
From primary to tertiary care - Op zoek naar het verhaal ... · Clinical rules de nieuwe generatie...
47
Transcript of From primary to tertiary care - Op zoek naar het verhaal ... · Clinical rules de nieuwe generatie...

Clinical rules de nieuwe generatie medicatiebewaking
Hugo van der Kuy
Erasmus MC
Voorheen Zuyderland

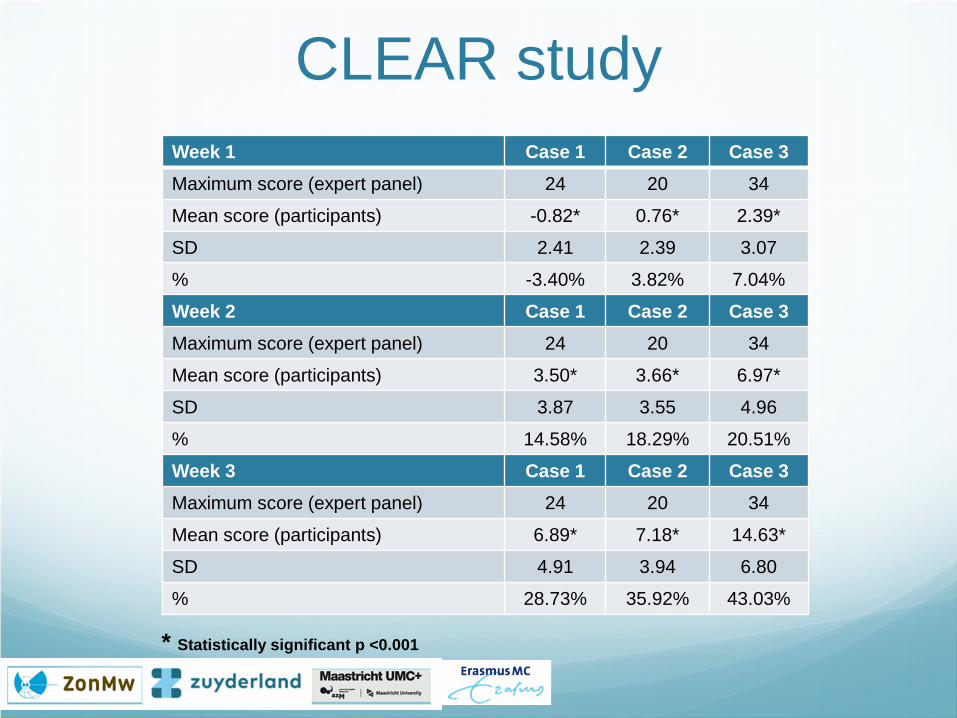
Week 1 Case 1 Case 2 Case 3 Maximum score (expert panel) 24 20 34
Mean score (participants) -0.82* 0.76* 2.39*
SD 2.41 2.39 3.07
% -3.40% 3.82% 7.04%
Week 2 Case 1 Case 2 Case 3 Maximum score (expert panel) 24 20 34
Mean score (participants) 3.50* 3.66* 6.97*
SD 3.87 3.55 4.96
% 14.58% 18.29% 20.51%
Week 3 Case 1 Case 2 Case 3 Maximum score (expert panel) 24 20 34
Mean score (participants) 6.89* 7.18* 14.63*
SD 4.91 3.94 6.80
% 28.73% 35.92% 43.03%
CLEAR study
* Statistically significant p <0.001
CLEAR study Clinical and Laboratory data Evaluation for an Appropriate medication Review
Week 1 Week 2 Week 3
Medication list Medication list Medication list Lab data Lab data Medical history
What is the score of the reviewer compared to the expert panel?
The expert panel had all the information from week 3!
CLEAR study Week 1 Case 1 Case 2 Case 3 Maximum score (expert panel) 24 20 34
Mean score (participants) -0.82* 0.76* 2.39*
SD 2.41 2.39 3.07
% -3.40% 3.82% 7.04%
Week 2 Case 1 Case 2 Case 3 Maximum score (expert panel) 24 20 34
Mean score (participants) 3.50* 3.66* 6.97*
SD 3.87 3.55 4.96
% 14.58% 18.29% 20.51%
Week 3 Case 1 Case 2 Case 3 Maximum score (expert panel) 24 20 34
Mean score (participants) 6.89* 7.18* 14.63*
SD 4.91 3.94 6.80
% 28.73% 35.92% 43.03%
* Statistically significant p <0.001
Business case • 800 patients in nursing homes
• Recommended at least 2 medication reviews/patient/year (reality is different)
• Average 1 hour per patient/review
• Total 1600 hours = 1 FTU
The solution? Automatic
Standardized/objective
Knowledge database
Less time consuming
More efficient (no or less unnecessary alerts) Efficiency current medicationsurveillance?
Around the clock surveillance
System independent
Available for more hospitals/Nursing Homes
CRR ● Clinical Rule Reporter
● Extracting 3 different files medication, patient characteristics, lab data
● Upload to CRE (A’dam)
● Daily evaluation 2000 patients
● Average time upload: 10-15 minutes
● Efficiency increase 15% 80%
● Feedback via email
Which rules? • Labdata (31 parameters) e.g. Renal function, K, Na, Leuco, INR, albumin
• Stopdata e.g. cytostatics, warfarin+LMWH • START/STOPP criteria e.g. Prolonged use of 1st generation antihistamines
• Indications NHG-standards (GP) e.g. myocard infarction, CHADS-2
• Possible medication errors e.g. MTX, bisphosphonates 1x per week
• Identification risk patients e.g. PPI-prophylaxis, opioids + laxatives
• Patient indexes e.g. risk of falling, risk of delirium, Drug Burden Index
Efficacy potassium
Efficacy potassium When potassium affecting medication is used and
potassium level is abnormal (<3.0 mmol/L or >5.0 mmol/L). 5%
Efficacy potassium When potassium affecting medication is used and
potassium level is abnormal (<3.0 mmol/L or >5.0 mmol/L).
The CR is divided in two separate rules: A hypopotassemia rule generating alerts if potassium
decreasing medication is used and the potassium level is decreased (<3.0 mmol/L).
A hyperpotassemia rule generating alerts if potassium increasing medication is used and the potassium level is increased (>5.5 mmol/L).
5%
+ 40%
Efficacy potassium When potassium affecting medication is used and
potassium level is abnormal (<3.0 mmol/L or >5.0 mmol/L).
The CR is divided in two separate rules: A hypopotassemia rule generating alerts if potassium
decreasing medication is used and the potassium level is decreased (<3.0 mmol/L).
A hyperpotassemia rule generating alerts if potassium increasing medication is used and the potassium level is increased (>5.5 mmol/L).
The clinical rules are further developed: The hypopotassemia rule generates alerts if potassium
decreasing medication is used, the potassium level is <3.0 mmol/L, and no potassium supplements are used.
The hyperpotassemia rule generates alerts if potassium increasing medication is used, the potassium level is >5.5 mmol/L, and no potassium binder is used.
5%
+ 40%
80%
Efficacy potassium When potassium affecting medication is used and potassium level
is abnormal (<3.0 mmol/L or >5.0 mmol/L).
The CR is divided in two separate rules: A hypopotassemia rule generating alerts if potassium
decreasing medication is used and the potassium level is decreased (<3.0 mmol/L).
A hyperpotassemia rule generating alerts if potassium increasing medication is used and the potassium level is increased (>5.5 mmol/L).
The clinical rules are further developed: The hypopotassemia rule generates alerts if potassium
decreasing medication is used, the potassium level is <3.0 mmol/L, and no potassium supplements are used.
The hyperpotassemia rule generates alerts if potassium increasing medication is used, the potassium level is >5.5 mmol/L, and no potassium binder is used.
The hypopotassemia CR is adjusted so that alerts are generated if the potassium levels are <2.0 mmol/L, despite the use of potassium supplements.
5%
+ 40%
80%
added

SCREAM
Supporting Clinical Rules Engine in the Adjustment of Medication
Hugo van der Kuy Clinical Pharmacologist The Netherlands Edvard Munch
SCREAM Primary endpoints:
death, fall, delirium, hospital admission: combined
>3000 patients (Orbis, Helmond, Envida, Novicare)
1 year
Randomisation: regular care versus regular care+CRR CRR is run on a weekly basis
Randomisation per nursing home physician
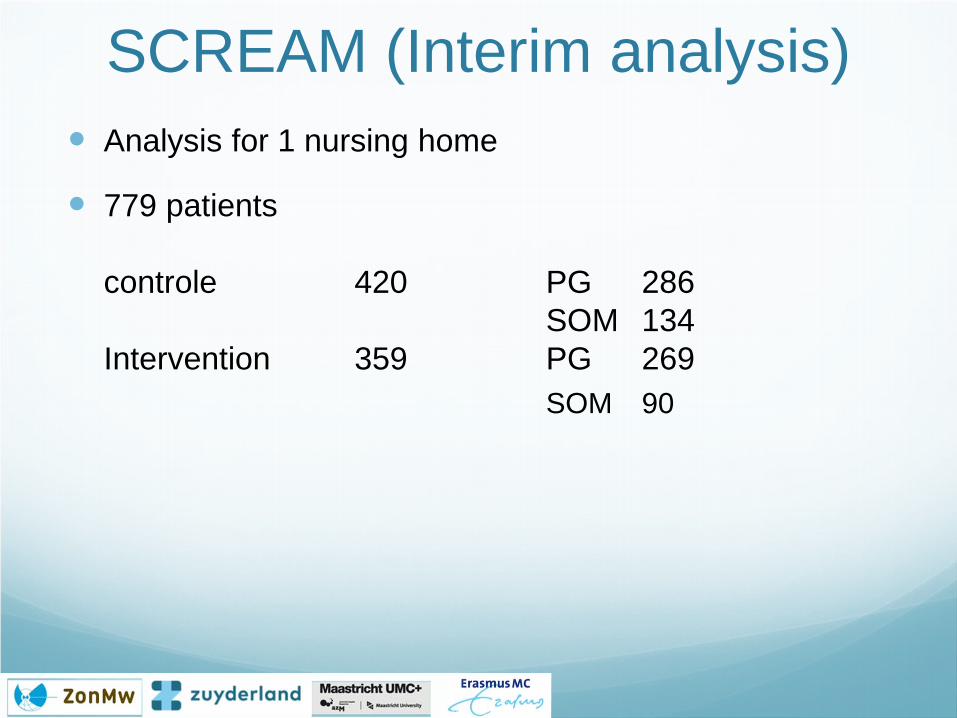
SCREAM (Interim analysis) Analysis for 1 nursing home
779 patients controle 420 PG 286 SOM 134 Intervention 359 PG 269 SOM 90
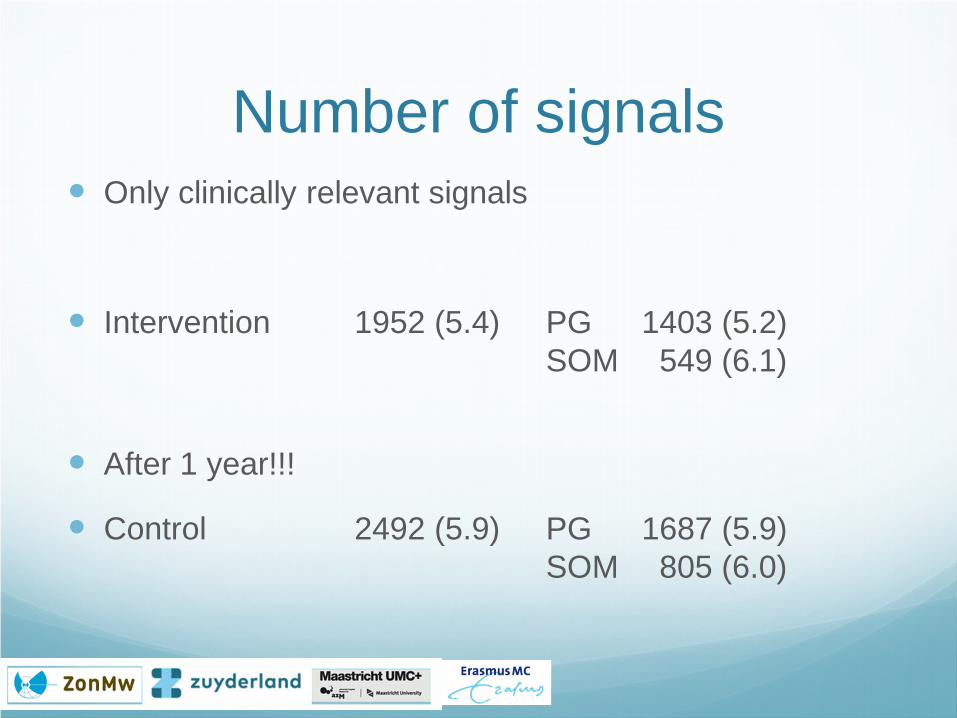
Number of signals Only clinically relevant signals
Intervention 1952 (5.4) PG 1403 (5.2) SOM 549 (6.1)
After 1 year!!!
Control 2492 (5.9) PG 1687 (5.9) SOM 805 (6.0)
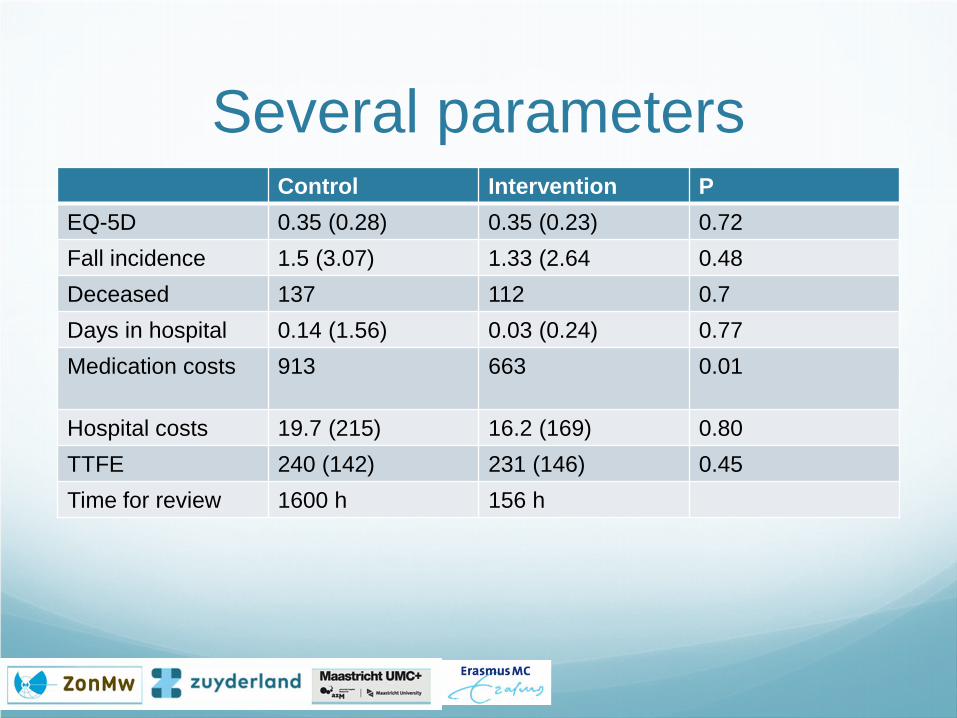
Several parameters Control Intervention P
EQ-5D 0.35 (0.28) 0.35 (0.23) 0.72 Fall incidence 1.5 (3.07) 1.33 (2.64 0.48 Deceased 137 112 0.7 Days in hospital 0.14 (1.56) 0.03 (0.24) 0.77 Medication costs 913 663 0.01
Hospital costs 19.7 (215) 16.2 (169) 0.80 TTFE 240 (142) 231 (146) 0.45 Time for review 1600 h 156 h
Conclusions This is the first interim analysis.
No clear benefit is seen yet on clinically relevant endpoints
Time for medication review is clearly reduced
Twice a year a review means that a patient is exposed too long to “not optimal medication”.
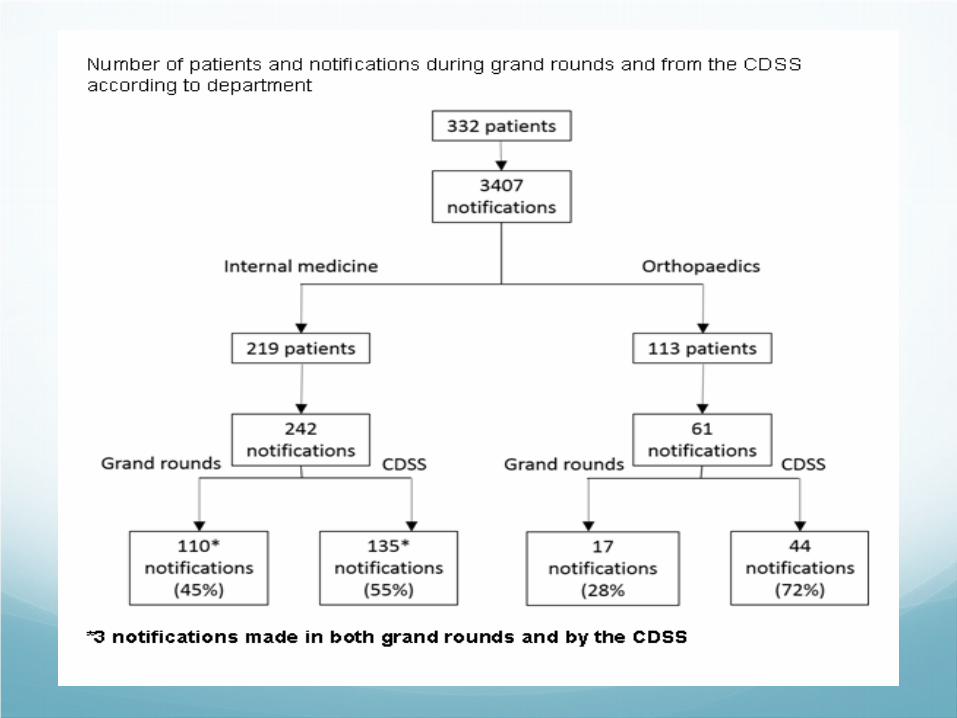
Added Value of the CRR in the hospital
Methods During 4 months observation of the weekly grand
rounds
Internal medicine and orthopedia
Remarks physicians were compared with alerts of the CRR
CRR consisted of 469 rules of which 120 were specialised for the hospital setting
Relevance of th remarks/alerts was determined by two internists
Notifications divided in subgroups
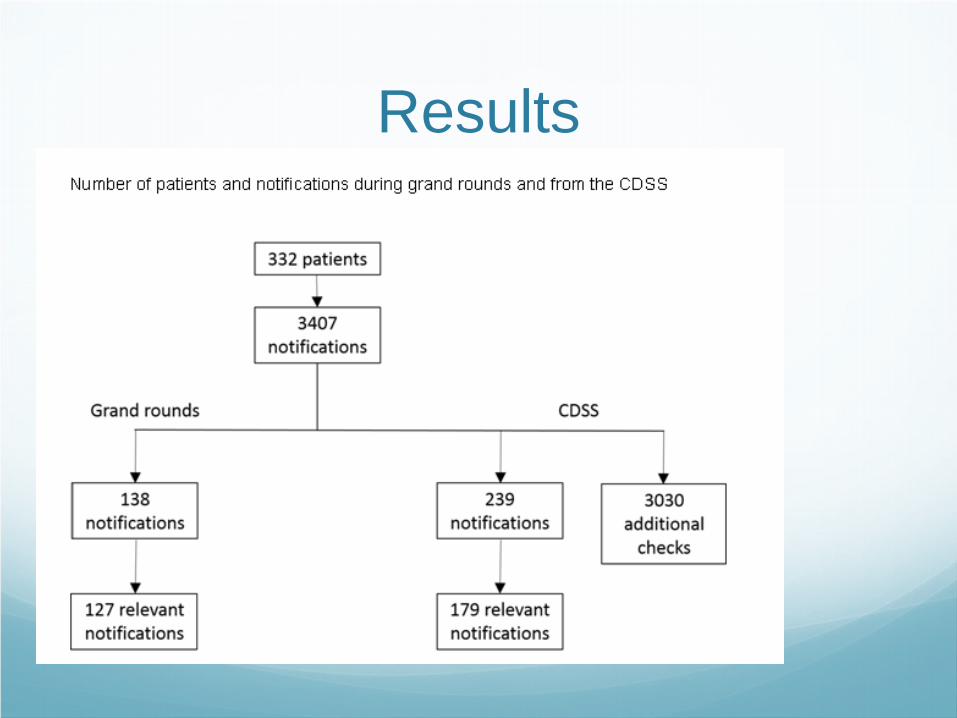
Results

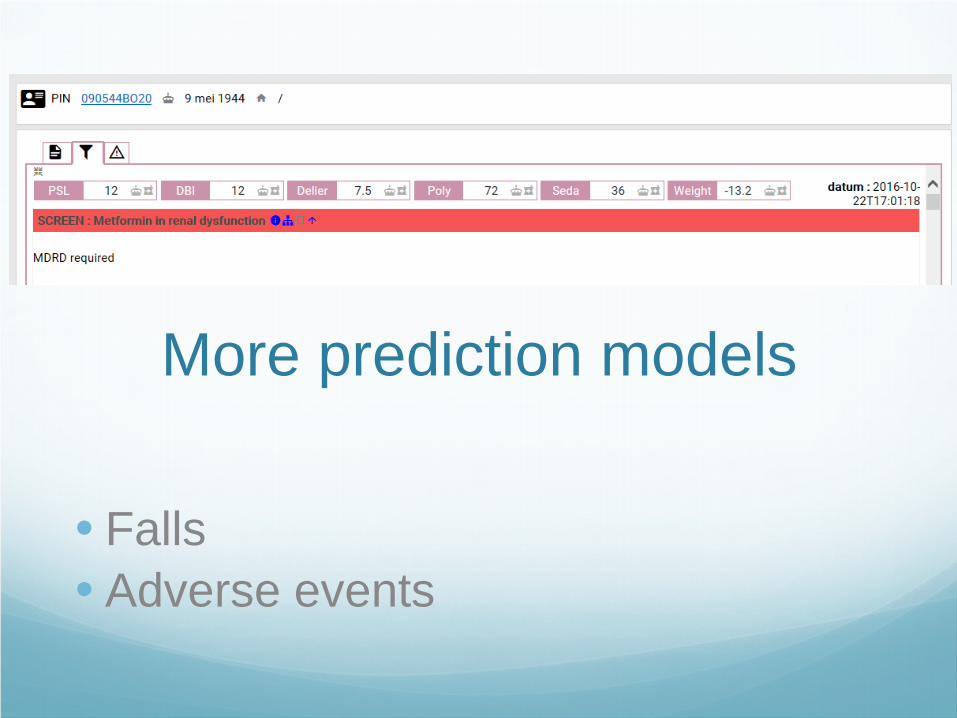
More prediction models
• Falls • Adverse events

DElier MOdel
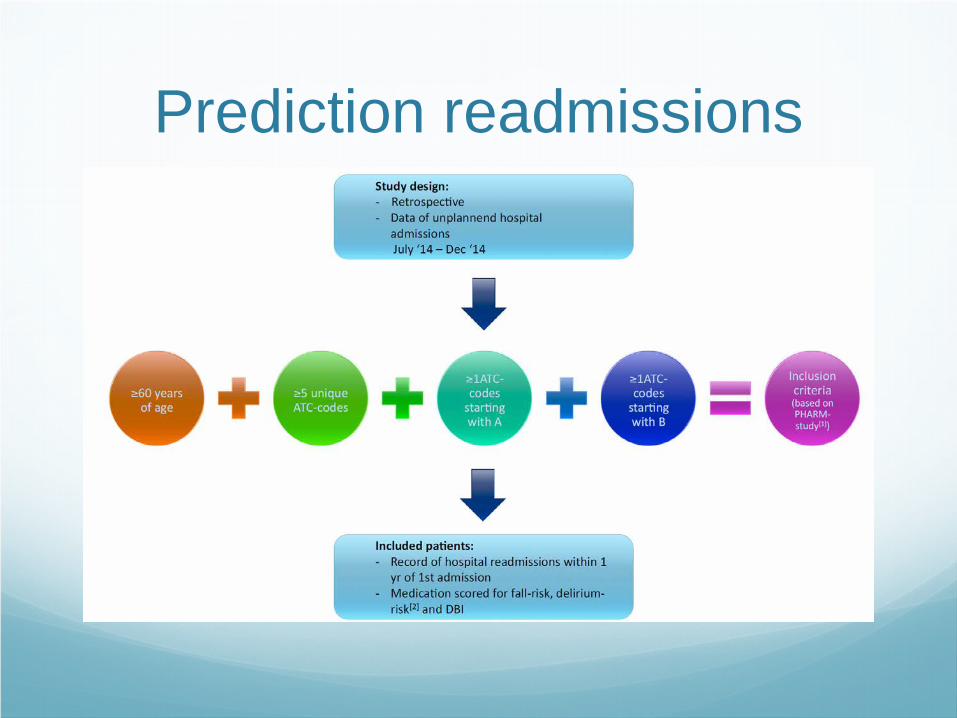
Prediction readmissions
CHECkUP Control in the Hospital by
Extensive Clinical rules for Unplanned hospitalisations in elderly Patients ZonMw
Studie opzet Doel: Reductie heropnames van ouderen met ongeplande opnames
Inclusie
Ouderen met ongeplande opnames Regio Heerlen, Maastricht en Sittard
2400 patienten opgedeeld in twee groepen
Interventie Bij ontslag CRR draaien Adviezen naar HA/APO Wekelijks herhalen via LSP + adviezen Vragenlijsten naar patient
Controle Geen adviezen naar HA/APO
Start Januari 2018

Further research Contribution patients prefer quality of life or longer life
What if we inform the patients with alerts?
What is the role of the CRR in POS?
What is the role of the CRR for outpatient management?
Can we use the CRR for HSMR reduction
What is the role of the CRR in primary care?

Helaas ervaar ik het nu anders……

Take home Medicationsurveillance is changing rapidly
Medication review and medication surveillance
Medication optimisation
Watch out, others will take over…

HSMR Een kwestie van verslaglegging?
HSMR
Twee aandachtspunten Lege voorgeschiedenis
De kwaliteit van de inhoud
Voorgeschiedenis wordt gebruikt om risico van patienten te classificeren

De lege voorgeschiednis
Actieplan 1 In September starten we met pilot lege
voorgeschiedenis
Gemandateerde krijgt overzicht met lege voorgeschiedenissen
Gaan we volgen gedurende 3 maanden
Daarna moet ieder specialisme onder de 10 per week zitten
In december evaluatie door MSB bestuur en terugkoppeling

Actieplan II Mbv CDSS van apotheek controle op voorgeschiedenis
Gaat in september lopen als pilot
(zaal) arts krijgt een mail met signaal
Via link afhandelen wat je er mee doet 0 ingevoerd in VG 0 Geneesmiddel is voor andere indicatie 0 Alert is ten onrechte afgegaan
Actieplan II Alleen opgenomen patienten worden gecontroleerd
Afhandeling per vakgroep kan gemonitord worden
Is in ontwikkeling actieve bijdrage verbeterd het systeem
Apotheek gaat voorlopig de mails versturen weten niet wat workload is
Evaluatie in december


![í í ¼ë °ì ´í · 2020. 6. 1. · kh Mupno{tvkl h|{vSkh OjvsvyPSupno{Oi~PSl {klsh OzljPW¥]W kTeusl}lsW¥Y\\ uTeksl}lsW¥Y\\ upno{jvsvy vmmSvu jvsvyi|yz{ vmmSvu kuy kuytvkl](https://static.fdocuments.in/doc/165x107/60b2227ae50e3105d060cebf/-2020-6-1-kh-mupnotvkl-hvskh-ojvsvypsupnooipsl-klsh.jpg)













![1) Alice’s Adventures in Wonderland · 1899 Alice’s avonturen in het wonderland [Alice’s adventures in the miracleland] Leiden: Boekhandel en Drukkerij voorheen E. J. Brill.](https://static.fdocuments.in/doc/165x107/5f98cf5cae29b2618b39eab2/1-aliceas-adventures-in-wonderland-1899-aliceas-avonturen-in-het-wonderland.jpg)

![fp=% ;w,u ,LdSi fp=% gkseysl baVjuS'kuy 'kgjksa vkokl · PDF filelfpoky; d sfopkj ugh agAaS bl idz k”ku e asiLz rrq fo”y’sk.k] ... qukbVsM us'kUl bdukfed ,.M lks'ky deh'ku QkWj](https://static.fdocuments.in/doc/165x107/5a717f667f8b9aa7538ce660/fp-wu-ldsi-fp-gkseysl-bavjuskuy-kgjksa-vkokl-xjhcksawwwcitiesallianceorgsitescitiesallianceorgfilescaimagespdf.jpg)