FROM THE EDITOR - Dr Jackie Jones, RN, PhD, with Toni ...
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1 4 EDITORIAL E vidence based practice is a framework for change and currently a driving force for reform in Australian health care contexts. Notably, a health service is made up of individuals who work together, systems of care and clinical encounters involving decision making (Muir-Gray 1997, p.155). Muir-Gray elaborates that key inter-related components of an evidence-based health service are: 1. Organisations designed with the capability to generate and the flexibility to incorporate evidence; and, 2. Individuals and teams who can find, appraise and use research evidence (Muir-Gray 1996, p.155). Having the best available research evidence alone will not help change practice; it requires an informed determination to confront existing norms and behaviour, and to challenge systems and organisational culture. It also requires consideration of patient values. When practice is not what it could be, what makes one individual feel the need to advocate for patients more strongly than others? Firtko and Jackson in this issue consider whistleblowing which they define as: ‘the reporting of information to an individual, group, or body that is not part of an organisation’s usual problem-solving strategy. Whistleblowing is a phenomenon where a party or parties take matters that would normally be held as confidential to an organisation, outside that organisation despite the personal risk, and potentially negative sequelae associated with the act’ (Firtko and Jackson 2005, p.52). When reflecting on whether the ends justify the means, Firtko and Jackson argue that they do, and so would Toni Hoffman, a whistleblowing nurse, when she says: ‘if the act of “whistleblowing” has the ability to remove the problem and open up the Pandora’s box that it has, the end does justify the means. When we are dealing with patients lives and are acting as patient advocates it will always do so’. In the case in point there were many who held similar concerns but who failed to act. Nurses have been shown in the past to interpret events differently and nurses may hold the belief that they would not be taken seriously should they wish to raise difficult concerns. Ahern and McDonald (2002, p.303) argue that the ‘dilemma for nurses is that nursing actions should be based on ethical codes of conduct, not on fear of job loss or reprisals’. They compared the beliefs of those nurses who blew the whistle with those who did not. These authors report that ‘participants who reported misconduct (whistleblowers) supported the belief that nurses were primarily responsible to the patient and should protect a patient from incompetent or unethical people. Participants who did not report misconduct (non-whistleblowers) supported the belief that nurses are obligated to follow a physician’s order at all times and that nurses are equally responsible to the patient, the physician and the employer. These Australian researchers suggest there is a difference in the interpretation of the seriousness of events and in individuals whose value system leads them to defer to authority. It could be said then the complex nature of authority and conflicting ideologies within an organisation in turn influences power and the potential for organisation violation. Speedy (2004, p.146) describes ‘ behaviours that are unacceptable to management’ or ‘organisation violations’ as those events deeply embedded in complex structures of culture, enactment of authority, and, organisational processes that disturb organisational goals which in turn may disrupt organisational functioning. Those who have power over those whose behaviour is being judged draw on a matter of perspective and can lead to a culture of intimidation (p.147-148). Speedy argues that knowledge about organisation violations can be used to enhance organisational environments and ultimately reform processes. In this way whistleblowing, as a form of resistance against organisational abuses such as bullying, emotional assault and maintaining an infirm status quo can be reconceptualised as contributing to a violation free environment by exposing underlying tensions, culture and power struggles. Being in a position of power does not preclude the desire for advocacy. Line managers in nursing are often criticised for upholding organisational goals above those of the nurse at the coal face. This particular whistleblower is the nurse unit manager of a small combined intensive/coronary care unit in Central Queensland. Toni explains that she had never thought she would ever become a whistleblower: ‘In 2003, I found myself in a very difficult situation where I believed there was something seriously wrong with the practices of a surgeon. My decision to become a whistleblower was not a “deliberate one”. My actions were deliberate, but I had no way of knowing what the outcome would be. My main concern was with the patients and potential patients.’ It is clear then that deliberations about resisting organisation violations are not just about the here and now but also about the future. She adds that she was FROM THE EDITOR - Dr Jackie Jones, RN, PhD, with Toni Hoffman, RN, NUM, Intensive/Coronary Care Unit ‘I HAD TO ACT’: IN CONVERSATION WITH A WHISTLEBLOWER
Transcript of FROM THE EDITOR - Dr Jackie Jones, RN, PhD, with Toni ...

Australian Journal of Advanced Nursing 2005 Volume 23 Number 14
EDITORIAL
Evidence based practice is a framework for changeand currently a driving force for reform inAustralian health care contexts Notably a health
service is made up of individuals who work togethersystems of care and clinical encounters involving decisionmaking (Muir-Gray 1997 p155) Muir-Gray elaboratesthat key inter-related components of an evidence-basedhealth service are
1 Organisations designed with the capability togenerate and the flexibility to incorporate evidenceand
2 Individuals and teams who can find appraise anduse research evidence (Muir-Gray 1996 p155)
Having the best available research evidence alone willnot help change practice it requires an informeddetermination to confront existing norms and behaviourand to challenge systems and organisational culture Italso requires consideration of patient values
When practice is not what it could be what makes oneindividual feel the need to advocate for patients morestrongly than others Firtko and Jackson in this issueconsider whistleblowing which they define as
lsquothe reporting of information to an individual groupor body that is not part of an organisationrsquos usualproblem-solving strategy Whistleblowing is aphenomenon where a party or parties take matters thatwould normally be held as confidential to an organisationoutside that organisation despite the personal risk andpotentially negative sequelae associated with the actrsquo(Firtko and Jackson 2005 p52)
When reflecting on whether the ends justify the meansFirtko and Jackson argue that they do and so would ToniHoffman a whistleblowing nurse when she says lsquoif theact of ldquowhistleblowingrdquo has the ability to remove theproblem and open up the Pandorarsquos box that it has theend does justify the means When we are dealing withpatients lives and are acting as patient advocates it willalways do sorsquo
In the case in point there were many who held similarconcerns but who failed to act
Nurses have been shown in the past to interpret eventsdifferently and nurses may hold the belief that they wouldnot be taken seriously should they wish to raise difficultconcerns Ahern and McDonald (2002 p303) argue thatthe lsquodilemma for nurses is that nursing actions should bebased on ethical codes of conduct not on fear of job lossor reprisalsrsquo They compared the beliefs of those nurseswho blew the whistle with those who did not Theseauthors report that lsquoparticipants who reported misconduct
(whistleblowers) supported the belief that nurses wereprimarily responsible to the patient and should protect apatient from incompetent or unethical people Participantswho did not report misconduct (non-whistleblowers)supported the belief that nurses are obligated to follow aphysicianrsquos order at all times and that nurses are equallyresponsible to the patient the physician and the employerThese Australian researchers suggest there is a differencein the interpretation of the seriousness of events and inindividuals whose value system leads them to defer toauthority It could be said then the complex nature ofauthority and conflicting ideologies within anorganisation in turn influences power and the potential fororganisation violation
Speedy (2004 p146) describes lsquo behaviours that areunacceptable to managementrsquo or lsquoorganisation violationsrsquoas those events deeply embedded in complex structures ofculture enactment of authority and organisationalprocesses that disturb organisational goals which in turnmay disrupt organisational functioning Those who havepower over those whose behaviour is being judged drawon a matter of perspective and can lead to a culture ofintimidation (p147-148) Speedy argues that knowledgeabout organisation violations can be used to enhanceorganisational environments and ultimately reformprocesses In this way whistleblowing as a form ofresistance against organisational abuses such as bullyingemotional assault and maintaining an infirm status quocan be reconceptualised as contributing to a violation freeenvironment by exposing underlying tensions culture andpower struggles
Being in a position of power does not preclude thedesire for advocacy Line managers in nursing are oftencriticised for upholding organisational goals above thoseof the nurse at the coal face This particular whistlebloweris the nurse unit manager of a small combinedintensivecoronary care unit in Central Queensland Toniexplains that she had never thought she would everbecome a whistleblower
lsquoIn 2003 I found myself in a very difficult situationwhere I believed there was something seriously wrongwith the practices of a surgeon My decision to become awhistleblower was not a ldquodeliberate onerdquo My actionswere deliberate but I had no way of knowing what theoutcome would be My main concern was with thepatients and potential patientsrsquo
It is clear then that deliberations about resistingorganisation violations are not just about the here andnow but also about the future She adds that she was
FROM THE EDITOR - Dr Jackie Jones RN PhD with Toni Hoffman RN NUMIntensiveCoronary Care Unit
lsquoI HAD TO ACTrsquo IN CONVERSATION WITH A WHISTLEBLOWER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 15
EDITORIAL
incredibly frustrated that senior management had nottaken her concerns seriously
lsquoI was frustrated that the situation was well known tomany people from within and without the establishmentstaff with much more authority than me The situationcould have been dealt with so much more easily andwithout the need for me to blow the whistlersquo
Ethical resistance demands political scholarship and asPeter et al (2004 p414) point out lsquoto increase nursesrsquocapacity to resist they could benefit from developingnegotiation and political action skills and participating ininstitutional committees such as ethics committees It ishowever most fundamental that they receive institutionalsupport and acknowledgement so that they have thefreedom to express their viewpoints values andexperiences without risk of punishmentrsquo
Perhaps it is timely that tertiary institutions look to thenursing union(s) for the lifetime of expertise they have inorder to develop and educate both new and existinggenerations of nurses in the art of organisation and theimportance of collective action in and betweenprofessional discourses in the art of political scholarship
One study in California (Seago and Ash 2002) foundthat in unionised hospitals they had 57 lower mortalityrates for patients suffering acute myocardial infarction Inproviding a context for nurses to have a voice at work bybuilding nurse resilience and capacity for resistance thisresearch found that a nursing union can indirectlyimprove patient outcomes Drawing on this evidence itcould be argued nursing unions may promote lsquostability instaff autonomy collaboration with medical doctors andpractice decisions that have been described as having apositive influence on the work environment and on patientoutcomes ( p150)
When Firtko and Jackson ask what the motivation forwhistleblowing is Toni identified patient safety as hermotivating factor She said lsquoMy main concern was withthe patients and potential patients My main concern wasto stop the surgeon and stop him quickly The patientswould then be safe and the nursing staff would berelievedrsquo
Firtko and Jackson in drawing on Speedy (2004)identify that some organisations create cultures ofreduced loyalty and can cause employees to feel violatedbetrayed and liable to seek reprisal This was not the casefor Toni who clarifies that she lsquoagonised for months overwhat to do [and] tried all of the other channelsrsquo Despitethe consequences she proceeded and highlights lsquoI wasvery aware that by going to a member of parliament I wasbreaking my health departmentrsquos code of conduct I wasaware I could lose my job I would lose favour within thesystem amongst the current executive and any futurepotential employers would view me as a liability Somepeople would be hurt and alliances and friendships withinmy small town would be fracturedrsquo
There are other considerations regarding the potential
impact of whistleblowing in particular this nurse thought
about the patients the ones who had lost loved ones many
months before and were well into the grieving process
She constantly asked herself what would this do to them
When it became obvious to Toni and others that nothing
was being done fast enough she emphatically states
lsquoI had to actrsquo
Albeit unknown territory for Toni as a nurse she did
not want to involve others so they would be implicated
and could also be in danger of losing their jobs She
explains lsquoI did ask one person if they wanted to
accompany me but they did not want to So I went alone
to see the Member of Parliament for my area I was very
fearful I did not know what he was going to dorsquo
The consequences of whistleblowing can be and are
far reaching for the whistleblower Nurses are placed in a
situation that they are unfamiliar such as lsquowith lawyers
and Queenrsquos Counsels the media and politiciansrsquo The
experience can challenge the very moral foundations of
the individual including having to earn everyonersquos trust
again Some unpleasant things have occurred as a result
of speaking out Toni said lsquoI have been threatened by
telephone and out in the community I have been vilified
on the stand and had to lsquocop itrsquo This situation was far
worse than I had ever imaginedrsquo
The experience was not all negative however as Toni
goes onlsquoThe public support has been incredible I have
received hundreds of letters of support hundreds of calls
and emails and I am stopped in the street frequently The
collegial support has been incredible with no negative
feedback A lot of the letters were signed ldquofrom an old
RNrdquo or ldquoan ex RNrdquo I think these people have been in my
situation some have acted and some havenrsquot but they
know what I went throughrsquo
The ramifications of whistleblowing for Toni Hoffman
have been huge A Royal Commission was established to
investigate her complaints and is in a position to make
some fundamental changes to the way health care is
carried out in Queensland The act of lsquowhistleblowingrsquo in
this instance did solve the problem and uncovered a
Pandorarsquos Box of systemic problems which in turn may
be addressed with recommendations received by the
Royal Commission
Nevertheless Queensland if not the rest of Australian
health service providers have an opportunity to reflect on
organisational violations structures that require change
and individuals who need the ethical fortitude and
collective support to actively stand out and improve
practice
EDITORIAL
REFERENCESAhern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38 (3)303-309
Firtko A and Jackson D 2005 Do the ends justify the means Nursing andthe dilemma of whistleblowing Australian Journal of Advanced Nursing23(1)51-56
Muir-Gray JA 1997 Evidence-based health care How to make health policyand management decisions Edinburgh Churchill Livingstone
Peter E Lunardi V and Macfarlane A 2004 Nursing resistance as ethicalaction literature review Journal of Advanced Nursing 46(4)403-416
Seago JA and Ash M 2002 Registered nurse union and patient outcomesJournal of Nursing Administration 32143-151
Speedy S 2004 Organisation violations Implications for leadership In DalyJ Speedy Sand Jackson D (eds) Nursing Leadership Sydney ChurchillLivingstone145-164
Australian Journal of Advanced Nursing 2005 Volume 23 Number 16
Australian Journal of Advanced Nursing 2005 Volume 23 Number 17
Trisha Dunning AM RN MEd PhD FRCNA DirectorEndocrinology and Diabetes Nursing Research Department of Endocrinology and Diabetes St Vincentrsquos Hospital School of Nursing The University of Melbourne MelbourneVictoria Australia
trishdunningsvhmorgau
Elizabeth Manias RN MPharm MNStud PhD FRCNA Schoolof Nursing The University of Melbourne Victoria Australia
Accepted for publication December 2004
ACKNOWLEDGEMENTSThe researchers are grateful to Megan Lalor for assistance with data collectionThe research was supported by an Eli Lilly Diabetes Education Research Grantand we thank Eli Lilly for making the grant available
MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
RESEARCH PAPER
Key words type 2 diabetes medication knowledge self-care
ABSTRACT
ObjectiveTo explore medication knowledge and self-
management practices of people with type 2 diabetes
DesignA one-shot cross sectional study using in-depth
interviews and participant observation
SettingDiabetes outpatient education centre of a university
teaching hospital
SubjectsPeople with type 2 diabetes n=30 17 males and 13
females age range 33-84 from a range of ethnic groups
Outcome measuresAbility to state name main actions and when to take
medicines Performance of specific medication-relatedtasks opening bottles and packs breaking tablets in halfadministering insulin and testing blood glucose
ResultsAverage medication use ge10years Respondents were
taking 86 different medicines mean 7plusmn297 SD Dosefrequency included two three and four times per day Allrespondents had ge2 diabetic complications plusmn othercomorbidities The majority (93) were informed abouthow and when to take their medicines but only 37were given information about side effects and 17 weregiven all possible seven items of information Youngerrespondents received more information than olderrespondents Older respondents had difficulty openingbottles and breaking tablets in half Twenty percentregularly forgot to take their medicines Increasingmedication costs was one reason for stopping medicinesor reducing the dose or dose interval The majority tested
their blood glucose but did not control test their metersand 33 placed used sharps directly into the rubbish
ConclusionPolypharmacy was common Medication knowledge
and self-management were inadequate and could lead toadverse events
INTRODUCTION
Diabetes is a chronic disease that affects 75 ofAustralians over 25 and 168 over 65 years(Dunstan et al 2000) Long term self-care and
education are needed to control blood glucose levels andreduce the risk of complications and adverse medication-related events
These necessary skills include blood glucose monitoringand medication administration Over time the complexity ofthe medication regime increases for people with type 2diabetes because of the associated complicationscomorbidities and pancreatic beta cell exhaustion (Olefsky etal 1999) This means the complexity of the self-care regimeincreases often at the same time as the person is growingolder and eyesight hearing fine motor skills and memoryand information processing are changing These changesmake it difficult for the individual to comply withrecommended self-care practices such as blood glucosetesting and medication management including insulinadministration
Anecdotal evidence suggests that many people withdiabetes do not have adequate knowledge about themedications they take stop medications and alter dosesinappropriately without consulting their doctors and do notunderstand the actions side effects or potential interactionsof the medications they take even those they have beentaking for years
In particular older people are more likely to have physicalproblems that make safe medication usage difficult and they
make significantly more insulin dose errors using syringes(DeBrew et al 1998) despite the advent of premixed insulinformulations such as Mixtard and modern insulin deliverydevices (Coscelli et al 1992) Inappropriate medication usageis likely to have an effect on blood glucose control andtherefore on health outcomes and diabetes-related healthcosts In addition inadequate medication self-care increasesthe likelihood of admission to a nursing home (Stradberg1984)
A number of researchers have examined medicationissues such as adherence by monitoring pill counts thefrequency of completing the full course of a medicationscript refill rates and ability to open medication packages(Matsuyama et al 1993 Paes et al 1997 Kriev et al 1999)These studies indicate omitting doses stopping medicationswithout consulting a doctor and inappropriately changingdoses are common behaviours However supplyingmedications to patients does not guarantee the medicationsare actually taken In fact a systematic review of randomisedcontrol trials showed that about half the medicines prescribedfor chronic diseases are not taken (Haynes et al 1996) Inaddition self-reported behaviour is subjective andproblematic For example people who say they do not followtreatment may report accurately while people who deny notfollowing recommendations may report inaccurately(Spector 1986)
The majority of these studies relied on self-report Actualpractices were not directly observed and no researcherreported asking about self-prescribed medicines andcomplementary therapy use There is a high rate ofcomplementary therapy use among people with diabetes(Egede et al 2002) and there are a growing number of reportsof undesirable drugherb interactions and adverse eventsrelating to the use of some complementary therapies bypeople with diabetes (Dunning 2003)
The impact of education on adherence is welldocumented (Kriev et al 1999) but adherence is a complexphenomenon and is difficult to predict Adherence isinfluenced by many factors and is dependent on anindividualrsquos problem-solving skills beliefs and attitudessocial situation and support and is complex and demanding(Jones 2003) The term is often used in a derogatory way thatdoes not take account of the fact that it has physicalpsychological attitudinal and social components Themajority of medication adherence studies focus on adherenceto the medication recommendations knowledge andbehaviour Only rarely have physical limitations andfinancial factors been explored with people with diabetesWhen they are it is usually with respect to oralhypoglycaemic agents (OHA) and insulin administration(Coscelli et al 1992 Tay et al 2001 Evans et al 2002)
People with diabetes frequently have complications andconcomitant diseases that make it difficult for them toperform some diabetes self-care tasks including managingtheir medications For example arthritis limits manualdexterity and makes it difficult to test blood glucose breaktablets administer insulin and open medication packagesDiabetes complications include reduced vision and
retinopathy yet consumer medication information andmedicine labels are often presented in small fonts that aredifficult to read even with glasses An important and rarelyconsidered factor is the impact of health professionalattitudes and beliefs and health system issues on anindividualrsquos willingness and ability to follow treatmentrecommendations
Regular diabetes complication screening is an Australianestablished nationally co-ordinated project known asANDIAB Home medication reviews were introduced morerecently but routine monitoring of medication self-careability and behaviours rarely occurs in a structured way andis not a focus of either of these processes Diabetesmanagement guidelines based on the Diabetes Control andComplications Trial (DCCT) (1993) and The UnitedKingdom Prospective Diabetes Study (UKPDS) (1998)stress the need to achieve good blood glucose lipid andblood pressure control and lsquotreating to targetrsquo That isachieving evidence-based metabolic blood pressure andweight targets The targets are getting lower as the evidencethat tight metabolic control prevents morbidity and mortalityaccumulates
As a consequence more medications are added to thetreatment regime which become more complexPolypharmacy is the norm and could be considered bestpractice in light of diabetes management guidelines thatrecommend aiming for normoglycaemia and normal lipidand blood pressure ranges For example people withdiabetes can expect to take three to four antihypertensiveagents as well as insulin or oral hypoglycaemic and lipidlowering agents for their diabetes as well as a range ofmedications for other diabetes complications or concomitantdiseases The cost of uncontrolled diabetes is high andcarries significant morbidity and mortality rates thereforepolypharmacy can be justified However it leads tocomplicated medication regimes that are more likely to leadto mistakes andor non-adherence
The Quality Use of Medicines (QUM) initiative has beena key component of the National Health Policy in Australiasince 1992 and is slowly being integrated into patientmedication self-management education programs The basictenets of QUM are the primacy of the patient collaborativemultidisciplinary practice a systems based approach thejudicious selection and use of medicines if medicines areindicated and regular outcome monitoring Researchindicates medicines use is less than optimal nationally andnurses have a shared professional responsibility for QUM(Griffiths et al 2001) This responsibility includes monitoringpatient medication self-management especially in chronicdisease such as diabetes where medicines are often requiredfor life A number of health professionals including diabeteseducators are responsible for instructing patients aboutappropriate medication usage
Despite the knowledge that good blood glucose controlreduces the long term complications of diabetes (DCCT1993 UKPDS 1998) and the availability of the technologyto achieve it good control is not achieved in many cases(Dunning 1994) Factors such as attitudes beliefs and self-
RESEARCH PAPER
8Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 19
care practices including appropriate use of medicines aresome of the intervening variables between having theknowledge applying it and achieving good metaboliccontrol
Non-adherence for whatever reason threatens theprovision of effective diabetes care Lustman (1995) statedthat seven out of 10 leading causes of death are linked tobehaviour If that is so more consideration of thebehavioural factors associated with diabetes medication self-management appears to be warranted
AIM OF THE STUDYThe study aimed to explore the medication knowledge
and self-management practices of people with type 2diabetes referred to the diabetes outpatient services by theirgeneral practitioners
For the purpose of the study medication knowledgeconsisted of seven specific items of information being ableto name all medicines being used what the medicine wasprescribed for the dose to take when the medicine should betaken potential side effects how to store the medicine andhow to dispose of unused or outdated medicines Self-management practices included being able to open medicinepackages break tablets in half administer insulin andmonitor blood glucose levels
METHODSA cross-sectional survey using structured interviews and
observations of respondents performing relevant medicationself-management practices was used to collect the data Theinterview questionnaire was developed specifically for thestudy
Face and content validity was established by consultingwith relevant experts and pilot testing the draft questionnaireon a representative group from the sampling population whowere subsequently excluded from the study Ethics approvalwas obtained from the relevant human research ethicscommittee
The sampling population and study sampleThe sampling population consisted of all people attending
the diabetes education centre of an inner city universityteaching hospital who were taking medications and able togive informed consent including those referred by theirgeneral practitioners (GP) Between 30 and 45 outpatientsare seen each week primarily by the diabetes educatorsClose links have been established with the referring GPsthrough a diabetes shared care scheme where GPs undertakediabetes management in consultation with the diabeteseducators and endocrinologists A large proportion ofpatients attending the centre are from multiculturalbackgrounds predominantly Vietnam Greece Turkey Italyand South East Asia
Patients were invited to participate when they presented tothe diabetes educator and were given written information
about the study Informed written consent was obtained ifthey agreed to participate and an appointment was made forthem to return to the diabetes education centre where thedata were collected
Participants were asked to bring all of the medicationsthey were taking including any complementary and over-the-counter medicines vitamin and mineral supplements andtheir usual blood glucose testing equipment to theappointment These requirements were written on anappointment card together with directions to the centre
The questionnaireThe questionnaire addressed four domains a) standard
demographic data to ascertain if there was any correlationbetween patient demographic characteristics and medicationmanagement practices b) medication type dose frequencyobtaining prescriptions and having them filled c) educationand knowledge and d) complementary and over-the-countermedicines
Participant observationsParticipants were observed undertaking specific
medication-related activities such as breaking tablets in halfopening medication packages preparing and administeringan insulin dose and testing their blood glucose and the resultsrecorded on a data base
Data analysisInterval and categorical data were analysed using
ANOVA and Chi Square respectively to ascertain anysignificant relationship between the variables Descriptivestatistics including means standard deviation and frequencycounts were used for the demographic data The Pearsoncorrelation coefficient was used to test the degree ofassociation between interval level data Content analysis wasused for the open questions where each question was readline-by-line to note any emerging themes (Morse 1994)Words phrases and sentences were classified into categoriesin which the number of occurrences of a particular categorygave an indicator of the relative importance of the behaviouror activity described
RESULTSThirty people were interviewed Each interview took
approximately two hours
1 Demographic data
Seventeen males and 13 females took part age range 33-84 years mean 687plusmn1335 SD A range of ethnicbackgrounds was represented including Turkish ItalianGreek Chinese and Vietnamese Twelve participants did notspeak English and an interpreter assisted with the interviewsHbA1c which provides an accurate measure of long termglucose control ranged from 57ndash109 (normal 45ndash6using High Pressure Liquid Chromatography [HPLC])Twenty-seven respondents had at least one diabeticcomplication and the majority had three or more The mostcommonly occurring complications were retinopathy
RESEARCH PAPER
macrovascular disease and neuropathy and erectiledysfunction Four were taking antidepressant medicines Themost common concomitant diseases were arthritis andthyroid disease
2 Medication usageOverall 86 different prescribed conventional medicines
and nine self-initiated or complementary medicines andsupplements were used Individuals were taking an averageof 74 medicines range 1ndash12plusmn297 SD Thirty three percentused insulin 46 were on OHAs and 20 were taking acombination of OHA and insulin
Overall respondents were on 10 differentantihypertensive agents six types of lipid lowering agentsthree different aspirin formulations and a range of othermedicines including anticoagulants and diuretics Themajority 66 were on twice a day OHAinsulin regimesTwenty-three percent were on daily and 10 on three times aday regimes Forty-six percent took their medicines beforemeals 36 after meals and 16 with meals Most had beenon medications for ge10 years range 1ndashge10
Complementary therapiesParticipants described complementary therapies as lsquousing
old medicines for current problemsrsquo lsquothings that improvewellbeing and quality of lifersquo and lsquosomething other thanregular medicinesrsquo In three cases the GP had referredpatients to a complementary therapist for massagechiropractic or relaxation Table 1 outlines the reasons peoplegave for using complementary therapies Twenty-threepercent used complementary and self-initiated medicationswhich included vitamin and mineral supplements aperientsanalgesics iron tablets cold remedies amino acidsupplements garlic aloe vera and tea tree essential oil on afoot ulcer
Obtaining medications
Seventy-three percent always obtained their medicinesfrom the same pharmacy and collected them themselvesThirty percent required assistance to obtain their medicinesdue to poor vision or difficulty getting to a pharmacy Inthese cases seven relatives (spouses daughters) collectedmedicines from the pharmacy and also helped with dosingOne pharmacist and one GP delivered medicines to thehomes of two participants
In the majority of cases (90) prescriptions were writtenby the GP which is consistent with centre policy Fifty-twopercent of GPs wrote repeat prescriptions without reviewingthe patient and left the script with the receptionist to becollected or sent the script directly to the pharmacist
Reported costs of medications per year ranged from lessthan $100 to more than $600 (mode $100) Thirty-sixpercent paid more for medications than they had in theprevious year mostly because they needed more medicationsand the cost of some medicines had increased
People used a range of strategies to pay for theirmedications including doing occasional work because thepension was inadequate employing budget strategies and
making sacrifices in other areas One person lsquokept mydiabetes medicines but threw the others away because of thecostrsquo and one lsquogot tired of taking them so I stopped Theywere not doing any good anywayrsquo Another respondentstopped all his medications because of the cost None ofthese respondents consulted their doctors before theystopped their medicines One person shared their diabetesmedicines and blood pressure tablets with a relative whohelped with the costs Fifteen were enrolled in the NationalDiabetes Services Scheme one in the Veteran AffairsScheme which are schemes set up by the AustralianGovernment to subsidise the cost of some non-medicinalproducts Three had private health insurance
Disposal of unused medicines andor sharpsEighty-three percent monitored their blood glucose at
home and they all used meters The majority 80 did notperform control tests on their meters to ensure they werereading accurately but did calibrate the meter with each newbatch of strips Thirty-three percent discarded used needlesand lancets (sharps) directly into the rubbish Unusedmedicines were generally left in the cupboard taken away bya relative or discarded into the rubbish
Education about medicinesEighty-three percent of respondents reported having
specific education about their medicines when they wereprescribed Table 2 shows a breakdown of the specificmedicine-related education items received The majoritywere given information about how to take (93) and whento take (93) medicines and ge50 accurately reported thisinformation for most of their medicines However only 37were given information about and could name possible sideeffects of their medicines The risk of hypoglycaemia withinsulin was the best known medicine side effect In additiononly 17 received all seven possible items of informationThe GP was the most frequently reported education providerTable 3 shows the mean differences between patients who
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 110
Table 1 Reasons participants gave for using complementarytherapies and the main therapies they used
Reason Therapies used
Arthritis MassageGlucosamine sulphate tabletsReiki
Reduce stress Mediationand improve wellbeing Aromatherapy
Improve immunity Vitamins and mineralsAromatherapy massage with thymebasil and clove oils
Reduce blood glucose Herbs and bitter melon prickly pear
Treat wounds fungal Tea tree essential oilinfections on feet Aloe vera gel
Treat colds EchinaceaLemon and honey drinks
Because they are holistic
They work with medicines to help feel better and control blood glucose
Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
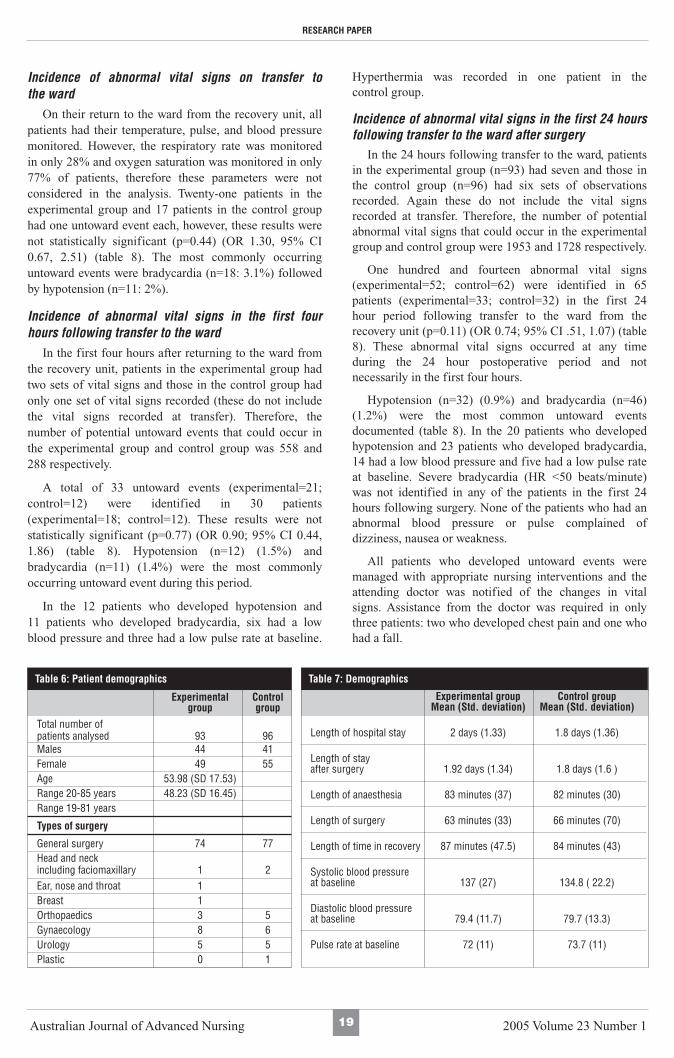
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

Australian Journal of Advanced Nursing 2005 Volume 23 Number 15
EDITORIAL
incredibly frustrated that senior management had nottaken her concerns seriously
lsquoI was frustrated that the situation was well known tomany people from within and without the establishmentstaff with much more authority than me The situationcould have been dealt with so much more easily andwithout the need for me to blow the whistlersquo
Ethical resistance demands political scholarship and asPeter et al (2004 p414) point out lsquoto increase nursesrsquocapacity to resist they could benefit from developingnegotiation and political action skills and participating ininstitutional committees such as ethics committees It ishowever most fundamental that they receive institutionalsupport and acknowledgement so that they have thefreedom to express their viewpoints values andexperiences without risk of punishmentrsquo
Perhaps it is timely that tertiary institutions look to thenursing union(s) for the lifetime of expertise they have inorder to develop and educate both new and existinggenerations of nurses in the art of organisation and theimportance of collective action in and betweenprofessional discourses in the art of political scholarship
One study in California (Seago and Ash 2002) foundthat in unionised hospitals they had 57 lower mortalityrates for patients suffering acute myocardial infarction Inproviding a context for nurses to have a voice at work bybuilding nurse resilience and capacity for resistance thisresearch found that a nursing union can indirectlyimprove patient outcomes Drawing on this evidence itcould be argued nursing unions may promote lsquostability instaff autonomy collaboration with medical doctors andpractice decisions that have been described as having apositive influence on the work environment and on patientoutcomes ( p150)
When Firtko and Jackson ask what the motivation forwhistleblowing is Toni identified patient safety as hermotivating factor She said lsquoMy main concern was withthe patients and potential patients My main concern wasto stop the surgeon and stop him quickly The patientswould then be safe and the nursing staff would berelievedrsquo
Firtko and Jackson in drawing on Speedy (2004)identify that some organisations create cultures ofreduced loyalty and can cause employees to feel violatedbetrayed and liable to seek reprisal This was not the casefor Toni who clarifies that she lsquoagonised for months overwhat to do [and] tried all of the other channelsrsquo Despitethe consequences she proceeded and highlights lsquoI wasvery aware that by going to a member of parliament I wasbreaking my health departmentrsquos code of conduct I wasaware I could lose my job I would lose favour within thesystem amongst the current executive and any futurepotential employers would view me as a liability Somepeople would be hurt and alliances and friendships withinmy small town would be fracturedrsquo
There are other considerations regarding the potential
impact of whistleblowing in particular this nurse thought
about the patients the ones who had lost loved ones many
months before and were well into the grieving process
She constantly asked herself what would this do to them
When it became obvious to Toni and others that nothing
was being done fast enough she emphatically states
lsquoI had to actrsquo
Albeit unknown territory for Toni as a nurse she did
not want to involve others so they would be implicated
and could also be in danger of losing their jobs She
explains lsquoI did ask one person if they wanted to
accompany me but they did not want to So I went alone
to see the Member of Parliament for my area I was very
fearful I did not know what he was going to dorsquo
The consequences of whistleblowing can be and are
far reaching for the whistleblower Nurses are placed in a
situation that they are unfamiliar such as lsquowith lawyers
and Queenrsquos Counsels the media and politiciansrsquo The
experience can challenge the very moral foundations of
the individual including having to earn everyonersquos trust
again Some unpleasant things have occurred as a result
of speaking out Toni said lsquoI have been threatened by
telephone and out in the community I have been vilified
on the stand and had to lsquocop itrsquo This situation was far
worse than I had ever imaginedrsquo
The experience was not all negative however as Toni
goes onlsquoThe public support has been incredible I have
received hundreds of letters of support hundreds of calls
and emails and I am stopped in the street frequently The
collegial support has been incredible with no negative
feedback A lot of the letters were signed ldquofrom an old
RNrdquo or ldquoan ex RNrdquo I think these people have been in my
situation some have acted and some havenrsquot but they
know what I went throughrsquo
The ramifications of whistleblowing for Toni Hoffman
have been huge A Royal Commission was established to
investigate her complaints and is in a position to make
some fundamental changes to the way health care is
carried out in Queensland The act of lsquowhistleblowingrsquo in
this instance did solve the problem and uncovered a
Pandorarsquos Box of systemic problems which in turn may
be addressed with recommendations received by the
Royal Commission
Nevertheless Queensland if not the rest of Australian
health service providers have an opportunity to reflect on
organisational violations structures that require change
and individuals who need the ethical fortitude and
collective support to actively stand out and improve
practice
EDITORIAL
REFERENCESAhern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38 (3)303-309
Firtko A and Jackson D 2005 Do the ends justify the means Nursing andthe dilemma of whistleblowing Australian Journal of Advanced Nursing23(1)51-56
Muir-Gray JA 1997 Evidence-based health care How to make health policyand management decisions Edinburgh Churchill Livingstone
Peter E Lunardi V and Macfarlane A 2004 Nursing resistance as ethicalaction literature review Journal of Advanced Nursing 46(4)403-416
Seago JA and Ash M 2002 Registered nurse union and patient outcomesJournal of Nursing Administration 32143-151
Speedy S 2004 Organisation violations Implications for leadership In DalyJ Speedy Sand Jackson D (eds) Nursing Leadership Sydney ChurchillLivingstone145-164
Australian Journal of Advanced Nursing 2005 Volume 23 Number 16
Australian Journal of Advanced Nursing 2005 Volume 23 Number 17
Trisha Dunning AM RN MEd PhD FRCNA DirectorEndocrinology and Diabetes Nursing Research Department of Endocrinology and Diabetes St Vincentrsquos Hospital School of Nursing The University of Melbourne MelbourneVictoria Australia
trishdunningsvhmorgau
Elizabeth Manias RN MPharm MNStud PhD FRCNA Schoolof Nursing The University of Melbourne Victoria Australia
Accepted for publication December 2004
ACKNOWLEDGEMENTSThe researchers are grateful to Megan Lalor for assistance with data collectionThe research was supported by an Eli Lilly Diabetes Education Research Grantand we thank Eli Lilly for making the grant available
MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
RESEARCH PAPER
Key words type 2 diabetes medication knowledge self-care
ABSTRACT
ObjectiveTo explore medication knowledge and self-
management practices of people with type 2 diabetes
DesignA one-shot cross sectional study using in-depth
interviews and participant observation
SettingDiabetes outpatient education centre of a university
teaching hospital
SubjectsPeople with type 2 diabetes n=30 17 males and 13
females age range 33-84 from a range of ethnic groups
Outcome measuresAbility to state name main actions and when to take
medicines Performance of specific medication-relatedtasks opening bottles and packs breaking tablets in halfadministering insulin and testing blood glucose
ResultsAverage medication use ge10years Respondents were
taking 86 different medicines mean 7plusmn297 SD Dosefrequency included two three and four times per day Allrespondents had ge2 diabetic complications plusmn othercomorbidities The majority (93) were informed abouthow and when to take their medicines but only 37were given information about side effects and 17 weregiven all possible seven items of information Youngerrespondents received more information than olderrespondents Older respondents had difficulty openingbottles and breaking tablets in half Twenty percentregularly forgot to take their medicines Increasingmedication costs was one reason for stopping medicinesor reducing the dose or dose interval The majority tested
their blood glucose but did not control test their metersand 33 placed used sharps directly into the rubbish
ConclusionPolypharmacy was common Medication knowledge
and self-management were inadequate and could lead toadverse events
INTRODUCTION
Diabetes is a chronic disease that affects 75 ofAustralians over 25 and 168 over 65 years(Dunstan et al 2000) Long term self-care and
education are needed to control blood glucose levels andreduce the risk of complications and adverse medication-related events
These necessary skills include blood glucose monitoringand medication administration Over time the complexity ofthe medication regime increases for people with type 2diabetes because of the associated complicationscomorbidities and pancreatic beta cell exhaustion (Olefsky etal 1999) This means the complexity of the self-care regimeincreases often at the same time as the person is growingolder and eyesight hearing fine motor skills and memoryand information processing are changing These changesmake it difficult for the individual to comply withrecommended self-care practices such as blood glucosetesting and medication management including insulinadministration
Anecdotal evidence suggests that many people withdiabetes do not have adequate knowledge about themedications they take stop medications and alter dosesinappropriately without consulting their doctors and do notunderstand the actions side effects or potential interactionsof the medications they take even those they have beentaking for years
In particular older people are more likely to have physicalproblems that make safe medication usage difficult and they
make significantly more insulin dose errors using syringes(DeBrew et al 1998) despite the advent of premixed insulinformulations such as Mixtard and modern insulin deliverydevices (Coscelli et al 1992) Inappropriate medication usageis likely to have an effect on blood glucose control andtherefore on health outcomes and diabetes-related healthcosts In addition inadequate medication self-care increasesthe likelihood of admission to a nursing home (Stradberg1984)
A number of researchers have examined medicationissues such as adherence by monitoring pill counts thefrequency of completing the full course of a medicationscript refill rates and ability to open medication packages(Matsuyama et al 1993 Paes et al 1997 Kriev et al 1999)These studies indicate omitting doses stopping medicationswithout consulting a doctor and inappropriately changingdoses are common behaviours However supplyingmedications to patients does not guarantee the medicationsare actually taken In fact a systematic review of randomisedcontrol trials showed that about half the medicines prescribedfor chronic diseases are not taken (Haynes et al 1996) Inaddition self-reported behaviour is subjective andproblematic For example people who say they do not followtreatment may report accurately while people who deny notfollowing recommendations may report inaccurately(Spector 1986)
The majority of these studies relied on self-report Actualpractices were not directly observed and no researcherreported asking about self-prescribed medicines andcomplementary therapy use There is a high rate ofcomplementary therapy use among people with diabetes(Egede et al 2002) and there are a growing number of reportsof undesirable drugherb interactions and adverse eventsrelating to the use of some complementary therapies bypeople with diabetes (Dunning 2003)
The impact of education on adherence is welldocumented (Kriev et al 1999) but adherence is a complexphenomenon and is difficult to predict Adherence isinfluenced by many factors and is dependent on anindividualrsquos problem-solving skills beliefs and attitudessocial situation and support and is complex and demanding(Jones 2003) The term is often used in a derogatory way thatdoes not take account of the fact that it has physicalpsychological attitudinal and social components Themajority of medication adherence studies focus on adherenceto the medication recommendations knowledge andbehaviour Only rarely have physical limitations andfinancial factors been explored with people with diabetesWhen they are it is usually with respect to oralhypoglycaemic agents (OHA) and insulin administration(Coscelli et al 1992 Tay et al 2001 Evans et al 2002)
People with diabetes frequently have complications andconcomitant diseases that make it difficult for them toperform some diabetes self-care tasks including managingtheir medications For example arthritis limits manualdexterity and makes it difficult to test blood glucose breaktablets administer insulin and open medication packagesDiabetes complications include reduced vision and
retinopathy yet consumer medication information andmedicine labels are often presented in small fonts that aredifficult to read even with glasses An important and rarelyconsidered factor is the impact of health professionalattitudes and beliefs and health system issues on anindividualrsquos willingness and ability to follow treatmentrecommendations
Regular diabetes complication screening is an Australianestablished nationally co-ordinated project known asANDIAB Home medication reviews were introduced morerecently but routine monitoring of medication self-careability and behaviours rarely occurs in a structured way andis not a focus of either of these processes Diabetesmanagement guidelines based on the Diabetes Control andComplications Trial (DCCT) (1993) and The UnitedKingdom Prospective Diabetes Study (UKPDS) (1998)stress the need to achieve good blood glucose lipid andblood pressure control and lsquotreating to targetrsquo That isachieving evidence-based metabolic blood pressure andweight targets The targets are getting lower as the evidencethat tight metabolic control prevents morbidity and mortalityaccumulates
As a consequence more medications are added to thetreatment regime which become more complexPolypharmacy is the norm and could be considered bestpractice in light of diabetes management guidelines thatrecommend aiming for normoglycaemia and normal lipidand blood pressure ranges For example people withdiabetes can expect to take three to four antihypertensiveagents as well as insulin or oral hypoglycaemic and lipidlowering agents for their diabetes as well as a range ofmedications for other diabetes complications or concomitantdiseases The cost of uncontrolled diabetes is high andcarries significant morbidity and mortality rates thereforepolypharmacy can be justified However it leads tocomplicated medication regimes that are more likely to leadto mistakes andor non-adherence
The Quality Use of Medicines (QUM) initiative has beena key component of the National Health Policy in Australiasince 1992 and is slowly being integrated into patientmedication self-management education programs The basictenets of QUM are the primacy of the patient collaborativemultidisciplinary practice a systems based approach thejudicious selection and use of medicines if medicines areindicated and regular outcome monitoring Researchindicates medicines use is less than optimal nationally andnurses have a shared professional responsibility for QUM(Griffiths et al 2001) This responsibility includes monitoringpatient medication self-management especially in chronicdisease such as diabetes where medicines are often requiredfor life A number of health professionals including diabeteseducators are responsible for instructing patients aboutappropriate medication usage
Despite the knowledge that good blood glucose controlreduces the long term complications of diabetes (DCCT1993 UKPDS 1998) and the availability of the technologyto achieve it good control is not achieved in many cases(Dunning 1994) Factors such as attitudes beliefs and self-
RESEARCH PAPER
8Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 19
care practices including appropriate use of medicines aresome of the intervening variables between having theknowledge applying it and achieving good metaboliccontrol
Non-adherence for whatever reason threatens theprovision of effective diabetes care Lustman (1995) statedthat seven out of 10 leading causes of death are linked tobehaviour If that is so more consideration of thebehavioural factors associated with diabetes medication self-management appears to be warranted
AIM OF THE STUDYThe study aimed to explore the medication knowledge
and self-management practices of people with type 2diabetes referred to the diabetes outpatient services by theirgeneral practitioners
For the purpose of the study medication knowledgeconsisted of seven specific items of information being ableto name all medicines being used what the medicine wasprescribed for the dose to take when the medicine should betaken potential side effects how to store the medicine andhow to dispose of unused or outdated medicines Self-management practices included being able to open medicinepackages break tablets in half administer insulin andmonitor blood glucose levels
METHODSA cross-sectional survey using structured interviews and
observations of respondents performing relevant medicationself-management practices was used to collect the data Theinterview questionnaire was developed specifically for thestudy
Face and content validity was established by consultingwith relevant experts and pilot testing the draft questionnaireon a representative group from the sampling population whowere subsequently excluded from the study Ethics approvalwas obtained from the relevant human research ethicscommittee
The sampling population and study sampleThe sampling population consisted of all people attending
the diabetes education centre of an inner city universityteaching hospital who were taking medications and able togive informed consent including those referred by theirgeneral practitioners (GP) Between 30 and 45 outpatientsare seen each week primarily by the diabetes educatorsClose links have been established with the referring GPsthrough a diabetes shared care scheme where GPs undertakediabetes management in consultation with the diabeteseducators and endocrinologists A large proportion ofpatients attending the centre are from multiculturalbackgrounds predominantly Vietnam Greece Turkey Italyand South East Asia
Patients were invited to participate when they presented tothe diabetes educator and were given written information
about the study Informed written consent was obtained ifthey agreed to participate and an appointment was made forthem to return to the diabetes education centre where thedata were collected
Participants were asked to bring all of the medicationsthey were taking including any complementary and over-the-counter medicines vitamin and mineral supplements andtheir usual blood glucose testing equipment to theappointment These requirements were written on anappointment card together with directions to the centre
The questionnaireThe questionnaire addressed four domains a) standard
demographic data to ascertain if there was any correlationbetween patient demographic characteristics and medicationmanagement practices b) medication type dose frequencyobtaining prescriptions and having them filled c) educationand knowledge and d) complementary and over-the-countermedicines
Participant observationsParticipants were observed undertaking specific
medication-related activities such as breaking tablets in halfopening medication packages preparing and administeringan insulin dose and testing their blood glucose and the resultsrecorded on a data base
Data analysisInterval and categorical data were analysed using
ANOVA and Chi Square respectively to ascertain anysignificant relationship between the variables Descriptivestatistics including means standard deviation and frequencycounts were used for the demographic data The Pearsoncorrelation coefficient was used to test the degree ofassociation between interval level data Content analysis wasused for the open questions where each question was readline-by-line to note any emerging themes (Morse 1994)Words phrases and sentences were classified into categoriesin which the number of occurrences of a particular categorygave an indicator of the relative importance of the behaviouror activity described
RESULTSThirty people were interviewed Each interview took
approximately two hours
1 Demographic data
Seventeen males and 13 females took part age range 33-84 years mean 687plusmn1335 SD A range of ethnicbackgrounds was represented including Turkish ItalianGreek Chinese and Vietnamese Twelve participants did notspeak English and an interpreter assisted with the interviewsHbA1c which provides an accurate measure of long termglucose control ranged from 57ndash109 (normal 45ndash6using High Pressure Liquid Chromatography [HPLC])Twenty-seven respondents had at least one diabeticcomplication and the majority had three or more The mostcommonly occurring complications were retinopathy
RESEARCH PAPER
macrovascular disease and neuropathy and erectiledysfunction Four were taking antidepressant medicines Themost common concomitant diseases were arthritis andthyroid disease
2 Medication usageOverall 86 different prescribed conventional medicines
and nine self-initiated or complementary medicines andsupplements were used Individuals were taking an averageof 74 medicines range 1ndash12plusmn297 SD Thirty three percentused insulin 46 were on OHAs and 20 were taking acombination of OHA and insulin
Overall respondents were on 10 differentantihypertensive agents six types of lipid lowering agentsthree different aspirin formulations and a range of othermedicines including anticoagulants and diuretics Themajority 66 were on twice a day OHAinsulin regimesTwenty-three percent were on daily and 10 on three times aday regimes Forty-six percent took their medicines beforemeals 36 after meals and 16 with meals Most had beenon medications for ge10 years range 1ndashge10
Complementary therapiesParticipants described complementary therapies as lsquousing
old medicines for current problemsrsquo lsquothings that improvewellbeing and quality of lifersquo and lsquosomething other thanregular medicinesrsquo In three cases the GP had referredpatients to a complementary therapist for massagechiropractic or relaxation Table 1 outlines the reasons peoplegave for using complementary therapies Twenty-threepercent used complementary and self-initiated medicationswhich included vitamin and mineral supplements aperientsanalgesics iron tablets cold remedies amino acidsupplements garlic aloe vera and tea tree essential oil on afoot ulcer
Obtaining medications
Seventy-three percent always obtained their medicinesfrom the same pharmacy and collected them themselvesThirty percent required assistance to obtain their medicinesdue to poor vision or difficulty getting to a pharmacy Inthese cases seven relatives (spouses daughters) collectedmedicines from the pharmacy and also helped with dosingOne pharmacist and one GP delivered medicines to thehomes of two participants
In the majority of cases (90) prescriptions were writtenby the GP which is consistent with centre policy Fifty-twopercent of GPs wrote repeat prescriptions without reviewingthe patient and left the script with the receptionist to becollected or sent the script directly to the pharmacist
Reported costs of medications per year ranged from lessthan $100 to more than $600 (mode $100) Thirty-sixpercent paid more for medications than they had in theprevious year mostly because they needed more medicationsand the cost of some medicines had increased
People used a range of strategies to pay for theirmedications including doing occasional work because thepension was inadequate employing budget strategies and
making sacrifices in other areas One person lsquokept mydiabetes medicines but threw the others away because of thecostrsquo and one lsquogot tired of taking them so I stopped Theywere not doing any good anywayrsquo Another respondentstopped all his medications because of the cost None ofthese respondents consulted their doctors before theystopped their medicines One person shared their diabetesmedicines and blood pressure tablets with a relative whohelped with the costs Fifteen were enrolled in the NationalDiabetes Services Scheme one in the Veteran AffairsScheme which are schemes set up by the AustralianGovernment to subsidise the cost of some non-medicinalproducts Three had private health insurance
Disposal of unused medicines andor sharpsEighty-three percent monitored their blood glucose at
home and they all used meters The majority 80 did notperform control tests on their meters to ensure they werereading accurately but did calibrate the meter with each newbatch of strips Thirty-three percent discarded used needlesand lancets (sharps) directly into the rubbish Unusedmedicines were generally left in the cupboard taken away bya relative or discarded into the rubbish
Education about medicinesEighty-three percent of respondents reported having
specific education about their medicines when they wereprescribed Table 2 shows a breakdown of the specificmedicine-related education items received The majoritywere given information about how to take (93) and whento take (93) medicines and ge50 accurately reported thisinformation for most of their medicines However only 37were given information about and could name possible sideeffects of their medicines The risk of hypoglycaemia withinsulin was the best known medicine side effect In additiononly 17 received all seven possible items of informationThe GP was the most frequently reported education providerTable 3 shows the mean differences between patients who
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 110
Table 1 Reasons participants gave for using complementarytherapies and the main therapies they used
Reason Therapies used
Arthritis MassageGlucosamine sulphate tabletsReiki
Reduce stress Mediationand improve wellbeing Aromatherapy
Improve immunity Vitamins and mineralsAromatherapy massage with thymebasil and clove oils
Reduce blood glucose Herbs and bitter melon prickly pear
Treat wounds fungal Tea tree essential oilinfections on feet Aloe vera gel
Treat colds EchinaceaLemon and honey drinks
Because they are holistic
They work with medicines to help feel better and control blood glucose
Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

EDITORIAL
REFERENCESAhern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38 (3)303-309
Firtko A and Jackson D 2005 Do the ends justify the means Nursing andthe dilemma of whistleblowing Australian Journal of Advanced Nursing23(1)51-56
Muir-Gray JA 1997 Evidence-based health care How to make health policyand management decisions Edinburgh Churchill Livingstone
Peter E Lunardi V and Macfarlane A 2004 Nursing resistance as ethicalaction literature review Journal of Advanced Nursing 46(4)403-416
Seago JA and Ash M 2002 Registered nurse union and patient outcomesJournal of Nursing Administration 32143-151
Speedy S 2004 Organisation violations Implications for leadership In DalyJ Speedy Sand Jackson D (eds) Nursing Leadership Sydney ChurchillLivingstone145-164
Australian Journal of Advanced Nursing 2005 Volume 23 Number 16
Australian Journal of Advanced Nursing 2005 Volume 23 Number 17
Trisha Dunning AM RN MEd PhD FRCNA DirectorEndocrinology and Diabetes Nursing Research Department of Endocrinology and Diabetes St Vincentrsquos Hospital School of Nursing The University of Melbourne MelbourneVictoria Australia
trishdunningsvhmorgau
Elizabeth Manias RN MPharm MNStud PhD FRCNA Schoolof Nursing The University of Melbourne Victoria Australia
Accepted for publication December 2004
ACKNOWLEDGEMENTSThe researchers are grateful to Megan Lalor for assistance with data collectionThe research was supported by an Eli Lilly Diabetes Education Research Grantand we thank Eli Lilly for making the grant available
MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
RESEARCH PAPER
Key words type 2 diabetes medication knowledge self-care
ABSTRACT
ObjectiveTo explore medication knowledge and self-
management practices of people with type 2 diabetes
DesignA one-shot cross sectional study using in-depth
interviews and participant observation
SettingDiabetes outpatient education centre of a university
teaching hospital
SubjectsPeople with type 2 diabetes n=30 17 males and 13
females age range 33-84 from a range of ethnic groups
Outcome measuresAbility to state name main actions and when to take
medicines Performance of specific medication-relatedtasks opening bottles and packs breaking tablets in halfadministering insulin and testing blood glucose
ResultsAverage medication use ge10years Respondents were
taking 86 different medicines mean 7plusmn297 SD Dosefrequency included two three and four times per day Allrespondents had ge2 diabetic complications plusmn othercomorbidities The majority (93) were informed abouthow and when to take their medicines but only 37were given information about side effects and 17 weregiven all possible seven items of information Youngerrespondents received more information than olderrespondents Older respondents had difficulty openingbottles and breaking tablets in half Twenty percentregularly forgot to take their medicines Increasingmedication costs was one reason for stopping medicinesor reducing the dose or dose interval The majority tested
their blood glucose but did not control test their metersand 33 placed used sharps directly into the rubbish
ConclusionPolypharmacy was common Medication knowledge
and self-management were inadequate and could lead toadverse events
INTRODUCTION
Diabetes is a chronic disease that affects 75 ofAustralians over 25 and 168 over 65 years(Dunstan et al 2000) Long term self-care and
education are needed to control blood glucose levels andreduce the risk of complications and adverse medication-related events
These necessary skills include blood glucose monitoringand medication administration Over time the complexity ofthe medication regime increases for people with type 2diabetes because of the associated complicationscomorbidities and pancreatic beta cell exhaustion (Olefsky etal 1999) This means the complexity of the self-care regimeincreases often at the same time as the person is growingolder and eyesight hearing fine motor skills and memoryand information processing are changing These changesmake it difficult for the individual to comply withrecommended self-care practices such as blood glucosetesting and medication management including insulinadministration
Anecdotal evidence suggests that many people withdiabetes do not have adequate knowledge about themedications they take stop medications and alter dosesinappropriately without consulting their doctors and do notunderstand the actions side effects or potential interactionsof the medications they take even those they have beentaking for years
In particular older people are more likely to have physicalproblems that make safe medication usage difficult and they
make significantly more insulin dose errors using syringes(DeBrew et al 1998) despite the advent of premixed insulinformulations such as Mixtard and modern insulin deliverydevices (Coscelli et al 1992) Inappropriate medication usageis likely to have an effect on blood glucose control andtherefore on health outcomes and diabetes-related healthcosts In addition inadequate medication self-care increasesthe likelihood of admission to a nursing home (Stradberg1984)
A number of researchers have examined medicationissues such as adherence by monitoring pill counts thefrequency of completing the full course of a medicationscript refill rates and ability to open medication packages(Matsuyama et al 1993 Paes et al 1997 Kriev et al 1999)These studies indicate omitting doses stopping medicationswithout consulting a doctor and inappropriately changingdoses are common behaviours However supplyingmedications to patients does not guarantee the medicationsare actually taken In fact a systematic review of randomisedcontrol trials showed that about half the medicines prescribedfor chronic diseases are not taken (Haynes et al 1996) Inaddition self-reported behaviour is subjective andproblematic For example people who say they do not followtreatment may report accurately while people who deny notfollowing recommendations may report inaccurately(Spector 1986)
The majority of these studies relied on self-report Actualpractices were not directly observed and no researcherreported asking about self-prescribed medicines andcomplementary therapy use There is a high rate ofcomplementary therapy use among people with diabetes(Egede et al 2002) and there are a growing number of reportsof undesirable drugherb interactions and adverse eventsrelating to the use of some complementary therapies bypeople with diabetes (Dunning 2003)
The impact of education on adherence is welldocumented (Kriev et al 1999) but adherence is a complexphenomenon and is difficult to predict Adherence isinfluenced by many factors and is dependent on anindividualrsquos problem-solving skills beliefs and attitudessocial situation and support and is complex and demanding(Jones 2003) The term is often used in a derogatory way thatdoes not take account of the fact that it has physicalpsychological attitudinal and social components Themajority of medication adherence studies focus on adherenceto the medication recommendations knowledge andbehaviour Only rarely have physical limitations andfinancial factors been explored with people with diabetesWhen they are it is usually with respect to oralhypoglycaemic agents (OHA) and insulin administration(Coscelli et al 1992 Tay et al 2001 Evans et al 2002)
People with diabetes frequently have complications andconcomitant diseases that make it difficult for them toperform some diabetes self-care tasks including managingtheir medications For example arthritis limits manualdexterity and makes it difficult to test blood glucose breaktablets administer insulin and open medication packagesDiabetes complications include reduced vision and
retinopathy yet consumer medication information andmedicine labels are often presented in small fonts that aredifficult to read even with glasses An important and rarelyconsidered factor is the impact of health professionalattitudes and beliefs and health system issues on anindividualrsquos willingness and ability to follow treatmentrecommendations
Regular diabetes complication screening is an Australianestablished nationally co-ordinated project known asANDIAB Home medication reviews were introduced morerecently but routine monitoring of medication self-careability and behaviours rarely occurs in a structured way andis not a focus of either of these processes Diabetesmanagement guidelines based on the Diabetes Control andComplications Trial (DCCT) (1993) and The UnitedKingdom Prospective Diabetes Study (UKPDS) (1998)stress the need to achieve good blood glucose lipid andblood pressure control and lsquotreating to targetrsquo That isachieving evidence-based metabolic blood pressure andweight targets The targets are getting lower as the evidencethat tight metabolic control prevents morbidity and mortalityaccumulates
As a consequence more medications are added to thetreatment regime which become more complexPolypharmacy is the norm and could be considered bestpractice in light of diabetes management guidelines thatrecommend aiming for normoglycaemia and normal lipidand blood pressure ranges For example people withdiabetes can expect to take three to four antihypertensiveagents as well as insulin or oral hypoglycaemic and lipidlowering agents for their diabetes as well as a range ofmedications for other diabetes complications or concomitantdiseases The cost of uncontrolled diabetes is high andcarries significant morbidity and mortality rates thereforepolypharmacy can be justified However it leads tocomplicated medication regimes that are more likely to leadto mistakes andor non-adherence
The Quality Use of Medicines (QUM) initiative has beena key component of the National Health Policy in Australiasince 1992 and is slowly being integrated into patientmedication self-management education programs The basictenets of QUM are the primacy of the patient collaborativemultidisciplinary practice a systems based approach thejudicious selection and use of medicines if medicines areindicated and regular outcome monitoring Researchindicates medicines use is less than optimal nationally andnurses have a shared professional responsibility for QUM(Griffiths et al 2001) This responsibility includes monitoringpatient medication self-management especially in chronicdisease such as diabetes where medicines are often requiredfor life A number of health professionals including diabeteseducators are responsible for instructing patients aboutappropriate medication usage
Despite the knowledge that good blood glucose controlreduces the long term complications of diabetes (DCCT1993 UKPDS 1998) and the availability of the technologyto achieve it good control is not achieved in many cases(Dunning 1994) Factors such as attitudes beliefs and self-
RESEARCH PAPER
8Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 19
care practices including appropriate use of medicines aresome of the intervening variables between having theknowledge applying it and achieving good metaboliccontrol
Non-adherence for whatever reason threatens theprovision of effective diabetes care Lustman (1995) statedthat seven out of 10 leading causes of death are linked tobehaviour If that is so more consideration of thebehavioural factors associated with diabetes medication self-management appears to be warranted
AIM OF THE STUDYThe study aimed to explore the medication knowledge
and self-management practices of people with type 2diabetes referred to the diabetes outpatient services by theirgeneral practitioners
For the purpose of the study medication knowledgeconsisted of seven specific items of information being ableto name all medicines being used what the medicine wasprescribed for the dose to take when the medicine should betaken potential side effects how to store the medicine andhow to dispose of unused or outdated medicines Self-management practices included being able to open medicinepackages break tablets in half administer insulin andmonitor blood glucose levels
METHODSA cross-sectional survey using structured interviews and
observations of respondents performing relevant medicationself-management practices was used to collect the data Theinterview questionnaire was developed specifically for thestudy
Face and content validity was established by consultingwith relevant experts and pilot testing the draft questionnaireon a representative group from the sampling population whowere subsequently excluded from the study Ethics approvalwas obtained from the relevant human research ethicscommittee
The sampling population and study sampleThe sampling population consisted of all people attending
the diabetes education centre of an inner city universityteaching hospital who were taking medications and able togive informed consent including those referred by theirgeneral practitioners (GP) Between 30 and 45 outpatientsare seen each week primarily by the diabetes educatorsClose links have been established with the referring GPsthrough a diabetes shared care scheme where GPs undertakediabetes management in consultation with the diabeteseducators and endocrinologists A large proportion ofpatients attending the centre are from multiculturalbackgrounds predominantly Vietnam Greece Turkey Italyand South East Asia
Patients were invited to participate when they presented tothe diabetes educator and were given written information
about the study Informed written consent was obtained ifthey agreed to participate and an appointment was made forthem to return to the diabetes education centre where thedata were collected
Participants were asked to bring all of the medicationsthey were taking including any complementary and over-the-counter medicines vitamin and mineral supplements andtheir usual blood glucose testing equipment to theappointment These requirements were written on anappointment card together with directions to the centre
The questionnaireThe questionnaire addressed four domains a) standard
demographic data to ascertain if there was any correlationbetween patient demographic characteristics and medicationmanagement practices b) medication type dose frequencyobtaining prescriptions and having them filled c) educationand knowledge and d) complementary and over-the-countermedicines
Participant observationsParticipants were observed undertaking specific
medication-related activities such as breaking tablets in halfopening medication packages preparing and administeringan insulin dose and testing their blood glucose and the resultsrecorded on a data base
Data analysisInterval and categorical data were analysed using
ANOVA and Chi Square respectively to ascertain anysignificant relationship between the variables Descriptivestatistics including means standard deviation and frequencycounts were used for the demographic data The Pearsoncorrelation coefficient was used to test the degree ofassociation between interval level data Content analysis wasused for the open questions where each question was readline-by-line to note any emerging themes (Morse 1994)Words phrases and sentences were classified into categoriesin which the number of occurrences of a particular categorygave an indicator of the relative importance of the behaviouror activity described
RESULTSThirty people were interviewed Each interview took
approximately two hours
1 Demographic data
Seventeen males and 13 females took part age range 33-84 years mean 687plusmn1335 SD A range of ethnicbackgrounds was represented including Turkish ItalianGreek Chinese and Vietnamese Twelve participants did notspeak English and an interpreter assisted with the interviewsHbA1c which provides an accurate measure of long termglucose control ranged from 57ndash109 (normal 45ndash6using High Pressure Liquid Chromatography [HPLC])Twenty-seven respondents had at least one diabeticcomplication and the majority had three or more The mostcommonly occurring complications were retinopathy
RESEARCH PAPER
macrovascular disease and neuropathy and erectiledysfunction Four were taking antidepressant medicines Themost common concomitant diseases were arthritis andthyroid disease
2 Medication usageOverall 86 different prescribed conventional medicines
and nine self-initiated or complementary medicines andsupplements were used Individuals were taking an averageof 74 medicines range 1ndash12plusmn297 SD Thirty three percentused insulin 46 were on OHAs and 20 were taking acombination of OHA and insulin
Overall respondents were on 10 differentantihypertensive agents six types of lipid lowering agentsthree different aspirin formulations and a range of othermedicines including anticoagulants and diuretics Themajority 66 were on twice a day OHAinsulin regimesTwenty-three percent were on daily and 10 on three times aday regimes Forty-six percent took their medicines beforemeals 36 after meals and 16 with meals Most had beenon medications for ge10 years range 1ndashge10
Complementary therapiesParticipants described complementary therapies as lsquousing
old medicines for current problemsrsquo lsquothings that improvewellbeing and quality of lifersquo and lsquosomething other thanregular medicinesrsquo In three cases the GP had referredpatients to a complementary therapist for massagechiropractic or relaxation Table 1 outlines the reasons peoplegave for using complementary therapies Twenty-threepercent used complementary and self-initiated medicationswhich included vitamin and mineral supplements aperientsanalgesics iron tablets cold remedies amino acidsupplements garlic aloe vera and tea tree essential oil on afoot ulcer
Obtaining medications
Seventy-three percent always obtained their medicinesfrom the same pharmacy and collected them themselvesThirty percent required assistance to obtain their medicinesdue to poor vision or difficulty getting to a pharmacy Inthese cases seven relatives (spouses daughters) collectedmedicines from the pharmacy and also helped with dosingOne pharmacist and one GP delivered medicines to thehomes of two participants
In the majority of cases (90) prescriptions were writtenby the GP which is consistent with centre policy Fifty-twopercent of GPs wrote repeat prescriptions without reviewingthe patient and left the script with the receptionist to becollected or sent the script directly to the pharmacist
Reported costs of medications per year ranged from lessthan $100 to more than $600 (mode $100) Thirty-sixpercent paid more for medications than they had in theprevious year mostly because they needed more medicationsand the cost of some medicines had increased
People used a range of strategies to pay for theirmedications including doing occasional work because thepension was inadequate employing budget strategies and
making sacrifices in other areas One person lsquokept mydiabetes medicines but threw the others away because of thecostrsquo and one lsquogot tired of taking them so I stopped Theywere not doing any good anywayrsquo Another respondentstopped all his medications because of the cost None ofthese respondents consulted their doctors before theystopped their medicines One person shared their diabetesmedicines and blood pressure tablets with a relative whohelped with the costs Fifteen were enrolled in the NationalDiabetes Services Scheme one in the Veteran AffairsScheme which are schemes set up by the AustralianGovernment to subsidise the cost of some non-medicinalproducts Three had private health insurance
Disposal of unused medicines andor sharpsEighty-three percent monitored their blood glucose at
home and they all used meters The majority 80 did notperform control tests on their meters to ensure they werereading accurately but did calibrate the meter with each newbatch of strips Thirty-three percent discarded used needlesand lancets (sharps) directly into the rubbish Unusedmedicines were generally left in the cupboard taken away bya relative or discarded into the rubbish
Education about medicinesEighty-three percent of respondents reported having
specific education about their medicines when they wereprescribed Table 2 shows a breakdown of the specificmedicine-related education items received The majoritywere given information about how to take (93) and whento take (93) medicines and ge50 accurately reported thisinformation for most of their medicines However only 37were given information about and could name possible sideeffects of their medicines The risk of hypoglycaemia withinsulin was the best known medicine side effect In additiononly 17 received all seven possible items of informationThe GP was the most frequently reported education providerTable 3 shows the mean differences between patients who
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 110
Table 1 Reasons participants gave for using complementarytherapies and the main therapies they used
Reason Therapies used
Arthritis MassageGlucosamine sulphate tabletsReiki
Reduce stress Mediationand improve wellbeing Aromatherapy
Improve immunity Vitamins and mineralsAromatherapy massage with thymebasil and clove oils
Reduce blood glucose Herbs and bitter melon prickly pear
Treat wounds fungal Tea tree essential oilinfections on feet Aloe vera gel
Treat colds EchinaceaLemon and honey drinks
Because they are holistic
They work with medicines to help feel better and control blood glucose
Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

Australian Journal of Advanced Nursing 2005 Volume 23 Number 17
Trisha Dunning AM RN MEd PhD FRCNA DirectorEndocrinology and Diabetes Nursing Research Department of Endocrinology and Diabetes St Vincentrsquos Hospital School of Nursing The University of Melbourne MelbourneVictoria Australia
trishdunningsvhmorgau
Elizabeth Manias RN MPharm MNStud PhD FRCNA Schoolof Nursing The University of Melbourne Victoria Australia
Accepted for publication December 2004
ACKNOWLEDGEMENTSThe researchers are grateful to Megan Lalor for assistance with data collectionThe research was supported by an Eli Lilly Diabetes Education Research Grantand we thank Eli Lilly for making the grant available
MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
RESEARCH PAPER
Key words type 2 diabetes medication knowledge self-care
ABSTRACT
ObjectiveTo explore medication knowledge and self-
management practices of people with type 2 diabetes
DesignA one-shot cross sectional study using in-depth
interviews and participant observation
SettingDiabetes outpatient education centre of a university
teaching hospital
SubjectsPeople with type 2 diabetes n=30 17 males and 13
females age range 33-84 from a range of ethnic groups
Outcome measuresAbility to state name main actions and when to take
medicines Performance of specific medication-relatedtasks opening bottles and packs breaking tablets in halfadministering insulin and testing blood glucose
ResultsAverage medication use ge10years Respondents were
taking 86 different medicines mean 7plusmn297 SD Dosefrequency included two three and four times per day Allrespondents had ge2 diabetic complications plusmn othercomorbidities The majority (93) were informed abouthow and when to take their medicines but only 37were given information about side effects and 17 weregiven all possible seven items of information Youngerrespondents received more information than olderrespondents Older respondents had difficulty openingbottles and breaking tablets in half Twenty percentregularly forgot to take their medicines Increasingmedication costs was one reason for stopping medicinesor reducing the dose or dose interval The majority tested
their blood glucose but did not control test their metersand 33 placed used sharps directly into the rubbish
ConclusionPolypharmacy was common Medication knowledge
and self-management were inadequate and could lead toadverse events
INTRODUCTION
Diabetes is a chronic disease that affects 75 ofAustralians over 25 and 168 over 65 years(Dunstan et al 2000) Long term self-care and
education are needed to control blood glucose levels andreduce the risk of complications and adverse medication-related events
These necessary skills include blood glucose monitoringand medication administration Over time the complexity ofthe medication regime increases for people with type 2diabetes because of the associated complicationscomorbidities and pancreatic beta cell exhaustion (Olefsky etal 1999) This means the complexity of the self-care regimeincreases often at the same time as the person is growingolder and eyesight hearing fine motor skills and memoryand information processing are changing These changesmake it difficult for the individual to comply withrecommended self-care practices such as blood glucosetesting and medication management including insulinadministration
Anecdotal evidence suggests that many people withdiabetes do not have adequate knowledge about themedications they take stop medications and alter dosesinappropriately without consulting their doctors and do notunderstand the actions side effects or potential interactionsof the medications they take even those they have beentaking for years
In particular older people are more likely to have physicalproblems that make safe medication usage difficult and they
make significantly more insulin dose errors using syringes(DeBrew et al 1998) despite the advent of premixed insulinformulations such as Mixtard and modern insulin deliverydevices (Coscelli et al 1992) Inappropriate medication usageis likely to have an effect on blood glucose control andtherefore on health outcomes and diabetes-related healthcosts In addition inadequate medication self-care increasesthe likelihood of admission to a nursing home (Stradberg1984)
A number of researchers have examined medicationissues such as adherence by monitoring pill counts thefrequency of completing the full course of a medicationscript refill rates and ability to open medication packages(Matsuyama et al 1993 Paes et al 1997 Kriev et al 1999)These studies indicate omitting doses stopping medicationswithout consulting a doctor and inappropriately changingdoses are common behaviours However supplyingmedications to patients does not guarantee the medicationsare actually taken In fact a systematic review of randomisedcontrol trials showed that about half the medicines prescribedfor chronic diseases are not taken (Haynes et al 1996) Inaddition self-reported behaviour is subjective andproblematic For example people who say they do not followtreatment may report accurately while people who deny notfollowing recommendations may report inaccurately(Spector 1986)
The majority of these studies relied on self-report Actualpractices were not directly observed and no researcherreported asking about self-prescribed medicines andcomplementary therapy use There is a high rate ofcomplementary therapy use among people with diabetes(Egede et al 2002) and there are a growing number of reportsof undesirable drugherb interactions and adverse eventsrelating to the use of some complementary therapies bypeople with diabetes (Dunning 2003)
The impact of education on adherence is welldocumented (Kriev et al 1999) but adherence is a complexphenomenon and is difficult to predict Adherence isinfluenced by many factors and is dependent on anindividualrsquos problem-solving skills beliefs and attitudessocial situation and support and is complex and demanding(Jones 2003) The term is often used in a derogatory way thatdoes not take account of the fact that it has physicalpsychological attitudinal and social components Themajority of medication adherence studies focus on adherenceto the medication recommendations knowledge andbehaviour Only rarely have physical limitations andfinancial factors been explored with people with diabetesWhen they are it is usually with respect to oralhypoglycaemic agents (OHA) and insulin administration(Coscelli et al 1992 Tay et al 2001 Evans et al 2002)
People with diabetes frequently have complications andconcomitant diseases that make it difficult for them toperform some diabetes self-care tasks including managingtheir medications For example arthritis limits manualdexterity and makes it difficult to test blood glucose breaktablets administer insulin and open medication packagesDiabetes complications include reduced vision and
retinopathy yet consumer medication information andmedicine labels are often presented in small fonts that aredifficult to read even with glasses An important and rarelyconsidered factor is the impact of health professionalattitudes and beliefs and health system issues on anindividualrsquos willingness and ability to follow treatmentrecommendations
Regular diabetes complication screening is an Australianestablished nationally co-ordinated project known asANDIAB Home medication reviews were introduced morerecently but routine monitoring of medication self-careability and behaviours rarely occurs in a structured way andis not a focus of either of these processes Diabetesmanagement guidelines based on the Diabetes Control andComplications Trial (DCCT) (1993) and The UnitedKingdom Prospective Diabetes Study (UKPDS) (1998)stress the need to achieve good blood glucose lipid andblood pressure control and lsquotreating to targetrsquo That isachieving evidence-based metabolic blood pressure andweight targets The targets are getting lower as the evidencethat tight metabolic control prevents morbidity and mortalityaccumulates
As a consequence more medications are added to thetreatment regime which become more complexPolypharmacy is the norm and could be considered bestpractice in light of diabetes management guidelines thatrecommend aiming for normoglycaemia and normal lipidand blood pressure ranges For example people withdiabetes can expect to take three to four antihypertensiveagents as well as insulin or oral hypoglycaemic and lipidlowering agents for their diabetes as well as a range ofmedications for other diabetes complications or concomitantdiseases The cost of uncontrolled diabetes is high andcarries significant morbidity and mortality rates thereforepolypharmacy can be justified However it leads tocomplicated medication regimes that are more likely to leadto mistakes andor non-adherence
The Quality Use of Medicines (QUM) initiative has beena key component of the National Health Policy in Australiasince 1992 and is slowly being integrated into patientmedication self-management education programs The basictenets of QUM are the primacy of the patient collaborativemultidisciplinary practice a systems based approach thejudicious selection and use of medicines if medicines areindicated and regular outcome monitoring Researchindicates medicines use is less than optimal nationally andnurses have a shared professional responsibility for QUM(Griffiths et al 2001) This responsibility includes monitoringpatient medication self-management especially in chronicdisease such as diabetes where medicines are often requiredfor life A number of health professionals including diabeteseducators are responsible for instructing patients aboutappropriate medication usage
Despite the knowledge that good blood glucose controlreduces the long term complications of diabetes (DCCT1993 UKPDS 1998) and the availability of the technologyto achieve it good control is not achieved in many cases(Dunning 1994) Factors such as attitudes beliefs and self-
RESEARCH PAPER
8Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 19
care practices including appropriate use of medicines aresome of the intervening variables between having theknowledge applying it and achieving good metaboliccontrol
Non-adherence for whatever reason threatens theprovision of effective diabetes care Lustman (1995) statedthat seven out of 10 leading causes of death are linked tobehaviour If that is so more consideration of thebehavioural factors associated with diabetes medication self-management appears to be warranted
AIM OF THE STUDYThe study aimed to explore the medication knowledge
and self-management practices of people with type 2diabetes referred to the diabetes outpatient services by theirgeneral practitioners
For the purpose of the study medication knowledgeconsisted of seven specific items of information being ableto name all medicines being used what the medicine wasprescribed for the dose to take when the medicine should betaken potential side effects how to store the medicine andhow to dispose of unused or outdated medicines Self-management practices included being able to open medicinepackages break tablets in half administer insulin andmonitor blood glucose levels
METHODSA cross-sectional survey using structured interviews and
observations of respondents performing relevant medicationself-management practices was used to collect the data Theinterview questionnaire was developed specifically for thestudy
Face and content validity was established by consultingwith relevant experts and pilot testing the draft questionnaireon a representative group from the sampling population whowere subsequently excluded from the study Ethics approvalwas obtained from the relevant human research ethicscommittee
The sampling population and study sampleThe sampling population consisted of all people attending
the diabetes education centre of an inner city universityteaching hospital who were taking medications and able togive informed consent including those referred by theirgeneral practitioners (GP) Between 30 and 45 outpatientsare seen each week primarily by the diabetes educatorsClose links have been established with the referring GPsthrough a diabetes shared care scheme where GPs undertakediabetes management in consultation with the diabeteseducators and endocrinologists A large proportion ofpatients attending the centre are from multiculturalbackgrounds predominantly Vietnam Greece Turkey Italyand South East Asia
Patients were invited to participate when they presented tothe diabetes educator and were given written information
about the study Informed written consent was obtained ifthey agreed to participate and an appointment was made forthem to return to the diabetes education centre where thedata were collected
Participants were asked to bring all of the medicationsthey were taking including any complementary and over-the-counter medicines vitamin and mineral supplements andtheir usual blood glucose testing equipment to theappointment These requirements were written on anappointment card together with directions to the centre
The questionnaireThe questionnaire addressed four domains a) standard
demographic data to ascertain if there was any correlationbetween patient demographic characteristics and medicationmanagement practices b) medication type dose frequencyobtaining prescriptions and having them filled c) educationand knowledge and d) complementary and over-the-countermedicines
Participant observationsParticipants were observed undertaking specific
medication-related activities such as breaking tablets in halfopening medication packages preparing and administeringan insulin dose and testing their blood glucose and the resultsrecorded on a data base
Data analysisInterval and categorical data were analysed using
ANOVA and Chi Square respectively to ascertain anysignificant relationship between the variables Descriptivestatistics including means standard deviation and frequencycounts were used for the demographic data The Pearsoncorrelation coefficient was used to test the degree ofassociation between interval level data Content analysis wasused for the open questions where each question was readline-by-line to note any emerging themes (Morse 1994)Words phrases and sentences were classified into categoriesin which the number of occurrences of a particular categorygave an indicator of the relative importance of the behaviouror activity described
RESULTSThirty people were interviewed Each interview took
approximately two hours
1 Demographic data
Seventeen males and 13 females took part age range 33-84 years mean 687plusmn1335 SD A range of ethnicbackgrounds was represented including Turkish ItalianGreek Chinese and Vietnamese Twelve participants did notspeak English and an interpreter assisted with the interviewsHbA1c which provides an accurate measure of long termglucose control ranged from 57ndash109 (normal 45ndash6using High Pressure Liquid Chromatography [HPLC])Twenty-seven respondents had at least one diabeticcomplication and the majority had three or more The mostcommonly occurring complications were retinopathy
RESEARCH PAPER
macrovascular disease and neuropathy and erectiledysfunction Four were taking antidepressant medicines Themost common concomitant diseases were arthritis andthyroid disease
2 Medication usageOverall 86 different prescribed conventional medicines
and nine self-initiated or complementary medicines andsupplements were used Individuals were taking an averageof 74 medicines range 1ndash12plusmn297 SD Thirty three percentused insulin 46 were on OHAs and 20 were taking acombination of OHA and insulin
Overall respondents were on 10 differentantihypertensive agents six types of lipid lowering agentsthree different aspirin formulations and a range of othermedicines including anticoagulants and diuretics Themajority 66 were on twice a day OHAinsulin regimesTwenty-three percent were on daily and 10 on three times aday regimes Forty-six percent took their medicines beforemeals 36 after meals and 16 with meals Most had beenon medications for ge10 years range 1ndashge10
Complementary therapiesParticipants described complementary therapies as lsquousing
old medicines for current problemsrsquo lsquothings that improvewellbeing and quality of lifersquo and lsquosomething other thanregular medicinesrsquo In three cases the GP had referredpatients to a complementary therapist for massagechiropractic or relaxation Table 1 outlines the reasons peoplegave for using complementary therapies Twenty-threepercent used complementary and self-initiated medicationswhich included vitamin and mineral supplements aperientsanalgesics iron tablets cold remedies amino acidsupplements garlic aloe vera and tea tree essential oil on afoot ulcer
Obtaining medications
Seventy-three percent always obtained their medicinesfrom the same pharmacy and collected them themselvesThirty percent required assistance to obtain their medicinesdue to poor vision or difficulty getting to a pharmacy Inthese cases seven relatives (spouses daughters) collectedmedicines from the pharmacy and also helped with dosingOne pharmacist and one GP delivered medicines to thehomes of two participants
In the majority of cases (90) prescriptions were writtenby the GP which is consistent with centre policy Fifty-twopercent of GPs wrote repeat prescriptions without reviewingthe patient and left the script with the receptionist to becollected or sent the script directly to the pharmacist
Reported costs of medications per year ranged from lessthan $100 to more than $600 (mode $100) Thirty-sixpercent paid more for medications than they had in theprevious year mostly because they needed more medicationsand the cost of some medicines had increased
People used a range of strategies to pay for theirmedications including doing occasional work because thepension was inadequate employing budget strategies and
making sacrifices in other areas One person lsquokept mydiabetes medicines but threw the others away because of thecostrsquo and one lsquogot tired of taking them so I stopped Theywere not doing any good anywayrsquo Another respondentstopped all his medications because of the cost None ofthese respondents consulted their doctors before theystopped their medicines One person shared their diabetesmedicines and blood pressure tablets with a relative whohelped with the costs Fifteen were enrolled in the NationalDiabetes Services Scheme one in the Veteran AffairsScheme which are schemes set up by the AustralianGovernment to subsidise the cost of some non-medicinalproducts Three had private health insurance
Disposal of unused medicines andor sharpsEighty-three percent monitored their blood glucose at
home and they all used meters The majority 80 did notperform control tests on their meters to ensure they werereading accurately but did calibrate the meter with each newbatch of strips Thirty-three percent discarded used needlesand lancets (sharps) directly into the rubbish Unusedmedicines were generally left in the cupboard taken away bya relative or discarded into the rubbish
Education about medicinesEighty-three percent of respondents reported having
specific education about their medicines when they wereprescribed Table 2 shows a breakdown of the specificmedicine-related education items received The majoritywere given information about how to take (93) and whento take (93) medicines and ge50 accurately reported thisinformation for most of their medicines However only 37were given information about and could name possible sideeffects of their medicines The risk of hypoglycaemia withinsulin was the best known medicine side effect In additiononly 17 received all seven possible items of informationThe GP was the most frequently reported education providerTable 3 shows the mean differences between patients who
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 110
Table 1 Reasons participants gave for using complementarytherapies and the main therapies they used
Reason Therapies used
Arthritis MassageGlucosamine sulphate tabletsReiki
Reduce stress Mediationand improve wellbeing Aromatherapy
Improve immunity Vitamins and mineralsAromatherapy massage with thymebasil and clove oils
Reduce blood glucose Herbs and bitter melon prickly pear
Treat wounds fungal Tea tree essential oilinfections on feet Aloe vera gel
Treat colds EchinaceaLemon and honey drinks
Because they are holistic
They work with medicines to help feel better and control blood glucose
Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

make significantly more insulin dose errors using syringes(DeBrew et al 1998) despite the advent of premixed insulinformulations such as Mixtard and modern insulin deliverydevices (Coscelli et al 1992) Inappropriate medication usageis likely to have an effect on blood glucose control andtherefore on health outcomes and diabetes-related healthcosts In addition inadequate medication self-care increasesthe likelihood of admission to a nursing home (Stradberg1984)
A number of researchers have examined medicationissues such as adherence by monitoring pill counts thefrequency of completing the full course of a medicationscript refill rates and ability to open medication packages(Matsuyama et al 1993 Paes et al 1997 Kriev et al 1999)These studies indicate omitting doses stopping medicationswithout consulting a doctor and inappropriately changingdoses are common behaviours However supplyingmedications to patients does not guarantee the medicationsare actually taken In fact a systematic review of randomisedcontrol trials showed that about half the medicines prescribedfor chronic diseases are not taken (Haynes et al 1996) Inaddition self-reported behaviour is subjective andproblematic For example people who say they do not followtreatment may report accurately while people who deny notfollowing recommendations may report inaccurately(Spector 1986)
The majority of these studies relied on self-report Actualpractices were not directly observed and no researcherreported asking about self-prescribed medicines andcomplementary therapy use There is a high rate ofcomplementary therapy use among people with diabetes(Egede et al 2002) and there are a growing number of reportsof undesirable drugherb interactions and adverse eventsrelating to the use of some complementary therapies bypeople with diabetes (Dunning 2003)
The impact of education on adherence is welldocumented (Kriev et al 1999) but adherence is a complexphenomenon and is difficult to predict Adherence isinfluenced by many factors and is dependent on anindividualrsquos problem-solving skills beliefs and attitudessocial situation and support and is complex and demanding(Jones 2003) The term is often used in a derogatory way thatdoes not take account of the fact that it has physicalpsychological attitudinal and social components Themajority of medication adherence studies focus on adherenceto the medication recommendations knowledge andbehaviour Only rarely have physical limitations andfinancial factors been explored with people with diabetesWhen they are it is usually with respect to oralhypoglycaemic agents (OHA) and insulin administration(Coscelli et al 1992 Tay et al 2001 Evans et al 2002)
People with diabetes frequently have complications andconcomitant diseases that make it difficult for them toperform some diabetes self-care tasks including managingtheir medications For example arthritis limits manualdexterity and makes it difficult to test blood glucose breaktablets administer insulin and open medication packagesDiabetes complications include reduced vision and
retinopathy yet consumer medication information andmedicine labels are often presented in small fonts that aredifficult to read even with glasses An important and rarelyconsidered factor is the impact of health professionalattitudes and beliefs and health system issues on anindividualrsquos willingness and ability to follow treatmentrecommendations
Regular diabetes complication screening is an Australianestablished nationally co-ordinated project known asANDIAB Home medication reviews were introduced morerecently but routine monitoring of medication self-careability and behaviours rarely occurs in a structured way andis not a focus of either of these processes Diabetesmanagement guidelines based on the Diabetes Control andComplications Trial (DCCT) (1993) and The UnitedKingdom Prospective Diabetes Study (UKPDS) (1998)stress the need to achieve good blood glucose lipid andblood pressure control and lsquotreating to targetrsquo That isachieving evidence-based metabolic blood pressure andweight targets The targets are getting lower as the evidencethat tight metabolic control prevents morbidity and mortalityaccumulates
As a consequence more medications are added to thetreatment regime which become more complexPolypharmacy is the norm and could be considered bestpractice in light of diabetes management guidelines thatrecommend aiming for normoglycaemia and normal lipidand blood pressure ranges For example people withdiabetes can expect to take three to four antihypertensiveagents as well as insulin or oral hypoglycaemic and lipidlowering agents for their diabetes as well as a range ofmedications for other diabetes complications or concomitantdiseases The cost of uncontrolled diabetes is high andcarries significant morbidity and mortality rates thereforepolypharmacy can be justified However it leads tocomplicated medication regimes that are more likely to leadto mistakes andor non-adherence
The Quality Use of Medicines (QUM) initiative has beena key component of the National Health Policy in Australiasince 1992 and is slowly being integrated into patientmedication self-management education programs The basictenets of QUM are the primacy of the patient collaborativemultidisciplinary practice a systems based approach thejudicious selection and use of medicines if medicines areindicated and regular outcome monitoring Researchindicates medicines use is less than optimal nationally andnurses have a shared professional responsibility for QUM(Griffiths et al 2001) This responsibility includes monitoringpatient medication self-management especially in chronicdisease such as diabetes where medicines are often requiredfor life A number of health professionals including diabeteseducators are responsible for instructing patients aboutappropriate medication usage
Despite the knowledge that good blood glucose controlreduces the long term complications of diabetes (DCCT1993 UKPDS 1998) and the availability of the technologyto achieve it good control is not achieved in many cases(Dunning 1994) Factors such as attitudes beliefs and self-
RESEARCH PAPER
8Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 19
care practices including appropriate use of medicines aresome of the intervening variables between having theknowledge applying it and achieving good metaboliccontrol
Non-adherence for whatever reason threatens theprovision of effective diabetes care Lustman (1995) statedthat seven out of 10 leading causes of death are linked tobehaviour If that is so more consideration of thebehavioural factors associated with diabetes medication self-management appears to be warranted
AIM OF THE STUDYThe study aimed to explore the medication knowledge
and self-management practices of people with type 2diabetes referred to the diabetes outpatient services by theirgeneral practitioners
For the purpose of the study medication knowledgeconsisted of seven specific items of information being ableto name all medicines being used what the medicine wasprescribed for the dose to take when the medicine should betaken potential side effects how to store the medicine andhow to dispose of unused or outdated medicines Self-management practices included being able to open medicinepackages break tablets in half administer insulin andmonitor blood glucose levels
METHODSA cross-sectional survey using structured interviews and
observations of respondents performing relevant medicationself-management practices was used to collect the data Theinterview questionnaire was developed specifically for thestudy
Face and content validity was established by consultingwith relevant experts and pilot testing the draft questionnaireon a representative group from the sampling population whowere subsequently excluded from the study Ethics approvalwas obtained from the relevant human research ethicscommittee
The sampling population and study sampleThe sampling population consisted of all people attending
the diabetes education centre of an inner city universityteaching hospital who were taking medications and able togive informed consent including those referred by theirgeneral practitioners (GP) Between 30 and 45 outpatientsare seen each week primarily by the diabetes educatorsClose links have been established with the referring GPsthrough a diabetes shared care scheme where GPs undertakediabetes management in consultation with the diabeteseducators and endocrinologists A large proportion ofpatients attending the centre are from multiculturalbackgrounds predominantly Vietnam Greece Turkey Italyand South East Asia
Patients were invited to participate when they presented tothe diabetes educator and were given written information
about the study Informed written consent was obtained ifthey agreed to participate and an appointment was made forthem to return to the diabetes education centre where thedata were collected
Participants were asked to bring all of the medicationsthey were taking including any complementary and over-the-counter medicines vitamin and mineral supplements andtheir usual blood glucose testing equipment to theappointment These requirements were written on anappointment card together with directions to the centre
The questionnaireThe questionnaire addressed four domains a) standard
demographic data to ascertain if there was any correlationbetween patient demographic characteristics and medicationmanagement practices b) medication type dose frequencyobtaining prescriptions and having them filled c) educationand knowledge and d) complementary and over-the-countermedicines
Participant observationsParticipants were observed undertaking specific
medication-related activities such as breaking tablets in halfopening medication packages preparing and administeringan insulin dose and testing their blood glucose and the resultsrecorded on a data base
Data analysisInterval and categorical data were analysed using
ANOVA and Chi Square respectively to ascertain anysignificant relationship between the variables Descriptivestatistics including means standard deviation and frequencycounts were used for the demographic data The Pearsoncorrelation coefficient was used to test the degree ofassociation between interval level data Content analysis wasused for the open questions where each question was readline-by-line to note any emerging themes (Morse 1994)Words phrases and sentences were classified into categoriesin which the number of occurrences of a particular categorygave an indicator of the relative importance of the behaviouror activity described
RESULTSThirty people were interviewed Each interview took
approximately two hours
1 Demographic data
Seventeen males and 13 females took part age range 33-84 years mean 687plusmn1335 SD A range of ethnicbackgrounds was represented including Turkish ItalianGreek Chinese and Vietnamese Twelve participants did notspeak English and an interpreter assisted with the interviewsHbA1c which provides an accurate measure of long termglucose control ranged from 57ndash109 (normal 45ndash6using High Pressure Liquid Chromatography [HPLC])Twenty-seven respondents had at least one diabeticcomplication and the majority had three or more The mostcommonly occurring complications were retinopathy
RESEARCH PAPER
macrovascular disease and neuropathy and erectiledysfunction Four were taking antidepressant medicines Themost common concomitant diseases were arthritis andthyroid disease
2 Medication usageOverall 86 different prescribed conventional medicines
and nine self-initiated or complementary medicines andsupplements were used Individuals were taking an averageof 74 medicines range 1ndash12plusmn297 SD Thirty three percentused insulin 46 were on OHAs and 20 were taking acombination of OHA and insulin
Overall respondents were on 10 differentantihypertensive agents six types of lipid lowering agentsthree different aspirin formulations and a range of othermedicines including anticoagulants and diuretics Themajority 66 were on twice a day OHAinsulin regimesTwenty-three percent were on daily and 10 on three times aday regimes Forty-six percent took their medicines beforemeals 36 after meals and 16 with meals Most had beenon medications for ge10 years range 1ndashge10
Complementary therapiesParticipants described complementary therapies as lsquousing
old medicines for current problemsrsquo lsquothings that improvewellbeing and quality of lifersquo and lsquosomething other thanregular medicinesrsquo In three cases the GP had referredpatients to a complementary therapist for massagechiropractic or relaxation Table 1 outlines the reasons peoplegave for using complementary therapies Twenty-threepercent used complementary and self-initiated medicationswhich included vitamin and mineral supplements aperientsanalgesics iron tablets cold remedies amino acidsupplements garlic aloe vera and tea tree essential oil on afoot ulcer
Obtaining medications
Seventy-three percent always obtained their medicinesfrom the same pharmacy and collected them themselvesThirty percent required assistance to obtain their medicinesdue to poor vision or difficulty getting to a pharmacy Inthese cases seven relatives (spouses daughters) collectedmedicines from the pharmacy and also helped with dosingOne pharmacist and one GP delivered medicines to thehomes of two participants
In the majority of cases (90) prescriptions were writtenby the GP which is consistent with centre policy Fifty-twopercent of GPs wrote repeat prescriptions without reviewingthe patient and left the script with the receptionist to becollected or sent the script directly to the pharmacist
Reported costs of medications per year ranged from lessthan $100 to more than $600 (mode $100) Thirty-sixpercent paid more for medications than they had in theprevious year mostly because they needed more medicationsand the cost of some medicines had increased
People used a range of strategies to pay for theirmedications including doing occasional work because thepension was inadequate employing budget strategies and
making sacrifices in other areas One person lsquokept mydiabetes medicines but threw the others away because of thecostrsquo and one lsquogot tired of taking them so I stopped Theywere not doing any good anywayrsquo Another respondentstopped all his medications because of the cost None ofthese respondents consulted their doctors before theystopped their medicines One person shared their diabetesmedicines and blood pressure tablets with a relative whohelped with the costs Fifteen were enrolled in the NationalDiabetes Services Scheme one in the Veteran AffairsScheme which are schemes set up by the AustralianGovernment to subsidise the cost of some non-medicinalproducts Three had private health insurance
Disposal of unused medicines andor sharpsEighty-three percent monitored their blood glucose at
home and they all used meters The majority 80 did notperform control tests on their meters to ensure they werereading accurately but did calibrate the meter with each newbatch of strips Thirty-three percent discarded used needlesand lancets (sharps) directly into the rubbish Unusedmedicines were generally left in the cupboard taken away bya relative or discarded into the rubbish
Education about medicinesEighty-three percent of respondents reported having
specific education about their medicines when they wereprescribed Table 2 shows a breakdown of the specificmedicine-related education items received The majoritywere given information about how to take (93) and whento take (93) medicines and ge50 accurately reported thisinformation for most of their medicines However only 37were given information about and could name possible sideeffects of their medicines The risk of hypoglycaemia withinsulin was the best known medicine side effect In additiononly 17 received all seven possible items of informationThe GP was the most frequently reported education providerTable 3 shows the mean differences between patients who
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 110
Table 1 Reasons participants gave for using complementarytherapies and the main therapies they used
Reason Therapies used
Arthritis MassageGlucosamine sulphate tabletsReiki
Reduce stress Mediationand improve wellbeing Aromatherapy
Improve immunity Vitamins and mineralsAromatherapy massage with thymebasil and clove oils
Reduce blood glucose Herbs and bitter melon prickly pear
Treat wounds fungal Tea tree essential oilinfections on feet Aloe vera gel
Treat colds EchinaceaLemon and honey drinks
Because they are holistic
They work with medicines to help feel better and control blood glucose
Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

Australian Journal of Advanced Nursing 2005 Volume 23 Number 19
care practices including appropriate use of medicines aresome of the intervening variables between having theknowledge applying it and achieving good metaboliccontrol
Non-adherence for whatever reason threatens theprovision of effective diabetes care Lustman (1995) statedthat seven out of 10 leading causes of death are linked tobehaviour If that is so more consideration of thebehavioural factors associated with diabetes medication self-management appears to be warranted
AIM OF THE STUDYThe study aimed to explore the medication knowledge
and self-management practices of people with type 2diabetes referred to the diabetes outpatient services by theirgeneral practitioners
For the purpose of the study medication knowledgeconsisted of seven specific items of information being ableto name all medicines being used what the medicine wasprescribed for the dose to take when the medicine should betaken potential side effects how to store the medicine andhow to dispose of unused or outdated medicines Self-management practices included being able to open medicinepackages break tablets in half administer insulin andmonitor blood glucose levels
METHODSA cross-sectional survey using structured interviews and
observations of respondents performing relevant medicationself-management practices was used to collect the data Theinterview questionnaire was developed specifically for thestudy
Face and content validity was established by consultingwith relevant experts and pilot testing the draft questionnaireon a representative group from the sampling population whowere subsequently excluded from the study Ethics approvalwas obtained from the relevant human research ethicscommittee
The sampling population and study sampleThe sampling population consisted of all people attending
the diabetes education centre of an inner city universityteaching hospital who were taking medications and able togive informed consent including those referred by theirgeneral practitioners (GP) Between 30 and 45 outpatientsare seen each week primarily by the diabetes educatorsClose links have been established with the referring GPsthrough a diabetes shared care scheme where GPs undertakediabetes management in consultation with the diabeteseducators and endocrinologists A large proportion ofpatients attending the centre are from multiculturalbackgrounds predominantly Vietnam Greece Turkey Italyand South East Asia
Patients were invited to participate when they presented tothe diabetes educator and were given written information
about the study Informed written consent was obtained ifthey agreed to participate and an appointment was made forthem to return to the diabetes education centre where thedata were collected
Participants were asked to bring all of the medicationsthey were taking including any complementary and over-the-counter medicines vitamin and mineral supplements andtheir usual blood glucose testing equipment to theappointment These requirements were written on anappointment card together with directions to the centre
The questionnaireThe questionnaire addressed four domains a) standard
demographic data to ascertain if there was any correlationbetween patient demographic characteristics and medicationmanagement practices b) medication type dose frequencyobtaining prescriptions and having them filled c) educationand knowledge and d) complementary and over-the-countermedicines
Participant observationsParticipants were observed undertaking specific
medication-related activities such as breaking tablets in halfopening medication packages preparing and administeringan insulin dose and testing their blood glucose and the resultsrecorded on a data base
Data analysisInterval and categorical data were analysed using
ANOVA and Chi Square respectively to ascertain anysignificant relationship between the variables Descriptivestatistics including means standard deviation and frequencycounts were used for the demographic data The Pearsoncorrelation coefficient was used to test the degree ofassociation between interval level data Content analysis wasused for the open questions where each question was readline-by-line to note any emerging themes (Morse 1994)Words phrases and sentences were classified into categoriesin which the number of occurrences of a particular categorygave an indicator of the relative importance of the behaviouror activity described
RESULTSThirty people were interviewed Each interview took
approximately two hours
1 Demographic data
Seventeen males and 13 females took part age range 33-84 years mean 687plusmn1335 SD A range of ethnicbackgrounds was represented including Turkish ItalianGreek Chinese and Vietnamese Twelve participants did notspeak English and an interpreter assisted with the interviewsHbA1c which provides an accurate measure of long termglucose control ranged from 57ndash109 (normal 45ndash6using High Pressure Liquid Chromatography [HPLC])Twenty-seven respondents had at least one diabeticcomplication and the majority had three or more The mostcommonly occurring complications were retinopathy
RESEARCH PAPER
macrovascular disease and neuropathy and erectiledysfunction Four were taking antidepressant medicines Themost common concomitant diseases were arthritis andthyroid disease
2 Medication usageOverall 86 different prescribed conventional medicines
and nine self-initiated or complementary medicines andsupplements were used Individuals were taking an averageof 74 medicines range 1ndash12plusmn297 SD Thirty three percentused insulin 46 were on OHAs and 20 were taking acombination of OHA and insulin
Overall respondents were on 10 differentantihypertensive agents six types of lipid lowering agentsthree different aspirin formulations and a range of othermedicines including anticoagulants and diuretics Themajority 66 were on twice a day OHAinsulin regimesTwenty-three percent were on daily and 10 on three times aday regimes Forty-six percent took their medicines beforemeals 36 after meals and 16 with meals Most had beenon medications for ge10 years range 1ndashge10
Complementary therapiesParticipants described complementary therapies as lsquousing
old medicines for current problemsrsquo lsquothings that improvewellbeing and quality of lifersquo and lsquosomething other thanregular medicinesrsquo In three cases the GP had referredpatients to a complementary therapist for massagechiropractic or relaxation Table 1 outlines the reasons peoplegave for using complementary therapies Twenty-threepercent used complementary and self-initiated medicationswhich included vitamin and mineral supplements aperientsanalgesics iron tablets cold remedies amino acidsupplements garlic aloe vera and tea tree essential oil on afoot ulcer
Obtaining medications
Seventy-three percent always obtained their medicinesfrom the same pharmacy and collected them themselvesThirty percent required assistance to obtain their medicinesdue to poor vision or difficulty getting to a pharmacy Inthese cases seven relatives (spouses daughters) collectedmedicines from the pharmacy and also helped with dosingOne pharmacist and one GP delivered medicines to thehomes of two participants
In the majority of cases (90) prescriptions were writtenby the GP which is consistent with centre policy Fifty-twopercent of GPs wrote repeat prescriptions without reviewingthe patient and left the script with the receptionist to becollected or sent the script directly to the pharmacist
Reported costs of medications per year ranged from lessthan $100 to more than $600 (mode $100) Thirty-sixpercent paid more for medications than they had in theprevious year mostly because they needed more medicationsand the cost of some medicines had increased
People used a range of strategies to pay for theirmedications including doing occasional work because thepension was inadequate employing budget strategies and
making sacrifices in other areas One person lsquokept mydiabetes medicines but threw the others away because of thecostrsquo and one lsquogot tired of taking them so I stopped Theywere not doing any good anywayrsquo Another respondentstopped all his medications because of the cost None ofthese respondents consulted their doctors before theystopped their medicines One person shared their diabetesmedicines and blood pressure tablets with a relative whohelped with the costs Fifteen were enrolled in the NationalDiabetes Services Scheme one in the Veteran AffairsScheme which are schemes set up by the AustralianGovernment to subsidise the cost of some non-medicinalproducts Three had private health insurance
Disposal of unused medicines andor sharpsEighty-three percent monitored their blood glucose at
home and they all used meters The majority 80 did notperform control tests on their meters to ensure they werereading accurately but did calibrate the meter with each newbatch of strips Thirty-three percent discarded used needlesand lancets (sharps) directly into the rubbish Unusedmedicines were generally left in the cupboard taken away bya relative or discarded into the rubbish
Education about medicinesEighty-three percent of respondents reported having
specific education about their medicines when they wereprescribed Table 2 shows a breakdown of the specificmedicine-related education items received The majoritywere given information about how to take (93) and whento take (93) medicines and ge50 accurately reported thisinformation for most of their medicines However only 37were given information about and could name possible sideeffects of their medicines The risk of hypoglycaemia withinsulin was the best known medicine side effect In additiononly 17 received all seven possible items of informationThe GP was the most frequently reported education providerTable 3 shows the mean differences between patients who
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 110
Table 1 Reasons participants gave for using complementarytherapies and the main therapies they used
Reason Therapies used
Arthritis MassageGlucosamine sulphate tabletsReiki
Reduce stress Mediationand improve wellbeing Aromatherapy
Improve immunity Vitamins and mineralsAromatherapy massage with thymebasil and clove oils
Reduce blood glucose Herbs and bitter melon prickly pear
Treat wounds fungal Tea tree essential oilinfections on feet Aloe vera gel
Treat colds EchinaceaLemon and honey drinks
Because they are holistic
They work with medicines to help feel better and control blood glucose
Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

macrovascular disease and neuropathy and erectiledysfunction Four were taking antidepressant medicines Themost common concomitant diseases were arthritis andthyroid disease
2 Medication usageOverall 86 different prescribed conventional medicines
and nine self-initiated or complementary medicines andsupplements were used Individuals were taking an averageof 74 medicines range 1ndash12plusmn297 SD Thirty three percentused insulin 46 were on OHAs and 20 were taking acombination of OHA and insulin
Overall respondents were on 10 differentantihypertensive agents six types of lipid lowering agentsthree different aspirin formulations and a range of othermedicines including anticoagulants and diuretics Themajority 66 were on twice a day OHAinsulin regimesTwenty-three percent were on daily and 10 on three times aday regimes Forty-six percent took their medicines beforemeals 36 after meals and 16 with meals Most had beenon medications for ge10 years range 1ndashge10
Complementary therapiesParticipants described complementary therapies as lsquousing
old medicines for current problemsrsquo lsquothings that improvewellbeing and quality of lifersquo and lsquosomething other thanregular medicinesrsquo In three cases the GP had referredpatients to a complementary therapist for massagechiropractic or relaxation Table 1 outlines the reasons peoplegave for using complementary therapies Twenty-threepercent used complementary and self-initiated medicationswhich included vitamin and mineral supplements aperientsanalgesics iron tablets cold remedies amino acidsupplements garlic aloe vera and tea tree essential oil on afoot ulcer
Obtaining medications
Seventy-three percent always obtained their medicinesfrom the same pharmacy and collected them themselvesThirty percent required assistance to obtain their medicinesdue to poor vision or difficulty getting to a pharmacy Inthese cases seven relatives (spouses daughters) collectedmedicines from the pharmacy and also helped with dosingOne pharmacist and one GP delivered medicines to thehomes of two participants
In the majority of cases (90) prescriptions were writtenby the GP which is consistent with centre policy Fifty-twopercent of GPs wrote repeat prescriptions without reviewingthe patient and left the script with the receptionist to becollected or sent the script directly to the pharmacist
Reported costs of medications per year ranged from lessthan $100 to more than $600 (mode $100) Thirty-sixpercent paid more for medications than they had in theprevious year mostly because they needed more medicationsand the cost of some medicines had increased
People used a range of strategies to pay for theirmedications including doing occasional work because thepension was inadequate employing budget strategies and
making sacrifices in other areas One person lsquokept mydiabetes medicines but threw the others away because of thecostrsquo and one lsquogot tired of taking them so I stopped Theywere not doing any good anywayrsquo Another respondentstopped all his medications because of the cost None ofthese respondents consulted their doctors before theystopped their medicines One person shared their diabetesmedicines and blood pressure tablets with a relative whohelped with the costs Fifteen were enrolled in the NationalDiabetes Services Scheme one in the Veteran AffairsScheme which are schemes set up by the AustralianGovernment to subsidise the cost of some non-medicinalproducts Three had private health insurance
Disposal of unused medicines andor sharpsEighty-three percent monitored their blood glucose at
home and they all used meters The majority 80 did notperform control tests on their meters to ensure they werereading accurately but did calibrate the meter with each newbatch of strips Thirty-three percent discarded used needlesand lancets (sharps) directly into the rubbish Unusedmedicines were generally left in the cupboard taken away bya relative or discarded into the rubbish
Education about medicinesEighty-three percent of respondents reported having
specific education about their medicines when they wereprescribed Table 2 shows a breakdown of the specificmedicine-related education items received The majoritywere given information about how to take (93) and whento take (93) medicines and ge50 accurately reported thisinformation for most of their medicines However only 37were given information about and could name possible sideeffects of their medicines The risk of hypoglycaemia withinsulin was the best known medicine side effect In additiononly 17 received all seven possible items of informationThe GP was the most frequently reported education providerTable 3 shows the mean differences between patients who
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 110
Table 1 Reasons participants gave for using complementarytherapies and the main therapies they used
Reason Therapies used
Arthritis MassageGlucosamine sulphate tabletsReiki
Reduce stress Mediationand improve wellbeing Aromatherapy
Improve immunity Vitamins and mineralsAromatherapy massage with thymebasil and clove oils
Reduce blood glucose Herbs and bitter melon prickly pear
Treat wounds fungal Tea tree essential oilinfections on feet Aloe vera gel
Treat colds EchinaceaLemon and honey drinks
Because they are holistic
They work with medicines to help feel better and control blood glucose
Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

Australian Journal of Advanced Nursing 2005 Volume 23 Number 111
RESEARCH PAPER
received education from their GPs alone and those whoreceived education from GPs and other education providersThere were no significant differences (p=005)
There was a negative correlation between age and totalpieces of education delivered suggesting younger patientsreceived more information about issues such as side effectsand how to store than older patients but the relationship wasnot statistically significant (p=005)
Ability to administer medicines
The majority were able to open their medicine bottles ordosettes but five people all over 65 and all women livingalone were not able to open a childproof cap Sevenindividuals who needed to break at least one tablet in halfwere not able to do so accurately even though three used apill cutter (two used a knife) Sixteen percent of participantsusing insulin did not dial up the correct dose
Twenty percent regularly forgot to take their medicationsand offered the following reasons
lsquoI am getting older and my memory is not what it used to bersquo
lsquoI forget to take my insulin to workrsquo
lsquoI do not forget insulin but forget the metformin quite oftenrsquo
lsquoI like to have a rest from pills when I am on holidays andeating outrsquo
lsquoIt is human nature to forgetrsquo
lsquoToo busy to remember-sometimes often actuallyrsquo
These participants adopted a number of strategies whenthey realised they had missed a dose The majority did notworry and took the medicines when the next dose was dueOthers took all or part of the dose whenever theyremembered and two individuals telephoned their doctorsfor advice
Perceptions of blood glucose controlAll respondents had HBA1c estimations performed at
least once in the past 12 months Ninety-nine percentindicated they had good blood glucose control but only oneparticipantrsquos HbA1c was in the target range (lt7)
Medication side effectsFifty percent of the respondents reported hypoglycaemic
episodes 43 had no hypoglycaemia and 3 were not sureEducation was associated with greater likelihood ofreporting hypoglycaemic episodes (r=022 p=024) whichrose to (r=-030 p=011) after correcting for the effect ofage The correlation between age and hypoglycaemicepisodes was negative at -013 That is older age wasassociated with a lower chance of having hypoglycaemicepisodes
Table 2 The seven specific education items related to medicines use participants were asked about in the study and the percentage ofpositive and negative responses
Medicine related information items Response category responses
How it works No 433Yes 567
How to store No 50Yes 50
How to take No 17Yes 83
When to take No 7Yes 93
Side effects No 63Yes 37
Special precautions No 70Yes 30
Appropriate disposal No 57Yes 43
Table 3 Mean differences between patients who received information from their GP only and those who received information from their GPandor other health professionals
GP only Mean difference GP and Other pMean difference
What medicine is for 337 273 0085
When to take medicine 353 364 0370
What the effects are 279 164 0004
How long effects last 189 145 0138
Side effects 195 118 0025
Correct dose 289 245 0192
Total knowledge of medicines 1642 1309 005
Pharmacist diabetes educator nurse
RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-

RESEARCH PAPER
There was no significant difference in the proportions ofwomen (54) versus men (54) reporting hypoglycaemicepisodes (Chi square =146 p=048) There was nosignificant relationship between smoking andhypoglycaemic episodes (p=083) 67 for smokers and50 for non-smokers indicating a trend toward significancethat may have been evident in a larger sample There was nosignificant relationship between alcohol and hypoglycaemiaepisodes with an equal proportion of self-reported drinkers(50) and non-drinkers (52) reporting hypoglycaemicepisodes
Participants reported side effects to some drugsvenlafaxine SR (drowsiness) isosorbide mononitrate(nausea) prednisolone (thirst) metformin (diarrhoea andnausea) and bruising following insulin injections All of thereported side effects were correctly attributed to the specific drug however some such as thirst anddrowsiness could have been a consequence ofhyperglycaemia
DISCUSSIONThe demographic characteristics of the sample were
similar to other studies undertaken in the same samplingpopulation (Dunning 1994 2003) This finding suggests thesample was representative of people who attend the diabetescentre and enhances the ability to transfer the findingsbeyond the sample However the results may not beapplicable to other settings
A number of participants reported forgetting to take theirmedications or discontinuing them if they could not affordthe cost Other researchers have demonstrated older patientsuse fewer medicines because of the costs (Tokarski 2004)Patients in Tokarskirsquos study said they continued to take theircore diabetes medications but cut back on analgesics andmedicines such as Viagra
Participants in our study adopted a number of strategieswhen they realised they had forgotten to take theirmedicines In some instances they lsquodid not worryrsquo and tookthe next scheduled dose With long acting medications thismay be appropriate behaviour and may not greatly affecttherapeutic blood levels However where drugs have anarrow therapeutic index or are needed in frequent dosesadequate blood levels of the drug may be compromised egwarfarin and digoxin
Conversely stopping medicines may reduce the risk ofadverse drug events Given the high incidence ofcomplications and comorbidities in individuals in the currentstudy medicines other than the lsquodiabetes medicinesrsquo werenecessary and stopping them increases the risk of long termcomplications
Other researchers have reported suboptimal compliancewith OHA (Evans et al 2002) Evans et al (2002) based theirconclusions on the number of medications actuallydispensed to patients (filled prescriptions) and found onethird of the individuals in the study did not obtain sufficientsupplies of OHAs Filled prescription rates were not used as
a measure of appropriate medicines self-management in thecurrent study It does not indicate actual or self-reportedmedicine use and does not take into account the physical andsocial limitations involved in managing medicines
Gilbert et al (2002) reported more than 80 ofindividuals missed medicine doses and suggested planningstrategies with individuals when medicines were prescribedso they would know what to do when they missed doses
In contrast only 20 of participants in the current studyregularly forgot to take their medicines and gave a range ofreasons for forgetting but none of the participants had beenspecifically told what to do if they missed a medication doseSless and Wiseman (1997) make a similar recommendationin Writing about medicines for people Usability guidelinesconsumer medicine information (Sless and Wiseman 1997)These are a set of guidelines primarily for pharmaceuticalcompanies which specify how to prepare information aboutmedicines for consumers The extent to which the relevantConsumer Medicine Information sheets (CMI) were utilisedin the current study is unknown
Participants were certainly on a high average number ofdrugs per day which equates to polypharmacyPolypharmacy is a complex issue and involves finding abalance between necessary drugs and the associated risk ofmultidrug use such as interactions in addition to increasingthe complexity of the regime It is not known whether thecomplexity of the regimen affected medicine use in the studyparticipants but it is likely given the evidence for such effectsin other populations Given the currently agreed stringentblood glucose lipid and blood pressure targetspolypharmacy may be best practice in diabetes management
One significant side effect of OHAs and insulin ishypoglycaemia The risk of hypoglycaemia due to druginteractions and age-related changes that affect drugpharmacodynamics and pharmacodynamics increases withpolypharmacy The incidence of hypoglycaemia was high inthe current study (50) but factors in addition to or otherthan drug interactions may have led to hypoglycaemia forexample reduced food intake and increased activity Therewere no reports of serious hypoglycaemia requiringhospitalisation and patients managed hypoglycaemiaappropriately
Twenty percent reported using complementary therapiesand over-the-counter medications which is consistent withother studies in the same population (Dunning 2003) Therewas no indication that patients substituted these therapies forconventional prescribed drugs although some individualswere taking herbal therapies to control blood glucose Thereis some evidence to support the blood glucose loweringeffects of both the preparations being used which may haveincreased the risk of hypoglycaemia if they were also takingOHAs or insulin Using hypoglycaemic herbs incombination with OHAs may enable lower dose of thesemedicines to be used which is consistent with QUMrecommendations to use the lowest possible effective dose
12Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Australian Journal of Advanced Nursing 2005 Volume 23 Number 113
RESEARCH PAPERRESEARCH PAPER
It was of concern that many patients were able to obtainrepeat prescriptions from their GP without having to see theGP GP visits represent ideal opportunities for medicationpractices and knowledge to be assessed which are missed ifthe patient is not actually seen GPs usually refer patients to adiabetes educator when insulin is required but diabeteseducators rarely provide specific detailed education aboutthe other medicines people are prescribed For instance mostparticipants received education about some aspects of howand when to take medicines but only 37 were informedabout potential side effects especially if they were elderlyHowever it is not clear if they had been given theinformation originally and forgot or whether the informationwas given in a way that was not relevant to the individualCertainly they did not appear to have been given CMI or tohave read the package insert that comes with all prescriptionmedicines in Australia CMI does not usually accompanycomplementary medicines and over-the-counter-medicines
Frequent reminders are important education strategiesand improve adherence Regular reviews of knowledge andself-care skills are necessary in any chronic disease wherephysical and mental changes can affect self-care The focusin diabetes care has been on regular screening forcomplications but systematic medication review has not beena focus of these programs Factual reminders (Germer et al1986 Tay et al 2001) and mailed reminders (Haynes et al1996) have been shown to improve adherence Homemedication reviews linking medicines review to annualreview offering individual education and involving patientsby seeking concordance rather than focusing on complianceare other ways of achieving effective medicines use (RoyalPharmaceutical Society of Great Britain 1997) Concordancein this sense refers to achieving agreed goals
The lack of appropriate disposal of used sharps (insulinneedles and lancets) reported by participants in our studywas a major concern although the extent to which itrepresents a health risk to other people is not known MostVictorian municipal councils have sharps disposal schemesin place and sharps disposal is a standard part of bloodglucose testing and insulin therapy teaching This findingcould not be explained but highlights the need to find otherways to ensure patients are aware of their responsibilities todispose of used sharps appropriately
Quality use of medicines (QUM) is central to AustraliarsquosNational Medicines Policy (NPS) The NPS aims to meetmedication-related service needs so that optimal healthoutcomes and cost-effective medication use is achievedThere are four main inter-related objectives of QUMselecting management options wisely choosing suitablemedicines if a medicine is necessary and using medicinessafely and effectively Although individuals were using alarge number of medications they appeared to be necessaryHowever individuals were not always using themappropriately and based on their responses were notadequately informed about appropriate use Likewise it is notpossible for individuals to achieve QUM if they cannotafford medicines and this was an issue for many individualsin our study
LIMITATIONS OF THE STUDYThe results of this study may not be able to be generalised
outside the study participants because of the small samplesize and the possibility of selection bias No information isavailable about patients who do not attend regularly fordiabetes or medicine review or who are managed in otherdiabetes services Nevertheless the researchers identifiedmajor concerns about medication knowledge and self-management by people with type 2 diabetes who regularlyattend the diabetes outpatient clinic
CONCLUSIONS AND IMPLICATIONS FORNURSING PRACTICE
Some inappropriate medication self-care practices andknowledge deficiencies were identified in the study Themajority of participants had received some medicineseducation but only a minority had received all sevenpossible items of information
The results support the need to ensure medicinesknowledge and use is part of routine diabetes educationpractice especially at regular complication reviews and whenmedicines or doses are changed CMI could be used as partof the medicines education process
Asking about complementary and self-initiated medicineuse should be standard nursing practice
Further research to determine which CMIs are mostuseful to people with diabetes and how to incorporate QUMstrategies into diabetes education and management iswarranted
REFERENCESCoscelli C Calabrese G Fedele D Pisu E Calderini C Bistoni S LapollaA Maur M Rossi A and Zapella A 1992 Use of premixed insulin among theelderly Reduction of errors in patient preparation of mixtures Diabetes Care15(11)1628-1630
DeBrew K Barba B and Tesh S 1998 Assessing medication knowledge andpractices of older adults Home Healthcare Nurse 16(10)688-691
Diabetes Control and Complications Trial Research Group (DCCT) 1993 Theeffect of intensive treatment of diabetes on the progression of long termcomplications of insulin dependent diabetes New England Journal of Medicine329977-986
Dunning T 2003 Complementary therapies and diabetes ComplementaryTherapies in Nursing and Midwifery 9(2)74-78
Dunning T 1994 How serious is diabetes Perceptions of patients and healthprofessionals Unpublished doctoral thesis Melbourne Deakin University
Dunstan D Zimmet P Welborn T Sicree R Armstrong T and Atkins RDiabesity and Associated Disorders in Australia - 2000 The AcceleratingEpidemic The Australian Diabetes Obesity and Lifestyle Study (AusDiab) 2001Melbourne The International Diabetes Institute
Egede L Xiaobou Y Zheng D and Silverstein M 2002 The prevalence andpattern of complementary and alternative medicine use in individuals withdiabetes Diabetes Care 25324-329
Evans J Donnan P and Morris A 2002 Adherence to oral hypoglycaemicagents prior to insulin therapy in type 2 diabetes Diabetic Medicine 19(8)685-688
Germer S Campbell I Smith A Sutherland I and Jones I 1986 Do diabeticsremember all they have been taught A survey of knowledge of insulin dependentdiabetes Diabetic Medicine 3(4)343-345
Gilbert A Roughead L and Sanson L 2002 Irsquove missed a dose What should Ido Australian Prescriber 25(1)16-18
RESEARCH PAPER
Australian Journal of Advanced Nursing 2005 Volume 23 Number 11414
Griffiths D Hunt S Napthine R and Birch M 2000 Quality use of medicinesand undergraduate nursing education Canberra Report to Pharmaceutic Healthand Rational Use of Medicines Committee
Haynes R McKibbon A and Kanani R 1996 Systematic review of randomisedtrials of interventions to assist patients to follow prescriptions for medicationsLancet 348383-386
Jones H Edwards L Vallis T Ruggiero L Rossi S Rossi J Greene GProchaska J and Zinman B 2003 Changes in diabetes self-care behaviours makea difference in glycemic control Diabetes Care 26(3)732-737
Kriev B Parker R Grayson D and Byrd G 1999 Effect of diabetes educationon glucose control Journal Louisiana State Medical Society 151(2)86-92
Lustman P 1995 International Conference Report of 55th annual meeting of theAmerican Diabetes Association Behaviouralpsychological aspects of diabetesPractical Diabetes 192
Matsuyama J Mason B and Jue S 1993 Pharmacy interventions using anelectronic med-event monitoring device Adherence data versus pill count Annalsof Pharmacology 27(7-8)851-855
Morse J 1994 Emerging from the data The cognitive process of analysis inqualitative inquiry in Morse J (ed) Critical Issues in Qualitative ResearchMethods Newbury Park Sage 23-43
Olefsky J 1999 Insulin resistance and pathogenesis of non-insulin dependentdiabetes mellitus Cellular and molecular mechanisms In Efendic S Ostenson
C and Vranic M (eds) Concepts in the Pathogenesis of NIDDM New YorkPlenum Publishing Corporation
Paes A Bakker A and Soe-Agnie C 1997 Impact of dose frequency on patientcompliance Diabetes Care 20(10)1512-1517
Royal Pharmaceutical Society of Great Britain 1997 From compliance toconcordance Achieving goals in medicine taking London Royal PharmaceuticalSociety
Sless D and Wiseman R 1997 Writing about medicines for people Usabilityguidelines for consumer medicine information Canberra CommunicationResearch Institute of Australia
Spector S 2000 Compliance with asthma therapy Are there solutions Journal ofAsthma 37(5)381-388
Stradberg L 1984 Drugs as a reason for nursing home admission JournalAmerican Health Care Association 10(20)20-22
Tay M Messersmith R and Large D 2001 What do people on insulin therapyremember about safety advice Journal of Diabetes Nursing 5(6)188-191
Tokarski C 2004 Older patients cut down on medications due to costs DiabetesCare 27(2)384-389
United Kingdom Prospective Study (UKPDS 33 34) 1998 Intensive bloodglucose control Lancet 352837-853 854-865
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
15
Ritin Fernandez RN MN (CritCare) Deputy Director SouthWestern Sydney Centre for Applied Nursing Research AdjunctResearch Fellow School of Nursing Family and CommunityHealth University of Western Sydney New South Wales Australia
ritinfernandezswsahsnswgovau
Rhonda Griffiths MSc (Hons) DrPH Research ProfessorSchool of Nursing Family and Community Health University ofWestern Sydney Director South Western Sydney Centre forApplied Nursing Research Director New South Wales Centrefor Evidence Based Health Care New South Wales Australia
Accepted for publication November 2004
ACKNOWLEDGEMENTSWe thank all the patients who participated in this trial and the nursing andmedical staff at the participating hospital for their support of the project Thanksalso to Megan Stephens for assistance with data collection Margaret Piper andPenny Murie for assistance with recruitment and Rachel Langdon for statisticaladvice and assistance
A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARDPROTOCOL FOR MONITORING POSTOPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
Key words postoperative post surgery monitoring vital signs observations
ABSTRACT
BackgroundMonitoring patientsrsquo vital signs is an important
component of postoperative observations
ObjectiveTo compare the safety and efficacy of the current
standard practice for monitoring postoperativeobservations in one hospital with an experimentalprotocol
MethodPatients who were classified as American Society of
Anaesthesiologists (ASA) Class 1 or 2 and who met theinclusion criteria were randomised to one of twogroups Following their return to the ward from therecovery unit these patients were monitored accordingto either the standard practice (n=96) or theexperimental protocol (n=93) Data collected includedpatient demographics medical and surgical historythe postoperative observations and the number andtype of untoward events
ResultsThe findings indicated that there was no
statistically significant difference in the incidence ofabnormal vital signs between the groups in the firstfour hours as well as within the 24 hours followingreturn to the ward from the recovery unitAdditionally none of the patients required eithertransfer to the intensive care unit high dependencyunit or management by the intensive care teamPatients in both groups were successfully dischargedwithin 24 hours following surgery
ConclusionThis study provides evidence to inform clinicians of
a safe and cost effective regime in the management ofthe patient in the postoperative period followingdischarge from the recovery to the ward Clinicianshowever must utilise clinical judgement to determinewhich patients require close monitoring during thepostoperative period
INTRODUCTION
Monitoring of patientsrsquo vital signs is an importantcomponent of postoperative observationsundertaken for the early detection of
complications that may require an intervention thuspreventing further clinical deterioration (Botti and Hunt1994) Research has demonstrated that 5 of patientsdevelop postoperative complications (Gamil and Fanning1991) 021 of patients developed an early postoperativeemergency within 48 hours after surgery (Lee et al 1998)and the incidence of mortality is 024 in the first 24hours following surgery (Gamil and Fanning 1991)
A large number of studies have been published whichprovide recommendations specifically for monitoringpatients in the recovery room however there has beenlimited research relating to management of patientsfollowing their transfer to the ward
The commonly monitored vital signs includetemperature pulse respiration and blood pressure (Evanset al 1999) Nurses usually assess these vital signs inaccordance with the individual hospital protocols (Botti and Hunt 1994) although the rationale for theseprotocols are rarely based on scientific evidence(Arsenault 1998 Burroughs and Hoffbrand 1990)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
16
Policies and protocols for monitoring patientsfollowing return to the ward varies between facilities aswell as between wards within each facility For examplehalf hourly monitoring for two hours hourly monitoringfor four hours and hourly monitoring for six hours havebeen reported (Zeitz and McCutcheon 2002)
Findings from a systematic review of the literature(Centre for Applied Nursing Research 1998) investigatingthe optimal frequency for monitoring patients on return tothe ward recommended that vital signs should bemonitored half hourly for two hours followed by fourthhourly for 24 hours if the patients were stable Howeverthe systematic review did not include recommendationsfor the type of observations therefore a further review ofthe literature was undertaken to identify the commoncomplications occurring in the first three postoperativedays and the associated vital signs to be monitored
The findings from this literature review identifiedhypotension as a common complication occurring withinthe first three hours after surgery (Gamil and Fanning1991) therefore the value of blood pressure monitoringwas confirmed Likewise the recording of pulse rate wasjustified because bradycardia has been reported as thesecond most common complication occurring within the first two hours after surgery (Field 1998) Theliterature also indicated that monitoring the temperaturein the first four hours has been frequently recorded todetect hyperthermia which is primarily an indicator ofinfection (Litwack 1997 Wipke-Tevis 1999) DVTpulmonary emboli atelectasis (Pett and Wernly 1988) and anastomotic breakdown Researchers have alsodemonstrated that these complications are uncommon inthe first few hours following surgery and are more likelyto occur from the second postoperative day (Heidenreichand Giuffre 1990)
The importance of monitoring the respiratory rate was debatable as adequate breathing did not necessarilyindicate optimal ventilation (Thompson 1983) Rathermonitoring oxygen saturation levels has beendemonstrated to be an important predictor of the patientrsquosrespiratory status (Moller et al 1992 Moller et al 1993Rosenberg et al 1989) With the availability of bedsidetechnology (pulse oximetry) to record the patientrsquosoxygen saturation monitoring the physiological results of respiration rather the respiratory rate is a much more appropriate indicator of respiratory status (Bayne1997)
Based on the findings of the systematic review and acomprehensive literature review of the commonlyoccurring complications in the early postoperative period and in consultation with expert clinicians anevidence based postoperative monitoring regime wasdeveloped The objective of this study was to investigatethe safety and efficacy of the evidence based regime for monitoring postoperative observations with theexisting standard practice
RESEARCH QUESTIONWhat is the effect of a modified regime compared to
existing practices for monitoring vital signs inpostoperative patients on their return to the ward from therecovery unit
MATERIALS AND METHODS A randomised controlled trial was undertaken
comparing the incidence and nature of untoward eventsthat occurred in the first 24 hours following return to theward after surgery in patients monitored according to thestudy protocol and those monitored according to thestandard hospital protocol This study design was chosendue to the ability of randomised controlled trials toeliminate selection bias thus making them the bestmethod to obtain evidence on the effects of health careinterventions
The study was conducted in a metropolitan healthservice in New South Wales Australia over sixconsecutive months As such a study had not beenpreviously undertaken it was determined that onlypatients classified by the American Society ofAnaesthesiologists (ASA) as Class 1 or 2 would beincluded The ASA Classification status (table 1) wasused as an estimate of operative risk (Wolters et al 1996)
Table 1 ASA Classification
ASA I The patient has no organic physiological biochemical or psychiatric disturbance The pathological process for which the operation is to be performed is localised and is not a systemic disturbance
ASA II Mild to moderate systemic disturbance caused either by the condition to be treated or by other pathophysiologic processes
ASAIII Severe systemic disturbance or disease from whatever cause even though it may not be possible to define the degree of disability
ASA IV Indicative of the patient with severe systemic disorder already life-threatening not always correctable by the operative procedure
ASA V The moribund patient who has little chance of survival but is submitted to operation in desperation
Patients having surgery under general anaesthesia wereidentified on admission to the peri-operative unit andassessed by the departmental staff to determine theireligibility for entry into the study Patients were eligiblefor the study if they were scheduled for surgery undergeneral anaesthesia between the ages of 18-80 yearstransferred to the ward from recovery and had aminimum length of stay of six hours following surgery
Patients who failed to give consent had surgery underspinal or local anaesthesia patient controlled anaesthesiafollowing surgery neurosurgery vascular surgery or weretransferred to the intensive care (ICU) or high
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
17
dependency units (HDU) from the recovery unit wereexcluded from the study The surgeons and anaesthetistsreviewed the experimental protocol and consented to havetheir patients participate in the study The study wasapproved by the South Western Sydney Area HealthService Research Ethics Committee and the University ofWestern Sydney Ethics Review Committee (HumanSubjects)
An intensive education program for staff in thesurgical wards was undertaken to provide details of thestudy procedures to be followed and the documentationto be completed for each client enrolled in the study
At the time of admission to the peri-operative unitpatients who met the inclusion criteria were informed ofthe study and written consent was obtained prior toallocation to a study group The randomisation sequencewas generated from a statistical table of random numbersand concealed in sequentially numbered opaque sealedenvelopes Following their return to the recovery unit aftersurgery envelopes containing the monitoring regime wereplaced by the nurse in charge in front of the patientsrsquomedical notes On transfer to the ward the envelopecontaining the protocol was located the random numberrecorded on the data sheet and the patient was monitoredaccording to the assigned protocol Nurses wereinstructed that in the event that a patient became unwelland required further monitoring the patient was to bediscontinued from the study and treatment commencedaccording to medicalnursing advice
Patients in the control group had their observationsmonitored according to the standard hospital protocol(table 2) while those in the experimental group had theirobservations monitored according the study protocol(table 3) Owing to the nature of the intervention it wasnot possible to blind the participants nurses or the datacollectors to the treatment allocation However in order tomaintain the rigour of the study and to avoid bias duringdocumentation the nurses and the data collectors werenot informed of the criteria used to describe abnormalvital signs
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate bloodpressure oxygen saturation and level of arousal to berecorded on return to the ward followed by fourth hourlyfor 24 hours if the patient is stable
Temperature to be recorded on return to the ward thenat the end of four hours followed by daily until dischargeif the patient is stable Respiratory rate pulse rate andblood pressure to be monitored and recorded on return tothe ward then one hourly for two hours followed by fourthhourly for 24 hours Oxygen saturation and level ofarousal to be monitored and recorded on return to the
ward then one hourly for two hours followed by fourhourly for 24 hours
Data collection was undertaken by an independent staffmember not associated with the research projectStandardised data collection was undertaken using a tooldeveloped by the researchers The data collector wasprovided with extensive education regarding transcriptionof the data and the data collection method Data collectedincluded the patientrsquos age gender date of admissionsurgery and discharge name of the surgical proceduremedical history ASA class duration of anaesthesiaduration of the procedure length of time in recovery theobservations recorded and any variations in the conditionof the patient during the first 24 hours following surgeryRandom audits by the researchers were conducted toensure accuracy of the data collected
Adverse outcomes of interest included the number ofpatients who developed any untoward events such as chestpain required management by an intensive care teamwere transferred to the ICUHDU for intense monitoringor had an abnormal vital sign An abnormal vital sign wasdefined as a value outside the predetermined parameters(Davis and Nomura 1990) (table 4)
Table 4 Definitions and parameters of abnormal vital signs for the purpose of this study
Fever Temperature of 383ordm or higher
Hypoventilation Respiratory rate of 10min or less
Hyperventilation Respiratory rate of 30 or more
Hypotension Fall in blood pressure (BP) gt20mm of Hg from baseline BP or systolic BP lt80mm of Hg
Hypertension Systolic BP gt180mm Hg and diastolic BP gt 120mm of Hg a rise in BP of 20 or more than the highest preoperative BP
Bradycardia Pulse lt60minSeverity classified B1 ndash50 ndash60minB2 lt50min
Tachycardia Pulse gt100minSeverity classified T1 100 ndash120minT2 gt120min
Hypoxia 02 saturation 90 or less
Statistical analysis Statistical analysis was carried out using SPSS version
10 Descriptive statistics were calculated for all variablesChi-square analysis was undertaken to determine thedifferences between the two groups All patients whowere monitored could potentially have up to five vitalsigns outside normal limits Therefore the analysis wasperformed on the number of occurrences of abnormalvital signs rather than the number of patients Forexample patients in the experimental group had two sets
Table 2 Standard protocol (control)
Table 3 Experimental protocol
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
18
of observations recorded in the first four hours followingtransfer to the ward
Therefore the total number of potential abnormal vitalsigns for this group of patients (n=93) would be 930 if allparameters ie temperature pulse respiratory rate bloodpressure and oxygen saturation were monitored at bothtimes As more frequent monitoring can result in anincrease in the detection of abnormal vital signs theproportion of the abnormal vital signs in each group wascalculated
RESULTS Two hundred and twenty seven patients who met the
inclusion criteria were randomised to either groupHowever 38 patients were subsequently excluded as theywere administered either spinal or local anaesthesia forthe surgical procedure or were commenced on PCAfollowing surgery These results are therefore based on ananalysis of 189 patients (experimental=93 control=96)Forty-two of these patients were not monitored accordingto the assigned protocol however their data have beenincluded in an intention to treat analysis (table 5)
There were no significant differences between theexperimental and control groups in any of the baselinecharacteristics (table 6) nor were there any statisticallysignificant differences in the observations recorded atadmission or in the recovery unit (table 7)
The majority of patients had a general surgicalprocedure (n=151) whilst the other operations involvedthe head and neck (including faciomaxillary) (n=3) earnose and throat (n=1) orthopaedics (n=8) gynaecology(n=14) urology (n=10) breast (n=1) and plastic surgery(n=1) (table 6)
Incidence of adverse outcomesDuring their period of hospitalisation none of the
patients in either group developed a postoperativeemergency that required management and treatment by anintensive care team or transfer to the ICUHDU
Two patients in the experimental group complained ofchest pain The first patient a 29 year old complained ofchest pain seven hours after transfer and was treated withintravenous Ranitidine The second patient a 36 year oldhad chest pain 15 hours after transfer was treated withsublingual nitrates and cardiac investigations wereundertaken The chest pain resolved within the hour inboth patients and they were discharged home thefollowing day
Five hours after returning to the ward one patient in thecontrol group tried to sit out of bed and fell Vital signsrecorded at the time of the fall were stable and the patientexhibited no signs or symptoms of complicationsalthough the patient was asked to remain in bed for afurther two hours and was discharged home the next day
Incidence of abnormal vital signsThe number of abnormal vital signs that were
documented has been reported in table 8 Ten patients inthe experimental group and five patients in the controlgroup had a pulse rate of less than 60 beatsminute atbaseline When these patientsrsquo data were removed fromthe analysis there was no statistically significantdifference in the number of abnormal vital signs at anypoint in the first 24 hour period Therefore the data fromthese patients were included in the final analysis
Although monitoring the respiratory rate and oxygensaturation was a requirement of the protocol these vitalsigns were monitored in less than 70 of all patientsAbnormal events relating to these vital signs havetherefore not been included in the final analysis In thosepatients who did have this vital observation monitorednone had tachypnoea or bradypnoea in the 24 hour periodand only one patient had an abnormal oxygen saturation(89) on transfer to the ward It could be postulated thatthe low level of oxygen could be due to the fact that thispatient had a diagnosis of pulmonary embolism and wastransferred to the ward without oxygen therapy Treatmentwith oxygen supplementation for one hour resulted in thepatient attaining normal oxygen saturation
Table 5 Flow chart of patients through the study
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
19
Incidence of abnormal vital signs on transfer to the ward
On their return to the ward from the recovery unit allpatients had their temperature pulse and blood pressuremonitored However the respiratory rate was monitoredin only 28 and oxygen saturation was monitored in only77 of patients therefore these parameters were notconsidered in the analysis Twenty-one patients in theexperimental group and 17 patients in the control grouphad one untoward event each however these results werenot statistically significant (p=044) (OR 130 95 CI067 251) (table 8) The most commonly occurringuntoward events were bradycardia (n=18 31) followedby hypotension (n=11 2)
Incidence of abnormal vital signs in the first fourhours following transfer to the ward
In the first four hours after returning to the ward fromthe recovery unit patients in the experimental group hadtwo sets of vital signs and those in the control group hadonly one set of vital signs recorded (these do not includethe vital signs recorded at transfer) Therefore thenumber of potential untoward events that could occur inthe experimental group and control group was 558 and288 respectively
A total of 33 untoward events (experimental=21control=12) were identified in 30 patients(experimental=18 control=12) These results were notstatistically significant (p=077) (OR 090 95 CI 044186) (table 8) Hypotension (n=12) (15) andbradycardia (n=11) (14) were the most commonlyoccurring untoward event during this period
In the 12 patients who developed hypotension and 11 patients who developed bradycardia six had a lowblood pressure and three had a low pulse rate at baseline
Hyperthermia was recorded in one patient in the control group
Incidence of abnormal vital signs in the first 24 hoursfollowing transfer to the ward after surgery
In the 24 hours following transfer to the ward patientsin the experimental group (n=93) had seven and those inthe control group (n=96) had six sets of observationsrecorded Again these do not include the vital signsrecorded at transfer Therefore the number of potentialabnormal vital signs that could occur in the experimentalgroup and control group were 1953 and 1728 respectively
One hundred and fourteen abnormal vital signs(experimental=52 control=62) were identified in 65patients (experimental=33 control=32) in the first 24hour period following transfer to the ward from therecovery unit (p=011) (OR 074 95 CI 51 107) (table8) These abnormal vital signs occurred at any timeduring the 24 hour postoperative period and notnecessarily in the first four hours
Hypotension (n=32) (09) and bradycardia (n=46)(12) were the most common untoward eventsdocumented (table 8) In the 20 patients who developedhypotension and 23 patients who developed bradycardia14 had a low blood pressure and five had a low pulse rateat baseline Severe bradycardia (HR lt50 beatsminute)was not identified in any of the patients in the first 24hours following surgery None of the patients who had anabnormal blood pressure or pulse complained ofdizziness nausea or weakness
All patients who developed untoward events weremanaged with appropriate nursing interventions and theattending doctor was notified of the changes in vitalsigns Assistance from the doctor was required in onlythree patients two who developed chest pain and one whohad a fall
Table 6 Patient demographics
Experimental Control group group
Total number of patients analysed 93 96Males 44 41Female 49 55Age 5398 (SD 1753)Range 20-85 years 4823 (SD 1645)Range 19-81 years
Types of surgery
General surgery 74 77Head and neck including faciomaxillary 1 2Ear nose and throat 1Breast 1Orthopaedics 3 5Gynaecology 8 6Urology 5 5Plastic 0 1
Table 7 Demographics
Experimental group Control group Mean (Std deviation) Mean (Std deviation)
Length of hospital stay 2 days (133) 18 days (136)
Length of stay after surgery 192 days (134) 18 days (16 )
Length of anaesthesia 83 minutes (37) 82 minutes (30)
Length of surgery 63 minutes (33) 66 minutes (70)
Length of time in recovery 87 minutes (475) 84 minutes (43)
Systolic blood pressure at baseline 137 (27) 1348 ( 222)
Diastolic blood pressure at baseline 794 (117) 797 (133)
Pulse rate at baseline 72 (11) 737 (11)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
20
Table 8 Incidence of abnormal vital signsTime Vital sign Experimental group Control group p value Odds ratio (95 CI)
No of abnormal vital signs () No of abnormal vital signs ()Transfer Temperature gt38 0 0
Bradycardia 13 5Tachycardia 2 3Hypotension 6 5Hypertension 0 4Total 21 (75) 17 (6) 044 130 (067 251)
4 hours Temperature gt38 2 1Bradycardia 8 3Tachycardia 4 2Hypotension 7 5Hypertension 0 0Total 21 (38) 12 (41) 077 090 (044 186)
24 hours Temperature gt38 6 7Bradycardia 24 22Tachycardia 8 5Hypotension 10 22Hypertension 4 6Total 52 (27) 62 (36) 011 074 (051 107)
DISCUSSION Various regimes for monitoring vital signs in the
postoperative period have been used although there islimited documentation of research relating to thispractice This randomised controlled trial was undertakento compare the safety and efficacy of a modified protocolto the usual hospital protocol for monitoring patients ontheir return to the ward from the recovery unit Theexperimental protocol was developed from the findings ofa systematic review literature review of commonlyoccurring complications in the first 24 hours followingsurgery and expert advice
The major difference between the two monitoringregimes was the number of times the patients weremonitored in the first four hours following return to theward from the recovery unit Although all patients weremonitored on transfer patients in the experimental groupwere monitored for a further two hours while patients inthe control group were monitored only once again in thefollowing four hours The main outcome of interest wasthe number of patients who required assistance of theintensive care team or transfer to the intensive care unitOther outcomes assessed included the number of patientswho developed abnormal vital signs or had any adversecomplications eg haemorrhage
Patients frequently exhibit abnormal vital signs duringrecovery from general anaesthesia and in only a minorityof cases does this progress and require interventionTherefore statistical analysis was undertaken on thenumber of abnormal vital signs documented in eachgroup rather than the number of patients who developedthe abnormal vital signs
The incidence of abnormal vital signs in the first 24hours following return to the ward from the recovery unitwas 3 Although not statistically significant a greaternumber of abnormal vital signs (n=21) were identified inthe experimental group compared to the control group
(n=12) in the first four hours This could be due to thefact that patients in the experimental group weremonitored more frequently than those in the controlgroup thus increasing the likelihood of detection ofabnormal vital signs
This study supports the findings of other researchers(Harley and Tsamassiros 1997) that following return tothe ward from the recovery unit if abnormal vital signshave not occurred in the first two and a half hours it isunlikely they will occur within the first four hours Theresults also demonstrated no statistically significantdifference in the incidence of abnormal vital signs in thefirst 24 hours thus supporting the feasibility and safety ofreduced frequency of monitoring vital signs following apatientrsquos return to the ward from the recovery unit
In this study the incidence of abnormal vital signs maybe underestimated due to poor compliance by nurses tothe monitoring schedules Although the monitoringregimes for both the experimental and control groupsincluded monitoring of the oxygen saturation it wasinteresting to note that this observation was monitored inless than 80 of all patients One would assume that thepatients who did not have their oxygen saturationmonitored would have their respiratory rate monitoredHowever this was not the case as there were patients whohad neither observation recorded
In this study bradycardia and hypotension were themost commonly occurring abnormal vital signs in thefirst 24 hours which supports the findings of otherresearchers However it should be noted that for thepurpose of this study bradycardia was defined as a pulserate of less than 60 beatsminute The majority of thepatients who had bradycardia postoperatively also had abaseline pulse rate of under 60 beatsminute
The majority (78) of abnormal vital signs occurredafter the first four hours indicating that all patientsfollowing surgery are at risk hence pertinent observations
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
21
are critical and nursing staff should be vigilant ascomplications can occur at any point along thepostoperative continuum
None of the patients in either group demonstrated anyserious or potentially life threatening events afterreturning to the ward In the three patients who developeduntoward events there was no association between thetime of occurrence of the abnormal vital sign and thetime since return to the ward
These results indicate that there is no associationbetween the frequency of observations in the first fourhours and outcomes for the type of patients included inthis study However as no adverse events were reported itis unclear whether monitoring the patient frequently in thefirst four hours assists in the early identification ofpatients at risk of postoperative complications
The results from this study have implications forclinicians and administrators and provide a platform forthe rational use of services aimed at optimising patientcare post surgery The regimes for postoperativemonitoring should be based upon the condition of thepatients the nursersquos clinical judgement and withconsideration of existing guidelines within the facilityMonitoring regimes should include appropriate vital signsto identify the complications that have been commonlyreported to occur following surgery Diligent visualobservation and communication with the patient is alsoimportant as part of the patientrsquos postoperative care
Monitoring appropriate vital signs based on clinicaljudgement will provide nursing staff with valuable timeand added flexibility to prioritise other nursinginterventions As the nursesrsquo role expands to include moreassessments planning teaching and evaluation it isimperative that clinical practice is based on evidencerather than tradition This research study reports on oneclinical practice that can be changed to achieve that goal
A major limitation of the study is the sample sizetherefore the findings of this study cannot be generalisedbeyond the population and setting where this study wasconducted Potential confounders of early postoperativeuntoward events include the type of surgery type ofanaesthesia and ASA classification of the patientsHowever as all the patients in the study had generalanaesthesia and were classified as ASA class 1 or 2 andmost of them had general surgery it can be concluded thatthe findings are only applicable to this population andcannot be generalised to other types of patients
Replication of this study in other settings with patientsclassified as ASA 3 and with other surgical procedureswill provide an evidence-based protocol for monitoringpatients in the postoperative unit
CONCLUSIONThe research including this study demonstrates that
current regimens for monitoring patients in the immediate
postoperative period may in fact be more intensive than isindicated by patient outcomes The data presented fails toprovide justification for routine frequent monitoring ofvital signs in the postoperative period following return tothe ward from the recovery unit However the resultscannot be generalised to all patients following surgeryClinicians however must utilise clinical judgement todetermine which patients require close monitoring duringthe postoperative period Further research needs to beundertaken to assess patient satisfaction with reducedmonitoring
REFERENCES Arsenault C 1998 Nursesrsquo guide to general anaesthesia part 2 Nursing 9828(5)32cc1-32cc5
Bayne CG 1997 Vital signs Are we monitoring the right parametersNursing Management 28(5)74-6
Botti M and Hunt J 1994 The routine of post anaesthetic observationsContemporary Nurse 3(2)52-57
Burroughs J and Hoffbrand BI 1990 A critical look at nursing observationsPostgraduate Medical Journal 66(779)370-2
Centre for Applied Nursing Research 1998 Postoperative observations Asystematic review Joanna Briggs Institute for Evidence Based Nursing andMidwifery Adelaide
Davis MJ and Nomura LA 1990 Vital signs of class 1 surgical patientsWestern Journal of Nursing Research 12(1)28-41
Evans D Hodgkinson B and Berry J 1999 Vital signs A systematic reviewThe Joanna Briggs Institute for Evidence Based Nursing and MidwiferyAdelaide
Field D 1998 Assessment of haemostasis Nursing Times 94(29)54-6
Gamil M and Fanning A 1991 The first 24 hours after surgery A study ofcomplications after 2153 consecutive operations Anaesthesia 46(9)712-5
Harley J and Tsamassiros J 1997 A pilot study analysing the occurrence andfrequency of reoccurring vital signs outside of normal parameters and otherabnormal symptoms exhibited in the postoperative phase of short term surgicalpatients Unpublished
Heidenreich T and Giuffre M 1990 Postoperative temperature measurementNursing Research 39(3)153-5
Lee A Lum ME OrsquoRegan WJ and Hillman KM 1998 Earlypostoperative emergencies requiring an intensive care team intervention Therole of ASA physical status and after-hours surgery Anaesthesia 53(6)529-35
Litwack K 1997 Practical points in the evaluation postoperative fever Journalof Perianesthesia Nursing 12(2)100-4
Moller JT Jensen PF Johannessen NW and Espersen K 1992Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatreand in the recovery room British Journal of Anaesthesia 68(2)146-50
Moller JT Johannessen NW Espersen K Ravlo O Pedersen BDJensen PF Rasmussen NH Rasmussen LS Pedersen T Cooper JB et al1993 Randomized evaluation of pulse oximetry in 20802 patientsPerioperative events and postoperative complications Anesthesiology78(3)445-53
Pett SB Jr and Wernly JA 1988 Respiratory function in surgical patientsPerioperative evaluation and management Surgical Annuals 20311-29
Rosenberg J Dirkes WE and Kehlet H 1989 Episodic arterial oxygendesaturation and heart rate variations following major abdominal surgeryBritish Journal of Anaesthesia 63(6)651-4
Thompson P 1983 Postoperative respiratory distress Life or death Journal ofPractical Nursing 33(9)19-22
Wipke-Tevis DD 1999 Vascular infections Medical and surgical therapiesJournal of Cardiovascular Nursing 13(2)70-81
Wolters U Wolf T Stutzer H and Schroder T 1996 ASA classification andperioperative variables as predictors of postoperative outcome British Journalof Anaesthesia 77(2)217-222
Zeitz K and McCutcheon H 2002 Policies that drive the nursing practice ofpostoperative observations International Journal of Nursing Studies39(8)831-839
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
22
ABSTRACT
ObjectivesTo assess health outcomes of home follow-up visits
after postpartum discharge and assess relationshipsbetween the number of home visits and selectedoutcomes among women who gave birth at twoQueensland Australia regional hospitals
DesignA cross sectional study Services provided during
the home visits were responsive to a womanrsquos needrather than having a structured protocol of services
Main Outcome Measures
The four measured health outcomes were 1)postpartum depression 2) confidence to undertakematernal roles 3) breastfeeding and 4) satisfactionwith postpartum care
ResultsOf 210 women who were invited to participate in
the study 143 (681) provided information Womenwho received a higher number of home visits hadsignificantly lower confidence to undertake maternalroles than those who received fewer home visits Therewas a positive correlation between the number ofhome follow-up visits and postpartum depressionamong women who gave birth at one hospital(Hospital B) but not at the other (Hospital A) Norelationship was found between the home postpartumvisits and the other outcomes
Conclusion
These results could be explained in that homefollow-up visits were offered to all women at HospitalA while Hospital B only provided home visits towomen who had a health risk due to their socialphysical and psychological characteristics The lack ofprotocol home visits and the characteristics of womenreceiving the visits were probably the major factorswhich influenced these limited beneficial outcomes
INTRODUCTION
In the past two decades many researchers (Ransjo-Arvidson et al 1998 Fraser et al 2000 Lieu et al2000) have assessed the outcomes of home follow-up
visits after postpartum discharge as hospitals havereduced the hospital stay of postpartum women after thebirth of their infants
Health outcomes of postpartum women and theirinfants who were discharged early and received homefollow-up visits were compared with women who had alonger hospital stay (Armstrong et al 1999 Kendrick et al2000) A wide range of outcomes have been measuredincluding maternal depression and satisfaction with careand hospital readmissions (Lieu et al 2000)
The results of these studies recommended theprovision of home visits to postpartum womenparticularly first time mothers single mothers andmothers who intend to breastfeed their infants Anothercommon and consistent outcome derived from thesestudies was that mothers who received home visits were
Sansnee Jirojwong PhD Senior Lecturer School of Nursingand Health Studies Central Queensland UniversityRockhampton Queensland AustraliasjirojwongcqueduauDolene Rossi MSc Lecturer School of Nursing and HealthStudies Central Queensland University RockhamptonQueensland Australia
Sandra Walker PhD Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
Barbara Ritchie MEdSt Senior Lecturer School of Nursing andHealth Studies Central Queensland University RockhamptonQueensland Australia
ACKNOWLEDGEMENTSCentral Queensland University provided research grants and the School ofNursing and Health Studies facilitated the completion of the study EmeritusProfessor Robert MacLennan provided significant comments throughout thestudy process We would also like to acknowledge assistance from thefollowing persons Russell E Weber N Oberhofer A Alick C Bradley DMr and Mrs Byrne Gall M Metcalfe A Nelsen S Rutherford C Stubbs Tand Tansley K
Accepted for publication December 2004
WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTERPOSTPARTUM HOSPITAL DISCHARGE
Key words postpartum home visit regional Australia health outcome rural
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
23
more likely to be satisfied with the postpartum care or tobe more confident to seek help from health care providersthan women who did not receive this care (De Koninck etal 2001)
The major approach relating to home visits afterpostpartum hospital discharge was having systematic andwell planned protocols in order to achieve specific healthoutcomes For example Barros (1994) and Brent (1995)developed a protocol of services during home visits topostpartum women in order to increase their exclusivebreastfeeding (see also Sikorski et al 2004) Suchevidence-based practices were strongly recommended byhealth policy makers as they demonstrated outcomesbased on a structured protocol of health services andsystematic investigations However the adoption of theseprotocols was limited due to a range of administrative andpractical factors
Other factors included lack of understanding of nursesand midwives relating to the process used to develop theprotocols of the best practices or their inability to obtainsuch protocols (Hay et al 1999) Results of the study byHay et al (1999) suggested that at relatively smallhospitals health issues need to be prioritised so thatappropriate protocols to deliver evidence-based practicescould be developed to address such issues
In September 2004 data based on six Queenslandregional hospitals gathered by the researchers of thisstudy showed there were three major patterns of homevisits provided to women after hospital postpartumdischarge
The first pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge There were objectivesfor the visits with a clear protocol for the visits
The second pattern was that nurses or midwives visitedall women who lived within a designated area at theirhomes after the hospital discharge No structured protocolwas written for the visits Referral of women who livedoutside of the boundary to other health centers might be made
The third pattern was that women who had specialneeds due to physical psychological or social problemswould receive home visits provided by nurses ormidwives after hospital discharge
The pattern of home visits adopted by healthorganisations varied from one to another relating to thenumber of visits time of initial and subsequent visits afterhospital discharge and the range of protocols for servicesIf required women or their infants were referred to otherhealth professionals such as social workers generalpractitioners or paediatricians for appropriate care Ingeneral care provided by nurses or midwives during thesehome visits aimed to prevent and detect complicationsamong the women and their infants Grullon and Grimes(1997) and Lieu et al (2000) who reviewed services
provided in many countries including the UnitedKingdom and the United States suggested these includedphysical psychological and social assessment healtheducation and anticipatory guidance
Studies in the United Kingdom the United States andCanada assessed the outcomes of these home follow-upvisits after postpartum discharge (Frank-Hanssen et al1999 Johnson et al 1999 Lieu et al 2000 Morrell et al2000 De Koninck et al 2001)
Comparing the results of one study with other studieswas problematic due to the difference in outcomemeasures study designs periods between hospitaldischarge and data collection protocol and content ofhome visits and types of health care providers (Frank-Hanssen et al 1999 Johnson et al 1999 Lieu et al 2000)For example Johnson et al (1999) assessed the success orcontinuation of breastfeeding while Lieu et al (2000)assessed a number of mother and infant outcomesincluding newborn re-admission newborn urgent clinicvisits maternal re-admission and maternal postpartumdepression Lieu et al (2000) used an experimental designand Frank-Hanssen et al (1999) used a cross-sectionaldescriptive design Only women who had vaginaldeliveries were included in the study by Meikle et al(1998) whereas Armstrong et al (1999) focusedspecifically on high-risk women excluding low riskwomen
In Australia all women and their infants are entitled toreceive publicly funded health care during the perinatalperiod (Australian Institute of Health and Welfare 2003)As mentioned earlier not all women received postpartumhome visits after hospital discharge The availability ofand accessibility to the home visit is influenced by manyfactors including hospital policies financial support andthe number of deliveries to justify cost-benefits Manywomen in rural or regional areas travelled long distancesto give birth in regional referral hospitals while thedistance and availability of midwives in localcommunities limited the delivery of post hospitaldischarge care No published data were available relatingto health outcomes of the unstructured post hospitaldischarge care among women in regional Australia
The major aim of this study was to assess healthoutcomes of unstructured home follow-up visits providedby midwives or nurses to women following the birth oftheir infants at two regional hospitals in QueenslandAustralia Specific objectives of this study were todescribe and compare characteristics of mothers who gavebirth at the study hospitals and to assess the relationshipbetween the number of home follow-up visits and thefollowing four outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeedingand 4) satisfaction with postpartum care The studyhospitals were specifically selected for their differentunstructured follow-up programs which reflected theactual postpartum services provided by many Australianhospitals The first hospital Hospital A had midwives
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
24
visit all women at their homes located within 15 kilometreradius while the second hospital Hospital B had selectivecriteria in the provision of services The study hospitalsand their home visit services will be briefly described inthe following section
Study hospitals and home follow-up visitsTwo major Queensland regional hospitals served the
dispersed population in more than 126000 squarekilometres (Queensland The Office of Economic andStatistical Research 2002) Some women traveled morethan 100 kilometres to use services at these hospitals
The annual number of births in each hospital wasapproximately 1000 Prior to the questionnaire design theauthors held discussions with six nurses and midwivesworking at the study hospitals and relevant healthorganisations in order to explore postpartum home visitprotocols specific services and anticipated outcomes ofhome visits provided by each study hospital
At Hospital A home visits were offered and providedto all postpartum women who lived within a 15 kilometreradius Midwives would make the initial visit within fivedays after the hospital discharge If needed subsequentvisits were also made
Women or their infants with long term health problemsor severe illness were referred to other healthprofessionals such as general practitioners communityhealth nurses social workers or paediatricians forappropriate care
Other women who lived outside the 15 kilometreradius might or might not receive home visits dependingon the policy of the womenrsquos nearest health centre AtHospital B the home visits were only provided bymidwives to women or infants with social physical orpsychological health problems These included drug usersand women in domestic violence relationships Midwivesat Hospital B would decide who would require a homevisit Both Hospital A and B did not have a formulatedprotocol of services during each visit to achieveanticipated outcomes by nurses or midwives who visitedwomen who gave birth No fixed number of visits wereprovided by visiting midwives
RESEARCH METHODPostpartum women who gave birth at the study
hospitals between August and December 2001 wereinvited to participate in the study Ethics committees ofrelevant organisations approved the study Two hundredand ten women (Hospital A = 102 Hospital B = 108)were approached and invited to participate in the studyOf these 172 (819) agreed to participate (Hospital A =76 745 Hospital B = 96 889) and later werefollowed-up by telephone interviews within four weeksafter hospital discharge These participating rates atHospitals A and B were significantly different
Reasons for non-participation were that they did notperceive the benefits of the study and they did not havetime
More than 80 of the women (143 women of 172831) were contacted after four to 10 telephone calls(average five calls) and took part in the study Eachwoman was contacted at various times of the dayincluding weekends A minimum of four telephone callswere made to each woman and up to 10 calls in totalThree research assistants who were registered nurseswere trained by the first author to conduct telephoneinterviews A manual was also developed to be used bythe research assistants and this described the purpose ofthe study and the questions included in the questionnaireA telephone interview ranged between 15 and 45 minutes(median 20 minutes)
The results of the discussions between the first authorand the nurses and the midwives and various studies were used as a guide to select outcomes of home visitsand design the questionnaire comprising open-ended andclosed-ended questions The following information was gathered from each participating womansociodemographic characteristics number of follow-uphome visits postpartum depression confidence toundertake maternal roles frequency of breastfeeding andsatisfaction with postpartum care
Information relating to obstetrics during pregnancydelivery and postpartum period of the participants wasbased on the hospital records A form was designed tocollect the recorded perinatal data of both the woman andher infant The information was transcribed by researchassistants These perinatal data included gestational agetype of delivery presentation of the infant plurality andthe presence of infant congenital anomaly at birth
Variables and their measurementsThe independent variable was home follow-up visits
measured by the womenrsquos reported number of home visitsprovided by nurses or midwives within four weeks aftertheir hospital discharge Maternal psychological healthwas assessed by using the standardised Edinburghpostpartum depression scale (Eberhard-Gran et al 2001)The possible score ranged from zero (no depression) to 30(high depression)
The studies by Ransjo-Arvidson et al (1998) Fraser etal (2000) and Kendrick et al (2000) were used as a guideto design five question items to assess confidence toundertake maternal roles This study assessed thewomanrsquos reported confidence to care for her baby relatingto bathing feeding dealing with the babyrsquos waking atnight the babyrsquos crying non-stop for more than one hourand having fever These tasks were later ranked as themost difficult (baby cried non-stop for more than onehour and having fever) and to the least difficult (bathing)by gaining the opinion of five midwives and fourpostpartum mothers The women responded by using afive point Likert scale from no confidence (one score) to
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
25
very confidence (four score) and unsure (zero score) toeach question item The possible score of the confidenceto undertake maternal roles ranged from zero (unsure) to20 (most confidence)
The studies by Jirojwong (1995) Lieu et al (2000) andDe Konick et al (2001) were used as a guide to design asingle question item to assess the womenrsquos overallsatisfaction with postpartum care Studies by Johnson etal (1999) and Sikorski et al (2003) were used to design aquestion item to assess breastfeeding by the self-reportedregularity of breastfeeding in the past seven days Theregularity of breastfeeding was used to categorise awoman into one of four groups exclusively breastfeeding(no bottle feeding) predominantly breastfeedingpredominantly bottle feeding and exclusively bottlefeeding (no breastfeeding)
A short hospital length of stay after birth was definedas postpartum hospital stay for not more than two days forwomen who had vaginal delivery and not more than fourdays for women who had caesarean delivery (Grullon andGrimes 1997)
Cronbachrsquos alpha was computed to assess internalreliability of two measurements the Edinburghpostpartum depression scale (083) and the confidence inmaternal roles (063) This internal reliability wascomputed based on the data of all 143 women in thestudy This was a satisfactory level of internal consistency(Nunnally 1978)
Descriptive and analytical data analysis methods wereused Number percentage range mean standarddeviations median and inter-quartile were used to analyseand present descriptive data In order to assess groupdifferences a chi-square test for categorical variables andthe studentrsquos t-test for continuous variables were used Asthe number of home visits was not normally distributednon-parametric methods were used to assess itsrelationship with the study outcomes The non-parametricKruskal-Wallis test was used to compare two or moregroups and the Spearman Rank correlation was used toassess a relationship between two continuous variables(Daniel 1995) The minimum statistical significance levelof 005 (p=005) was used as a criterion for rejecting anull hypothesis
RESULTS
The womenThe details of social demographic and obstetric
characteristics of the women who gave birth at Hospital Aand Hospital B are shown in table 1 Information relatingto home visit after postpartum hospital discharge is alsoincluded in table 1 The average age of women was 28years more than 50 of the women completed highschool education 40 lived in a family where the mainincome earners were manual workers 40 lived in afamily where the main income earners were professionalworkers 87 were married or in a de facto relationship
13 had private health insurance and 28 were first timemothers The average length of hospital stay after deliveryat both hospitals was approximately three days There wasno significant difference between the followingcharacteristics of the women who gave birth at Hospital Aand the women who gave birth at Hospital B age thehighest level of education occupation of main familyincome earner marital status the type of healthinsurance being a first time mother and the length ofhospital stay after birth
Compared with the percentage of women who gavebirth at Hospital B a significantly higher percentage ofwomen who gave birth at Hospital A had an assisteddelivery including caesarean section forceps assisteddelivery or vacuum assisted delivery However a lowerpercentage of the women who gave birth at Hospital Ahad recorded complications during their perinatal periodcompared with the percentage of women who had suchcomplications at Hospital B These contradictory findingswere unexpected The average length of hospital stay afterdelivery at Hospital A and Hospital B were 34 days and37 days respectively This difference was not statisticallysignificant
Approximately one-third (n=52 364 of 143 women)had home visits by midwives ranging from zero to sevenvisits Of all 63 women who gave birth at Hospital A 46(73) received at least one postpartum home visit Theaverage number of visits was 22 Among 80 women whogave birth at Hospital B only six women (75) who metthe criteria of having home visit (see lsquoStudy hospitalrsquo andlsquoHome follow-up visitsrsquo section) received at least onehome visit The number of home visits ranged from zeroto two with the average number of home visits being 01As expected the numbers of home visits provided towomen who gave birth at both hospitals were statisticallysignificantly different
The number of home visits and the characteristics of women Table 2 shows the number of home visits categorised bydifferent social demographic and obstetric characteristicsof women Women who were single widowed or divorcedreceived a significantly higher number of home visitsthan the number of home visits provided to marriedwomen or women who were in a de facto relationshipWomen who did not have complications during theperinatal period received a significantly higher number ofhome visits than the number of home visits provided towomen who had perinatal complications These findingsdid not differ after taking into account women who hadperinatal complications and gave birth at each hospitalThis was an unexpected finding
Thirteen of the 19 women at Hospital A who experiencedperinatal complications received home visits Of 51women at Hospital B who experienced perinatalcomplications only three received home visits The lengthof hospital stay after birth among those who had
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
26
Table 1 Social demographic and obstetrics characteristics of postpartum women who gave births at two study hospitals (a)
Characteristic
Maternal Age (year)Number of womenRangeMean (SD)
t (df)p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df) p
Occupation of main family income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Number of womenRange of hospital stayMean (SD)
t (df) p
Postpartum home visitNumber of womenNumber of visits
012345 or higher
Range of postpartum home visitMean (SD)t (df)p
6217-39
2756 (55)
17 (270)34 (540)12 (190)
13 (206)25 (397)25 (397)
52 (825)11 (175)
54 (857)9 (143)
14 (222)49 (778)
28 (444)35 (556)
19 (302)44 (698)
631-16
341 (21)
63 (1000)
17 (270)4 (63)
16 (254)9 (143)
10 (159)7 (111)
0-722 (18)
7915-40
287 (57)
21 (263)51 (637)8 (100)
14 (174)33 (413)33(413)
72 (900)8 (100)
70 (875)10 (125)
26 (325)54 (675)
52 (650)28 (350)
51 (638)29 (362)
801-7
372 (15)
80 (1000)
74 (925)4 (50)2 (25)
000
0-201 (04)
14115-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
1431-16
359 (180)
143 (1000)
91 (636)8 (56)
18 (126)9 (63)
10 (70)7 (49)
0-7104 (16)
-123 (139) p = 022
263 (2) p = 027
023 (2) p = 089
170 (1) p = 019
010 (1) p = 076
185 (1) p = 017
604 (1)p = 001
1592 (1) p lt 0001
103 (141) p = 030
30 (50)p= 0005
Hospital A Hospital B Total (b)
Number () Number () Number ()
Note a) Pearson Chi-square test was used to assess a relationship between two categorical variables and the student t-test was used to assess a relationshipbetween the difference of two means b) Total number may not be equal to 143 due to missing data
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
27
Table 2 Relationship between social demographic and obstetrics characteristics of postpartum women and the number of home visits afterhospital postpartum discharge (c)
Characteristic
Maternal age (year)RangeMean (SD)
Correlation Coefficient (r) p
Motherrsquos highest level of educationLower than high schoolHigh school or equivalentUniversity undergraduate education or equivalent
Chi-square (df)p
Occupation of family main income earnerUnemployed or studentManual workerProfessional worker
Chi-square (df)p
Marital StatusMarried or de facto relationshipSingle widowed or divorced
Chi-square (df)p
Type of health insurancePublicPrivate
Chi-square (df)p
Number of pregnancyFirst Second and higher
Chi-square (df)p
Type of deliveryNormal deliveryCaesarean section forceps and vacuum delivery
Chi-square (df)p
Complication during perinatal periodHad complicationNo complication
Chi-square (df)p
Length of hospital stay after delivery (day)Correlation Coefficient (r) p
141 (1000)15-40
282 (56)
38 (266)85 (594)20 (140)
27 (189)58 (406)58 (406)
124 (867)
19 (133)
124 (867)19 (133)
40 (280)103 (720)
80 (559)63 (441)
70 (490)73 (510)
143 (1000)
0-7
0-70-60-6
0-70-60-6
0-6
0-7
0-70-5
0-60-7
0-70-6
0-50-7
0-7
-
0 (02)0 (02)0 (03)
0 (02)0 (02)0 (02)
0 (02)
2 (03)
0 (02)0 (03)
0 (02)0 (02)
0 (02)0 (02)
0 (0 025)0 (03)
-
-015 068
130 (2)052
133 (2)052
548(1)002
014 (1)07
002(1)089
281 (1)009
924 (1) 0002
-005 06
Number of women () b
pRange Median (inter-quartile)
Number of home visits
Note (b) Total number may not be equal to 143 due to missing data(c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables
complications at both hospitals (average 42 days SD=21
days) was significantly longer that the length of hospital
stay among women who did not (average 3 days SD=12
days) The data are not shown in the table
Results also showed that no statistically significant
difference occurred between the number of home visits
and the womenrsquos level of education occupation of main
family income earner type of health insurance being a
first time mother or the type of delivery There was no
correlation between the number of home visits and thewomenrsquos age and their length of hospital stay afterdelivery
Outcomes of home visitTables 3a and 3b show the median inter-quartile and
range of home visits provided to women who gave birth atboth study hospitals and were categorised according totheir health outcomes 1) postpartum depression 2)confidence to undertake maternal roles 3) breastfeeding
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
28
Table 3b Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Breastfeeding in the last 7 daysExclusively breastfeedingPredominantly breastfeeding Predominantly bottle feedingExclusively bottle feeding
Chi-square (df) p
Satisfaction with postpartum careVery satisfiedSatisfiedLittle satisfiedDissatisfied
Chi-square (df) p
Hospital A Hospital B TotalHealth Outcomes Number of Home Visit Number of Home Visit Number of Home Visit
Number of Range Median Number of Range Median Number of Range Medianwomen () (Inter-quartile) women () (Inter-quartile) women () (Inter-quartile)
and 4) satisfaction with postpartum care The resultsindicated that all women in the study regardless of homevisits or other characteristics had a relatively lowdepression level and a high level of confidence toundertake maternal roles We were unable to control forother confounding factors using multivariate data analysesbecause of a small sample size of few cells
The majority of women (573 of 143 women)reported that they exclusively breastfed their babies whileapproximately 30 never breastfed their babies Thisinformation was based on the self-reported regularity ofbreastfeeding in the past seven days The majority of thewomen (n=88 615 of 143 women) reported they werevery satisfied with postpartum care while only 7 saidthey were not satisfied with the care
There was no significant relationship between thenumber of home visits provided to women who gave birthat Hospital A and their health outcomes However therewas a significant association between the number of
home visits provided to women who gave birth atHospital B and the womenrsquos postpartum depression andtheir confidence to undertake maternal roles Thedirection of a relationship between the number of homevisits and these health outcomes was contrary to theexpectation of health personnel at the study hospitalsResults indicated that an increasing number of homevisits were related to an increasing level of postpartumdepression The higher number of home visits was alsorelated to a lower level of the womenrsquos confidence toundertake maternal roles among the women who gavebirth at Hospital B
The data from both hospitals indicated a positiverelationship between the number of home visits and awomanrsquos confidence to undertake maternal rolesHowever there was no positive correlation between thenumber of home visits and the Edinburgh postpartumdepression scale
Table 3a Relationships between the health outcomes of postpartum women and the number of home follow-up visits (c)
Health Outcomes Hospital A Hospital B Total
Postpartum depression (score)Number of women 63 80 143
Range of score 0-23 0-19 0-23Median (Inter-quartile) 5 (18) 35 (1 875) 4 (18)
Correlation Coefficient (r) p 013 030 023 004 016 006
Confidence of maternal rolesNumber of women 63 80 143
Range of score 10-20 12-20 10-20Median (Inter-quartile) 15 (14 17) 17 (16 19) 17 (15 18)
Correlation Coefficient (r) p -010 046 -034 0002 -034 lt0001
Note (b) Total number may not be equal to 143 due to missing data (c) The Kruskall-Wallis non-parametric test used to assess a relationship between the number of home visits and categorical variables and the Spearman rankcorrelation was used to assess a relationship between the number of home visits and continuous variables plt005 plt0005
34 (540)10 (159)019 (301)101 (2)060
45 (714)12 (190)5 (80)1 (16)4024 (3)026
0-60-7-0-6
0-70-60-20
2 (0325)2 (04)
-2 (24)
2 (05 4)2 (025375)
2 (02)0
48 (600)5 (62)4 (50)
23 (288)254 (3)
047
43 (538)28 (350)
5 (62)4 (50)
312 (3)
0-20-20-10-1
0-20-20-10-1
0 (00)0 (00)
0 (0 15)0 (00)
0 (00)0 (00)
0 (0 05)0 (0 075)
82 (573)15 (105)
4 (28)42 (294)229 (3)
051
88 (615)40 (280)10 (70)5 (35)
409 (3)025
0-60-70-20-6
0-70-60-20-1
0 (02)0 (03)
0 (015)0 (02)
0 (0 275)0 (01)0 (02)
0 (0 05)
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
29
DISCUSSION AND IMPLICATIONSWomen who gave birth at both hospitals had similar
social and demographic characteristics The women in thestudy had a slightly longer hospital stay (36 days) aftertheir birth compared with the 2000 national average (28days of public hospitals) (Australian Institute of Healthand Welfare 2003) Although the women in the study weresimilar to the women who gave birth in Queensland inrelation to their age and marital status it was unlikelythey represented all women who gave birth in Queenslandas there was a lower percentage of first time mothers(28) than the percentage of first time mothers inQueensland (401) (Australian Institute of Health andWelfare 2003)
As expected the women who gave birth at Hospital Ahad a significantly higher number of home visitscompared to the number of home visits provided to thewomen who gave birth at Hospital B The length of stayafter delivery at both hospitals was not significantlydifferent However the results at both hospitals aftertaking perinatal complications into consideration showedthat women who had complications had a longerpostpartum hospital stay than women who did not
The study results did not find that women who hadshort hospital stay after the birth of their babies receivedhome visits so they could gain benefits of continuinghealth services The overall results indicated thatunstructured home visits to women after hospitalpostpartum discharge did not provide positive healthoutcomes Nurses and midwives responded to a womanrsquoscircumstance and identified needs rather than using astructured protocol during a short period of home visitsThe lack of positive health outcomes could probably beexplained by a longer postpartum hospital stay amongwomen who had perinatal complications Further studiesneed to investigate specific services provided to womenduring hospital stay and compare them to the servicesprovided during postpartum home visits
The study data showed the number of home visits wasrelated to a high level of depression and a low level ofconfidence to undertake maternal roles Caution is neededto interpret these results as only a few women who gavebirth at Hospital B during the study period received thehome visits The lack of selection criteria to provide homevisits by Hospital A self selection to receive care by thewomen and a perceived personal need to have home visitscould be reasons for the lack of positive health outcomesfound in Hospital A However the social and obstetriccharacteristics of the women who gave birth at Hospital Bcould contribute to the negative outcomes of the homevisits by nurses or midwives We were unable to controlthe extraneous factors including marital status due to thesmall number of women who gave birth at Hospital B andhad home visits It was beyond the scope of this study toexplore health outcomes of home visits taking into
account various confounding factors using multiplevariate analyses since the number of each group would betoo small to permit any meaningful pattern to emerge
The lack of positive health outcomes needs furtherinvestigation For example self-selection to receive homevisits and the womenrsquos expectation of services might haveinfluenced the satisfaction level reported by the womenOther social support from family members and healthpersonnel might have affected the decision to seek carefor themselves and their infants Also prior intention notto breast-feed an infant may not have changed with only afew home visits
Only one disadvantaged group women who weresingle widowed or divorced received a higher number ofhome visits compared to other groups of womenSurprisingly the women who had complications duringthe perinatal period had a fewer number of home visitscompared to the women who did not have complicationsThis was probably due to their longer hospital stay Thesources of support including general practitionersobstetricians family members and friends provided towomen who had complications were not assessed in thisstudy This might be different to the sources of support towomen without complications and this needs furtherstudy There was also contradictory information betweenthe percentage of assisted deliveries and complicationsduring perinatal periods We were unable to validate thisinformation to identify whether there was any discrepancyin the information recorded by health professionalsbetween both hospitals
We did not explore other sources of information givento the women during their pregnancy so were unable toassess how these might influence postpartum healthoutcomes The study also did not explore health educationcontent given by midwives The women who participatedin the study were also unlikely to represent all womenwho gave birth in the study area We were unable to assessthe effects of the difference of response rates betweenboth hospitals on the study results The small number ofwomen who gave birth at Hospital B and received homevisits limited the ability to consider both social andobstetrics factors of the women during the assessment ofa relationship between the number of home visits andhealth outcomes
REFERENCESArmstrong K L Fraser J A Dadds M R and Morris J 1999 Arandomized controlled trial of nurse home visiting to vulnerable families withnewborns Journal of Paediatrics and Child Health 35237-244
Australian Institute of Health and Welfare 2003 Australiarsquos mothers and babies2000 AIHW Cat No PER21 Canberra AIHW National Perinatal StatisticalUnit
Barros FC Halpern R Victora CG Teixera AM and Beria J 1994 Arandomized intervention study to increase breastfeeding prevalence in southernBrazil Revista de Saude Publica 28(4)277-283
Brent NB Redd B Dworetz A DrsquoAmico FD and Greenberg J 1995Breastfeeding in a low-income population Archives of Pediatric and AdolescentMedicine 149(7)798-803
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
30
Daniel WW 1995 Biostatistics A foundation for analysis in the healthsciences New York John Wiley amp Sons
De Koninck M Blais R Joubert P and Gagnon C 2001 Comparingwomenrsquos assessment of midwifery and medical care in Quebec CanadaJournal of Midwifery amp Womenrsquos Health 46(2)60-67
Eberhard-Gran M Eskild A Tambs K Opjordsmoen S and Samuelsen SO 2001 Review of validation studies of the Edinburgh Postnatal DepressionScale Acta Psychiatric Scandinavian 104(4)243-249
Frank-Hanssen MA Hanson KS and Anderson MA 1999 Postpartumhome visits Infant outcomes Journal of Community Health Nursing16(1)17-28
Fraser JA Armstrong KL Morris JP and Dadds MR 2000 Homevisiting intervention for vulnerable families with newborns Follow-up resultsof a randomized controlled trial Child Abuse amp Neglect 241399-1429
Grullon KE and Grimes DA 1997 The safety of early postpartumdischarge A review and critique Obstetrics and Gynecology 90860-865
Hay D Jirojwong S Ritchie B Walker S and Wilson M 1999 Researchreport Evidence based practice Rockhampton Australia Central QueenslandUniversity (unpublished manuscript)
Jirojwong S 1995 Psychosocial factors relating to the use of antenatal servicesamong pregnant women in Southern Thailand Unpublished PhD MelbourneUniversity of Melbourne
Johnson TS Brennan RA and Flynn-Tymkow CD 1999 A home visitprogram for breastfeeding education and support The Journal of ObstetricGynecologic and Neonatal Nursing 28(5)480-485
Kendrick D Elkan R Hewitt M Dewey M Blair M Robinson JWilliams D and Brummell K 2000 Does home visiting improve parentingand the quality of the home environment A systematic review and metaanalysis Archives of Disease in Childhood 82443-451
Lieu TA Braveman PA Escobar GJ Fischer AF Jensvold NG andCapra AM 2000 A randomized comparison of home and clinic follow-upvisits after early postpartum hospital discharge Pediatrics 1051058-1065
Meikle SF Lyons E Hulac P and Orleans M 1998 Rehospitalizations and outpatient contacts of mothers and neonates after hospital discharge after vaginal delivery American Journal of Obstetrics and Gynecology179(1)166-171
Morrell CJ Spiby H Stewart P Walters S and Morgan A 2000 Costs andeffectiveness of community postnatal support workers Randomised controlledtrial British Medical Journal 321593-598
Nunnally JC 1978 Psychometric theory New York McGraw-Hill
Queensland The Office of Economic and Statistical Research 2002Queensland regional profilesURLhttpwwwoesrqldgovaudatapublicationsreg_prowide_bahellipwbbhtAccessed 16 June 2002
Ransjo-Arvidson AB Chintu K Ngrsquoandu N Eriksson B Susu BChristensson K and Diwan V K 1998 Maternal and infant health problemsafter normal childbirth A randomised controlled study in Zambia Journal ofEpidemiology and Community Health 52(6)385-391
Sikorski J Renfrew MJ Pindoria S and Wade A 2003 Support forbreastfeeding mothers A systematic review Paediatric and PerinatalEpidemiology 17(4)407-417
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
31
Penny Paliadelis RN BN MN (Hons) Lecturer School ofHealth University of New England Armidale New South WalesAustralia
ppaliadeuneeduau
Mary Cruickshank PhD Senior Lecturer School of HealthUniversity of New England Armidale New South Wales Australia
Donna Wainohu RN Nurse Unit Manager Ongoing andExtended Care Services Armidale Community Health New EnglandArea Health Service Armidale New South Wales Australia
Rhonda Winskill RN PaedIntCareCert BSocSci MN PaediatricRural Outreach Clinical Nurse Consultant Northern Child HealthNetwork Metford New South Wales Australia
Helen Stevens RN BN Paediatric Clinical Nurse Specialist NewEngland Area Health Service Armidale New South Wales Australia
Accepted for publication November 2004
IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFSAND PRACTICES OF PAEDIATRIC NURSES
Key words paediatric nursing child-centred care clinical practice guidelines
ABSTRACT
Objective This study explored paediatric nursesrsquo perceptions
of how they include and involve parents in the care ofhospitalised children
DesignThis qualitative study used individual unstructured
interviews to gather data the data was analysed usingthematic coding
SettingPaediatric wards within two regional area health
services of New South Wales Australia
SubjectsFourteen paediatric nurses were asked to describe
their beliefs and practices regarding the clinicalapplication of family-centred care
Main outcome measurePaediatric nursesrsquo beliefs and practices about
family-centred care were explored in an effort toexplain how the concept was implemented
ResultsThe findings are presented as four interconnected
themes The first describes how participants eitherallocated tasks to parents or retained them the secondrelates to the nursesrsquo professional identity the thirdtheme identifies barriers and constraints to theimplementation of family-centred care while the
fourth describes the nursesrsquo beliefs about theirresponsibilities when delivering family-centred care
ConclusionsTogether these findings suggest that while nurses
endorse the concept of family-centred care theimplementation into practice is more problematic Whileit is not possible to generalise these findings to otherpaediatric nurses the authors believe the insight gainedwill resonate with paediatric nurses internationally Thefindings from this study are being used as the basis forthe development of clinical practice guidelines to assistpaediatric nurses to more consistently apply theconcepts of family-centred care to their practice
INTRODUCTION
This collaborative project arose from discussionsbetween a group of paediatric nurses and a nurseacademic during a paediatric education day held in
regional New South Wales Australia The discussioncentred on how difficult it can be to actively involveparents in the care of their sick child The cliniciansrsquoconcerns focused on the variability of the roles and tasksparents are encouraged to undertake in paediatric wardsthe power and knowledge differential between health careprofessionals and parents and the lack of time availablefor nurses to build rapport with parents
The concept of lsquofamily-centred carersquo is used todescribe the way in which families and significant othersare included and involved in the health care ofhospitalised children (Coyne 1996) In developed countriesmost paediatric wards claim to be lsquofamily-centredrsquo which
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
means that these wards adopt a philosophy where parents areacknowledged as being central to their childrsquos existence and aretherefore vital in the decision-making process regarding the careof their child (Shields 2001)
However previous research has indicated that family-centred care remains an idealistic notion in manypaediatric settings (Espezel and Canam 2003 Fenwick et al2001 Shields et al 2003)
So while most paediatric nurses accept that the conceptof family-centred care is important the application of thisconcept into practice is not always evident This studysought to explore ways in which a group of paediatricnursesrsquo incorporated this concept into their clinicalpractice The results of this study will further enhancenursing knowledge regarding the clinical application offamily-centred care and the findings will be used to developclinical practice guidelines during the next stage of this project
BACKGROUND TO THE STUDYHistorically hospitals maintained rigid visiting policies
preventing parents from seeing their child for long periods oftime However since the early 1950s it has been recognisedthat hospitalisation is stressful for children Two reports fromthe British Ministry of Health (1946 1959) identified thatchildren in hospital required emotional support and should bevisited frequently by their parents These early reports wereamong the first to advocate that mothers should be allowed tolsquoroom-inrsquo with their hospitalised child Within a short spaceof time similar findings evolved from Canadian and NorthAmerican studies so that by 1963 health care practices andpolicies in most developed countries had recognised thebeneficial effect of having a family member stay with ahospitalised child (Poster and Betz 1963)
A review of the more recent literature shows thathospitalisation is considered to be traumatic particularlyfor infants and children less than five years of age This isbecause young children lack the appropriate coping skillsnecessary to deal with the stresses of illness painseparation from family and an unfamiliar environment(Coyne 1996 Morse and Pooler 2002 Sheldon 1997)Allowing parents to stay with their hospitalised child hasbeen identified as a significant step toward reducing thetraumatic effects of hospitalisation on children (Shields 2001)
In 1996 Coyne concluded from a study whichexamined parental participation in the care of hospitalisedchildren that lsquothe concept of parental participation wasboth complex and underdevelopedrsquo and added that thisleads to lsquodifferent interpretations of parental participationby health professionals in their effort to apply the conceptin practicersquo (Coyne 1996 p740) In 1997 a literaturereview by Sheldon identified that nurses acknowledgedparents know their child better than anyone but stillbelieved that in practice nurses were better than parentsin looking after a hospitalised child
Recently the concept of parental involvement in thecare of hospitalised children has also come to includeparental involvement in decision-making as well asparticipation in the care provided This concept has beenlinked to an increase in consumerism in healthcare(Galvin et al 2000 Espezel and Canam 2003)
Today parents families or the childrsquos primary care giverexpect to be actively involved in health care decision-makingas well as the delivery of care However parental involvementin the health care of hospitalised children does not alwaysoccur Kristensson-Hallstrom (2000 p1029) believes thereason for this is that while paediatric nurses claim to supportfamily-centred care their practices do not always reflect thisclaim Galvin et al (2000 p625) agrees stating that lsquowithinthe hospital culture there may be resistance to incorporatingthe patient and family into decision-making and involvementwith carersquo Similarly Hutchfield (1999) found family-centredcare remains an idealistic notion and while nurses espouse theconcept of family-centred care in reality they lsquoregulate theamount of parental participation in the childrsquos carersquo (Espezeland Canam 2003 p35)
The findings of a recent study by Shields et al (2003)identified that unless nurses have the time energy andmotivation to build rapport with parents then effectivecollaboration regarding the childrsquos care is unlikely tooccur So while the literature indicates paediatric nursesaccept the concept of family participation in the care ofhospitalised children there is a lack of empirical evidenceregarding its implementation This study sought toexplore paediatric nursesrsquo perceptions of this concept andits incorporation into their clinical practice
Clinical practice guidelinesAt present there are no evidence-based clinical practice
guidelines available in NSW Australia that articulate howpaediatric nurses can best implement the concept offamily-centred care into their practice Clinical practiceguidelines in nursing are a way of providing consistentlyhigh quality care by adhering to recognised evidence-based standards The care provided should then beevaluated using continuous quality improvementstrategies (Whittenmore and Grey 2002) However to beeffective clinical practice guidelines need to be based oncurrent evidence and appropriate for the clinicalenvironment in which they are to be implemented(Whittenmore and Grey 2002 Sabatier 2002) Thus theresearch team for this study consisted of nurse academicsand paediatric clinical nurses who worked together onevery phase of this pilot study The aim of the next stageof this project is to introduce clinical practice guidelinesthat will be relevant to paediatric nursing practicethroughout New South Wales Australia
METHODThe aim of this collaborative study was to explore how
paediatric nursing staff included and involved familymembers in the care of the hospitalised child
RESEARCH PAPER
32
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
The specific objectives were to
bull explore paediatric nursesrsquobeliefs regarding the involvementof family members in the care of hospitalised children
bull identify whether paediatric nursesrsquo include and involvefamily members in the care of sick children in hospital
bull identify the challenges andor barriers faced by paediatricnurses in implementing family-centred care and
bull the data to develop clinical practice guidelines that willassist paediatric nurses to provide family-centred care
STUDY DESIGNA qualitative approach was used as beliefs perceptions
and experiences needed to be explored According toRowe and McAllister (2002 p8) qualitative inquiry canprovide a means of understanding the contextual nature ofnursing and informs clinical practice in a way that mayallow for changes to occur
Population and sample methodThe population from which the sample was drawn was
paediatric nurses who care for hospitalised children in thepaediatric wards of two hospitals in regional NSW
A purposive sample was recruited by invitingpaediatric nurses employed in both hospitals to participatein the study Willing participants with a diverse range ofpaediatric experience were selected to be interviewed byone of two interviewers
ProceduresThe data collection consisted of individual interviews
and validation of themes was conducted to ensure rigour and trustworthiness Fourteen participants wereindividually interviewed using broad prompting questionssuch as lsquoCan you describe how you involve parents in thecare of their children during hospitalisation Or lsquoIn yourpractice how do you apply the concept of family-centredcarersquo Each 30-50 minute interview was audio taped withthe participantrsquos permission and the tapes transcribed
Data analysisThe transcripts of the interview tapes were read and
re-read by all members of the research team The analysisused thematic coding to identify key concepts and themes inthe data This method of data analysis allowed the researchersto extract the essence of the experiences as described by theparticipants and present these as themes designed to describethe key elements (Roberts and Taylor 1998)
In order to agree on the emerging themes a two-stepmethod of analysis was used First the transcripts fromeach of the two locations were analysed by theinterviewers Second clean copies of the transcripts wereexchanged and re-analysed by each member of the teamin order to check for consistency of the emerging themes
Following analysis of the interview data a summary offindings was disseminated to all participants who werethen invited to make suggestions and comments Togetherboth sets of data will be used to develop preliminaryclinical practice guidelines
EthicsEthical approval to commence this project was given by a
university human research ethics committee and bothrelevant area health service human research ethicscommittees Willing participants were provided with aninformation sheet asked to sign a written consent form prior toparticipating in the study Participants were informed that theiridentity and place of employment would not be revealed
RESULTSThe researchers identified four major themes in relation
to paediatric nurses descriptions of how they implement theconcept of family-centred care These themes are titledlsquotasks and rolesrsquo lsquoempowerment issuesrsquo lsquobarriers andconstraintsrsquo and lsquocare and protectionrsquo
Theme 1 Tasks and rolesAll participants described particular tasks or roles they
commonly allocated to willing parents or primary caregiversas well as tasks and roles felt were best left to nurses Insome instances participants indicated they made decisionsabout which jobs and roles to allocate to parents based on thenursesrsquo assessment of the motivation andor perceived skilllevel of the parents The following is a list of tasks and roles allthe participants regularly allowed willing parents to perform
bull Staying with the child at all times to calm and comfort(generally this applied to only one parent or care-giverat a time)
bull Meeting hygiene needs (eg bathing showering washing)
bull Feeding or helping at meal times
bull Meeting elimination needs (eg taking the child to thetoilet changing nappies emptying urine bottles)
bull Accompanying the child to the anaesthetic bay (ifallowed by the medical officer)
bull Entertaining the child (eg organising games stories videos)
bull Advising nursing staff of the childrsquos status (particularlyany changes in the childrsquos condition)
Only a few participants described allowing someparents to perform the following tasks but this onlyoccurred after the parent had been instructed andobserved for competency
bull Giving medications
bull Changing dressings
bull Recording fluid balance
All participants felt strongly about the importance ofperforming their nursing tasks and roles Many of the
RESEARCH PAPER
33
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
participants made comments about caring for the patientand the family by protecting them from unpleasant sightsand sounds and particularly unpleasant procedures Allparticipants talked about the importance of retaining theirprofessional role with one participant commenting lsquoWecannot expect parents to take on our role as nurseshellip nurseshave to continue to be nursesrsquo This is consistent withGalvin et al (2000 p626) who found that lsquostaff memberperceptions are that working collaboratively with families isa threat to their professional identityrsquo One participantobviously felt this threat when commenting lsquoThings arebeing taken away from us and handed over to the parentsrsquoThese comments highlight the concerns a number of theparticipants felt regarding role erosion For example oneparticipant stressed that lsquoas nurses we canrsquot lose the skillswe trained forhellip the parents are there to support the childhellipI mean they can be involved but not take away our rolersquo
These comments are consistent with the findings of arecent study conducted by Espezel and Canam (2003 p40)who found that even when parents described the parent-nurserelationship as positive it was rarely collaborative in nature
Evident in all the interviews was the important role nursesbelieved they played in providing a communication conduitbetween the medical officers and the child and parents bylsquotranslatingrsquo medical terms into laypersonrsquos language and bychecking for parentsrsquo understanding of the childrsquos conditionand care requirements One participant explained this rolelsquoItrsquos up to us to keep the parents fully informedrsquo Whileanother participant explained that after the doctorsrsquo rounds thenurse goes back to the family and explains the jargon bylsquoacting as an interpreter between the doctor and the familyrsquo
Again according to a study by Espezel and Canam(2003) parental expectations of a nursersquos role includednurses acting as a mediator between parents and doctorsFurthermore Espezel and Canam (2003) found parentsviewed nurses positively as long as they lsquotranslatedrsquomedical information successfully
Theme 2 Empowerment issuesThis theme related closely to the participantsrsquo
assumptions and beliefs about their professional identityas a nurse Each participant made comments concerningtheir power as health care professionals In all instancesthe participantsrsquo descriptions were consistent with thoseof Hewitt (2002 p440) who describes the powerexercised by health care professionals as lsquobenevolentpaternalismrsquo
Hewitt (2002) goes on to say that despite the bestintentions of the nurse this form of power restricts theautonomy of patients and families All participants discussedthese empowerment issues in terms of what they wouldlsquoallowrsquo parents to do making it clear that the decision toinclude parents in care delivery rested with the nurse Theircomments are condensed into the following key points
bull Nurses believe they are the ones to lsquoset the boundaryrsquoregarding the role and tasks that parents can perform forthe hospitalised child
bull Nurses assume control of the decision-making processesfor the care of the child by educating lsquotellingrsquo andadvising parents of their childrsquos condition and treatment
bull Parents must ask nursesrsquo permission before making anydecisions in relation to the care of the hospitalised child
bull Nurses discourage parents from assuming responsibilityfor anything other than basic parental duties duringhospitalisation and lsquonursingrsquo skills are only taught ifparents need lsquoadvancedrsquo skills to provide home care
bull Nurses feel strongly that parents should not take onlsquonursingrsquo responsibilities as they need to focus on thechild not the nursing tasks
All participants felt strongly that they were lsquothe knowledgeexpertsrsquo in providing nursing care for sick children This beliefwas reflected in many of the comments such as
lsquoSkilled nursing jobs should be done by the nursing staffand the nurturing and comforting and the unskilled jobslike bathing and changing left to the parentsrsquo
lsquoNurses just go and do things because sometimes nursesknow best and kids are better with nursing staff than theyare with parentsrsquo
lsquoI wouldnrsquot encourage parents to be giving drugs andthings like thathellip because if anything goes wrong Irsquom theone who takes the raprsquo
One participant commented that lsquoI donrsquot believe weshould involve parents [in nursing duties] unless itrsquosteaching them something for when they go out of thehospital environment
This sentiment was echoed in all the interviewsHowever in many of the interviews the participantsqualified their comments by explaining that if they hadmore time to spend with families providing educationand support then they may be more comfortable inallowing parents to assume greater responsibility for thenursing care of the child
According to Espezel and Canam (2003) and Shieldset al (2003) paediatric nurses readily promote family-centred care as a concept but the clinical applicationremains problematic for a number of reasons which aredescribed in the next theme
Theme 3 Barriers and constraintsAll participants described barriers and constraints they
believed prevented them from providing family-centred careas effectively as they might Unanimously all participantsstressed they would like more time to involve and educateparents This included more time to assess parentalcompetence and provide more advanced knowledge and skills
The barriers described were varied but all participantsagreed staff shortages heavy workloads and time constraints
RESEARCH PAPER
34
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
impacted on their ability to give sufficient time to eachfamily Some of the comments related to these barriers were
lsquoWersquore often under time pressure and understaffed so itisnrsquot always possible to explain proceduresrsquo
lsquoIn a very busy ward itrsquos easier to do it yourselfhellip itrsquos atimeframe thingrsquo
lsquoWhen itrsquos really busy itrsquos hard to be able to spend timewith them [parents] teaching them thingsrsquo
Espezel and Canam (2003) believe inadequate staffinglevels and the desire for cost-effectiveness in health caresignificantly influences the incongruence between thetheory and practice of family-centred care
Other issues participants described as constraints inproviding effective family-centred care are summarised below
bull A lack of guidelines andor policies for the nurse regardingthe role of parents when children are hospitalised
bull Nursesrsquo concerns regarding the extent of their legal andprofessional responsibilities for the care of thehospitalised child
bull Parents who indicate an unwillingness or inability to be involved
bull Lack of structure and guidance about how to implementfamily-centred care particularly for staff new to apaediatric setting
bull Outdated nursing habits eg lsquodoing the job yourselfrsquobecause it is quicker
bull Poor communication between nurses and parents
bull Nurses and parents lack of confidence in their respectiveroles new parents who were unsure of their parentingskills and nurses who lacked confidence in theirknowledge andor skills
bull The nursesrsquo need to be seen as lsquothe expertrsquo exemplifiedby an inabilityunwillingness to share knowledge
bull Nurses who do not have the energy or motivation toteach and involve parents often because they areoverworked andor lsquoburnt outrsquo
bull The nursing management practice of reducing staffinglevels when parents are present to lsquocarersquo for youngchildren and infants in the belief that the nursesrsquoworkload is reduced by their presence
Many of these barriers are consistent with those describedin the literature (Espezel and Canam 2003 Galvin et al 2000Hutchfield 1999 Shields 2001 Shields et al 2003) Howeverthe researchers suspect that removal of these barriers may notaddress the problem of including parents as more equalpartners in care for the reasons discussed in the final theme
Theme 4 Care and protectionAll of the participants described the importance of
assuming responsibility for the care and protection offamilies not just the individual patient Therefore at
times the nurses made decisions regarding theinvolvement of parents based on the assumption thatparents expected nurses to make such decisions
All the participants talked about protecting the parentsfrom stress when children were acutely ill and had to havepainful or unpleasant procedures performed The rationale forthis belief was that parents needed to provide the nurturingand comfort for their children thus it was not acceptable fornurses to expect parents to be involved in painful or unpleasantprocedures which would only add to their stress levels
These assumptions are evident in all the transcriptssome examples are
lsquoI asked ldquowould one of you like to come inrdquohellip but by thelooks on their faces they were scared stiff So I said Irsquoll justbring him back to you when itrsquos over for a cuddlersquo
lsquoIf a child is going to die I want to protect them [parents]from it instead of saying ldquoyes it may happenrdquorsquo
lsquoSome may think you should say to parents ldquoyou need to dothisrdquo but itrsquos not fair when parents are stressed anyway Weneed to fulfil our role and look after the child and the parentsrsquo
Sometimes I ask parents to leave because itrsquos easier forthem and the child to cope
There were many other comments related to this themeand they have been summarised as follows
bull Nurses felt parents should assume their usual caring rolewhile the child is hospitalised and not participate innursing duties because this would cause the parentsadditional stress in an already stressful situation
bull Nurses believe parents are often very tired when a childis hospitalised and therefore nurses should protect themfrom any additional responsibilities
bull Nurses felt strongly that parents have clear expectationsof what a nurse should do and nurses need to live up tothose expectations in order to build a positiverelationship with parents
bull Nurses assumed parents may feel guilty when their child issick because they may not have the time or energy to giveundivided attention to that child particularly if there areother children at home or unavoidable work commitmentstherefore nurses need to assume a primary caring role
bull Nurses were role models for parents and as such nursesneed to reassure and educate parents regarding the care of thechild and nurses should not abdicate this responsibility
bull Nurses believe parents do not want to make decisions atthis time but look to the experts eg doctors and nursesto decide the caretreatment needed
All participants described adopting this protectivepaternalistic role explaining it was this responsibility thatmotivated them to exclude parents at times In particularall participants described discouraging parents fromwitnessing procedures that could be distressing
RESEARCH PAPER
35
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
In their capacity as carers the participants felt they had aresponsibility to assume the decision-making role whenparents were tired or stressed Furthermore all participantsbelieved that by protecting parents from unpleasant eventsthey were lsquocaringrsquo for the whole family that is they wereactually implementing lsquofamily-centred carersquo
Interestingly Shields et al (2003) describes thehospitalisation of a child as an indication that help isneeded The nurses in this study all believed that bycaring for and protecting the family they were providingthe help needed in a lsquofamily-centredrsquo way
ASSUMPTIONS AND LIMITATIONSThe findings from this qualitative study cannot be
generalised to a wider population of paediatric nurses but theresults may resonate with nurses who work with sickchildren One assumption on which this study is based is thatthe implementation of family-centred care is a positivepractice worth striving toward Additionally the research teamacknowledges that observation of practice and interviewswith other stakeholders (for example children parents andfamilies) would have added further valuable dimensions tothis study but financial and time constraints did not allow forthese additional data collection strategies at this stage of theproject However it is anticipated that further studies willinclude interviews with other stakeholders and observation ofpractice as data collection methods
IMPLICATIONS AND CONCLUSIONThe findings of this study showed that the paediatric
nurses who participated all believed strongly in thelsquofamily-centred carersquo concept yet they found theapplication in practice to be somewhat challenging
The challenges described by the participants were linked tothe nursesrsquobeliefs about their own professional role their desireto see themselves as the lsquoexpertsrsquo in the care of hospitalisedchildren and the barriers they identified that makeimplementation of family-centred care difficult for them
Overwhelmingly all participants described their role asinvolving not only providing nursing care for the patientand family but also protecting family members frompainful or unpleasant experiences This belief seems tocause the nurses the most conflict when they discussedthe practical implications of parental participation
The clinical implications of this small study are thatthe decisions of the participants about the degree ofinvolvement of parents were influenced by the nursesrsquoneed to fulfil their caring role As well there werelegitimate concerns about the legal implications ofparents assuming traditionally lsquonursingrsquo duties
Based on these findings the next stage of this project willfocus on the development of clinical practice guidelines aimedat clarifying the nursesrsquo professional and legal responsibilitieswhen delivering family-centred care In addition the findings
of this study may encourage nurses to reflect on how theyinvolve families in caring for a sick child The next stage of thisstudy involves talking to larger groups of paediatric nurseswho will be asked to comment on the clinical applicability ofthe draft guidelines prior to introducing them into a numberof paediatric settings in New South Wales
In summary this collaborative project has providedsignificant insight into nursesrsquo assumptions beliefs andexperiences of implementing family-centred care
The findings have explicated an aspect of paediatricnursing practice from a cliniciansrsquo perspective and willbe invaluable as the basis for the development of clinicalpractice guidelines to assist nurses in the implementationof this concept into practice
Finally the significance of this project is grounded inthe belief that children are hospitalised in order to receiveexpert nursing care therefore enhancing the consistencyof nursing practice will be beneficial to children andfamilies during hospitalisation
REFERENCESBritish Ministry of Health 1946 Report of the care of children committee (TheCurtis Report) LondonHMSO
British Ministry of Health 1959 The welfare of children in hospital (The PlattReport) London HMSO
Coyne I 1996 Parental participation A concept analysis Journal of AdvancedNursing 23(4)733-740
Espezel H and Canam C 2003 Parent-nurse interactions Care of hospitalisedchildren Journal of Advanced Nursing 44(1)34-41
Fenwick J Barclay L and Schmied V 2001 Struggling to mother Aconsequence of inhibitive nursing interactions in the neonatal nursery Journalof Perinatal and Neonatal Nursing 15(2)49-64
Galvin E Boyers L Schwartz P and Jones M 2000 Challenging theprecepts of family-centred care Testing a philosophy Pediatric Nursing26(6)625-632
Hewitt J 2002 A critical review of the arguments debating the role of the nurseadvocate Journal of Advanced Nursing 37(5)439-445
Hutchfield K 1999 Family-centred care A concept analysis Journal ofAdvanced Nursing 29(5)1178-1187
Kristensson-Hallstrom I 2000 Parental participation in pediatric surgical careAORN Journal 71(5)1021-1029
Morse J and Pooler C 2002 Patient-family-nurse interactions in the trauma-resuscitation room American Journal of Critical Care 11(3)240-249
Poster E and Betz C 1963 Allaying the anxiety of hospitalised children using stressimmunisation techniques Issues in Comprehensive Paediatric Nursing 6227-233
Roberts A and Taylor B 1998 Nursing research processes An Australianperspective Melbourne Nelson
Rowe J and McAllister M 2002 The craft of teaching qualitative researchLinking methodology to practice Collegian 9(3)9-14
Sabatier K 2002 A collaborative model for nursing practice and educationNursing Education Perspectives 23(4)178-182
Sheldon L 1997 Hospitalising children A review of the effects NursingStandard 12(1)44-47
Shields L 2001 A review of the literature from developed and developingcountries relating to the effects of hospitalisation on children and parentsInternational Nursing Review 48(1)29-37
Shields L Kristensson-Hallstrom I and OrsquoCallaghan M 2003 Anexamination of the needs of parents of hospitalised children Comparingparentsrsquo and staffrsquos perceptions Scandinavian Journal of Caring Sciences17(2)176-184
Whittenmore R and Grey M 2002 The systematic development of nursingInterventions Journal of Nursing Scholarship Second quarter115-120
RESEARCH PAPER
36
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
37
Dianne Pelletier RN BScN BEdStud MSciSoc DipEdNsgFCN(NSW) FRCNA Senior Lecturer Faculty of NursingMidwifery and Health University of Technology Sydney NewSouth Wales Australia
DiannePelletierutseduau
Professor Judith Donoghue RN RM BA(Hons) PhD DNEFCN(NSW) Acute Care Nursing Professorial Unit University ofTechnology Sydney and South Eastern Health New SouthWales Australia
Professor Christine Duffield RN BScN MHP PhD FCN(NSW)FCHSE Director of the Centre for Health Services ManagementUniversity of Technology Sydney New South Wales Australia
Accepted for publication January 2005
ACKNOWLEDGEMENTSThe authors wish to thank Wendy Wise who as research assistant contributedto the statistical analysis and development of graphs
UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OFAUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
Key words nursing workforce graduate education career paths
ABSTRACT
BackgroundThe challenge posed by the worldwide nursing
shortage is significant not only for workforce andfacility planners but also for those who educate nursesfor practice and nurses themselves The provision of skilled and competent advanced nurses is clearly a goal of postgraduate educationAn increasing shortage of skilled and qualifiednursing staff to provide the required level of care isevident in Australia
ObjectiveTo determine the impact of graduate education
on registered nursesrsquo personal and professionaldevelopment
DesignA longitudinal descriptive and co-relational study of
postgraduate nursing students using postal survey
SampleFive cohorts (1998-2002) of nurses who had
graduated from university with a graduate diploma ormaster of nursing qualification were all surveyed oversix years post graduation (n=151)
Results The study showed the greatest motivator to change
jobs was greater job satisfaction self esteem andtheir ability to carry out their role exceeded their job satisfaction one quarter wanted to change their career and the strongest facilitator and the
strongest barrier to career advancement were theirpersonal situation
ConclusionThis paper focuses on recent career moves
motivation intentions and influencing factors six years after completion of their tertiary studiesThis information is critical in choosing retentionstrategies and workforce planning
INTRODUCTION
In the 20 years since the transfer of nursing educationinto the higher education sector in Australia graduateprograms for nurses have proliferated with many
specialist clinical courses having moved to universitiesAlthough master level nursing courses have beenavailable in this country since the early 1980s they wererelatively few until the transfer of the hospital basednursing programs to the tertiary sector in 1985 Also atthis time the graduate diploma developed as anincreasingly popular educational option as it becameavailable in different Australian states Students oftentransferred from the graduate diploma program to themasters program and completed that programAlternatively they graduated with the graduate diplomaand returned at a later date to convert it to a masterrsquosqualification after further study
Also nurses began to evaluate the graduate coursesoffered in Australia (Simsen and Holroyd 1997 Boore1996) Simsen and Holyroyd (1997 p370) assert that
Postgraduate nursing education supports a tertiary-based vertical career path which not only facilitates
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
38
professional career development but also gives nursingparity with other professions that have well-establishedpostgraduate education structures
In reporting the findings of a longitudinal studyfollowing graduates from a higher degree program it isthese professional career development activities that areof primary interest to the researchers Consequently theliterature review will focus on these aspects but will alsoinclude workforce issues Consideration of the impact ofgraduate study on competence and advanced practice orcritical thinking and research or other dimensions will becovered in less depth
This paper presents the findings from a 10-yearlongitudinal study of registered nurses (RNs) whocompleted a graduate diploma or master of nursing coursework degree The purpose of the study was to determinethe impact of graduate education on their personal andprofessional development
One element of this was the perceived impact of theireducation on their career advancement or movementsinitially after graduation (Pelletier et al 1998a) and sixyears later The study commenced with a pilot in 1991(Pelletier et al 1994) and five cohorts of students (1992-1996) were surveyed every two years for six years post-graduation The final questionnaire for each cohort wascompleted from 1998 to 2002 The findings related to theearly impact on their professional growth behaviour andcare activities have been reported elsewhere (Pelletier etal 1998b) as has the perceived effect of their study on thepractice and quality of care (Pelletier et al 2002)
LITERATURE REVIEWWhether achieved through sound knowledge and
practice in the research process (Sandor et al 1998) or at other points in the programs (Dexter et al 1997 Sandoret al 1998 Vaughan-Wrobel et al 1997) critical andanalytic thinking are valued and seen as goals of masterslevel education for nurses (Girot 2000) Boore (1996)studied a masters program which claimed its goals wereto develop the nursersquos knowledge and skills to supporttheir role as an advanced nurse and to develop nurses witha capacity for nursing research Increasingly descriptionsof advanced nursing practice are using words such asanalysis critical thinking synthesis of informationestablishing priorities reflection and creativity (Davis1993) While it is believed these are qualities which canbe achieved through postgraduate education researchevidence has not identified significant differences incritical thinking skills in practice at different stages oftheir studies (Girot 2000) Girot (2000) did find asignificant improvement in decision-making skills as aresult of graduate education So what motivates nurses tostudy at the graduate level
An early study of nurses found that students weremotivated by career advancement and the opportunitiesoffered by access to higher education (Thurber 1988)
Watson and Wells (1987) found professional growthpersonal growth and professional socialisation were the main motivators to pursue study to masterrsquos level Winson (1993) undertook a longitudinal study ofnurses who had completed master or doctoral level thesesor were doing so The study showed there was a strongtendency after one to two years for these nurses to moveinto positions that permitted them more autonomy
Another UK study found personal development andgrowth rather than career advancement were the mainmotivating factors for graduate study (Fraser andTitherington 1991) Boorersquos study (1996) revealed about20 were motivated by the enhancement of career pathsbut the majority were motivated by the coursersquosrelationship to practice and potential to increase theircompetence In contrast an Australian study evaluating atertiary critical care course found students stronglybelieved the course would contribute to their achievementof a promotion (Chaboyer and Retsas 1996) AnotherAustralian study (Pelletier et al 1998c) found themotivating factors to be personal or job satisfaction(42) increased professional status (22) and better jobopportunities (17)
The literature is quite consistent on what facilitates andblocks efforts to study - time support and recognitionThe majority of clinical students in Boorersquos (1996) studyreceived time off and only 25 received no financialsupport Lack of financial support and time off as well aslack of recognition in promotional opportunities wererecognised in Simsen and Holroydrsquos (1997) studyTrewthewie in her qualitative study (1999) foundrespondents would have liked more support from theirinstitutions in the form of time off and funding She also recommended on the basis of her findings that nurses with graduate qualifications be recognised and remunerated by their employers
The work environmentThe Australian work environment has changed
significantly in recent years and most probably many of the respondents in the study reported here would have felt the impact of these changes In developedcountries the nursesrsquo workload has been affected byincreased patient acuity shortened lengths of stay morechronic lifestyle diseases and improved life expectancyan increase in patient age and the number of severely ill patients (AIHW 2001 Aiken et al 2001 Diers andBozzo 1997 Duffield and OrsquoBrien-Pallas 2002 Jakoband Rothen 1997 OrsquoBrien-Pallas et al 2001) In addition the workforce is ageing (DEST 2002) andnurses are potentially retiring faster than they can bereplaced (OrsquoBrien-Pallas et al 2004) and they are being actively recruited to other industries (Duffield andFranks 2001 Duffield et al 2004)
Unacceptable and unsafe work environments andexperiences impact negatively on retention (Duffield and OrsquoBrien-Pallas 2002) as do the perception of poor
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
39
rewards (monetary and a lack of recognition relative to efforts put into the job) (Aiken et al 2001 Fagin 2001 OrsquoBrien-Pallas 2000) Hospital restructuringand downsizing have an impact on staff satisfaction andwell being (Burke 2003) and these factors may havecontributed to the respondentsrsquo decision to change their position
Given economic uncertainty in Australia in both the health and higher education sectors and theiraccountability for the use of public monies it is importantthat educational providers monitor the outcomes of theirendeavours As students are likely to be paying more in the future for their education either as direct fees or through increased HECS (Higher EducationContribution Scheme) charges the value of the productthey are purchasing will need to be made more explicitparticularly in an increasingly competitive market The need for evaluation of the outcomes of graduateeducation continues to be argued (Bethune and Jackling 1997 Dexter et al 1997) and Jordan (2000) callsfor better tools and methods to do so
METHOD
DesignThis is a longitudinal descriptive and co-relational
study of postgraduate nursing students on completion oftheir studies and for six years afterwards
SampleThe respondents were nurses who graduated from a
graduate nursing course in a metropolitan Australianuniversity between 1992 and 1996 The programs wereessentially focused on management or a clinical specialtyResearch subjects were included especially in the thirdyear of the master program The sample did not includethose doing a master of nursing by research thesisStudents may have entered the program on the basis of anundergraduate degree or on the basis of experience andprior learning (Donoghue et al 2002) The demographicprofile of the cohort collected on commencement of thisproject was undertaken on completion of their studies six years before the time of completion of the finalquestionnaire in the series Questionnaire D which is the focus of this article
Ninety three percent were female and 30 weremarried Ages ranged from 21-58 with a mean age of 35Attrition and loss of participants is inevitable in alongitudinal study This means that while this profile isreflective of the original population it cannot beconsidered exact for those still responding six years later
Procedure A questionnaire was used on each of the four
occasions The first (A) was completed at university andsubsequently B C and D were sent to students by mailand returned by self addressed stamped envelope Each of
the five cohorts was followed every two years for sixyears post graduation via questionnaire A variety ofstrategies were used to reduce loss of participants Theseinclude contacting professional bodies clinical venuesand fellow academics to try to track non-responders Lossrates are reported in table 1
InstrumentThe final questionnaire (D) had 28 questions divided
into sections using 15 tick box questions and 13 questionswith a five point Likert Scale It was developed by theauthors and has not been validated Demographic datawere collected at the time of graduation only and not onsubsequent surveys The areas explored in questionnaireD were position career moves (including motivationimpact and related factors) goals and career and studyplans Findings from the fourth and final questionnaire(D) in each cohortrsquos series are reported here
ResultsParticipantsrsquo current positions and whether these
had changed in the previous two years were explored (see table 2) and a great deal of variation is obvious Over half of two cohorts had changed jobs in the previoustwo years This move was perceived to be upward by 43(in 2002) down from 75 in 2000 Twenty to 28perceived it as downward and from 13-28 perceived it as horizontal in nature From 28-83 felt it increasedtheir salary whereas 8-36 felt their salary went downFrom 8-71 felt their salary had not changed as a result of the move
The level of personal significance of this career move was very high at 71-100 for all cohorts Their perception of the influence of their study on themove is also strong with 50-80 feeling it had amoderate or high influence However from 8-29 felttheir qualification had not influenced their success
Motivation for changing jobs was explored (see Figure1) and the percentage of participants who did so andindicated lsquoquite a bitrsquo or a lsquogreat dealrsquo for each motivatingfactor is shown While there was no consistently strongmotivator across the cohorts the desire to increase theirjob satisfaction shows most strongly with the exception of the 2002 cohort Balancing life and satisfaction are of equal importance to the 1999 and 2002 cohorts Career advancement is more predominant in recent yearsand the need for balance in their life is stronger with earlier cohorts
Table 1 Number of participants completing questionnaire A (on graduation) and questionnaire D (six years later)
On graduation Six years later lost1992 70 1998 33 531993 90 1999 36 601994 82 2000 33 591995 80 2001 32 601996 81 2002 28 70
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
40
The next questions are not tied to their career move butfocus on their current circumstances All participants (notjust those who had changed jobs) were asked to indicatetheir self perception of self esteem ability to carry outtheir role and their job satisfaction (Figure 2) The percentage rates for strong positive responses arepresented It is apparent that self esteem is lowest in the 2000 cohort and that the ability to carry out their work role is consistently strong and out strips jobsatisfaction itself
Perceptions on three beliefs about their currentworking circumstances were explored Only half to two-thirds of the participants indicated that they hadlsquosufficientrsquo control over their career and future despitehaving strong tertiary qualifications From 60-80 feltthat they had gained recognition from others Less thanhalf of them were interested in further study
Current goals of participants are presented in table 3and their intention to remain in nursing over five to 10years is shown in table 4 The most significant factors thatfacilitate or hinder their career advancement are presentedin tables 5 and 6 Approximately half of each cohortintends to remain in nursing for the next five years butfrom 19-33 are uncertain From 21-30 intend toremain 10 years but 25-41 of them are uncertain of this
No group identified a single factor that would stronglyfacilitate their career goals However the 1996 cohort wasinfluenced most by their personal situation and least bytheir qualifications with the reverse picture for the 2002
cohort The strongest factor at a little over third was jobavailability for the 1998 cohort
Barriers featured more strongly than facilitating factorswith personal situation the highest or equal highest for allcohorts Financial and other support was most importantat 24 for the 1998 cohort and much less for others Jobavailability remains a factor for 156 of the 2002 cohortdespite the nursing shortage
Participantsrsquo study activities were explored and from 3 of the 1998 cohort to 12 of the 2000 cohortwere studying in a nursing-related course six years afterentering the study following completion of theirpostgraduate qualification Within nursing 3 of onecohort was studying either at the graduate diploma or coursework masters level with a total of 8 across two cohorts at the masters thesis level and a total of 11 across three cohorts doing doctoral studies From16-25 across the cohorts were studying outside the fieldof nursing
DISCUSSIONThe study has a number of limiting factors to be
acknowledged before the results are discussed The totalsample size of 151 is small and care must be taken whengeneralising findings However as longitudinal studiesare uncommon and retention is always problematic thesmall number retained in the study is not surprisingHaving a subset within this of those who changedpositions reduces the numbers further to 59 The non-
Table 2 Position held at time of questionnaire completion ie six years after graduation () and who changed positioning last two years
in 1998 in 1999 in 2000 in 2001 in 2002n=33 n=36 n=33 n=32 n=28
RN 24 17 19 28 21CNS 27 22 23 6 29NUM 21 14 36 3 18Educator 12 8 0 12 4CNC 6 11 9 16 4Unemployed 3 11 5 6 14Other 6 17 8 28 11Changed position 36 45 55 54 29
CNS = Clinical Nurse Specialist NUM = Nurse Unit Manager CNC = Clinical Nurse ConsultantNote Missing variable percentages not included in this table
Figure 1 Changing my job was STRONGLY motivated by my desire to
Figure 2 Percentage indicating their self perception on three characteristics
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
41
validation of the instrument used might be regarded asanother limitation
However some insights were gained from the resultsThe five cohorts (1998-2002) were all surveyed six yearspost graduation and as such they are relatively seniorwithin the health care system
It is not surprising a number would have changed jobsas career advancement was a strong motivating factor inthe literature for graduate study In this study seeking jobsatisfaction is the strongest motivating factor slightlyahead of lsquoadvancing the careerrsquo This is supportedsomewhat by the findings that upward mobility and moremoney were not a result of the move as approximately athird of some cohorts felt their salary dropped or themove was downward or horizontal in nature (The drop in
salary was probably due to moving off penalty awardsbecause of shift work) This emphasis on the importanceof job satisfaction while not surprising is furtherevidence of the need for managers to seek strategies bothto measure and enhance this in the current climate ofnursing shortages However from 40-60 made thecareer move possibly downward or sideways and at noextra pay with the motivation to balance work life andfamily This reinforces the importance for managers ofinitiatives such as child care flexible rostering and othersdesigned to keep nurses in the workplace
The success in achieving more job satisfaction may beevident in the very high perceptions of their self esteemand their capacity to carry out their role But theirperception of their job satisfaction does not hold up asstrongly with only 55 of the 2002 ranking it highly This
Table 4 Do you intend to remain employed in nursing for the next five years Next 10 years
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Yes 51 30 58 28 46 29 46 29 53 22No 9 27 8 25 13 36 14 36 6 25Uncertain 33 36 19 33 33 25 29 25 28 41Note Missing variable percentages not included in this table
Table 5 Facilitate career advancement rank no 1 Highest reported item in percentage
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 21 17 16 14 6
Diversity of skills 12 6 12 11 3
Job availability 9 36 16 14 19
Motivation 9 8 13 11 14
Post grad education 6 11 17 14 25
Note Missing variable percentages not included in this table
Table 6 Main barriers to career advancement rank no 1 Highest reported percentage item
1996 n=33 1998 n=36 2000 n=33 2001 n=32 2002 n=28
Personal situation 30 33 17 18 25
Lack career path 0 17 17 18 3
Job availability 15 6 8 7 16
Experience 0 6 4 4 13
Course recognition 0 6 4 4 13
Hospital funding and support 24 14 4 7 13
Note Missing variable percentages not included in this table
Table 3 Highest reported current goal in percentage
1998 n=33 1999 n=36 2000 n=33 2001 n=32 2002 n=28Change career 27 23 25 25 19Advance career 12 6 12 10 25Increase management involvement 15 6 4 4 6Professional development 6 6 7 7 6Other 15 8 0 0 6Note Missing variable percentages not included in this table
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
42
may cause managers to review the elements that comprisejob satisfaction since a high self-esteem and capacity tofulfil the role would be part of this but the inclusion oftheir degree of autonomy might have strengthened theresults here The high level of self-esteem may beconsidered surprising but this may be due to the fact thatthe majority (66) of respondents were holding moresenior positions than that of RN in the form of specialistmanagerial or consultant roles for example
Managers may be heartened to find that the majorityhad experienced a high level of recognition from others inthe workplace and that they had sufficient control of theircareer and future The former might strengthen theirallegiance to their workplace and retention of highlyqualified nurses in whatever position must be amanagerial goal in the current climate The perceiveddegree of control over their career and future may seemsomewhat surprising since there may be some perceptionthat nurses are a relatively powerless group Howeverwhile a lack of control within a clinical or managerialwork environment may be understandable the moreglobal nature of this question may have encouraged amore positive response Certainly as the nursing shortageincreases particularly for specialist well qualified nurseswhich these participants are they may have felt a greatersense of control with more options open should theychose to change jobs
While almost half the sample had changed jobs in thetwo years prior to completing this questionnaire they mayalso have changed positions in the previous four yearsWhile there have been few changes to the career ladder inthis period in New South Wales new roles are emergingin the form of practice nurses and nurse practitioners Re-structuring in institutions is at the very least alteringtraditional career paths as middle management positionsdisappear particularly in nursing On the other hand the increased rate of casualisation (Creegan et al 2003)may generate more career opportunities for full-timeemployees at the expense of those working part-time and casually
In terms of career movement or job change animportant aspect that was not explored was whether theirmove was out of nursing However there is evidenceemerging that nurses are actively being recruited intopositions outside nursing and indeed the health industryas a whole (Duffield et al 2004 Duffield and Franks2001) This trend is likely to be exacerbated by registerednurses who are not only very experienced but alsopossess a higher degree
It is perhaps not surprising that only a quarter or lessof the participants felt their graduate qualification playeda major role in the success of their job application since itwas achieved six years prior Their subsequent workexpertise may well have had a greater impact Also forthe latter cohorts over half had completed an additionalgraduate course which they may have seen as havingmore impact These latter cohorts are likely to be a
younger population and their responses signal what mightbe seen as a pattern of lsquolife longrsquo learning or efforts tocarry out some form of career development plan Again aweakness is that the study did not determine if thecompleted courses were outside nursing However it diddetermine that from 16-25 of each cohort was studyingoutside nursing and only 3-12 within nursing Thisfinding is supported by other Australian work whichshows many nurses gained non-nursing qualificationsprior to moving to positions outside the health industry(Duffield et al 2004)
The intention of the respondents to remain in nursingwill be of interest to workforce planners About half of allcohorts intend to remain five years which is not highsince they are only six years out from having gained a significant professional qualification The level ofuncertainty in staying is 20-30 This fits with thepattern of doing study outside nursing and again fits witha trend for nurses to move outside the nursing field(Duffield et al 2004)
Not surprisingly in the intention to remain 10 yearsthe numbers drop to 22-30 which would take accountthe fact that more have reached retirement age (OrsquoBrien-et al 2004) as well as the continued shift out ofnursing Understandably the number indicating they areuncertain of their intention rises to 41 in 2002 but wasalso at 36 in 1998 so it is not directly attributable to thecurrent difficult work environment
In the context of factors that would facilitate theircareer advancement it seems over the time of the studythe personal situation has become less important whichmay reflect some of the initiatives regarding flexiblerostering increased part time opportunities and child careor the passage of time
Job availability a strong factor for the 1999 cohort issubstantial at 19 for the 2002 cohort Since the nursingshortage reduces the impact of this factor in mostcircumstances it may be the lack of availability ofmanagement positions especially middle managementthat are the concern Alternatively it may be that it is ofimportance to those seeking positions outside nursingThe 2002 cohort puts more emphasis on the impact ofpostgraduate education reflected in their higher levels ofcompletion of courses and studying both inside and out ofnursing Again this may reflect the trend for the morerecent groups who are presumably younger to plan andwork towards a career following a life long learning trackThese inter-generational differences will continue tochallenge employers to provide ever changing andchallenging workplaces (Creegan et al 2003)
In Australia as in other developed countries thenursing shortage and ageing work force make itincreasingly imperative for administrators to lsquounderstandrsquotheir workforce and what motivates them to study tomove and hopefully to stay in the health service sectorThey are an invaluable asset
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
43
REFERENCESAiken LH Clarke SP Sloane DM Sochalski JA Busse R Clarke HGiovannetti P Hunt J Rafferty AM and Shamian J 2001 Nursesrsquo reportson hospital care in five countries Health Affairs 2043-53
Australian Institute of Health and Welfare 2001 Nursing Labour Force 1999AIHW cat no HWL 20 Canberra1-115
Bethune E and Jacklin N 1997 Critical thinking skills The role of priorexperience Journal of Advanced Nursing 26(5)1005-12
Boore J 1996 Postgraduate education in nursing A case study Journal ofAdvanced Nursing 23(3)620-629
Bourke RJ 2003 Survivors and victims of hospital restructuring anddownsizing Who are the real victims International Journal of NursingStudies 40(8)903-909
Chaboyer W and Retsas A 1996 Critical care graduate diploma Nursingstudents needs identified in evaluation Australian Critical Care 9(1)15-19
Creegan R Duffield C and Forrester K 2003 Casualisation of the nursingworkforce in Australia Driving forces and implications Australian HealthReview 26(1)201-208
Davis BD 1993 An international approach to masterrsquos-level preparation forclinical nurse specialists Journal of Advanced Nursing 18(9)1429-33
Dexter P Applegate M Backer J Claytor K Keffer J Norton B andRoss B 1997 A proposed framework for teaching and evaluating criticalthinking in nursing Journal of Professional Nursing 13(3)160-7
Diers D and Bozzo J 1997 Nursing resource definition in DRGs NursingEconomic$ 15(3)124-30
Donoghue J Pelletier D and Duffield C 2002 Recognition of prior learningas university entry criteria is successful in postgraduate nursing studentsInnovation in Education and Training International IETI 39(1)54-62
Duffield C and Franks H 2001 The role and preparation of first-line nursemanagers in Australia Where are we going and how do we get there Journalof Nursing Management 9(2)87-91
Duffield C and OrsquoBrien-Pallas L 2002 The nursing workforce in Canada and Australia Two sides of the same coin Australian Health Review 25(2)136-144
Duffield C Aitken L OrsquoBrien-Pallas L and Wise W 2004 Nursing A stepping stone to future careers Journal of Nursing Administration 34(5)238-245
Fagin CM 2001 When care becomes a burden Diminishing access toadequate nursing wwwmilbankorg010216faginhtml 2-24
Fraser M and Titherington R 1991 Where are they now The career paths ofgraduates from post-registration degrees in nursing in England InternationalJournal of Nursing Studies 28(3)257-265
Girot E 2000 Graduate nurses Critical thinkers or better decision makersJournal of Advanced Nursing 31(2)288-297
Jakob SM and Rothen HU 1997 Intensive care 1980-1995 Change inpatient characteristics nursing workload and outcome Intensive CareMedicine 23(11)1165-1170
Jordan S 2000 Educational impact and patient outcomes Exploring the gapJournal of Advanced Nursing 31(2)461-471
OrsquoBrien-Pallas L 2000 Where to from here Canadian Journal of NursingResearch 33(4)3-14
OrsquoBrien-Pallas L Thomson D Alksnis C and Bruce S 2001a Theeconomic impact of nurse staffing decisions Time to turn down another roadHospital Quarterly 442-50
OrsquoBrien-Pallas L Duffield C and Alksnis C 2004 Who will be there tonurse Retention of nurses nearing retirement Journal of NursingAdministration 34(6)298-302
Pelletier D Donoghue J Duffield C and Adams A 1998a The impact ofgraduate education on the career paths of nurses Australian Journal ofAdvanced Nursing 15(3)23-30
Pelletier D Donoghue J Duffield C and Adams A 1998b Nursesrsquoperceptions of their professional growth on completion of two years ofpostgraduate education Australian Journal of Advanced Nursing 16(2)26-32
Pelletier D Donoghue J Duffield C Adams A and Brown D 1998c Whyundertake higher degrees in nursing Journal of Nursing Education 37(9)422-4
Pelletier D Donoghue J and Duffield C 2002 Australian nursesrsquo perceptionof the impact of their postgraduate studies on their patient care relatedactivities Nurse Education Today 23(6)434-42
Pelletier D Duffield C Gallagher G Soars L Donoghue J and Adams A1994 The effects of graduate education on clinical practice and career paths A pilot study Nurse Education Today 14(4)314-321
Sandor MK Clark M Campbell D Rains AP and Cascio R 1998Evaluating critical thinking skills in a scenario-based community health courseJournal of Community Health Nursing 15(1)21-9
Simsen B and Holyroyd E 1997 Developing a framework for the future A qualitative perspective on postgraduate nursing education in Hong KongNurse Education Today17(5)370-375
Thurber FW 1988 A comparison of RN students in two types of baccalaureatecompletion programs Journal of Nursing Education 27(6)266-273
Trewthewie D 1999 Six registered nursesrsquo perceptions of their ability to use their master of nursing knowledge in their practice Unpublished study submitted for the Master of Nursing Degree Flinders University South Australia
Vaughan-Wrobel BC OrsquoSullivan P and Smith L 1997 Evaluating criticalthinking skills of baccalaureate nursing students Journal of Nursing Education36(10)485-8
Watson P and Wells N 1987 Nursesrsquo attitudes towards the advantages ofmasters degree preparation in nursing Journal of Nursing Education 2663-68
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
44
Tessa Pascoe MRCNA RN RM BN BCommEd Policy AdvisorNursing in General Practice Project Royal College of NursingAustralia Canberra Australian Capital Territory Australia
tessarcnaorgau
Elizabeth Foley FRCNA AFCHSE RN MEd Director NursingPolicy and Strategic Developments Royal College of NursingAustralia Canberra Australian Capital Territory Australia
Ronelle Hutchinson BA (Hons) Policy Advisor Nursing inGeneral Practice The Royal Australian College of GeneralPractitioners South Melbourne Victoria Australia
Ian Watts BSW DipSocPlan CertHealthEcon National ManagerGP Advocacy and Support The Royal Australian College ofGeneral Practitioners South Melbourne Victoria Australia
Lyndall Whitecross MBBS FRACGP Grad Dip Family Med GPAdvisor The Royal Australian College of General PractitionersSouth Melbourne Victoria Australia
Teri Snowdon BA(Hons) BSW(Hons) NSW ARMIT NationalManager Quality Care and Research The Royal Australian Collegeof General Practitioners South Melbourne Victoria Australia
Accepted for publication December 2004
THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
Key words general practice workforce roles primary care nursing workforce practice nurses
ABSTRACT
ObjectiveTo describe the workforce characteristics and
current responsibilities of nurses working inAustralian general practice settings
Design Survey research combining qualitative and
quantitative data collected through telephone interview
Subjects222 enrolled (RN Division 2 in Victoria) and
registered nurses (RN Division 1 in Victoria) working ingeneral practice in rural and urban areas of Australia
ResultsGeneral practice nurses in Australia are likely to be
RNs (847) who work on a part-time basis (753)in a medium to large practice (937) Often the nursehas worked less than five full time equivalent years(523) in a general practice environment and is likelyto work in a practice where at least one other nurseworks (644) The nurse is likely to have some post-basic formal education (659) and to haveparticipated in professional development in the pasttwo years (949) The nurse performs a diverse rangeof activities within the general practice No substantialdifferences were found in the workforce characteristicsor role of urban and rural general practice nurses
Conclusion It appears that nurses working in general practice
are no longer the lsquohandmaidenrsquo to the doctor but areprofessionals who perform a vast range of clinicaladministrative and organisational responsibilitieswithin the general practice primary health care setting
INTRODUCTION
Registered and enrolled nurses working in generalpractices in Australia enhance the quality ofprimary health care provided to the general public
However the value of general practice nursing has notalways been recognised and historically the nurse wasviewed as a lsquohandmaidenrsquo to the doctor
Increasingly Australian general practice nursing isbeing recognised by the nursing and medical professionsas a specialised area of nursing General practice nursingis supported by the Australian Government through theNursing in General Practice 2001 Budget Initiative whichincludes a financial incentive to GPs in areas of workforcepressure to employ a practice nurse and through the recentMedicarePlus package The MedicarePlus packageextends this incentive to further urban areas of workforcepressure and has introduced general practice nurse MBSitems Through this initiative the Australian Governmenthas given overt recognition to general practice nursesrsquoroles in coordinating clinical care tasks supporting bettermanagement of chronic diseases undertaking populationhealth activities and providing clinical support whichenables GPs to focus on diagnosis and clinical care (seeCondon et al 2000 Lockwood and Maguire 2000Bonawit and Watson 1996 Patterson et al 1999 for furtherdiscussion on the activities undertaken by nurses inAustralian general practices)
Despite this increased enthusiasm and supportrelatively little is known about the working lives of nursesemployed in general practice in Australia While a fewsmall research studies have been conducted in Australiathese have focused on specific geographic areas and nonational study of the workforce characteristics and rolesof nurses in general practice has been undertaken
The Royal College of Nursing Australia (RCNA) andthe Royal Australian College of General Practitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
45
(RACGP) have completed a project funded by the
Australian Government Department of Health and Ageing
to explore the current and future roles of nurses working
in general practice This paper will discuss the results
from a national telephone survey of nurses working in
general practice carried out as one of the project
activities Specifically the workforce characteristics and
the roles and activities of nurses working in general
practice will be examined
METHODOLOGY
A survey of nurses working in general practice was
designed drawing on published and unpublished research
undertaken in Australia and internationally on the role
and educational needs of nurses in general practice (see
Vincent et al 2002 Hanna 2001 Condon et al 2000
Meadley 2000 Patterson et al 1999 Ross et al 1994) The
survey contained 19 quantitative and qualitative questions
focusing on workforce characteristics educational
background and needs current nursing activities and
future aspirations
The survey was administered to enrolled and registered
nurses currently working in general practice settings in
Australia The convenience sample of nurses was
recruited through a national marketing campaign Nurses
volunteering for the study were surveyed by telephone
outside of working hours The survey took approximately
15-25 minutes to complete
As part of the research brief from the Australian
Government at least 50 of the sample was to be drawn
from rural or remote areas of Australia The standard
classification for geography employed for the survey was
the Rural Remote and Metropolitan Area (RRMA)
classification system Survey participants were classified
into a RRMA category (capital city other metropolitan
rural or remote areas) based on the location of their
primary general practice employer Due to the small
number of participants from remote areas the categories
lsquoruralrsquo and lsquoremotersquo were collapsed into one ruralremote
category for reporting purposes
RESULTS
Workforce characteristicsThe resulting sample for the survey included 222
nurses currently working in general practice with 586of the sample being drawn from rural and remote areas ofAustralia Table 1 displays the RRMA classifications ofruralremote and capitalmetropolitan for the nursersquos mainpractice by the State and Territory of the practice
Table 2 outlines the breakdown in the sample by nurseclassification The majority of the sample consisted ofregistered nurses (n=188) with relatively few enrollednurses (n=34) participating This ratio of registered toenrolled nurses appears consistent with other research ongeneral practice nursing in Australia which found highnumbers of RNs compared with ENs (see Patterson et al1999 Bonawit and Watson 1996)
The survey results clearly indicate that the majority ofthe general practice nursing workforce are part-timeemployees and this is consistent across rural and urbanareas of Australia Table 3 demonstrates that 753 of thesample work less than 35 hours per week
While the general practice nursing workforce is largelyemployed on a part-time basis many of these nurses arealso relatively new to nursing within a general practiceenvironment Table 4 indicates that just over half thesample (523) have worked in general practice nursingfor less than five full time equivalent (FTE) yearsHowever 261 of the sample have an extended history ofworking in general practice for more than ten years Thisratio of experience appears to be relatively consistentregardless of the rurality of the practice in which the nurseis employed
The Practice Nurse Incentive Program may havefacilitated a number of recent recruits to general practicenursing in areas of high workforce need and these nursesare likely to fall into the lsquoless than onersquo or lsquoone to fiversquo
Table 1 Percentage of sample by RRMA classification of main practice and State or Territory of main practice
NSW VIC QLD SA WA TAS NT ACT Total
Capitalmetro (RRMA 1-2) 36 125 117 32 68 14 00 22 414
Ruralremote (RRMA 3-7) 90 104 212 54 27 85 09 05 586
Total 126 229 329 86 95 99 09 27 1000
Table 2 Percentage of sample by nurse classification and RRMAclassification of main practice
Nurse Rural Capital Total classification remote metro areas
Registered nurse 862 826 847
Enrolled nurse 138 174 153
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
46
year categories for this survey Alternatively it is possiblethat general practice nursing as an occupation experiencesa high staff turnover with nurses entering general practicewith the intention of remaining for a short period (due tothe attractiveness of part time work for example) Withoutlongitudinal data about the general practice nursingworkforce this remains speculative
Table 5 demonstrates that when asked to identify theregistration status of other nurses they work with ingeneral practice nearly two thirds of the sample (644)responded that they work in a practice where at least oneother nurse works However over a third of the sample(356) indicated that they are the sole nurse in theirpractice Interestingly there appear to be substantiallymore nurses working alone in metropolitan areas than inrural areas however the study was not designed todetermine the reasons for this
When asked to identify the number of GPs theparticipants worked with (including full-time part-timecasual and contracted GPs) at their main practice ofemployment just under half the nurses sampled (473)worked in medium sized practices of two to five GPs Asimilar proportion (464) were employed in largepractices and worked with more than six GPs A relativelysmall percentage (63) of those surveyed worked in soloGP practices Table 6 suggests that nurses in Australiangeneral practice tend to be employed in medium to largepractices Bonawit and Watson (1996) also found thatVictorian general practice nurses were most commonlyemployed in practices with three or more GPs General
practice nurses are more likely to work in a medium sizedpractice in rural locations and in large practices in urbanlocations This may reflect fewer numbers of largepractices in rural areas with the natural result that fewernurses are employed in such practices
Regarding the formal education undertaken sinceenrolmentregistration as a nurse 342 of the nursessampled had not undertaken any additional formaltraining However this still leaves a substantial number ofnurses who had undertaken additional formal trainingincluding undergraduate degrees (78) postgraduatediplomascertificates (11) and masters degrees (2) In relation to the attainment of additional formaleducation rural and urban general practice nurses appearto be very similar
Most (949) of the nurses surveyed have beenengaged in some form of professional development in thepast two years Table 7 indicates that over half of thisprofessional development (514) was accessed throughin-services conferences study days workshops andseminars Other forms of professional development withsignificant nurse participation included membership withprofessional associations (89) and professionaldevelopment accessed through general practice nursenetwork meetings (77) A number of other professionaldevelopment opportunities were identified and theserepresented a varied mix of activities accessed throughlocalised services There appeared to be relatively few
Table 3 Percentage of sample by hours usually worked as anurse in general practice by RRMA classification of main practice
Hours per week Rural Capital Total remote metro areas
Less than 17 200 141 176
17-35 546 620 577
More than 35 254 239 248
Total responses 1000 1000 1000
Table 6 Percentage of sample by number of GPs working innursersquos (main) practice by RRMA classification of main practice
Number of GPs Rural Capital Total remote metro areas
One 77 43 63
Two-Five 554 359 473
More than six 369 598 464
Total responses 1000 1000 1000
Table 4 Percentage of sample by full-time equivalent years workedas a nurse in general practice by RRMA classification of main practice
FTE years Rural Capital Total remote metro areas
Less than one 108 54 86
1-5 438 435 437
6-10 231 196 216
More than 10 223 315 261
Total responses 1000 1000 1000
Table 5 Percentage of sample by registration status of the nurses workingwith survey participants by RRMA classification of main practice
Nurse classification Rural Capital Total of colleague remote metro areas
None (solo nurse) 308 424 356
Other registered nurses 462 478 468
Other enrolled nurses 100 54 81
Both registered andenrolled nurses 131 43 95
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
47
differences between the types of professional developmentundertaken by rural and urban nurses working in generalpractice The RACGPRCNA Nursing in General PracticeFinal Report submitted to the Australian GovernmentDepartment of Health and Ageing called for a nationallyconsistent approach to education for general practicenurses in Australia
The current role of general practice nursesIn order to identify the current role of nurses working
in general practice the survey participants were asked toidentify how frequently they undertook a variety ofactivities at work either lsquodaily-weeklyrsquo lsquomonthlyrsquolsquooccasionallyrsquo or lsquonot at allrsquo
Table 8 identifies the percentage of the sample whoperformed each activity For ease of analysis the responsesto lsquodaily-weeklyrsquo lsquomonthlyrsquo and lsquooccasionallyrsquo have beencollapsed in this table to the percentage of nurses wholsquoperformrsquo those activities This is compared with thepercentage of the activities that the nurses lsquonever performrsquo
The 32 activities which are shaded in table 8 have beenidentified as the core activities of a nursersquos role in generalpractice as over 75 of the sample performed these atleast occasionally Whilst 75 is in some ways anarbitrary number it was theorised that if a substantialmajority or over 75 of the nurses surveyed undertookthese activities then these activities could be said to beintegral to the average role of a nurse working in
Australian general practice The non-shaded activitiesrepresent additional activities that whilst not central tothe role are valuable activities that some nurses doundertake
It is clear that a number of the National Health Priorityareas as identified by the Australian GovernmentDepartment of Health and Ageing are incorporated intothe core roles of nurses in general practice It is evidentthat nurses are providing care in asthma diabetes andcardiovascular health in general practice However theNational Health Priority areas of cancer control mentalhealth injury prevention and arthritis and musculoskeletalconditions do not currently form a core component of thecurrent role of nurses in general practice
If the core activities of nurses working in generalpractice are examined in relation to the RRMAclassification of the main practice in which the nurse isemployed it becomes evident that nurses working in rurallocations are undertaking essentially the same coreactivities as nurses working in urban locations
As seen in Table 9 those core activities in whichperformance varies by a minimum of 10 between ruraland urban nurses have been shaded Whilst the coreactivities of rural and urban general practice nurses appearto be essentially the same there are two notabledifferences Substantially more rural nurses perform earsyringing than do urban nurses Also of interest is thedisparity between the percentage of rural and urban nursesundertaking sterilisation activities There is over 10difference in the number of urban nurses performing thisactivity when compared with their rural counterparts Thisdifference needs to be considered in the context of thearrangement and availability of other resources to generalpractices in rural locations It is possible that ruralcommunities may have developed alternative structures forensuring sterile equipment is available including usingmore disposable equipment or using resources such as thelocal hospital central sterilising unit or a central sterilisingfacility
LIMITATIONSThe overall representativeness of the sample for the
survey is not known Whilst it could be argued that thesample size is relatively small there exists no baselinedata for identifying the absolute population of generalpractice nurses in Australia Of consideration is the largeproportion of ruralremote nurses in the sample It seemsunlikely that the population of general practice nurses inAustralia would be skewed with so many employed inruralremote areas However given the need to exploregeographic impacts on the role of the nurse in the contextof the project as a whole it was important that asignificant proportion of rural and remote nurses besampled
There appeared to be reasonable representation fromeach state and territory with the exception of New South
Table 7 Percentage of sample by type of professional developmentcompleted in past two years by RRMA classification of main practice
Type of professional Rural Capital Total development remote metro areas
In-services conferences study days or seminars 532 488 514
Via membership of professional associations 90 88 89
Network meetings with other general practice nurses 69 88 77
Onlinedistance education 43 32 38
On-the-job training by GP 48 24 38
Reading professional journals 32 40 35
On-the-job training by nurses 11 24 16
On-the-job training by practice manager 11 08 10
Other 122 144 131
None 43 64 51
Total responses 1000 1000 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
48
Table 8 Activities undertaken by nurses percentage of respondents
Activities undertaken Perform Never Totalperform perform
Liaise with other health professionals and community organisations 995 05 1000
Monitor vital signs 995 05 1000
Wound care and management 977 23 1000
Minor procedures 977 23 1000
Monitorassess sick patients 973 27 1000
First aid or emergency procedures 973 27 1000
Clinical data entry and retrieval 968 32 1000
Removal of sutures 968 32 1000
Stocksstores management 968 32 1000
Triage 968 32 1000
Provide oxygennebuliser therapy 964 36 1000
Communicate test results to GP and patients 959 41 1000
Cold chain monitoring 941 59 1000
Injectionsmedication administration 941 59 1000
Reception duties 928 72 1000
Maintaining updating policies and procedures 928 72 1000
Pulmonary assessments 923 77 1000
Immunisation 910 90 1000
Sterilisation 905 95 1000
Cardiac assessment 905 95 1000
Undertake patient counseling 892 108 1000
Referral management 892 108 1000
Maintenance of S8 drugs and Doctorrsquos bag 865 135 1000
Pathologyspecimen collection 865 135 1000
Manage recall register 856 144 1000
Communicate new research to other staff 829 171 1000
Diabetes education 806 194 1000
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 775 234 1000
Developmaintain clinical reports 770 230 1000
Diabetes assessment and management 766 234 1000
Chronic disease management 757 243 1000
Asthma education 752 248 1000
Ear syringing 734 266 1000
Injury prevention education 716 284 1000
Applicationremoval of plaster 703 297 1000
Assist with research or clinical audits 676 324 1000
Full physical assessments 626 374 1000
Dietweight management 622 378 1000
Cardiovascular health and strokes education 617 383 1000
Drug and alcohol education 581 419 1000
Arthritis and musculoskeletal conditions education 554 446 1000
Cancer education 550 450 1000
Case management including case conferencing 514 486 1000
Antenatal checks 482 518 1000
Lactation advicesupport 450 550 1000
Audiometry assessment 432 568 1000
Child health assessment 423 577 1000
Mental health assessment 383 617 1000
Mental health education 383 617 1000
Family planning 297 703 1000
Womenrsquos health 261 739 1000
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
49
Table 9 Percentage of sample undertaking core activities by RRMA classification of main practice
Activities undertaken Ruralremote Capitalmetro Totalperform perform perform
Liaise with other health professionals and community organisations 992 1000 995
Monitor vital signs 992 1000 995
Wound care and management 969 989 977
Minor procedures 969 989 977
Monitorassess sick patients 969 978 973
First aid or emergency procedures 962 989 973
Clinical data entry and retrieval 977 957 968
Removal of sutures 962 978 968
Stocksstores management 954 989 968
Triage 962 978 968
Provide oxygennebuliser therapy 954 978 964
Communicate test results to GP and patients 962 957 959
Cold chain monitoring 931 957 941
Injectionsmedication administration 962 913 941
Reception duties 931 924 928
Maintaining updating policies and procedures 923 935 928
Pulmonary assessments 931 913 923
Immunisation 915 902 910
Sterilisation 862 967 905
Cardiac assessment 923 880 905
Undertake patient counseling 877 913 892
Referral management 854 946 892
Maintenance of S8 drugs and Doctorrsquos bag 869 859 865
Pathologyspecimen collection 892 826 865
Manage recall register 831 891 856
Communicate new research to other staff 862 783 829
Diabetes education 800 815 806
Enhanced Primary Care activities such as Health Assessments Care Planning or Home Visits 777 772 775
Developmaintain clinical reports 769 772 770
Diabetes assessment and management 769 762 766
Chronic disease management 723 804 757
Asthma education 769 728 752
Ear syringing 785 663 734
Wales with only 126 of the nurses sampled beingemployed there Close examination revealed that only36 of the sample was drawn from metropolitan NSW -an under-representation of nurses given the largepopulation in the Sydney region However there is nosubstantial reason to suspect that the sample is notrepresentative of the larger general practice nursingpopulation
CONCLUSIONThe results from the national telephone survey provide
a description of the typical general practice nurse inAustralia Overall a typical general practice nurse is anRN who works on a part-time basis in a medium to large
practice Most often the nurse has worked less than fiveyears (full time equivalent) in the general practiceenvironment and is likely to be working in a generalpractice where at least one other nurse works TheAustralian general practice nurse is likely to have somepost-basic formal education and is likely to haveparticipated in professional development in the past twoyears
One of the most interesting results to emerge from thissurvey is the apparently limited impact of rurality on theworkforce characteristics and roles of nurses working ingeneral practice in Australia There were essentially nosubstantial differences in the workforce characteristicsbetween nurses who worked in capitalmetropolitan areas
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
RESEARCH PAPER
50
and those who worked in rural and remote areas When itcame to the current role of the nurse in general practicethe core roles were essentially the same for rural and urbannurses
REFERENCESBonawit V and Watson L 1996 Nurses who work in general medicalpractices A Victorian survey Australian Journal of Advanced Nursing13(4)28-34
Condon J Willis E and Litt J 2000 The role of the practice nurse Anexploratory study Australian Family Physician 29(3)272-277
Hanna L 2001 Continued neglect of rural and remote nursing in AustraliaThe link with poor health outcomes Australian Journal of Advanced Nursing19(1)36-45
Lockwood A and Maguire F 2000 General practitioners and nursescollaborating in general practice Australian Journal of Primary HealthInterchange 6(2)19-29
Meadley L 2000 Applied project in clinical education Newcastle NSWUniversity of New England
OrsquoConnor M and Parker E 1995 Health promotion principles and practice inthe Australian context Sydney Allen and Unwin
Patterson E Del Mar C and Najman J 2000 Medical receptionists ingeneral practice Who needs a nurse International Journal of NursingPractice 6(5)229-236
Ross RM Bower PJ and Sibbald BS 1994 Practice nurses Characteristicsworkload and training needs British Journal of General Practice 44(378)15-18
Vincent D Hogan C and Sweeney M 2001 Clinical nurse in generalpractice project report Melbourne Royal Australian College of GeneralPractitioners
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
SCHOLARLY PAPER
51
Angela Firtko RN DipAppSci MHlthScEd CertCardiacNursingAssociate Lecturer School of Nursing Family and CommunityHealth College of Social and Health Sciences University ofWestern Sydney New South Wales Australia
Debra Jackson RN PhD Professional Fellow School ofNursing Family and Community Health College of Social andHealth Sciences University of Western Sydney New SouthWales Australia
debrajacksonuwseduau
Accepted for publication December 2004
DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OFWHISTLEBLOWING
Key words whistleblowing nursing ethics misconduct media
ABSTRACT
BackgroundPatient advocacy and a desire to rectify misconduct
in the clinical setting are frequently cited reasons forwhistleblowing in nursing and healthcare
AimThis paper explores current knowledge about
whistleblowing in nursing and critiques currentdefinitions of whistleblowing The authors draw onpublished perspectives of whistleblowing including themedia to reflect on the role of the media in healthrelated whistleblowing
ConclusionWhistleblowing represents a dilemma for nurses It
strikes at the heart of professional values and raisesquestions about the responsibilities nurses have tocommunities and clients the profession andthemselves In its most damaging formswhistleblowing necessarily involves a breach of ethicalstandards particularly confidentiality Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services thenthe ends definitely justify the means
INTRODUCTION
When considering whistleblowing as an optionfor nurses many questions arise Thesequestions include
bull Whose interests are being served
bull Who could be damaged
bull What is the motivation for whistleblowing
bull What are the consequences of whistleblowing to the whistleblowers and the organisation
bull Is there any other way to draw attention to the issue
bull Will the act of whistleblowing solve the problem
bull Do the ends justify the means
Aim of this paperThis paper aims to explore current knowledge about
whistleblowing in relation to nursing The specificobjectives are to
bull Propose a definition of whistleblowing that is compatiblewith nursing
bull Examine the dilemmas associated with whistleblowing asit relates to nursing
bull Explore the repercussions of whistleblowing asrepresented in the literature
bull Draw on key published perspectives about The BristolAffair to focus on the role the media can play in healthrelated whistleblowing
Defining whistleblowingWhistleblowing may seem to be a taken-for-granted
term that has a clear meaning and little room forinterpretation However a search of published definitions
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
reveals various understandings and meanings associatedwith the term In their paper on whistleblowing Ahernand McDonald (2002) defined it as any reporting ofmisconduct in the workplace Elsewhere McDonald andAhern (2002 p16) define nurse whistleblowers as lsquoanurse who identifies an incompetent unethical or illegalsituation in the workplace and reports it to someone whomay have the power to stop the wrongrsquo These definitionsare problematic because they do not delineate betweenreporting to outside agencies such as the media andreporting undesirable events according to acceptedorganisational guidelines In effect the aforementioneddefinitions position reporting questionable practices orundesirable outcomes to individuals groups or bodiesthat are part of a discipline or an organisationrsquos usualproblem-solving strategy as whistleblowing
Definitions that position all forms of reporting aswhistleblowing raise the issue of whether whistleblowingis internal or external to an organisation It is ourcontention that internal reporting - that is reportingwhich is adhered to as part of guidelines for employeessuch as completion of incident forms for poor patientoutcomes or unforeseen events verbal reporting to linemanagers or other appropriate staff is ideal professionalconduct and should be encouraged Such reporting iscarried out in the interests of quality improvementincident debriefing clinical supervision and maintenanceof professional standards and integrity in practice
Describing internal reporting of undesirable outcomesor poor practice as whistleblowing could make it seem insome way undesirable or as having detrimentalramifications and therefore something to be avoidedAlerting professional bodies or to structures internal to anorganisation about poor practice or other issues ofconcern is wholly acceptable and desirable behaviour Forone thing it does not necessarily involve a breach ofconfidentiality which occurs when external avenues areinvolved Furthermore using approved internal orprofessional problem-solving structures as mechanisms todraw attention to internal problems and to improvepractice is the minimum required standard for all healthprofessionals including students and should be anaccepted work-related event
On the contrary far from being a typical and commonevent whistleblowing is an extraordinary event It isassociated with stress and personal risk (Ahern andMcDonald 2002) It may involve the whistleblowerundergoing personal inner conflict about the decision to blow the whistle and it may be associated withbreaching ethical codes such as confidentiality In orderto justify such a breach all appropriate internal avenuesthat exist to right the wrong must first be exhausted(Fletcher et al 1998) Fletcher et al (1998) also states thatwhere internal avenues have not been exhaustedwhistleblowing can raise concerns about whistleblowermotives and suggests revenge and desire for attention aspossible motivating factors
Understanding the public nature of whistleblowing iscrucial to understanding the risks and dilemmasassociated with the phenomenon Wilmot (2000 p1051)define whistleblowing as lsquothe public exposure oforganisational wrongdoingrsquo but also acknowledged itsinherent antagonistic nature when he positioned it as lsquopartof a spectrum of increasingly confrontative actionsagainst miscreant organisations by their employeesrsquo(Wilmot 2000 p1051) Dawson (2000 p2) provided amore detailed definition and raised the issue of privilegedinformation He defined whistleblowing as a lsquodeliberatevoluntary disclosure of individual or organisationalmalpractice by a person who has had privileged access todata events or information about an actual suspected oranticipated wrongdoing within an organisation that iswithin its ability to controlrsquo (Dawson 2000 p2)
When considering whistleblowing in nursing wesought a definition that captured the idea that it involvestaking privileged information to an individual or bodywho would not normally be involved with organisationalproblem-solving Thus for the purposes of this paper weconsider whistleblowing to be the reporting ofinformation to an individual group or body that is notpart of an organisationrsquos usual problem-solving strategyWhistleblowing is a phenomenon where a party or partiestake matters that would normally be held as confidentialto an organisation outside that organisation despite thepersonal risk and potentially negative sequelae associatedwith the act
The whistleblowerIliffe (2002) constructed whistleblowing as an imposed
rather than a chosen situation She suggested thatwhistleblowers are lsquoordinaryrsquo people who find theywitness or otherwise become aware of situations thatforce them into a decision of having to speak out orremain silent Both decisions carry consequencesWhistleblowers are generally cast in the literature as braveand courageous individuals who act to maintainstandards against the might of an organisation (Jacksonand Raftos 1997) and who do so sometimes at greatpersonal cost (Iliffe 2002) An alternative view and onethat is sometimes promulgated by targeted organisationsis that whistleblowers are malcontents who will stop atnothing to pursue their own agenda regardless of thedestructive and negative sequelae for colleagues andorganisations
In their discussion on whistleblowing in nursingMcDonald and Ahern (2002) proposed the concept of thenon-whistleblowers which she defined as a nurse who onidentifying incompetence illegal or unethical practicesadopts methods other than whistleblowing to resolve thesituation or address the allegations
Possible strategies include talking directly with anursing unit manager about the issues or reporting theissues on an incident form or similar document(McDonald and Ahern 2002) We suggest that these
SCHOLARLY PAPER
52
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
actions are in keeping with reporting and reflectionassociated with maintaining professional standards andintegrity in practice and would hesitate to label personsengaging in these activities as non-whistleblowers
Organisational culture and whistleblowingHealth care institutions are hierarchical structures and
so carry all the entrenched flaws and difficulties of suchstructures Furthermore some organisations create andmaintain cultures in which mistrust abounds Speedy(2004 p156) states that when employee trust is violatedlsquoa climate of suspicion and vigilance against wrongdoingrsquois created These organisations create cultures of reducedloyalty and can cause employees to feel violated betrayedand liable to seek reprisal (Speedy 2004) which in turnbecomes a motive or factor in whistleblowing In makingthe plea that lsquowhen all is said as done the whistleblowermust blow the whistle for the right moral reasonrsquo Fletcheret al (1998 p2) positions examination of and reflectionon the motives for whistleblowing as crucial steps fornurses considering whistleblowing
Speedy (2004) also suggested that health careorganisations may have a greater potential for abuse ofworkers than other organisations The abuse can take theform of marginalising and silencing people and in general making it difficult for people to speak out againstissues or practices that trouble them (Speedy 2004)Health professionals are socialised into a culture ofsilence (Jackson and Raftos 1997) which contributes to aclimate in which whistleblowing rightly or wrongly isone of the few avenues open to health professionals who are troubled by poor practice and see a pressingneed for change
The dilemmas associated with whistleblowingWhistleblowing is represented in the literature as an
avenue of last resort (Jackson and Raftos 1997 Wilmot2000) Wilmot (2000) states that whistleblowing can belikened to a spectrum At one end of the spectrum is theworse case scenario where the effects of whistleblowingare disruptive and experienced as negative to allconcerned On the other end of the spectrumwhistleblowing may inflict minimal scars on theorganisation or stakeholders (Wilmot 2000)
In an ideal world there would be no dilemmaassociated with blowing the whistle on poor practice orother institutional short-comings The dilemmas arisewhen nurses go outside organisations with privilegedinformation in an attempt to have their concernsaddressed However it can be argued that nurses are leftwith little choice The literature provides numerousaccounts of whistleblowing employees who have mademany attempts to rectify wrong doing through internalchannels however when they are unsuccessful they turnto external channels in an effort to be heard (Jackson andRaftos 1997) This type of whistleblowing has been
described as a lsquomorally courageous actionrsquo (Fletcher et al1998 p2)
Primarily whistleblowing raises dilemmas for nursesaround issues such as patient advocacy and duty of careand can raise conflicts around organisational andprofessional allegiances Tensions arise between theperceived need to effectively problem-solve and the needto adopt a lsquodamage-controlrsquo stance in terms of damage to institutions Undermining public institutions such ashospitals and health facilities has far-reaching effects to the community the institution serves The lack ofcommunity confidence in and antipathy towardsinstitutional staff (who may not have any association withthe alleged poor practices) that can arise as a result ofwhistleblowing can be devastating Furthermorequestions about natural justice arise in that individualsand organisations may be subject to public attack in waysthat are very difficult to respond to
Thus whistleblowing presents nurses with aconundrum Brodie (1998) describes it as a moraldilemma stating that nurses choosing to blow the whistlelsquodo so out of social consciousness and moralcommitmentrsquo (Brodie 1998 p1) Patient advocacy is alsocommonly associated with whistleblowing acts (Ahernand McDonald 2002 Mallik 1997) Wilmot (2000)suggested that whistleblowing can be a calculated act ofsabotage which raises another view However regardlessof motive it is undoubtedly a most difficult decision that has moral practical ethical and professionalimplications (Wilmot 2000) Once the decision is taken toblow the whistle the accusations can take on a life of theirown Often there can be no turning back - particularlywhen the allegations became public
The repercussions of whistleblowingWrestling with the system as a result of feeling
compelled to speak out and take action comes at a cost Inhierarchical organisational structures seniority counts Ithas been suggested that within the health professionsthose who challenge the abilities of superiors or theintegrity of organisations are viewed as the problemrather than the issues they raise (Faunce and Bolsin 2003)In this way attention is drawn away from the issues raisedby whistleblowers to the whistleblowers themselves
Once an act of whistleblowing occurs there are anumber of documented detrimental personal andprofessional repercussions (De Maria 1994 Jackson andRaftos 1997 Ahern and McDonald 2002) The literaturepaints a bleak picture for whistleblowers and the evidencesuggests that whistleblowing acts affect whistleblowers ina number of ways These effects include feelings ofdisillusionment powerlessness intense frustrationconflict anger and isolation in the whistleblowers (Brodie1998 De Maria 1994 Jackson and Raftos 1997)Disciplinary action hostility ridicule ostracism scrutinyand personal attacks may come from colleagues and theinstitution (Brodie 1998 De Maria 1994 Jackson and
SCHOLARLY PAPER
53
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Raftos 1997) Other problems for whistleblowers caninclude insomnia headaches and fatigue (McDonald andAhern 2002)
The literature reveals a culture in which whistleblowersare subject to a number of official and unofficialreprisals including workplace violence and intimidation(Ahern and McDonald 2002) Some writers suggest thatwhistleblowers contemplate resignation (Jackson andRaftos 1997 McDonald and Ahern 2002) It may be thatthe degree of animosity and resentment is so great that thewhistleblower has no choice but to leave the organisationThe most common form of official reprisal is formalreprimand and being castigated by management (DeMaria 1994) The second type of reprisal include punitivetransfers which were often initiated to ease tension in theworkplace (De Maria 1994) De Maria (1994) identifiedthree common unofficial reprisals experienced by staff asostracism scrutiny and personal attacks
Where nurse whistleblowing is concerned most oftenall stakeholders (nursing organisation other nursescommunity professions whole hospital staff) are affectedby the allegations raised by the whistleblowersIrritability cynicism and isolation are reported in theworkplace (McDonald and Ahern 2002) McDonald andAhern (2002) found that whistleblowers and non-whistleblowers experienced similar percentages ofphysical illness such as altered energy levels sleepdisturbances and digestive system disturbances whilenon-whistleblowers had a higher percentage of emotionalillness from feelings of shame guilt and unworthiness
As Wilmot (2000) suggested whistleblowing isinherently adversarial and confrontational It pits partiesagainst each other and creates a climate of hostility andmistrust In addition to the effects on the whistleblowerswhistleblowing can create a panic-type reaction in whichorganisations rush to prepare themselves for the externalscrutiny that is certain to follow Furthermore staff notdirectly involved in the allegations or the whistleblowingactivities are under siege because they are also placedunder scrutiny During this time organisations remainbound by confidentiality and are often not able to telltheir side of the story to the public Damaginginformation can continue to be promulgated whileorganisations and other staff are not able to respondeffectively
The media and whistleblowingThe media is a fairly common if controversial means
whistleblowers use to draw attention to their particularissue Lipley (2001) reported a case in the UK in which anurse wrote to a newspaper alleging that elderly inpatientswere not receiving adequate care to the point that theirlives were jeopardised Findings of an appeals tribunalruled that writing to a newspaper was a reasonable andacceptable way of raising concerns (Lipley 2001)
Later in the article there is mention of the anger andoffence felt by the colleagues of the whistleblowers whoseactions had cast them into the unpleasant heat of publicscrutiny without benefit of being able to defendthemselves (Lipley 2001) Although the whistleblower inLipleyrsquos paper later apologised to his colleagues one isleft wondering if there are not more appropriately equallyeffective and potentially less damaging ways that nursesand other concerned health workers can raise issues ofconcern
Unwanted media attention can place nurses and otherstaff under unfair scrutiny The adversarial and combativeaspects of whistleblowing are never more evident thanwhen the media is involved Both the whistleblowers andthe lsquooffenderrsquo organisation are subject to the harsh gaze ofpublic scrutiny Whistleblowers may be inexperienced indealing with the media and may be themselves cast in apoor light However whistleblowers and the lsquooffenderrsquoorganisations are not the only ones who suffer Bystandersincluding other organisational staff can get caught in theskirmishes as they too are scrutinised and sometimesblamed despite the fact that their story is seldom toldRelatives of patients and members of the community canalso become implicated in the reactionary rush thatfollows
However it is neither possible nor desirable to merelydismiss the media The media has a role as public lsquowatchdogrsquo and a mandate to keep the public informed The media is especially important in health because there is a perception that the health professions areunused to being held publicly accountable The role of themedia in whistleblowing can spark bitter controversy inthe medical community However there are occasionswhere the media have rightfully raised concerns abouthealth practices or practitioners with very positiveeffects In some cases journalists have adopted the role of whistleblower
The following exchange highlights two perspectivesabout the role of the media in publicising the events thatbecame known as The Bristol Affair Emeritus ProfessorPeter Dunn aired his views that lsquobiased misleading andoften inaccurate informationrsquo caused untold damage inthis case
lsquoMany colleagues patients and friends of JamesWisheart Janardin Dhasmana and John Roylance willhave been deeply shocked by the unjust way in which thethree men have been treated Every sympathy is due tothose who have lost loved ones However whereas doctorswill readily understand the aggressive grief some parentshave shown their anger should surely be reserved for thenews media (and their informants) that have misdirectedthis grief against the Bristol surgeons using a sustainedstream of biased misleading and often inaccurateinformation And the defendantsrsquo explanations remainedalmost entirely unreported after they presented their caseThe confidence of the public in the medical profession hasbeen badly damaged by this affair and by its handling by
SCHOLARLY PAPER
54
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
the GMC [General Medical Council] So too has themorale of doctors If justice is to be done confidencerestored and doctors are not to act defensively in thefuture the forthcoming public inquiry must set the recordstraightrsquo (Dunn 1998 p1144)
James Garrett head of the current affairs team thatinitially publicised the story issued a response in asubsequent issue of the British Medical Journal in whichhe asserted that painstaking research was carried out toensure accuracy
lsquoIt was my programme in March 1996 about the Bristolheart surgery tragedy for Channel 4rsquos current affairsseries Dispatches that prompted the General MedicalCouncil (GMC) to investigate what it subsequentlybecame clear was the medical scandal of the centurySince then I and my colleagues have continued to reporton these cases I wish to reply to Dunnrsquos allegations aboutmedia reporting of the tragedy I am presumably one ofthose whom he pronounces guilty of ldquousing a sustainedstream of biased misleading and often inaccurateinformationrdquo According to Dunn bereaved parentsshould direct their grief and anger over the death of theirchildren towards people like me rather than the surgeonswho operated on the children and have since been foundguilty of serious professional misconduct ldquoShoot themessengerrdquo is the age old response of those who dislikethe message The Dispatches programme was researchedpainstakingly over many months to ensure the accuracy ofthe story it told Had it been ldquomisleadingrdquo orldquoinaccuraterdquo it would surely have attracted a writ fordefamation from one or more of the three doctors whowere named However no writ followed the originalprogramme or any of the four documentaries and dozensof shorter reports that HTV has produced since Dunncomplains that the views of the three doctors havereceived inadequate attention in the media I havepersonally written many letters to James WisheartJanardin Dhasmana and John Roylance seeking toreport their views None of them has taken up my offerwhich remains open Their refusal to contributenotwithstanding HTV reported the defence they made atthe GMC Interviews with lay supporters - which we havealso broadcast - are ultimately no substitute for thedoctorsrsquo own wordshellip Dunn should look closer to homefor people to blame if the public does not like what weshowed them and demands reformrsquo (Garrett 1998p1592)
Investigative journalists in particular tend to take greatcare to provide balance in their arguments and carefullycheck and cross check their sources In many cases they have provided crucial and timely information A compelling example of media whistleblowing tookplace in New Zealand as a result of the publication of anarticle in the mainstream media exposing unethicalexperimentation on women The article was the catalystfor an investigation led by Judge Dame Silvia Cartwrightinto the treatment of women with abnormal cervical
smears the National Womenrsquos Hospital in Auckland Theinquiry culminated in The Cartwright Report (1988)which resulted in a series of recommendations to improvewomenrsquos health care raise awareness of ethical issuesand place patientrsquos rights firmly on the agenda (WomenrsquosHealth Action Trust 1998)
This type of media involvement plays a crucial role inprotecting the public and in making the health professionsaccountable In the end it has probably saved many livesThe media was also instrumental in raising public alarmat the events occurring at Chelmsford Hospital in SydneyAustralia These concerns led to The Chelmsford HospitalInquiry (Hart 1996) and revealed (arguably) the worstcase of psychiatric malpractice in Australian history Asevidenced in Justice Slatteryrsquos comments the secrecysurrounding practices at the hospital was entrenched andwithout the influence of the media may have remainedso
lsquohellip there was a systematic cloak of secrecy about thetreatments a blanket on the disclosure of informationrelating to it and a fraudulent cover-up of deaths andother incidents at the hospitalrsquo (Slattery cited in Bagnallundated)
Clearly history has shown the media can play apowerful role in raising public awareness about health-related practices and wrongdoings in health organisationsFurthermore as has been demonstrated in the examplespresented here the media has the power to be a potentcatalyst for inquiry processes that compels healthprofessionals to reflect on their attitudes and practicesand to effect positive changes in health care practice
However the other side of the coin is that while raisingmatters in the media certainly has the effect of placingthem firmly under the public gaze the sources ofinformation cannot be guaranteed or even identified insome cases Though most reporting in the media isresponsible the nature of health care is that both sides areoften not able to lsquotell their storiesrsquo Accused individualsand organisations remain bound by confidentiality Legaladvisors might advise accused parties not to talk to themedia As a result information may not be balanced orcompletely accurate and may be taken out of contextMisinformation can cause alarm and panic that canquickly spread Although altruism and the lsquopublic goodrsquomay be cited as possible motivating factors forwhistleblowing in the first place things can quickly getout of control
In the final analysis the whistleblower needs to make aconsidered decision about approaching the media If theychoose to do so they need to carefully select the type ofmedia to approach The accountability for such decisionsrests with the whistleblower and they must live with theoutcomes of their decisions
SCHOLARLY PAPER
55
Australian Journal of Advanced Nursing 2005 Volume 23 Number 1
Looking ahead Solving the whistleblowing dilemmaIt could be argued that if health care organisations had
appropriate and sound internal structures in place toensure employees concerns are addressed whistleblowingwould never occur However as matters stand theliterature is replete with examples of nurseemployeesexhausting all internal avenues with management andorganisations as they strive to draw attention to andrectify the wrong doing (eg Jackson and Raftos 1997)
In Australian nursing there is an evident paucity ofinformation relating to whistleblowing In the February2002 Australian Nursing Journal Iliffe describedwhistleblowing as a difficult area and asked nurses torespond and debate the issue At that time she drewattention to the fact that no policy concerningwhistleblowing was currently in place to guide nurses andhighlighted it as an important omission (Iliffe 2002) Inconclusion Iliffe called for discussion and debate aboutissues related to whistleblowing and indicated a need forpolicy to be developed to deal with whistleblowingsituations (Iliffe 2002)
Recommendations for the establishment of a specifictask force to assist staff who may be involved in awhistleblowing situation have been made in Australia(Jackson and Raftos1997) The responsibility could betaken by an existing national body or an independentbody could be formed The group could provide aplatform for nurses to discuss issues aroundwhistleblowing and could provide information andsupport for whistleblowers (Jackson and Raftos1997)
Medicine has begun to act to effect change Faunce andBolsin (2003) reported that the Australian NationalUniversity has initiated strategies within the medicalcurriculum so that students will be able to understand theinter-relationship between human rights ethical and legalprincipals and how they intersect with safety and qualityissues Students will be exposed to simulated learningexperiences including whistleblowing Nursing too needsto look to turning around the enculturation processes thatcondone abusive and poor practices
CONCLUSIONClearly whistleblowing presents nursing with a
continuing ethical and moral dilemma It is importantnurses engage in a debate about whistleblowing andexamine ways to ensure standards are met and protect therights of patients and the wider community Nurses mustbe prepared to examine themselves and must continue toadvocate for patients clients and communities Nursesmust not avert their gaze when abuse neglect orviolations of individual and community rights occur
However it is not acceptable for nurses who blow thewhistle to experience the extreme personal andprofessional sequelae described in the literatureFurthermore there must be mechanisms for ensuringrights and addressing abusive neglectful and otherwiseunacceptable practices without raising public panic andwithout creating unendurable conditions for nurses andother personnel who remain and continue to provideservices and to reflect rectify and rebuild
Finally to answer the question we pose in the title ofthis paper - do the ends justify the means Despite thepain that can be associated with whistleblowing if theends are improved professional standards enhancedoutcomes rectification of wrongdoings and increasedsafety for patients and staff in our health services then wesay the answer is a resounding yes - the ends definitelyjustify the means
REFERENCES Ahern K and McDonald S 2002 The beliefs of nurses who were involved in awhistleblowing event Journal of Advanced Nursing 38(3)303-309
Bagnall G Undated Personally speaking wwwmeactionukorgukpersonallyspeakinghtm Retrieved 230304
Brodie P 1998 Ethics Whistleblowing A moral dilemma Plastic SurgicalNursing 18(1)56-58
Dawson S 2000 Whistleblowing A broad definition and some issues forAustralia wwwuoweduauartsstsbmartindissentdocumentsDawsonhtmlRetrieved 230304
De Maria W 1994 Wounded workers Queensland whistleblower studyDepartment of Social Work and Social Policy The University of Queensland
Dunn P 1998 The Wisheart affair Paediatric cardiological services in Bristol1990-5 British Medical Journal 3171144-1145
Faunce T and Bolsin S 2003 If doctors donrsquot understand ethics itrsquos time tostart teaching them Sydney Morning Herald 191203
Fletcher J Sorrell J and Cipriano Silva M 1998 Whistleblowing as a failureof organizational ethics Online Journal of Issues in Nursing 311-13
Garrett J 1998 lsquoDispatchesrsquo programme was painstakingly researched and didnot attract writ for defamation British Medical Journal 3171592
Hart B 1996 One manrsquos nightmare Medicine for profit Green Left Weeklywwwgreenleftorgauback1996239239p13htm
Iliffe J 2002 Whistleblowing A difficult decision Australian NursingJournal 9(7)1
Jackson D and Raftos M 1997 In uncharted waters Confronting the cultureof silence in a residential care institution International Journal of NursingPractice 3(1)34-39
Lipley N 2001 Whistleblower who wrote to newspaper wins tribunal NursingStandard 16(12)4
Mallik M 1997 Advocacy in nursing A review of the literature Journal ofAdvanced Nursing 25(1)130-138
McDonald S and Ahern K 2002 Physical and emotional effects ofwhistleblowing Journal of Psychosocial Nursing and Mental Health Services40(1)14-27
Speedy S 2004 Organisation violations Implications for leadership In Daly JSpeedy S and Jackson D (ed) Nursing Leadership Churchill LivingstoneSydney 145-164
Wilmot S 2000 Nurses and whistleblowing The ethical issues Journal ofAdvanced Nursing 32(5)1051-1057
Womenrsquos Health Action Trust 1998 Selections from Womenrsquos Health Watchwwwwomens-healthorgnzpublicationsWHWwhwdec98htm
SCHOLARLY PAPER
56
- FROM THE EDITOR
- MEDICATION KNOWLEDGE AND SELF-MANAGEMENT BY PEOPLE WITH TYPE 2 DIABETES
- A COMPARISON OF AN EVIDENCE BASED REGIME WITH THE STANDARD PROTOCOL FOR MONITORING POST OPERATIVE OBSERVATION A RANDOMISED CONTROLLED TRIAL
- WHAT WERE THE OUTCOMES OF HOME FOLLOW-UP VISITS AFTER POSTPARTUM HOSPITAL DISCHARGE
- IMPLEMENTING FAMILY-CENTRED CARE AN EXPLORATION OF THE BELIEFS AND PRACTICES OF PAEDIATRIC NURSES
- UNDERSTANDING THE NURSING WORKFORCE A LONGITUDINAL STUDY OF AUSTRALIAN NURSES SIX YEARS AFTER GRADUATE STUDY
- THE CHANGING FACE OF NURSES IN AUSTRALIAN GENERAL PRACTICE
- DO THE ENDS JUSTIFY THE MEANS NURSING AND THE DILEMMA OF WHISTLEBLOWING
-