard regulation; no regulations to ensure public
reporting of actual care levels; no requirement to increase care
as a pre-condition of increased funding; and no regulations
pertaining to reporting and complaints of abuse, neglect and
harm or suspected incidents. The entire submission is available
on the OHC’s website at www.ontariohealthcoalition.ca.
ohc neWs
Taking Hospital Cuts to TaskONA President Linda Haslam-Stroud, First Vice-President Vicki McKenna, Region 2 Vice-President Anne Clark, ONA Local leaders, members and staff take part in the two-day Ontario Health Coalition’s (OHC) Strategy Summit on Ontario’s Planned Hospital Cuts, Downsizing and Restructuring. The purpose of the summit, held in downtown Toronto earlier this year, was to bring OHC activists and local munic-ipal councilors together to provide a briefing on the extent of hospi-tal cuts across the province, identify trends and firm up messaging and strategies to fight back. Pictured are (sitting, left to right): Shirley Schuurman, Local 36; Region 2 Vice-President Anne Clark; Local 100 Coordinator Jill Ross; Jeanne Soden, Local 36. Standing (left to right): Lawrence Walter, ONA Government Relations Officer; Local 35 Coordinator Shirley Roebuck; Local 99 Coordinator Connie Phelan; Dianne Strachan, Local 100.
62324-2_ONA Front Line V9.indd 17 6/19/09 2:48:45 PM
June 200918
huMan righTs anD eQuiTY
Critical Illness Survivor Plan is underwritten by Western Life Assurance Company andadministered by Johnson Inc. MEDOC® is a registered trademark of Johnson Inc.MEDOC® is underwritten by Royal & Sun Alliance Insurance Company of Canada andis administered by Johnson Inc. Johnson Inc. and Royal & SunAlliance InsuranceCompany of Canada share common ownership. All other available benefits are underwritten by Manulife Financial and administered by Johnson Inc. Some conditions may apply. LRP.04.09
Voluntary Benefits
A Benefitfor Everyone,Active or Retired
For more information, contactthe ONA Program Administrator:
Johnson Inc.1595 16th Ave., Suite 700Richmond Hill, ON L4B 3S5(905) 764.4959 (local)1.800.461.4155 (toll-free)
• Long Term Disability• Extended Health Care &
Semi–Private Hospital• Dental Care• Critical Illness• Life Insurance• Accidental Death &
Dismemberment• MEDOC® Travel Insurance
ONA2a_Apr09, 2.625x10.25_CMYK:Layout 1 4/21/
rIgHTS
Nurse on ESA family leave for scheduled qualifying days entitled to holiday pay
ONA & London Health Sciences Centre
(Rayner, March 25, 2009) After the shift schedule covering the holiday period had been posted, in early December the grievor started an initial eight-week Employment Standards Act (ESA) Family Leave to care for her dying mother. As a result, she did not work the scheduled shifts immediately preceding and following the Christmas, Boxing Day and New Year’s Day holidays. The hospital did not give her credit for those holidays, claiming she was disqualified by Article 15.02.
Although the language of that article seems on the surface to be contradictory, the arbitra-tor agreed with the Union that the grievor was entitled to the three days’ holiday pay on the ba-sis that she had been “excused by the hospital.” He added that this conclusion would only ap-ply in circumstances where the nurse was origi-nally scheduled to work the qualifying days (this might not be the case for a longer leave).
Consecutive weekend premium payable for three extended tours in one weekend
ONA & Rouge Valley Health System
(Johnston, April 22, 2009)Everyone agreed that the grievor was entitled to one-and-one-half times pay for a weekend, as it was her second consecutive weekend worked. The question was: which shifts should attract the premium that weekend? She worked ex-tended tours beginning each Friday, Saturday and Sunday at approximately 7 p.m. However, the employer only paid the premium for two of those shifts.
The arbitrator held that the parties had clearly defined weekend for the purpose of this provision as the time between 7 p.m. Friday and 7 a.m. Monday. The grievor had worked three
The following is a sampling of recent key awards and/or decisions in one or more of the following areas: rights arbitration, interest arbitration, Workplace Safety and Insurance Board (WSIB), Long-Term Disability (LTD) and Ontario Labour Relations Board. A complete listing of recent awards and decisions can be found in the members’ secure section of ONA’s website at www.ona.org.
As part of ONA’s steadfast commitment to human rights and equity, the Board of Directors has approved a set of strategies for 2009 to improve communications to and between our members, thereby increasing their knowledge base in this important area.
The strategies were developed earlier this year following the results of a survey given to delegates of the Human Rights and Equity Caucus last November. The survey asked participants to rate the effectiveness of the human rights and equity strategies implemented in 2008. Based on those results, the team identified gaps in services and developed strategies for 2009 to address those areas.
The 2009 strategies include: • Highlighting human rights and equity education programs in ONA communication
vehicles, detailing our members’ experiences on the effectiveness of the programs, what was learned, etc.
• Informing members about the wealth of material ONA provides in French.• Developing short and snappy “Frequently Asked Questions” documents, which have
proved popular with our members in the past, on homophobia, addictions and mental health issues.
• Creating a “tips” sheet to assist members on the steps to follow when returning towork, either from a workplace injury or illness.
• Developing strategies to promote the use of employer-based bulletin boards so we candisseminate human rights and equity-related materials to our members right at their work sites.
• Creating an e-mail listing for any member who wishes to support human rights andequity issues to mirror the designated group e-mail listing. Please contact the ONA Human Rights and Equity Team if you would like to receive regular updates. Call (416) 964-1979 or (toll-free) 1-800-387-5580, press 0 and follow the operator’s prompts to access the voicemail boxes (English: 7768; French: 7769). Or e-mail Region 3 Vice-President Andy Summers, who holds the Human Rights and Equity portfolio, at [email protected].
“It has always been the commitment of ONA to listen to our members, and develop and increase services based on their feedback,” said ONA President Linda Haslam-Stroud. “These strategies will go a long way towards ensuring our members are informed on the key issues in human rights and equity. That will help us work together to ensure all members receive the respect and support to which we are entitled.” BFL
HR&E 2009 Strategies Highlight Member Communications
Be a Part of the 2009
Fairmont Royal York Hotel, Toronto - November 10, 2009.
Ontario Nurses’ Association
Attention ONA Members!
Human Rights and Equity CaucusHuman Rights and Equity Caucus
For more information, log onto the members’ section of the ONA website: www.ona.org
aWarDs anD Decisions
62324-2_ONA Front Line V9.indd 18 6/19/09 2:48:49 PM
19June 2009
Critical Illness Survivor Plan is underwritten by Western Life Assurance Company andadministered by Johnson Inc. MEDOC® is a registered trademark of Johnson Inc.MEDOC® is underwritten by Royal & Sun Alliance Insurance Company of Canada andis administered by Johnson Inc. Johnson Inc. and Royal & SunAlliance InsuranceCompany of Canada share common ownership. All other available benefits are underwritten by Manulife Financial and administered by Johnson Inc. Some conditions may apply. LRP.04.09
Voluntary Benefits
A Benefitfor Everyone,Active or Retired
For more information, contactthe ONA Program Administrator:
Johnson Inc.1595 16th Ave., Suite 700Richmond Hill, ON L4B 3S5(905) 764.4959 (local)1.800.461.4155 (toll-free)
• Long Term Disability• Extended Health Care &
Semi–Private Hospital• Dental Care• Critical Illness• Life Insurance• Accidental Death &
Dismemberment• MEDOC® Travel Insurance
ONA2a_Apr09, 2.625x10.25_CMYK:Layout 1 4/21/
rIgHTS
Nurse on ESA family leave for scheduled qualifying days entitled to holiday pay
ONA & London Health Sciences Centre
(Rayner, March 25, 2009) After the shift schedule covering the holiday period had been posted, in early December the grievor started an initial eight-week Employment Standards Act (ESA) Family Leave to care for her dying mother. As a result, she did not work the scheduled shifts immediately preceding and following the Christmas, Boxing Day and New Year’s Day holidays. The hospital did not give her credit for those holidays, claiming she was disqualified by Article 15.02.
Although the language of that article seems on the surface to be contradictory, the arbitra-tor agreed with the Union that the grievor was entitled to the three days’ holiday pay on the ba-sis that she had been “excused by the hospital.” He added that this conclusion would only ap-ply in circumstances where the nurse was origi-nally scheduled to work the qualifying days (this might not be the case for a longer leave).
Consecutive weekend premium payable for three extended tours in one weekend
ONA & Rouge Valley Health System
(Johnston, April 22, 2009)Everyone agreed that the grievor was entitled to one-and-one-half times pay for a weekend, as it was her second consecutive weekend worked. The question was: which shifts should attract the premium that weekend? She worked ex-tended tours beginning each Friday, Saturday and Sunday at approximately 7 p.m. However, the employer only paid the premium for two of those shifts.
The arbitrator held that the parties had clearly defined weekend for the purpose of this provision as the time between 7 p.m. Friday and 7 a.m. Monday. The grievor had worked three
The following is a sampling of recent key awards and/or decisions in one or more of the following areas: rights arbitration, interest arbitration, Workplace Safety and Insurance Board (WSIB), Long-Term Disability (LTD) and Ontario Labour Relations Board. A complete listing of recent awards and decisions can be found in the members’ secure section of ONA’s website at www.ona.org.
extended tours in that period and was en-titled to premium pay for all of them. The grievance was allowed.
WSIB
Poor return to work plan leads to further injury
South Hospital
(February 6, 2009)This Post-Op Recovery Unit nurse injured her low back in a patient lift incident in November 2005. The WSIB paid loss of earnings (LOE) benefits for two weeks, and the nurse returned to seven months of modified work. Less than two weeks after resuming full duties with no restrictions, she worked three shifts with a particularly heavy assignment, and suffered a recur-rence identical to the original injury.
Her doctor ordered her off work for four weeks, at the end of which she suffered a severe anxiety reaction and panic attacks. WSIB denied entitlement to the recurrence and the psychological disability on the ba-sis that she had returned to regular duties and was, therefore, “completely recovered” from the November 2005 injury.
At the hearing, the worker testified about the stressful nature of the so-called “modified” work and ONA showed how the nurse had not really been accommodat-ed; her “modified work plan” consisted of “regular nursing duties within your restric-tions.” There were, in fact, no modifications to the worker’s regular duties – she had to accommodate herself, which meant contin-uously asking for help and refusing to assist other staff on a very busy unit.
ONA’s evidence persuaded the appeals officer to award entitlement for the June 2006 recurrence, permanent impairment, and psy-chological disability due to the injury.
The worker will receive full LOE from June 16, 2006 to February 8, 2007, when she was cleared for return to work by her doctors. However, because the employer would not let her return until January 2008, the claims ad-judicator will have to determine LOE benefits past February 8, 2007. The worker will also receive a Non-Economic Loss (NEL) assess-ment and award.
Importance to ONA: This is a win for the injured ONA member, and adds to ONA’s growing body of evidence that employers and claims adjudicators do not understand the need for real, safe modified work. Return to work plans that abandon injured workers to fend for themselves not only ignore employ-ers’ legislated health and safety obligations, they lead to stress and further injury for al-ready vulnerable, injured workers. ONA is using this and other cases to press WSIB to ensure that injured workers are returned to work that is safe for them to do.
LTD
“Best foot forward” practice may “cut off your nose”
Hospital, Region 5
(January 22, 2009)This member was suffering from severe depres-sion and was followed by her family physician due to lack of available psychiatric care.
She saw one psychiatrist, who was also a colleague. The member made every effort to appear her best before her colleague. This psy-chiatrist reported to the carrier that her absence was related to work dissatisfaction and that she was unsure that she wished to return to work.
When he was asked to clarify his letter to the carrier, the psychiatrist declined to do so. Six months later, an independent medical ex-amination determined that she was ready to return to work. The carrier determined that she could have returned earlier as well and re-fused to alter its termination of benefits. The member obtained medical clearance to return to work and the hospital worked actively to support her return.
aWarDs anD Decisions
62324-2_ONA Front Line V9.indd 19 6/19/09 2:48:49 PM

onTario nurses’ associaTion
85 Grenville St., Ste. 400
Toronto ON M5S 3A2
Due to a great deal of persistence on the part of the member and her ONA represen-tatives, benefits were finally reinstated. But in the meantime, the carrier had delayed deal-ing with the appeal by waiting eight weeks to release the member’s file in which the initial psychiatrist’s letter was found.
It is essential to be honest and forthright with caregivers – even when they are col-leagues – and not try to hide symptoms, as this may lead to negative decisions.
Non-compliance causes delaysHospital, Region 4
(January 14, 2009)The member was suffering from degenerative disc disorder. The carrier denied initial ben-efits on the grounds that there was no indi-cation of medical restrictions or limitations. It asked for more medical evidence and then, when it was provided, treated the new evi-dence as an “appeal.”
The member, unfortunately, was not fully compliant, which was also problematic for the appeal, but in the end did undergo a functional abilities evaluation and an updated Magnetic Resonance Imaging. Finally, the results sup-ported the member’s entitlement to benefits, but an outstanding dispute over the first day of illness is being addressed through a grievance.
The new Hospitals of Ontario Disability Income Plan (HOODIP) carrier needs to be monitored for its performance in several ways. In this case, it was the failure to distinguish be-tween responding to a request for more evidence when no decision had been made, and a medical appeal submitted when a decision had already been made to deny or terminate benefits.
Members should report to their ONA rep-resentatives any correspondence that seems unreasonable.
Not responding to carrier’s requests causes problems
Hospital, Region 1
(February 11, 2009) The carrier denied initial entitlement to ben-efits to a member suffering from depression. The member had not responded to a list of questions from the carrier, and her physician had not responded to a request for clarifica-tion.
ONA did not see the physician’s letter un-til a copy of the file was received. ONA had requested a review of the claim to identify necessary information before seeking addi-tional medical evidence.
After declining the claim, the carrier re-ceived additional medical information, which they had requested, but did not view. They said they had received our intent to appeal and would not review the information until we indicated in writing that we wanted them to do so. This resulted in a month’s delay in getting benefits approved. The good news is that the member did receive her benefits, with full retroactivity, but the carrier’s delay was unnecessary.
Lessons learned: Respond promptly to the carrier’s request for information, and ask your physicians to do the same.
Age and medical inability to retrain help to support a claim
Hospital, Region 4
(January 19, 2009)The carrier terminated the member’s benefits at the change of definition, stating that there wasn’t enough medical evidence to support ongoing benefits in the “any occupation” phase. This happened after the employer had changed carriers (because the Ontario Hospi-tal Association had changed the Hospitals of Ontario Disability Income Plan).
The member, now at the end of her long nursing career and suffering from conditions af-fecting her shoulder/arm/wrist, is medically un-able to retrain at this time. She is clearly disabled from her own occupation by weakness in her dominant arm and hand, impaired fine motor coordination, numbness and occasional paraly-sis of this limb. The carrier, however, said that she could retrain for a managerial position.
ONA obtained good evidence from the member’s physiotherapist, and a secondary diagnosis from a specialist. Benefits were re-instated retroactive to the date of the original entitlement.
Lessons learned: Remember to get re-ports from paramedical professionals such as physiotherapists.
oFl neWs
E the Ontario Federation of Labour (OFL) has launched
a Drive to Work Caravan, a province-wide tour
to find out how the recession is really affecting
working people. The tour, which began on June 8, 2009, and runs for three weeks, will
talk to thousands of Ontarians and listen to what they say we need to do to preserve and
create good jobs and maintain strong public services for healthy communities. For more
information, log onto www.ofl.ca or the OFL’s dedicated website at www.drivetowork.ca.
aWarDs anD Decisions
62324-2_ONA Front Line V9.indd 20 6/19/09 2:48:49 PM