From molecule to man by Peter V. Coveney
53
From Molecule to Man: the Virtual Physiological Human, Computational Biology & the Future of Biomedicine Peter V. Coveney Centre for Computational Science University College London
-
Upload
technopapa -
Category
Documents
-
view
499 -
download
0
description
Transcript of From molecule to man by Peter V. Coveney

From Molecule to Man: the Virtual Physiological Human, Computational Biology & the Future of Biomedicine
Peter V. Coveney Centre for Computational Science University College London

VPH and Computational Biology Issues
Presentation Outline
• Context
• VPH Initiative – VPH Projects – Role of VPH NoE
• Centre for Computational Science Research
• UCL/Yale Partnership
• “Digital Me” – a vision of future healthcare provision

1993 2009 1997 2005 2006 2007 2008
Molecular Biology
Microcomputers/home computers
Grid Computing
Finite Elements
VPH/Physiome History
FP7 call 2 Objective ICT-2007.5.3: Virtual Physiological Human
Systems Biology
Human Genome Project

VPH and Computational Biology Issues Integrative and systems biology
• Data produced by sequencing 10TB per day per machine • Integrating over all relevant length and timescales • Requires integration of suitable compute and data facilities,
connected by high performance networks. • VPH seen as paradigm case for putative BBSRC Digital
Organisms programme. • Exploiting ‘big data’ – seizing new opportunities to generate
knowledge and impact as we enter an era of data intensive science.
• Tools, resources and facilities – providing the tools, technologies and infrastructures that are essential for 21st century bioscience.
• Increase the uptake of systems-based approaches in the private sector.

VPH and Computational Biology Issues
Overall € 340 M over 4 years (2007-2010) Challenge 5
• Predictive Medicine–Virtual Physiological Human (VPH Initiative) – Modelling/simulation of human physiology and disease € 72
M in 2007 - € 5 M in 2009 - € 68 M in 2010 • Personalisation of Healthcare
– Personal Health Systems (PHS), € 72 M in 2007 - € 63 M in 2009
• Patient safety (PS) - avoiding medical errors – € 30 M in 2007 - € 30 M in 2009
Funding: Budget for research supported by the European Commission ICT - Health unit in FP7

VPH and Computational Biology Issues
The VPH Initiative is currently in its 3rd Call. It focuses on:
• Keep the overall VPH vision: – Early diagnostics & Predictive medicine – Personalised (Patient-specific) healthcare solution
• By means of: – Modelling & simulation of human physiology and disease related
processes – Emphasis on tools/infrastructure for bio-med researchers+clinicians
• VPH in 2010 – Call 6 opens November 2009 , closing 13 April 2010 – Budget € 63M

VPH and Computational Biology Issues
Overall planning for the elaboration of the EU Workprogramme 2011-12:
• Orientation paper developed by Christmas 2009
• First draft of the Workprogramme by February 2010
• Final draft of the Workprogramme by May 2010

VPH and Computational Biology Issues
• Elaboration of WP2011-12: – Drafted by the Commission – Based on community inputs (research/clinical/industry)
• The NoE Vision Document is an essential input for the VPH – It presents the view of the Community at large on gaps,
challenges and future direction and informs EC policy
• There will be annual updates with open consultation in the community through the NoE website.
• Don’t miss this opportunity to contribute!

VPH and Computational Biology Issues
The VPH Initiative (VPH – I) & VPH Network of Excellence
• Collaborative projects within the call meet objectives associated with specific challenges
• VPH NoE connects all of these projects, and must focus on addressing issues of common concern that affect VPH-I projects collectively – research infrastructure – training – dissemination

Virtual Physiological Human
• Funded under EU FP 7 (call 2) • 15 projects: 1 NoE, 3 IPs, 9 STREPs, 2 CAs, and new
projects in negotiation phase
“a methodological and technological framework that, once established, will enable collaborative investigation of the human body as a single complex system ... It is a way to share observations, to derive predictive hypotheses from them, and to integrate them into a constantly improving understanding of human physiology/pathology, by regarding it as a single system.”
VPH Call 6 currently open – deadline13th April 2010

VPH- I FP7 current projects
Networking NoE
Osteoporosis IP
Alzheimer's/ BM & diagnosis STREP
Heart /CV disease STREP
Cancer STREP
Liver surgery STREP
Heart/ LVD surgery STREP
Oral cancer/ BM D&T STREP
CV/ Atheroschlerosis IP
Breast cancer/ diagnosis STREP
Vascular/ AVF & haemodialysis STREP
Liver cancer/RFA therapy STREP
Security and Privacy in VPH CA
Grid access CA
Heart /CV disease STREP
Industry
Clinics Other
Parallel VPH projects

VPH NoE • VPH NoE - Virtual Physiological Human
Network of Excellence
• Primary purpose to strengthen the VPH community and provide tools and services for researchers in the field
• Support VPH-I projects directly
© VPH NoE, 2008
Start Date 2008-06-01
End Date 2012-11-30
Project Funding 7.99M€ EU funding)
VPH and Computational Biology Issues

VPH and Computational Biology Issues
Specifically, the VPH NoE will: • Identify user needs, define standards, ontologies and
applications, and develop VPH ToolKit • Develop VPH training activities and materials: Joint advanced
degree programme, interdisciplinary study groups, focused journal issues, textbook
• Provide research/news dissemination services and international EU/international networking
Project Coordinators: Vanessa Díaz-Zuccarini / Miriam Mendes (UCL) Scientific Coordinators: Peter Coveney (UCL), Peter Kohl (Oxford)
http://www.vph-noe.eu

VPH and Computational Biology Issues
• 14 Core Partners – 4 UK (UCL, UOXF, UNOTT, USFD) – 3 France (CNRS, INRIA, ERCIM) – 2 Spain (UPF, IMIM) – 1 Germany (EMBL [EBI]) – 1 Sweden (KI) – 1 Belgium (ULB) – 1 New Zealand (UOA) – 1 Italy (IOR)
• Associate / General Members – 38 General (academic) and Associate (Industrial) Members – … and growing

VPH and Computational Biology Issues
Future results and impacts • Create a more cohesive VPH research community,
both within and beyond the EU. • Enhance recognition at national level of importance of
modelling and simulation in biomedicine • Increase Industrial and Clinical awareness of VPH
modelling • Increase emphasis on interdisciplinary training in
biological and biomedical/engineering physics curricula

WP1
- M
anag
emen
t
WP2
- Ex
empl
ar P
roje
cts
WP3 - VPH ToolKit
WP4: INTEGRATION
AND TRAINING ACTIVIES
WP5: SPREADING EXCELLENCE
Vert
ical
inte
grat
ion
Project Structure VPH and Computational Biology Issues

WP1 - Management
WP2 – Exemplar Projects
WP3 – VPH Toolkit WP4 – Integration & Training activities
WP5 - Networking/Communication and Spreading Excellence within the VPH NoE/VPH-I
Project Structure VPH and Computational Biology Issues

VPH NoE General Assembly - Key Legislative Body
(Includes all membership types) Annual Meetings (coinciding with Project Meetings) Delegates Executive Powers to Steering Committee
Steering Committee:
Key Executive Body Includes Consortium Agreement Signatories Quarterly meetings to lead implementation of NoE WPs Takes advice from Advisory Boards May set up Task Forces on Policy Issues (such as on IP, Ethics, Gender)
Delegates day-to-day project management to WP1 - Management
Clinical Advisory Board
Industry Advisory Board
Scientific Advisory Board
Project Office UCL European Research & Development Office Contract management and project implementation
WP3 WP4 WP5 WP2
EC Project Officer
Other VPH Projects
Other VPH Projects
Other VPH Projects
Other VPH Projects
Other VPH Projects
WP1

WP2
© VPH NoE, 2008
EPs work towards integration amongst VPH researchers, in order to address specific research problems or challenges.
• Provide solid examples of horizontal and vertical model/data integration
• Two-way symbiosis with the development of VPH ToolKit (WP3), guiding ToolKit development
• WP2 activity began with preparation of VPH Research Strategy Document, which pinpoints priority research areas for calls
VPH and Computational Biology Issues

WP2
© VPH NoE, 2008
• 2008-2009: five integrative research projects carried out by VPH core members - seed Exemplar Projects
• 2009+: annual open call for EP proposals from NoE core membership • Individual EP support given as 6-12-month grant to support
personnel costs only • Reviewed by a WP2 Board with advice from Scientific,
Clinical and Industrial Advisory Boards
• 2010 call will be issued shortly to partners and general members. Focus on sustainability of the WP3 Toolkit
VPH and Computational Biology Issues

WP3
© VPH NoE, 2008
• The toolkit will be a shared and mutually accessible source of research equipment, managerial and research infrastructures, facilities and services
• Other VPH projects, including the Exemplar Projects (EPs), will add to and draw capacity from it
• Can only be achieved through the integration of disparate knowledge and research infrastructure
The VPH ToolKit aims to become the technical and methodological framework to support and enable VPH research.
VPH and Computational Biology Issues

© VPH NoE, 2008
• Activities include: • Creation of mark up languages for model and
data encapsulation • VPH software tools and GUIs • Model and data repositories • Grid access using VPH ToolKit • Workflow environments & middleware
WP3 VPH and Computational Biology Issues

WP4
© VPH NoE, 2008
• Training initiatives in integrative and systems biology, both event-based (Study Groups) and allowing rotation between labs within the VPH NoE (early- and in-career)
• Development of distance learning/training resources for VPH and associated virtual/interactive communication methods, possible joint (inter-university) degree programme
• Development of VPH publishing (textbook and journal special issues)
Development of a portfolio of interdisciplinary training activities including a formal consultation on, and assessment of, VPH careers
VPH and Computational Biology Issues

© VPH NoE, 2008
• Address training and career development for both early and in-career VPH researchers
• Make use of existing studies for interdisciplinary Europe-wide Study programme
– Marie Curie programme
• Identify and quantify demand for career paths
– Healthcare/clinical scientist
– Industry
– Academia
• Ultimate goal: design and implement actions directed at the development of VPH research education and careers
WP4 VPH and Computational Biology Issues

© VPH NoE, 2008
• Development of the VPH NoE website (public and private faces)
• Publish annual scientific roadmaps which chart Network progress/assist in ongoing planning of activities
• Publish VPH special issues in world-class journals • Design, prepare and produce a wide array of VPH
dissemination materials and events, including 6 monthly VPH-I newsletter
Development of an International VPH Gateway to facilitate interaction and co-operation between VPH initiative projects and practitioners
WP5 VPH and Computational Biology Issues

© VPH NoE, 2008
WP5 Activities VPH and Computational Biology Issues
• VPH NoE website development with dedicated WP and VPH I pages. • Coordination of the consultation for the ‘Vision Document’ to inform future
EC VPH calls and programs • VPH special issues published in Phil Trans R Soc A • Creation of VPH-I working group and Scientific, Industrial and Clinical
Boards. • Dissemination strategy includes continual updates on developments in
WP2, WP3 and WP4 and VPH-I projects via the VPH NoE website, internet sites, mailing lists and newsletters
• Organisation of workshops to foster engagement with Industry
• VPH 2010 – 30 September/ 1st October 2010, Brussels
First conference in a new VPH series of high profile conferences. Call for papers open, please visit website.

http://www.vph-noe.eu/VPH2010
30 September – 1 October 2010 Brussels, Belgium
© VPH NoE, 2008
First of a series of VPH conferences supported by the European Commission (DG-INFSO)
• Dedicated to the VPH Initiative
• Representatives from VPH groups, Clinics and Industry
• Open to all (register online)
Abstracts by 1st May 2010
VPH2010

Centre for Computational Science
Advancing science through computers
• Computational Science
• Algorithms, code development & implementation
• High performance & distributed computing
• Visualisation & computational steering
• Condensed matter physics & chemistry, materials & life sciences
• Translational medicine, e-Health & VPH

CCS – Accessing Federated Resources
DEISA
UK NGS
Leeds
Manchester
Oxford
RAL
HPCx
NGS
GridSAM
UNICORE
Yale resources
TeraGrid
Globus
Globus
AHE

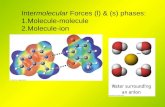
Biomedical application have “non-standard” requirements
• Ability to co-reserve resources (HARC) • Launch emergency simulations (SPRUCE) • Uniform interface for federated access • Access to back end nodes: steering, visualisation • Lightpath network connections • Cross site simulations (MPIg) • Support for software (ReG steering toolkit etc)

These requirements impact resource provider policies
• TeraGrid, NGS & HPCx starting to support advanced reservation with HARC
• DEISA evaluating HARC deployment on their systems
• Some TeraGrid sites support emergency jobs with SPRUCE
• Lightpath connections in place between Manchester - Oxford NGS nodes and Manchester - UCL
• MPIg and RealityGrid steering deployed on NGS and TeraGrid resources

HIV-1 Protease is a common target for HIV drug therapy
• Enzyme of HIV responsible for protein maturation
• Target for Anti-retroviral Inhibitors • Example of Structure Assisted Drug
Design • 9 FDA inhibitors of HIV-1 protease
So what’s the problem? • Emergence of drug resistant
mutations in protease • Render drug ineffective • Drug resistant mutants have emerged for all FDA inhibitors
Monomer B 101 - 199
Monomer A 1 - 99
Flaps
Leucine - 90, 190
Glycine - 48, 148
Catalytic Aspartic Acids - 25, 125
Saquinavir
P2 Subsite
N-terminal C-terminal
CCS -HIV drug design/drug treatment

CCS - Determination of protein-drug binding affinities
Simulation and calculation workflow
Applications used include: NAMD, CHARMM, AMBER… Thermodynamic decomposition
• explains the distortions in enthalpy/entropy balance caused by the L90M and G48V mutations
• absolute drug binding energies are in excellent agreement (1 – 1.5kcal/mol) with experimental values
Binding of saquinavir to wildtype and resistant HIV-1 proteases L90M and G48V/L90M
Rapid and accurate prediction of binding free energies for saquinavir-bound HIV-1 proteases. Stoica I, Sadiq SK, Coveney PV. J Am Chem Soc. 2008 Feb 27;130(8):2639-48. Epub 2008 Jan 29.
Doable in days

• Eventual aim is to provide tools that allow simulations to be used in a clinical context
• Require large number of simulations to be constructed and run automatically – To investigate generalisation – Automation is critical for clinical use
• Turn-around time scale of around a week is required • Trade off between accuracy and simulation turn around time
Binding Affinity Calculator (BAC)
A distributed automated high throughput binding affinity calculator for HIV-1 proteases with relevant drugs
Automation of binding affinity calculation
“Automated molecular simulation based binding affinity calculator for ligand-bound HIV-1 proteases”. Sadiq SK, Wright D, Watson SJ, Zasada SJ, Stoica I, Coveney PV. J Chem Inf Model. 2008 48(9):1909-19.

The GENIUS project aims to model large scale patient specific cerebral blood flow in clinically relevant time frames
Objectives:
• To study cerebral blood flow using patient-specific image-based models. • To provide insights into the cerebral blood flow & anomalies.
• To develop tools and policies by means of which users can better exploit
the ability to reserve and co-reserve HPC resources. • To develop interfaces which permit users to easily deploy and monitor
simulations across multiple computational resources. • To visualize and steer the results of distributed simulations in real time Yields patient-specific information which helps plan embolisation of arterio-venous malformations, aneurysms, etc.
Grid enabled neurosurgical imaging using simulation

Arterio-venous malformations (AVM) Example neuropathology

Modelling vascular blood flow - HemeLB
Efficient fluid solver for modelling brain bloodflow
• Uses the lattice-Boltzmann method
• Efficient algorithm for sparse geometries
• Machine-topology aware graph growing partitioning technique, to help minimise the issue of cross-site latencies
• Optimized inter- and intra-machine communications
• Full checkpoint capabilities.
M. D. Mazzeo and P. V. Coveney, "HemeLB: A high performance parallel lattice-Boltzmann code for large scale fluid flow in complex geometries", Computer Physics Communications, 178, (12), 894-914, (2008).

38
CCS - Haemodynamic simulation and visualisation
• First step is the conversion of MRA or 3DRA data (DICOM format) to a 3D model, vasculature is of high contrast, 200 - 400 µm resolution, 5003 - 10003 voxels
• 3DRA - 3-dimensional rotational angiography, vasculature is obtained using digital subtraction imaging with a high-contrast x-ray absorbing fluid.
• Each voxel is a solid (vascular wall), fluid, fluid next to a wall, a fluid inlet or a fluid outlet • Arterial simulations typically have 1-3 inlets and ~50 outlets, • We apply oscillating pressures at inlet and oscillating or constant one at the outlets, for
example. • Real-time in-situ visualisation of the data using streamlines, iso-surfacing or volume
rendering (stress, velocity or pressure). • New insights into physiology of human brain
HemeLB
Velocity field obtained with our ray tracer
Reconstruction and boundary condition set-up; fluid sites, inlet and outlet sites in
red, black and green respectively;

39
Book computing resources in advance or have a system by which simulations can be run urgently.
Move imaging data around quickly over high-bandwidth low-latency dedicated links.
Interactive simulations and real-time visualization for immediate feedback.
15-20 minute turnaround
Translational Impact

UCL-Yale Computational Biomedicine collaboration
• Aims: Pool the computational, information management and analysis resources of two of the world’s greatest universities and their associated hospitals: – Yale University Hospital – UCL Partners (Great Ormond Street, Moorfields Eye Hospital, Royal Free
Hospital and UCL Hospitals Trust).
• break-through science and speed up its translation to better medicine.
• Far-reaching transformative consequences for UK and US science, medicine and industry.
Yale – UCL Collaboration

Yale – UCL Collaboration
• Overview of Yale- UCL Collaboration
• World Ranking Yale 3, UCL 4. • Framework Agreement signed 8 Oct 2009 by Malcolm
Grant & the President of Yale Richard Levin & leaders of associated hospitals
• Joint resources committed to research & education with aims: – Enhance scope & quality of research both basic & clinical – Attract the best students to a joint PhD programme – Drive translation within the Collaboration – Lead improvement in patient care

Yale – UCL Collaboration
Governance
• Joint Strategy Committee
• Scientific Advisory Board
• Strategic Advisory Board

Yale – UCL Collaboration
Achievements (first 12 months)
Bottom up approach Basic research: 10 joint projects started Clinical research: 2 UCL research clinics started in Yale
Hospital, 1 Yale clinic in UCLP. (1st NIH grant $4.7m). Bioinformatics: “The Coveney Plan” Drug Discovery: 3 projects (1 patent) First into Man: First project completed Hospitals: Exchange of managers

Future
• Enthusiasm across Biomedicine & Life Sciences • Establish translation with Collaborative • Joint fund raising • Split PhD starts September 2011 • Joint Hospital Management Institute • Governance running
Yale – UCL Collaboration

UK, EU and Global Benefits of the Collaboration • Major contribution to UK Digital Economy - positioning the UK at the centre of globally
integrated healthcare data management
• Strengthening UK expertise in information management – Expanding market, skills and employment opportunities in information management
• New paradigm will transform healthcare in the UK – Improving health and well being of UK citizens through better patient data management – Bespoke treatments and specific drugs for the patient using digital information and clinical expertise – Will help contain health costs and improve patient wellbeing
• Develop and invest in these future technologies now – No unified management of & funding mechanisms for data, network and computing – Current funding is fragmented - networks (JISC), computing (EPSRC, STFC) and data (BBSRC) – Investment case in point: EBI was placed in the UK owing to superior networking technology which was
invested in ahead of time – UK HPC likely to be embedded within EU via DEISA/PRACE – UCL is in an excellent position with strong links to EBI, NIH, Sanger, Wellcome, MRC & BBSRC
(including planned Digital Organism programme)
Yale – UCL Collaboration

UCL-Yale integrated technological platform • Current and future biomedical research that the UCL-Yale
Collaboration will tackle all share the common themes of being compute- and data-intensive – The effective integration of distributed data, computing and networks is central
to success
• Data: Standards, transparency, security and ethics • Computing: Access to high-performance computational resources in
UK, EU and USA • Networks: Establishment of persistent high-bandwidth, high QoS
connections between: – Data producers (e.g. Sanger, EBI, …) – Researchers (UCL, Yale) – Clinicians (UCLP, Yale Hospital) – Compute resources (DEISA, TeraGrid e.g.), initially at 10Gbs, rising to 100Gb/s
and to 1Tb/s by 2020
Yale – UCL Collaboration

Transatlantic 10Gb link TeraGrid 40Gb backbone
DEISA 10Gb network
JA.NET (UK) 40Gb network

UCL-Yale Collaboration in Biomedicine
• The Collaboration has already established joint projects which are totally integrated
• Cardiovascular science is the first discipline to have been integrated over the last year
• First joint grant was awarded from the NIH in September 2009 (genetics of congenital heart disease)
• Women’s health, cancer, neuroscience and surgery will be integrated during 2010
Yale – UCL Collaboration

UCL-Yale Collaboration in Biomedicine: Examples
• Cardiovascular clinical genetics - whole genome high throughput analysis at Yale is being applied to UCL patient databases.
• Cardiovascular imaging – Combined power of multiple imaging modalities available within the Collaboration, for patients, volunteers and large and small animals, is world-leading.
• Cardiovascular research clinics – UCL staff have established clinics for congenital heart disease and familial sudden
death at Yale – Yale staff have established a program for treatment for chronic total occlusion of
coronary arteries within UCLP.
Yale – UCL Collaboration

What role will integration play in medicine?
• Up to 1990: anecdote-based medicine (based on personal experience of the physician)
• 1990-2010: evidence-based medicine (based on consensus treatment protocols derived from population studies)
• 2020: truly personalised medicine, based on models derived from individual patient profiles (genotypes and phenotypes)
• Making decisions from these rich data will require huge amounts of computation, as well as integration of network, computing, and data resources – globally.
Digital Me

A vision of future healthcare • Personalised, Predictive, Integrative... • An integrated anatomical, physiological, biochemical,
genotypical model of me • Integrates my health “chronicle” with models derived from
populations with similar phenotypes • Lets me understand and take control of my own life and health –
“$2000 genome” in 3-5 years? • Used for:
– Patient education • “what is happening to me?” • “what are you going to do to me?”
– Management of chronic diseases – Clinical decision support
Digital Me

Population Information
Personal Information
52
Predictive Models
Epidemi-ology
Therapy outcomes
Lifestyle
Clinical
Genotypes
Visualisations
Devices
Sensors
Genotype
Digital Me
Many of the individual components of this figure already exist and work, however they need to
be integrated
Digital Me

Between now and 2020 What developments will make Digital Me possible?
• Desk-side supercomputing with 1,000s or even 1,000,000s of cores willprovide the necessary power to run patient specific simulations at low cost
• Distributed, ‘grid’, ‘cloud’ or ‘utility’ computing could make the computational power required for large scale simulations available transparently, and integrated in to the clinical workflow
• Computational models could be routinely constructed and stored with a patient’s EHR (electronic health records) to use when needed – A radical evolution of healthcare – Encourages individual’s responsibility for own health management of chronic
diseases – Reduction of need to access central resources
Digital Me